“Conoscere il risultato a lungo termine dopo ablazione FA...
39
“Conoscere il risultato a lungo termine dopo ablazione della FA è pre‐requisito per indicazioni appropriate” Prof. Fiorenzo Gaita ‐ Università di Torino, Dipartimento di Cardiologia Asti Key points: • 1‐What does it mean efficacy for AF ablation at the present today? • 2‐Which are the long‐term results of AF ablation? • 3‐Which are the predictors of long‐term failure of AF ablation?
Transcript of “Conoscere il risultato a lungo termine dopo ablazione FA...

“Conoscere il risultato a lungo termine dopo ablazione della FA è pre‐requisito per indicazioni appropriate”
Prof. Fiorenzo Gaita ‐ Università di Torino, Dipartimento di Cardiologia Asti
Key points:• 1‐What does it mean efficacy for AF ablation at the present today?• 2‐Which are the long‐term results of AF ablation?• 3‐Which are the predictors of long‐term failure of AF ablation?
Atrial Fibrilation
CMP?
valvularidiopathic
vagal
focal
SSS adrenergic
pericarditis
conduction delay

Disorganized atrial electrical activuty in only one region of the atria
F. Gaita et al. JACC 2001;37:534
Paroxysmal AF Persistent AF
Disorganized atrial electrical activity in more than one region of the atria
Long-lasting and Permanent AF
Disorganized atrial electrical activity in all the regions of the atria
Clinical Classification and substrate of AF

Different AF ablation methods

Tsai Circulation 1999; Jais Circulation 2000; Schreieck J Cardiovasc Electrophy 2002
RF ablation catheter
4 mm 4 mm 8 mm
RF ablation cooled catheter
RF ablation catheter

Evolution of AF catheter ablation strategy over the years (Oct. 1994 /Nov. 2009) = 2052 pts
11%
35%
0
20
40
60
80
100
Paroxysmal
1994–97RA Lines
Pts = 35
Complications =
0%
1998“Culprit” PV
17%
9%
0
20
40
60
80
100
Paroxysmal
Pts = 25
Complications =
13,0%
1999-2001All PV + Carto
0
20
40
60
80
100
Paroxysmal
58%
23%
Pts = 245
36%
24%
Pers
/Perm
Complications =
1,4%
2002-2005PV + 7 lines +RM
+Carto
0
20
40
60
80
100
Paroxysmal
78%
10%
Pts = 746
55%
24%
Pers/
Perm
Complications =
0,7%
2006-07PV + 7 lines
+Merge
0
20
40
60
80
100
Paroxysmal
82%
8%
Pts = 500
Complications =
0,6%
65%
21%
Pers/
Perm
Success w/o drugsSuccess with drugs
2008-09PV + 7 lines
+Merge
0
20
40
60
80
100
Parossistica
85%
6%
Pts = 501
Complications =
0,5%
74%
18%
Pers/
Perm
Procedure duration
6 h.
Procedure duration2,30 h.
Procedureduration
4 h.
Procedureduration4,30 h.
Procedureduration2,00 h.
Procedureduration2,00 h.
RX: 88’ RX: 94’ RX: 62’ RX: 44’ RX: 15’ RX: 8’
F-up:
1 year
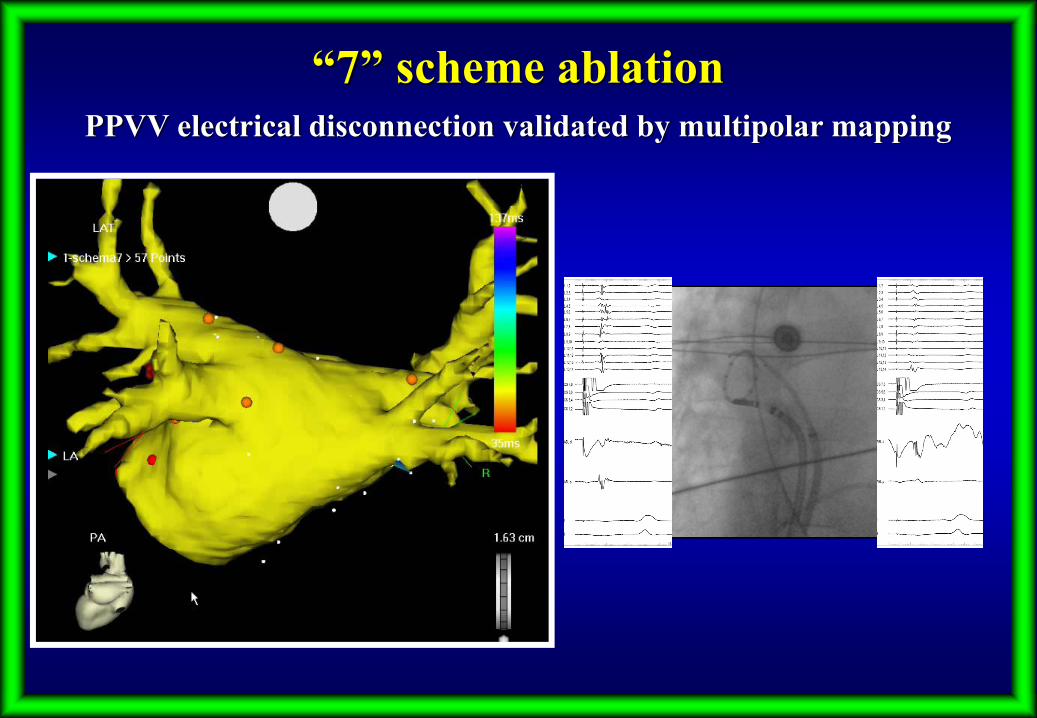
“7” scheme ablationPPVV electrical disconnection validated by multipolar mapping

Three ablation options: a) Isolation of PVb) Isolation of other thoracic veins (SVC and CS)c) Ablation of fractionated atrial potentials
Haissaguerre et al. JCE 2005: 16; 1125-1137
Multifaceted approach in persistent long-lasting AF60 pts with long-lasting persistent AF (Mean duration of AF 17±27 months)
F-up: 11±6 monthsSuccess rate:SR w/out drugs: 53/60 (89%)SR with drugs: 57/60 (95%)
Success outcome: absence of all documented arrhythmia beyond the 2nd month after ablation
Complications: 1 cardiac tamponade
2 right phrenic nerve damage
1st STEP:randomization of one of the three options
2nd STEP:1° step +
randomization of the two remaining options
AF termiantion?
AF termiantion?
no
3rd STEP:adding of the
last option
no
4th STEP:adding Linear left atrial ablation
STOP
yesyes
AF termiantion?
yesno23pts (38%) required a
second procedure and 4
(7%) pts required a third
procedure
20
17
12
3
0
5
10
15
20
25
1 2 3 4
Cumulative incidence of AF termination
5% 25% 53% 87%

1• WHAT DOES IT MEAN EFFICACY FOR AF ABLATION
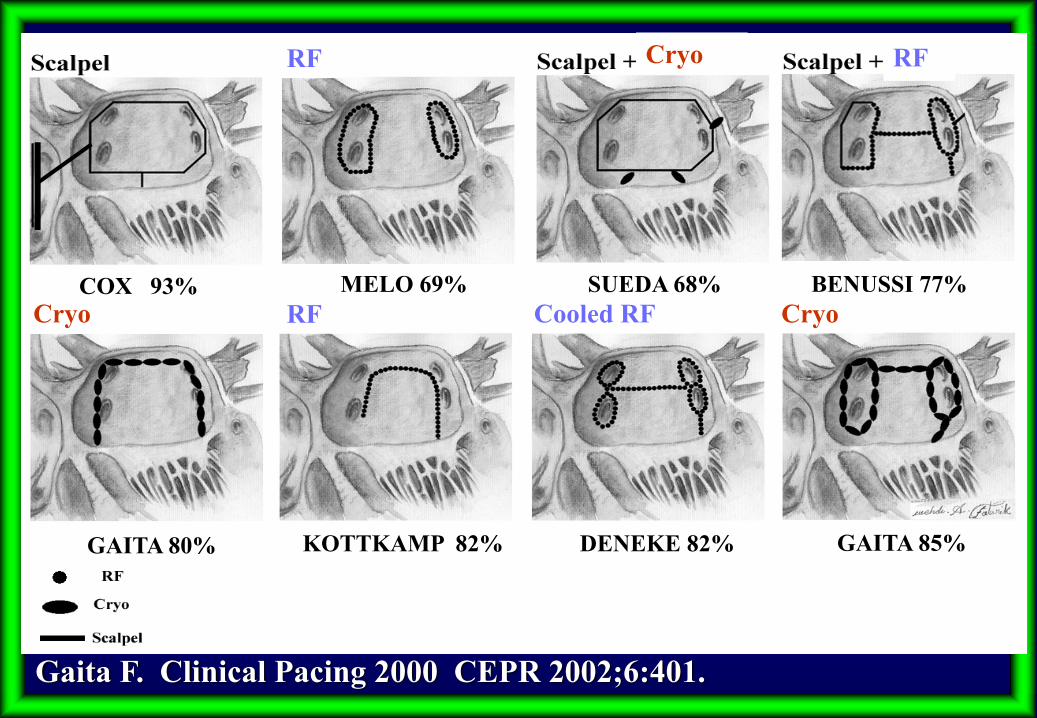
Gaita F. Clinical Pacing 2000 CEPR 2002;6:401.
BENUSSI 77%
RF
RF Cooled RF
RF
Cryo Cryo
Cryo
COX 93%
DENEKE 82%
MELO 69% SUEDA 68%
GAITA 80% KOTTKAMP 82% GAITA 85%

Surgical cryoablation: results with drugsPt
s in
SR w
ith d
rugs
U 7
PV
105 pts (3 groups of 35 pts)
Chronic AF and Valvular Heart Disease
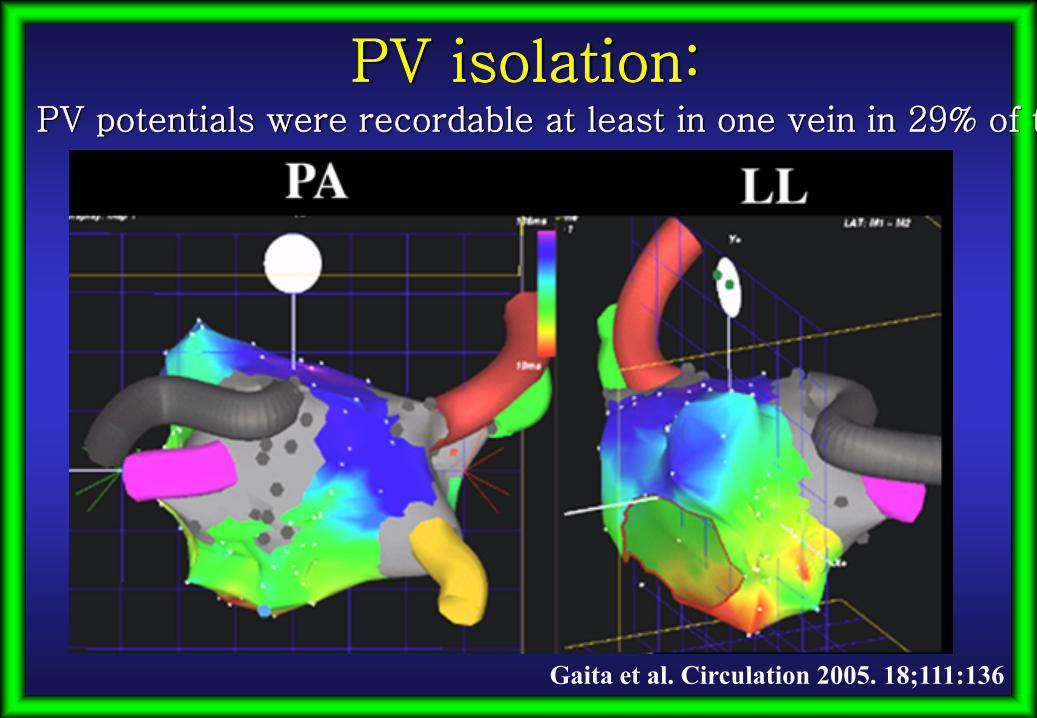
Gaita et al. Circulation 2005:18;111:136
PV
Weeks

Sinus rhythm
Gaita et al. Circulation 2005. 18;111:136
…without knowing if the intended surgical lines were obtained
without drugs
20%
57%
with drugs
59%
90%

Missingsegment
Gaita et al. Circulation 2005. 18;111:136
The line between RIPV-MA was missing in
all the pts with “U” lesion; 41% of them also showed other patterns of incomplete
“7” lesion

Gaita et al. Circulation 2005. 18;111:136
In 35% of the pts with “7” lesion, the surgically intended lesion was not
achieved
Gaita et al. Circulation 2005. 18;111:136
PV isolation:PV potentials were recordable at least in one vein in 29% of t

Pts i
n SR
with
out d
rugs
U7
PV
Chronic AF and Valvular Heart Disease
Gaita et al. Circulation 2005. 18;111:136
PV
Surgical cryoablation: results without drugs and with proof of complete lesions

PV isolation + LA linear lesionsPV Isolation Fractionated
electrograms
7182
67 7469
83 83
78
87
83
0
20
40
60
80
100
Gaita 2004
Nademanee 2004
Pappone 2001
Oral 2003
Haissaguerree 2004
Oral 2003
Haissaguerre 2000
90 pts 179 pts 40 pts 35 pts
Haissaguerre 2004
40 pts 35 pts 84 pts
Hocini 2005
Hocini 2005
45 pts 45 pts
%
73%
Mean
389 pts
83%
57 pts
F-up: 36mos
82%
Mean
204 pts
PAROXYSMAL AF: efficacy at 1 year of transcatheter ablation (without drugs)

48
22
37
68 71 74 76
0
20
40
60
80
100
PV isolation + LA linear lesions
Gaita 2004
Nademanee 2004
Pappone 2001
PV Isolation
Oral 2002
Haissaguerree 2004
Fractionated electrograms
Oral 2006
72 pts 12 pts 58 pts 77 pts135 pts
Wei Lim 2006
51 pts
%
36%
Mean
135 pts
Mean
71%
270 pts
76%
60 pts
PERS/PERM AF: efficacy at 1 year of transcatheter ablation (without drugs)
2•LONG-TERM EFFICACY

Katritsis Europace 08
PVI (segmental ablation Lasso)*Antral ablation (Lasso + ICE)*Circumferential ablation (Carto)* more effective
Last procedure65% 2 or more
procedures
93% at 1y
21% at 2y
73% at 1y
35% at 2y
Long-term follow-up after PV segmental ablation for paroxysmal atrial fibrillation (39 pts)
I procedure

Transcatheter ablation of Paroxysmal AFPVI vs PVI + linear lesions
PVI + linear lesions
PVI
Gaita et al. CIRCULATION Arrhythmia Electrophysiol. 2008;1:269-275
Maintenance of SR during 36 months:
PVI + linear lesions
PVI
After one procedure After redo procedure
53%
29%
62%
85%

Transcatheter ablation of Persistent/Permanent AF PVI vs PVI + linear lesions
PVI + linear lesions
PVI
Gaita et al. CIRCULATION Arrhythmia Electrophysiol. 2008;1:269-275
Maintenance of SR during 36 months:
PVI + linear lesions
PVI
After one procedure After redo procedure
41%
75%
39%19%

3•PREDICTOR OF LONG-TERM FAILURE

Univariate analysisVariables Postablation AT Successes Unajusted OR P value
(95% CI)Age (years) 57,88 ± 11,25 58,57 ± 9,96 0,99 (0,96-1,03) 0,702Gender [n (%)]
F 8 (16%) 13 (13%)M 42 (84%) 86 (87%) 0,79 (0,31-2,06) 0,635
BMI (kg/m2) 27,52 ± 2,11 24,34 ± 2,13 2,11 (1,63-2,73) <0,001AF type [n (%)]
Paroxysmal 24 (48%) 84 (85%)Persistent 26 (52%) 15 (15%) 7,35 (3,05-17,7) <0,001
AF age of onset (years) 49,62 ± 10,64 51,2 ± 10,09 0,99 (0,95-1,02) 0,374AF duration (years) 68 ± 55,35 59,03 ± 42,78 1 (1-1,01) 0,277Previous cardioversions (CV/pts) 1,58 ± 1,72 0,88 ± 1,37 1,34 (1,07-1,68) 0,010Hypertension [n (%)] 22 (44%) 35 (35%) 1,44 (0,72-2,88) 0,306Structural heart disease [n (%)] 15 (30%) 10 (10,1%)
Dilated cardiomyopathy 2 (4%) 2 (2%) 1 (0,03-29,81) 1,000Hypertrophic cardiomyopathy 7 (14%) 5 (5%) 1,4 (0,07-28,12) 0,826
Valvular heart disease 5 (10%) 2 (2%) 2,5 (0,1-62,6) 0,577Congenital heart disease 1 (2%) 1 (1%)
Left atrial volume (ml) 209,82 ± 37,61 122,07 ± 32,01 1,1 (1,06-1,14) <0,001Right anatomical variants [n (%)] 26 (52%) 13 (13%) 7,17 (3,2-16,03) <0,001Left anatomical variants [n (%)] 16 (32%) 13 (13%) 3,11 (1,35-7,16) 0,008Dysthyroidism [n (%)] 13 (26%) 16 (16%) 1,82 (0,8-4,17) 0,155Fluoroscopy time (min) 53,82 ± 26,28 47,91 ± 24,2 1,01 (1-1,02) 0,175Rhythm at the beginning of the procedure [n (%)]
SR 29 (58%) 69 (70%) 0,6 (0,3-1,22) 0,157AF 21 (42%) 30 (30%)
Continuous variables are given as mean ± SD.CI = confidence interval; OR = odds ratio. In Press JCM 2010
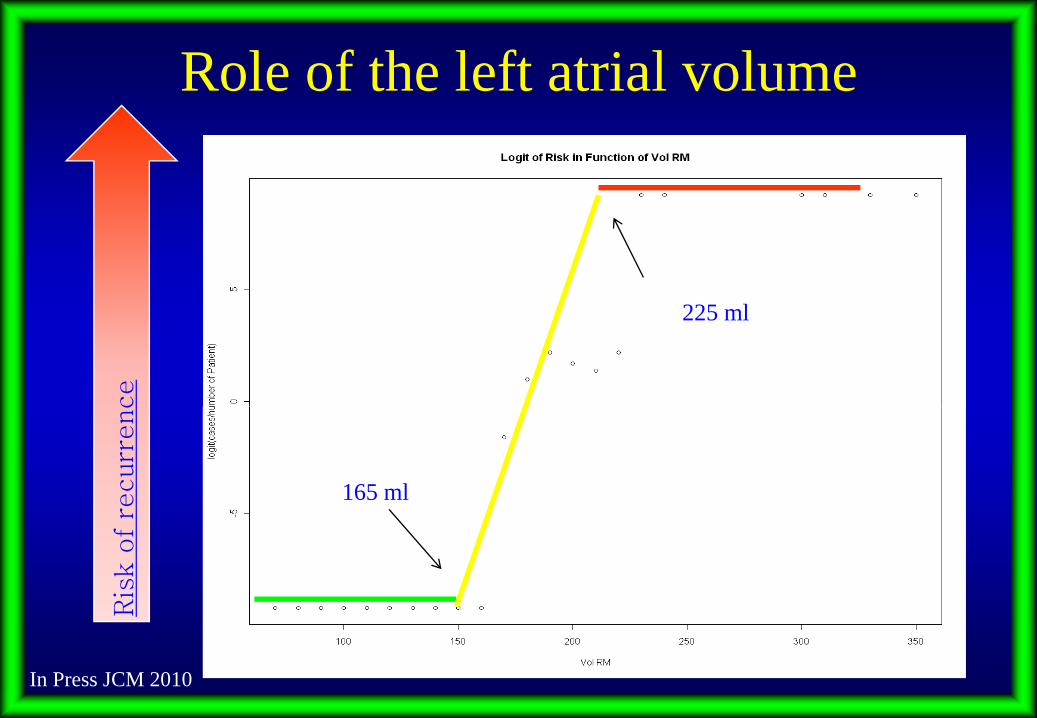
Role of the left atrial volumeR
isk
of
recurr
ence
165 ml
225 ml
In Press JCM 2010

Pre-procedural predictors of atrial fibrillation recurrence after circumferential pulmonary vein
ablation
Berruezo A. et al. European Heart J (2007) 28, 836-841
148 pts, Paroxysmal AF 60%,M 82%, mean age 52±11,
Hypertension 33%,
Multivariable analysis:indipendent predictors of AF recurrence
after ablation procedure
Linear relationship with the increase LAD and AF
recurrences.
Hypertension increase the mean predicted proportion of pts with AF
recurrences at each LAD

Long-term efficacy for Segmental Pulmonary Vein Isolationin pts with Paroxysmal Atrial Fibrillation
Sawhney N et al.Am J Cardiol 2009;104:366-372
86% at 1 y79% at 2 y
56% > 5 y
LONG-TERM EFFICACY AFTER ONEPROCEDURE OFF ANTIARRHYTHMIC DRUGS
71 Pts with paroxysmal AF who uderwent PVI; 31 pts (44%) underwent ≥ 1 repeat ablations.
After multiple procedures 58 pts (81%)were free of symptomatic AF off antiarrhythmic drugs at 63± 5 months after their initial ablation
Age 60±9, M 77%, Hypertension 37%, Structural Heart dis. 10%, CHADS2 score 0.5, Duration of AF (y) 4.5±1.2

Sawhney N et al.Am J Cardiol 2009;104:366-372
Five-Years Outcomes After Segmental Pulmonary Vein Isolation for Paroxysmal Atrial Fibrillation
RISK FACTOR DEVELOPING RECURRENT ATRIAL FIBRILLATION
HYPERTENSION WAS AN INDIPENDENT PREDICTOR OF AF
RECURRENCE
NO HYPERTENSION
HYPERTENSION

Bertaglia E et al. Europace 2009
229 pts, drug refractory AF 177 (78%) free from any arrhythmia during a 12 months FU
CLINICAL CHARACTERISTIC LONG-TERM EFFICACY
55% at 6 y
87% at 2 y
65% at 4 y
Circumferential PV ablation
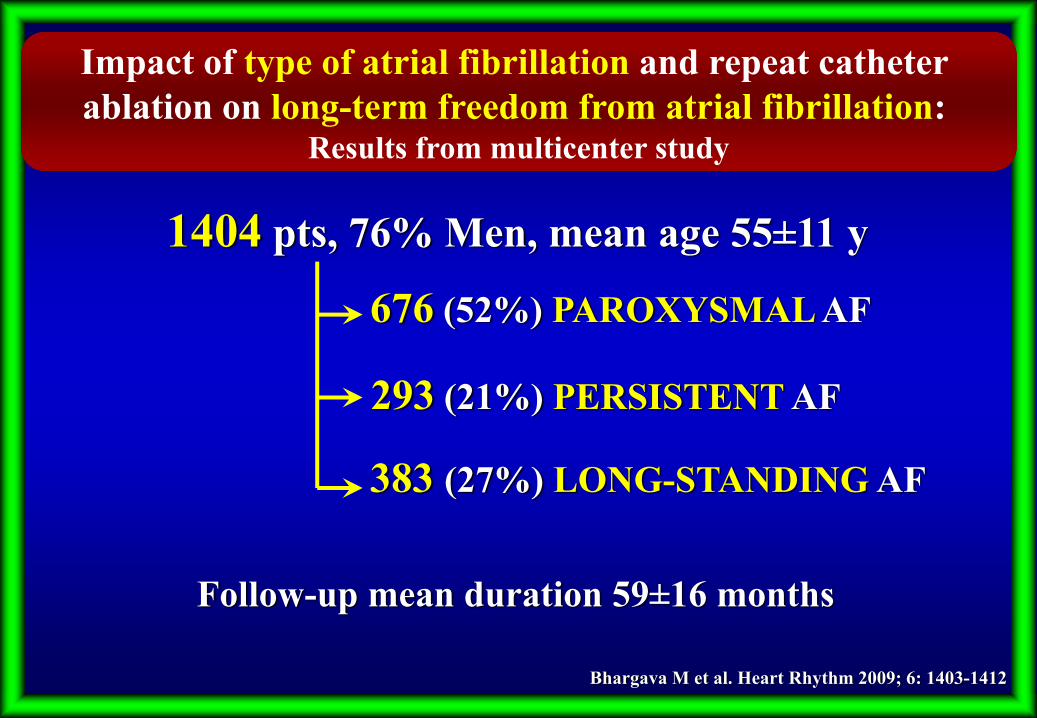
Impact of type of atrial fibrillation and repeat catheter ablation on long-term freedom from atrial fibrillation:
Results from multicenter study
Bhargava M et al. Heart Rhythm 2009; 6: 1403-1412
383 (27%) LONG-STANDING AF
1404 pts, 76% Men, mean age 55±11 y
676 (52%) PAROXYSMAL AF
293 (21%) PERSISTENT AF
Follow-up mean duration 59±16 months

Bhargava M et al. Heart Rhythm 2009; 6: 1403-1412
AFTER REDO ABLATION
Freedom from AF/AT:-PAF 89%
-PERSISTENT 71%-LONG-STANDING 68%
Impact of type of atrial fibrillation and repeat catheter ablation on long-term freedom from atrial fibrillation:
Results from multicenter study

153 pts, age 56±10, M 85%, Long-lasting persistent AF 54%Mean duration sustained AF 21.8 ±33 months
23 pts (15%) non-termination130 pts (85%) procedural termination (108 via intermediate AT- 22 DC to SR)
64/130 (49%) pts repeat Procedures (6 AF and 58 AT)
15/23 (65%) pts repeatprocedures (9 AF and 7 AT)
Median Follow up 34 months
Long-term Follow-up of persistent atrial fibrillation ablation using termination as a procedural endpoint
O’Neill M., Haissaguerre M et al European Heart Jourtnal (2009) 30,1105-1112

O’Neill M. Haissaguerre M. et al European Heart Journal (2009) 30:1105-1112
124/130 (95%)
12/23 (52%)
ATRIAL FIBRILLATION TERMINATION AND LONG-TERM FOLLOW UP (34 months)
AFTER ONE PROCEDURE
79/153 (52%) pts uderwentrepeat procedures
8/23 (35%)
66/130 (51%)
AFTER THE LAST PROCEDURE

O’Neill M. et al European Heart Journal (2009) 30:1105-1112
90%
54%50%
100%
Long-term Follow-up of persistent atrial fibrillation ablation using termination as a procedural endpoint
Duration of persistent AFprior to the ablation procedure
AF cycle lenght measured in the left atrial appendage
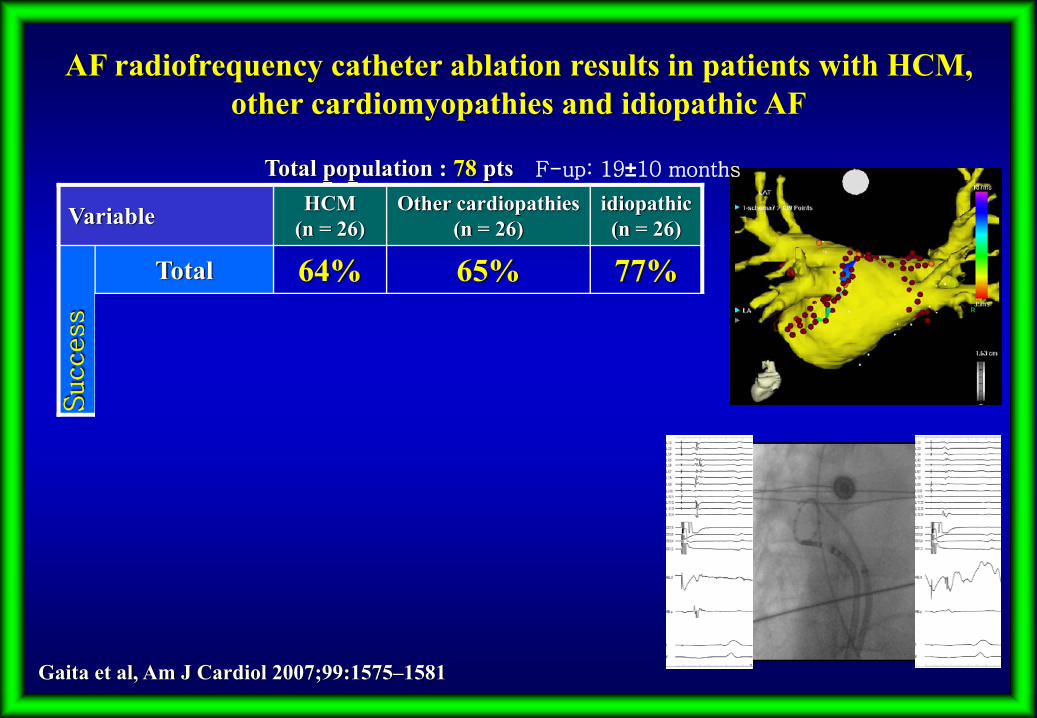
Variable HCM(n = 26)
Other cardiopathies(n = 26)
idiopathic (n = 26)
Total 64% 65% 77%PAF 77% 77% 85%FA
Perst/Perm 50% 54% 69%
Success
Total population : 78 pts
AF radiofrequency catheter ablation results in patients with HCM, other cardiomyopathies and idiopathic AF
Gaita et al, Am J Cardiol 2007;99:1575–1581
F-up: 19±10 months

24/41 pts (59%) with redo procedure
PAF 25 (71%) - Pers/Perm 16 (61%)
Mean F-up34±16
months
Final success rate41/61 pts (67%)
Cardiology Department – Asti , Florence and Bordeaux
32/61 total pts (52%) with redo
procedure
Major complications: none
Long term f-up results in patients with HCM and AF RFCA

0
10
20
30
40
50
60
70
I I I I I I
NYHA Functional Class
p=0.02
RFC
A Fa
ilure
(%)
0
10
20
30
40
50
60
Parox Persist Perm
p=0.44
Type of AF
RFC
A Fa
ilure
(%)
0
10
20
30
40
50
60
70
<130 130-150 >150
p<0.001
Left Atrial Volume (ml)
RFC
A Fa
ilure
(%)
Predictors of outcome
In Press Europace 2010

•In a long term follow-up the “PVI + linear
lesions” scheme is significantly more
effective than the “PVI alone” , but often
multiple ablation sessions are required
•Absence of recurrences at 12 month follow up
can not be considered permanent success sinceAF recurrences are possible in the long-termespecially utilizing the “PVI” ablation scheme.
CONCLUSIONS

Duration of continuous AF
FAILURE SUCCESS
Increased Left Atrial Size
CONCLUSIONS