Cattaneo le urgenze in ematologia 21 maggio 2011
52
Farmaci antiaggreganti Marco Cattaneo Clinica Medica Ospedale San Paolo – Università degli Studi di Milano
-
Upload
cmid -
Category
Health & Medicine
-
view
1.107 -
download
1
description
Transcript of Cattaneo le urgenze in ematologia 21 maggio 2011

Farmaci antiaggreganti
Marco Cattaneo
Clinica MedicaOspedale San Paolo – Università degli Studi di Milano
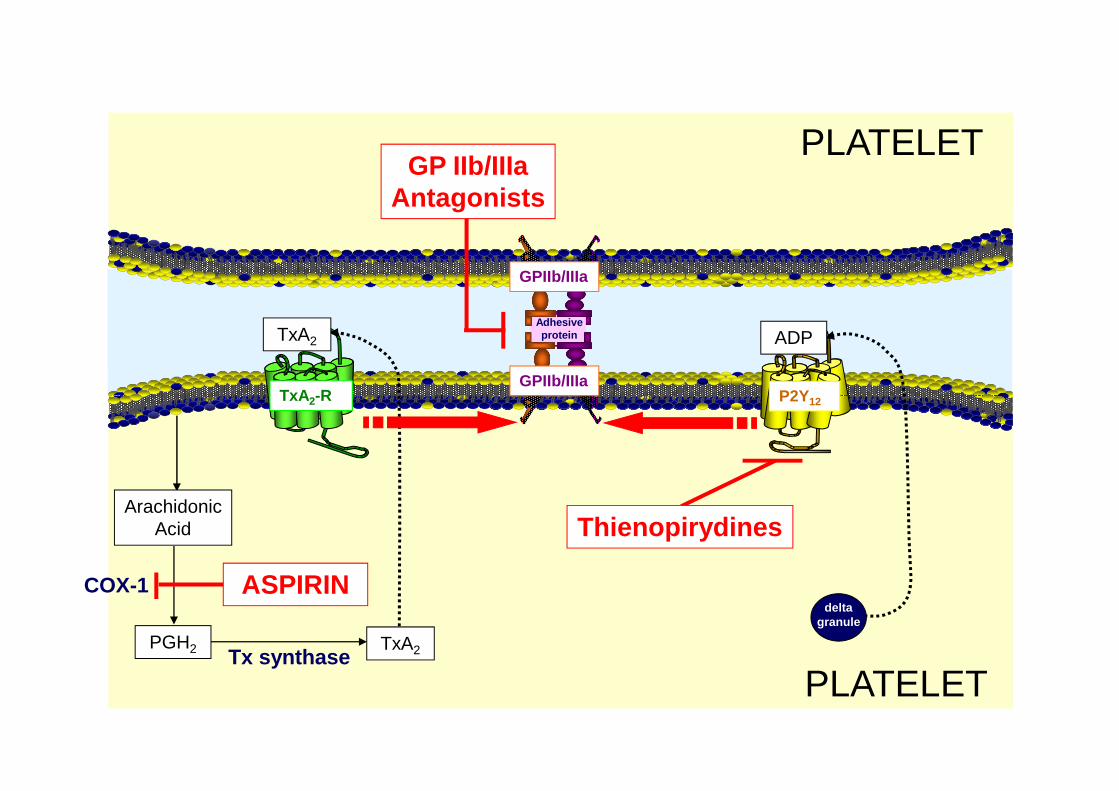
P2Y12TxA2-R
TxA2 ADP
GPIIb/IIIa
GPIIb/IIIa
PLATELET
Adhesiveprotein
GP IIb/IIIaAntagonists
P2Y12TxA2-R
PGH2
ArachidonicAcid
COX-1
Tx synthase
ASPIRIN
TxA2
Thienopirydines
PLATELET
deltagranule
Characteristics of the ideal antithrombotic agent
•Potent antithrombotic effect•Low risk•Predictable pharmakodynamic profile, making monitoring unnecessary•Rapid onset•Rapid onset•Rapid offset*•Availability of an antidote•No interaction with food or adjunctive medicines commonly used•Low cost* For safety reasons, a drug with rapid offset is generally preferable to a drug with long-lasting effects, although the use of the latter might minimize the negative effects of poor compliance.
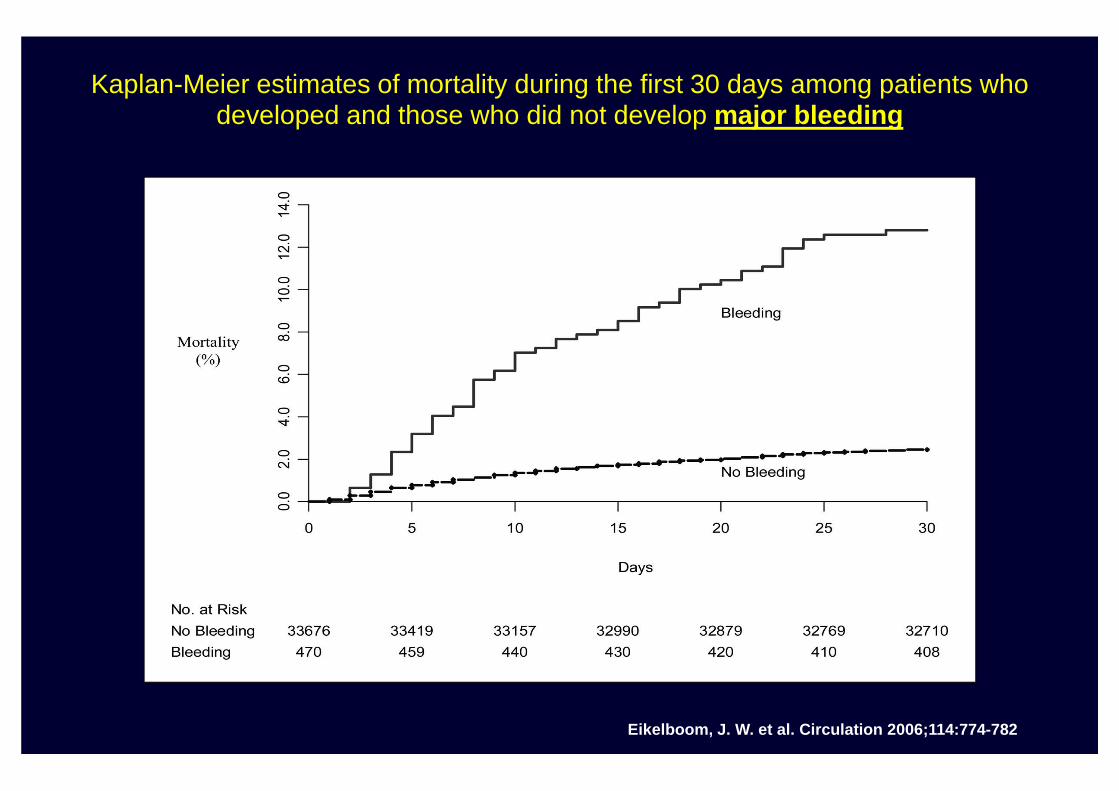
Kaplan-Meier estimates of mortality during the first 30 days among patients who developed and those who did not develop major bleeding
Eikelboom, J. W. et al. Circulation 2006;114:774-782
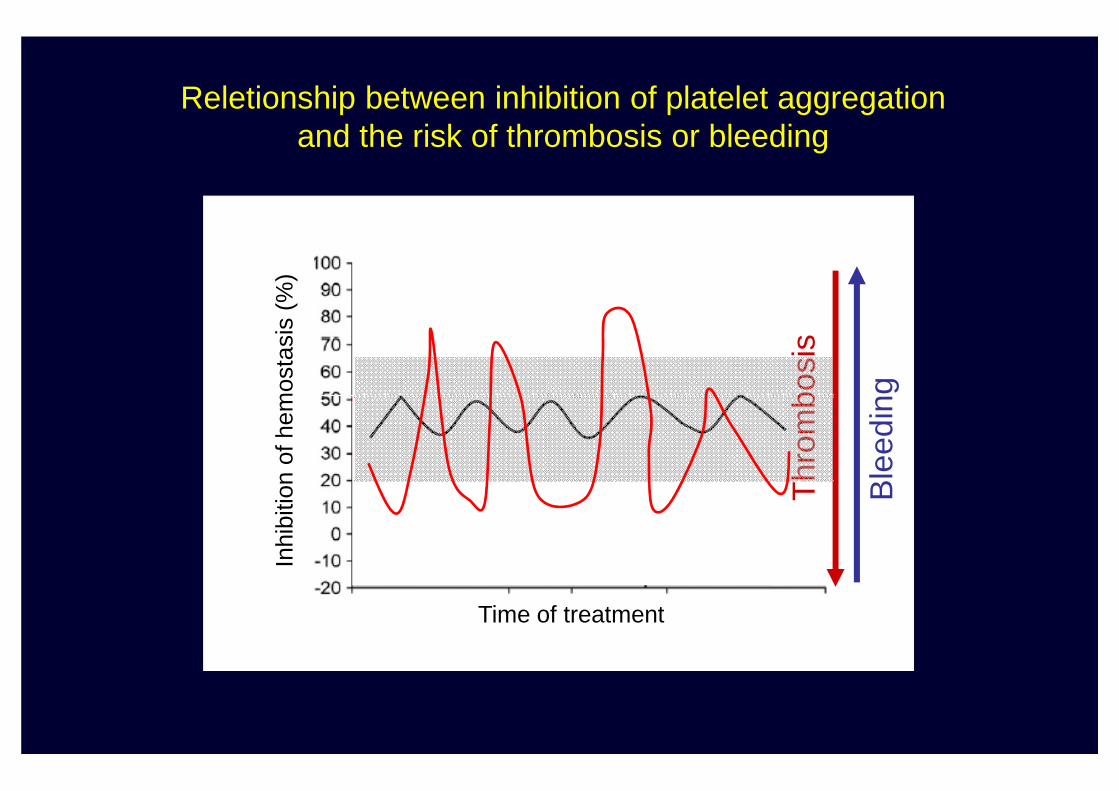
“Responders”
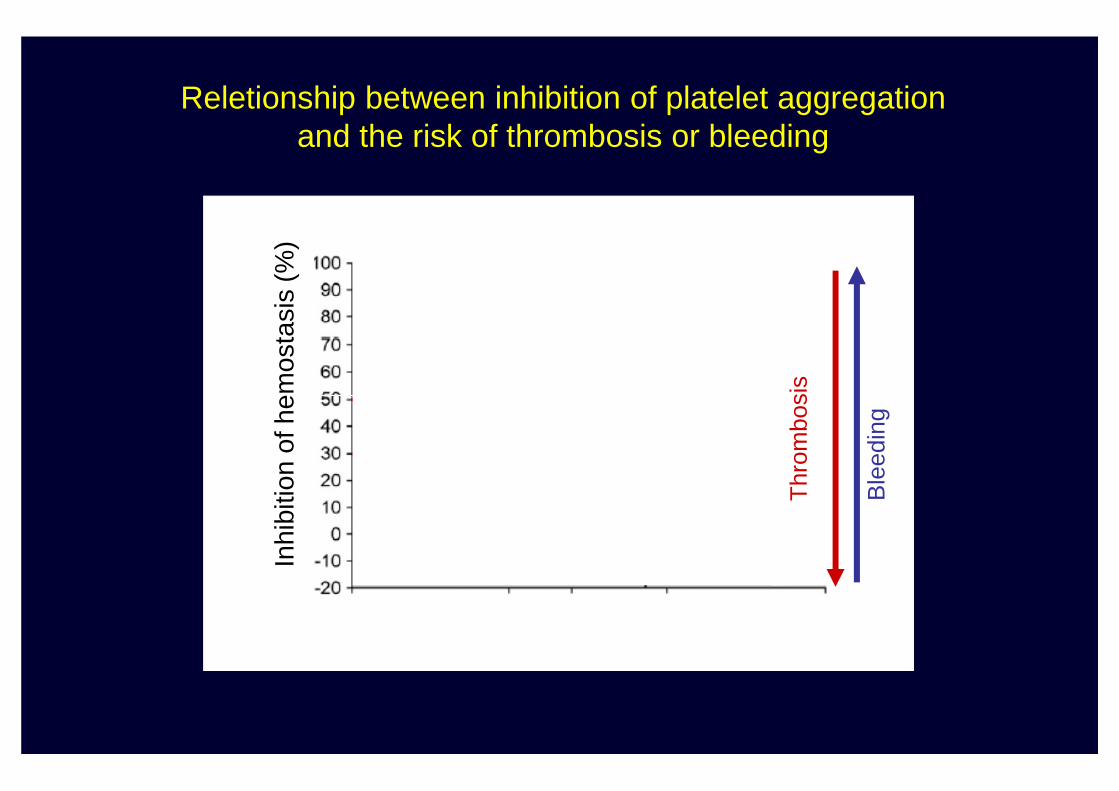
Thr
ombo
sis
Inhi
bitio
n of
hem
osta
sis
(%)
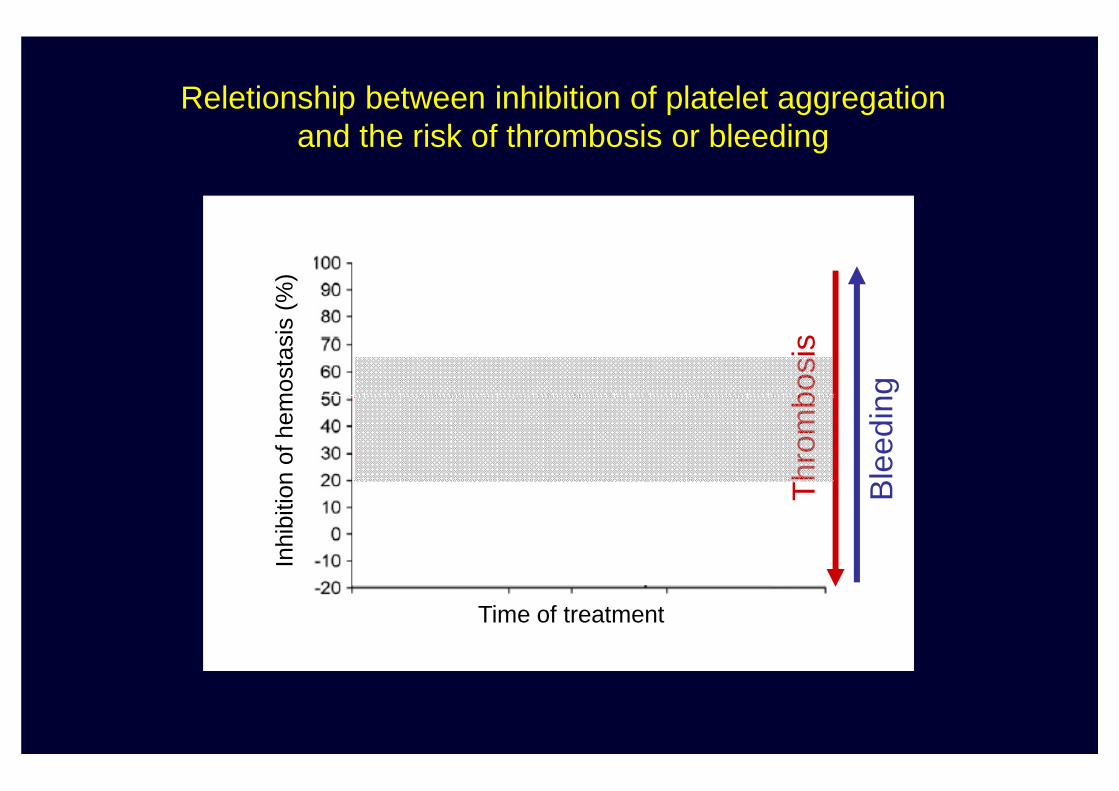
Reletionship between inhibition of platelet aggregationand the risk of thrombosis or bleeding
“Non Responders”
Ble
edin
g
Thr
ombo
sis
Inhi
bitio
n of
hem
osta
sis
(%)
Characteristics of the ideal antithrombotic agent
•Potent antithrombotic effect•Low risk•Predictable pharmakodynamic profile, making monitoring unnecessary•Rapid onset•Rapid onset•Rapid offset*•Availability of an antidote•No interaction with food or adjunctive medicines commonly used•Low cost* For safety reasons, a drug with rapid offset is generally preferable to a drug with long-lasting effects, although the use of the latter might minimize the negative effects of poor compliance.
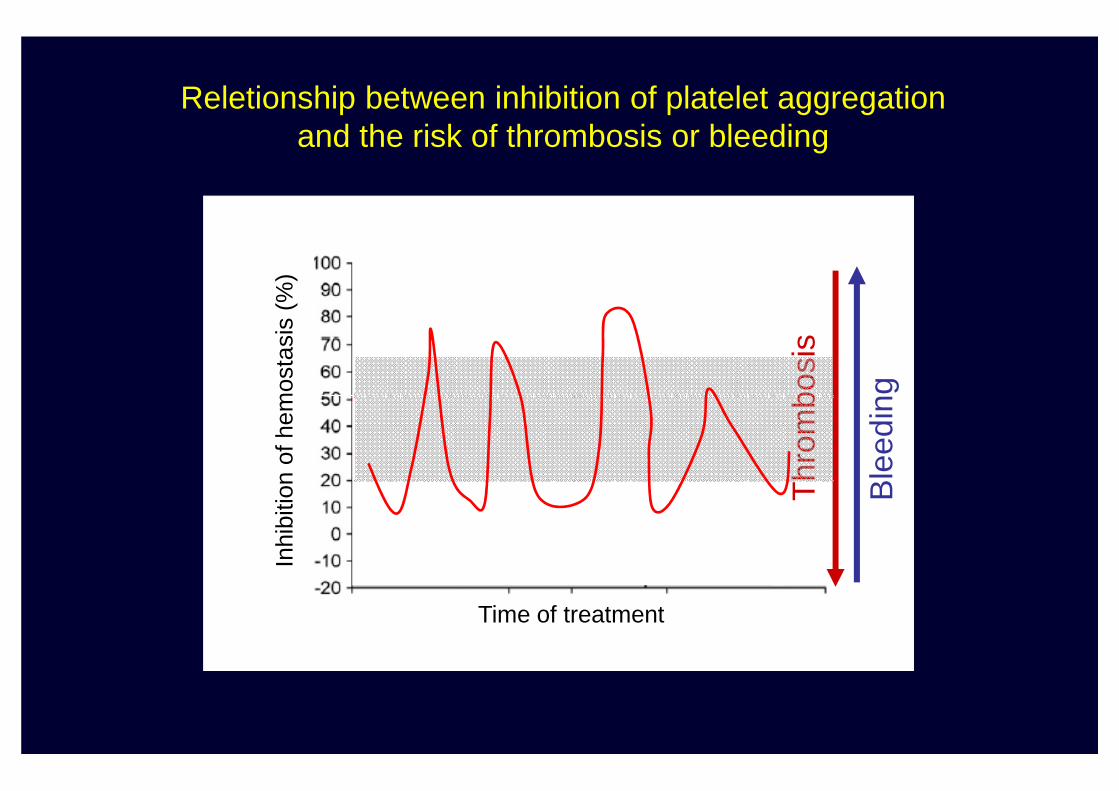
Reletionship between inhibition of platelet aggregationand the risk of thrombosis or bleeding
“Responders”
Ble
edin
g
Thr
ombo
sis
Inhi
bitio
n of
hem
osta
sis
(%)
“Non Responders”
Ble
edin
g
Thr
ombo
sis
Time of treatment
Inhi
bitio
n of
hem
osta
sis
(%)
Reletionship between inhibition of platelet aggregationand the risk of thrombosis or bleeding
“Responders”
Ble
edin
g
Thr
ombo
sis
Inhi
bitio
n of
hem
osta
sis
(%)
“Non Responders”
Ble
edin
g
Thr
ombo
sis
Time of treatment
Inhi
bitio
n of
hem
osta
sis
(%)
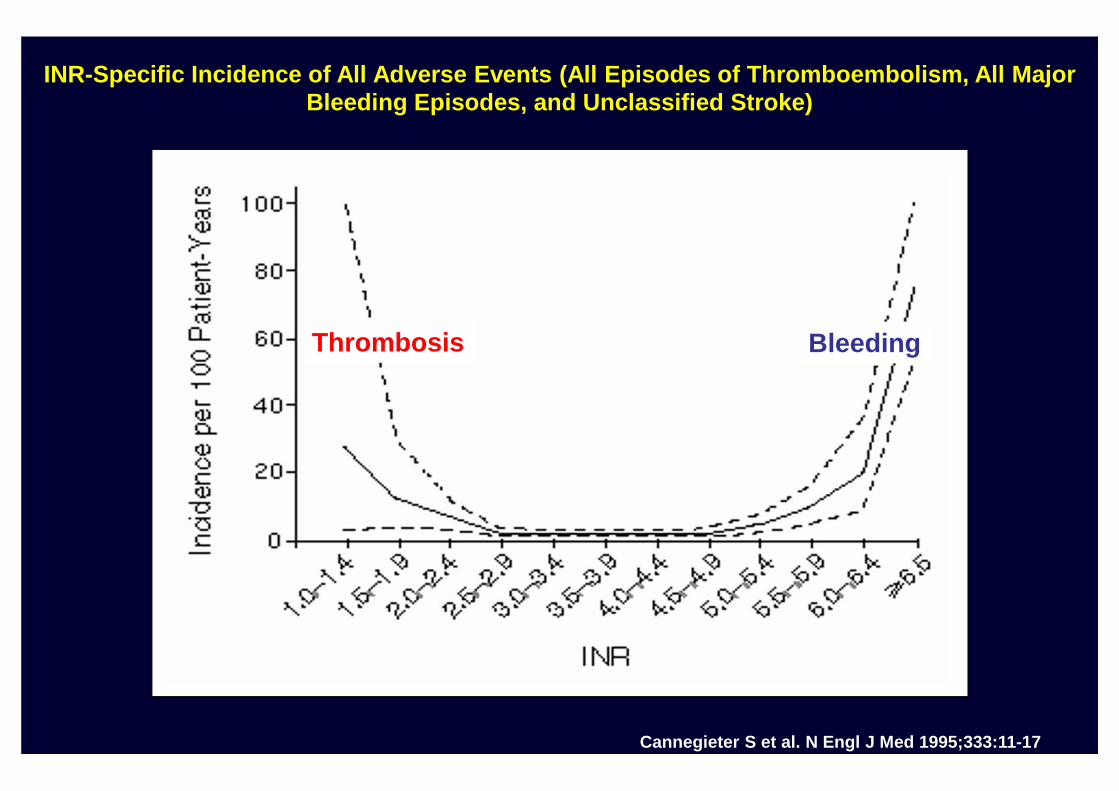
INR-Specific Incidence of All Adverse Events (All Episodes of Thromboembolism, All Major Bleeding Episodes, and Unclassified Stroke)
Thrombosis Bleeding
Cannegieter S et al. N Engl J Med 1995;333:11-17
Reletionship between inhibition of platelet aggregationand the risk of thrombosis or bleeding
“Responders”
Ble
edin
g
Thr
ombo
sis
Inhi
bitio
n of
hem
osta
sis
(%)
“Non Responders”
Ble
edin
g
Thr
ombo
sis
Time of treatment
Inhi
bitio
n of
hem
osta
sis
(%)
ANTICOAGULANT
Need for laboratorymonitoring
“Evolution” of antithrombotic treatment
monitoring
No Need for laboratorymonitoring
ANTIPLATELET
Need for laboratorymonitoring
ANTICOAGULANT
Need for laboratorymonitoring
“Evolution” of antithrombotic treatment
monitoring
No need for laboratorymonitoring
monitoring
No Need for laboratorymonitoring

ASPIRINASPIRIN
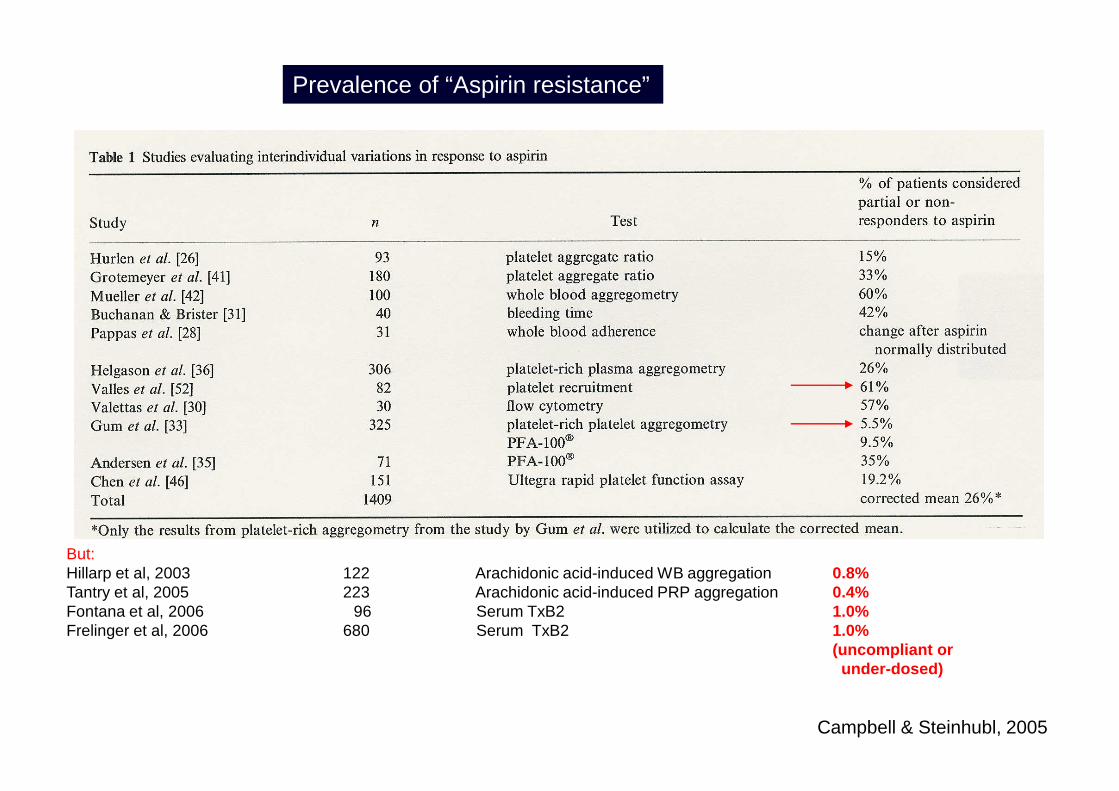
Prevalence of “Aspirin resistance”
But:Hillarp et al, 2003 122 Arachidonic acid-induced WB aggregation 0.8%Tantry et al, 2005 223 Arachidonic acid-induced PRP aggregation 0.4%Fontana et al, 2006 96 Serum TxB2 1.0%Frelinger et al, 2006 680 Serum TxB2 1.0%
(uncompliant orunder-dosed)
Campbell & Steinhubl, 2005

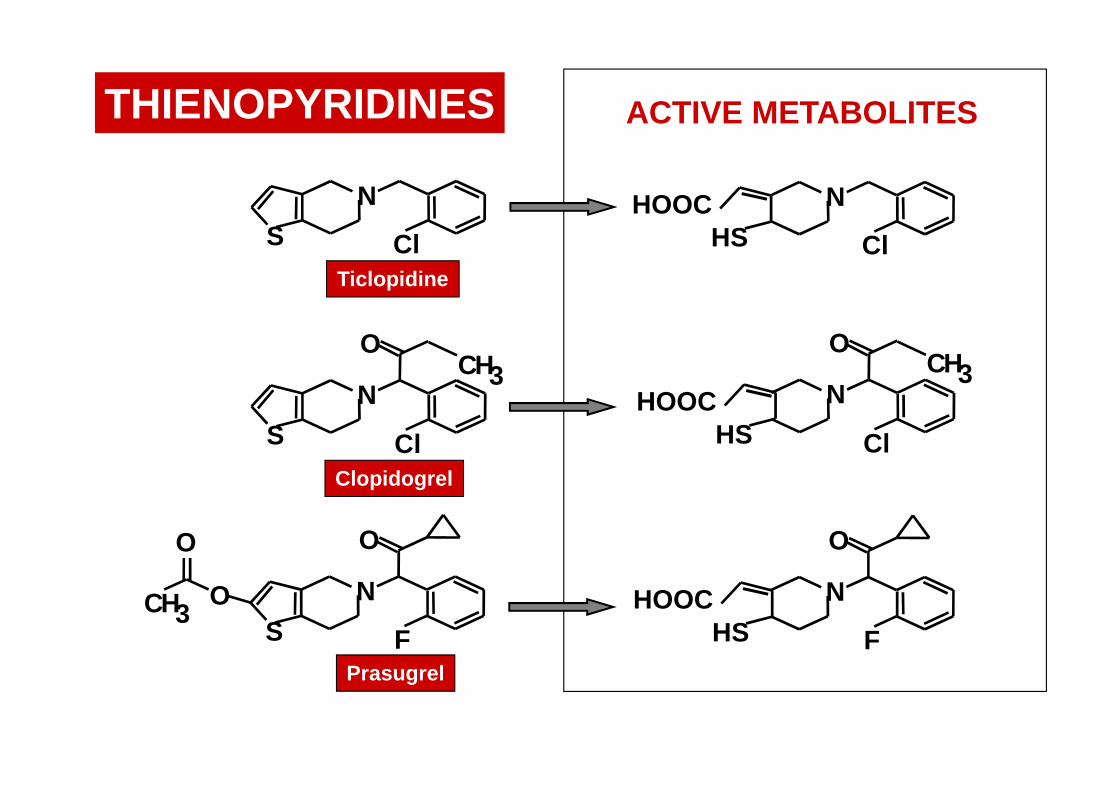
THIENOPYRIDINESTHIENOPYRIDINES
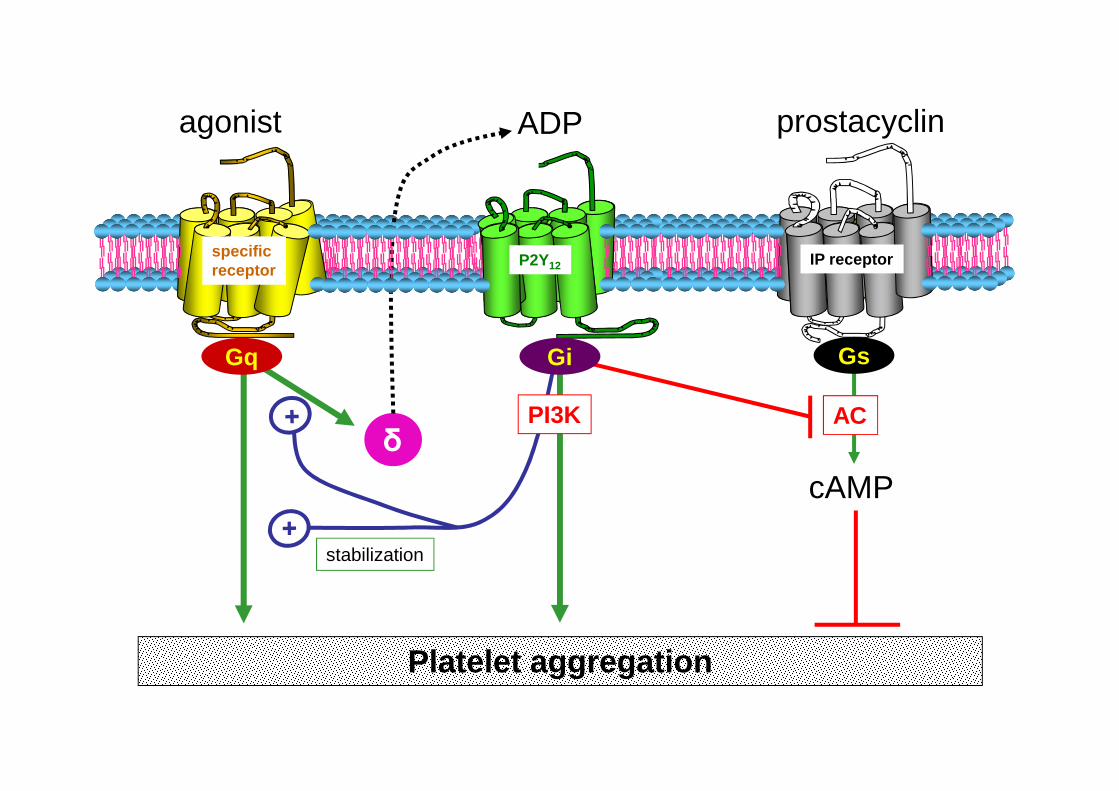
specificreceptor
ADP
P2Y12 IP receptor
ADPagonist prostacyclin
GsGiGq
Platelet aggregation
δ
stabilization
cAMP
PI3K AC
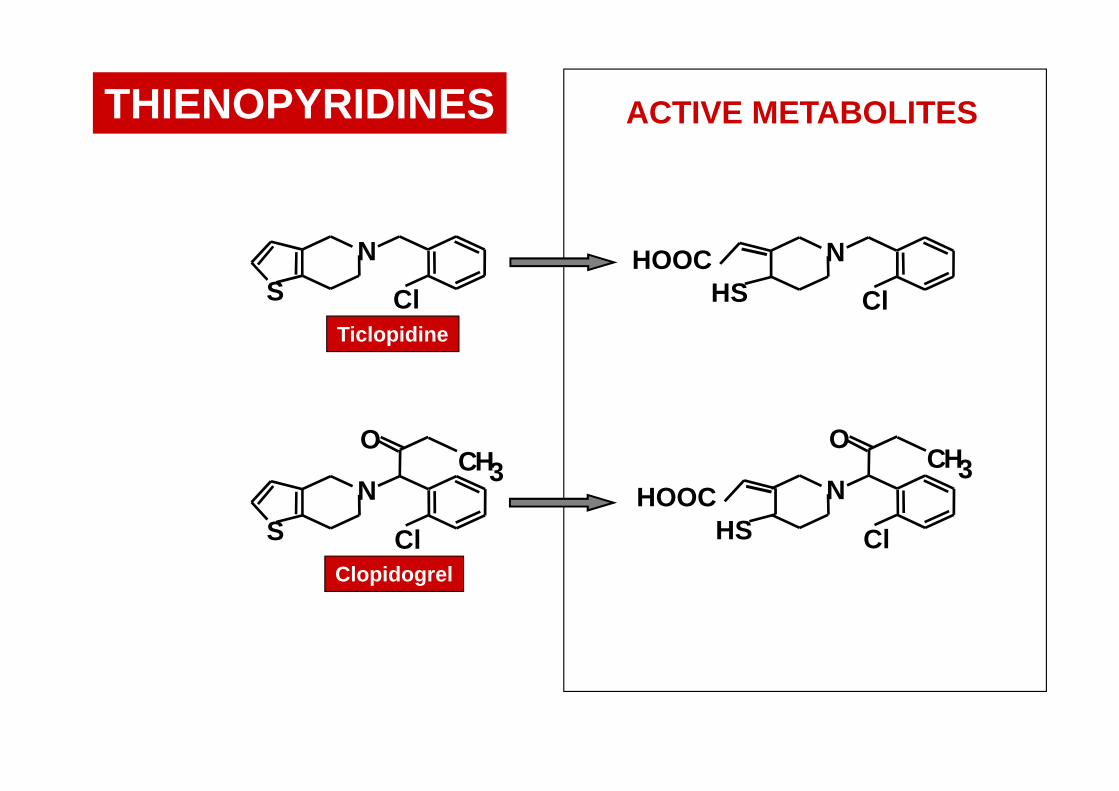
N
ClHSHOOCN
ClS
Ticlopidine
ACTIVE METABOLITESTHIENOPYRIDINES
N
OCH3
ClHSHOOCN
O
S
CH3
ClClopidogrel
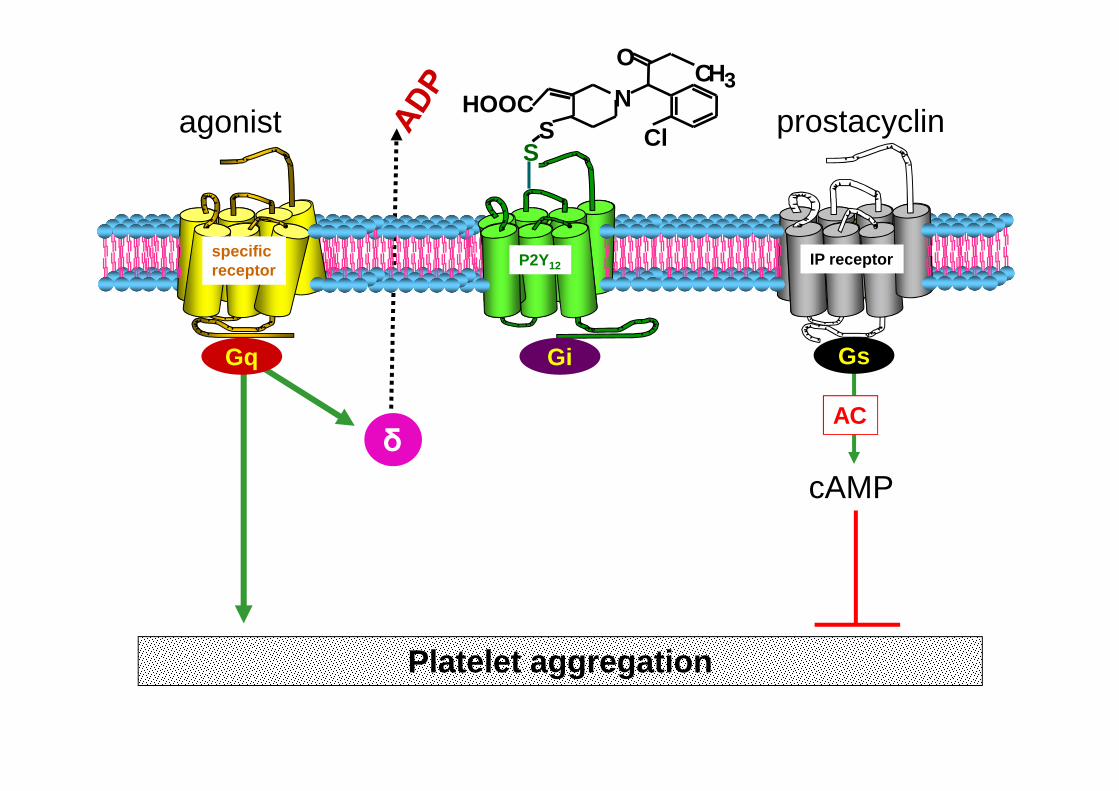
specificreceptor
P2Y12 IP receptor
agonist prostacyclin
GsGiGq
ADP
N
OCH3
ClSHOOC
S
Platelet aggregation
δ
cAMP
AC
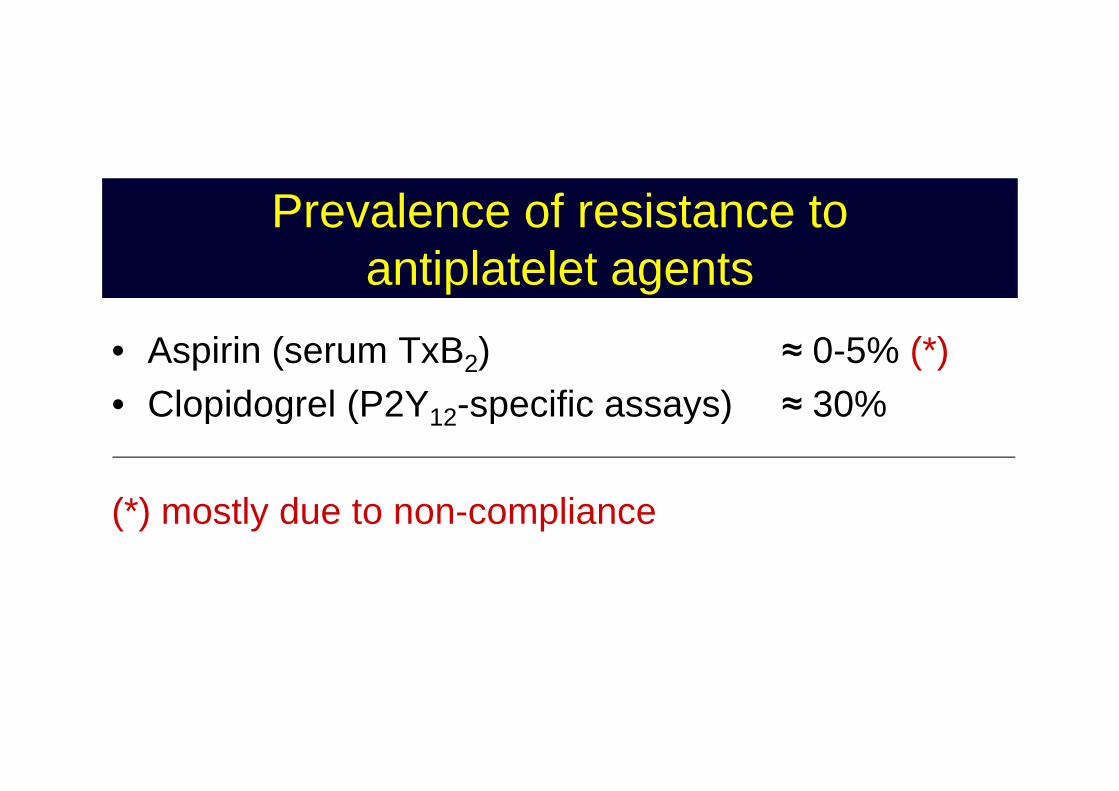
Prevalence of resistance toantiplatelet agents
• Aspirin (serum TxB2) ≈ 0-5% (*)• Clopidogrel (P2Y -specific assays) ≈ 30%• Clopidogrel (P2Y12-specific assays) ≈ 30%
(*) mostly due to non-compliance
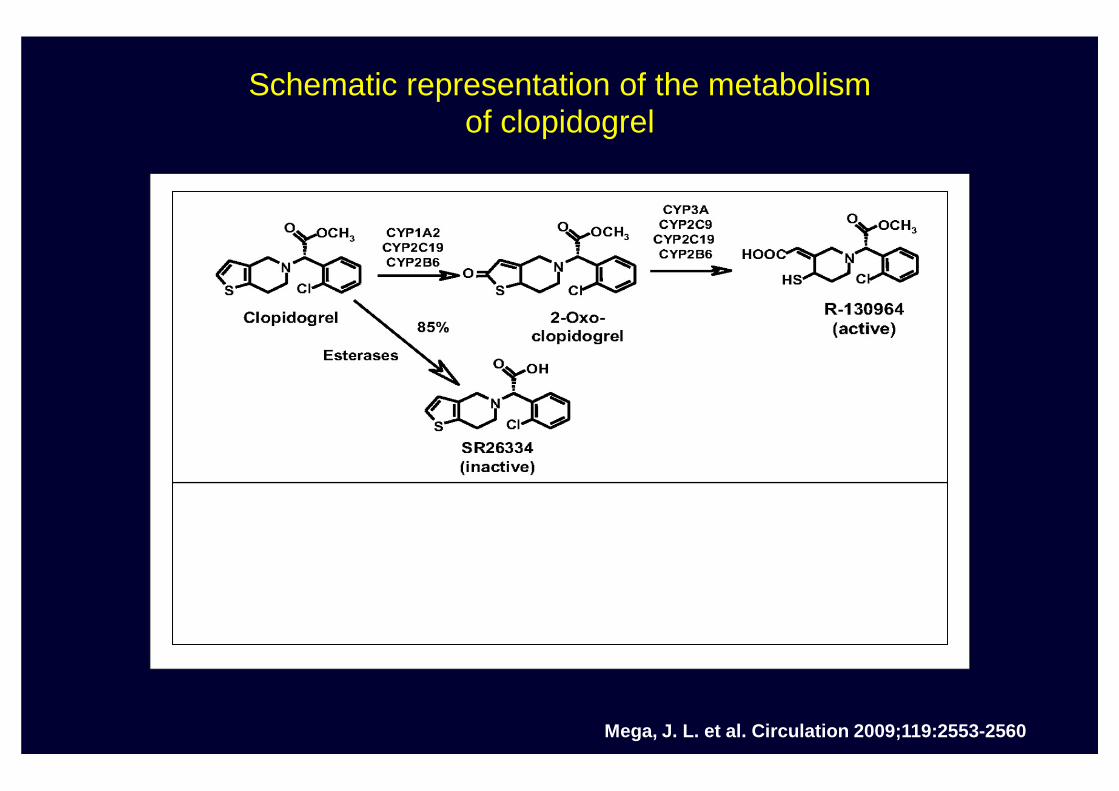
Schematic representation of the metabolismof clopidogrel
Mega, J. L. et al. Circulation 2009;119:2553-2560
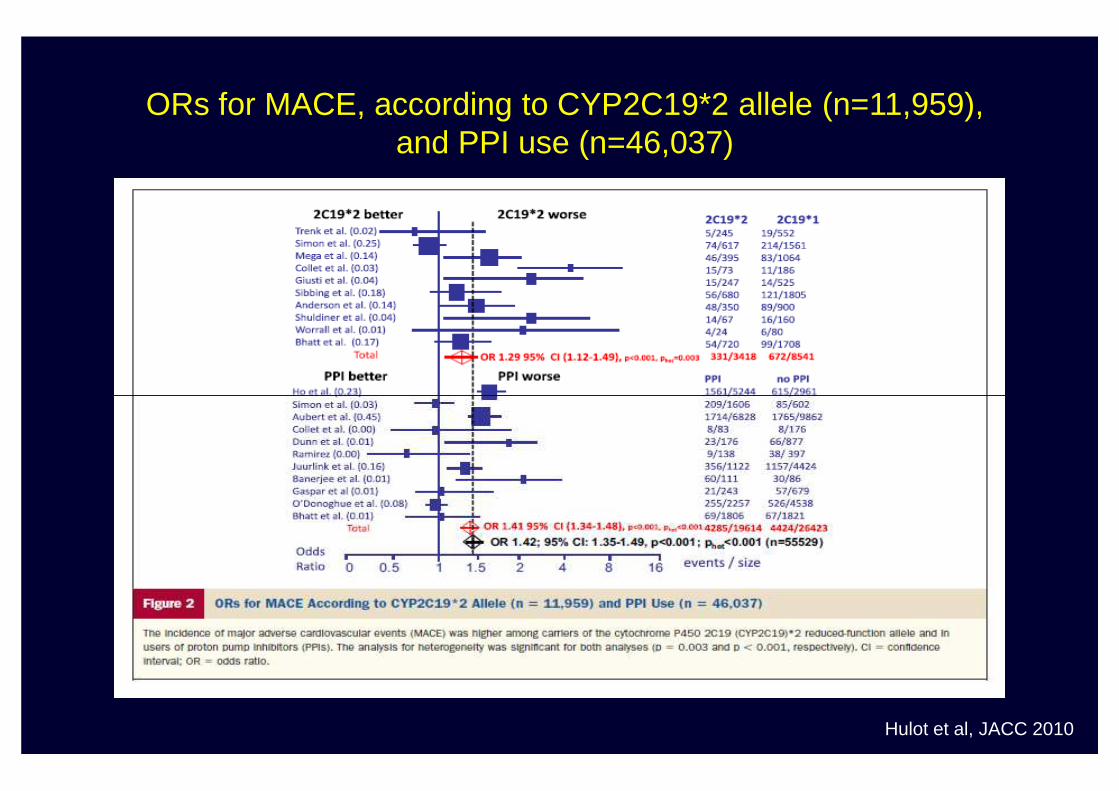
ORs for MACE, according to CYP2C19*2 allele (n=11,959),and PPI use (n=46,037)
Hulot et al, JACC 2010
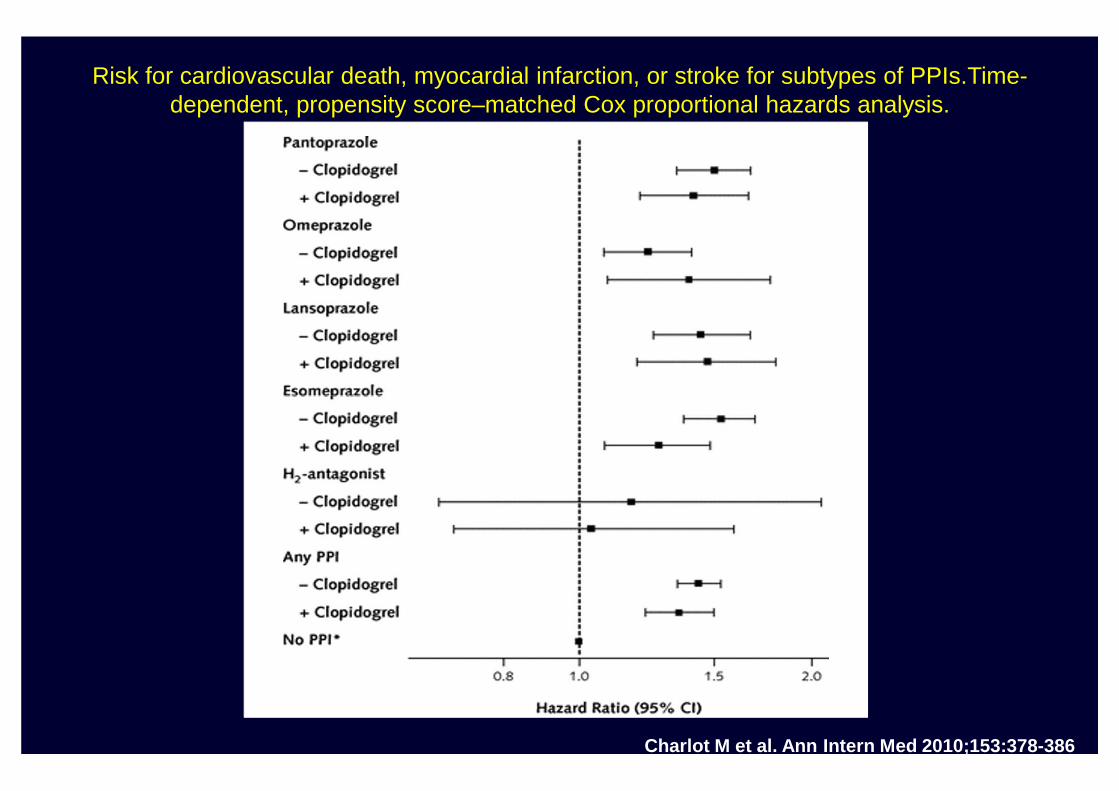
Risk for cardiovascular death, myocardial infarction, or stroke for subtypes of PPIs.Time-dependent, propensity score–matched Cox proportional hazards analysis.
Charlot M et al. Ann Intern Med 2010;153:378-386
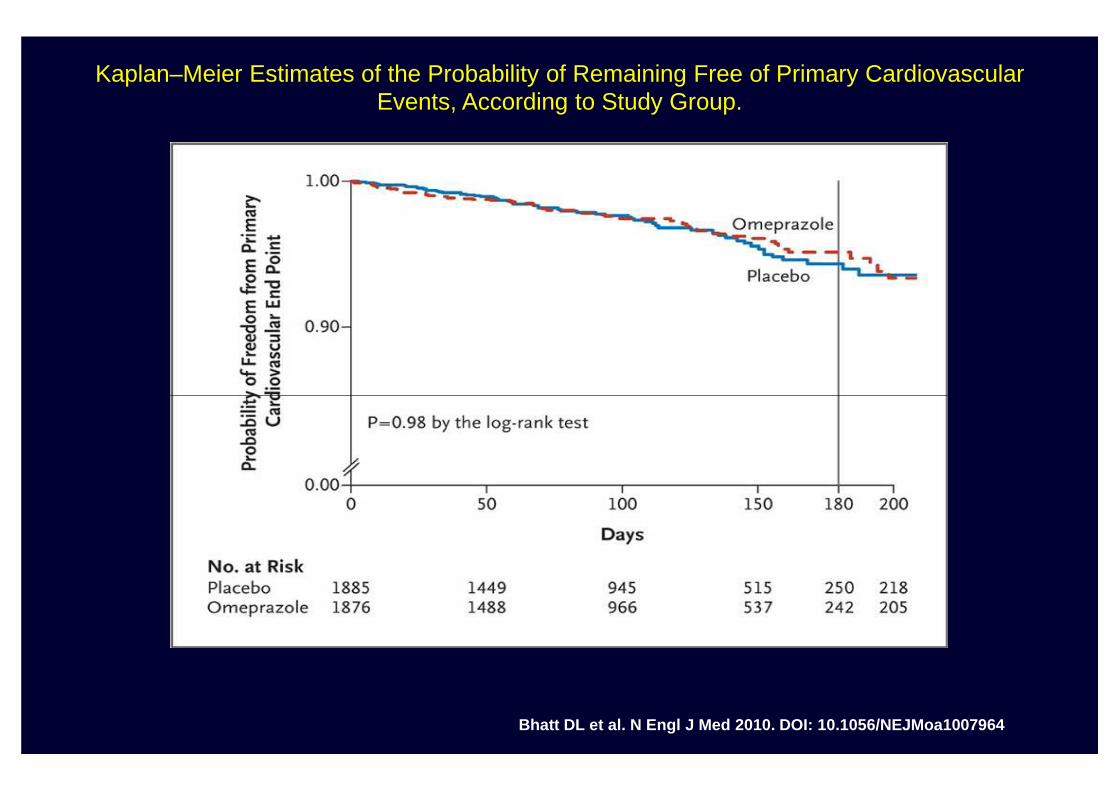
Kaplan–Meier Estimates of the Probability of Remaining Free of Primary Cardiovascular Events, According to Study Group.
Bhatt DL et al. N Engl J Med 2010. DOI: 10.1056/NEJMoa1007964
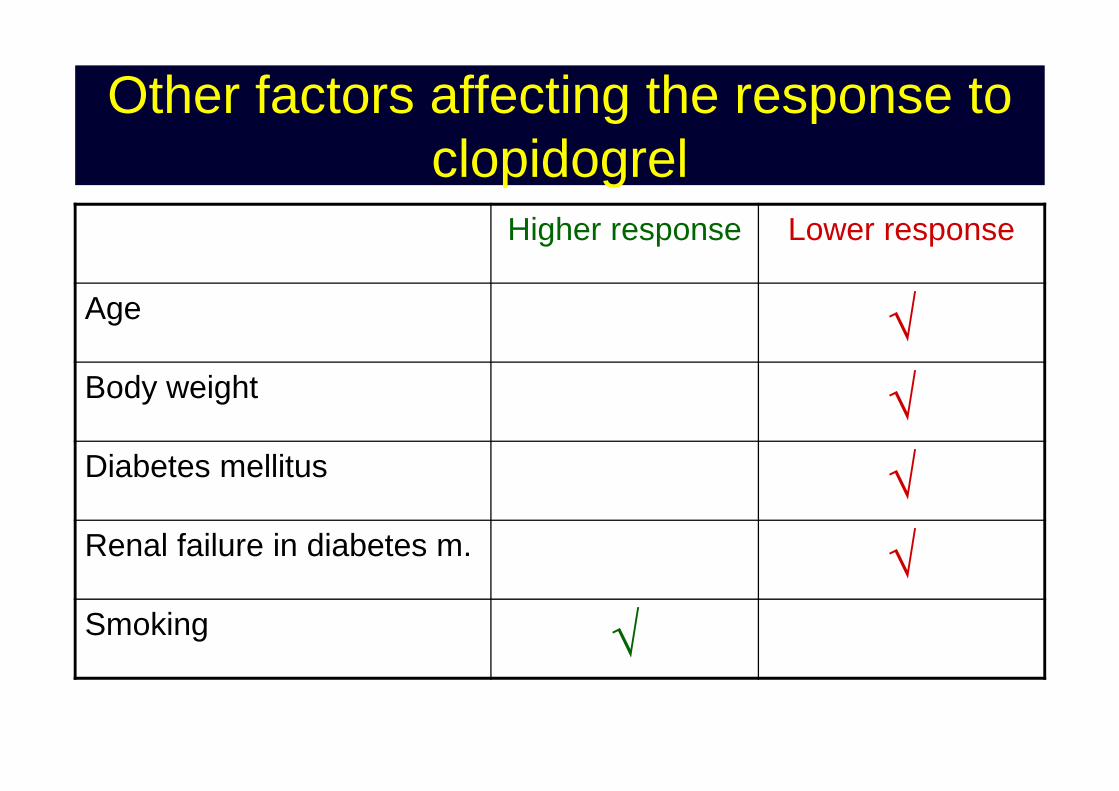
Other factors affecting the response to clopidogrel
Higher response Lower response
Age √Body weight √Body weight √Diabetes mellitus √Renal failure in diabetes m. √Smoking √
Response variability (“resistance”) to Clopidogrel
The solution?The solution?
“Tailored treatment”:increase the dose of Clopidogrel in poor responders
(based on the results of plateletplatelet functionfunction teststests))
IsIs itit the right the right approachapproach??
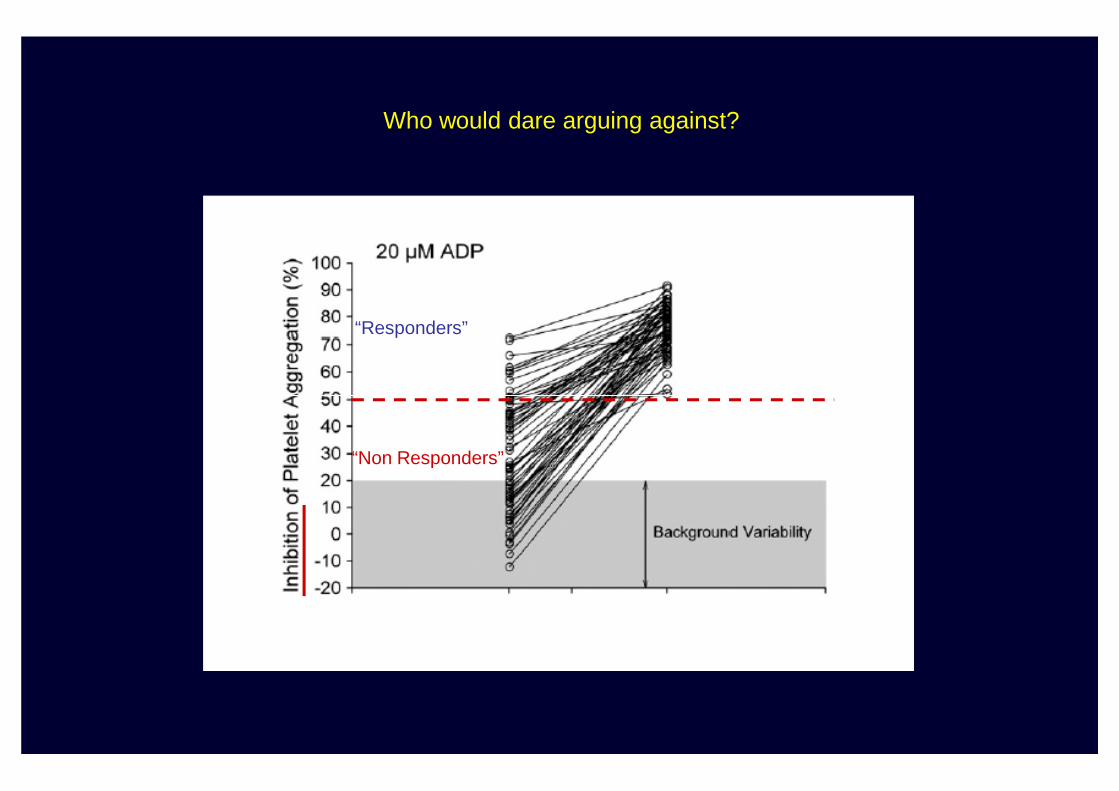
“Responders”
Who would dare arguing against?
“Non Responders”
Laboratory monitoring of clopidogrel therapyQuestions that need to be answered
• Which test of platelet function?• Is it really effective?• Is it the solution for all patients?• Is it safe?• Is it safe?• Is it cost-effective?

Studio GRAVITASStudio GRAVITAS
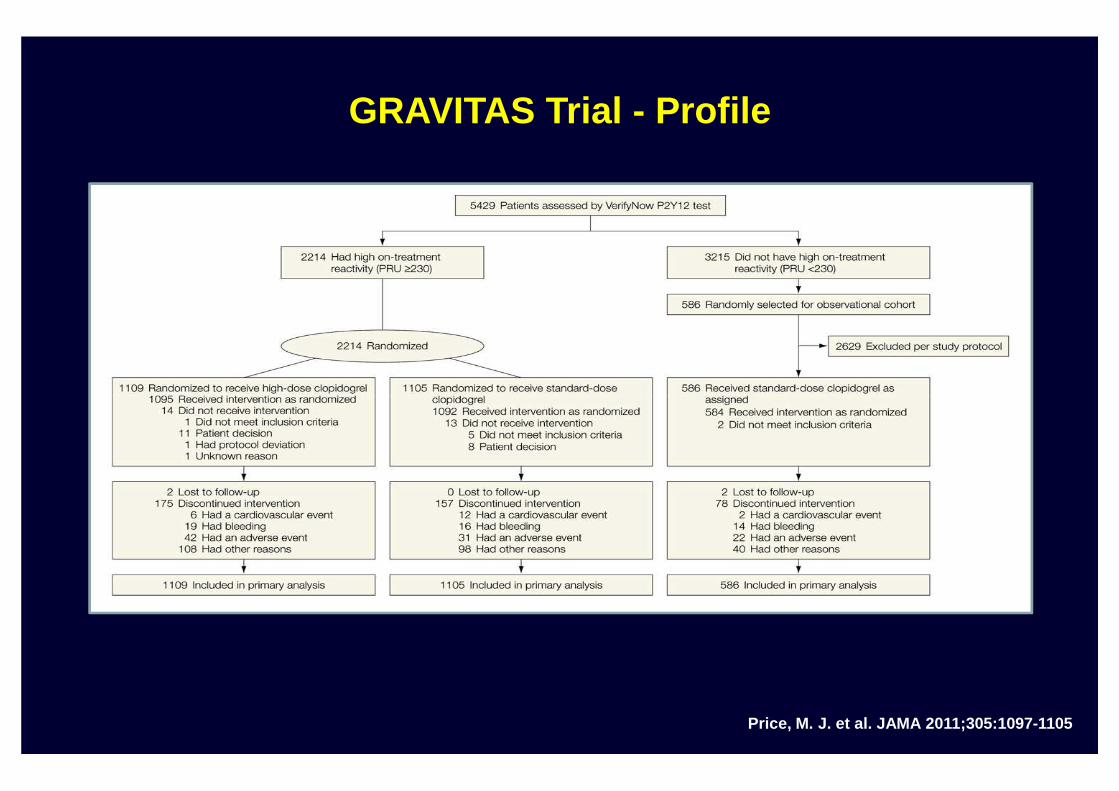
GRAVITAS Trial - Profile
Price, M. J. et al. JAMA 2011;305:1097-1105
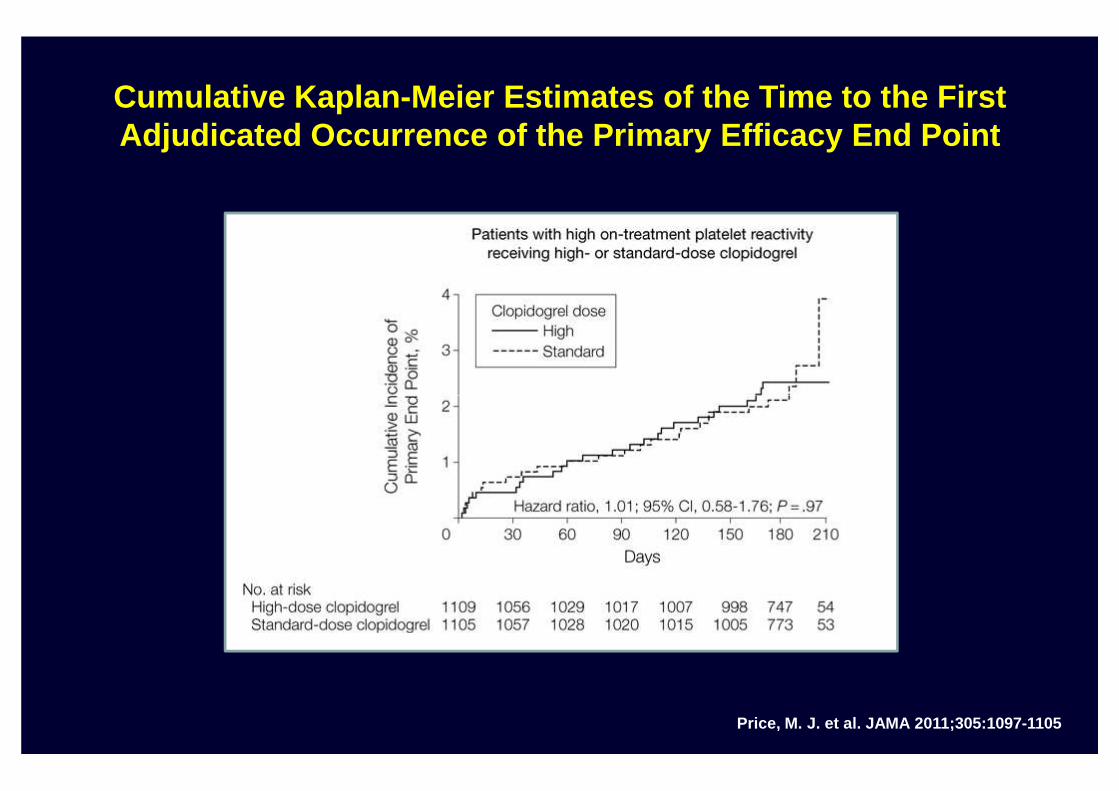
Cumulative Kaplan-Meier Estimates of the Time to the First Adjudicated Occurrence of the Primary Efficacy End Point
Price, M. J. et al. JAMA 2011;305:1097-1105
Response variability (“resistance”) to Clopidogrel
Another solution?
Change the drug!
Another solution?
N
ClHSHOOC
N
OCH3
HOOC
N
ClS
Ticlopidine
N
OCH3
ACTIVE METABOLITESTHIENOPYRIDINES
N
F
O
HSHOOC
N
ClHSHOOCN
S ClClopidogrel
N
F
O
S
O
OCH3
Prasugrel
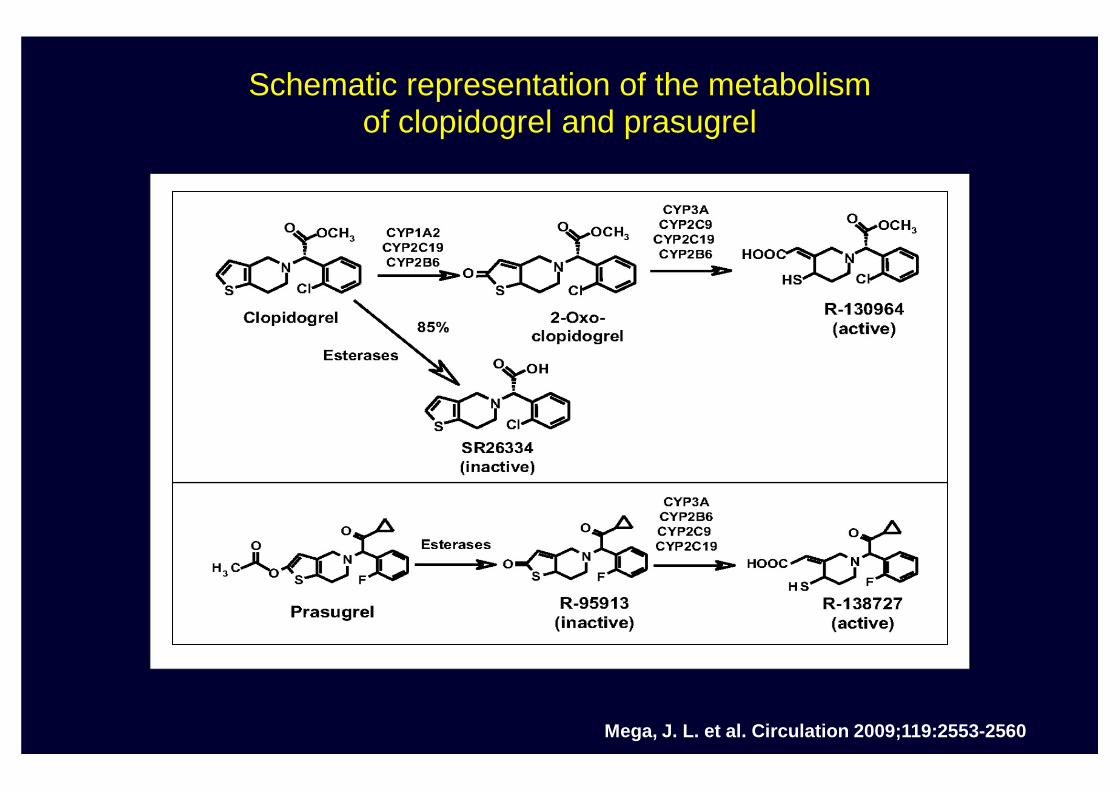
Schematic representation of the metabolismof clopidogrel and prasugrel
Mega, J. L. et al. Circulation 2009;119:2553-2560
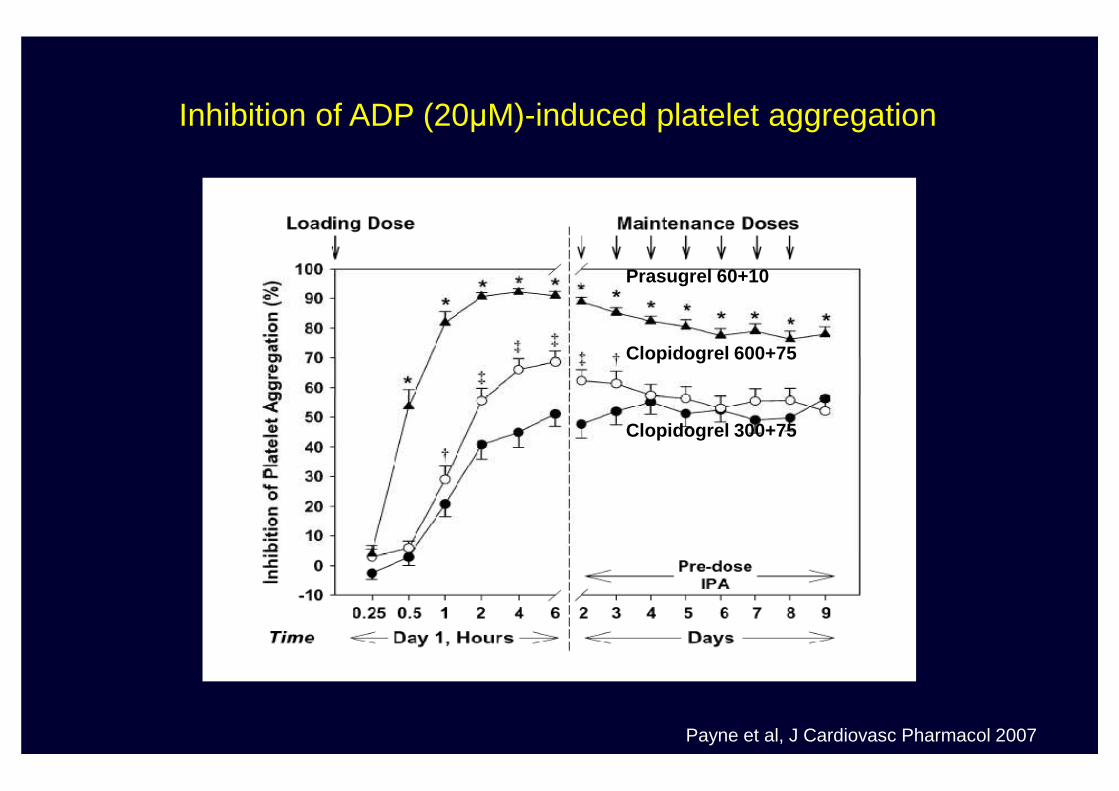
Prasugrel 60+10
Clopidogrel 600+75
Inhibition of ADP (20µM)-induced platelet aggregation
Clopidogrel 300+75
Payne et al, J Cardiovasc Pharmacol 2007
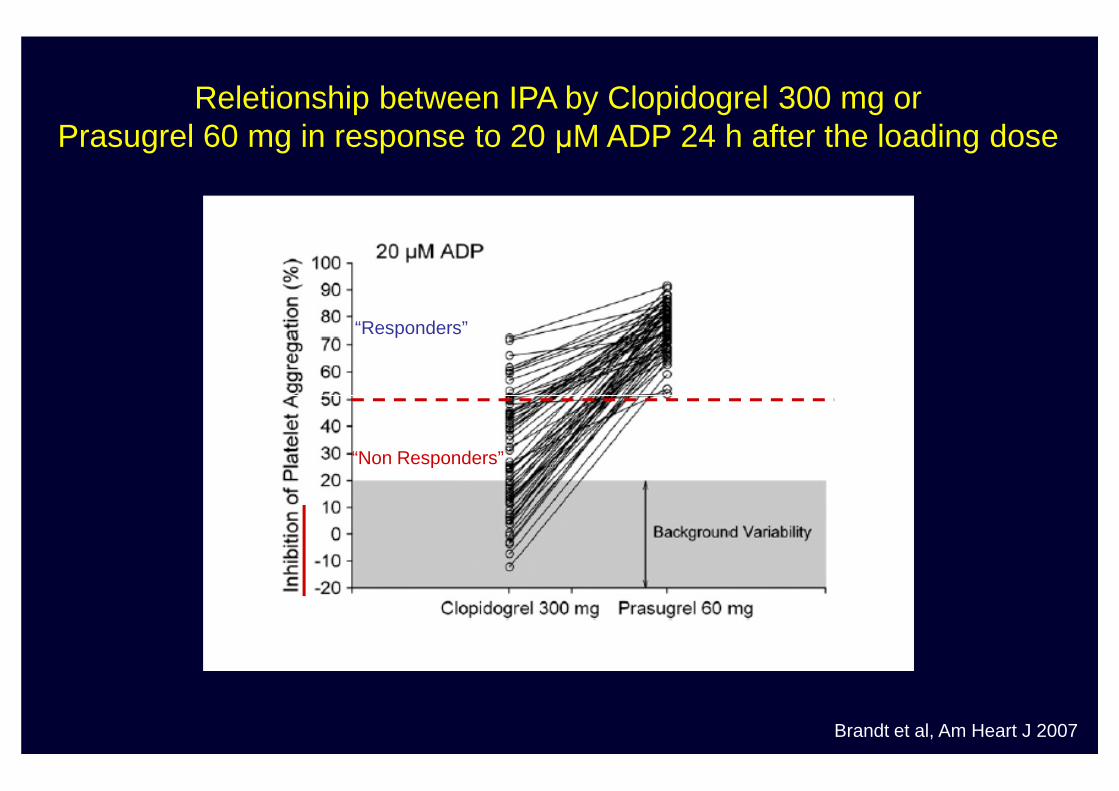
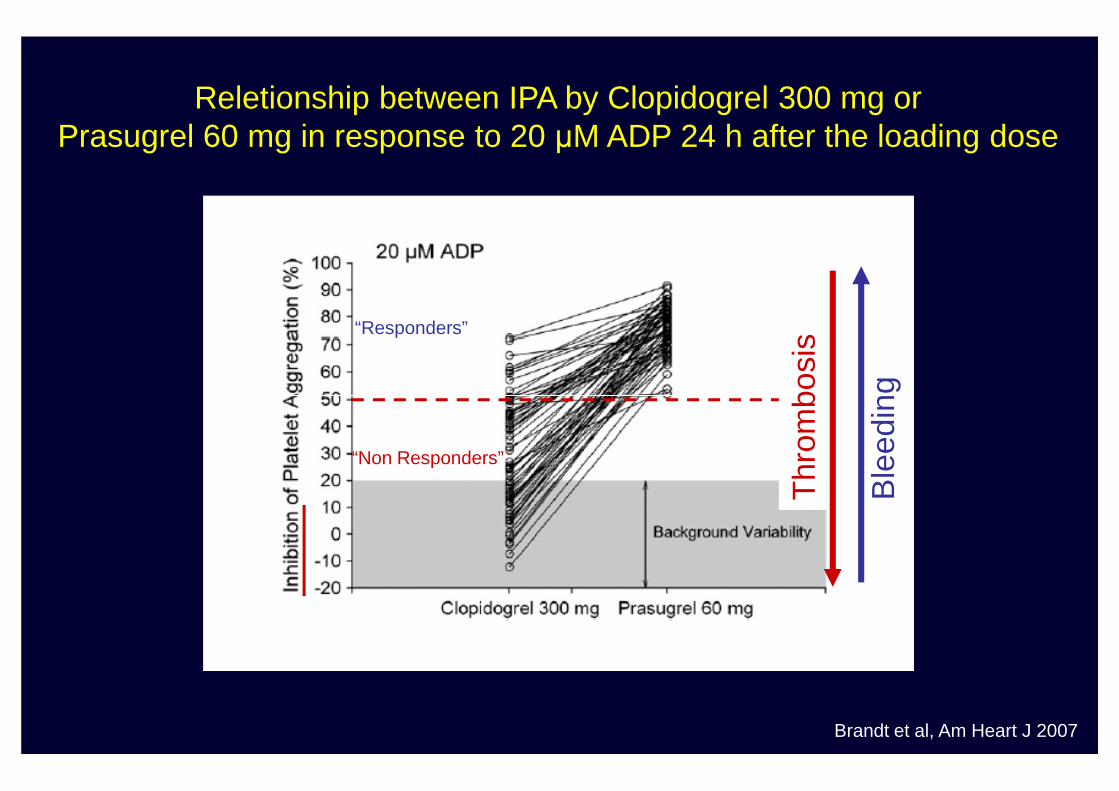
Reletionship between IPA by Clopidogrel 300 mg orPrasugrel 60 mg in response to 20 µM ADP 24 h after the loading dose
“Responders”
Brandt et al, Am Heart J 2007
“Non Responders”
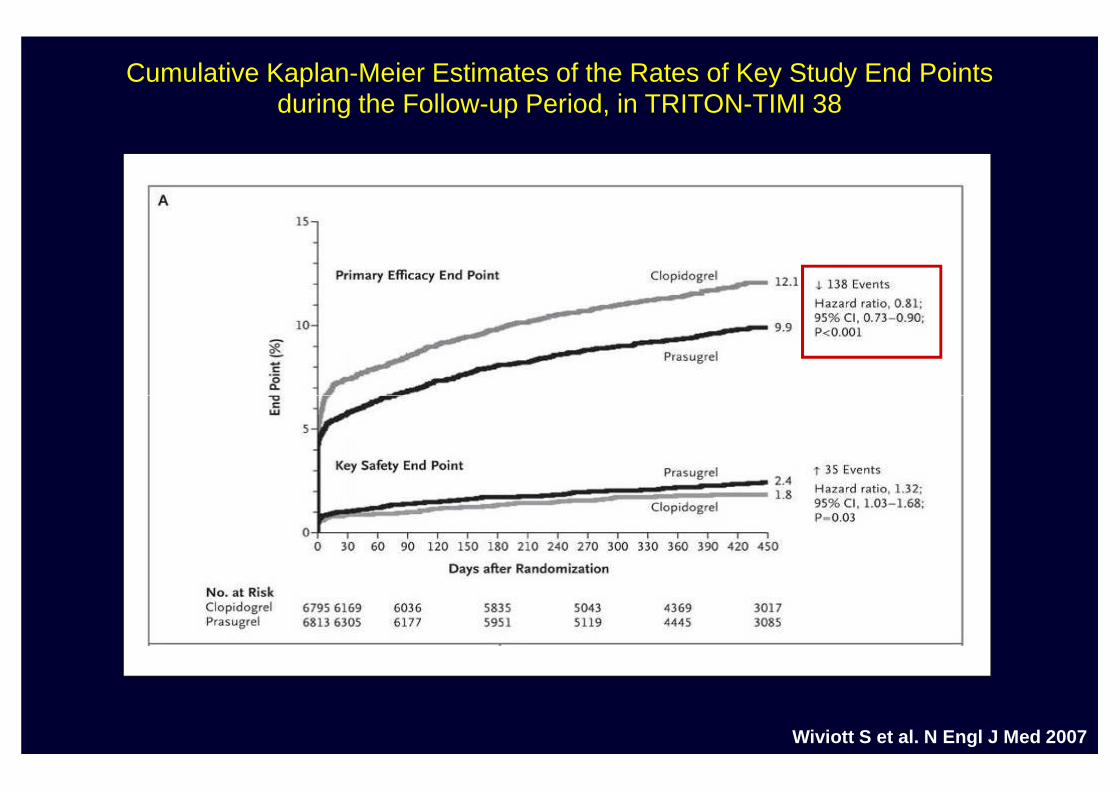
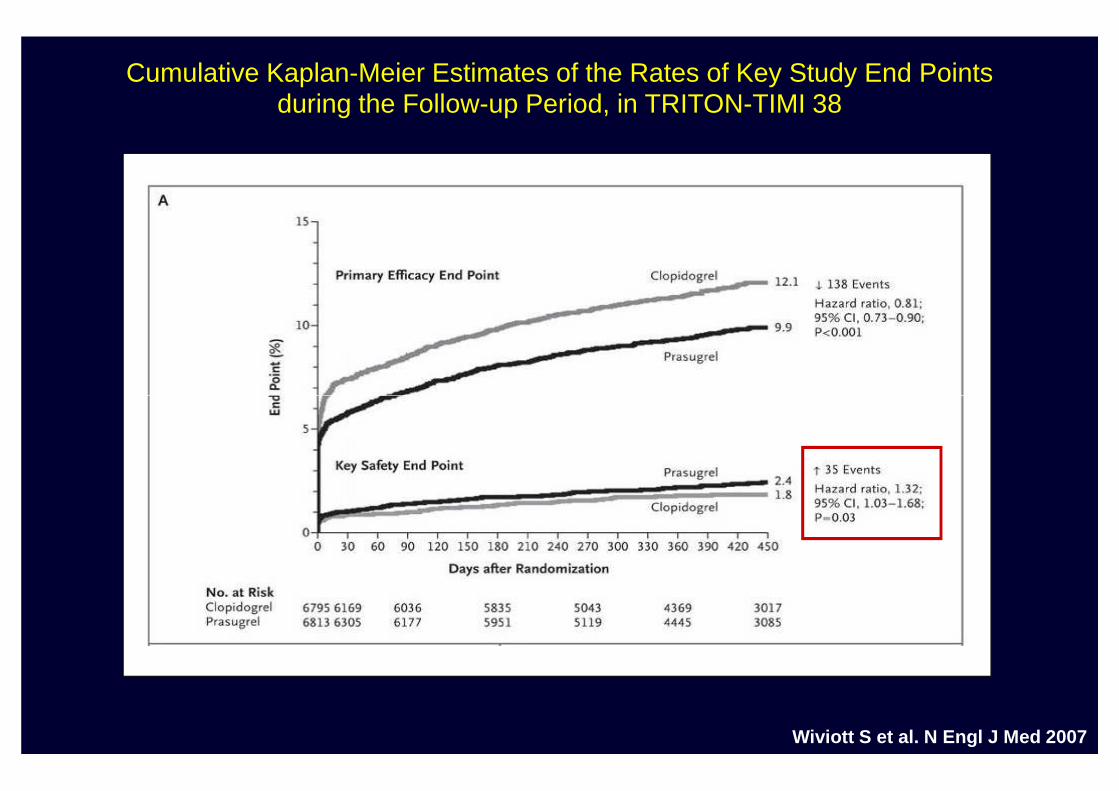
Cumulative Kaplan-Meier Estimates of the Rates of Key Study End Pointsduring the Follow-up Period, in TRITON-TIMI 38
Wiviott S et al. N Engl J Med 2007
Cumulative Kaplan-Meier Estimates of the Rates of Key Study End Pointsduring the Follow-up Period, in TRITON-TIMI 38
Wiviott S et al. N Engl J Med 2007
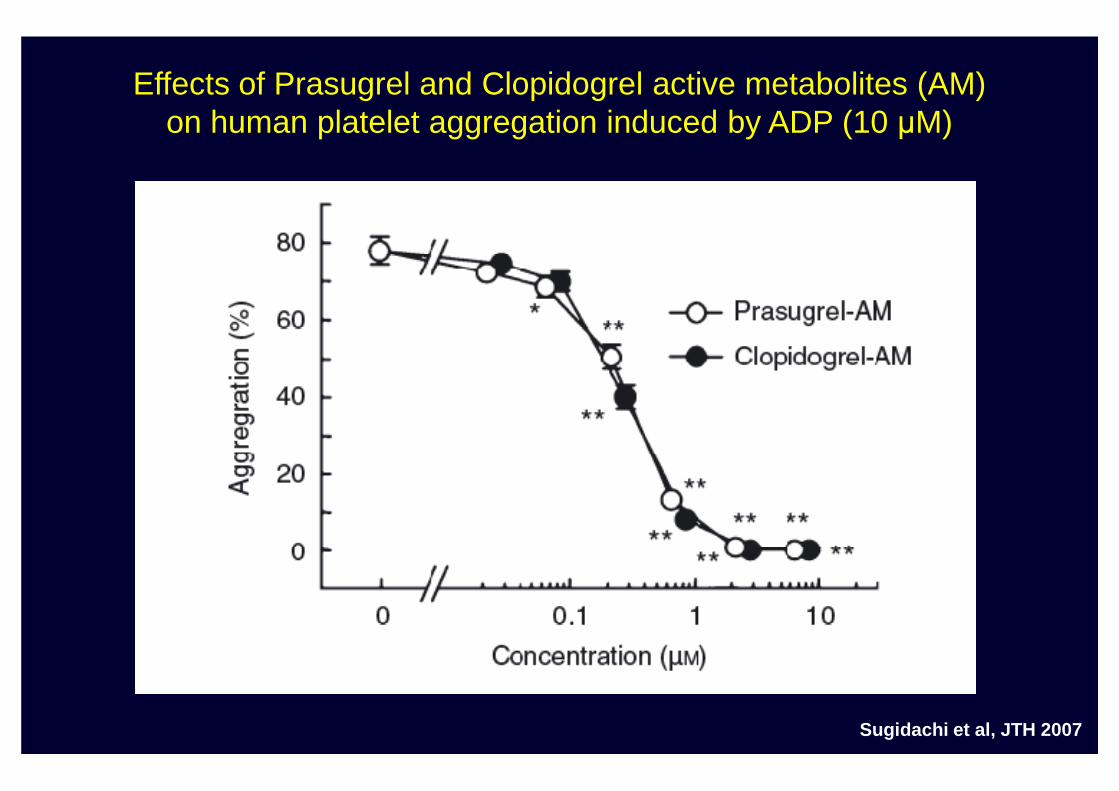
Effects of Prasugrel and Clopidogrel active metabolites (AM)on human platelet aggregation induced by ADP (10 µM)
Sugidachi et al, JTH 2007
Reletionship between drug-induced inhibition of hemostasisand the risk of thrombosis or bleeding
“Responders”
Inhi
bitio
n of
hem
osta
sis
(%)
Ble
edin
g
Thr
ombo
sis
“Non Responders”
Inhi
bitio
n of
hem
osta
sis
(%)
Ble
edin
g
Thr
ombo
sis
Reletionship between IPA by Clopidogrel 300 mg orPrasugrel 60 mg in response to 20 µM ADP 24 h after the loading dose
“Responders”
Ble
edin
g
Thr
ombo
sis
Brandt et al, Am Heart J 2007
“Non Responders”
Ble
edin
g
Thr
ombo
sis
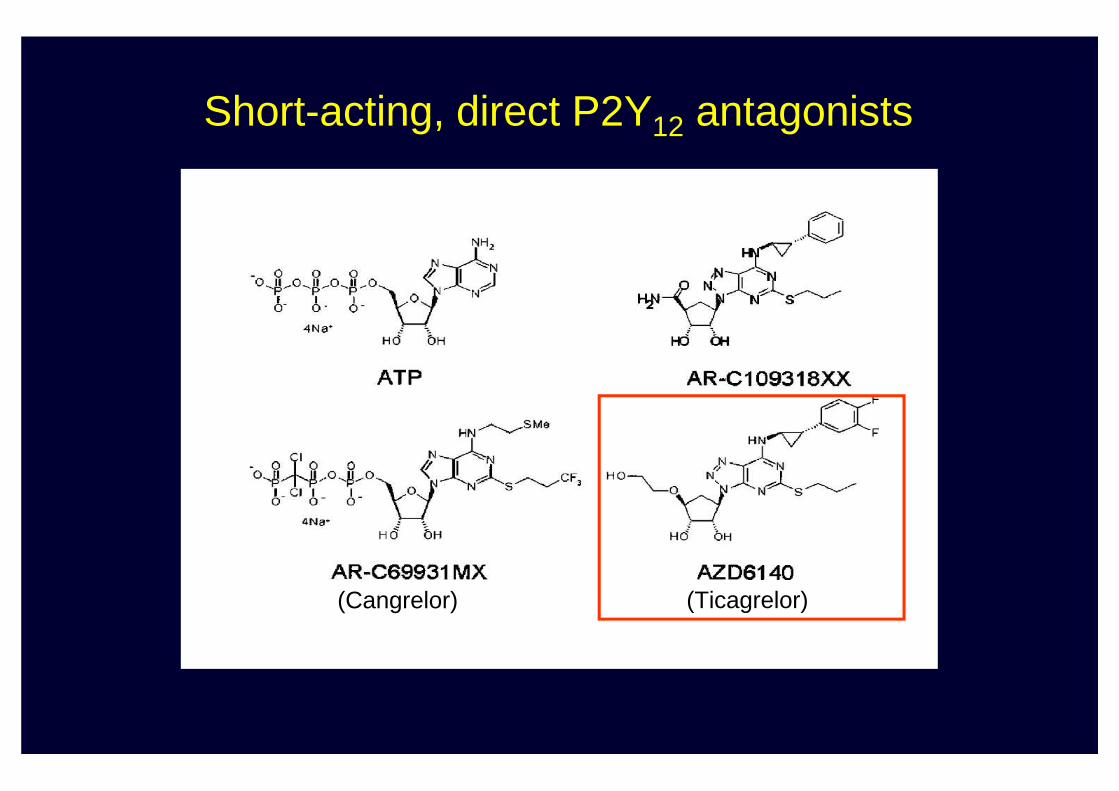
Short-acting, direct P2Y12 antagonists
(Cangrelor) (Ticagrelor)
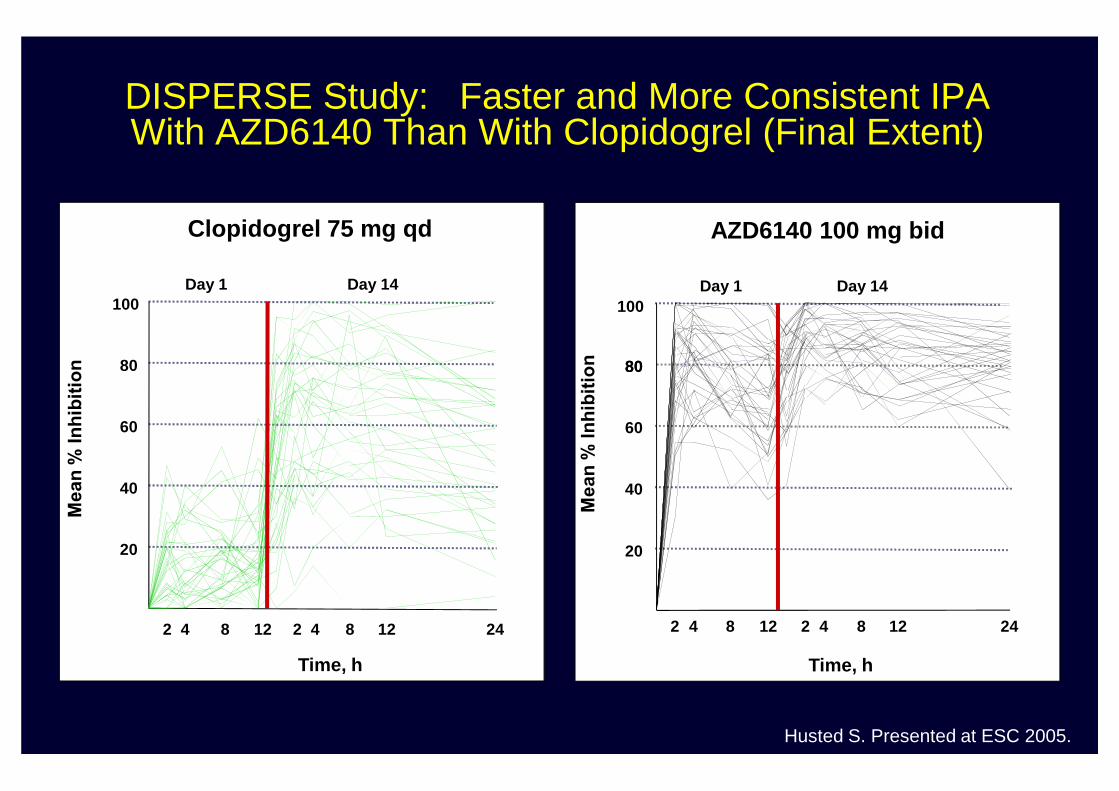
Clopidogrel 75 mg qd
80
100Day 1 Day 14
AZD6140 100 mg bid
80
100Day 1 Day 14
80
DISPERSE Study: Faster and More Consistent IPA With AZD6140 Than With Clopidogrel (Final Extent)
Husted S. Presented at ESC 2005.
Time, h
20
40
60
2 4 8 12 2 4 8 12 24
Time, h
20
40
60
2 4 8 12 2 4 8 12 24
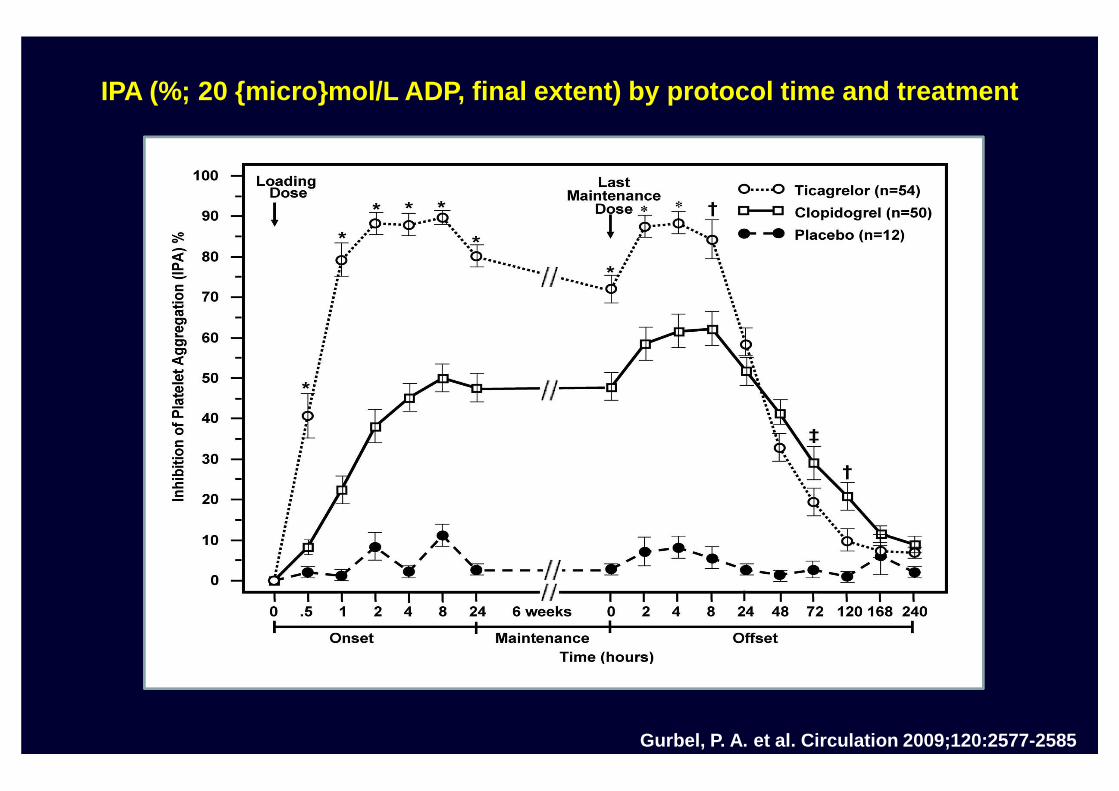
IPA (%; 20 {micro}mol/L ADP, final extent) by protocol time and treatment
Gurbel, P. A. et al. Circulation 2009;120:2577-2585
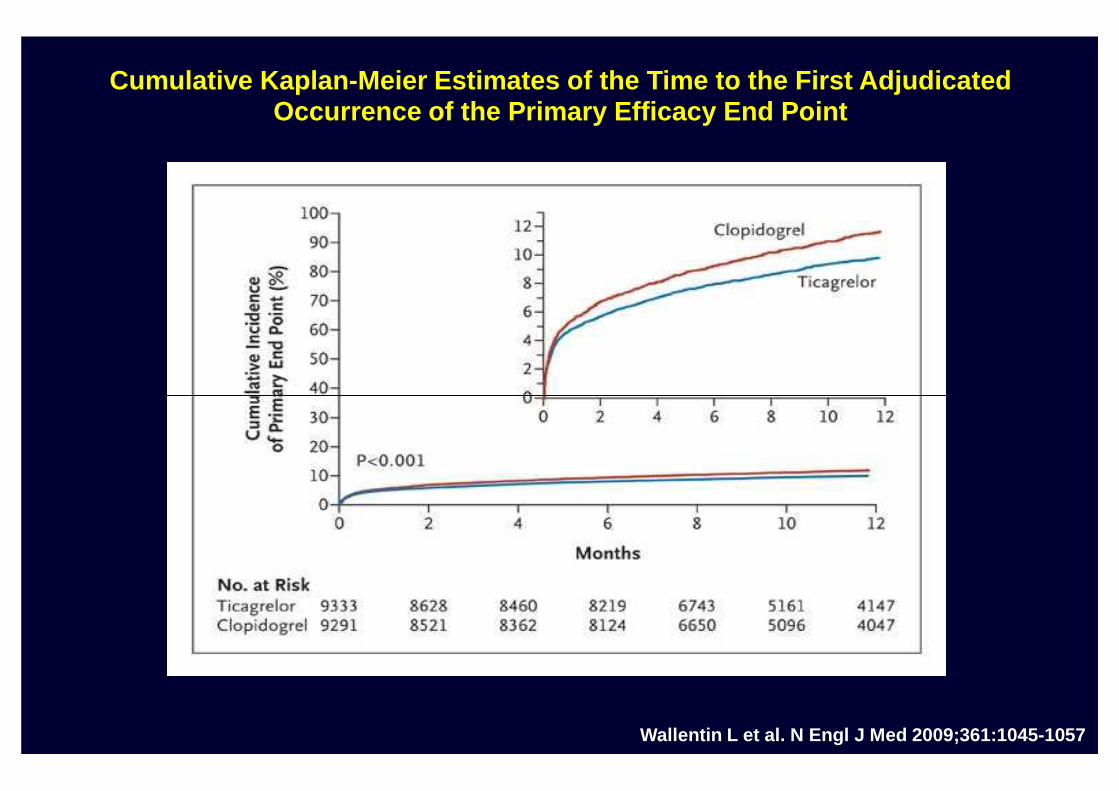
Cumulative Kaplan-Meier Estimates of the Time to the First Adjudicated Occurrence of the Primary Efficacy End Point
Wallentin L et al. N Engl J Med 2009;361:1045-1057
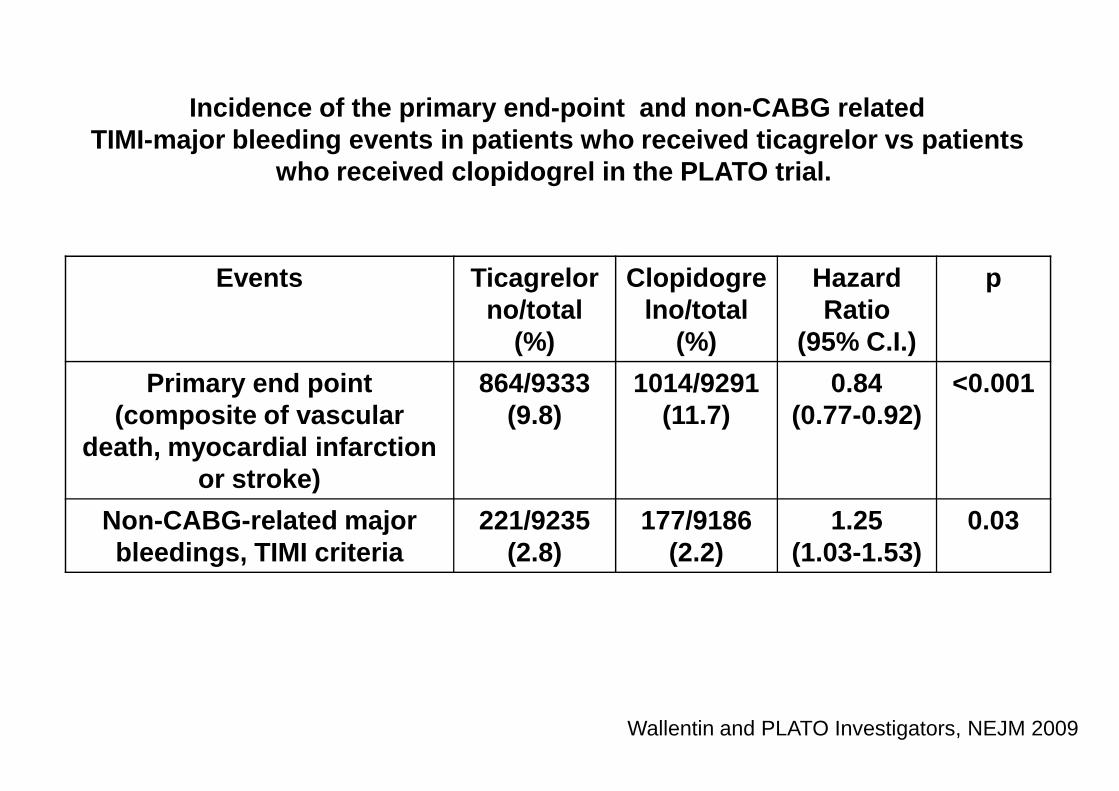
Incidence of the primary end-point and non-CABG relatedTIMI-major bleeding events in patients who received ticagrelor vs patients
who received clopidogrel in the PLATO trial.
Events Ticagrelorno/total
(%)
Clopidogrelno/total
(%)
Hazard Ratio
(95% C.I.)
p
Primary end point 864/9333 1014/9291 0.84 <0.001Primary end point (composite of vascular
death, myocardial infarction or stroke)
864/9333(9.8)
1014/9291(11.7)
0.84(0.77-0.92)
<0.001
Non-CABG-related major bleedings, TIMI criteria
221/9235(2.8)
177/9186(2.2)
1.25(1.03-1.53)
0.03
Wallentin and PLATO Investigators, NEJM 2009
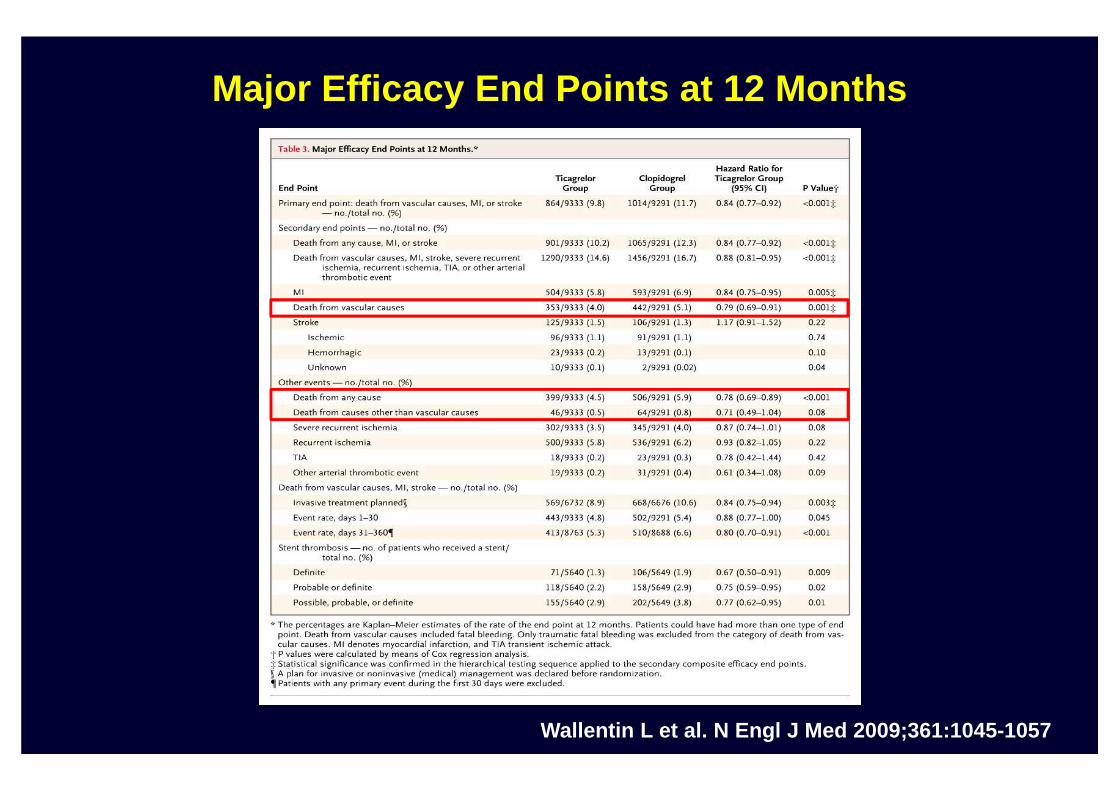
Major Efficacy End Points at 12 Months
Wallentin L et al. N Engl J Med 2009;361:1045-1057
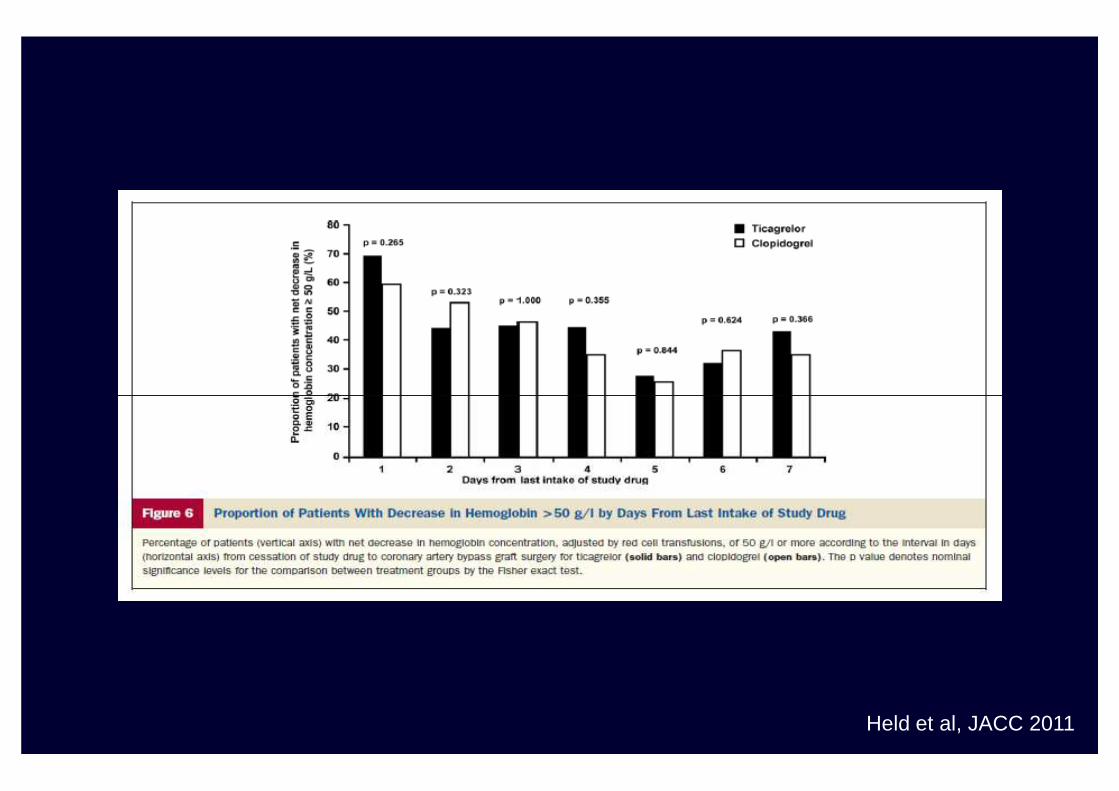
Held et al, JACC 2011
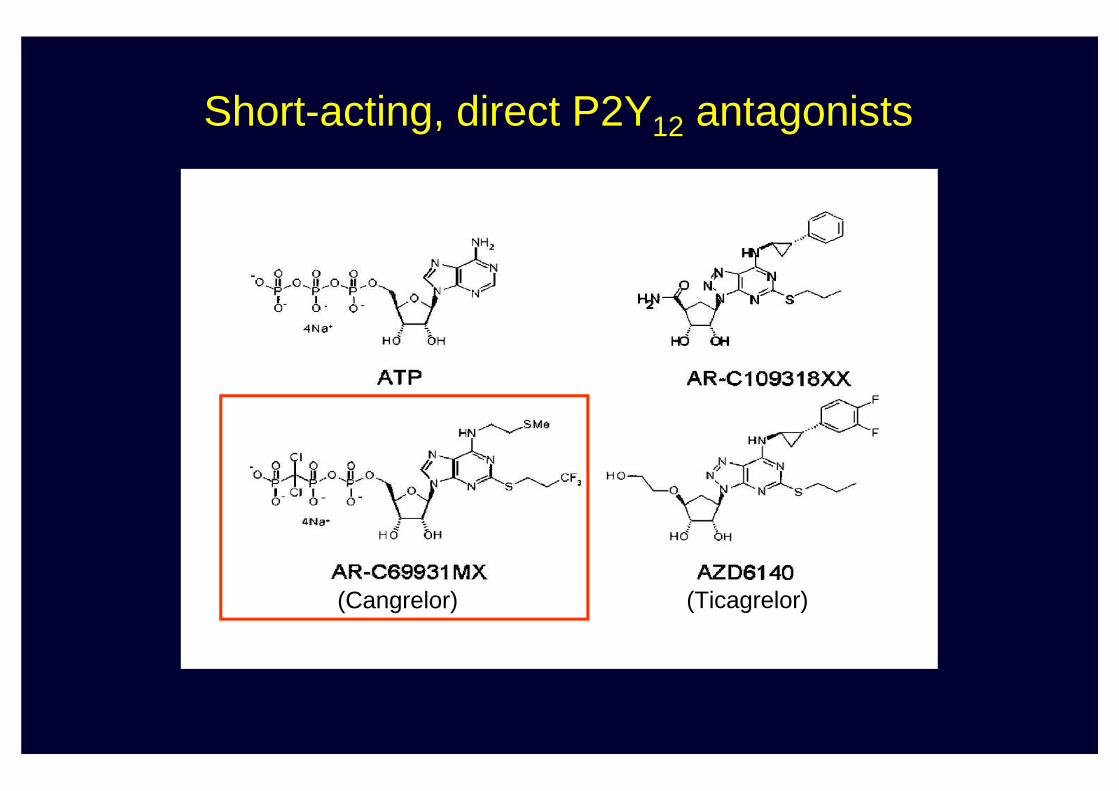
Short-acting, direct P2Y12 antagonists
(Cangrelor) (Ticagrelor)
ELINOGREL
• Elinogrel is direct-acting, competitive, reversible P2Y12 non-nucleotide antagonist
• IC50 ~2-3 µM in ADP aggregation (PRP)
• Highly selective for P2Y12 (does not inhibit P2Y1 or other purinergic receptors)
• Oral bioavailability ~50%
• T1/2 ~12 h (BID drug) (Elimination: 50% renal, 50% hepatic)
• Tmax 2-6 h
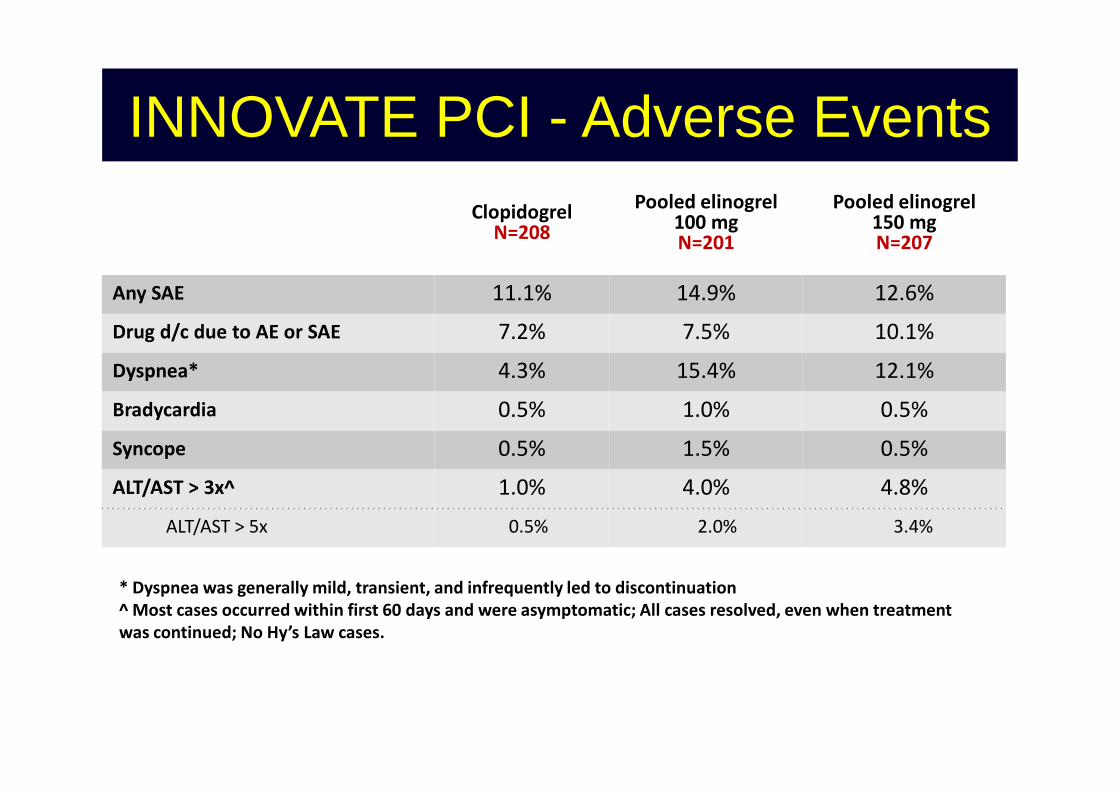
INNOVATE PCI - Adverse EventsClopidogrel
N=208
Pooled elinogrel 100 mg N=201
Pooled elinogrel 150 mg N=207
Any SAE 11.1% 14.9% 12.6%
Drug d/c due to AE or SAE 7.2% 7.5% 10.1%
Dyspnea* 4.3% 15.4% 12.1%
0.5% 1.0% 0.5%Bradycardia 0.5% 1.0% 0.5%
Syncope 0.5% 1.5% 0.5%
ALT/AST > 3x^ 1.0% 4.0% 4.8%
ALT/AST > 5x 0.5% 2.0% 3.4%
* Dyspnea was generally mild, transient, and infrequently led to discontinuation
^ Most cases occurred within first 60 days and were asymptomatic; All cases resolved, even when treatment
was continued; No Hy’s Law cases.
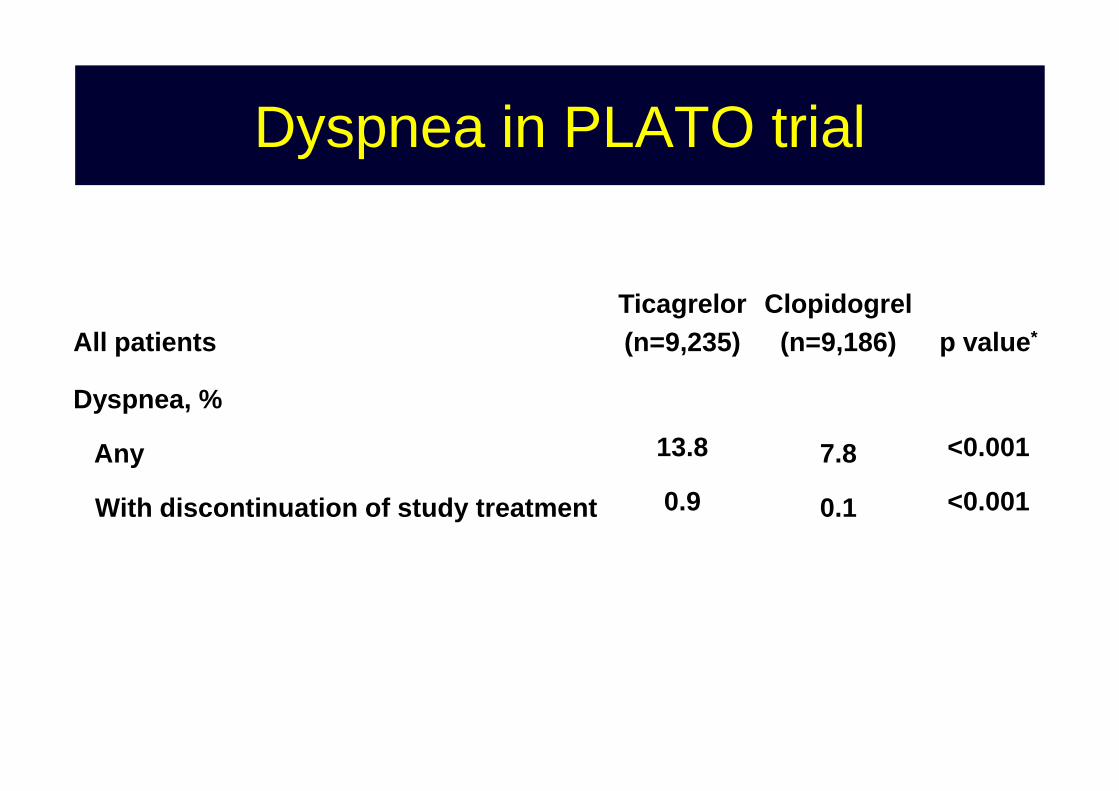
Dyspnea in PLATO trial
All patientsTicagrelor(n=9,235)
Clopidogrel(n=9,186) p value*
Dyspnea, % Dyspnea, %
Any
With discontinuation of study treatment
13.8
0.9
7.8
0.1
<0.001
<0.001
CangrelorCangrelor and and dyspnoeadyspnoea
• CHAMPION PCI: a dyspnoea adverse event was reported in 1.0% of patients receiving cangrelor and 0.4% of patients receiving only clopidogrel (P = 0.001)clopidogrel (P = 0.001)
• CHAMPION PLATFORM: a dyspnoea adverse event was reported in 1.4% of patients receiving cangrelor and 0.5% of patients receiving placebo (P = 0.002)