“News da San Antonio” Nuovi dati ... - Congressi AIRO · Funding Cancer Research UK, UK Medical...
89
Catia Angiolini Dipartimento di Oncologia-SC Oncologia Medica “News da San Antonio” Nuovi dati clinici sul trattamento farmacologico del carcinoma mammario.
Transcript of “News da San Antonio” Nuovi dati ... - Congressi AIRO · Funding Cancer Research UK, UK Medical...

Azienda Sanitaria Firenze
Catia Angiolini Dipartimento di Oncologia-SC Oncologia Medica
“News da San Antonio” Nuovi dati clinici sul trattamento farmacologico
del carcinoma mammario.

Azienda Sanitaria Firenze 2
“News da SABCS e del 2012”: nuovi dati clinici sul trattamento farmacologico del carcinoma mammario.
! terapia adiuvante " Ormonoterapia (TAM / LET)
" Anticorpi monoclonali (trastuzumab e bevacizumab)
" Chemioterapia adiuvante dopo recidiva di malattia
! terapia della malattia metastatica " 2012: everolimus / pertuzumab / T-DM1
" SABCS: Fulvestrant / Bevacizumab / Eribulina
" Nuovi target: CDK PD 0332991

Azienda Sanitaria Firenze 3
Terapia adiuvante

!"#!$%&%!'()*+,-%"+./0123,4%#/,536%!5+1,7-%$8/6-36%%%%
9:%*7%;%<3+67%/2%+'()*+,-%-+./0123,%1,%=>?%'173+734%3223@-7%1,%-83%2167-%A%73@/,'%'3@+'3%+2-36%'1+5,/717!
B6373,-3'%/,%C38+D2%/2%-83%%!"#!$%@/DD+C/6+-1*3%56/)E%
%!DD%+)-8/67%'3@D+63%,/%63D3*+,-%@/,2D1@-%/2%1,-3637-F!
"#$!%$&'$('!)*+#,&!-#$.+*!"/01',(20!�!-#$.+*!34+*#1/!#$5!6+,+#*.4!-+$&+*!#&!73!8+#9&4!".(+$.+!-+$&+*!�!:+.+0;+*!<=>?!@AB@!34(,!1*+,+$&#&('$!(,!&4+!($&+99+.&2#9!1*'1+*&/!'C!%3D%"E!!-'$&#.&!!%3D%"F-3"7E'GE#.E2H!!C'*!1+*0(,,('$!&'!*+1*'52.+!'*!5(,&*(;2&+E!

Articles
www.thelancet.com Published online December 5, 2012 http://dx.doi.org/10.1016/S0140-6736(12)61963-1 1
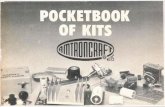
Long-term eff ects of continuing adjuvant tamoxifen to 10 years versus stopping at 5 years after diagnosis of oestrogen receptor-positive breast cancer: ATLAS, a randomised trialChristina Davies, Hongchao Pan, Jon Godwin, Richard Gray, Rodrigo Arriagada, Vinod Raina, Mirta Abraham, Victor Hugo Medeiros Alencar, Atef Badran, Xavier Bonfi ll, Joan Bradbury, Michael Clarke, Rory Collins, Susan R Davis, Antonella Delmestri, John F Forbes, Peiman Haddad, Ming-Feng Hou, Moshe Inbar, Hussein Khaled, Joanna Kielanowska, Wing-Hong Kwan, Beela S Mathew, Bettina Müller, Antonio Nicolucci, Octavio Peralta, Fany Pernas, Lubos Petruzelka, Tadeusz Pienkowski, Balakrishnan Rajan, Maryna T Rubach, Sera Tort, Gerard Urrútia, Miriam Valentini, Yaochen Wang, Richard Peto, for the Adjuvant Tamoxifen: Longer Against Shorter (ATLAS) Collaborative Group*
SummaryBackground For women with oestrogen receptor (ER)-positive early breast cancer, treatment with tamoxifen for 5 years substantially reduces the breast cancer mortality rate throughout the fi rst 15 years after diagnosis. We aimed to assess the further eff ects of continuing tamoxifen to 10 years instead of stopping at 5 years.
Methods In the worldwide Adjuvant Tamoxifen: Longer Against Shorter (ATLAS) trial, 12 894 women with early breast cancer who had completed 5 years of treatment with tamoxifen were randomly allocated to continue tamoxifen to 10 years or stop at 5 years (open control). Allocation (1:1) was by central computer, using minimisation. After entry (between 1996 and 2005), yearly follow-up forms recorded any recurrence, second cancer, hospital admission, or death. We report eff ects on breast cancer outcomes among the 6846 women with ER-positive disease, and side-eff ects among all women (with positive, negative, or unknown ER status). Long-term follow-up still continues. This study is registered, number ISRCTN19652633.
Findings Among women with ER-positive disease, allocation to continue tamoxifen reduced the risk of breast cancer recurrence (617 recurrences in 3428 women allocated to continue vs 711 in 3418 controls, p=0·002), reduced breast cancer mortality (331 deaths vs 397 deaths, p=0·01), and reduced overall mortality (639 deaths vs 722 deaths, p=0·01). The reductions in adverse breast cancer outcomes appeared to be less extreme before than after year 10 (recurrence rate ratio [RR] 0·90 [95% CI 0·79–1·02] during years 5–9 and 0·75 [0·62–0·90] in later years; breast cancer mortality RR 0·97 [0·79–1·18] during years 5–9 and 0·71 [0·58–0·88] in later years). The cumulative risk of recurrence during years 5–14 was 21·4% for women allocated to continue versus 25·1% for controls; breast cancer mortality during years 5–14 was 12·2% for women allocated to continue versus 15·0% for controls (absolute mortality reduction 2·8%). Treatment allocation seemed to have no eff ect on breast cancer outcome among 1248 women with ER-negative disease, and an intermediate eff ect among 4800 women with unknown ER status. Among all 12 894 women, mortality without recurrence from causes other than breast cancer was little aff ected (691 deaths without recurrence in 6454 women allocated to continue versus 679 deaths in 6440 controls; RR 0·99 [0·89–1·10]; p=0·84). For the incidence (hospitalisation or death) rates of specifi c diseases, RRs were as follows: pulmonary embolus 1·87 (95% CI 1·13–3·07, p=0·01 [including 0·2% mortality in both treatment groups]), stroke 1·06 (0·83–1·36), ischaemic heart disease 0·76 (0·60–0·95, p=0·02), and endometrial cancer 1·74 (1·30–2·34, p=0·0002). The cumulative risk of endometrial cancer during years 5–14 was 3·1% (mortality 0·4%) for women allocated to continue versus 1·6% (mortality 0·2%) for controls (absolute mortality increase 0·2%).
Interpretation For women with ER-positive disease, continuing tamoxifen to 10 years rather than stopping at 5 years produces a further reduction in recurrence and mortality, particularly after year 10. These results, taken together with results from previous trials of 5 years of tamoxifen treatment versus none, suggest that 10 years of tamoxifen treatment can approximately halve breast cancer mortality during the second decade after diagnosis.
Funding Cancer Research UK, UK Medical Research Council, AstraZeneca UK, US Army, EU-Biomed.
IntroductionFor women with oestrogen receptor (ER)-positive breast cancer, treatment for 5 years with adjuvant tamoxifen substantially reduces the rate of recurrence not only during the treatment period but throughout the fi rst
decade, and reduces breast cancer mortality by about a third throughout the fi rst 15 years (including years 10–14), with little net eff ect on other mortality.1 Although 5 years of tamoxifen is more eff ective than is 1–2 years of treat ment,1,2 whether 10 years of treatment
Published OnlineDecember 5, 2012http://dx.doi.org/10.1016/S0140-6736(12)61963-1
See Online/Commenthttp://dx.doi.org/10.1016/S0140-6736(12)62038-8
*Members listed at end of paper
Clinical Trial Service Unit and Epidemiological Studies Unit (CTSU), University of Oxford, UK (C Davies MBChB, H Pan PhD, Prof R Gray MSc, Prof R Collins FMedSci, A Delmestri PhD, Y Wang MD, Prof R Peto FRS); Glasgow Caledonian University, Glasgow, UK (J Godwin DPhil); Institut Gustave-Roussy, Villejuif, France (Prof R Arriagada MD); Institute Rotary Cancer Hospital, All-India Institute of Medical Sciences, New Delhi, India (Prof V Raina MD); Instituto Cardiovascular Rosario (ICR), Rosario, Argentina (M Abraham MD); Instituto do Cancer do Ceará (ICC), Fortaleza, Brazil (V H Medeiros Alencar MD); National Cancer Institute, Cairo University, Cairo, Egypt (Prof H Khaled MD, A Badran PhD); Sant Pau Biomedical Research Institute (IIB Sant Pau-CIBERESP), Barcelona, Spain (X Bonfi ll MD, S Tort MD, G Urrútia MD); School of Public Health and Preventive Medicine, Monash University, Melbourne, Victoria, Australia (Prof S R Davis MBBS, J Bradbury); Queens University, Belfast, UK (Prof M Clarke DPhil); Australia and New Zealand Breast Cancer Trials Group, University of Newcastle, Newcastle, NSW, Australia (Prof J F Forbes MD); Cancer Institute, Tehran University of Medical Sciences, Tehran, Iran (Prof P Haddad MD); Kaohsiung Medical University
Articles
www.thelancet.com Published online December 5, 2012 http://dx.doi.org/10.1016/S0140-6736(12)61963-1 1
Long-term eff ects of continuing adjuvant tamoxifen to 10 years versus stopping at 5 years after diagnosis of oestrogen receptor-positive breast cancer: ATLAS, a randomised trialChristina Davies, Hongchao Pan, Jon Godwin, Richard Gray, Rodrigo Arriagada, Vinod Raina, Mirta Abraham, Victor Hugo Medeiros Alencar, Atef Badran, Xavier Bonfi ll, Joan Bradbury, Michael Clarke, Rory Collins, Susan R Davis, Antonella Delmestri, John F Forbes, Peiman Haddad, Ming-Feng Hou, Moshe Inbar, Hussein Khaled, Joanna Kielanowska, Wing-Hong Kwan, Beela S Mathew, Bettina Müller, Antonio Nicolucci, Octavio Peralta, Fany Pernas, Lubos Petruzelka, Tadeusz Pienkowski, Balakrishnan Rajan, Maryna T Rubach, Sera Tort, Gerard Urrútia, Miriam Valentini, Yaochen Wang, Richard Peto, for the Adjuvant Tamoxifen: Longer Against Shorter (ATLAS) Collaborative Group*
SummaryBackground For women with oestrogen receptor (ER)-positive early breast cancer, treatment with tamoxifen for 5 years substantially reduces the breast cancer mortality rate throughout the fi rst 15 years after diagnosis. We aimed to assess the further eff ects of continuing tamoxifen to 10 years instead of stopping at 5 years.
Methods In the worldwide Adjuvant Tamoxifen: Longer Against Shorter (ATLAS) trial, 12 894 women with early breast cancer who had completed 5 years of treatment with tamoxifen were randomly allocated to continue tamoxifen to 10 years or stop at 5 years (open control). Allocation (1:1) was by central computer, using minimisation. After entry (between 1996 and 2005), yearly follow-up forms recorded any recurrence, second cancer, hospital admission, or death. We report eff ects on breast cancer outcomes among the 6846 women with ER-positive disease, and side-eff ects among all women (with positive, negative, or unknown ER status). Long-term follow-up still continues. This study is registered, number ISRCTN19652633.
Findings Among women with ER-positive disease, allocation to continue tamoxifen reduced the risk of breast cancer recurrence (617 recurrences in 3428 women allocated to continue vs 711 in 3418 controls, p=0·002), reduced breast cancer mortality (331 deaths vs 397 deaths, p=0·01), and reduced overall mortality (639 deaths vs 722 deaths, p=0·01). The reductions in adverse breast cancer outcomes appeared to be less extreme before than after year 10 (recurrence rate ratio [RR] 0·90 [95% CI 0·79–1·02] during years 5–9 and 0·75 [0·62–0·90] in later years; breast cancer mortality RR 0·97 [0·79–1·18] during years 5–9 and 0·71 [0·58–0·88] in later years). The cumulative risk of recurrence during years 5–14 was 21·4% for women allocated to continue versus 25·1% for controls; breast cancer mortality during years 5–14 was 12·2% for women allocated to continue versus 15·0% for controls (absolute mortality reduction 2·8%). Treatment allocation seemed to have no eff ect on breast cancer outcome among 1248 women with ER-negative disease, and an intermediate eff ect among 4800 women with unknown ER status. Among all 12 894 women, mortality without recurrence from causes other than breast cancer was little aff ected (691 deaths without recurrence in 6454 women allocated to continue versus 679 deaths in 6440 controls; RR 0·99 [0·89–1·10]; p=0·84). For the incidence (hospitalisation or death) rates of specifi c diseases, RRs were as follows: pulmonary embolus 1·87 (95% CI 1·13–3·07, p=0·01 [including 0·2% mortality in both treatment groups]), stroke 1·06 (0·83–1·36), ischaemic heart disease 0·76 (0·60–0·95, p=0·02), and endometrial cancer 1·74 (1·30–2·34, p=0·0002). The cumulative risk of endometrial cancer during years 5–14 was 3·1% (mortality 0·4%) for women allocated to continue versus 1·6% (mortality 0·2%) for controls (absolute mortality increase 0·2%).
Interpretation For women with ER-positive disease, continuing tamoxifen to 10 years rather than stopping at 5 years produces a further reduction in recurrence and mortality, particularly after year 10. These results, taken together with results from previous trials of 5 years of tamoxifen treatment versus none, suggest that 10 years of tamoxifen treatment can approximately halve breast cancer mortality during the second decade after diagnosis.
Funding Cancer Research UK, UK Medical Research Council, AstraZeneca UK, US Army, EU-Biomed.
IntroductionFor women with oestrogen receptor (ER)-positive breast cancer, treatment for 5 years with adjuvant tamoxifen substantially reduces the rate of recurrence not only during the treatment period but throughout the fi rst
decade, and reduces breast cancer mortality by about a third throughout the fi rst 15 years (including years 10–14), with little net eff ect on other mortality.1 Although 5 years of tamoxifen is more eff ective than is 1–2 years of treat ment,1,2 whether 10 years of treatment
Published OnlineDecember 5, 2012http://dx.doi.org/10.1016/S0140-6736(12)61963-1
See Online/Commenthttp://dx.doi.org/10.1016/S0140-6736(12)62038-8
*Members listed at end of paper
Clinical Trial Service Unit and Epidemiological Studies Unit (CTSU), University of Oxford, UK (C Davies MBChB, H Pan PhD, Prof R Gray MSc, Prof R Collins FMedSci, A Delmestri PhD, Y Wang MD, Prof R Peto FRS); Glasgow Caledonian University, Glasgow, UK (J Godwin DPhil); Institut Gustave-Roussy, Villejuif, France (Prof R Arriagada MD); Institute Rotary Cancer Hospital, All-India Institute of Medical Sciences, New Delhi, India (Prof V Raina MD); Instituto Cardiovascular Rosario (ICR), Rosario, Argentina (M Abraham MD); Instituto do Cancer do Ceará (ICC), Fortaleza, Brazil (V H Medeiros Alencar MD); National Cancer Institute, Cairo University, Cairo, Egypt (Prof H Khaled MD, A Badran PhD); Sant Pau Biomedical Research Institute (IIB Sant Pau-CIBERESP), Barcelona, Spain (X Bonfi ll MD, S Tort MD, G Urrútia MD); School of Public Health and Preventive Medicine, Monash University, Melbourne, Victoria, Australia (Prof S R Davis MBBS, J Bradbury); Queens University, Belfast, UK (Prof M Clarke DPhil); Australia and New Zealand Breast Cancer Trials Group, University of Newcastle, Newcastle, NSW, Australia (Prof J F Forbes MD); Cancer Institute, Tehran University of Medical Sciences, Tehran, Iran (Prof P Haddad MD); Kaohsiung Medical University

"#$!%$&'$('!)*+#,&!-#$.+*!"/01',(20!�!-#$.+*!34+*#1/!#$5!6+,+#*.4!-+$&+*!#&!73!8+#9&4!".(+$.+!-+$&+*!�!:+.+0;+*!<=>?!@AB@!34(,!1*+,+$&#&('$!(,!&4+!($&+99+.&2#9!1*'1+*&/!'C!%3D%"E!!-'$&#.&!!%3D%"F-3"7E'GE#.E2H!!C'*!1+*0(,,('$!&'!*+1*'52.+!'*!5(,&*(;2&+E!
%!"#!$4%O`PO%X/.3,J%=>?J%9:%*7%;%<3+67%-+./0123,%%%%%%%%%%%%%%%%%%%%%%>=H[>>=aH=%%%%%%%%%%%%%%%%%%%%%%%%%%%%%G>=!$"%H!aH=>%]b>"!#Z"c%

Articles
www.thelancet.com Published online December 5, 2012 http://dx.doi.org/10.1016/S0140-6736(12)61963-1 7
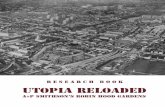
Number of events Log-rank O – E Variance of O – E Event rate ratio (95% CI) p value*
Continue tamoxifen to 10 years
Stop tamoxifen at 5 years
Mortality analyses, by ER status
ER-positive (3428 vs 3418)†
Any death 639 722 –47·7 340·2 0·87 (0·78–0·97) 0·01
Death with recurrence 331 397 –32·9 182·0 0·83 (0·72–0·96) 0·01
Death without recurrence 308 325 –14·8 158·1 0·91 (0·78–1·06) 0·24
ER unknown (2401 vs 2399)†
Any death 625 635 –10·5 314·6 0·97 (0·87–1·08) 0·55
Death with recurrence 302 334 –18·4 158·7 0·89 (0·76–1·04) 0·15
Death without recurrence 323 301 7·9 155·9 1·05 (0·90–1·23) 0·53
ER-negative (625 vs 623)†
Any death 123 116 3·5 59·7 1·06 (0·82–1·37) 0·66
Death with recurrence 63 63 0·0 31·5 1·00 (0·71–1·42) 0·99
Death without recurrence 60 53 3·4 28·2 1·13 (0·78–1·63) 0·52
Any ER status (6454 vs 6440)†
Any death 1387 1473 –54·7 714·5 0·93 (0·86–1·00) 0·04
Death with recurrence 696 794 –50·9 372·2 0·87 (0·79–0·97) 0·008
Death without recurrence‡ 691 679 –3·8 342·3 0·99 (0·89–1·10) 0·84
Analyses of events without prior recurrence‡, any ER status
Death without recurrence
Vascular death
Stroke 62 59 0·8 30·2 1·03 (0·72–1·46) 0·89
Pulmonary embolus 10 8 0·8 4·5 1·21 (0·48–3·04) 0·69
Heart disease§ 178 205 –16·1 95·7 0·85 (0·69–1·03) 0·10
Neoplastic death
Endometrial cancer¶ 17 11 2·8 7·0 1·49 (0·71–3·13) 0·29
Other neoplastic disease 78 75 0·4 38·2 1·01 (0·74–1·39) 0·94
Other death
Specifi ed cause 171 161 2·3 82·9 1·03 (0·83–1·28) 0·80
Unspecifi ed cause 175 160 5·1 83·7 1·06 (0·86–1·32) 0·58
Second cancer incidence
Contralateral breast cancer 419 467 –28·9 221·5 0·88 (0·77–1·00) 0·05
Endometrial cancer¶ 116 63 24·8 44·8 1·74 (1·30–2·34) 0·0002
Primary liver cancer 3 3 –0·0 1·5 0·99 (0·20–4·90) 0·99
Colorectal cancer 46 52 –3·8 24·5 0·86 (0·58–1·27) 0·44
Unspecifi ed site 254 251 –1·3 126·2 0·99 (0·83–1·18) 0·91
Non-neoplastic disease (ever hospitalised or died)
Stroke 130 119 3·8 62·2 1·06 (0·83–1·36) 0·63
Pulmonary embolus 41 21 9·7 15·5 1·87 (1·13–3·07) 0·01
Ischaemic heart disease 127 63 –20·2 72·5 0·76 (0·60–0·95) 0·02
Gallstones 75 66 3·7 35·2 1·11 (0·80–1·54) 0·54
Cataract 72 63 3·5 33·7 1·11 (0·79–1·56) 0·54
Bone fracture 62 70 –4·9 33·0 0·86 (0·61–1·21) 0·39
The log-rank analyses of death with recurrence are done by subtraction of the log-rank analyses of death without recurrence from those of any death. If O – E is negative, its value is about half the number of events prevented; if V is its variance, event rate ratio is exp([O – E] / V). ER=oestrogen receptor. *Two-sided. †In parentheses: number of women allocated to continue tamoxifen vs number allocated to control. ‡Delay of recurrence by continuation of tamoxifen increases woman-years at risk before recurrence by about 3% in ER-positive disease; the log-rank analyses allow for this, but crude comparisons of total numbers of events before recurrence do not. §Mainly heart disease, but includes all vascular causes apart from stroke and pulmonary embolus. ¶Mainly endometrial adenocarcinoma, but includes all other uterine tumours apart from cervical cancer; analyses of uterine tumour incidence exclude women with hysterectomy recorded at trial entry.
Table 2: Eff ects of allocation (continue tamoxifen to 10 years vs stop at 5 years) on mortality with and without previous recurrence in each category of ER status at entry, and on various outcomes without previous recurrence in all women of any ER status

Articles
www.thelancet.com Published online December 5, 2012 http://dx.doi.org/10.1016/S0140-6736(12)61963-1 9
although the real fi nding is not the point estimate but the CI (which shows that the reduction could be as little as a third rather than a half).
However, both in trials of 5 years of tamoxifen1 and in ATLAS, there was a diff erence of only about 80% between the prevalence of tamoxifen use in the two treatment groups, so the estimates in table 3 are likewise of what would be seen in trials of 10 years of tamoxifen compared with no tamoxifen that had only about 80% compliance. The risk reduction achievable by full compliance with 10 years of tamoxifen should, therefore, be appreciably greater, strengthening the conclusion that breast cancer mortality during the second decade after diagnosis (or at least during years 10–14) can be approximately halved. Thus, good evidence now exists that 10 years of tamoxifen in ER-positive disease produces substantial reductions in rates of recurrence and in breast cancer mortality not only during the fi rst decade (while treatment continues) but also during the second decade (after it ends).
Continued follow-up of ATLAS will eventually yield further evidence about eff ects on breast cancer outcomes during the second decade after diagnosis. Before then, substantial additional information about events during the second decade will have been contributed by the other trials of continuing tamoxifen to 10 years versus stopping at 5 years (particularly aTTom, the UK counterpart of ATLAS, which reported little benefi t during years 5–9 but has not yet reported on outcomes during the second decade13). EBCTCG meta-analyses of ATLAS, aTTom, and the smaller trials will eventually clarify the eff ects on breast cancer outcomes 10–14 years after diagnosis (panel).
Tamoxifen produces favourable lipid profi le changes19–21 and the ATLAS results do suggest some protection against ischaemic heart disease. Because, however, no signifi cant protection against heart disease was seen in trials of tamoxifen versus no tamoxifen,1,2 the apparent reduction in ATLAS might be largely a chance fi nding (especially since the apparent protection was against events after the treatment period, and long-term follow-up of trials of cholesterol-lowering statin treatment fi nd little further benefi t after treatment ends22). Conversely, although the US Food and Drug Administration lists stroke as a possible side-eff ect,5,23 no apparent increase in stroke incidence or mortality was seen during the treatment period either in ATLAS or in the trials of 5 years of tamoxifen.1
However, defi nite long-term side-eff ects of tamoxifen do exist, which require longer follow-up and meta-analyses of all relevant trials for fi nal assessment. In both ATLAS and the trials of 5 years of tamoxifen versus no treatment,1,2 tamoxifen increases the incidence of endo-metrial cancer in postmenopausal women who had not had a hysterectomy before trial entry. Although there is little risk in premenopausal women, life-table calcu-lations for older women (together with allowance for the imperfect compliance with treatment allocations in trials) suggest that actual use of 5 years of adjuvant tamoxifen would produce an absolute 15 year endometrial
cancer risk of about 2–3%,1 and that use of 10 years rather than 5 years of tamoxifen would produce an additional risk by year 15 of about 2%.
The death rate from endometrial cancer was, however, only about a tenth of the incidence rate, suggesting that full compliance with 10 years of tamoxifen in post-menopausal women would produce a 15 year risk of a few per thousand of eventually dying from the excess of uterine cancer. This risk is greatly outweighed in ER-positive disease by the decrease in breast cancer mortality.
Panel: Research in context
Systematic reviewThe Early Breast Cancer Trialists’ Collaborative Group (EBCTCG) periodically reviews trials of adjuvant tamoxifen versus no tamoxifen in early breast cancer and of longer versus shorter tamoxifen durations. The EBCTCG’s meta-analyses1,2 show that, in oestrogen receptor (ER)-positive disease, 5 years of adjuvant tamoxifen substantially decreases breast cancer recurrence, breast cancer mortality, and overall mortality (despite small absolute increases in endometrial cancer and pulmonary embolus). Previous trials have not, however, answered the question of how 10 years of tamoxifen compares with only 5 years. Because the decrease in breast cancer mortality produced by 5 years of tamoxifen continues to be substantial for a decade after treatment ends (ie, throughout the fi rst 15 years after diagnosis), trials of 10 years versus 5 years of tamoxifen will need to be followed up for at least 15 years from diagnosis.
InterpretationThe Adjuvant Tamoxifen: Longer Against Shorter (ATLAS) trial, with a mean of 7·6 years of further follow-up after entry at year 5, shows that recurrence and breast cancer mortality during the second decade after diagnosis are reduced more eff ectively by 10 years of adjuvant tamoxifen than by 5 years. Although known side-eff ects were increased (at least in postmenopausal women) by longer treatment, the absolute reduction in breast cancer mortality was an order of magnitude greater than the absolute increase in mortality due to these side-eff ects. Taken together with the results from trials of 5 years of tamoxifen versus none, the results from ATLAS show that 10 years of eff ective endocrine therapy can approximately halve breast cancer mortality during years 10–14 after diagnosis. Longer follow-up of ATLAS (and a meta-analysis of all such trials) will be needed to assess the full benefi ts and hazards throughout the second decade.
A: eff ects in meta-analyses of the trials of 5 years of tamoxifen vs none1
(n=10 645)
B: eff ects in the ATLAS trial of continuing tamoxifen to 10 years vs stopping at 5 years (n=6846)
C: estimated eff ects in a trial of 10 years of tamoxifen vs none (product of A and B)
Recurrence
0–4 years 0·53 (0·48–0·57)* 1 0·53 (0·48–0·57)*
5–9 years 0·68 (0·60–0·78)* 0·90 (0·79–1·02) 0·61 (0·51–0·73)*
≥10 years 0·94 (0·79–1·12) 0·75 (0·62–0·90)† 0·70 (0·54–0·91)†
Breast cancer mortality
0–4 years 0·71 (0·62–0·80)* 1 0·71 (0·62–0·80)*
5–9 years 0·66 (0·58–0·75)* 0·97 (0·79–1·18) 0·64 (0·50–0·82)‡
≥10 years 0·73 (0·62–0·86)‡ 0·71 (0·58–0·88)§ 0·52 (0·40–0·68)*
(A) Trials of 5 years of tamoxifen (n=10 645; ~80% complied). (B) ATLAS trial of 10 years vs 5 years of tamoxifen (n=6846; ~80% diff erence in tamoxifen use [fi gure 2]). (C) Hypothetical trial of 10 years of tamoxifen vs none (with ~80% compliance). Two-sided p values in this table relate to particular time periods; values elsewhere combine all time periods. ER=oestrogen receptor. *p<0·00001. †p<0·01. ‡p=0·0001. §p=0·0016.
Table 3: Event rate ratios (95% CIs) in ER-positive disease, by time period from diagnosis

Relative effectiveness of letrozole compared with tamoxifen for
patients with lobular carcinoma in the BIG 1-98 trial
Otto Metzger Filho, Anita Giobbie-Hurder, Elizabeth Mallon, Giuseppe
Viale, Eric P. Winer, Beat Thürlimann, Richard D. Gelber, Marco Colleoni, Bent Ejlertsen, Hervé Bonnefoi, Alan S. Coates, Aron
Goldhirsch for the BIG 1-98 Collaborative Group

� Lobular carcinoma is mostly represented by Luminal A (low proliferative tumors) followed by Luminal B (high proliferative tumors) by gene expression profiling 1
1. Metzger et al. SABCS 2011 P01-02-05 2. Viale et al. JCO 2008
Background
� In a previous analysis of BIG 1-98 the magnitude of benefit of letrozole vs. tamoxifen was greater among patients with high proliferative tumors (determined by Ki 67 labeling index) 2
N = 183
Luminal A Luminal B HER2 Basal Normal
This presentation is the intellectual property of the author/presenter. Contact [email protected] for permission to reprint

2-Arm Option
Tamoxifen Letrozole
Letrozole Letrozole Tamoxifen
0 2 5 YEARS
A B C D
Tamoxifen
Tamoxifen Letrozole
A B
4-Arm Option
N=1,828 Enrolled
1998-2000
N=3,094 Enrolled
1999-2003
N=4,922
N=911 N=917
N=1548 N=1546
BIG 1-98 Analytic Cohort Postmenopausal HR+ BC
12-year update (Lancet Oncol 2011)
This presentation is the intellectual property of the author/presenter. Contact [email protected] for permission to reprint

Disease-free survival
This presentation is the intellectual property of the author/presenter. Contact [email protected] for permission to reprint

Luminal A
Luminal B
Disease-free survival
Interaction p-value 0.049
Interaction p-value
0.23
This presentation is the intellectual property of the author/presenter. Contact [email protected] for permission to reprint

Overall survival
This presentation is the intellectual property of the author/presenter. Contact [email protected] for permission to reprint

!
HERA TRIAL: 2 years versus 1 year of trastuzumab after adjuvant chemotherapy in women with HER2-positive early breast
cancer at 8 years of median follow-up

OBSERVATION n=1698
Women with locally determined HER2-positive invasive early breast cancer
Surgery + (neo)adjuvant CT � RT
Centrally confirmed IHC 3+ or FISH+ ������������
Randomization
1 year Trastuzumab 8 mg/kg 6 mg/kg 3 weekly schedule
n=1703
2 years Trastuzumab 8 mg/kg 6 mg/kg 3 weekly schedule
n=1701
After ASCO 2005, option of switch to Trastuzumab
HERA TRIAL DESIGN ACCRUAL 2001 2005 (N=5102)
CT, chemotherapy; RT, radiotherapy

BASELINE CHARACTERISTICS Trastuzumab Trastuzumab
1 Year 2 Years N=1552 N=1553
Nodal Status Any Nodal Status, neo-adjuvant chemo 10.7% 10.8%
Node-negative, adjuvant chemo 32.9% 32.8%
1-3 Nodes Positive, adjuvant chemo 29.3% 29.6%
��4 Nodes Positive, adjuvant chemo 27.1% 26.9%
Adjuvant Chemotherapy Regimen No Anthracyclines 6.1% 5.9%
Anthracyclines w/o Taxanes 68.5% 68.6%
Anthracyclines + Taxanes 25.5% 25.6%
HERA was a global trial with the exception of the United States

Dise
ase-
free
surv
ival
(%)
Years from randomization
89.1%
86.7% 81.0%
81.6% 75.8%
76.0%
DFS FOR 2 YEARS VS. 1 YEAR TRASTUZUMAB AT 8 YRS MFU
100
80
60
40
20
0 0 1 2 3 4 5 6 7 8 9
No. at risk Trastuzumab 2 years 1553 1553 1442 1361 1292 1223 1153 1051 633 194 Trastuzumab 1 year 1552 1552 1413 1319 1265 1214 1180 1071 649 205
Trastuzumab 1 year
Trastuzumab 2 years
Pts Events HR (2 vs 1) 95% CI p-value 2 years 1553 367 0.99 (0.85-1.14) 0.86 1 year 1552 367

Ove
rall
Surv
ival
(%)
Years from randomization No. at risk Trastuzumab 2 years 1553 1553 1525 1485 1438 1382 1317 1193 708 208 Trastuzumab 1 year 1552 1552 1513 1461 1413 1364 1329 1218 732 225
100
80
60
40
20
0 0 1 2 3 4 5 6 7 8 9
OS FOR 2 YEARS VS. 1 YEAR TRASTUZUMAB AT 8 YRS MFU
97.4%
96.5% 91.4%
92.6% 86.4%
87.6%
Trastuzumab 1 year
Trastuzumab 2 years
Pts Events HR (2 vs 1) 95% CI p-value 2 years 1553 196 1.05 (0.86-1.28) 0.63 1 year 1552 186

CUMULATIVE INCIDENCE OF CARDIAC ENDPOINTS*
* Competing risk analysis with disease-free survival events considered as competing risks The majority of cardiac events are reversible (Procter et al. JCO 2010)
No. at risk Trastuzumab 2 years 1673 1533 1423 1345 1276 1207 1137 1038 637 186
Trastuzumab 1 year 1682 1536 1399 1306 1254 1203 1169 1063 659 203
Primary or Secondary
1673 1466 1323 1248 1182 1116 1047 952 589 171
1682 1488 1350 1257 1206 1158 1125 1017 629 190
Prob
abili
ty
Years from randomization
0.15
0.10
0.05
0.00 0 1 2 3 4 5 6 7 8 9
Trastuzumab 1 year Trastuzumab 2 years
Prob
abili
ty
Years from randomization
0.15
0.10
0.05
0.00 0 1 2 3 4 5 6 7 8 9
Trastuzumab 1 year Trastuzumab 2 years
Primary

Trastuzumab plus Adjuvant Chemotherapy for HER2-positive
Breast Cancer: Final Planned Joint Analysis of Overall Survival from NSABP B-31 and NCCTG N9831
EH Romond1,2, VJ Suman3, J-H Jeong1,4, GW Sledge, Jr.5, CE Geyer, Jr.1,6, S Martino7, P Rastogi1,8, J Gralow9, SM Swain1,10,
E Winer11, G Colon-Otero12, C Hudis13, S Paik1, N Davidson8, EP Mamounas14, JA Zujewski15, N Wolmark16, EA Perez12
1National Surgical Adjuvant Breast and Bowel Project Operations and Biostatistical Centers; 2University
of Kentucky; 3Mayo Clinic; 4Department of Biostatistics, University of Pittsburgh Graduate School of Public Health; 5IU Simon Cancer Center; 6University of Texas Southwestern Medical Center;
7The Angeles Clinic and Research Institute; 8University of Pittsburgh Cancer Institute; 9University of Washington; 10Medstar Washington Hospital Center; 11Dana-Farber Cancer Institute; 12Mayo Clinic, Jacksonville; 13Memorial Sloan-Kettering Cancer Center; 14Aultman Hospital; 15Division of Cancer Therapy and Diagnosis, Cancer Therapy Evaluation Program, National Cancer Institute, National
Institutes of Health, DHHS; 16Allegheny Cancer Center Allegheny General Hospital
San Antonio Breast Cancer Symposium � December 4-8, 2012 Abstract #S5-5

NSABP B-31
NCCTG N9831
Arm 1 Arm 2
Arm A
Arm B Arm C
= doxorubicin/cyclophosphamide (AC) 60/600 mg/m2 q 3 wk x 4 = paclitaxel (P) 175 mg/m2 q 3 wk x 4 = paclitaxel (P) 80 mg/m2/wk x 12 = trastuzumab (H) 4mg/kg LD + 2 mg/kg/wk x 51

Joint Statistical Analysis
� Median follow-up: 8.4 years � Data lock: 15 Sept 2012
� Primary endpoint: DFS � analyzed by intent-to-treat
� Secondary endpoint: OS � analyzed by intent-to-treat
� First interim analysis occurred in 2005 after 355 DFS events
� Definitive survival analysis at 710 OS events

� 102 women (5%) assigned to the treatment arm did not receive trastuzumab because of cardiac symptoms or decrease in LVEF that precluded initiation of the antibody. These are included in the trastuzumab arm in the ITT analysis.
� 413 women (20.4%) assigned to the control arm received trastuzumab after the first interim analysis reported positive results in 2005. These are included in the control arm in the ITT analysis.

N9831/B-31 Disease-Free Survival
2028 1959 1848 1747 1675 1611 1514 1293 910 619 350 2018 1887 1689 1529 1423 1329 1232 1027 705 449 255
% E
vent
-Fre
e
Years from Randomization No. at risk
AC � P
AC � P+H
N Events ��������������������� ����� ������������
HRadj=0.60 (95% CI: 0.53-0.68) P<0.0001
62.2%
73.7%
64.9%
76.8% 81.4%
69.5%
11.5%
San Antonio Breast Cancer Symposium, December 4-8, 2012

B-31/N9831 Overall Survival
2028 1995 1959 1897 1843 1785 1709 1506 1085 735 439 2018 1962 1883 1806 1730 1640 1534 1336 944 604 353
Years from Randomization
% S
urvi
val
No. at risk
AC � P
AC � P+H 84.0% 87.0%
89.8%
75.2% 79.4%
84.3%
HRadj=0.63 (95% CI 0.54-0.73) P<0.0001
N Events ���������������������� �������������������
90.3%
93.2%
���� ���� ���� ����
8.8%
San Antonio Breast Cancer Symposium, December 4-8, 2012

OS According to Subgroups ACTH vs. ACT (reference group)
Factor N No. of Events ACT ACTH HR
<40 years 40-49 50-59 60+ years ER- and PR- ER+ or PR+ 0-2cm 2.1-5.0cm 5.1cm+ LN 0 LN 1-3 LN 4-9 LN 10+ Good Intermediate Poor
654 1373 1336
683 1828 2215 1598 2096
345 282
2144 1084
536 76
1123 2801
65 121 129 103 212 206 129 239 50 11
161 133 113
8 108 299
45 87 90 64
149 137 67
176 42
9 104 103 70
1 59
219
0.67 0.65 0.68 0.51 0.65 0.61 0.51 0.68 0.58 0.94 0.59 0.72 0.56 0.11 0.52 0.67
HR with 95% CI
0.5 1 1.5 2
Age
Hormone Receptor Tumor Size
Nodal Status
Histologic Grade
0.0






San Antonio Breast Cancer Symposium, Cancer Therapy and Research Center at UT Health Science Center � December 4�8, 2012
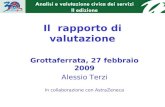
Primary results of BEATRICE, a randomized phase III trial evaluating
adjuvant bevacizumab-containing therapy in triple-negative breast cancer
D Cameron1, J Brown2, R Dent3, C Jackisch4, J Mackey5, X Pivot6, G Steger7, T Suter8, M Toi9, M Parmar10,
L Bubuteishvili-Pacaud11, V Henschel11, R Laeufle11, R Bell12
1University of Edinburgh and NHS Lothian, Edinburgh, UK; 2University of Leeds, Leeds, UK; 3Sunnybrook Health Sciences Center and University of Toronto, Toronto,
ON, Canada and National Cancer Center, Singapore, Singapore; 4Klinikum Offenbach, Offenbach, Germany; 5Cross Center Institute, Edmonton, Canada;
6University Hospital Jean Minjoz, Besançon, France; 7Medical University of Vienna, Vienna, Austria; 8Bern University Hospital, Inselspital, Switzerland; 9Kyoto University, Kyoto, Japan; 10MRC Clinical Trials Unit, London, UK; 11F Hoffmann-La Roche Ltd,
Basel, Switzerland; 12Andrew Love Cancer Centre, Geelong, Australia

San Antonio Breast Cancer Symposium, Cancer Therapy and Research Center at UT Health Science Center � December 4�8, 2012
Copyrights for this presentation are held by the author/presenter. Contact [email protected] for permission to reprint and/or distribute
BEATRICE: Randomized open-label multicenter phase III trial
Stratification factors: � Axillary nodal status (0 vs 1�3 vs ��) � Adjuvant chemotherapy (anthracycline vs
taxane vs anthracycline + taxane) � Hormone receptor status (negative vs low) � Surgery (breast-conserving vs mastectomy)
Resected triple-negativea
(centrally confirmed) invasive early breast
cancer (N=2591)
� ���������������������standard CT (4�8 cycles)
BEV (5 mg/kg/wk equivalent)
7
BEV monotherapy (total duration 1 year)
Chemotherapy options: � Taxane based (���������� � Anthracycline based (���������� � Anthracycline + taxane (3�4 cycles
each)
aHER2-negative and hormone receptor negative or low (total Allred score of 2 or 3; intensity score 1, proportion score 1 or 2)
� ���������������������standard CT (4�8 cycles)
Observation

San Antonio Breast Cancer Symposium, Cancer Therapy and Research Center at UT Health Science Center December 48, 2012
Copyrights for this presentation are held by the author/presenter. Contact [email protected] for permission to reprint and/or distribute
Primary endpoint: IDFSa 1.0
0.8
0.6
0.4
0.2
0
No. at risk: CT + BEV 1301 1244 1193 1129 1058 814 409 122 4 0 CT 1290 1221 1151 1086 994 772 383 105 2 0
0 6 12 18 24 30 36 42 48 54 Time (months)
Est
imat
ed p
roba
bilit
y
CT (N=1290)
CT + BEV (N=1301)
Median duration of follow-up, months 31.5 32.0 Events, n (%) 205 (15.9) 188 (14.5) 3-year IDFS rate, % (95% CI)
82.7 ���������
83.7 ���������
Stratified HR (95% CI) Log-rank p-value
0.87 (0.72���07)
0.1810
aIntent to treat, not censored for non-protocol therapy

San Antonio Breast Cancer Symposium, Cancer Therapy and Research Center at UT Health Science Center � December 4�8, 2012
Copyrights for this presentation are held by the author/presenter. Contact [email protected] for permission to reprint and/or distribute
Interim OS (59% of required events)
1.0
0.8
0.6
0.4
0.2
0
No. at risk: CT + BEV 1301 1264 1234 1196 1130 863 443 128 4 0 CT 1290 1248 1215 1169 1087 831 424 113 4 0
0 6 12 18 24 30 36 42 48 54 Time (months)
Est
imat
ed p
roba
bilit
y
CT (N=1290)
CT + BEV (N=1301)
Events, n (%) 107 (8.3) 93 (7.1) Stratified HR (95% CI) Log-rank p-value
0.84 (0.64�����)
0.2318

San Antonio Breast Cancer Symposium, Cancer Therapy and Research Center at UT Health Science Center � December 4�8, 2012
Copyrights for this presentation are held by the author/presenter. Contact [email protected] for permission to reprint and/or distribute
���������������������� ����� by treatment phase
AE, No. of patients (%)
Chemotherapy phase Observation or single-agent BEV phase
CT (N=1271)
CT + BEV (N=1288)
CT (N=1271)
CT + BEV (N=1288)
All grade ���AESIs 33 (3) 143 (11) 12 (<1) 122 (9) ATE 2 (<1) 2 (<1) 1 (<1) 4 (<1) VTE 15 (1) 21 (2) 4 (<1) 1 (<1) Bleeding 2 (<1) 8 (<1) 2 (<1) 0 CHF/LVD 3 ( <1) 12 (<1) 1 (<1) 24 (2) Hypertension 6 (<1) 88 (7) 4 (<1) 70 (5) Fistula/abscess 2 (<1) 0 0 1 (<1) Gastrointestinal perforation 0 6 (<1) 0 0 Proteinuria 1 (<1) 8 (<1) 0 24 (2) RPLS 0 1 (<1) 0 1 (<1) Wound-healing complication 3 (<1) 3 (<1) 0 1 (<1)
ATE = arterial thromboembolic event; CHF = congestive heart failure; LVD = left ventricular dysfunction; RPLS = reversible posterior leukoencephalopathy syndrome; VTE = venous thromboembolic event.

San Antonio Breast Cancer Symposium, Cancer Therapy and Research Center at UT Health Science Center � December 4�8, 2012
Copyrights for this presentation are held by the author/presenter. Contact [email protected] for permission to reprint and/or distribute
Conclusions
� First randomized phase III trial specifically in early TNBC � 3-year IDFS better than anticipated
� BEATRICE demonstrated no statistically significant improvement in invasive DFS with the addition of ������������������������ ������� � IDFS HR = 0.87 (95% CI: 0.72���07; p=0.1810)
� Adverse events overall consistent with the established safety profile in mBC1
1Cortes J, et al. Ann Oncol 2012 mBC = metastatic breast cancer

!"#$%#&'#('$)*+",&$-"#.+*$!/01',(20$ 3+.+04+*$5678$9:;9$
<=(,$1*+,+#&"&('#$(,$&=+$(#&+>>+.&2">$1*'1+*&/$'?$&=+$"2&='*@1*+,+#&+*A$-'#&".&$,&+?"#A"+4(B'#C'>'D(+A.=$?'*$1+*0(,,('#$&'$*+1*(#&$"#E@'*$E(,&*(42&+A$
-=+0'&=+*"1/$F*'>'#D,$!2*G(G">$?'*$H,'>"&+E$I'.">$'*$J+D('#">$J+.2**+#.+$'?$)*+",&$-"#.+*K$<=+$-%ILJ$<*(">
!A$%+4(8 !A$M+>4+*8$HA$IN#D8$!AOA$%#E+*,'#8$%A$J'4(E'2P8$QA$Q"*&R#8$OASAJA$T'*&(+*8$UAFA$Q"0'2#",8$-AUA$M+/+*8$O*A8$JA$Q"(4".=8$JA3A$M+>4+*8$TA$S'>0"*C8$HA$S"1#(*8$?'* &=+$!"#$% <*(">$H#G+,&(D"&'*,
!=+0'&=+*"1/$",$"EV2G"#&$?'*$#$.">>/ %+.2**+#&$)*+",&$-"#.+*AH)-!M$ ��� ������������������:9$W)LLM8$MUH-%Q8$H)-!MX

!"#$%#&'#('$)*+",&$-"#.+*$!/01',(20$� 3+.+04+*$5678$9:;9$
<=(,$1*+,+#&"&('#$(,$&=+$(#&+>>+.&2">$1*'1+*&/$'?$&=+$"2&='*@1*+,+#&+*A$-'#&".&$,&+?"#A"+4(B'#C'>'D(+A.=$?'*$1+*0(,,('#$&'$*+1*(#&$"#E@'*$E(,&*(42&+A$
������������U>(D(4(>(&/ -*(&+*("
� @0+,/)0*,072/-+27 7(.27)234A(+)+-B0(327)+-.:++-3.- 4*+",&$WH)<JX .=+,&$d">> 0",&+.&'0/$,."*$"#E@'*$,C(#$ "P(>>"*/ '* (#&+*#"> 0"00"*/ >/01= #'E+,
�!(5*7-/- B+(,,)-C.0,0(3 (8 +-.:++-3.- T+D"&(G+$'* 0(.*',.'1(.">>/ (#G'>G+E 0"*D(#,
�'( -104-3.- (8 ,:*+2.7210.:72+ 7<5*; 3(4-,�'( -104-3.- (8 40,/23/ 5-/2,/2,0,

!"#$%#&'#('$)*+",&$-"#.+*$!/01',(20$� 3+.+04+*$5678$9:;9$
<=(,$1*+,+#&"&('#$(,$&=+$(#&+>>+.&2">$1*'1+*&/$'?$&=+$"2&='*@1*+,+#&+*A$-'#&".&$,&+?"#A"+4(B'#C'>'D(+A.=$?'*$1+*0(,,('#$&'$*+1*(#&$"#E@'*$E(,&*(42&+A$
-%ILJ$<*(">
DE%FG%H
D/+2/2
� F*('*$-=+0'6<P� UJ`$"#E@'* FJ`� I'."&('#$HIJJ
%"'I$J&KG
'(.;-5(/;-+2*<
!;-5(/;-+2*< L G34(.+03- /;-+2*<8(+ G%L)234A(+ M%L)
L NG%OP40+-./-4)/;-+2*< Q(*/0(327R
� !;-5(/;-+2*< .;(,-3 =< 031-,/0B2/(+,%-.(55-342/0(3������4+:B,S)>)/( T)5(3/;, (8 /;-+2*<

!"#$%#&'#('$)*+",&$-"#.+*$!/01',(20$� 3+.+04+*$5678$9:;9$
<=(,$1*+,+#&"&('#$(,$&=+$(#&+>>+.&2">$1*'1+*&/$'?$&=+$"2&='*@1*+,+#&+*A$-'#&".&$,&+?"#A"+4(B'#C'>'D(+A.=$?'*$1+*0(,,('#$&'$*+1*(#&$"#E@'*$E(,&*(42&+A$
!&"&(,&(.">$-'#,(E+*"&('#,
�L*(D(#">$,"01>+$,(b+$?'*$fJ$\$:A^5Z^^$1"&(+#&,8$[5^$3Y!$+G+#&,$� I'd$"..*2">$*"&+
� T+d+*8$0'*+$+??+.&(G+$.=+0'&=+*"1(+,
�%0+#E0+#&$[8$9::7KJ+G(,+E$,"01>+$,(b+$?'*$fJ$\$:A_9_c$1"&(+#&,8$;95$+G+#&,� c6/+"*$3Y!$?'*$&=+$'4,+*G"&('#$D*'21K$c:g
� ;6� \$:A78$>'D*"#C � \$:A:c8$;$(#&+*(0 "#">/,(,

!"#$%#&'#('$)*+",&$-"#.+*$!/01',(20$� 3+.+04+*$5678$9:;9$
<=(,$1*+,+#&"&('#$(,$&=+$(#&+>>+.&2">$1*'1+*&/$'?$&=+$"2&='*@1*+,+#&+*A$-'#&".&$,&+?"#A"+4(B'#C'>'D(+A.=$?'*$1+*0(,,('#$&'$*+1*(#&$"#E@'*$E(,&*(42&+A$
!&"&(,&(.">$-'#,(E+*"&('#,
� O"#2"*/$[;8$9:;:->',2*+$'?$&=+$&*(">$d(&=$;_9$1"&(+#&,8$#'$(#&+*(0$"#">/,(,
�%#">/,(,$1>"#$W%1*(>8$9:;:X�����������$"+,(+)"-./)$(.+01(-+$1(+&(.2'-+3"44"0+/!+5(')1(#+3"/5+*('5#+02$1+'+&2-2&/&+3"44"0+/!+"3+678+*('5#�

!"#$%#&'#('$)*+",&$-"#.+*$!/01',(20$� 3+.+04+*$5678$9:;9$
<=(,$1*+,+#&"&('#$(,$&=+$(#&+>>+.&2">$1*'1+*&/$'?$&=+$"2&='*@1*+,+#&+*A$-'#&".&$,&+?"#A"+4(B'#C'>'D(+A.=$?'*$1+*0(,,('#$&'$*+1*(#&$"#E@'*$E(,&*(42&+A$
���������� �3(,+",+6?*++ !2*G(G">

!"#$%#&'#('$)*+",&$-"#.+*$!/01',(20$� 3+.+04+*$5678$9:;9$
<=(,$1*+,+#&"&('#$(,$&=+$(#&+>>+.&2">$1*'1+*&/$'?$&=+$"2&='*@1*+,+#&+*A$-'#&".&$,&+?"#A"+4(B'#C'>'D(+A.=$?'*$1+*0(,,('#$&'$*+1*(#&$"#E@'*$E(,&*(42&+A$
3Y!$UJ$!&"&2,
UJ` UJ6
i#(G"*("&+ H#&+*".&('#$&+*0K$<*+"&0+#&$P$UJK$F$\$:A:55$

!"#$%#&'#('$)*+",&$-"#.+*$!/01',(20$� 3+.+04+*$5678$9:;9$
<=(,$1*+,+#&"&('#$(,$&=+$(#&+>>+.&2">$1*'1+*&/$'?$&=+$"2&='*@1*+,+#&+*A$-'#&".&$,&+?"#A"+4(B'#C'>'D(+A.=$?'*$1+*0(,,('#$&'$*+1*(#&$"#E@'*$E(,&*(42&+A$
-%ILJ$<*("> ��LG+*">>$!2*G(G">

!"#$%#&'#('$)*+",&$-"#.+*$!/01',(20$� 3+.+04+*$5678$9:;9$
<=(,$1*+,+#&"&('#$(,$&=+$(#&+>>+.&2">$1*'1+*&/$'?$&=+$"2&='*@1*+,+#&+*A$-'#&".&$,&+?"#A"+4(B'#C'>'D(+A.=$?'*$1+*0(,,('#$&'$*+1*(#&$"#E@'*$E(,&*(42&+A$
-%ILJ$<*("> ��-'#.>2,('#,� %EV2G"#&$.=+0'&=+*"1/$*+E2.+E$&=+$*(,C$'?
� 3Y!$+G+#&,$4/$5;g$WUJ`$_gk$UJ6 _7gX
� 3+"&=$4/$cZg$WUJ`$_:gk$UJ6 c^gX
� %EV2G"#&$.=+0'&=+*"1/$,='2>E$4+$*+.'00+#E+E$?'*$1"&(+#&,$d(&=$.'01>+&+>/$*+,+.&+E$(,'>"&+E$>'.">$'*$*+D('#">$*+.2**+#.+$'?$4*+",&$."#.+*� <=+$E"&" "*+ ,&*'#D+,& ?'* 1"&(+#&, d(&=UJ6#+D"&(G+$*+.2**+#.+,
� I'#D+* ?'>>'d621 (, #++E+E ?'* 1"&(+#&, d(&=UJ61',(&(G+$*+.2**+#.+,

Azienda Sanitaria Firenze 48
Malattia metastatica

original article
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
n engl j med 366;6 nejm.org february 9, 2012520
Everolimus in Postmenopausal Hormone-Receptor–Positive Advanced Breast Cancer
José Baselga, M.D., Ph.D., Mario Campone, M.D., Ph.D., Martine Piccart, M.D., Ph.D., Howard A. Burris III, M.D., Hope S. Rugo, M.D.,
Tarek Sahmoud, M.D., Ph.D., Shinzaburo Noguchi, M.D., Michael Gnant, M.D., Kathleen I. Pritchard, M.D., Fabienne Lebrun, M.D., J. Thaddeus Beck, M.D.,
Yoshinori Ito, M.D., Denise Yardley, M.D., Ines Deleu, M.D., Alejandra Perez, M.D., Thomas Bachelot, M.D., Ph.D., Luc Vittori, M.Sc., Zhiying Xu, Ph.D., Pabak Mukhopadhyay, Ph.D., David Lebwohl, M.D.,
and Gabriel N. Hortobagyi, M.D.
From Massachusetts General Hospital Cancer Center, Harvard Medical School, Boston (J.B.); Institut de Cancérologie de l’Ouest/René Gaudu cheau, Nantes Saint Herblain, France (M.C.); Institute Jules Bordet, Brussels (M.P., F.L.); Sarah Can-non Research Institute, Nashville (H.A.B., D.Y.); University of California, San Francis-co, Helen Diller Family Comprehensive Cancer Center, San Francisco (H.S.R.); Novartis, East Hanover, NJ (T.S., Z.X., P.M., D.L.); Osaka University, Depart-ment of Breast and Endocrine Surgery, Osaka, Japan (S.N.); the Department of Surgery, Comprehensive Cancer Center, Medical University of Vienna, Vienna (M.G.); Sunnybrook Odette Cancer Cen-tre and the University of Toronto, Toronto (K.I.P.); Highlands Oncology Group, Fay-etteville, AR (J.T.B.); Cancer Institute Hos-pital of Japanese Foundation for Cancer Research, Ariake, Tokyo (Y.I.); Oncology Center, AZ Nikolass, Sint-Niklaas, Bel-gium (I.D.); Memorial Cancer Institute, Hollywood, FL (A.P.); Centre Léon-Bérard, Lyon, France (T.B.); Novartis Pharma, Ba-sel, Switzerland (L.V.); and the University of Texas M.D. Anderson Cancer Center, Houston (G.N.H.). Address reprint re-quests to Dr. Baselga at the Division of Hematology/Oncology, Massachusetts General Hospital Cancer Center, 55 Fruit St., Lawrence House 108, Boston, MA 02114, or at [email protected].
This article (10.1056/NEJMoa1109653) was published on December 7, 2011, and up-dated on December 13, 2011, at NEJM.org.
N Engl J Med 2012;366:520-9.Copyright © 2011 Massachusetts Medical Society.
A bs tr ac t
BackgroundResistance to endocrine therapy in breast cancer is associated with activation of the mammalian target of rapamycin (mTOR) intracellular signaling pathway. In early studies, the mTOR inhibitor everolimus added to endocrine therapy showed antitu-mor activity.MethodsIn this phase 3, randomized trial, we compared everolimus and exemestane versus exemestane and placebo (randomly assigned in a 2:1 ratio) in 724 patients with hor-mone-receptor–positive advanced breast cancer who had recurrence or progression while receiving previous therapy with a nonsteroidal aromatase inhibitor in the adjuvant setting or to treat advanced disease (or both). The primary end point was progression-free survival. Secondary end points included survival, response rate, and safety. A preplanned interim analysis was performed by an independent data and safety monitoring committee after 359 progression-free survival events were observed.ResultsBaseline characteristics were well balanced between the two study groups. The median age was 62 years, 56% had visceral involvement, and 84% had hormone-sensitive disease. Previous therapy included letrozole or anastrozole (100%), tamoxifen (48%), fulvestrant (16%), and chemotherapy (68%). The most common grade 3 or 4 adverse events were stomatitis (8% in the everolimus-plus-exemestane group vs. 1% in the placebo-plus-exemestane group), anemia (6% vs. <1%), dyspnea (4% vs. 1%), hyper-glycemia (4% vs. <1%), fatigue (4% vs. 1%), and pneumonitis (3% vs. 0%). At the interim analysis, median progression-free survival was 6.9 months with everolimus plus exemestane and 2.8 months with placebo plus exemestane, according to assess-ments by local investigators (hazard ratio for progression or death, 0.43; 95% confi-dence interval [CI], 0.35 to 0.54; P<0.001). Median progression-free survival was 10.6 months and 4.1 months, respectively, according to central assessment (hazard ratio, 0.36; 95% CI, 0.27 to 0.47; P<0.001).ConclusionsEverolimus combined with an aromatase inhibitor improved progression-free survival in patients with hormone-receptor–positive advanced breast cancer previously treated with nonsteroidal aromatase inhibitors. (Funded by Novartis; BOLERO-2 ClinicalTrials .gov number, NCT00863655.)
The New England Journal of Medicine Downloaded from nejm.org on November 21, 2012. For personal use only. No other uses without permission.
Copyright © 2012 Massachusetts Medical Society. All rights reserved.
original article
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
n engl j med 366;6 nejm.org february 9, 2012520
Everolimus in Postmenopausal Hormone-Receptor–Positive Advanced Breast Cancer
José Baselga, M.D., Ph.D., Mario Campone, M.D., Ph.D., Martine Piccart, M.D., Ph.D., Howard A. Burris III, M.D., Hope S. Rugo, M.D.,
Tarek Sahmoud, M.D., Ph.D., Shinzaburo Noguchi, M.D., Michael Gnant, M.D., Kathleen I. Pritchard, M.D., Fabienne Lebrun, M.D., J. Thaddeus Beck, M.D.,
Yoshinori Ito, M.D., Denise Yardley, M.D., Ines Deleu, M.D., Alejandra Perez, M.D., Thomas Bachelot, M.D., Ph.D., Luc Vittori, M.Sc., Zhiying Xu, Ph.D., Pabak Mukhopadhyay, Ph.D., David Lebwohl, M.D.,
and Gabriel N. Hortobagyi, M.D.
From Massachusetts General Hospital Cancer Center, Harvard Medical School, Boston (J.B.); Institut de Cancérologie de l’Ouest/René Gaudu cheau, Nantes Saint Herblain, France (M.C.); Institute Jules Bordet, Brussels (M.P., F.L.); Sarah Can-non Research Institute, Nashville (H.A.B., D.Y.); University of California, San Francis-co, Helen Diller Family Comprehensive Cancer Center, San Francisco (H.S.R.); Novartis, East Hanover, NJ (T.S., Z.X., P.M., D.L.); Osaka University, Depart-ment of Breast and Endocrine Surgery, Osaka, Japan (S.N.); the Department of Surgery, Comprehensive Cancer Center, Medical University of Vienna, Vienna (M.G.); Sunnybrook Odette Cancer Cen-tre and the University of Toronto, Toronto (K.I.P.); Highlands Oncology Group, Fay-etteville, AR (J.T.B.); Cancer Institute Hos-pital of Japanese Foundation for Cancer Research, Ariake, Tokyo (Y.I.); Oncology Center, AZ Nikolass, Sint-Niklaas, Bel-gium (I.D.); Memorial Cancer Institute, Hollywood, FL (A.P.); Centre Léon-Bérard, Lyon, France (T.B.); Novartis Pharma, Ba-sel, Switzerland (L.V.); and the University of Texas M.D. Anderson Cancer Center, Houston (G.N.H.). Address reprint re-quests to Dr. Baselga at the Division of Hematology/Oncology, Massachusetts General Hospital Cancer Center, 55 Fruit St., Lawrence House 108, Boston, MA 02114, or at [email protected].
This article (10.1056/NEJMoa1109653) was published on December 7, 2011, and up-dated on December 13, 2011, at NEJM.org.
N Engl J Med 2012;366:520-9.Copyright © 2011 Massachusetts Medical Society.
A bs tr ac t
BackgroundResistance to endocrine therapy in breast cancer is associated with activation of the mammalian target of rapamycin (mTOR) intracellular signaling pathway. In early studies, the mTOR inhibitor everolimus added to endocrine therapy showed antitu-mor activity.MethodsIn this phase 3, randomized trial, we compared everolimus and exemestane versus exemestane and placebo (randomly assigned in a 2:1 ratio) in 724 patients with hor-mone-receptor–positive advanced breast cancer who had recurrence or progression while receiving previous therapy with a nonsteroidal aromatase inhibitor in the adjuvant setting or to treat advanced disease (or both). The primary end point was progression-free survival. Secondary end points included survival, response rate, and safety. A preplanned interim analysis was performed by an independent data and safety monitoring committee after 359 progression-free survival events were observed.ResultsBaseline characteristics were well balanced between the two study groups. The median age was 62 years, 56% had visceral involvement, and 84% had hormone-sensitive disease. Previous therapy included letrozole or anastrozole (100%), tamoxifen (48%), fulvestrant (16%), and chemotherapy (68%). The most common grade 3 or 4 adverse events were stomatitis (8% in the everolimus-plus-exemestane group vs. 1% in the placebo-plus-exemestane group), anemia (6% vs. <1%), dyspnea (4% vs. 1%), hyper-glycemia (4% vs. <1%), fatigue (4% vs. 1%), and pneumonitis (3% vs. 0%). At the interim analysis, median progression-free survival was 6.9 months with everolimus plus exemestane and 2.8 months with placebo plus exemestane, according to assess-ments by local investigators (hazard ratio for progression or death, 0.43; 95% confi-dence interval [CI], 0.35 to 0.54; P<0.001). Median progression-free survival was 10.6 months and 4.1 months, respectively, according to central assessment (hazard ratio, 0.36; 95% CI, 0.27 to 0.47; P<0.001).ConclusionsEverolimus combined with an aromatase inhibitor improved progression-free survival in patients with hormone-receptor–positive advanced breast cancer previously treated with nonsteroidal aromatase inhibitors. (Funded by Novartis; BOLERO-2 ClinicalTrials .gov number, NCT00863655.)
The New England Journal of Medicine Downloaded from nejm.org on November 21, 2012. For personal use only. No other uses without permission.
Copyright © 2012 Massachusetts Medical Society. All rights reserved.

• Refractory to letrozole or anastrozole defined as:– Disease recurrence while on therapy or within 12 months after end of treatment,
if letrozole or anastrozole received as adjuvant treatment or– Progression during therapy or within one month, if letrozole or anastrozole
received as treatment for advanced disease
Treatment until disease progression or unacceptable toxicity
Eligibility Criteria (N=724)• Postmenopausal ER+• Recurrence or
progression after letrozole or anastrozole
RAND
OM
IZAT
ION
(2:1
) EVE 10 mg PO daily +EXE 25 mg PO daily
(n=485)
Placebo PO daily +EXE 25 mg PO daily
(n=239)
Endpoints• PFS • OS• ORR• Clinical benefit
rate• Time to ECOG
PS deterioration• Safety• QoL
Stratification by• Sensitivity to prior endocrine therapy• Visceral metastases
Baselga J et al. N Engl J Med 2012;366:520-529
BOLERO-2: Phase III Trial of Exemestane���� Everolimus in ABC

Piccart-Gebhart M et al. Paper presented at: 2012 American Society of Clinical Oncology Annual Meeting; June 1-5, 2012; Chicago, IL.

BOLERO-2 (18-month follow-up): PFS in Subgroups
Piccart-Gebhart M et al. Paper presented at: 2012 American Society of Clinical Oncology Annual Meeting; June 1-5, 2012; Chicago, IL.

RESULTS'(con,nued)'
Abbrevia(ons:-CI,-confidence-interval;-EVE,-everolimus-(10-mg/day);-EXE,-exemestane-(25-mg/day);-HR,-hazard-ra(o;-PBO,-placebo;-PFS,-progressionPfree-survival.-
0'
20'
40'
60'
Progression:Free'Survival,'%'
Progression:Free'Survival,'%'
80'
100'
A' B'
Time,'wk' Time,'wk'0' 6' 12' 18' 24' 30' 36' 42' 48' 54' 60' 66' 72' 78' 84' 90' 96'102'108'114'
EVE'+'EXE'PBO'+'EXE'
EVE'+'EXE'PBO'+'EXE'
188/271'Events/Pa,ents'(n)'
116/135'
Number'of'Pa,ents'S,ll'at'Risk'
271'240' 192'157' 128' 107' 88' 72' 52' 38' 25' 22' 16' 12' 11' 7' 5' 4' 1' 0'135'108' 66' 44' 32' 23' 18' 14' 11' 8' 4' 4' 3' 1' 0' 0' 0' 0' 0' 0'
EVE'+'EXE'PBO'+'EXE'
6.83'months'
Median'PFS'
2.76'months'EVE'+'EXE'PBO'+'EXE'
HR'='0.47'(95%'CI'='0.37,'0.60)' HR'='0.41'(95%'CI'='0.31,'0.55)'
9.86'months'
Median'PFS'
4.21'months'
0'
20'
40'
60'
80'
100'
0' 6' 12' 18' 24' 30' 36' 42' 48' 54' 60' 66' 72' 78' 84' 90' 96'102'108'114'120'
EVE'+'EXE'PBO'+'EXE'
Number'of'Pa,ents'S,ll'at'Risk'214'196'174'147'129'114' 97' 86' 72' 53' 41' 28' 19' 12' 11' 6' 5' 4' 1' 1' 0'104' 82' 66' 52' 35' 27' 21' 16' 10' 7' 6' 4' 2' 2' 1' 1' 1' 0' 0' 0' 0'
Censoring'Times'
EVE'+'EXE'PBO'+'EXE'
122/214'Events/Pa,ents'(n)'
84/104'
Censoring'Times'
Figure'1.'Kaplan:Meier'curve'for'PFS'in'pa,ents'(A)'with'and'(B)'without''visceral'involvement.''
Campone et al ESMO 2012

RESULTS'(con,nued)'
0'
20'
40'
60'
80'
100'
Time,'wk'0' 6' 12' 18' 24' 30' 36' 42' 48' 54' 60' 66' 72' 78' 84' 90' 96' 102'108'
EVE'+'EXE'PBO'+'EXE'
Number'of'Pa,ents'S,ll'at'Risk'105' 95' 88' 75' 72' 65' 53' 47' 41' '30' '20' '13' 7' 6' 5' 3' 2' 1' 0'46' 35' 30' 24' 19' 14' 12' 10' 5' 3' 1' 1' 1' 0' 0' 0' 0' 0' 0'
Progression:Free'Survival,'%'
EVE'+'EXE'PBO'+'EXE'
48/105'Events/Pa,ents'(n)'
33/46'
EVE'+'EXE'PBO'+'EXE'
12.88'months'
Median'PFS'
5.29'months'
HR'='0.33'(95%'CI'='0.21,'0.53)'
Censoring'Times'
Figure'2.'Kaplan:Meier'curve'for'PFS'in'pa,ents'with'bone:only'metastases.-
Campone et al ESMO 2012

n engl j med 366;2 nejm.org january 12, 2012 109
The new england journal of medicineestablished in 1812 january 12, 2012 vol. 366 no. 2
Pertuzumab plus Trastuzumab plus Docetaxel for Metastatic Breast Cancer
José Baselga, M.D., Ph.D., Javier Cortés, M.D., Sung-Bae Kim, M.D., Seock-Ah Im, M.D., Roberto Hegg, M.D., Young-Hyuck Im, M.D., Laslo Roman, M.D., José Luiz Pedrini, M.D., Tadeusz Pienkowski, M.D.,
Adam Knott, Ph.D., Emma Clark, M.Sc., Mark C. Benyunes, M.D., Graham Ross, F.F.P.M., and Sandra M. Swain, M.D., for the CLEOPATRA Study Group*
A bs tr ac t
From the Massachusetts General Hospi-tal Cancer Center and Harvard Medical School, Boston (J.B.); the Vall d’Hebron Institute of Oncology, Barcelona (J.C.); the Department of Oncology, Asan Medi-cal Center, University of Ulsan College of Medicine (S.-B.K.), the Division of Hema-tology and Medical Oncology, Department of Internal Medicine, Seoul National Uni-versity College of Medicine (S.-A.I.), and the Division of Hematology and Medical Oncology, Department of Internal Medi-cine, Samsung Medical Center, Sung-kyunkwan University School of Medicine (Y.-H.I.) — all in Seoul, South Korea; Hospital Pérola Byington and Faculdade de Medicina da Universidade de São Paulo, São Paulo (R.H.); Leningrad Regional On-cology Dispensary, St. Petersburg, Russia (L.R.); Centro de Pesquisas Médicas e En-saios Clínicos–Mastology Unit of Conceição Hospital, Porto Alegre, Brazil (J.L.P.); Cen-trum Onkologii, Warsaw, Poland (T.P.); Roche, Welwyn, United Kingdom (A.K., E.C., G.R.); Genentech, South San Fran-cisco, CA (M.C.B.); and Washington Can-cer Institute, MedStar Washington Hospital Center, Washington, DC (S.M.S.). Address reprint requests to Dr. Baselga at the Mas-sachusetts General Hospital Cancer Center, 55 Fruit St., Lawrence House 108, Boston, MA 02114, or at [email protected].
*The investigators in the Clinical Evalua-tion of Pertuzumab and Trastuzumab (CLEOPATRA) study are listed in the Supplementary Appendix, available at NEJM.org.
This article (10.1056/NEJMoa1113216) was published on December 7, 2011, at NEJM .org.
N Engl J Med 2012;366:109-19.Copyright © 2011 Massachusetts Medical Society.
BackgroundThe anti–human epidermal growth factor receptor 2 (HER2) humanized monoclo-nal antibody trastuzumab improves the outcome in patients with HER2-positive met-astatic breast cancer. However, most cases of advanced disease eventually progress. Pertuzumab, an anti-HER2 humanized monoclonal antibody that inhibits receptor dimerization, has a mechanism of action that is complementary to that of trastuz-umab, and combination therapy with the two antibodies has shown promising ac-tivity and an acceptable safety profile in phase 2 studies involving patients with HER2-positive breast cancer.
MethodsWe randomly assigned 808 patients with HER2-positive metastatic breast cancer to receive placebo plus trastuzumab plus docetaxel (control group) or pertuzumab plus trastuzumab plus docetaxel (pertuzumab group) as first-line treatment until the time of disease progression or the development of toxic effects that could not be effectively managed. The primary end point was independently assessed pro-gression-free survival. Secondary end points included overall survival, progression-free survival as assessed by the investigator, the objective response rate, and safety.
ResultsThe median progression-free survival was 12.4 months in the control group, as com-pared with 18.5 months in the pertuzumab group (hazard ratio for progression or death, 0.62; 95% confidence interval, 0.51 to 0.75; P<0.001). The interim analysis of overall survival showed a strong trend in favor of pertuzumab plus trastuzumab plus docetaxel. The safety profile was generally similar in the two groups, with no increase in left ventricular systolic dysfunction; the rates of febrile neutropenia and diarrhea of grade 3 or above were higher in the pertuzumab group than in the control group.
ConclusionsThe combination of pertuzumab plus trastuzumab plus docetaxel, as compared with placebo plus trastuzumab plus docetaxel, when used as first-line treatment for HER2-positive metastatic breast cancer, significantly prolonged progression-free survival, with no increase in cardiac toxic effects. (Funded by F. Hoffmann–La Roche/Genen-tech; ClinicalTrials.gov number, NCT00567190.)
The New England Journal of Medicine Downloaded from nejm.org on November 21, 2012. For personal use only. No other uses without permission.
Copyright © 2012 Massachusetts Medical Society. All rights reserved.

CLEOPATRA: Study Design
Baselga J, et al. Cancer Res. 2011;71(24 Suppl):Abstract S5-5. Baselga J, et al. N Engl J Med. 2011 December 7. [Epub ahead of print].
MBC, metastatic breast cancer; PD, progressive disease
Patients with HER2-positive MBC centrally confirmed
(N = 808)
Placebo + trastuzumab n = 406
Randomization was stratified by geographic region and prior treatment status (neo/adjuvant chemotherapy received or not)
Study dosing q3w: � Pertuzumab/Placebo: 840 mg loading dose, 420 mg maintenance � Trastuzumab: 8 mg/kg loading dose, 6 mg/kg maintenance � Docetaxel: 75 mg/m2, escalating to 100 mg/m2 if tolerated
1:1
n = 402
Docetaxel* �������������������
PD
Pertuzumab + trastuzumab
Docetaxel* �������������������
PD
* <6 cycles allowed for unacceptable toxicity or PD; >6 cycles allowed at investigator discretion

clinicaloptions.com/oncology Optimal Testing and Treatment of Patients With HER2-Positive Breast Cancer
100 90 80 70 60 50 40 30 20 10
0
Patie
nts
With
out P
rogr
essi
on (%
)
Mos 0 5 10 15 20 25 30 35 40
Ptz + TH: 18.5 Pbo + TH: 12.4
HR: 0.62 (95% CI: 0.51-0.75; P < .0001)
Patients at Risk, n Ptz + TH
Pbo + TH 402 406
0 0
345 311
267 209
139 93
83 42
32 17
10 7
0 0
Median PFS, Mos
CLEOPATRA: Independently Assessed PFS
Baselga J, et al. N Engl J Med. 2012;366:109-119.

clinicaloptions.com/oncology Optimal Testing and Treatment of Patients With HER2-Positive Breast Cancer
Patient Subgroup Median PFS, Mos HR (95% CI) Placebo +
Trastuzumab + Docetaxel
Pertuzumab + Trastuzumab +
Docetaxel Previous (neo)adjuvant trastuzumab treatment (n = 88)
10.4 16.9 0.62 (0.35-1.07)
No previous (neo)adjuvant trastuzumab treatment (n = 288)
12.6 21.6 0.60 (0.43-0.83)
CLEOPATRA: PFS by Previous Trastuzumab Therapy
Baselga J, et al. N Engl J Med. 2012;366:109-119.

clinicaloptions.com/oncology Optimal Testing and Treatment of Patients With HER2-Positive Breast Cancer
1.5 1.5 3.8 8.3 14.6
20.8
74.6 65.2
5.5 4.2
0 10 20 30 40 50 60 70 80 90
100
Ptz + TH (n = 343)
Pbo + TH (n = 336)
CR PR SD PD Not evaluable
Patie
nts
(%)
ORR: 80.2%
ORR: 69.3%
CLEOPATRA: Response Rates
Baselga J, et al. N Engl J Med. 2012;366:109-119.

clinicaloptions.com/oncology Optimal Testing and Treatment of Patients With HER2-Positive Breast Cancer
0 5 10 15 20 25 30 35 40 45 0
10
20
30
40
50
60
70
80
90
100
Patients at Risk, n Ptz + TH 402 387 367 251 161 87 31 4 0 0
406 383 347 228 143 67 24 2 0 0 Pbo + TH
Mos
Ptz + TH
Pbo + TH
HR: 0.64 (95% CI: 0.47-0.88;
P = .005)
OS
(%)
Median follow-up: 19.3 mos
OS: Predefined Interim Analysis
Baselga J, et al. N Engl J Med 2012;366:109-119.

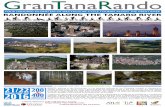
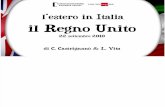
Structure of T-DM1 and mechanisms of action.
LoRusso P M et al. Clin Cancer Res 2011;17:6437-6447
©2011 by American Association for Cancer Research





!"#$%#&'#('$)*+",&$-"#.+*$!/01',(20$�$����������������� �������������$
34(,$1*+,+#&"&('#$(,$&4+$(#&+55+.&2"5$1*'1+*&/$'6$789-%:$"#;$7)7$
Phase III trial evaluating the addition of bevacizumab to endocrine therapy as first-line treatment for advanced breast cancer �
First efficacy results from the LEA study. Miguel Martin1*, Sibylle Loibl2*, Gunter von Minckwitz2, Serafín Morales3,Carmen Crespo4, Antonio Anton5, Ángel
Guerrero6, Bahriye Aktas7, Winfried Schoenegg8, Montserrat Muñoz9, José Ángel Garcia-Saenz10, Miguel Gil11, Manuel Ramos12, Eva Carrasco13, Cornelia Liedtke14, Grischa Wachsmann15, Keyur Mehta2, Juan R De la Haba16, On behalf of
GEICAM (Spanish Breast Cancer Research Group) and GBG (German Breast Group). *contributed equally
1Instituto de Investigación Sanitaria Gregorio Marañón, Madrid, Spain; 2GBG (German Breast Group), Neu-Isenburg, Germany; 3H.
Arnau Vilanova de Lérida, Spain; 4Hospital U. Ramón y Cajal, Spain; 5Hospital Universitario Miguel Servet, Spain; 6Instituto Valenciano de Oncología, Spain; 7University Women�s Hospital Essen, Germany; 8Medical Practice Berlin, Germany; 9Hospital
Clinic i Provincial, Spain; 10Hospital Clínico U. San Carlos, Spain; 11Instituto Catala d' Oncología Hospitalet, Spain; 12Centro Oncológico de Galicia, Spain; 13GEICAM (Spanish Breast Cancer Research Group), Spain; 14University Women�s Hospital
Muenster, Germany; 15Klinikum Boeblingen, Germany and 16Hospital U. Reina Sofía, Spain.

!"#$%#&'#('$)*+",&$-"#.+*$!/01',(20$�$����������������� �������������$
34(,$1*+,+#&"&('#$(,$&4+$(#&+55+.&2"5$1*'1+*&/$'6$789-%:$"#;$7)7$
Background
� Preclinical1 and retrospective clinical2,3,4 data suggest that high vascular endothelial growth factor (VEGF) levels in tumor tissue from breast cancer are associated with a decreased response to endocrine therapy.
� Clinical data suggest that the down regulation of VEGF may overcome resistance and improve efficacy to hormonal therapy4.
� The combination of endocrine therapy and bevacizumab has shown to be safe and active in phase II trials5,6
� We designed the phase III LEA study to address the hypothesis that anti-VEGF treatment can delay resistance to endocrine therapy in patients with hormone-receptor positive advanced breast cancer.
<=$>+$5"$?"@"$AB$%%-C$DE<<F$D=$G(#;+*4'50$)B$A-H$DEEEF$I=$:"#;+*,$JB$-"#.+*$DEEIF$K=$C/;L#$GB$A-H$
DEEMF$M=N+**+*'O3'**+,B$-)-$DE<EF$P=3*"(#"$$3%B$A-H$DE<E$

!"#$%#&'#('$)*+",&$-"#.+*$!/01',(20$�$����������������� �������������$
34(,$1*+,+#&"&('#$(,$&4+$(#&+55+.&2"5$1*'1+*&/$'6$789-%:$"#;$7)7$
Study Design and treatment
N= 380 patients unresectable locally advanced or metastatic breast cancer HR+/HER2-
Binational, multicentric, randomised, open label phase III study
Letrozole (2.5 mg/d) or Fulvestrant 250mg i.m. 1 q28
Letrozole (2.5 mg/d) or Fulvestrant 250mg i.m. q28d + Bevacizumab (15 mg/kg q3w)
R
Stratification criteria:
� Adjuvant AI (yes/no)
� Nº lesions (one/multiple)
� Measurable lesions (yes/no)
� Country (Spain/Germany)
Till disease progression
ET
ET-B
83Q$8#;'.*(#+$34+*"1/F$)Q$)+R".(S20"@$

!"#$%#&'#('$)*+",&$-"#.+*$!/01',(20$�$����������������� �������������$
34(,$1*+,+#&"&('#$(,$&4+$(#&+55+.&2"5$1*'1+*&/$'6$789-%:$"#;$7)7$
Progression-free Survival
18.4 months
13.8 months
HR: 0.83 (0.65-1.06)

!"#$%#&'#('$)*+",&$-"#.+*$!/01',(20$�$����������������� �������������$
34(,$1*+,+#&"&('#$(,$&4+$(#&+55+.&2"5$1*'1+*&/$'6$789-%:$"#;$7)7$
Overall Survival
?C$<=<TP$
Events
ET n= 189
ET-B n= 191
OS, median (months) 42 41
P-value, log-rank HR (95% CI)
0.469 1.18 (0.77-1.81)
OS events (Total) 42 42 Censored 147 149

!"#$%#&'#('$)*+",&$-"#.+*$!/01',(20$�$����������������� �������������$
34(,$1*+,+#&"&('#$(,$&4+$(#&+55+.&2"5$1*'1+*&/$'6$789-%:$"#;$7)7$
Conclusions
� The LEA study fails to demonstrate a statistically significant increase in PFS for ET plus bevacizumab vs ET alone:
� Median PFS: 18.4 months for ET-B vs 13.8 months for ET, p=0.14
� HR: 0.83 (0.65-1.06)
� An increase of smaller magnitude (i.e. <31% reduction in PFS with bevacizumab) cannot be ruled out
� Adding bevacizumab to ET as first-line therapy had no impact on overall survival
� Biomarker studies can help to select the population that might benefit from bevacizumab in addition to hormonal treatment

A Phase III, Open-Label, Randomized, Multicenter Study Of Eribulin Mesylate Versus Capecitabine In Patients With
Locally Advanced Or Metastatic Breast Cancer Previously Treated With
Anthracyclines And Taxanes Peter A. Kaufman,1 Ahmad Awada,2 Christopher Twelves,3
Louise Yelle,4 Edith A. Perez,5 Jantien Wanders,6 Martin S. Olivo,7 Yi He,7 Corina E. Dutcus,7 Javier Cortes8
1Norris Cotton Cancer Center, Dartmouth-Hitchcock Medical Center, Lebanon, NH, USA; 2Medical Oncology Clinic, Jules Bordet Institute, Brussels, Belgium; 3Leeds Institute of
������������������������������������������������������������� ���4Department of Medicine, University of Montreal, Montreal, Canada; 5Mayo Medical Clinic, Jacksonville, FL, USA;
6Eisai Ltd, Hatfield, UK; 7Eisai Inc., Woodcliff Lake, NJ, USA; 8Vall �������� University Hospital, Barcelona, Spain

Study Rationale � Eribulin is the only chemotherapeutic agent with a demonstrated
survival benefit for patients with heavily pre-treated MBC
� ��� ���������������������3rd-line� patients with MBC): � ��2 �� ���� ��� ������ ��� �������������5 regimens in total),
including an anthracycline and a taxane in the adjuvant or metastatic setting
� 2.5-month improvement in OS for eribulin versus treatment of ��������� ������� ��13.1 vs 10.6 months; p=0.041; HR, 0.81; 95% CI 0.66, 0.99)
� Capecitabine is a widely used therapy in MBC, including 1st-, 2nd- and 3rd-line setting for MBC
� Approved for the treatment of patients with MBC whose disease is resistant to both paclitaxel and an anthracycline-containing regimen
Cortes et al. Lancet 2011;377:914-23
San Antonio Breast Cancer Symposium - Cancer Therapy and Research Center at UT Health Science Center � December 4-8, 2012
This presentation is the intellectual property of the author

Study Design
� Global, randomized, open-label Phase III trial (Study 301)
� Stratification: Geographical region, HER2 status
Equivalent to 1.23 mg/m2 eribulin
Capecitabine 1250 mg/m2 BID orally Days 1-14, q21 days
Eribulin mesylate
1.4 mg/m2 2- to 5-min IV Day 1 & 8 q21 days
Randomization 1:1
Co-primary endpoint � OS and PFS Secondary endpoints � Quality of life � ORR � Duration of response � 1-, 2- and 3-year survival � Tumor-related symptom
assessments � Safety parameters � Population PK (eribulin
arm only)
Patients (N=1102) Locally advanced or MBC � �3 prior chemotherapy
����������2 for advanced disease)
� Prior anthracycline and taxane in (neo)adjuvant setting or for locally advanced or MBC
San Antonio Breast Cancer Symposium - Cancer Therapy and Research Center at UT Health Science Center December 4-8, 2012
This presentation is the intellectual property of the author

Patient and Disease Characteristics
ITT population �Determined by independent assessment; missing patients for sites of disease were 1% for eribulin and 1% for capecitabine �Assays carried out and defined locally Unknown patients for eribulin and capecitabine were: HER2 status 17% and 16% ; ER status 11% and 10%; PR status 12% and 12%, respectively
Eribulin (n=554) Capecitabine (n=548)
Median age (range) 54.0 (24-80) 53.0 (26-80) ECOG performance, % 0 45 42
1 53 55 2+ 2 3
Number of prior chemotherapy regimens for advanced disease, %
0 21 19 1 50 53 2 28 27
>2 1 1 Sites of disease�, % Visceral 84 88
Non-visceral only 15 11 HER2 status�, % Positive 16 15
Negative 68 69 ER status�, % Positive 47 51
Negative 42 39 PR status�, % Positive 41 43
Negative 47 45 Triple (ER/PR/HER2) negative, % 27 25
San Antonio Breast Cancer Symposium - Cancer Therapy and Research Center at UT Health Science Center � December 4-8, 2012
This presentation is the intellectual property of the author

Overall Survival Su
rviv
al p
roba
bilit
y
Time (months) 0
0.0�
0.2�
0.4�
0.6�
0.8�
1.0�
56�52�48�44�40�36�32�28�24�20�16�12�8�4�
HR� 0.879 (95% CI 0.770, 1.003) p value�=0.056
Median OS (months)
Eribulin (n=554) 15.9 Capecitabine (n=548) 14.5
ITT population; �HR Cox model including geographic region and HER2 status as strata �p value from stratified log-rank test based on clinical database
San Antonio Breast Cancer Symposium - Cancer Therapy and Research Center at UT Health Science Center � December 4-8, 2012
This presentation is the intellectual property of the author

HR� 0.977 (95% CI 0.857, 1.114) p value�=0.736
HR� 1.079 (95% CI 0.932, 1.250) p value�=0.305
Time (months)
Investigator Review Independent Review
1.0�
0.8�
0.6�
0.4�
0.2�
0.0�
Surv
ival
pro
babi
lity
�
Time (months)�0� 4� 8� 12� 16� 20� 24� 28� 32� 36� 40� 44� 0 4 8 12 16 20 24 28 32
1.0
0.8
0.6
0.4
0.2
0.0
Surv
ival
pro
babi
lity
36 40 44
ITT population; �HR Cox model including geographic region and HER2 status as strata �p value from stratified log-rank test based on clinical database
Median (months)
Eribulin (n=554) 4.1
Capecitabine (n=548) 4.2
Median (months)
Eribulin (n=554) 4.2
Capecitabine (n=548) 4.1
Progression-Free Survival San Antonio Breast Cancer Symposium - Cancer Therapy and Research Center at UT Health Science Center � December 4-8, 2012
This presentation is the intellectual property of the author

Conclusions
� This trial does not demonstrate a statistically significant superiority of eribulin vs capecitabine in either OS or PFS � Median OS: eribulin 15.9 months, capecitabine 14.5 months
HR, 0.879 (95%CI: 0.770, 1.003)
� Pre-specified exploratory analyses suggest particular patient subgroups may have greater therapeutic benefit with eribulin and may warrant further study � Triple negative HR, 0.702 (95%CI: 0.545, 0.906) � ER negative HR, 0.779 (95%CI: 0.635, 0.955) � HER2 negative HR, 0.838 (95%CI: 0.715, 0.983)
� Eribulin and capecitabine have similar overall activity in this trial that included patients in the 1st-, 2nd-, or 3rd-line setting � The AE profiles of eribulin and capecitabine are consistent with
their previously known side effects
San Antonio Breast Cancer Symposium - Cancer Therapy and Research Center at UT Health Science Center � December 4-8, 2012
This presentation is the intellectual property of the author

F inal analysis of overall survival for the Phase I I I C O N F IR M trial:
fulvestrant 500 mg versus 250 mg
Angelo Di L eo, Guy Jerusalem, Lubos Petruzelka, Igor N . Bondarenko, Rustem K hasanov, Didier Verhoeven, José L . Pedrini,
Iva Smirnova, M ikhail R . L ichinitser , K elly Pendergrass, Sally Garnett, Yuri Rukazenkov, M iguel Martin, on behalf of the C O N F IR M investigators
San Antonio Breast Cancer Symposium � Cancer Therapy and Research Center at U T H ealth Science Center � December 4-8, 2012
This presentation is the intellectual property of the author/presenter. Contact them at [email protected] for permission to reprint and/or distribute

;F=#'(+.$%+OX77)/A)G8Q)G8XQ)$%")G6PQ)
$%")+,'%)Y6[)GR)))))))))))))))))))))))))))))))))))))))))))))))))
;F=#'(+.$%+O6X7)/A)G8Q)G8XQ)$%")G6PQ)
$%")+,'%)Y6[)GR)))))))))))))))))))))))))))))))))))))))))))))))))
L,$(')555)4:B;5I2)+.*$=W);F=#'(+.$%+)X77)/A)#'.(F()6X7)/A
VW%XK\
GYG%()-+9>,I)#,9-
H(%?9<,#,*"
&;7%9$%d8;7
("4)?<"%9-%H-+9%2U
9$%P,#0,-%G%=$%9N%H%8+b
/"4"9%"#%)4.%5GCB.%58;75%EFGE%)-+%Z%74,-%O-694'%EFGF%O6#%EF[EDJKFLYBS]BC\FF'%%
5)-%8-#9-,9%;$")<#%7)-6"$%5=>?9<,@>%� 7)-6"$%20"$)?=%)-+%("<")$60%7"-#"$%)#%12%3")4#0%56,"-6"%7"-#"$%� /"6">A"$%BCD.%EFGE

Primary endpoint: progression-free survival 1.0
0.8
0.6
0.4
0.2
0 4 8 12 16 20 24 28 32 36 40 44 48
Proportion of patients progression-free
Time (months)
216 199
163 144
113 85
90 60
54 35
37 25
19 12
12 4
7 3
3 1
2 1
0 0
362 374
Patients at risk: 500 mg 250 mg
Fulvestrant 500 mg Fulvestrant 250 mg
HR = 0.80; 95% CI: 0.68, 0.94; p=0.006
Median PFS (months) Fulvestrant 500 mg 6.5 Fulvestrant 250 mg 5.5
0.0
Di Leo A et al. J Clin Oncol 2010; 28: 4594-4600 CI, confidence interval; HR, hazard ratio; PFS, progression-free survival
San Antonio Breast Cancer Symposium � Cancer Therapy and Research Center at U T H ealth Science Center � December 4-8, 2012
This presentation is the intellectual property of the author/presenter. Contact them at [email protected] for permission to reprint and/or distribute

0.1 0
0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1.0
0 4 8 12 16 20 24 28 32 36 40 44 48 52 56 60 64 68 72 76 80
Fulvestrant 500 mg Fulvestrant 250 mg
362 333 288 254 227 202 178 163 141 123 114 98 81 64 47 30 26 15 8 1 0 500 mg 374 338 299 261 223 191 164 137 112 96 87 74 64 48 37 22 14 8 3 2 0 250 mg
Time (months)
Proportion of patients alive
Patients at risk:
HR (95% CI) 0.81 (0.69, 0.96)
p-value 0.016a
aNominal value, cannot be claimed as statistically significant
Median time to death (months) Fulvestrant 500 mg 26.4 Fulvestrant 250 mg 22.3
Overall survival (final analysis at 75% maturity � full analysis set)
San Antonio B reast Cancer Symposium � Cancer Therapy and Research Center at U T H ealth Science Center � December 4-8, 2012
This presentation is the intellectual property of the author/presenter. Contact them at [email protected] for permission to reprint and/or distribute

Conclusions � F inal OS analysis at 75% maturity shows that fulvestrant 500 mg is associated
with 4.1-month increase in median OS and a 19% reduction in the r isk of death compared with fulvestrant 250 mg
� These results are consistent with the previously reported PFS and OS data
(J C lin Oncol. 28: 4594-00, 2010)
� Analysis of 1st subsequent therapies does not support any imbalance between the two study arms
� Only 2% of patients crossed-over from 250 to 500 mg. However , activity for 500 mg after pre-treatment with 250 mg is unknown
� The safety results do not support any clinically relevant difference between
fulvestrant 250 and 500 mg and they are consistent with the previously reported safety profile of fulvestrant 500 mg
San Antonio Breast Cancer Symposium � Cancer Therapy and Research Center at U T H ealth Science Center � December 4-8, 2012
This presentation is the intellectual property of the author/presenter. Contact them at [email protected] for permission to reprint and/or distribute

LG)7^^6PP8`
?'+.0c0='
O)86X)`)6]X)/A)L7)YG)RR)))))))))))))))))))))))))))))))))))))))))))))))))
?'+.0c0='
O)6]X)/A)L7)YG)R
L,$(')I$%"0/*c'")55)-.*$=)01)
?'+.0c0=')T LG)7^^6PP8
Bd)8eX
8W8)I$%"0/*c$+*0%
JITQ)K'.6)�\\234)0.)?!34
8(+ ?*%')-,'.$9>
C+=)C#+D.%&@A%#C/8EF##12/1
\\)!==)9$+*'%+()C'.')JITQ)K'.6)VQ)NF+)*%)+,')('&0%")9,$(')
01)+,'))(+F">))O%d)PPR)$%)$""*+*0%$=).'(+.*&+*0%)C$()+,$+)
+,'))9$+*'%+()),$")+0),$#')$/9=*1*'")44BG8)$/9)$%"`0.)
=0(()01)98e])
5)-%8-#9-,9%;$")<#%7)-6"$%5=>?9<,@>%� 7)-6"$%20"$)?=%)-+%("<")$60%7"-#"$%)#%12%3")4#0%56,"-6"%7"-#"$%� /"6">A"$%BCD.%EFGE

("?$,-#"+%N$9>%h",-A"$Q%(8'%:;<#=!'3'->#'?#)@"A<&4#V"P%i9$`.%ViY%j)$4)-+%56,"-6"[%EFF\'%k%EFF\%j)$4)-+%56,"-6"'
!%)'@$/9=')01)$)%'C)+$.A'+*%A)$A'%+-$.A'+()!)4>&=*%)G'9'%"'%+)o*%$(')LG)7^^6PP8
\B
'@+'%+)01)9IN9,0(9,0.>=$+*0%
3 4G46
"'9,0(9,0.>=$+*0%
,>909,0(9,0.>=$+*0%G 4Goa`e
2
< 8
I)90*%+
D
< 6
-$.A'+)01)LG)7^^6PP8
98e 5Boa$
,>9'.9,0(9,0.>=$+*0%B"@A%!$@%<. (A%)-+)449P<%?$9Q$"<<,9-
4Go6J
4Go6
4G46
!
!
5)-%8-#9-,9%;$")<#%7)-6"$%5=>?9<,@>%� 7)-6"$%20"$)?=%)-+%("<")$60%7"-#"$%)#%12%3")4#0%56,"-6"%7"-#"$%� /"6">A"$%BCD.%EFGE

F E B \ D GF GE GB G\ GD EF EE EB E\ ED-*/')O20%+,R
F
F'G
F'E
F'K
F'B
F'S
F'\
F'X
F'D
F']
G'F
L.0A.'((*0%V;.'')DF.#*#$=)L.0N$
N*=*+>
LG)7^^6PP8)T)?'+.0c0='L.0A.'((*0%);.'')DF.#*#$=)
KI)d)7]^i)O45)7]68V 7]e^R9 f)7]778
LG)T)?J-W))6e]8)/0%+,(
?J-W))i]X)/0%+,(
5)-%8-#9-,9%;$")<#%7)-6"$%5=>?9<,@>%� 7)-6"$%20"$)?=%)-+%("<")$60%7"-#"$%)#%12%3")4#0%56,"-6"%7"-#"$%� /"6">A"$%BCD.%EFGE

LG)PP8)T)?J-O%)d)[^R
?J-)O%)d)iiR
B'F+.09'%*$ X8 8?'FH09'%*$ 8a 7;$+*AF' 6 8!%'/*$ a 8B$F('$ 6 8K0+)1=F(, 7 7!=09'&*$ 7 7!.+,.$=A*$ 7 8G*$..,'$ a 7
LG)7^^6PP8)T)?'+.0c0='<.$"')^)`)a)-0@*&*+>
5)-%8-#9-,9%;$")<#%7)-6"$%5=>?9<,@>%� 7)-6"$%20"$)?=%)-+%("<")$60%7"-#"$%)#%12%3")4#0%56,"-6"%7"-#"$%� /"6">A"$%BCD.%EFGE

Azienda Sanitaria Firenze 88
Conclusioni
Terapia adiuvante: " 10 anni di TAM (..)
" LETROZOLO in lobulari
" durata del TRASTUZUMAB: 1 anno
" Chemioterapia diuvante dopo recidiva (ER neg ..)
" nessun ruolo di Bevacizumab TN
Terapia della malattia metastatica " NUOVI FARMACI (coming soon) .. Everolimus / Pertuzumab / T-DM1
" Dose Fulvestrant 500 mg
" No Bevacizumab in I linea con OT
" Eribulina / Capecitabina
" NUOVO TARGET:

Azienda Sanitaria Firenze 89
Grazie per l’attenzione