
2005 roma, convegno regionale, la terapia di resincronizzazione cardiaca nello scompenso cardiaco
43
“ “ Cardiac Resynchronization Cardiac Resynchronization Therapy ” Therapy ” Stefano Nardi, MD AZIENDA OSPEDALIERA SANTA MARIA TERNI AZIENDA OSPEDALIERA SANTA MARIA TERNI DIPARTIMENTO CARDIOTORACOVASCOLARE DIPARTIMENTO CARDIOTORACOVASCOLARE STRUTTURA COMPLESSA DI CARDIOLOGIA STRUTTURA COMPLESSA DI CARDIOLOGIA UNITA’ OPERATIVA DI ARITMOLOGIA CARDIACA UNITA’ OPERATIVA DI ARITMOLOGIA CARDIACA LABORATORIO DI ELETTROFISIOLOGIA ED LABORATORIO DI ELETTROFISIOLOGIA ED ELETTROSTIMOLAZIONE ELETTROSTIMOLAZIONE
-
Upload
centro-diagnostico-nardi -
Category
Health & Medicine
-
view
54 -
download
0
Transcript of 2005 roma, convegno regionale, la terapia di resincronizzazione cardiaca nello scompenso cardiaco

“ “ Cardiac Resynchronization Cardiac Resynchronization Therapy ”Therapy ”
Stefano Nardi, MD
AZIENDA OSPEDALIERA SANTA MARIA TERNIAZIENDA OSPEDALIERA SANTA MARIA TERNIDIPARTIMENTO CARDIOTORACOVASCOLAREDIPARTIMENTO CARDIOTORACOVASCOLARE STRUTTURA COMPLESSA DI CARDIOLOGIA STRUTTURA COMPLESSA DI CARDIOLOGIA
UNITA’ OPERATIVA DI ARITMOLOGIA CARDIACA UNITA’ OPERATIVA DI ARITMOLOGIA CARDIACA LABORATORIO DI ELETTROFISIOLOGIA ED ELETTROSTIMOLAZIONE LABORATORIO DI ELETTROFISIOLOGIA ED ELETTROSTIMOLAZIONE
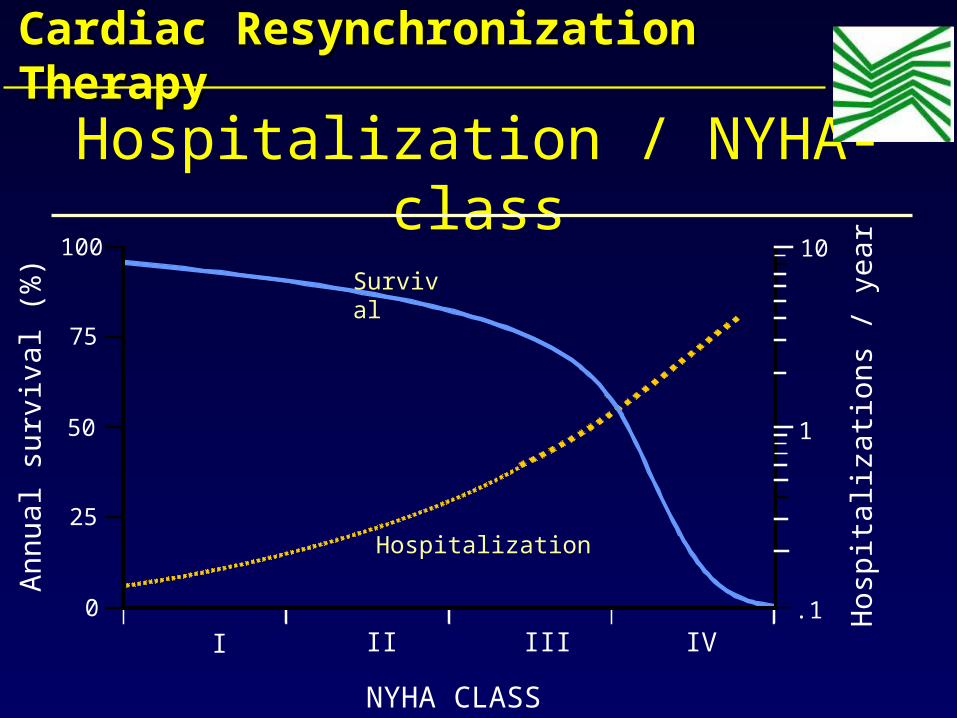
NYHA CLASS
Annual su
rviv
al (%
)
Hosp
italiz
ati
ons
/ year
100
75
50
25
0
I II III IV
1
10Survival
Hospitalization
.1
Hospitalization / NYHA-class
Cardiac Resynchronization Cardiac Resynchronization TherapyTherapy
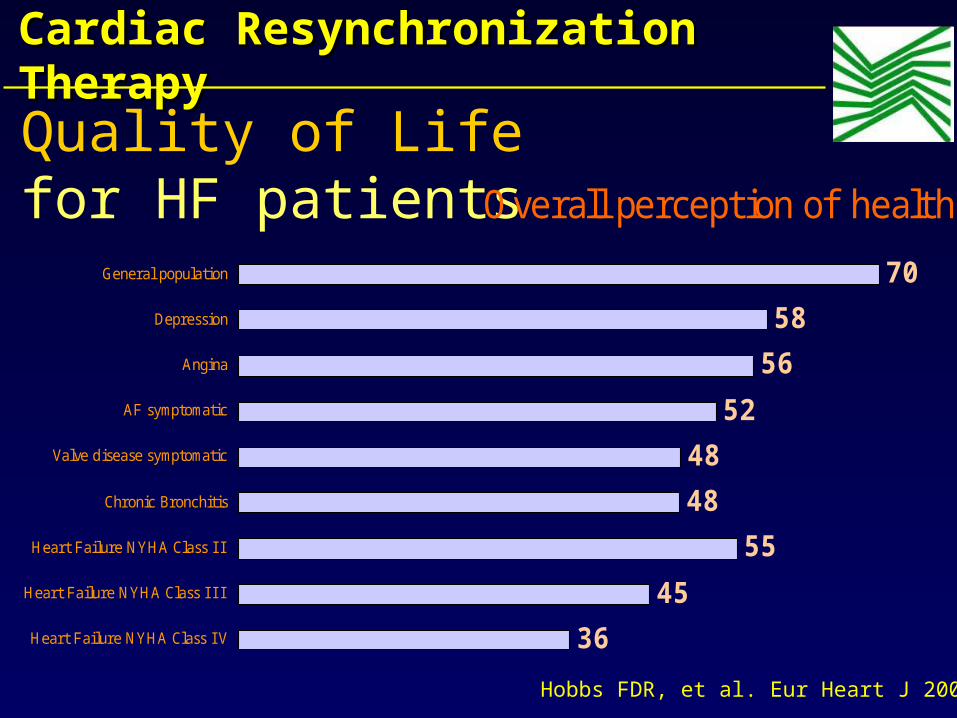
Quality of Life for HF patients Overall perception of health
36
45
55
48
48
52
56
58
70
Heart Failure NYHA Class I V
Heart Failure NYHA Class I I I
Heart Failure NYHA Class I I
Chronic Bronchitis
Valve disease symptomatic
AF symptomatic
Angina
Depression
General population
Hobbs FDR, et al. Eur Heart J 2002
Cardiac Resynchronization Cardiac Resynchronization TherapyTherapy
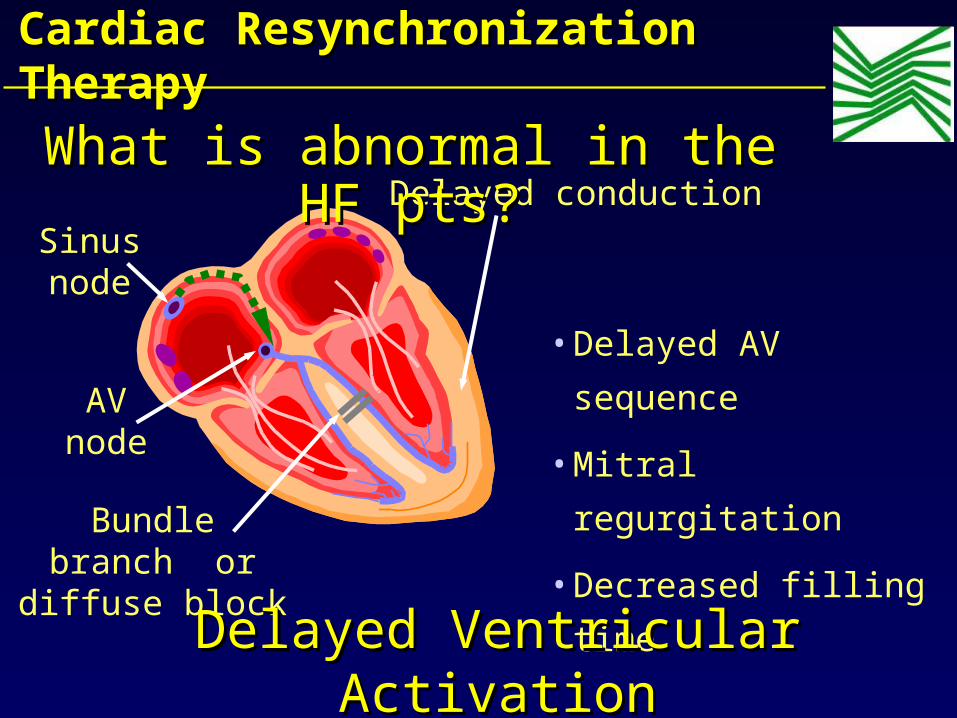
Sinusnode
AVnode
Bundlebranch or
diffuse block
Delayed conduction
•Delayed AV
sequence
•Mitral regurgitation
•Decreased filling
time
Delayed Ventricular Delayed Ventricular ActivationActivation
What is abnormal in the HF What is abnormal in the HF pts?pts?
Cardiac Resynchronization Cardiac Resynchronization TherapyTherapy
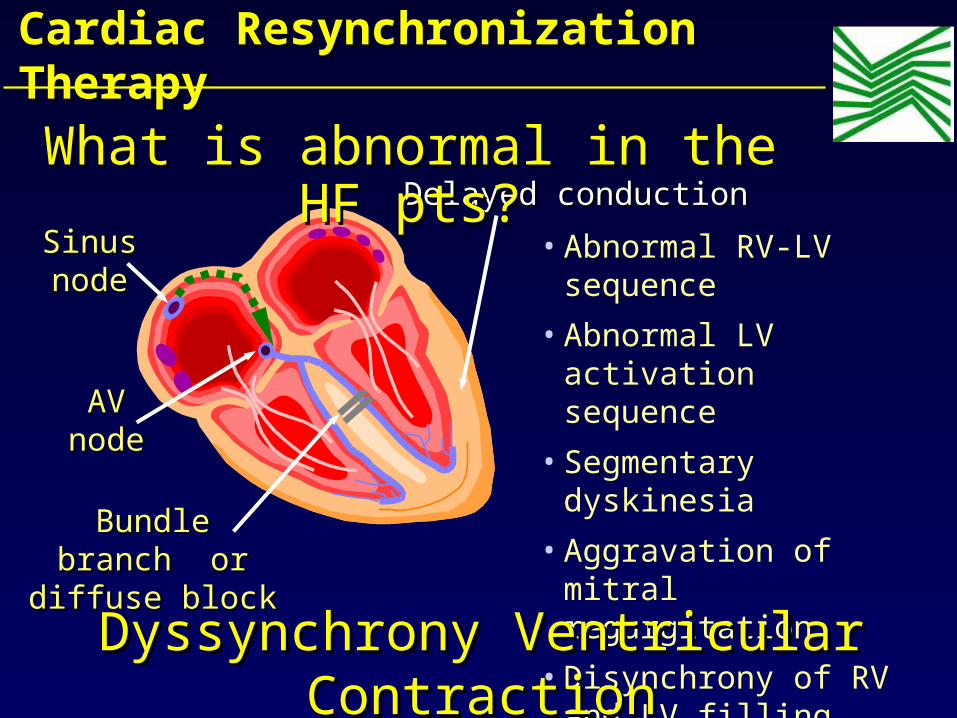
SinusSinusnodenode
AVAVnodenode
BundleBundlebranch orbranch or
diffuse blockdiffuse block
Delayed conductionDelayed conduction
• Abnormal RV-LV sequence
• Abnormal LV activation sequence
• Segmentary dyskinesia
• Aggravation of mitral regurgitation
• Disynchrony of RV and LV filling flowsDyssynchrony Ventricular Dyssynchrony Ventricular
ContractionContraction
What is abnormal in the HF What is abnormal in the HF pts?pts?
Cardiac Resynchronization Cardiac Resynchronization TherapyTherapy
• Reduced LVEF remains the single most important risk factor for overall mortality and SCD.1
• Increased risk is measurable at EF above 30%, but an EF ≤30% is the single most powerful independent predictor for SCD.2
1Prior SG, Aliot E, Blonstrom-Lundqvist C, et al. Task Force on Sudden Cardiac Death of the European Society of Cardiology. Eur Heart J, Vol. 22; 16; August 2001.
2 Myerburg RJ, Castellanos A. Cardiac Arrest and Sudden Cardiac Death, in Braunwald E, Zipes DP, Libby P, Heart Disease, A textbook of Cardiovascular Medicine. 6th ed. 2001. W.B. Saunders, Co., p. 895.
Relationship of SCD Relationship of SCD and LV Dysfunctionand LV Dysfunction
Cardiac Resynchronization Cardiac Resynchronization TherapyTherapy

Which is the prognostic value of QRS width ?• VEST study analysis
• NYHA Class II – IV pz
• 3,654 ECGs digitally scanned
• Age, creatinine, LVEF, heart rate, and QRS duration found to be independent predictors of mortality
• Relative risk of widest QRS group 5x greater than narrowest
60%
70%
80%
90%
100%
0 60 120 180 240 300 360Days in Trial
Cu
mu
lati
ve S
urv
ival
QRS Duration (msec)
<9090-120
120-170170-220
>220
Adapted from Gottipaty et al. JACC 1999; 33(2):145A (abstract 847-4)
Cardiac Resynchronization Cardiac Resynchronization TherapyTherapy
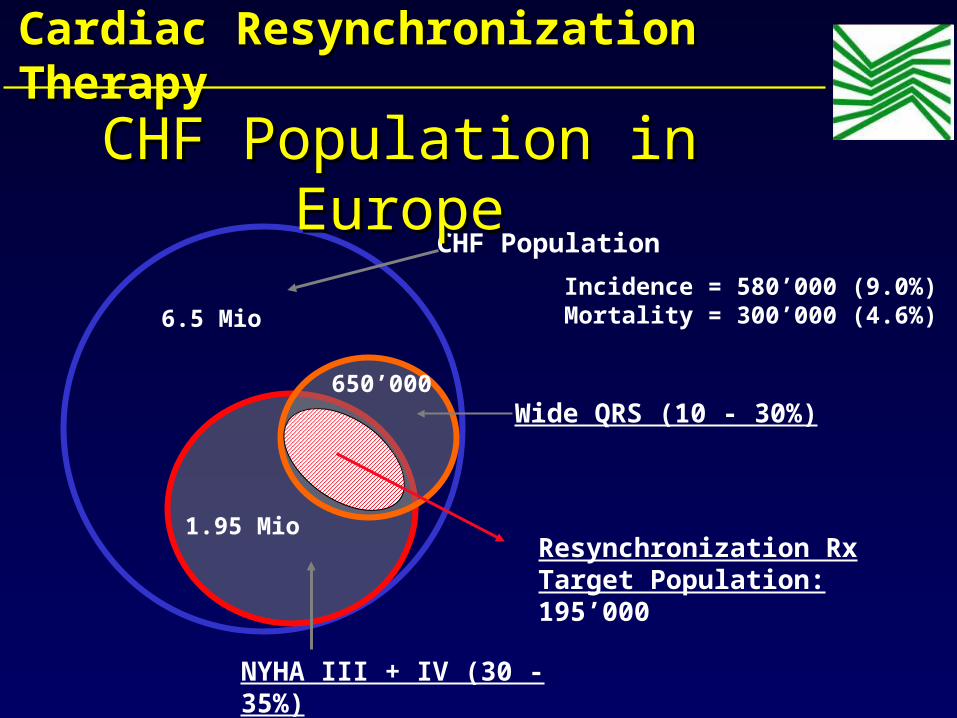
CHF Population
6.5 Mio
NYHA III + IV (30 - 35%)
1.95 Mio
Wide QRS (10 - 30%)
Resynchronization Rx Target Population:195’000
650’000
Incidence = 580’000 (9.0%)Mortality = 300’000 (4.6%)
CHF Population in CHF Population in EuropeEurope
Cardiac Resynchronization Cardiac Resynchronization TherapyTherapy
•WHO? Which criteria ?
•WHEN? Which NYHA class ?
•WHERE? RV+LV / LV ?
•WHY? Symptoms / Mortality ?
KEY QUESTIONSKEY QUESTIONS
Cardiac Resynchronization Cardiac Resynchronization TherapyTherapy
• Optimizes AV contraction sequence
• Reduces pre-systolic mitral regurgitation
• Improves atrial preloading of the ventricle
• Increases filling time
Mechanism IMechanism IAtrio-Ventricular SynchronyAtrio-Ventricular Synchrony
Cardiac Resynchronization Cardiac Resynchronization TherapyTherapyWhat does pacing What does pacing changechange??
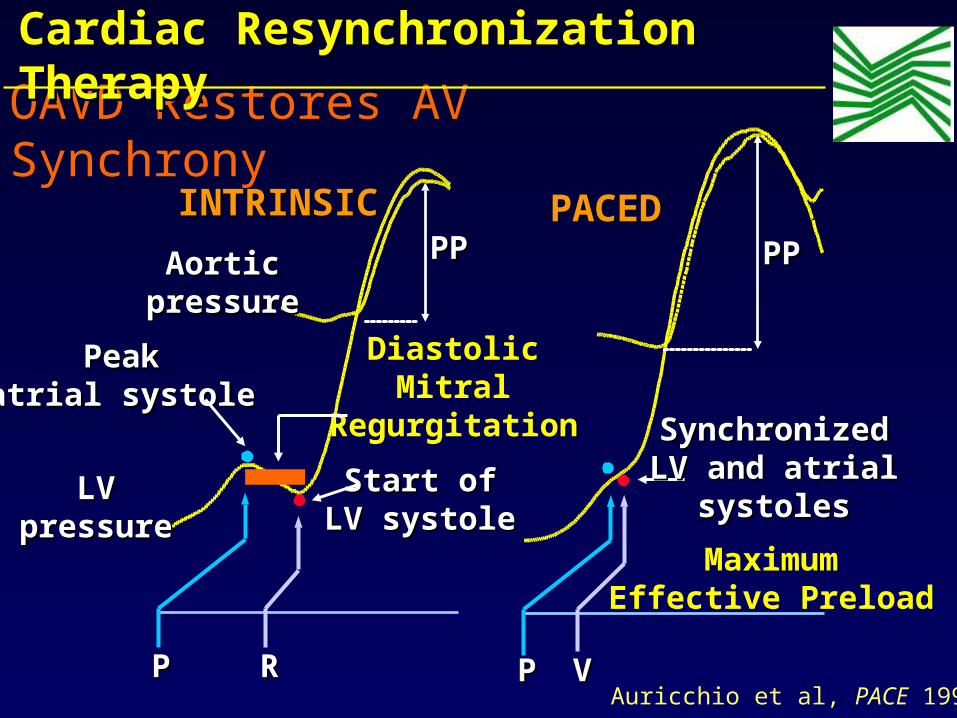
OAVD Restores AV Synchrony
PP RR
INTRINSICINTRINSIC
AorticAorticpressurepressure
LVLVpressurepressure
PPPP
PeakPeakatrial systoleatrial systole
Start ofStart ofLV systoleLV systole
DiastolicMitral
Regurgitation
MaximumEffective Preload
PP VV
PACEDPACEDPPPP
SynchronizedSynchronizedLV and atrialLV and atrial
systolessystoles
Auricchio et al, PACE 1998
Cardiac Resynchronization Cardiac Resynchronization TherapyTherapy
• Optimizes ventricular activation
• Increases pumping effectiveness
• Reduces regional wall stress (WMSI)
• Decreases mitral regurgitation
• Resynchronizes ventricular filling flows
• Decreases filling pressures
Cardiac Resynchronization Cardiac Resynchronization TherapyTherapy
Mechanism IIMechanism IIVentricular CoordinationVentricular Coordination
What does pacing What does pacing changechange??
LV Lead Implant Historical Evolution
• Thoracic epicardial LV lead - 1994 1
• RV lead adapted for transvenous LV implant - 1996 2
• CS lead adapted for transvenous LV implant -1997 3
• Special designed transvenous LV lead - 1998 4
• Guiding catheter sheath for LV lead delivery -1998 5
1. Bakker et al. PACE 1994; 2. Cazeau et al. PACE 1996; 3.Daubert et al. PACE 1997; 4. Gras et al. PACE 1998 5. Lurie et al. Circulation 1998
Cardiac Resynchronization Cardiac Resynchronization TherapyTherapy

Blanc et al., Circulation 199723 pts mean SD
90
100
110
120
130
140
150
SYSTOLIC SYSTOLIC Blood PressureBlood Pressure
RVARVA LV BVRVORVOBASBAS
mm
Hg
mm
Hg
p<.01p<.03
0
10
20
30
40
Pulmonary Capillary Pulmonary Capillary Wedge PressureWedge Pressure
RVARVA LV BVBVRVORVOBASBAS
p<.01p<.01
Acute studies
Cardiac Resynchronization Cardiac Resynchronization TherapyTherapy
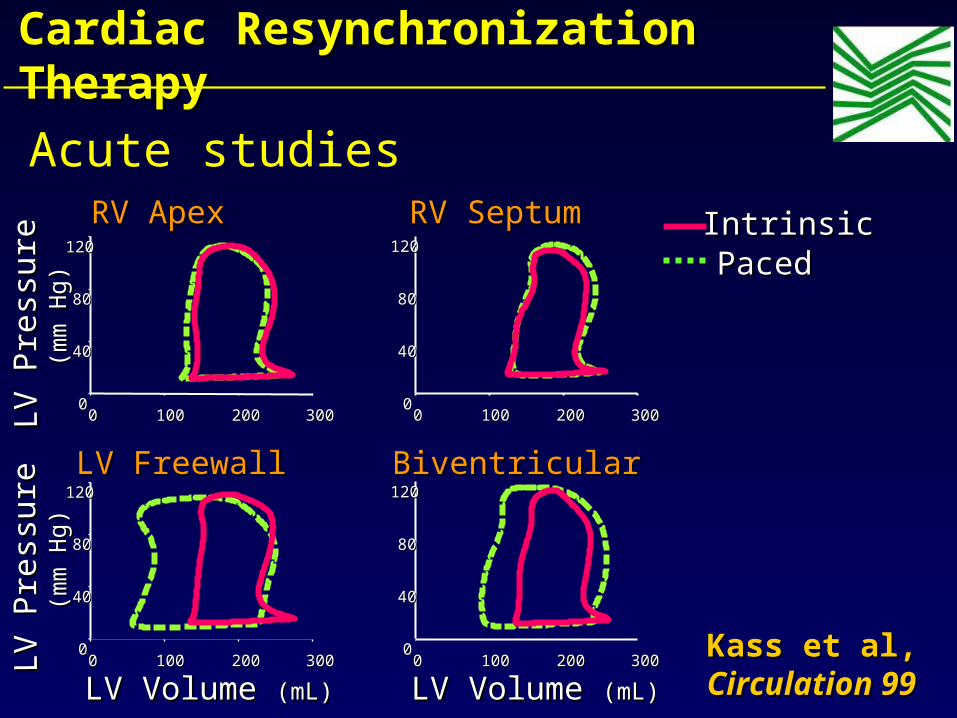
Kass et al, Kass et al, Circulation 99Circulation 99
IntrinsicIntrinsicPacedPaced
00 100100 200200 30030000
4040
8080
120120
RV SeptumRV Septum
00 100100 200200 30030000
4040
8080
120120BiventricularBiventricular
00 100100 200200 30030000
4040
8080
120120
RV ApexRV Apex
00 100100 200200 30030000
4040
8080
120120LV FreewallLV Freewall
LV Volume LV Volume (mL)(mL)
LV P
ress
ure
LV P
ress
ure
(m
m H
g)
(mm
Hg
)LV
Pre
ssu
reLV
Pre
ssu
re
(mm
Hg
)(m
m H
g)
LV Volume LV Volume (mL)(mL)
Acute studies
Cardiac Resynchronization Cardiac Resynchronization TherapyTherapy

Auricchio et al., NASPE ‘99
PATH-CHF: Inclusion Criteria (42 pts)
• Dilated cardiomyopathy of any etiology• NYHA Class III (> 6 months) or NYHA IV• Optimal individual drug therapy • QRS duration >120 msec • PR Interval >150 msec• Sinus rate > 55 bpm• No conventional pacemaker indication
PATH CHF
Cardiac Resynchronization Cardiac Resynchronization TherapyTherapy
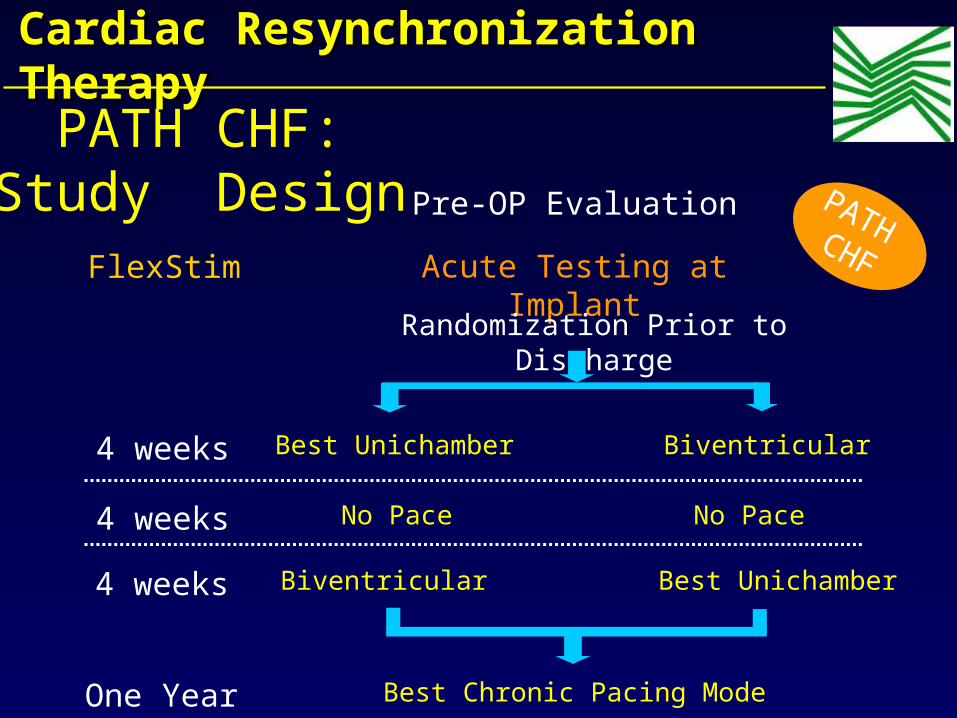
4 weeks
4 weeks
One Year
4 weeks
Acute Testing at Implant
Randomization Prior to Discharge
Pre-OP Evaluation
Best Unichamber Biventricular
No Pace No Pace
Biventricular Best Unichamber
Best Chronic Pacing Mode
FlexStim
PATH CHF:Study Design PATH CHF
Cardiac Resynchronization Cardiac Resynchronization TherapyTherapy
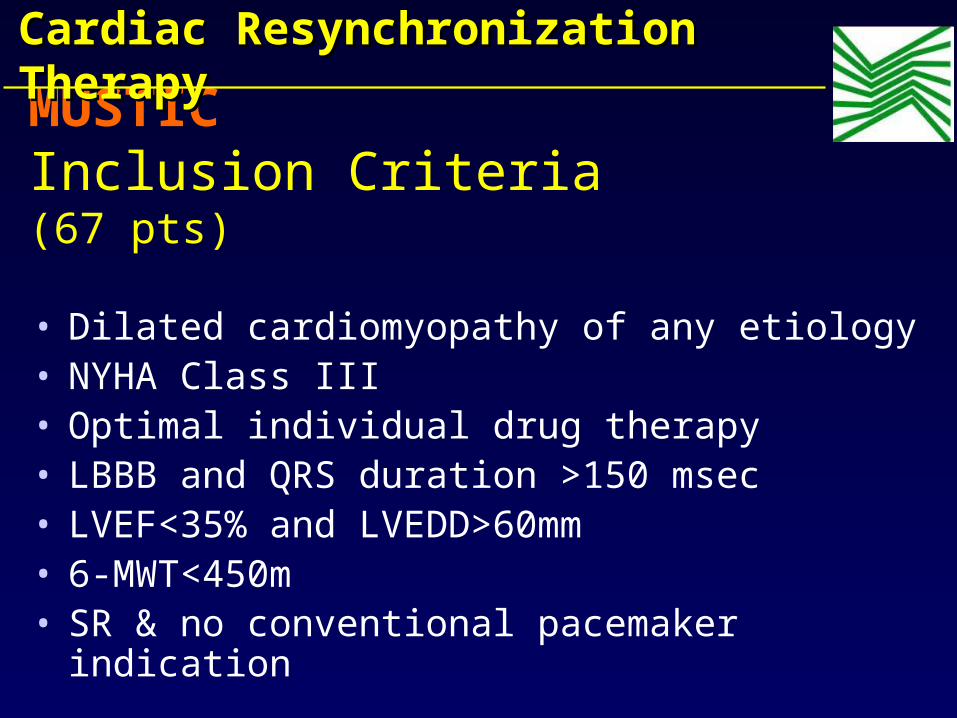
MUSTIC Inclusion Criteria (67 pts)
• Dilated cardiomyopathy of any etiology• NYHA Class III • Optimal individual drug therapy • LBBB and QRS duration >150 msec • LVEF<35% and LVEDD>60mm• 6-MWT<450m• SR & no conventional pacemaker indication
Cardiac Resynchronization Cardiac Resynchronization TherapyTherapy

Results Active pacing
Inactivepacing
p
6-min w (m) 399 ± 100 326 ± 134 .0001
QOL score 29.6 ± 21.3
43.2 ± 22.8
.0002
VO2 (ml/min/Kg) 16.2 ± 4.7 15 ± 4.9 0.02
S.Cazeau et al NEJM 2001;344:873-80S.Cazeau et al NEJM 2001;344:873-80
Cardiac Resynchronization Cardiac Resynchronization TherapyTherapyMUSTIC Results (67 pts)
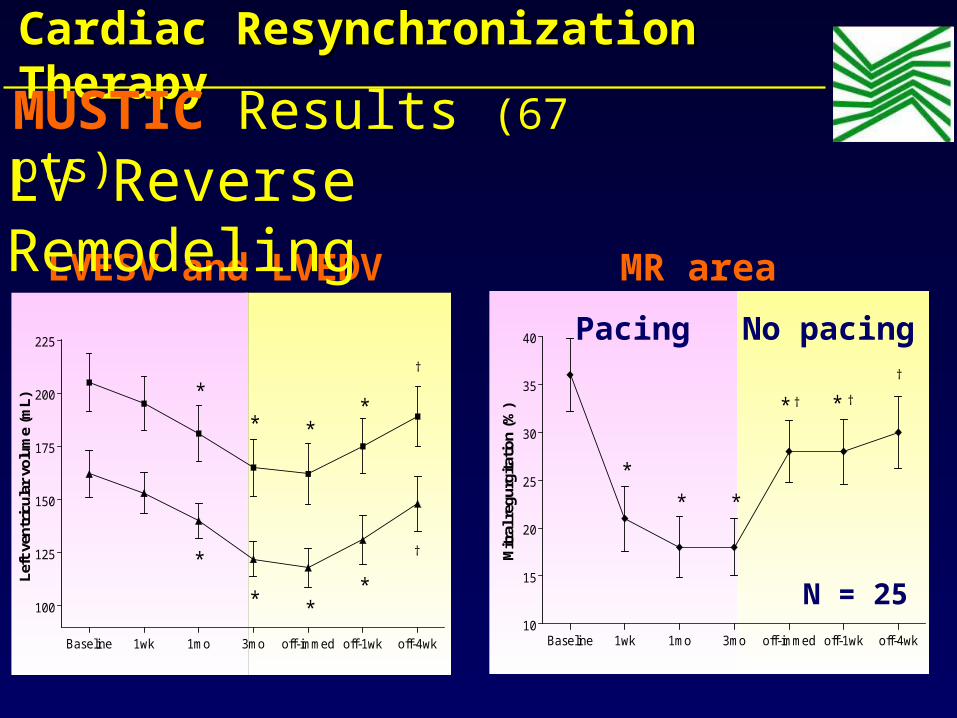
Baseline 1wk 1mo 3mo off-immed off-1wk off-4wk10
15
20
25
30
35
40
*
* †
*
*
*
†
†
Mitr
al r
egur
gita
tion
(%)
MR area
Baseline 1wk 1mo 3mo off-immed off-1wk off-4wk
100
125
150
175
200
225
**
*
*
†
* *
*
†
Left
ven
tric
ular
vol
ume
(mL) *
LVESV and LVEDV
LV Reverse Remodeling
Pacing No pacing
N = 25
Cardiac Resynchronization Cardiac Resynchronization TherapyTherapyMUSTIC Results (67 pts)

MIRACLE Inclusion Criteria (571 pts)
• Moderate or severe HF (NYHA III-IV)• Stable optimal HF medical therapy regimen for
>1mo Diuretics (93-94%) ACE-I or ARB (90-93%) if tollerated β-blocker (55-62%) at stable regimen for>3 months
• QRS duration ≥150 msec • LVEF ≤35% or LVEDD ≥55mm (echo measure)• Sinus rate > 55 bpm • 6 MWT <450m
Cardiac Resynchronization Cardiac Resynchronization TherapyTherapy
Abraham WT, Fisher WG, Smith AL, et al. N Engl J Med 2002;346:1845-1853
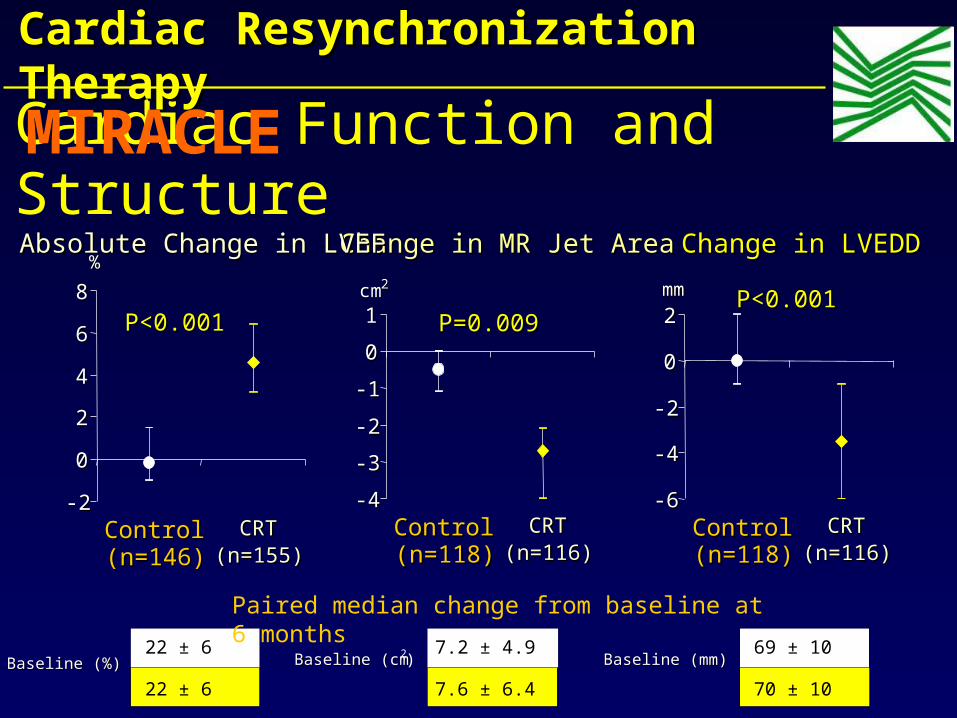
Change in MR Jet AreaChange in MR Jet Area
-4-4
-3-3
-2-2
-1-1
00
11
ControlControl(n=118)(n=118)
CRTCRT(n=116)(n=116)
cmcm22
P<0.001P<0.001 P=0.009P=0.009
Change in LVEDDChange in LVEDD
-6-6
-4-4
-2-2
00
22
ControlControl(n=118)(n=118)
CRTCRT(n=116)(n=116)
mmmm P<0.001P<0.001
Absolute Change in LVEFAbsolute Change in LVEF
-2-2
00
22
44
66
88
ControlControl(n=146)(n=146)
CRTCRT(n=155)(n=155)
%%
Baseline (mm)Baseline (mm)69 ± 10
70 ± 10
Baseline (cmBaseline (cm2)7.2 ± 4.9
7.6 ± 6.4Baseline (%)Baseline (%)
22 ± 6
22 ± 6
Paired median change from baseline at 6 months
Cardiac Function and Structure
Cardiac Resynchronization Cardiac Resynchronization TherapyTherapyMIRACLE
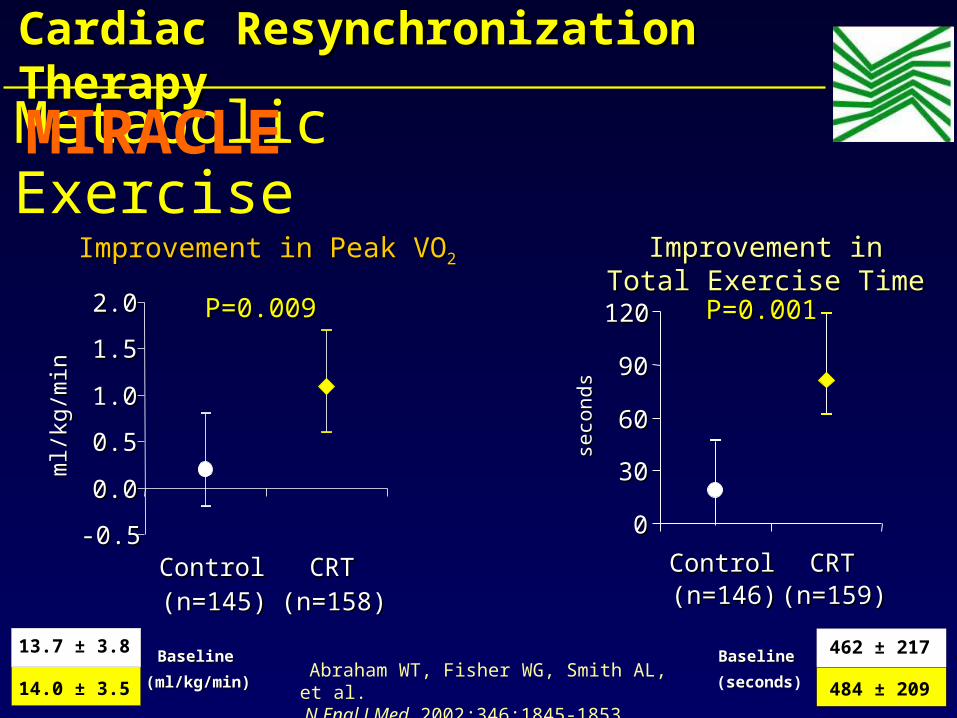
Improvement in Peak VOImprovement in Peak VO22
-0.5-0.5
0.00.0
0.50.5
1.01.0
1.51.5
2.02.0
ControlControl(n=145)(n=145)
CRTCRT(n=158)(n=158)
ml/kg
/min
ml/kg
/min
P=0.009P=0.009
Improvement in Improvement in Total Exercise TimeTotal Exercise Time
00
3030
6060
9090
120120
ControlControl(n=146)(n=146)
CRTCRT(n=159)(n=159)
seco
nds
seco
nds
P=0.001P=0.001
Baseline Baseline
(ml/kg/min)(ml/kg/min)
13.7 ± 3.8
14.0 ± 3.5
BaselineBaseline
(secondsseconds)
462 ± 217
484 ± 209
Metabolic Exercise
Cardiac Resynchronization Cardiac Resynchronization TherapyTherapyMIRACLE
Abraham WT, Fisher WG, Smith AL, et al. N Engl J Med 2002;346:1845-1853
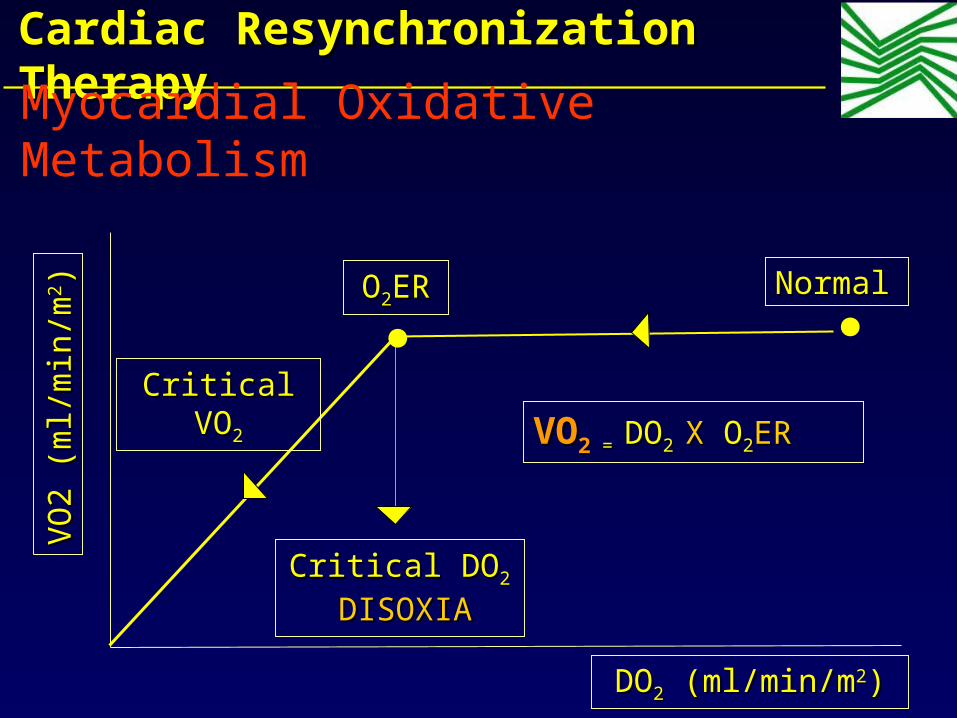
VO
2 (
ml/m
in/m
VO
2 (
ml/m
in/m
22))
DODO22 (ml/min/m (ml/min/m22))
Cardiac Resynchronization Cardiac Resynchronization TherapyTherapy
OO22ERER
Critical DOCritical DO2 2
DISOXIADISOXIA
Critical VOCritical VO22
VOVO22 = = DODO2 2 X X OO22ERER
NormalNormal
Myocardial Oxidative Metabolism

Control 225 214 204 197 191 179 70
CRT 228 218 213 209 204 201 99
Patients At RiskPatients At Risk
70%70%
75%75%
80%80%
85%85%
90%90%
95%95%
100%100%
00 11 22 33 44 55 66
Months After RandomizationMonths After Randomization
Eve
nt F
ree
Eve
nt F
ree
Sur
viva
lS
urvi
val (
%)
(%
)
CRTCRT
ControlControlP = 0.033P = 0.033Relative risk = 0.60; Relative risk = 0.60; 95% CI (0.37, 0.96)95% CI (0.37, 0.96)
Time to Death or Worsening HF requiring Hospitalization
Cardiac Resynchronization Cardiac Resynchronization TherapyTherapyMIRACLE
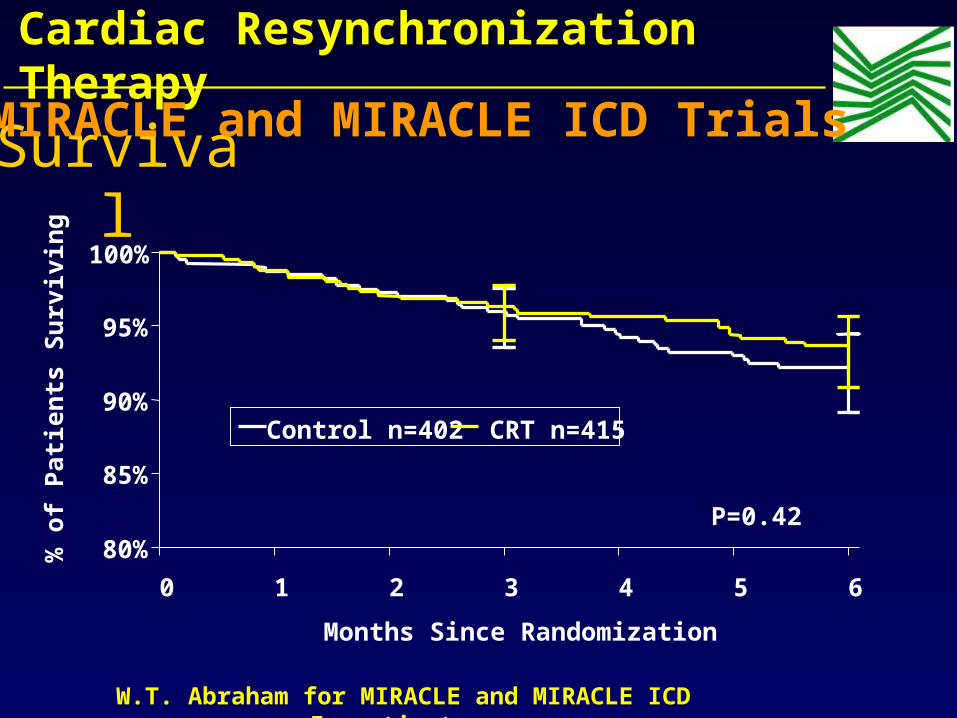
Survival
80%
85%
90%
95%
100%
0 1 2 3 4 5 6
Months Since Randomization
% o
f P
atie
nts
Su
rviv
ing
Control n=402 CRT n=415
P=0.42
W.T. Abraham for MIRACLE and MIRACLE ICD Investigators
Cardiac Resynchronization Cardiac Resynchronization TherapyTherapy
MIRACLE and MIRACLE ICD Trials

QOL & Functional Capacity 6 Months in Moderate to Severe HF
- 20
- 15
- 10
- 5
0
P<0.001 P=0.02 P=0.017P<0.001
QoL Score(MLWHF)
Avg. Change
0%20%40%60%80%
MIRACLE MUSTIC SR MIRACLE ICD Contak CD
P<0.001 P=0.006P=0.007
Data sources:MIRACLE: Circulation 2003;107:1985-90 MUSTIC SR: NEJM 2001;344:873-80MIRACLE ICD:JAMA 2003;289:2685-94 Contak CD: JACC 2003;2003;42:1454-59
Control CRT
NYHA ClassProportion
Changing 1 or more Classes
Improve.
Not Reported
Cardiac Resynchronization Cardiac Resynchronization TherapyTherapy
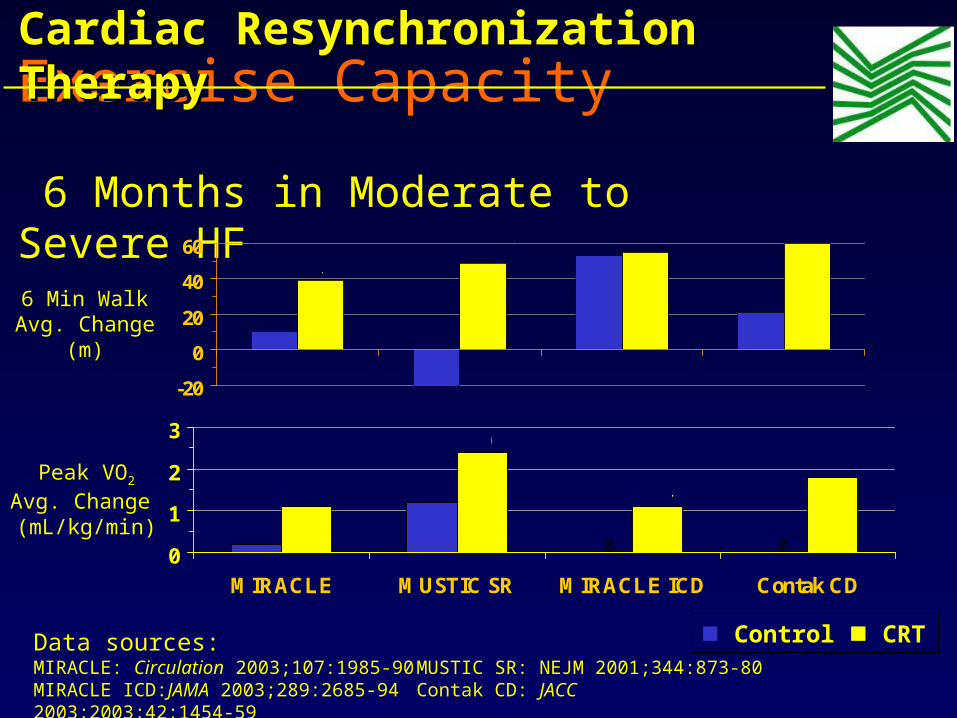
Exercise Capacity 6 Months in Moderate to Severe HF
-20
0
20
40
60 P<0.001 P=0.36 P=0.029
P<0.001
6 Min WalkAvg. Change
(m)
000
1
2
3
MIRACLE MUSTIC SR MIRACLE ICD Contak CD
P<0.001
P=0.029
P=0.04P=0.003
Data sources:MIRACLE: Circulation 2003;107:1985-90 MUSTIC SR: NEJM 2001;344:873-80MIRACLE ICD:JAMA 2003;289:2685-94 Contak CD: JACC 2003;2003;42:1454-59
Control CRT
Peak VO2
Avg. Change (mL/kg/min)
Cardiac Resynchronization Cardiac Resynchronization TherapyTherapy
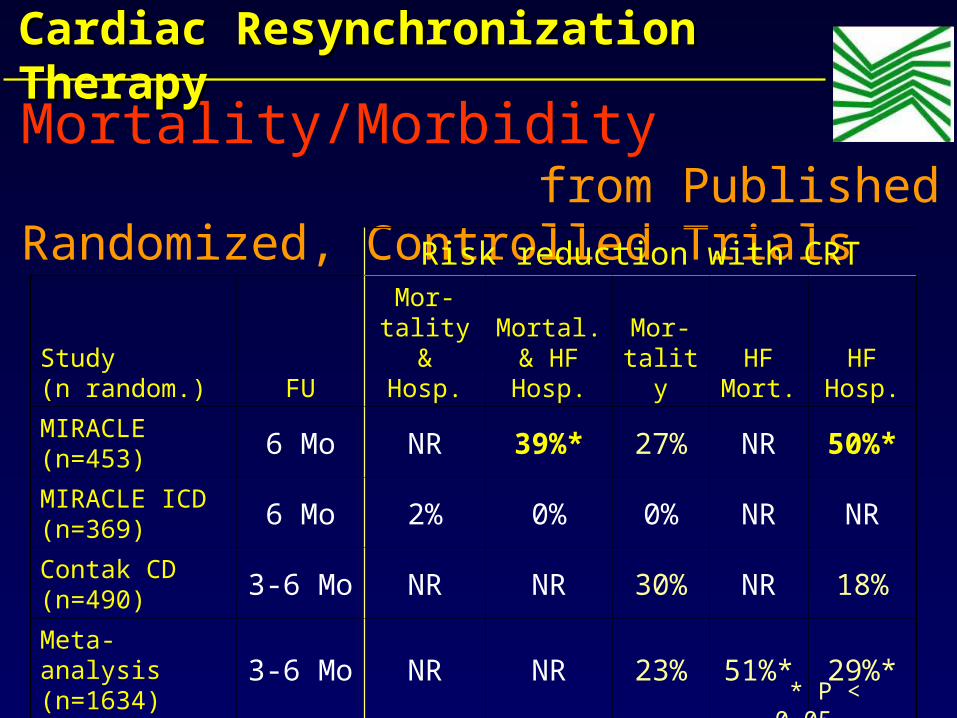
Mortality/Morbidity from Published Randomized, Controlled Trials Risk reduction with CRT
Study (n random.) FU
Mor-tality & Hosp.
Mortal. & HF Hosp.
Mor-tality
HF Mort.
HF Hosp.
MIRACLE (n=453) 6 Mo NR 39%* 27% NR 50%*
MIRACLE ICD (n=369) 6 Mo 2% 0% 0% NR NR
Contak CD (n=490) 3-6 Mo NR NR 30% NR 18%
Meta-analysis (n=1634) 3-6 Mo NR NR 23% 51%* 29%*
* P < 0.05
Cardiac Resynchronization Cardiac Resynchronization TherapyTherapy
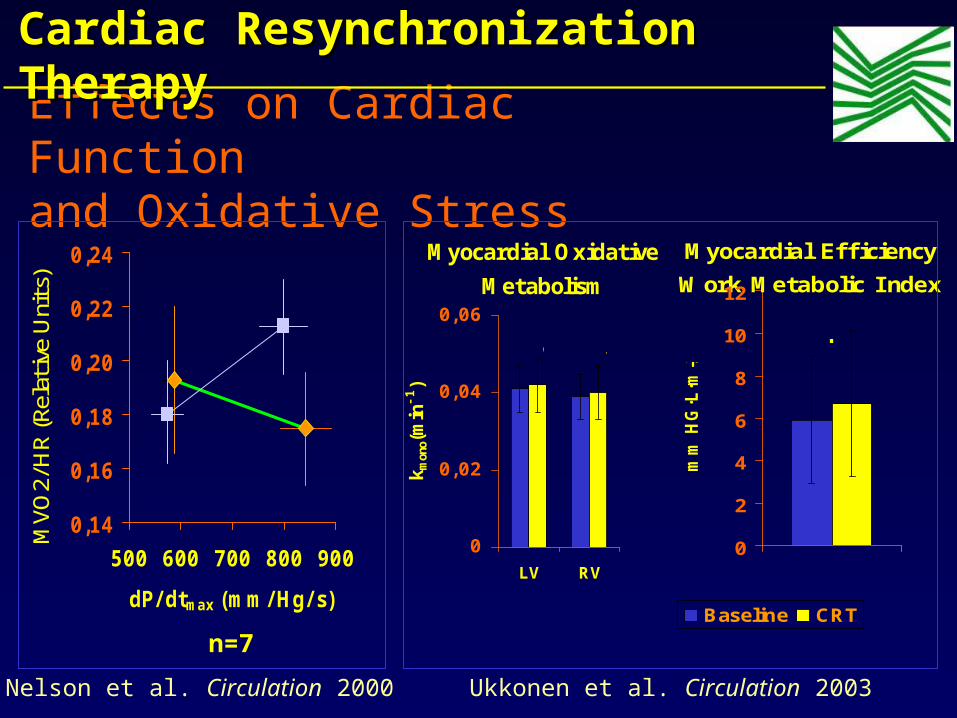
Effects on Cardiac Function and Oxidative Stress
0,14
0,16
0,18
0,20
0,22
0,24
500 600 700 800 900
dP/ dtmax (mm/ Hg/ s)
MVO
2/H
R (R
elat
ive
Uni
ts) Dobutamin
LV Pacing
P<0.05
Nelson et al. Circulation 2000
Myocardial Oxidative
Metabolism
0
0,02
0,04
0,06
LV RV
k mon
o(m
in-1)
p=0.86
p=0.62
n=8
Myocardial Efficiency
Work Metabolic Index
0
2
4
6
8
10
12
mm
HG
·L·m
-2
Baseline CRT
p =0.024
Ukkonen et al. Circulation 2003
n=7
Cardiac Resynchronization Cardiac Resynchronization TherapyTherapy

CRT Does Not Promote Ventricular Arrhythmias
• Analyzed 1,044 patients with ICDs from 2 trials:– CONTAK CD– MIRACLE ICD
• Odds ratio (CI):0.92 (0.67 – 1.27)
Patients with VT or
VF during Follow-up
17,2%18,4%
No CRT CRT
Prop
orti
on
Bradley DJ, et al. JAMA 2003
Cardiac Resynchronization Cardiac Resynchronization TherapyTherapy

Baseline ex CPX
ImplantAttempt
SuccessfulImplant
ControlICD
CRTCRT + ICD
Pre-dischargeRandomization
6 Month Follow-up
6 Month Follow-up
CRT
DoubleBlinded
StableMedicalTherapy
1week
•Class NYHA II
•Intent to treat analyses
•Comparison between groups
•Core labs: metabolic exercise, echocardiography, and neurohormone data
CRT
Long term follow up every 6 months
CPX
Cardiac Resynchronization Cardiac Resynchronization TherapyTherapyMIRACLE ICD II

210 Class II 429 Class III/IV
98 Completed 6M FU 82 Completed 6M FU
2 Death 2
1 Missed 6M FU 1
101 Control (ICD+OPT) 85 CRT (CRT+ICD+OPT)
639 Enrolled and Implant Attempted
19 Unsuccessful 191 (91%) Successful
186 Randomized
5 not randomized- 1 death- 4 LV lead dislodge.
Cardiac Resynchronization Cardiac Resynchronization TherapyTherapyMIRACLE ICD II

Left Ventricular End Systolic Diameter
200
250
300
350
400cm3
Base 6 Mo
P=0.01
Reverse Remodeling in Class II CHF
Left Ventricular End Diastolic Diameter
200
250
300
350
400cm3
Base 6 Mo
P=0.04
Left Ventricular Ejection Fraction
20
22
24
26
28
30%
Base 6 Mo
P=0.02
Control (n=85) CRT (n=69)
Cardiac Resynchronization Cardiac Resynchronization TherapyTherapyMIRACLE ICD II
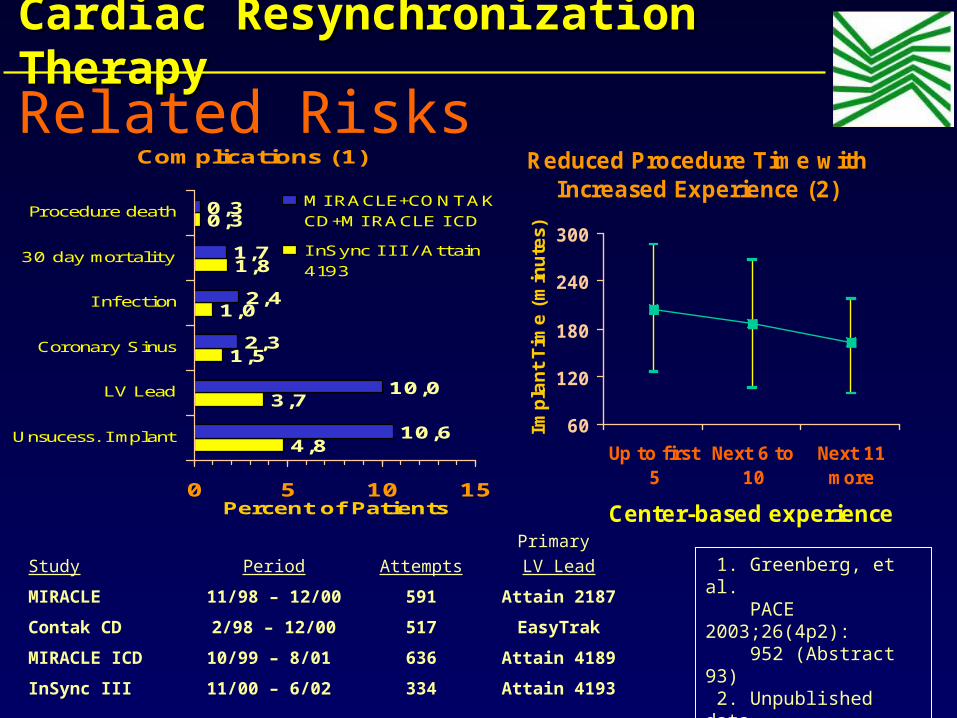
Cardiac Resynchronization Cardiac Resynchronization TherapyTherapyRelated Risks
Complications (1)
4,8
3,7
1,5
1,0
1,8
0,3
10,6
10,0
2,3
2,4
1,7
0,3
0 5 10 15
Unsucess. I mplant
LV Lead
Coronary Sinus
I nfection
30 day mortality
Procedure death
Percent of Patients
MI RACLE+CONTAKCD+MI RACLE I CD
I nSync I I I / Attain4193
Reduced Procedure Time with Increased Experience (2)
60
120
180
240
300
Up to first5
Next 6 to10
Next 11more
Center-based experienceIm
pla
nt Tim
e (
min
ute
s) P < 0.001
Study Period AttemptsPrimary LV Lead
MIRACLE 11/98 – 12/00 591 Attain 2187
Contak CD 2/98 – 12/00 517 EasyTrak
MIRACLE ICD 10/99 – 8/01 636 Attain 4189
InSync III 11/00 – 6/02 334 Attain 4193
1. Greenberg, et al. PACE 2003;26(4p2): 952 (Abstract 93)
2. Unpublished data. Medtronic. Inc.
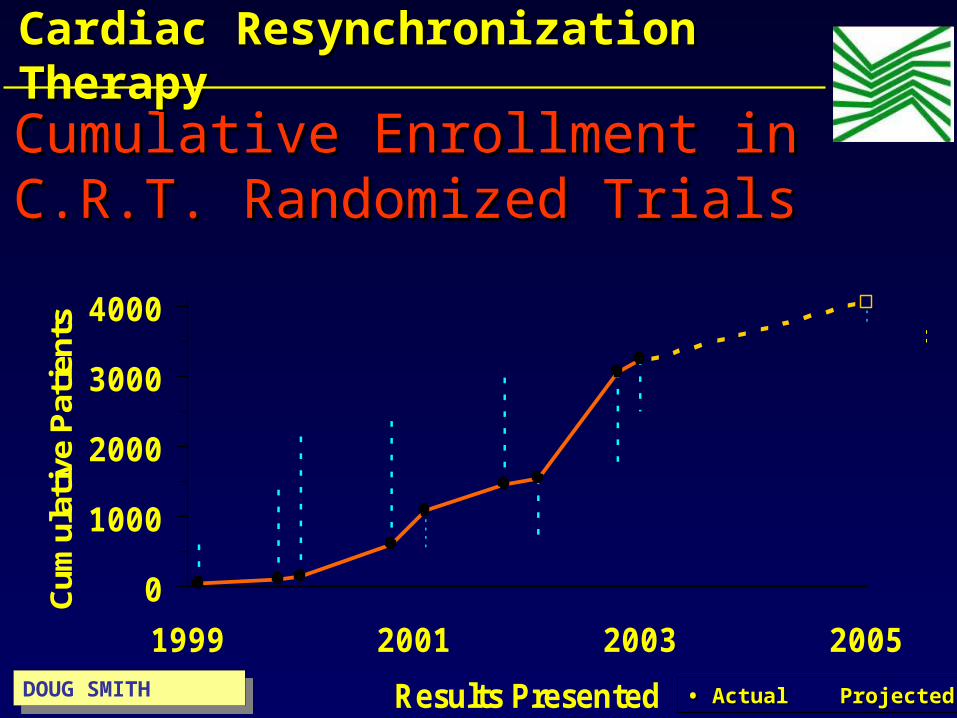
Cumulative Enrollment in Cumulative Enrollment in C.R.T. Randomized TrialsC.R.T. Randomized Trials
0
1000
2000
3000
4000
1999 2001 2003 2005
Results Presented
Cum
ulat
ive
Pat
ient
s
PATH CHF
MUSTI C SR
MUSTI C AFMI RACLE
CONTAK CD
MI RACLE I CD
PATH CHF I I
COMPANI ON
MI RACLE I CD I I
CARE HF
• • Actual Projected�Actual Projected�DOUG SMITHDOUG SMITH
Cardiac Resynchronization Cardiac Resynchronization TherapyTherapy

0
5000
10000
15000
Baseline Post-implant
Intensive care
Cardiology
Others
Patient Cost Baseline: 12,784 Euro Patient Cost (Implant included): 12,362 EuroPatient Cost Post-implant: 1,680 Euro
Hospital costs per patient
Cost EffectivenessAnalysis of Biventricular Pacing in HF
Curnis A 2001
Cardiac Resynchronization Cardiac Resynchronization TherapyTherapy

Relative Cost of CRTCost per patient
$0$20$40$60
CRT+ICD
CRT
Hip/ knee replace
PTCA
CABG
Dialysis
$ thousands
Total Annual Expenditures
$0 $5 $10 $15 $20
$ BillionsDoug Smith:
Doug Smith:
Cardiac Resynchronization Cardiac Resynchronization TherapyTherapy
Weight of Evidence: CRT• More than 4000 patients evaluated in
randomized controlled trials
• Consistent improvement in QOL, functional status, and exercise capacity
• Strong evidence for reverse remodeling– ↓ LV volumes and dimensions LV ejection fraction– ↓ Mitral regurgitation
Courtesy of Dr. Bill Abraham
Cardiac Resynchronization Cardiac Resynchronization TherapyTherapy
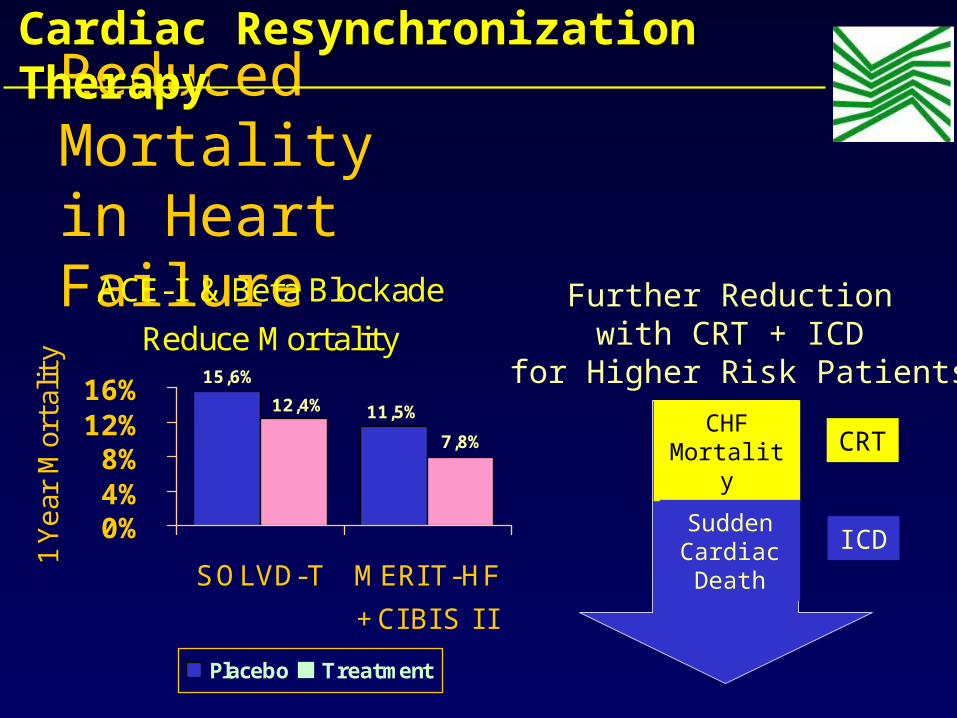
Reduced Mortality in Heart Failure
ACE-I & Beta Blockade
Reduce Mortality
11,5%
15,6%
12,4%
7,8%
0%4%8%
12%16%
SOLVD-T MERI T-HF
+ CI BI S I I
1 Yea
r M
orta
lity
Placebo Treatment
Further Reduction with CRT + ICD
for Higher Risk Patients
CHFMortality
SuddenCardiac Death
CRT
ICD
Cardiac Resynchronization Cardiac Resynchronization TherapyTherapy
Cardiac Resynchronization Cardiac Resynchronization TherapyTherapy
• CRT in NYHA class II ? • Which implication in pts with unstable Haemodinamic profile ? • CRT in chronic Atrial Fibrillation ?
• CRT in Right Bundle Branch Block ?
• QRS<120ms or QTc dispersion ?
• “Up-grading” in RVA pacing ?
Actual Key QuestionsActual Key Questions

Creating Realistic patients expectations
Cardiac Resynchronization Cardiac Resynchronization TherapyTherapy
• Approximately two-third of patients should experience improvement (responders vs. non-responders)1
• Some patients may not experience immediate improvement
• Have patients set their own goals of what they would like to do following CRT: Grocery shopping, Decreasing Lasix dose Walking to the mailbox without stopping, Lying flat to sleep
• Encourage them to be part of the group that responds to their therapy
Cardiac Resynchronization Cardiac Resynchronization TherapyTherapy
Creating Realistic patients expectations


















