Resincronizzazione cardiaca: opportunità sospinta anche dalle … · 2018-03-29 ·...
51
Resincronizzazione cardiaca: opportunità sospinta anche dalle nuove tecnologie? Davide Giorgi, MD U.O. Cardiologia Elettrofisiologia e Cardiostimolazione P.O. San Luca Lucca (Italy)
Transcript of Resincronizzazione cardiaca: opportunità sospinta anche dalle … · 2018-03-29 ·...

Resincronizzazione cardiaca: opportunità sospinta anche dalle nuove
tecnologie?
Davide Giorgi, MD
U.O. Cardiologia
Elettrofisiologia e Cardiostimolazione
P.O. San Luca
Lucca (Italy)

La CRT Oggi: efficace e riconosciuta…
Ponikowski P, Voors AA & al.
2016 ESC GL acute & chronic HF. Eur Heart J 2016 May
Indicazione di classe I / II (a-b) in pz HF-sintomatici con:
- terapia medica ottimale
- LVEF ridotta
- dissincronia elettrica (QRS>130ms)
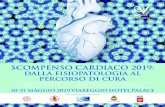
… ma ci sono ancora molti NON-Responder
Daubert JC & al. Heart Rhythm 2012 (CRT consensus document)
45%
20%
Daubert JC & al. Eur Heart J 2016;
doi:10.1093/eurheartj/ehw270
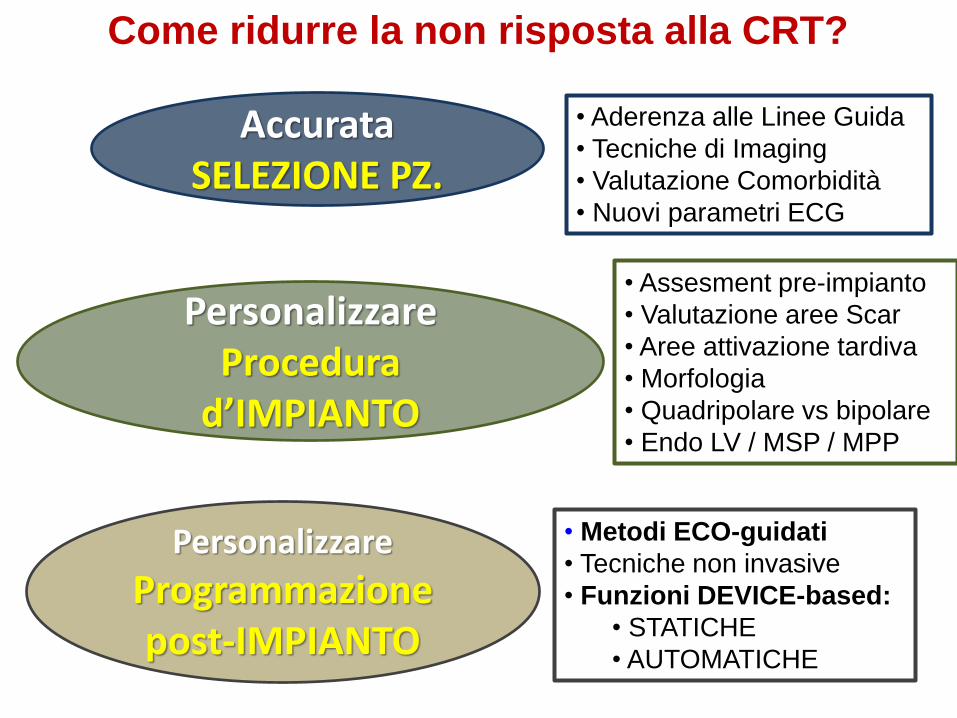
Come ridurre la non risposta alla CRT?
AccurataSELEZIONE PZ.
• Aderenza alle Linee Guida
• Tecniche di Imaging
• Valutazione Comorbidità
• Nuovi parametri ECG
PersonalizzareProcedura
d’IMPIANTO
• Assesment pre-impianto
• Valutazione aree Scar
• Aree attivazione tardiva
• Morfologia
• Quadripolare vs bipolare
• Endo LV / MSP / MPP
Personalizzare
Programmazione post-IMPIANTO
• Metodi ECO-guidati
• Tecniche non invasive
• Funzioni DEVICE-based:
• STATICHE
• AUTOMATICHE
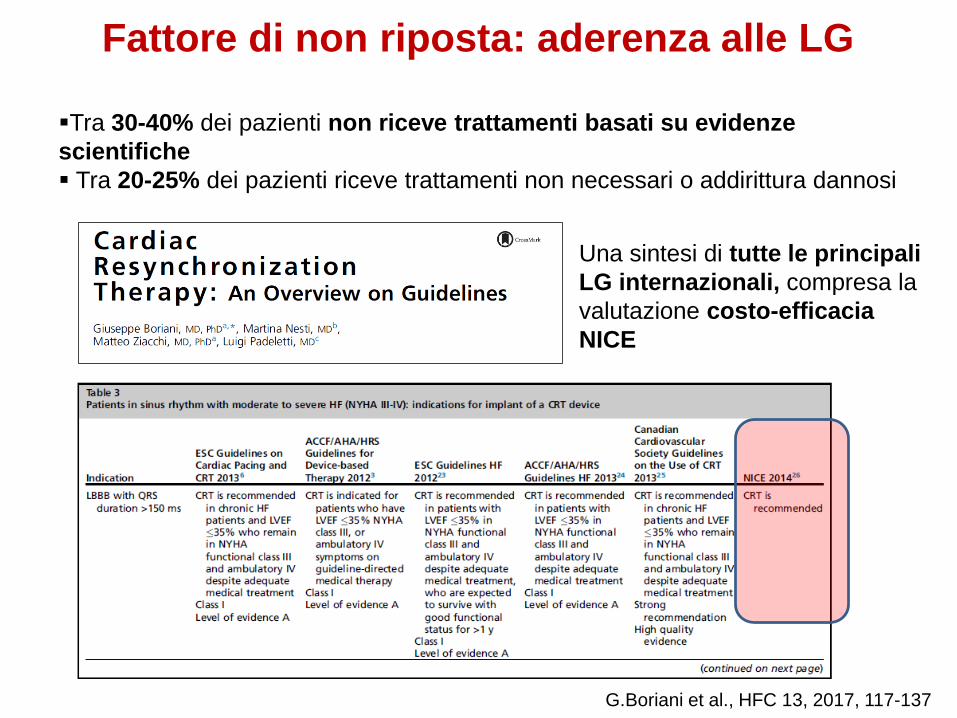
Fattore di non riposta: aderenza alle LG
▪Tra 30-40% dei pazienti non riceve trattamenti basati su evidenze
scientifiche
▪ Tra 20-25% dei pazienti riceve trattamenti non necessari o addirittura dannosi
Una sintesi di tutte le principali
LG internazionali, compresa la
valutazione costo-efficacia
NICE
G.Boriani et al., HFC 13, 2017, 117-137
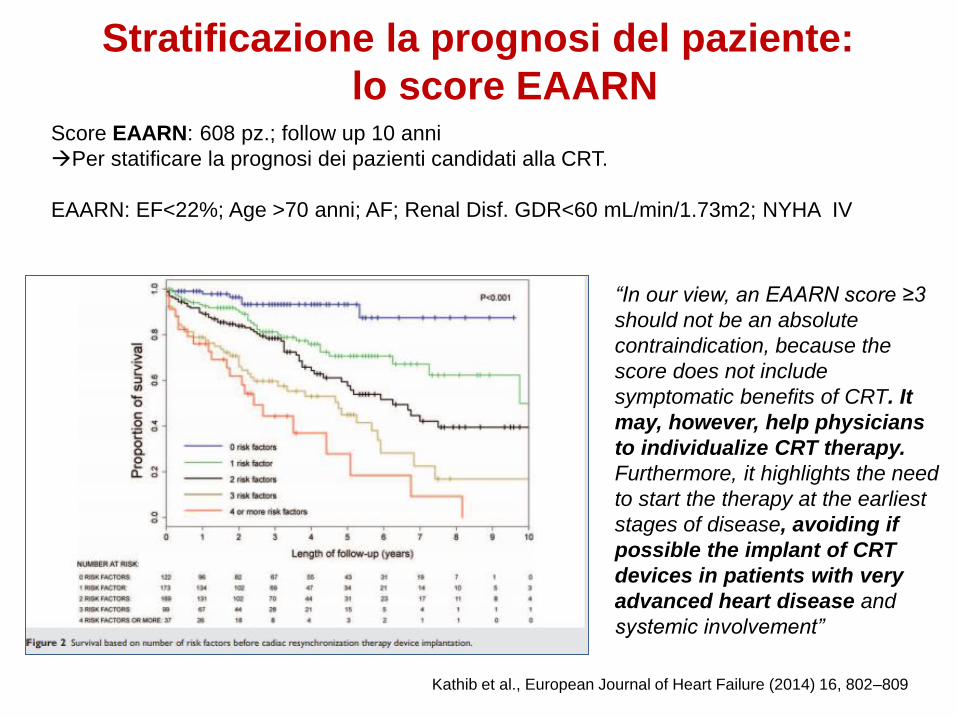
Stratificazione la prognosi del paziente:
lo score EAARN
Kathib et al., European Journal of Heart Failure (2014) 16, 802–809
Score EAARN: 608 pz.; follow up 10 anni
Per statificare la prognosi dei pazienti candidati alla CRT.
EAARN: EF<22%; Age >70 anni; AF; Renal Disf. GDR<60 mL/min/1.73m2; NYHA IV
“In our view, an EAARN score ≥3
should not be an absolute
contraindication, because the
score does not include
symptomatic benefits of CRT. It
may, however, help physicians
to individualize CRT therapy.
Furthermore, it highlights the need
to start the therapy at the earliest
stages of disease, avoiding if
possible the implant of CRT
devices in patients with very
advanced heart disease and
systemic involvement”
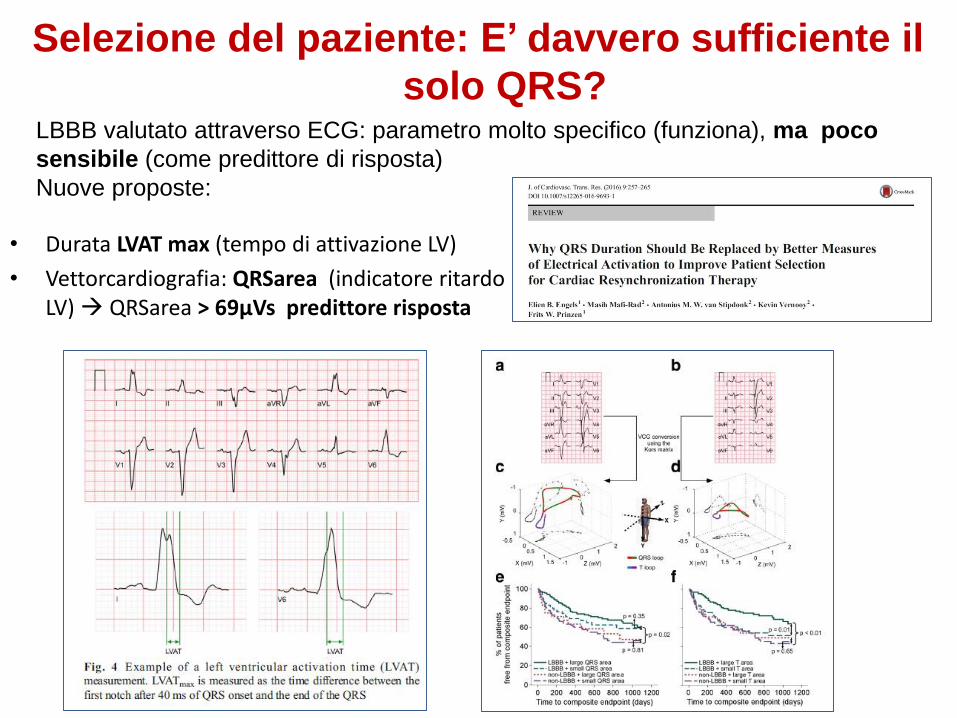
• Durata LVAT max (tempo di attivazione LV)
• Vettorcardiografia: QRSarea (indicatore ritardo LV) QRSarea > 69μVs predittore risposta
Selezione del paziente: E’ davvero sufficiente il
solo QRS?LBBB valutato attraverso ECG: parametro molto specifico (funziona), ma poco
sensibile (come predittore di risposta)
Nuove proposte:

• Misure Echo standard
• Echo speckle tracking difficoltà riproduzione risultati con software diversi (standardizzazione)
Selezione del paziente tramite imaging
Everdingen et al., Cardiovasc Ultrasound. 2017 Oct 18;15(1):25. Doltra et al.Volume 7, Issue 10, October 2014, Pages 969-979
Non accordo su possibilità di stratificazione pz attraverso valutazione dissincronia
meccanica per imaging (studio Prospect)
Problema: non standardizzazione delle misure
Echo speckle tracking
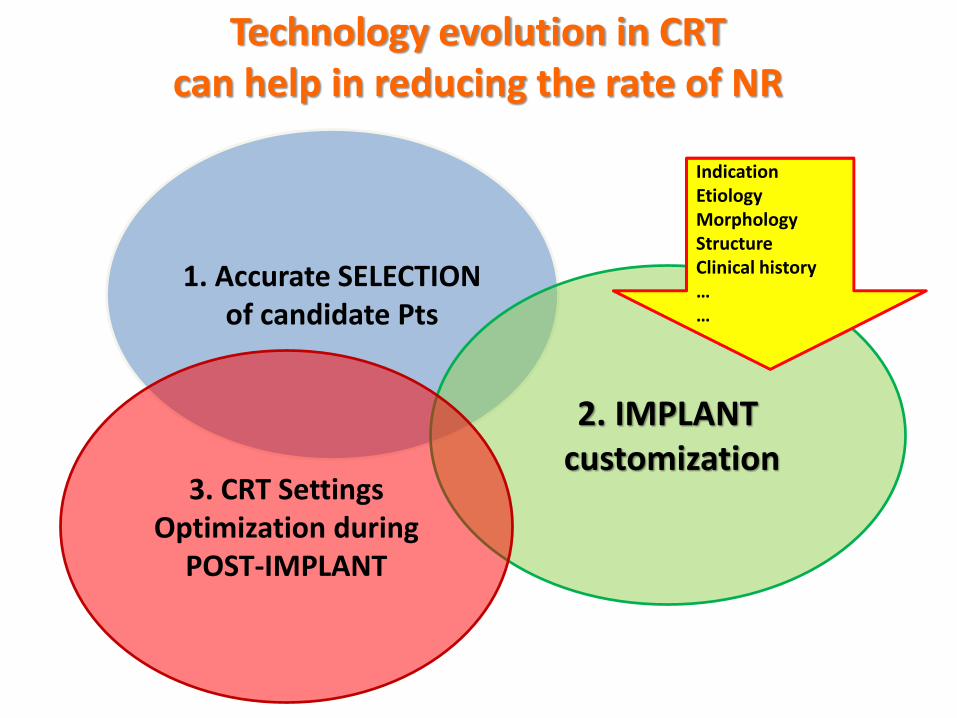
Technology evolution in CRT can help in reducing the rate of NR
1. Accurate SELECTIONof candidate Pts
2. IMPLANT customization
3. CRT SettingsOptimization during
POST-IMPLANT
IndicationEtiologyMorphologyStructureClinical history……
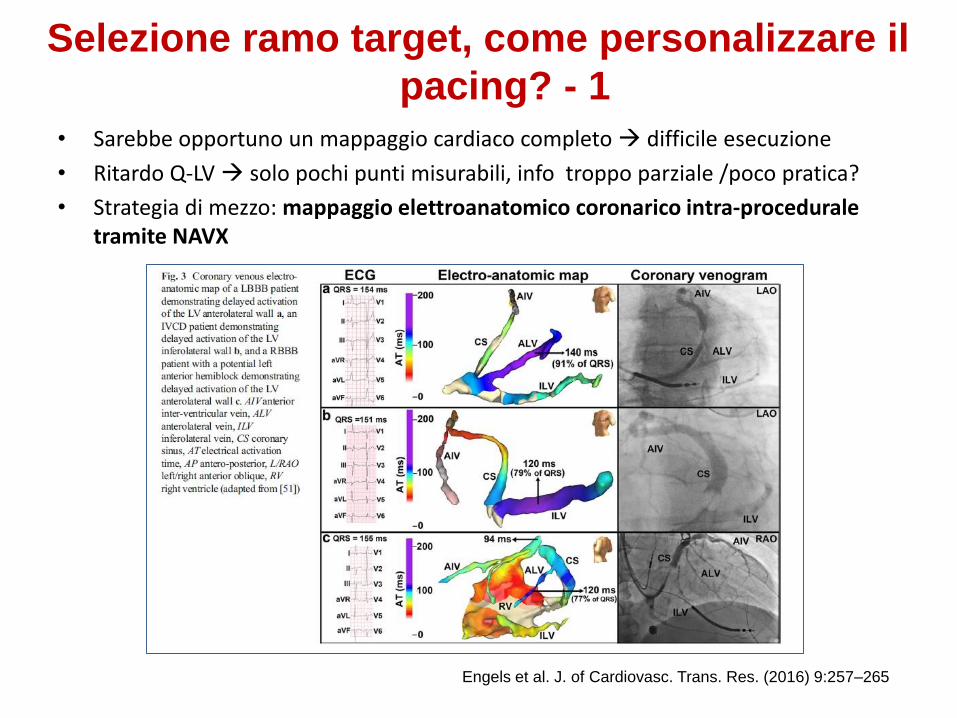
• Sarebbe opportuno un mappaggio cardiaco completo difficile esecuzione
• Ritardo Q-LV solo pochi punti misurabili, info troppo parziale /poco pratica?
• Strategia di mezzo: mappaggio elettroanatomico coronarico intra-proceduraletramite NAVX
Selezione ramo target, come personalizzare il
pacing? - 1
Engels et al. J. of Cardiovasc. Trans. Res. (2016) 9:257–265

• Body surface Activation Mapping (BSAM, non invasiva)
• Parametro: SDAT (deviazione standard delle attivazioni)
• SDAT si riduce del 20% con stimolazione BIV vs basale
• Ulteriore riduzione del 26% nel ramo target (tutte eziologie dei pz.)
• Pazienti con LBBB e QRS>150 ↑ SDAT basale ↑ riduzione SDAT
Selezione ramo target, come personalizzare il
pacing? - 2
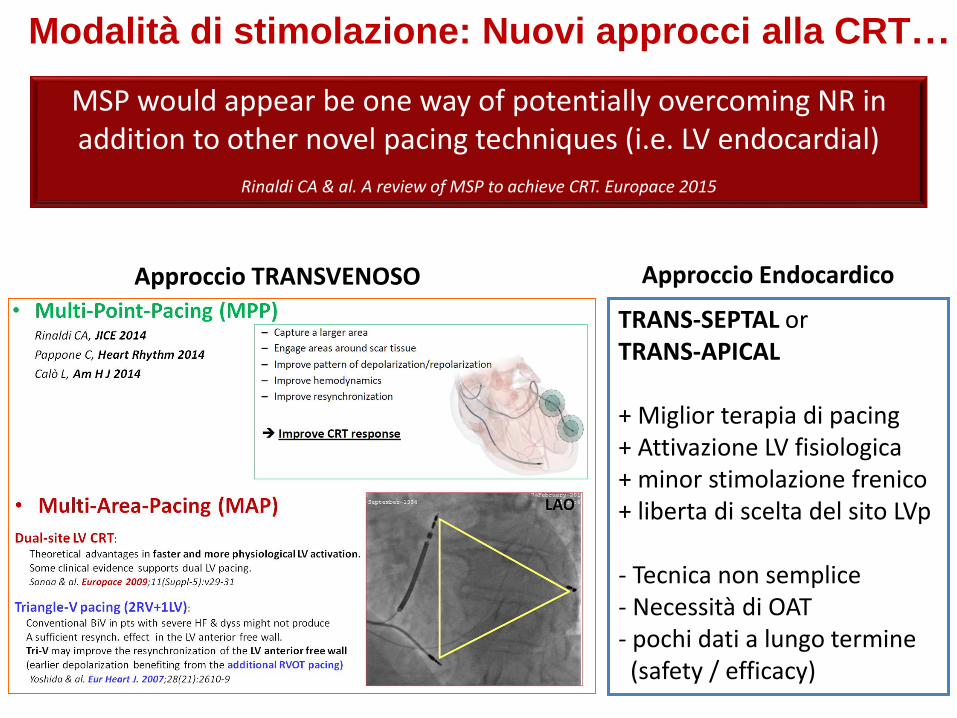
Modalità di stimolazione: Nuovi approcci alla CRT…
MSP would appear be one way of potentially overcoming NR in addition to other novel pacing techniques (i.e. LV endocardial)
Rinaldi CA & al. A review of MSP to achieve CRT. Europace 2015
TRANS-SEPTAL orTRANS-APICAL
+ Miglior terapia di pacing+ Attivazione LV fisiologica+ minor stimolazione frenico+ liberta di scelta del sito LVp
- Tecnica non semplice- Necessità di OAT - pochi dati a lungo termine(safety / efficacy)
Approccio TRANSVENOSO Approccio Endocardico

Evoluzione della terapia CRT
LV1-RV (@ t0)
LV2-RV (@ t1)
BIP LV 4P LV 4P LV+ MPP
BIVp (RV+LV1):
• 1 LV vector (non-progr.)
• 1 among few LV vectors
• Ritardo RV-LV progr.
BIVp (RV+LV1):
• 1 among many LV vect.
• Progr. RV-LV delay
MPP (RV + 2 LV vectors)
• 2 among many LV vect.
• Progr. RV-LV delay• LV1-LV2 sequential• LV1-LV2 simultaneous
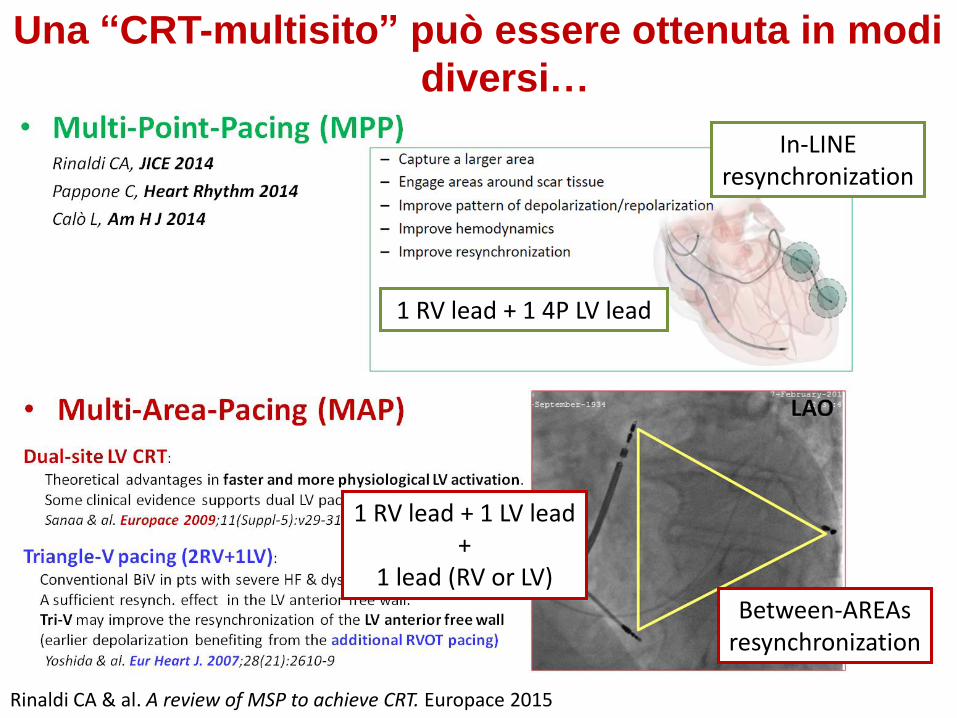
Una “CRT-multisito” può essere ottenuta in modi
diversi…
with a single LV lead or more leads …
Rinaldi CA & al. A review of MSP to achieve CRT. Europace 2015
In-LINEresynchronization
1 RV lead + 1 4P LV lead
Between-AREAsresynchronization
1 RV lead + 1 LV lead+
1 lead (RV or LV)

Multi-Area-Pacing in CRT dedicated technologies
…CRT-D systemmodified header with 3 V ports
• SKIPS using Y-ADAPTORS• ALLOWS hypothetical TriV configur.:
• Dual-site LV
• Dual-site RV
Dual-site LV
(1RV+2LV)
Dual-site RV
(2RV+1LV)
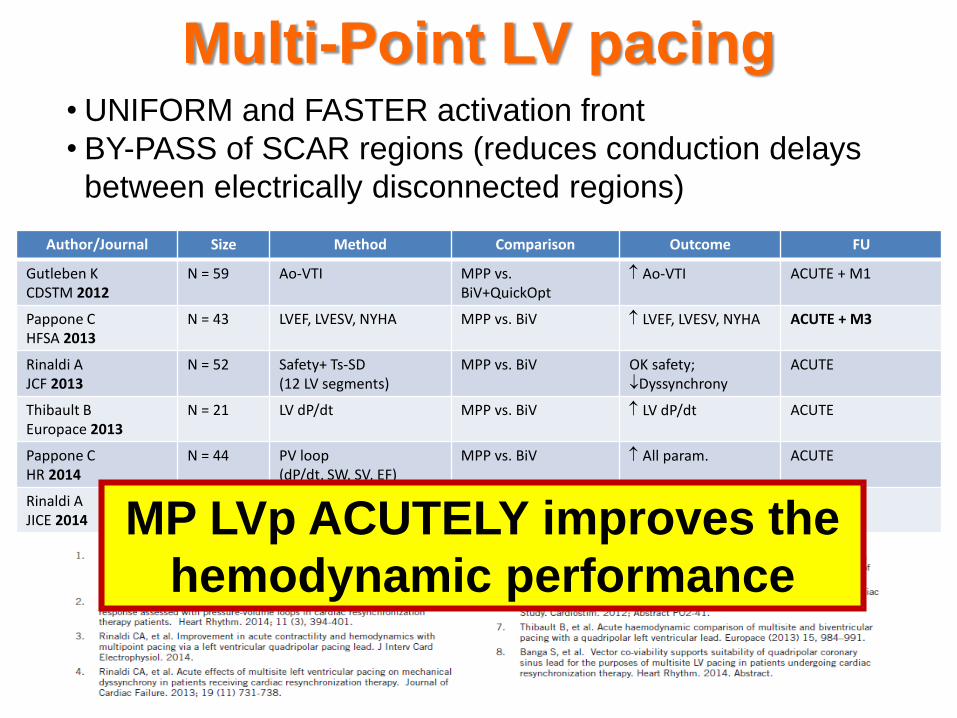
Multi-Point LV pacing• UNIFORM and FASTER activation front
• BY-PASS of SCAR regions (reduces conduction delays
between electrically disconnected regions)
Author/Journal Size Method Comparison Outcome FU
Gutleben KCDSTM 2012
N = 59 Ao-VTI MPP vs. BiV+QuickOpt
Ao-VTI ACUTE + M1
Pappone CHFSA 2013
N = 43 LVEF, LVESV, NYHA MPP vs. BiV LVEF, LVESV, NYHA ACUTE + M3
Rinaldi AJCF 2013
N = 52 Safety+ Ts-SD(12 LV segments)
MPP vs. BiV OK safety;Dyssynchrony
ACUTE
Thibault BEuropace 2013
N = 21 LV dP/dt MPP vs. BiV LV dP/dt ACUTE
Pappone CHR 2014
N = 44 PV loop(dP/dt, SW, SV, EF)
MPP vs. BiV All param. ACUTE
Rinaldi AJICE 2014
N = 40 Strain-echoLVOT-VTI
MPP vs. BiV All param. ACUTE
MP LVp ACUTELY improves the
hemodynamic performance

1717
STUDIO MPP-IDE, MULTICENTRICO; N = 381 PZ RANDOMIZZATI (1:1) BIV VS. MPP
Una stimolazione LV Multi-Point « mirata »migliora il tasso di responder (vs. BiV)
Bi-V arm MPP arm
70%
100%
25%
75%
29.9%
70.1%
Endpoint primario di efficacia1
Non-inferiority
Tasso di
Non
responder
Tasso di
Responder
La stimolazione LV MP con un ritardo minimo tra i 2 vettori
di stimolazione LV ha fornito il miglior tasso di risposta1
1. Tomassoni GF.et al. Late-Breaking Clinical Trials I, LBCT01-03 - Safety and efficacy of Multipoint
Pacing in Cardiac Resynchronization Therapy: The MultiPoint Pacing (MPP) IDE Study. Presented
at Heart Rhythm 2016 - 05/05/16.
< 30 mm SpacialSeparation (n=115)
≥ 30 mm Spatial Separation & > 5 ms Timing Delay
(n=32)
≥ 30 mm Spatial Separation & 5 ms
Timing Delay (n=52)
63%
87%
69%
Analisi ancillare1
Tasso di risposta nei sottogr. del
braccio MPP
60%
100%

Zanon F & al. MPP by a LV 4P lead improves the acute hemodynamic response to CRT compared with conventional BiVp at any site.
Heart Rhythm 2015
ACUTE effects of MP LVpn = 29 pts - mean age 72 yrs NYHA II/III: 17%/83%
Ischemic CMP 62% Mean EF 29% - mean QRS 183ms
LBBB 66%, RBBB 21%, IVCD 7% PM-dependant 7%
All pts, all veinsWORST site (dP/dt)
BEST site (dP/dt)

Zanon F & al. Optimization of LVp site plus MPP improves remodeling and clinical response to CRT at 1 year. Heart Rhythm 2016
MP LVp: mid & long-term OUTCOMES
bip LV lead bip or 4P LV lead +
LV site optim.
4P LV lead +
LV site optim +
MPP ON
Hemod. / Clinical Response @ 1Y FU:1. ESVi: delta-LVESV>15%
2. NYHA: delta > -1 class
3. Packer: death / HFH / NYHA > -1
Multi-Point LVp “AMPLIFIES” the
hemodynamic and clinical response to CRT
n = 110 CRT-D pts

CRT3P-MPP
Umar F et al. Europace 2016;18:1227-34
A novel approach for
CRT in ISCHEMIC pts
with extensive scar
New frontiers of MP LVp:
ISCHEMIC PTS
Proprietary and confidential — do not distribute
2012First MPP device
implanted in Italy
MPP Experience : esperienza
1475 pazienti arruolati!
10 studi in acuto - 239 pz
5 studi in cronico - 936 pz
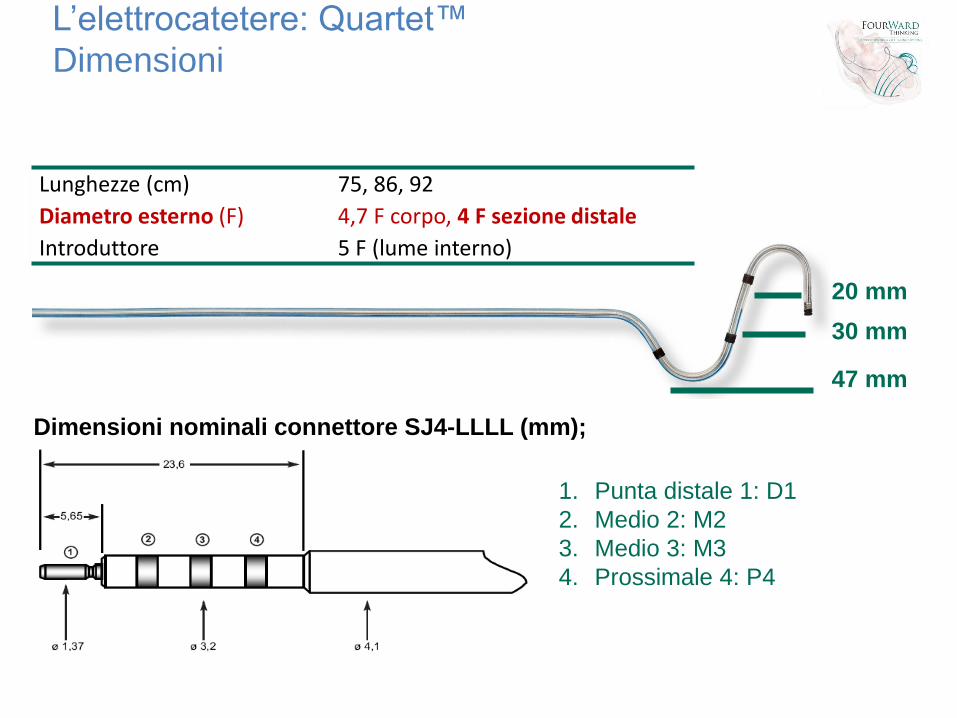
L’elettrocatetere: Quartet™
Dimensioni
47 mm
30 mm
20 mm
Lunghezze (cm) 75, 86, 92
Diametro esterno (F) 4,7 F corpo, 4 F sezione distale
Introduttore 5 F (lume interno)
1. Punta distale 1: D1
2. Medio 2: M2
3. Medio 3: M3
4. Prossimale 4: P4
Dimensioni nominali connettore SJ4-LLLL (mm);
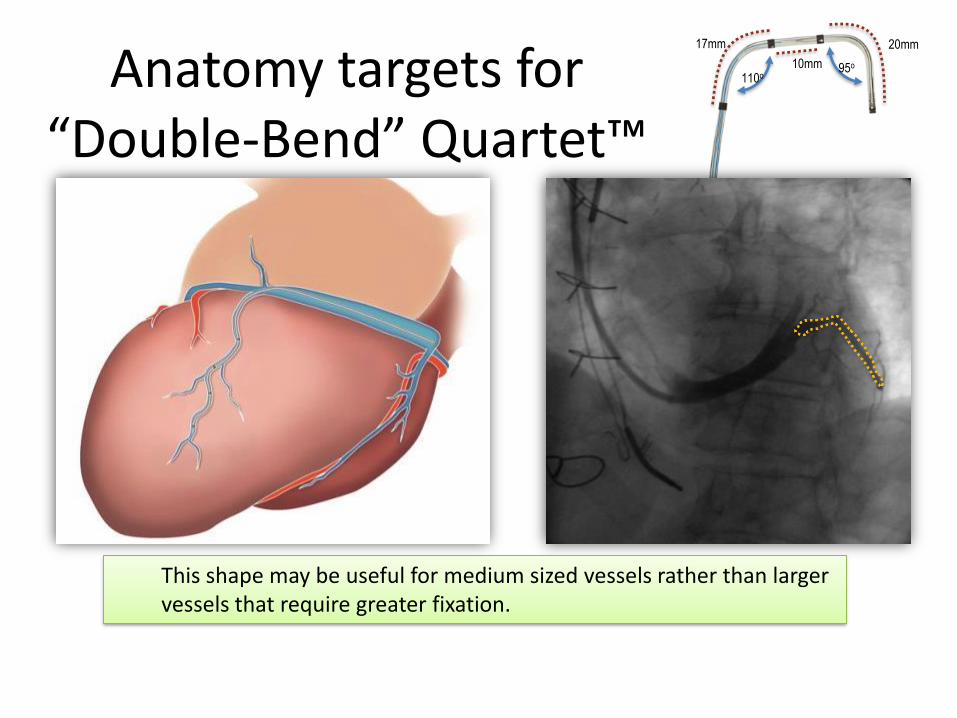
20mm
10mm
17mm
95o
110oAnatomy targets for “Double-Bend” Quartet™
LV LEAD
This shape may be useful for medium sized vessels rather than larger vessels that require greater fixation.
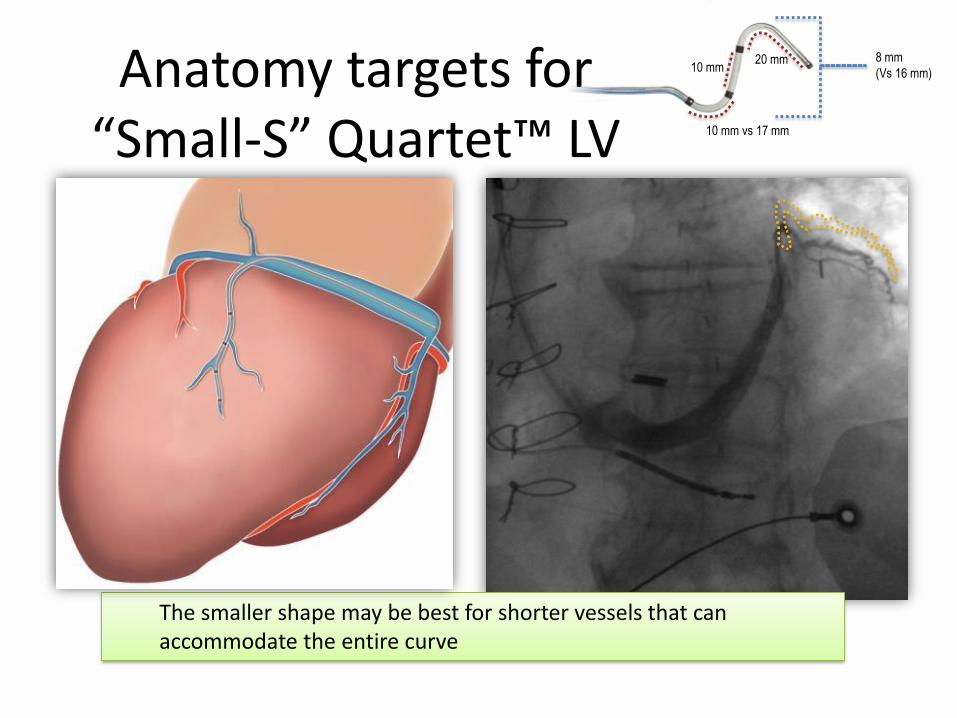
Anatomy targets for “Small-S” Quartet™ LV
Lead
The smaller shape may be best for shorter vessels that can accommodate the entire curve
20 mm10 mm
10 mm vs 17 mm
8 mm
(Vs 16 mm)

Anatomy targets on “wide-spaced” Quartet™
LV LEAD
This shape and spacing may be best for longer vessels that can accommodate the large S-curve and all electrodes.
20 mm
27mm (vs 10 mm)
13 mm
(vs 17 mm)16 mm

L’elettrocatetere: Quartet™Benefici
P4
M3
M2
D1
Ridurre la necessità direintervento/revisione chirurgica
Offrire opzioni per la gestione di PNS e altre soglie di stimolazione
Garantire la scelta del miglior sito distimolazione senza comprometterela stabilità dell’elettrodo
Diminuire i costi per ospedalizzazionie revisione chirurgica vs Bipolare

MultiPointTM PacingMultiPoint™ pacing delivers two pulses from the Quartet™ LV lead per pacing cycle, resulting in a more uniform ventricular contraction
• Allows LV first or RV first
• Delays between pulses are programmable
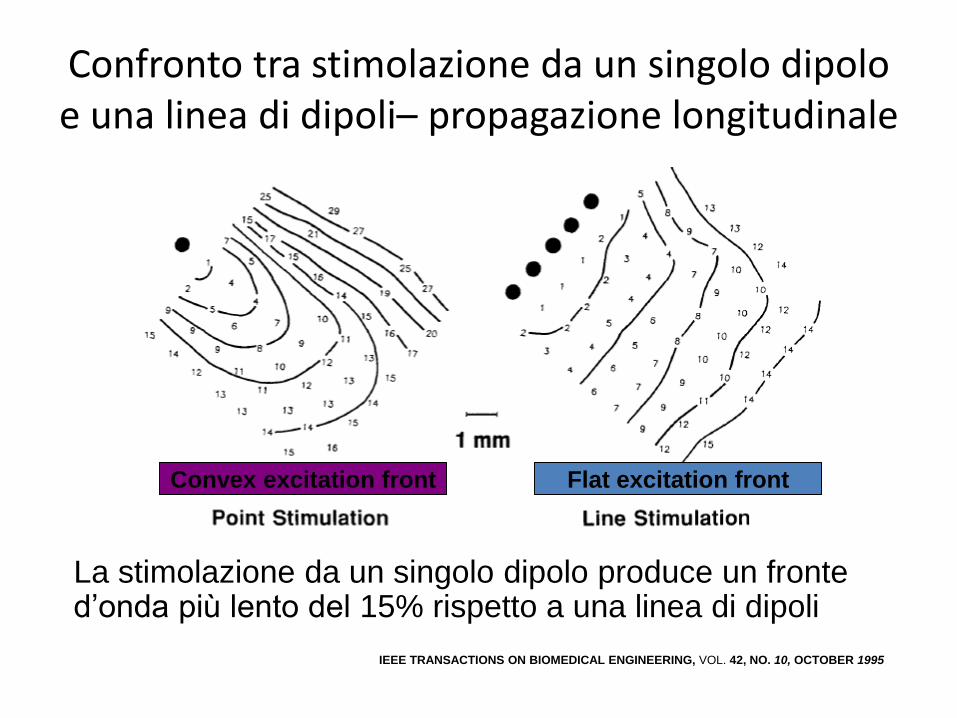
Confronto tra stimolazione da un singolo dipoloe una linea di dipoli– propagazione longitudinale
Convex excitation front Flat excitation front
La stimolazione da un singolo dipolo produce un fronte d’onda più lento del 15% rispetto a una linea di dipoli
IEEE TRANSACTIONS ON BIOMEDICAL ENGINEERING, VOL. 42, NO. 10, OCTOBER 1995
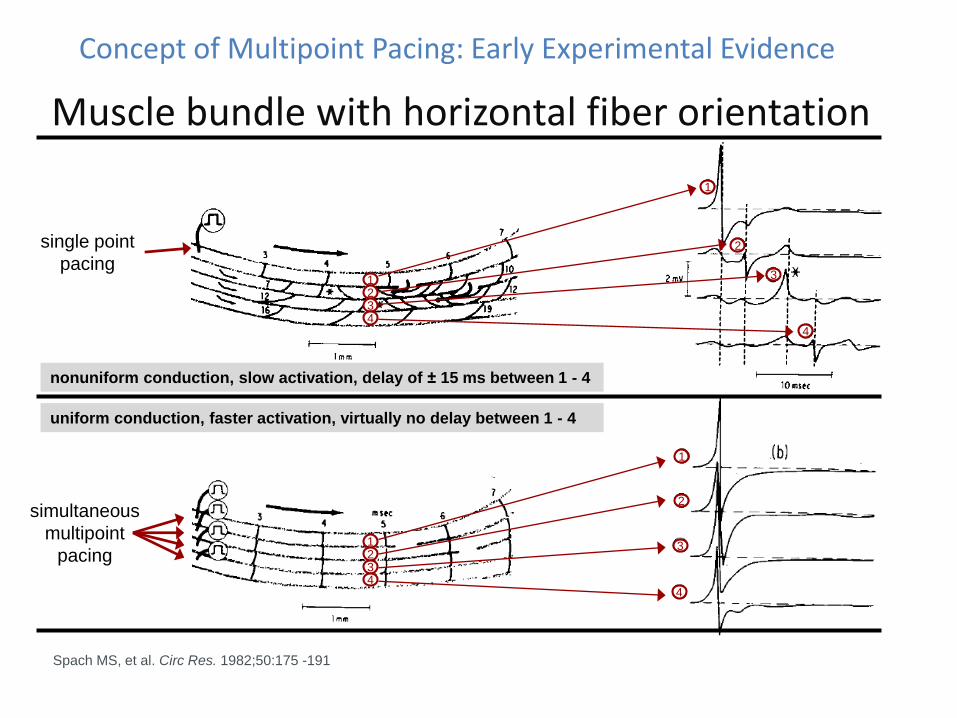
Concept of Multipoint Pacing: Early Experimental Evidence
Muscle bundle with horizontal fiber orientation
Spach MS, et al. Circ Res. 1982;50:175 -191
nonuniform conduction, slow activation, delay of ± 15 ms between 1 - 4
single point
pacing
simultaneous
multipoint
pacing
uniform conduction, faster activation, virtually no delay between 1 - 4
1234
1234
1
2
3
4
1
2
3
4
30
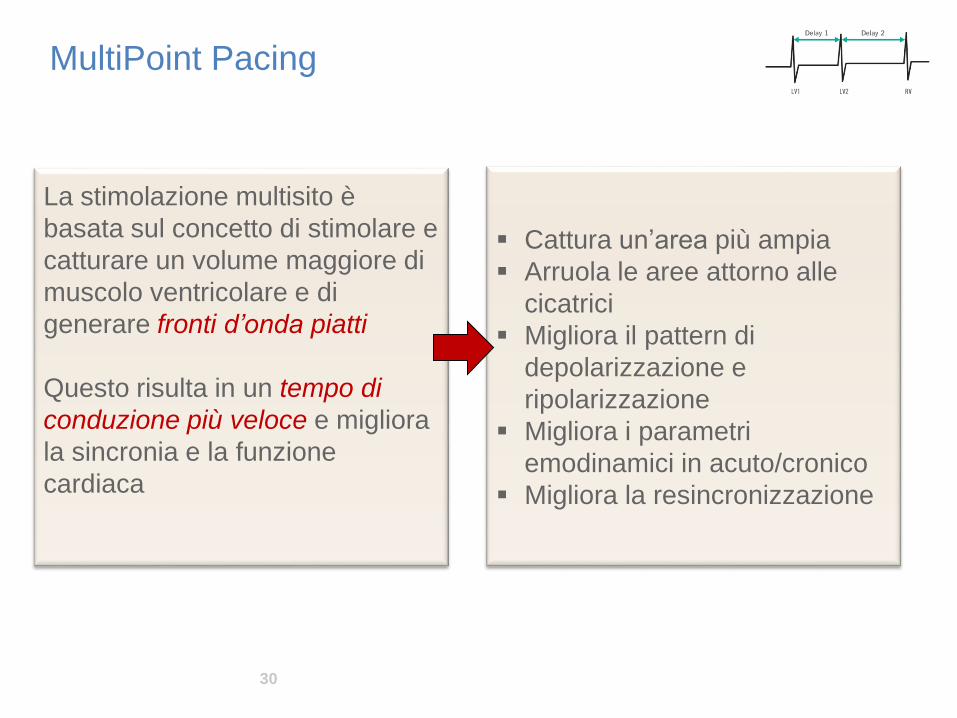
MultiPoint Pacing
La stimolazione multisito è
basata sul concetto di stimolare e
catturare un volume maggiore di
muscolo ventricolare e di
generare fronti d’onda piatti
Questo risulta in un tempo di
conduzione più veloce e migliora
la sincronia e la funzione
cardiaca
▪ Cattura un’area più ampia
▪ Arruola le aree attorno alle
cicatrici
▪ Migliora il pattern di
depolarizzazione e
ripolarizzazione
▪ Migliora i parametri
emodinamici in acuto/cronico
▪ Migliora la resincronizzazione

LBBB patients with longer RV-LV activation delay at CRT implantation had greater improvement in NT-proBNP, EF, and significantly better clinical outcome1
Reduction of risk of HF
hospitalization or death
for RV-LV delay ≥ 86 ms56%
Kosztin M. et al. Europace Journal, June 2015 (n=125)1
Reduction of risk of HF
hospitalization or death
for RV-LV delay ≥ 86 ms
and LBBB77%
1. Kosztin M. et al. Longer right to left ventricular activation delay at cardiac resynchronization therapy implantation is associated with improved clinical outcome in left
bundle branch block patients . Europace Journal, June 2015. Prospective, observational, cohort study. Patients with EF ≤ 35%, QRS ≥ 120ms and successful CRT
implantation. 2.2 years median time follow-up.
Longer RVS-LVS interval at pacing site: independent predictor of CRT response?
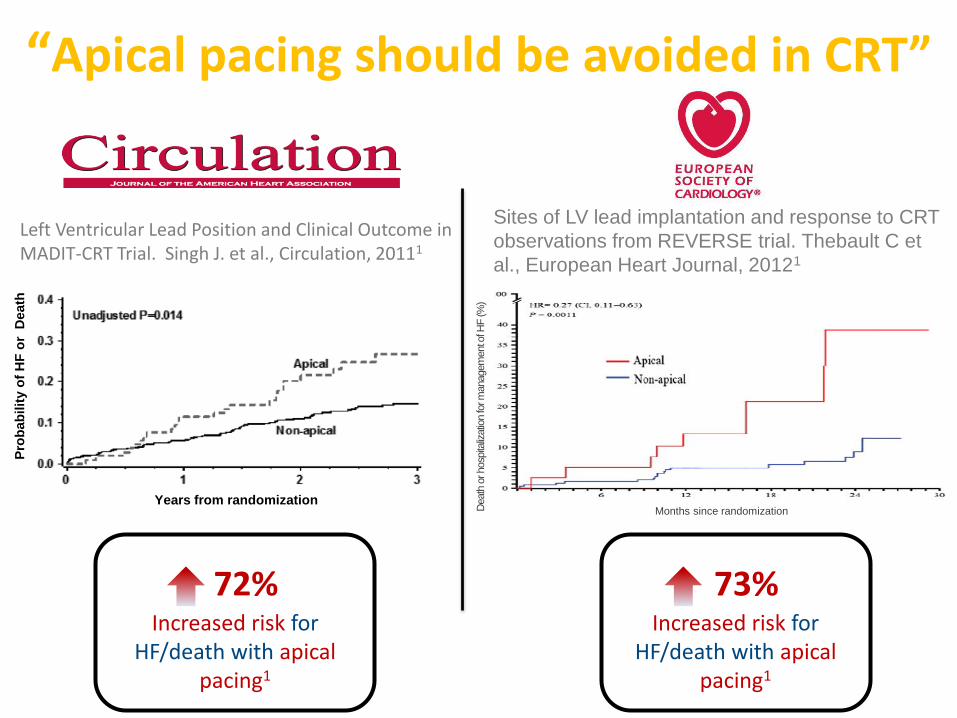
“Apical pacing should be avoided in CRT”
72%Increased risk for
HF/death with apical pacing1
Years from randomization
Pro
bab
ilit
y o
f H
F o
r D
eath
Left Ventricular Lead Position and Clinical Outcome in MADIT-CRT Trial. Singh J. et al., Circulation, 20111
Death
or hosp
italiz
atio
n fo
r m
anagem
ent o
f HF (%
)
Months since randomization
Sites of LV lead implantation and response to CRT
observations from REVERSE trial. Thebault C et
al., European Heart Journal, 20121
73% Increased risk for
HF/death with apical pacing1
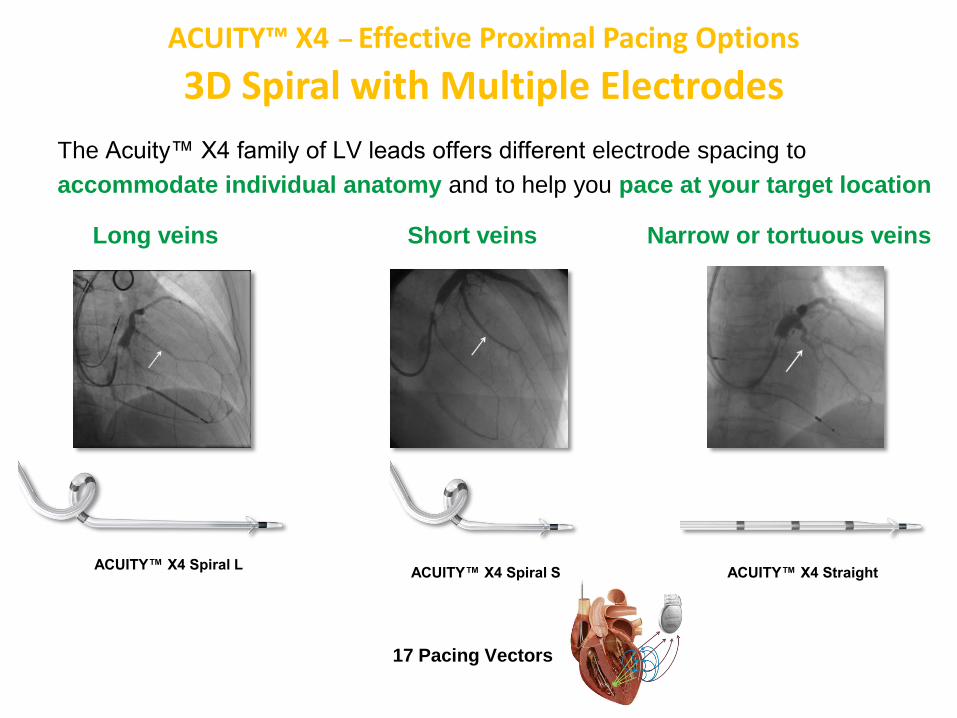
Long veins Short veins Narrow or tortuous veins
ACUITY™ X4 Spiral LACUITY™ X4 Spiral S ACUITY™ X4 Straight
The Acuity™ X4 family of LV leads offers different electrode spacing to
accommodate individual anatomy and to help you pace at your target location
ACUITY™ X4 – Effective Proximal Pacing Options
3D Spiral with Multiple Electrodes
17 Pacing Vectors
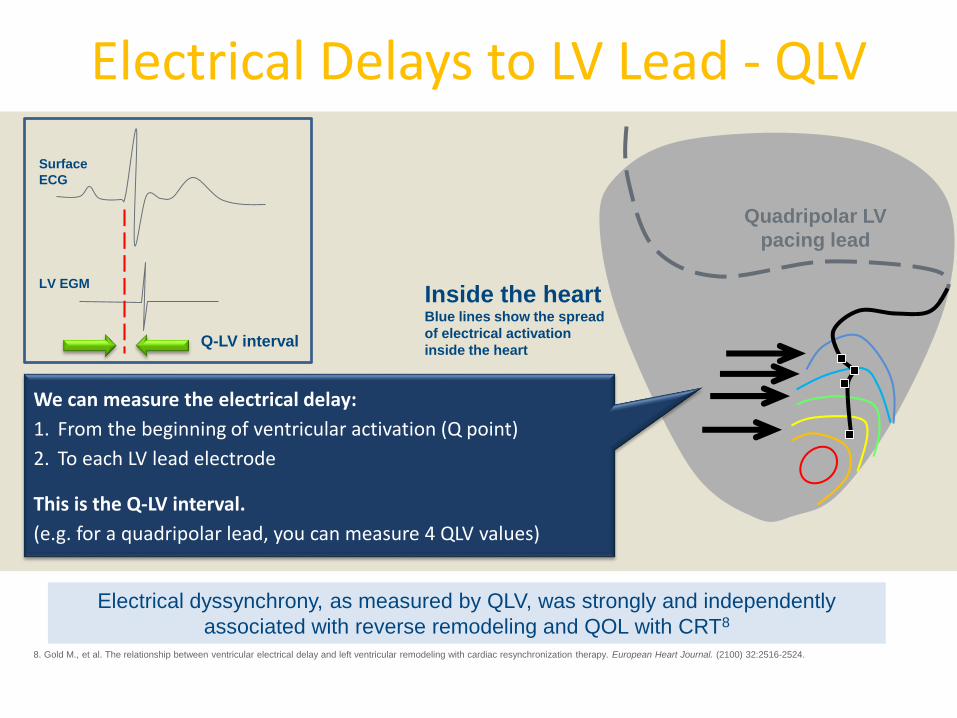
Electrical Delays to LV Lead - QLV
Inside the heartBlue lines show the spread
of electrical activation
inside the heart
Quadripolar LV
pacing lead
We can measure the electrical delay:
1. From the beginning of ventricular activation (Q point)
2. To each LV lead electrode
This is the Q-LV interval.
(e.g. for a quadripolar lead, you can measure 4 QLV values)
Q-LV interval
Surface
ECG
LV EGM
8. Gold M., et al. The relationship between ventricular electrical delay and left ventricular remodeling with cardiac resynchronization therapy. European Heart Journal. (2100) 32:2516-2524.
Electrical dyssynchrony, as measured by QLV, was strongly and independently
associated with reverse remodeling and QOL with CRT8

Example of RVS-LVS delay test results from a Rally X4 Study patient. Data on file
Boston Scientific Reference Guide for X4 CRT-D and CRT-D 359209-001 EN Europe 2013-04. AUTOGEN X4 reference guide supplement (part# 359386-001)
One additional click
for a potential lifetime benefit
VectorGuide™ is designed to quickly identify the
best of 17 vectors options based on clinically
relevant tests including RVS-LVS delay
Maximizing CRT response:VectorGuide Identify the longest RVS-LVS interval

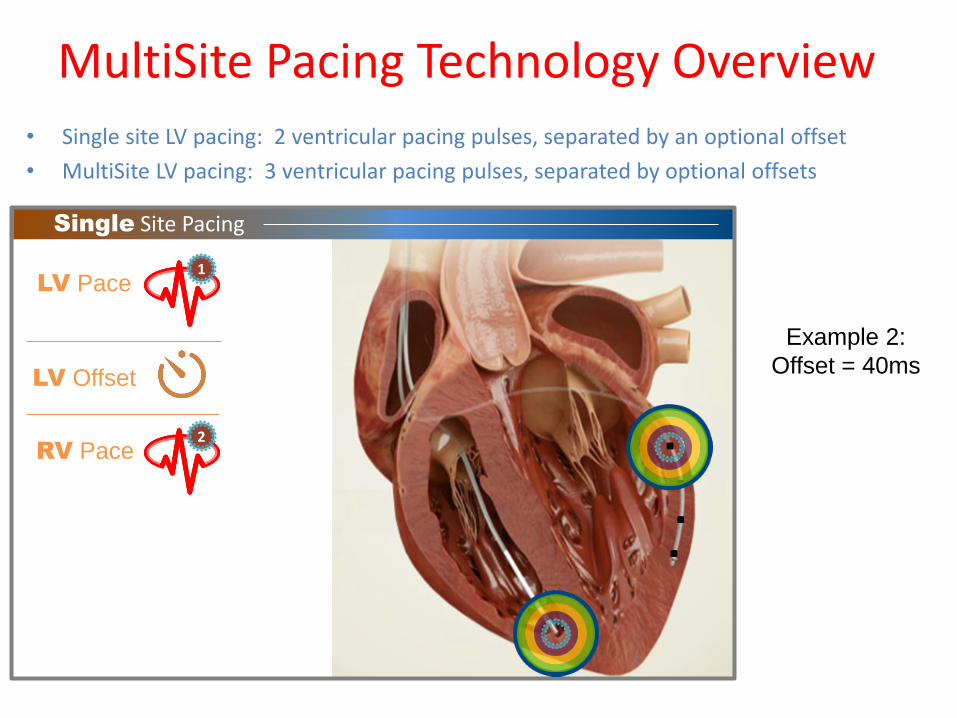
Single Site Pacing
• Single site LV pacing: 2 ventricular pacing pulses, separated by an optional offset
• MultiSite LV Pacing: 3 ventricular pacing pulses, separated by optional offsets
MultiSite Pacing Technology Overview
LV Pace1
RV Pace
LV Offset
2
Example 1:
Offset = 0ms
Single Site Pacing
• Single site LV pacing: 2 ventricular pacing pulses, separated by an optional offset
• MultiSite LV pacing: 3 ventricular pacing pulses, separated by optional offsets
LV Pace1
RV Pace
LV Offset
2
Example 2:
Offset = 40ms
MultiSite Pacing Technology Overview

MultiSite Pacing
1st
LV Pace (LVa)1
2nd
LV Pace (LVb)
RV Pace3
LVaLVb Offset
LVbRV Offset
2
• Single site LV pacing: 2 ventricular pacing pulses, separated by an optional offset
• MultiSite LV pacing: 3 ventricular pacing pulses, separated by optional offsets
Example 1:
No Offset“simultaneous pacing”
MultiSite Pacing Technology Overview
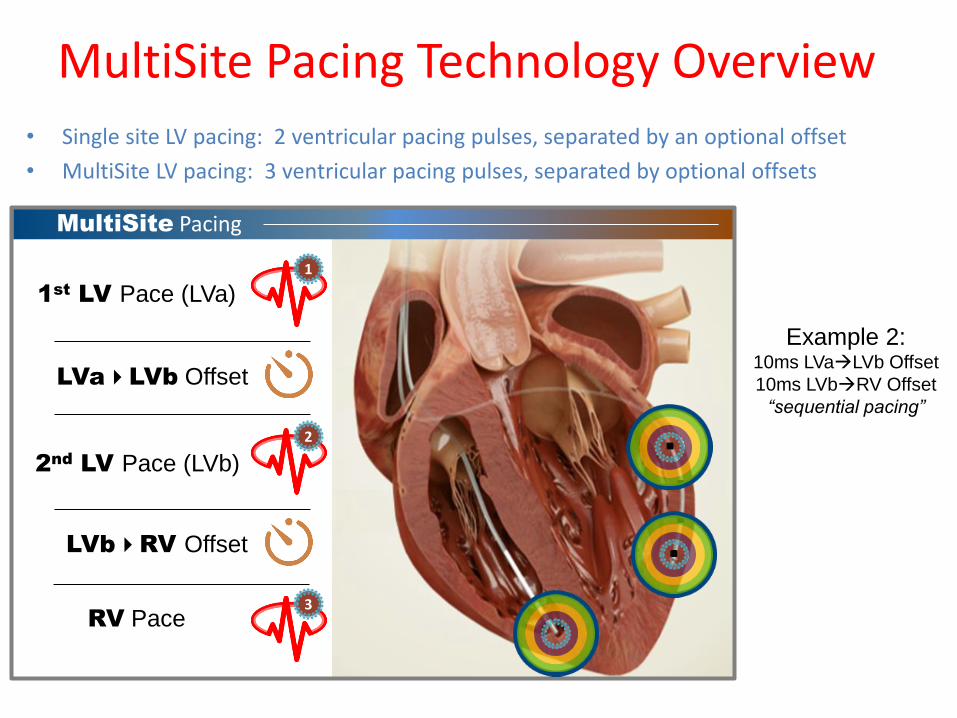
MultiSite Pacing
1st
LV Pace (LVa)1
2nd
LV Pace (LVb)
RV Pace3
LVaLVb Offset
LVbRV Offset
2
• Single site LV pacing: 2 ventricular pacing pulses, separated by an optional offset
• MultiSite LV pacing: 3 ventricular pacing pulses, separated by optional offsets
Example 2:10ms LVaLVb Offset
10ms LVbRV Offset
“sequential pacing”
MultiSite Pacing Technology Overview

4040
Tutte le case oggi propongono una soluzione MP
MPP sincro & sequenziale
216 combinazioni
MPP su un canale
5 combinazioni
MPP sincro & sequenziale
106 combinazioni
MPP sequenziale
60 combinazioni
MPP sincrono (doppio canale)
48 combinazioni
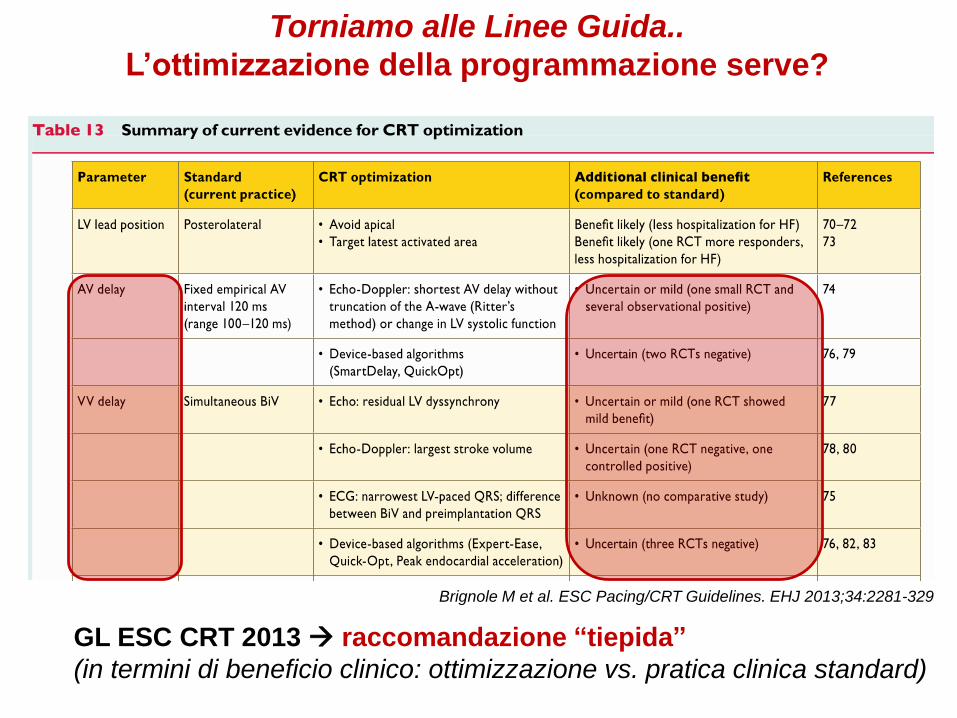
Torniamo alle Linee Guida..
L’ottimizzazione della programmazione serve?
Brignole M et al. ESC Pacing/CRT Guidelines. EHJ 2013;34:2281-329
GL ESC CRT 2013 raccomandazione “tiepida”
(in termini di beneficio clinico: ottimizzazione vs. pratica clinica standard)

Tecnologie “DEVICE-based” per ottimizzare AVD &/or VVD
Lunati M & al.
JAFIB 2014 Aug/Sep Vol.
7(2)
QuickOpt (SJM)IEGM-based
SmartDelay (BSx)
IEGM-based
STATIC optimization(during FU visit only)
SonR (LivaNova-Sorin)Hemodynamic method
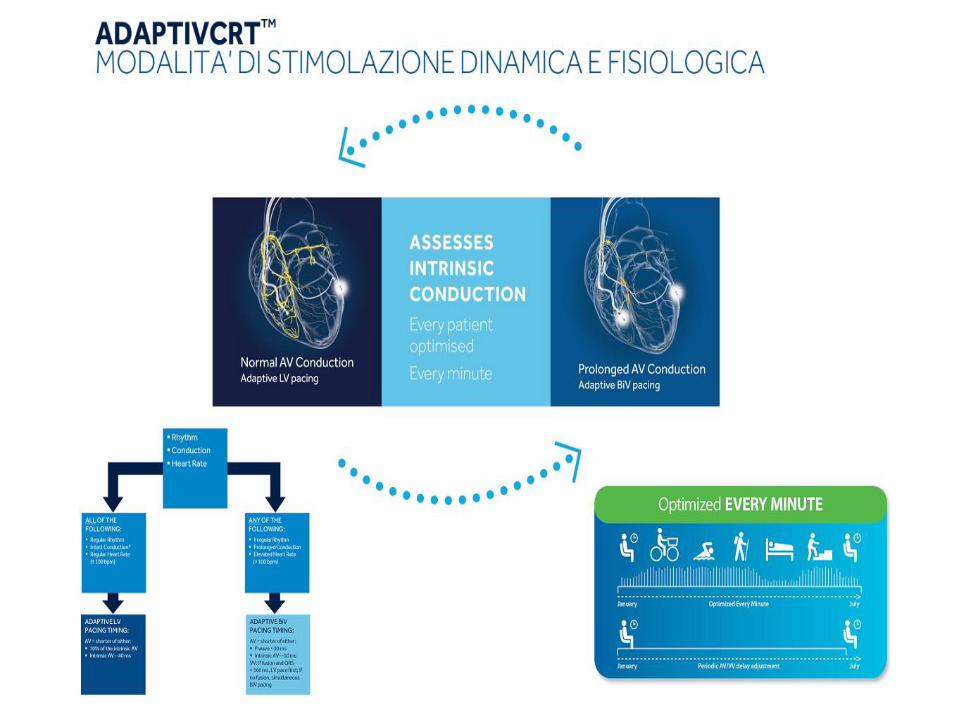
Adaptive-CRT (Mdt)IEGM-based
AUTOMATIC optimiz.
(continuous over time)
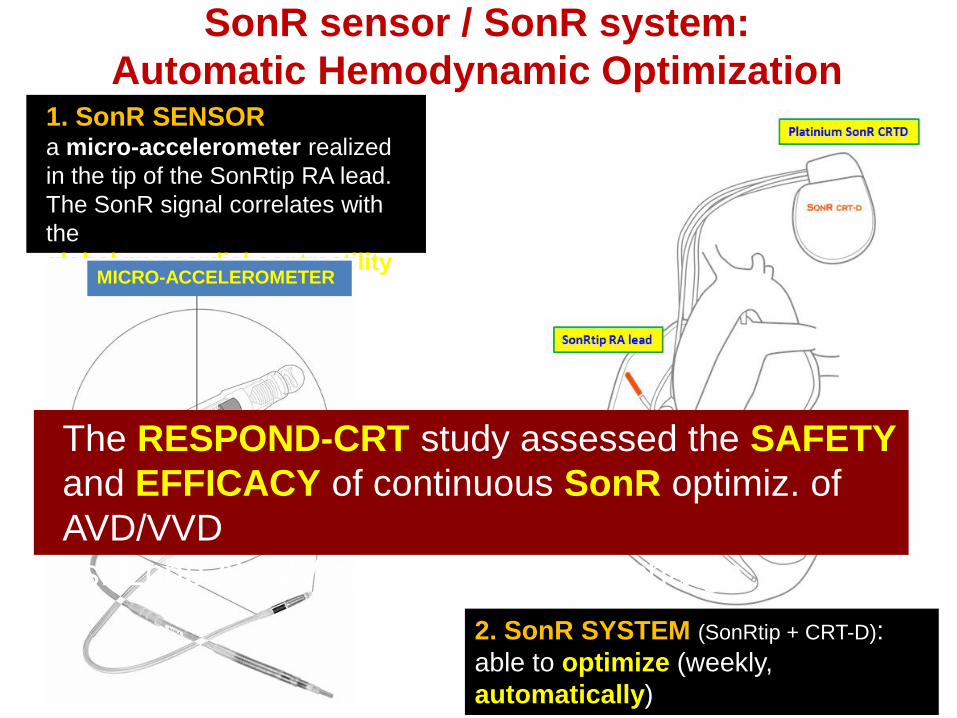
SonR sensor / SonR system:
Automatic Hemodynamic Optimization1. SonR SENSORa micro-accelerometer realized
in the tip of the SonRtip RA lead.
The SonR signal correlates with
the
global myocardial contractilityMICRO-ACCELEROMETER
2. SonR SYSTEM (SonRtip + CRT-D):
able to optimize (weekly,
automatically)
AVD & VVD, at rest & under effort
The RESPOND-CRT study assessed the SAFETY
and EFFICACY of continuous SonR optimiz. of
AVD/VVD
vs. Echo AV/VV optimization at discharge
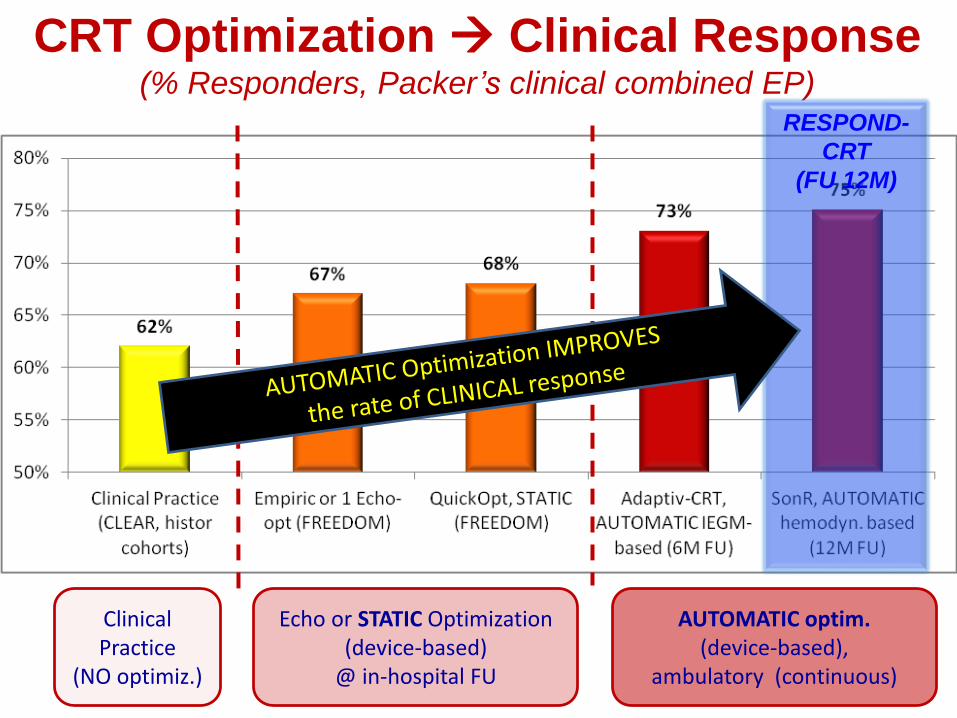
CRT Optimization Clinical Response(% Responders, Packer’s clinical combined EP)
ClinicalPractice
(NO optimiz.)
Echo or STATIC Optimization(device-based)
@ in-hospital FU
AUTOMATIC optim.(device-based),
ambulatory (continuous)
RESPOND-
CRT
(FU 12M)
Proprietary and confidential — do not distribute
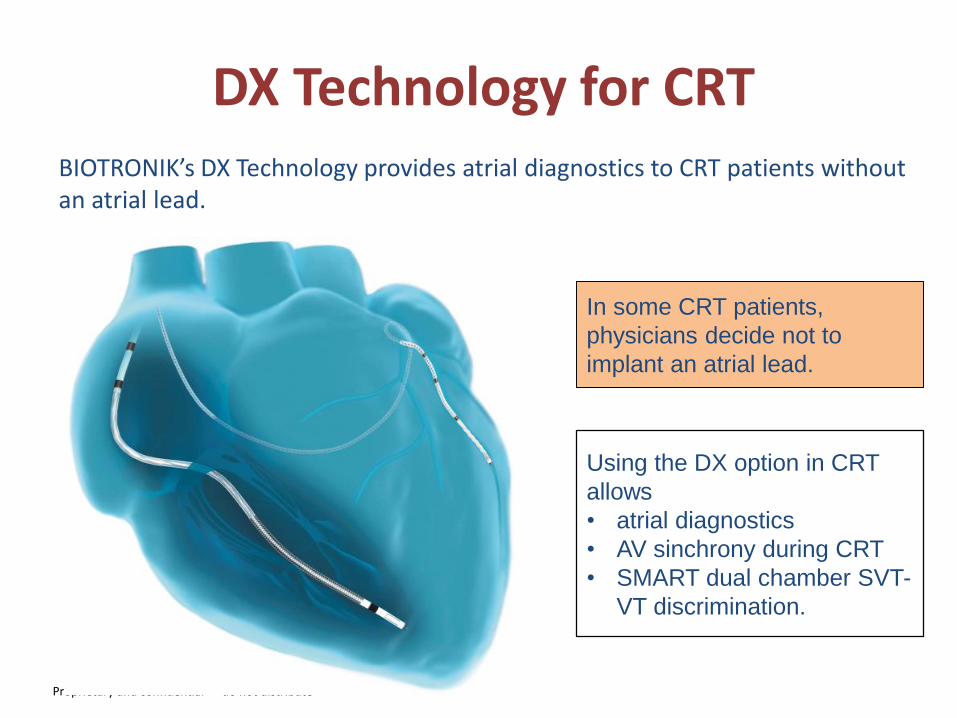
DX Technology for CRTBIOTRONIK’s DX Technology provides atrial diagnostics to CRT patients without an atrial lead.
In some CRT patients,
physicians decide not to
implant an atrial lead.
Using the DX option in CRT
allows
• atrial diagnostics
• AV sinchrony during CRT
• SMART dual chamber SVT-
VT discrimination.

Advantages of two leads CRT: complications risk reduction
The risk of atrial lead complications resulting
in reinterventions was 1.3% (ICD/CRT-D),
and the risk of left ventricular lead
complications was 1.8% (CRT-D).
50 dual chamber ICD: 5 atrial lead
dislodgments, and 1 atrial lead had
to be revised because of
undersensing, event rate 12%.
DX Technology for CRT: why

Proprietary and confidential — do not distribute
Heart failure diagnostic tools and reports help you take a multifactorial approach to
treating patients—by leveraging all of these sensors at once, our reports deliver
more accurate results that help you make more informed decisions.
Daily Heart Rate
Heart Rate Variability (SDANN)
AT/AF Burden
RV Rating during AT/AF
% LV Paced
V-Therapy
Thoracic Impedance
Activity Level
Night Heart Rate
Respiratory Rate
Weight
Blood Pressure
Sleep Incline
Heart Failure Sensor Suite
Proprietary and confidential — do not distribute
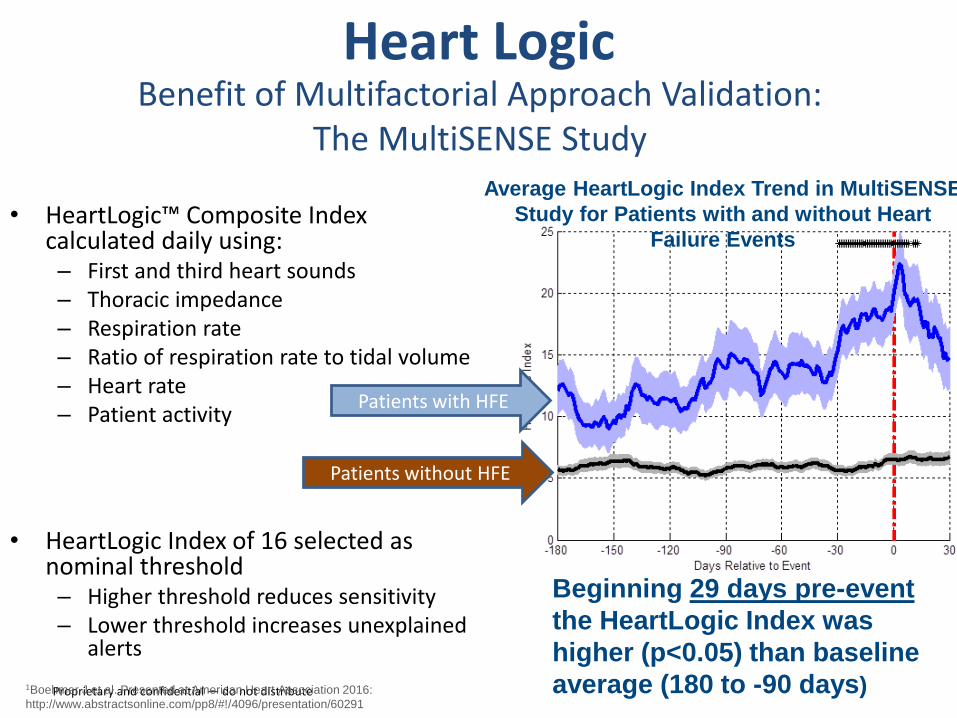
• HeartLogic™ Composite Index calculated daily using:– First and third heart sounds– Thoracic impedance– Respiration rate– Ratio of respiration rate to tidal volume– Heart rate– Patient activity
• HeartLogic Index of 16 selected as nominal threshold– Higher threshold reduces sensitivity– Lower threshold increases unexplained
alerts
Average HeartLogic Index Trend in MultiSENSE
Study for Patients with and without Heart
Failure Events
Patients with HFE
Patients without HFE
Beginning 29 days pre-event
the HeartLogic Index was
higher (p<0.05) than baseline
average (180 to -90 days)1Boehmer J et al. Presented at American Heart Association 2016:
http://www.abstractsonline.com/pp8/#!/4096/presentation/60291
Heart LogicBenefit of Multifactorial Approach Validation:
The MultiSENSE Study
51
Conclusioni
▪ Nonostante la CRT sia riconosciuta come terapia efficace ed abbia un ruolo
ben preciso nelle LG HF più recenti, ancora oggi si osservano tassi elevati di
NR.
▪La tecnologie di ultima generazione possono contribuire in modo
significativo alla riduzione del tasso di NR, in particolare attraverso:
-Nuovi parametri per la selezione / stratificazione dei pazienti candidati
alla CRT
-Ottimizzazione della configurazione di pacing
-Monitoraggio dello stato emodinamico del paziente
-Ottimizzazione sistematica ed emodinamica dei parametri di
stimolazione
▪Il ruolo della stimolazione Multi Point come strumento di riduzione del tasso
di NR deve ancora essere chiarito. I moderni dispositivi ad elevata longevità,
permetteranno un utilizzo più estensivo di questa modalità di pacing.
.