Vol. 14 - n. 1 - Gennaio-Aprile 2016€¦ · 5 D ep ar tm n ofSug y,R d i lP b cHh sU v B I -...
36
Transcript of Vol. 14 - n. 1 - Gennaio-Aprile 2016€¦ · 5 D ep ar tm n ofSug y,R d i lP b cHh sU v B I -...


1
Questo numero della Rivista Italiana di Medicina dell'Adolescenza è dedicato ad alcune problematiche auxo-endo-crinologiche dell'età adolescenziale. In particolare, la terapia con ormone dell'accrescimento, l'insorgenza della pubertàprecoce dopo trauma cranico, il coma mixedematoso e la valutazione della presumibile età cronologica di un minore,senza documenti, in conflitto con la legge.
Per “accertamento dell’età” si intende la procedura utilizzata per determinare l’età approssimativa di un individuo.Pur non riscontrandosi né nel contesto nazionale né in ambito comunitario un approccio uniforme nelle modalità operative,il termine “accertamento dell’età” tende ad essere più comunemente utilizzato per indicare l’uso di esami di tipo medico,volti a stimare l’età cronologica di un individuo attraverso una valutazione della sua età biologica (UNHCR, Field Handbookfor the Implementation of UNHCR BID Guidelines, 2011,http:// www. refworld.org /docid /4e4a57d02.html, ultima cons. 30 ottobre 2013). L’accertamento dell’età dei minori, senza documenti in conflitto con la legge, è generalmente dispostodall’autorità giudiziaria o di pubblica sicurezza. Le metodiche usate oggi in Italia per determinare l’età biologica di un indivi-duo si basano quasi sempre sulla valutazione dello stadio puberale e della maturazione scheletrica, effettuata con la radio-grafia mano-polso, refertata con il metodo di Greulich e Pyle (GP) o Tanner e Whitehouse (TW-2 o TW-3).
La questione dell’accertamento dell’età anagrafica tramite studio auxologico effettuato con esame radiograficoè, come noto, una questione delicata e controversa. Uno studio condotto in Danimarca, su 159 soggetti provenienti dadiverse aree geografiche, esaminati a più riprese da diversi operatori, ha evidenziato che utilizzando il metodo GP nel95% dei casi esaminati la differenza nella determinazione dell’età era di circa un anno. Altri studi, utilizzando il metodoTW-2 hanno registrato differenze tra età scheletrica ed età ossea comprese in un range tra - 0,1 anni e +1,4 anni (con una tendenza alla sovrastima dell’età scheletrica); mentre con il metodo TW-3 queste differenze sono risultate inun range più contenuto. Ne deriva che gli esiti di un esame radiologico del polso, seppur statisticamente affidabili, sonosuscettibili, nel caso individuale, di un margine di errore di varia ampiezza.
Queste considerazioni sono state riprese anche da Benso e Milani in un documento del 2013 (Alcune consi-derazioni sull'uso forense dell'età biologica. www.asgi.it/wp content/uploads /public/1_2013_ accertamento_eta_mater). Gli Autori ci ricordano che "sino a oggi, non vi sono dati sufficienti che permettano di adattare queste meto-diche alle etnie per le quali più frequentemente sono richieste stime dell’età anagrafica. Ciò non significa che i metodiper la valutazione dell’età scheletrica sono del tutto inutili. Il loro scopo originale non era la determinazione dell’età ana-grafica in soggetti privi di documenti, ma la valutazione della differenza tra età anagrafica e biologica in diverse condi-zioni auxologiche, sia fisiologiche, per stimare il potenziale di crescita residuo, sia d’interesse clinico, per diagnostica-re e monitorare malattie croniche, turbe nutrizionali, carenze ormonali, terapie sostitutive...." .
Il margine di errore è legato anche alla competenza dell’operatore. Uno studio condotto su 47 soggetti ha atte-stato una significativa variabilità intra-operatore (correlata all’esperienza di quest’ultimo), con tendenza alla sottostima del-l’età. In sostanza, gli operatori più esperti hanno stimato l’età con una variabilità compresa tra -1,5 mesi e ± 7,6 mesi,mentre gli operatori meno esperti hanno manifestato una maggiore variabilità compresa tra 2,7 mesi e ± 10,3 mesi.
In conclusione, non esistono metodi scientifici capaci di determinare con esattezza l’età cronologica di una per-sona, soprattutto in età critica quale quella degli adolescenti. Un esame medico non può fornire che una stima dell’etàcronologica di un individuo ed è, per sua natura, soggetto ad un margine di errore, quantificabile in un range la cuiampiezza è inevitabilmente determinata da vari fattori. Ne deriva che nessuna valutazione è precisa ed attendibile e diconseguenza un margine d’incertezza rimane sempre. È auspicabile che ulteriori ricerche e la combinazione di più meto-di, non invasivi, possano migliorare questa valutazione. In tutti i casi, gli aspetti etici dovranno essere tenuti in dovutaconsiderazione nella preparazione delle linee guida per l'uso forense dell'accertamento dell'età biologica di un individuo.
Vincenzo De Sanctis
Editoriale
00_Cop edit som 04/05/16 17:00 Pagina 1

333
Abbonamento annuale (3 numeri) Euro 30,00.Pagamento: conto corrente postale n. 1010097192 intestato a:Edizioni Scripta Manent s.n.c., via Bassini 41, 20133 MilanoÈ vietata la riproduzione totale o parziale, con qualsiasi mezzo, di articoli, illustrazioni e fotografiesenza l’autorizzazione scritta dell’Editore.L’Editore non risponde dell’opinione espressa dagli Autori degli articoli e delle immagini da loro utilizzate.Ai sensi della legge 675/96 è possibile in qualsiasi momento opporsi all’invio della rivista comunicandoper iscritto la propria decisione a: Edizioni Scripta Manent s.n.c. Via Bassini, 41 - 20133 Milano
DIRETTORE SCIENTIFICOVincenzo De Sanctis (Ferrara)
COMITATO DI REDAZIONESilvano Bertelloni (Pisa)
Giampaolo De Luca (Amantea, Cosenza)Bernadette Fiscina (New York, USA)
Giuseppe Raiola (Catanzaro)Tito Livio Schwarzenberg (Roma)
COMITATO EDITORIALEAntonietta Cervo (Pagani, Salerno)
Salvatore Chiavetta (Palermo)Michele De Simone (L’Aquila)
Teresa De Toni (Genova)Piernicola Garofalo (Palermo)
Maria Rita Govoni (Ferrara)Domenico Lombardi (Lucca)
Carlo Pintor (Cagliari)Luigi Ranieri (Catanzaro)
Leopoldo Ruggiero (Lecce)Giuseppe Saggese (Pisa)
INTERNATIONALEDITORIAL BOARDMagdy Omar Abdou (Alexandria, Egypt)Mujgan Alikasifoglu (Istanbul, Turkey)
Mike Angastiniotis (Nicosia, Cyprus)German Castellano Barca (Torrelavega, Spain)
Elsaid Bedair (Doha, Qatar)Monica Borile (El Bolson, Argentina)
Roberto Curi Hallal (Rio de Janeiro, Brasil)Yardena Danziger (Petah-Tiqva, Israel)
Oya Ercan (Istanbul, Turkey)Helena Fonseca (Lisbon, Portugal)
Daniel Hardoff (Haifa, Israel)Christos Kattamis (Athens, Greece)
Nogah Kerem (Haifa, Israel)Karaman Pagava (Tbilisi, Georgia)Praveen C. Sobti (Ludhiana - Punjab, India)
Ashraf Soliman (Doha, Qatar)Joan-Carles Suris (Lausanne, Switzerland)
SEGRETARIA DI REDAZIONELuana Tisci (Ferrara)
STAFF EDITORIALEDirettore Responsabile Pietro Cazzola
Direttore Scientifico Donatella TedeschiDirezione Marketing Antonio Di Maio
Direttore Amministrativo Cristina BrambillaGrafica e impaginazione Cinzia Levati
Consulenza Grafica Piero MerliniSocio Fondatore Armando Mazzù†
Scripta Manent s.n.c. Via Bassini, 41 - 20133 MilanoTel. 0270608091 - 0270608060 / Fax 0270606917E-mail: [email protected]
Registrazione Tribunale di Milano n. 404 del 23/06/2003
Stampa: Lalitotipo s.r.l.Settimo Milanese (MI)
Vol. 14 - n. 1 - Gennaio-Aprile 2016
Sommario
Editoriale pag. 1Vincenzo De Sanctis
An essential approach to the age assessment in undocumented minors in conflict with the law pag. 5Vincenzo De Sanctis, Ashraf T. Soliman, Nada A Soliman, Rania Elalaily, Paola Delbon, Salvatore Di Maio, Giuseppe Millimaggi
Aderenza e compliance al trattamento con ormone della crescita pag. 12Fabio Buzi
Linear Growth and Nutritional Parameters in Adolescents with Severe Atopic Dermatitis pag. 19Mohammad Ehlayel, Ashraf Soliman, Vincenzo De Sanctis
FRONT LINELa terapia ‘appropriata’…un personal trainer o un tapis roulant? pag. 23Solveig Cogliani
CASE REPORTMyxoedema coma: A report in an adolescent with aplastic anemia and iron overload pag. 25Vincenzo De Sanctis, Ashraf T. Soliman, Heba Elsedfy,Nada A. Soliman, Rania Elalaily, Ihab Zaki Elhakim
CASE REPORTPrecocious puberty in a girl following severe traumatic brain injury (TBI) in early childhood: A simple coincidence or a possible consequence? pag. 29Vincenzo De Sanctis, Ashraf T. Soliman, Heba Elsedfy, Nada A. Soliman, Rania Elalaily, Ashraf Adel
Potential diagnostic and therapeutic use of Continuous Glucose Monitoring System (CGMS) in Thalassemia Major: A short presentation of personal experience pag. 32Ashraf Soliman, Mohamed Yassin, Fawzia Alyafie, Rania Elalaily, Nada A. Soliman, Heba Elsedfy, Vincenzo De Sanctis
ORGANO UFFICIALE
00_Cop edit som 04/05/16 17:00 Pagina 3

An essential approach to the age assessment in undocumented minors
in conflict with the law
SummaryIn forensic contexts, assigning an age to a living child of unknown identity may be necessary when the child is
suspect in a crime, when penal codes differentiate law and punishment for children of different ages or if the child is a refugee.The age of criminal responsibility in the UK is the lowest in Europe with other European Union Member States setting the ageof criminal responsibility between 14 and 16 years. In the absence of a known birth date, any assessment of age will be difficult.The age assessment should include a comprehensive physical description of the person including: physical development, bonematurity which is observed on radiographs as the development and fusion of the long bone growth centres (e.g. in the handand wrists) and dental age estimation (including grading tooth development both clinically and on dental radiographs)Currently there is no medical test or a group of tests that will absolutely and accurately let us know the exact chronological ageof a human being. There will always be an uncertainty related to the estimate, and correctly expressing this uncertainty is justas important as the actual estimate.More research is needed to define more precisely the best standard approach for age estimation based on a combination of dif-ferent methods. Furthermore, professionals working with children should always strive to take ethical guidelines into considera-tion in making decisions of such minors.
Key words: Undocumented minors, age assessment, current laws, European Countries.
Un approccio alla valutazione dell’età di un minore, senza documenti, in conflitto con la legge
RiassuntoLa valutazione della presumibile età cronologica (PEC) di un minore, senza documenti, in conflitto con la legge è
un tema di rilevante attualità. L’età dell’imputabilità nel Regno Unito è la più bassa in Europa, mentre negli altri Paesi varia dai 14ai 16 anni. Usualmente per la valutazione della PEC vengono presi in considerazione i seguenti parametri: esame fisico, valutazionedella maturità ossea e dei denti. Nessuna valutazione è precisa ed attendibile e di conseguenza un margine d’incertezza rimanesempre. È auspicabile che ulteriori ricerche e la combinazione di più metodi possano migliorare questa valutazione nei minori. In tutti i casi, gli aspetti etici dovranno essere tenuti in considerazione nella preparazione delle linee guida.
Parole chiave: Minori senza documenti, valutazione dell’età, legge, Comunità Europea.
Vincenzo De Sanctis 1, Ashraf T Soliman 2, Nada A Soliman 3, Rania Elalaily 4, Paola Delbon 5,Salvatore Di Maio 6, Giuseppe Millimaggi 7
1 Pediatric and Adolescent Outpatient Clinic, Quisisana Hospital, Ferrara, Italy; 2 Department of Pediatrics, Division of Endocrinology, Alexandria University Children's Hospital, Alexandria, Egypt;
3 Ministry of Health , Alexandria, Egypt; 4 Department of Primary Health Care, Abu Nakhla Hospital, Doha, Qatar;
5 Department of Surgery, Radiology and Public Health, Public Health and Humanities Section, University of Brescia, Italy - Centre of Bioethics Research (with the contribution of Fondazione Poliambulanza); 6 Emeritus Director in Pediatrics, “Santobono - Pausilipon” Hospital, Neaples, Italy;
7 Radiology Clinic, Quisisana Hospital, Ferrara, Italy.
5
Introduction
The definition of “children in conflict with the law” varies dependingon the domestic law. The definition which has been mainly adop-ted refers to anyone with a minimum age who comes into contactwith the justice system as a result of having committed or beingsuspected or accused of committing an offence. A culpabilityaction is an act which has been committed by an individual which
is considered by society as wrong, damaging to other individualsor society as a whole or is otherwise unacceptable. Adults are pre-sumed culpable for their criminal acts while young children aregenerally not found legally responsible for their wrongful acts.Adolescents fall on a continuum between these two poles (1-3).It is important to remember that culpability is only one factor rele-
De Sanctis_StesuraMAGAM 2 05/05/16 09:23 Pagina 5

6
vant to punishment. Punishment is generally taken to have seve-ral purposes, including retribution, deterrence, protection ofsociety through incapacitation and rehabilitation (1).
Background
The rapid rise in adolescent crime in the late 1980s and early1990s led to increased fears for public safety, and since 1992,many states have adopted additional procedures for transferringadolescents to adult criminal court (4).In the USA in the late 1980s to early 1990s witnessed a rapidincrease in juvenile homicide rates. From 1984 to 1993, firearm homicides among juveniles increa-sed over 200 percent, a much greater increase than that seen inother age groups (5). This wave of juvenile violence received great public attention,generated considerable fear among the public, and led many
Rivista Italiana di Medicina dell’Adolescenza
Volume 14, n. 1, 2016
An essential approach to the age assessment in undocumented minors in conflict with the law
Country Minumum age of criminal responsabilityAustria 14Belgium 18 (16 for serious offences)Bulgaria 14Czech Republic 15Denmark 15England and Wales 10Estonia 14Finland 15France 13 (but educational measures can be
imposed from the age of 10)Germany 14Greece 13 (but educational measures can be
imposed from the age of 8)Hungary 14Iceland 15Italy 14Latvia 14Lithuania 14Luxembourg 18Netherlands 12Northern Ireland 12Norway 15Poland 13Portugal 16Romania 14Russian Federation 14Scotland 8Slovakia 14/15Spain 16 (14 in Catalonia)Sweden 15Turkey 12
Mexico *6-12Bangladesh 7India 7Myanmar 7Nigeria 7Pakistan 7South Africa 7Sudan 7Tanzania 7Thailand 7United States **7Indonesia 8Kenya 8Ethiopia 9Iran ***9Philippines 9Nepal 10
Ukraine 10Turkey 11Korea, Rep. 12Morocco 12Uganda 12Algeria 13Uzbekistan 13China 14Japan 14Russian Federation 14Viet Nam 14Egypt 15Argentina 16Brazil ****18Colombia ****18Peru ****18
Table 1.Age of law responsibility in European countries.
Table 2.Age of criminal responsibility in non European countries(Minimum age at which children are subject to penal law incountries with 10 million or more children under 18 years old;Sources: CRC Country Reports (1992-1996); Juvenile Justice andJuvenile Delinquency in Central and Eastern Europe, 1995;United Nations, Implementation of UN Mandates on JuvenileJustice in ESCAP, 1994; Geert Cappelaere, Children's RightsCentre, University of Gent, Belgium).
Legend: *Most states 11 or 12 years; age 11 for federal crimes; ** Age determined by state, minimum age is 7 in most states under common law;*** Age 9 for girls, 15 for boys; **** Official age of criminal responsibility, from age12 children's actions are subject to juvenile legal proceedings.
state legislatures to take in consideration criminal responsibility,and, by implication, the imposition of adult punishment (1). In forensic contexts, assigning an age to a living child of unk-nown identity may be necessary when the child is suspected ofa crime, when penal codes differentiate law and punishment forchildren of different ages or if the child is a refugee (6).
Age of law responsibility in different counties
The age of criminal responsibility in the UK is the lowest inEurope with other European Union Member States setting theage of criminal responsibility between 14 and 16 (Table 1) . This age limit for law responsibility is even lower in some nonEuropean countries (Table 2). It has been reported in the UK through a study undertaken in2007 that nearly 3,000 crimes committed in a single year werecommitted by children under the age of 10 years. The figures show that 1,300 crimes and more than 60 sex offen-ces were committed by suspects under 10 (7).
De Sanctis_StesuraMAGAM 2 05/05/16 09:23 Pagina 6

plete personality development, mental illness, and reactive attitu-des toward the offense (1).In the present paper, the Authors set out state-of-the art for ageestimation methods for specific case groups and define the mini-mum requirements for reference. In addition, issues relating toquality of assessment are discussed.
The age assessment
In the absence of a known birth date, any assessment of age willbe difficult .The age assessment should include a comprehensi-ve physical description of the person including: physical deve-lopment, bone maturity which is observed on radiographs as thedevelopment and fusion of the long bone growth centres (e.g. inthe hand and wrists) and dental age estimation (including gra-ding tooth development both clinically and on dental radio-graphs) (10).
a. Physical description The most appropriate approach is to use a holistic evaluation,incorporating narrative accounts, physical assessment ofpuberty and growth, and cognitive, behavioural and emotionalassessments. This process consists in assessing height and wei-ght, body mass index, as any visible signs of sexual maturity.There are clearly defined methods for rating puberty as descri-bed by Marshall and Tanner (13, 14). These give the ages ofvarious stages of attainment of pubertal appearances, startingon average at 11 years in both males and females and goingthrough to the final stages acquired two or three years later.Axillary hair growth, acne, facial hair growth and laryngeal promi-nence development should also be registered.Any visible marks and comment on what weight will be attachedto report, for example a general physical examination should beperformed to describe any signs of a pathological condition whichmay interfere with the maturation rate because in circumstancesof illness, undernutrition, extreme stress and disrupted socialisa-tion, tools used to assess age are likely to be less reliable.
Advantages and disadvantages The main advantage of this method is that it is relatively simple anddoes not require any radiation exposure. However, anthropometricmeasurements do not take into consideration variations betweenethnicity, race, nutritional intake and socioeconomic background.The evaluation of sexual maturity has the greatest margin of errorand should be used for age determination only in conjunction withskeletal maturity and tooth development. There are individuals who enter puberty at the age of nine andsometimes before that, while others only do so at the age of 15 or16 without implication of a disease. Thus, at the age of 14, it is possible to find a boy who is still pre-pubertal , another who is in the middle of puberty and another one
Essential sources of law responsibility for minors in Italy
Italian criminal law is codified in the Codice Penale (CriminalCode), in special legislation, and, with regard to procedural rules,in the Codice di Procedura Penale (Code of Criminal Procedure).The Italian Criminal Code is divided into a general part, whichcontains the provisions that can be applied to all offences, and aspecific part, which provides for single criminal offences.Criminal offences are divided into two main categories: crimesand misdemeanours. Another fundamental principle of Italian lawis that neither a citizen nor a foreigner can plead ignorance of thelaw as an excuse for not complying with the law . In Italy, the mini-mum age of criminal responsibility is set at 14 years (Article 97 ofthe Criminal Code). Any minor who has not attained that age can-not be indicted for any type of illegal activity whatsoever; since itis presumed that the minor is incapable of understanding andintent. In certain circumstances, persons aged below 14 can berecognized as being socially dangerous and can therefore besubjected to security measures.It must also be noted that persons aged between 14 and 18years are not presumed to have the capacity of understandingand intent. In order to establish whether a minor aged between14 and 18 years should be subjected to a penalty, the adjudica-ting body must, for each case and on the basis of the concreteevidence put before the court, ascertain whether the perpetratorof the crime had reached an adequate level of maturity and psy-chological development at the moment of the offence to under-stand the seriousness of the act (Article 98 of the Criminal Code).If the offender had attained the age of eighteen when the offencewas committed, and is therefore considered an adult, it is presu-med that he/she is capable of understanding and acting intentio-nally and is therefore criminally liable. This presumption may be rebutted, however, if it is proved that theoffender was unable to understand and act intentionally at themoment of the offence, due to infirmity (Article 88 of the CriminalCode) or other causes. If this is proved, the offender cannot beconsidered liable for the offence and therefore no penalty can beimposed on him/her, with the exception of those security measu-res that may be applied if the offender is recognized to be social-ly dangerous (8, 9).
Aim of present work
A forensic evaluator assessing adolescent culpability faces acomplex task including age assessment in undocumentedminors ,appreciation of wrongfulness, ability to conform to law,developmental course of aggression and impulsivity, psychoso-cial immaturity (including time sense, susceptibility to peer pres-sure, risk-taking, and ability to empathize), environmental cir-cumstances, peer group norms, out-of-character action, incom-
Rivista Italiana di Medicina dell’Adolescenza
Volume 14, n. 1, 2016
7
An essential approach to the age assessment in undocumented minors in conflict with the law
De Sanctis_StesuraMAGAM 2 05/05/16 09:23 Pagina 7

8
who has already reached adulthood. The same may occur withgirls, at even an earlier age (15, 16).
b. X-ray hand bone ageBone age is a way of describing the degree of maturation ofchild's bones. As a person grows from fetal life throughchildhood, puberty, and finishes growth as a young adult, thebones of the skeleton change in size and shape. These changescan be seen by X-ray. The "bone age" of a child is the averageage at which children reach this stage of bone maturation.Skeletal maturity or bone age describes the degree of biologicalmaturation. The technique for assessing skeletal maturity consi-sts of visual inspection of the developing bones. Various areas ofthe skeleton have been used: the foot, the ankle, the hip, theelbow, the hand-wrist, and the cervical vertebrae (Table 3).The hand-wrist radiograph is commonly used for skeletal deve-lopmental assessment. Most investigators have found significantcorrelation among maturation stages derived from hand-wristradiographs, changes in height during pubertal growth periodand facial growth (17-19).The most common method of skeletal maturity assessment usesa radiograph of the left hand and wrist to determine the differentstages in bone maturation. There are two different techniques,namely the Tanner and Whitehouse II and III (TWII–III) andGreulich and Pyle (20-22).
Advantages and disadvantages The Greulich and Pyle method is faster and easier to score and itis often the preferred method for a clinical application. All bone age estimation methods have some errors. In otherwords if the same X-ray is assessed either by the same or diffe-rent assessors the assigned bone age may vary ( intra-observerand inter-observer error) (23, 24). A number of studies have inve-stigated these effects and in summary have demonstrated anaverage intra-observer error of between 2 and 9 months and anaverage inter-observer error between 1 and 12 months. However,these were average errors and the error range in these studieswas 0 to over 2 years. Combining both the intra- and inter-obser-
ver, variation differences of over 12 months frequently occur (25-30). Variation using computer software to define bone ages isless and varies between 0 and 6 months (31, 32).Pubertal variation has a major impact on bone age estimation.Obesity tends to advance bone age maturation while malnutritionand conditions that reduce fat mass such as anorexia nervosadelay it. Any chronic illness during childhood may also delaybone age maturation. Severe neglect can also cause bone agedelay while placing such children in a more caring environmentcan result in earlier puberty and an advanced bone age. Thus many factors need to be considered when trying to establi-sh age based on bone age estimation alone (31-33).
c. The dental maturity for the assessment of chronological ageThe last physiologic measure is dental maturity, which can bedetermined by the stage of tooth eruption or the stage of toothformation. The latter is proposed as a more reliable criterion fordetermining dental maturation. Relationships between the calci-fication stages of individual teeth and skeletal maturity have beenpreviously reported. Racial variations in the relationships havealso been suggested (34, 35). There are several different types ofdental examination that could be used to assess the age of per-sons in different age ranges. The Demirjian and Nolla methodsare one of the most frequently used in estimating chronologicalage due to its simplicity, intra-examiner agreement, ease of stan-dardization and ability to be reproduced, having been used andtested across a wide range of populations (36, 37).
Demirjian methodThe Demirjian method is a system based on eight stages (fromA to H) of dental maturity in the seven left permanent mandibularteeth, observable through orthopantomographs.Each tooth was attributed a stage and converted in quantitativevalues by applying a specific table, the scores of the seven teethare summed as a function of sex and the sum of dental maturity isobtained on a scale of 0 to 100. This total is converted in dentalage using a table for converting the results of dental maturity. A proper Demirjian’s evaluation of dental maturity involves dentalpanoramic X-rays and a complex assessment based on calcifica-tion stages for the seven left permanent mandibular teeth. In childhood (0-14 years) radiological examination of dental deve-lopment includes all tooth types. In adolescence (14-21 years), thethird molars are the only teeth undergoing maturation, this maydecrease accuracy. In both cases, sex and race influence toothdevelopment, so those factors have to be taken into account. Thismethod has been widely used in different populations (38).
Nolla methodThe Nolla method allows classification of dental developmentfrom stage one (1 - no sign of calcification with the presence ofcrept), to stage ten (10 - apical end completed). The orthopanto-
Rivista Italiana di Medicina dell’Adolescenza
Volume 14, n. 1, 2016
An essential approach to the age assessment in undocumented minors in conflict with the law
Estimated age of fusionBone Proximal/ Distal/
medial end lateral endHumerus (upper arm) 10-15 years 9-15 yearsRadius (lower arm) 14-19 years 16-22 yearsFemur (upper leg) 15,5-19,55 years 14.5-22 yearsTibia (lower leg) 15,5-22 years 14.5-19.5 yearsClavicle (collarbone) 19-30 years 19-20 years
Table 1.Examples of five different long bones and the expected agewhere epiphyseal fusion occurs (From: Dabba JJ.Forensis 101.Epiphyseal fusion. www.jenjdanna.com).
De Sanctis_StesuraMAGAM 2 05/05/16 09:23 Pagina 8

Furthermore, there is strong concern over the dental and bonetesting procedures conducted by dentists and physicians whoare attempting to determine the age of young individuals for legalreasons (48). Inaccurate results would lead authorities to impri-son some children with adult prisoners, which is unsafe and inap-propriate for minors (49). For example, the Australian Society ofForensic Odontology gave evidence that wisdom teeth can startdeveloping ‘from mid-teens to early 20s’. For these reasons, theInternational Organization for Forensic Odonto-Stomatology(IOFOS) has published recommended procedures for qualityassurance in forensic dental age estimation (50).
d. Other methodsThe Iliac crest (Risser?s) test ,which requires an X-ray of the pel-vic girdle, is thought to be a relatively reliable method for asses-sing age between the ages of 12 to 16 years. However, theimpact of irradiation to the gonad has to be considered. Recentdata from Denmark suggest that analysis of X-ray of the shoulderarea yields the most accurate results regarding actual age (51).The use of non-ionizing radiation methods including magneticresonance imaging (MRI) and ultrasound is attractive. Similarreservations, as X-ray evaluation, must apply due to considerablevariation in the MRI-assessed rate of bone development duringadolescence and age of attainment of maturity. Further research is needed to validate the MRI approach toassessing age in normal populations before considering its useas a routine method for undocumented minors (32, 33).
Ethical aspects
Professionals working with children should always strive to takeethical guidelines into consideration in making decisions affec-ting these children. Even though the radiation dose from an X-rayof the hand is small (equivalent to 0.00017 mSv, i.e. 1-h exposu-re to background radiation in many cities) (52), clinicians have toconsider whether or not the advantages outweigh the risks ofinflicting radiation upon an individual. This is because ionizing radiation is a consistently identified andpotentially modifiable risk factor for meninigioma (brain tumour)(53, 54).
The use of multifactorialapproaches for the assessmentof chronological age
Most submissions to the inquiry openly acknowledge that thereis no single reliable scientific method for determining a person’sage. However, some go on to suggest that a ‘multifactorial’approach will provide more reliable assessment employing acombination of medical age assessment processes.
mograph of each tooth is assessed individually and comparedwith the stage of the Nolla table. The dental age calculated cor-responds to the sum of the Nolla scores. This method requiresvery consistent discrimination by the observer in assessing den-tal maturity through radiography.
Advantages Estimating age from the teeth has several advantages over ske-letal ageing. The development of both the deciduous and per-manent teeth can be studied from the embryonic period untilearly adult life. In addition, it is commonly observed that, for agiven chronological age, dental age shows less variability thandoes skeletal age (39-41). For younger individuals, age estima-tion was more accurate due to the presence of many developingteeth, particularly the canines, premolars, as well as first andsecond molars; the intervals between morphological stages areshorter for individuals younger than 16 years of age and therefo-re, dental age estimation of these subjects is more accurate.Dental development is less affected than bone by adverse envi-ronmental circumstances such as nutrition and disturbances ofendocrine function. The reasons of less variability in dental age are not fully under-stood. A possible reason is that the development of all the deci-duous dentition and part of the permanent dentition takes placebefore birth in a protected environment whereas skeletal growthand development, even though having a strong genetic basis, isexposed for an increasing length of time to external factors suchas variations in nutrition, socio-economic status.
Disadvantages• Demirjian method use orthopantomograms which are difficult
to obtain in young children, due to both technical reasons, aswell as legal and ethical considerations (42).
• Since simultaneous evaluation of seven left mandibular teethare required, this cannot applied to children with lacking teethdue to an inborn or acquired defect (42).
• This method may not express, agenesis of teeth, distinctiveretardation of dental development (excluding third molars),and systemic diseases and various developmental stages ofthe tooth (43).
• This method does not give maturity scores for stages 1-4 incase of 1st molar, central and lateral incisor; thus excludingthe individuals below the age of 4-4.5 years (44).
• The accuracy of Demirjian method decreases in estimatingthe dental age in girls over 11 and boys over 13 years old. Thefact that overestimation was more pronounced in grown-upchildren could perhaps be linked to the puberty and this resultwas in agreement with the studies Bagherian et al. (45).
• Examining crown and root growth and maturation radio-graphically can be varying due to different reasons such as:poor resolution of the radiographic images and biologicalvariation among various populations studied (46,47)
Rivista Italiana di Medicina dell’Adolescenza
Volume 14, n. 1, 2016
9
An essential approach to the age assessment in undocumented minors in conflict with the law
De Sanctis_StesuraMAGAM 2 05/05/16 09:23 Pagina 9

10
Conclusions
Age estimation presents a complex problem and requires consi-derable experience in recognizing significant changes andallowing for their variability with in any particular population. Age determination has great importance in many clinical deci-sions, being commonly used in pediatrics, legal medicine, foren-sic sciences, anthropology, odontopediatrics and orthodontics.Increased immigration and mixing of populations, due to the glo-balized economy resulting from the increased migratory flow,sets legal problems of various orders, with increasing importan-ce of determining the chronological age of children, youths andyoung adults. So, estimating chronological age is important inassessing the legal adult age of people without documents forjudicial purposes. In practice, age determination is extremely dif-ficult to do with certainty, and no single approach to this can berelied on. Moreover, for young people aged 15–18 it is even lesspossible to be certain about age. There may also be difficulties indetermining whether a young person, who might be as old as 23,could in fact be under the age of 18.Therefore, there is a need both for identifying the best combina-tion of methods and for finding the best approach for combiningthem and arriving at age estimates and associated uncertainties.Furthermore, there is also a need for a satisfactory way to scien-tifically determine the margin of error when combing methods,and there is a need for studies based on data from differentmethods that are acquired simultaneously from a single referen-ce population.
References
1. Ash P. But he knew it was wrong: evaluating adolescent culpability. JAm Acad Psychiatry Law. 2012; 40:21-32.
2. Blustein J. Adolescence and criminal responsibility. Int J ApplPhilos.1985; 2:1-17.
3. Richards N.Criminal children. Law Philos. 1997; 16: 63-89.
4. Sickmund M. Juveniles in court. Washington, DC: U.S. Departmentof Justice, Office of Juvenile Justice and Delinquency Prevention,NCJ 195420, June, 2003.
5. Snyder HN, Sickmund M, Poe-Yamagata E. Juvenile Offenders andVictims: 1996 Update on Violence. Washington, DC: Office ofJuvenile Justice and Delinquency Prevention, 1996.
6. Focardi M, Pinchi V, De Luca F, et al. Age estimation for forensicpurposes in Italy: ethical issues. Int J Legal Med. 2014; 128:515-22.
7. International Juvenile justice and related issues: from zimmer.csufresno. edu/~haralds / FOREIGNJUVJUS.htm.
8. htp://www.studiocelentano.it/codici/cp/index.htm – accessed at20.02.2010.
9. htp://www.giustizia.it/cassazione/leggi/dpr 448_88.html – accessedat 20.02.2010.
10. European migration network. Policies on reception, return andintegration arrangements for, and numbers of unaccompanied
minors - an EU comparative study. May 2010. [Internet]. [cited 2012Aug 30th]; Available from:http://emn.intrasoftintl.com/Downloads/prepareShowFiles.do?directoryID=115
11. Schmeling A, Grundmann C, Fuhrmann A, et al. Criteria for ageestimation in living individuals. Int J Legal Med. 2008; 122:457-60.
12. De Sanctis V, Soliman AT, Soliman NA, et al. Pros and cons for themedical age assessments in unaccompanied minors: A mini-review.Submitted for publication.
13. Marshall WA, Tanner JM. Variations in pattern of pubertal changes ingirls. Arch Dis Child. 1969; 44:291-303.
14. Marshall WA, Tanner JM. Variations in the Pattern of PubertalChanges in Boys. Arch Dis Child. 1970; 45:13-23.
15. Levenson R, Sharma A. The health of refugee children – guidelinesfor paediatricians.London: Royal College of Paediatrics and ChildHealth, 1999.
16. The Royal College of Paediatrics and Child Health. Policy statementon the assessment of the age of refugee children. 2007. Available atwww.rcpch.ac.uk/Publications/Publications-list-by-title. [AccessedDecember 2007].
17. Kullman L. Accuracy of two dental and one skeletal age estimationmethod in Swedish adolescents. Forensic Sci Int. 1995;75:225-36.
18. Kullman L, Johanson G, Akesson L. Root development of the lowerthird molar and its relation to chronological age. Swed Dent J. 1992;16:161-7.
19. Arany S, lino M, Yoshioka N. Radiographic survey of third molardevelopment in relation to chronological age among Japanesejuveniles. J Forensic Sci. 2004; 49:534-8.
20. Greulich WW, Pyle SI. Radiographic Atlas of Skeletal Development ofthe Hand and Wrist. 2nd ed. Stanford (USA): Stanford UniversityPress; 1959.
21. Tanner JM, Whitehouse RH, Marshall WA, Healy MJR, Goldstein H.Assessment of Skeletal Maturity and Prediction of Adult Height.London (UK): Academic Press; 1975.
22. Tanner JM, Healy MJR, Goldstein H, Cameron N. Assessment ofSkeletal Maturity and Prediction of Adult Height (TW3 method).London (UK): Saunders; 2001.
23. Beunen GP, Malina RM, Lefevre J, et al. Skeletal maturation, somaticgrowth and physical fitness in girls 6-16 years of age. Int J SportsMed. 1997; 18:413-419.
24. Bull RK, Edwards PD, Kemp PM, Fry S, et al . Bone age assessment:a large scale comparison of the Greulich and Pyle, and Tanner andWhitehouse (TW2) methods. Arch Dis Child. 1999; 81:172-3.
25. King DG, Steventon DM, O’Sullivan MP, et al. Reproducibility of boneages when performed by radiology registrars: an audit of Tanner andWhitehouse II versus Greulich and Pyle methods. Br J Radiol. 1994;67:848-851.
26. Bland JM, Altman DG. Statistical methods for assessing agreementbetween two methods of clinical measurement. Lancet 1986; 1:307-10.
27. Ontell FK, Ivanovic M, Ablin DS, et al. Bone age in children of diverseethnicity. Am J Roentgenol. 1996; 167:1395-8.
28. Mora S, Boechat MI, Pietka E, et al. Skeletal age determinations inchildren of European and African descent: applicability of theGreulich and Pyle standards. Pediatr Res. 2001; 50:624-8.
29. Groell R, Lindbichler F, Riepl T, et al. The reliability of bone agedetermination in central European children using the Greulich andPyle method. Br J Radiol. 1999; 72:461-4.
Rivista Italiana di Medicina dell’Adolescenza
Volume 14, n. 1, 2016
An essential approach to the age assessment in undocumented minors in conflict with the law
De Sanctis_StesuraMAGAM 2 05/05/16 09:23 Pagina 10

44. Khorate MM, Dinkar AD, Ahmed J. Accuracy of age estimationmethods from orthopantomograph in forensic odontology: Acomparative study. Forensic Sci Int. 2014; 234:184.e1-8.
45. Bagherian A, Sadeghi M. Assessment of dental maturity of childrenaged 3.5 to 13.5 years using the Demirjian method in an Iranianpopulation. J Oral Sci. 2011; 53:37-42
46. Liversidge HM, Lyons F, Hector MP. The accuracy of three methodsof age estimation using radiographic measurements of developingteeth. Forensic Sci Int. 2003; 131:22–9.
47. Liversidge HM, Smith BH, Maber M. Bias and accuracy of ageestimation using developing teeth in 946 children. Am J PhysAnthropol. 2010; 143:545–54.
48. Taylor JDevelopment of the Australian Society of ForensicOdontology disaster victim identification forensic odontology guide. JForensic Odontostomatol. 2009; 27:56-63.
49. Solheim T, Vonen A. Dental age estimation, quality assurance andage estimation of asylum seekers in Norway. Forensic Sci Int. 2006;159(Suppl 1):S56-60.
50. http://www.odont.uio.no/foreninger/iofos/quality/Age-IOFOS.htm
51. Ranta H. Age Assessment of a Child, University of Helsinki,Department of Forensic Medicine, Annex 7 of Separated Children inEurope Programme, Report of the Workshop on Age Assessmentand Identification, Bucharest 20-22 March 2003.
52. Engebretsen L, Steffen K, Balhr R, et al. The International OlympicCommittee statement on age determination in high level youngathletes. Br J Sports Med. 2010; 44:476-88.
53. Claus EB, Calvocoressi L, Bondy ML, et al. Dental X-rays and Risk ofMeningioma. Cancer 2012 (early view)http://onlinelibrary.wiley.com/doi/10.1002/cncr.26625/pdf (20 April2012, date last accessed).
54. The Economist. Little and not often please - confirmation that dentalx-rays can be bad for you, 14 April 2012www.economist.com/node/21552538 (20 April 2012, date lastaccessed).
30. Garamendi PM, Landa MI, Ballesteros J, et al. Reliability of themethods applied to assess age minority in living subjects around 18years old. A survey on a Moroccan origin population. Forensic SciInt. 2005; 154:3-12.
31. De Sanctis V, Di Maio S, Soliman AT, et al. Hand X-ray in pediatricendocrinology: Skeletal age assessment and beyond. Indian JEndocrinol Metab. 2014; 18 (Suppl 1):S63-71.
32. De Sanctis V, Soliman AT, Di Maio S, Bedair S. Are the newautomated methods for bone age estimation advantageous over themanual approaches? Pediatr Endocrinol Rev. 2014; 12:200-2005.
33. De Simone M, Farello G, Palumbo M, et al. Growth charts, growthvelocity and bone development in childhood obesity. Int J ObesRelat Metab Disord. 1995; 19:851-7.
34. McKenna CJ, James H, Taylor JA, Townsend GC. Tooth developmentstandards for South Australia. Aust Dent J. 2002; 47:223-7.
35. Panchbhai AS. Dental radiographic indicators, a key to ageestimation. Dentomaxillofac Radiol. 2011; 40:199-212.
36. Demirjian A, Goldstein H, Tanner JM. A new system of dental ageassessment. Hum Biol. 1973; 45:211-27.
37. Nolla CM: The development of the permanent teeth. J Dent Child.1960; 27:254-66.
38. Al-Emran S. Dental age assessment of 8.5 to 17 Year-old Saudi childrenusing Demirjian’s method. J Contemp Dent Pract. 2008; 9:64-71.
39. Garn SM, Lewis AB, Polachek DL. Variability of Tooth Formation. JDent Res. 1959; 38:135-48.
40. Moorrees CFA, Fanning EA, Hunt EE. Formation and resorption of threedeciduous teeth in children. Am J Phys Anthropol. 1963; 21:99-108.
41. Morrees CFA, Fanning EA, Hunt EE. Age variation of formation stagesfor ten permanent teeth. J Dent Res.1963; 42:1490-502.
42. Stavrianos C, Mastagas D, Stavrianou I, Karaiskou O. Dental ageestimation of adults: A review of methods and principles. Res J MedSci. 2008; 2:258-68.
43. Rózylo-Kalinowska I, Kiworkowa-Raczkowska E, Kalinowski P. Dentalage in Central Poland. Forensic Sci Int. 2008; 174:207-16.
Rivista Italiana di Medicina dell’Adolescenza
Volume 14, n. 1, 2016
11
An essential approach to the age assessment in undocumented minors in conflict with the law
Correspondence:
Vincenzo de Sanctis, MDPediatric and Adolescent Outpatient ClinicQuisisana Private Accredited HospitalViale Cavour, 128 - Ferrara (Italy)Phone: 0532 207622E-mail: [email protected]
De Sanctis_StesuraMAGAM 2 05/05/16 09:23 Pagina 11

12
Aderenza e compliance al trattamento con ormone della crescita
Adherence and compliance to GH treatment
SummaryGrowth hormone (GH) is now being used since many years for the treatment of various growth disorders in
childhood and adolescence. Its efficacy in promoting growth is influenced by several factors, among which adherence (A) andcompliance (C) have been recognised as of primary importance for the growth response to treatment. Many studies on A/C toGH therapy have now been published, showing a wide range of A/C percentages (10% - 95%), possibly due to the different cri-teria in defining and evaluating A/C. All together, the different studies have demonstrated association between A/C and age,socio-economic condition, treatment duration and modalities (injection devices). A positive correlation has been shownbetween A/C and growth velocity, confirming the importance of A/C for the growth response to GH treatment. Different inter-ventions have been suggested aiming at improving A/C, including share, between physician, patient and caregivers, of treat-ment modalities, decision to treat and choice of injection device, together with explanation and discussion of the rationale andaim of therapy. This review of the scientific literature on these issues reports the data available so far on this topic.
Key words: Growth hormone, growth disorders, GH treatment, adherence, compliance.
RiassuntoL’ormone della crescita (GH) è ormai da tempo utilizzato nel trattamento di diverse patologie dell’accrescimen-
to sia in età pediatrica che adolescenziale. La sua efficacia è influenzata da numerosi fattori, tra i quali l’aderenza (A) / compli-ance (C) è stata riconosciuta di primaria importanza per la risposta accrescitiva alla terapia. Sono stati pubblicati molti studisull’A/C al trattamento con GH, con una gamma di percentuali di A/C molto ampia (tra il 10 e il 95% circa), verosimilmente dovu-ta ai diversi criteri di definizione di A/C e ai diversi metodi di valutazione di A/C. Nell’insieme, gli studi pubblicati hanno dimostra-to associazione tra A/C (o non-A/C) ed età, condizione socio-economica, durata del trattamento e modalità e dispositivi diiniezione. È stata dimostrata una correlazione positiva tra A/C e velocità di crescita sotto trattamento, che conferma l’impor-tanza della A/C sulla risposta accrescitiva al GH. Sono stati suggeriti vari interventi per migliorare A/C, tra cui la condivisione,tra medico, paziente e suoi genitori, delle modalità di trattamento, della decisione di trattare e della scelta del dispositivo diiniezione, oltre alla comunicazione e discussione del razionale e delle finalità del trattamento. Questa revisione della letteratu-ra discute i dati finora disponibili sull’argomento.
Parole chiave: Ormone della crescita, disordini accrescitivi, trattamento con GH, aderenza, compliance.
Fabio Buzi
S.C. Pediatria, A.S.S.T. Mantova – “C. Poma”
Introduzione
L’ormone della crescita (GH) è ormai in uso da più di 50 anni neltrattamento delle patologie della crescita, inizialmente comeormone estrattivo (da ipofisi umane) e, dagli anni ’80 del secoloscorso, come ormone ricombinante umano (rhGH) (1).La finalità principale della terapia con rhGH è quella di normaliz-zare la velocità di crescita dei piccoli pazienti nel minor tempopossibile e di far loro raggiungere un statura finale il più possibi-le adeguata al modello familiare, minimizzando rischi e costi deltrattamento (2). Attualmente, oltre al deficit di GH, le indicazionial trattamento in Europa comprendono il deficit accrescitivo
secondario a s. di Turner (TS), s. di Prader-Willi (PWS), insuffi-cienza renale cronica (CRF), deficit di gene SHOX (SHOX-D) epeso e/o lunghezza alla nascita piccoli per età gestazionale(SGA); in altri Paesi a queste indicazioni si aggiungono acondro-plasia, s. di Noonan (NS) e bassa statura idiopatica (ISS).Il successo della terapia con GH non è costante in tutte le con-dizioni, e diverse possono essere le ragioni di un insuccesso o diun successo solo parziale. È stato infatti dimostrato che la rispo-sta accrescitiva al trattamento con GH è funzione delle modalitàdello stesso: dose di GH e frequenza delle somministrazioni son
Buzi sinistra_StesuraMAGAM 2 05/05/16 09:39 Pagina 12

Rivista Italiana di Medicina dell’Adolescenza
Volume 14, n. 1, 2016
13
Aderenza e compliance al trattamento con ormone della crescita
infatti direttamente proporzionali all’efficacia, e la risposta nel 1°anno di terapia (in termini di velocità di crescita e guadagnoaccrescitivo) dipende da diverse variabili, alcune direttamenteproporzionali, come dose di GH e frequenza delle somministra-zioni, e altre negativamente correlate (età all’inizio del trattamen-to, età ossea, velocità di crescita pre – trattamento). Esiste inoltre una variabilità individuale di risposta da attribuire adiversi gradi di resistenza al GH e variabili genetiche individuali (3);tuttavia grande importanza è sempre stata attribuita la grado diaderenza / compliance del singolo paziente.
Aderenza e Compliance
I concetti di “Aderenza”(A) e di “Compliance” (C) a una terapiadifferiscono leggermente dal punto di vista semantico (4), anchese sono spesso usati come sinonimi in Medicina. A rigore, l’A consiste nell’esecuzione corretta della terapia neimodi e tempi della somministrazione, mentre il concetto di Cimplica anche un atteggiamento di condiscendenza, condivisio-ne e allineamento al razionale della terapia stessa. Più specificamente, l’A può essere definita come “il grado concui il comportamento di una persona, rispetto all’assunzione diuna terapia, al seguire una dieta e/o attuare cambiamenti di stiledi vita, rispetta le raccomandazioni concordate con un operatoredi salute”(5); la C invece può essere definita come “il grado concui il comportamento del paziente … coincide con la prescrizio-ne clinica”(6). Altri Autori distinguono addirittura A e C da “concordanza(Concordance)”: “partecipazione del paziente al processo deci-sionale” (7). Nel presente articolo saranno usati indifferentemen-te come termini sovrapponibili, dato che appartengono in questocontesto alla medesima problematica. Allo stesso modo, le defi-nizioni di non-aderenza (non-A) (e non-compliance: non-C) pos-sono variare: alcuni autori specificano cut-off fissi, come una Ainferiore all’80 o al 95% (8), mentre altri considerano la non-Acome “quella sufficiente a interferire significativamente con il rag-giungimento dell’obiettivo terapeutico” (9).La non-C in Medicina è stata identificata nel tempo come unimportante problema di salute pubblica, che comporta anche unnotevole carico finanziario sull’attuale sistema sanitario.La ricerca in questo settore è stata quindi molto vasta, finalizza-ta alla comprensione, misurazione e risoluzione della non-C, enell’insieme è stato osservato che da un terzo alla metà deipazienti non rispettano i consigli e le prescrizioni mediche (10).Mentre in passato però il ruolo del paziente era praticamente rite-nuto secondario rispetto a quello del prescrittore/somministratoredi terapia, nel corso del tempo il ruolo decisionale del pazientenella gestione del trattamento ha assunto un’importanza sempremaggiore, anche in seguito al prevalere della patologia cronica suquella acuta: in questo senso il coinvolgimento del paziente (e deisuoi genitori/tutori se in età pediatrica) è di fondamentale impor-
tanza, sia in termini di informazione rispetto alla terapia che diautonomia decisionale rispetto alla esecuzione o meno della stes-sa, alla scelta del tipo di trattamento e delle sue modalità.L’A in Pediatria è particolare in quanto non è limitata al solopaziente, ma si estende ai genitori/tutori, e anche perché il bam-bino spesso non è consapevole dell’importanza e delle finalitàdella terapia ed è quindi riluttante ad assumerla (11).Le ragioni di una non-A /non-C possono essere così sintetizzate: • fastidio / scomodità; trattamenti a lungo termine (ad es.
necessità di assunzioni multiple nella giornata per lunghiperiodi: mesi – anni – a vita), specie se a somministrazioneiniettiva: si pensi ad es. a una terapia insulinica nel diabetemellito di tipo I, con 4 iniezioni sottocutanee al giorno secon-do le indicazioni correnti (12, 13),
• regimi terapeutici complessi (ad es. trattamenti multipli e misti,come in endocrinopatie multiple o in forme sindromiche condeficit multi – organo),
• età (ad es. tipicamente l’età adolescenziale, in cui è frequentela ribellione e/o il rifiuto della malattia e della sua terapia),
• dinamiche individuali e familiari (depressione, disagio sociale,problemi economici e organizzativi, ecc.),
• livello di comprensione dei benefici del trattamento e delleconseguenze della non-C da parte del paziente/famiglia.
È evidente da tutto ciò che i pazienti a cui viene somministratol’ormone della crescita per mezzo di iniezioni sottocutanee quoti-diane per molti anni consecutivi sono ad alto rischio di non-C, conconseguente fallimento o scarsa efficacia della terapia stessa.Il trattamento con rhGH, come è noto, è molto costoso: il costoannuale per un bambino di 30 kg, ad esempio, varia da 15000 a20000 dollari, e il costo annuale per far raggiungere ad adole-scenti una statura finale ottimale può raggiungere i 50000 dollari(14). Pertanto una non-C può anche condurre a un notevolespreco economico oltre che incidere negativamente sulla rispo-sta accrescitiva al trattamento.
Metodi per misurare A/C
A e C possono essere valutati con diversi metodi, ciascuno convantaggi e svantaggi: non esistendo un metodo ideale, vienesuggerito di usare più metodi combinati per ottimizzare l’affida-bilità (8).I metodi più frequentemente usati sono stati i seguenti:a. piani terapeutici prescritti o rinnovati: incrociando le prescri-
zioni fatte dal Centro con le prescrizioni eseguite dal medicocurante: questo vale laddove le prescrizioni vengano effettua-te dal medico di territorio su indicazione del Centro, e nondove la prescrizione avvenga direttamente da parte del Centroattraverso la farmacia dell’ospedale. Utilizzato in vari studi (13, 15, 16), questo metodo ha il van-taggio di essere relativamente oggettivo, non invadente ed
Buzi sinistra_StesuraMAGAM 2 05/05/16 09:39 Pagina 13

14
Rivista Italiana di Medicina dell’Adolescenza
Volume 14, n. 1, 2016
Aderenza e compliance al trattamento con ormone della crescita
d. sono stati anche proposti metodi basati sulla misurazione delGH nelle urine delle 12 ore precedenti il controllo, che correla-no con la A: sono stati infatti osservati livelli di GH urinario piùelevati in caso di A, che diminuivano significativamente anchesolo dopo 2 dosi mancate.Tuttavia queste metodiche hanno evidenti problemi di appli-cazione pratica (17), come pure il dosaggio dei livelli siericidi IGF-I. Questi ultimi sono infatti normalmente utilizzati dallamaggior parte dei clinici per valutare l’efficacia della terapiae controllarne la sicurezza, mentre non ne è chiaramentedimostrata l’affidabilità come indicatori di A (21), data anchela eterogeneità delle variabili che possono influenzarne i livel-li (22-24).
Studi clinici su C/A
Diversi studi hanno valutato la prevalenza di non-A / non-C inpazienti pediatrici trattati con GH; la percentuale di non-A / non-C mostra un’ampia variabilità, dal 5 all’80%, certamente a causadei diversi metodi di valutazione e della definizione di A/C. Le principali caratteristiche degli studi sono riassunte in Tabella 1.
economico, con dati semplici da ottenere (può servirsi adesempio di questionari da inviare al medico curante) e pos-siede un buon grado di concordanza con altri metodi di misu-ra di A (8, 17, 18). Ha tuttavia lo svantaggio di fornire solo unamisura grossolana della A (8, 16);
b. questionari compilati dal paziente e/o genitori /tutori: presenta-no concordanza da moderata a forte con i metodi precedente-mente esposti e hanno, come questi, il vantaggio di esseresemplici ed economici (19). Principale svantaggio è la scarsasensibilità per la non-A (spesso < 50%), che può essere attri-buita a difficoltà di ricordare i particolari della somministrazionedel farmaco e/o il timore di affrontare discussioni o di deluderei sanitari. Altro svantaggio è l’aspetto temporale: i pazienti ricor-dano meglio quanto accaduto negli ultimi giorni o sono piùattenti alla terapia nei giorni che precedono il controllo;
c. un altro metodo, certamente più affidabile, è quello della forni-tura diretta del farmaco da parte della farmacia del Centro diriferimento con l’obbligo di restituzione delle fiale utilizzate alCentro stesso al momento del successivo controllo: questometodo e i suoi vantaggi / svantaggi verrà discusso successi-vamente a proposito dello studio di Cutfield et al. (20) sullanon-A al trattamento con GH.
Referenza N° Metodo Definizione % bibliografica pazienti di non-A/C non-A/C
(26) 188 Questionario compilato >5 iniezioni perse dall’ultimo controllo 51da chi somministrava GH >10 iniez. Perse dall’ultimo controllo 19
(27) 107 Colloquio con paziente genitori ≥ 3 iniezioni perse / mese 10
(28) 177 Questionario compilato Mancata compliance a tutti 16-42da chi somministrava GH gli aspetti della terapia
(29) 29 (CRF) Questionario compilato ≥ 1 iniez. persa / mese 62dal paziente e/o genitori ≥ 6 iniez. perse / mese 7
(30) 473 Questionario somministrato ≥ 5 iniez. perse dall’ultimo controllo 6da infermiere a paziente e/o genitori
(31) 17 (CRF) Colloquio con i genitori <1 iniezione persa / sett. 35-82≥ 1 iniez. persa /sett. 6-9
(32) 631 Non definito ≥ 3 iniez. perse / mese 15-24≥ 15 iniez. Perse / mese 6-13
(33) 50 Conto delle fiale Non specificamente definita 5-8
(13) 6487 Rinnovo prescrizioni Non rinnovo prescrizione 5-10nel 1° anno di terapia
(16) 75 Prescrizioni rilasciate >1 iniez. persa / sett. 39>2 iniez. perse / sett. 23
(34) 882 Questionario compilato non-C occasionale 64-77da paziente / genitori non-C e scetticismo
(20) 175 N° fiale richieste / mese >1 iniezione persa / sett 34N° fiale restituite / mese 1 iniezione persa / sett. 66
Tabella 1.Principali studi su non-A / non-C al trattamento con rhGH (da ref. 25, modificata).
Buzi sinistra_StesuraMAGAM 2 05/05/16 09:39 Pagina 14

Rivista Italiana di Medicina dell’Adolescenza
Volume 14, n. 1, 2016
15
Aderenza e compliance al trattamento con ormone della crescita
Come si evince dalla Tabella 1 la maggior parte degli studi basala percentuale di non-A/C sulla somministrazione di questionariautocompilati o addirittura sul colloquio con il paziente e /o geni-tori / tutori in occasione della visita di controllo, con tutti i limiti diaffidabilità già esposti. Lo studio che utilizza una metodologia piùprecisa (incroci tra numero di fiale necessarie per il trattamentoprescritte e numero di fiale utilizzate ritirate al momento del con-trollo) è quello di Cutfield et al., condotto in Nuova Zelanda su175 pazienti con bassa statura di diversa eziologia (GHD, TS,ISS, SGA, PWS) (20). Più in particolare, la C è stata valutata condue modalità:• numero di fiale di GH richieste per mese per paziente (GHreq,
basate su autoreferenza verbale da parte di chi assisteva ilpaziente),
• numero di fiale restituite (GHret) entrambe espresse come percentuale del numero di fiale pre-scritte per ciascun paziente. Una C soddisfacente era definitacome l’85% o più di A al trattamento prescritto, equivalente allaperdita media di una iniezione / settimana. I pazienti (N° 175)vennero divisi in 3 gruppi:- C elevata (≤ 1 dose persa / settimana)- C media (>1 and <3 dosi perse / settimana),- C bassa (≥ 3 dosi perse / settimana).
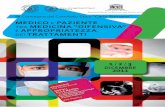
La percentuale globale di non-C risultò del 66% (73/110) sullabase di GHret e addirittura del 34% (59/172) sulla base di GHreq.Calcolando la perdita di efficacia in base al tasso di non-C, gliautori osservarono che, sui 6-8-mesi di osservazione della velocitàdi crescita, la perdita di >1 dose per settimana si traduceva in unadiminuita efficacia del trattamento in termini di velocità di crescita,direttamente proporzionale al numero di dosi perse (Figura 1).
alcuna restrizione finanziaria personale alla disponibilità di GH;questo si ripercuote anche sull’efficacia, visto che i pazienti cheperdevano più di una dose / settimana mostravano una crescitasignificativamente ridotta rispetto a quelli con buona C.Inoltre lo studio mostrava che il metodo di valutazione della Cbasato sul numero di fiale restituite (“GHret”) è più efficace eobiettivo nel valutare la C rispetto a quello dell’autodichiarazioneda parte delle famiglie del numero di fiale usate (GHreq), anchese GHret potrebbe sottovalutare la C a causa di possibili fialerotte, perse o semplicemente non restituite, in quanto la restitu-zione non era un presupposto necessario per ricevere il rinnovodella fornitura del farmaco. Il metodo “GHreq” non differirebbeinoltre dai metodi usati per valutare la C in precedenti studi,basati su questionari compilati dai pazienti (16, 26, 30, 32, 34):infatti i genitori potrebbero non voler ammettere di aver perso odimenticato somministrazioni per imbarazzo o timore di essererimproverati dai sanitari.Un sistema alternativo potrebbe essere l’uso di dispositivi elet-tronici con la memorizzazione della dose di farmaco sommini-strata, che fornirebbero una valutazione più affidabile della C delpaziente. Il limite di questi dispositivi è soprattutto nel costo enella maggiore complessità di utilizzo.In un recente studio multicentrico su 217 pazienti trattati con GHper diverse cause (GHD, TS, SGA, ecc.) in Turchia (35) gli Autorihanno suddiviso i pazienti, in base alla percentuale di A, in 4gruppi: A eccellente (0% di dosi perse), A buona (fino a 5%), Adiscreta (5-10%) e A scarsa (>10%). La percentuale di aderenzadiminuiva con il passare dei mesi di trattamento: i pazienti con Aeccellente / buona mostravano velocità di crescita significativa-mente superiore a quelli con A discreta / scarsa, così come i livel-li di IGF-I correlavano direttamente con la percentuale di A.Un altro studio recente sull’A al trattamento con GH è stato effet-tuato su pazienti pediatrici con Insufficienza Renale Cronica(CRF), nell’ambito di un ampio studio collaborativo tra 55 Centridi Nefrologia Pediatrica del Nord America (Chronic KidneyDisease in Children – CkiD – study)(36). L’A al trattamento conGH era valutata insieme a quella di altri farmaci (Vitamina D, che-lanti del fosforo, eritropoietina, alcali, ferro) e correlata alla rispo-sta accrescitiva. La definizione di non-A era dicotomica: i pazien-ti riferivano a ogni visita di controllo se avevano perso almenouna dose / settimana di qualsiasi dei farmaci prescritti: la non-Aera definita come la perdita di almeno 1 dose per ciascun far-maco considerato. Questa definizione quindi, oltre ad essereautoriferita (con le limitazioni già discusse più sopra) non tenevaconto della severità della non-A (se cioè veniva persa una o 2 o3 o più dosi, per cui il paziente che perdeva una sola dose eraassimilato a quelli che ne perdevano di più). Mentre non venivatrovata alcuna correlazione tra non-A alle altre terapie diverse dalGH, i pazienti aderenti al trattamento con GH mostravano gua-dagno staturale maggiore rispetto a quelli non aderenti, in cuinon veniva osservato alcun guadagno accrescitivo. In particola-re, i pazienti aderenti al GH mostravano un incremento annuo
Figura 1.SDS di velocità di crescita (HVSDS, media ± SD) su 6-8 mesi inbase al livello di compliance al trattamento con GH (Cutfield WSet al. 2011) (v. testo).
Gli Autori conclusero che lo studio indicava che la non-C è moltofrequente in Nuova Zelanda nonostante un contesto in cui esisteun contatto regolare con gli operatori sanitari e in cui non c’è
HVSDS
Compliancebassa media elevata0
1
2
3
4
Buzi sinistra_StesuraMAGAM 2 05/05/16 09:39 Pagina 15

16
Rivista Italiana di Medicina dell’Adolescenza
Volume 14, n. 1, 2016
Aderenza e compliance al trattamento con ormone della crescita
Il 48% dei genitori riferiva mancanza di libertà di scelta del dispo-sitivo di somministrazione del GH che più si adattasse al lorofiglio; la quasi totalità riteneva che i loro figli e loro stessi avreb-bero tratto vantaggio dall’autosomministrazione, dopo adeguatoaddestramento; il 37% riferiva che i loro figli vivevano con ansiala terapia con GH, e l’83% avrebbe apprezzato un supporto psi-cologico per superare tale ansia.Allo stesso modo la metà circa dei genitori avrebbe auspicatosupporto psicologico per superare l’aumento della riluttanza allaterapia da parte dei figli che si presentava con l’età puberale.In sostanza, quindi, gli autori sottolineavano come la compren-sione delle finalità e delle implicazioni del trattamento con GHveniva percepito dai genitori come presupposto per ottenere unamigliore A alla terapia e che i loro dati suggerivano la necessitàdel coinvolgimento dei genitori nel processo decisionale nellascelta del dispositivo, fondamentale per migliorare l’accettazionedel trattamento e ridurre i problemi emotivi dei loro figli.Tuttavia proprio uno dei più recenti studi sull’A in 103 pazientitrattati con rhGH ha al contrario rilevato come proprio la auto-somministrazione sembri essere un predittore negativo di A altrattamento, insieme all’età puberale (46); l’A in questi pazientiera inoltre inferiore a quella di 97 soggetti pediatrici in trattamen-to con L-Tiroxina, sottolineando l’importanza della via di sommi-nistrazione (iniettiva per il GH e orale per la L-Tiroxina) come fat-tore che influenza A/C, come già detto più sopra.Resta comunque valida la raccomandazione del massimo coin-volgimento del paziente e dei suoi famigliari nella decisione di ini-ziare il trattamento e nella scelta del dispositivo: come accenna-to più sopra, in questo caso ai concetti di A e C (obiettivi da per-seguire che concorrono all’efficacia del trattamento) si aggiungequello di “concordanza”: quest’ultima infatti riguarda più stretta-mente il rapporto tra il paziente e il clinico e si basa sulla convin-zione che le due figure debbano “lavorare insieme”, in accordocon la moderna visione della condivisione dell’informazione coni paziente e della sua responsabilizzazione per una decisioneterapeutica informata e consapevole (51).
Caso Clinico
DF giunge all’osservazione presso il nostro AmbulatorioAuxoendocrinologico per rallentamento della crescita.Anamnesi familiare negativa per patologie di rilievo; staturamaterna 168 cm (≥ 75° percentile); statura paterna 170 cm (≥ 10°percentile);statura media genitoriale corretta per genere: 163 cm(=50° percentile);Anamnesi fisiologica: secondogenita; ritardo intrauterino diaccrescimento (IUGR); nata alla 38° settimana da parto con tagliocesareo con peso 2020 g (< 3° percentile) e lunghezza 43 cm (< 3° percentile); Apgar 10 – 10; allattamento al seno materno;postnatalità nella norma.Anamnesi patologica remota: nulla di rilevante.
medio di 0.18 SDS in altezza rispetto a nessun cambiamento peri non-aderenti; inoltre, tra i pazienti aderenti, quelli con altezza<3° percentile mostravano un incremento medio annuo di 0.33SDS in altezza. Questi risultati sono comunque molto significati-vi se si tiene presente che nella CRF il ritardo accrescitivo è dinatura multifattoriale (37) e che non vi è carenza di GH ma unaforma di resistenza all’ormone stesso (38), per cui la rispostaaccrescitiva al GH non è sempre ottimale e necessita di dosi piùelevate che nel deficit di GH “classico”.
Metodi per migliorare C/A
Possibili strategie per migliorare la A al trattamento con GH com-prendono: riduzione della frequenza di somministrazione conformulazioni di GH a lunga durata di azione, attualmente ancorain fase di studio; uso di dispositivi di iniezione automatici o diaghi sempre più fin per ridurre il dolore o il timore del dolore e,sempre per questa finalità, utilizzo di dispositivi senza ago (need-le-free). I dispositivi di somministrazione differiscono tra loro peralcune caratteristiche importanti che possono facilitarne l’uso erendere meno fastidiosa l’iniezione. Queste caratteristiche com-prendono: passaggi nella preparazione dell’iniezione, modalitàdi ricostituzione del farmaco (polvere + liquido o preparato giàliquido), dispositivi “usa e getta” monodose o multidose, dispo-sitivi needle-free, modalità di conservazione (in frigorifero o sta-bili a temperatura ambente) e dispositivi di iniezione elettronicicon possibilità di memorizzazione delle dosi somministrate col-legabili on-line al PC o altri dispositivi elettronici del medico/infer-miere, che permetterebbero un più efficace controllo dell’A altrattamento. A questo proposito diversi studi hanno sottolineatol’utilità di dispositivi sempre più perfezionati nel migliorare l’ac-cettabilità del trattamento da parte dei pazienti (12, 27, 39-46).Questi studi (per lo più sostenuti da Aziende Farmaceutiche delsettore, e pertanto con un possibile bias di oggettività, ma nonper questo meno meritevoli di attenzione) sottolineano di volta involta i vantaggi di formulazioni liquide rispetto a quelle da misce-lare e/o che non necessitano di refrigerazione rispetto a quelleda conservare in frigorifero, o di dispositivi di somministrazioneautomatici rispetto a manuali, elettronici rispetto a meccanici osenz’ago rispetto a quelli con ago.Sebbene non vi siano dati nell’ambito del trattamento con GH,per trattamenti con altri farmaci è stato osservato un migliora-mento dell’A con calendari cartacei giornalieri (47) o incentivieconomici (48), o fornendo maggiore supporto e informazione aipazienti e alle loro famiglie sui benefici della terapia e sulle con-seguenze della non-C (49). Questo aspetto è sottolineato in uno studio olandese condottosu 69 genitori di bambini in trattamento con GH, che attraversoun questionario valutava le opinioni dei genitori circa il tratta-mento dei loro figli, con particolare attenzione alle loro percezio-ni sulla comunicazione e il supporto da parte dei sanitari (50).
Buzi sinistra_StesuraMAGAM 2 05/05/16 09:39 Pagina 16

Rivista Italiana di Medicina dell’Adolescenza
Volume 14, n. 1, 2016
17
Aderenza e compliance al trattamento con ormone della crescita
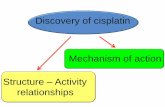
Anamnesi mirata: scarso accrescimento per cui eseguitiesami di screening da parte del Curante per scarsa crescita,risultati negativi.Alla prima visita: età 8.3 anni; altezza (Ht) 115.2 cm (-2.49 SDS);peso 19.5 kg (< 3° percentile); condizioni generali buone; obiet-tività nella norma; impubere; età ossea (TW3): 7.8 “anni”.Controllo a 9.2 anni: Ht 118.5 cm (-2.54 SDS); peso kg 21.1 (< 3° perc.); velocità di crescita (HV) 3.9 cm/anno (-2.2 SDS);test di stimolo per GH (clonidina): picco di GH dopo stimolo nellanorma (>10 ng/ml).Successivo controllo: età 9.7 anni; Ht 120.5 cm (-2.61 SDS);peso 22.2 kg; HV: 3.9cm/anno (-1.96 SDS).Impubere. Viene consigliatotrattamento con GH in baseai criteri della nota AIFA 39.Inizia trattamento con GHall’età di 10 anni, previaesecuzione di OGTT, IGF-Ie RMN ipotalamo - ipofisi,tutti risultati nella norma.Dose 6.6 mg/settimana (0.3mg/kg/settimana).1° controllo dopo inizioterapia: età 10.6 anni; Ht126.8 (-2.29 SDS); peso24 kg; stadi puberali(Tanner) B2 PH1; HV: 7.3cm/anno (+1.75 SDS).2° controllo sotto tratta-mento: età 11.1 anni; Ht130.6 cm (-2.15 SDS);peso 25.5 kg; HV 7.8 cm/anno (+1.24 SDS); stadipuberali B3 PH1; condi-zioni buone, obiettivitànella norma.3° controllo sotto tratta-mento: età 12.1 anni; Ht139.3 cm (-1.76 SDS);peso 32.0 kg; HV 9.0 cm/anno (+0.61 SDS); stadipuberali B3 PH3; condi-zioni buone, obiettività nella norma.4° controllo sotto trattamento: età 13.2 anni; Ht 145.0 cm (-1.66 SDS); peso 38.6 kg; HV 5.7 cm/ anno (-1.71 SDS); stadipuberali B3 PH3; condizioni buone, obiettività nella norma.5° controllo sotto trattamento: età 13,7 anni; Ht 147.0 cm (-1.82 SDS); peso 39.1 kg; HV: 4.4 cm/anno (-0.08 SDS); stadipuberali B4 PH4; condizioni buone, obiettività nella norma.La paziente non ha mai presentato o deposto effetti indeside-rati; la bimba si è detta soddisfatta della crescita che l’ha por-
tata a valori di statura più adeguati a quelli delle sue coetanee.I valori di glicemia, fT4, TSH e IGF-I si sono sempre mantenutinella norma; non è ancora comparso menarca e, data la cre-scita tuttora > 2 cm /anno, la paziente proseguirà il trattamen-to fino a crescita < 2 cm/anno e saldatura delle cartilagini diaccrescimento (Figura 2).Commento: la paziente è stata portata alla nostra attenzione in etàgià piuttosto avanzata e quando ancora il trattamento con GH deibambini nati SGA non era previsto dalle regole europee e italiane; èstata posta in terapia con GH non appena entrata in vigore la nor-mativa sul trattamento; la crescita sotto GH è stata certamente
influenzata dall’esordiopuberale fisiologico dellapaziente, ma il trattamentoè iniziato prima che com-parissero i primi segnipuberali, per cui nei primi 6mesi di terapia la rispostaaccrescitiva è da attribuirsialla sola terapia con GH.
Bibliografia1. Hintz RL. Growthhormone: uses and abuses.BMJ. 2004; 328:907-8.2. Growth HormoneResearch Society:Consensus guidelines forthe diagnosis and treatmentof growth hormone (GH)deficiency in children andadolescence: summarystatement of the GHResearch Society. J ClinEndocrinol Metab. 2000;85:3990-3.3. Ranke MB, Lindberg A,Chatelain P, et al. Derivationand validation of amathematical model forpredicting the response toexogenous recombinanthuman growth hormone(GH) in prepubertal childrenwith idiopathic GHdeficiency. J Clin EndocrinolMetab. 1999; 84:1174-83. 4. Bissonette JM.Adherence: a conceptanalysis. J Adv Nurs. 2008;63:634-43.
5. World Health Organisation. Adherence to long-term therapies:evidence for action 2003.http://www.who.int/chp/knowledge/publications/adheence_report/en
6. Haynes RB, Taylor DW, Sackett DL. Compliance in health care.Baltimore, John Hopkins 1979.
7. Hindmarsh PC, Brook CGD. Compliance with growth hormonetreatment – is it a problem? Horm Res. 1999; 51(Suppl.3):104-8.
8. Orsterberg L, Blaschke T. Adherence to medication. N Engl JMed.2005; 353:487-97.
9. O’Hanrahan M, O’Malley K. Compliance with drug treatment. BMJ.1981; 283:298-300.
Figura 2.
Buzi sinistra_StesuraMAGAM 2 05/05/16 09:39 Pagina 17

18
Rivista Italiana di Medicina dell’Adolescenza
Volume 14, n. 1, 2016
Aderenza e compliance al trattamento con ormone della crescita
34. Rosenfeld RG, Bakker B. Compliance and persistence in pediatricand adult patients receiving growth hormone therapy. Endocr Pract.2008; 14:143-54.
35. Kucukemre B, Aycan Z, Syklar Z, et al. Adherence to growthhormone therapy: results of a multicentre study. Endocr Pract 2014;20:46-51.
36. Akchurin OM, Schneider MF, Mulqueen L. Medication Adherenceand Growth in Children with CKD. Clin J Am Soc Nephrol. 2014;9:1519-25.
37. Bacchetta J, Harambat J, Cochat P, et al. The consequences ofchronic kidney disease on bone metabolism and growth in children.Nephrol Dial Transplant. 2012; 27:3063-71.
38. Mahesh S, Kaskel F. Growth hormone axis in chronic kidney disease.Pediatr Nephrol. 2008; 23:41-8.
39. Bozzola M, Cole M, Halldin-Stenlid M, et al. Treatment adherencewith the easypod growth hormone electronic auto-injector andpatient acceptance: survey results from 824 children and theirparents. BMC Endocrine Disord. 2011; 11:4.
40. Hokken-Koelega A, Keller A, Rakov V, et al. Patients acceptance,ease of use, and preference for Norditropin NordiFlex with NordiFlexPenMate: results from n open-label, user survey of everyday use.Endocrinol. 2011; 803948.
41. Tauber M, Jaquet D, Jesuran-Perelroizen M, et al. User assessmentof Norditropin NordiFlex®, a new prefilled growth hormone pen: aPhase IV multicenter prospective study. Patient Preference andAdherence 2013; 7:455-62.
42. Hartmann K, Ittner J, Müller-Rossberg E, et al. Growth HormoneTreatment Adherence in Prepubertal and Pubertal Children withDifferent Growth Disorders. Horm Res Pediatr 2013; 80:1-5.
43. Spoudeas HA, Bajaj P, Sommerford N. Maintaining persistence andadherence with subcutaneous growth-hormone therapy in children:comparing jet-delivery and needle-based devices. Patient PreferAdherence. 2014; 8:1255-63.
44. Partsch C-J, Schnabel D, Ehtisham S, et al. Acceptability of thereusable SurePal™ self-injection device for Omnitrope® amongpediatric patients: results from a questionnaire-based, cross-sectional, multicenter observational study. Med Devices (Auckl).2015; 8:389-93.
45. Kappelgaard AM, Metzinger CP, Schnabel D. A web-based surveyassessing the impact of storage flexibility on the daily life of patientsand caregivers administering growth hormone. Expert Rev MedDevices .2015; 12(5):517-27.
46. Lass N, Reinehr T. Low treatment adherence in pubertal childrentreated with thyroxine and growth hormone. Horm Res Pediatr.2015;84:1-8.
47. Gabriel M, Gagnon JP, Bryan CK. Improved patients compliancethrough use of a daily drug reminder chart. Am J Public Health.1977; 67:968-9.
48. Giuffrida A, Torgerson DJ. Should we pay the patient? Review offinancial incentives to enhance patient compliance. BMJ. 1997;315:703-7.
49. U.S. Office of Inspector General. Medication regimens: causes ofnoncompliance. Report 1990 OEI-04-89-89121.
50. van Dongen N, Kaptein AA. Parents’ views on growth hormonetreatment for their children: psychosocial issues. Patient PreferAdherence. 2012; 6:547-53.
51. Laing P. Growth failure and hormone therapy. Brit J Nurs. 2014; 23(6Suppl):S3-S9.
Dichiarazione di conflitto d’interesse: “La pubblicazione di questo artico-lo ha ricevuto assistenza editoriale e redazionale da Airon Communications.r.l. e un supporto non condizionato da Novo Nordisk S.p.A”
10. Donovan JL. Patient decision making. The missing ingredient incompliance research. Int J Technol Assess Health Care. 1995;11:443-55.
11. Matsui DM. Drug compliance in pediatrics: clinical and researchissues. Pediatr Clin North Am. 1997; 44:1-14.
12. Main KM, Jorgensen JT, Hertel NT, et al. Automatic needle insertiondiminishes pain during GH injection. Acta Paediatr 1995; 84:331-4.
13. Haverkamp F, Johansson L, Dumas H, et al. Observations ofnonadherence to recombinant human growth hormone therapy inclinical practice. Clin Ther 2008; 30:307-16.
14. Allen DB. Growth hormone therapy for short stature: is the benefitworth the burden? Pediatrics 2006; 118:343-8.
15. Hunter I, DeVries C, Morris A, et al. Human growth hormone therapy:poor adherence equals poor growth. Arch Dis Child. 2000;82(Suppl.1):A8.
16. Kapoor RR, Burke SA, Sparrow SE, et al. Monitoring of concordancein growth hormone therapy. Arch Dis Child. 2008; 3:147-8.
17. Svarstad BL, Chewning BA, Sleath BL, Claesson C. The BriefMedication Questionnaire: a tool for screening patient adherenceand barriers to adherence. Patient Educ Couns 1999; 37:113-24.
18. Steiner JF, Prochazka AV. The assessment of refill compliance usingpharmacy records: methods, validity, and applications. J ClinEpidemiol 1997; 50:105-16.
19. Rickles NM, Svarstad BL. Relationships between multiple self-reported nonadherence measures and pharmacy records. ResSocial Adm Pharm 2007; 3:363-77.
20. Cutfield WS, Derraik JGB, Gunn AJ, et al. Non-compliance withgrowth hormone treatment in children is common and impairs lineargrowth. PLoS One 2011; 6:e16223,1-3.
21. Wilkins JP, Suman OE, Benjamin DA, Herndon DN. Comparison ofself-reported and monitored compliance of daily injection of humangrowth hormone in burned children. Burns 2003; 29:697-701.
22. Cutfield WS, Lundgren F. Insulin-like growth factor I and growthresponses during the first year of growth hormone treatment in KIGSpatients with idiopathic growth hormone deficiency, acquired growthhormone deficiency, Turner syndrome and born small for gestationalage. Horm Res. 2009; 71(Suppl.1):39-45.
23. Tillmann V, Patel L, Gill MS, et al. Monitoring serum insulin-likegrowth factor-I (IGF-I), IGF binding protein-3 (IGFBP-3), IGF-I/IGFBP-3molar ratio and leptin during growth hormone treatment fordisordered growth. Clin Endocrinol (Oxf) 2000; 53:329-36.
24. Bouhours-Nouet N, Gatelais F, Boux de Casson F, et al. The insulin-like growth factor-I response to growth hormone is increased inprepubertal children with obesity and tall stature. J Clin EndocrinolMetab. 2007; 92:629-35.
25. Fisher BG, Acerini CL. Understanding the Growth Hormone TherapyAdherence Paradigm: A Systematic Review. Horm Res Paediatr2013; 79:189-96.
26. Smith SL, Hindmarsh PC, Brook CG. Compliance with growthhormone treatment–are they getting it? Arch Dis Child. 1993; 68:91-3.
27. Stanhope R, Buchanan C, Butler G, et al. An open-label acceptabilitystudy of Norditropin SimpleXx - a new liquid growth hormoneformulation. J Pediatr Endocrinol Metab. 2001; 14:735-40.
28. Smith SL, Hindmarsh PC, Brook CG. Compliance with growthhormone treatment – are they getting it? Arch Dis Child. 1995; 73:277.
29. Rees L. Compliance with growth hormone therapy in chronic renalfailure and post transplant. Pediatr Nephrol. 1997; 11:752-4.
30. Oyarzabal M, Aliaga M, Chueca M, et al. Multicentre survey oncompliance with growth hormone therapy: what can be improved?Acta Paediatr. 1998; 87:387-91.
31. Postlethwaite RJ, Eminson DM, Reynolds JM, et al. Growth in renalfailure: a longitudinal study of emotional and behavioural changesduring trials of growth hormone treatment. Arch Dis Child. 1998;78:222-9.
32. Desrosiers P, O’Brien F, Blethen S. Patient outcomes in the GHMonitor: the effect of delivery device on compliance and growth.Pediatr Endocrinol Rev. 2005; 2:327-31.
33. Wickramasuriya BPN, Casey A, Akhtar S, et al. Factors determiningpatient choice of device for GH therapy. Horm Res. 2006; 65:18-22.
Corrispondenza:
Dr Fabio BuziS.C. Pediatria, A.S.S.T. Mantova – “C. Poma”Mail: [email protected]
Buzi sinistra_StesuraMAGAM 2 05/05/16 09:39 Pagina 18

Linear Growth and Nutritional Parameters in Adolescents
with Severe Atopic Dermatitis
SummaryIntroduction: Atopic dermatitis (AD) is a chronic inflammatory condition affecting local immunity and skin hydra-
tion. Severe AD may affect growth and weight gain in infants and children but its effects on growth and nutrition in adolescentsare not yet well known. Main objectives of study: To measure the effect of AD on linear growth and to evaluate some nutritional parameters in adole-scents with severe AD. Methods: We studied linear growth and body mass index (BMI) in 18 adolescents with severe AD (Scoring Atopic Dermatitis- SCORAD index > 41) seen at the Pediatric Allergy and Immunology Clinic of Hamad General Hospital of Doha (Qatar)between June 2014-2015 with severe AD. Anthropometric data was collected and serum total protein, albumin, 25OHD, zincand IgE concentrations were measured.Results: The height standard deviation score (Ht-SDS) was <-2 in 1/18 (5.5%) and < -1 in 27.8 % of them. Their BMI was 16.7± 3.6 Kg/m2. In 16.7 % of adolescents with AD the BMI < 14 Kg/m2 (BMI-SDS < -2). Hypoalbuminemia (serum albumin con-centration < 4 g/dl) and hypoproteinemia (serum total protein concentration < 64 g/dl) were found in 22.2% and 11.1 %, respec-tively. SCORAD was higher in adolescents with hypoalbuminemia and low BMI compared to those with normoalbuminemia andBMI (67.9 ±22.1 vs 58.3±22.5; p = 0.045). Vitamin D deficiency and zinc deficiency (< 9.95 µmol/L) were diagnosed in 31% ofpatients and 33.3% of patients, respectively. Anthropometric data (Ht-SDS, BMI) and nutritional parameters (serum albumin, zincand 25OHD concentrations) did not correlate significantly with the severity of the disease (SCORAD index).Conclusions: Adolescents with severe AD had high prevalence of hypoalbuminemia, zinc and vitamin D deficiency. Albuminloss may lead to malnutrition and low BMI in these patients. Therefore, it is mandatory to closely monitor linear growth and nutri-tional parameters in patients with severe AD, and to treat early any nutritional deficiency.
Key words: Atopic dermatitis, Adolescents, Growth, BMI, Zinc, Vitamin D.
Accrescimento e parametri nutrizionali in adolescenti con severa dermatite atopica
RiassuntoGli Autori hanno valutato gli effetti sulla crescita ed alcuni parametri nutrizionali in 18 giovani adolescenti (11.8 ±
1.7 anni) con dernatite atopica severa (Scoring Atopic Dermatitis - SCORAD index > 51). La statura espressa in SDS (Ht-SDS) èrisultata <-2 in 1/18 (5.5%) ragazzi and < -1 in 27.8 %. Nel 22.2% è stata diagnosticata una ipoalbuminemia ed in un terzo deipazienti un deficit di vitamina D e zinco. Pertanto, un’attenta valutazione dell'accrescimento e dello stato nutizionale è necessarionei soggetti con dermatite atopica allo scopo di diagnosticare e trattare precocemente il deficit nutrizionale.
Parole chiave: Dermatite atopica, Adolescenti, Accrescimento, BMI, Zinco, Vitamina D.
Mohammad Ehlayel 1,2, Ashraf Soliman 1,3, Vincenzo De Sanctis 4
1,2 Weill-Cornell Medical College and Section of Pediatric Allergy Immunology, Hamad Medical Corp, Doha, Qatar;1,3 Weill-Cornell Medical College and Section of Pediatric Endocrinology, Alexandria University, Egypt;
4 Pediatric and Adolescent Outpatient Clinic, Quisisana Hospital, Ferrara, Italy.
19
Introduction
Atopic dermatitis (AD) is an intensely itchy, chronic eczematousdisorder stemming from complex genetic and environmental fac-tors that contribute to an excessive immune response to allergenscoupled with epidermal barrier dysfunction (1). The terms ‘atopiceczema’ and ‘atopic dermatitis’ are synonymous. Research on AD
has focused mainly on infancy and early childhood, with few sur-veys in adolescents (1). According to recent data, recurrence rate is around 2.4%, andhigh persistence rates of disease symptoms are seen amongadolescents, especially those with positive personal or parental
Ehlayel_StesuraMAGAM 2 02/05/16 14:33 Pagina 19

20
atopic background, high socioeconomic status, and female gen-der, and high-risk occupations (2). Some infants and children withthe severe form of AD suffer from growth failure, hypoalbumine-mia, anemia and edema. In addition, delayed puberty and skeletalmaturation is described in older children and adolescents with AD.These manifestations are attributed in part to extensive loss ofprotein through the skin. The administration of steroids can result in rapid healing of theskin, conservation of albumin and correction of the anemia.However, the negative effect of steroids on linear growth stillposes a risk on the growing child (3-5). The effect of severe AD on growth and nutritional parameters inadolescents have not been fully studied before. We report ourexperience in 18 adolescents with severe AD.
Patients and Methods
We studied linear growth in all adolescents with severe AD whoattended for the first time to the Pediatric Allergy/ImmunologyClinic at Hamad Medical Center (HMC) in Doha (Qatar) during theperiod from June 2014 to June 2015. Their AD severity was mea-sured according to Scoring Atopic Dermatitis (SCORAD) score.We measured their weight, height, body mass index (BMI) andrecorded their height Z scores (Ht-SDS) using WHO growth charts.Their laboratory tests included complete and differential bloodcount (CBC), renal and hepatic functions, serum IgE, IgG, IgA,IgM, serum zinc (Zn) and vitamin D (25-OHD) concentrations.Exclusion criteria included those adolescents with chronic disea-se other than AD, such as: asthma, food intolerance, or allergicrhinitis and associated psychological problems which couldinfluence growth. The proposal of the study was approved by theEthics committee of HMC.
Results
Eighteen adolescents (8 males and 10 females) aged 11.8 ± 1.7years (Age range: 11- 16 years) with severe AD (SCORAD > 51)were studied. Patients had normal renal and hepatic functions.Anthropometric and laboratory data are presented in Table 1.
Rivista Italiana di Medicina dell’Adolescenza
Volume 14, n. 1, 2016
Linear Growth and Nutritional Parameters in Adolescents with Severe Atopic Dermatitis
Age BMI HtSDS Alb Protein 25OHD Total IgE AEC Hb Zinc yr Kg/m2 g/L g/L ng/ml kU/L cells/mcL g/dl µmol/L
Mean 10.3 16.7 -0.3 43.8 74.9 13.9 3713.2 876.0 12.9 8.7SD 2.1 3.6 1.1 4.5 6.2 6.6 8308.8 829.6 0.8 1.6
Table 1.Anthropometric and lab data of Adolescents with Severe AD.
Legend: BMI = body mass index; Alb = serum albumin; Protein = serum total protein ; AEC = Absolute eosinophilic count; 25OHD = 25 hydroxy vitamin D; Hb = hemoglobin; Zinc = serum zinc level.
The Ht-SDS was < -2 in 1/18 (5.5 %) and < -1 in 27.8 % of them.Their BMI was 16.7 ± 3.6 Kg/m2. In 16.7 % of adolescents theBMI < 14 Kg/m2 (BMI-SDS < -2). Hypoalbuminemia (serumalbumin concentration < 4 g/dl) and hypoproteinemia (serumtotal protein concentration < 64 g/dl) were found in 22.2% and11.1 %, respectively. Vitamin D deficiency (25-OH vitamin D < 20ng/ml) was found in 31% of the studied patients (4/13) and 25-OHD insufficiency (25-OH vitamin D between 2-20 ng/ml) wasfound in the remaining patients (9/13). Zinc deficiency (<9.95µmol/L) was diagnosed in 33.3% of patients. None of the patientshad anemia (hemoglobin concentration < 12 g/L).SCORAD was higher in adolescents with hypoalbuminemia andlow BMI compared to those with normoalbuminemia and BMI(67.9 ± 22.1 vs 58.3 ± 22.5; p = 0.045) but did not correlate withany of the auxological parameters (Ht-SDS and BMI) nor withalbumin, total protein and zinc concentrations.
Discussion
Atopic dermatitis (eczema) is amongst the most common disor-ders of the skin in young people around the world. "Atopic"means that there is typically a genetic tendency toward allergicdisease. AD is a chronic or recurrent inflammatory skin diseasethat usually begins in the first few years of life and is often the ini-tial indication that a child may later develop asthma and/or aller-gic rhinitis (hay fever). Acute eczema/dermatitis is characterisedby oedema, erythema, vesiculation, exudation and crusting.Microscopy shows collections of serum in the stratum corneum,moderate to marked spongiosis, intraepidermal vesiculation,moderate to marked sub-epidermal oedema in the papillary der-mis and lymphocytes in the upper dermis. Chronic eczema /der-matitis is characterised by lichenification (1, 2). Studies on thenatural history of atopic dermatitis document up to 60% sponta-neous clearing by puberty (1, 2). Cutaneous symptoms of nutri-tional disorders can be the result of poor nutrient intake/anorexia,zinc deficiency and nutritional deficiencies. The severity of der-matitis in individual cases can be measured and monitored inseveral ways. We used the SCORAD index to classify the AD assevere. In our adolescents, the BMI was low and Ht-SDS wasbelow -1 and -2 in 27.8 % and 5.5 %, respectively.
Ehlayel_StesuraMAGAM 2 02/05/16 14:34 Pagina 20

microbial peptide activity, and promote the integrity of the per-meability barrier, correction of VDD and supplementation can pro-vide a possible therapeutic intervention in this disease.Some data suggest that vitamin D deficiency may be related tothe severity of AD and advocate the need for studies evaluatingthe use of vitamin D as a potential treatment in patients with thisdisease. A double-blind randomized controlled trial utilized aregimen of 1,000 IU/day of vitamin D for one month during thewinter in children with winter-related AD (5 subjects received sup-plementation versus placebo in 6 subjects). Baseline changes inglobal assessments of skin showed that the vitamin D treatmentgroup had a significant improvement in baseline score compa-red to placebo (21-23).In conclusion, severe AD in adolescents may adversely affecttheir linear growth and weight gain through different mechani-sms. Loss of albumin through the inflamed skin, low zinc andvitamin D status must be compensated by proper medical treat-ment of inflammatory cutaneous condition and by appropriatenutritional support. The judicious use of steroids and other drugs to inhibit severeinflammation and decrease inflammatory mediators may impro-ve growth in these patients.
Unfortunately, the difference in patients' standing height versusmidparental scores were not available. We recommend serialgrowth measurements in all children and adolescents with seve-re AD in order to detect early changes on growth pattern.These patients had a high prevalence of hypoalbuminemia andhypoproteinemia (22.2 % and 11.1 %, respectively) due to loss ofalbumin and globulins through the diseased skin. Albumin lossmay lead to malnutrition and explain in part their low BMI. In sup-port to our findings, Baum et al. reported high prevalence ofdelayed growth and skeletal maturation in children with AD (6).Furthermore, hypoproteinemia can be a life-threatening conditionowing to hypovolemic shock as a result of hypoproteinemia andvascular infarction as a result of thrombocythemia (7).One third of our patients had high prevalence of Zn deficiencywhich may contribute to their impairment of growth. Zinc is theintrinsic metal component or activating cofactor for more than 70important enzyme systems, including carbonic anhydrase, alka-line phosphatases, dehydrogenases and carboxypeptidases.It is involved in the regulation of nucleoproteins and the activity ofvarious inflammatory cells and plays a role in growth, tissuerepair and wound healing, carbohydrate tolerance and synthesisof testicular hormones. Therefore, in patients with severe AD, Zn deficiency may negati-vely affect linear growth and pubertal development and deterio-rates and increases the risk and severity of their skin inflamma-tion and infection (8-11).Linear bone growth is adversely affected in children with chronicinflammatory disorders. Atopic dermatitis is one of the chronicinflammatory conditions which is associated with the release ofmany inflammatory cytokines in the circulation. In the chronicphase of AD activation of Th-1 lymphocytes which producemainly IFN-γ, TNF-α, IL-8 and IL-12. These cytokines can impairthe GH-IGF-I axis at several levels. First, cytokines, in particular IL-1β, have been shown to decreaseGH secretion in vivo. Second, infusion of IL-1β and TNF-α indu-ces profound anorexia susceptible to decrease circulating IGF-I.Third, IL-1β and TNF-α, can stimulate secretion of stress hormo-nes as glucocorticoids and these hormones can, in turn, inducea state of GH resistance. In addition, a direct effect of cytokineson hepatocyte IGF-I gene expression has been suggested.However, the role of high inflammatory cytokines and mediatorson growth, in such children has not been studied so far (12-20).Treatment with steroids, which inhibits inflammation and releaseof these markers, results in dramatic improvement of dermatitisand rapid correction of hypoalbuminaemia, oedema and anae-mia in severe AD (12-20). In order to verify these assumptions itis necessary to research the interaction of these inflammatorymarkers on linear growth, growth factors and skeleton in childrenand adolescents suffering from atopic disorders (Figure 1).This study showed high prevalence of vitamin D deficiency and/orinsufficiency in adolescent patients with AD. Given the potentialfor vitamin D to suppress inflammatory responses, enhance anti-
Rivista Italiana di Medicina dell’Adolescenza
Volume 14, n. 1, 2016
21
Linear Growth and Nutritional Parameters in Adolescents with Severe Atopic Dermatitis
Figure 1.Possible mechanisms of delayed growth in patients with atopic dermatitis.
Ehlayel_StesuraMAGAM 2 02/05/16 14:34 Pagina 21

22
References
1. Simpson EL, Hanifin JM. Atopic dermatitis. Med Clin N Am. 2006;90:149-67.
2. Peters AS, Kellberger J, Vogelberg C, et al. Prediction of theincidence, recurrence, and persistence of atopic dermatitis inadolescence: a prospective cohort study. J Allergy Clin Immunol.2010; 126:590-5.
3. Ferguson AC, Murray AB, Tze WJ. Short stature and delayed skeletalmaturation in children with allergic disease. J Allergy Clin Immunol.1982; 69:461-6.
4. Abrahamov A, Schifmann R, Goldstein R, et al. Growth failure due toprotein loss in dermatitis. Eur J Pediatr. 1986; 145:223-6.
5. Baum WF1, Schneyer U, Lantzsch AM, et al. Delay of growth anddevelopment in children with bronchial asthma, atopic dermatitis andallergic rhinitis. Exp Clin Endocrinol Diabetes. 2002; 110:53-9.
6. Nomura I, Katsunuma T, Tomikawa M, et al. Hypoproteinemia insevere childhood atopic dermatitis: a serious complication. PediatrAllergy Immunol. 2002; 13:287-94.
7. Gibson RS. Assessment of trace-elements. In: Gibson RS. Principlesof nutritional assessment. Oxford, United Kingdom: Oxford UniversityPress, 1990; 511-76.
8. Shankar AH, Prasad AS. Zinc and immune function: the biologicalbasis of altered resistance to infection. Am J Clin Nutr. 1998; 68(Suppl 2):447S-63S.
9. Prasad AS. Zinc and immunity. Mol Cell Biochem. 1998; 188:63-9.
10. Osama S, AbuNada, Marwan O, et al. Nutritional assessment of zincamong adolescents in the Gaza Strip-Palestine. Open J Epidemiol.2013; 3:105-10.
11. Tintle S, Shemer A, Suárez-Fariñas M, et al. Reversal of atopicdermatitis with narrow-band UVB phototherapy and biomarkers fortherapeutic response. J Allergy Clin Immunol. 2011; 128:583-93.
12. Hayashida S, Uchi H, Moroi Y, et al. Decrease in circulating Th17cells correlates with increased levels of CCL17, IgE and eosinophilsin atopic dermatitis. J Dermatol Sci. 2011; 61:180-6.
13. Jahnz-Rozyk K, Targowski T, Paluchowska E, et al. Serum thymusand activation-regulated chemokine, macrophage-derivedchemokine and eotaxin as markers of severity of atopic dermatitis.Allergy.2005; 60:685-8.
14. Raap U, Wichmann K, Bruder M, et al. Correlation of IL-31 serumlevels with severity of atopic dermatitis. J Allergy Clin Immunol. 2008;122:421-3.
15. Raap U, Weißmantel S, Gehring M, et al. IL-31 significantly correlateswith disease activity and Th2 cytokine levels in children with atopicdermatitis. Pediatr Allergy Immunol. 2012; 23:285-8.
16. Brandt EB, Sivaprasad U. Th2 Cytokines and Atopic Dermatitis. JClin Cell Immunol. 2011; 2(3). pii: 110.
17. Leung DY, Bieber T. Atopic dermatitis. Lancet. 2003; 361:151-60.
18. Farquharson C, Ahmed SF. Inflammation and linear bone growth:the inhibitory role of SOCS2 on GH/IGF-1 signaling. Pediatr Nephrol.2013; 28:547-56.
19. Ferguson AC, Murray AB, Tze WJ. Short stature and delayed skeletalmaturation in children with allergic disease. J Allergy Clin Immunol.1982; 69:461-6.
20. Thissen JP, J Verniers J. Inhibition by Interleukin-1� and TumorNecrosis Factor -� of the Insulin - Like Growth Factor I MessengerRibonucleic Acid Response to Growth Hormone in Rat Hepatocyte.Endocrinology, 1997; 138,3:1078-84.
21. Searing DA, Leung DY. Vitamin D in Atopic Dermatitis, Asthma andAllergic Diseases. Immunol Allergy Clin North Am. 2010; 30:397-409.
22. Peroni DG, Piacentini GL, Cametti E. Correlation between serum 25-hydroxyvitamin D levels and severity of atopic dermatitis in children.Br J Dermatol. 2011; 164,5:1078-82.
23. Sidbury R, Sullivan AF, Thadhani RI, et al. Randomized controlledtrial of vitamin D supplementation for winter-related atopic dermatitisin Boston: a pilot study. Br J Dermatol. 2008; 159:245-7.
Rivista Italiana di Medicina dell’Adolescenza
Volume 14, n. 1, 2016
Linear Growth and Nutritional Parameters in Adolescents with Severe Atopic Dermatitis
Correspondence:
Ashraf T Soliman MD PhD FRCPProfessor of Pediatrics and EndocrinologyHamad Medical Centre, Doha, QatarMail: [email protected]
Ehlayel_StesuraMAGAM 2 02/05/16 14:34 Pagina 22

23
I limiti dell’autonomia prescrittiva: il quesito
Per fare un esempio, traendolo dalla medicina dello sport, si puòpensare alla formula di Karvonen: essa è utilizzata per misurare ilparametro di intensità nell'esercizio cardiovascolare e per pianifi-care l'allenamento sportivo sulla base della frequenza cardiaca(ritmo cardiaco). Perché? Perché essa costituisce – a differenza dialtre formule approssimative - il metodo più accurato per misura-re la percentuale della frequenza cardiaca massima individuale,perché nello stabilirne i valori tiene conto di parametri soggettivi.Ed il punto del quesito oggetto della presente indagine è tutto qui,ovvero nell’individuazione della cura. Se è vero che il SistemaSanitario Nazionale ha subito varie modifiche che hanno visto ilpassaggio e la trasformazione da un sistema fondato sulla visio-ne universalistica ed egualitaria all’emersione dei c.d. livelli essen-ziali di assistenza e all’emergere della necessità di ripianamentodei disavanzi, non si può prescindere dai principi fondamentalidel nostro ordinamento, che sono impressi dalla Carta costituzio-nale e dal ricordare che il concetto di appropriatezza terapeuticarisulta già puntualmente disciplinato dalla legge dello Stato: al centro di tale contesto normativo rimane certamente l’individuo.Così per tornare all’approccio iniziale, ogni paziente è diverso,per così dire, ha una frequenza cardiaca differente, con la con-seguenza che l’allenamento (ovvero la terapia) più appropriatonon potrà essere un generico percorso sul tapirulan, eguale pertutti, ma dovrà consistere in un training personalizzato, individua-to dal medico curante. Tali considerazioni, peraltro non prescin-dono dal dato economico, in quanto, sia il concetto di appro-priatezza terapeutica, ne contiene in sé il significato, sia – in effetti – la terapia ‘migliore’ o meglio più appropriata, sarà perl’appunto anche quella in grado di avere efficacia nel minortempo possibile, di ridurre il tempo di ricovero ospedaliero, diridurre al massimo gli sprechi con indubbie ripercussioni positi-ve anche sul contenimento della spesa sanitaria globale.
Conclusioni
Quale autonomia prescrittiva? Non può essere che “Tutta”, ovve-ro tutta quella necessaria a consentire la scelta del farmaco più
La terapia ‘appropriata’…un personal trainer o un tapis roulant?
Il tema dell’autonomia prescrittiva è strettamente connesso all’e-satta individuazione del concetto di appropriatezza terapeutica.È di questi mesi il vivace dibattito sul nuovo decreto che dovreb-be garantire ‘l'appropriatezza’ delle prestazioni sanitarie, in un’ot-tica di razionalizzazione e contenimento della spesa, per ottene-re risparmi nel settore, anche attraverso lo stop ad esami e visiteinutili, ovvero "inappropriate". Per tali esami, infatti, è stato stima-to un costo ogni anno di circa 13 mld per il Servizio SanitarioNazionale. Peraltro, le Regioni saranno chiamate a garantireun'applicazione omogenea dei nuovi criteri di appropriatezza sututto il territorio.Non può sfuggire come si tratti di un tema molto complesso, incui ogni approccio non può che seguire un metodo sistemico,integrato da aspetti etici, economici 1 e giuridici, tenendo in con-siderazione esigenze diverse:
la necessità di garantire a tutti le cure, contenendo gli spre-chi e l’imprescindibile libertà del medico di scegliere la curapiù adeguata al singolo paziente, i principi di libera concorrenza,la specificità dei farmaci biotecnologici.
In tale contesto, la problematica dell’autonomia prescrittiva èquestione che attiene alla prescrizione dei farmaci biotecnologi-ci, quanto alle indagini diagnostiche, e per affrontarla non puòche sottolinearsi che il centro di ogni discorso non può che esse-re e deve rimanere l’uomo. Ed, in quest’ottica, anche la letturadell’art. 32 della Costituzione, deve avvenire alla luce degli altridiritti e doveri scolpiti nella Carta costituzionale, quali l’obbligo diadempiere ai doveri di solidarietà, quello di rispettare la dignitàdella persona, di assicurare il pari trattamento a tutti gli individui,e soprattutto, il fondamentale obbligo di rispettare la libertà indi-viduale che si esplica anche nell’inviolabile diritto di scelta dellacura da intraprendere.Da tale affermazione ne discendono necessariamente altre due:
da un lato, il medico, nella sua scienza e coscienza, dovràsentirsi libero di prescrivere al paziente le cure che egli riten-ga maggiormente idonee a raggiungere un beneficio;dall’altro, le procedure di acquisizione dei farmaci dovrannoconsentire una approvvigionamento adeguato alle indicazio-ni ‘date’ e ‘rilevate’ dai medici curanti.
Solveig CoglianiMagistrato del TAR - Lazio.
Cogliani FrontLine_Tanas_figli_Dieting 28/04/16 11:51 Pagina 23

24
Rivista Italiana di Medicina dell’Adolescenza
Volume 14, n. 1, 2016
La terapia ‘appropriata’…un personal trainer o un tapis roulant?
appropriato alla luce del concetto di appropriatezza terapeutica(di cui all’Accordo collettivo nazionale reso esecutivo dal d.P.R. n.270 del 2000, ed alla luce delle responsabilità già previste dal-l’ordinamento, cfr. il d.l. n. 323 del 1996, come conv. In l. n. 425del 1996) e del principio di autonomia prescrittiva nella scelta delpresidio diagnostico-terapeutico da applicare di cui all’art. 12 delcodice deontologico.Per prescrizione appropriata si intende, infatti: quella che risultitale da garantire (per quantità, qualità e modalità di sommini-strazione della cura) – un miglioramento delle condizioni delpaziente, sicché da essa è già espulso ogni comportamento pre-scrittivo che induca il paziente ad un consumo di farmaci incon-gruo o inadeguato. Afferma il richiamato Accordo che è oneredel medico “lo sviluppo e la diffusione del corretto uso del farma-co nell’ambito della quotidiana attività assistenziale”.In tale contesto, dunque, l’efficacia dell’intervento, che concretail concetto di appropriatezza, consiste nel comportamento delmedico che deve sempre finalizzare la prescrizione al fine di otti-mizzare il rapporto mezzi (farmaci-indagini) al risultato ovvero almiglioramento della salute del paziente in modo da raggiungereil massimo risultato con il minimo impiego di principio attivo.La funzione del medico prescrittore è già dunque, secondo la nor-mativa vigente, quella di rendere possibile l’assunzione di unonere a carico dell’amministrazione sanitaria, essa è necessaria-mente connessa al concetto di ‘appropriatezza terapeutica’, comeprecisato, in quanto il medico nell’adempiere al proprio compito:
è tenuto ad assicurare “l’appropriatezza nell’utilizzo dellerisorse messe a disposizione dalla Azienda per l’erogazionedei livelli essenziali ed appropriata assistenza”,
ricerca “la sistematica riduzione degli sprechi nell’uso dellerisorse disponibili mediante adozione di principi di qualità e dimedicina basata sulle evidenze scientifiche”,
effettua le sue prescrizioni, secondo “scienza e coscienza”.
Il medico è sì coinvolto, dunque, negli aspetti gestionali, essen-do tenuto ad un corretto uso del farmaco, ma la scelta terapeu-tica rientra nella sua esclusiva sfera volitiva e, dunque, nella suaesclusiva responsabilità innanzitutto etica e deontologica.Non si tratta di un’illimitata discrezionalità del medico, perché lagiurisprudenza ha evidenziato che il medico ha l’obbligo di atte-nersi ai criteri dettati in sede nazionale e che il suo comporta-mento può essere sindacato in relazione alle scelte compiutedalla generalità degli altri medici, salvo comunque la possibilitàper il medico prescrittore di poter provare la particolarità dellapatologia trattata.
Nota
Sul punto, con specifico riferimento alle procedure di evidenzapubblica per le forniture, non possono che assumere rilievo leindicazioni contenute nella nuova direttiva appalti 24/2014/UEriguardo al concetto di economicamente vantaggioso, laddove ilconsiderando n. 90 rivaluta come criterio di selezione delle offer-te quello della “qualità”.
Corrispondenza:
Solveig CoglianiMagistrato del TAR LazioE-mail: [email protected]: 3207983834
Cogliani FrontLine_Tanas_figli_Dieting 28/04/16 11:51 Pagina 24

25
mended in case regular transfusions become a persistent require-ment when serum ferritin levels exceed 1,000 ng/ml (1, 2, 6).We report a 14 years old girl who developed myxedema coma, arare life-threatening condition, that has not been reported before inpatients with AA and iron overload.
Case history
A 14 year-old girl was admitted last November to the Departmentof Pediatrics for weakness, altered mental status and abdominalpain of one-day duration. A diagnosis of non severe (moderate)aplastic anemia (NSAA) was made at the age of 4 years and since
Introduction
Aplastic anemia (AA) is a rare disorder characterized by hypocel-lular bone marrow in the absence of an abnormal infiltrate resultingin progressive pancytopenia. The incidence is 2-3/million inhabi-tants/year, in Europe, but higher in East Asia. Acquired aplasticanemia may develop at any age. The age distribution of the disea-se shows two peaks, one between 10 and 25 years, and a secondamong the over 60 year-olds. There is no sex predilection (1, 2).The severity of the disease is graded according to the blood countparameters and bone marrow findings (Table 1). Survival in severeaplastic anemia (SAA) has markedly improved in the past 2 deca-des because of advances in hematopoietic stem cell transplanta-tion, immunosuppressive and biologic drugs, and supportive carewith red cell (leukocyte-depleted blood products) and platelet tran-sfusions (4-8). Immunosuppressive therapy, including cyclosporinand antithymocyte globulin, is used in patients for whom bonemarrow transplantation is not an option, with response rates of60–80% (6-8). However, supportive care with red blood cell tran-sfusions is also essential in many patients. Iron overload can, the-refore, become a significant problem in regularly transfusedpatients, leading to organ damage, particularly in the liver, endo-crine glands and heart (1, 2, 6). Iron chelation therapy is recom-
Myxoedema coma: A report in an adolescent
with aplastic anemia and iron overload
SummaryWe report a 14 year old girl who developed myxedema
coma, a rare life-threatening condition that has not been reportedbefore in patients with aplastic anemia and iron overload. Treatmentconsisted of L-thyroxine, supportive measures and appropriate mana-gement of infection. In addition, the patient was treated with gluco-corticoids in stress doses. After 17 days of hospitalization she wasdischarged in stable condition on L-thyroxine (75 µg daily) and inten-sive iron chelation therapy. After 35 days, the FT4 and TSH levels werein the normal range.
Key words: Myxedema coma, Aplastic anemia, Iron overload,Treatment.
Coma mixedematoso in una adolescente con anemiaaplastica ed emosiderosi
Riassunto Viene descritto un caso clinico di coma mixedemato-
so in una ragazza di 14 anni in terapia trasfusionale e chelante dal-l’età di 4 anni. Gli autori descrivono gli aspetti diagnostici e terapeu-tici ed il decorso clinico. La ragazza è stata dimessa dopo 17 giornidi ricovero ospedaliero in condizioni stabili ed in trattamento con L-tiroxina e terapia chelante intensiva. La funzionalità tiroidea è rien-trata nella normalità dopo 35 giorni.
Parole chiave: Coma mixedematoso, Anemia aplastica,Emosiderosi, Terapia.
Vincenzo De Sanctis 1, Ashraf T. Soliman 2, Heba Elsedfy 3,Nada A. Soliman 4, Rania Elalaily 5, Ihab Zaki Elhakim 2
1 Pediatric and Adolescent Outpatient Clinic, Quisisana Hospital, Ferrara, Italy; 2 Department of Pediatrics, Division of Endocrinology,
Alexandria University Children's Hospital, Alexandria, Egypt; 3 Department of Pediatrics, Ain Shams University, Cairo, Egypt;
4 Ministry of Health, Alexandria, Egypt; 5 Department of Primary Health Care (PHC), Doha, Qatar.
Case ReportCase Report
Severe aplastic anemia (SAA) Very severe aplastic anemia (VSAA) Non severe (moderate) aplastic anemia (NSAA)
•Bone marrow cellularity < 25% Same as SAA with absolute neutrophil •Bone marrow •Two of three peripheral blood criteria: count (ANC) < 200/µL cellularity < 25%
- Absolute neutrophil count (ANC) < 500/µL •Peripheral blood - Platelet count < 20,000/µL cytopenias do not- Corrected reticulocyte count <1% fulfil criteria for SAA
Table 1.Classification of aplastic anemia based on severity of pancytopenia (from Ref. 1 and 8; modified).
De Sanctis_CASE REPORT_Dati ok 05/05/16 09:47 Pagina 25

26
Rivista Italiana di Medicina dell’Adolescenza
Volume 14, n. 1, 2016
Myxoedema coma: A report in an adolescent with aplastic anemia and iron overload
than she received regular scheduled blood transfusions and che-lation therapy with deferioxamine (40 mg/kg of body weight).On examination she was pale, hypothermic (temperature 34.5 °C)and bradycardic (48 beats/min) with fine crackles at base of leftlung, pretibial edema, delayed relaxation phase of the Achillestendon. Abdomen was soft with hepatomegaly and no masses.Pupils were equally round and reactive to light. Fundoscopicexam was normal. Tympanic membranes were clear. Oropharynx was clear. There was no goiter or surgical scar of thy-roidectomy. She was short with no signs of pubertal development(Tanner stage breast 1 and pubic hair 1). The blood pressure was90/60 mmHg. The peripheries were very cold to touch, with acapillary refill of more than 4 seconds. The Glasgow Coma Scale(GCS) score in conjunction with designed diagnostic scoringsystem for myxedema coma followed by the Indiana UniversitySchool of Medicine, Indianapolis was 9 (a score ≥ 7 is conside-red to be highly suggestive/diagnostic of myxedema coma)(Tabele 2) (9). One year before hospital admission her TSH valuewas 6.7 mU/L (normal: 0.5-4.0 mU/L). TSH and free T4 wereordered. Further testing included a chest radiograph that showedmild cardiomegaly and left lower lobe pneumonia. Urine, throatand blood cultures were also obtained. Sinus bradycardia, lowvoltage complexes, prolongation of the QT interval and nonspe-cific ST-T changes in electrocardiogram were recorded. An echo-cardiogram documented normal left ventricular ejection fractionwith the presence of mild pericardial effusion. Additionally, com-plete blood count, serum electrolytes, glucose, cardiac enzymes,C-reactive protein, and liver function tests were ordered. Clinical,biochemical and hormonal profiles are reported in Table 3.
Arterial blood gas testing revealed hypercapnia (PaCO2 48 mm Hg)and a pH of 7.35. Serum ferritin level was high (2570 ng/ml; nor-mal values: < 250 ng/ml). The hypothermia was treated withpassive rewarming using ordinary blankets and a warm room.Broad-spectrum of antibiotics and hydrocortisone IV were star-ted. Given the lack of imminent life threatening conditions, thepatients was treated with L-thyroxine (initial dose 4 µg/kg/ bodyweight) through a nasogastric tube followed by 100 µg dailyorally. Thyroid function was checked frequently (every 3 days).Hyponatremia and hypoglycemia were corrected with salineand free water restriction, and intravenous dextrose. The patient’s body temperature progressively increased to 36°C over a period of about 36 hours. Over the next 4 days thebiochemical parameters returned to normal values and after 17days of hospitalization she was discharged in stable conditionon L-thyroxine (75 µg daily) and intensive iron chelation therapy.After 35 days, the FT4 and TSH levels were in the normalrange. Thyroid ultrasound showed reduced volume of glandand inhomogeneity of the parenchyma.
Discussion
Myxedema coma is a syndrome that results from the intensereduction of the thyroid hormone synthesis. Patients rarely pre-sent with coma, thus a more accurate term may be myxedemacrisis. It is characterized by an altered mental status, defectivethermoregulation, and other symptoms related to slowing offunction in multiple organs. Therefore, the diagnosis should beconsidered in any patient with coma or depressed mental statuswho also has hypothermia, hyponatremia, and/or hypercapnia.Myxedema coma is difficult to distinguish from sepsis, and sinceinfection is often the precipitating event in a patient with preexistinghypothyroidism, generally the patients must receive empiric anti-biotics until sepsis is ruled out (10, 11). In our patient the physicalexamination findings combined with clinical history strongly sug-gested a myxedema crisis. The following illnesses were includedin the differential diagnosis: sepsis, myxedema coma, toxic inge-stion and Addisonian crisis. The results of FT4 and TSH confirmedthe diagnosis. Treatment consisted of L-thyroxine, supportive mea-sures and appropriate management of infection. In addition, thepatient was treated with glucocorticoids in stress doses (Table 4).The ideal mode of therapy and doses of thyroid hormone therapyin myxedema coma remain controversial due to the rarity of thecondition and lack of clinical trials. Three different regimens have been suggested (12):1. intravenous or oral T4,2. intravenous T3 or3. a combination of T4 and T3. Giving T4 intravenously has been
advocated because absorption via the oral route is variableand unpredictable (13). However, one study showed that theclinical response obtained by oral T4 occurred promptly evenin a case of myxoedema ileus (14).
GCS 0-10 = 4 points11-13 = 3 points14 = 2 points,5 = 0 points
TSH > 30 = 2 points15-30 = 1 point
T4 below normal 1 point
Hypothermia (temperature < 96 F) 1 point
Bradycardic (HR < 60) 1 point
Precipitating illness present 1 point
Scoring Myxedema coma ≥ 7likely = 5-7unlikely < 5
Table 2.Diagnostic criteria for myxedema coma (Six criteria and points assigned).
From: Chiong and Mariash et al.: Development of an objective tool forthe diagnosis of myxoedema coma. Endocrinology Review. Indianapolis:Indiana University School of Medicine; 2011. p. 24‑6; GCS – Glasgowcoma scale, TSH – Thyroid‑stimulating hormone, HR – Heart rate
De Sanctis_CASE REPORT_Dati ok 05/05/16 09:47 Pagina 26

27
Myxoedema coma: A report in an adolescent with aplastic anemia and iron overload Rivista Italiana di Medicina dell’Adolescenza
Volume 14, n. 1, 2016
The American Thyroid Association recommends combination the-rapy with T4 and T3 (15). T4 given IV has a long half-life, so it canbe administered once-daily. Liothyronine (T3) has a short half-lifeand must be administered every 8 hours. Because of concernsabout abrupt onset and fluctuating concentrations in tissues,coadministration of T3 with T4 is recommended. Furthermore, therate of conversion of T4 to the active hormone T3 can be reducedin these patients.T3 has a quicker onset of action than T4, asincreases in body temperature and oxygen consumption has beenreported to be faster with T3 therapy compared to T4. T3 therapyis given in adults as bolus of 5-20 µg intravenously and to be con-
tinued at a dosage of 2.5-10 µg every8 hours depending on the patient'sage and coexistent cardiac risk fac-tors (16, 17). Our patient, due to lackof imminent life threatening condi-tions and because of severe hemosi-derosis was treated with L-thyroxine(initial dose 4 µg/kg/body weight)through a nasogastric tube followedby 100 µg daily orally. She graduallyimproved and after 17 days of hospi-talization was discharged in stablecondition on L-thyroxine (75 µg daily)and intensive iron chelation therapy. The prognosis for patients withmyxedema coma is difficult to definebecause of the small number ofcases reported in the literature. One study reported a mortality rate ofabout 30 percent, while another sug-gests the mortality rate may be ashigh as 60 percent. Factors associa-ted with a poor prognosis includeadvanced age, bradycardia and per-sistent hypothermia (18, 19). Interestingly, Dutta et al. recentlyreported from their series of 23 con-secutive patients with myxedemacoma that L-thyroxine treatmentdefaulters had more severe manife-stations compared with de novosubjects. Moreover, these authorsidentified various predictors of mor-tality including hypotension, brady-cardia at presentation, need formechanical ventilation, hypothermiaunresponsive to treatment, sepsis,intake of sedative drugs, lowerGlasgow Coma Score (GCS), highAPACHE II score and high SequentialOrgan Failure Assessment (SOFA)
score. The latter SOFA score had the best predicted value (20).In conclusion, a high index of suspicions is needed among clini-cians in order to rapidly recognize this condition for making anearly diagnosis. Treatment should be commenced on clinicalgrounds while waiting for laboratory results. It is also vital thatthese patients receive intensive care level treatment with closemonitoring of their cardiovascular parameters and level of con-sciousness. It is also essential to check periodically the endocrinefunction of these patients to identify and treat the condition preci-pitating the coma. Follow-up care after discharge is necessary toensure adherence with thyroid hormone replacement.
Clinical and laboratory findings Results
Age 14.2 years
Sex Female
Clinical findingsHeight: cm (percentile) 143 - < 3rd centileWeight: kg (percentile) 39 - < 1st centileTanner stage (Breast-Pubic hair) 1 - 1Body temperature (°C and °F) 34.5 (93.9)Blood pressure (mmHg) 95/60Glasgow Coma Score 9/15Myxoedema Coma Score* 9Heart rate (beats/min) 48Respiratory rate (breaths/min) 10Pulse oximetry on ambient air 95%
Etiology of myxedema Hemosiderosis and infection
Hormonal assayFT3 (normal:2.6–7.0 pmol/L) 2.0FT4 (normal: 10-22 pmol/L) <5.9TSH (normal: 0.5-4.0 mU/L) 57.7PRL (normal: 5-20 ng/mL) 8.8Thyroglobulin antibodies (normal:< 4 IU/mL) < 4Thyroid peroxidase antibodies (normal:<9 IU/mL) < 9Cortisol level (normal:5-25 µg/dL) 12.5 µg/dL
CultureThroat NegativeBlood NegativeUrine Negative
Chest X-ray Pneumonia
Laboratory findingsHemoglobin (normal: 11.3-14.1 gm/dL) 7.6White blood cells (5-13 x 109/L) 3.330Serum glucose (normal: 65-99 mg/dL) 94Serum creatinine (normal 0.3 - 1.1 mg/dL) 1.2Calcium ( normal: 8.4-10.2 mg/dL) 8.8Sodium (normal: 135-146 mmol/L) 128Potassium (normal: 3.4- 4.4 mmol/L) 4.5C-Reactive Protein Test (normal: 0-10 mg/dL) 13.6Creatine kinase MB (normal: < 7.6 µg/L) 5Alanine transaminase [ALT] (normal: ≤ 40 U/L) 62
Specific myxedema measuresIntravenous glucose +Hyponatremia correction +Oral thyroxine +Hydrocortisone +
Duration of hospital stay 17 days
Table 3.Clinical, laboratory findings and management of myxedema crisis in our patient.
De Sanctis_CASE REPORT_Dati ok 05/05/16 09:47 Pagina 27

28
References
1. Davies JK, Guinan EC. An update on the management of severeidiopathic aplastic anemia in children. Br J Haem. 2007; 136:549-64.
2. Miano M, Dufour C. The diagnosis and treatment of aplastic anemia:a review. Int J Hematol. 2015; 101:527-35.
3. Niemeyer C, Baumann I. Classification of Childhood Aplastic Anemiaand Myelodysplastic Syndrome. Hematology Am Soc Hematol EducProgram. 2011; 2011:84-9.
4. Barone A, Lucarelli A, Onofrillo D, et al. Diagnosis and managementof acquired aplastic anemia in childhood. Guidelines from theMarrow Failure Study Group of the Pediatric Haemato-OncologyItalian Association (AIEOP). Blood Cells Mol Dis. 2015; 55:40-7.
5. Schrezenmeier H and Bacigalupo A (Eds.): Aplastic Anemia -Pathophysiology and Treatment. Cambridge University Press 2000.
6. Bacigalupo A, Passweg J. Diagnosis and treatment of acquiredaplastic anemia. Hematol Oncol Clin North Am. 2009; 23:159-70.
7. Passweg J, Marsh JC. Aplastic anemia: first-line treatment byimmunosuppression and sibling marrow transplantation. HematologyAm Soc Hematol Educ Program.2010: 2010;36-42.
8. Scheinberg P, Wu CO, Nunez O, Young NS. Long-term outcome ofpediatric patients with severe aplastic anemia treated withantithymocyte globulin and cyclosporine. J Pediatr. 2008; 153:814-9.
9. Chiong YV, Bammerlin E, Mariash CN. Development of an objectivetool for the diagnosis of myxedema coma. Transl Res. 2015;166:233-43.
10. Kwaku MP, Burman KD. Myxedema coma. J Intensive Care Med.2007; 22:224-31.
11. Klubo-Gwiezdzinska J, Wartofsky L. Thyroid emergencies. Med ClinNorth Am. 2012; 96:385-403.
12. Beynon J, Akhtar S, Kearney T. Predictors of outcome in myxoedemacoma. Crit Care. 2008; 12:111.
13. Holvey DN, Goodner CJ, Nicoloff JT, Dowling JT. Treatment of
Myxedema Coma with Intravenous Thyroxine. Arch Intern Med. 1964;113:89-96.
14. Arlot S, Debussche X, Lalau JD, Mesmacque A, Tolani M, QuichaudJ, Fournier A. Myxoedema coma: response of thyroid hormones withoral and intravenous high-dose L-thyroxine treatment. Intensive CareMed. 1991; 17:16-8.
15. Jonklaas J, Bianco AC, Bauer AJ, Burman KD, Cappola AR, Celi FS,et al. Guidelines for the treatment of hypothyroidism: prepared by theamerican thyroid association task force on thyroid hormonereplacement.Thyroid. 2014; 24:1670-751.
16. MacKerrow SD, Osborn LA, Levy H, et al. Myxedema-associatedcardiogenic shock treated with intravenous triiodothyronine. AnnIntern Med. 1992; 117:1014-5.
17. Arlot S, Debussche X, Lalau JD, et al. Myxoedema coma: responseof thyroid hormones with oral and intravenous high-dose L-thyroxinetreatment. Intensive Care Med. 1991; 17:16-8.
18. Mathew V, Misgar RA, Ghosh S, et al. Myxedema coma: a new look intoan old crisis. J Thyroid Res. 2011; 2011:493462. Epub 2011 Sep 15.
19. Rodriguez I, Fluiters E, Perez-Mendez LF, et al. Factors associatedwith mortality of patients with myxoedema coma: prospective studyin 11 cases treated in a single institution. J Endocrinol. 2004;180:347-50.
20. Dutta P1, Bhansali A, Masoodi SR, et al. Predictors of outcome inmyxoedema coma: a study from a tertiary care centre. Crit Care.2008; 12: R1. Epub 2008 Jan 3.
Rivista Italiana di Medicina dell’Adolescenza
Volume 14, n. 1, 2016
Myxoedema coma: A report in an adolescent with aplastic anemia and iron overload
Corrispondenza:
Vincenzo de Sanctis, MDPediatric and Adolescent Outpatient Clinic, Quisisana Hospital
44100 Ferrara, ItalyPhone:39 0532 770243
E-mail: [email protected]
Airway management Maintenance of adequate airway is crucial, since most patients have depressed mental status along with respiratory failure. The diaphragmatic weakness induced byhypothy roidism is reversed by thyroid hormone replacement. Mechanical ventilationmay be necessary.
Supportive measures Treat hypothermia with passive rewarming using ordinary blankets and a warm room. The use of a rectal probe helps to determine the true core temperature and to monitor rewarming. If mechanical ventilation is prolonged, total parenteral nutrition may be required.
Infection Infection should always be considered and empiric broad-spectrum of antibiotics be considered until appropriate cultures are proven negative.
Thyroid hormone replacement The ideal mode of therapy and doses of thyroid hormone therapy in myxedema coma remain controversial due to the rarity of the condition and lack of clinical trials.At present, oral and intravenous T4 and T3 are used. Remember that starting IV levothyroxine without treating adrenal insufficiency can precipitate an adrenal crisis.
Glucocorticoid therapy Patients with primary hypothyroidism may have concomitant primary adrenal insuffi-ciency. Furthermore, there is a potential risk of precipitating acute adrenal insuffi-ciency caused by the accelerated metabolism of cortisol that follows T4 therapy. Intravenous hydrocortisone is preferred at a rate of 50mg every 6 hours.
Severe hyponatremia The hyponatremia is a result of decreased free water clearance due to elevated levels of antidiuretic hormone and/or diminished blood flow to the kidneys. Correct severe hyponatremia with saline and free water restriction.
Hypoglycemia Hypoglycemia may be a result of the down-regulation of metabolism seen in hypothyroidism; it may also indicate the possibility of adrenal insufficiency. Correct hypoglycemia with intravenous dextrose.
Hypotension Bradycardia, low cardiac output and overall blood volume deficit frequently exacer-bate the hypotension. Is usually corrected with thyroid hormone therapy. Infusion of dextrose saline solutions and vasopressors if required.
Table 4.Medical care of myxedema coma (From: Wall CR. Myxedema coma: diagnosis and treatment. Am Fam Physician. 2000; 62:2485-90; modified).
De Sanctis_CASE REPORT_Dati ok 05/05/16 09:47 Pagina 28

29
Case report
An 8.8 yr girl was admitted to our Paediatric Endocrinology servi-ce for assessment of early puberty starting one year before refer-ral (Tanner stage B2 at the age of 7.6 years). She was born fol-lowing a normal pregnancy with a birth weight of 3.16 kg andlength of 52 cm as the first child of non-consanguineous parents.At the age of 4.7 yr she was admitted to the Paediatric IntensiveCare for severe head trauma [Glasgow Coma Score (GCS) < 8]secondary to an accidental fall. Magnetic resonance imaging(MRI) demonstrated mild cerebral edema and absence of focalhypothalamic injury.On physical examination, her height (Ht) was 127 cm (23° per-centile), weight was 31.2 kg (72° percentile), body mass index(BMI) was 19.3 kg/m2 and head circumference was at 25th per-
Introduction
Precocious puberty (PP) in girls is defined as the development ofsecondary sexual characteristics before the age of 8 years 1, 2.Its incidence constitutes 1:5000 - 1:10 000 and occurs more fre-quently in girls than in boys 1, 2. There are two types of PP, central and peripheral. Central preco-cious puberty arises from the early maturation of hypothalamic-pituitary axis. Peripheral precocious puberty arises from premature secretion ofsex steroids from gonads or other sites, or due to exogenousexposure. PP can be either isosexual or heterosexual, complete orpartial, and intermittent (un-sustained), or progressive.True PP is usually progressive and reflects the normal sequence ofpubertal hormonal maturation occurring at a noticeably earlier age.Early gonadotropin maturation stimulates the gonads to secretesex steroids which promote the development of somatic sexualcharacteristics. In addition sex steroids accelerate skeletal matura-tion and induce a growth spurt that influences final adult height 1, 2.Therefore, early recognition of PP is important for two main rea-sons: to diagnose the underlying aetiology and to slow the acce-lerated skeletal maturation to prevent its negative effect on finaladult height.In girls, true PP accounts for > 80% of the cases of central PP.The most frequently detected brain abnormalities associated withtrue PP include hypothalamic hamartomas, optic gliomas, astrocy-tomas, pineal tumours, post-infectious encephalitis, hydrocepha-lus, neurofibromatosis and previous CNS injury 3-7. True PP is rare following external head trauma. We describe thelong-term follow-up of a girl who developed central PP within threeyears of severe exogenous head trauma.
Precocious puberty in a girl following severe
traumatic brain injury(TBI) in early childhood:
A simple coincidence or a possible consequence?
SummaryTrue precocious puberty (PP) is rare following external
head trauma. We describe the long term follow-up of a girl who deve-loped PP at the age of 7.6 years, after three years of severe head trau-ma. Severe brain injury may be associated with hypothalamic-pituitarydysfunction including PP; however, the mechanism is not yet well-understood. The current case report highlights the importance ofclose monitoring of patients following significant head trauma.Children exhibiting signs of early puberty need prompt evaluation bythe appropriate Paediatric medical subspecialist.The diagnosis should include detailed anamnesis and clinical exami-nation, measurement of pituitary and sex hormones, assessment ofbone age and imaging of the hypothalamic-pituitary area and gonads.Therapy with a gonadotropin-releasing hormone agonist (GnRH) maybe indicated, in selected cases.
Key words: Central precocious puberty, Severe traumatic brain injury,Follow-up.
Pubertà precoce centrale in una bambina prepubere successiva a severo trauma cranico: Una semplice coincidenza o una possible conseguenza?
Riassunto La comparsa di una pubertà precoce centrale in
seguito ad un trauma cranico è un evento di rara osservazione.Gli Autori riportano la personale esperienza in una bambina di 7 annie 6 mesi. Viene sottolineata l’importanza della anamnesi, dei testsdiagnostici e neuroradiologici. Inoltre viene ribadita l’indicazione adeffettuare un attento monitoraggio clinico, auxologico ed endocrinonei bambini che hanno subito un trauma cranico severo.
Parole chiave: Pubertà precoce centrale, Trauma cranico severo,Follow-up.
Vincenzo De Sanctis1, Ashraf T. Soliman 2, Heba Elsedfy 3,Nada A. Soliman 4, Rania Elalaily 5, Ashraf Adel 6
1 Pediatric and Adolescent Outpatient Clinic, Quisisana Hospital, Ferrara, Italy; 2 Department of Pediatrics, Division of Endocrinology,
Alexandria University Children's Hospital, Alexandria, Egypt; 3 Department of Pediatrics, Ain Shams University, Cairo, Egypt;
4 Ministry of Health, Alexandria, Egypt; 5 Department of Primary Health Care (PHC), Doha, Qatar,
6 General Pediatrics, Hamad General Hospital, Doha, Qatar
Case ReportCase Report
De Sanctis_CASE REPORT_Dati ok 05/05/16 09:53 Pagina 29

30
Rivista Italiana di Medicina dell’Adolescenza
Volume 14, n. 1, 2016
Precocious puberty in a girl following severe traumatic brain injury (TBI) in early childhood:
A simple coincidence or a possible consequence?
centile. Breast and pubic hair were at Tanner stage 3. No goitre was present. Blood pressure was 105/55 mmHg. Her psychomotor development was normal. Her blood cellcount, renal and liver function tests and the levels of plasma glu-cose and electrolytes were in the normal range. Serum thyroid stimulating hormone (TSH), basal follicle stimulatinghormone (FSH) and luteinizing hormone (LH) levels were withinnormal limits (FSH: from 6 to < 11 years = < 0.1-4.3 IU/liter; LH:from 6 to < 11 years = <0.1-5.0 IU/liter). After provocation testwith intravenous GnRH 2.5 µg/Kg, serum LH and FSH rose topeak levels of 17.2 IU/liter and 6.4 IU/liter (IMMULITE 1000 DPC,Los Angeles, CA), respectively. Basal 17 ß estradiol was 249.5pmol/liter (normal values from 6 to < 11 years = < 73.4-216.53pmol/liter). Basal levels of cortisol (19.5 µg/dL), prolactin (13 ng/ml), IGF-1 (185 ng/ml), dehydroepiandrosterone sulphate(DHEAS) (30 µg/dl); and 17 hydroxiprogesterone (0.95 ng/ml)were in the normal range for sex and Tanners’ pubertal staging 8, 9.Bone age as determined by Tanner Whitehouse RUS-method IIIwas 10.8 yr. Pelvic ultrasound showed a bulky uterus (4.2 cm inlength with endometrial thickness of 5.7 mm) and her ovarieswere 2.5 and 2.8 ml in volume with two large follicles (0.9 cm and1 cm). Brain MRI showed a normal pituitary gland with a mildupper convexity compatible with the activation of the hypothala-mic-pituitary gonadal axis.Clonidine stimulation test was performed to exclude partialgrowth hormone deficiency (GHD). This was done because ofthe reported high prevalence of GHD after TBI (up to 42%) 10, 11.Basal GH was 1.1 ng/ml and the peak was normal (16.2 ng/ml). Her parents refused treatment with LH-RH analogue.The patient was regularly followed up every 4 months. The pace of her pubertal development was normal and she hadher first menstrual period at the age of 9.10 yr (the age of menar-che in the mother was 12 years). At that time her height was144.6 cm (86° percentile), weight was 43.2 kg (91° percentile)and bone age was 12.6 yr. Pubertal assessment according toTanner staging was B5 and PH4. In the following 3 years men-strual cycles were regular. The patient’s final height is 152 cm (4° percentile), (mother’s Ht: 160 cm - 31th percentile; father’s Ht:170 cm - 20th percentile).
Discussion
There is a considerable risk of developing pituitary dysfunctionafter TBI in children, adolescents and adults. Road-traffic acci-dent, falls, sport injuries, child abuse and shaking injury are themost common etiological factors for paediatric TBI 12-15.The commonest post-TBI chronic endocrinopathies includehypothalamic-pituitary dysfunctions and diabetes insipidus.Studies have reported that anterior pituitary hormone abnormali-ties may improve, remain stable, or deteriorate in the first 12-36months following head injury 16, 17.
The precise mechanism by which exogenous head trauma cau-ses PP remains unknown. However, the clinical features of thesechildren are consistent with the hypothesis that extra-hypothala-mic areas which restrain pituitary gonadotropin secretion beforepuberty, when damaged by the trauma (as demonstrated byMRI), can result in early activation of hypothalamic-pituitary-gonadal axis pubertal axis. Direct mechanical injury and/orhypoxic insult to the hypothalamus, pituitary stalk or pituitarygland secondary to haemorrhage, edema, and increased intra-cranial pressure are incriminated 12, 16, 17. CPP is rare following external head trauma. Our patient wasadmitted to the outpatient pediatric endocrine clinic at the age of8.8 years for assessment of early puberty, starting one year befo-re referral. There was no family history for precocious puberty.The biochemical criteria for diagnostic confirmation of CPP varyin the literature but are mostly based on the LH response duringa standard GnRH test 18. In our patient, LH response to GnRH sti-mulation (> 5 IU/liter) in accordance with the recent consensusguidelines established the diagnosis of central PP following hersevere TBI reported in early childhood 18-20.At the first examination the BMI was in the normal range and theMRI showed normal anatomy of the hypothalamic-pituitary region.The progression of pubertal changes with precocity varies.Some children show a normal tempo of sexual maturation from thetime that puberty is initiated, whereas others show a staccato pat-tern of maturation that progress to a more gradual pubertal deve-lopment. Others who begin early puberty show steady progressionbut often at a tempo that is much slower than with normal puberty.Although the average interval from normal breast development tomenarche is 2 to 2.5 years, about 20% of girls do not menstruatefor 4 or more years after the first signs of puberty 1, 2, 21.In our girl, the interval between Tanner stage B 2 to menarchewas normal (2.5 years).Previous studies on the biochemical evaluation of girls with CPPpost-TBI are not well detailed. Only a few case reports or smallcase series have highlighted a link between TBI and hypothala-mic-pituitary hormone abnormalities. In a recent systematicreview, 25 patients were reported 23. The youngest patient was2.1 yr old and one-third were below 6 years at their first endocri-ne evaluation. The time interval from the occurrence of TBI andthe age at first endocrine assessment ranged between 3 monthsand 3 years 22, 23. The follow up of these patients was not regular.Some had a fast progressive puberty, one had menarche at theage of 7.5 yr and some were treated with LH-RH analogues.A delay in referring the patient for endocrine evaluation wasreported by some authors 23.In conclusion, CPP is rare following external head trauma.Although some Authors believe that the rate of precociouspuberty after TBI is unlikely to exceed that of the normal popula-tion, others believe that the occurrence of CPP after TBI, is not asimple coincidence but a possible consequence of TBI 23.The majority of patients who develop CPP after TBI had severe
De Sanctis_CASE REPORT_Dati ok 05/05/16 09:53 Pagina 30

31
Precocious puberty in a girl following severe traumatic brain injury (TBI) in early childhood:
A simple coincidence or a possible consequence?
Rivista Italiana di Medicina dell’Adolescenza
Volume 14, n. 1, 2016
injury as assessed by Glasgow Coma Scale or by significantstructural damage (skull fractures, intracranial haemorrhage orcerebral injury) detected by CT or MRI 23. Children exhibiting signs of early puberty need prompt evaluationby an expert paediatric specialist. The diagnosis should includedetailed history and clinical examination, measurement of pitui-tary and sex hormones, assessment of bone age and imaging ofthe hypothalamus-pituitary area and gonads. Close long-termclinical follow-up of children after severe TBI is required to eva-luate their rate of growth and pubertal development. Therapy witha gonadotropin-releasing hormone agonist may be indicated, inselected cases.
References1. Brito VN, Latronico AC, Arnhold IJ, Mendonca BB. Update on the
etiology, diagnosis and therapeutic management of sexual precocity.Arq Bras Endocrinol Metabol. 2008; 52:18-31.
2. Partsch CJ, Heger S, Sippell WG. Management and outcome ofcentral precocious puberty. Clin Endocrinol (Oxf) 2002; 56:129-148.
3. Choi JH, Shin YL, Yoo HW. Predictive factors for organic centralprecocious puberty and utility of simplified gonadotropin-releasinghormone tests. Pediatr Int. 2007; 49:806-810.
4. Ng SM, Kumar Y, Cody D, et al. Cranial MRI scans are indicated in allgirls with central precocious puberty. Arch Dis Child. 2003; 88:414-418.
5. Mogensen SS, Aksglaede L, Mouritsen A, et al. Pathological andincidental findings on brain MRI in a single-center study of 229consecutive girls with early or precocious puberty. PLoS One. 2012;7(1):e29829.
6. Mogonsen SS, Aksglaede L, Mouritsen A, et al. Diagnostic work-upof 449 consecutive girls who were referred to be evaluated forprecocious puberty. J Clin Endocrinol Metab. 2011; 96:1393-1401.
7. Cisternino M, Arrigo T, Pasquino AM, et al. Etiology and ageincidence of precocious puberty in girls: a multicentric study.J Pediatr Endocrinol Metab. 2000; 13:695-701.
8. Sørensen K, Aksglaede L, Petersen JH, et al. Serum IGF1 and insulinlevels in girls with normal and precocious puberty. Eur J Endocrinol.2012; 166:903-910.
9. Kanbur-Oksüz N, Derman O, Kinik E. Correlation of sex steroids withIGF-1 and IGFBP-3 during different pubertal stages.Turk J Pediatr.2004; 46:315-321.
10. Soliman AT, Adel A, Soliman NA, et al. Pituitary deficiency followingtraumatic brain injury in early childhood: A review of the literature.Georgian Med News. 2015; 244-245:62-71.
11. De Sanctis V, Sprocati M, Govoni M R, Raiola G. Assessment oftraumatic brain injury and anterior pituitary dysfunction inadolescents. Georgian Med News. 2008; 156:18-23.
12. Bondanelli M, Ambrosio MR, Zatelli MC, et al. Hypopituitarism aftertraumatic brain injury. Eur J Endocrinol. 2005;152:679-691.
13. Parslow RC, Morris KP, Tasker RC, et al. Traumatic Brain Injury StudySteering Group and pediatric intensive care Society Study Group.Epidemiology of traumatic brain injury in children receiving intensivecare in the UK. Arch Dis Child. 2005; 90:1182-1187.
14. Benoit R, Watts DD, Dwyer K, et al. Windows 99: a source ofsuburban pediatric trauma. J Trauma. 2000; 49:477-481.
15. Barlow KM, Minns RA. Annual incidence of shaken impact syndromein young children. Lancet. 2000; 356:1571-1572.
16. Iglesias P, Gómez-Pan A, Diez JJ.Spontaneous recovery from post-traumatic hypopituitarism. J Endocrinol Invest.1996; 19:320-323.
17. Kaufman HH, Timberlake G, Voelker J, Pait TG. Medicalcomplications of head injury. Med Clin North Am. 1993; 77:43-60.
18. Carel JC, Eugster EA, Rogol A, et al. Consensus statement on theuse of gonadotropin-releasing hormone analogs in children.Pediatrics. 2009; 123:e752-e762.
19. Neely EK, Wilson DM, Lee PA, et al. Spontaneous serumgonadotropin concentrations in the evaluation of precocious puberty.J Pediatr. 1995; 127:47-52.
20. Neely EK, Hintz RL, Wilson DM, et al. Normal ranges forimmunochemiluminometric gonadotropin assays. J Pediatr. 1995;127:40-46.
21. Haqq A, Noston B, La Franchi S. Precocious puberty. Chapter 16.www.glowm.com/resources/glowm/cd/pages/v5/v5c016.html
22. Shaul PW, Towbin RB, Chernausek SD. Precocious puberty followingsevere head trauma. Am J Dis Child. 1985; 139:467-469.
23. De Sanctis V, Soliman AT, Elsedfy H, et al. Precocious pubertyfollowing traumatic brain injury in early childhood: A review of theliterature. Pediatr Endocrinol Rev. 2015; 13:458-464.
Corrispondenza:
Vincenzo de Sanctis, MDPediatric and Adolescent Outpatient Clinic, Quisisana Hospital44100 Ferrara, ItalyPhone:39 0532 770243 E-mail: [email protected]
De Sanctis_CASE REPORT_Dati ok 05/05/16 09:53 Pagina 31

Potential diagnostic and therapeutic use of Continuous Glucose Monitoring Systems (CGMS)in Thalassemia Major: A short presentation of personal experience
AbstractThe prevalence of diabetes insulin dependent (DM) and impaired glucose tolerance (IGT) in adolescents and young adults with TM con-ventionally treated with desferioxamine (DFO) varies in different series (up to 10.5 % and 24 %, respectively). The most accurate methodwith which to evaluate altered glucose metabolism in patients with TM is still controversial. It has been demonstrated recently that thecontinuous glucose monitoring system (CGMS) is a useful and valid tool in defining glucose metabolism in children and adults affected byTM with early glucose derangements. CGMS is also an useful method to detect the variability of glucose fluctuations and offers the oppor-tunity for better assessment of glucose homeostasis in TM patients and response to therapy. The Authors report their experience for thediagnosis and treatment of glucose abnormalities in thalassemia.
Key words: Thalassemia major, Glucose abnormalities, Continuous Glucose Monitoring System (CGMS).
Ashraf Soliman1, Mohamed Yassin2, Fawzia Alyafie3, Rania Elalaily4, Nada A. Soliman5, Heba Elsedfy6, Vincenzo De Sanctis7
1 Departments of Pediatric, Alexandria University Children’s Hospital, Alexandria-Egypt; 2 National Center for Cancer Care and Research, Department of Hematology and BMT, Hamad Medical Corporation, Doha, Qatar; 3 Pediatric Endocrine Section Hamad Medical Center, Doha, Qatar; 4 Ministry of Health, Alexandria, Egypt; 5 Department of Primary Health Care, Abu Nakhla Hospital, Doha, Qatar; 6 Department of Pediatrics, Ain Shams University, Cairo, Egypt; 7 Pediatric and Adolescent Outpatient Clinic, Quisisana Hospital, Ferrara - Italy.
Soliman - ENDO-THAL_Kattamis_Transfusional_He#D7779 28/04/16 12:16 Pagina 32

33
Potential diagnostic and therapeutic use of Continuous Glucose Monitoring Systems (CGMS) in Thalassemia Major: A short presentation of personal experience
Endo-ThalRivista Italiana di Medicina dell’Adolescenza - Volume 14, n. 1, 2016
IntroductionGlucose tolerance abnormalities and diabetesmellitus are common complications in tha-lassemia patients. Pancreatic iron loading in tha-lassemia major (TM) patients begins after the firstdecade of life and the incidence increases withage. While glucose intolerance occurs at an earli-er stage during adolescence, diabetes frequentlyoccurs at later stages and is usually secondary toiron overload and subsequent chronic liver dis-ease (1-4). Up to 25% of patients with TM mayhave isolated impaired fasting plasma glucose(IFG) a condition considered as a pre-diabeticstate. However; it is not known how many TMpatients with IFG may progress over the years todiabetes (1,2). The prevalence of diabetes insulindependent (DM) and impaired glucose tolerance(IGT) in adolescents and young adults with TMconventionally treated with desferioxamine(DFO) varies in different series (up to 10.5 %and 24 %, respectively) (1-4). In general, 51% ofTM patients have impaired insulin secretion,32% have increased insulin secretion and 19%have delayed insulin secretion (4) These condi-tions are believed to precede the clinical expres-sion of diabetes mellitus. Elevated serum ferritinconcentrations and hepatitis C infection have longbeen considered as important factors associatedwith the development of abnormal glucose toler-ance in TM patients (1-4). Zinc deficiency mightlead to an exacerbation of the inability of thepancreas to secrete sufficient amounts of insulinin response to oral glucose load in TM patients(5, 6). A family history of diabetes does not seemto be not a significant predictor for future dia-betes risk (5-7). The considerable variation in theoccurrence of glycemic abnormalities can be par-tially explained by the marked differences in thecohort’s genetic background, transfusion regi-mens, degree of chelation, screening methodused and also relates to the ages of patients beingstudied, with lower rates in younger patients.
Diagnostic value of CGMS in patients with TMThe most accurate method with which to evalu-ate altered glucose metabolism in patients withTM is still controversial. Even if the annual oralglucose tolerance test (OGTT) by the age of 10years is the recommended method, a diagnosis of‘normal’ glucose tolerance during OGTT does
not exclude abnormal postprandial glucose levelsat home (1, 2, 8). There is now evidence that theOGTT method, evaluating fasting and 2-h postload glucose, may miss episodes of hypergly-caemia (8-10). Furthermore, the credibility of HbA1c has been questioned because the hemoglo-bin composition of patients’ erythrocytes areconsiderably modified, due to regular and fre-quent transfusions. The results may be falselyincreased or decreased depending on the prox-imity to transfusion, shortened erythrocyte lifes-pan and the assay used (11-15).It has been demonstrated recently that the contin-uous glucose monitoring system (CGMS) is a use-ful and valid tool in defining glucose metabolismin children and adults affected by TM with earlyglucose derangements (10–15). Indeed, theCGMS allows monitoring of glycaemic profilesthroughout a period of 72 h for a total of 288 gly-caemic registrations per day. It identifies glycaemicexcursions and constitutes a valid device to under-stand the 24-h glycaemic trend and profiles.Rimondi et al. investigated the value of using CGMSin six TM patients with abnormal glucose home-ostasis after an oral glucose tolerance test (OGTT)(10). Two-hour OGTT glucose values and CGMSfluctuations were classified as normal if < 7.8mmol/l, impaired if 7.8 to 11.1 mmol/l, diabetic if> 11.1 mmol/l. The TM patients spent from 1 to23% of the time with a blood glucose level from7.8 to 11.1 mmol/l. In five patients the CGMS con-firmed the impaired glucose tolerance diagnosisand in one patient the CGMS excluded the diag-nosis of diabetes. A case report in Oman studiedthe use of CGM as a follow-up tool in a TM patientwith abnormal glucose homeostasis (16).Both studies suggest that CGM is a usefulmethod to detect glucose levels in these patients.Similarly, we studied 16 adolescents with TM(19.75 ± 3 years) using OGTT and CGMS for 3days. Using OGTT 25% had IFG, 12.5% had IGTand one of them had diabetes. Using CGMS themaximum BG (3h postprandial) 25% had diabetesand 56% had IGT. Serum ferritin concentrationswere correlated significantly with the fasting BGand the 2-h blood glucose levels in the OGTT aswell as with the average BG recorded by CGM (17).Albaker et al. showed that using CGMS detecteddiabetes state in 2 thalassemic patients who hadHbA1C in the impaired glucose range. Further-more, the study showed a direct relationshipbetween the time of the first transfusionand theCGM results (18).
Soliman - ENDO-THAL_Kattamis_Transfusional_He#D7779 28/04/16 12:16 Pagina 33

34
Endo-ThalRivista Italiana di Medicina dell’Adolescenza - Volume 14, n. 1, 2016
Potential diagnostic and therapeutic use of Continuous Glucose Monitoring Systems (CGMS) in Thalassemia Major: A short presentation of personal experience
Personal experience Patient 1A 15 year old male with TM presented with noc-turia. His FBG was 5.6 mmol/L and OGTT showeda BG level at 2hrs of 8.5 mmol/l. His CGMSshowed a diabetic range of BG after dinner andovernight. Based on this tracing, a basal insulin(Glargine) was prescribed at night. A satisfactoryresponse was recorded by CGMS (Figure 1).
Patient 2A 14 year old girl with TM with no symptomsrelated to glycemic abnormalities. Her FBG was4.9 mmol/L and an OGTT showed a BG level at 2hrs of 6.9 mmol/L (IGT). CGMS tracing showedprolonged persistent hyperglycemia after lunchsuggesting a need for prandial insulin to cover hercarbohydrate load. Insulin aspart before lunchproperly controlled her glycemia (Figure 2).
Patient 3A 13 year old boy with TM had a normal FBG
Therapeutic (monitoring)value of CGMS in patientswith TM
CGMS is a useful method to detect the variabili-ty of glucose fluctuations and offers the opportu-nity for better assessment of glucose homeostasisin TM patients and response to therapy (8, 10,16, 18).CGMS was useful in documenting a poorglycemic control in a 27-year-old woman, withprolonged periods of hyper- and hypoglycemia.Her blood sugar levels showed suboptimal con-trol (erratic, unexplainable blood glucose read-ings throughout the day that ranged between120 and 300 mg/dL [6.6–16.7 mmol/L]),withsignificant hyperglycemia in the morning.Based on these results, her insulin regimen wasadjusted and the blood glucose levels were great-ly improved throughout and the patient was ableto meet her target blood glucose range (72–140mg/dL [4–7.8 mmol/L]) in 70% of the time (8).
Figure 1. CGMS before and after insulin glargine (each day different color of curve).
Soliman - ENDO-THAL_Kattamis_Transfusional_He#D7779 28/04/16 12:16 Pagina 34

35
Potential diagnostic and therapeutic use of Continuous Glucose Monitoring Systems (CGMS) in Thalassemia Major: A short presentation of personal experience
Figure 3. Effect of transfusion (packed blood red cell; blue arrow) on blood glucose using CGMS.
Figure 2. CGMS before and after insulin aspart (each day different color of curve).
Endo-ThalRivista Italiana di Medicina dell’Adolescenza - Volume 14, n. 1, 2016
Soliman - ENDO-THAL_Kattamis_Transfusional_He#D7779 28/04/16 12:16 Pagina 35

36
Endo-ThalRivista Italiana di Medicina dell’Adolescenza - Volume 14, n. 1, 2016
Potential diagnostic and therapeutic use of Continuous Glucose Monitoring Systems (CGMS) in Thalassemia Major: A short presentation of personal experience
(4.5 mmol/L) and OGTT (2h BG =7.6 mmo/l).Applying CGMS monitoring showed IGT state.Furthermore, the effect of packed red cell transfu-sion showed marked reduction of his BG beforemeals and overnight. This is the first case to docu-ment the rapid beneficial effect of blood transfusionon glycemia in a thalassemic patient (Figure 3).
ConclusionsAdvances in TM care have led to improved sur-vival and quality of life in patients with TM; how-ever, many chronic endocrine diseases haveemerged as a result of potential endocrine compli-cations by routine screening and a high index ofsuspicion is imperative for patients with TM toreceive timely treatment.Our results demonstratethat the CGMS is a useful method to detect thevariability of glucose fluctuations and offers theopportunity for better assessment of glucosehomeostasis in TM patients. Proper and early ironchelation or the use of intensive iron chelation inthose with high iron load the new oral chelatorshave been shown to decrease or reverse theseglycemic abnormalities.In addition, optimizationof insulin therapy with the help of CGMS appearsto be clinically useful and cost-effective approach.
References1. De Sanctis V, Soliman A, Yassin M. Iron overload and glu-
cose metabolism in subjects with β-thalassaemia major: anoverview. Curr Diabetes Rev. 2013; 9:332-41.
2. De Sanctis V, Soliman AT, Elsedfy H, et al. Diabetes AndGlucose Metabolism In Thalassemia Major: An Update.Expert Rev Hematol. 2015 Dec 24. [Epub ahead of print]
3. Chern JP, Lin KH, Lu MY, et al. Abnormal glucose tolerancein transfusion-dependent betathalassemic patients. DiabetesCare. 2001; 24:850-854.
4. Cario H, Holl RW, Debatin KM, Kohne E. Insulin sensitivi-ty and beta-cell secretion in thalassaemia major with sec-ondary haemochromatosis: assessment by oral glucose toler-ance test. Eur J Pediatr. 2003; 162:139-46.
5. Fung EB, Gildengorin G, Talwar S, et al. Zinc status affectsglucose homeostasis and insulin secretion in patients withthalassemia.Nutrients. 2015; 7:4296-4307.
6. Dehshal MH, Hooghooghi AH, Kebryaeezadeh A, et al. Zincdeficiency aggravates abnormal glucose metabolism in tha-lassemia major patients.Med Sci Monit. 2007; 13:CR235-9.
7. De Sanctis V, Zurlo MG, Senesi E, et al. Insulin dependentdiabetes in thalassemia. Arch Dis Child. 1988; 63:58-62.
8. Soliman A, De Sanctis V, Yassin M, Elalaily R. TherapeuticUse and Diagnostic Potential of Continuous Glucose Moni-toring Systems (CGMS) in Adolescents. Adv Diab Metab.2014; 2:21-30.
9. Choudhary A, Giardina P, Antal Z, Vogiatzi M. Unreliableoral glucose tolerance test and HbA1C in Beta Thalas-saemia Major-A case for continuous glucose monitoring? BrJ Haematol. 2013; 162:132-53.
10. Rimondi F, Banin P, Gamberini MR, De Sanctis V. The con-tinuous glucose monitoring system (CGMS) in patients withbeta-thalassemia major and impaired glucose homeostasis:preliminary results. Pediatr Endocrinol Rev. 2008; 6 Suppl1:190-2.
11. Sacks DB. Hemoglobin variants and hemoglobin A1Canalysis: problem solved ? Clin Chem. 2003; 49:1245-7.
12. Spencer DH, Grossman BJ, Scott MG. Red cell transfusiondecreases hemoglobin A1C in patients with diabetes. ClinChem. 2011; 57:344-6.
13. Bry L, Chen PC, Sacks DB. Effects of hemoglobin variantsand chemically modified derivatives on assays for glycohe-moglobin. Clin Chem. 2001; 47:153-63.
14. Tahara Y, Shima K. Kinetics of HbA1c, glycated albumin,and fructosamine and analysis of their weight functionsagainst preceding plasma glucose level. Diabetes Care.1995; 18:440-7.
15. Choudhary A, Giardina P, Antal Z, Vogiatzi M.Unreliableoral glucose tolerance test and HbA1C in Beta Thalas-saemia Major-A case for continuous glucose monitoring? BrJ Haematol. 2013; 162:132-53.
16. Al-Futaisi A, Wali Y, El-Beshlawi I, et al.Case Study: usinga continuous glucose monitoring system in a patient withdiabetes and beta-thalassemia hemoglobinopathy. PediatrHematol Oncol. 2009; 26:515-9.
17. Soliman AT, Yasin M, El-Awwa A, De Sanctis V. Detection ofglycemic abnormalities in adolescents with beta thalassemiausing continuous glucose monitoring and oral glucose toler-ance in adolescents and young adults with β-thalassemiamajor: Pilot study. Indian J Endocrinol Metab. 2013;17:490-5.
18. Albaker WI, Yousef AA, Khamis AH, et al. The continuousglucose monitoring system (CGMS) in patients with beta-thalassemia major. Saudi J Med Med Sci. 2013; 1:88-93.
Declaration of Interest: The authors report no conflicts of interest.
Correspondence:Ashraf T Soliman
Department of Pediatrics, Division of Endocrinology, Alexandria University Children's Hospital,
Alexandria, EgyptWeill Cornell Medical College, Qatar and General Pediatrics,
Hamad General Hospital, DohaMail: [email protected]
Soliman - ENDO-THAL_Kattamis_Transfusional_He#D7779 28/04/16 12:16 Pagina 36

Obiettivo della rivistaLa Rivista Italiana di Medicina dell’Adolescenza, organoufficiale della Società Italiana di Medicina del l’Ado le -scenza, si propone di favorire la cultura e la conoscenzadegli aspetti medici, etici, educativi e psicosociali dellaetà adolescenziale con l’obiettivo di migliorare l’approc-cio all’assistenza e alle problematiche dell’età evolutiva.La Rivista Italiana di Medicina dell’Adolescenza, quadri-mestrale, pubblica articoli di aggiornamento, articoli originali, casi clinici, esperienze sul campo, rassegnespecialistiche di Esperti di diverse discipline mediche(pediatria, medicina legale, dermatologia, ginecologia,andrologia, odontoiatria, diagnostica di laboratorio e perimmagini, medicina dello sport).Front line accetta contributi, esperienze di medici e nonmedici che si occupano di adolescenti. Per questa rubrica non sono necessari l’abstract e la bibliografia.Endothal è l'organo ufficiale dell’Association of ClinicalEndocrinologists for Thalassaemia and AdolescentMedicine (A-CET-A). Magam news pubblica i contributi scientifici del Me dit -erranean and Middle East Action Group for Ado lescentMedicine.
Preparazione degli articoliIl primo Autore deve dichiarare all’Editor in Chief che i -contributi sono inediti ed il loro contenuto conforme alla legislazione vigente anche in materia di etica della ricerca(Vedi http://www.icmje.org/urm_main.html). La redazione si riserva di modificare i testi nella forma peruniformarli alle caratteristiche della rivista.Gli articoli devono essere dattiloscritti con doppio spaziosu fogli A4 (210 x 297 mm), lasciando 20 mm per i mar-gini superiore, inferiore e laterali.La prima pagina deve contenere: titolo, nome e cogno-me (per esteso) degli Autori, istituzione di ap partenenzae relativo indirizzo (telefono, fax, indirizzo di posta elet-tronica).La seconda pagina deve contenere un riassunto in ita-liano ed in inglese, il titolo in inglese e 2-5 parolechiave in italiano ed in inglese.Per la bibliografia, che deve essere essenziale (limitataad un massimo di 25 voci), attenersi agli “UniformRequirements for Manuscript submitted to BiomedicalJournals” (New Eng J Med 1997; 336:309). Le referenze bibliografiche devono essere numerate pro-gressivamente nell’ordine in cui sono citate nel testo (innumeri arabi tra parentesi). I titoli delle riviste devono essere abbreviate secondo lostile utilizzato nell’Index Medicus (la lista può essereeventualmente ottenuta al seguente sito web: http://www.nlm.nih.gov). Per gli articoli con più Autori vanno riportati i primi tre seguiti da et al.La lunghezza del testo deve essere compresa tra 1.500 e2.500 parole.
1. I manoscritti devono essere preparati seguendo rigo-rosamente le norme per gli Autori.
2. Gli Autori, se necessario, devono indicare che lo stu-dio è stato approvato dal Comitato Etico, che è statoottenuto il consenso informato scritto per lo studio edil permesso per la pubblicazione nel testo di eventua-li fotografie del paziente.
3. L’Autore è tenuto a dichiarare l’eventuale presenza diconflitti di interesse, la quale sarà segnalata in casodi pubblicazione.
4. L'articolo verrà sottoposto al giudizio di due Referee edeventualmente dell'Editor in Chief.
5. Gli Autori dovranno seguire le raccomandazioni ri -portate nel sito http://www.icmje.org/urm_main.htmlper la prepa razione dei lavori scientifici e gli aspetti eticidella ricerca.
La pubblicazione dei lavori scientifici è gratuita.
Articoli standard di rivisteParkin MD, Clayton D, Black RJ et al. Childhood leukaemiain Europe after Chernobil: 5 year follow-up. Br J Cancer1996; 73:1006-1010.
Articoli con organizzazioni come autoreThe Cardiac Society of Australia and New Zealand.Clinical exercise stress testing. Safety and performanceguidelines. Med J Aust 1996; 164:282-286.
Articoli in supplementi al fascicoloPayne DK, Sullivan MD, Massie MJ. Women’s psycholo-gical reactions to breast cancer. Semin Oncol 1996; 23(Suppl 2):89-92.
LibriRingsven MK, Bond D. Gerontology and leadership skill fornurses. 2nd ed. Albany (NY): Delmar Publisher; 1996.
Capitolo di un libroPhilips SJ, Whisnant JP. Hypertension and stroke. In:Laragh JH, Brenner BM, editors. Hypertension: pathophy-siology, diagnosis, and management. 2nd ed. New York:Raven Press; 1995, p. 465-470.
Figure e TabellePer le illustrazioni tratte da altre pubblicazioni è necessa-rio che l’Autore fornisca il permesso scritto di riprodu -zione. Le figure (disegni, grafici, schemi, fotografie) devono es-sere numerate con numeri arabi secondo l’ordine con cuivengono citate nel testo ed accompagnate da didascalieredatte su un foglio separato.Le fotografie possono essere inviate come immagini elet-troniche (formato JPEG o TIFF).Ciascuna tabella deve essere redatta su un singolo fo-glio, recare una didascalia ed essere numerata con nu-meri arabi secondo l’ordine con cui viene citata nel testo.
Come e dove inviare gli articoliIl testo dattiloscritto, il materiale iconografico ed il di-schetto magnetico (formato PC o Mac) contenente il filecon il testo e le tabelle devono essere spediti al seguen-te indirizzo:
Dott. Vincenzo De SanctisEditor in Chief
Rivista Italiana di Medicina della AdolescenzaOspedale Privato Accreditato QuisisanaViale Cavour, 128 - 44121 Ferrara
e-mail: [email protected]
Una volta che il manoscritto ha ricevuto l'approvazio-ne della sua versione definitiva, viene messo nel ca-lendario delle pubblicazioni e pubblicato alla primaoccasione possibile, tenendo in considerazione il piano Editoriale della testata.
Con la pubblicazione del manoscritto gli Autori trasferi-scono la proprietà ed i diritti d’Autore all’Editore ScriptaManent s.n.c. Milano.
Istruzioni agli Autori
Cop_Cop edit som 28/04/16 11:37 Pagina III