VEGF A e Anti VEGFR Mab Dott. Domenico...
52
Roma, 26 giugno 2015 Anti VEGF‐A e Anti VEGFR Mab front line o strategia di sequenza? Dott. Domenico Corsi
Transcript of VEGF A e Anti VEGFR Mab Dott. Domenico...

Roma, 26 giugno 2015, g g
Anti VEGF‐A e Anti VEGFR Mabfront line o strategia di sequenza?
Dott. Domenico Corsi
Dr. Domenico Corsi
In ottemperanza alla normativa ECM ed al principio di trasparenza delle fonti di finanziamento ed i i i i di i i i li i i i i i f idei rapporti con soggetti portatori di interessi commerciali in campo sanitario, si informano idiscenti che negli ultimi due anni si sono avuti i seguenti rapporti anche di finanziamento consoggetti portatori di interessi commerciali in campo sanitario:
AMGEN, MERCK SERONO, ROCHE, SANOFI AVENTIS, ITALFARMACO, PROSTAKAN,
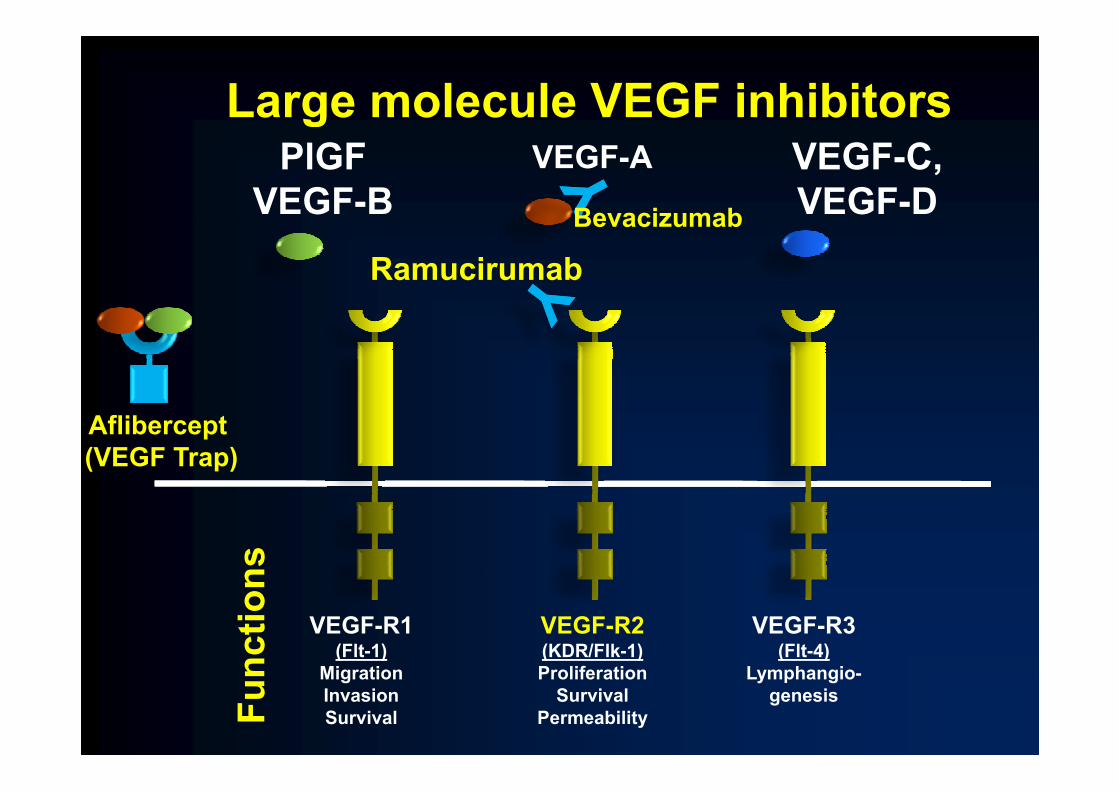
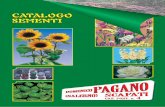
Large molecule VEGF inhibitorsVEGF-APlGF
VEGF-B VEGF-C, VEGF-D
g
BevacizumabBevacizumab
Ramucirumab
Aflibercept(VEGF Trap)
ns
VEGF-R1(Flt-1)
VEGF-R3(Flt-4)
VEGF-R2(KDR/Flk-1)nc
tion
MigrationInvasionSurvival
Lymphangio-genesis
ProliferationSurvival
PermeabilityFun
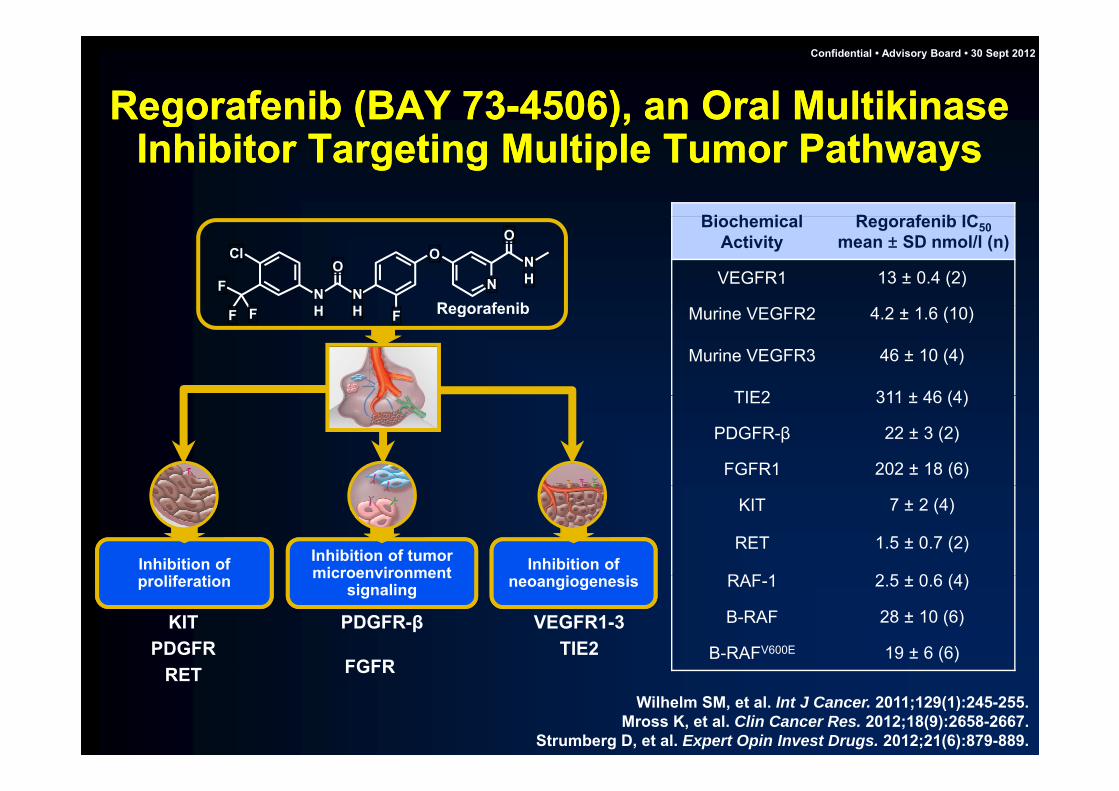
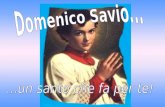
Regorafenib (BAY 73-4506), an Oral Multikinase Regorafenib (BAY 73-4506), an Oral Multikinase Confidential • Advisory Board • 30 Sept 2012
g ( )Inhibitor Targeting Multiple Tumor Pathways
g ( )Inhibitor Targeting Multiple Tumor Pathways
Bi h i l R f ib IC
Regorafenib
Cl
FO
OO
NH
NH
NH
N
BiochemicalActivity
Regorafenib IC50mean ± SD nmol/l (n)
VEGFR1 13 ± 0.4 (2)
RegorafenibFF F HH Murine VEGFR2 4.2 ± 1.6 (10)
Murine VEGFR3 46 ± 10 (4)
TIE2 311 ± 46 (4)TIE2 311 ± 46 (4)
PDGFR-β 22 ± 3 (2)
FGFR1 202 ± 18 (6)
Inhibition of Inhibition of tumor microenvironmentInhibition of
f
KIT 7 ± 2 (4)
RET 1.5 ± 0.7 (2)
RAF 1 2 5 0 6 (4)
KITPDGFR
PDGFR-β
FGFR
VEGFR1-3TIE2
neoangiogenesismicroenvironment signalingproliferation RAF-1 2.5 ± 0.6 (4)
B-RAF 28 ± 10 (6)
B-RAFV600E 19 ± 6 (6)
Wilhelm SM, et al. Int J Cancer. 2011;129(1):245-255.Mross K, et al. Clin Cancer Res. 2012;18(9):2658-2667.
Strumberg D, et al. Expert Opin Invest Drugs. 2012;21(6):879-889.
RET FGFR
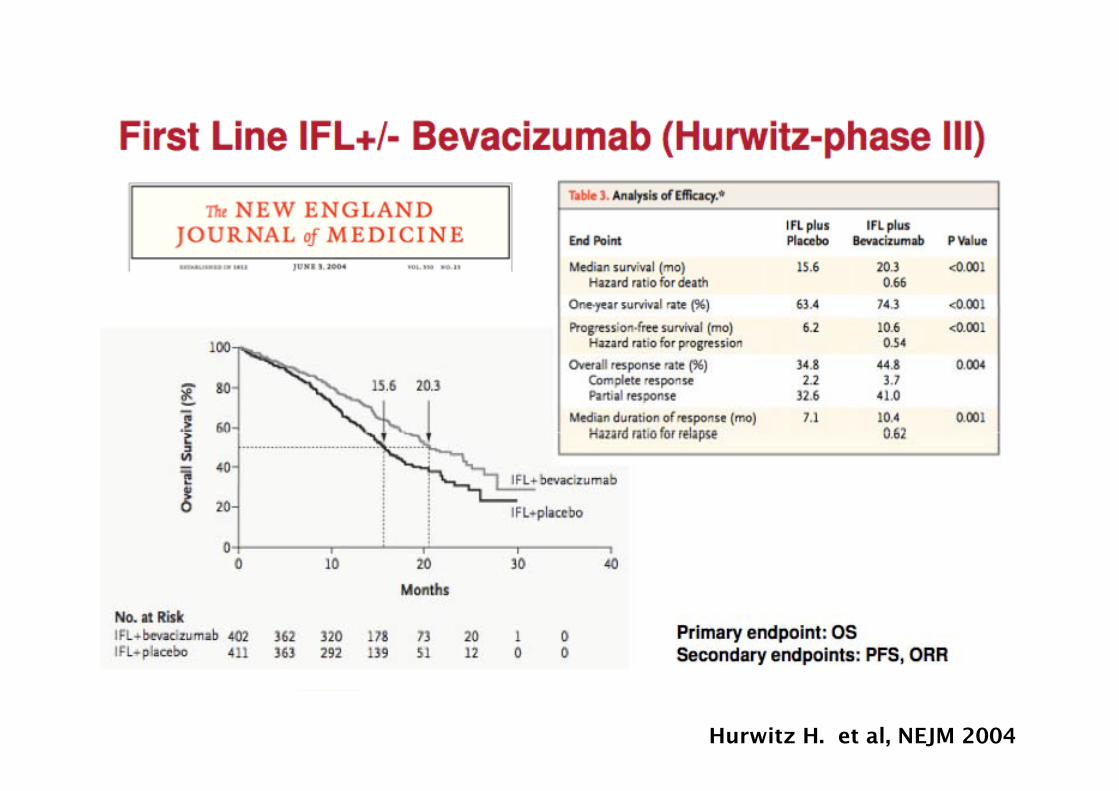
Hurwitz H. et al, NEJM 2004

Hurwitz H. et al, The Oncologist 2009

Hurwitz H. et al, The Oncologist 2009
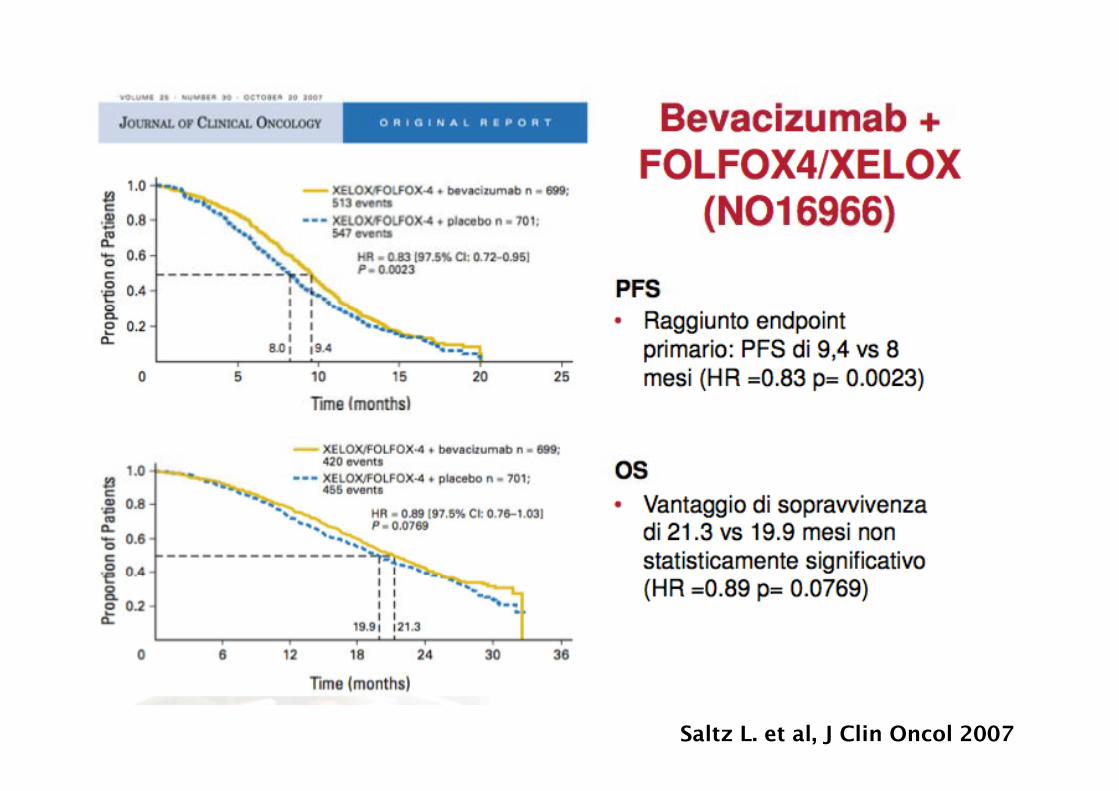
Saltz L. et al, J Clin Oncol 2007

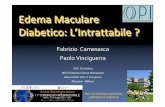
AVEX - Study designAVEX - Study designy gy gCapecitabine 1000 mg/m2 b.i.d.
days 1–14, q21d
Previously untreated mCRC age ≥70 years
y , q+
Bevacizumab 7.5 mg/kg day 1, q21d
Randomize mCRC, age ≥70 years
N=280
Capecitabine 1000 mg/m2 b.i.d. days 1–14 q21d
1:1
Stratification factors:Stratification factors:days 1 14, q21d
– ECOG PS (0–1 vs 2)– Geographic region– ECOG PS (0–1 vs 2)– Geographic region• Key inclusion criteria
– ECOG PS 0–2– Prior adjuvant chemotherapy allowed if completed >6 month before inclusion– Not optimal candidates for a combination chemotherapy with irinotecan or oxaliplatin
• Key exclusion criteria• Key exclusion criteria– Prior chemotherapy for mCRC or prior adjuvant anti-VEGF treatment– Clinically significant cardiovascular disease– Current or recent use of aspirin (>325 mg/day) or other NSAIDCurrent or recent use of aspirin (>325 mg/day) or other NSAID – Use of full-dose anticoagulants or thrombolytic agents
Cunningham et al, Lancet Oncol 2013

AVEX - PFSAVEX - PFSAVEX PFSAVEX PFS
1.0
0.8
Cape + BEV (n=140) Cape (n=140)
estim
ate
0.6HR=0.53 (95% CI: 0.41–0.69)
P<0.001
PFS
e 0.4
0.2
0.0
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38 40
Ti ( th )
5.1 mo 9.1 mo
Number at riskCape + BEV
Cape
140 121 99 80 68 55 41 28 23 16 13 9 8 3 2 2 2 2 1 0 0
140 109 82 56 38 25 13 9 6 4 4 2 1 1 1 1 1 1 1 1 0
Time (months)
p
Cunningham et al, Lancet Oncol 2013

AVEX - Overall survivalAVEX - Overall survival
1 0 Cape + BEV (n=140)1.0
0.8HR=0.79 (95% CI: 0.57–1.09)
Cape + BEV (n=140) Cape (n=140)
0.6
0 4estim
ate
HR 0.79 (95% CI: 0.57 1.09)P=0.182
0.4
0.2
OS
∆ 3.9 mos0.0
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38 40 42 44 46
Ti ( h )
16.8 mo 20.7 mo
Number at riskCape + BEV
Cape
140 126 120 106 95 89 81 67 60 51 44 40 34 24 16 15 12 10 8 6 5 4
140 120 108 94 85 73 62 57 49 37 33 23 19 13 11 10 9 7 6 5 5 3
Time (months)
2
1
0
0
Cunningham et al, Lancet Oncol 2013
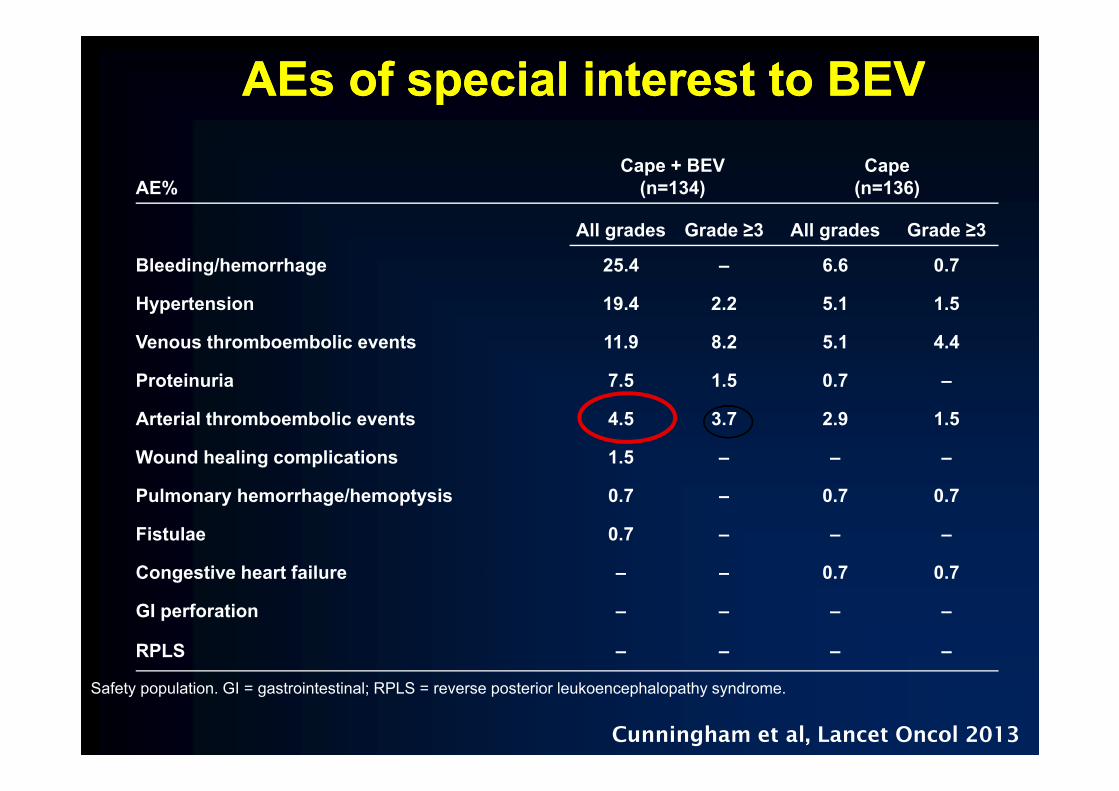
AEs of special interest to BEVAEs of special interest to BEV
AE%Cape + BEV
(n=134)Cape
(n=136)
All grades Grade ≥3 All grades Grade ≥3
Bleeding/hemorrhage 25.4 – 6.6 0.7
Hypertension 19 4 2 2 5 1 1 5Hypertension 19.4 2.2 5.1 1.5
Venous thromboembolic events 11.9 8.2 5.1 4.4
Proteinuria 7.5 1.5 0.7 –
Arterial thromboembolic events 4.5 3.7 2.9 1.5
Wound healing complications 1.5 – – –
Pulmonary hemorrhage/hemoptysis 0.7 – 0.7 0.7
Fistulae 0.7 – – –
Congestive heart failure – – 0 7 0 7Congestive heart failure 0.7 0.7
GI perforation – – – –
RPLS – – – –
Safety population. GI = gastrointestinal; RPLS = reverse posterior leukoencephalopathy syndrome.
Cunningham et al, Lancet Oncol 2013
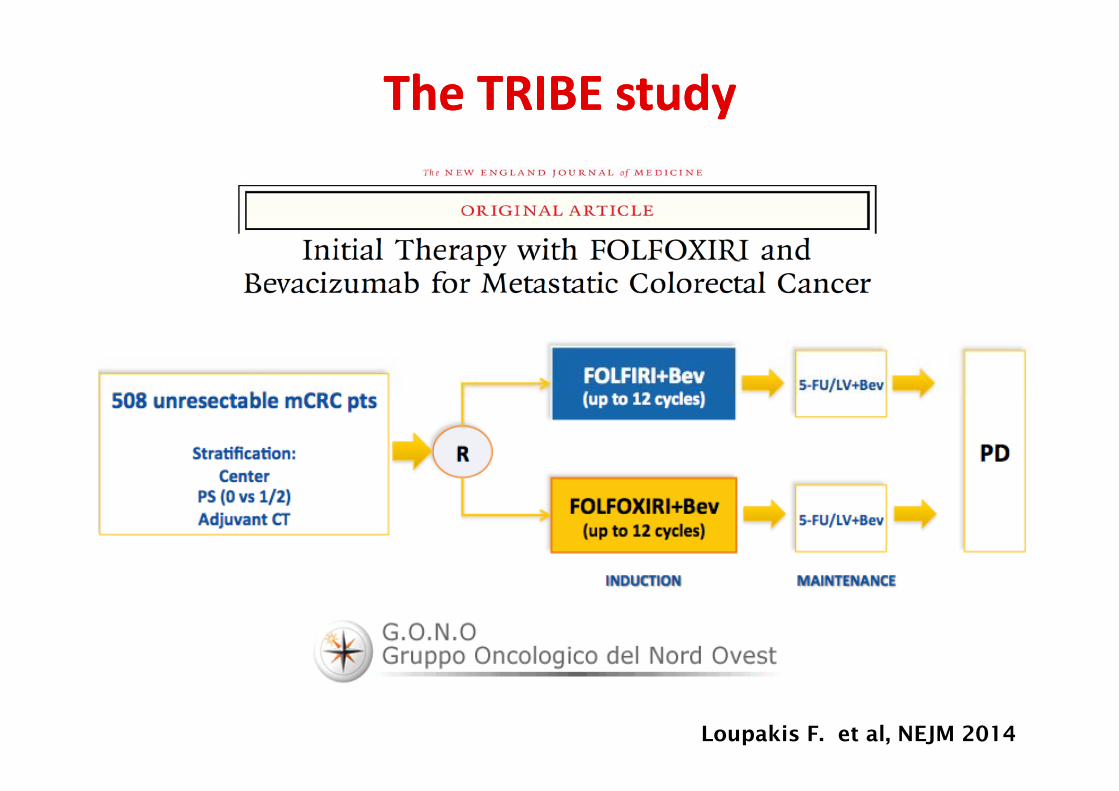
The TRIBE The TRIBE studystudy
Loupakis F. et al, NEJM 2014

TRIBE: TRIBE: UpdatedUpdated PFS PFS resultsresultsMedian follow up: 48.1 mos
(74% of death events)
FOLFIRI b N 256 / P d 236FOLFIRI + bev: N = 256 / Progressed = 236FOLFOXIRI + bev: N = 252 / Progressed = 232
FOLFIRI + bev, median PFS : 9.7 mos,FOLFOXIRI + bev, median PFS : 12.3 mos
HR: 0.77 [0.65‐0.93]p=0.006
Cremolini C. et al, ASCO GI 2015

TRIBE: TRIBE: SecondarySecondary endpointendpoint -- OSOSUpdatedUpdated OS OS resultsresults
Median follow up: 48.1 mos(74% of death events)
UpdatedUpdated OS OS resultsresults
FOLFIRI + bev: N = 256 / Died = 200FOLFOXIRI + bev: N = 252 / Died = 174
(74% of death events)
FOLFIRI + bev, median OS : 25.8 mosFOLFOXIRI + bev, median OS : 29.8 mos
HR 0 80 [0 65 0 98]HR: 0.80 [0.65‐0.98]p=0.030
5ys-OS rate
24.9% vs 12.4%
Cremolini C. et al, ASCO GI 2015

ToxicityToxicity ProfileProfile –– SafetySafety populationpopulationG3/4 adverse events, % patients
FOLFIRI + bevN=254
FOLFOXIRI + bevN=250
p
yy yy p pp p
Nausea 3 3 1.000
Vomiting 3 4 0.492
Diarrhea 11 19 0.012
Stomatitis 4 9 0.048
Neutropenia 20 50 <0.001
Febrile neutropenia 6 9 0.315
Neurotoxicity 0 5 <0.001
Hypertension 2 5 0.157
Venous Thrombosis 6 7 0.593
Arterial Thrombosis 2 1 1.000
Bleeding 1 1 1.000
adapted from Loupakis et al., NEJM 2014

FOLFOXIRI+bevFOLFOXIRI+bev: : usualusual questionsquestions
✓ Is it for everyone?
✓ Is it for everyone?
NO!NO!
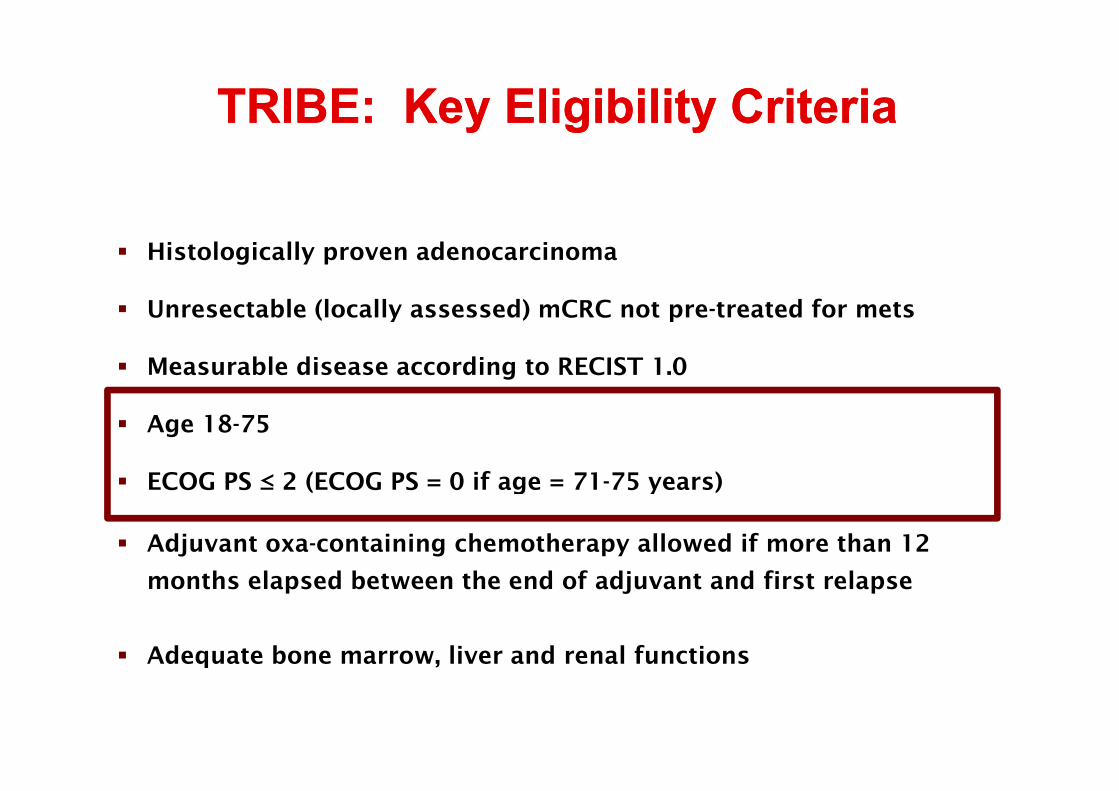
TRIBE: Key TRIBE: Key EligibilityEligibility CriteriaCriteriayy g yg y
Histologically proven adenocarcinoma
Unresectable (locally assessed) mCRC not pre treated for metsUnresectable (locally assessed) mCRC not pre-treated for mets
Measurable disease according to RECIST 1.0
Age 18-75
ECOG PS ≤ 2 (ECOG PS = 0 if age = 71-75 years)ECOG PS ≤ 2 (ECOG PS = 0 if age = 71 75 years)
Adjuvant oxa-containing chemotherapy allowed if more than 12
th l d b t th d f dj t d fi t lmonths elapsed between the end of adjuvant and first relapse
Adequate bone marrow, liver and renal functionsq ,
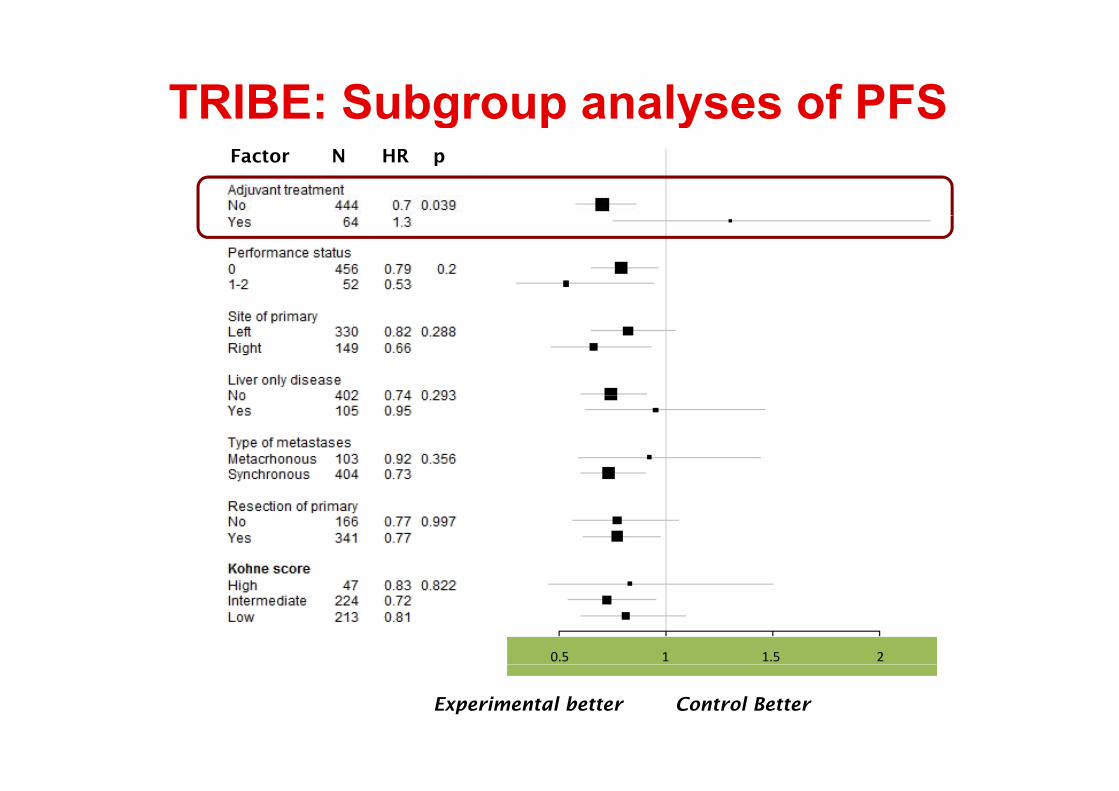
TRIBE: Subgroup analyses of PFSFactor N HR p
g p y
0.5 1 1.5 2
Experimental better Control Better
FOLFOXIRI+bevFOLFOXIRI+bev: : usualusual questionsquestions
✓ Is it for everyone?
✓ Is it for everyone?
✓ Is it just for potentially resectable patients?✓ Is it just for potentially resectable patients?
NO!NO!
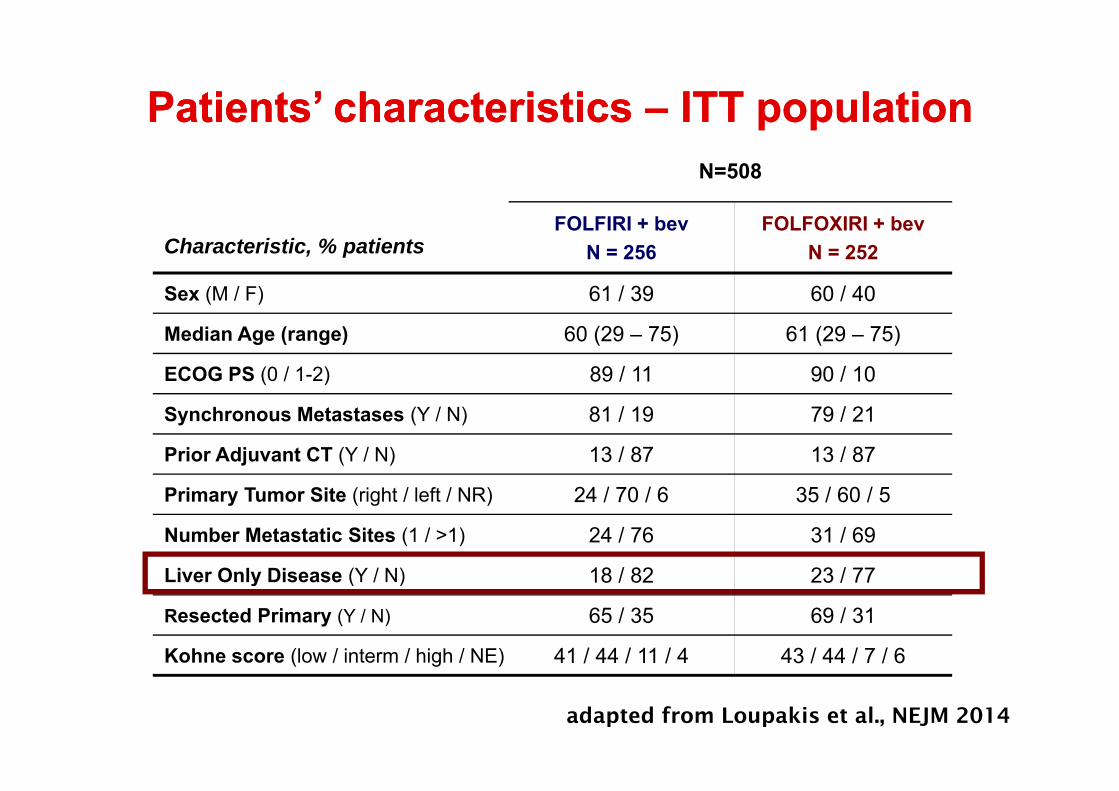
PatientsPatients’ ’ characteristicscharacteristics –– ITT ITT populationpopulationN=508
O O O
p pp p
Characteristic, % patientsFOLFIRI + bev
N = 256FOLFOXIRI + bev
N = 252
Sex (M / F) 61 / 39 60 / 40
Median Age (range) 60 (29 – 75) 61 (29 – 75)
ECOG PS (0 / 1-2) 89 / 11 90 / 10
Synchronous Metastases (Y / N) 81 / 19 79 / 21
Prior Adjuvant CT (Y / N) 13 / 87 13 / 87
Primary Tumor Site (right / left / NR) 24 / 70 / 6 35 / 60 / 5
Number Metastatic Sites (1 / >1) 24 / 76 31 / 69
Liver Only Disease (Y / N) 18 / 82 23 / 77Liver Only Disease (Y / N) 18 / 82 23 / 77
Resected Primary (Y / N) 65 / 35 69 / 31
Kohne score (low / interm / high / NE) 41 / 44 / 11 / 4 43 / 44 / 7 / 6( g )
adapted from Loupakis et al., NEJM 2014

TRIBE:TRIBE: SecondarySecondary ResectionResection ofof MetastasesMetastasesTRIBE: TRIBE: SecondarySecondary ResectionResection ofof MetastasesMetastases
FOLFIRI + bevArm A
N = 256
FOLFOXIRI + bevArm BN = 252
pN 256 N 252
Secondary surgery with radical intent 21% 26% 0.210
R0 secondary surgery 12% 15% 0.327
Liver-only subgroup N = 46 N = 59
Secondary surgery with radical intent 41% 39% 1.000
R0 secondary surgery 28% 32% 0.823
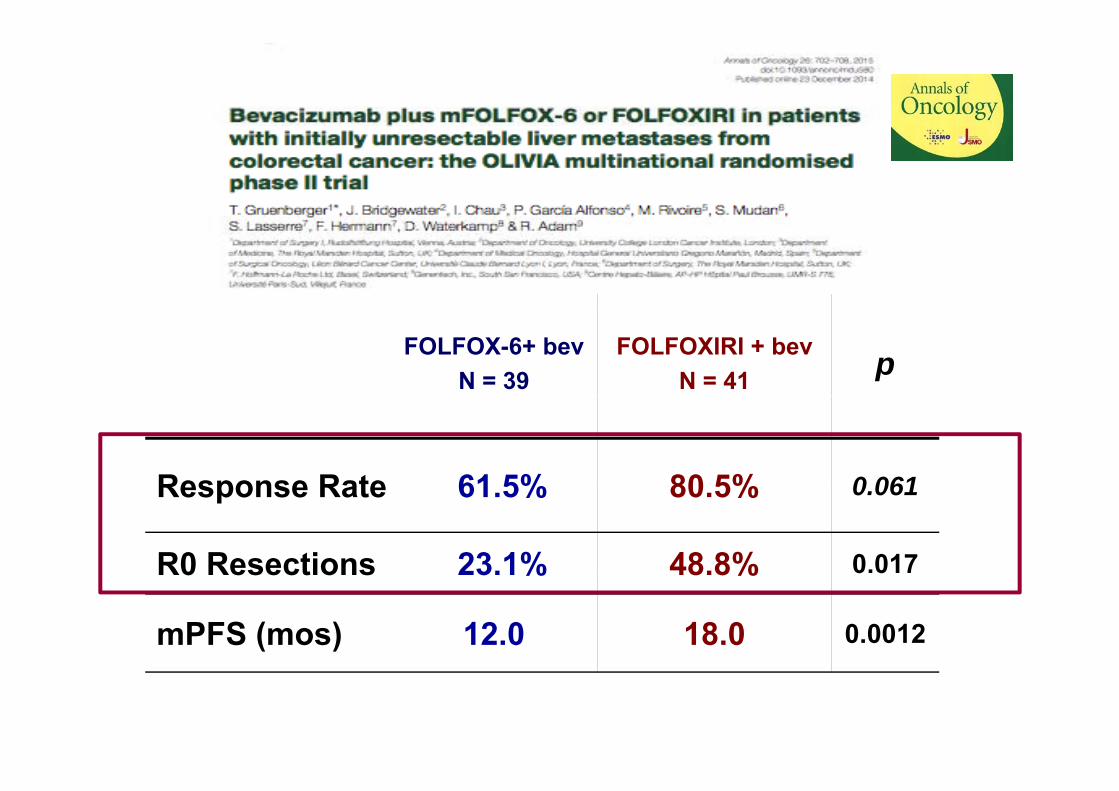
FOLFOX-6+ bevN = 39
FOLFOXIRI + bevN = 41 p
Response Rate 61 5% 80 5% 0 061Response Rate 61.5% 80.5% 0.061
R0 Resections 23.1% 48.8% 0.0170 esect o s 3 % 8 8%
mPFS (mos) 12.0 18.0 0.0012

FOLFOXIRI+bevFOLFOXIRI+bev: : usualusual questionsquestionsqq
✓ Is it for everyone?
✓ Is it just for potentially resectable patients?
✓ Is it only for mutants?
NO!NO!

TRIBE TRIBE studystudy subgroupsubgroup analysesanalyses of PFS of PFS ––yy g pg p yymolecularmolecular characteristicscharacteristics
Factor N HR p
0 4 0 6 0 8 10.4 0.6 0.8 1
Experimental better Control Better
Loupakis et al., NEJM 2014

UpdatedUpdated survivalsurvival resultsresults accordingaccording to to molecularmolecular subtypessubtypes
• Fit patients with BRAF mutant mCRC may benefit the most, butsurvival gap is mantainedsurvival gap is mantained
• OS in all wt patients is 41.5 monthsp
• Consider FOLFOXIRI+Bev in fit mCRC patients, independentlyfrom mutational status
Is the patient fit for FOLFOXIRI?Is the patient fit for FOLFOXIRI?
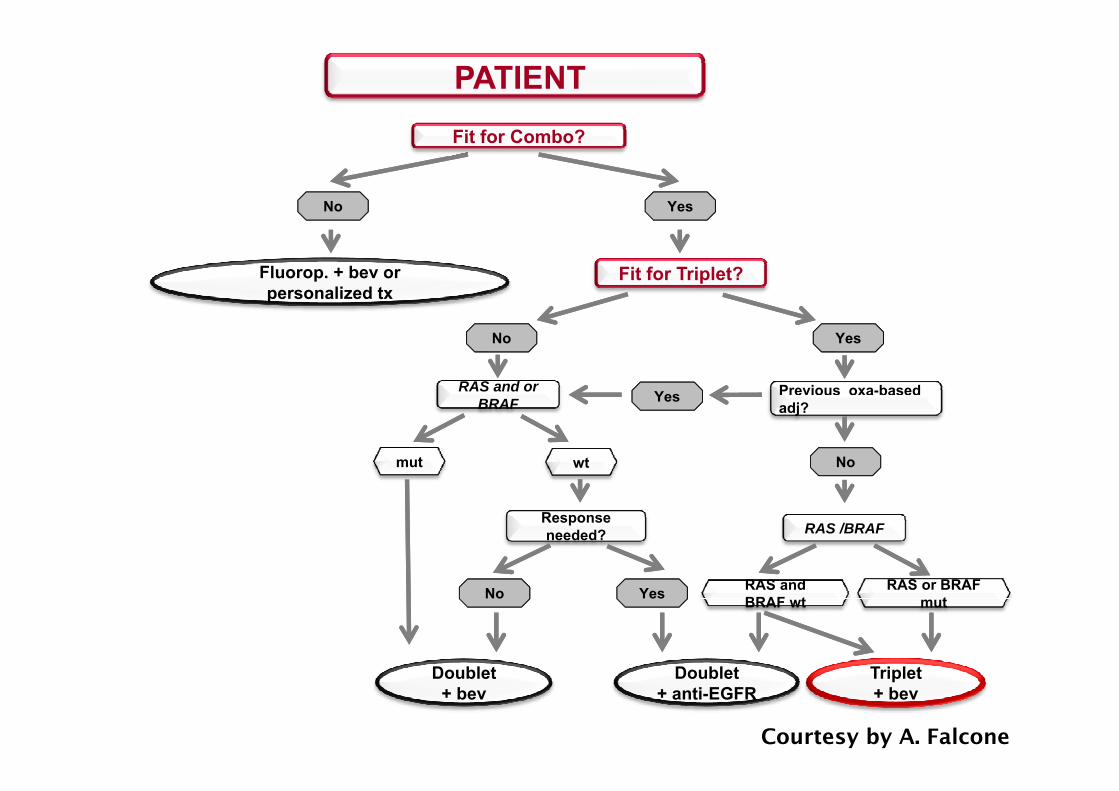
PATIENTFit for Combo?
No Yes
Fluorop. + bev or personalized tx
Fit for Triplet?
No Yes
Previous oxa-basedRAS and or Yes
adj?BRAF Yes
Nomut wt
RAS /BRAFResponseneeded?
No Yes RAS and BRAF wt
RAS or BRAF mut
Doublet+ bev
Triplet+ bev
Doublet+ anti-EGFR
Courtesy by A. Falcone

Phase III studies with randomization Phase III studies with randomization maintenance versus observationmaintenance versus observation
CAPOX + BEVPreviously
C C
CAIRO31
Cape + BEVCR
RE
CAPOX + BEV(18 weeks)untreated mCRC
(N=558)R
Observation
PD
• Primary endpoint: superiority in PFS2 (maintenance and re-induction)
PRSD
IND
AIO 02072 FP + BEV
Primary endpoint: superiority in PFS2 (maintenance and re induction)
R
FP + oxaliplatin +BEV
(24 weeks)
Previously untreated mCRC
(N=852)
AIO 02072
RPDCR
PRSD
FP + BEV
BEV
RE
IND(N 852)
Observation
• Primary endpoint: non-inferiority in time to failure of strategy (TFS)
D
1. Koopman, et al. ASCO 2014 2. Hegewisch-Becker, et al. ESMO2014 FP = fluoropyrimidine

CapeOx+Bevx6 Cape-BEV MT
(months)CFI
(months)
HRPMT
R PD1PFS1 8.5 4.1 0.43
<0.0001
0 67
MT
PD2RPFS2 11.7 8.5 0.67
<0.0001
TT2PD 13 9 11 1 0.68CFI
C O B Cape-BEV
PFS1
TT2PD 13.9 11.1 <0.0001
OS 21.6 18.1 0.890 22N=558
CapeOx+Bevx6
PFS1 0.22MT:Low-dose Cape (625 mg/m2 BID daily)+ BEV (7 5 mg/KG every 3 wks)
N 558
PFS2+ BEV (7.5 mg/KG every 3 wks)
TT2PDPFS2: time from R until PD upon re-introduction of XELOX-BTT2PD i f R il PD f PFS1
Simkens LHJ et al Lancet Oncology 2015
TT2PD: time from R until PD upon any treatment after PFS1MT: Maintenance therapyCFI: Chemotherapy-free interval
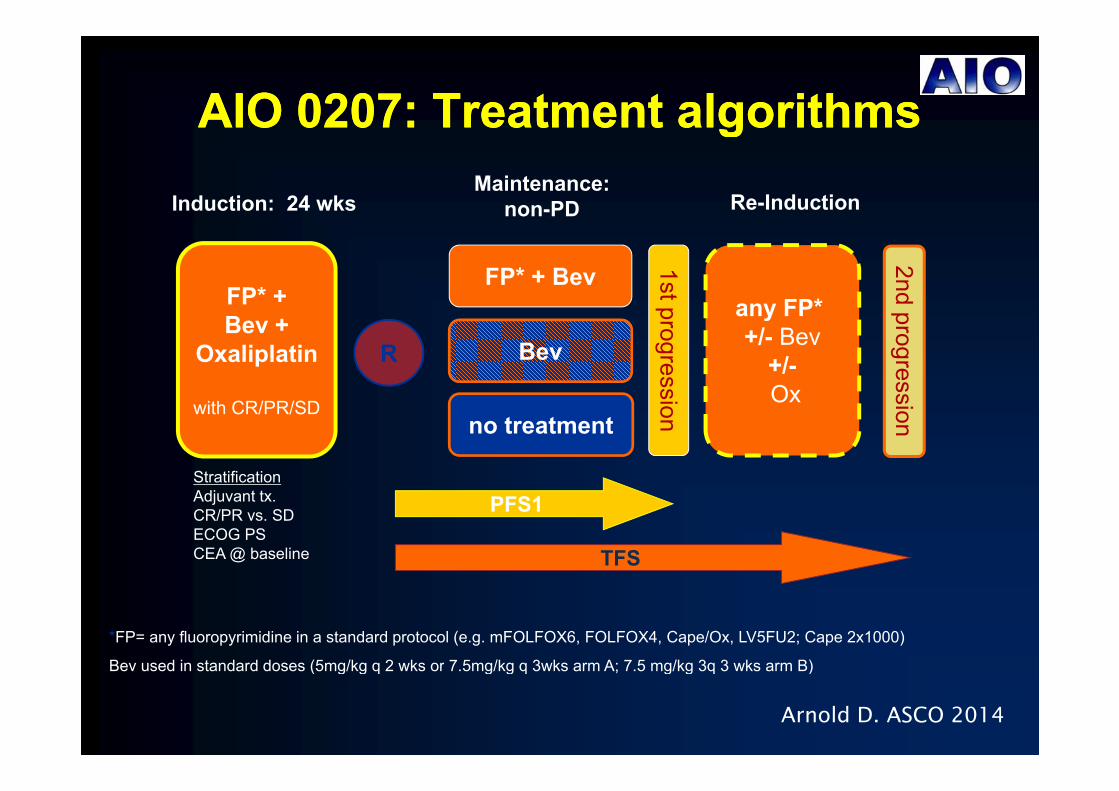
AIO 0207: Treatment algorithmsAIO 0207: Treatment algorithmsAIO 0207: Treatment algorithmsAIO 0207: Treatment algorithms
Induction: 24 wksMaintenance:
non-PD Re-Induction
FP* + Bevany FP*
non PD
1st
2nd FP* + any FP* +/- Bev
+/-Ox
BevR
progress
progress
Bev +Oxaliplatin
Oxno treatment
sion
sion
Stratification
with CR/PR/SD
PFS1
TFS
Adjuvant tx.CR/PR vs. SDECOG PSCEA @ baseline
*FP= any fluoropyrimidine in a standard protocol (e.g. mFOLFOX6, FOLFOX4, Cape/Ox, LV5FU2; Cape 2x1000)
Bev used in standard doses (5mg/kg q 2 wks or 7 5mg/kg q 3wks arm A; 7 5 mg/kg 3q 3 wks arm B)Bev used in standard doses (5mg/kg q 2 wks or 7.5mg/kg q 3wks arm A; 7.5 mg/kg 3q 3 wks arm B)
Arnold D. ASCO 2014

AIO 0207: SummaryAIO 0207: SummaryAIO 0207: SummaryAIO 0207: Summary
• Using a TFS strategy, following 6 months with FP/Ox/Bev • Using a TFS strategy, following 6 months with FP/Ox/Bev g gy g• Maintenance with Bev is non-inferior to FP/Bev• Non-inferiority can not be concluded for no active
g gy g• Maintenance with Bev is non-inferior to FP/Bev• Non-inferiority can not be concluded for no active
treatment
• PFS1 improves with treatment intensity: FP/Bev is better
treatment
• PFS1 improves with treatment intensity: FP/Bev is better• PFS1 improves with treatment intensity: FP/Bev is better than Bev alone, and this is better than no treatment.
• PFS1 improves with treatment intensity: FP/Bev is better than Bev alone, and this is better than no treatment.
• Preliminary OS showed no difference between treatment arms.
• Preliminary OS showed no difference between treatment arms.
• Re-induction rates were much lower than expected: 37% overall, decreasing with maintenance intensity
• Re-induction rates were much lower than expected: 37% overall, decreasing with maintenance intensity37% overall, decreasing with maintenance intensity37% overall, decreasing with maintenance intensity
Arnold D. ASCO 2014

TRIBE-2: Study design
FOLFOX + PD1 PD2PD2
FOLFIRI + bev* PD1 PD2PD2
5FU/bev bev* 5FU/bev
R1:1
N=650
FOLFOXIRI + bev* PD1 PD2
5FU/bevFOLFOXIRI
+ bev* 5FU/bev
Primary objective: PFS2
*all repeated for 8 cycles (4 months) followed by maintenance with 5FU/bev until PD
Primary objective: PFS2
followed by maintenance with 5FU/bev until PD

Giantonio BJ. et al. J Clin Oncol 2005

BRiTE: median OS by post-progression treatmenty p p g
GrotheyGrothey A et al. J A et al. J ClinClin OncolOncol 20082008

Kopetz S. et al. J Clin Oncol 2010
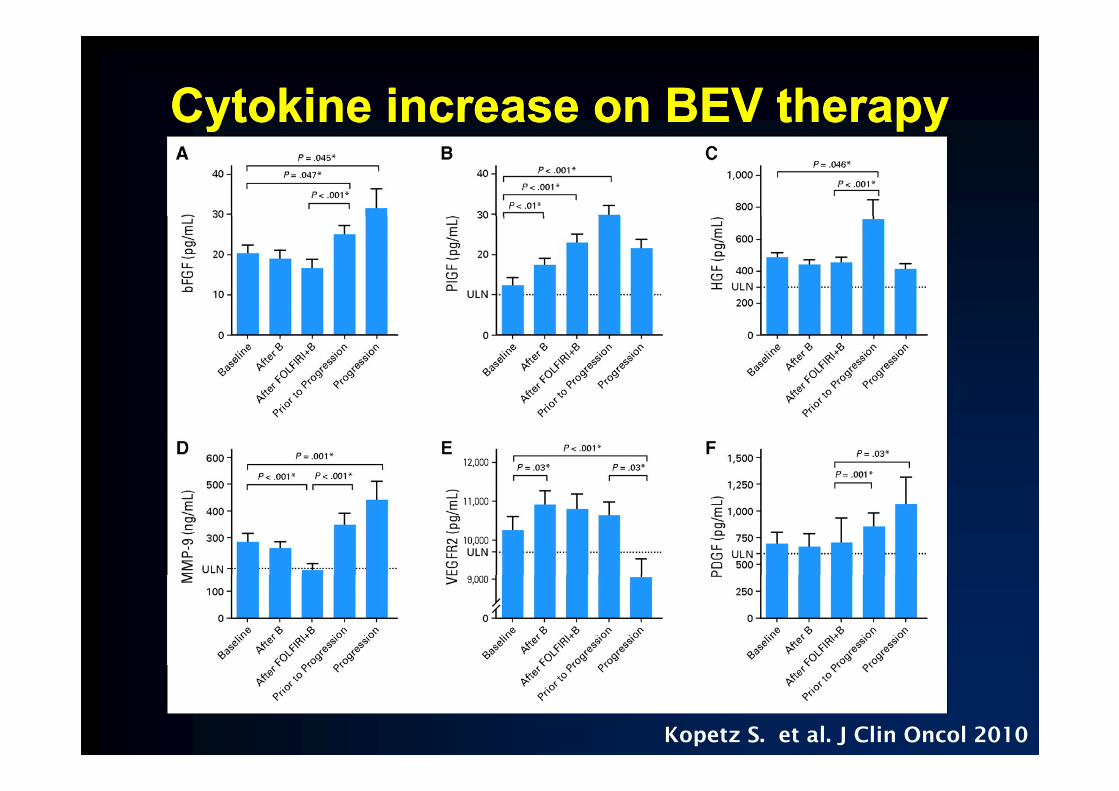
Cytokine increase on BEV therapyCytokine increase on BEV therapyy pyy py
Kopetz S. et al. J Clin Oncol 2010
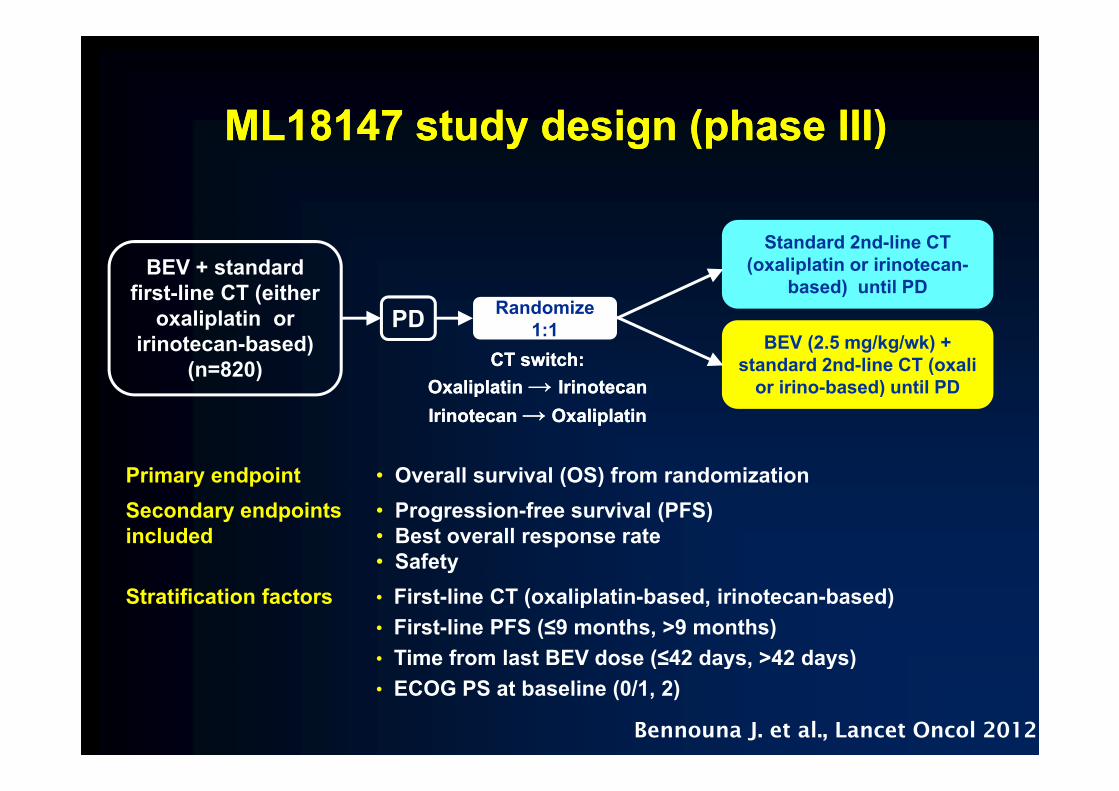
ML18147 study design (phase III)ML18147 study design (phase III)ML18147 study design (phase III)ML18147 study design (phase III)
BEV + standard first-line CT (either
Randomize
Standard 2nd-line CT (oxaliplatin or irinotecan-
based) until PD
oxaliplatin oririnotecan-based)
(n=820)
Randomize 1:1 BEV (2.5 mg/kg/wk) +
standard 2nd-line CT (oxalior irino-based) until PD
PD CT switch:
Oxaliplatin → IrinotecanCT switch:
Oxaliplatin → Irinotecan )pIrinotecan→ Oxaliplatin
pIrinotecan→ Oxaliplatin
Primary endpoint • Overall survival (OS) from randomizationy p ( )Secondary endpoints included
• Progression-free survival (PFS)• Best overall response rate• Safety
Stratification factors • First-line CT (oxaliplatin-based, irinotecan-based)• First-line PFS (≤9 months, >9 months)• Time from last BEV dose (≤42 days, >42 days)Time from last BEV dose (≤42 days, 42 days)• ECOG PS at baseline (0/1, 2)
Bennouna J. et al., Lancet Oncol 2012
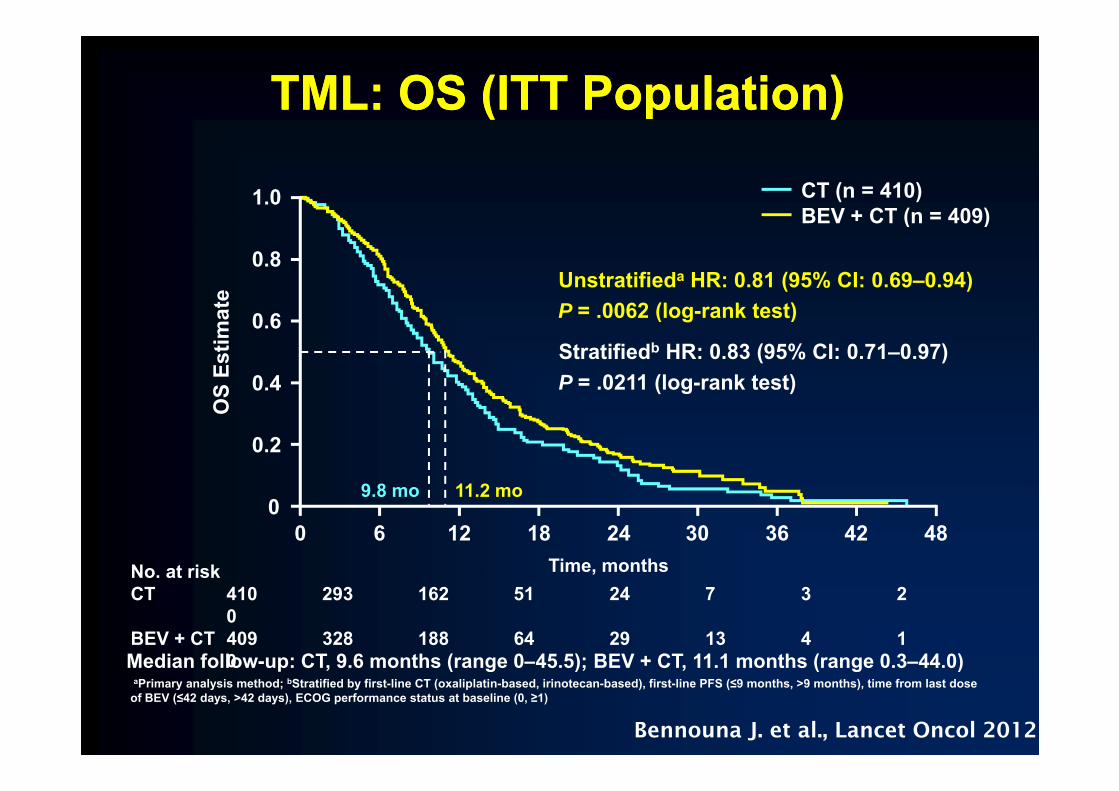
TML: OS (ITT Population)TML: OS (ITT Population)
1.0 CT (n = 410)BEV + CT (n = 409)
te
0.8
BEV + CT (n = 409)
Unstratifieda HR: 0.81 (95% CI: 0.69–0.94)P 0062 (l k t t)
S Es
timat 0.6
0.4
P = .0062 (log-rank test)
Stratifiedb HR: 0.83 (95% CI: 0.71–0.97)P = .0211 (log-rank test)
OS
0.2
9 8 11 2
Time, months
00 6 12 18 24 30 36 42 48
No at risk
9.8 mo 11.2 mo
No. at riskCT 410 293 162 51 24 7 3 2
0BEV + CT 409 328 188 64 29 13 4 1
0Median follow-up: CT 9 6 months (range 0–45 5); BEV + CT 11 1 months (range 0 3–44 0)0aPrimary analysis method; bStratified by first-line CT (oxaliplatin-based, irinotecan-based), first-line PFS (≤9 months, >9 months), time from last dose of BEV (≤42 days, >42 days), ECOG performance status at baseline (0, ≥1)
Median follow up: CT, 9.6 months (range 0 45.5); BEV + CT, 11.1 months (range 0.3 44.0)
Bennouna J. et al., Lancet Oncol 2012

Progression-free survival (ITT population)Progression-free survival (ITT population)
CT (n=410)1.0
0.8
CT (n=410)BEV + CT (n=409)
estim
ate
0.6Unstratifieda HR: 0.68 (95% CI: 0.59–0.78) p<0.0001 (log-rank test)
Stratifiedb HR: 0.67 (95% CI: 0.58–0.78)
PFS
e
0.4
0.2
Stratified HR: 0.67 (95% CI: 0.58 0.78)p<0.0001 (log-rank test)
00 6 12 18 24 30 36 42
4.1 5.7
Time (months)No. at riskCT 410 119 20 6 4 0 0 0BEV + CT 409 189 45 12 5 2 2
0aPrimary analysis method. bStratified by first-line CT (oxaliplatin-based, irinotecan-based), first-line PFS (≤9 months, >9 months), time from last dose of BEV (≤42 days, >42 days), ECOG PS at baseline (0, ≥1)
Bennouna J. et al., Lancet Oncol 2012

VELOUR VELOUR –– VEGFVEGF--trap with trap with irinotecanirinotecan in in coLOrectalcoLOrectalcancer aftercancer after failURefailURe ofof oxaliplatinoxaliplatincancer after cancer after failURefailURe of of oxaliplatinoxaliplatin
RA
Aflibercept 4 mg/kg IV, day 1 + FOLFIRI
2 k
Metastatic Colorectal
NDO
q2 weeks
1:1 Disease
600600
Cancer OMI
1:1 Disease Progression Death
Stratification factors: IZE
Placebo IV, day 1+ FOLFIRIq2 weeks
600600• ECOG PS (0 vs 1 vs 2)• Prior bevacizumab (Y/N)
q
OS 12 06 13 5 HR 0 817 0 0032OS: 12.06 v 13.5 HR = 0.817 p =0.0032 Van Cutsem E. et al., J Clin Oncol 2012
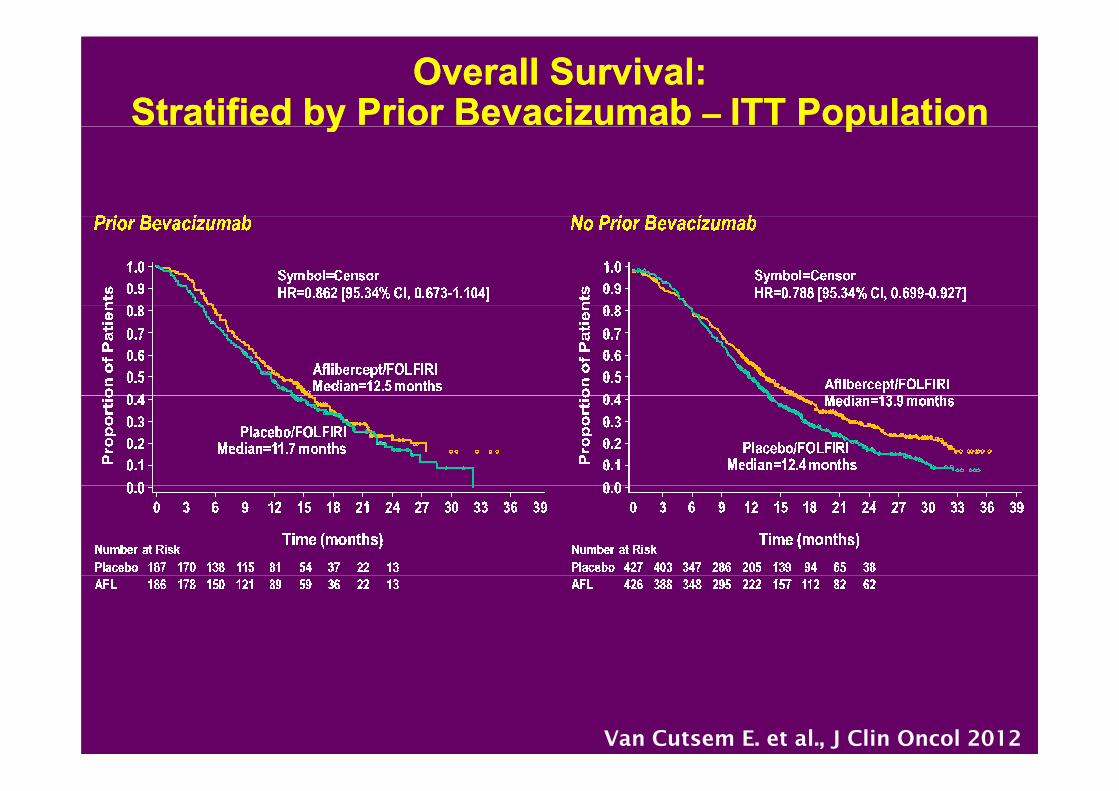
Overall Survival: Stratified by Prior Bevacizumab – ITT Population
Overall Survival: Stratified by Prior Bevacizumab – ITT Populationy py p
Van Cutsem E. et al., J Clin Oncol 2012

Progression-Free Survival: Stratified by Prior Bevacizumab – ITT Population
Progression-Free Survival: Stratified by Prior Bevacizumab – ITT Populationy py p
Van Cutsem E. et al., J Clin Oncol 2012

Slide 3
Tabernero J et al Lancet Oncol 2015

RAISE: OVERALL SURVIVALRAISE: OVERALL SURVIVAL
RAISE: Overall Survival
Tabernero J et al Lancet Oncol 2015

RAISE: PROGRESSION FREE SURVIVALRAISE: PROGRESSION FREE SURVIVAL
RAISE: Progression-free Survival
Tabernero J et al Lancet Oncol 2015

RAISE: AE OF SPECIAL INTERESTRAISE: AE OF SPECIAL INTEREST
RAISE: Adverse Events of Special Interest
Tabernero J et al Lancet Oncol 2015
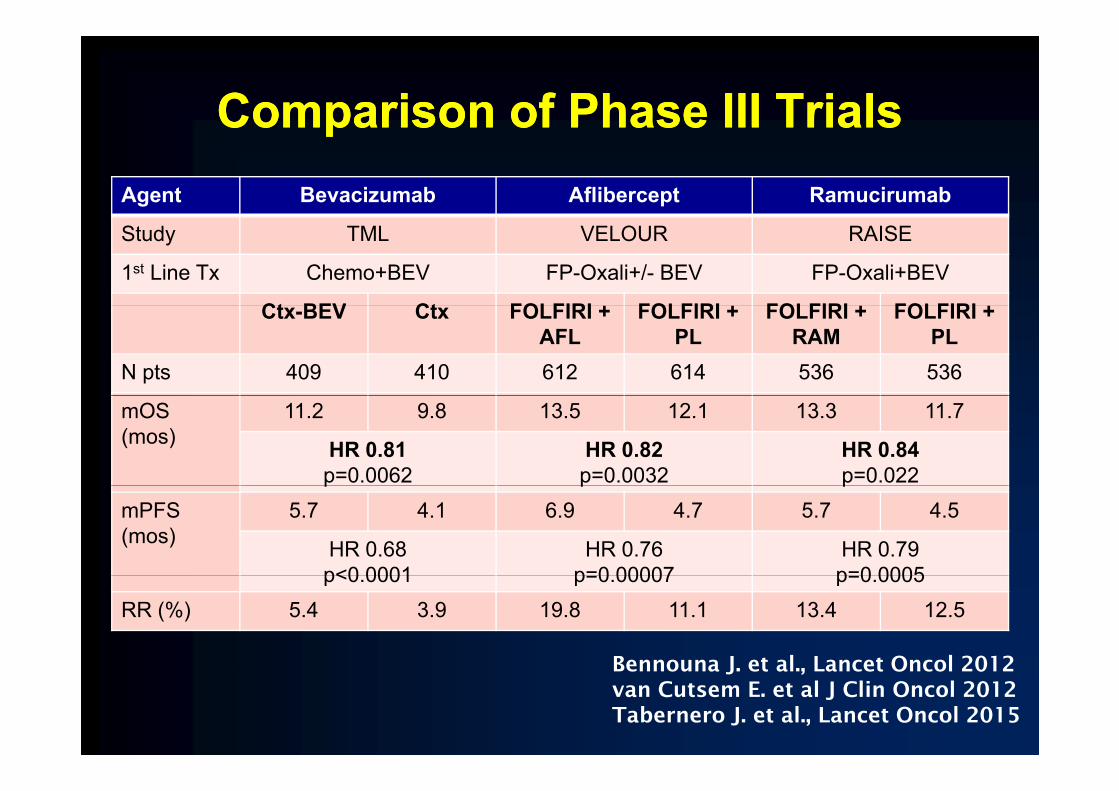
Comparison of Phase III TrialsComparison of Phase III TrialsComparison of Phase III TrialsComparison of Phase III TrialsAgent Bevacizumab Aflibercept Ramucirumab
Study TML VELOUR RAISE
1st Line Tx Chemo+BEV FP-Oxali+/- BEV FP-Oxali+BEV
Ct BEV Ct FOLFIRI + FOLFIRI + FOLFIRI + FOLFIRI +Ctx-BEV Ctx FOLFIRI + AFL
FOLFIRI + PL
FOLFIRI + RAM
FOLFIRI + PL
N pts 409 410 612 614 536 536
mOS(mos)
11.2 9.8 13.5 12.1 13.3 11.7
HR 0.81p=0.0062
HR 0.82p=0.0032
HR 0.84p=0.022p p p
mPFS(mos)
5.7 4.1 6.9 4.7 5.7 4.5
HR 0.68p<0 0001
HR 0.76p=0 00007
HR 0.79p=0 0005p<0.0001 p=0.00007 p=0.0005
RR (%) 5.4 3.9 19.8 11.1 13.4 12.5
Bennouna J et al Lancet Oncol 2012Bennouna J. et al., Lancet Oncol 2012van Cutsem E. et al J Clin Oncol 2012Tabernero J. et al., Lancet Oncol 2015
Antiangiogenic therapy beyond progression
•• The Chemotherapy partner is important
g g py y p g
•Optimal sequence in antiangiogenic switch is notdefineddefined• No data in the highly selected subgroup of patients
ith RAS d BRAF ild t twith RAS and BRAF wild-type tumours.•In 2015 need to assess and compare financialtoxicity• Is there a role for the combination of antiangiogenicIs there a role for the combination of antiangiogenicdrugs in MCRC?
I th l f flib t i b• Is there a role for aflibercept or ramucirumabbeyond second line?

CORRECT study designCORRECT study design
RAN
RAN
Regorafenib + BSC 160 mg orally once daily
Primary Endpoint:
mCRC after standard
NDOM I Z
NDOM I Z
g y y3 weeks on, 1 week off
2 : 1
Endpoint: OS
90% power to detect 33.3%
therapy ZAT I ON
ZAT I ON
Placebo + BSC 3 weeks on, 1 week off
detect 33.3% increase
(HR=0.75), with 1-sided overall
0 025
• Multicenter randomized double-blind placebo-controlled phase III• Multicenter randomized double-blind placebo-controlled phase III
NN ,α=0.025
• Multicenter, randomized, double-blind, placebo-controlled, phase III• 2:1 randomization• Strat. factors: prior anti-VEGF therapy, time from diagnosis of mCRC,
geographical region
• Multicenter, randomized, double-blind, placebo-controlled, phase III• 2:1 randomization• Strat. factors: prior anti-VEGF therapy, time from diagnosis of mCRC,
geographical region• Global trial: 16 countries, 114 active centers
• 1,052 patients screened, 760 patients randomized within 10 months• Secondary endpoints: PFS, ORR, DCR
• Global trial: 16 countries, 114 active centers• 1,052 patients screened, 760 patients randomized within 10 months
• Secondary endpoints: PFS, ORR, DCRSecondary endpoints: PFS, ORR, DCR• Tertiary endpoints: duration of response / stable disease, QOL, pharmacokinetics,
biomarkers
Secondary endpoints: PFS, ORR, DCR• Tertiary endpoints: duration of response / stable disease, QOL, pharmacokinetics,
biomarkersGrothey A. et al., Lancet 2012
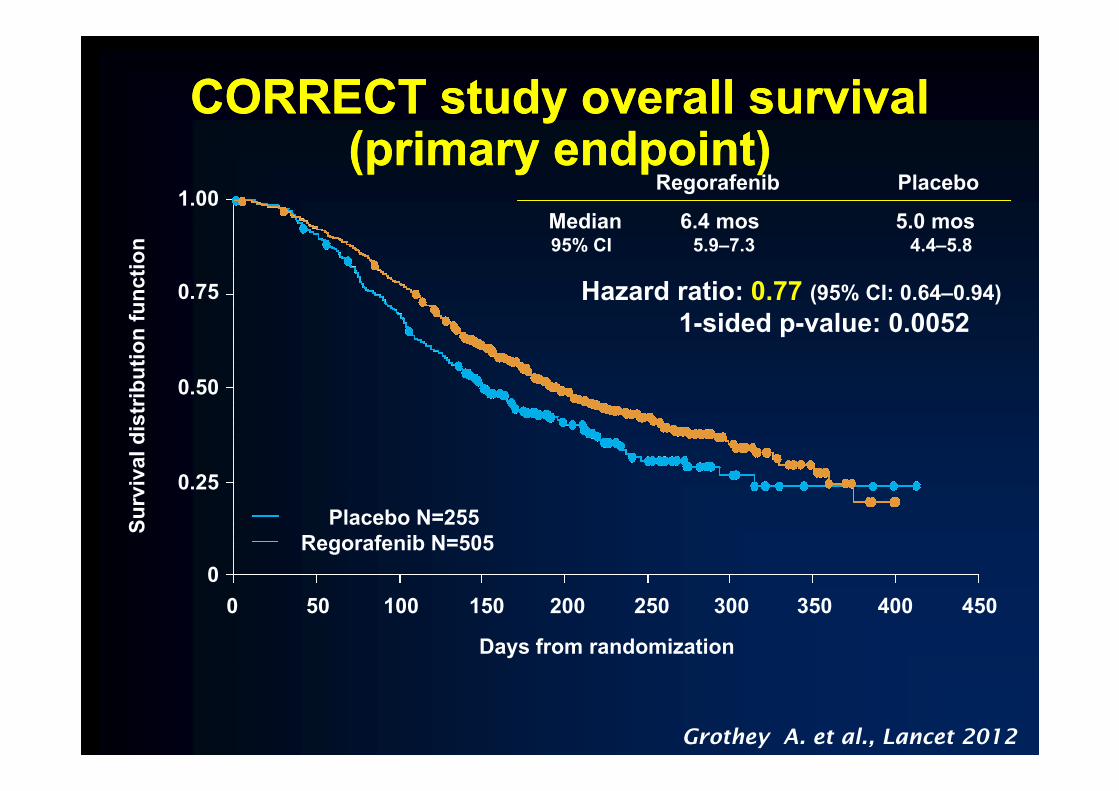
CORRECT study overall survival CORRECT study overall survival (primary endpoint)(primary endpoint)
1.00M di 6 4 5 0
Regorafenib Placebo
0.75
unct
ion
Median 6.4 mos 5.0 mos95% CI 5.9–7.3 4.4–5.8
Hazard ratio: 0.77 (95% CI: 0.64–0.94)
0.50ibut
ion
fu 1-sided p-value: 0.0052
0 25ival
dis
tri
0.25
0
Surv
Placebo N=255Regorafenib N=505
0200100500 150 300250 400350 450
Days from randomization
Grothey A. et al., Lancet 2012

Drug-Related Treatment-Emergent Adverse Drug-Related Treatment-Emergent Adverse g gEvents Occurring in ≥10% of Patientsg g
Events Occurring in ≥10% of PatientsAdverse Event %
Regorafenib (n = 500) Placebo (n = 253)Adverse Event, %
All grades Grade 3 Grade 4 All grades Grade 3 Grade 4Hand-foot skin reaction 46.6 16.6 0 7.5 0.4 0
Fatigue 47.4 9.2 0.4 28.1 4.7 0.4
Hypertension 27.8 7.2 0 5.9 0.8 0
Diarrhea 33.8 7.0 0.2 8.3 0.8 0
Rash/desquamation 26 0 5 8 0 4 0 0 0Rash/desquamation 26.0 5.8 0 4.0 0 0
Anorexia 30.4 3.2 0 15.4 2.8 0
Mucositis, oral 27.2 3.0 0 3.6 0 0
Thrombocytopenia 12.6 2.6 0.2 2.0 0.4 0
Fever 10.4 0.8 0 2.8 0 0
Nausea 14.4 0.4 0 11.1 0 0
Bleeding 11.4 0.4 0 2.8 0 0
Voice changes 29.4 0.2 0 5.5 0 0
Weight loss 13.8 0 0 2.4 0 0Weight loss 13.8 0 0 2.4 0 0
*Grade 5 drug-related AEs: 1.0% in regorafenib arm vs 0% in placebo arm
Grothey A, Van Cutsem E, et al. Lancet. 2013;381:303-312.

Conclusion anti-VEGF TherapyConclusion anti-VEGF TherapyConclusion anti VEGF TherapyConclusion anti VEGF Therapy• Clinical synergism between
fl i idi + b i b• Clinical synergism between
fl i idi + b i bfluoropyrimidine + bevacizumab
• BEV combinable with FOLFOXIRI (TRIBE)
fluoropyrimidine + bevacizumab
• BEV combinable with FOLFOXIRI (TRIBE)• BEV combinable with FOLFOXIRI (TRIBE)
• Duration of VEGF inhibition matters
• BEV combinable with FOLFOXIRI (TRIBE)
• Duration of VEGF inhibition matters• Duration of VEGF-inhibition matters• Maintenance strategies• Treatment beyond progression
• Duration of VEGF-inhibition matters• Maintenance strategies• Treatment beyond progressionTreatment beyond progression
• Three positive phase III trials for prolonged
Treatment beyond progression
• Three positive phase III trials for prolonged p p p gVEGF inhibition beyond progression
• No compelling arguments for aflibercept
p p p gVEGF inhibition beyond progression
• No compelling arguments for afliberceptp g g por ramucirumab over bevacizumab
p g g por ramucirumab over bevacizumab