SURVEY SUL CONFLITTO DI INTERESSE IN ONCOLOGIA...
86
SURVEY SUL CONFLITTO DI INTERESSE IN ONCOLOGIA PROMOSSO DAL CIPOMO 1-31 MARZO PARTECIPATE TUTTI www.cipomo.it ; nicsonet.it
Transcript of SURVEY SUL CONFLITTO DI INTERESSE IN ONCOLOGIA...

SURVEY SUL CONFLITTO DI INTERESSE IN ONCOLOGIA PROMOSSO DAL CIPOMO 1-31 MARZO
PARTECIPATE TUTTI www.cipomo.it; nicsonet.it

LINEE GUIDA AIOM: LA TERAPIA ANTIEMETICA
Fausto RoilaS.C. Oncologia Medica, Terni

CONFLICT OF INTEREST: DISCLOSURE
No conflict of interest

Coordinatore Fausto Roila AIOM Oncologia Medica - A.O. S.Maria - Terni
Segretario Lucia Mentuccia AIOM Oncologia Medica - Ospedale SS Trinità - Sora (FR)
Estensori Claudia Caserta AIOM Oncologia - A.O. Santa Maria - Terni
Sonia Fatigoni Oncologia - A.O. Santa Maria - Terni
Revisori Silvana Chiara AIOM Oncologia Medica - A.O.U. San Martino-IST - Genova
Alessandra Fabi AIOM Oncologia Medica I - I.F.O. Regina Elena - Roma
Maria Cristina Locatelli AIOM Oncologia Medica - A.O. S.Carlo Borromeo - Milano
Ernesto Maranzano AIRO Radioterapia oncologica - A.O. Santa Maria - Terni
Mimma Raffaele AIOM Oncologia - Inrca-Ist.naz.rip.e Cura Anziani - Roma

EMETOGENIC POTENTIAL OF SINGLEINTRAVENOUS CHEMOTHERAPY AGENTS
EMETIC RISK AGENT
HIGH
CisplatinMechlorethamineStreptozocinCyclophosphamide > 1500 mg/m2
CarmustineDacarbazineAC or EC regimens (breast cancer pts)

ANTIEMETICS FOR THE PREVENTION OF CISPLATIN-INDUCED ACUTE AND DELAYED EMESIS

day 1 days 2-3 day 4 Aprepitant 125 mg 80 mg -Ondansetron 32 mg - -Dexamethasone 12 mg 8 mg 8 mg
Ondansetron 32 mg - -Dexamethasone 20 mg 8 mg bid 8 mg bid
Aprepitant p.o. Ondansetron i.v. Dexamethasone p.o.
TWO RCT ON APREPITANT (2003)

Protocol 052 Protocol 054AOD OD AOD OD
No. pts 264 266 283 286
Complete response (%)
Day 1 89 78 11% 83 68 15%
Day 2-5 75 56 19% 68 47 21%
no nausea (%) 48 44 49 39
RESULTS

MASCC/ESMO 2010 RECOMMENDATIONS ON ANTIEMETIC PROPHYLAXIS
ACUTE DELAYED
Cisplatin 5HT3+DEX+Apr DEX+Apr

SINGLE-DOSE FOSAPREPITANT FOR THE PREVENTION OF CHEMOTHERAPY-INDUCED NAUSEA AND VOMITING ASSOCIATED WITH CISPLATIN THERAPY: RANDOMIZED, DOUBLE-BLIND STUDY PROTOCOL EASE
Grunberg S, et al. J Clin Oncol 2011; 29: 1495-501

D1 D2 D3 D4
Aprepitant po 125 mg 80 mg 80 mg -Ondansetron 32 mg - - -Dexamethasone 12 mg 8 mg 8 mg 8mg
Fosaprepitant iv 150 mg - - -Ondansetron 32 mg - - -Dexamethasone 12 mg 8mg 8 mg bid 8 mg bid
ondansetron iv desametasone po
STUDY DESIGN (2247 pts)

RESULTS (% COMPLETE RESPONSE)
FOD AOD pday 1 89.0 88.0 n.s.
days 2-5 74.3 74.2 n.s.
days 1-5 71.9 72.3 n.s.

Efficacy and safety of NEPA, an oral combination of netupitant and palonosetron, for prevention of chemotherapy-induced nausea and vomiting following highly emetogenic chemotherapy: a randomized dose-ranging pivotal study
Hesketh PJ, et al. Ann Oncol 2014; 25: 1340-1346

D1 D2-3 D4PALO Palo 0.50mg+ Dex 8 mg bid Dex 8 mg bid
Dex 20 mg po
NEPA100 netu100 +Palo Dex 4 mg bid Dex 4 mg bid+ Dex 12 mg po
NEPA200 netu200 +Palo Dex 4 mg bid Dex 4 mg bid+ Dex 12 mg po
NEPA300 netu300 +Palo Dex 4 mg bid Dex 4 mg bid+ Dex 12 mg po
APR+OND apr 125mg + Apr 80mg + Dex 4 mg bidOND 32mg iv + Dex 4 mg bidDex 12 mg po
DESIGN OF THE STUDY (694 pts)

D1-D5 D1 D2-D5PALO 76.5 89.7 80.1
NEPA100 87.4* 93.3 90.4*
NEPA200 87.6* 92.7 91.2*
NEPA300 89.6* 98.5* 90.4*
APR+OND 86.6 94.8* 88.8*
* Statistically significant with respect to PALO
RESULTS (% COMPLETE RESPONSE)

Safety and efficacy of rolapitant, for prevention of chemotherapy-induced nausea and vomiting after administration of cisplatin-based highly emetogenic chemotherapy in patients with cancer: two randomised, active-controlled, double-blind, phase III trials
Rapoport BL, et al. Lancet Oncol 2015; 16: 1079-89

D1 D2-3 D4 Rolapitant 200 mg - -Granisetron 10 µg/kg - -Dexamethasone 20 mg 8 mg bid 8 mg bid
Granisetron 10 µg/kg - -Dexamethasone 20 mg 8 mg bid 8 mg bid
Rolapitant po Granisetron iv Dexamethasone po
STUDY DESIGN

RGD GD P
Day 1 83.4 3.9% 79.5 n.s.
Day 2-5 70.1 8.2% 61.9 0.043
Day 1-5 67.5 60.4 n.s.
no nausea (%) 55.5 44.0 0.009
RESULTS (555 pts)

RGD GD P
Day 1 83.7 10% 73.7 0.005
Day 2-5 72.7 14.3% 58.4 <0.001
Day 1-5 70.1 56.5 <0.001
RESULTS (532 pts)

- The addition of an NK1 receptor antagonists in ptssubmitted to cisplatin chemotherapy increased the complete response on day 1 from 4% to 15% and on days 2-5 from 8% to 21%.
- Part of this increase is due to a dependence effect (the betterresults achieved on the day 1 which induced an increase of the complete responses on days 2-5)
CONCLUSIONS
APREPITANT VERSUS METOCLOPRAMIDE, BOTH COMBINED WITH DEXAMETHASONE, FOR THE PREVENTION OF CISPLATIN-INDUCED DELAYED EMESIS: A RANDOMIZED, DOUBLE-BLIND STUDY
Roila F, et al. Ann Oncol 2015; 26: 1248-1253

METHODSSTUDY DESIGN- A randomized double-blind study comparing aprepitant versus metoclopramide, both combined with dexamethasone, was carried out in naive cancer pts treated with cisplatin-based chemotherapy.-Before chemotherapy, all patients were treated with intravenous palonosetron 0.25 mg and dexamethasone 12 mg and oral aprepitant 125 mg
ANTIEMETIC TREATMENTS-Oral dexamethasone 8 mg once daily on days 2-4 plus aprepitant 80 mg daily on days 2-3-Oral dexamethasone 8 mg bid on days 2-4 plus metoclopramide 20 mg 4 times daily on days 2-4

RESULTS IN THE DELAYED PHASE (284 pts)MTC +
DEXAPR + DEX p
No. of patients (%) 137 (%) 147 (%)RESPONSEScomplete response 113 (82.5) 118 (80.3) n.s.
complete protection 102 (74.5) 108 (73.5) n.s.
total control 97 (70.8) 102 (69.4) n.s.
no vomiting 120 (87.6) 129 (87.8) n.s.
no nausea 100 (73.0) 105 (71.4) n.s.
no significant nausea (VAS < 25 mm)
111 (81.0) 114 (77.6) n.s.
mean number of emetic episodes (sd) 7.9 (7.4) 8.4 (11.8) n.s.
mean maximum severity of nausea (sd) 44.8 (25.5) 44.9 (26.2) n.s.
mean duration of nausea, hours (sd) 13.5 (16.5) 15.4 (19.0) n.s.
CONCLUSIONS
- Recently EMA reduced the dose and the duration of the antiemetic treatment with oral metoclopramide to 10 mg TID for maximum 1 week (risk of neurological side effects such asshort-term extrapyramidal disorders). Therefore, ourmetoclopramide regimen is not utilizable in the clinicalpractice.

MASCC/ESMO 2016 RECOMMENDATIONS
ACUTE DELAYEDCisplatin 5HT3+DEX+NK1 DEX
5HT3+DEX+APR DEX+APR or MTC

ANTIEMETICS FOR THE PREVENTION OF ACUTE AND DELAYED EMESIS INDUCED BY AC/EC REGIMENS

MASCC/ESMO 2010 RECOMMENDATIONS
ACUTE DELAYED
AC 5HT3+DEX+Apr Apr

D1 D2-3 Aprepitant 125 mg 80 mg Ondansetron 8/8 mg -Desametasone 12 mg -
Ondansetron 8/8 mg 8/8 mgDexamethasone 20 mg -
Aprepitant po Ondansetron po Dexamethasone po
Breast cancer ptstreated with CTX ± DOX or EPI (2005)
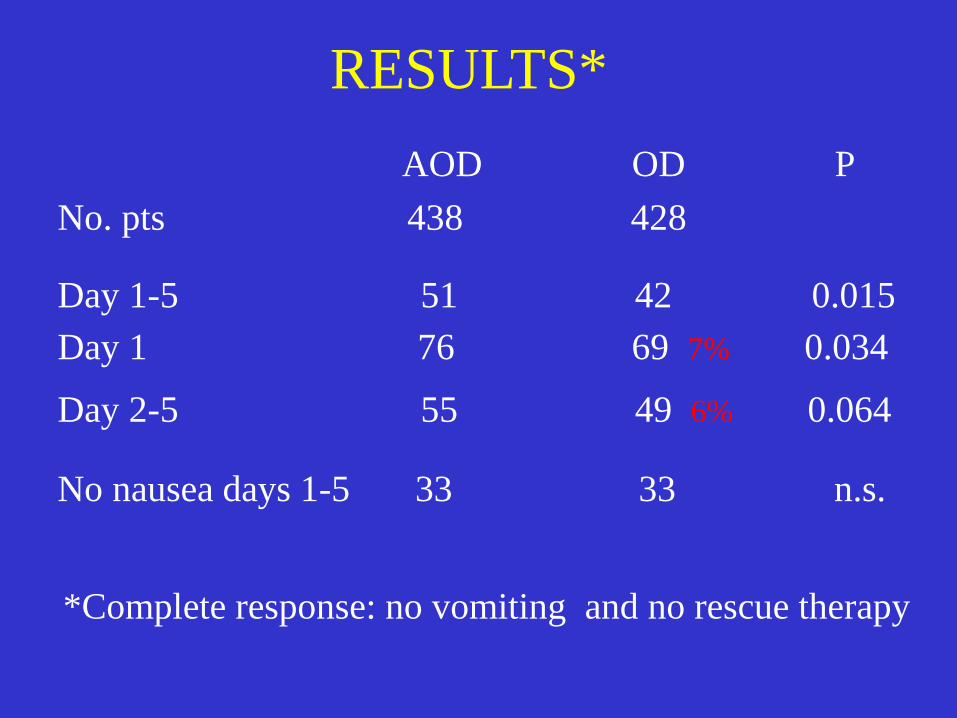
AOD OD P No. pts 438 428
Day 1-5 51 42 0.015Day 1 76 69 7% 0.034
Day 2-5 55 49 6% 0.064
No nausea days 1-5 33 33 n.s.
*Complete response: no vomiting and no rescue therapy
RESULTS*

A randomized phase III study evaluating the efficacy and safety of NEPA, a fixed-dose combination of netupitant and palonosetron, for prevention of chemotherapy-induced nausea and vomiting following moderately emetogenic chemotherapy
Aapro M, et al. Ann Oncol 2014; 25: 1328-1333

Double-blind, randomized study in chemotherapy-naive patients undergoing anthracycline-cyclophosphamide chemotherapy submitted to:
- oral NEPA + oral dexamethasone 12 mg(NEPA= NETU 300 mg + PALO 0.50 mg)
- oral PALO 0.50 mg + oral dexamethasone 20 mg
Primary endpoint: complete response during delayed phase
DESIGN OF THE STUDY (1455 pts)

D2-D5 D1 D1-D5
PALO + DEX 69.5 7.4% 85.0 3.4% 66.6
NEPA + DEX 76.9* 88.4** 74.3*
* P = 0.001** P = 0.047
RESULTS (% COMPLETE RESPONSE)
Safety and efficacy of rolapitant for prevention of chemotherapy-induced nausea and vomiting after administation of moderately emetogenic chemotherapy or anthacycline and cyclophosphamide regimens in patients with cancer: a randomised, active-controlled, double-blind, phase 3 trial
Schwartzberg LS et al. Lancet Oncol 2015; 16: 1071-78

D1 D2-3 Rolapitant 200 mg -Granisetron 2mg 2 mg Dexamethasone 20 mg
Granisetron 2 mg 2 mg Dexamethasone 20 mg
Rolapitant po Granisetron po Dexamethasone po Primary Endpoint: complete response on days 2-5
STUDY DESIGN (1332 pts)

RGD GD P
Day 1 83.5 3.2% 80.3 n.s.
Day 2-5 71.3 9.7% 61.6 <0.001
Day 1-5 68.6 57.8 <0.001
RESULTS (% complete response)

- The addition of an NK1 receptor antagonists increased the complete response in pts submitted to AC/EC on day 1 from 3% to 7% and on days 2-5 from 6% to 10%
- Part of this increase is due to a dependence effect (the better results achieved on the day 1 which induced an increase of the complete responses on days 2-5)
CONCLUSIONS

Aprepitant versus dexamethasone for preventing chemotherapy-induced delayed emesis in patients with breast cancer: a randomized double-blind study
Roila F, et al. J Clin Oncol 2014; 32: 101-106

METHODS- A randomized double-blind study comparing aprepitant versus dexamethasone was carried out in naive breast cancer patients treated with anthracyclines + cyclophosphamide
- Before chemotherapy, all patients were treated with intravenous palonosetron 0.25 mg and dexamethasone 8 mg plus oral aprepitant 125 mg
- On days 2 and 3 patients randomly received oral dexamethasone 4 mg bid or aprepitant 80 mg qd
Primary endpoint was rate of complete response (no vomiting, no rescue treatment) from days 2-5 after chemotherapy

RESULTS IN THE DELAYED PHASE (551 PTS)Dexameth. Aprepit. P
ValueNo. of patients (%) 273 (%) 278 (%)
Complete response 217 (79.5) 221 (79.5) n.s.
Complete protection 164 (60.1) 152 (54.7) n.s.
Total control 131 (48.0) 120 (43.2) n.s.
No vomiting 250 (91.6) 248 (89.2) n.s.
No nausea 134 (49.1) 122 (43.9) n.s.
No significant nausea 174 (63.7) 158 (56.8) n.s.
Mean number of emetic episodes (sd)* 5.7 (6.5) 9.2 (9.4) n.s.
Mean maximum severity of nausea (sd)° 42.8 (25.9) 45.5 (24.1) n.s.
Mean duration of nausea, hours (sd)° 14.1 (18.4) 16.6 (21.4) n.s.
* in patients who had delayed vomiting (dexamethasone: 23 patients; aprepitant: 30 patients)° in patients suffering from delayed nausea (dexamethasone: 139 patients; aprepitant: 156 patients)

- No comparative studies have been carried out to identify differences in efficacy and toxicity between the three NK-1 receptor antagonists.
- Therefore, when available, the choice may be dependent on the respective convenience and cost.
NK-1 RECEPTOR ANTAGONISTS

OLANZAPINE• Olanzapine is an antipsychotic approved drug that blocks
multiple neurotransmitters in the central nervous system: dopamine D1, D2, D3 receptors, serotonin 5-HT2a, 5.HT2c, 5-HT3 and 5-HT6 receptors, α1 adrenergic receptors, muscarinic receptors and histamine H1 receptors.
• Some phase II studies seems to suggest an important antiemetic activity

OLANZAPINE VERSUS APREPITANT FOR THE PREVENTION OF CHEMOTHERAPY-INDUCED NAUSEA AND VOMITING: A RANDOMIZED PHASE III STUDY
Navari RM , et al. J Support Oncol 2011; 9: 188-195

g. 1 g. 2 g. 3 g. 4 Aprepitant po 125 mg 80 mg 80 mg -Palonosetron iv 0.25 mg - - -Dexamethasone 12 mg 4mg bid 4mg bid 4mg bid
Olanzapine po 10 mg 10 mg 10 mg 10 mgPalonosetron iv 0.25 mg - - -Dexamethasone 20 mg - - -
dexamethasone iv on day 1 and orally on day 2-4
DESIGN OF THE STUDY (241 pts)

RESULTS (% COMPLETE RESPONSES)
OPD APD pDay 1 97.0 87.0 n.s.
Day 2-5 77.0 73.0 n.s.
Day 1-5 77.0 73.0 n.s.

SHORTCOMINGS• It is an open study
• Due to the small sample size, the study was only powered to investigate large differences such as a 15% difference in complete response on day 1-5.
• It was not defined if the study was designed as a superiority, non inferiority or equivalence study.
• An unplanned interim analysis was carried out but the significance level was not modified according to Bonferroni’s inequality.
OLANZAPINE FOR THE PREVENTION OF CHEMOTHERAPY-INDUCED NAUSEA AND VOMITING
Navari RM , et al. N Engl J Med 2016; 375: 134-42

DAY 1 2 3 4Fosaprepitant iv 150 mg - - -5-HT3 RA iv day 1 - - -Dexamethasone po 12 mg 8 mg 8 mg 8 mg
Olanzapine po 10 mg 10 mg 10 mg 10 mgFosaprepitant iv 150 mg - - -5-HT3 RA iv day 1 - - -Dexamethasone po 12 mg 8 mg 8mg 8 mg
DESIGN OF THE STUDY (380 pts)

RESULTS (% NO NAUSEA)
OFPD FPD pDay 1 73.8 45.3 <0.001
Day 2-5 42.4 25.4 0.001
Day 1-5 37.3 21.9 0.002

RESULTS (% COMPLETE RESPONSES)
OFPD FPD pDay 1 85.7 64.6 <0.001
Day 2-5 66.9 52.4 0.007
Day 1-5 63.6 51.8 <0.001
A DOUBLE-BLIND RANDOMIZED PHASE II STUDY OF 10 MG VERSUS 5 MG OLANZAPINE FOR EMESIS INDUCED BY HIGHLY EMETOGENIC CHEMOTHERAPY WITH CISPLATIN
Hashimoto H, et al. J Clin Oncol 2016; 34 (suppl; abstr 10111)

GIORNO 1 2 3 4Olanzapina os 5 mg 5 mg 5 mg 5 mgAprepitant os 125 mg 80 80Palonosetron ev 0.75 mg - - -Desametasone os 9.9 mg 6.6 mg 6.6 mg 6.6 mg
Olanzapina os 10 mg 10 mg 10 mg 10 mgAprepitant os 125 mg 80 80 -Palonosetron ev 0.75 mg - - -Desametasone os 9.9 mg 6.6 mg 6.6 mg 6.6 mg
DISEGNO DELLO STUDIO (153 pts)

RESULTS (% COMPLETE RESPONSES)
OFPD 10mg OFPD 5mg pDay 1 100.0 98.7 n.sDay 2-5 77.6 85.7 n.s.Day 1-5 77.6 85.7 n.s
Sedation 53.3 45.5 n.s

ANTIEMETICS FOR THE PREVENTION OF ACUTE AND DELAYED EMESIS INDUCED BY MODERATELY
EMETOGENIC CHEMOTHERAPY

EMETIC RISK AGENT
MODERATE
OxaliplatinCytarabine > 1 gr/m2
CarboplatinIfosfamideCyclophosphamide < 1500 mg/m2
DoxorubicinDaunorubicinEpirubicinIdarubicinIrinotecanBendamustineAlentuzumabAzacitidine
EMETOGENIC POTENTIAL OF SINGLEINTRAVENOUS CHEMOTHERAPY AGENTS

MODERATELY EMETOGENIC CHEMOTHERAPY
• The category of MEC includes antineoplastic agents with a very large risk of emesis (30% to 90%) if no antiemetics are used. This broad range makes it difficult to give one recommendation for antiemetic treatment that is appropriate for all the drugs of this category.

• For the prevention of acute emesis induced by MEC we have to use a 5-HT3 antagonist plus dexamethasone
• In pts receiving MEC with known potential for delayed emesis (e.g., oxaliplatin, doxorubicin, cyclophosphamide), the use of dexamethasone for days 2-3 can be considered. No routine prophylaxis can be recommended for all other pts receiving MEC.
2016 MASCC/ESMO RECOMMENDATIONS
NK1 ANTAGONISTS FOR THE PROPHYLAXIS OF CARBOPLATIN-INDUCED ACUTE AND DELAYED
EMESIS

NK1 ANTAGONISTS FOR CARBOPLATIN-BASED CT
• Six studies evaluated the role of the addition of a NK1antagonist to a 5-HT3 antagonist plus dexamethasonein carboplatin-treated pts.
• Three of the six studies presented a subgroup analysisor post hoc analysis of studies involving both AC andnon-AC-treated pts.
• In these studies the addition of an NK1 antagonistincreased the complete response by approximately 10-15%.

NK1 ANTAGONISTS FOR CARBOPLATIN-BASED CT
• In a phase III, double-blind study, 297 naїve patientswith ovarian, endometrial and cervical cancerscheduled to receive carboplatin plus paclitaxel, wererandomized patients to aprepitant or placebo, bothcombined to a 5-HT3 antagonist plus dexamethasone(Yahata H, Int J Clin Oncol 2016; 21: 491-497)
• The primary endpoint was complete response, novomiting and no significant nausea on days 2-5.

NK1 ANTAGONISTS FOR CARBOPLATIN-BASED CT
• All the primary endpoints were significantly superiorwith the addition of aprepitant (complete response61.6% versus 47.3%, no vomiting 78.2% versus 54.8%and no significant nausea 85.4% versus 74.7%).

• For the prevention of carboplatin-induced acute nausea and vomiting a combination of a NK1 antagonist, dexamethasone and a 5-HT3 antagonist is recommended
• If patients received fosaprepitant, netupitant or rolapitant on day 1, no antiemetic prophylaxis for delayed emesis is required. If pts received aprepitanton day 1, aprepitant on days 2 and 3 is recommeded
2016 MASCC/ESMO RECOMMENDATIONS

MASCC/ESMO 2016 RECOMMENDATIONS
ACUTE DELAYEDCarboplatin 5HT3+DEX+NK1 -
5HT3+DEX+APR APR
Oxaliplatin 5HT3+DEX DEX*
Other MEC 5HT3+DEX DEX*
* In pts receiving MEC with known potential for delayed emesis
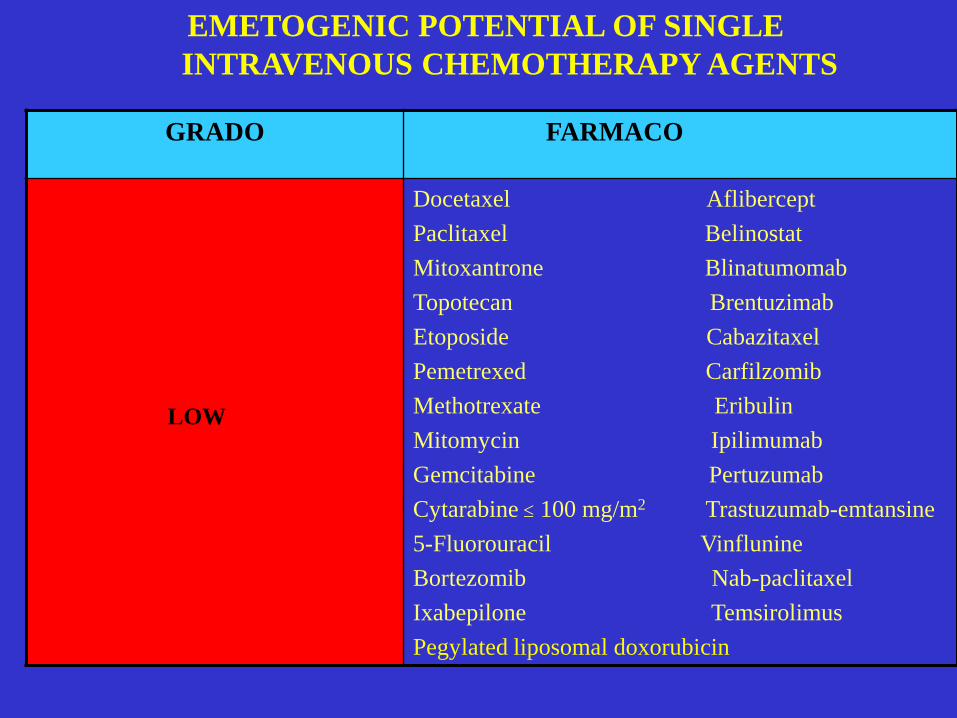
EMETOGENIC POTENTIAL OF SINGLEINTRAVENOUS CHEMOTHERAPY AGENTS
GRADO FARMACO
LOW
Docetaxel AfliberceptPaclitaxel BelinostatMitoxantrone BlinatumomabTopotecan BrentuzimabEtoposide CabazitaxelPemetrexed CarfilzomibMethotrexate EribulinMitomycin IpilimumabGemcitabine PertuzumabCytarabine ≤ 100 mg/m2 Trastuzumab-emtansine5-Fluorouracil VinflunineBortezomib Nab-paclitaxelIxabepilone TemsirolimusPegylated liposomal doxorubicin

MASCC/ESMO 2016 RECOMMENDATIONS
ACUTE DELAYEDLow emetogenic DEX or 5HT3 -chemotherapy or a dopamine RA

EMETOGENIC POTENTIAL OF SINGLEINTRAVENOUS CHEMOTHERAPY AGENTS
GRADO FARMACO
MINIMAL
BleomycinBusulfan2-ChlorodeoxyadenosineFludarabineVinblastineVincristineVinorelbineNivolumabOfatumumabPembrolizumabPixantronePralatrexateBevacizumab

MASCC/ESMO 2016 RECOMMENDATIONS
ACUTE DELAYEDMinimal emetogenic no antiemetics no antiemeticschemotherapy

RECOMMENDED DOSES OF 5-HT3 RAAgent Route Antiemetics
Ondansetron IV 8 mg or 0.15 mg/kgoral 16 mg
Granisetron IV 1 mg or 0.01 mg/kgoral 2 mg (or 1mg)
Dolasetron oral 100 mg
Tropisetron IV 5 mgoral 5 mg
Palonosetron IV 0.25 mgoral 0.5 mg

RECOMMENDED DOSES OF DEXAMETHASONE
dexamethasone dose and scheduleHigh risk
acute emesis 20 mg once [12 mg when used fos(aprepitant)or netupitant]
delayed emesis 8 mg bid for 3-4 days [8 mg once daily whenused with (fo)aprepitant or netupitant]
Moderate riskacute emesis 8 mg oncedelayed emesis 8 mg daily (or 4 mg bid) for 2-3 days
Low riskacute emesis 4 – 8 mg once

RECOMMENDED DOSES OF NK1 RANK1 receptor antagonist dose and scheduleAprepitant and fosaprepitant
acute emesis APR 125 mg once on the day of CT oror FOS 150 mg iv once on the day of CT
delayed emesis 80 mg orally once daily for the 2 daysafter CT; or none if FOS is used
Rolapitant 180 mg orally once on the day of CT
Netupitant 300 mg netupitant/0.5 mg palonosetronorally once on the day of CT

PREVENTION OF NAUSEA AND VOMITING INDUCED BY MULTIPLE-DAY CISPLATIN
CHEMOTHERAPY

Randomized Phase III Double-Blind Placebo-Controlled Crossover Study Evaluating the Oral Neurokinin-1 Antagonist Aprepitant in Combination with a 5HT3 Receptor Antagonist and Dexamethasone in Patients with Germ Cell Tumors Receiving 5 day Cisplatin CombinationChemotherapy Regimens: a Hoosier Oncology Group (HOG) Study
Albany C, et al, J Clin Oncol 2012; 30: 3998-4003

day 1-2 day 3 day 4-5 day 6-7 day 8 Aprepitant ─ 125 mg 80 mg 80 mg ─5-HT3 r.a. ● ● ● ─ ─Dex 20 mg ─ ─ 4mgx2 4mgx2
Placebo ─ ● ● ● ─5-HT3 r.a. ● ● ● ─ ─Dex 20 mg ─ ─ 8mgx2 4mgx2
oral aprepitant 5-HT3 iv oral dexamethasone
DESIGN OF THE STUDY (69 PTS)

RESULTS (% COMPLETE RESPONSE)
APR PL pDay 1-5 47.0 15.0 <0.0001
Day 6-8 63.0 35.0 <0.0004
Day 1-8 42.0 13.0 <0.0001

MASCC/ESMO 2016 RECOMMENDATIONS
ACUTE DELAYEDMultiple-day CDDP NK1+5HT3+DEX DEX chemotherapy

BREAKTHROUGH CHEMOTHERAPY-INDUCED EMESIS AND REFRACTORY EMESIS

MASCC/ESMO 2016 RECOMMENDATIONS
Breakthrough CT-induced - olanzapineEmesis
Refractory emesis - another 5-HT3 - add DA or benzodiazepines- metopimazine- NK1 antagonist

PREVENTION OF ANTICIPATORY NAUSEA AND VOMITING

MASCC/ESMO 2016 RECOMMENDATIONS
Anticipatory nausea - use the best control of acute andand vomiting delayed nausea and vomiting
- benzodiazepines (alprazolam,diazepam and lorazepam)
- behavioural therapies (progressivemuscle relaxation training, hypnosisand systematic desensitisation

PREVENTION OF NAUSEA AND VOMITING INDUCED BY HIGH-DOSE CHEMOTHERAPY

MASCC/ESMO 2016 RECOMMENDATIONS
ACUTE DELAYEDHigh dose CT APR+5HT3+DEX APR

PREVENTION OF RADIOTHERAPY-INDUCED NAUSEA AND VOMITING
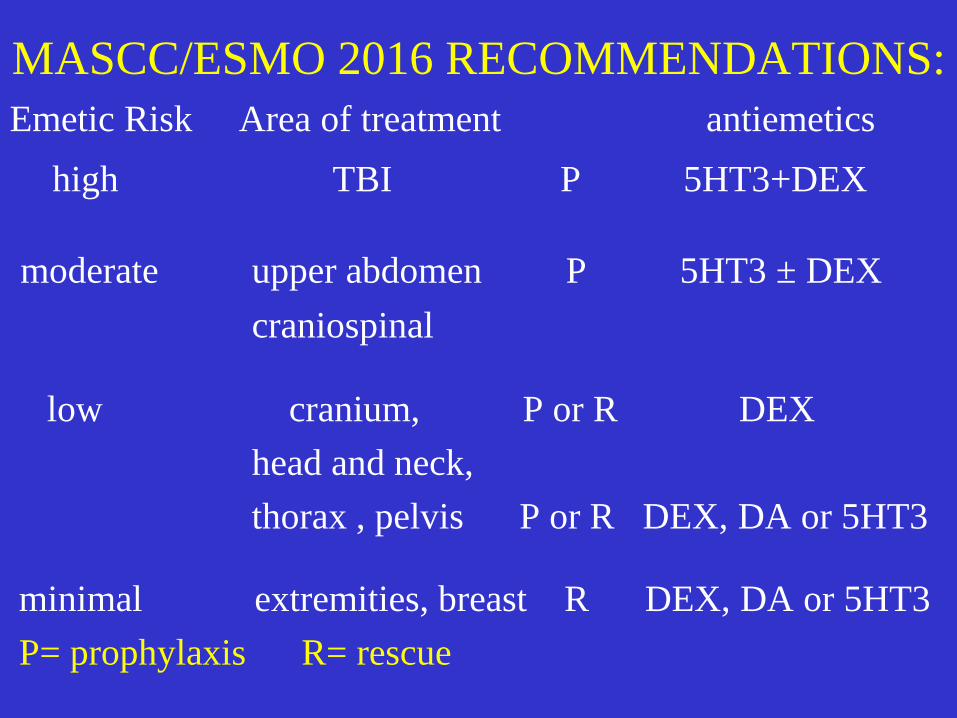
MASCC/ESMO 2016 RECOMMENDATIONS: Emetic Risk Area of treatment antiemetics
high TBI P 5HT3+DEX
moderate upper abdomen P 5HT3 ± DEXcraniospinal
low cranium, P or R DEX head and neck, thorax , pelvis P or R DEX, DA or 5HT3
minimal extremities, breast R DEX, DA or 5HT3P= prophylaxis R= rescue
MASCC/ESMO 2016 RECOMMENDATIONS:
Emetic Risk = concomitant chemo-radiotherapy
antiemetic prophylaxis should be according to the guidelinesfor chemotherapy-induced nausea and vomiting. However, in case the emetic risk of RT is higher than that of the concomitant CT, then the risk level of RT has to be chosento tailor the antiemetic regimen

EFFICACY AND SAFETY OF FOSAPREPITANT FOR THE PREVENTION OF NAUSEA AND EMESIS DURING 5 WEEKS OF CHEMORADIOTHERAPY FOR CERVICAL CANCER (THE GAND-EMESIS STUDY): A MULTINATIONAL, RANDOMISED, PLACEBO-CONTROLLED, DOUBLE-BLIND, PHASE 3 TRIAL
Ruhlmann CH , et al. Lancet Oncol 2016;

- Fosaprepitant vs placebo in 246 cervical cancer pts submitted to fractionated radiotherapy and weekly CDDP (40 mg/m2) for 5 weeks. All pts received palonosetron 0.25 mg iv and oral DEX 16 mg before CDDP and oral DEX 8 mg bid on day 2, 4mg bid on day 3 and 4 mg on day 4. The antiemetic treatment was repeated for 5 weeks
- Primary endpoint: proportion of pts with sustained no emesis after 5 weeks
STUDY DESIGN

- The proportion of pts with sustained no emesis after 5 weeks was significantly superior with fosaprepitant (65.7% vs 48.7%).
- Fosaprepitant was superior even in the day 1- day 35 rates of complete response, no emesis, no nausea and no rescue medication.
- Antiemetic treatments were generally well tolerated
RESULTS