Strategie terapeutiche: Esperienze ed opinioni a confrontochped.it/gico/rel cisti ovariche lelli...
31
CATTEDRA e U.O. DI CHIRURGIA PEDIATRICA CATTEDRA e U.O. DI CHIRURGIA PEDIATRICA U.O. DI CLINICA OSTETRICO U.O. DI CLINICA OSTETRICO - - GINECOLOGICA GINECOLOGICA UNIVERSITA’ DEGLI STUDI “G. D’ANNUNZIO” CHIETI UNIVERSITA’ DEGLI STUDI “G. D’ANNUNZIO” CHIETI - - PESCARA PESCARA XXXVIII Congresso Nazionale S.I.C.P. Riunione del Gruppo di Studio di Chirurgia Oncologica Firenze 27 Settembre 2007 Celentano Celentano C., Lelli Chiesa P., Lisi G. C., Lelli Chiesa P., Lisi G. Lesioni cistiche dell’ovaio in epoca neonatale, prepubere, adolescenziale Strategie terapeutiche: Esperienze ed opinioni a confronto
Transcript of Strategie terapeutiche: Esperienze ed opinioni a confrontochped.it/gico/rel cisti ovariche lelli...

CATTEDRA e U.O. DI CHIRURGIA PEDIATRICACATTEDRA e U.O. DI CHIRURGIA PEDIATRICA
U.O. DI CLINICA OSTETRICOU.O. DI CLINICA OSTETRICO--GINECOLOGICAGINECOLOGICA
UNIVERSITA’ DEGLI STUDI “G. D’ANNUNZIO” CHIETI UNIVERSITA’ DEGLI STUDI “G. D’ANNUNZIO” CHIETI -- PESCARAPESCARA
XXXVIII Congresso Nazionale S.I.C.P.Riunione del Gruppo di Studio di Chirurgia Oncologica
Firenze 27 Settembre 2007
XXXVIII Congresso Nazionale S.I.C.P.Riunione del Gruppo di Studio di Chirurgia Oncologica
Firenze 27 Settembre 2007
CelentanoCelentano C., Lelli Chiesa P., Lisi G.C., Lelli Chiesa P., Lisi G.
Lesioni cistiche dell’ovaioin epoca neonatale, prepubere, adolescenziale
Strategie terapeutiche:Esperienze ed opinioni a confronto
Lesioni cistiche dell’ovaioin epoca neonatale, prepubere, adolescenziale
Strategie terapeutiche:Esperienze ed opinioni a confronto

CISTI OVARICHE NEONATALI
OPZIONI TERAPEUTICHEOPZIONI TERAPEUTICHE
•• aspirazione prenataleaspirazione prenatale
•• aspirazione percutanea aspirazione percutanea postnatale postnatale
•• waitwait and and seesee
•• intervento chirurgicointervento chirurgicoLaparotomicoLaparotomico
LaparoscopicoLaparoscopico
aspirazioneaspirazione
fenestraturafenestratura
marsupializzazionemarsupializzazione
cistectomiacistectomia
ovariectomiaovariectomia
annessectomiaannessectomia
Cisti ovariche fetali
Aspirazione prenataleAspirazione prenatale
Brandt and Helmrath, 2005
“There are no good data to support
the effectiveness of prenatal aspiration
in preventing ovarian torsion, and concern by
many physicians exists regarding the risk of
the procedure to both fetus and mother.”

Cisti ovariche neonatali
Aspirazione percutanea Aspirazione percutanea postnatalepostnataleCONTRO
Rischi associati significativi (in caso di diagnosi non certa)
Risultati non superiori al wait and see*
Rischio torsione postnatale già basso
No nella cisti complex (emorragia – peritonite)
PRO
Mini invasiva
rischio torsione
morbidità
rischio recidiva
INDICAZIONI Cisti massive semplici sintomatiche
(insufficienza respiratoria o compressione cavale)
*“There are no good prospective data to confirm that aspiration is more effective than simple observation.” Brandt and Helmrath, 2005
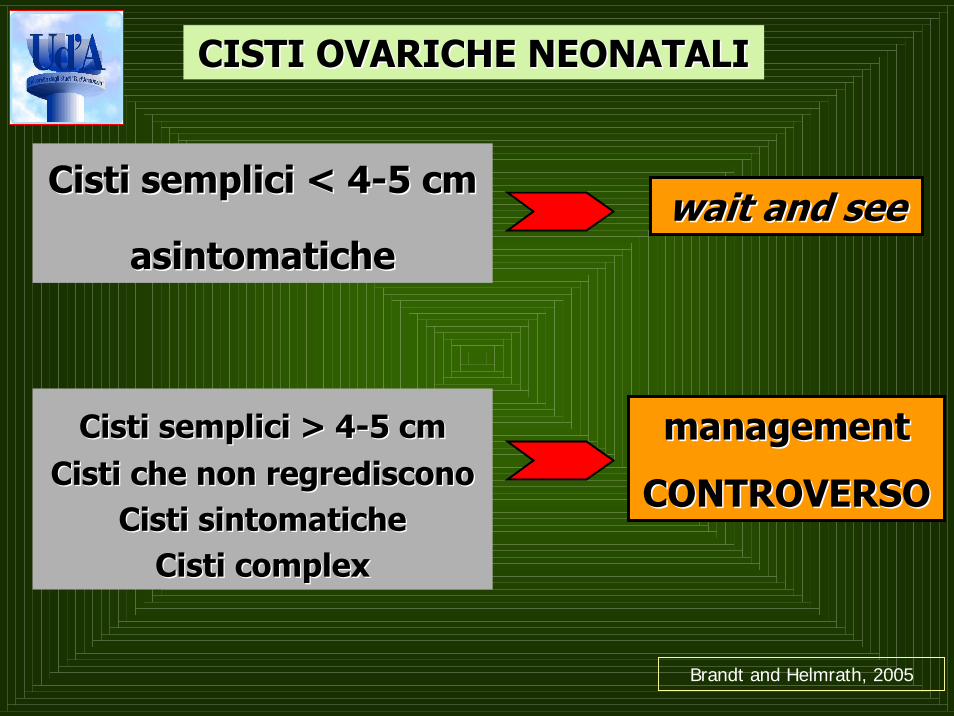
CISTI OVARICHE NEONATALICISTI OVARICHE NEONATALI
Cisti semplici < 4Cisti semplici < 4--5 cm5 cm
asintomaticheasintomatichewaitwait and and seesee
Cisti semplici > 4Cisti semplici > 4--5 cm5 cmCisti che non regrediscono Cisti che non regrediscono
Cisti sintomatiche Cisti sintomatiche Cisti Cisti complexcomplex
managementmanagement
CONTROVERSOCONTROVERSO
Brandt and Helmrath, 2005

* Cisti ovarica di diametro > 5 cm stabile al monitoraggio US
CISTI OVARICHE NEONATALI ≥≥5 cm o 5 cm o complexcomplex(casistica 2000-2007)
17
8
semplici
9
complex
Wait and see
Intervento chirurgico 2*
Risoluzione6

CISTI OVARICHE NEONATALI
TRATTAMENTO CHIRURGICO
LAPAROTOMIA
9
LAPAROSCOPIA
2
1 Cisti complexDetorsione
Ovariectomia TU
1 cisti semplice
(Ø 5 cm)
Unroofing
8 Cisti complex 1 cisti semplice
(Ø 7 cm)
“Cistectomia”
(assenza tessuto ovarico residuo)
7 Ovariectomia
1 Cistectomia
11

“Expected cyst resolution is 50% by 1 month, 75% by 2 months, and 90% by 3 months of age.”
Strickland J., 2004
“…resolution of a cyst may take considerable time, even up to 10 months, particularly for larger cysts.”
Chiaramonte et al, 2001
waitwait and and seeseeFINO A QUANDO ?FINO A QUANDO ?
“Since the incidence of malignancy in neonatal cysts approaches zero, postnatal management for asymptomatic, simple cyst involves observation with regular ultrasound review.” Templeman C, Strickland J, 2004

TRATTAMENTO DI ATTESATRATTAMENTO DI ATTESA
PREREQUISITIPREREQUISITI
1. cisti sicuramente di origine ovarica
2. no chiara componente solida alla ecografia (per quanto debris e setti da
emorragia siano accettabili)
3. α-fetoproteine (?) e βHCG normali
4. paziente asintomatica
CISTI OVARICHE NEONATALI
Masse cistiche addominali neonatali
Diagnosi differenziale
• Duplicazione intestinale
• Cisti mesenterica
• Cisti omentale
• Cisti del coledoco
• Pseudocisti meconiale
• Linfangioma
• Cisti del dotto onfalomesenterico
• Cisti renali ed ureterali
• Cisti epatiche
• Cisti uracale
• Idrometrocolpo
• Mielomeningocele anteriore

“There is general consensus that
cysts larger than 5 cm in diameter may be
at increased risk of torsion.”Nyberg DA et al, 2002

30 sett e.g.
36 x 35 mm
34 sett e.g.
59 x 50 mm
7 gg di vita
40 x 37 mm27 gg di vita
35 x 26 mm
67 gg di vita
18 x 13 mm

CISTI OVARICHE FETALI/NEONATALI
TORSIONETORSIONE27 – 78%40% ?
•• aderenze infiammatorieaderenze infiammatorie occlusione intestinaleocclusione intestinale
•• emorragia emorragia intracisticaintracistica
•• rottura della cistirottura della cisti
•• ostruzioni vie urinarieostruzioni vie urinarie
•• autoauto--amputazione della cistiamputazione della cisti
•• PeritonitePeritonite
•• (S.I.D.S.)(S.I.D.S.)
ascite
peritonite


“….Cysts with torsion sometimes adhere to the
bowel loops, which may lead to other complications such as
intestinal obstruction and/or rupture with peritonitis. For
these reasons we believe that surgical interventionshould be performed as early as possible if torsion is
suspected.” Kuroiwa M. et al, 2004
“In patients with presumed prenatal torsion who
subsequently have two ovaries on US, hemorrhage into the cyst,
rather than torsion may have been responsible for the initial
sonographic appearance. Alternatively, viable ovarian tissue may
have been prevent despite the torsion, allowing recovery of the
ovary with time.” Brandt and Helmrath, 2005

“Given the large number of cases that end in oophorectomy in some surgical series, it is not apparent that surgery offers any advantages over expectant management.”
“The decision to observe, rather than surgically treat neonatal cysts is supported by data that show that surgical intervention most often leads to oophorectomy, rather than an ovarian sparing procedure.”
Brandt and Helmrath, 2005
Nyberg DA et al, 2002




CISTI OVARICHE IN PAZIENTI PREPUBERI
TERAPIA
“Because of the present, albeit low risk of
malignancy , any ovarian cyst in the
prepubertal child that persist or is complexwarrants surgical resection.” Brandt and Helmrath, 2005
“The management will depend upon the diagnosis however: preservation of ovarian tissue should be the primary concern.” Templemann C, 2004

4 CISTI OVARICHE in età PREPUBERALE
Età media 5.2 a.; range 1.8-9.5 a.
TRATTAMENTO CHIRURGICO
LAPAROTOMIA
3 CASILAPAROSCOPIA
1 CASO
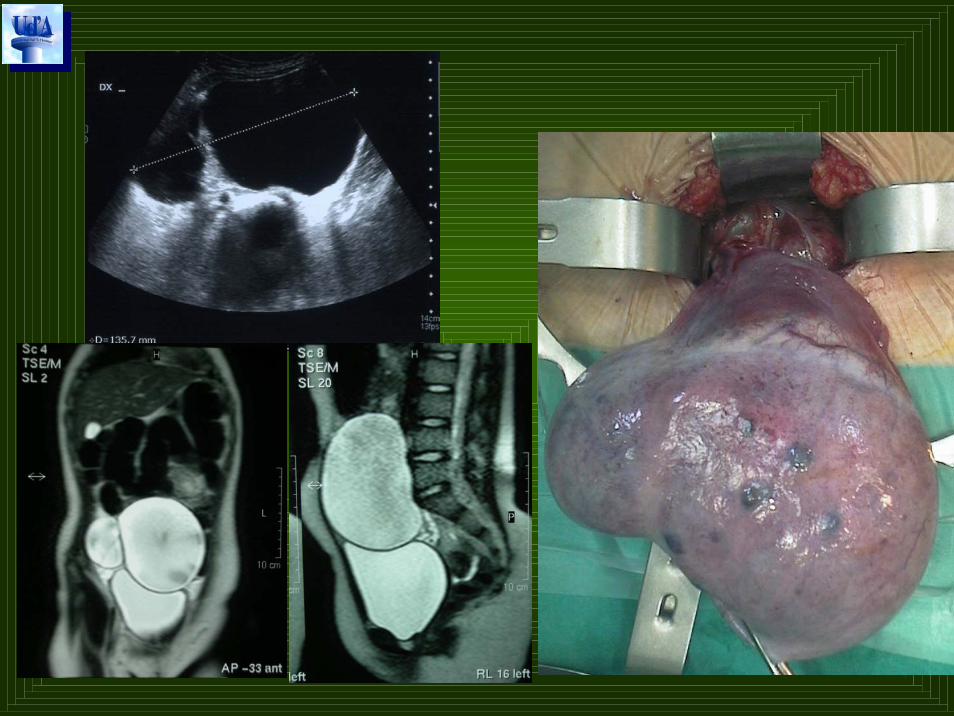
1 cisti US semplice con sottili setti interni (Ø 13 x 11 cm)
RMN:
Markers nella norma
DetensioneUnroofing
1 Cisti ovaricatorta (Ø 6 cm)
2 masse ovarichesolido-cistiche
(Ø 10 x 6 cm)
1 Ovariectomia
1 Salpingovariectomia
Ovariectomia
4 TERATOMI CISTICI OVARICI
3 MATURI - 1 IMMATURO (grado 1)
2nd lookovariectomia

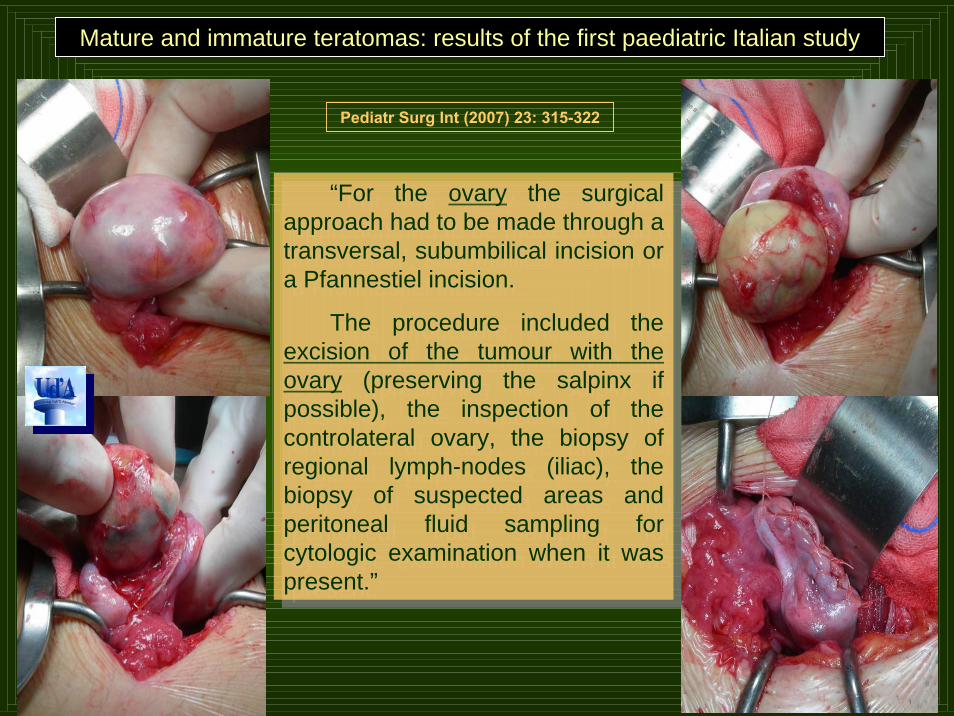
“For the ovary the surgicalapproach had to be made through a transversal, subumbilical incision or a Pfannestiel incision.
The procedure included the excision of the tumour with the ovary (preserving the salpinx if possible), the inspection of the controlateral ovary, the biopsy of regional lymph-nodes (iliac), the biopsy of suspected areas and peritoneal fluid sampling forcytologic examination when it waspresent.”
“For the ovary the surgicalapproach had to be made through a transversal, subumbilical incision or a Pfannestiel incision.
The procedure included the excision of the tumour with the ovary (preserving the salpinx if possible), the inspection of the controlateral ovary, the biopsy of regional lymph-nodes (iliac), the biopsy of suspected areas and peritoneal fluid sampling forcytologic examination when it waspresent.”
Mature and immature teratomas: results of the first paediatric Italian study
Pediatr Surg Int (2007) 23: 315-322

Quint E.H., Smith Y.R.
Ovarian surgery in premenarchal girlsJ Pediatr Adolesc Gynecol 12: 27, 1999
“Torsion was the most common diagnosis in
our study group and was usually unsuspected.
Premenarchal ovarian surgery usually included
removal of the entire ovary. However, because
malignancies are uncommon in this population
(9.6%), a cystectomy should be considered
when appropriate and technically feasible.”

“Conservative management with untwisting the ovary and pexing both retained detorsed and controlateral ovaries especially in idiopathic torsions should be considered in cases of ovarian torsion in children.”
Celik A. et al
Long-term results of conservative management of adnexal torsion in children
J Pediat Surg 40: 704, 2005
Aziz D. et al
Ovarian torsion in children: is oophorectomy necessary?J Pediat Surg 39: 750, 2004
“…Detorsion is the procedure of choice for most cases
of ovarian torsion.”


Torsione cisti ovarica
OOFORECTOMIA
Appendicectomia? SI
Fissazione ovaio residuo? ???*
*“Because the long-term effect of oophoropexy on fertility is uncertain,
it may be reasonable to recommend controlateral oophoropexy only when a
normal appearing ovary has torsed, and this situation may be difficult to assess
at surgery.” Quint E.H., Smith Y.R., 1999

GRAZIE PER LA VOSTRA ATTENZIONE !