Stato arte trattamenti - studio-vedette.it arte trattamenti.pdf · Stato dell’arte dei...
75
Stato dell’arte dei trattamenti contributo di VEdeTTE Pier Paolo Pani Medicina Tossicodipendenze Ser.T. AUSL 8, Cagliari
Transcript of Stato arte trattamenti - studio-vedette.it arte trattamenti.pdf · Stato dell’arte dei...

Stato dell’arte dei trattamenticontributo di VEdeTTE
Pier Paolo PaniMedicina TossicodipendenzeSer.T. AUSL 8, Cagliari

PREVALENZA USO DI DROGHE NELLA POPOLAZIONE GENERALE
(USO NELLA VITA ITALIA 2004)
Cannabis
CocainaEroina
0
15
30
45Prevalenza %
Uso nella vita

EroinaCocaina(USA) Cocaina
(Olanda)
0
20
40
60
80
100
%
DIPENDENZA: PREVALENZA FRA I CONSUMATORI
dipendenza
uso
Cohen, 1990; NSDUH, 2003.

AddictionA chronic but A chronic but
treatabletreatable conditioncondition
But “relapses” are common But “relapses” are common ----like some medical problems!like some medical problems!

August Vollmer, Police Administrator, 1936

OPIOID ADDICTION: GENERAL STATEMENT
Any treatment (methadone maintenance, therapeuticcommunity, drug-free treatment) is better thennothing.
The effects of treatment tend to be less evident after leaving the program.

Myths about the treatment of addiction Charles P O'Brien, A Thomas McLellan
The Lancet 1996; 347: 237-40

COSTO DELLA TOSSICODIPENDENZA
0
100
200
300
Euro al giorno
strada carcere Ser.T. Comunità

Components of Comprehensive Components of Comprehensive Drug Addiction TreatmentDrug Addiction Treatment
www.drugabuse.gov

Drug Abuse Reporting ProgramFirst National Evaluation of Treatment Effectiveness
Funded by the Funded by the National National
Institute on Institute on Drug AbuseDrug Abuse
Sells, Simpson, Sells, Simpson, DemareeDemaree, & Joe , & Joe 6 books & 150 papers published (funded 19706 books & 150 papers published (funded 1970--19901990))
1969-7335 Cities
139 Programs~44,000 Patients
All treatment typesFollow-ups: 1,3,6,12 Yrs

Drug Abuse Treatment Outcome StudiesThird National Evaluation of Treatment Effectiveness
Funded by the Funded by the National National
Institute on Institute on Drug AbuseDrug Abuse
1991-9311 Cities
96 Programs~10,000 Patients
All treatment typesFollow-up: 1 & 5 Yrs
60 Studies Published (or In Press)60 Studies Published (or In Press) ––Psychology of Addictive BehaviorsPsychology of Addictive Behaviors (Dec 97)(Dec 97)
Drug and Alcohol DependenceDrug and Alcohol Dependence (Dec 99) (Dec 99) Archives of General PsychiatryArchives of General Psychiatry (June 99; In press)(June 99; In press)
Journal of Adolescent Research Journal of Adolescent Research (In press)(In press)
53
64
52
29
53
3343 42
30
0
20
40
60
80
100
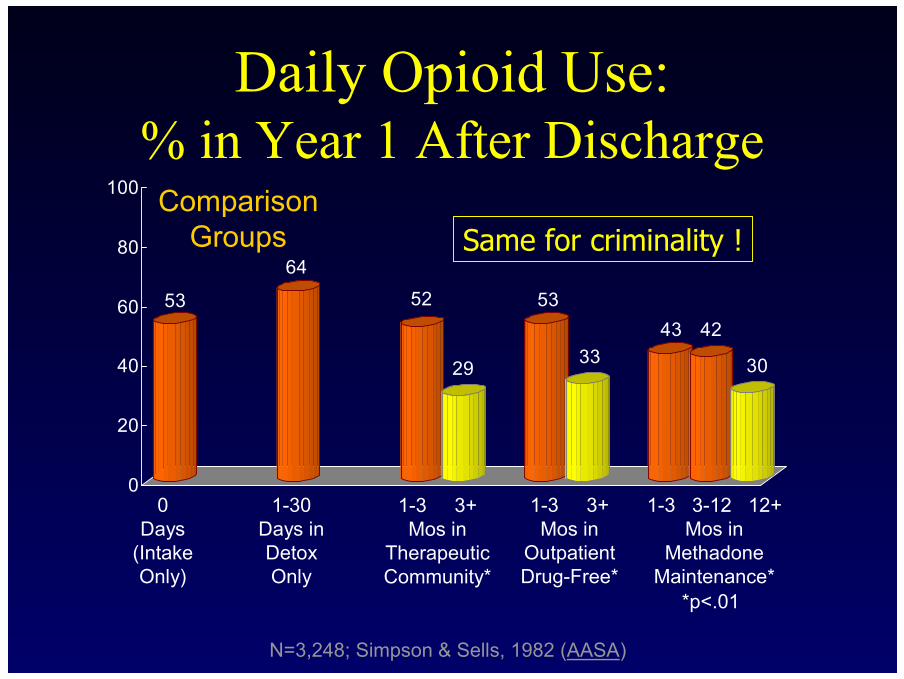
Daily Opioid Use: % in Year 1 After Discharge
0Days
(IntakeOnly)
1-30Days inDetoxOnly
1-3 3+Mos in
TherapeuticCommunity*
1-3 3+Mos in
OutpatientDrug-Free*
1-3 3-12 12+Mos in
MethadoneMaintenance*
N=3,248; Simpson & Sells, 1982 (AASA)
*p<.01
ComparisonGroups Same for criminality !
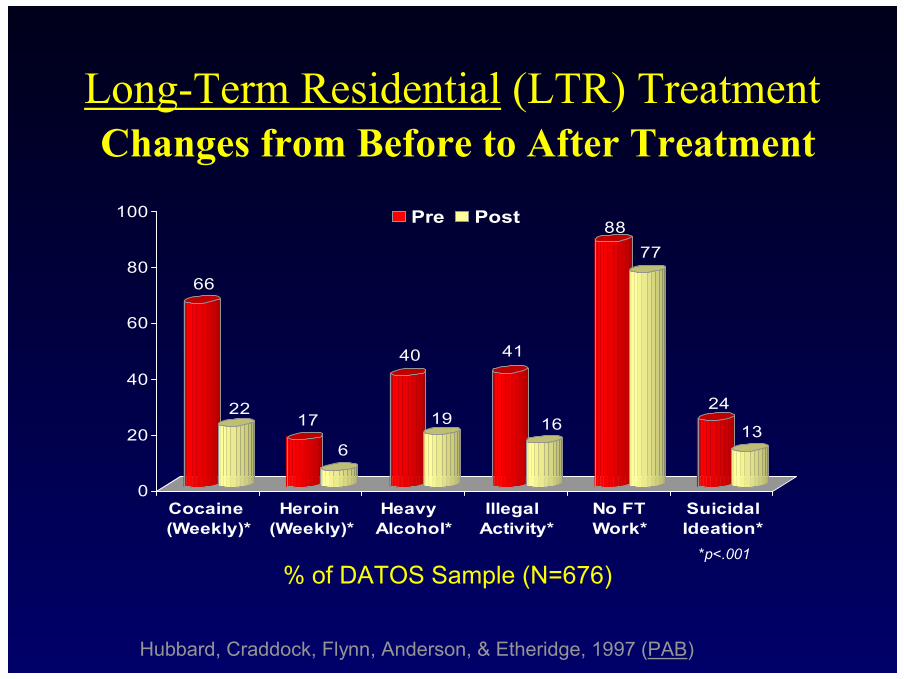
Long-Term Residential (LTR) TreatmentChanges from Before to After Treatment
66
2217
6
40
19
41
16
8877
24
13
0
20
40
60
80
100
Cocaine (Weekly)*
Heroin (Weekly)*
Heavy Alcohol*
Illegal Activity*
No FTWork*
SuicidalIdeation*
Pre Post
% of DATOS Sample (N=676)*p<.001
Hubbard, Craddock, Flynn, Anderson, & Etheridge, 1997 (PAB)

Outpatient Drug-Free (ODF) TreatmentChanges from Before to After
Treatment
42
1825
9
31
1522
14
8276
1911
0
20
40
60
80
100
Cocaine (Weekly)*
Marijuana (Weekly)*
Heavy Alcohol*
Illegal Activity*
No FTWork*
SuicidalIdeation*
Pre Post
% of DATOS Sample (N=764)*p<.001
Hubbard, Craddock, Flynn, Anderson, & Etheridge, 1997 (PAB)

42
22
89
28
15 16
29
14
85 82
1713
0
20
40
60
80
100
Cocaine (Weekly)*
Heroin (Weekly)*
Heavy Alcohol
Illegal Activity*
No FTWork
SuicidalIdeation
Pre Post
% of DATOS Sample (N=727)
Outpatient Methadone Treatment (OMT)Changes from Before to After Treatment
*p<.001
Hubbard, Craddock, Flynn, Anderson, & Etheridge, 1997 (PAB)

METHADONE EFFECTIVENESS
There is strong evidence from clinical trials that heroin-dependent individualshave much better outcomes in terms of illicit drug consumption and othercriminal behavior when they are maintained on methadone than when they arenot treated at all, when they are simply detoxified and released, or whenmethadone is tapered down and terminated arbitrarily.
Methadone clinics have significantly higher retention rates among opioid-dependent populations than do other treatment modalities for similar patients.
When assessed following discharge from methadone treatment, patients who stayed in treatment longer have better outcomes than patients who left earlier.
Patients do much better, generally, when they are stabilized on higher rather than lower doses.

THERAPEUTIC COMMUNITY EFFECTIVENESS
TC patients end virtually all illicit drug taking and other criminal behaviorwhile in residence.
They perform better (in terms of reduced drug taking and other criminalactivity and increased social productivity) after discharge than beforeadmission.
They also have better outcomes at follow-up than individuals who simplyundergo detoxification or who contact but do not enter a TC program.
The length of stay is the strongest predictor of outcomes at follow-up, with graduates having the best outcomes at that point.
Attrition from TCs is typically high—above the rates for MM but belowthe rates for OPNM treatment.).

L’OTTIMIZZAZIONE DEL TRATTAMENTO
• Ritenzione
• Dose dei farmaci agonisti
• integrazione e personalizzazione
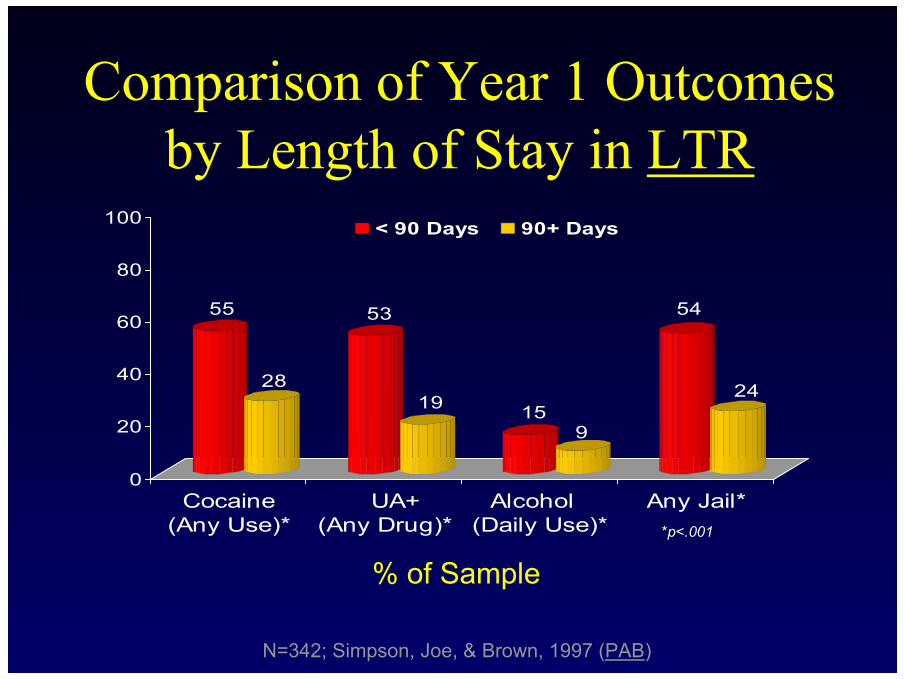
Comparison of Year 1 Outcomes by Length of Stay in LTR
55
28
53
19 159
54
24
0
20
40
60
80
100
Cocaine (Any Use)*
UA+ (Any Drug)*
Alcohol (Daily Use)*
Any Jail*
< 90 Days 90+ Days
% of Sample*p<.001
N=342; Simpson, Joe, & Brown, 1997 (PAB)

MMTP EFFECT OF THE DOSE OF METHADONE
0.21
0.47
2.2
OR / RR
0.12 - 0.38<60 vs >80
0.33 - 0.67drop-out<60 vs 60-80Caplehorn etal., 1994
use of heroin80 vs 40Caplehorn etal., 1993
IC 95%OutcomeDose

METHADONE:ANTIWITHDRAWAL AND ANTICRAVING EFFECT
Time
Plas
ma
conc
entr
atio
n
INTOXICATION
ABSTINENCE
TOLERANCE
AnticravingAnticraving DoseDose
AntiwithdrawalAntiwithdrawal DoseDose

METHADONE DOSAGES:FREQUENCE DISTRIBUTION
05
101520253035404550
0-25 25-50 50-75 75-100 100-125 125-150 150-175 > 175
Methadone (mg)

METHADONE PHARMACOKINETIC:DOSE- CONCENTRATION RELATIONSHIP
0100200300400500600700800900
1000
0 25 50 75 100 125 150 175 200 225 250
methadone (mg)
Plas
ma
conc
entr
atio
n (n
g/m
l)

FACTORS INVOLVED IN DETERMINATION METHADONE DOSE
• Tolerance level• Genetic factors (metabolic)• Physiologic factors (diet, pregnancy)• Pharmacological interferences• Physical pathology• Psychic pathology


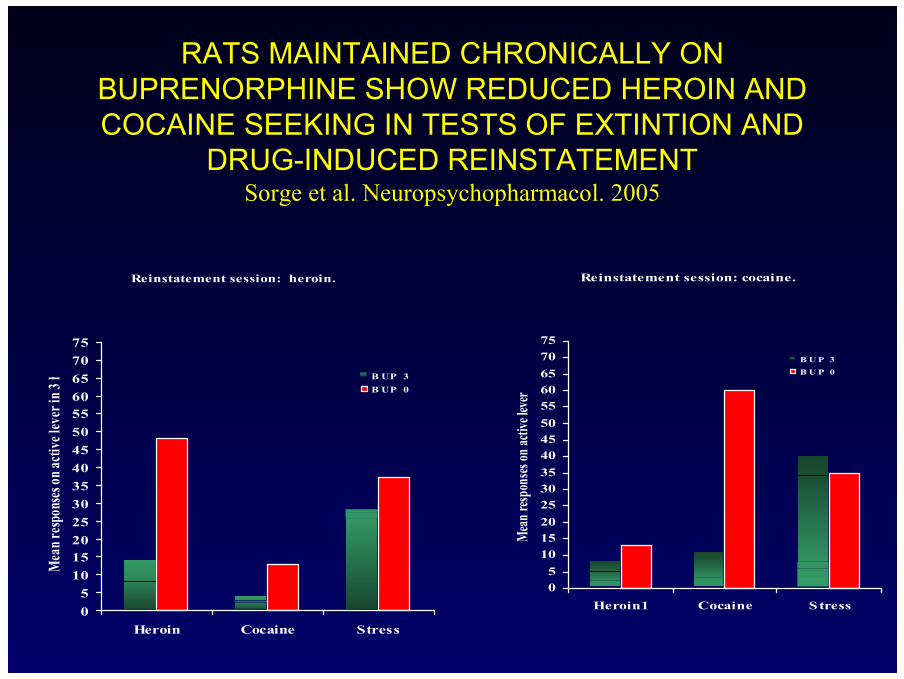
RATS MAINTAINED CHRONICALLY ON BUPRENORPHINE SHOW REDUCED HEROIN AND COCAINE SEEKING IN TESTS OF EXTINTION AND
DRUG-INDUCED REINSTATEMENTSorge et al. Neuropsychopharmacol. 2005
Inc re a s e in e xtra c e llo la r do pa m ine in nuc le us a c c um be ns in re s po ns e to a c ute inje c t io ns o f
he ro in.
0
100
200
300
400
-40 0 40 80 120Tim e
B UP 3B UP 1.5B UP 0
Inc re a s e in e xtra c e llo la r do pa m ine in nuc le us a c c um be ns in re s po ns e to a c ute inje c t io ns o f
c o c a ine .
0
400
800
1200
-40 0 40 80 120Tim e
B U P 3B U P 1.5B U P 0

RATS MAINTAINED CHRONICALLY ON BUPRENORPHINE SHOW REDUCED HEROIN AND COCAINE SEEKING IN TESTS OF EXTINTION AND
DRUG-INDUCED REINSTATEMENTSorge et al. Neuropsychopharmacol. 2005
Ext in tio n s e s s io n: he ro in.
0
5
10
15
20
25
30
35
40
45
50
55
60
1 2 3 4 5 6
Mea
n resp
onse
s on a
ctive
leve
r in 3
h B UP 3B UP 0
Ext int io n s e s s io n: c o c a ine .
0
5
10
15
20
25
30
35
40
45
50
55
60
1 2 3 4 5 6
Mea
n resp
onses
on ac
tive l
ever
B U P 3B U P 0
RATS MAINTAINED CHRONICALLY ON BUPRENORPHINE SHOW REDUCED HEROIN AND COCAINE SEEKING IN TESTS OF EXTINTION AND
DRUG-INDUCED REINSTATEMENTSorge et al. Neuropsychopharmacol. 2005
Reinstatement session: heroin.
05
1015202530354045505560657075
Heroin Cocaine Stress
Mea
n resp
onse
s on a
ctive
leve
r in 3
h B UP 3B UP 0
Reinstatement session: cocaine.
05
1015202530354045505560657075
Heroin1 Cocaine Stress
Mea
n resp
onses
on ac
tive l
ever
B U P 3B U P 0


FOUR DOMAINS IN THE EVALUATION OF TREATMENT

LA PERSONALIZZAZIONE DEL TRATTAMENTO
Il clinico vorrebbe sapere come può aiutare al meglio il suo paziente e in che modo la conoscenza della
condizione dello stesso può aiutarlo a mettere assieme il
migliore programma di trattamento.
COSA AGGIUNGE VEDETTE
• Ci informa su aspetti non esplorabili daitrial clinici.
• Permette di verificare cosa accade nellarealtà del trattamento.

Methadone Maintenance 50 – 80%
LAAM Maintenance 50 – 80%
Buprenorphine-Naloxone Maintenance 40 – 50%**
Naltrexone Maintenance 10 – 20%
“Drug Free” (non-pharmacotherapeutic) 5 – 20%
Short-term Detoxification (any mode) 5 – 20% (limited data)
Opiate Addiction Treatment Outcome*
* One year retention in treatment and/or follow-up with significant reduction or elimination of illicit use of opiates
** Maximum effective dose (24mgsl) equal to 60 to 70 mg/d methadone. Data base on 6 month follow-up only.
Kreek, 1996; 2001; 2003

The “Black Box” of Treatment?The “Black Box” of Treatment?The “Black Box” of Treatment?
Retention Predicts Outcomes• Findings Consistent from National
Studies1970s (44,000 admissions in DARP)1980s (11,000 admissions in TOPS)1990s (10,000 admissions in DATOS)
Also in England’s NTORS (1990s)!
• Conclusions from Major ReviewsInstitute of Medicine (’90, ’96, & ’98)

Patient Retention Rates for Programs(beyond minimum “thresholds”)
65%75% 76%
21% 16% 15%3+ Mos inLong-TermResidential
(n=17)
3+ Mos in Outpatient Drug-Free
(n=14)
12+ Mos inOutpatient
Methadone (n=10)
Simpson, Joe, Broome, Hiller, Knight, Rowan-Szal, 1997 (PAB)
BestProgram
PoorestProgram

Patient Problems in LTR Programs
6782
9686 86
75
416
42 33 44 29
Alcohol
Poly-Drug
Criminal In
vl
Psychological
Family/Friends
Unemployment
Highest %
Lowest %

Programs with Lower Retention had more “troubled” caseloads!
Admissions to these programs had --–More cocaine & alcohol problems–More time in previous treatments –More psychological problems
But these patient problems did not explainall program differences in retention rates!
Simpson, Joe, Broome, Hiller, Knight, Rowan-Szal, 1997 (PAB)

Fine

Elements of a “Model”for Treatment Process?
SufficientRetentionSufficientSufficientRetentionRetention
PosttreatmentPosttreatment
Drug UseDrug UseDrug Use
CrimeCrimeCrime
Social AdjSocial AdjSocial Adj
?PatientFactorsPatientPatientFactorsFactors
PsychologicalPsychologicalFunctioning,Functioning,
MotivationMotivation,,
& Problem& ProblemSeveritySeverity

Conclusions•• Treatment Treatment reducesreduces drug use & crimedrug use & crime
–– Problem severity & retention of patientsProblem severity & retention of patients–– Setting, program functioning, & staff skillsSetting, program functioning, & staff skills
•• Treatment programs are Treatment programs are differentdifferent–– Types of patients servedTypes of patients served–– Engagement & retention of patientsEngagement & retention of patients–– Readiness for change & resources availableReadiness for change & resources available
•• Pressing issuesPressing issues for treatment fieldfor treatment field–– “Treatment process” (quality & “Treatment process” (quality &
performance)performance)–– “Technology transfer” (research“Technology transfer” (research--toto--
0
50
100
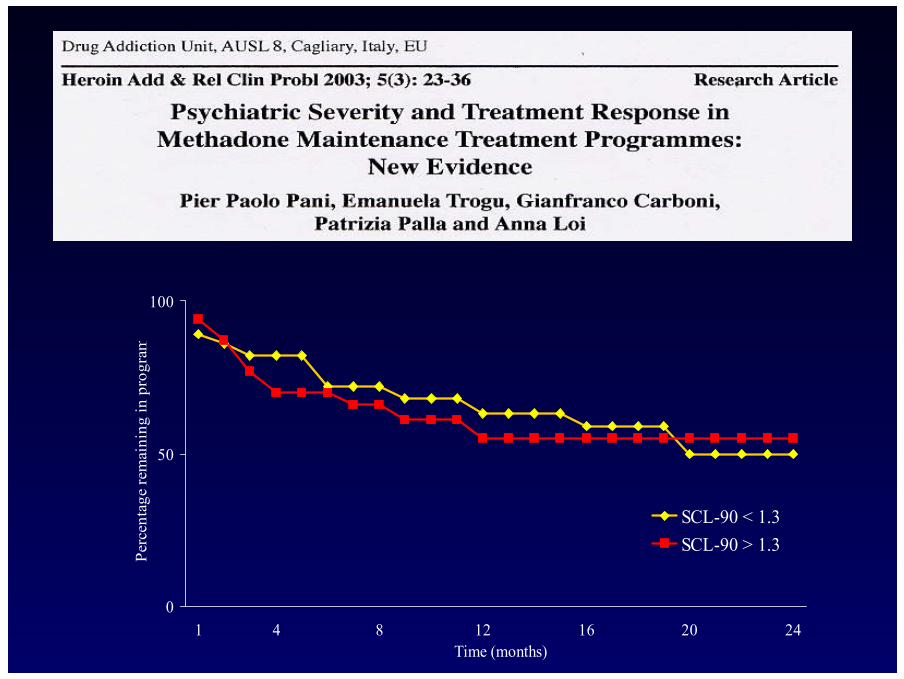
1 4 8 12 16 20 24Time (months)
Perc
enta
ge re
mai
ning
in p
rogr
am
SCL-90 < 1.3SCL-90 > 1.3

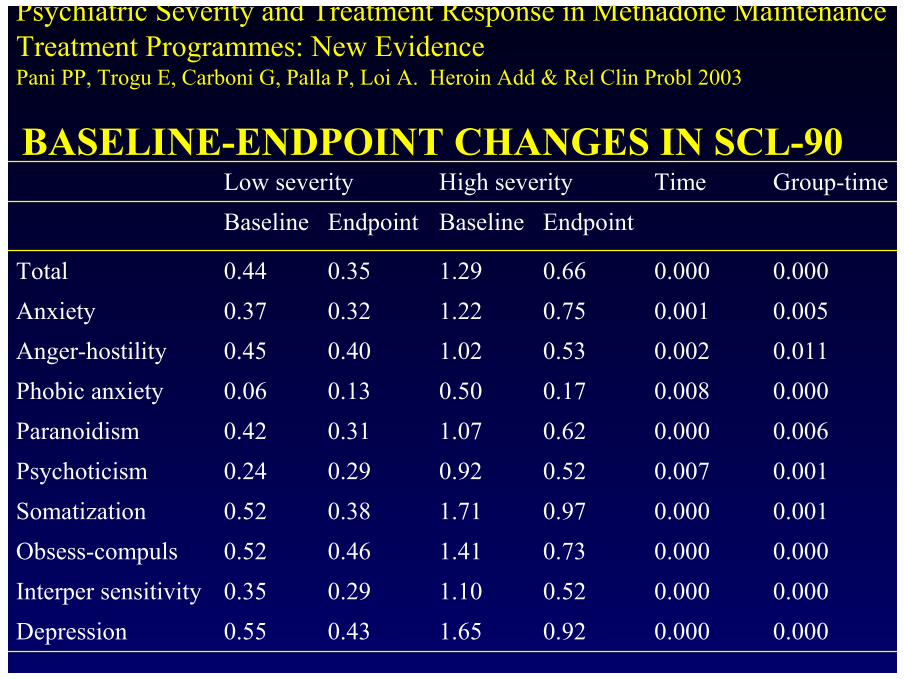
Psychiatric Severity and Treatment Response in Methadone Maintenance Treatment Programmes: New EvidencePani PP, Trogu E, Carboni G, Palla P, Loi A. Heroin Add & Rel Clin Probl 2003
URINE POSITIVENESS FOR MORPHINE (PCC)URINE POSITIVENESS FOR MORPHINE (PCC)
0
20
40
60
80
100
1 2 3 4 54 month periods
Perc
enta
ge o
f urin
alys
es p
ositi
ve
SCL-90 < 1.3SCL-90 > 1.3

Psychiatric Severity and Treatment Response in Methadone Maintenance Treatment Programmes: New EvidencePani PP, Trogu E, Carboni G, Palla P, Loi A. Heroin Add & Rel Clin Probl 2003
URINE POSITIVENESS FOR COCAINE PER MONTHURINE POSITIVENESS FOR COCAINE PER MONTH
0
20
40
60
80
100
1 2 3 4 5 64 months- period
Perc
enta
ge o
f urin
alys
es p
ositi
ve
SCL-90 < 1.3SCL-90 > 1.3

Psychiatric Severity and Treatment Response in Methadone Maintenance Treatment Programmes: New EvidencePani PP, Trogu E, Carboni G, Palla P, Loi A. Heroin Add & Rel Clin Probl 2003
BASELINE BASELINE –– ENDPOINT HEROIN CRAVINGENDPOINT HEROIN CRAVING
0
20
40
60
80
100
Baseline Endpoint
Her
oin
crav
ing
SCL-90 < 1.3SCL-90 > 1.3
Psychiatric Severity and Treatment Response in Methadone Maintenance Treatment Programmes: New EvidencePani PP, Trogu E, Carboni G, Palla P, Loi A. Heroin Add & Rel Clin Probl 2003
BASELINEBASELINE--ENDPOINT CHANGES IN SCLENDPOINT CHANGES IN SCL--9090
0.0000.0000.521.100.290.35Interper sensitivity
0.0050.0010.751.220.320.37Anxiety
0.0010.0000.971.710.380.52Somatization
0.0060.0000.621.070.310.42Paranoidism0.0000.0080.170.500.130.06Phobic anxiety0.0110.0020.531.020.400.45Anger-hostility
0.0000.0000.661.290.350.44Total
0.0010.0070.520.920.290.24Psychoticism
0.0000.0000.921.650.430.55Depression
0.0000.0000.731.410.460.52Obsess-compuls
EndpointBaselineEndpointBaselineGroup-timeTimeHigh severityLow severity

PROSPECTIVE PSYCHIATRIC SEVERITY STUDYPROSPECTIVE PSYCHIATRIC SEVERITY STUDY
BASELINE BASELINE –– ENDPOINT SCLENDPOINT SCL--90: 90: TOTALTOTAL
0
2
Baseline Endpoint
SCL
-90
Tot
al
SCL-90 < 1.3SCL-90 > 1.3
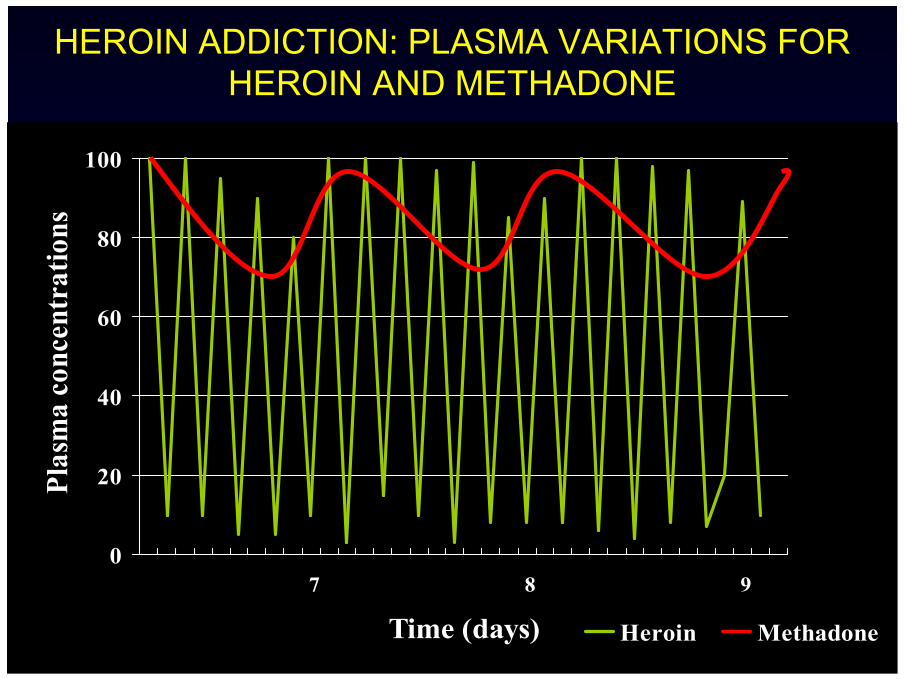
HEROIN ADDICTION: PLASMA VARIATIONS FOR HEROIN AND METHADONE
0
20
40
60
80
100
7 8 9
Time (days)
Plas
ma
conc
entr
atio
ns
Heroin Methadone

METHADONE:ANTIWITHDRAWAL AND ANTICRAVING EFFECT
Time
Plas
ma
conc
entr
atio
n
INTOXICATION
ABSTINENCE
TOLERANCE
AnticravingAnticraving DoseDose
AntiwithdrawalAntiwithdrawal DoseDose

RELATIONSHIP BETWEEN THE DOSE OF RELATIONSHIP BETWEEN THE DOSE OF METHADONE AND THE USE OF HEROINMETHADONE AND THE USE OF HEROIN
0,1
1,0
10,0
40 80
dose of methadone (mg)
use
of
her
oin
(O
R)

Clinical guidelines for the use of methadoneConsensus panel on methadone treatment,
Pietrasanta 2001
“In a range between 80 - 120 mg/day usuallywe get the therapeutic response in terms of
control of heroin use”.

METHADONE DOSAGES:FREQUENCE DISTRIBUTION
05
101520253035404550
0-25 25-50 50-75 75-100 100-125 125-150 150-175 > 175
Methadone (mg)

METHADONE PHARMACOKINETIC:DOSE- CONCENTRATION RELATIONSHIP
0100200300400500600700800900
1000
0 25 50 75 100 125 150 175 200 225 250
methadone (mg)
Plas
ma
conc
entr
atio
n (n
g/m
l)

FACTORS INVOLVED IN DETERMINATION METHADONE DOSE
• Tolerance level• Genetic factors (metabolic)• Physiologic factors (diet, pregnancy)• Pharmacological interferences• Physical pathology• Psychic pathology


Methadone dose of heroin addicts with Axis I Methadone dose of heroin addicts with Axis I psychiatric psychiatric comorbiditycomorbidity (Maremmani, (Maremmani, etet al.,al.,. J Addict . J Addict DisDis, 2000), 2000)..
99
Mean
154
Mean
TOnly heroin addicted patients
Dually diagnosed patients
P <.0014984Methadone dose
SDSD

METHADONE PHARMACOKINETIC:DOSE- CONCENTRATION RELATIONSHIP
0100200300400500600700800900
1000
0 25 50 75 100 125 150 175 200 225 250
methadone (mg)
Plas
ma
conc
entr
atio
n (n
g/m
l)

METHADONE INTERFERENCES: CLINICAL CASE
0100200300400500600700800900
1000
0 25 50 75 100 125 150 175 200 225 250
Methadone dose (mg)
Pla
sma c
on
cen
trati
on
(n
g/m
l)
A.Y.Methadone = 100 mgPlasma concentration = 57 ng/ml (14 hours after intake)Craving = 80 (range: 0 – 100). Medications: carbamazepine
X.J.Methadone = 180 mgPlasma concentration = 52 ng/mlCraving = 70 for cocaine, 0 forheroin.Medications: carbamazepine

MEDICATIONS INTERFERING WITH METHADONE
INCREASE PLASMA CONCENTRATION:
Surefluvoxaminefluconazolchetoconazol
PossibleCimetidinciprofloxacinfluoxetineNefazodoneparoxetine
REDUCE PLASMA CONCENTRATION:
SureBarbituratescarbamazepinefenitoinerifampicineamprenavirabacavirefavirenznevirapina
Possiblealcooldidanosineritonavirstavudineascorbic acid ed other urine acidifiants.
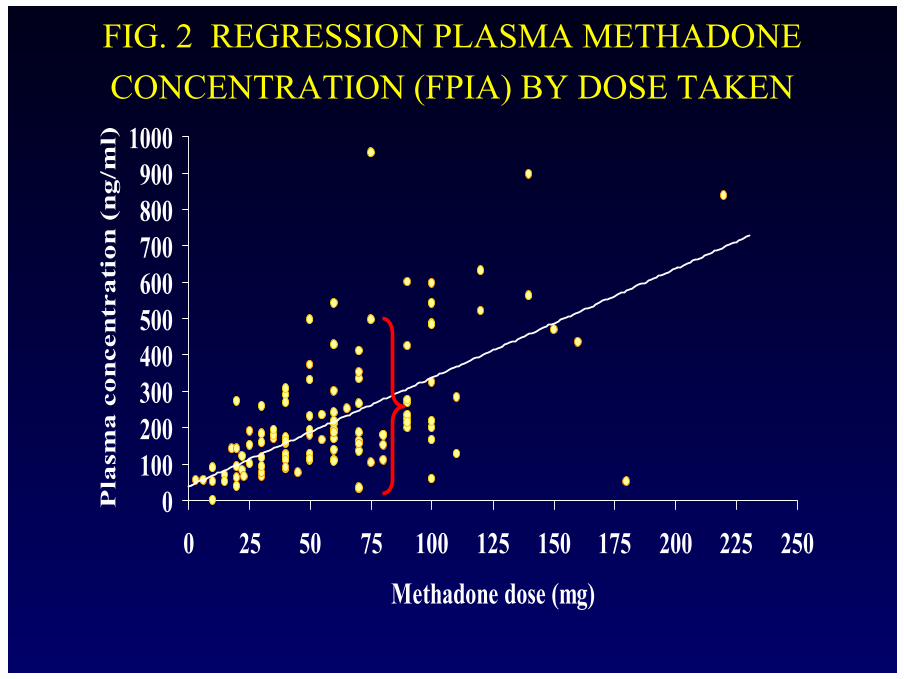
FIG. 2 REGRESSION PLASMA METHADONE CONCENTRATION (FPIA) BY DOSE TAKEN
0100200300400500600700800900
1000
0 25 50 75 100 125 150 175 200 225 250
Methadone dose (mg)
Pla
sma c
on
cen
tra
tion
(n
g/m
l)

A 17 fold variation has been found in the dose of methadone needed to obtain a 250 ng/ml plasma concentration of R-methadone (Eap etal., 2000).

METHADONE CONCENTRATION TRESHOLD
0100200300400500600700800900
1000
0 25 50 75 100 125 150 175 200 225 250
Methadone dose (mg)
Pla
sma
con
cen
trati
on
(n
g/m
l)
Treshold R-S,(Eap et al., 2002)
Treshold R-S,(Dole, 1988; Loimer 1992
)

PHARMACOLOGY OF BUPRENORPHINE
Buprenorphine acts asPartial agonist for µ receptors
Antagonist for κ receptors
Buprenorphine has a high affinity for µand (less) for κ receptors
OPIOID RECEPTORS
κδµ

OPIOID ACTIVITY
antagonistpartialagonist
agonist

AFFINITY
Buprenorphine Morphine
Opioidreceptor

Buprenorphine is reinforcing but does not produce “rush”-like effects
PHARMACOLOGY OF BUPRENORPHINE
Buprenorphine does not induce significant physicaldependence
The possibility of buprenorphine lethal overdoseis remote
Buprenorphine effectively suppresses heroinself-administration
Buprenorphine may be administered sublingually
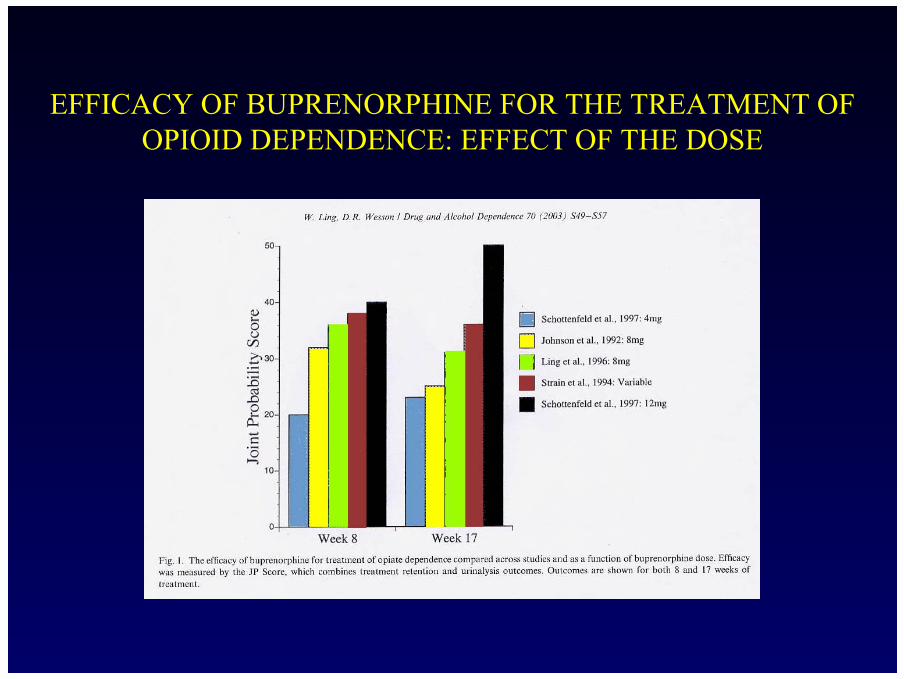
EFFICACY OF BUPRENORPHINE FOR THE TREATMENT OF OPIOID DEPENDENCE: EFFECT OF THE DOSE

BUPRENORPHINE: DOSE EFFECT RELATIONSHIP
Dose
Effe
ct
Methadone
Buprenorphine

BUPRENORPHINE PLASMA CONCENTRATION: CRONIC ADMINISTRATION
0
1
2
3
4
5
6
7
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38
Time (hours)
Conc
entra
tion
(ng/
ml)

SUBLINGUAL BUPRENORPHINE (8 mg liquid): VARIABILITY IN PLASMA CONCENTRATION
Schuh et al., 1999 (modified).
0
2
4
6
8
10
12
14
24h 15m 30m 60m 120m 180m 360m
Time
Conc
entra
tion
(ng/
ml)

OPIOID AGONISTS IN HEROIN ADDICTION: APPROPRIATE DOSE
• No withdrawal complains• No use of heroin• No craving• No sedation, euforia

• In Italy, a widepublic treatment network (500 services) givescurrently assistance to about 150.000heroin addicts.

METHADONE MAINTENANCE COST
020406080
100120140160180200
Euro/day
meth street Jail