
Sindrome di Brugada e QT lungo - asiam-aggiornamentomedico.it · Aritmie Fatali: Eziologia. Kaufman...
101
Sindrome di Brugada e QT lungo Paolo Pieragnoli Università degli Studi di Firenze Firenze – 16 Giugno 2018 Stadio Artemio Franchi I sessione – La Morte Improvvisa
Transcript of Sindrome di Brugada e QT lungo - asiam-aggiornamentomedico.it · Aritmie Fatali: Eziologia. Kaufman...
Sindrome di Brugada
e QT lungo
Paolo Pieragnoli
Università degli Studi di Firenze
Firenze – 16 Giugno 2018
Stadio Artemio Franchi
I sessione – La Morte Improvvisa
Morte Improvvisa / Definizione
Morte naturale, preceduta da
improvvisa perdita della conoscenza,
che si verifica entro 1 ora dall’inizio
dei sintomi, in soggetti con o senza
cardiopatia nota preesistente, ma in
cui l’epoca e la modalità di morte
sono imprevedibili.Myerburg RJ, Castellanos A 1980; Task-force on SD of ESC. Eur Heart J 2001; 22: 1374-1450
FILIPPIDE muore improvvisamente subito dopo aver
annunciato agli Ateniesi la vittoria di MARATONA
PROBLEMA ANTICO !
“Chi si libera spesso e
violentemente, senza apparente
motivo, muore all’improvviso.”
Ippocrate “Aforismi”
A Roncisvalle, Orlando “sente che la morte lo
prende tutto. Dalla testa, scende verso il
cuore”. Egli “sente che il suo tempo è finito”.1
Tristano “sentì che la sua vita si perdeva,
comprese che stava per morire”.2
“Nipote mia, mi sento vicino a morire”.3
1 La Chanson de Roland2 Le Roman de Tristan et Iseult3 Cervantes, Don Chisciotte
L’uomo è stato per millenni il padrone assoluto
della sua morte e delle circostanze della sua
morte . . .
Di rado la morte era improvvisa, anche in caso
di incidente o di guerra, e la morte improvvisa
era molto temuta, non solo perché non dava il
tempo di pentirsi, ma perché privava l’uomo
della sua morte.
Ariès “Storia della morte in Occidente”
MI – Epidemiologia / Italia
• Incidenza → 1 x 1000 Abit.
• Numero casi x anno → 57.000
• Numero casi x giorno → 156
• 1 caso ogni 9 minuti
• 10 % di tutte le cause di morte
• 40 % di tutti i decessi x causa cardiaca
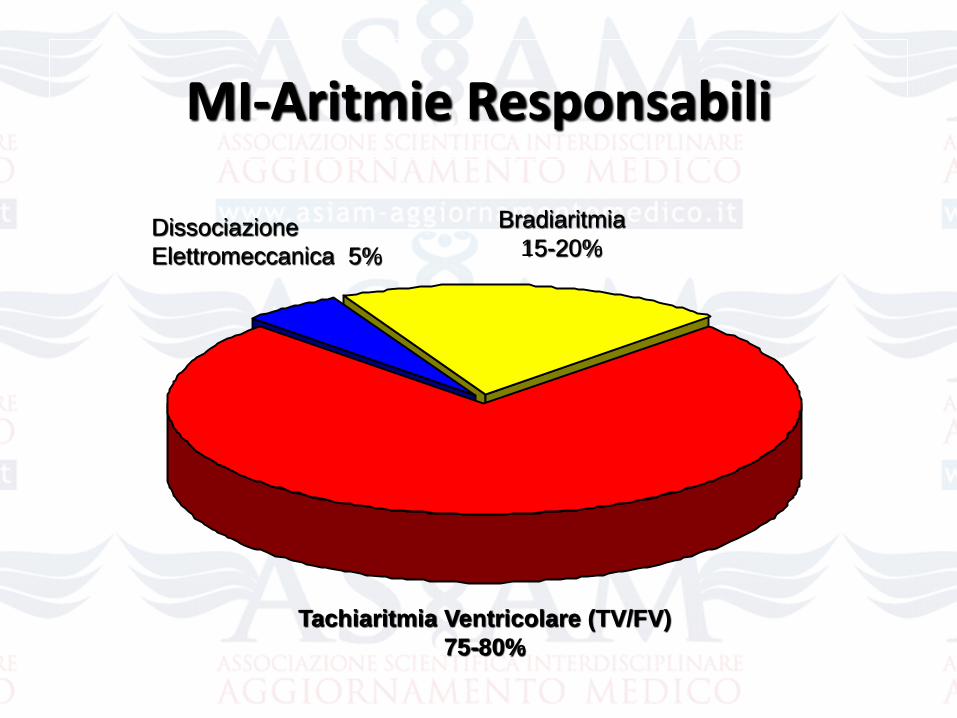
MI-Aritmie Responsabili
Bradiaritmia
15-20%
Tachiaritmia Ventricolare (TV/FV)
75-80%
Dissociazione
Elettromeccanica 5%
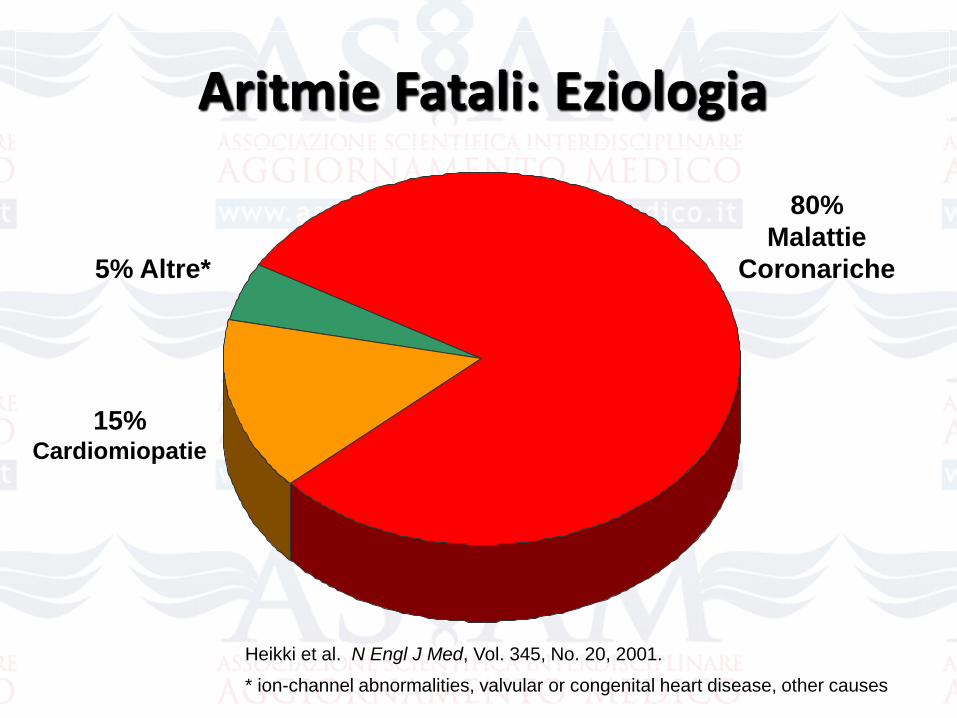
80%
Malattie
Coronariche
Heikki et al. N Engl J Med, Vol. 345, No. 20, 2001.
* ion-channel abnormalities, valvular or congenital heart disease, other causes
15%Cardiomiopatie
5% Altre*
Aritmie Fatali: Eziologia
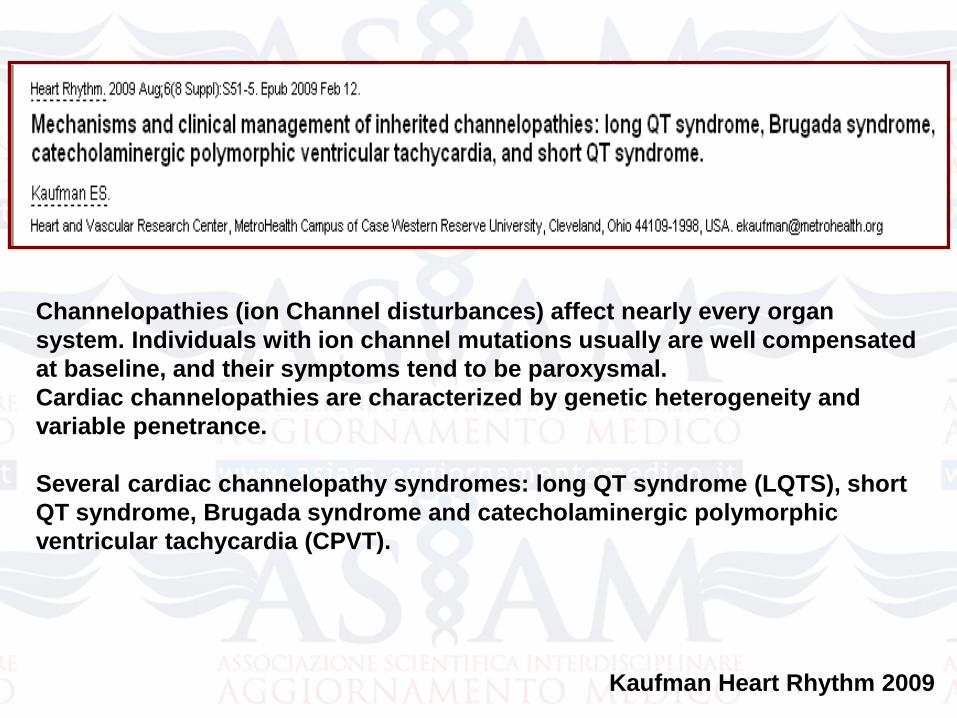
Kaufman Heart Rhythm 2009
Channelopathies (ion Channel disturbances) affect nearly every organ
system. Individuals with ion channel mutations usually are well compensated
at baseline, and their symptoms tend to be paroxysmal.
Cardiac channelopathies are characterized by genetic heterogeneity and
variable penetrance.
Several cardiac channelopathy syndromes: long QT syndrome (LQTS), short
QT syndrome, Brugada syndrome and catecholaminergic polymorphic
ventricular tachycardia (CPVT).
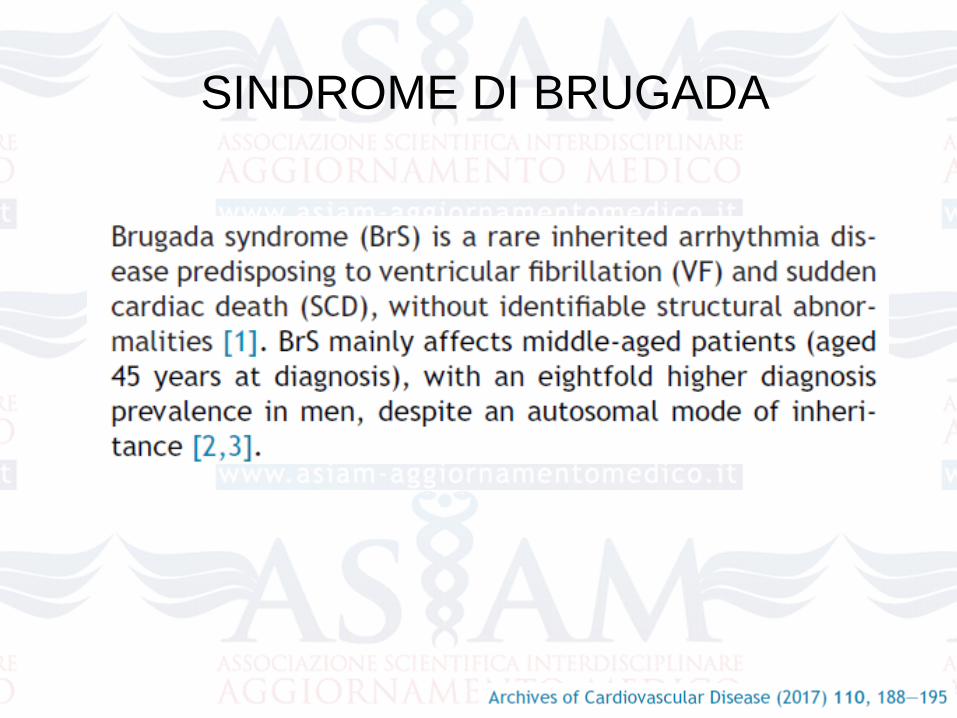
SINDROME DI BRUGADA
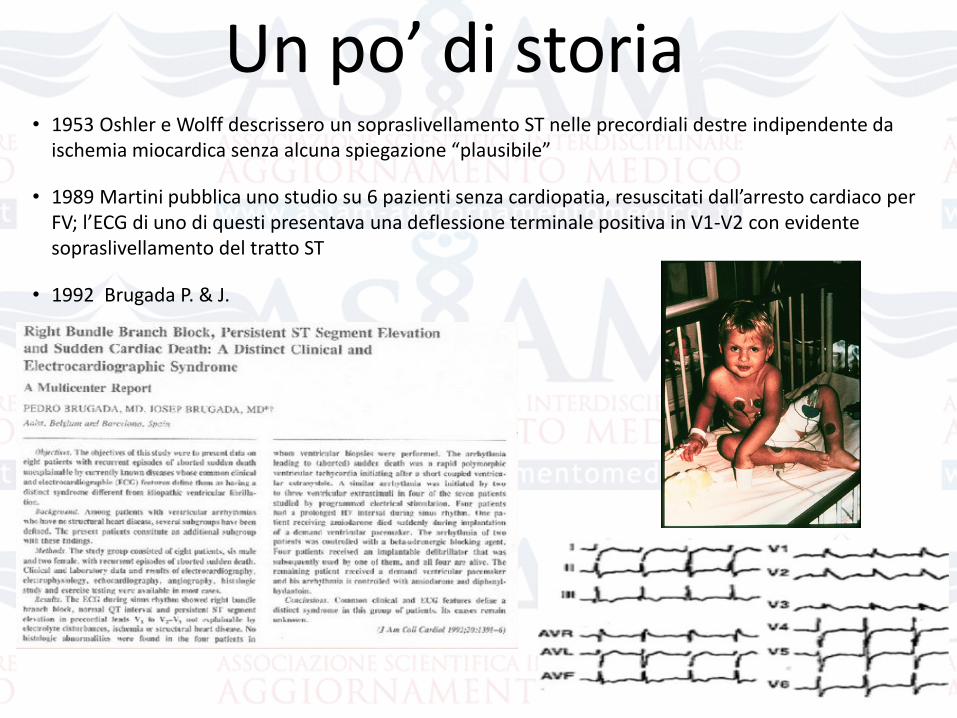
Un po’ di storia• 1953 Oshler e Wolff descrissero un sopraslivellamento ST nelle precordiali destre indipendente da
ischemia miocardica senza alcuna spiegazione “plausibile”
• 1989 Martini pubblica uno studio su 6 pazienti senza cardiopatia, resuscitati dall’arresto cardiaco per FV; l’ECG di uno di questi presentava una deflessione terminale positiva in V1-V2 con evidente sopraslivellamento del tratto ST
• 1992 Brugada P. & J.
Epidemiologia della Sindrome di Brugada
Sindrome di Brugada: responsabile dal 4% al 12% di tutte le morti SD and for up to 20% of SD in subjects withoutconcomitant cardiopathy.
Its prevalence has been estimated in 5 of 10000 inhabitants, although this rate should be understood cautiously, first, because many patients present concealed forms of the disease, thus making it likely that the real prevalence ishigher, and second, because important ethnic and geographicdifferences have been described.
Antzelevitch C et al. Circulation 2005
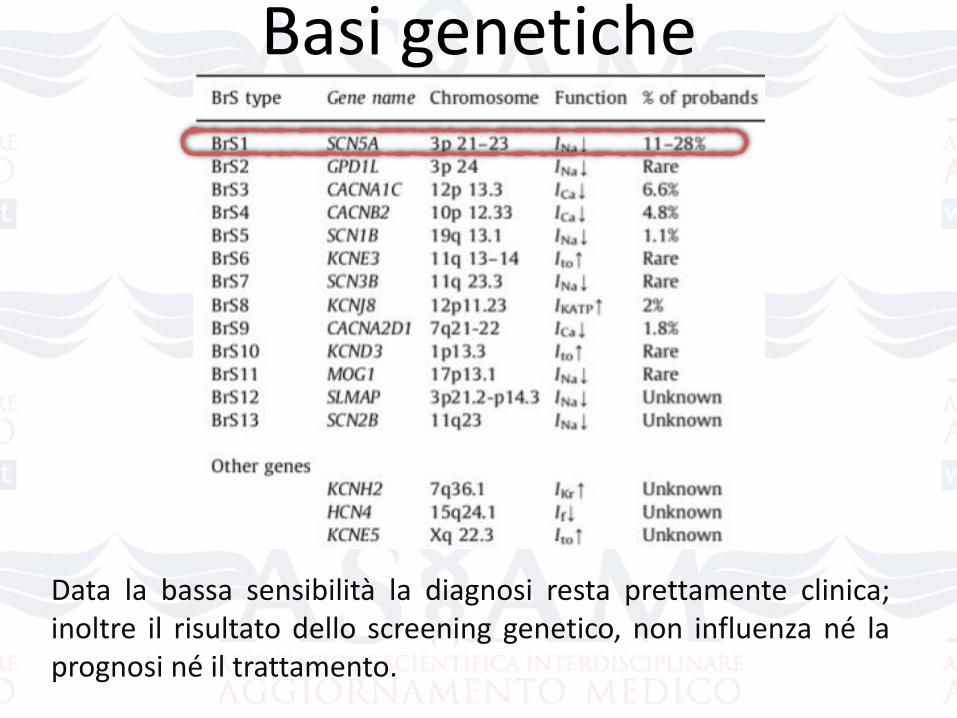
Basi genetiche
Data la bassa sensibilità la diagnosi resta prettamente clinica;inoltre il risultato dello screening genetico, non influenza né laprognosi né il trattamento.
12
30
4
4
0mVolts
-85mV
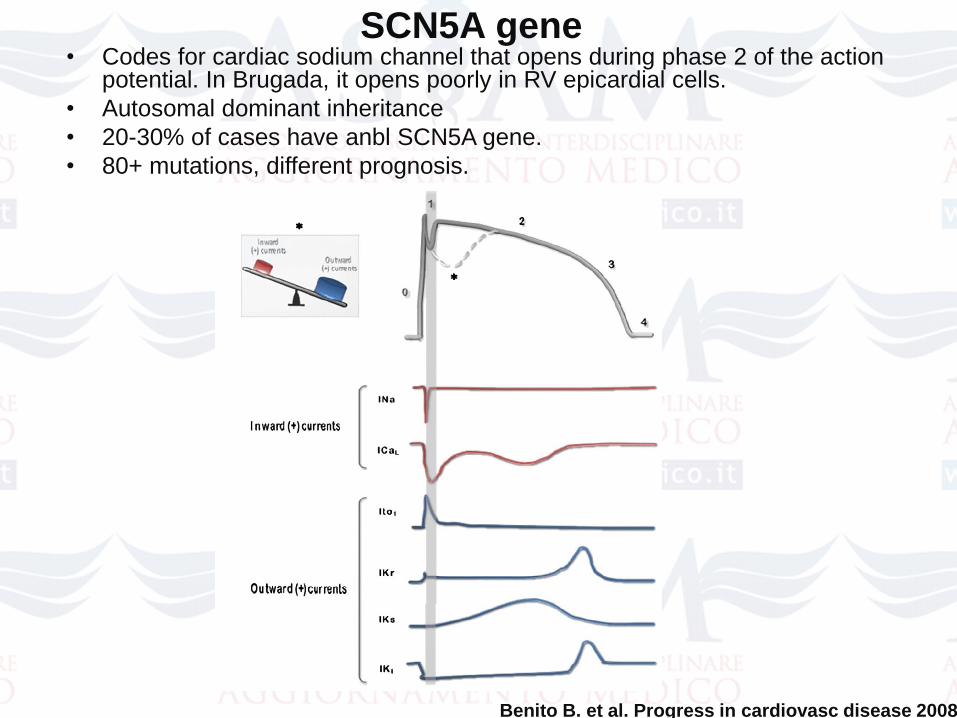
• Codes for cardiac sodium channel that opens during phase 2 of the action potential. In Brugada, it opens poorly in RV epicardial cells.
• Autosomal dominant inheritance
• 20-30% of cases have anbl SCN5A gene.
• 80+ mutations, different prognosis.
SCN5A gene
Benito B. et al. Progress in cardiovasc disease 2008
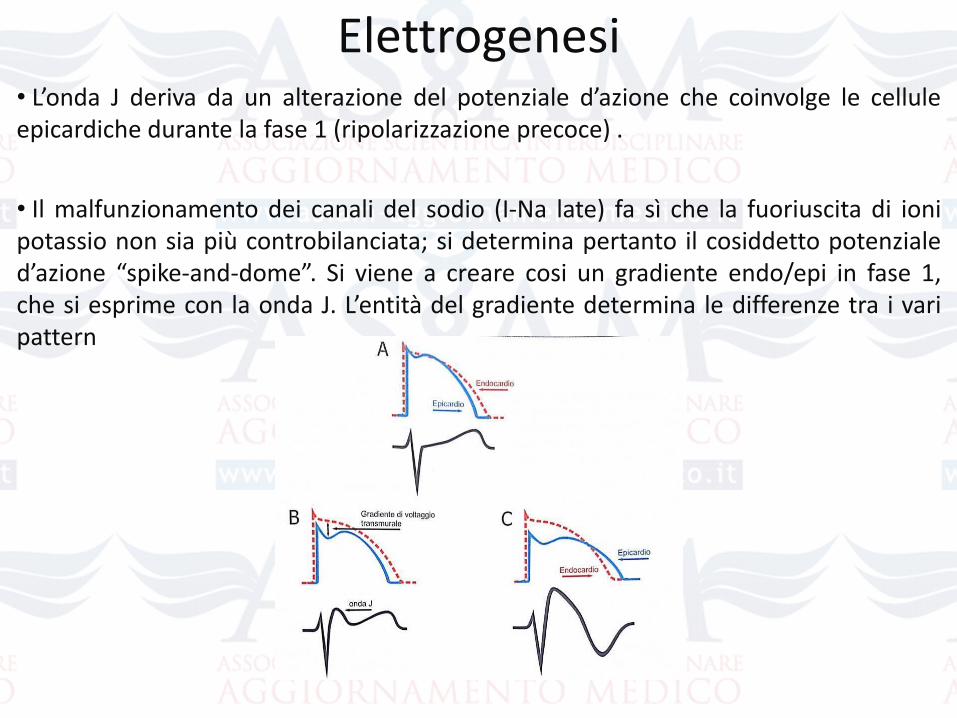
Elettrogenesi• L’onda J deriva da un alterazione del potenziale d’azione che coinvolge le celluleepicardiche durante la fase 1 (ripolarizzazione precoce) .
• Il malfunzionamento dei canali del sodio (I-Na late) fa sì che la fuoriuscita di ionipotassio non sia più controbilanciata; si determina pertanto il cosiddetto potenzialed’azione “spike-and-dome”. Si viene a creare cosi un gradiente endo/epi in fase 1,che si esprime con la onda J. L’entità del gradiente determina le differenze tra i varipattern
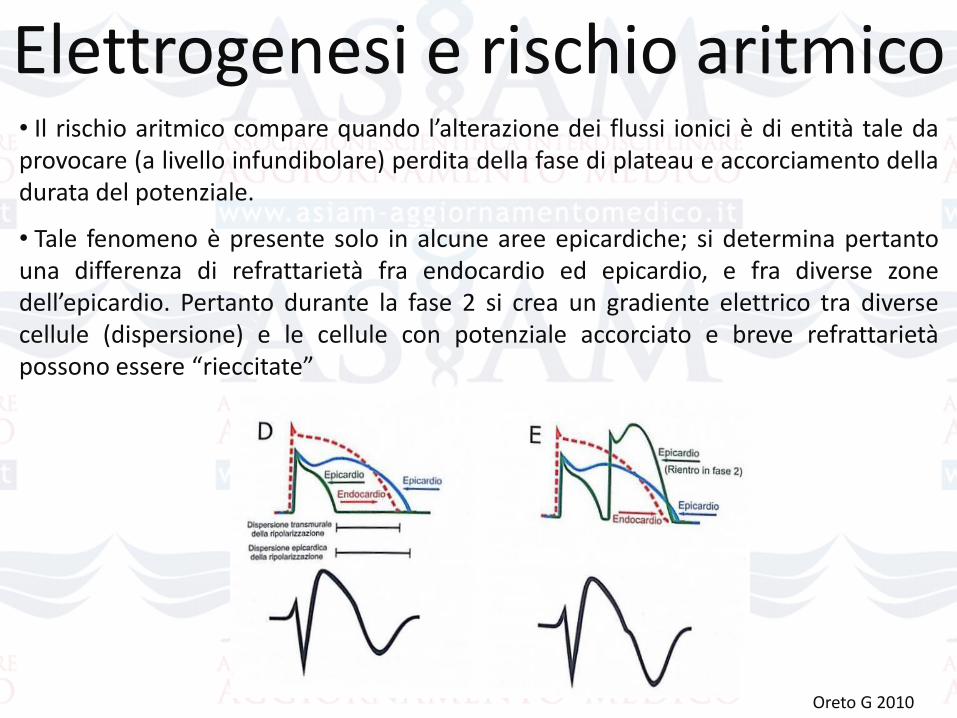
• Il rischio aritmico compare quando l’alterazione dei flussi ionici è di entità tale daprovocare (a livello infundibolare) perdita della fase di plateau e accorciamento delladurata del potenziale.
• Tale fenomeno è presente solo in alcune aree epicardiche; si determina pertantouna differenza di refrattarietà fra endocardio ed epicardio, e fra diverse zonedell’epicardio. Pertanto durante la fase 2 si crea un gradiente elettrico tra diversecellule (dispersione) e le cellule con potenziale accorciato e breve refrattarietàpossono essere “rieccitate”
Elettrogenesi e rischio aritmico
Oreto G 2010
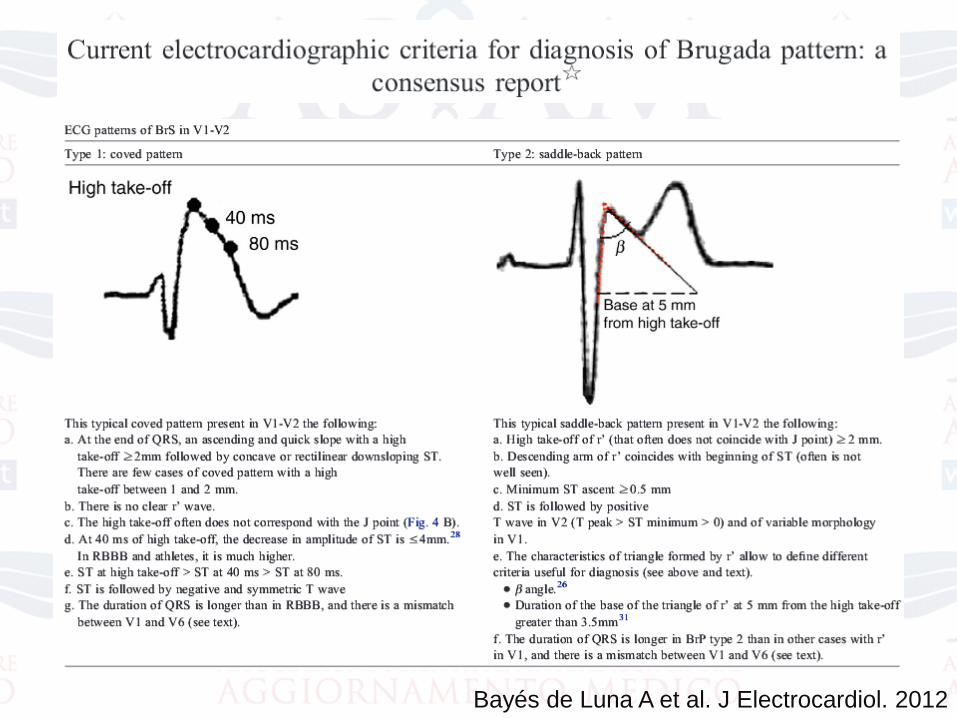
Bayés de Luna A et al. J Electrocardiol. 2012
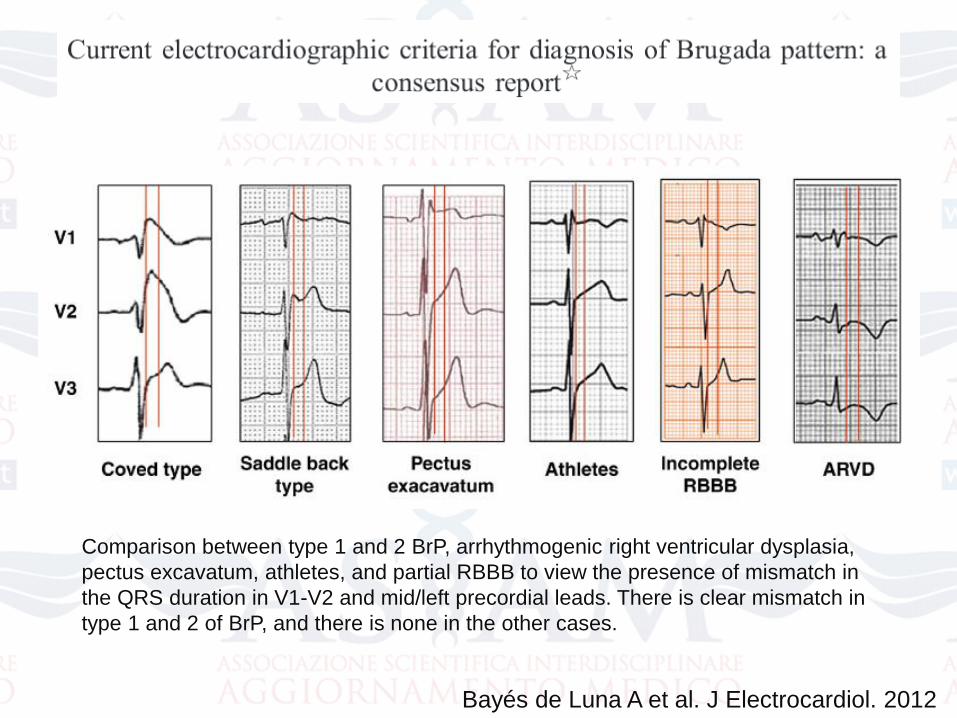
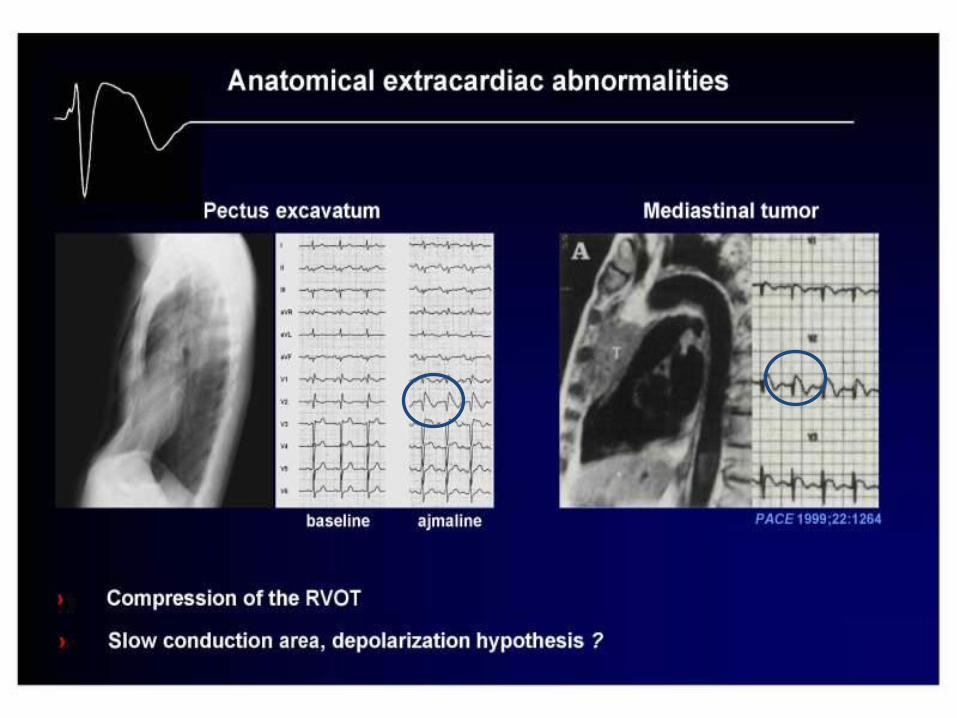
Comparison between type 1 and 2 BrP, arrhythmogenic right ventricular dysplasia,
pectus excavatum, athletes, and partial RBBB to view the presence of mismatch in
the QRS duration in V1-V2 and mid/left precordial leads. There is clear mismatch in
type 1 and 2 of BrP, and there is none in the other cases.
Bayés de Luna A et al. J Electrocardiol. 2012
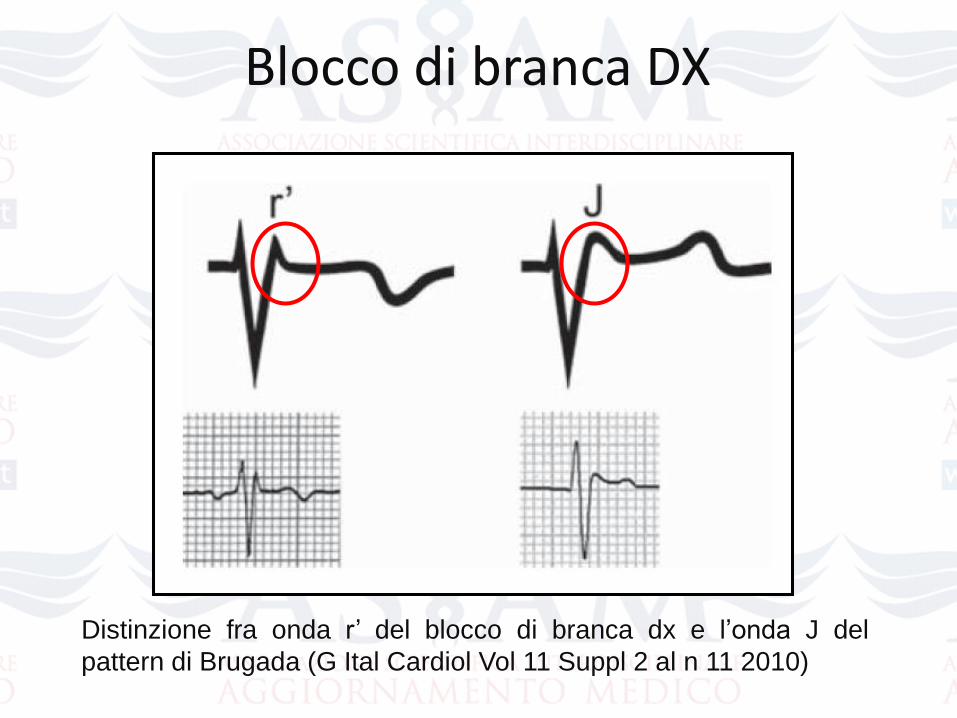
Blocco di branca DX
Distinzione fra onda r’ del blocco di branca dx e l’onda J del
pattern di Brugada (G Ital Cardiol Vol 11 Suppl 2 al n 11 2010)
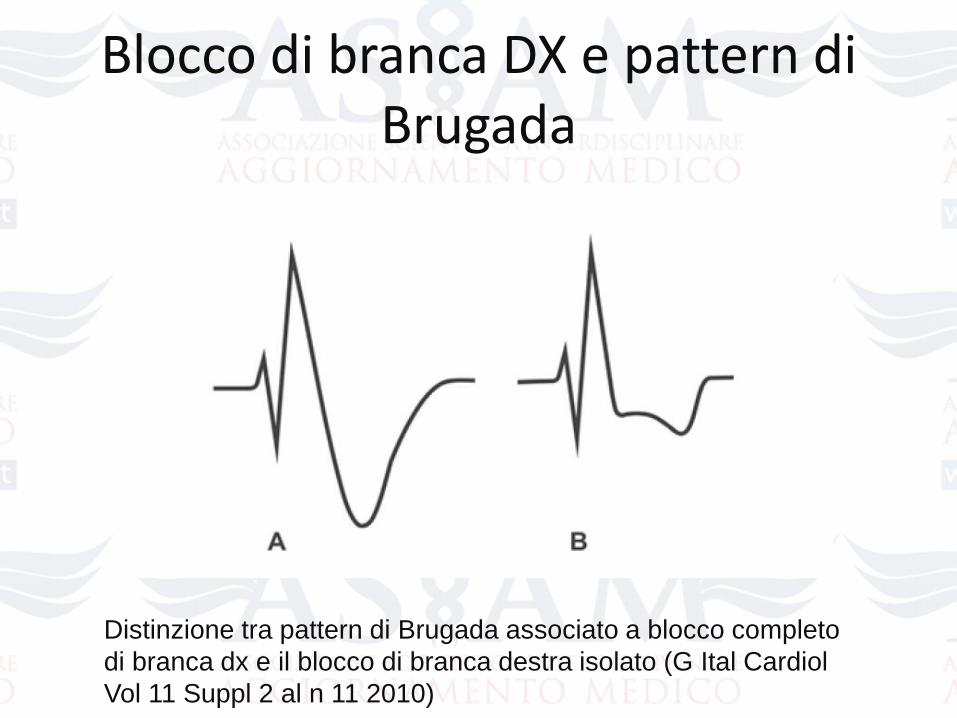
Blocco di branca DX e pattern di Brugada
Distinzione tra pattern di Brugada associato a blocco completo
di branca dx e il blocco di branca destra isolato (G Ital Cardiol
Vol 11 Suppl 2 al n 11 2010)
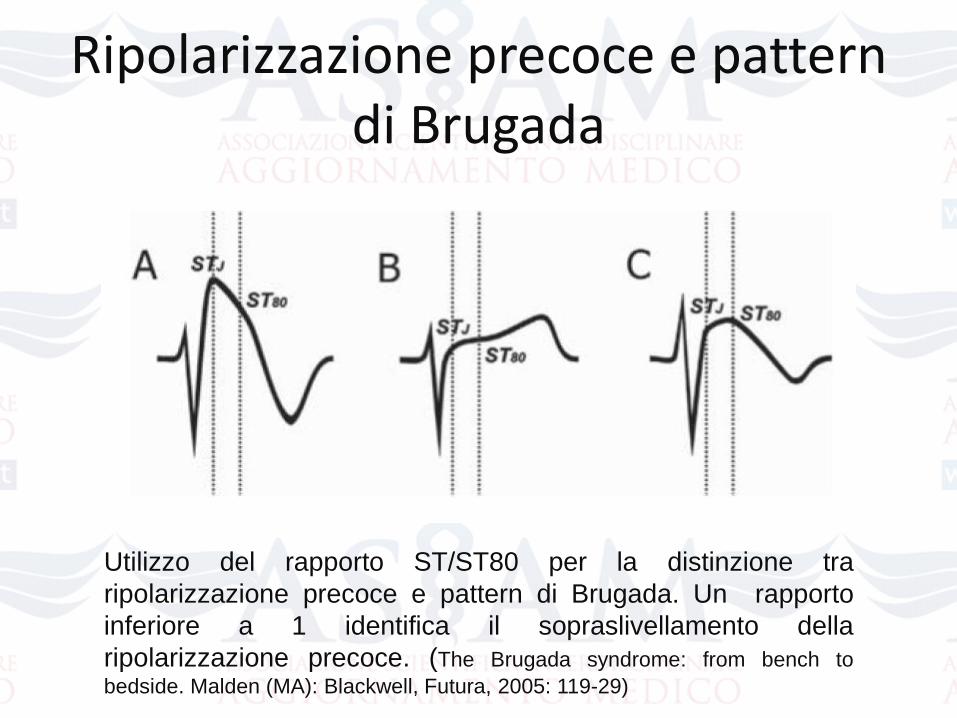
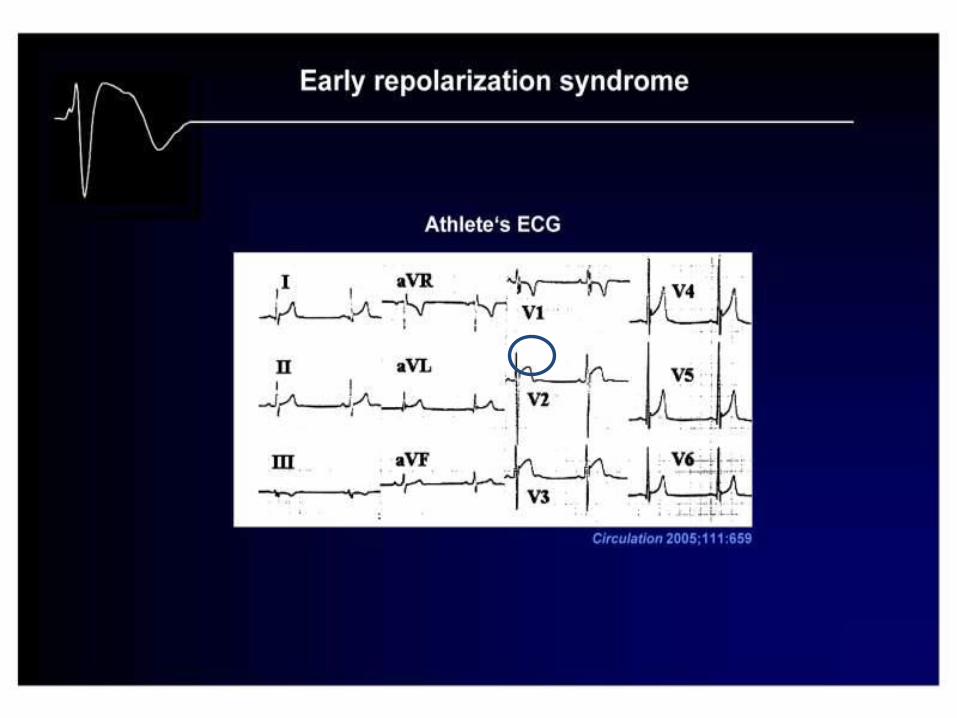
Ripolarizzazione precoce e pattern di Brugada
Utilizzo del rapporto ST/ST80 per la distinzione tra
ripolarizzazione precoce e pattern di Brugada. Un rapporto
inferiore a 1 identifica il sopraslivellamento della
ripolarizzazione precoce. (The Brugada syndrome: from bench to
bedside. Malden (MA): Blackwell, Futura, 2005: 119-29)
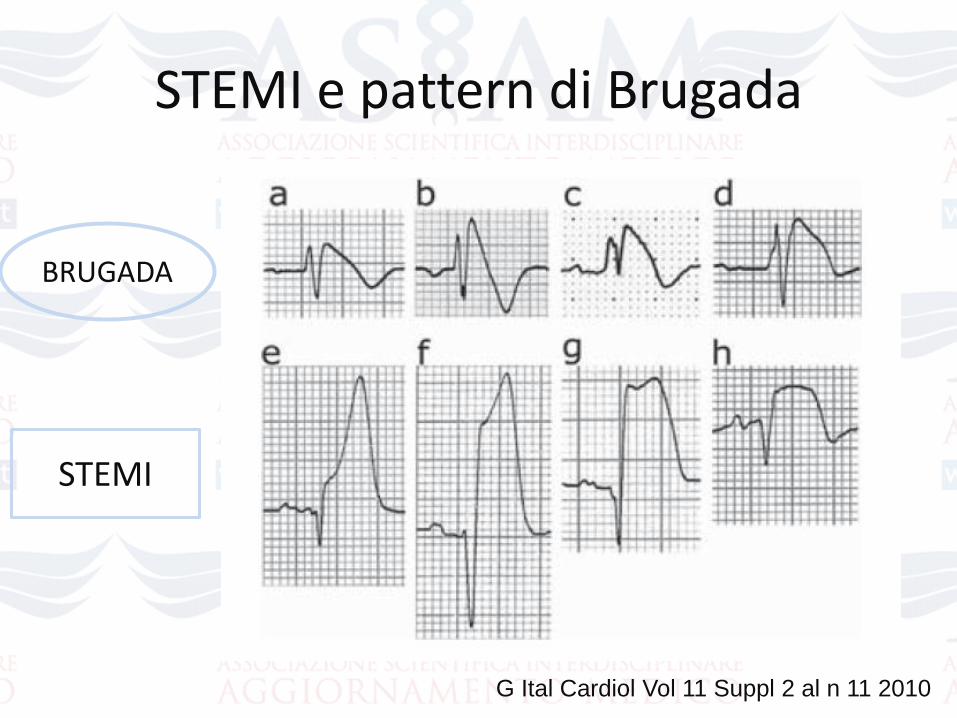
STEMI e pattern di Brugada
BRUGADA
STEMI
G Ital Cardiol Vol 11 Suppl 2 al n 11 2010
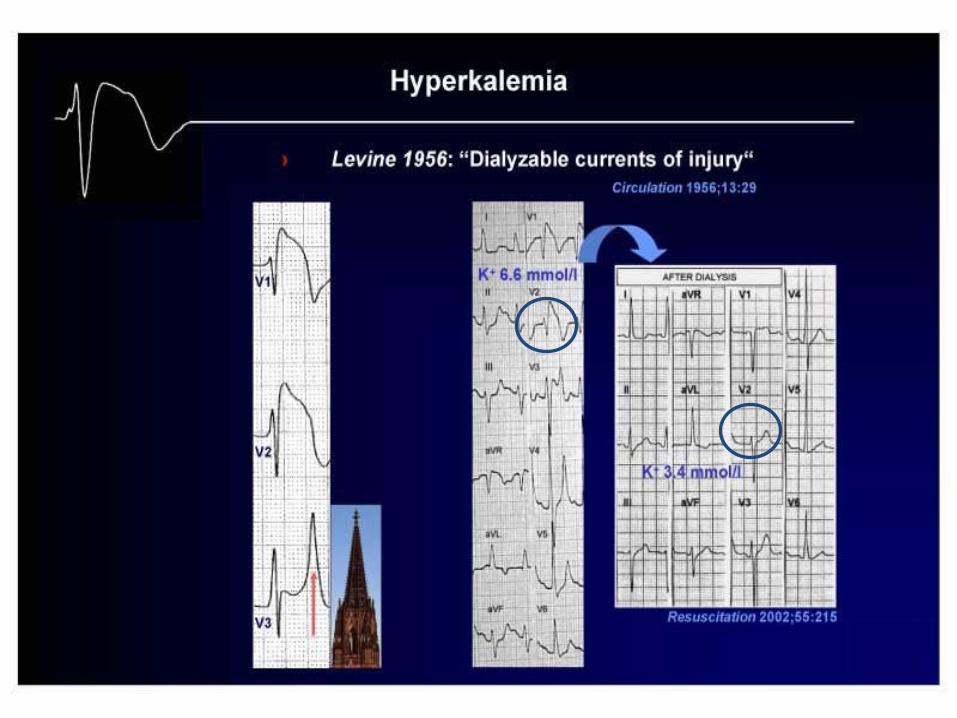
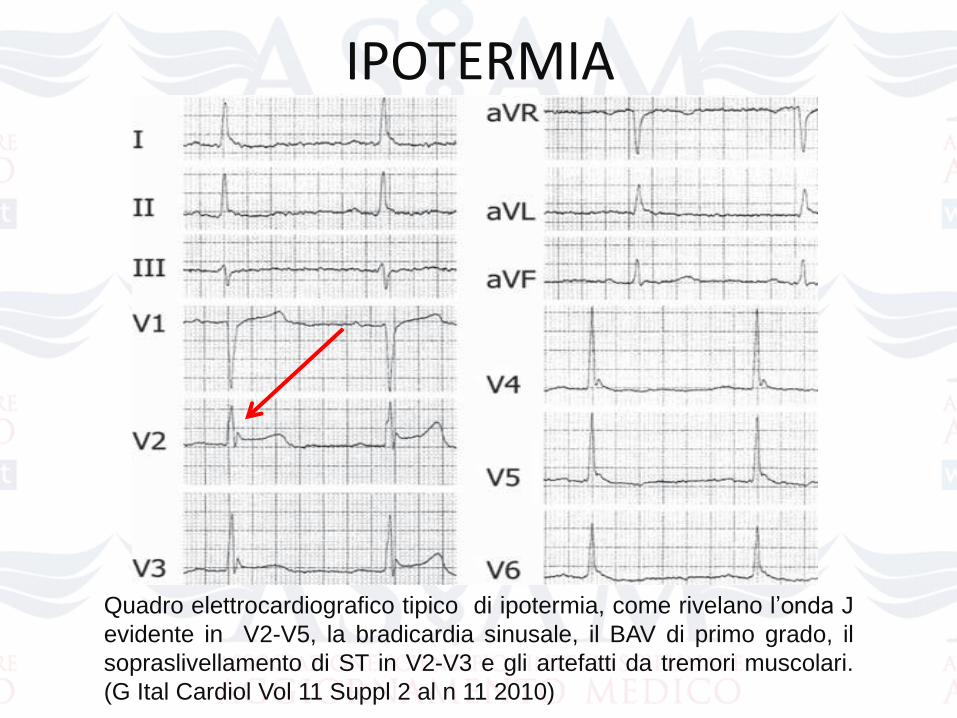
IPOTERMIA
Quadro elettrocardiografico tipico di ipotermia, come rivelano l’onda J
evidente in V2-V5, la bradicardia sinusale, il BAV di primo grado, il
sopraslivellamento di ST in V2-V3 e gli artefatti da tremori muscolari.
(G Ital Cardiol Vol 11 Suppl 2 al n 11 2010)
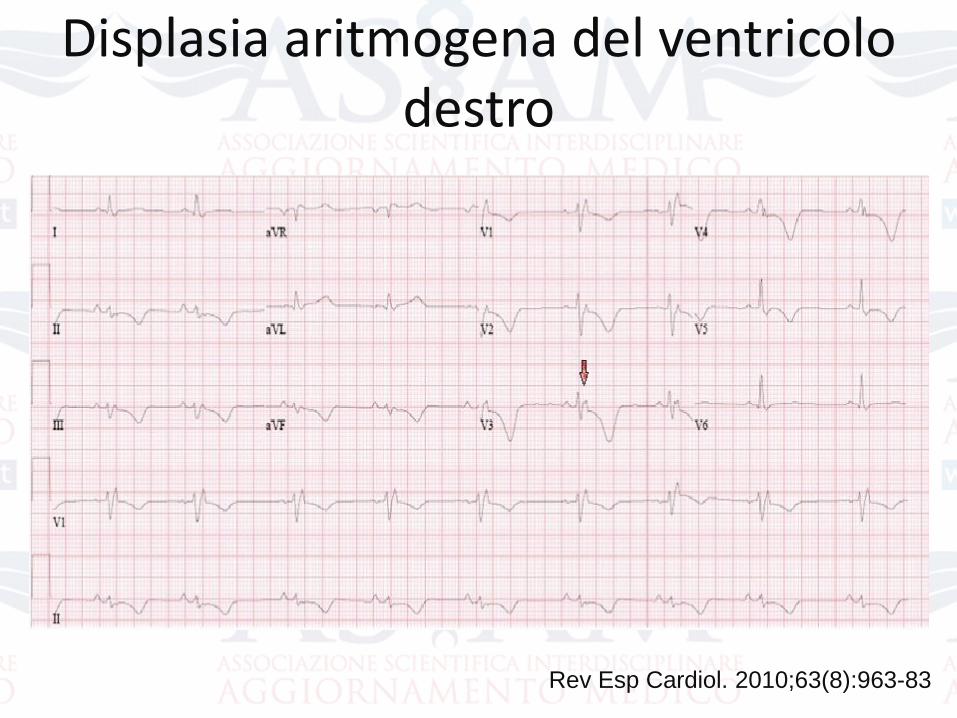
Displasia aritmogena del ventricolo destro
Rev Esp Cardiol. 2010;63(8):963-83
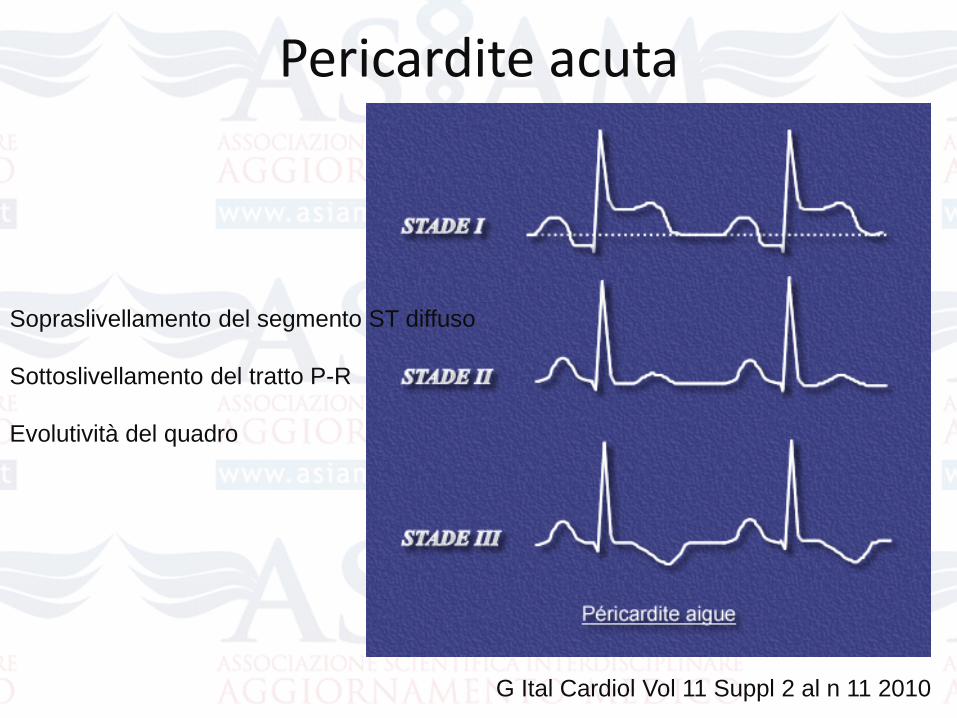
Sopraslivellamento del segmento ST diffuso
Sottoslivellamento del tratto P-R
Evolutività del quadro
Pericardite acuta
G Ital Cardiol Vol 11 Suppl 2 al n 11 2010
Sindrome di BrugadaCriteri diagnostici
Pattern ECG tipo 1 spontaneo o dopo farmaci AA del I
gruppo in associazione ad una delle seguenti condizioni:
FV o TV polimorfa documentate
Storia familiare di MI (età<45 anni)
Presenza di ECG di tipo 1 in membri della famiglia
Inducibilità di aritmie ventricolari con la SEP
Sincopi o respiro agonico notturno
To increase diagnostic sensitivity, the expert consensus statement of 2013 on inherited
arrhythmogenic diseases omits any clinical criterion and demands diagnostic ECG
changes in only one right precordial lead .
The saddle-back type 2 and type 3 ECG patterns are suspicious for, but not diagnostic
of BrS and the two patterns have now been grouped together into one type 2 ECG
(saddle-back pattern). When encountering a type 2 ECG the diagnosis of BrS may only
be made after drug-induced conversion to a type 1 ECG.
Because of frequent fluctuations between diagnostic, non-diagnostic, and normal ECGs
without ST-segment changes, repeated ECG recordings should be performed for
accurate risk stratification.
In asymptomatic patients, other ECG changes may support the diagnosis (5), such as:
● First-degree atrioventricular block
● Right bundle branch block
● Fragmented QRS complex
● Increased ST-segment elevation during exercise or during the recovery phase after
exercise
● Ventricular extrasystoles with left bundle branch block pattern
● Atrial fibrillation
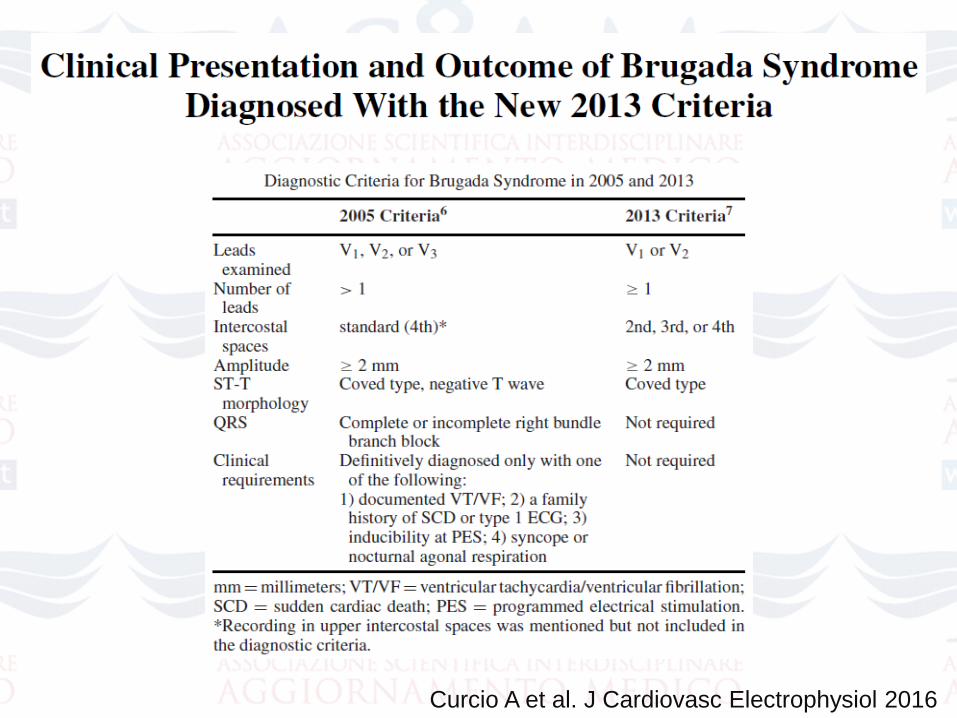
Curcio A et al. J Cardiovasc Electrophysiol 2016
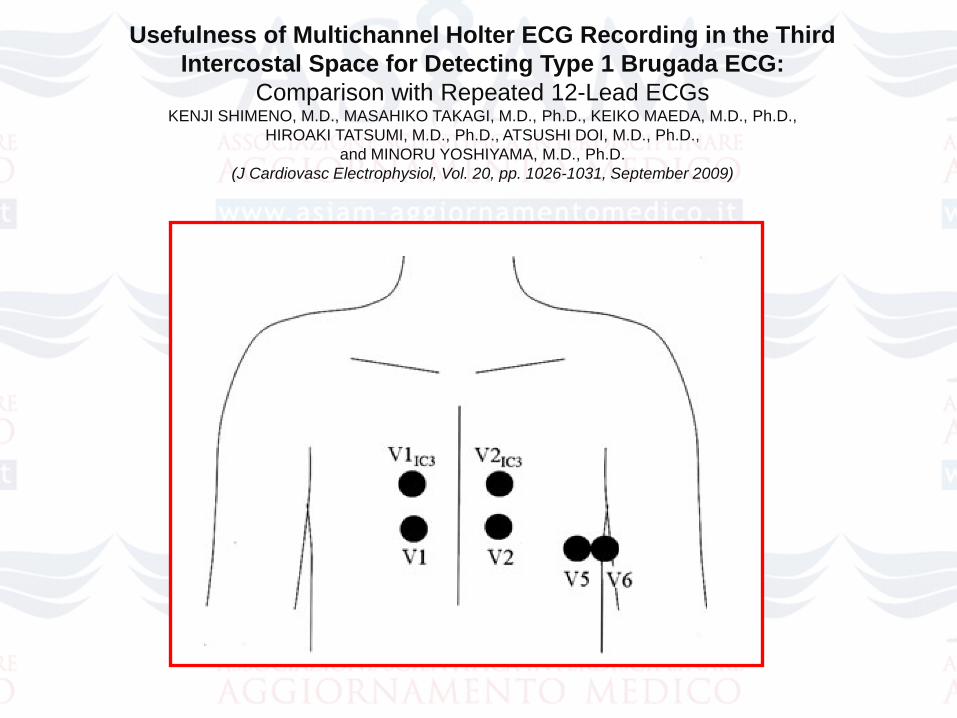
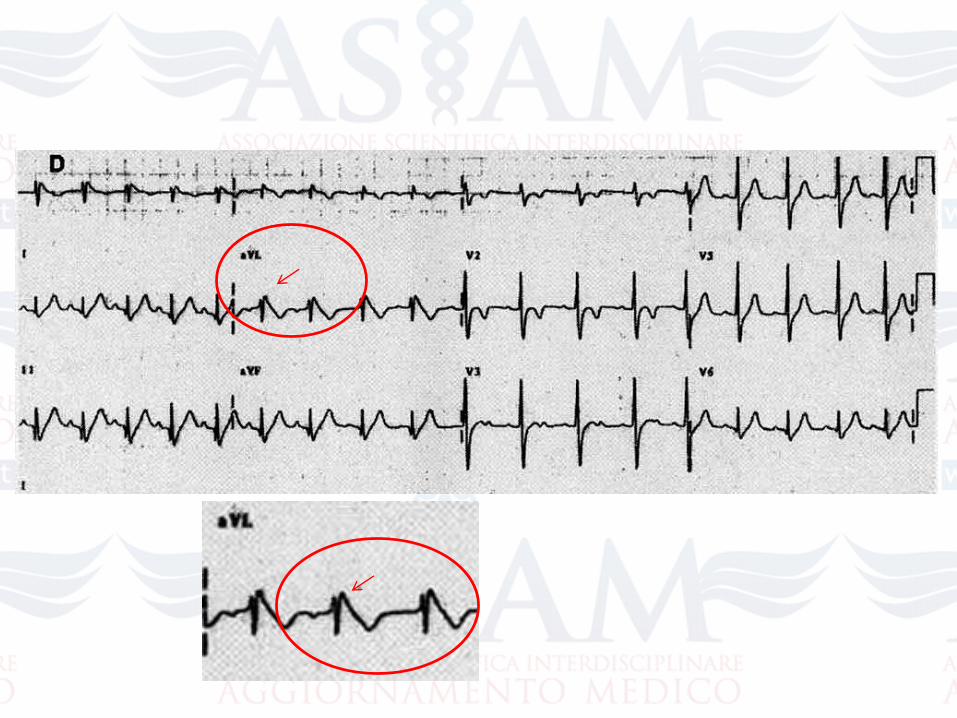
Usefulness of Multichannel Holter ECG Recording in the Third
Intercostal Space for Detecting Type 1 Brugada ECG:
Comparison with Repeated 12-Lead ECGsKENJI SHIMENO, M.D., MASAHIKO TAKAGI, M.D., Ph.D., KEIKO MAEDA, M.D., Ph.D.,
HIROAKI TATSUMI, M.D., Ph.D., ATSUSHI DOI, M.D., Ph.D.,
and MINORU YOSHIYAMA, M.D., Ph.D.
(J Cardiovasc Electrophysiol, Vol. 20, pp. 1026-1031, September 2009)
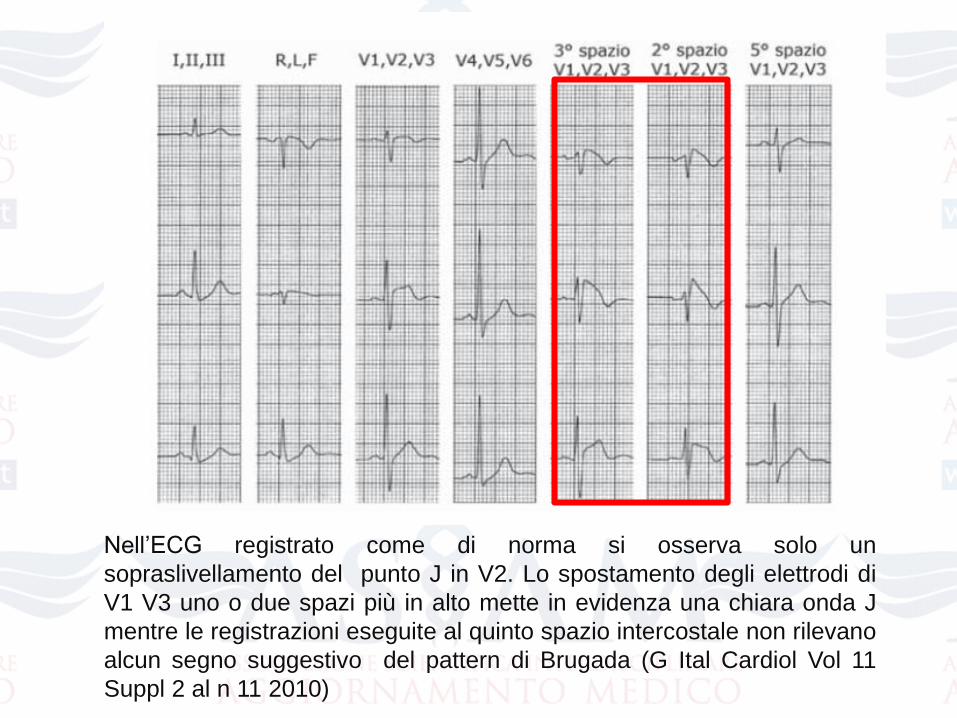
Nell’ECG registrato come di norma si osserva solo un
sopraslivellamento del punto J in V2. Lo spostamento degli elettrodi di
V1 V3 uno o due spazi più in alto mette in evidenza una chiara onda J
mentre le registrazioni eseguite al quinto spazio intercostale non rilevano
alcun segno suggestivo del pattern di Brugada (G Ital Cardiol Vol 11
Suppl 2 al n 11 2010)
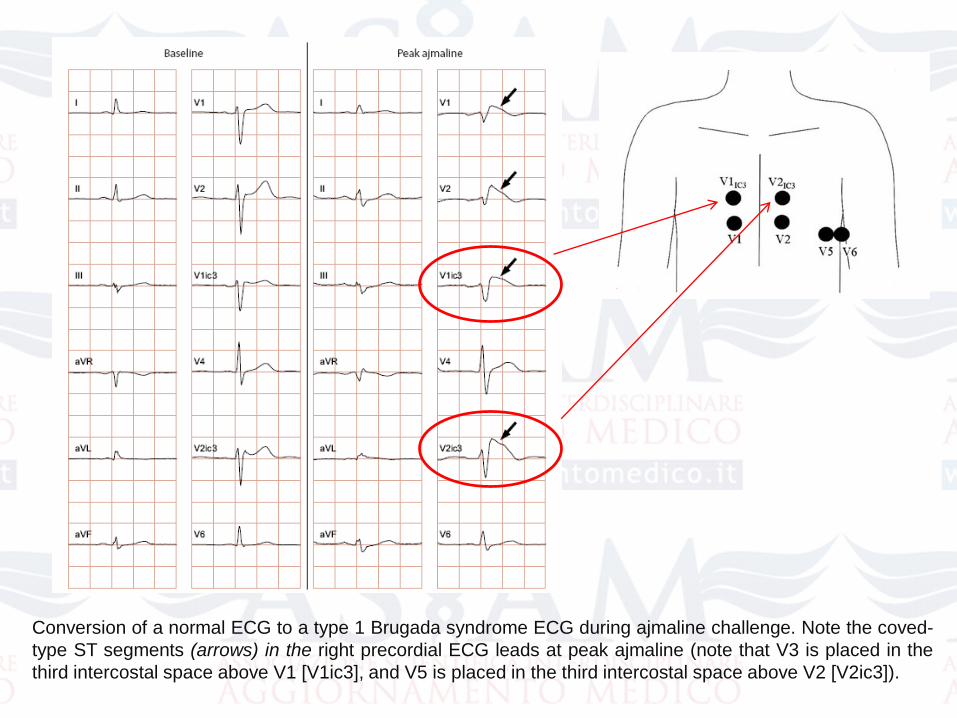
Conversion of a normal ECG to a type 1 Brugada syndrome ECG during ajmaline challenge. Note the coved-
type ST segments (arrows) in the right precordial ECG leads at peak ajmaline (note that V3 is placed in the
third intercostal space above V1 [V1ic3], and V5 is placed in the third intercostal space above V2 [V2ic3]).
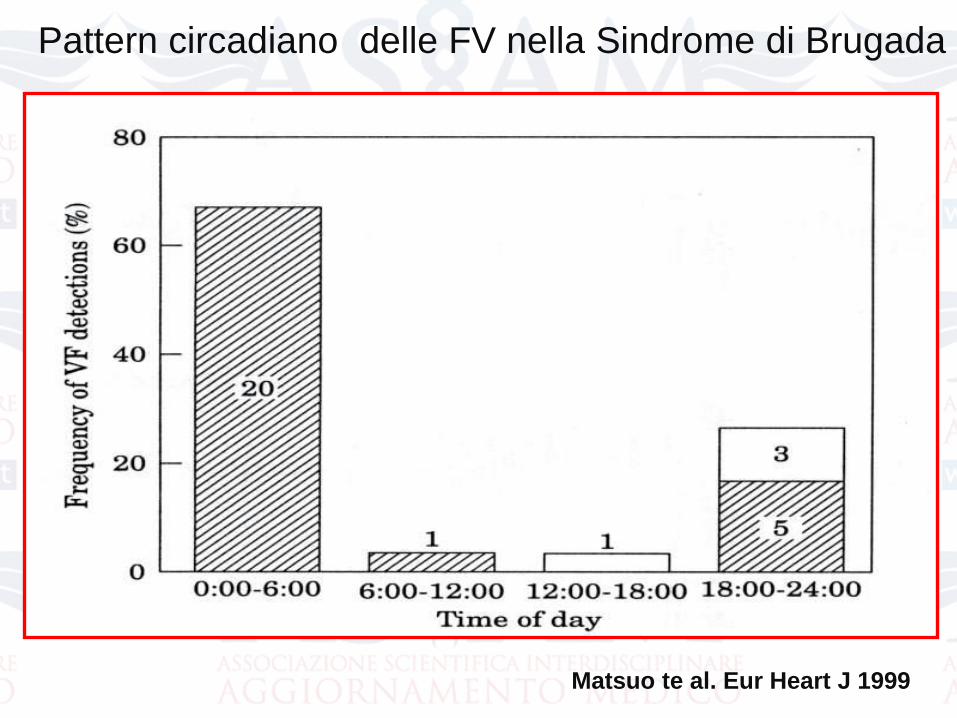
Pattern circadiano delle FV nella Sindrome di Brugada
Matsuo te al. Eur Heart J 1999
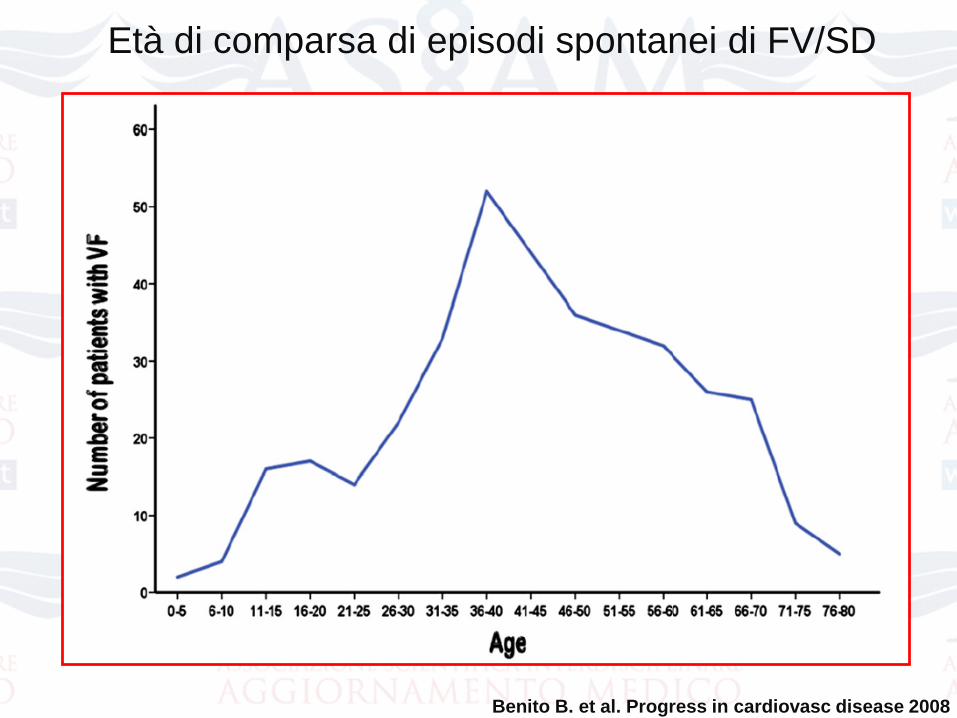
Età di comparsa di episodi spontanei di FV/SD
Benito B. et al. Progress in cardiovasc disease 2008
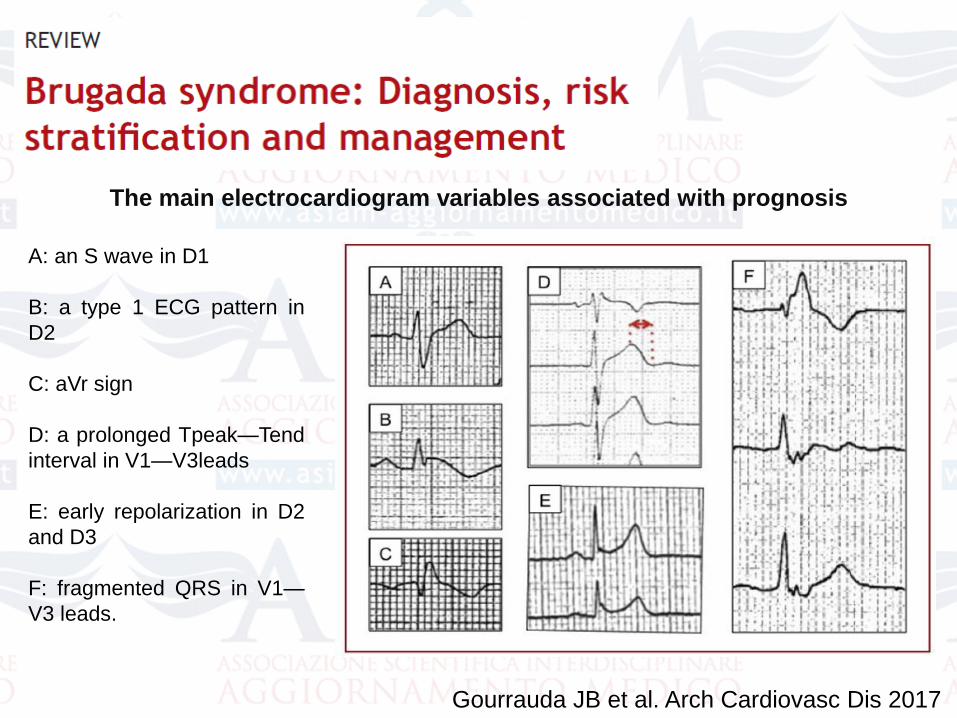
Gourrauda JB et al. Arch Cardiovasc Dis 2017
A: an S wave in D1
B: a type 1 ECG pattern in
D2
C: aVr sign
D: a prolonged Tpeak—Tend
interval in V1—V3leads
E: early repolarization in D2
and D3
F: fragmented QRS in V1—
V3 leads.
The main electrocardiogram variables associated with prognosis
Stratificazione del rischioRischio intermedio- rischio basso
• I pazienti con sincope hanno un rischio intermedio , essendo un gruppo estremamente eterogeneo potenzialmente costituito deipazienti con sincope aritmica e sincope neuromediata/non aritmica
Olde Nordkamp LR Heart Rhythm 2015
• I pazienti asintomatici hanno un rischio basso, ma non banale, di eventi cardiaci ( 0,5-1,5 % / anno ) e sono pertanto l'obiettivoprincipale della stratificazione del rischio. In questi pazienti ilvalore dello studio elettrofisiologico per la stratificazione del rischio rimane ad oggi il punto di maggior dibattito
Probst V et al FINGER registry Circulation 2010
Priori SG et al PRELUDE registry JACC 2012
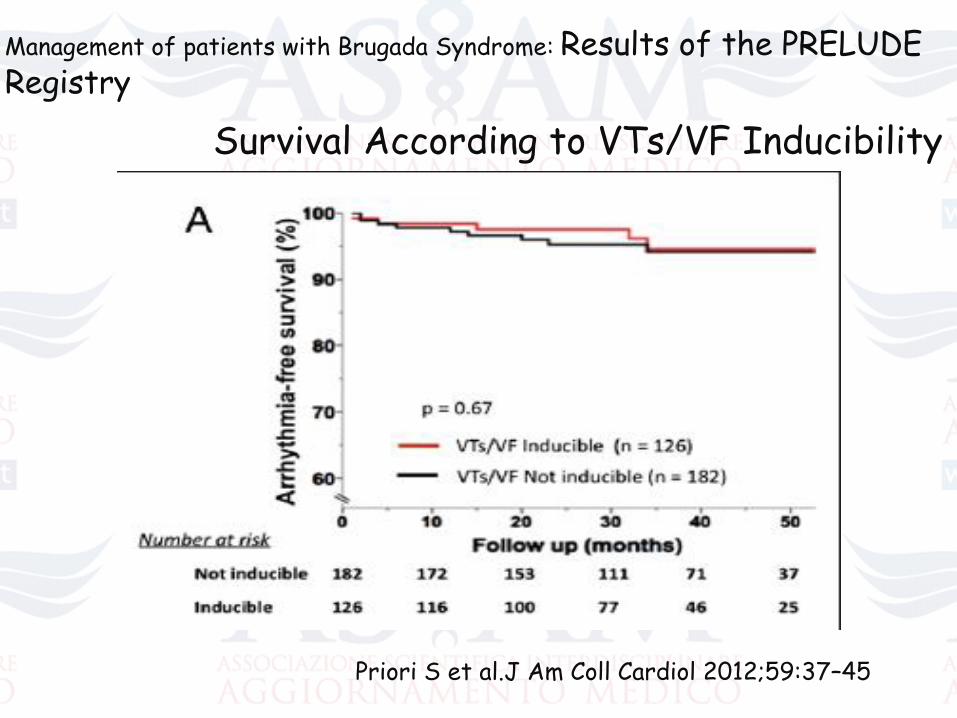
Management of patients with Brugada Syndrome: Results of the PRELUDE Registry
Survival According to VTs/VF Inducibility
Priori S et al.J Am Coll Cardiol 2012;59:37–45
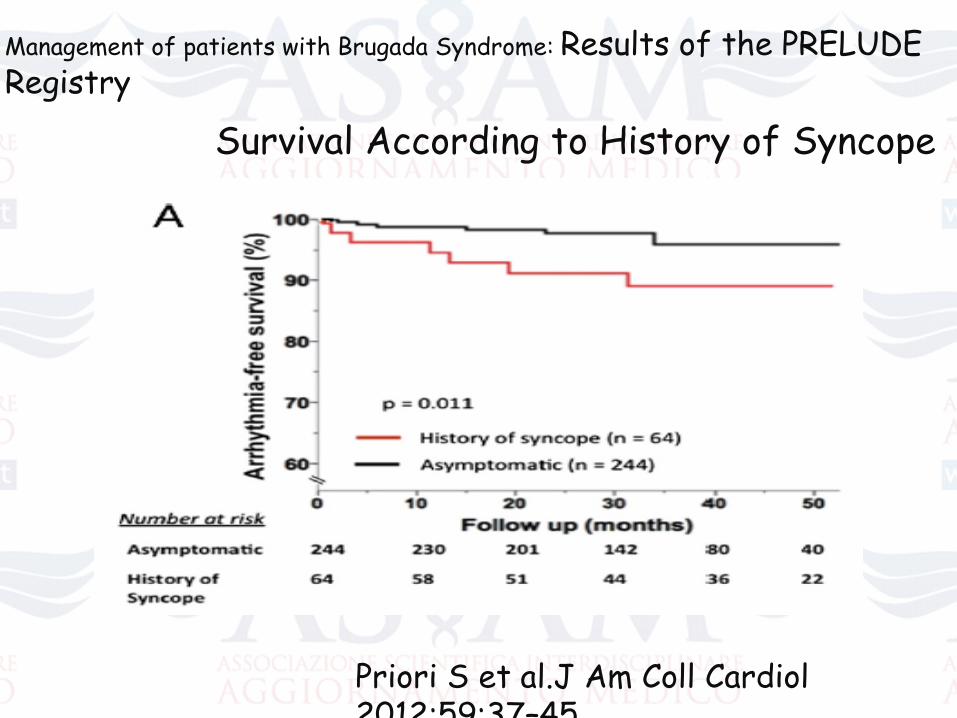
Management of patients with Brugada Syndrome: Results of the PRELUDE Registry
Survival According to History of Syncope
Priori S et al.J Am Coll Cardiol2012;59:37–45
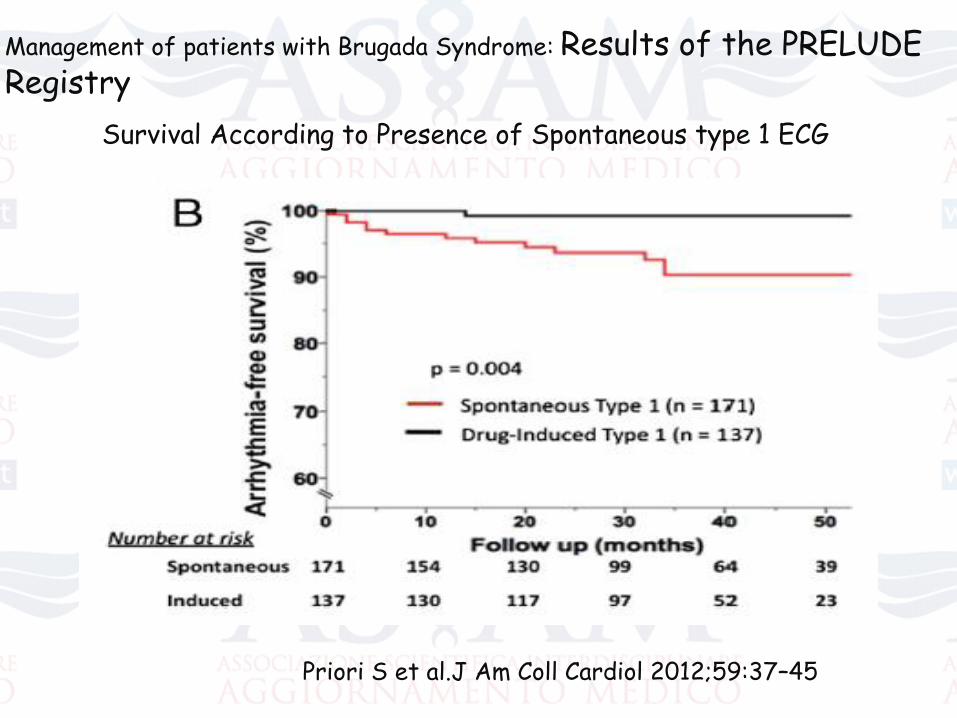
Management of patients with Brugada Syndrome: Results of the PRELUDE Registry
Survival According to Presence of Spontaneous type 1 ECG
Priori S et al.J Am Coll Cardiol 2012;59:37–45
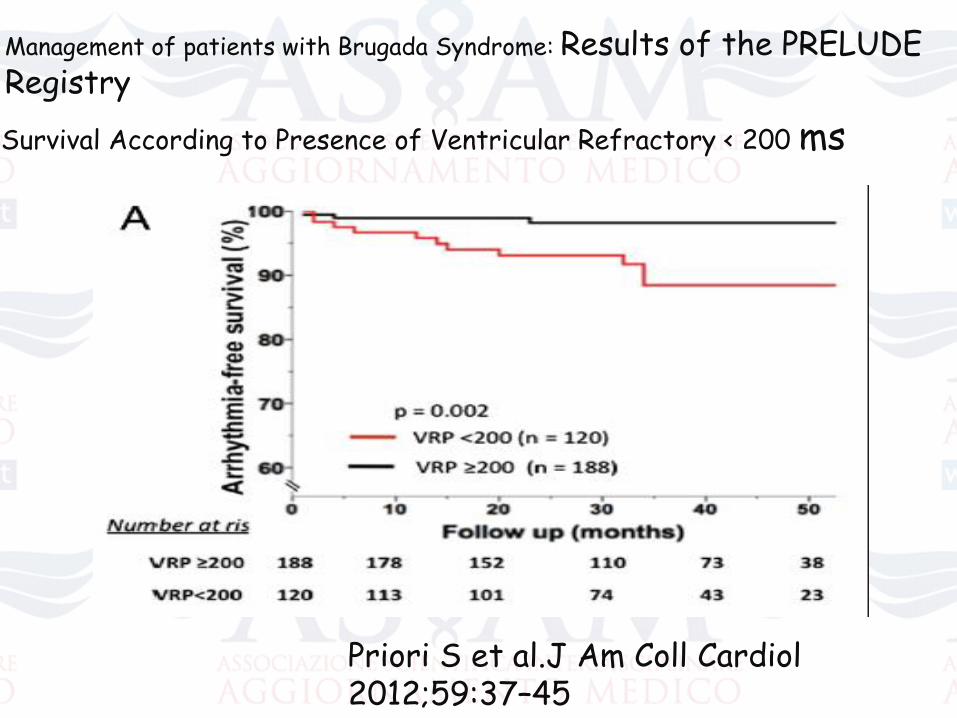
Management of patients with Brugada Syndrome: Results of the PRELUDE Registry
Survival According to Presence of Ventricular Refractory < 200 ms
Priori S et al.J Am Coll Cardiol2012;59:37–45
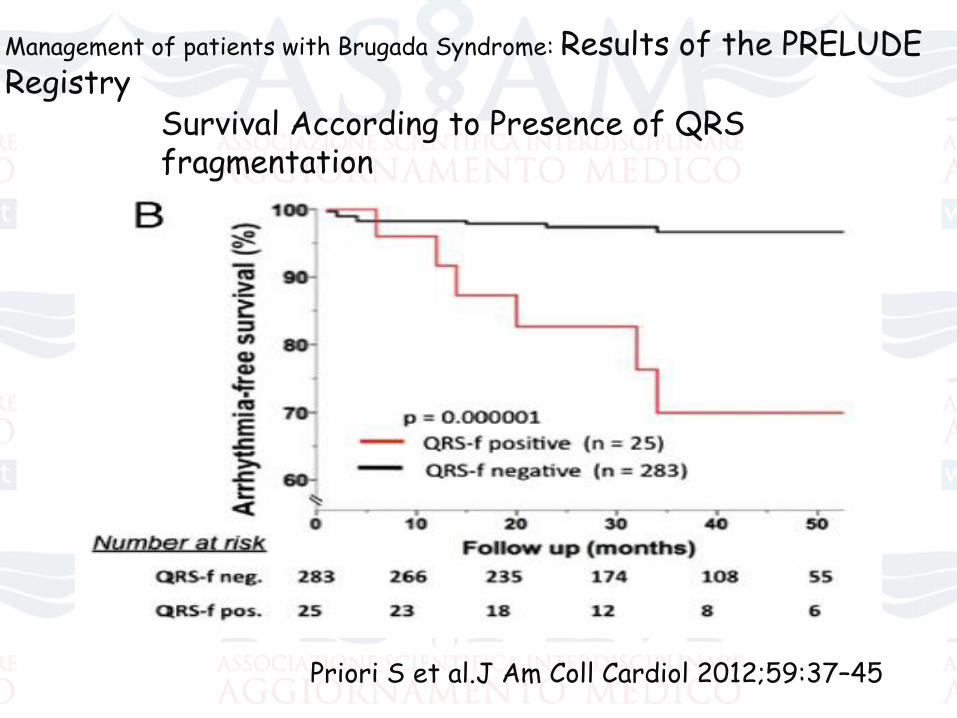
Management of patients with Brugada Syndrome: Results of the PRELUDE Registry
Survival According to Presence of QRS fragmentation
Priori S et al.J Am Coll Cardiol 2012;59:37–45
Priori S et al.J Am Coll Cardiol 2012;59:37–45
CONCLUSION: Our data show that VT/VF inducibility is unable
to identify high-risk patients, whereas the presence of a
spontaneous type I ECG, history of syncope, ventricular
effective refractory period 200 ms, and QRS fragmentation
seem useful to identify candidates for prophylactic implantable
cardioverter defibrillator.
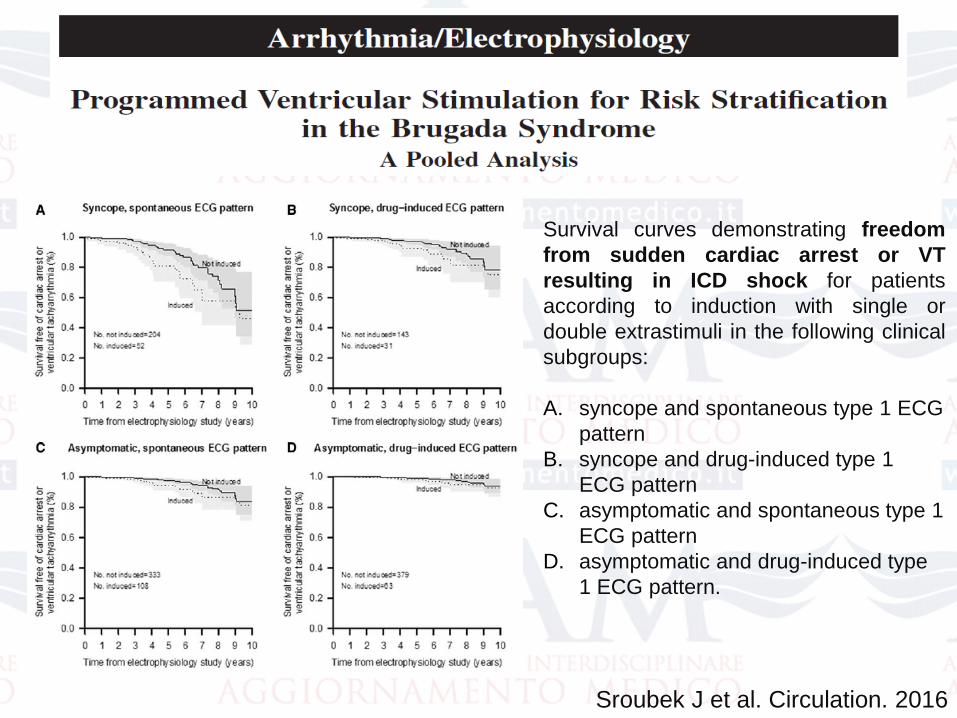
Sroubek J et al. Circulation. 2016
Survival curves demonstrating freedom
from sudden cardiac arrest or VT
resulting in ICD shock for patients
according to induction with single or
double extrastimuli in the following clinical
subgroups:
A. syncope and spontaneous type 1 ECG
pattern
B. syncope and drug-induced type 1
ECG pattern
C. asymptomatic and spontaneous type 1
ECG pattern
D. asymptomatic and drug-induced type
1 ECG pattern.
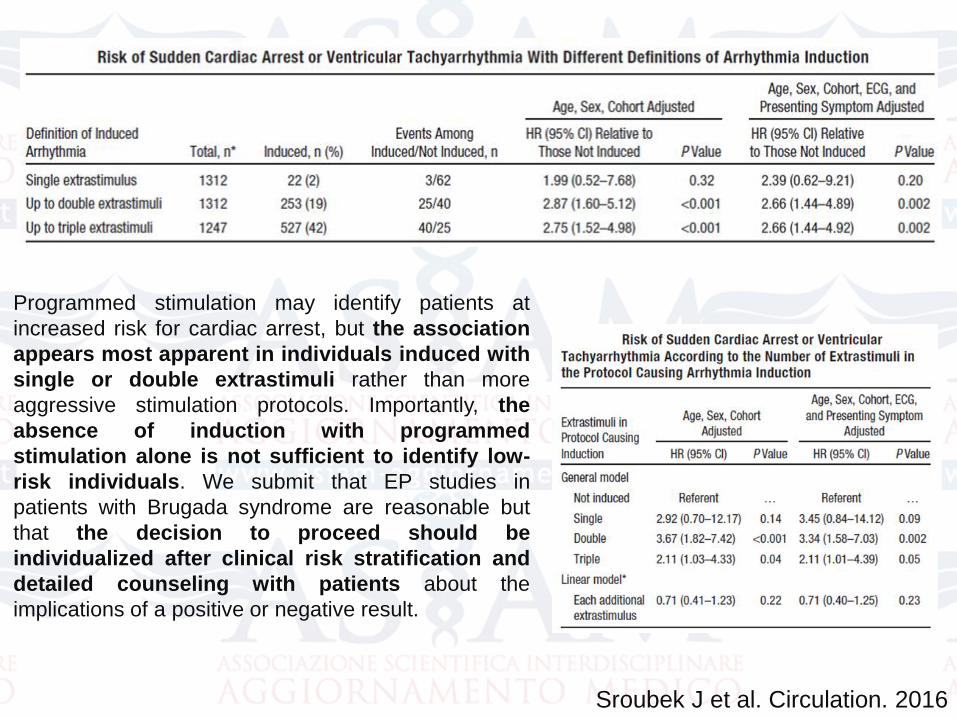
Programmed stimulation may identify patients at
increased risk for cardiac arrest, but the association
appears most apparent in individuals induced with
single or double extrastimuli rather than more
aggressive stimulation protocols. Importantly, the
absence of induction with programmed
stimulation alone is not sufficient to identify low-
risk individuals. We submit that EP studies in
patients with Brugada syndrome are reasonable but
that the decision to proceed should be
individualized after clinical risk stratification and
detailed counseling with patients about the
implications of a positive or negative result.
Sroubek J et al. Circulation. 2016
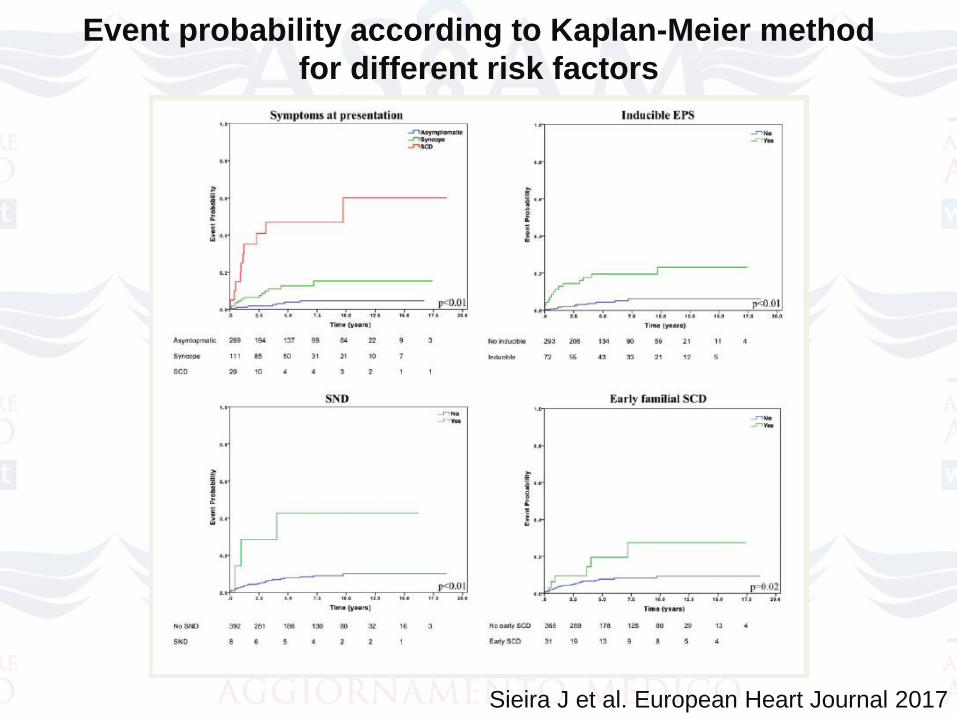
Event probability according to Kaplan-Meier method
for different risk factors
Sieira J et al. European Heart Journal 2017
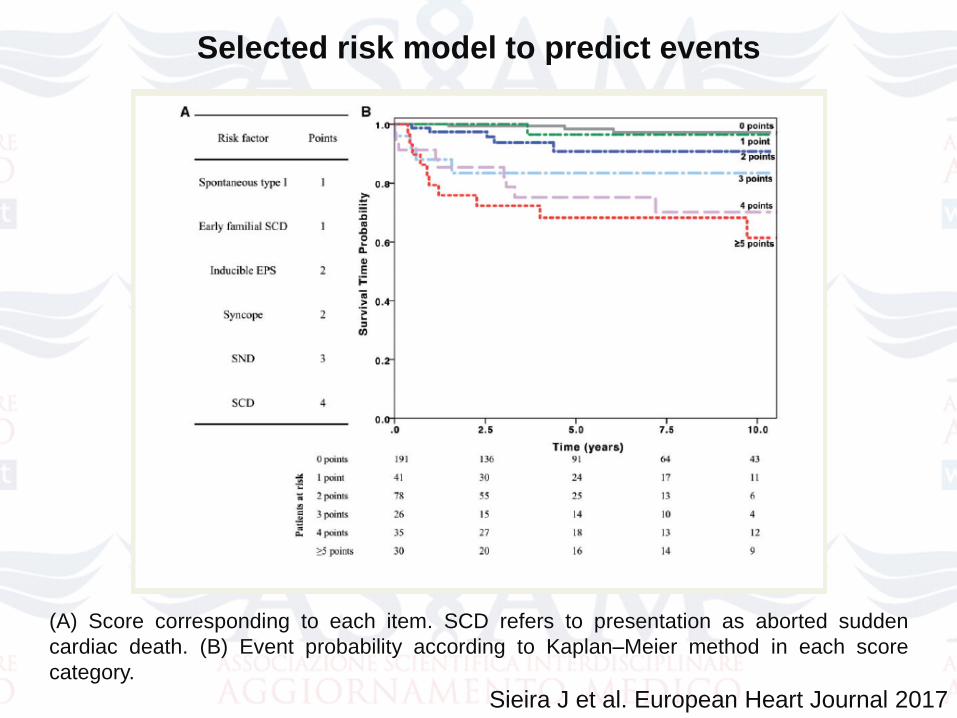
(A) Score corresponding to each item. SCD refers to presentation as aborted sudden
cardiac death. (B) Event probability according to Kaplan–Meier method in each score
category.
Selected risk model to predict events
Sieira J et al. European Heart Journal 2017
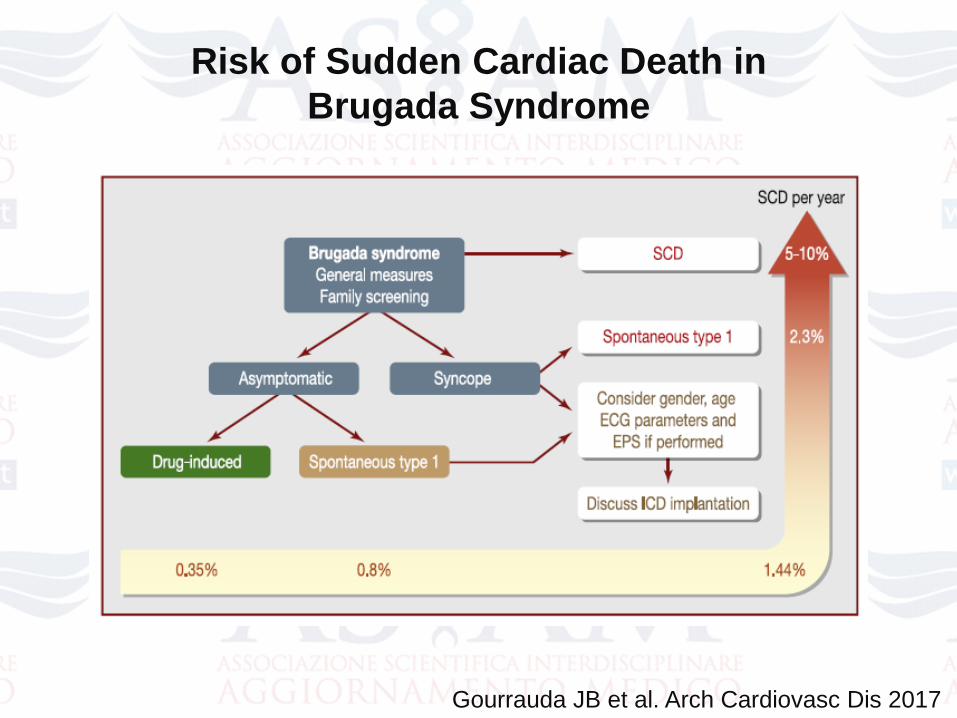
Risk of Sudden Cardiac Death in
Brugada Syndrome
Gourrauda JB et al. Arch Cardiovasc Dis 2017
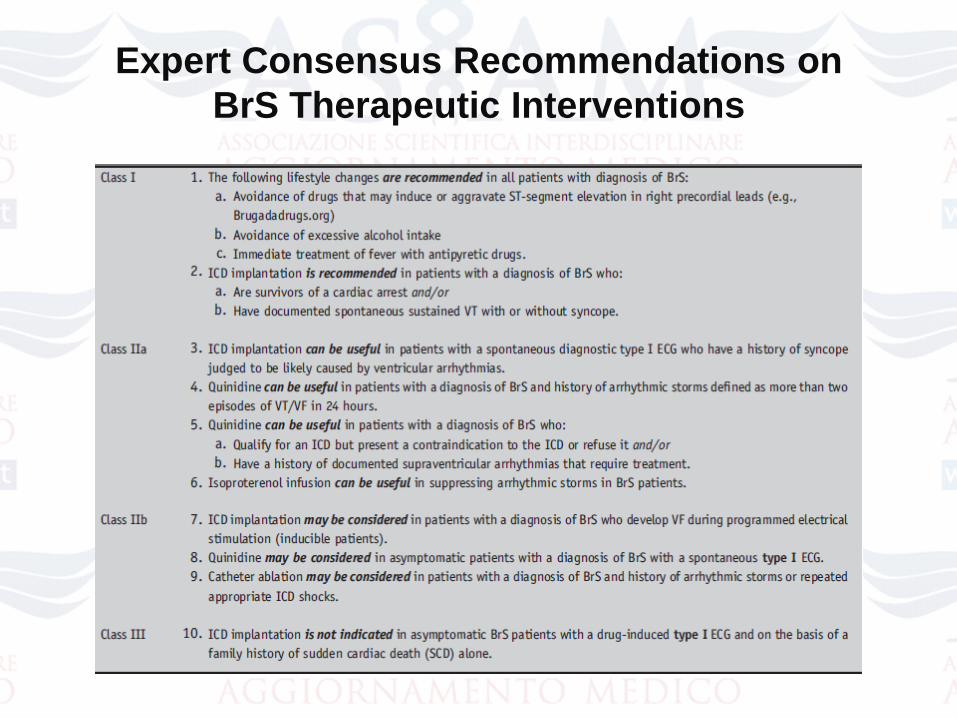
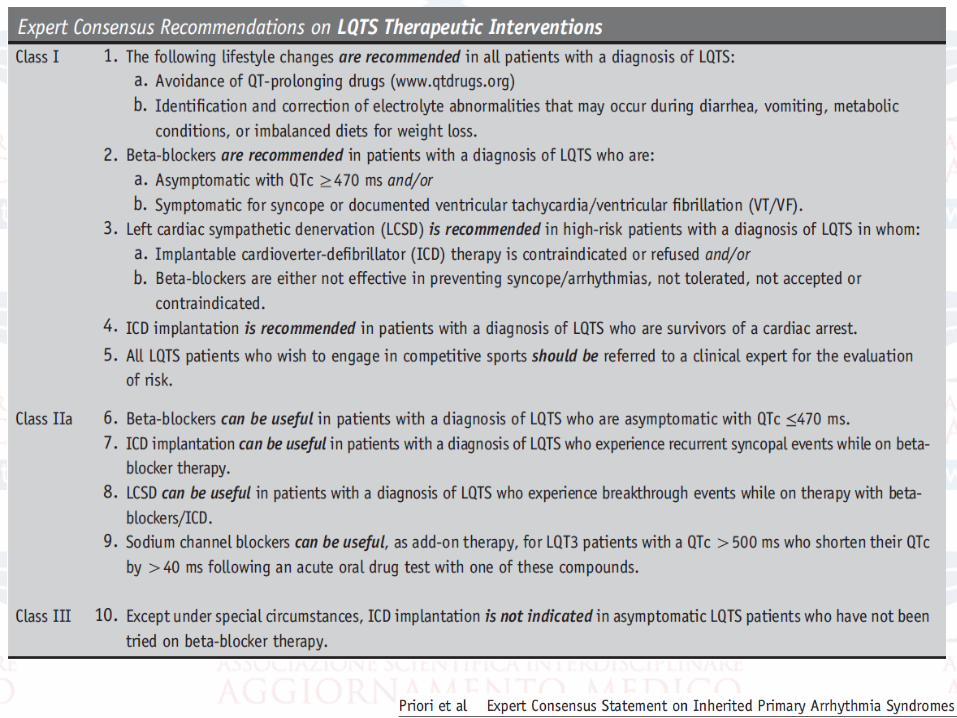
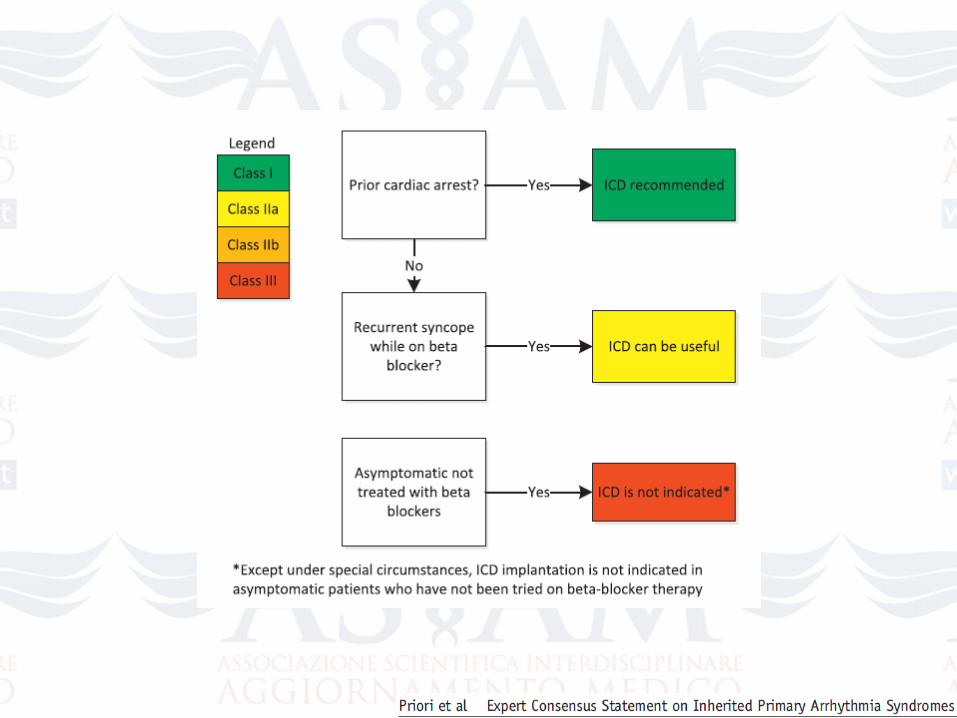
Expert Consensus Recommendations on
BrS Therapeutic Interventions
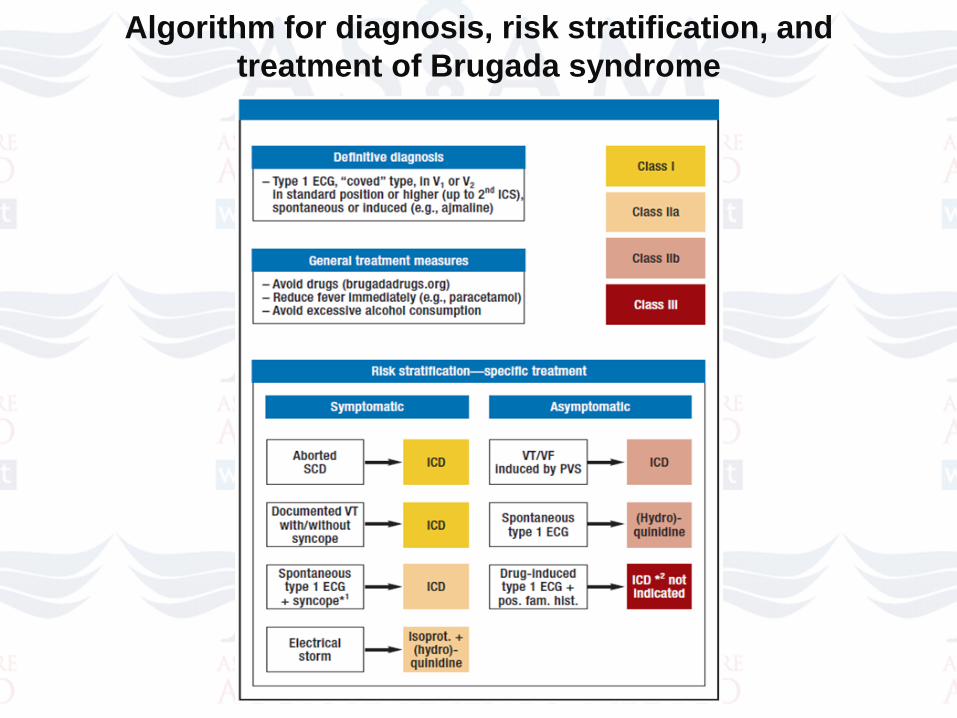
Algorithm for diagnosis, risk stratification, and
treatment of Brugada syndrome
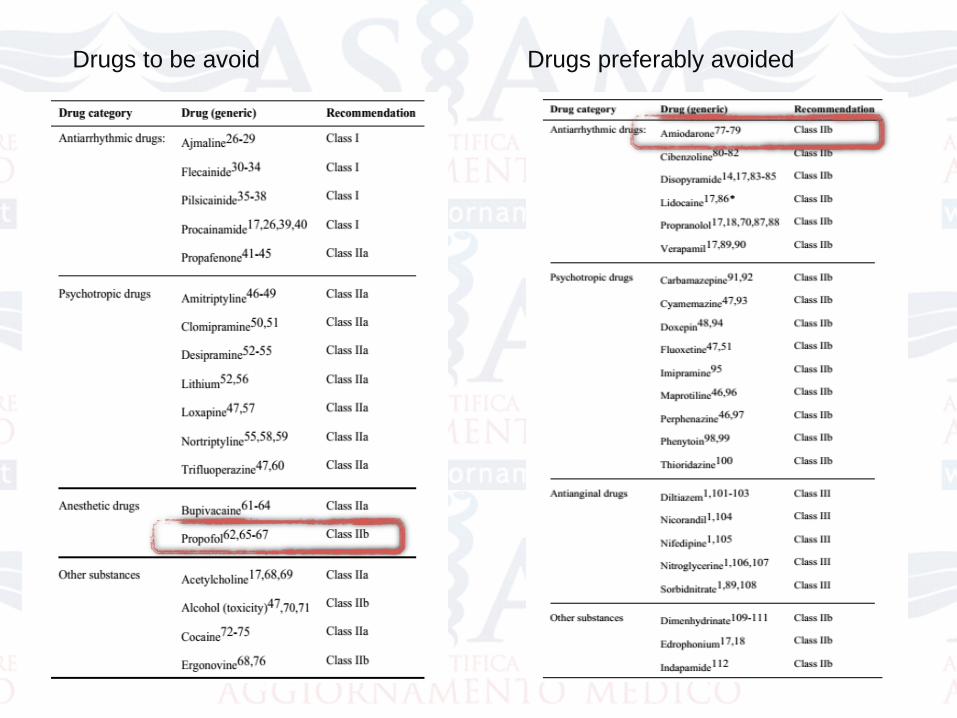
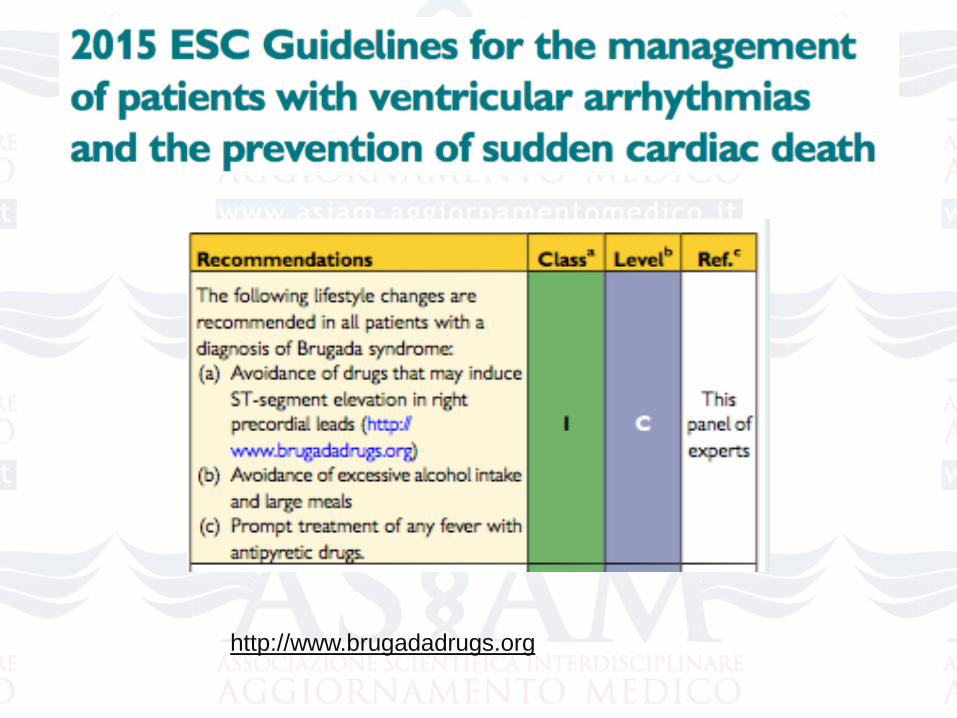
Drugs to be avoid Drugs preferably avoided
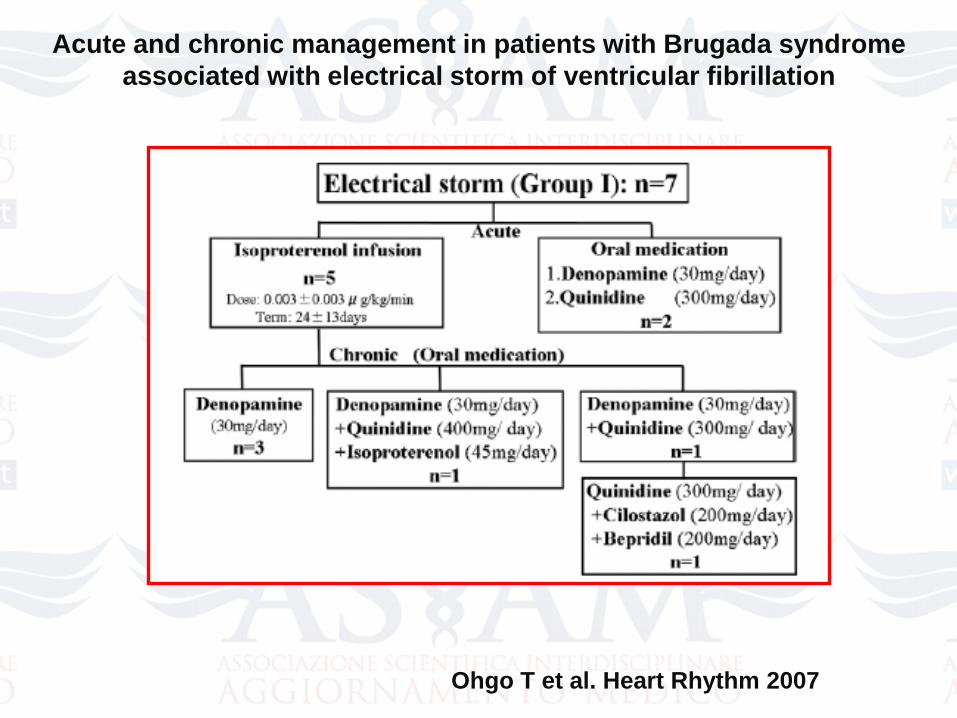
Ohgo T et al. Heart Rhythm 2007
Acute and chronic management in patients with Brugada syndrome
associated with electrical storm of ventricular fibrillation
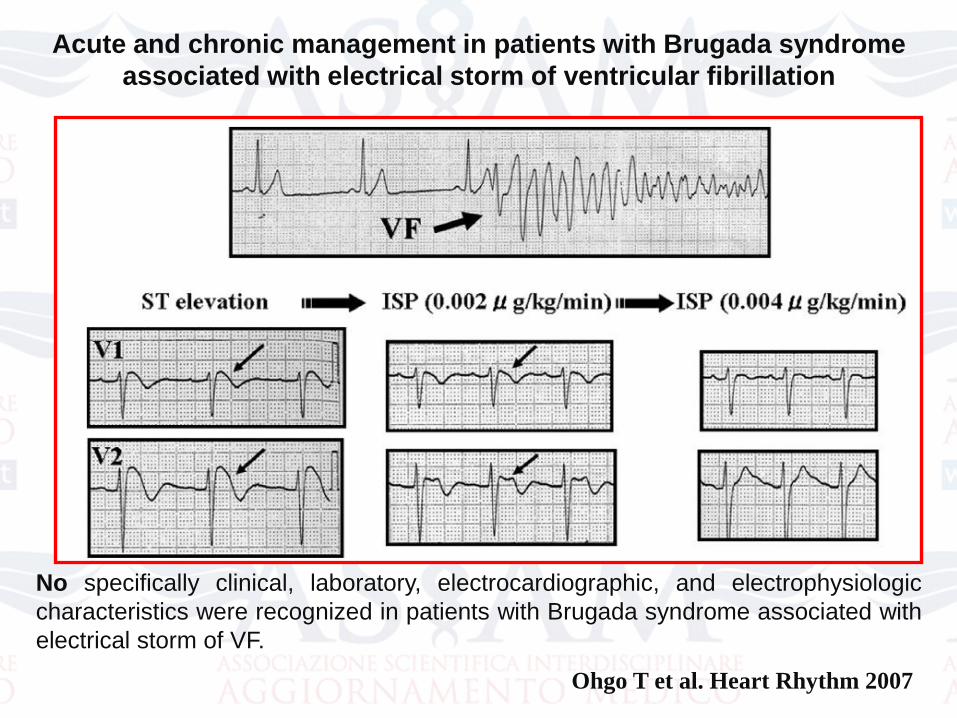
Acute and chronic management in patients with Brugada syndrome
associated with electrical storm of ventricular fibrillation
No specifically clinical, laboratory, electrocardiographic, and electrophysiologic
characteristics were recognized in patients with Brugada syndrome associated with
electrical storm of VF.
Ohgo T et al. Heart Rhythm 2007
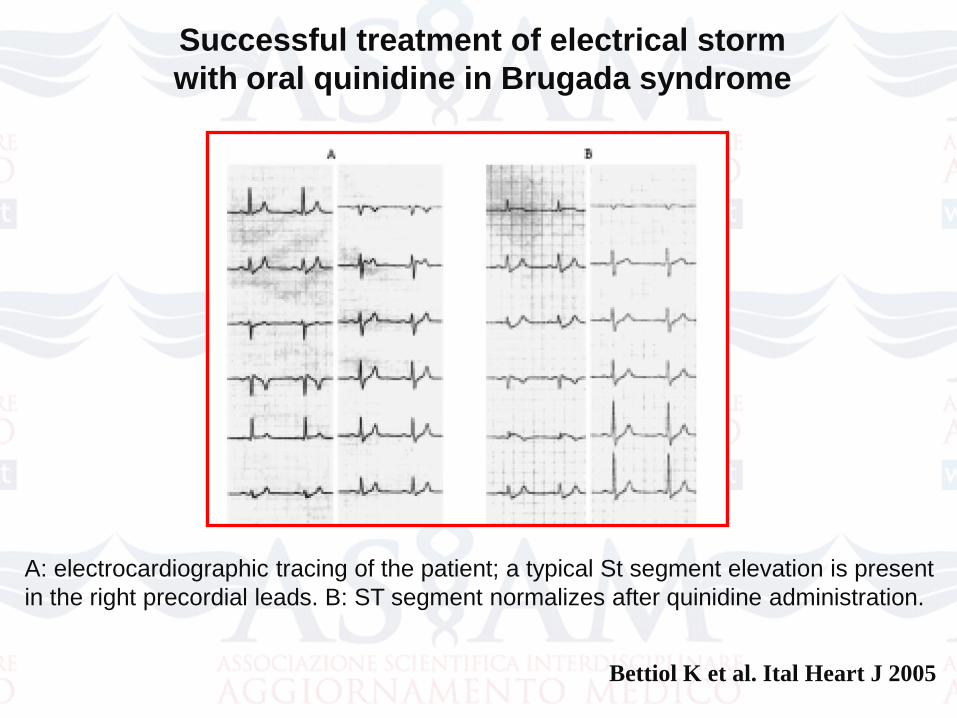
Successful treatment of electrical storm
with oral quinidine in Brugada syndrome
A: electrocardiographic tracing of the patient; a typical St segment elevation is present
in the right precordial leads. B: ST segment normalizes after quinidine administration.
Bettiol K et al. Ital Heart J 2005
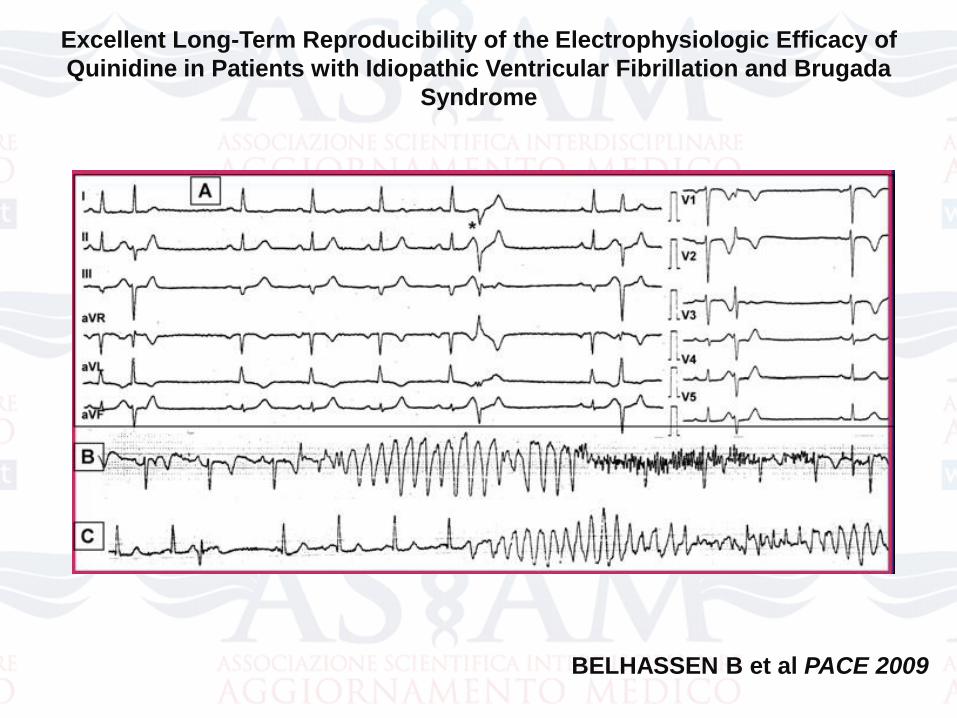
Excellent Long-Term Reproducibility of the Electrophysiologic Efficacy of
Quinidine in Patients with Idiopathic Ventricular Fibrillation and Brugada
Syndrome
BELHASSEN B et al PACE 2009
Farmaci antiaritmici nella S di Br
• Chinidina: blocca la corrente Ito; elimina i rientri in fase 2; effettovagolitico
Belhassen 2004: chinidina 1500 mg/die;
Hermida 2004: chinidina 600-900 mg/die;
Mitzurawo 2006: chinidina 300-600 mg/die; prevenzione inducibiltàrispettivamente nel 88%,76%, 44%.
• Procainamide: proaritmia.
• Disopiramide: blocca i canali K+ ed anche Ito;effetto vagolitico.
• Farmaci AA classe 1C: proaritmia
• Farmaci AA classe 2: betabloccanti. Non prevengono la MI
Sacher F et al, Circulation 2006
The aim of this study was to evaluate long-term outcome in a
large series of patients implanted with an ICD for a diagnosis of
Brugada syndrome.
The major finding of this study is that during a follow-up period of
> 3 years after implantation, there is a 2.5 fold greater
frequency of inappropriate (20%) than appropriate shocks
(8%), with an overall complication rate of 28%.
No arrhythmic death occurred at implantation or during
follow-up in this young, otherwise healthy population.
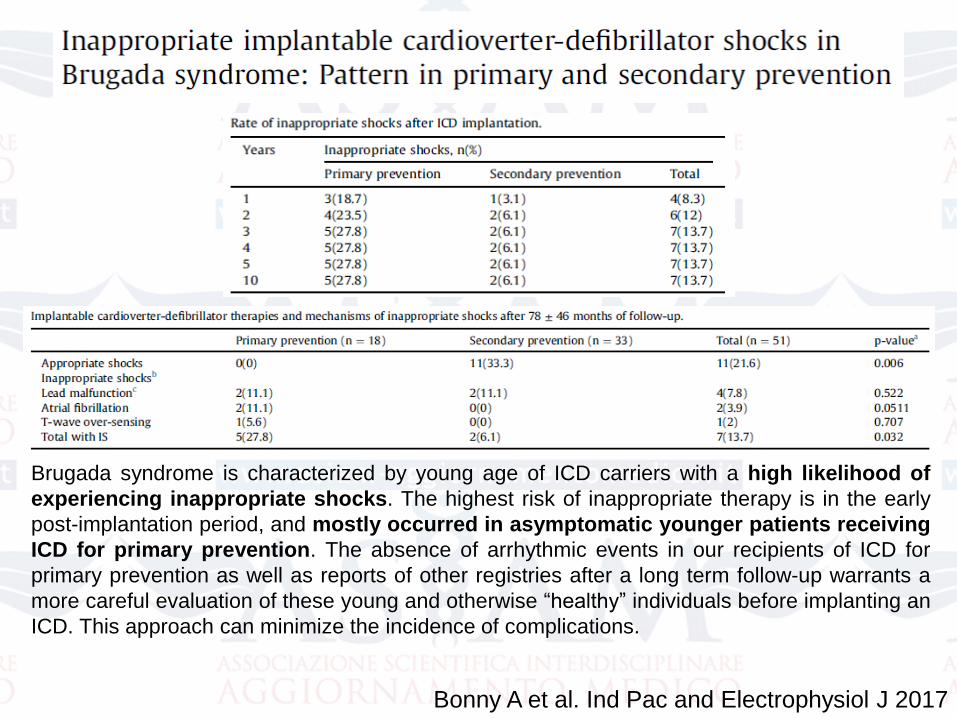
Brugada syndrome is characterized by young age of ICD carriers with a high likelihood of
experiencing inappropriate shocks. The highest risk of inappropriate therapy is in the early
post-implantation period, and mostly occurred in asymptomatic younger patients receiving
ICD for primary prevention. The absence of arrhythmic events in our recipients of ICD for
primary prevention as well as reports of other registries after a long term follow-up warrants a
more careful evaluation of these young and otherwise “healthy” individuals before implanting an
ICD. This approach can minimize the incidence of complications.
Bonny A et al. Ind Pac and Electrophysiol J 2017
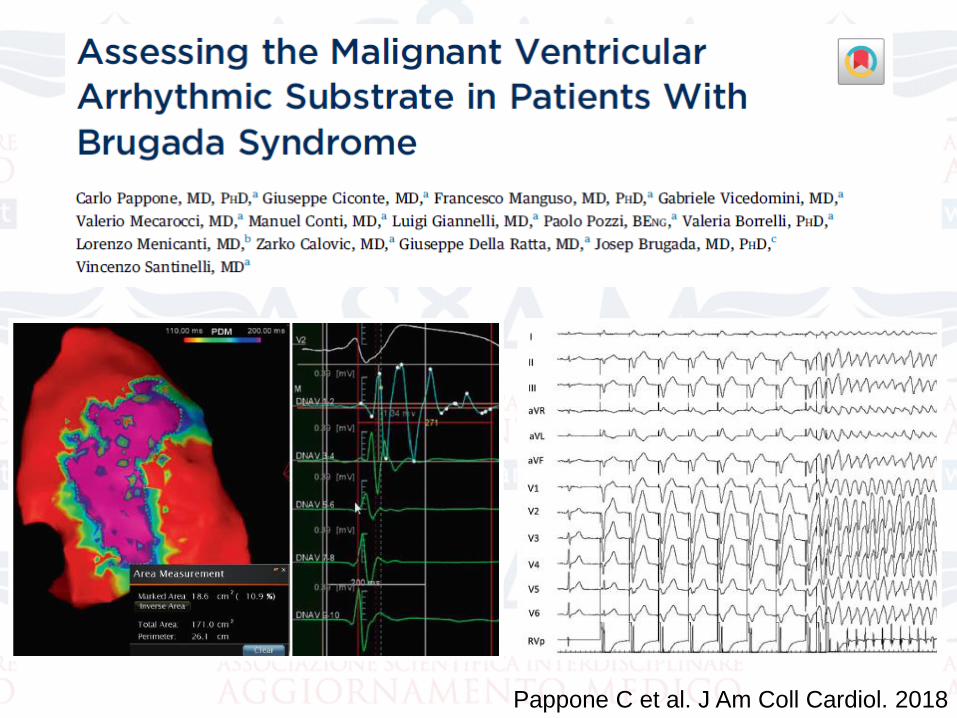
Pappone C et al. J Am Coll Cardiol. 2018
Pappone C et al. J Am Coll Cardiol. 2018
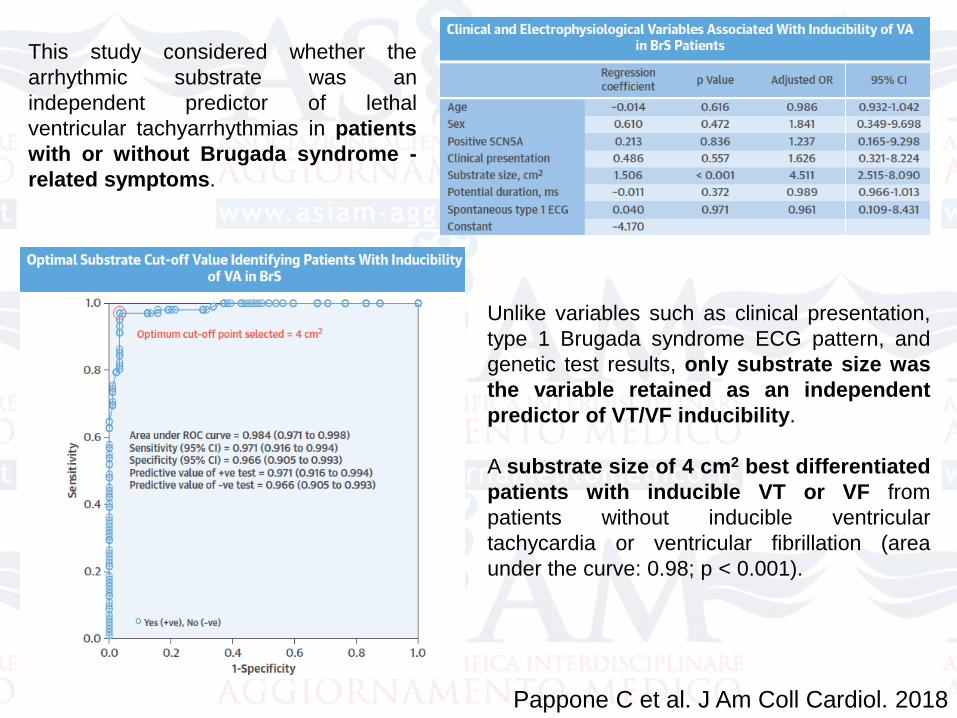
Unlike variables such as clinical presentation,
type 1 Brugada syndrome ECG pattern, and
genetic test results, only substrate size was
the variable retained as an independent
predictor of VT/VF inducibility.
A substrate size of 4 cm2 best differentiated
patients with inducible VT or VF from
patients without inducible ventricular
tachycardia or ventricular fibrillation (area
under the curve: 0.98; p < 0.001).
This study considered whether the
arrhythmic substrate was an
independent predictor of lethal
ventricular tachyarrhythmias in patients
with or without Brugada syndrome -
related symptoms.
This study demonstrates that among patients with BrS
the extent of substrate is the only independent
predictor of inducibility of VT or VF and may serve
as a new marker for risk stratification and therapy.
Substrate elimination by RF catheter ablation is
associated with no VT or VF inducibility.
Understanding the site and electrophysiology of
arrhythmic substrate can facilitate recognition of
patients at higher risk for VT or VF, thus providing
an understanding of therapeutic options and limitations
and suggesting avenues for future investigations.
Conclusions
Pappone C et al. J Am Coll Cardiol. 2018
Pappone C et al. Circ Arrhythm Electrophysiol. 2017
Pappone C et al. Circ Arrhythm Electrophysiol. 2017
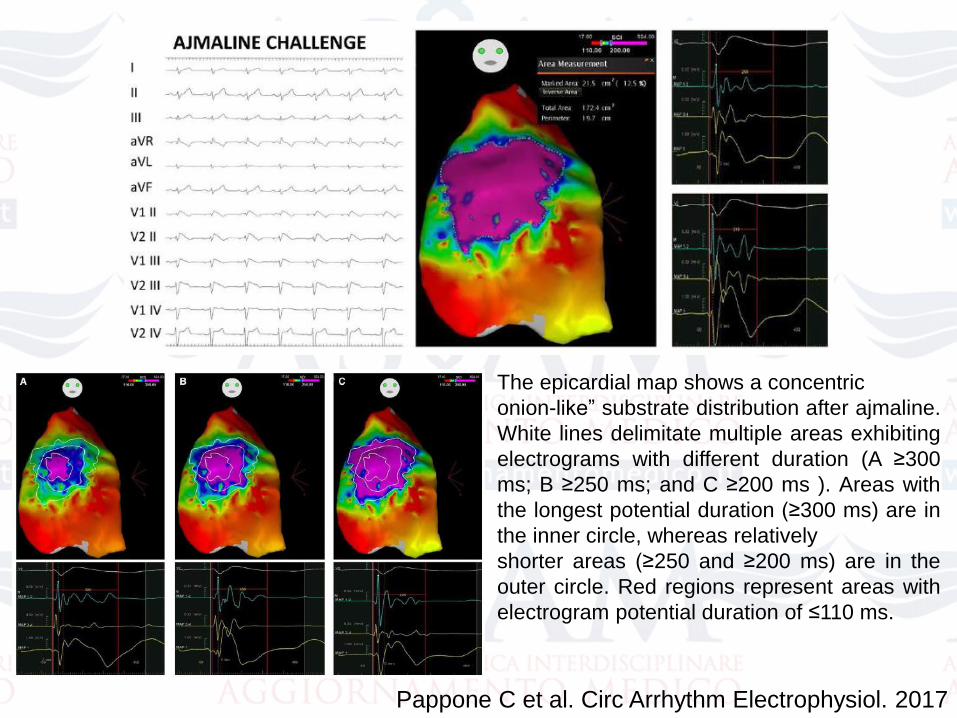
The epicardial map shows a concentric
onion-like” substrate distribution after ajmaline.
White lines delimitate multiple areas exhibiting
electrograms with different duration (A ≥300
ms; B ≥250 ms; and C ≥200 ms ). Areas with
the longest potential duration (≥300 ms) are in
the inner circle, whereas relatively
shorter areas (≥250 and ≥200 ms) are in the
outer circle. Red regions represent areas with
electrogram potential duration of ≤110 ms.
Pappone C et al. Circ Arrhythm Electrophysiol. 2017
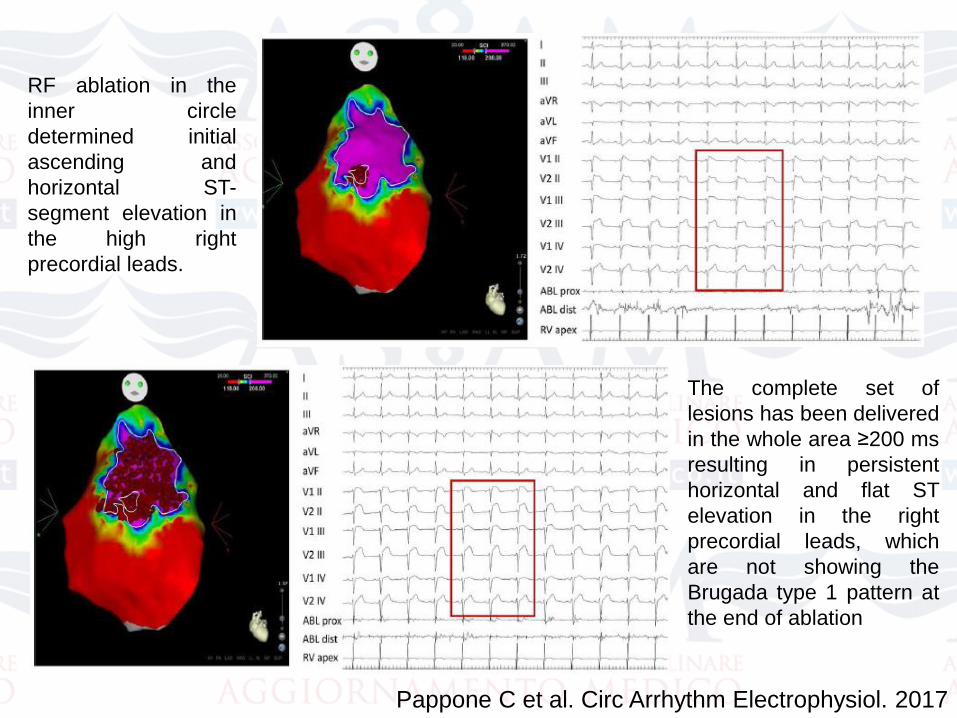
RF ablation in the
inner circle
determined initial
ascending and
horizontal ST-
segment elevation in
the high right
precordial leads.
The complete set of
lesions has been delivered
in the whole area ≥200 ms
resulting in persistent
horizontal and flat ST
elevation in the right
precordial leads, which
are not showing the
Brugada type 1 pattern at
the end of ablation
In summary, the results of this prospective study in a large cohort
of consecutive BrS patients with various clinical
presentations, who represent the vast majority of patients
currently diagnosed with BrS, have provided new information and
insights into understanding of the pathophysiological substrate,
mechanism, and management of the disease. We conclude that
electro-physiologically and anatomically welldefined extensive
abnormal epicardial areas, as exposed by ajmaline administration,
are the primary site for BrS substrate and are responsible for type
1 BrS-ECG pattern and VT/VF inducibility. Persistent ECG pattern
normalization without VF inducibility even after repeated
ajmaline challenge suggests that substrate ablation can be
considered as a potential therapy for preventing recurrent
VT/VF.
Conclusions
Pappone C et al. Circ Arrhythm Electrophysiol. 2017
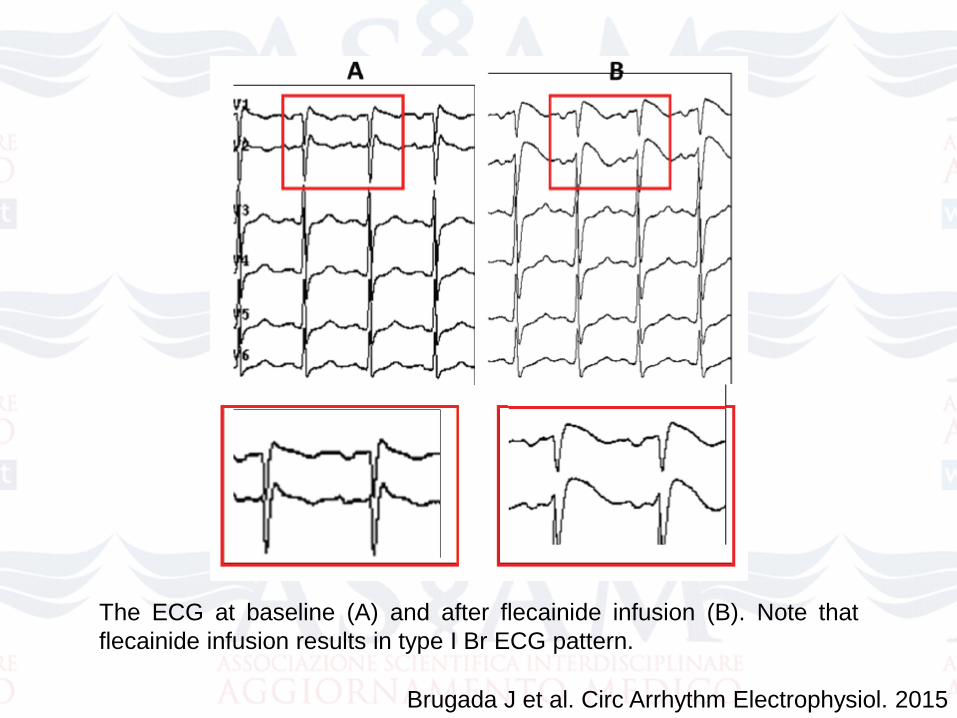
The ECG at baseline (A) and after flecainide infusion (B). Note that
flecainide infusion results in type I Br ECG pattern.
Brugada J et al. Circ Arrhythm Electrophysiol. 2015
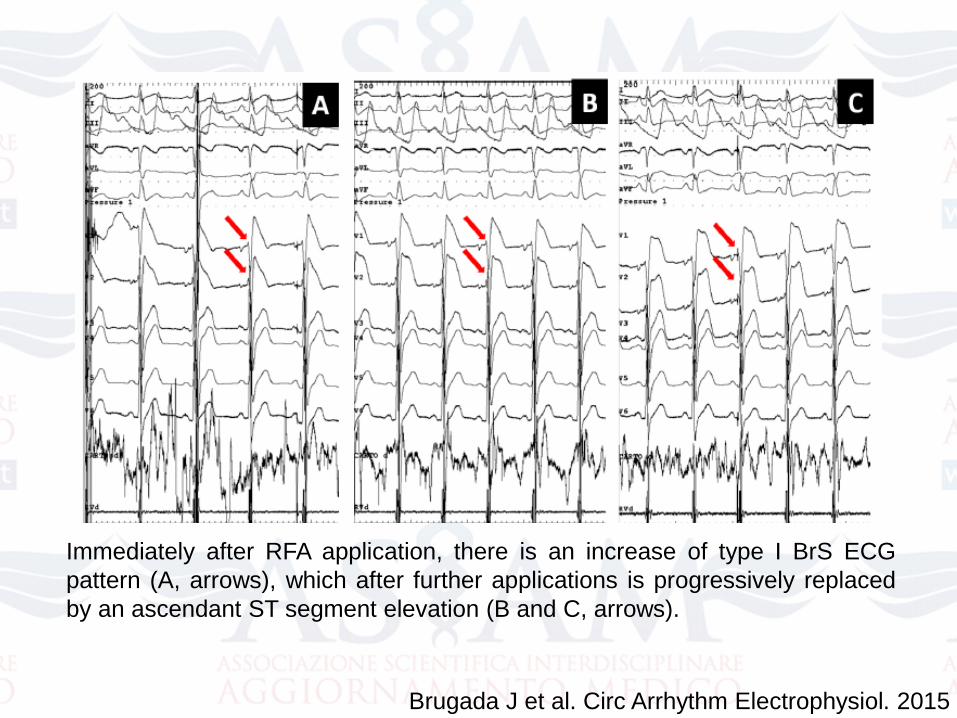
Immediately after RFA application, there is an increase of type I BrS ECG
pattern (A, arrows), which after further applications is progressively replaced
by an ascendant ST segment elevation (B and C, arrows).
Brugada J et al. Circ Arrhythm Electrophysiol. 2015
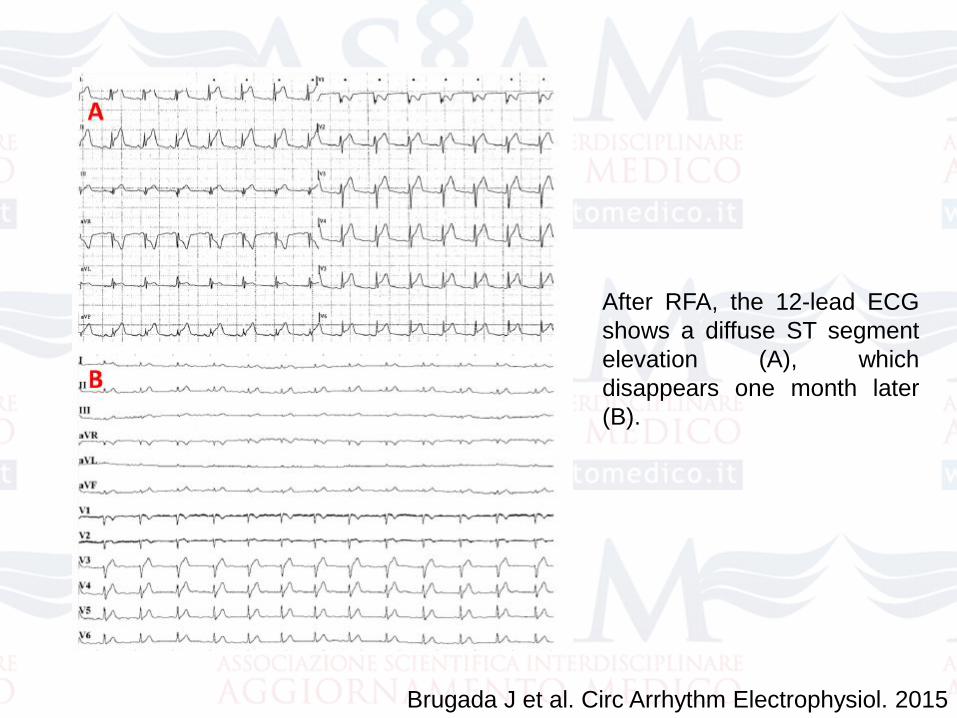
After RFA, the 12-lead ECG
shows a diffuse ST segment
elevation (A), which
disappears one month later
(B).
Brugada J et al. Circ Arrhythm Electrophysiol. 2015
30 BrS patients compared with 30
sex-,body surface area-, and age-
matched normal volunteers.
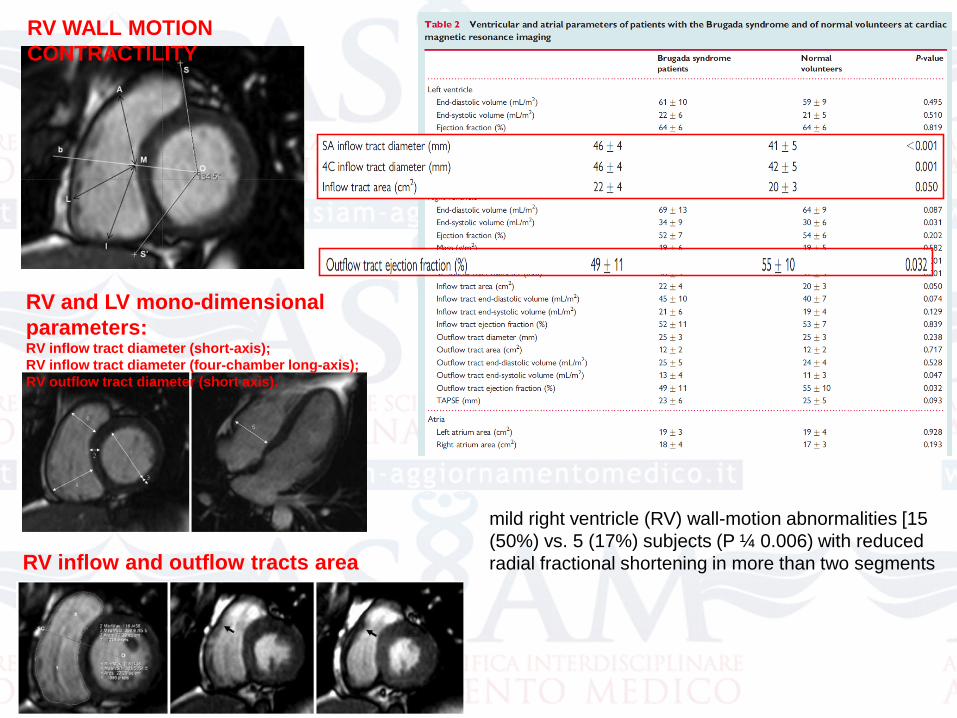
RV WALL MOTION
CONTRACTILITY
RV and LV mono-dimensional
parameters: RV inflow tract diameter (short-axis);
RV inflow tract diameter (four-chamber long-axis);
RV outflow tract diameter (short axis).
RV inflow and outflow tracts area
mild right ventricle (RV) wall-motion abnormalities [15
(50%) vs. 5 (17%) subjects (P ¼ 0.006) with reduced
radial fractional shortening in more than two segments
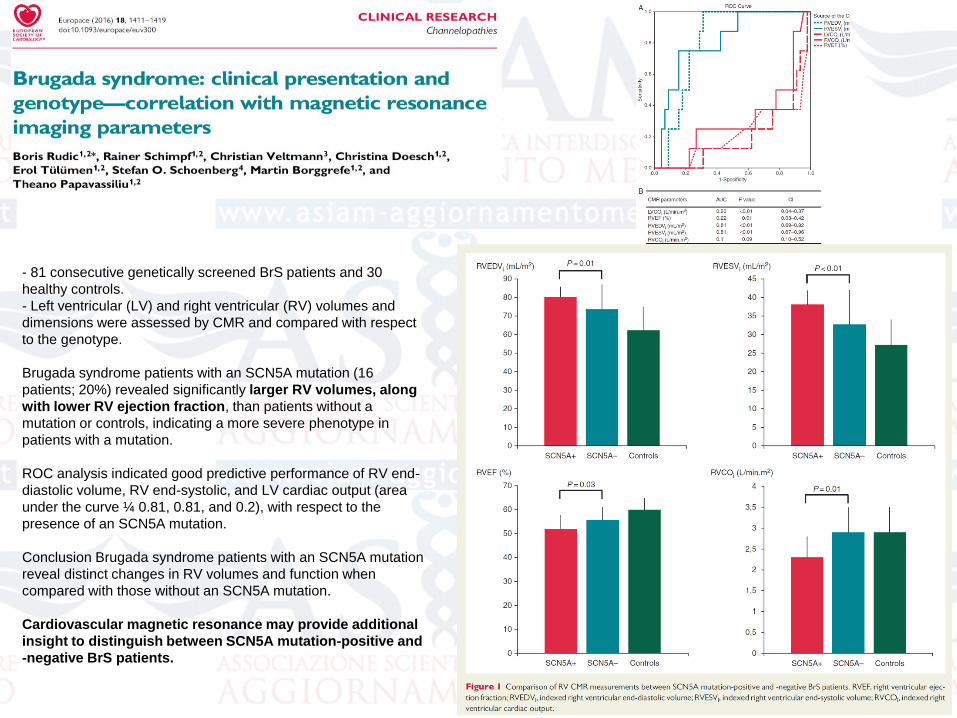
- 81 consecutive genetically screened BrS patients and 30
healthy controls.
- Left ventricular (LV) and right ventricular (RV) volumes and
dimensions were assessed by CMR and compared with respect
to the genotype.
Brugada syndrome patients with an SCN5A mutation (16
patients; 20%) revealed significantly larger RV volumes, along
with lower RV ejection fraction, than patients without a
mutation or controls, indicating a more severe phenotype in
patients with a mutation.
ROC analysis indicated good predictive performance of RV end-
diastolic volume, RV end-systolic, and LV cardiac output (area
under the curve ¼ 0.81, 0.81, and 0.2), with respect to the
presence of an SCN5A mutation.
Conclusion Brugada syndrome patients with an SCN5A mutation
reveal distinct changes in RV volumes and function when
compared with those without an SCN5A mutation.
Cardiovascular magnetic resonance may provide additional
insight to distinguish between SCN5A mutation-positive and
-negative BrS patients.
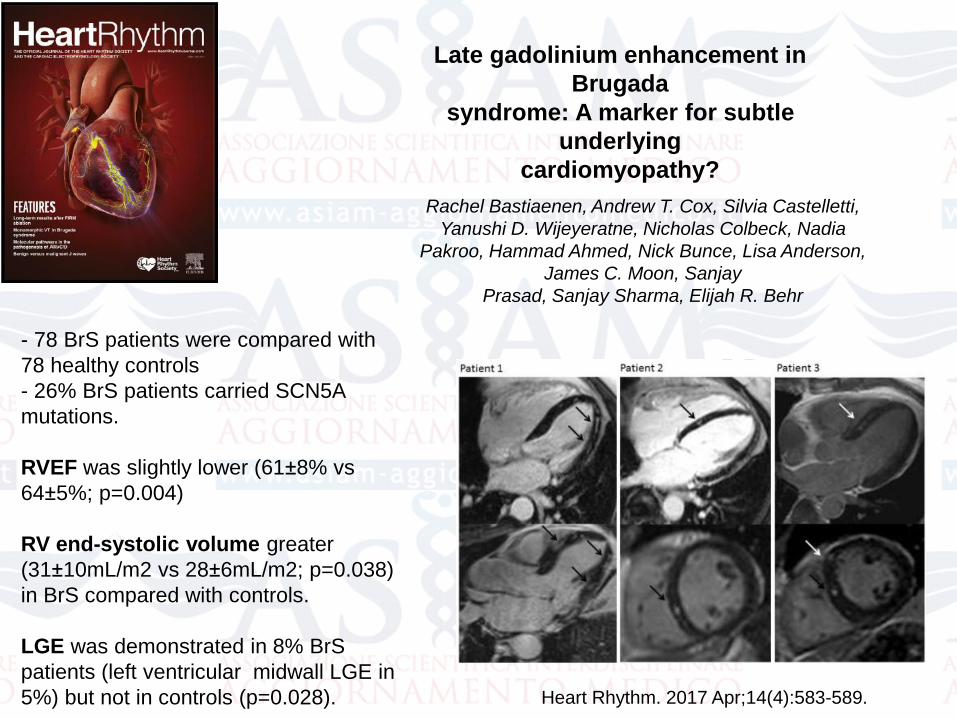
- 78 BrS patients were compared with
78 healthy controls
- 26% BrS patients carried SCN5A
mutations.
RVEF was slightly lower (61±8% vs
64±5%; p=0.004)
RV end-systolic volume greater
(31±10mL/m2 vs 28±6mL/m2; p=0.038)
in BrS compared with controls.
LGE was demonstrated in 8% BrS
patients (left ventricular midwall LGE in
5%) but not in controls (p=0.028).
Late gadolinium enhancement in
Brugada
syndrome: A marker for subtle
underlying
cardiomyopathy?
Rachel Bastiaenen, Andrew T. Cox, Silvia Castelletti,
Yanushi D. Wijeyeratne, Nicholas Colbeck, Nadia
Pakroo, Hammad Ahmed, Nick Bunce, Lisa Anderson,
James C. Moon, Sanjay
Prasad, Sanjay Sharma, Elijah R. Behr
Heart Rhythm. 2017 Apr;14(4):583-589.
Atrial Fibrillation and Brugada SyndromeJ Am Coll Cardiol 2008;51:1149–53
The arrhythmogenic substrate in Brugada syndrome may not
be restricted to the ventricles, and atrial arrhythmias are being
increasingly reported (from 6% to 38%)
The presence of a prominent transient outward current in atria
and the observation that episodes of AF are triggered by
closely coupled atrial extrasystoles point to the possibility that
a substrate similar to that responsible for ventricular
arrhythmogenesis underlies the development of AF in patients
with Brugada syndrome.
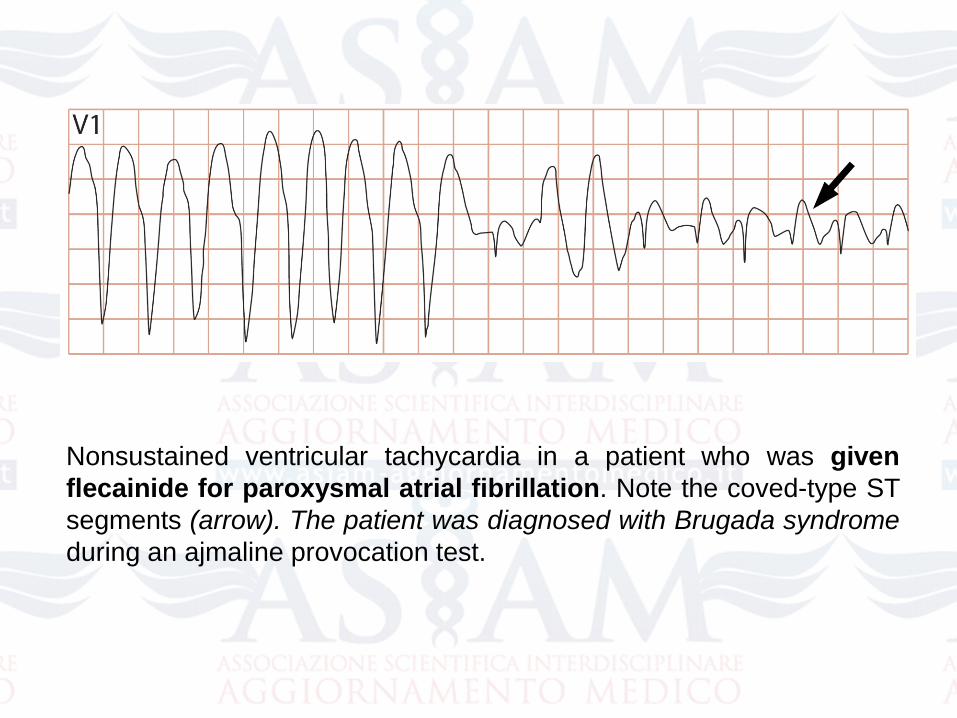
Nonsustained ventricular tachycardia in a patient who was given
flecainide for paroxysmal atrial fibrillation. Note the coved-type ST
segments (arrow). The patient was diagnosed with Brugada syndrome
during an ajmaline provocation test.
Efficacy of Pulmonary Vein Isolation in
Paroxysmal Atrial Fibrillation Patients With a
Brugada Electrocardiogram
Conclusions
Because of the concerns of proarrhythmias with antiarrhythmic
drugs, PVI may be an effective strategy for highly symptomatic
patients with AF who have a Brugada ECG pattern.
Yamada T et al. Circ J 2008
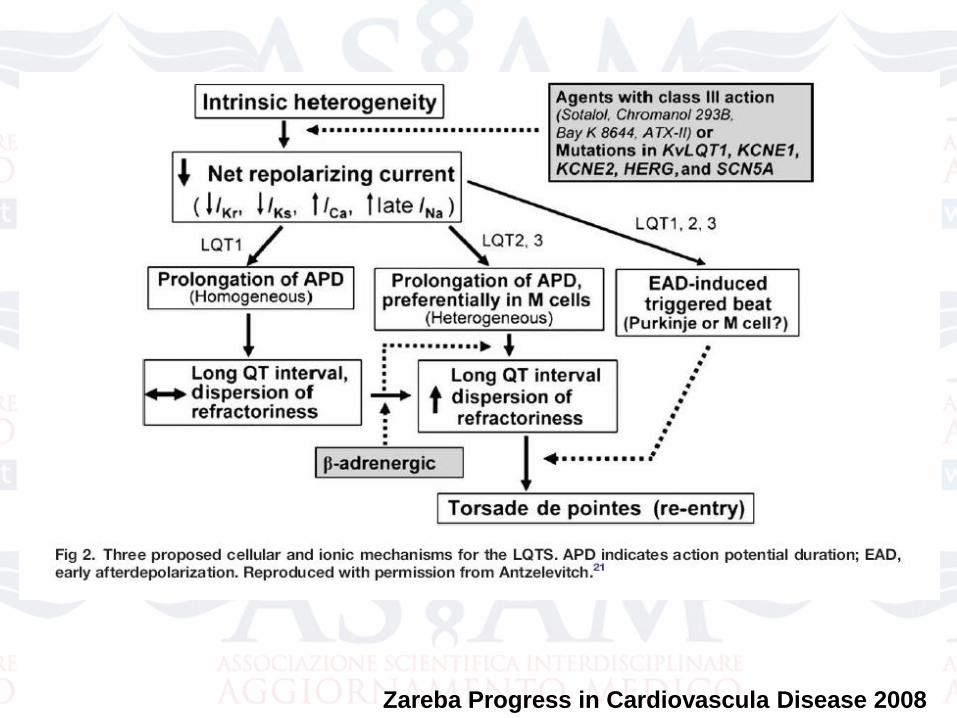
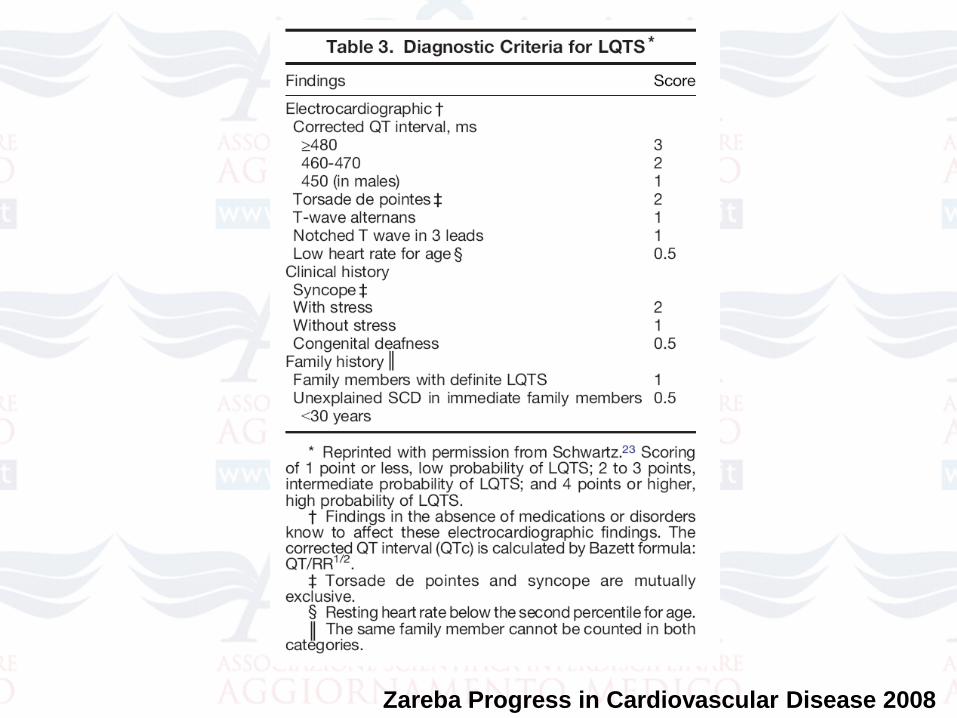
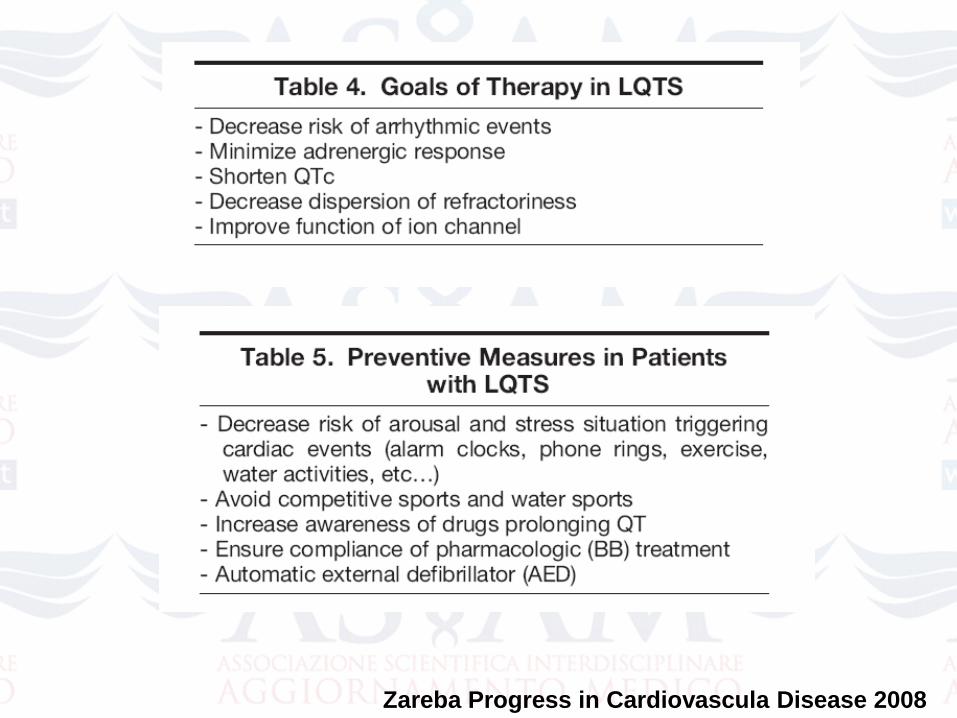
Zareba Progress in Cardiovascula Disease 2008
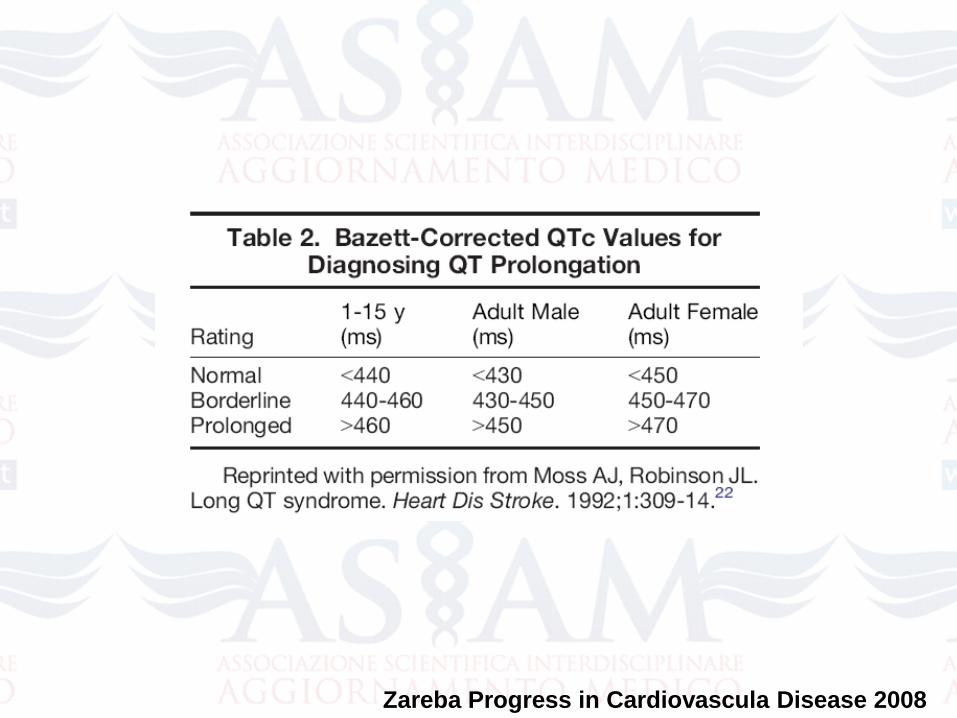
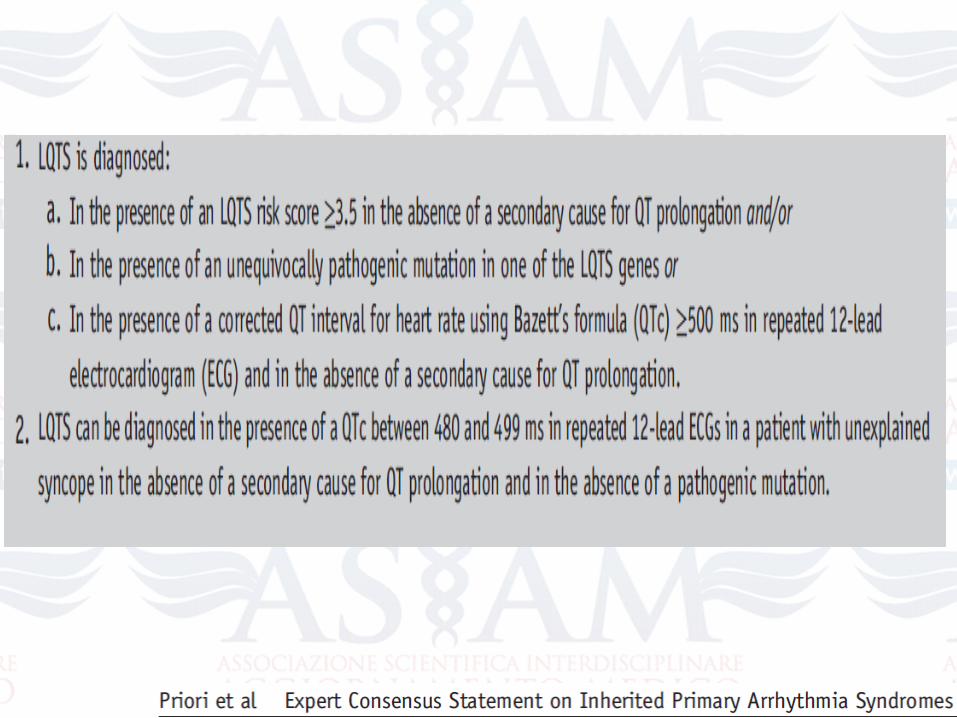
Zareba Progress in Cardiovascula Disease 2008
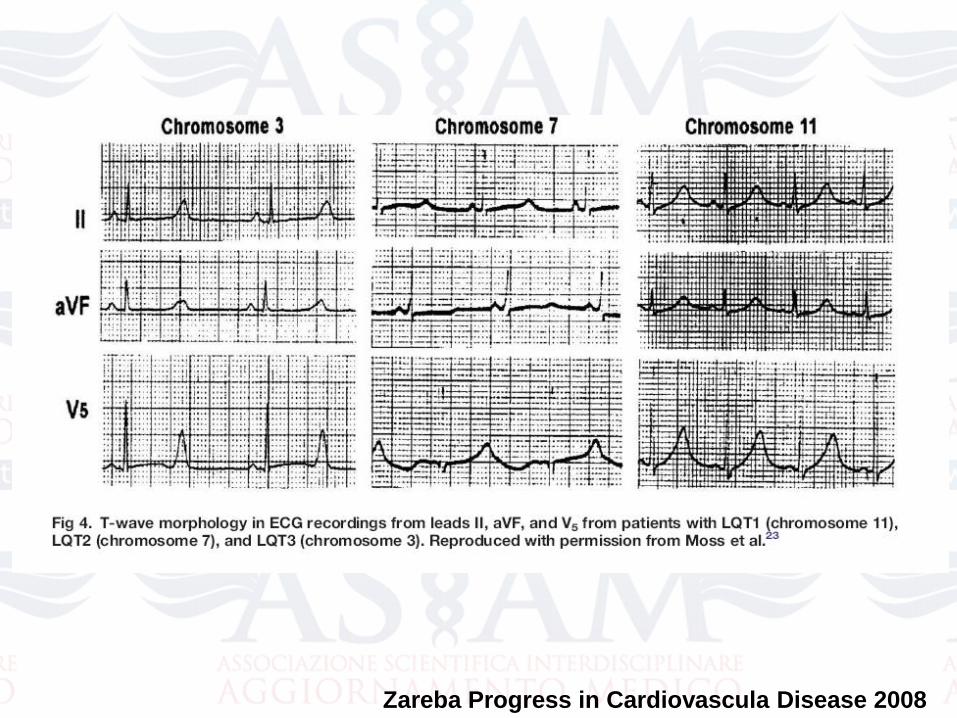
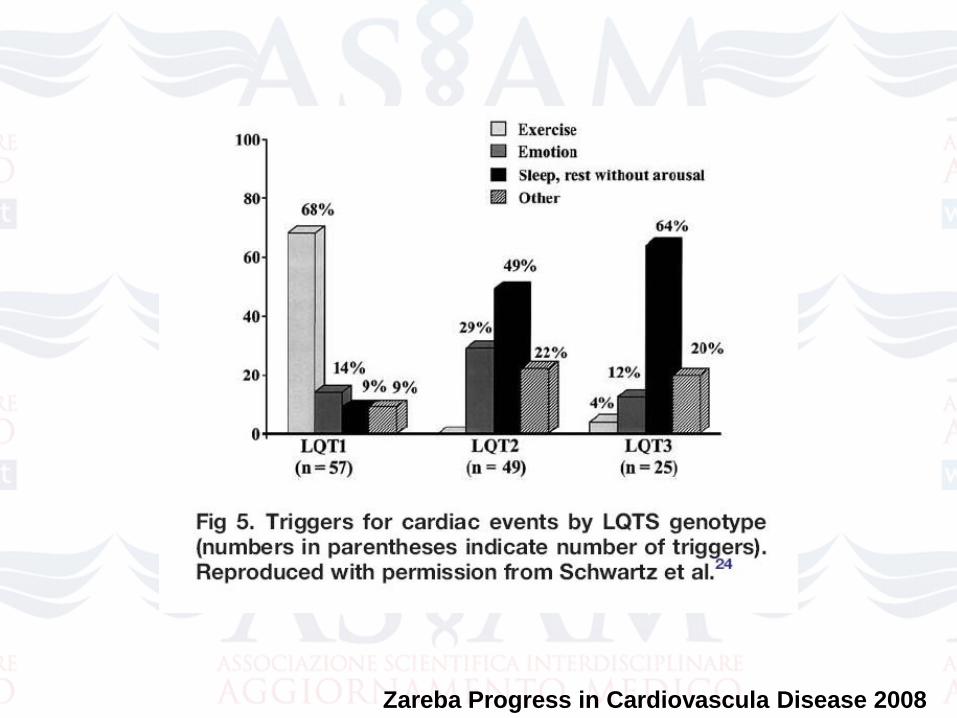
Zareba Progress in Cardiovascula Disease 2008
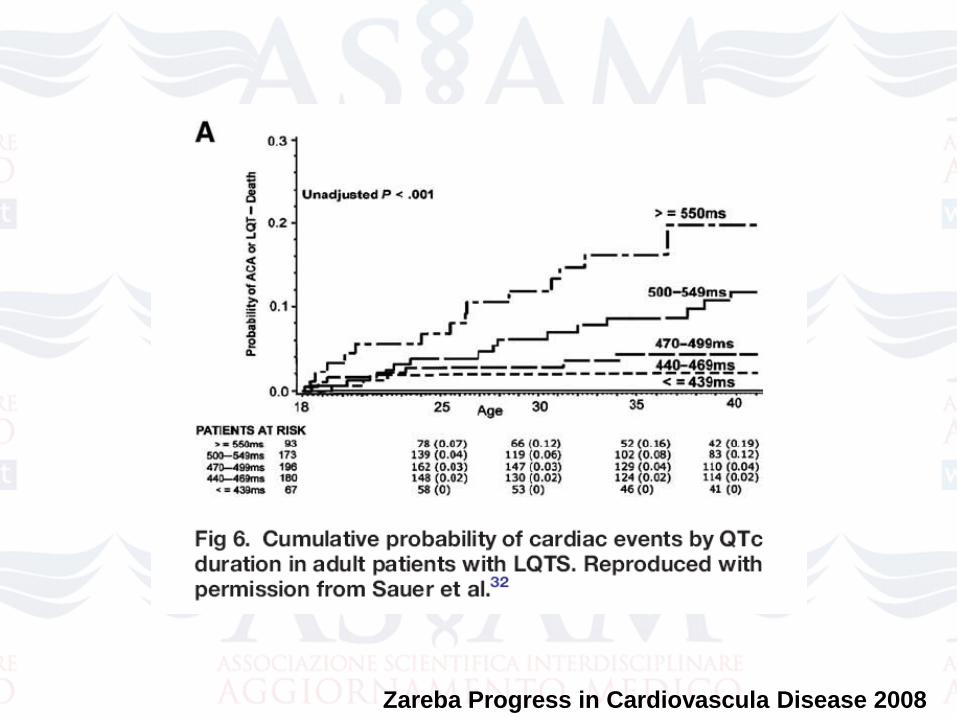
Zareba Progress in Cardiovascula Disease 2008
Zareba Progress in Cardiovascula Disease 2008
Zareba Progress in Cardiovascula Disease 2008
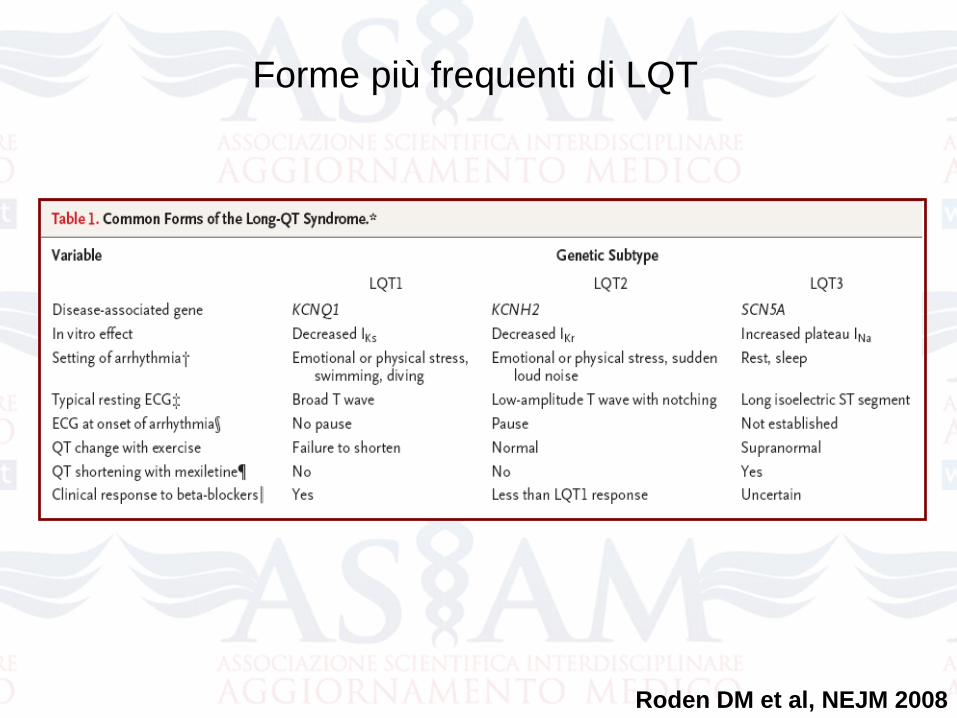
Roden DM et al, NEJM 2008
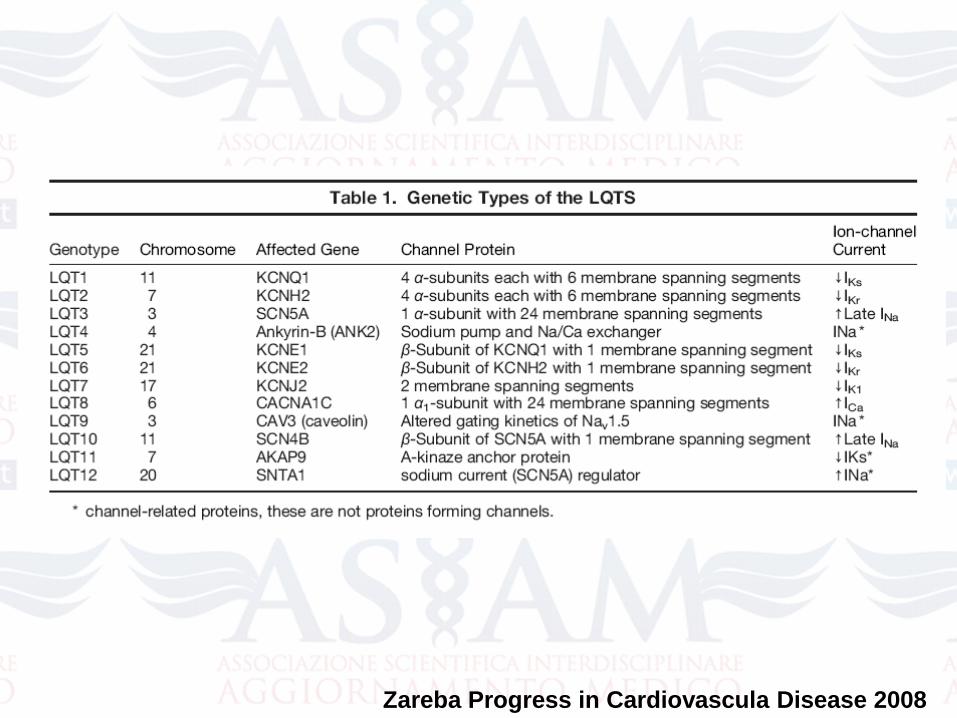
Forme più frequenti di LQT
Zareba Progress in Cardiovascular Disease 2008
Zareba Progress in Cardiovascula Disease 2008
Zareba Progress in Cardiovascula Disease 2008
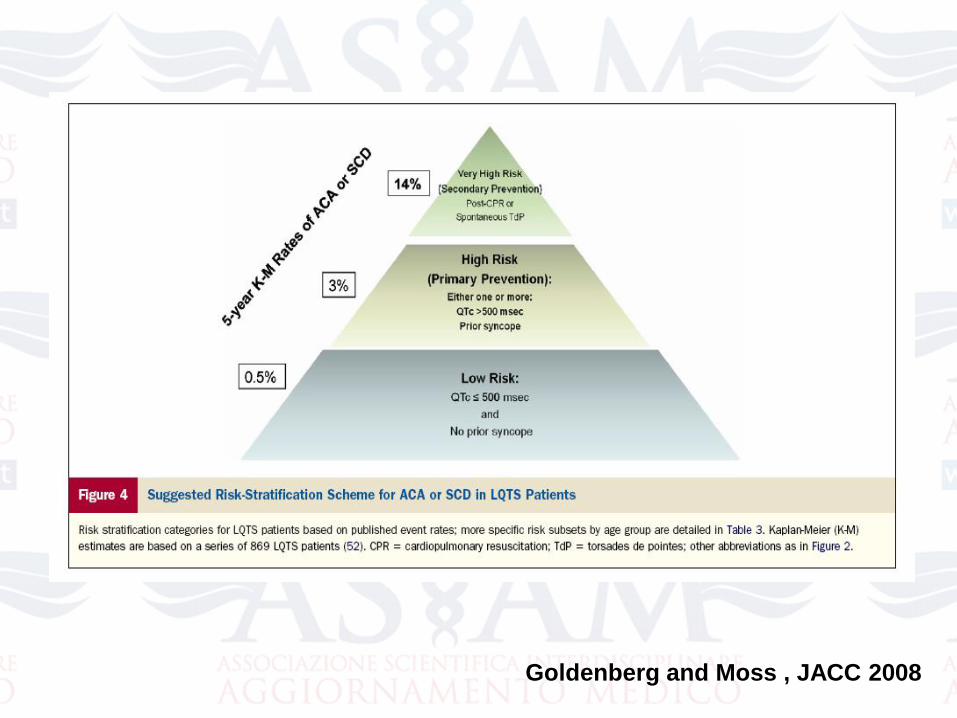
Goldenberg and Moss , JACC 2008
Zareba Progress in Cardiovascula Disease 2008