
Quali opzioni alternative nell’anziano con fibrillazione ......Antithrombotic therapy in the...
24
Quali opzioni alternative nell’anziano con fibrillazione atriale che non può essere anticoagulato? Stefano Fumagalli, MD, PhD, FEHRA Unità di Terapia Intensiva Geriatrica e Unità di Aritmologia Geriatrica, AOU Careggi e Università di Firenze
Transcript of Quali opzioni alternative nell’anziano con fibrillazione ......Antithrombotic therapy in the...

Quali opzioni alternative nell’anziano con fibrillazione
atriale che non può essere anticoagulato?
Stefano Fumagalli, MD, PhD, FEHRA
Unità di Terapia Intensiva Geriatrica e Unità di Aritmologia Geriatrica,
AOU Careggi e Università di Firenze

Mant J et al. Lancet 2007
Years since randomization
Part
icip
an
ts w
ith
ou
t
pri
mary
even
t (%
)
Follow-up = 2.7 ± 1.2 years
973 patients aged ≥75 years
(mean age: 81.5 ± 4.2 years)
Warfarin
N = 24 / 488
1.8% per year
Aspirin
N = 48 / 485
3.8% per year
Primary endpoint: fatal / disabling stroke (ischemic / hemorrhagic),
intracranial hemorrhage, or clinically significant arterial embolism
RR Warfarin vs. ASA = 0.48 95%CI = 0.28 - 0.80 - P = 0.003

Years
Cu
mu
lati
ve I
ncid
en
ce
Connolly SJ, 2009
N = 3882
N = 3772
Follow-up
3.6 years
Events - N = 408 (3.3% per year)
Events - N = 296 (2.4% per year)
RR = 0.72
95%CI 0.62-0.83
p<0.001
Secondary outcome: incidence of stroke
The ACTIVE-A (Effect of Clopidogrel Added to Aspirin in
Patients with Atrial Fibrillation) Investigators
2016 ESC Guidelines for the management of atrial fibrillation developed
in collaboration with EACTS
VKA therapy prevents S/SE, myocardial infarction, and vascular death
better than single or dual antiplatelet therapy
Antiplatelet therapy increases bleeding risk, especially DAPT with
bleeding rates that are similar to those on OAC
Thus, antiplatelet therapy cannot be recommended for stroke
prevention in AF patients
Antiplatelet mono-therapy is not recommended for stroke prevention
in AF patients, regardless of stroke risk (Class III, Harm)

Greater Net
Clinical Benefit
Inadequate
Stroke
Prophylaxis
Approach to AF stroke risk reduction in elderly adults
Desai Y,
JAGS 2017

Previous major
bleeding; 47
High risk of
bleeding; 35
CAD mandating
Triple Therapy;
22
Stroke with OAC; 16
The main indication for LAAO in the AMPLATZER Cardiac Plug - ACP
Registry (N=1047; Age: 75+8 years; CHA2DS2-VASc: 4.5+1.6; 2008-13)
Freixa X,
Am J Cardiol 2016

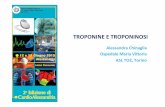
Placement of the Watchman device to sequester the
left atrial appendage from the systemic circulation
The device is a self- expanding
nickel titanium structure
available in 5 sizes.
The atrial surface is covered by
a permeable polyester fabric
and affixed to the LAA ostium
by anchors to minimize the
possibility of embolization.
Implantation is performed via a
trans-septal approach.
Reddy VY,
JACC 2017

Isch
em
ic S
tro
ke R
isk
(Even
ts p
er
100 P
Y)
Baseline CHA2DS2-VASc Score
Untreated AF
Treated with
Warfarin
Stroke Prevention in NVAF With LAA Closure. The ischemic stroke rates of
NVAF patients are shown as a function of the baseline CHA2DS2-VASc score
Reddy VY,
JACC 2017

All Subjects Warfarin Naive
Not Warfarin Naive
QoL c
ha
ng
e
Mental Component
Score
Physical Component
Score
Mental Component
Score
Physical Component
Score
QoL c
ha
ng
e
Change in QOL by Treatment - Device (N=361) vs. Warfarin (N=186) - as
Evaluated with the SF-12 (Baseline vs. 12 months; Age: 72 y; CHADS2: 2.2)
+0.4
-2.0
0.0
-0.9
+1.3
-3.6
-0.1 +0.7
+0.1
-1.7
0.0
-1.2
Alli O,
JACC 2013

Procedural complications post-FDA approval of
Watchman (2015-2016; N=3822; successful: 95.6%)
Reddy VY,
JACC 2017
1
0,6
0,3
0,08
0,29
0,08 0,02 0,03
0
0,5
1
1,5
Pati
en
ts (
%)
Procedure time – 50 minutes
Age – 76 years (N=426)
CHA2DS2-VASc – 4.0 (N=426)

0,066
0,025
0,051
0,013
0
0,02
0,04
0,06
0,08
0,1
First Second
Device Warfarin
18-m
on
th r
ate
PREVAIL Primary Efficacy Endpoints as evaluated at the final 5-year analysis
(N=407; randomization – D 2 : W 1)
Endpoint
First Primary - Stroke, SE,
and CV/Unexplained Death
Second Primary - Ischemic
Stroke or SE >7 Days
Endpoint
*: Statistical non-inferiority
NOT achieved
*
Reddy VY,
JACC 2017

1,7
0,2
1,8
0,7
0,5
2
0
1
2
3
Ischemic Hemorrhagic DeathCV/Unk
Device Warfarin
Even
t (1
00 P
Y)
Efficacy rates as evaluated at the final 5-year analysis in the PREVAIL
(N=407) and in the PROTECT AF (N=707) studies (randomization – 2:1)
All P=NS
Stroke
Reddy VY,
JACC 2017
1,3
0,2
1 1,1 1,1
2,3
0
1
2
3
Ischemic Hemorrhagic DeathCV/Unk
P=0.005
P=0.009
Stroke
PREVAIL PROTECT AF

Hazard Ratio (95% CI)
Stroke Prevention in NVAF With LAA Closure, in a meta-analysis combining
the randomized PROTECT AF (N=707) and PREVAIL (N=407) trial cohorts
(Age – WATCHMAN: 73 years; Warfarin: 73 years; FU: 4.3 PY)
Reddy VY,
JACC 2017
CHA2DS2-VASc
WATCHMAN: 3.6+1.4
Warfarin: 3.9+1.5
P=0.02

Antithrombotic therapy in the PROTECT AF (N=707) and the
PREVAIL (N=407) trials
Reddy VY,
JACC 2017
After implantation, patients were treated with an antithrombotic
regimen to allow time for device endothelialization:
1) warfarin with a goal INR between 2.0 to 3.0 and aspirin (81 mg)
for 45 days;
2) following TEE demonstrating adequate LAAC (no peridevice
leak), warfarin was discontinued, and clopidogrel (75 mg) and
aspirin (81-325 mg) were instituted until the 6-month timepoint;
3) clopidogrel was discontinued and aspirin (325 mg) was
continued indefinitely.
In the warfarin arms, the target INR remained between 2.0 to 3.0
throughout follow-up

Forest plot of the ORs of embolic stroke incidence on Day 30 and at the
latest follow-up by group (7 studies; LAA – N=1716, 65 y; non-LAA – N=1937, 64 y)
30-Day
Latest FU
1.0 vs. 2.2%
OR=0.43
1.4 vs. 4.1%
OR=0.48
Favours LAA Favours no LAA Tsai YC, European Journal of Cardio-Thoracic Surgery 2015

Median and interquartile values of the modified Rankin score at baseline,
stroke presentation, 3 and 12 months after the cerebrovascular event
In the ACP Registry (follow-up: 13 months)
Freixa X,
Am J Cardiol 2016
Stroke – 9/1047 (0.9%)
TIA – 9/1047 (0.9%)
ICH - 0
Death – 45/1047 (4.3%)
The median time of stroke or
TIA presentation was 420
days (IQR 234-671) after
LAAO
N=17 (94%) were on single-
antiplatelet therapy when
the event occurred

4140
6068
106 124
0.37
0.80
3.21
5.93
vWF – p<0.001 MP-TF – p<0.001
F1.2 – p=0.270 PAI-1 – p=0.001 vWF: von Willebrand
Factor
MP-TF: Microparticle
tissue factor
F1.2: Prothrombin
fragment 1+2
PAI-1: Plasminogen
activator inhibitor
Control (n=25)
AF (n=30)
Control (n=25)
AF (n=30)
Levels of biomarkers in control and AF groups
Liles J, 2016
Clinical and Applied
Thrombosis/Hemostasis

yearly thereafter. The study protocol was approved by thelocal Ethics Committee and all patients provided signedinformed consent.
Fasting blood samples were collected before the pro-cedureonthesameday of LAACandat 7, 30, and180daysafter theprocedure. Blood wascollected into 4 Vacutainertubesprefilled with 0.5 ml of 3.2%buffered sodiumcitrate(BectonDickinson) that werekept onicefor amaximumof2 hours before centrifugation at 2000g at 4 C for 15 mi-nutes. Plasmaand serumwerepipetted into plastic vials inaliquots and stored at 70 C until analysis. Enzyme im-munoassays wereused for determining laboratory levelsofF1þ2(Stago), TAT(Stago), sPselectin(R&DSystems), andsCD40 L (R&D Systems).
Categorical data are expressed as percentages, andcontinuous variablesasmean (SD) or median (interquartilerange). Comparisonsbetweengroupswereperformedusingthechi-squaretest for categorical variablesandthestudent ttest for numerical variables. An ANOVA for repeatedmeasureswasperformedto test for equal meansat differenttimes. Posteriori comparisons were performed using theTukey’smethod. Statistical significancewasassumedwithap value 0.05. Statistical analyses were performed usingSASversion 9.3 (SASInstitute, Cary, North Carolina).
Results
The main baseline and procedural characteristics of thestudy population are listed in Table 1. The results ofcoagulation system activation (as assessed by F1þ2 andTAT) are listed in Figure1. Mean baseline levelsof F1þ2and TAT were 0.27 nmol/L and 4.68 ng/ml, respectively.There was a significant change in both F1þ2 and TATlevels after LAAC (p <0.001 for both markers). F1þ2levels increased by 68%at day 7 (95%confidenceinterval[CI] 46 to 90) and gradually decreased, yet remained 20%higher than baselineby day 30 (95%CI 8 to 32) and 16%
Table1
Baseline, procedural, andin-hospital characteristicsof thestudy population
Variables n¼43
BaselineCharacteristics
Age(years) 76 9
Men 23 (54%)
Body massindex (kg/m2) 28 6
Hypertension 41 (95%)
Diabetesmellitus 16 (37%)
Coronary artery disease 21 (49%)
Previousheart failure 12 (28%)
LEVF (%) 54 11
Chronic renal failure 17 (40%)
Previous liver disease 3 (7%)
Atrial fibrillation type
Paroxysmal 20 (47%)
Persistent/Permanent 23 (54%)
Thromboembolic events
Stroke 15 (35%)
Transient ischemic attack 7 (16%)
Prior bleeding 39 (91%)
LabileINR* 1 (2%)
CHADS2 score 3 (2-4)
CHA2DS2-VASc score 4 (3-6)
HAS-BLED score 4 (3-5)
Procedural Characteristicsand In-Hospital Outcomes
LAA ClosureDeviceImplanted
ACP 16 (37%)
Watchman 27 (63%)
In-hospital events
Stroke 0
Major bleeding 0
Minor bleeding 1 (2%)
Pericardial effusion requiring intervention 1 (2%)
Prosthesisembolization 0
Hospital stay, days 1 [1-2]
Antithrombotic treatment at discharge
Aspirin 13 (30%)
Clopidogrel 3 (7%)
Aspirinþ clopidogrel 27 (63%)
Variablesarepresented as%, mean (SD), or median (IQR).
ACP ¼ Amplatzer cardiac plug; ASD ¼ atrial septal defect;
INR ¼ international normalized ratio; IQR ¼ interquartile range;
LAA ¼ left atrial appendage; LVEF ¼ left-ventricle ejection fraction;
PFO¼patent foramen ovale; TIA ¼ transitory ischemic attack.
* Labile INR was defineas <60%time in therapeutic range (INR 2-3
inclusive).
Figure1. Changesinthemarkersof coagulationactivationafter LAAC. (A)
Changes in F1þ2 levels after LAAC. (B) Changes in TAT levels after
LAAC.
88 TheAmerican Journal of Cardiology (www.ajconline.org)
yearly thereafter. The study protocol was approved by thelocal Ethics Committee and all patients provided signedinformed consent.
Fasting blood samples were collected before the pro-cedureonthesamedayof LAACandat 7, 30, and180daysafter theprocedure. Blood wascollected into 4 Vacutainertubesprefilled with 0.5 ml of 3.2%buffered sodiumcitrate(BectonDickinson) that werekept onicefor amaximumof2 hours before centrifugation at 2000g at 4 C for 15 mi-nutes. Plasmaand serumwerepipetted into plastic vials inaliquots and stored at 70 C until analysis. Enzyme im-munoassayswereused for determining laboratory levelsofF1þ2(Stago),TAT(Stago), sPselectin(R&DSystems), andsCD40 L (R&D Systems).
Categorical data are expressed as percentages, andcontinuousvariablesasmean (SD) or median (interquartilerange). Comparisonsbetweengroupswereperformedusingthechi-squaretest for categorical variablesandthestudent ttest for numerical variables. An ANOVA for repeatedmeasureswasperformedto test for equal meansat differenttimes. Posteriori comparisons were performed using theTukey’smethod. Statistical significancewasassumedwithap value 0.05. Statistical analyses were performed usingSASversion 9.3 (SASInstitute, Cary, North Carolina).
Results
The main baseline and procedural characteristics of thestudy population are listed in Table 1. The results ofcoagulation system activation (as assessed by F1þ2 andTAT) are listed in Figure1. Mean baseline levelsof F1þ2and TAT were 0.27 nmol/L and 4.68 ng/ml, respectively.There was a significant change in both F1þ2 and TATlevels after LAAC (p <0.001 for both markers). F1þ2levels increased by 68%at day 7 (95%confidenceinterval[CI] 46 to 90) and gradually decreased, yet remained 20%higher than baselineby day 30 (95%CI 8 to 32) and 16%
Table1
Baseline, procedural, andin-hospital characteristicsof thestudy population
Variables n¼43
BaselineCharacteristics
Age(years) 76 9
Men 23 (54%)
Body mass index (kg/m2) 28 6
Hypertension 41 (95%)
Diabetesmellitus 16 (37%)
Coronary artery disease 21 (49%)
Previousheart failure 12 (28%)
LEVF (%) 54 11
Chronic renal failure 17 (40%)
Previous liver disease 3 (7%)
Atrial fibrillation type
Paroxysmal 20 (47%)
Persistent/Permanent 23 (54%)
Thromboembolic events
Stroke 15 (35%)
Transient ischemic attack 7 (16%)
Prior bleeding 39 (91%)
LabileINR* 1 (2%)
CHADS2 score 3 (2-4)
CHA2DS2-VASc score 4 (3-6)
HAS-BLED score 4 (3-5)
Procedural Characteristicsand In-Hospital Outcomes
LAA ClosureDeviceImplanted
ACP 16 (37%)
Watchman 27 (63%)
In-hospital events
Stroke 0
Major bleeding 0
Minor bleeding 1 (2%)
Pericardial effusion requiring intervention 1 (2%)
Prosthesisembolization 0
Hospital stay, days 1 [1-2]
Antithrombotic treatment at discharge
Aspirin 13 (30%)
Clopidogrel 3 (7%)
Aspirinþ clopidogrel 27 (63%)
Variablesarepresented as%, mean (SD), or median (IQR).
ACP ¼ Amplatzer cardiac plug; ASD ¼ atrial septal defect;
INR ¼ international normalized ratio; IQR ¼ interquartile range;
LAA ¼ left atrial appendage; LVEF ¼ left-ventricle ejection fraction;
PFO¼patent foramen ovale; TIA ¼ transitory ischemic attack.
* Labile INR was define as <60% time in therapeutic range (INR 2-3
inclusive).
Figure1. Changesinthemarkersof coagulationactivationafter LAAC. (A)
Changes in F1þ2 levels after LAAC. (B) Changes in TAT levels after
LAAC.
88 TheAmerican Journal of Cardiology (www.ajconline.org)
Pro
thro
mb
in f
rag
me
nt
1+
2
(nm
ol/L
)
Th
rom
bin
-an
tith
rom
bin
III
(ng
/mL
)
P<0.001 P<0.001 * *
*
Changes in the markers of coagulation activation after LAAC
(N=43; Age: 76+9 years; CHA2DS2-VASc: 4)
*: p<0.05 vs. Baseline
Rodés-Cabau J, Am J Cardiol 2017
Changes in Coagulation and Platelet Activation Markers
Following Transcatheter Left Atrial AppendageClosure
JosepRodés-Cabau, MD*, GillesO’Hara, MD, Jean-Michel Paradis, MD, Mathieu Bernier, MD,TaniaRodriguez-Gabella, MD, Ander Regueiro, MD, KimO’Connor, MD, Jonathan Beaudoin, MD,
Rishi Puri, MBBS, MélanieCôté, MSc, and Jean Champagne, MD
The recommendations for antithrombotic treatment after left atrial appendage closure(LAAC) remain empirical, and no data exist on thechanges in hemostatic markersasso-ciated with LACC. Theobjectiveof thepresent study istodeterminethepresence, degree,and timing of changes in themarkersof platelet and coagulation activation after LAAC.Forty-threepatients(mean age76– 9years, 23men) with atrial fibrillation whounderwentsuccessful LACCwith theWatchman(n [ 27) or Amplatzer CardiacPlug(n [ 16) deviceswere included in thestudy. Patients received antiplatelet therapy after LAAC (aspirin Dclopidogrel: 27patients; singleantiplatelet therapy with aspirin or clopidogrel: 16patients).Prothrombin fragment 1D2 and thrombin-antithrombin III were used as markers ofcoagulation activation, and soluble P-selectin and soluble CD40 ligand were used asmarkersof platelet activation. Measurementsof all hemostatic markerswereperformed atbaseline just before the procedure, followed by days 7, 30, and 180 after LAAC. Pro-thrombin fragment 1D 2and thrombin-antithrombin levelsincreased from0.27nmol/L and4.68 ng/ml, respectively, at baseline to peak values of 0.43 nmol/L and 9.76 ng/ml,respectively, at 7days, partially returningtobaselinelevelsat days30and 180after LAAC(p<0.001for bothmarkers). Noclinical or procedural factorswereassociated withagreaterincrease in themarkersof coagulation activation after LAAC. Levelsof solubleP-selectinand soluble CD40 ligand did not change at any time after LAAC. In conclusion, trans-catheter LAAC is associated with significant activation of the coagulation system, yetwithout evidenceof significant platelet activation. Ó2017Elsevier Inc. All rightsreserved.(Am J Cardiol 2017;120:87e91)
Transcatheter left atrial appendage closure (LAAC)has emerged as an alternative to anticoagulation for pre-venting thromboembolic events in patients with atrialfibrillation.1 Although most complications associatedwith LAAC havedecreased with time, the occurrence ofdevice thrombosis remains a concern, with an incidenceof 4%to 6%.2,3 The typeand duration of antithrombotictherapiesafter LAAChaveevolvedempirically. Althoughtransient (6 weeks) anticoagulation therapy has beenrecommended in some studies,4,5 others have used dualantiplatelet therapy within the 3 to 6 months after theprocedure.3,5,6 More recently, single antiplatelet therapyimmediately after LAAC has also been suggested.7
However, there is currently no biologic basis supportingaspecific approach, and deciphering specific alternationsof platelet and coagulation activation after LAAC couldbe useful for guiding the type and duration of antith-rombotic therapy after LAAC. Soluble P-selectin (sPse-lectin) and CD40 ligand (CD40L) have been wellvalidated as markers of platelet activation,8,9 andprothrombin fragment 1þ2 (F1þ2) and thrombin-
antithrombin III (TAT) as markers of coagulation acti-vation.10 Thepurposeof thepresent study istodeterminethe presence, degree, and timing of the changes in themarkersof platelet (sPselectin, sCD40L) and coagulation(F1þ2, TAT) activation after LAAC.
Methods
A total of 43 patientswith atrial fibrillation who under-went LAACbecauseof contraindicationstoanticoagulationtherapy were included in the study. The procedures wereperformedthroughthetransfemoral approach, under generalanesthesia with transesophageal echocardiographic guid-ance. Details specific to the LAAC procedure have beendetailed elsewhere.4e6 The device (Watchman [BostonScientific, Natick, MA] or Amplatzer Cardiac Plug [ACP;St Jude Medical, Minneapolis, MN]) was selected accord-ing to left atrial appendage anatomy and physician’s pref-erence. Dual antiplatelet therapy (aspirin 80 mg/day þclopidogrel 75 mg/day) for 45 days and then aspirinindefinitely was thestandard therapy after LAAC, but sin-gle antiplatelet therapy was an alternative option in thosepatientsat very highrisk of recurrent bleeding(HAS-BLEDscore >3). The final decision was left at the discretion ofthe physician responsible for the patient. A control trans-esophageal echocardiography (TEE) was performed at6 weeks after LAAC, and patients underwent clinicalfollow-up at 6 and 12 months after the procedure, and
Department of Cardiology, Quebec Heart & Lung Institute, Laval
University, QuebecCity, Quebec, Canada. Manuscript receivedJanuary 28,
2017; revised manuscript received and accepted March 16, 2017.
Seepage91 for disclosure information.
*Corresponding author: Tel: (418) 6568711; fax: (418) 6564544.
E-mail address: [email protected](J. Rodés-Cabau).
0002-9149/17/$ - seefront matter Ó 2017 Elsevier Inc. All rights reserved. www.ajconline.org
http://dx.doi.org/10.1016/j.amjcard.2017.03.253
Antithrombotic Tx ASA – 30%
Clopidogrel – 7%
ASA and Clopidogrel – 63%

Recommendations Class Level
After surgical occlusion or exclusion of the LAA, it is
recommended to continue OAC in at-risk patients with
AF for stroke prevention
I B
LAA occlusion may be considered for stroke prevention
in patients with AF and contra-indications for long-term
OAC treatment (e.g. those with a previous life-
threatening bleed without a reversible cause)
IIb B
Surgical occlusion or exclusion of the LAA may be
considered for stroke prevention in patients with AF
undergoing cardiac surgery
IIb B
Surgical occlusion or exclusion of the LAA may be
considered for stroke prevention in patients undergoing
thoracoscopic AF surgery
IIb B
Recommendations for occlusion or exclusion of the LAA
ESC GUIDELINES
2016 ESC Guidelines for the management of atrial
fibrillat ion developed in collaboration with EACTS
The Task Force for the management of at r ial fibr illat ion of the
European Society of Cardiology (ESC)
Developed with the special cont r ibut ion of the European Heart
Rhythm Associat ion (EHRA) of the ESC
Endorsed by the European Stroke Organisat ion (ESO)
Authors/Task Force Members: Paulus Kirchhof (Chairperson) (UK/Germany),*
Stefano Benussi*1 (Co-Chairperson) (Switzer land), Dipak Kotecha (UK),
Anders Ahlsson1 (Sweden), Dan Atar (Norway), Barbara Casadei (UK),
Manuel Castella1 (Spain), Hans-Chr istoph Diener2 (Germany), Hein Heidbuchel
(Belgium), Jeroen Hendr iks (The Nether lands), Gerhard Hindr icks (Germany),
Antonis S. Manolis (Greece), Jonas Oldgren (Sweden), Bogdan Alexandru Popescu
(Romania), Ulr ich Schot t en (The Nether lands), Bart Van Put te1 (The Nether lands),
and Panagiot is Vardas (Greece)
Document Reviewers: Stefan Agewall (CPG Review Co-ordinat or) (Norway), John Camm (CPG Review
Co-ordinator ) (UK), Gonzalo Baron Esquivias (Spain), W erner Budts (Belgium), Scipione Carer j (Italy),
Filip Casselman (Belgium ), Antonio Coca (Spain), Raffaele De Cater ina (Italy), Spir idon Deftereos (Greece),
Dobromir Dobrev (Germany), Jose M. Ferro (Portugal), Gerasimos Filippatos (Greece), Donna Fitzsimons (UK),
* Correspondingauthors: Paulus Kirchhof, Institute of Cardiovascular Sciences, University of Birmingham, SWBH and UHB NHStrusts, IBR, Room 136, Wolfson Drive, Birmingham
B15 2TT, United Kingdom, Tel: + 44 121 4147042, E-mail: [email protected]; Stefano Benussi, Department of Cardiovascular Surgery, University Hospital Zurich, Ramistrasse
100, 8091 Zurich, Switzerland, Tel: + 41(0)788933835, E-mail: [email protected] ing the European Associat ion for Cardio-Thoracic Surgery (EACTS)2Represent ing the European Stroke Associat ion (ESO)
ESC Commit tee for Pract ice Guidelines (CPG) and Nat ional Cardiac Societ ies Reviewers can be found in the Appendix.
ESC ent it ies having part icipated in the development of this document:
Associat ions: European Association for Cardiovascular Prevention and Rehabilitation (EACPR), European Association of Cardiovascular Imaging (EACVI), European Heart Rhythm
Association (EHRA), Heart Failure Association (HFA).
Councils: Council on Cardiovascular Nursing and Allied Professions, Council for Cardiology Practice, Council on Cardiovascular Primary Care, Council on Hypertension.
W orking Groups: Cardiac Cellular Electrophysiology, Cardiovascular Pharmacotherapy, Grown-up Congenital Heart Disease, Thrombosis, Valvular Heart Disease.
Thecontent of these European Society of Cardiology (ESC) Guidelines hasbeen published for personal and educational use only.No commercial use isauthorized.No part of the ESC
Guidelines may be translated or reproduced in any form without written permission from the ESC. Permission can be obtained upon submission of awritten request to Oxford Uni-
versity Press, the publisher of the European Heart Journal and the party authorized to handle such permissions on behalf of the ESC ([email protected]).
Disclaimer . The ESC Guidelines represent the viewsof the ESC and were produced after careful consideration of the scientific and medical knowledge and the evidence available at
the time of their publication. The ESC is not responsible in the event of any contradiction, discrepancy and/or ambiguity between the ESC Guidelines and any other official recom-
mendations or guidelines issued by the relevant public health authorities, in particular in relation to good use of healthcare or therapeutic strategies. Health professionals are encour-
aged to take the ESC Guidelines fully into account when exercising their clinical judgment, as well as in the determination and the implementation of preventive, diagnostic or
therapeutic medical strategies; however, the ESC Guidelines do not override, in any way whatsoever, the individual responsibility of health professionals to make appropriate and
accurate decisions in consideration of each patient’s health condition and in consultation with that patient and, where appropriate and/or necessary, the patient’s caregiver. Nor
do theESC Guidelines exempt health professionals from takinginto full and careful consideration the relevant official updated recommendations or guidelines issued by thecompetent
public health authorities, in order to manage each patient’s case in light of the scientifically accepted datapursuant to their respective ethical and professional obligations. It isalso the
health professional’s responsibility to verify the applicable rules and regulations relating to drugs and medical devices at the time of prescription.
& The European Society of Cardiology 2016. All rights reserved. For permissions please email: [email protected].
doi:10.1093/europace/euw295
Europace (2016) 18, 1609–1678
Downloaded from https://academic.oup.com/europace/article-abstract/18/11/1609/2437601
by Biblioteca di Scienze, Universita' degli Studi di Firenze useron 20 November 2017
Kirchhof P,
Europace 2017

Adequately powered controlled trials are urgently needed
to inform the best use of these devices, including
1. LAA occluders in patients who are truly unsuitable for
OAC or in patients who suffer a stroke on OAC,
2. randomized comparisons of LAA occluders with
NOACs, and
3. assessment of the minimal antiplatelet therapy
acceptable after LAA occlusion.
Still unsolved issues …
ESC GUIDELINES
2016 ESC Guidelines for the management of atrial
fibrillat ion developed in collaboration with EACTS
The Task Force for the management of at r ial fibr illat ion of the
European Society of Cardiology (ESC)
Developed with the special cont r ibut ion of the European Heart
Rhythm Associat ion (EHRA) of the ESC
Endorsed by the European Stroke Organisat ion (ESO)
Authors/Task Force Members: Paulus Kirchhof (Chairperson) (UK/Germany),*
Stefano Benussi*1 (Co-Chairperson) (Switzer land), Dipak Kotecha (UK),
Anders Ahlsson1 (Sweden), Dan Atar (Norway), Barbara Casadei (UK),
Manuel Castella1 (Spain), Hans-Chr istoph Diener2 (Germany), Hein Heidbuchel
(Belgium), Jeroen Hendr iks (The Nether lands), Gerhard Hindr icks (Germany),
Antonis S. Manolis (Greece), Jonas Oldgren (Sweden), Bogdan Alexandru Popescu
(Romania), Ulr ich Schot t en (The Nether lands), Bart Van Put te1 (The Nether lands),
and Panagiot is Vardas (Greece)
Document Reviewers: Stefan Agewall (CPG Review Co-ordinat or) (Norway), John Camm (CPG Review
Co-ordinator ) (UK), Gonzalo Baron Esquivias (Spain), W erner Budts (Belgium), Scipione Carer j (Italy),
Filip Casselman (Belgium ), Antonio Coca (Spain), Raffaele De Cater ina (Italy), Spir idon Deftereos (Greece),
Dobromir Dobrev (Germany), Jose M. Ferro (Portugal), Gerasimos Filippatos (Greece), Donna Fitzsimons (UK),
* Correspondingauthors: Paulus Kirchhof, Institute of Cardiovascular Sciences, University of Birmingham, SWBH and UHB NHStrusts, IBR, Room 136, Wolfson Drive, Birmingham
B15 2TT, United Kingdom, Tel: + 44 121 4147042, E-mail: [email protected]; Stefano Benussi, Department of Cardiovascular Surgery, University Hospital Zurich, Ramistrasse
100, 8091 Zurich, Switzerland, Tel: + 41(0)788933835, E-mail: [email protected] ing the European Associat ion for Cardio-Thoracic Surgery (EACTS)2Represent ing the European Stroke Associat ion (ESO)
ESC Commit tee for Pract ice Guidelines (CPG) and Nat ional Cardiac Societ ies Reviewers can be found in the Appendix.
ESC ent it ies having part icipated in the development of this document:
Associat ions: European Association for Cardiovascular Prevention and Rehabilitation (EACPR), European Association of Cardiovascular Imaging (EACVI), European Heart Rhythm
Association (EHRA), Heart Failure Association (HFA).
Councils: Council on Cardiovascular Nursing and Allied Professions, Council for Cardiology Practice, Council on Cardiovascular Primary Care, Council on Hypertension.
W orking Groups: Cardiac Cellular Electrophysiology, Cardiovascular Pharmacotherapy, Grown-up Congenital Heart Disease, Thrombosis, Valvular Heart Disease.
Thecontent of these European Society of Cardiology (ESC) Guidelines hasbeen published for personal and educational use only.No commercial use isauthorized.No part of the ESC
Guidelines may be translated or reproduced in any form without written permission from the ESC. Permission can be obtained upon submission of awritten request to Oxford Uni-
versity Press, the publisher of the European Heart Journal and the party authorized to handle such permissions on behalf of the ESC ([email protected]).
Disclaimer . The ESC Guidelines represent the viewsof the ESC and were produced after careful consideration of the scientific and medical knowledge and the evidence available at
the time of their publication. The ESC is not responsible in the event of any contradiction, discrepancy and/or ambiguity between the ESC Guidelines and any other official recom-
mendations or guidelines issued by the relevant public health authorities, in particular in relation to good use of healthcare or therapeutic strategies. Health professionals are encour-
aged to take the ESC Guidelines fully into account when exercising their clinical judgment, as well as in the determination and the implementation of preventive, diagnostic or
therapeutic medical strategies; however, the ESC Guidelines do not override, in any way whatsoever, the individual responsibility of health professionals to make appropriate and
accurate decisions in consideration of each patient’s health condition and in consultation with that patient and, where appropriate and/or necessary, the patient’s caregiver. Nor
do theESC Guidelines exempt health professionals from takinginto full and careful consideration the relevant official updated recommendations or guidelines issued by thecompetent
public health authorities, in order to manage each patient’s case in light of the scientifically accepted datapursuant to their respective ethical and professional obligations. It isalso the
health professional’s responsibility to verify the applicable rules and regulations relating to drugs and medical devices at the time of prescription.
& The European Society of Cardiology 2016. All rights reserved. For permissions please email: [email protected].
doi:10.1093/europace/euw295
Europace (2016) 18, 1609–1678
Downloaded from https://academic.oup.com/europace/article-abstract/18/11/1609/2437601
by Biblioteca di Scienze, Universita' degli Studi di Firenze useron 20 November 2017
Kirchhof P,
Europace 2017

Conclusioni
I risultati dei principali “trial” clinici e degli studi di mondo reale
dimostrano che, per la CVE, i NOACs hanno efficacia e sicurezza
sovrapponibili a quelle degli AVK
Ulteriori vantaggi dei NOACs da prendere in considerazione per la
CVE sono: la “maggiore” aderenza alla terapia, il non dover
ritardare lo svolgimento della procedura, una efficacia
sovrapponibile a quella degli AVK nella dissoluzione della trombosi
in auricola, una minor compromissione della funzione renale
I NOACs sarebbero già preferibili per le loro proprietà “note” (1-
rapidi inizio e termine del loro effetto, 2- comportamento prevedibile
senza necessità di monitoraggio, 3- minori interazioni
farmacologiche)

90,1
2,7 3,9 2,6
0
20
40
60
80
100
Success Death Safety Efficacy
Pati
en
ts (
%)
Success of the procedure and incidence of safety and efficacy events
N=75 – Age: 83+3 years
CHA2DS2-VASc: 5.2+1.4
Prior bleeding on OAC: 29.3%
Oral anticoagulation: 44%
Procedural time: 65 minutes
Fluoroscopy time: 13 minutes
Baseline & 12 months evaluation
Gafoor S, Catheter and
Cardiov Interv 2014

So
lub
le P
-sele
cti
n (
ng
/mL
)
So
lub
le C
D40 lig
an
d (
pg
/mL
)
P=0.639 P=0.311
Changes in the markers of platelet activation after LAAC
(N=43; Age: 76+9 years; CHA2DS2-VASc: 4)
Rodes-Cabau J,
Am J Cardiol 2017
Antithrombotic Tx
ASA – 30%
Clopidogrel – 7%
ASA and Clopidogrel – 63%

Pro
thro
mb
in f
rag
men
t 1+
2
(nm
ol/L
)
Th
rom
bin
-an
tith
rom
bin
III
(ng
/mL
)
P<0.001 P<0.001 * *
*
Changes in the markers of coagulation activation after LAAC
(N=43; Age: 76+9 years; CHA2DS2-VASc: 4)
*: p<0.05 vs. Baseline
Rodes-Cabau J,
Am J Cardiol 2017
Antithrombotic Tx
ASA – 30%
Clopidogrel – 7%
ASA and Clopidogrel – 63%

by day 180 (95% CI 3 to 28, p¼0.18 vs baseline). TATlevels increased by 143%from baselineat day 7 (95% CI79 to 206) and decreased over time, yet remained signifi-cantly greater than baselineat days30 (55%, 95%CI 14 to96) and180(55%, 95%CI 16 to94, p¼0.01vsbaseline).Thedegreeof increase in F1þ2 and TAT levelsaccordingto the main clinical and procedural factors are listed inTable2. Neither clinical nor procedural variablecorrelatedsignificantly with thedegreeof increase in both F1þ2 andTAT levels. Theresultsof platelet activationasassessedbysPselectin and sCD40L levels are listed in Figure2. Therewerenosignificant changesinsPselectin (baseline29.9ng/ml, p ¼ 0.639) and sCD40L (baseline 678.4 pg/ml, p ¼0.311) at any time after LAAC. The results of plateletactivation according to theantiplatelet treatment at hospitaldischarge (dual vs single antiplatelet therapy) are listed inFigure3. No significant changes in platelet activation wereobserved irrespective of the type of antiplatelet regimenafter LAAC.
Table 3 describes clinical events during the follow-upperiod. After a mean follow-up of 21 20 months, therewereno thromboembolic events. Onepatient (2.3%) had athrombus attached to a Watchman device as assessed byTEE6 weeksafter theprocedure. Thepatient had receiveddual antiplatelet therapy after LAAC. Warfarin therapy was
initiated and the thrombus completely resolved within8weeks. Thispatient demonstratedanincreaseinF1þ2andTAT levelsfrom0.13 to 0.17 (26%increase) and from2.9to 4.1 (40%increase), respectively, at 7 days after LAAC.TheF1þ2andTAT levelsremainedhigher thanbaselineat30 daysafter LAAC(0.21 nmol/L for F1þ2, 3.7 ng/ml forTAT).
Discussion
LAACwasassociatedwithasignificant activationof thecoagulation system, which reached peak levels7 daysafterthe procedure, and partially returned to baseline levels byday 30. However, mild increments in themarkersof coag-ulation activation persisted at 6 months after LAAC. Nospecific clinical or procedural factors were found to asso-ciatewithgreater coagulationsystemactivation. LAACwasnot associated with any significant increase in plateletactivation.
Experimental studieshaveshownthat theWatchmanandACPdevicesarepartially or completely endotheliazedat 30to 90 days after LAAC.11e13 These devices are thereforeexposed to circulating blood during the initial weeks after
Table2
Degreeof activationof thecoagulationmarkers, according tobaselineand
procedural variables
Variables DF1þ2 (%) p value DTAT (%) p value
Age(years)
<76 (n¼18) 76 (44-108) 0.80 191 (74-308) 0.35
76 (n¼25) 68 (42-94) 141 (77-204)
Sex
Male(n¼23) 71 (41-100) 0.63 120 (41-100) 0.22
Female(n¼20) 73 (46-100) 209 (98-320)
Diabetes
Yes(n¼16) 78 (42-113) 0.57 139 (54-224) 0.69
No (n¼27) 68 (44-93) 175 (92-258)
Previousheart failure
Yes(n¼12) 55 (14-96) 0.15 87 (26-148) 0.10
No (n¼31) 78 (55-101) 193 (114-272)
Chronic renal failure
Yes(n¼17) 63 (35-91) 0.61 114 (51-1780) 0.30
No (n¼26) 77 (49-104) 192 (102-281)
Atrial fibrillation type
Paroxysmal (n¼23) 64 (38-89) 0.46 179 (79-278) 0.96
Chronic (n¼20) 81 (49-113) 142 (78-207)
Stroke
Yes(n¼15) 61 (34-88) 0.73 194 (41-348) 0.97
No (n¼28) 77 (50-104) 147 (91-202)
LAACDevice
ACP(n¼16) 84 (49-119) 0.34 236 (102-370) 0.06
Watchman (n¼27) 65 (40-89) 122 (64-179)
Antiplatelet therapy
Single(n¼16) 75 (49-101) 0.35 212 (75-349) 0.32
Dual (n¼27) 70 (42-98) 135 (76-194)
Peri-deviceleak>3mm
Yes(n¼5) 70 (-47-187) 0.55 199 (-68-466) 0.73
No (n¼38) 72 (52-91) 157 (94-221)
Abbreviationsasin Table1.
Figure 2. Changes in the markers of platelet activation after LAAC. (A)
Changes in sPselectin levels after LAAC. (B) Changes in sCD40L levels
after LAAC.
Arrhythmiasand Conduction Disturbances/Hemostatic Markersand LAAC 89
by day 180 (95% CI 3 to 28, p¼0.18 vs baseline). TATlevels increased by 143% from baseline at day 7 (95% CI79 to 206) and decreased over time, yet remained signifi-cantly greater than baselineat days30 (55%, 95%CI 14 to96) and180(55%, 95%CI 16 to94, p¼0.01vsbaseline).Thedegreeof increase in F1þ2 and TAT levelsaccordingto the main clinical and procedural factors are listed inTable2. Neither clinical nor procedural variablecorrelatedsignificantly with thedegreeof increase in both F1þ2 andTAT levels. Theresultsof platelet activationasassessedbysPselectin and sCD40L levels are listed in Figure 2. Therewerenosignificant changes insPselectin (baseline29.9 ng/ml, p ¼ 0.639) and sCD40L (baseline 678.4 pg/ml, p ¼0.311) at any time after LAAC. The results of plateletactivation according to theantiplatelet treatment at hospitaldischarge (dual vs single antiplatelet therapy) are listed inFigure3. No significant changes in platelet activation wereobserved irrespective of the type of antiplatelet regimenafter LAAC.
Table 3 describes clinical events during the follow-upperiod. After a mean follow-up of 21 20 months, therewereno thromboembolic events. Onepatient (2.3%) had athrombus attached to a Watchman device as assessed byTEE6 weeksafter theprocedure. Thepatient had receiveddual antiplatelet therapy after LAAC. Warfarin therapy was
initiated and the thrombus completely resolved within8weeks. Thispatient demonstratedanincreaseinF1þ2andTAT levelsfrom0.13 to 0.17 (26%increase) and from2.9to 4.1 (40% increase), respectively, at 7 days after LAAC.TheF1þ2andTAT levelsremainedhigher thanbaselineat30 daysafter LAAC(0.21 nmol/L for F1þ2, 3.7 ng/ml forTAT).
Discussion
LAACwasassociatedwithasignificant activationof thecoagulation system, which reached peak levels7 daysafterthe procedure, and partially returned to baseline levels byday 30. However, mild increments in themarkersof coag-ulation activation persisted at 6 months after LAAC. Nospecific clinical or procedural factors were found to asso-ciatewithgreater coagulationsystemactivation. LAACwasnot associated with any significant increase in plateletactivation.
Experimental studieshaveshownthat theWatchmanandACPdevicesarepartially or completely endotheliazedat 30to 90 days after LAAC.11e13 These devices are thereforeexposed to circulating blood during the initial weeks after
Table2
Degreeof activation of thecoagulation markers, according tobaselineand
procedural variables
Variables DF1þ2 (%) p value DTAT (%) p value
Age(years)
<76 (n¼18) 76 (44-108) 0.80 191 (74-308) 0.35
76 (n¼25) 68 (42-94) 141 (77-204)
Sex
Male(n¼23) 71 (41-100) 0.63 120 (41-100) 0.22
Female(n¼20) 73 (46-100) 209 (98-320)
Diabetes
Yes(n¼16) 78 (42-113) 0.57 139 (54-224) 0.69
No (n¼27) 68 (44-93) 175 (92-258)
Previousheart failure
Yes(n¼12) 55 (14-96) 0.15 87 (26-148) 0.10
No (n¼31) 78 (55-101) 193 (114-272)
Chronic renal failure
Yes(n¼17) 63 (35-91) 0.61 114 (51-1780) 0.30
No (n¼26) 77 (49-104) 192 (102-281)
Atrial fibrillation type
Paroxysmal (n¼23) 64 (38-89) 0.46 179 (79-278) 0.96
Chronic (n¼20) 81 (49-113) 142 (78-207)
Stroke
Yes(n¼15) 61 (34-88) 0.73 194 (41-348) 0.97
No (n¼28) 77 (50-104) 147 (91-202)
LAACDevice
ACP(n¼16) 84 (49-119) 0.34 236 (102-370) 0.06
Watchman (n¼27) 65 (40-89) 122 (64-179)
Antiplatelet therapy
Single(n¼16) 75 (49-101) 0.35 212 (75-349) 0.32
Dual (n¼27) 70 (42-98) 135 (76-194)
Peri-deviceleak>3mm
Yes(n¼5) 70 (-47-187) 0.55 199 (-68-466) 0.73
No (n¼38) 72 (52-91) 157 (94-221)
Abbreviationsasin Table1.
Figure 2. Changes in the markers of platelet activation after LAAC. (A)
Changes in sPselectin levels after LAAC. (B) Changes in sCD40L levels
after LAAC.
Arrhythmiasand Conduction Disturbances/Hemostatic Markersand LAAC 89
So
lub
le P
-se
lecti
n (
ng
/mL
)
So
lub
le C
D4
0 l
iga
nd
(p
g/m
L)
P=0.639 P=0.311
Changes in the markers of platelet activation after LAAC
(N=43; Age: 76+9 years; CHA2DS2-VASc: 4)
Rodés-Cabau J, Am J Cardiol 2017
Changes in Coagulation and Platelet Activation Markers
Following Transcatheter Left Atrial AppendageClosure
JosepRodés-Cabau, MD*, GillesO’Hara, MD, Jean-Michel Paradis, MD, Mathieu Bernier, MD,TaniaRodriguez-Gabella, MD, Ander Regueiro, MD, KimO’Connor, MD, Jonathan Beaudoin, MD,
Rishi Puri, MBBS, MélanieCôté, MSc, and Jean Champagne, MD
The recommendations for antithrombotic treatment after left atrial appendage closure(LAAC) remain empirical, and no data exist on thechanges in hemostatic markersasso-ciated with LACC. Theobjectiveof thepresent study istodeterminethepresence, degree,and timing of changes in themarkersof platelet and coagulation activation after LAAC.Forty-threepatients(mean age76– 9years, 23men) with atrial fibrillation whounderwentsuccessful LACCwith theWatchman(n [ 27) or Amplatzer CardiacPlug(n [ 16) deviceswere included in thestudy. Patients received antiplatelet therapy after LAAC (aspirin Dclopidogrel: 27patients; singleantiplatelet therapy with aspirin or clopidogrel: 16patients).Prothrombin fragment 1D2 and thrombin-antithrombin III were used as markers ofcoagulation activation, and soluble P-selectin and soluble CD40 ligand were used asmarkersof platelet activation. Measurementsof all hemostatic markerswereperformed atbaseline just before the procedure, followed by days 7, 30, and 180 after LAAC. Pro-thrombin fragment 1D 2and thrombin-antithrombin levelsincreased from0.27nmol/L and4.68 ng/ml, respectively, at baseline to peak values of 0.43 nmol/L and 9.76 ng/ml,respectively, at 7days, partially returningtobaselinelevelsat days30and 180after LAAC(p<0.001for bothmarkers). Noclinical or procedural factorswereassociated withagreaterincrease in themarkersof coagulation activation after LAAC. Levelsof solubleP-selectinand soluble CD40 ligand did not change at any time after LAAC. In conclusion, trans-catheter LAAC is associated with significant activation of the coagulation system, yetwithout evidenceof significant platelet activation. Ó2017Elsevier Inc. All rightsreserved.(Am J Cardiol 2017;120:87e91)
Transcatheter left atrial appendage closure (LAAC)has emerged as an alternative to anticoagulation for pre-venting thromboembolic events in patients with atrialfibrillation.1 Although most complications associatedwith LAAC havedecreased with time, the occurrence ofdevice thrombosis remains a concern, with an incidenceof 4%to 6%.2,3 The typeand duration of antithrombotictherapiesafter LAAChaveevolvedempirically. Althoughtransient (6 weeks) anticoagulation therapy has beenrecommended in some studies,4,5 others have used dualantiplatelet therapy within the 3 to 6 months after theprocedure.3,5,6 More recently, single antiplatelet therapyimmediately after LAAC has also been suggested.7
However, there is currently no biologic basis supportingaspecific approach, and deciphering specific alternationsof platelet and coagulation activation after LAAC couldbe useful for guiding the type and duration of antith-rombotic therapy after LAAC. Soluble P-selectin (sPse-lectin) and CD40 ligand (CD40L) have been wellvalidated as markers of platelet activation,8,9 andprothrombin fragment 1þ2 (F1þ2) and thrombin-
antithrombin III (TAT) as markers of coagulation acti-vation.10 Thepurposeof thepresent study istodeterminethe presence, degree, and timing of the changes in themarkersof platelet (sPselectin, sCD40L) and coagulation(F1þ2, TAT) activation after LAAC.
Methods
A total of 43 patientswith atrial fibrillation who under-went LAACbecauseof contraindicationstoanticoagulationtherapy were included in the study. The procedures wereperformedthroughthetransfemoral approach, under generalanesthesia with transesophageal echocardiographic guid-ance. Details specific to the LAAC procedure have beendetailed elsewhere.4e6 The device (Watchman [BostonScientific, Natick, MA] or Amplatzer Cardiac Plug [ACP;St Jude Medical, Minneapolis, MN]) was selected accord-ing to left atrial appendage anatomy and physician’s pref-erence. Dual antiplatelet therapy (aspirin 80 mg/day þclopidogrel 75 mg/day) for 45 days and then aspirinindefinitely was thestandard therapy after LAAC, but sin-gle antiplatelet therapy was an alternative option in thosepatientsat very highrisk of recurrent bleeding(HAS-BLEDscore >3). The final decision was left at the discretion ofthe physician responsible for the patient. A control trans-esophageal echocardiography (TEE) was performed at6 weeks after LAAC, and patients underwent clinicalfollow-up at 6 and 12 months after the procedure, and
Department of Cardiology, Quebec Heart & Lung Institute, Laval
University, QuebecCity, Quebec, Canada. Manuscript receivedJanuary 28,
2017; revised manuscript received and accepted March 16, 2017.
Seepage91 for disclosure information.
*Corresponding author: Tel: (418) 6568711; fax: (418) 6564544.
E-mail address: [email protected](J. Rodés-Cabau).
0002-9149/17/$ - seefront matter Ó 2017 Elsevier Inc. All rights reserved. www.ajconline.org
http://dx.doi.org/10.1016/j.amjcard.2017.03.253
Antithrombotic Tx ASA – 30%
Clopidogrel – 7%
ASA and Clopidogrel – 63%
![PASSENGER 42 - Mariani ascensori · PASSENGER42 ' (FjZhid i^ed Y^ ZaZkVidgZ ]V aV egZgd\Vi^kV Y^ ediZg ZhhZgZ XdbVcYVid ^c VhhdajiV h^XjgZooV ... VaaV bVcdkgV VY jdbd egZhZciZ! cZ](https://static.fdocumenti.com/doc/165x107/5c4dbb1e93f3c3176074c285/passenger-42-mariani-passenger42-fjzhid-ied-y-zazkvidgz-v-av-egzgdvikv.jpg)

![Laboratorio Informatica LT 2019 2020 D - units.it€¦ · vy vl]h y ordg '70bruwrpbuhjbuhjulg pb:*6 b+' pdw qxp vwu frqyhuwh l qxphul lq vwulqjkh dowulphqwl od frqfdwhqd]lrqh gl vwulqjkh](https://static.fdocumenti.com/doc/165x107/5f6e7a0a9807f4198d0d928b/laboratorio-informatica-lt-2019-2020-d-unitsit-vy-vlh-y-ordg-70bruwrpbuhjbuhjulg.jpg)


![Il compagno don Camillo tra letteratura e cinema: Italia, … La canzone Oj vy, koni stal´nye [Oh voi, cavallid’acciaio], no-ta anche come La marcia dei trattoristi, fu la celebrata](https://static.fdocumenti.com/doc/165x107/5b03799d7f8b9a8c688c3985/il-compagno-don-camillo-tra-letteratura-e-cinema-italia-la-canzone-oj-vy.jpg)




![Archimede 2014 new - · PDF filecontenitore laterale che funge da supporto al piano lavoro). ... TLSHTPUL JVTL ^P[O LKNL VW[PVUZ 0[ JHU LP[OLY TH[JO [OL [VW VY OH]L H WVSPZOLK](https://static.fdocumenti.com/doc/165x107/5aab4d4d7f8b9a693f8bbc52/archimede-2014-new-contenitore-laterale-che-funge-da-supporto-al-piano-lavoro.jpg)
![AS 09 064-074 - Automazione Plusautomazione-plus.it/.../uploads/sites/3/2014/12/AS_09_064-074.pdf · W^cVbZcid Xdc ]VgYlVgZ Y^ XVaXdad e^ heZX^" [^X^ XdbZ VY ZhZbe^d ^ cdiZWdd` d](https://static.fdocumenti.com/doc/165x107/5ad07bf57f8b9a56098e6887/as-09-064-074-automazione-plusautomazione-plusituploadssites3201412as09064-074pdfwcvbzcid.jpg)


![Un Designer per le Imprese per le Imprese.pdfg^hedcYVcd VY jcV ad\^XV Y^ egdYjo^dcZ ÆAdl 8dhiÇ! Xdc egdXZhh^ egdYjii^k^ e^ hZbea^X^ ZY Z[ÒX^Zci^! Z X]Z egZkZYV aÉji^a^ood Y^ bViZg^Va^](https://static.fdocumenti.com/doc/165x107/5e7b306005ffac1ab81bcd92/un-designer-per-le-imprese-per-le-impresepdf-ghedcyvcd-vy-jcv-adxv-y-egdyjodcz.jpg)


