Prof. Silvio Brusaferro
92
Pazienti insoddisfatti e operatori in burn out: un outcome da evitare Silvio Brusaferro Accreditamento, gestione del rischio Clinico e valutazione delle Performance sanitarie Dipartimento di Patologia e Medicina Sperimentale e Clinica Università degli Studi di Udine
Transcript of Prof. Silvio Brusaferro

Pazienti insoddisfatti e operatori in burn out: un outcome da evitare
Silvio Brusaferro
Accreditamento, gestione del rischio Clinico e valutazione delle
Performance sanitarie
Dipartimento di Patologia e Medicina Sperimentale e Clinica Università degli Studi di Udine

Mi presento …
• Silvio Brusaferro – Professore Ordinario Igiene e Medicina
Preventiva – Dipartimento di scienze mefdiche e biologiche - Università degli Studi di Udine
– Direttore SOC Accreditamento, Rischio clinico e Valutazione delle performance
Azienda Ospedaliero Universitario “S.Maria della Misericordia” Udine
– Tel 0432 559206, fax 0432 559239, – email: [email protected]

L’intervento
• Il concetto di salute ed le aspettative del paziente • La centralità del cittadino • Alcuni dati • Verso cittadini più attivi e soddisfatti • E i professionisti ?

Il concetto di salute e le aspettative del paziente

Definizione di salute “definizione O.M.S.”
“Health is a state of complete physical, mental, and social well-being and not
merely the absence of disease or infirmity”
“La salute è uno stato di completo benessere fisico, psichico
e sociale e non solo l’assenza di malattia o infermità”

Definizione di salute (A.Seppilli 1966)
la salute non è una condizione statica di equilibrio perfetto; al contrario, essa consiste
in uno sforzo continuo di adattamento alle mutevoli condizioni ambientali.
La salute è una condizione di armonico equilibrio funzionale, fisico e psichico,
dell’individuo dinamicamente integrato nel suo ambiente naturale e sociale

Concetto di salute “L’uomo per serbare salute e benessere, per tutelare e migliorare la qualità della vita, deve
mantenersi in equilibrio col suo mondo” Cosmacini
“Il segreto della salute e della felicità risiede nella capacità di adattarsi con successo, anche il
minimo possibile, alle condizioni eternamente mutevoli del mondo: il prezzo che si paga per gli
insuccessi di questo grande processo di adattamento sono la malattia e l’infelicità”
Hans Selye

Definizione di salute
La salute va intesa non come un fenomeno statico di esclusivo dominio dei servizi sanitari, ma come un
processo dinamico e multidimensionale, individuale ed allo stesso tempo sociale, che comprende un
pattern di fluttuazioni, autotrasformazioni ed autotrascendenza che comporta crisi e transizioni. Ciò rende spesso impossibile il tracciare delle linee nette tra Salute e malattia. La Salute e la malattia
non sono punti opposti di un continuum
Di Stanislao, Kickbusch

Kickbusch, 1987
Diventando la misura della capacità di un individuo o di un gruppo di realizzare la proprie
aspirazioni e i propri bisogni e di mutare o adattarsi all’ambiente, la salute è qualcosa di più
dei suoi componenti: è tenuta insieme da assunzioni spirituali ed emozionali di benessere,
da percezioni di sé e dei rapporti con gli altri”


la morte è inevitabile; la maggior parte delle malattie gravi non può essere
guarita; gli antibiotici non servono per curare l'influenza; le protesi artificiali ogni tanto si rompono; gli ospedali sono luoghi pericolosi; ogni medicamento ha anche degli effetti secondari; la maggioranza degli interventi medici danno solo benefici
marginali e molti non funzionano affatto; gli screening producono anche risultati falsi negativi e falsi
positivi; ci sono modi migliori di spendere i soldi che utilizzarli per
acquistare tecnologia medico-sanitaria.



Doing Something About It
Society
Intervention Level
Individual
Healthy Chronic Conditions
Impaired Health Spectrum
Disabled End of Life
Laws, Regulations & Resources Allocation
Community Design
Education & Awareness
Costs & Prompts
Behavioral Prevention Programs Care & Disease Management
Social Support & Coping Resources
Tailored Pharmaceutical Treatment
Surveillance & Prevention of Complications
Case Management
??? End of Life Planning Assisted Living


La centralità del paziente

Elementi essenziali per un sistema sanitario (STEEEP)
Sicuro: evitare i danni al paziente
• Tempestivo: riduce al minimo ritardi inutili
Efficiente: evita le attese
• Equo: la stessa qualità di cura è garantita per tutti, a prescindere da razza, sesso, locazione geografica e disponibilità economiche
Efficace: è basato su conoscenze scientifiche (evitando sovra o sottoutilizzi)
Centrato sul Paziente: è rispettoso e attento alle preferenze, esigenze e valori dei singoli pazienti
Commette on Quality of Health Care in America Crossing the quality chasm: a new health system for the 21st century Washington, DC:National Academy Press, 2001

Il concetto di valore nell’assistenza sanitaria
(value in healthcare) (Michael Porter)
• In qualsiasi campo , migliorare la performance e accountability dipende dall’avere degli obiettivi condivisi che uniscono gli interessi e le attività di tutti i soggetti interessati (stakeholders)
• Il concetto di valore si riferisce al risultato raggiunto in rapporto al costo richiesto
• Definire e misurare il valore è essenziale per comprendere la performance di qualsiasi organizzazione e per oreintare il miglioramento continuo
• Nella assistenza sanitaria , il valore è definito come l’esito in termini di salute per il paziente raggiunto per ogni dollaro speso.

Condizioni iniziali del paziente
processi indicatori
struttura
Esiti di salute
Compliance paziente
Misurare il valore nei sistemi sanitari
Soddisfazione del paziente
Esiti di salute riportati dal paziente



programma "Health for Growth”
• Objettivo 2: incrementare l’accesso ad una assistenza sanitaria migliore e più sicura per tutti i cittadini Europei.
• L’azione mirerà ad incrementare:
– L’accesso a informazioni e competenze mediche per condizioni specifiche;
– Lo sviluppo di soluzioni e linee guida per migliorare la qualità e la sicurezza dell’assistenza ai pazienti;
– Le azioni a supporto dei diritti dei pazienti relativamente a
• Assistenza transfrontaliera,
• Malattie rare ed uso prudente degli antibiotici
• Elevati standard di qualità e sicurezza per organi e sostanze di origine umana usare in medicina

Programma "Health for Growth”
• Obiettivo 3: promuovere la buona salute e prevenire le patologie affrontando i fattori di rischio chiave: – Fumo
– Alcool
– obesità
– Questo include il rafforzare e disseminare le migliori pratiche con rapporto costo efficacia della prevenzione favorevole.
• Obiettivo 4: proteggere le persone dai rischi transfrontalieri

Principali sfide da affrontare con il programma
• Safety.
– Occorre rinforzare il coordinamento delle autorità nazionali
– Affrontare i rischi legati alla globalizzazione delle catene di produzione
– C’è una domanda crescente di servizi sicuri anche per gli anziani e la necessità di affrontare una crescente sensibilità ai problemi della sicurezza degli alimenti.

• Informazione e educazione ai consumatori
– C’è necessità di
• Informazioni comparabili, affidabili, facilmente utilizzabili per i consumatori;
• Affrontare i problemi della scarsa conoscenza dei diritti da parte dei consumatori
• Di dati robusti su come il mercato sta rispondendo ai consumatori
• Far crescere il ruolo delle organizzazioni dei consumatori;
Principali sfide da affrontare con il programma

• Diritti dei consumatori e reale soddisfazione
– Vi è necessità di assicurare ai consumatori che i loro diritti sono tutelati nei vari paesi allo stesso modo che nel loro
• Rafforzare la collaborazione transfrontaliera
– C’è bisogno di incrementare la consapevolezza su ECC-Net (network of European Consumer Centres) tra i consumatori e di rinforzare la sua efficacia.
Principali sfide da affrontare con il
programma

• Vi è inoltre l’esigenza di affrontare alcune nuove sfide sociali :
– La complessità delle decisioni per i consumatori
– La necessità di adottare modelli di consumo sostenibili
– La necessità di affrontare le sfide della digitalizzazione
– L’invecchiamento della popolazione
– L’incremento della esclusione sociale e dei consumatori vulnerabili
Principali sfide da affrontare con il
programma



© Active Citizenship Network, 2002
2
EUROPEAN CHARTER OF PATIENTS’ RIGHTS *
Presented in Brussels on 15 November 2002
* This document is the result of the work of a Cittadinanzattiva-Active Citizenship Network group composed of
Giuseppe Cotturri, Stefano A. Inglese, Giovanni Moro, Charlotte Roffiaen and Consuelo Scattolon, who produced a
first draft in July, 2002. The draft was discussed in Rome on 7 September. The participants in the Rome seminar were:
Ekkehard Bahlo, Deutsche Gesellschaft für Versicherte und Patienten e. V. (DGVPV); Pascale Blaes, Fédération Belge
contre le Cancer; Fátima Carvalho Lopes, APOVITA, Portugal; Ana Etchenique, Confederacion de Consumidores y
usurarios (CECU), Spain; Ioannis Iglezakis, KE.P.KA, Greece; Stefano A. Inglese, Cittadinanzattiva / Tribunal for
Patients’ Rights, Italy; Stephen A. McMahon, Irish Patients Association Ltd; Giovanni Moro, Active Citizenship
Network; Margrethe Nielsen, Danish Consumer Council; Teresa Petrangolini, Cittadinanzattiva, Italy; Ysbrand
Poortman, Vereniging Samenwerkende Ouder- en Patiëntenorganisaties (VSOP), The Netherlands; Charlotte Roffiaen,
Active Citizenship Network; Martin Rusnak, International Neurotrauma Research Organization, Austria; Bas Treffers,
Nederlandse Patiënten Consumenten Federatie (NPCF); Simon Williams, The Patients Association, UK. This text was
also presented and discussed during the Conference “The Future Patient” held the 14 – 15 November 2002 in Brussels
organized by Active Citizenship Network (ACN), International Association of Patients’ Organization (IAPO), Ippr,
Picker Institute Europe, Merck Sharpe & Dome. The present text has been prepared based on these discussions. The
ACN also would like to thank George France for his careful review of the text. Of course, the content of the text is the
exclusive responsibility of Active Citizenship Network.

La certa dei diritti dei pazienti
Diritto a:
1. Alla prevenzione
2. All’accesso alle cure
3. All’informazione
4. Al consenso
5. Alla libero scelta
6. Alla privacy
7. Al rispetto dei tempi del paziente
Diritto a :
8. Al rispetto degli standard di qualità
9. Alla sicurezza
10. All’innovazione
11. Ad evitare sofferenze e dolore non necessari
12. Al trattamento personalizzato
13. A lamentare disservizi
14. Alla compensazione

1. Accesso equo per i pazienti
2. Conivolgimento dei pazienti
3. Prospettiva dei pazienti
4. Organizzazioni di Pazienti sostenibili
5. Unità dei pazienti


• Popolazione e comunità: mantenimento della salute pubblica • Consumatore, utente e cliente: aspettative ed esperienze del
paziente • Benessere dello staff: salute personale e sociale e morale • Competenze dello staff: ottenere e mantenere la conoscenza
e le abilità individuali • Pratica clinica: definire e testare l’efficacia contro l’evidenza
scientifica • La erogazione del servizio: gestione e buona organizzazione • Rischio, salute e sicurezza: promuovere un ambiente sicuro
per le cure • La gestione delle risorse: evitare spreco di abilità, tempo,
materiale e denaro • Comunicazione: informazione interne ed esterne e cartelle
CAPITOLI ALL’INTERNO DEI QUALI SI
PONGONO STANDARD E MISURE



ANNALS OF FAM ILY M EDICINE ✦ WWW.ANNFAM M ED.ORG ✦ VOL. 9, NO. 2 ✦ M ARCH/APRIL 2011
155
Measuring Patients’ Perceptions of Patient-Centered Care: A Systematic Review of Tools for Family Medicine
ABSTRACT
PURPOSE Patient-centered care is widely acknowledged as a core value in family
medicine. In this systematic review, we aimed to identify and compare instru-
ments, subscales, or items assessing patients’ perceptions of patient-centered care
in family medicine.
METHODS We conducted a systematic literature review using the MEDLINE,
Embase, and Cochrane databases covering 1980 through April 2009, with a spe-
ci c search strategy for each database. The search strategy was supplemented with
searching by hand and expert suggestions. We looked for articles meeting all of
the following criteria: (1) describing self-administered instruments measuring patient
perceptions of patient-centered care; (2) reporting quantitative or psychometric
results of development or validation; (3) being relevant to an ambulatory family
medicine context. The quality of each article retained was assessed using a modi-
ed version of the Standards for Reporting of Diagnostic Accuracy. Instrument’
items were mapped to dimensions of a patient-centered care conceptual framework.
RESULTS Of the 3,045 articles identi ed, 90 were examined in detail, and 26,
covering 13 instruments, met our inclusion criteria. Two instruments (5 articles)
were dedicated to patient-centered care: the Patient Perception of Patient-Cen-
teredness and the Consultation Care Measure, and 11 instruments (21 articles)
included relevant subscales or items.
CONCLUSIONS The 2 instruments dedicated to patient-centered care address key
dimensions but are visit-based, limiting their applicability for the study of care
processes over time, such as chronic illness management. Relevant items from the
11 other instruments provide partial coverage of the concept, but these instru-
ments were not designed to provide a speci c assessment of patient-centered care.
Ann Fam Med 2011;9:155-164. doi:10.1370/afm.1226.
INTRODUCTION
In the 1950s American humanistic psychologist Carl R. Rogers developed
the concept of client-centered therapy.1-3 This approach was promoted
in the medical fi eld by psychoanalyst Michael Balint, who introduced
the term “patient-centered medicine.” 4,5 A number of authors compared
traditional medical approaches with patient-centered care. Today, patient-
centered care is widely acknowledged as a core value in family medicine.6-8
It has been associated with positive outcomes: reduction of malpractice
complaints and improvements in physician satisfaction, consultation time,
patients’ emotional state, and medication adherence.9,10 Patient-centered care
may also increase patient satisfaction and empowerment, as well as reduce
symptom severity, use of health care resources, and health care costs.11
Although many authors refer to the patient-centered care concept, defi -
nitions often differ.10,12-19 The model developed by Stewart et al10 is most
frequently cited in family medicine.11,14,20 It proposes 6 dimensions: exploring
Catherine Hudon, MD, MSc, CFPC1,2
Martin Fortin MD, MSc, CFPC1,2
Jeannie L. Haggerty, PhD3
Mireille Lambert, MA2
Marie-Eve Poitras, RN, MSC2
1Département de Médecine de Famille,
Université de Sherbrooke, Québec, Canada
2Centre de Santé et de Services Sociaux de
Chicoutimi, Québec, Canada
3Département de Médecine de Famille,
Université McGill, Québec, Canada
Confl icts of interest: authors report none.
CORRESPONDING AUTHOR
Catherine Hudon, MD, MSc, CFPC
305, St-Vallier
Chicoutimi, Québec
Canada G7H 5H6
ANNALS OF FAM ILY M EDICINE ✦ WWW.ANNFAM M ED.ORG ✦ VOL. 9, NO. 2 ✦ M ARCH/APRIL 2011
155
Measuring Patients’ Perceptions of Patient-Centered Care: A Systematic Review of Tools for Family Medicine
ABSTRACT
PURPOSE Patient-centered care is widely acknowledged as a core value in family
medicine. In this systematic review, we aimed to identify and compare instru-
ments, subscales, or items assessing patients’ perceptions of patient-centered care
in family medicine.
METHODS We conducted a systematic literature review using the MEDLINE,
Embase, and Cochrane databases covering 1980 through April 2009, with a spe-
ci c search strategy for each database. The search strategy was supplemented with
searching by hand and expert suggestions. We looked for articles meeting all of
the following criteria: (1) describing self-administered instruments measuring patient
perceptions of patient-centered care; (2) reporting quantitative or psychometric
results of development or validation; (3) being relevant to an ambulatory family
medicine context. The quality of each article retained was assessed using a modi-
ed version of the Standards for Reporting of Diagnostic Accuracy. Instrument’
items were mapped to dimensions of a patient-centered care conceptual framework.
RESULTS Of the 3,045 articles identi ed, 90 were examined in detail, and 26,
covering 13 instruments, met our inclusion criteria. Two instruments (5 articles)
were dedicated to patient-centered care: the Patient Perception of Patient-Cen-
teredness and the Consultation Care Measure, and 11 instruments (21 articles)
included relevant subscales or items.
CONCLUSIONS The 2 instruments dedicated to patient-centered care address key
dimensions but are visit-based, limiting their applicability for the study of care
processes over time, such as chronic illness management. Relevant items from the
11 other instruments provide partial coverage of the concept, but these instru-
ments were not designed to provide a speci c assessment of patient-centered care.
Ann Fam Med 2011;9:155-164. doi:10.1370/afm.1226.
INTRODUCTION
In the 1950s American humanistic psychologist Carl R. Rogers developed
the concept of client-centered therapy.1-3 This approach was promoted
in the medical fi eld by psychoanalyst Michael Balint, who introduced
the term “patient-centered medicine.” 4,5 A number of authors compared
traditional medical approaches with patient-centered care. Today, patient-
centered care is widely acknowledged as a core value in family medicine.6-8
It has been associated with positive outcomes: reduction of malpractice
complaints and improvements in physician satisfaction, consultation time,
patients’ emotional state, and medication adherence.9,10 Patient-centered care
may also increase patient satisfaction and empowerment, as well as reduce
symptom severity, use of health care resources, and health care costs.11
Although many authors refer to the patient-centered care concept, defi -
nitions often differ.10,12-19 The model developed by Stewart et al10 is most
frequently cited in family medicine.11,14,20 It proposes 6 dimensions: exploring
Catherine Hudon, MD, MSc, CFPC1,2
Martin Fortin MD, MSc, CFPC1,2
Jeannie L. Haggerty, PhD3
Mireille Lambert, MA2
Marie-Eve Poitras, RN, MSC2
1Département de Médecine de Famille,
Université de Sherbrooke, Québec, Canada
2Centre de Santé et de Services Sociaux de
Chicoutimi, Québec, Canada
3Département de Médecine de Famille,
Université McGill, Québec, Canada
Confl icts of interest: authors report none.
CORRESPONDING AUTHOR
Catherine Hudon, MD, MSc, CFPC
305, St-Vallier
Chicoutimi, Québec
Canada G7H 5H6
ANNALS OF FAMILY MEDICINE ✦ WWW.ANNFAMMED.ORG ✦ VOL. 9, NO. 2 ✦ MARCH/APRIL 2011
155
Measuring Patients’ Perceptions of Patient-Centered Care: A Systematic Review of Tools for Family Medicine
ABSTRACT
PURPOSE Patient-centered care is widely acknowledged as a core value in family
medicine. In this systematic review, we aimed to identify and compare instru-
ments, subscales, or items assessing patients’ perceptions of patient-centered care
in family medicine.
METHODS We conducted a systematic literature review using the MEDLINE,
Embase, and Cochrane databases covering 1980 through April 2009, with a spe-
ci c search strategy for each database. The search strategy was supplemented with
searching by hand and expert suggestions. We looked for articles meeting all of
the following criteria: (1) describing self-administered instruments measuring patient
perceptions of patient-centered care; (2) reporting quantitative or psychometric
results of development or validation; (3) being relevant to an ambulatory family
medicine context. The quality of each article retained was assessed using a modi-
ed version of the Standards for Reporting of Diagnostic Accuracy. Instrument’
items were mapped to dimensions of a patient-centered care conceptual framework.
RESULTS Of the 3,045 articles identi ed, 90 were examined in detail, and 26,
covering 13 instruments, met our inclusion criteria. Two instruments (5 articles)
were dedicated to patient-centered care: the Patient Perception of Patient-Cen-
teredness and the Consultation Care Measure, and 11 instruments (21 articles)
included relevant subscales or items.
CONCLUSIONS The 2 instruments dedicated to patient-centered care address key
dimensions but are visit-based, limiting their applicability for the study of care
processes over time, such as chronic illness management. Relevant items from the
11 other instruments provide partial coverage of the concept, but these instru-
ments were not designed to provide a speci c assessment of patient-centered care.
Ann Fam Med 2011;9:155-164. doi:10.1370/afm.1226.
INTRODUCTION
In the 1950s American humanistic psychologist Carl R. Rogers developed
the concept of client-centered therapy.1-3 This approach was promoted
in the medical fi eld by psychoanalyst Michael Balint, who introduced
the term “patient-centered medicine.” 4,5 A number of authors compared
traditional medical approaches with patient-centered care. Today, patient-
centered care is widely acknowledged as a core value in family medicine.6-8
It has been associated with positive outcomes: reduction of malpractice
complaints and improvements in physician satisfaction, consultation time,
patients’ emotional state, and medication adherence.9,10 Patient-centered care
may also increase patient satisfaction and empowerment, as well as reduce
symptom severity, use of health care resources, and health care costs.11
Although many authors refer to the patient-centered care concept, defi -
nitions often differ.10,12-19 The model developed by Stewart et al10 is most
frequently cited in family medicine.11,14,20 It proposes 6 dimensions: exploring
Catherine Hudon, MD, MSc, CFPC1,2
Martin Fortin MD, MSc, CFPC1,2
Jeannie L. Haggerty, PhD3
Mireille Lambert, MA2
Marie-Eve Poitras, RN, MSC2
1Département de Médecine de Famille,
Université de Sherbrooke, Québec, Canada
2Centre de Santé et de Services Sociaux de
Chicoutimi, Québec, Canada
3Département de Médecine de Famille,
Université McGill, Québec, Canada
Confl icts of interest: authors report none.
CORRESPONDING AUTHOR
Catherine Hudon, MD, MSc, CFPC
305, St-Vallier
Chicoutimi, Québec
Canada G7H 5H6
ANN ALS OF FAM ILY M EDICINE ✦ WWW.ANNFAM M ED.ORG ✦ VOL. 9, NO. 2 ✦ M ARCH/APRIL 2011
156
M EASURIN G PERCEPTIONS OF PATIEN T-CEN TERED CARE
both the disease and the illness experience, understand-
ing the whole person, fi nding common ground, incor-
porating prevention and health promotion, enhancing
the patient-doctor relationship, and being realistic. Mead
and Bower14 reviewed the conceptual and empirical lit-
erature to develop a model of the various aspects of the
doctor-patient relationship encompassed by the concept
of patient-centered care. They identifi ed the following
dimensions: biopsychosocial perspective, patient-as-
person, sharing power and responsibility, therapeutic alli-
ance, and doctor-as-person.
A clear conceptual framework is an essential fi rst
step for measurement. In the absence of a clear con-
sensual model in the literature, we decided to keep
the 4 dimensions common to Stewart et al and Mead
and Bower’s review: (1) disease and illness experience
(patient-as-person in Mead and Bower’s model), (2)
whole person (biopsychosocial perspective), (3) com-
mon ground (sharing power and responsibility), and (4)
patient-doctor relationship (therapeutic alliance). Fig-
ure 1 represents the patient-centered care framework
used as the conceptual basis in our review.
Various methodological approaches have been taken
in designing instruments to measure patient-centered
care, the 2 most predominant being direct observation of
the clinical encounter (structured objective checklist) and
self-assessment of the patient’s or the physician’s experi-
ence of the encounter.21 Many studies have shown that
measures of the patients’ perceptions are more successful
at predicting outcomes than either observation or physi-
cians’ perceptions.9-11,22 Experts also claim that patient-
administered questionnaires are the best way to measure
patient-centered care attributes of primary health care.23
In this study, we aimed to identify and compare
instruments, subscales, or items assessing patients’ per-
ceptions of patient-centered care in family medicine.
METHODS
Our review process was based on important domains
and elements identifi ed by the Agency for Healthcare
Rersearch and Quality for systematic reviews.24
Inclusion Criteria
We looked for articles meeting all of the following
criteria: (1) describing self-administered instruments
measuring at least 2 dimensions of the conceptual
framework of patient-centered care, (2) reporting
quantitative or psychometric results of development
or validation, and (3) being relevant to the context of
ambulatory family medicine.
Search Strategy and Article Selection
We conducted an electronic literature search of the
MEDLINE (1980–), Embase (1980–), and Cochrane
(1991–) databases for English and French articles pub-
lished between 1980 and April 2009. An information
specialist developed and ran specifi c strategies for each
database (Supplemental Appendix 1, available online
at http://www.annfammed.org/cgi/content/full/
9/2/155/DC1). The following MeSH terms and
key words were used: “patient-centered care” and
its linguistic variations, “questionnaire,” “process assess-
ment (health care),” “quality assurance, health care,”
“psychometrics,” “validation studies,” “reproducibility of
results,” “factor analysis, statistical,” “outcome and pro-
cess assessment (health care),” and “outcome assessment
(health care).” To broaden the scope of our research, we
also applied the following search strategy to the same
databases using “patient-centered care” and its linguistic
variations, “family practice,” “primary health care,” “pri-
mary medical care,” and “primary care.”
We also examined reference lists for additional
relevant articles (searching by hand). In addition, we
consulted experts to identify articles describing instru-
ments, including subscales or items that assess dimen-
sions of patient-centered care.
All search results were transferred to a reference
database (Refworks), and duplicates were eliminated.
Titles and abstracts were read by one team member
(M.L.) to exclude articles that were not eligible. We
excluded references clearly not meeting our inclusion
criteria and retained all other references for complete
reading. If there was any doubt, the full article was
retrieved and read to apply selection criteria. Two
Figure 1. Conceptual framework of patient-
centered care (PCC).
Patient-as-person Bio-psychosocial
perspective
Therapeutic
alliance
Sharing power
and responsibility
Disease and
illness experience
Patient-doctor
relationship
Common ground
PCC model (Mead and Bower)
PCC model (Stewart et al)
Whole person
ANNALS OF FAM ILY M EDICINE ✦ WWW.ANNFAM M ED.ORG ✦ VOL. 9, NO. 2 ✦ M ARCH/APRIL 2011
155
Measuring Patients’ Perceptions of Patient-Centered Care: A Systematic Review of Tools for Family Medicine
ABSTRACT
PURPOSE Patient-centered care is widely acknowledged as a core value in family
medicine. In this systematic review, we aimed to identify and compare instru-
ments, subscales, or items assessing patients’ perceptions of patient-centered care
in family medicine.
METHODS We conducted a systematic literature review using the MEDLINE,
Embase, and Cochrane databases covering 1980 through April 2009, with a spe-
ci c search strategy for each database. The search strategy was supplemented with
searching by hand and expert suggestions. We looked for articles meeting all of
the following criteria: (1) describing self-administered instruments measuring patient
perceptions of patient-centered care; (2) reporting quantitative or psychometric
results of development or validation; (3) being relevant to an ambulatory family
medicine context. The quality of each article retained was assessed using a modi-
ed version of the Standards for Reporting of Diagnostic Accuracy. Instrument’
items were mapped to dimensions of a patient-centered care conceptual framework.
RESULTS Of the 3,045 articles identi ed, 90 were examined in detail, and 26,
covering 13 instruments, met our inclusion criteria. Two instruments (5 articles)
were dedicated to patient-centered care: the Patient Perception of Patient-Cen-
teredness and the Consultation Care Measure, and 11 instruments (21 articles)
included relevant subscales or items.
CONCLUSIONS The 2 instruments dedicated to patient-centered care address key
dimensions but are visit-based, limiting their applicability for the study of care
processes over time, such as chronic illness management. Relevant items from the
11 other instruments provide partial coverage of the concept, but these instru-
ments were not designed to provide a speci c assessment of patient-centered care.
Ann Fam Med 2011;9:155-164. doi:10.1370/afm.1226.
INTRODUCTION
In the 1950s American humanistic psychologist Carl R. Rogers developed
the concept of client-centered therapy.1-3 This approach was promoted
in the medical fi eld by psychoanalyst Michael Balint, who introduced
the term “patient-centered medicine.” 4,5 A number of authors compared
traditional medical approaches with patient-centered care. Today, patient-
centered care is widely acknowledged as a core value in family medicine.6-8
It has been associated with positive outcomes: reduction of malpractice
complaints and improvements in physician satisfaction, consultation time,
patients’ emotional state, and medication adherence.9,10 Patient-centered care
may also increase patient satisfaction and empowerment, as well as reduce
symptom severity, use of health care resources, and health care costs.11
Although many authors refer to the patient-centered care concept, defi -
nitions often differ.10,12-19 The model developed by Stewart et al10 is most
frequently cited in family medicine.11,14,20 It proposes 6 dimensions: exploring
Catherine Hudon, MD, MSc, CFPC1,2
Martin Fortin MD, MSc, CFPC1,2
Jeannie L. Haggerty, PhD3
Mireille Lambert, MA2
Marie-Eve Poitras, RN, MSC2
1Département de Médecine de Famille,
Université de Sherbrooke, Québec, Canada
2Centre de Santé et de Services Sociaux de
Chicoutimi, Québec, Canada
3Département de Médecine de Famille,
Université McGill, Québec, Canada
Confl icts of interest: authors report none.
CORRESPONDING AUTHOR
Catherine Hudon, MD, MSc, CFPC
305, St-Vallier
Chicoutimi, Québec
Canada G7H 5H6


Aree principali di ricerca
– La gestione intraorganizzazione
– La gestione interorganizzazione
– Le relazioni con il paziente
– Governance e accountability
Working conference “Health Services Research In Europe” April 2011

Alcuni dati

Percezione e ruolo del cittadino

45° Rapporto Censis sulla situazione sociale del Paese/2011 Roma, 2 dicembre 2011 –
La sanità e il rischio di una sostenibilità solo finanziaria
• Nel periodo 2001-2010 le Regioni con Piano di rientro hanno registrato un incremento della spesa del 19% contro il +26,9% del resto delle Regioni.
• Ma la cura a cui è sottoposto il Servizio sanitario non sta generando effetti positivi secondo i cittadini.
• Nell’ultimo biennio i dati dell’indagine Forum per la Ricerca Biomedica-Censis indicano che – è solo l’11% a ritenere migliorato il servizio sanitario della
propria regione,
– quasi il 29% ha registrato un peggioramento
– circa il 60% una sostanziale stabilità.

45° Rapporto Censis sulla situazione sociale del Paese/2011 Roma, 2 dicembre 2011 –
La sanità e il rischio di una sostenibilità solo finanziaria
• Il futuro della sanità per i cittadini è segnato da alcune paure: – un’accentuazione delle differenze di qualità tra le sanità
regionali (35,2%), – che l’interferenza della politica danneggi la qualità della
sanità (35%), – che i disavanzi rendano indispensabili robusti tagli
all’offerta (21,8%), – che non si sviluppino le tipologie di strutture e servizi
necessarie, come l’assistenza domiciliare territoriale (18%), – che l’invecchiamento della popolazione e la diffusione
delle patologie croniche producano un intasamento delle strutture e dei servizi (16,3%).

Special EUROBAROMETER 3 6 3 “I NTERNAL MARKET: AW ARENESS, PERCEPTI ONS AND I MPACTS”
54
29% of EU citizens in Austria believe that doctors ought to have a qualification from their
own country, as do 28% of people in Finland. However, only 1% of people in Cyprus, 2%
in Luxembourg and 6% in Malta share this view.
I m portance of a doctor’s country of qualificat ion by individ ual Mem ber State
Attitudes towards medical training tend to also be reflected in people’s opinion of the
origin of training for hairdressers. 94% of people in Cyprus say the country of origin
makes no difference to them, as do 92% of people in Luxembourg and Sweden.
However, only 45% of people in Austria and 56% of people in Italy agree. 21% of EU
citizens in Austria think that hairdressers should be qualified in specific EU Member
States only, as do 12% in Italy.
Special EUROBAROMETER 3 6 3 “I NTERNAL MARKET: AW ARENESS, PERCEPTI ONS AND I MPACTS”
54
29% of EU citizens in Austria believe that doctors ought to have a qualification from their
own country, as do 28% of people in Finland. However, only 1% of people in Cyprus, 2%
in Luxembourg and 6% in Malta share this view.
I m portance of a doctor’s country of qualificat ion by individual Mem ber State
Attitudes towards medical training tend to also be reflected in people’s opinion of the
origin of training for hairdressers. 94% of people in Cyprus say the country of origin
makes no difference to them, as do 92% of people in Luxembourg and Sweden.
However, only 45% of people in Austria and 56% of people in Italy agree. 21% of EU
citizens in Austria think that hairdressers should be qualified in specific EU Member
States only, as do 12% in Italy.
Special EUROBAROMETER 363 “I NTERNAL MARKET: AW ARENESS, PERCEPTI ONS AND I MPACTS”
54
29% of EU citizens in Austria believe that doctors ought to have a qualification from their
own country, as do 28% of people in Finland. However, only 1% of people in Cyprus, 2%
in Luxembourg and 6% in Malta share this view.
I mportance of a doctor’s country of qualification by individual Member State
Attitudes towards medical training tend to also be reflected in people’s opinion of the
origin of training for hairdressers. 94% of people in Cyprus say the country of origin
makes no difference to them, as do 92% of people in Luxembourg and Sweden.
However, only 45% of people in Austria and 56% of people in Italy agree. 21% of EU
citizens in Austria think that hairdressers should be qualified in specific EU Member
States only, as do 12% in Italy.





Il percorso del paziente




drfoster 2010





SCUOLA SUPERIORE Sant’Anna Pisa - MeS Report Network delle Regioni 2010
Fasce per la valutazione

il bersaglio interregionale



Verso cittadini più attivi e soddisfatti

Cosa viene richiesto al professionista che opera in sanità
• Competenza : Quello che gli individui conoscono o sono in grado di fare in termini di conoscenza, abilità ed attitudini.
• Capacità di adattamento: L’ambito nel quale un individuo può adattarsi al cambiamento, generare nuove conoscenze e continuare a migliorare le sue performance.
• Auto riflessione critica : Processo strutturato che facilita il riflettere su se stessi e sul proprio operato.

• Fattori interni – Stato di salute
– Conoscenze sulla salute
– Convinzioni ed abilità nel ricercare la salute
– Valori ed obiettivi di salute
– Capacità di autogestione
– Efficacia nel prendere le decisioni rigutadanti la salute
– Motivazione intrinseca a raggiungere gli esiti di salute desiderati
– Aspettative positive rispetto agli esiti di salute
• Fattori esterni – Norme sociali
– Reti sociali e capitale sociale
– Influenza di gruppi cui si appartiene
– Circostanze materiali
– Sicurezza sociale, politica ed economica
– Accesso ed utilizzo di servizi sanitari
– Caratteristiche dei sistemi di assistenza e di sanità pubblica

Biology and Genetic Predisposition
Genes Personality
Risk seeking/risk averse
Intermediate Social Context
Social norms Social networks (e.g., family, school)
Group membership/expectations Neighborhood/community
Life circumstances Foundation from childhood
Public Health and Health Care System
Access to High-quality prevention and treatment Cultural barriers to optimal use of resources
Health values and norms Finance and interactive environment
Macro, Social, Political, and Economic Environment
Economics opportunities Political empowerment
Human security Social structures (e.g., class hierarchy)
Public moral norms and values Distributional norms
Human rights/discrimination Governance principles
Health Capability
Confidence and ability to be effective in achieving optimal health given biologic and genetic disposition;
intermediate and the broader social, political, and economic environment; and access to the public health
and health care system


IL CAMBIAMENTO E’ PERMANENTE
1. PRE-RIFLESSIONE
4.AZIONE
3.PREPARAZIONE
2.RIFLESSIONE 6.RICADUTA
5.MANTENIMENTO
Fasi del modello per il cambiamento
1. nessuna intenzione di
cambiare nei prossimi anni
2. cambiamento considerato
ma non nell’immediato futuro
3. pianificazione del
cambiamento nel mese
successivo
4. fase instabile di recente
acquisizione del cambiamento
5. adozione del comportamento
(da almeno X mesi)
Il ciclo può reiterarsi per 3 – 7 volte prima di garantire
un comportamento stabile



The JCAHO patient safety event taxonomy Chang A, et al. Int J Qual Health Care 2005, 17:95-105.



Evaluating Internet Health Information :
Tutorial
• Provider: – Chi è responsabile della gestione del sito? – Perchè gestiscono il sito? – Sono contabili?
• Finanziamento – Da dove provengono i fondi che permettono il
funzionamento del sito? – Il sito ha degli annunci? – Sono ben identificati?
• Qualità – Da dove provengono le informazioni? – Come sono selezionate? – Degli espertivalutano le informazioni che
vengono pubblicate sul sito? – Il sito è aggiornato? – Vengono evitati annunci sensazionali e/o
incredibili?
• Privacy – Il sito chiede dati personali? – Viene specificato come verranno usati? – Ti disturba come verranno usati?

CENSIS rapporto 2010

CENSIS rapporto 2010

CENSIS rapporto 2010

CENSIS rapporto 2010

The impact of a celebrity Promotional Campaign on the use of Colon
Cancer Screening: the Katie Couric effect
Arch Intern Med 2003; 163: 1601-1605

SPECI AL EUROBAROMETER 3 3 8 "Ant im icrobia l Resistance ”
1
Special Eurobarometer 338
Antimicrobial Resistance
Fieldwork: November - December 2009
Publication: April 2010
Euro
baro
me
ter
338
/Wave
72
.5 –
TN
S O
pin
ion &
So
cia
l
Survey commissioned by the Directorate-General for Health and Consumers and coordinated by the Directorate-General Communication (“Research and Political Analysis” Unit).
This document does not represent the views of the European Commission.
The interpretations and opinions expressed are solely those of the authors.
Summary

SPECI AL EUROBAROMETER 3 3 8 "Ant im icrobia l Resistance”
9
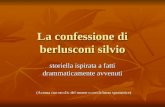
1 .3 The reason w hy respondents last took ant ibiot ics
A relative majority of respondents (20%) said that they last took antibiotics for flu,
although it is known that antibiotics are ineffective against viruses. 14% also said that
they had taken them for a cold, 17% to treat bronchitis and 15% for a sore throat.
QD1c What was the reason for last taking antibiotics that you used?
(MULTI PLE ANSWERS POSSI BLE) - EU
(Asked to respondents saying that they have taken any antibiotics in the last 12 months -
base = 10803)
17%
9%
6%
5%
1%
14%
15%
4%
2%
20%
8%
7%
20%
9%
Flu
Bronchitis (...)
Sore throat
Cold
Cough
Fever
Rhinopharyngitis (...)
Urinary tract infection
Skin or wound infection
Headache
Pneumonia (...)
Diarrhoea
Other (SPONTANEOUS)
DK
Respondents in Spain (32%), followed by those in Austria (31%), Cyprus (28%),
Bulgaria and Malta (26%), Greece (25%), Slovakia (24%), Italy and Germany (23%)
are the most likely to have taken antibiotics for flu.
Likewise, citizens in Romania (40%), Bulgaria (32%), Latvia (30%), Greece and
Cyprus (27% each), Spain (24%) and Hungary and Austria (23% each) are the most
likely to have made the mistake of taking antibiotics to treat a cold.
Young people are more likely than older respondents to take antibiotics (23% of those
in the 15-24 age group have taken them for flu, compared with 16% of those aged 55
or over; the same applies to their use to treat colds, at 16% and 11% respectively.
Respondents w ith a bet ter object ive know ledge of ant ibiot ics seem to behave
m ore responsibly: thus, among the most knowledgeable respondents, only 8% have
taken antibiotics for flu and 3% for a cold

SPECI AL EUROBAROMETER 3 3 8 "Ant im icrobia l Resistance”
18
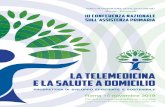
3 .2 Means of conveying inform at ion
W hen asked to ident ify their sources of inform at ion about not taking
ant ibiot ics unnecessarily, a lm ost a third of Europeans ( 3 0 % ) replied that they
had been advised by their doctor . 29% said they had seen an advertisement on
television, while 15% said that their source was a newspaper article or the TV news.
QD3b Where did you first get this information about not taking any antibiotics unnecessarily? - EU
(Asked to respondents saying that they have got any information about not taking any antibiotics
unnecessarily in the last 12 months - base = 9975)
29%
4%
2%
2%
5%
15%
4%
2%
2%
30%
5%
A doctor told me
I saw it on a TV advertisement
I read it in a newspaper or I saw it on the TV news
A pharmacist told me
A family member or friend told me
I saw it in a leaflet or on a poster
Another health professional (e.g. nurse, physical therapist) told
me
I heard it on the radio
I saw it on the Internet
Other
DK
The role played by doctors is particularly important in Hungary and Italy (59% each),
Romania (53%), the Czech Republic (48%)3. However, respondents in France (10%),
Sweden (13%), Malta (16%), Ireland and Latvia (19%) were the least likely to
mention a doctor as a source of information.
Respondents in France (71% compared with a European average of 29%) are by far
the most likely to have seen a TV advertisement on the subject, followed by those in
Belgium (51%), Luxembourg (40%), Spain (33%), Greece (32%) and Malta (30%).
Respondents in Sweden (47%), Finland (35%), Germany and Cyprus (34% each) are
the most likely to have obtained the information from a newspaper or the TV news
(compared with a European average of 15%).

SPECI AL EUROBAROMETER 3 3 8 "Ant im icrobia l Resistance”
18
3 .2 Means of conveying inform at ion
W hen asked to ident ify their sources of inform at ion about not taking
ant ibiot ics unnecessarily, a lm ost a third of Europeans ( 3 0 % ) replied that they
had been advised by their doctor . 29% said they had seen an advertisement on
television, while 15% said that their source was a newspaper article or the TV news.
QD3b Where did you first get this information about not taking any antibiotics unnecessarily? - EU
(Asked to respondents saying that they have got any information about not taking any antibiotics
unnecessarily in the last 12 months - base = 9975)
29%
4%
2%
2%
5%
15%
4%
2%
2%
30%
5%
A doctor told me
I saw it on a TV advertisement
I read it in a newspaper or I saw it on the TV news
A pharmacist told me
A family member or friend told me
I saw it in a leaflet or on a poster
Another health professional (e.g. nurse, physical therapist) told
me
I heard it on the radio
I saw it on the Internet
Other
DK
The role played by doctors is particularly important in Hungary and Italy (59% each),
Romania (53%), the Czech Republic (48%)3. However, respondents in France (10%),
Sweden (13%), Malta (16%), Ireland and Latvia (19%) were the least likely to
mention a doctor as a source of information.
Respondents in France (71% compared with a European average of 29%) are by far
the most likely to have seen a TV advertisement on the subject, followed by those in
Belgium (51%), Luxembourg (40%), Spain (33%), Greece (32%) and Malta (30%).
Respondents in Sweden (47%), Finland (35%), Germany and Cyprus (34% each) are
the most likely to have obtained the information from a newspaper or the TV news
(compared with a European average of 15%).

SPECI AL EUROBAROMETER 3 3 8 "Ant im icrobia l Resistance”
21
Respondents in Cyprus (90%), Malta (88%), Greece (86%), Bulgaria and Romania
(84%)5 are the most likely to say that in future they will always consult a doctor if they
think they need an antibiotic. Respondents in Denmark (56%), Cyprus (41%), Estonia
(40%), Malta, the Netherlands, Romania and Sweden (35%) are the most likely to say
that they will no longer take antibiotics without a doctor’s prescription.
The highest scores for stopping self-medication were recorded in Romania (39%),
Bulgaria (34%), Latvia (30%) and Denmark (27%).
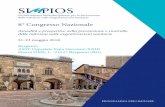
3 .5 The m ost t rustw orthy sources of inform at ion
When asked which source of information they would use to obtain trustworthy
information about antibiotics, a very large majority of Europeans said that they would
choose a doctor (88% on average).
QD4 Which of the following sources of information would you use in order to get trustworthy
information on antibiotics?
( MAXI MUM 3 ANSWERS) - EU
42%
4%
5%
4%
2%
10%
18%
2%
1%
2%
1%
3%
5%
5%
88%
6%
A doctor
A pharmacy
A hospital
A nurse
Family or friends
Another health care facility
The Internet site from the National Government\the Ministry of
Health
The Internet site from the (NATIONAL PUBLIC HEALTH
INSTITUTE)
Another health related Internet site
A Health Medical Encyclopedia
The Internet site on Public Health from the EU
A national, independent public health body or organisation
A health related magazine
A newspaper or magazine
I am not looking for information on antibiotics (SPONTANEOUS)
Other (SPONTANEOUS)
5 The results for this question must be analysed with caution given the weakness of some bases in some
countries

Il problema dalla alfabetizzazione sanitaria (health literacy)
La alfabetizzazione sanitaria (Health Literacy) viene definita come il grado in cui un individuo ha la capacità di ottenere , elaborare e comprendere informazioni di base sulla salute e
sui servizi ad essa correlati per poter adottare scelte appropriate

Il problema dalla alfabetizzazione sanitaria (health literacy)
• L’US Department of Health and Human Services nel rapporto Healthy People 2010 sottolinea che la alfabetizzazione sanitaria include la abilità di comprendere istruzioni relative a
– prescrizioni di farmaci,
– spostamenti di appuntamenti,
– opuscoli informativi,
– consensi informati,
– indicazioni del medico
• L alfabetizzazione sanitaria non richiede semplicemente di sapere leggere ma anche allo stesso tempo di ascoltare e saper prendere delle decisioni riferite a problemi di Salute

L’alfabetizzazione sanitaria è correlata agli esiti di salute
• Cancer Treatment – (Merriman, Betty, CA: A Cancer Journal for Physicians,
May/June 2002)
• Diabetes – (Schillinger, Dean, JAMA, July 24/31, 2002)
• Asthma – (Williams, MV, Chest, October 1998)
• Hypertension and Diabetes – (Williams MV, Archives of Internal Medicine, January 26,
1998)

E i professionisti ?

• Assistenza clinica processo di decisioni condivise
– Medico : esperto ed autorevole nelle scienze mediche
– Paziente : è colui che definisce I valori e le preferenze
• Popolazione e sistemi sanitari
– L’approccio basato sui soli interessi del singolo paziente deve tener conto del valore di offrire a tutti i pazienti un accesso equo all’assistenza necessaria

• La relazione medico paziente – è stata pesantemente infuenzata dal movimento
per I diritti umani
– L’assistenza è guidata da indirizzi basati su decisioni condivise
• La sfida è trovare un equilibrio tra – L’aspettativa del paziente rispetto al proprio
medico
– L’attenzione del medico ad utilizzare saggiamente le risorse in modo efficiente ed onesto.

Systems view of professionalism

• There is persuasive rationale for the active involvement of patients in health care professional education.
• There is promise and some evidence of benefits to students, patients, teachers and communities.
• However, we know too little of how to do it and how to optimise its impact, and we have too little systematic development and evaluation.

Quando pianifichi per 1 anno, pianta del grano.
Quando pianifichi per un decennio, pianta degli alberi.
Quando pianifichi per la vita, forma ed educa le persone
Proverbio Cinese
Grazie per l’attenzione !