Novità in tema di terapia delle emofilie - ER Congressi · 2017-05-29 · limitations,...
33
Transcript of Novità in tema di terapia delle emofilie - ER Congressi · 2017-05-29 · limitations,...

Relazioniconsogge9portatoridiinteressicommercialiincamposanitario
Aisensidell’art.3.3sulConfli3odiInteressi,pag.17delRegolamentoApplica=vodell’AccordoStato-Regionedel 5 novembre 2009, io so3oscri3o Do3. MarcoMarie3a dichiaro che negli ul=mi due anni ho avuto iseguen= rappor= ricevendo compens individuali consoggeG portatori di interessi commerciali in camposanitario:
! PartecipazioneadAdvisoryBoardperl’AziendaNovo-Nordisk
! Relazioni a congressi per la di3a Kedrion,Orphan,Novo-Nordisk,Werfen

Da dove veniamo? Che siamo? Dove andiamo?
Paul Gauguin, 1897

Da dove veniamo? Che siamo? Dove andiamo?
Paul Gauguin, 1897

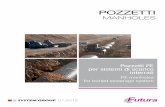
Haemophiliatreatment
pre-1930 1940 1950 1960 1970 1980 1990
ImmobilizaTon,ice,rest,analgesia
Wholebloodtransfusion
Plasma
Cryoprecipitate
1970Limitedplasma-derivedreplacementmaterialMainlyon-demand,in-hospitaltreatment
Earlycripplingarthropathy
Bleeding-relateddeaths:47%(NL)
Lifeexpectancy:59yrs(Sweden)25yrs(Finland)

Haemophiliatreatment
pre-1930 1940 1950 1960 1970 1980 1990
ImmobilizaTon,ice,rest,analgesia
Wholebloodtransfusion
Plasma
Cryoprecipitate
Intermediate-purityFVIIIconcentrate
Heat-treatedhigh-purityFVIIIconcentrate
Low-purityFVIIIconcentrate
NewerrecombinantFVIIIproducts
FirstrecombinantFVIIIproduct
2000 2010
Darbyetal,AIDS2004

Haemophiliatreatment
2000Plasma-derivedand
recombinantconcentrateslargelyavailable
DiffusionofprophylaxisHomeTreatment
Minimaljointdiseaseinpa=entsonprophylaxisBleeding-relateddeaths:
<10%(NL)
Lifeexpectancy:71yrs(Italy,NL)


All that is gold does not glitter,
Not all those who wander are lost
JRR Tolkien
The Lord of the Rings
All that glisters is not gold,
Often have you heard that told
William Shakespeare The Merchant of Venice

" Venous access: intravenous route ofadministra=on
" Infusion frequency: half-lifeFVIII∼12hrs,FIX∼20hrs
" Inhibitors" Costsandavailabilityofconcentrates" Barriertohighlydemandingregimens:
# Prophylaxis# ImmunetoleranceinducTon# Majorsurgery
Currentchallenges
fortreatmentofhemophilia

Da dove veniamo? Che siamo? Dove andiamo?
Paul Gauguin, 1897

REVIEW ARTICLE
Advances in the treatment of bleeding disordersF . PEYVANDI ,*† I . GARAGIOLA† and E . B IGUZZ I**Angelo Bianchi Bonomi Hemophilia and Thrombosis Center, Fondazione IRCCS Ca’ Granda Ospedale Maggiore Policlinico, Luigi Villa
Foundation; and †Department of Pathophysiology and Transplantation, Universit!a degli Studi di Milano, Milan, Italy
To cite this article: Peyvandi F, Garagiola I, Biguzzi E. Advances in the treatment of bleeding disorders. J Thromb Haemost 2016;
14: 2095–106.
Summary. Historically, the bleeding episodes in subjectswith coagulation disorders were treated with substitutiontherapy, initially with whole blood and fresh frozenplasma, and more recently with specific factor concen-trate. Currently, patients with hemophilia have the possi-bility of choosing different effective and safe treatments,including novel extended half-life and alternative hemo-static drugs. The availability of novel extended half-lifeproducts could probably overcome current prophylaxislimitations, particularly in hemophilia B patients, byreducing the frequency of injections, achieving a highertrough level, and improving the quality of life of thepatients. In addition, subcutaneous administration ofalternative therapeutics would simplify prophylaxis inpatients with hemophilia A and B with and without inhi-bitors. Regarding von Willebrand disease, a recombinantvon Willebrand factor was recently developed to controlbleeding episodes in patients with this disease, in additionto available von Willebrand factor/factor VIII concen-trates. The management of patients affected by rare bleed-ing disorders (RBDs) is still a challenge, owing to thelimited number of specific products, which are mainlyavailable only in countries with high resources. Someimprovements have recently been achieved by the produc-tion of new recombinant factor (F) XIII A subunit-derived and FX plasma-derived products for the treatmentof patients affected by FXIII and FX deficiency. In addi-tion, the development of novel alternative therapeutics,such as anti-tissue factor pathway inhibitor, ALN-AT3,and ACE910, for patients with hemophilia might alsohave a role in the treatment of patients affected by RBDs.
Keywords: disease management; hemophilia; inheritedblood coagulation disorders; innovative therapy; vonWillebrand disease.
Introduction
Rare diseases are life-threatening or chronically debilitat-ing diseases with a prevalence of less than one per 2000according to the European Union or one per 1250according to the USA [1]. Only a few of the 5000 recog-nized rare diseases have a prevalence approaching thoselimits, with the remaining majority being even less com-mon, such as inherited deficiencies of plasma proteinsinvolved in blood coagulation. Hemophilia A and B arethe most recognized and common hereditary hemorrhagicdisorders caused by deficiency or dysfunction of bloodcoagulation factor (F) VIII or FIX, with prevalence ratesof approximately one in 5000 and one in 30 000 male livebirths, respectively. Together with von Willebrand disease(VWD), a defect of primary hemostasis with a prevalenceranging from 1% to one in 10 000, these disorders consti-tute 95–97% of all inherited deficiencies of coagulationfactors [2,3]. Rare bleeding disorders (RBDs), includingdeficiency of fibrinogen, FII, FV, combined FV + FVIII,FVII, FX, FXI, and FXIII, represent 3–5% of allinherited coagulation disorders, with prevalence rates ofthe presumably homozygous forms or compoundheterozygous forms in the general population rangingfrom approximately one in 2 million for FII and FXIIIdeficiencies to one in 500 000 for FVII deficiency [4].The most recent annual global survey of the WorldFederation of Hemophilia reports that > 287 000 peopleare affected by a coagulation disorder across 106 coun-tries in the world, with 62.2% having hemophilia A or B,24.3% having VWD, and 13.5% having other bleedingdisorders [5].
Bleeding episodes can occur either spontaneously, or atthe time of trauma, or invasive procedures and surgery[2–4]. Management decisions and the choice of therapycommonly rely on type of clotting factor deficiency, sever-ity of disease, type of bleeding episode, and minimalresidual activity in the patient’s plasma.
Correspondence: Flora Peyvandi, Angelo Bianchi Bonomi
Hemophilia and Thrombosis Center, Fondazione IRCCS C!a Granda
Ospedale Maggiore Policlinico, Department of Pathophysiology and
Transplantation, University of Milan, Via Pace, 9-20122, Milan,
Italy.
Tel.: +39 025 503 8491; fax: +39 025 410 0125.
E-mail: [email protected]
Received 29 June 2016
Manuscript handled by: P. H. Reitsma
Final decision: P. H. Reitsma, 15 August 2016
© 2016 International Society on Thrombosis and Haemostasis
Journal of Thrombosis and Haemostasis, 14: 2095–2106 DOI: 10.1111/jth.13491
REVIEW ARTICLE
Advances in the treatment of bleeding disordersF . PEYVANDI ,*† I . GARAGIOLA† and E . B IGUZZ I**Angelo Bianchi Bonomi Hemophilia and Thrombosis Center, Fondazione IRCCS Ca’ Granda Ospedale Maggiore Policlinico, Luigi Villa
Foundation; and †Department of Pathophysiology and Transplantation, Universit!a degli Studi di Milano, Milan, Italy
To cite this article: Peyvandi F, Garagiola I, Biguzzi E. Advances in the treatment of bleeding disorders. J Thromb Haemost 2016;
14: 2095–106.
Summary. Historically, the bleeding episodes in subjectswith coagulation disorders were treated with substitutiontherapy, initially with whole blood and fresh frozenplasma, and more recently with specific factor concen-trate. Currently, patients with hemophilia have the possi-bility of choosing different effective and safe treatments,including novel extended half-life and alternative hemo-static drugs. The availability of novel extended half-lifeproducts could probably overcome current prophylaxislimitations, particularly in hemophilia B patients, byreducing the frequency of injections, achieving a highertrough level, and improving the quality of life of thepatients. In addition, subcutaneous administration ofalternative therapeutics would simplify prophylaxis inpatients with hemophilia A and B with and without inhi-bitors. Regarding von Willebrand disease, a recombinantvon Willebrand factor was recently developed to controlbleeding episodes in patients with this disease, in additionto available von Willebrand factor/factor VIII concen-trates. The management of patients affected by rare bleed-ing disorders (RBDs) is still a challenge, owing to thelimited number of specific products, which are mainlyavailable only in countries with high resources. Someimprovements have recently been achieved by the produc-tion of new recombinant factor (F) XIII A subunit-derived and FX plasma-derived products for the treatmentof patients affected by FXIII and FX deficiency. In addi-tion, the development of novel alternative therapeutics,such as anti-tissue factor pathway inhibitor, ALN-AT3,and ACE910, for patients with hemophilia might alsohave a role in the treatment of patients affected by RBDs.
Keywords: disease management; hemophilia; inheritedblood coagulation disorders; innovative therapy; vonWillebrand disease.
Introduction
Rare diseases are life-threatening or chronically debilitat-ing diseases with a prevalence of less than one per 2000according to the European Union or one per 1250according to the USA [1]. Only a few of the 5000 recog-nized rare diseases have a prevalence approaching thoselimits, with the remaining majority being even less com-mon, such as inherited deficiencies of plasma proteinsinvolved in blood coagulation. Hemophilia A and B arethe most recognized and common hereditary hemorrhagicdisorders caused by deficiency or dysfunction of bloodcoagulation factor (F) VIII or FIX, with prevalence ratesof approximately one in 5000 and one in 30 000 male livebirths, respectively. Together with von Willebrand disease(VWD), a defect of primary hemostasis with a prevalenceranging from 1% to one in 10 000, these disorders consti-tute 95–97% of all inherited deficiencies of coagulationfactors [2,3]. Rare bleeding disorders (RBDs), includingdeficiency of fibrinogen, FII, FV, combined FV + FVIII,FVII, FX, FXI, and FXIII, represent 3–5% of allinherited coagulation disorders, with prevalence rates ofthe presumably homozygous forms or compoundheterozygous forms in the general population rangingfrom approximately one in 2 million for FII and FXIIIdeficiencies to one in 500 000 for FVII deficiency [4].The most recent annual global survey of the WorldFederation of Hemophilia reports that > 287 000 peopleare affected by a coagulation disorder across 106 coun-tries in the world, with 62.2% having hemophilia A or B,24.3% having VWD, and 13.5% having other bleedingdisorders [5].
Bleeding episodes can occur either spontaneously, or atthe time of trauma, or invasive procedures and surgery[2–4]. Management decisions and the choice of therapycommonly rely on type of clotting factor deficiency, sever-ity of disease, type of bleeding episode, and minimalresidual activity in the patient’s plasma.
Correspondence: Flora Peyvandi, Angelo Bianchi Bonomi
Hemophilia and Thrombosis Center, Fondazione IRCCS C!a Granda
Ospedale Maggiore Policlinico, Department of Pathophysiology and
Transplantation, University of Milan, Via Pace, 9-20122, Milan,
Italy.
Tel.: +39 025 503 8491; fax: +39 025 410 0125.
E-mail: [email protected]
Received 29 June 2016
Manuscript handled by: P. H. Reitsma
Final decision: P. H. Reitsma, 15 August 2016
© 2016 International Society on Thrombosis and Haemostasis
Journal of Thrombosis and Haemostasis, 14: 2095–2106 DOI: 10.1111/jth.13491
REVIEW ARTICLE
Advances in the treatment of bleeding disordersF . PEYVANDI ,*† I . GARAGIOLA† and E . B IGUZZ I**Angelo Bianchi Bonomi Hemophilia and Thrombosis Center, Fondazione IRCCS Ca’ Granda Ospedale Maggiore Policlinico, Luigi Villa
Foundation; and †Department of Pathophysiology and Transplantation, Universit!a degli Studi di Milano, Milan, Italy
To cite this article: Peyvandi F, Garagiola I, Biguzzi E. Advances in the treatment of bleeding disorders. J Thromb Haemost 2016;
14: 2095–106.
Summary. Historically, the bleeding episodes in subjectswith coagulation disorders were treated with substitutiontherapy, initially with whole blood and fresh frozenplasma, and more recently with specific factor concen-trate. Currently, patients with hemophilia have the possi-bility of choosing different effective and safe treatments,including novel extended half-life and alternative hemo-static drugs. The availability of novel extended half-lifeproducts could probably overcome current prophylaxislimitations, particularly in hemophilia B patients, byreducing the frequency of injections, achieving a highertrough level, and improving the quality of life of thepatients. In addition, subcutaneous administration ofalternative therapeutics would simplify prophylaxis inpatients with hemophilia A and B with and without inhi-bitors. Regarding von Willebrand disease, a recombinantvon Willebrand factor was recently developed to controlbleeding episodes in patients with this disease, in additionto available von Willebrand factor/factor VIII concen-trates. The management of patients affected by rare bleed-ing disorders (RBDs) is still a challenge, owing to thelimited number of specific products, which are mainlyavailable only in countries with high resources. Someimprovements have recently been achieved by the produc-tion of new recombinant factor (F) XIII A subunit-derived and FX plasma-derived products for the treatmentof patients affected by FXIII and FX deficiency. In addi-tion, the development of novel alternative therapeutics,such as anti-tissue factor pathway inhibitor, ALN-AT3,and ACE910, for patients with hemophilia might alsohave a role in the treatment of patients affected by RBDs.
Keywords: disease management; hemophilia; inheritedblood coagulation disorders; innovative therapy; vonWillebrand disease.
Introduction
Rare diseases are life-threatening or chronically debilitat-ing diseases with a prevalence of less than one per 2000according to the European Union or one per 1250according to the USA [1]. Only a few of the 5000 recog-nized rare diseases have a prevalence approaching thoselimits, with the remaining majority being even less com-mon, such as inherited deficiencies of plasma proteinsinvolved in blood coagulation. Hemophilia A and B arethe most recognized and common hereditary hemorrhagicdisorders caused by deficiency or dysfunction of bloodcoagulation factor (F) VIII or FIX, with prevalence ratesof approximately one in 5000 and one in 30 000 male livebirths, respectively. Together with von Willebrand disease(VWD), a defect of primary hemostasis with a prevalenceranging from 1% to one in 10 000, these disorders consti-tute 95–97% of all inherited deficiencies of coagulationfactors [2,3]. Rare bleeding disorders (RBDs), includingdeficiency of fibrinogen, FII, FV, combined FV + FVIII,FVII, FX, FXI, and FXIII, represent 3–5% of allinherited coagulation disorders, with prevalence rates ofthe presumably homozygous forms or compoundheterozygous forms in the general population rangingfrom approximately one in 2 million for FII and FXIIIdeficiencies to one in 500 000 for FVII deficiency [4].The most recent annual global survey of the WorldFederation of Hemophilia reports that > 287 000 peopleare affected by a coagulation disorder across 106 coun-tries in the world, with 62.2% having hemophilia A or B,24.3% having VWD, and 13.5% having other bleedingdisorders [5].
Bleeding episodes can occur either spontaneously, or atthe time of trauma, or invasive procedures and surgery[2–4]. Management decisions and the choice of therapycommonly rely on type of clotting factor deficiency, sever-ity of disease, type of bleeding episode, and minimalresidual activity in the patient’s plasma.
Correspondence: Flora Peyvandi, Angelo Bianchi Bonomi
Hemophilia and Thrombosis Center, Fondazione IRCCS C!a Granda
Ospedale Maggiore Policlinico, Department of Pathophysiology and
Transplantation, University of Milan, Via Pace, 9-20122, Milan,
Italy.
Tel.: +39 025 503 8491; fax: +39 025 410 0125.
E-mail: [email protected]
Received 29 June 2016
Manuscript handled by: P. H. Reitsma
Final decision: P. H. Reitsma, 15 August 2016
© 2016 International Society on Thrombosis and Haemostasis
Journal of Thrombosis and Haemostasis, 14: 2095–2106 DOI: 10.1111/jth.13491
Table1Ne
wtherapeu
ticagents
forhemop
hiliaAan
dB
Deficiency
Product
Technolog
yMean
t 1/2(h)
(minimum
–maximum
)Clearance
(mLh!1 kg!1 )Estim
atedtime
to1%after
doseof50
lUkg!1
(days)
Clinicaltr
ialsRefer
ences
Hemophil
iaABAY
94-9027
Site-specifi
cPEGyla
tion(60-
kDaPEG
)18.4
(13.7–28.1
)1.4
5Phas
eIII(NCT
01580293)
[13]
N8-GP
Site-specifi
cglycoPE
Gylation
(40-kDaP
EG)19(1
1.6–27.3)
1.46.5
PhaseIII
(NCT01480
180)[14]
Adynovate (BAX855)
Controlled
PEGylatio
n(29
20-kDaPE
G)14.3–
16.02.47
4Appr
ovedbyth
eFDAin
2015[15]
Eloctate;E
locta(rFV
III–Fc)
Fcfusion
18.8(14.3
–24.5)
24.9
Approved
bytheFD
Ain2014
Approved
bytheEM
Ain2015
[16]
rVIII-Sing
leChain
(CSL627)
Single-cha
inrFVIII
14.52.64
NAPhas
eII/III(N
CT0148692
7)[18]
Hemophil
iaBN9-G
PSite-d
irectedgly
coPEGyla
tion(40-k
DaPEG)
93(85–111
)0.7
22Phas
eIII(NCT
01333111)
[19]
Alprolix(r
FIX–Fc)
Fcfusion
82.1(71.4
–94.5)
3.211.2
Approved
bytheFD
Ain2014
[20]Idelv
ion(rFIX
-FP)Albu
minfusion
91.570.75
14Appr
ovedbyth
eFDAin
2016Appr
ovedbyth
eEMAin
2016[24]
Hemophil
icpatients
withinhib
itorsrFVI
Ia-FP (CSL689)
Albuminf
usion8.5
NANA
PhaseII/I
II(NCT02
484638)
[38]
rFVIIa–CT
P(MO
D-5014)
CTPfusio
nThre
e-fold tofour-fo
ld*NA
NAPhas
eII/IIa(N
CT0241879
3)[40]
CTP,carbo
xyltermin
alpeptide
;EMA,E
uropeanM
edicinesA
gency;FD
A,USFo
odandD
rugAdmin
istration;
NA,data
notavaila
ble;PEG,
polyethyle
neglycol;
rFIX,reco
mbinantf
ac-torI
X;rFVIIa,
recombinan
tactivated
factorVII
;rFVIII,r
ecombinan
tfactorV
III.*Thes
tudyshow
sonlythe
increasein
half-lifeof
thedrug.
© 2016 International Society on Thrombosis and Haemostasis
Treatment of bleeding disorders 2097

REVIEW ARTICLE
Advances in the treatment of bleeding disordersF . PEYVANDI ,*† I . GARAGIOLA† and E . B IGUZZ I**Angelo Bianchi Bonomi Hemophilia and Thrombosis Center, Fondazione IRCCS Ca’ Granda Ospedale Maggiore Policlinico, Luigi Villa
Foundation; and †Department of Pathophysiology and Transplantation, Universit!a degli Studi di Milano, Milan, Italy
To cite this article: Peyvandi F, Garagiola I, Biguzzi E. Advances in the treatment of bleeding disorders. J Thromb Haemost 2016;
14: 2095–106.
Summary. Historically, the bleeding episodes in subjectswith coagulation disorders were treated with substitutiontherapy, initially with whole blood and fresh frozenplasma, and more recently with specific factor concen-trate. Currently, patients with hemophilia have the possi-bility of choosing different effective and safe treatments,including novel extended half-life and alternative hemo-static drugs. The availability of novel extended half-lifeproducts could probably overcome current prophylaxislimitations, particularly in hemophilia B patients, byreducing the frequency of injections, achieving a highertrough level, and improving the quality of life of thepatients. In addition, subcutaneous administration ofalternative therapeutics would simplify prophylaxis inpatients with hemophilia A and B with and without inhi-bitors. Regarding von Willebrand disease, a recombinantvon Willebrand factor was recently developed to controlbleeding episodes in patients with this disease, in additionto available von Willebrand factor/factor VIII concen-trates. The management of patients affected by rare bleed-ing disorders (RBDs) is still a challenge, owing to thelimited number of specific products, which are mainlyavailable only in countries with high resources. Someimprovements have recently been achieved by the produc-tion of new recombinant factor (F) XIII A subunit-derived and FX plasma-derived products for the treatmentof patients affected by FXIII and FX deficiency. In addi-tion, the development of novel alternative therapeutics,such as anti-tissue factor pathway inhibitor, ALN-AT3,and ACE910, for patients with hemophilia might alsohave a role in the treatment of patients affected by RBDs.
Keywords: disease management; hemophilia; inheritedblood coagulation disorders; innovative therapy; vonWillebrand disease.
Introduction
Rare diseases are life-threatening or chronically debilitat-ing diseases with a prevalence of less than one per 2000according to the European Union or one per 1250according to the USA [1]. Only a few of the 5000 recog-nized rare diseases have a prevalence approaching thoselimits, with the remaining majority being even less com-mon, such as inherited deficiencies of plasma proteinsinvolved in blood coagulation. Hemophilia A and B arethe most recognized and common hereditary hemorrhagicdisorders caused by deficiency or dysfunction of bloodcoagulation factor (F) VIII or FIX, with prevalence ratesof approximately one in 5000 and one in 30 000 male livebirths, respectively. Together with von Willebrand disease(VWD), a defect of primary hemostasis with a prevalenceranging from 1% to one in 10 000, these disorders consti-tute 95–97% of all inherited deficiencies of coagulationfactors [2,3]. Rare bleeding disorders (RBDs), includingdeficiency of fibrinogen, FII, FV, combined FV + FVIII,FVII, FX, FXI, and FXIII, represent 3–5% of allinherited coagulation disorders, with prevalence rates ofthe presumably homozygous forms or compoundheterozygous forms in the general population rangingfrom approximately one in 2 million for FII and FXIIIdeficiencies to one in 500 000 for FVII deficiency [4].The most recent annual global survey of the WorldFederation of Hemophilia reports that > 287 000 peopleare affected by a coagulation disorder across 106 coun-tries in the world, with 62.2% having hemophilia A or B,24.3% having VWD, and 13.5% having other bleedingdisorders [5].
Bleeding episodes can occur either spontaneously, or atthe time of trauma, or invasive procedures and surgery[2–4]. Management decisions and the choice of therapycommonly rely on type of clotting factor deficiency, sever-ity of disease, type of bleeding episode, and minimalresidual activity in the patient’s plasma.
Correspondence: Flora Peyvandi, Angelo Bianchi Bonomi
Hemophilia and Thrombosis Center, Fondazione IRCCS C!a Granda
Ospedale Maggiore Policlinico, Department of Pathophysiology and
Transplantation, University of Milan, Via Pace, 9-20122, Milan,
Italy.
Tel.: +39 025 503 8491; fax: +39 025 410 0125.
E-mail: [email protected]
Received 29 June 2016
Manuscript handled by: P. H. Reitsma
Final decision: P. H. Reitsma, 15 August 2016
© 2016 International Society on Thrombosis and Haemostasis
Journal of Thrombosis and Haemostasis, 14: 2095–2106 DOI: 10.1111/jth.13491
REVIEW ARTICLE
Advances in the treatment of bleeding disordersF . PEYVANDI ,*† I . GARAGIOLA† and E . B IGUZZ I**Angelo Bianchi Bonomi Hemophilia and Thrombosis Center, Fondazione IRCCS Ca’ Granda Ospedale Maggiore Policlinico, Luigi Villa
Foundation; and †Department of Pathophysiology and Transplantation, Universit!a degli Studi di Milano, Milan, Italy
To cite this article: Peyvandi F, Garagiola I, Biguzzi E. Advances in the treatment of bleeding disorders. J Thromb Haemost 2016;
14: 2095–106.
Summary. Historically, the bleeding episodes in subjectswith coagulation disorders were treated with substitutiontherapy, initially with whole blood and fresh frozenplasma, and more recently with specific factor concen-trate. Currently, patients with hemophilia have the possi-bility of choosing different effective and safe treatments,including novel extended half-life and alternative hemo-static drugs. The availability of novel extended half-lifeproducts could probably overcome current prophylaxislimitations, particularly in hemophilia B patients, byreducing the frequency of injections, achieving a highertrough level, and improving the quality of life of thepatients. In addition, subcutaneous administration ofalternative therapeutics would simplify prophylaxis inpatients with hemophilia A and B with and without inhi-bitors. Regarding von Willebrand disease, a recombinantvon Willebrand factor was recently developed to controlbleeding episodes in patients with this disease, in additionto available von Willebrand factor/factor VIII concen-trates. The management of patients affected by rare bleed-ing disorders (RBDs) is still a challenge, owing to thelimited number of specific products, which are mainlyavailable only in countries with high resources. Someimprovements have recently been achieved by the produc-tion of new recombinant factor (F) XIII A subunit-derived and FX plasma-derived products for the treatmentof patients affected by FXIII and FX deficiency. In addi-tion, the development of novel alternative therapeutics,such as anti-tissue factor pathway inhibitor, ALN-AT3,and ACE910, for patients with hemophilia might alsohave a role in the treatment of patients affected by RBDs.
Keywords: disease management; hemophilia; inheritedblood coagulation disorders; innovative therapy; vonWillebrand disease.
Introduction
Rare diseases are life-threatening or chronically debilitat-ing diseases with a prevalence of less than one per 2000according to the European Union or one per 1250according to the USA [1]. Only a few of the 5000 recog-nized rare diseases have a prevalence approaching thoselimits, with the remaining majority being even less com-mon, such as inherited deficiencies of plasma proteinsinvolved in blood coagulation. Hemophilia A and B arethe most recognized and common hereditary hemorrhagicdisorders caused by deficiency or dysfunction of bloodcoagulation factor (F) VIII or FIX, with prevalence ratesof approximately one in 5000 and one in 30 000 male livebirths, respectively. Together with von Willebrand disease(VWD), a defect of primary hemostasis with a prevalenceranging from 1% to one in 10 000, these disorders consti-tute 95–97% of all inherited deficiencies of coagulationfactors [2,3]. Rare bleeding disorders (RBDs), includingdeficiency of fibrinogen, FII, FV, combined FV + FVIII,FVII, FX, FXI, and FXIII, represent 3–5% of allinherited coagulation disorders, with prevalence rates ofthe presumably homozygous forms or compoundheterozygous forms in the general population rangingfrom approximately one in 2 million for FII and FXIIIdeficiencies to one in 500 000 for FVII deficiency [4].The most recent annual global survey of the WorldFederation of Hemophilia reports that > 287 000 peopleare affected by a coagulation disorder across 106 coun-tries in the world, with 62.2% having hemophilia A or B,24.3% having VWD, and 13.5% having other bleedingdisorders [5].
Bleeding episodes can occur either spontaneously, or atthe time of trauma, or invasive procedures and surgery[2–4]. Management decisions and the choice of therapycommonly rely on type of clotting factor deficiency, sever-ity of disease, type of bleeding episode, and minimalresidual activity in the patient’s plasma.
Correspondence: Flora Peyvandi, Angelo Bianchi Bonomi
Hemophilia and Thrombosis Center, Fondazione IRCCS C!a Granda
Ospedale Maggiore Policlinico, Department of Pathophysiology and
Transplantation, University of Milan, Via Pace, 9-20122, Milan,
Italy.
Tel.: +39 025 503 8491; fax: +39 025 410 0125.
E-mail: [email protected]
Received 29 June 2016
Manuscript handled by: P. H. Reitsma
Final decision: P. H. Reitsma, 15 August 2016
© 2016 International Society on Thrombosis and Haemostasis
Journal of Thrombosis and Haemostasis, 14: 2095–2106 DOI: 10.1111/jth.13491
REVIEW ARTICLE
Advances in the treatment of bleeding disordersF . PEYVANDI ,*† I . GARAGIOLA† and E . B IGUZZ I**Angelo Bianchi Bonomi Hemophilia and Thrombosis Center, Fondazione IRCCS Ca’ Granda Ospedale Maggiore Policlinico, Luigi Villa
Foundation; and †Department of Pathophysiology and Transplantation, Universit!a degli Studi di Milano, Milan, Italy
To cite this article: Peyvandi F, Garagiola I, Biguzzi E. Advances in the treatment of bleeding disorders. J Thromb Haemost 2016;
14: 2095–106.
Summary. Historically, the bleeding episodes in subjectswith coagulation disorders were treated with substitutiontherapy, initially with whole blood and fresh frozenplasma, and more recently with specific factor concen-trate. Currently, patients with hemophilia have the possi-bility of choosing different effective and safe treatments,including novel extended half-life and alternative hemo-static drugs. The availability of novel extended half-lifeproducts could probably overcome current prophylaxislimitations, particularly in hemophilia B patients, byreducing the frequency of injections, achieving a highertrough level, and improving the quality of life of thepatients. In addition, subcutaneous administration ofalternative therapeutics would simplify prophylaxis inpatients with hemophilia A and B with and without inhi-bitors. Regarding von Willebrand disease, a recombinantvon Willebrand factor was recently developed to controlbleeding episodes in patients with this disease, in additionto available von Willebrand factor/factor VIII concen-trates. The management of patients affected by rare bleed-ing disorders (RBDs) is still a challenge, owing to thelimited number of specific products, which are mainlyavailable only in countries with high resources. Someimprovements have recently been achieved by the produc-tion of new recombinant factor (F) XIII A subunit-derived and FX plasma-derived products for the treatmentof patients affected by FXIII and FX deficiency. In addi-tion, the development of novel alternative therapeutics,such as anti-tissue factor pathway inhibitor, ALN-AT3,and ACE910, for patients with hemophilia might alsohave a role in the treatment of patients affected by RBDs.
Keywords: disease management; hemophilia; inheritedblood coagulation disorders; innovative therapy; vonWillebrand disease.
Introduction
Rare diseases are life-threatening or chronically debilitat-ing diseases with a prevalence of less than one per 2000according to the European Union or one per 1250according to the USA [1]. Only a few of the 5000 recog-nized rare diseases have a prevalence approaching thoselimits, with the remaining majority being even less com-mon, such as inherited deficiencies of plasma proteinsinvolved in blood coagulation. Hemophilia A and B arethe most recognized and common hereditary hemorrhagicdisorders caused by deficiency or dysfunction of bloodcoagulation factor (F) VIII or FIX, with prevalence ratesof approximately one in 5000 and one in 30 000 male livebirths, respectively. Together with von Willebrand disease(VWD), a defect of primary hemostasis with a prevalenceranging from 1% to one in 10 000, these disorders consti-tute 95–97% of all inherited deficiencies of coagulationfactors [2,3]. Rare bleeding disorders (RBDs), includingdeficiency of fibrinogen, FII, FV, combined FV + FVIII,FVII, FX, FXI, and FXIII, represent 3–5% of allinherited coagulation disorders, with prevalence rates ofthe presumably homozygous forms or compoundheterozygous forms in the general population rangingfrom approximately one in 2 million for FII and FXIIIdeficiencies to one in 500 000 for FVII deficiency [4].The most recent annual global survey of the WorldFederation of Hemophilia reports that > 287 000 peopleare affected by a coagulation disorder across 106 coun-tries in the world, with 62.2% having hemophilia A or B,24.3% having VWD, and 13.5% having other bleedingdisorders [5].
Bleeding episodes can occur either spontaneously, or atthe time of trauma, or invasive procedures and surgery[2–4]. Management decisions and the choice of therapycommonly rely on type of clotting factor deficiency, sever-ity of disease, type of bleeding episode, and minimalresidual activity in the patient’s plasma.
Correspondence: Flora Peyvandi, Angelo Bianchi Bonomi
Hemophilia and Thrombosis Center, Fondazione IRCCS C!a Granda
Ospedale Maggiore Policlinico, Department of Pathophysiology and
Transplantation, University of Milan, Via Pace, 9-20122, Milan,
Italy.
Tel.: +39 025 503 8491; fax: +39 025 410 0125.
E-mail: [email protected]
Received 29 June 2016
Manuscript handled by: P. H. Reitsma
Final decision: P. H. Reitsma, 15 August 2016
© 2016 International Society on Thrombosis and Haemostasis
Journal of Thrombosis and Haemostasis, 14: 2095–2106 DOI: 10.1111/jth.13491
remarkably longer than the standard rFIX half-life. Thetimes needed to reach 1% of FIX activity were 22 daysand 11.2 days, respectively, for N9-GP and rFIX–Fc(Table 1) [19–21].
In 2014, the FDA approved the first bioengineeredrFIX with an EHL, produced with the Fc-fusion technol-ogy (Alprolix), to treat bleeding in hemophilia B patients.
The albumin fusion technology has also been investi-gated as a method of half-life prolongation for rFIX.Albumin is the most abundant protein found in humanplasma, and has a naturally long half-life of ~ 3 weeks. Anovel recombinant fusion protein linking FIX with albu-min (rFIX-FP, Idelvion) showed a five-fold improvement,with a half-life of 92 h (Table 1) [22]. rIX-FP has alsoshown a marked improvement in pharmacokinetic profileover currently marketed FIX products [23]. Data fromthe phase III study indicate that rIX-FP is safe and effec-tive for preventing and treating bleeding episodes inpatients with hemophilia B at dosing regimens of40 IU kg!1 weekly and 75 IU kg!1 every 2 weeks [24].At the beginning of 2016, the FDA approved Idelvion forthe treatment of hemophilia B patients, and, morerecently, the EMA also approved it.
Clinical implications (acute bleeding, prophylaxis, and
surgery)
In the on-demand setting, the efficacy of the new EHLcoagulation products seems to be comparable to that ofstandard coagulation factors, and the impact of EHLrFVIII is less remarkable than that of EHL rFIX productsin the management of acute bleeding (e.g. the increase indosing interval). More data are required in order todevelop accurate and evidence-based conclusions. Table 2shows doses and frequencies of treatment for the controlof acute bleeding in patients with hemophilia A and B.
Starting from pharmacokinetic and data from phase IIIclinical trials, a prophylactic regimen with EHL rFVIIIproducts may be considered, with dosing of 25–65 IU kg!1 at 3–5-day intervals maintaining a safe trough
level [25]. More frequent or higher doses may be requiredin children aged < 6 years because of increased clearance,as for standard concentrates.
The extension of the half-life of rFVIII leads to a 30–35% reduction in the frequency of injections. In particu-lar, in a patient affected with severe hemophilia A whoreceives two or three injections weekly of a standardFVIII concentrates (156–182 infusions per year), injec-tions with newer EHL drugs might be reduced to twiceweekly (102 per year) or one every 3 days or 5 days[26,27]. This prophylactic schedule would probably main-tain a higher trough level with a lower risk of bleeding.
For hemophilia B treatment, 50 IU kg!1 weekly or100 IU kg!1 every 12–14 days of EHL rFIX agents canachieve a safe trough level in absence of bleeding events[28]. The good performance of EHL rFIX products couldconsiderably simplify the prophylactic regimens ofhemophilia B patients. For instance, in patients affectedwith severe hemophilia B receiving two injections perweek (104 injections per year) of standard FIX concen-trates, the use of EHL concentrates could allow the num-ber of injections to be reduced to once every 1–3 weeks(18–52 injections per year) [26,27]. Therefore, the fre-quency of injections will be reduced by 50% with a factortrough level being maintained well above 1%, making thistherapy less distressing to the patient and improvingadherence to treatment. A higher trough level could alsobe achieved in adolescent patients with an active life, withreduction of the intervals to once weekly.
One aim of using the EHL products could be toachieve a higher trough level with an almost similar or aslightly reduced number of injections for hemophilia Apatients, and a significant decrease in the number of injec-tions, with presumably a higher trough level, forhemophilia B patients. The real benefit of the use of EHLproducts should be monitored by careful long-term obser-vation, and treatment options and schedules could alsobe individualized.
Subjects undergoing surgery should be treated accord-ing to the type of procedure, with doses expected to
Table 2 Dose and frequency of treatment for the control of acute bleeding in patients with hemophilia A and B [16,20,29]
Type of bleeding
Dose (IU kg!1) Frequency of dosing (h)
rFVIII standard rFVIII EHL rFVIII standard rFVIII EHL
Minor/moderate 20–30 20–30 12–24 24–48Major (life-threatening hemorrhages) 40–50 40–50 8–24 12–24
Type of bleeding
Dose (IU kg!1) Frequency of dosing (h)
rFIX standard rFIX EHL rFIX standard rFIX EHL
Minor/moderate 40–60 30–60 12–24 48Major (life-threatening hemorrhages) 60–80 80–100 12 to 24 24 for the first 3 days,
and then every 48
EHL, extended half-life; rFIX, recombinant factor IX; rFVIII, recombinant factor VIII.
© 2016 International Society on Thrombosis and Haemostasis
2098 F. Peyvandi et al

REVIEW ARTICLE
Advances in the treatment of bleeding disordersF . PEYVANDI ,*† I . GARAGIOLA† and E . B IGUZZ I**Angelo Bianchi Bonomi Hemophilia and Thrombosis Center, Fondazione IRCCS Ca’ Granda Ospedale Maggiore Policlinico, Luigi Villa
Foundation; and †Department of Pathophysiology and Transplantation, Universit!a degli Studi di Milano, Milan, Italy
To cite this article: Peyvandi F, Garagiola I, Biguzzi E. Advances in the treatment of bleeding disorders. J Thromb Haemost 2016;
14: 2095–106.
Summary. Historically, the bleeding episodes in subjectswith coagulation disorders were treated with substitutiontherapy, initially with whole blood and fresh frozenplasma, and more recently with specific factor concen-trate. Currently, patients with hemophilia have the possi-bility of choosing different effective and safe treatments,including novel extended half-life and alternative hemo-static drugs. The availability of novel extended half-lifeproducts could probably overcome current prophylaxislimitations, particularly in hemophilia B patients, byreducing the frequency of injections, achieving a highertrough level, and improving the quality of life of thepatients. In addition, subcutaneous administration ofalternative therapeutics would simplify prophylaxis inpatients with hemophilia A and B with and without inhi-bitors. Regarding von Willebrand disease, a recombinantvon Willebrand factor was recently developed to controlbleeding episodes in patients with this disease, in additionto available von Willebrand factor/factor VIII concen-trates. The management of patients affected by rare bleed-ing disorders (RBDs) is still a challenge, owing to thelimited number of specific products, which are mainlyavailable only in countries with high resources. Someimprovements have recently been achieved by the produc-tion of new recombinant factor (F) XIII A subunit-derived and FX plasma-derived products for the treatmentof patients affected by FXIII and FX deficiency. In addi-tion, the development of novel alternative therapeutics,such as anti-tissue factor pathway inhibitor, ALN-AT3,and ACE910, for patients with hemophilia might alsohave a role in the treatment of patients affected by RBDs.
Keywords: disease management; hemophilia; inheritedblood coagulation disorders; innovative therapy; vonWillebrand disease.
Introduction
Rare diseases are life-threatening or chronically debilitat-ing diseases with a prevalence of less than one per 2000according to the European Union or one per 1250according to the USA [1]. Only a few of the 5000 recog-nized rare diseases have a prevalence approaching thoselimits, with the remaining majority being even less com-mon, such as inherited deficiencies of plasma proteinsinvolved in blood coagulation. Hemophilia A and B arethe most recognized and common hereditary hemorrhagicdisorders caused by deficiency or dysfunction of bloodcoagulation factor (F) VIII or FIX, with prevalence ratesof approximately one in 5000 and one in 30 000 male livebirths, respectively. Together with von Willebrand disease(VWD), a defect of primary hemostasis with a prevalenceranging from 1% to one in 10 000, these disorders consti-tute 95–97% of all inherited deficiencies of coagulationfactors [2,3]. Rare bleeding disorders (RBDs), includingdeficiency of fibrinogen, FII, FV, combined FV + FVIII,FVII, FX, FXI, and FXIII, represent 3–5% of allinherited coagulation disorders, with prevalence rates ofthe presumably homozygous forms or compoundheterozygous forms in the general population rangingfrom approximately one in 2 million for FII and FXIIIdeficiencies to one in 500 000 for FVII deficiency [4].The most recent annual global survey of the WorldFederation of Hemophilia reports that > 287 000 peopleare affected by a coagulation disorder across 106 coun-tries in the world, with 62.2% having hemophilia A or B,24.3% having VWD, and 13.5% having other bleedingdisorders [5].
Bleeding episodes can occur either spontaneously, or atthe time of trauma, or invasive procedures and surgery[2–4]. Management decisions and the choice of therapycommonly rely on type of clotting factor deficiency, sever-ity of disease, type of bleeding episode, and minimalresidual activity in the patient’s plasma.
Correspondence: Flora Peyvandi, Angelo Bianchi Bonomi
Hemophilia and Thrombosis Center, Fondazione IRCCS C!a Granda
Ospedale Maggiore Policlinico, Department of Pathophysiology and
Transplantation, University of Milan, Via Pace, 9-20122, Milan,
Italy.
Tel.: +39 025 503 8491; fax: +39 025 410 0125.
E-mail: [email protected]
Received 29 June 2016
Manuscript handled by: P. H. Reitsma
Final decision: P. H. Reitsma, 15 August 2016
© 2016 International Society on Thrombosis and Haemostasis
Journal of Thrombosis and Haemostasis, 14: 2095–2106 DOI: 10.1111/jth.13491
REVIEW ARTICLE
Advances in the treatment of bleeding disordersF . PEYVANDI ,*† I . GARAGIOLA† and E . B IGUZZ I**Angelo Bianchi Bonomi Hemophilia and Thrombosis Center, Fondazione IRCCS Ca’ Granda Ospedale Maggiore Policlinico, Luigi Villa
Foundation; and †Department of Pathophysiology and Transplantation, Universit!a degli Studi di Milano, Milan, Italy
To cite this article: Peyvandi F, Garagiola I, Biguzzi E. Advances in the treatment of bleeding disorders. J Thromb Haemost 2016;
14: 2095–106.
Summary. Historically, the bleeding episodes in subjectswith coagulation disorders were treated with substitutiontherapy, initially with whole blood and fresh frozenplasma, and more recently with specific factor concen-trate. Currently, patients with hemophilia have the possi-bility of choosing different effective and safe treatments,including novel extended half-life and alternative hemo-static drugs. The availability of novel extended half-lifeproducts could probably overcome current prophylaxislimitations, particularly in hemophilia B patients, byreducing the frequency of injections, achieving a highertrough level, and improving the quality of life of thepatients. In addition, subcutaneous administration ofalternative therapeutics would simplify prophylaxis inpatients with hemophilia A and B with and without inhi-bitors. Regarding von Willebrand disease, a recombinantvon Willebrand factor was recently developed to controlbleeding episodes in patients with this disease, in additionto available von Willebrand factor/factor VIII concen-trates. The management of patients affected by rare bleed-ing disorders (RBDs) is still a challenge, owing to thelimited number of specific products, which are mainlyavailable only in countries with high resources. Someimprovements have recently been achieved by the produc-tion of new recombinant factor (F) XIII A subunit-derived and FX plasma-derived products for the treatmentof patients affected by FXIII and FX deficiency. In addi-tion, the development of novel alternative therapeutics,such as anti-tissue factor pathway inhibitor, ALN-AT3,and ACE910, for patients with hemophilia might alsohave a role in the treatment of patients affected by RBDs.
Keywords: disease management; hemophilia; inheritedblood coagulation disorders; innovative therapy; vonWillebrand disease.
Introduction
Rare diseases are life-threatening or chronically debilitat-ing diseases with a prevalence of less than one per 2000according to the European Union or one per 1250according to the USA [1]. Only a few of the 5000 recog-nized rare diseases have a prevalence approaching thoselimits, with the remaining majority being even less com-mon, such as inherited deficiencies of plasma proteinsinvolved in blood coagulation. Hemophilia A and B arethe most recognized and common hereditary hemorrhagicdisorders caused by deficiency or dysfunction of bloodcoagulation factor (F) VIII or FIX, with prevalence ratesof approximately one in 5000 and one in 30 000 male livebirths, respectively. Together with von Willebrand disease(VWD), a defect of primary hemostasis with a prevalenceranging from 1% to one in 10 000, these disorders consti-tute 95–97% of all inherited deficiencies of coagulationfactors [2,3]. Rare bleeding disorders (RBDs), includingdeficiency of fibrinogen, FII, FV, combined FV + FVIII,FVII, FX, FXI, and FXIII, represent 3–5% of allinherited coagulation disorders, with prevalence rates ofthe presumably homozygous forms or compoundheterozygous forms in the general population rangingfrom approximately one in 2 million for FII and FXIIIdeficiencies to one in 500 000 for FVII deficiency [4].The most recent annual global survey of the WorldFederation of Hemophilia reports that > 287 000 peopleare affected by a coagulation disorder across 106 coun-tries in the world, with 62.2% having hemophilia A or B,24.3% having VWD, and 13.5% having other bleedingdisorders [5].
Bleeding episodes can occur either spontaneously, or atthe time of trauma, or invasive procedures and surgery[2–4]. Management decisions and the choice of therapycommonly rely on type of clotting factor deficiency, sever-ity of disease, type of bleeding episode, and minimalresidual activity in the patient’s plasma.
Correspondence: Flora Peyvandi, Angelo Bianchi Bonomi
Hemophilia and Thrombosis Center, Fondazione IRCCS C!a Granda
Ospedale Maggiore Policlinico, Department of Pathophysiology and
Transplantation, University of Milan, Via Pace, 9-20122, Milan,
Italy.
Tel.: +39 025 503 8491; fax: +39 025 410 0125.
E-mail: [email protected]
Received 29 June 2016
Manuscript handled by: P. H. Reitsma
Final decision: P. H. Reitsma, 15 August 2016
© 2016 International Society on Thrombosis and Haemostasis
Journal of Thrombosis and Haemostasis, 14: 2095–2106 DOI: 10.1111/jth.13491
REVIEW ARTICLE
Advances in the treatment of bleeding disordersF . PEYVANDI ,*† I . GARAGIOLA† and E . B IGUZZ I**Angelo Bianchi Bonomi Hemophilia and Thrombosis Center, Fondazione IRCCS Ca’ Granda Ospedale Maggiore Policlinico, Luigi Villa
Foundation; and †Department of Pathophysiology and Transplantation, Universit!a degli Studi di Milano, Milan, Italy
To cite this article: Peyvandi F, Garagiola I, Biguzzi E. Advances in the treatment of bleeding disorders. J Thromb Haemost 2016;
14: 2095–106.
Summary. Historically, the bleeding episodes in subjectswith coagulation disorders were treated with substitutiontherapy, initially with whole blood and fresh frozenplasma, and more recently with specific factor concen-trate. Currently, patients with hemophilia have the possi-bility of choosing different effective and safe treatments,including novel extended half-life and alternative hemo-static drugs. The availability of novel extended half-lifeproducts could probably overcome current prophylaxislimitations, particularly in hemophilia B patients, byreducing the frequency of injections, achieving a highertrough level, and improving the quality of life of thepatients. In addition, subcutaneous administration ofalternative therapeutics would simplify prophylaxis inpatients with hemophilia A and B with and without inhi-bitors. Regarding von Willebrand disease, a recombinantvon Willebrand factor was recently developed to controlbleeding episodes in patients with this disease, in additionto available von Willebrand factor/factor VIII concen-trates. The management of patients affected by rare bleed-ing disorders (RBDs) is still a challenge, owing to thelimited number of specific products, which are mainlyavailable only in countries with high resources. Someimprovements have recently been achieved by the produc-tion of new recombinant factor (F) XIII A subunit-derived and FX plasma-derived products for the treatmentof patients affected by FXIII and FX deficiency. In addi-tion, the development of novel alternative therapeutics,such as anti-tissue factor pathway inhibitor, ALN-AT3,and ACE910, for patients with hemophilia might alsohave a role in the treatment of patients affected by RBDs.
Keywords: disease management; hemophilia; inheritedblood coagulation disorders; innovative therapy; vonWillebrand disease.
Introduction
Rare diseases are life-threatening or chronically debilitat-ing diseases with a prevalence of less than one per 2000according to the European Union or one per 1250according to the USA [1]. Only a few of the 5000 recog-nized rare diseases have a prevalence approaching thoselimits, with the remaining majority being even less com-mon, such as inherited deficiencies of plasma proteinsinvolved in blood coagulation. Hemophilia A and B arethe most recognized and common hereditary hemorrhagicdisorders caused by deficiency or dysfunction of bloodcoagulation factor (F) VIII or FIX, with prevalence ratesof approximately one in 5000 and one in 30 000 male livebirths, respectively. Together with von Willebrand disease(VWD), a defect of primary hemostasis with a prevalenceranging from 1% to one in 10 000, these disorders consti-tute 95–97% of all inherited deficiencies of coagulationfactors [2,3]. Rare bleeding disorders (RBDs), includingdeficiency of fibrinogen, FII, FV, combined FV + FVIII,FVII, FX, FXI, and FXIII, represent 3–5% of allinherited coagulation disorders, with prevalence rates ofthe presumably homozygous forms or compoundheterozygous forms in the general population rangingfrom approximately one in 2 million for FII and FXIIIdeficiencies to one in 500 000 for FVII deficiency [4].The most recent annual global survey of the WorldFederation of Hemophilia reports that > 287 000 peopleare affected by a coagulation disorder across 106 coun-tries in the world, with 62.2% having hemophilia A or B,24.3% having VWD, and 13.5% having other bleedingdisorders [5].
Bleeding episodes can occur either spontaneously, or atthe time of trauma, or invasive procedures and surgery[2–4]. Management decisions and the choice of therapycommonly rely on type of clotting factor deficiency, sever-ity of disease, type of bleeding episode, and minimalresidual activity in the patient’s plasma.
Correspondence: Flora Peyvandi, Angelo Bianchi Bonomi
Hemophilia and Thrombosis Center, Fondazione IRCCS C!a Granda
Ospedale Maggiore Policlinico, Department of Pathophysiology and
Transplantation, University of Milan, Via Pace, 9-20122, Milan,
Italy.
Tel.: +39 025 503 8491; fax: +39 025 410 0125.
E-mail: [email protected]
Received 29 June 2016
Manuscript handled by: P. H. Reitsma
Final decision: P. H. Reitsma, 15 August 2016
© 2016 International Society on Thrombosis and Haemostasis
Journal of Thrombosis and Haemostasis, 14: 2095–2106 DOI: 10.1111/jth.13491
maintain acceptable therapeutic levels of FVIII or FIXactivity. Preoperative plasma levels of 60–80% for FIXand of 80–100% for FVIII are recommended for patientsundergoing major surgery, and 50–80% of FIX andFVIII for patients undergoing minor surgery [29]. Treat-ment should be continued in the postoperative period tomaintain similar recommended levels for standard rFVIIIand rFIX (approximately 30–60% for FIX and 40–80%for FVIII) for the following 1–3 days for minor surgeryand 10–14 days for major surgery. In all cases, the doseand frequency of infusion may be adapted to the type ofsurgical procedure, blood loss, and individual response totreatment. Each subject undergoing a surgical procedureshould undergo pharmacokinetic assessment, if this hasnot already been performed, and careful observationshould be ensured during the first 72 h for patients under-going major surgery and during the first 24 h for thoseundergoing minor surgery.
In the surgical setting, available data on EHL productsare limited to a few patients (23 with rFVIII–Fc and 15with BAX855) [30,31]. The hemostatic response duringthe perioperative period for these procedures was ratedby investigators/surgeons as excellent or good with bothproducts [30,31]. The dosing frequency adopted withrFVIII–Fc is similar to that of standard rFVIII, whichrequires a median total dose of 62.50 IU kg!1 on the dayof surgery and a median rFVIII–Fc dose per injection (in-cluding a loading dose) of 58.31 IU kg!1 (range 45–102 IU kg!1) for minor and major surgery (Table 3). Incontrast, rFIX–Fc allows a marked reduction in dosingfrequency for major surgical procedures, with an amountof rFIX–Fc less than that observed in historical studies ofstandard FIX products. The mean dose of rFIX–Fc onthe day of surgery (day 0) was 84.16 IU kg!1, the mean
dose on subsequent days (days 1–14) ranged from49.12 IU kg!1 to 64.61 IU kg!1, and no subject was trea-ted every day during the surgical period (days 0–14)(Table 4) [32]. In studies with the standard FIX products,subjects who underwent major surgical proceduresreceived continuous infusion with a mean doseof 154 IU kg!1 daily, and the average dose on the day ofsurgery was 254.9 IU kg!1, representing a combination ofcontinuous and bolus doses [33,34].
A surgical trial with N9-GP was also conducted in pre-viously treated hemophilia B patients. All patientsreceived a preoperative bolus injection of 80 IU kg!1,and subsequently a fixed dose of 40 IU kg!1 repeated atthe investigator’s discretion (Table 4) [35]. Again, periop-erative consumption and number of injections were lowerthan reported for any other FIX product [36]. A subanal-ysis of phase III trials showed that a single dose ofrIX-FP was sufficient to maintain hemostasis during theprocedures. The median rIX-FP consumption in fiveorthopedic surgical procedures was 87 IU kg!1 preopera-tively (day 0), 51 IU kg!1 postoperatively (days 1–2), and340 IU kg!1 overall (days 0–14), with a range of six toseven injections (Table 4) [37].
The EHL rFVIII products might have a small impacton dosing frequency during the first 48 h in the surgicalsetting. In contrast, EHL rFIX products enable a markedreduction in dosing frequency for major surgical proce-dures. Additional clinical experience is needed to make aclear recommendation.
Recombinant rFVIIa
The management of bleeding in hemophilic patients withinhibitors requires bypassing agent therapies, such as
Table 3 Dose and frequency for standard and extended half-life(EHL) products in the management of hemophilia A patients under-going minor and major surgical procedures
Dose(IU kg!1)
Frequency(h)
Durationof therapy(days) References
rFVIII standard productMinor 25–40 Every 12–24 1–3 [29]MajorPreoperative 40–50 A single-dose injectionPostoperative 30–40 Every 8–24 1–7 [29]
FVIII EHLMinor 62.50* Every 24 l [30]MajorPreoperativeandintraoperative
58.3† A single-dose injection
58.8‡ Every 24 7 [30]
rFVIII, recombinant factor VIII. *Median total dose required on theday of surgery (range 23.38–188.68 IU kg!1). †Median rFVIII EHLdose per injection. ‡Median total dose (including loading dose) of58.8 IU kg!1 with a range of 50–102 IU kg!1 during the preopera-tive and intraoperative periods.
Table 4 Dose and frequency for standard and extended half-life(EHL) products in the management of hemophilia B patients under-going minor and major surgery procedures
Dose(IU kg!1)
Frequency(h)
Durationof therapy(days) References
rFIX standard productMinor 50–80 Every 24 l [29]MajorPreoperative 60–80 A single-dose injection [29]Postoperative 40–60 Every 8–24 7 [29]
FIX EHLMinor 50–80 A single injection may be sufficient.
Repeat as needed after 24–48 hMajorPreoperative 84.16* A single-dose injection [32]
80 A single-dose injection [35]87† A single-dose injection [37]
Postoperative 49.12–64.61* 24–48 1–14 [32]40 24–96 13 [35]51 24–72 14 [37]
rFIX, recombinant factor IX. *Mean dose. †Median consumption.
© 2016 International Society on Thrombosis and Haemostasis
Treatment of bleeding disorders 2099
maintain acceptable therapeutic levels of FVIII or FIXactivity. Preoperative plasma levels of 60–80% for FIXand of 80–100% for FVIII are recommended for patientsundergoing major surgery, and 50–80% of FIX andFVIII for patients undergoing minor surgery [29]. Treat-ment should be continued in the postoperative period tomaintain similar recommended levels for standard rFVIIIand rFIX (approximately 30–60% for FIX and 40–80%for FVIII) for the following 1–3 days for minor surgeryand 10–14 days for major surgery. In all cases, the doseand frequency of infusion may be adapted to the type ofsurgical procedure, blood loss, and individual response totreatment. Each subject undergoing a surgical procedureshould undergo pharmacokinetic assessment, if this hasnot already been performed, and careful observationshould be ensured during the first 72 h for patients under-going major surgery and during the first 24 h for thoseundergoing minor surgery.
In the surgical setting, available data on EHL productsare limited to a few patients (23 with rFVIII–Fc and 15with BAX855) [30,31]. The hemostatic response duringthe perioperative period for these procedures was ratedby investigators/surgeons as excellent or good with bothproducts [30,31]. The dosing frequency adopted withrFVIII–Fc is similar to that of standard rFVIII, whichrequires a median total dose of 62.50 IU kg!1 on the dayof surgery and a median rFVIII–Fc dose per injection (in-cluding a loading dose) of 58.31 IU kg!1 (range 45–102 IU kg!1) for minor and major surgery (Table 3). Incontrast, rFIX–Fc allows a marked reduction in dosingfrequency for major surgical procedures, with an amountof rFIX–Fc less than that observed in historical studies ofstandard FIX products. The mean dose of rFIX–Fc onthe day of surgery (day 0) was 84.16 IU kg!1, the mean
dose on subsequent days (days 1–14) ranged from49.12 IU kg!1 to 64.61 IU kg!1, and no subject was trea-ted every day during the surgical period (days 0–14)(Table 4) [32]. In studies with the standard FIX products,subjects who underwent major surgical proceduresreceived continuous infusion with a mean doseof 154 IU kg!1 daily, and the average dose on the day ofsurgery was 254.9 IU kg!1, representing a combination ofcontinuous and bolus doses [33,34].
A surgical trial with N9-GP was also conducted in pre-viously treated hemophilia B patients. All patientsreceived a preoperative bolus injection of 80 IU kg!1,and subsequently a fixed dose of 40 IU kg!1 repeated atthe investigator’s discretion (Table 4) [35]. Again, periop-erative consumption and number of injections were lowerthan reported for any other FIX product [36]. A subanal-ysis of phase III trials showed that a single dose ofrIX-FP was sufficient to maintain hemostasis during theprocedures. The median rIX-FP consumption in fiveorthopedic surgical procedures was 87 IU kg!1 preopera-tively (day 0), 51 IU kg!1 postoperatively (days 1–2), and340 IU kg!1 overall (days 0–14), with a range of six toseven injections (Table 4) [37].
The EHL rFVIII products might have a small impacton dosing frequency during the first 48 h in the surgicalsetting. In contrast, EHL rFIX products enable a markedreduction in dosing frequency for major surgical proce-dures. Additional clinical experience is needed to make aclear recommendation.
Recombinant rFVIIa
The management of bleeding in hemophilic patients withinhibitors requires bypassing agent therapies, such as
Table 3 Dose and frequency for standard and extended half-life(EHL) products in the management of hemophilia A patients under-going minor and major surgical procedures
Dose(IU kg!1)
Frequency(h)
Durationof therapy(days) References
rFVIII standard productMinor 25–40 Every 12–24 1–3 [29]MajorPreoperative 40–50 A single-dose injectionPostoperative 30–40 Every 8–24 1–7 [29]
FVIII EHLMinor 62.50* Every 24 l [30]MajorPreoperativeandintraoperative
58.3† A single-dose injection
58.8‡ Every 24 7 [30]
rFVIII, recombinant factor VIII. *Median total dose required on theday of surgery (range 23.38–188.68 IU kg!1). †Median rFVIII EHLdose per injection. ‡Median total dose (including loading dose) of58.8 IU kg!1 with a range of 50–102 IU kg!1 during the preopera-tive and intraoperative periods.
Table 4 Dose and frequency for standard and extended half-life(EHL) products in the management of hemophilia B patients under-going minor and major surgery procedures
Dose(IU kg!1)
Frequency(h)
Durationof therapy(days) References
rFIX standard productMinor 50–80 Every 24 l [29]MajorPreoperative 60–80 A single-dose injection [29]Postoperative 40–60 Every 8–24 7 [29]
FIX EHLMinor 50–80 A single injection may be sufficient.
Repeat as needed after 24–48 hMajorPreoperative 84.16* A single-dose injection [32]
80 A single-dose injection [35]87† A single-dose injection [37]
Postoperative 49.12–64.61* 24–48 1–14 [32]40 24–96 13 [35]51 24–72 14 [37]
rFIX, recombinant factor IX. *Mean dose. †Median consumption.
© 2016 International Society on Thrombosis and Haemostasis
Treatment of bleeding disorders 2099
maintain acceptable therapeutic levels of FVIII or FIXactivity. Preoperative plasma levels of 60–80% for FIXand of 80–100% for FVIII are recommended for patientsundergoing major surgery, and 50–80% of FIX andFVIII for patients undergoing minor surgery [29]. Treat-ment should be continued in the postoperative period tomaintain similar recommended levels for standard rFVIIIand rFIX (approximately 30–60% for FIX and 40–80%for FVIII) for the following 1–3 days for minor surgeryand 10–14 days for major surgery. In all cases, the doseand frequency of infusion may be adapted to the type ofsurgical procedure, blood loss, and individual response totreatment. Each subject undergoing a surgical procedureshould undergo pharmacokinetic assessment, if this hasnot already been performed, and careful observationshould be ensured during the first 72 h for patients under-going major surgery and during the first 24 h for thoseundergoing minor surgery.
In the surgical setting, available data on EHL productsare limited to a few patients (23 with rFVIII–Fc and 15with BAX855) [30,31]. The hemostatic response duringthe perioperative period for these procedures was ratedby investigators/surgeons as excellent or good with bothproducts [30,31]. The dosing frequency adopted withrFVIII–Fc is similar to that of standard rFVIII, whichrequires a median total dose of 62.50 IU kg!1 on the dayof surgery and a median rFVIII–Fc dose per injection (in-cluding a loading dose) of 58.31 IU kg!1 (range 45–102 IU kg!1) for minor and major surgery (Table 3). Incontrast, rFIX–Fc allows a marked reduction in dosingfrequency for major surgical procedures, with an amountof rFIX–Fc less than that observed in historical studies ofstandard FIX products. The mean dose of rFIX–Fc onthe day of surgery (day 0) was 84.16 IU kg!1, the mean
dose on subsequent days (days 1–14) ranged from49.12 IU kg!1 to 64.61 IU kg!1, and no subject was trea-ted every day during the surgical period (days 0–14)(Table 4) [32]. In studies with the standard FIX products,subjects who underwent major surgical proceduresreceived continuous infusion with a mean doseof 154 IU kg!1 daily, and the average dose on the day ofsurgery was 254.9 IU kg!1, representing a combination ofcontinuous and bolus doses [33,34].
A surgical trial with N9-GP was also conducted in pre-viously treated hemophilia B patients. All patientsreceived a preoperative bolus injection of 80 IU kg!1,and subsequently a fixed dose of 40 IU kg!1 repeated atthe investigator’s discretion (Table 4) [35]. Again, periop-erative consumption and number of injections were lowerthan reported for any other FIX product [36]. A subanal-ysis of phase III trials showed that a single dose ofrIX-FP was sufficient to maintain hemostasis during theprocedures. The median rIX-FP consumption in fiveorthopedic surgical procedures was 87 IU kg!1 preopera-tively (day 0), 51 IU kg!1 postoperatively (days 1–2), and340 IU kg!1 overall (days 0–14), with a range of six toseven injections (Table 4) [37].
The EHL rFVIII products might have a small impacton dosing frequency during the first 48 h in the surgicalsetting. In contrast, EHL rFIX products enable a markedreduction in dosing frequency for major surgical proce-dures. Additional clinical experience is needed to make aclear recommendation.
Recombinant rFVIIa
The management of bleeding in hemophilic patients withinhibitors requires bypassing agent therapies, such as
Table 3 Dose and frequency for standard and extended half-life(EHL) products in the management of hemophilia A patients under-going minor and major surgical procedures
Dose(IU kg!1)
Frequency(h)
Durationof therapy(days) References
rFVIII standard productMinor 25–40 Every 12–24 1–3 [29]MajorPreoperative 40–50 A single-dose injectionPostoperative 30–40 Every 8–24 1–7 [29]
FVIII EHLMinor 62.50* Every 24 l [30]MajorPreoperativeandintraoperative
58.3† A single-dose injection
58.8‡ Every 24 7 [30]
rFVIII, recombinant factor VIII. *Median total dose required on theday of surgery (range 23.38–188.68 IU kg!1). †Median rFVIII EHLdose per injection. ‡Median total dose (including loading dose) of58.8 IU kg!1 with a range of 50–102 IU kg!1 during the preopera-tive and intraoperative periods.
Table 4 Dose and frequency for standard and extended half-life(EHL) products in the management of hemophilia B patients under-going minor and major surgery procedures
Dose(IU kg!1)
Frequency(h)
Durationof therapy(days) References
rFIX standard productMinor 50–80 Every 24 l [29]MajorPreoperative 60–80 A single-dose injection [29]Postoperative 40–60 Every 8–24 7 [29]
FIX EHLMinor 50–80 A single injection may be sufficient.
Repeat as needed after 24–48 hMajorPreoperative 84.16* A single-dose injection [32]
80 A single-dose injection [35]87† A single-dose injection [37]
Postoperative 49.12–64.61* 24–48 1–14 [32]40 24–96 13 [35]51 24–72 14 [37]
rFIX, recombinant factor IX. *Mean dose. †Median consumption.
© 2016 International Society on Thrombosis and Haemostasis
Treatment of bleeding disorders 2099
maintain acceptable therapeutic levels of FVIII or FIXactivity. Preoperative plasma levels of 60–80% for FIXand of 80–100% for FVIII are recommended for patientsundergoing major surgery, and 50–80% of FIX andFVIII for patients undergoing minor surgery [29]. Treat-ment should be continued in the postoperative period tomaintain similar recommended levels for standard rFVIIIand rFIX (approximately 30–60% for FIX and 40–80%for FVIII) for the following 1–3 days for minor surgeryand 10–14 days for major surgery. In all cases, the doseand frequency of infusion may be adapted to the type ofsurgical procedure, blood loss, and individual response totreatment. Each subject undergoing a surgical procedureshould undergo pharmacokinetic assessment, if this hasnot already been performed, and careful observationshould be ensured during the first 72 h for patients under-going major surgery and during the first 24 h for thoseundergoing minor surgery.
In the surgical setting, available data on EHL productsare limited to a few patients (23 with rFVIII–Fc and 15with BAX855) [30,31]. The hemostatic response duringthe perioperative period for these procedures was ratedby investigators/surgeons as excellent or good with bothproducts [30,31]. The dosing frequency adopted withrFVIII–Fc is similar to that of standard rFVIII, whichrequires a median total dose of 62.50 IU kg!1 on the dayof surgery and a median rFVIII–Fc dose per injection (in-cluding a loading dose) of 58.31 IU kg!1 (range 45–102 IU kg!1) for minor and major surgery (Table 3). Incontrast, rFIX–Fc allows a marked reduction in dosingfrequency for major surgical procedures, with an amountof rFIX–Fc less than that observed in historical studies ofstandard FIX products. The mean dose of rFIX–Fc onthe day of surgery (day 0) was 84.16 IU kg!1, the mean
dose on subsequent days (days 1–14) ranged from49.12 IU kg!1 to 64.61 IU kg!1, and no subject was trea-ted every day during the surgical period (days 0–14)(Table 4) [32]. In studies with the standard FIX products,subjects who underwent major surgical proceduresreceived continuous infusion with a mean doseof 154 IU kg!1 daily, and the average dose on the day ofsurgery was 254.9 IU kg!1, representing a combination ofcontinuous and bolus doses [33,34].
A surgical trial with N9-GP was also conducted in pre-viously treated hemophilia B patients. All patientsreceived a preoperative bolus injection of 80 IU kg!1,and subsequently a fixed dose of 40 IU kg!1 repeated atthe investigator’s discretion (Table 4) [35]. Again, periop-erative consumption and number of injections were lowerthan reported for any other FIX product [36]. A subanal-ysis of phase III trials showed that a single dose ofrIX-FP was sufficient to maintain hemostasis during theprocedures. The median rIX-FP consumption in fiveorthopedic surgical procedures was 87 IU kg!1 preopera-tively (day 0), 51 IU kg!1 postoperatively (days 1–2), and340 IU kg!1 overall (days 0–14), with a range of six toseven injections (Table 4) [37].
The EHL rFVIII products might have a small impacton dosing frequency during the first 48 h in the surgicalsetting. In contrast, EHL rFIX products enable a markedreduction in dosing frequency for major surgical proce-dures. Additional clinical experience is needed to make aclear recommendation.
Recombinant rFVIIa
The management of bleeding in hemophilic patients withinhibitors requires bypassing agent therapies, such as
Table 3 Dose and frequency for standard and extended half-life(EHL) products in the management of hemophilia A patients under-going minor and major surgical procedures
Dose(IU kg!1)
Frequency(h)
Durationof therapy(days) References
rFVIII standard productMinor 25–40 Every 12–24 1–3 [29]MajorPreoperative 40–50 A single-dose injectionPostoperative 30–40 Every 8–24 1–7 [29]
FVIII EHLMinor 62.50* Every 24 l [30]MajorPreoperativeandintraoperative
58.3† A single-dose injection
58.8‡ Every 24 7 [30]
rFVIII, recombinant factor VIII. *Median total dose required on theday of surgery (range 23.38–188.68 IU kg!1). †Median rFVIII EHLdose per injection. ‡Median total dose (including loading dose) of58.8 IU kg!1 with a range of 50–102 IU kg!1 during the preopera-tive and intraoperative periods.
Table 4 Dose and frequency for standard and extended half-life(EHL) products in the management of hemophilia B patients under-going minor and major surgery procedures
Dose(IU kg!1)
Frequency(h)
Durationof therapy(days) References
rFIX standard productMinor 50–80 Every 24 l [29]MajorPreoperative 60–80 A single-dose injection [29]Postoperative 40–60 Every 8–24 7 [29]
FIX EHLMinor 50–80 A single injection may be sufficient.
Repeat as needed after 24–48 hMajorPreoperative 84.16* A single-dose injection [32]
80 A single-dose injection [35]87† A single-dose injection [37]
Postoperative 49.12–64.61* 24–48 1–14 [32]40 24–96 13 [35]51 24–72 14 [37]
rFIX, recombinant factor IX. *Mean dose. †Median consumption.
© 2016 International Society on Thrombosis and Haemostasis
Treatment of bleeding disorders 2099

AJH Educational Material
2017 Clinical trials update: Innovations in hemophilia therapy
Jan Hartmann1 and Stacy E. Croteau2*
A surge in therapeutic clinical trials over recent years is paving the way for transformative treatment options forpatients with hemophilia. The introduction of recombinant factor concentrates in the early 1990s facilitated theuse of prophylactic replacement as standard care for hemophilia rather than on-demand treatment. This hasrevolutionized health outcomes for hemophilia patients, enabling participation in physical activities and reducingdebilitating, chronic joint damage. Challenges of prophylactic factor infusion include the frequency of infusionsneeded to maintain factor levels greater than 1%, patient adherence, reliable intravenous access, anddevelopment of neutralizing alloantibodies (“inhibitors”). Novel therapeutics seek to improve upon current factorconcentrates by several different mechanisms: (1) extending the half-life of circulating exogenous factor protein,(2) replacing the gene necessary for production of endogenous factor protein, (3) employing bispecific antibodytechnology to mimic the coagulation function of factor VIII, (4) disrupting anticoagulant proteins, such as tissuefactor pathway inhibitor (TFPI) or antithrombin (AT3) with antibodies, aptamers, or RNA interference technology.Emerging treatment options may reduce the frequency of (extended half-life products) or eliminate (genetherapy) the need for scheduled factor concentrate infusions, or provide a subcutaneous administration option(bispecific antibody, AT3, and TFPI targeting therapies). In addition, the nonfactor replacement strategies providea promising treatment option for patients with inhibitors, presently the greatest unmet medical need inhemophilia. This review highlights current and recently completed clinical trials that are driving a paradigm shiftin our approach to hemophilia care for patients with and without inhibitors.Am. J. Hematol. 91:1252–1260, 2016. VC 2016 Wiley Periodicals, Inc.
! EpidemiologyFactor VIII (FVIII) deficiency (Hemophilia A) and factor IX (FIX) deficiency (Hemophilia B) affect approximately 20,000 individuals in the U.S.and over 400,000 individuals globally. The incidence of these X-linked bleeding disorders is estimated at 1 in 5,000 and 1 in 30,000 male births,respectively, without racial or ethnic predilection [1]. Despite being rare diseases, Hemophilia A and B have a significant impact on patient healthoutcomes and national health economies. Severe hemophilia (factor level <1%) typically presents in male infants with either spontaneous bleedingevents or excessive bleeding/bruising with mild trauma such as circumcision, vaccination, or learning to ambulate. This phenotype can also, rarely,manifest in females as the result of Turner syndrome, skewed lionization, or compound heterozygous variants. In the absence of a family historyto prompt a diagnostic investigation, moderate disease (1–5%) or mild disease (5–50%) may only be diagnosed later in life following a hemostaticchallenge. The bleeding phenotype of “carriers” also warrants consideration. While many females may be asymptomatic, others will have factorlevels in the mild hemophilia range and may have clinically significant bleeding symptoms, such as heavy menstrual bleeding, post-procedure orpostpartum bleeding requiring treatment [2,3].
! Pathophysiology and Current Management of HemophiliaFVIII is a glycoprotein that serves as a co-factor to amplify the rate of FX activation by FIXa (serine protease). The absence or reduction of
FVIII or FIX results in impaired thrombin generation and clot formation. Over 4,000 pathogenic variants in FVIII and FIX genes have been iden-tified. The most common mutation in severe FVIII deficiency is intron 22 inversion; however, nonsense mutations, insertions/deletions, and othervariants also occur and result in absent or reduced functional protein. FIX deficiency more frequently results from point mutations (http://www.factorviii-db.org, http://www.factorix.org) [4].
Without factor replacement, bleed events for patients with hemophilia may be life threatening or result in chronic disability from recur-rent hemarthrosis and intramuscular bleeding [5]. Prophylactic factor concentrate replacement is now standard care for adult andpediatric patients with severe hemophilia [6–8]. Unfortunately, in much of the world access to factor concentrates remains a primary barri-er to care.
1Haemonetics Corporation, 400 Wood Road, Braintree, Massachusetts, 02184; 2Dana Farber/Boston Children’s Cancer and Blood Disorders Center and Harvard MedicalSchool, 450 Brookline Ave, Dana 3, Boston, Massachusetts, 02215
Disclosures: Dr. Hartmann is a Vice President and the Head of Strategic Programs at Haemonetics. Previously he was an Associate Partner in the global Med-ical Affairs practice at McKinsey & Co., Inc., where he led the hemophilia disease area team at the time of authoring this manuscript. During the last 2 yearswhile at McKinsey, Dr. Hartmann did not work directly on any hemophilia or bleeding disorder projects for products or manufacturers discussed in thisreview.Dr. Croteau has served as a consultant to Bayer, Baxalta, CSL-Behring, Dimension Therapeutics, Emergent Biosciences, Novo Nordisk, Pfizer, and Octapharma.Her institution receives research funding from Baxalta, Dimension Therapeutics, Hoffmann-La Roche and Octapharma.*Correspondence to: S. E. Croteau; E-mail: [email protected] grant sponsor: National Hemophilia Foundation (NHF)-Baxter.Received for publication: 6 July 2016; Revised: 18 August 2016; Accepted: 24 August 2016Am. J. Hematol. 91:1252–1260, 2016.Published online: 26 August 2016 in Wiley Online Library (wileyonlinelibrary.com).DOI: 10.1002/ajh.24543
VC 2016 Wiley Periodicals, Inc.
1252 American Journal of Hematology, Vol. 91, No. 12, December 2016 doi:10.1002/ajh.24543
UPDATES IN CLINICAL TRIALS FOR HEMATOLOGICAL DISEASES AJHAJHAJH Educational Material
2017 Clinical trials update: Innovations in hemophilia therapy
Jan Hartmann1 and Stacy E. Croteau2*
A surge in therapeutic clinical trials over recent years is paving the way for transformative treatment options forpatients with hemophilia. The introduction of recombinant factor concentrates in the early 1990s facilitated theuse of prophylactic replacement as standard care for hemophilia rather than on-demand treatment. This hasrevolutionized health outcomes for hemophilia patients, enabling participation in physical activities and reducingdebilitating, chronic joint damage. Challenges of prophylactic factor infusion include the frequency of infusionsneeded to maintain factor levels greater than 1%, patient adherence, reliable intravenous access, anddevelopment of neutralizing alloantibodies (“inhibitors”). Novel therapeutics seek to improve upon current factorconcentrates by several different mechanisms: (1) extending the half-life of circulating exogenous factor protein,(2) replacing the gene necessary for production of endogenous factor protein, (3) employing bispecific antibodytechnology to mimic the coagulation function of factor VIII, (4) disrupting anticoagulant proteins, such as tissuefactor pathway inhibitor (TFPI) or antithrombin (AT3) with antibodies, aptamers, or RNA interference technology.Emerging treatment options may reduce the frequency of (extended half-life products) or eliminate (genetherapy) the need for scheduled factor concentrate infusions, or provide a subcutaneous administration option(bispecific antibody, AT3, and TFPI targeting therapies). In addition, the nonfactor replacement strategies providea promising treatment option for patients with inhibitors, presently the greatest unmet medical need inhemophilia. This review highlights current and recently completed clinical trials that are driving a paradigm shiftin our approach to hemophilia care for patients with and without inhibitors.Am. J. Hematol. 91:1252–1260, 2016. VC 2016 Wiley Periodicals, Inc.
! EpidemiologyFactor VIII (FVIII) deficiency (Hemophilia A) and factor IX (FIX) deficiency (Hemophilia B) affect approximately 20,000 individuals in the U.S.and over 400,000 individuals globally. The incidence of these X-linked bleeding disorders is estimated at 1 in 5,000 and 1 in 30,000 male births,respectively, without racial or ethnic predilection [1]. Despite being rare diseases, Hemophilia A and B have a significant impact on patient healthoutcomes and national health economies. Severe hemophilia (factor level <1%) typically presents in male infants with either spontaneous bleedingevents or excessive bleeding/bruising with mild trauma such as circumcision, vaccination, or learning to ambulate. This phenotype can also, rarely,manifest in females as the result of Turner syndrome, skewed lionization, or compound heterozygous variants. In the absence of a family historyto prompt a diagnostic investigation, moderate disease (1–5%) or mild disease (5–50%) may only be diagnosed later in life following a hemostaticchallenge. The bleeding phenotype of “carriers” also warrants consideration. While many females may be asymptomatic, others will have factorlevels in the mild hemophilia range and may have clinically significant bleeding symptoms, such as heavy menstrual bleeding, post-procedure orpostpartum bleeding requiring treatment [2,3].
! Pathophysiology and Current Management of HemophiliaFVIII is a glycoprotein that serves as a co-factor to amplify the rate of FX activation by FIXa (serine protease). The absence or reduction of
FVIII or FIX results in impaired thrombin generation and clot formation. Over 4,000 pathogenic variants in FVIII and FIX genes have been iden-tified. The most common mutation in severe FVIII deficiency is intron 22 inversion; however, nonsense mutations, insertions/deletions, and othervariants also occur and result in absent or reduced functional protein. FIX deficiency more frequently results from point mutations (http://www.factorviii-db.org, http://www.factorix.org) [4].
Without factor replacement, bleed events for patients with hemophilia may be life threatening or result in chronic disability from recur-rent hemarthrosis and intramuscular bleeding [5]. Prophylactic factor concentrate replacement is now standard care for adult andpediatric patients with severe hemophilia [6–8]. Unfortunately, in much of the world access to factor concentrates remains a primary barri-er to care.
1Haemonetics Corporation, 400 Wood Road, Braintree, Massachusetts, 02184; 2Dana Farber/Boston Children’s Cancer and Blood Disorders Center and Harvard MedicalSchool, 450 Brookline Ave, Dana 3, Boston, Massachusetts, 02215
Disclosures: Dr. Hartmann is a Vice President and the Head of Strategic Programs at Haemonetics. Previously he was an Associate Partner in the global Med-ical Affairs practice at McKinsey & Co., Inc., where he led the hemophilia disease area team at the time of authoring this manuscript. During the last 2 yearswhile at McKinsey, Dr. Hartmann did not work directly on any hemophilia or bleeding disorder projects for products or manufacturers discussed in thisreview.Dr. Croteau has served as a consultant to Bayer, Baxalta, CSL-Behring, Dimension Therapeutics, Emergent Biosciences, Novo Nordisk, Pfizer, and Octapharma.Her institution receives research funding from Baxalta, Dimension Therapeutics, Hoffmann-La Roche and Octapharma.*Correspondence to: S. E. Croteau; E-mail: [email protected] grant sponsor: National Hemophilia Foundation (NHF)-Baxter.Received for publication: 6 July 2016; Revised: 18 August 2016; Accepted: 24 August 2016Am. J. Hematol. 91:1252–1260, 2016.Published online: 26 August 2016 in Wiley Online Library (wileyonlinelibrary.com).DOI: 10.1002/ajh.24543
VC 2016 Wiley Periodicals, Inc.
1252 American Journal of Hematology, Vol. 91, No. 12, December 2016 doi:10.1002/ajh.24543
UPDATES IN CLINICAL TRIALS FOR HEMATOLOGICAL DISEASES AJHAJH
AJH Educational Material
2017 Clinical trials update: Innovations in hemophilia therapy
Jan Hartmann1 and Stacy E. Croteau2*
A surge in therapeutic clinical trials over recent years is paving the way for transformative treatment options forpatients with hemophilia. The introduction of recombinant factor concentrates in the early 1990s facilitated theuse of prophylactic replacement as standard care for hemophilia rather than on-demand treatment. This hasrevolutionized health outcomes for hemophilia patients, enabling participation in physical activities and reducingdebilitating, chronic joint damage. Challenges of prophylactic factor infusion include the frequency of infusionsneeded to maintain factor levels greater than 1%, patient adherence, reliable intravenous access, anddevelopment of neutralizing alloantibodies (“inhibitors”). Novel therapeutics seek to improve upon current factorconcentrates by several different mechanisms: (1) extending the half-life of circulating exogenous factor protein,(2) replacing the gene necessary for production of endogenous factor protein, (3) employing bispecific antibodytechnology to mimic the coagulation function of factor VIII, (4) disrupting anticoagulant proteins, such as tissuefactor pathway inhibitor (TFPI) or antithrombin (AT3) with antibodies, aptamers, or RNA interference technology.Emerging treatment options may reduce the frequency of (extended half-life products) or eliminate (genetherapy) the need for scheduled factor concentrate infusions, or provide a subcutaneous administration option(bispecific antibody, AT3, and TFPI targeting therapies). In addition, the nonfactor replacement strategies providea promising treatment option for patients with inhibitors, presently the greatest unmet medical need inhemophilia. This review highlights current and recently completed clinical trials that are driving a paradigm shiftin our approach to hemophilia care for patients with and without inhibitors.Am. J. Hematol. 91:1252–1260, 2016. VC 2016 Wiley Periodicals, Inc.
! EpidemiologyFactor VIII (FVIII) deficiency (Hemophilia A) and factor IX (FIX) deficiency (Hemophilia B) affect approximately 20,000 individuals in the U.S.and over 400,000 individuals globally. The incidence of these X-linked bleeding disorders is estimated at 1 in 5,000 and 1 in 30,000 male births,respectively, without racial or ethnic predilection [1]. Despite being rare diseases, Hemophilia A and B have a significant impact on patient healthoutcomes and national health economies. Severe hemophilia (factor level <1%) typically presents in male infants with either spontaneous bleedingevents or excessive bleeding/bruising with mild trauma such as circumcision, vaccination, or learning to ambulate. This phenotype can also, rarely,manifest in females as the result of Turner syndrome, skewed lionization, or compound heterozygous variants. In the absence of a family historyto prompt a diagnostic investigation, moderate disease (1–5%) or mild disease (5–50%) may only be diagnosed later in life following a hemostaticchallenge. The bleeding phenotype of “carriers” also warrants consideration. While many females may be asymptomatic, others will have factorlevels in the mild hemophilia range and may have clinically significant bleeding symptoms, such as heavy menstrual bleeding, post-procedure orpostpartum bleeding requiring treatment [2,3].
! Pathophysiology and Current Management of HemophiliaFVIII is a glycoprotein that serves as a co-factor to amplify the rate of FX activation by FIXa (serine protease). The absence or reduction of
FVIII or FIX results in impaired thrombin generation and clot formation. Over 4,000 pathogenic variants in FVIII and FIX genes have been iden-tified. The most common mutation in severe FVIII deficiency is intron 22 inversion; however, nonsense mutations, insertions/deletions, and othervariants also occur and result in absent or reduced functional protein. FIX deficiency more frequently results from point mutations (http://www.factorviii-db.org, http://www.factorix.org) [4].
Without factor replacement, bleed events for patients with hemophilia may be life threatening or result in chronic disability from recur-rent hemarthrosis and intramuscular bleeding [5]. Prophylactic factor concentrate replacement is now standard care for adult andpediatric patients with severe hemophilia [6–8]. Unfortunately, in much of the world access to factor concentrates remains a primary barri-er to care.
1Haemonetics Corporation, 400 Wood Road, Braintree, Massachusetts, 02184; 2Dana Farber/Boston Children’s Cancer and Blood Disorders Center and Harvard MedicalSchool, 450 Brookline Ave, Dana 3, Boston, Massachusetts, 02215
Disclosures: Dr. Hartmann is a Vice President and the Head of Strategic Programs at Haemonetics. Previously he was an Associate Partner in the global Med-ical Affairs practice at McKinsey & Co., Inc., where he led the hemophilia disease area team at the time of authoring this manuscript. During the last 2 yearswhile at McKinsey, Dr. Hartmann did not work directly on any hemophilia or bleeding disorder projects for products or manufacturers discussed in thisreview.Dr. Croteau has served as a consultant to Bayer, Baxalta, CSL-Behring, Dimension Therapeutics, Emergent Biosciences, Novo Nordisk, Pfizer, and Octapharma.Her institution receives research funding from Baxalta, Dimension Therapeutics, Hoffmann-La Roche and Octapharma.*Correspondence to: S. E. Croteau; E-mail: [email protected] grant sponsor: National Hemophilia Foundation (NHF)-Baxter.Received for publication: 6 July 2016; Revised: 18 August 2016; Accepted: 24 August 2016Am. J. Hematol. 91:1252–1260, 2016.Published online: 26 August 2016 in Wiley Online Library (wileyonlinelibrary.com).DOI: 10.1002/ajh.24543
VC 2016 Wiley Periodicals, Inc.
1252 American Journal of Hematology, Vol. 91, No. 12, December 2016 doi:10.1002/ajh.24543
UPDATES IN CLINICAL TRIALS FOR HEMATOLOGICAL DISEASES AJHAJH
" EHL factor concentrates build on the familiarmanagement strategies of conven=onal factorconcentrates
" The challengesof frequent IV infusions,pa=entadherence,andinhibitorriskremain.
" The degree to which the addi=on of thesevarious moie=es increase, decrease, or have aneutraleffectonimmunogenicityremainsunderinves=ga=on.

AJH Educational Material
2017 Clinical trials update: Innovations in hemophilia therapy
Jan Hartmann1 and Stacy E. Croteau2*
A surge in therapeutic clinical trials over recent years is paving the way for transformative treatment options forpatients with hemophilia. The introduction of recombinant factor concentrates in the early 1990s facilitated theuse of prophylactic replacement as standard care for hemophilia rather than on-demand treatment. This hasrevolutionized health outcomes for hemophilia patients, enabling participation in physical activities and reducingdebilitating, chronic joint damage. Challenges of prophylactic factor infusion include the frequency of infusionsneeded to maintain factor levels greater than 1%, patient adherence, reliable intravenous access, anddevelopment of neutralizing alloantibodies (“inhibitors”). Novel therapeutics seek to improve upon current factorconcentrates by several different mechanisms: (1) extending the half-life of circulating exogenous factor protein,(2) replacing the gene necessary for production of endogenous factor protein, (3) employing bispecific antibodytechnology to mimic the coagulation function of factor VIII, (4) disrupting anticoagulant proteins, such as tissuefactor pathway inhibitor (TFPI) or antithrombin (AT3) with antibodies, aptamers, or RNA interference technology.Emerging treatment options may reduce the frequency of (extended half-life products) or eliminate (genetherapy) the need for scheduled factor concentrate infusions, or provide a subcutaneous administration option(bispecific antibody, AT3, and TFPI targeting therapies). In addition, the nonfactor replacement strategies providea promising treatment option for patients with inhibitors, presently the greatest unmet medical need inhemophilia. This review highlights current and recently completed clinical trials that are driving a paradigm shiftin our approach to hemophilia care for patients with and without inhibitors.Am. J. Hematol. 91:1252–1260, 2016. VC 2016 Wiley Periodicals, Inc.
! EpidemiologyFactor VIII (FVIII) deficiency (Hemophilia A) and factor IX (FIX) deficiency (Hemophilia B) affect approximately 20,000 individuals in the U.S.and over 400,000 individuals globally. The incidence of these X-linked bleeding disorders is estimated at 1 in 5,000 and 1 in 30,000 male births,respectively, without racial or ethnic predilection [1]. Despite being rare diseases, Hemophilia A and B have a significant impact on patient healthoutcomes and national health economies. Severe hemophilia (factor level <1%) typically presents in male infants with either spontaneous bleedingevents or excessive bleeding/bruising with mild trauma such as circumcision, vaccination, or learning to ambulate. This phenotype can also, rarely,manifest in females as the result of Turner syndrome, skewed lionization, or compound heterozygous variants. In the absence of a family historyto prompt a diagnostic investigation, moderate disease (1–5%) or mild disease (5–50%) may only be diagnosed later in life following a hemostaticchallenge. The bleeding phenotype of “carriers” also warrants consideration. While many females may be asymptomatic, others will have factorlevels in the mild hemophilia range and may have clinically significant bleeding symptoms, such as heavy menstrual bleeding, post-procedure orpostpartum bleeding requiring treatment [2,3].
! Pathophysiology and Current Management of HemophiliaFVIII is a glycoprotein that serves as a co-factor to amplify the rate of FX activation by FIXa (serine protease). The absence or reduction of
FVIII or FIX results in impaired thrombin generation and clot formation. Over 4,000 pathogenic variants in FVIII and FIX genes have been iden-tified. The most common mutation in severe FVIII deficiency is intron 22 inversion; however, nonsense mutations, insertions/deletions, and othervariants also occur and result in absent or reduced functional protein. FIX deficiency more frequently results from point mutations (http://www.factorviii-db.org, http://www.factorix.org) [4].
Without factor replacement, bleed events for patients with hemophilia may be life threatening or result in chronic disability from recur-rent hemarthrosis and intramuscular bleeding [5]. Prophylactic factor concentrate replacement is now standard care for adult andpediatric patients with severe hemophilia [6–8]. Unfortunately, in much of the world access to factor concentrates remains a primary barri-er to care.
1Haemonetics Corporation, 400 Wood Road, Braintree, Massachusetts, 02184; 2Dana Farber/Boston Children’s Cancer and Blood Disorders Center and Harvard MedicalSchool, 450 Brookline Ave, Dana 3, Boston, Massachusetts, 02215
Disclosures: Dr. Hartmann is a Vice President and the Head of Strategic Programs at Haemonetics. Previously he was an Associate Partner in the global Med-ical Affairs practice at McKinsey & Co., Inc., where he led the hemophilia disease area team at the time of authoring this manuscript. During the last 2 yearswhile at McKinsey, Dr. Hartmann did not work directly on any hemophilia or bleeding disorder projects for products or manufacturers discussed in thisreview.Dr. Croteau has served as a consultant to Bayer, Baxalta, CSL-Behring, Dimension Therapeutics, Emergent Biosciences, Novo Nordisk, Pfizer, and Octapharma.Her institution receives research funding from Baxalta, Dimension Therapeutics, Hoffmann-La Roche and Octapharma.*Correspondence to: S. E. Croteau; E-mail: [email protected] grant sponsor: National Hemophilia Foundation (NHF)-Baxter.Received for publication: 6 July 2016; Revised: 18 August 2016; Accepted: 24 August 2016Am. J. Hematol. 91:1252–1260, 2016.Published online: 26 August 2016 in Wiley Online Library (wileyonlinelibrary.com).DOI: 10.1002/ajh.24543
VC 2016 Wiley Periodicals, Inc.
1252 American Journal of Hematology, Vol. 91, No. 12, December 2016 doi:10.1002/ajh.24543
UPDATES IN CLINICAL TRIALS FOR HEMATOLOGICAL DISEASES AJHAJHAJH Educational Material
2017 Clinical trials update: Innovations in hemophilia therapy
Jan Hartmann1 and Stacy E. Croteau2*
A surge in therapeutic clinical trials over recent years is paving the way for transformative treatment options forpatients with hemophilia. The introduction of recombinant factor concentrates in the early 1990s facilitated theuse of prophylactic replacement as standard care for hemophilia rather than on-demand treatment. This hasrevolutionized health outcomes for hemophilia patients, enabling participation in physical activities and reducingdebilitating, chronic joint damage. Challenges of prophylactic factor infusion include the frequency of infusionsneeded to maintain factor levels greater than 1%, patient adherence, reliable intravenous access, anddevelopment of neutralizing alloantibodies (“inhibitors”). Novel therapeutics seek to improve upon current factorconcentrates by several different mechanisms: (1) extending the half-life of circulating exogenous factor protein,(2) replacing the gene necessary for production of endogenous factor protein, (3) employing bispecific antibodytechnology to mimic the coagulation function of factor VIII, (4) disrupting anticoagulant proteins, such as tissuefactor pathway inhibitor (TFPI) or antithrombin (AT3) with antibodies, aptamers, or RNA interference technology.Emerging treatment options may reduce the frequency of (extended half-life products) or eliminate (genetherapy) the need for scheduled factor concentrate infusions, or provide a subcutaneous administration option(bispecific antibody, AT3, and TFPI targeting therapies). In addition, the nonfactor replacement strategies providea promising treatment option for patients with inhibitors, presently the greatest unmet medical need inhemophilia. This review highlights current and recently completed clinical trials that are driving a paradigm shiftin our approach to hemophilia care for patients with and without inhibitors.Am. J. Hematol. 91:1252–1260, 2016. VC 2016 Wiley Periodicals, Inc.
! EpidemiologyFactor VIII (FVIII) deficiency (Hemophilia A) and factor IX (FIX) deficiency (Hemophilia B) affect approximately 20,000 individuals in the U.S.and over 400,000 individuals globally. The incidence of these X-linked bleeding disorders is estimated at 1 in 5,000 and 1 in 30,000 male births,respectively, without racial or ethnic predilection [1]. Despite being rare diseases, Hemophilia A and B have a significant impact on patient healthoutcomes and national health economies. Severe hemophilia (factor level <1%) typically presents in male infants with either spontaneous bleedingevents or excessive bleeding/bruising with mild trauma such as circumcision, vaccination, or learning to ambulate. This phenotype can also, rarely,manifest in females as the result of Turner syndrome, skewed lionization, or compound heterozygous variants. In the absence of a family historyto prompt a diagnostic investigation, moderate disease (1–5%) or mild disease (5–50%) may only be diagnosed later in life following a hemostaticchallenge. The bleeding phenotype of “carriers” also warrants consideration. While many females may be asymptomatic, others will have factorlevels in the mild hemophilia range and may have clinically significant bleeding symptoms, such as heavy menstrual bleeding, post-procedure orpostpartum bleeding requiring treatment [2,3].
! Pathophysiology and Current Management of HemophiliaFVIII is a glycoprotein that serves as a co-factor to amplify the rate of FX activation by FIXa (serine protease). The absence or reduction of
FVIII or FIX results in impaired thrombin generation and clot formation. Over 4,000 pathogenic variants in FVIII and FIX genes have been iden-tified. The most common mutation in severe FVIII deficiency is intron 22 inversion; however, nonsense mutations, insertions/deletions, and othervariants also occur and result in absent or reduced functional protein. FIX deficiency more frequently results from point mutations (http://www.factorviii-db.org, http://www.factorix.org) [4].
Without factor replacement, bleed events for patients with hemophilia may be life threatening or result in chronic disability from recur-rent hemarthrosis and intramuscular bleeding [5]. Prophylactic factor concentrate replacement is now standard care for adult andpediatric patients with severe hemophilia [6–8]. Unfortunately, in much of the world access to factor concentrates remains a primary barri-er to care.
1Haemonetics Corporation, 400 Wood Road, Braintree, Massachusetts, 02184; 2Dana Farber/Boston Children’s Cancer and Blood Disorders Center and Harvard MedicalSchool, 450 Brookline Ave, Dana 3, Boston, Massachusetts, 02215
Disclosures: Dr. Hartmann is a Vice President and the Head of Strategic Programs at Haemonetics. Previously he was an Associate Partner in the global Med-ical Affairs practice at McKinsey & Co., Inc., where he led the hemophilia disease area team at the time of authoring this manuscript. During the last 2 yearswhile at McKinsey, Dr. Hartmann did not work directly on any hemophilia or bleeding disorder projects for products or manufacturers discussed in thisreview.Dr. Croteau has served as a consultant to Bayer, Baxalta, CSL-Behring, Dimension Therapeutics, Emergent Biosciences, Novo Nordisk, Pfizer, and Octapharma.Her institution receives research funding from Baxalta, Dimension Therapeutics, Hoffmann-La Roche and Octapharma.*Correspondence to: S. E. Croteau; E-mail: [email protected] grant sponsor: National Hemophilia Foundation (NHF)-Baxter.Received for publication: 6 July 2016; Revised: 18 August 2016; Accepted: 24 August 2016Am. J. Hematol. 91:1252–1260, 2016.Published online: 26 August 2016 in Wiley Online Library (wileyonlinelibrary.com).DOI: 10.1002/ajh.24543
VC 2016 Wiley Periodicals, Inc.
1252 American Journal of Hematology, Vol. 91, No. 12, December 2016 doi:10.1002/ajh.24543
UPDATES IN CLINICAL TRIALS FOR HEMATOLOGICAL DISEASES AJHAJH
AJH Educational Material
2017 Clinical trials update: Innovations in hemophilia therapy
Jan Hartmann1 and Stacy E. Croteau2*
A surge in therapeutic clinical trials over recent years is paving the way for transformative treatment options forpatients with hemophilia. The introduction of recombinant factor concentrates in the early 1990s facilitated theuse of prophylactic replacement as standard care for hemophilia rather than on-demand treatment. This hasrevolutionized health outcomes for hemophilia patients, enabling participation in physical activities and reducingdebilitating, chronic joint damage. Challenges of prophylactic factor infusion include the frequency of infusionsneeded to maintain factor levels greater than 1%, patient adherence, reliable intravenous access, anddevelopment of neutralizing alloantibodies (“inhibitors”). Novel therapeutics seek to improve upon current factorconcentrates by several different mechanisms: (1) extending the half-life of circulating exogenous factor protein,(2) replacing the gene necessary for production of endogenous factor protein, (3) employing bispecific antibodytechnology to mimic the coagulation function of factor VIII, (4) disrupting anticoagulant proteins, such as tissuefactor pathway inhibitor (TFPI) or antithrombin (AT3) with antibodies, aptamers, or RNA interference technology.Emerging treatment options may reduce the frequency of (extended half-life products) or eliminate (genetherapy) the need for scheduled factor concentrate infusions, or provide a subcutaneous administration option(bispecific antibody, AT3, and TFPI targeting therapies). In addition, the nonfactor replacement strategies providea promising treatment option for patients with inhibitors, presently the greatest unmet medical need inhemophilia. This review highlights current and recently completed clinical trials that are driving a paradigm shiftin our approach to hemophilia care for patients with and without inhibitors.Am. J. Hematol. 91:1252–1260, 2016. VC 2016 Wiley Periodicals, Inc.
! EpidemiologyFactor VIII (FVIII) deficiency (Hemophilia A) and factor IX (FIX) deficiency (Hemophilia B) affect approximately 20,000 individuals in the U.S.and over 400,000 individuals globally. The incidence of these X-linked bleeding disorders is estimated at 1 in 5,000 and 1 in 30,000 male births,respectively, without racial or ethnic predilection [1]. Despite being rare diseases, Hemophilia A and B have a significant impact on patient healthoutcomes and national health economies. Severe hemophilia (factor level <1%) typically presents in male infants with either spontaneous bleedingevents or excessive bleeding/bruising with mild trauma such as circumcision, vaccination, or learning to ambulate. This phenotype can also, rarely,manifest in females as the result of Turner syndrome, skewed lionization, or compound heterozygous variants. In the absence of a family historyto prompt a diagnostic investigation, moderate disease (1–5%) or mild disease (5–50%) may only be diagnosed later in life following a hemostaticchallenge. The bleeding phenotype of “carriers” also warrants consideration. While many females may be asymptomatic, others will have factorlevels in the mild hemophilia range and may have clinically significant bleeding symptoms, such as heavy menstrual bleeding, post-procedure orpostpartum bleeding requiring treatment [2,3].
! Pathophysiology and Current Management of HemophiliaFVIII is a glycoprotein that serves as a co-factor to amplify the rate of FX activation by FIXa (serine protease). The absence or reduction of
FVIII or FIX results in impaired thrombin generation and clot formation. Over 4,000 pathogenic variants in FVIII and FIX genes have been iden-tified. The most common mutation in severe FVIII deficiency is intron 22 inversion; however, nonsense mutations, insertions/deletions, and othervariants also occur and result in absent or reduced functional protein. FIX deficiency more frequently results from point mutations (http://www.factorviii-db.org, http://www.factorix.org) [4].
Without factor replacement, bleed events for patients with hemophilia may be life threatening or result in chronic disability from recur-rent hemarthrosis and intramuscular bleeding [5]. Prophylactic factor concentrate replacement is now standard care for adult andpediatric patients with severe hemophilia [6–8]. Unfortunately, in much of the world access to factor concentrates remains a primary barri-er to care.
1Haemonetics Corporation, 400 Wood Road, Braintree, Massachusetts, 02184; 2Dana Farber/Boston Children’s Cancer and Blood Disorders Center and Harvard MedicalSchool, 450 Brookline Ave, Dana 3, Boston, Massachusetts, 02215
Disclosures: Dr. Hartmann is a Vice President and the Head of Strategic Programs at Haemonetics. Previously he was an Associate Partner in the global Med-ical Affairs practice at McKinsey & Co., Inc., where he led the hemophilia disease area team at the time of authoring this manuscript. During the last 2 yearswhile at McKinsey, Dr. Hartmann did not work directly on any hemophilia or bleeding disorder projects for products or manufacturers discussed in thisreview.Dr. Croteau has served as a consultant to Bayer, Baxalta, CSL-Behring, Dimension Therapeutics, Emergent Biosciences, Novo Nordisk, Pfizer, and Octapharma.Her institution receives research funding from Baxalta, Dimension Therapeutics, Hoffmann-La Roche and Octapharma.*Correspondence to: S. E. Croteau; E-mail: [email protected] grant sponsor: National Hemophilia Foundation (NHF)-Baxter.Received for publication: 6 July 2016; Revised: 18 August 2016; Accepted: 24 August 2016Am. J. Hematol. 91:1252–1260, 2016.Published online: 26 August 2016 in Wiley Online Library (wileyonlinelibrary.com).DOI: 10.1002/ajh.24543
VC 2016 Wiley Periodicals, Inc.
1252 American Journal of Hematology, Vol. 91, No. 12, December 2016 doi:10.1002/ajh.24543
UPDATES IN CLINICAL TRIALS FOR HEMATOLOGICAL DISEASES AJHAJH
" Interes=ngly, uptake of these products in theimmediatepostlicensureperiodhasbeenmodest
" EHL products have accentuated the variability ofpa=enthalf-life.
" The real-world impact of EHL products on health-related quality of life and health economics are alsounderinves=ga=on

Da dove veniamo? Che siamo? Dove andiamo?
Paul Gauguin, 1897

Whyishemophiliaanexcellenttargetforgenetherapy
" Singlegenedisorder" Small absolute amounts of cloGng factors innormalplasma(fVIII50ng/ml,fIX5µg/ml)
" 1/10 of these values sufficient for normalhemostasis
" Biologically ac=ve factors can be produced in awidevarietyofcells
" Large animal models are available (hemophilicdogs)

AJH Educational Material
2017 Clinical trials update: Innovations in hemophilia therapy
Jan Hartmann1 and Stacy E. Croteau2*
A surge in therapeutic clinical trials over recent years is paving the way for transformative treatment options forpatients with hemophilia. The introduction of recombinant factor concentrates in the early 1990s facilitated theuse of prophylactic replacement as standard care for hemophilia rather than on-demand treatment. This hasrevolutionized health outcomes for hemophilia patients, enabling participation in physical activities and reducingdebilitating, chronic joint damage. Challenges of prophylactic factor infusion include the frequency of infusionsneeded to maintain factor levels greater than 1%, patient adherence, reliable intravenous access, anddevelopment of neutralizing alloantibodies (“inhibitors”). Novel therapeutics seek to improve upon current factorconcentrates by several different mechanisms: (1) extending the half-life of circulating exogenous factor protein,(2) replacing the gene necessary for production of endogenous factor protein, (3) employing bispecific antibodytechnology to mimic the coagulation function of factor VIII, (4) disrupting anticoagulant proteins, such as tissuefactor pathway inhibitor (TFPI) or antithrombin (AT3) with antibodies, aptamers, or RNA interference technology.Emerging treatment options may reduce the frequency of (extended half-life products) or eliminate (genetherapy) the need for scheduled factor concentrate infusions, or provide a subcutaneous administration option(bispecific antibody, AT3, and TFPI targeting therapies). In addition, the nonfactor replacement strategies providea promising treatment option for patients with inhibitors, presently the greatest unmet medical need inhemophilia. This review highlights current and recently completed clinical trials that are driving a paradigm shiftin our approach to hemophilia care for patients with and without inhibitors.Am. J. Hematol. 91:1252–1260, 2016. VC 2016 Wiley Periodicals, Inc.
! EpidemiologyFactor VIII (FVIII) deficiency (Hemophilia A) and factor IX (FIX) deficiency (Hemophilia B) affect approximately 20,000 individuals in the U.S.and over 400,000 individuals globally. The incidence of these X-linked bleeding disorders is estimated at 1 in 5,000 and 1 in 30,000 male births,respectively, without racial or ethnic predilection [1]. Despite being rare diseases, Hemophilia A and B have a significant impact on patient healthoutcomes and national health economies. Severe hemophilia (factor level <1%) typically presents in male infants with either spontaneous bleedingevents or excessive bleeding/bruising with mild trauma such as circumcision, vaccination, or learning to ambulate. This phenotype can also, rarely,manifest in females as the result of Turner syndrome, skewed lionization, or compound heterozygous variants. In the absence of a family historyto prompt a diagnostic investigation, moderate disease (1–5%) or mild disease (5–50%) may only be diagnosed later in life following a hemostaticchallenge. The bleeding phenotype of “carriers” also warrants consideration. While many females may be asymptomatic, others will have factorlevels in the mild hemophilia range and may have clinically significant bleeding symptoms, such as heavy menstrual bleeding, post-procedure orpostpartum bleeding requiring treatment [2,3].
! Pathophysiology and Current Management of HemophiliaFVIII is a glycoprotein that serves as a co-factor to amplify the rate of FX activation by FIXa (serine protease). The absence or reduction of
FVIII or FIX results in impaired thrombin generation and clot formation. Over 4,000 pathogenic variants in FVIII and FIX genes have been iden-tified. The most common mutation in severe FVIII deficiency is intron 22 inversion; however, nonsense mutations, insertions/deletions, and othervariants also occur and result in absent or reduced functional protein. FIX deficiency more frequently results from point mutations (http://www.factorviii-db.org, http://www.factorix.org) [4].
Without factor replacement, bleed events for patients with hemophilia may be life threatening or result in chronic disability from recur-rent hemarthrosis and intramuscular bleeding [5]. Prophylactic factor concentrate replacement is now standard care for adult andpediatric patients with severe hemophilia [6–8]. Unfortunately, in much of the world access to factor concentrates remains a primary barri-er to care.
1Haemonetics Corporation, 400 Wood Road, Braintree, Massachusetts, 02184; 2Dana Farber/Boston Children’s Cancer and Blood Disorders Center and Harvard MedicalSchool, 450 Brookline Ave, Dana 3, Boston, Massachusetts, 02215
Disclosures: Dr. Hartmann is a Vice President and the Head of Strategic Programs at Haemonetics. Previously he was an Associate Partner in the global Med-ical Affairs practice at McKinsey & Co., Inc., where he led the hemophilia disease area team at the time of authoring this manuscript. During the last 2 yearswhile at McKinsey, Dr. Hartmann did not work directly on any hemophilia or bleeding disorder projects for products or manufacturers discussed in thisreview.Dr. Croteau has served as a consultant to Bayer, Baxalta, CSL-Behring, Dimension Therapeutics, Emergent Biosciences, Novo Nordisk, Pfizer, and Octapharma.Her institution receives research funding from Baxalta, Dimension Therapeutics, Hoffmann-La Roche and Octapharma.*Correspondence to: S. E. Croteau; E-mail: [email protected] grant sponsor: National Hemophilia Foundation (NHF)-Baxter.Received for publication: 6 July 2016; Revised: 18 August 2016; Accepted: 24 August 2016Am. J. Hematol. 91:1252–1260, 2016.Published online: 26 August 2016 in Wiley Online Library (wileyonlinelibrary.com).DOI: 10.1002/ajh.24543
VC 2016 Wiley Periodicals, Inc.
1252 American Journal of Hematology, Vol. 91, No. 12, December 2016 doi:10.1002/ajh.24543
UPDATES IN CLINICAL TRIALS FOR HEMATOLOGICAL DISEASES AJHAJHAJH Educational Material
2017 Clinical trials update: Innovations in hemophilia therapy
Jan Hartmann1 and Stacy E. Croteau2*
A surge in therapeutic clinical trials over recent years is paving the way for transformative treatment options forpatients with hemophilia. The introduction of recombinant factor concentrates in the early 1990s facilitated theuse of prophylactic replacement as standard care for hemophilia rather than on-demand treatment. This hasrevolutionized health outcomes for hemophilia patients, enabling participation in physical activities and reducingdebilitating, chronic joint damage. Challenges of prophylactic factor infusion include the frequency of infusionsneeded to maintain factor levels greater than 1%, patient adherence, reliable intravenous access, anddevelopment of neutralizing alloantibodies (“inhibitors”). Novel therapeutics seek to improve upon current factorconcentrates by several different mechanisms: (1) extending the half-life of circulating exogenous factor protein,(2) replacing the gene necessary for production of endogenous factor protein, (3) employing bispecific antibodytechnology to mimic the coagulation function of factor VIII, (4) disrupting anticoagulant proteins, such as tissuefactor pathway inhibitor (TFPI) or antithrombin (AT3) with antibodies, aptamers, or RNA interference technology.Emerging treatment options may reduce the frequency of (extended half-life products) or eliminate (genetherapy) the need for scheduled factor concentrate infusions, or provide a subcutaneous administration option(bispecific antibody, AT3, and TFPI targeting therapies). In addition, the nonfactor replacement strategies providea promising treatment option for patients with inhibitors, presently the greatest unmet medical need inhemophilia. This review highlights current and recently completed clinical trials that are driving a paradigm shiftin our approach to hemophilia care for patients with and without inhibitors.Am. J. Hematol. 91:1252–1260, 2016. VC 2016 Wiley Periodicals, Inc.
! EpidemiologyFactor VIII (FVIII) deficiency (Hemophilia A) and factor IX (FIX) deficiency (Hemophilia B) affect approximately 20,000 individuals in the U.S.and over 400,000 individuals globally. The incidence of these X-linked bleeding disorders is estimated at 1 in 5,000 and 1 in 30,000 male births,respectively, without racial or ethnic predilection [1]. Despite being rare diseases, Hemophilia A and B have a significant impact on patient healthoutcomes and national health economies. Severe hemophilia (factor level <1%) typically presents in male infants with either spontaneous bleedingevents or excessive bleeding/bruising with mild trauma such as circumcision, vaccination, or learning to ambulate. This phenotype can also, rarely,manifest in females as the result of Turner syndrome, skewed lionization, or compound heterozygous variants. In the absence of a family historyto prompt a diagnostic investigation, moderate disease (1–5%) or mild disease (5–50%) may only be diagnosed later in life following a hemostaticchallenge. The bleeding phenotype of “carriers” also warrants consideration. While many females may be asymptomatic, others will have factorlevels in the mild hemophilia range and may have clinically significant bleeding symptoms, such as heavy menstrual bleeding, post-procedure orpostpartum bleeding requiring treatment [2,3].
! Pathophysiology and Current Management of HemophiliaFVIII is a glycoprotein that serves as a co-factor to amplify the rate of FX activation by FIXa (serine protease). The absence or reduction of
FVIII or FIX results in impaired thrombin generation and clot formation. Over 4,000 pathogenic variants in FVIII and FIX genes have been iden-tified. The most common mutation in severe FVIII deficiency is intron 22 inversion; however, nonsense mutations, insertions/deletions, and othervariants also occur and result in absent or reduced functional protein. FIX deficiency more frequently results from point mutations (http://www.factorviii-db.org, http://www.factorix.org) [4].
Without factor replacement, bleed events for patients with hemophilia may be life threatening or result in chronic disability from recur-rent hemarthrosis and intramuscular bleeding [5]. Prophylactic factor concentrate replacement is now standard care for adult andpediatric patients with severe hemophilia [6–8]. Unfortunately, in much of the world access to factor concentrates remains a primary barri-er to care.
1Haemonetics Corporation, 400 Wood Road, Braintree, Massachusetts, 02184; 2Dana Farber/Boston Children’s Cancer and Blood Disorders Center and Harvard MedicalSchool, 450 Brookline Ave, Dana 3, Boston, Massachusetts, 02215
Disclosures: Dr. Hartmann is a Vice President and the Head of Strategic Programs at Haemonetics. Previously he was an Associate Partner in the global Med-ical Affairs practice at McKinsey & Co., Inc., where he led the hemophilia disease area team at the time of authoring this manuscript. During the last 2 yearswhile at McKinsey, Dr. Hartmann did not work directly on any hemophilia or bleeding disorder projects for products or manufacturers discussed in thisreview.Dr. Croteau has served as a consultant to Bayer, Baxalta, CSL-Behring, Dimension Therapeutics, Emergent Biosciences, Novo Nordisk, Pfizer, and Octapharma.Her institution receives research funding from Baxalta, Dimension Therapeutics, Hoffmann-La Roche and Octapharma.*Correspondence to: S. E. Croteau; E-mail: [email protected] grant sponsor: National Hemophilia Foundation (NHF)-Baxter.Received for publication: 6 July 2016; Revised: 18 August 2016; Accepted: 24 August 2016Am. J. Hematol. 91:1252–1260, 2016.Published online: 26 August 2016 in Wiley Online Library (wileyonlinelibrary.com).DOI: 10.1002/ajh.24543
VC 2016 Wiley Periodicals, Inc.
1252 American Journal of Hematology, Vol. 91, No. 12, December 2016 doi:10.1002/ajh.24543
UPDATES IN CLINICAL TRIALS FOR HEMATOLOGICAL DISEASES AJHAJH
AJH Educational Material
2017 Clinical trials update: Innovations in hemophilia therapy
Jan Hartmann1 and Stacy E. Croteau2*
A surge in therapeutic clinical trials over recent years is paving the way for transformative treatment options forpatients with hemophilia. The introduction of recombinant factor concentrates in the early 1990s facilitated theuse of prophylactic replacement as standard care for hemophilia rather than on-demand treatment. This hasrevolutionized health outcomes for hemophilia patients, enabling participation in physical activities and reducingdebilitating, chronic joint damage. Challenges of prophylactic factor infusion include the frequency of infusionsneeded to maintain factor levels greater than 1%, patient adherence, reliable intravenous access, anddevelopment of neutralizing alloantibodies (“inhibitors”). Novel therapeutics seek to improve upon current factorconcentrates by several different mechanisms: (1) extending the half-life of circulating exogenous factor protein,(2) replacing the gene necessary for production of endogenous factor protein, (3) employing bispecific antibodytechnology to mimic the coagulation function of factor VIII, (4) disrupting anticoagulant proteins, such as tissuefactor pathway inhibitor (TFPI) or antithrombin (AT3) with antibodies, aptamers, or RNA interference technology.Emerging treatment options may reduce the frequency of (extended half-life products) or eliminate (genetherapy) the need for scheduled factor concentrate infusions, or provide a subcutaneous administration option(bispecific antibody, AT3, and TFPI targeting therapies). In addition, the nonfactor replacement strategies providea promising treatment option for patients with inhibitors, presently the greatest unmet medical need inhemophilia. This review highlights current and recently completed clinical trials that are driving a paradigm shiftin our approach to hemophilia care for patients with and without inhibitors.Am. J. Hematol. 91:1252–1260, 2016. VC 2016 Wiley Periodicals, Inc.
! EpidemiologyFactor VIII (FVIII) deficiency (Hemophilia A) and factor IX (FIX) deficiency (Hemophilia B) affect approximately 20,000 individuals in the U.S.and over 400,000 individuals globally. The incidence of these X-linked bleeding disorders is estimated at 1 in 5,000 and 1 in 30,000 male births,respectively, without racial or ethnic predilection [1]. Despite being rare diseases, Hemophilia A and B have a significant impact on patient healthoutcomes and national health economies. Severe hemophilia (factor level <1%) typically presents in male infants with either spontaneous bleedingevents or excessive bleeding/bruising with mild trauma such as circumcision, vaccination, or learning to ambulate. This phenotype can also, rarely,manifest in females as the result of Turner syndrome, skewed lionization, or compound heterozygous variants. In the absence of a family historyto prompt a diagnostic investigation, moderate disease (1–5%) or mild disease (5–50%) may only be diagnosed later in life following a hemostaticchallenge. The bleeding phenotype of “carriers” also warrants consideration. While many females may be asymptomatic, others will have factorlevels in the mild hemophilia range and may have clinically significant bleeding symptoms, such as heavy menstrual bleeding, post-procedure orpostpartum bleeding requiring treatment [2,3].
! Pathophysiology and Current Management of HemophiliaFVIII is a glycoprotein that serves as a co-factor to amplify the rate of FX activation by FIXa (serine protease). The absence or reduction of
FVIII or FIX results in impaired thrombin generation and clot formation. Over 4,000 pathogenic variants in FVIII and FIX genes have been iden-tified. The most common mutation in severe FVIII deficiency is intron 22 inversion; however, nonsense mutations, insertions/deletions, and othervariants also occur and result in absent or reduced functional protein. FIX deficiency more frequently results from point mutations (http://www.factorviii-db.org, http://www.factorix.org) [4].
Without factor replacement, bleed events for patients with hemophilia may be life threatening or result in chronic disability from recur-rent hemarthrosis and intramuscular bleeding [5]. Prophylactic factor concentrate replacement is now standard care for adult andpediatric patients with severe hemophilia [6–8]. Unfortunately, in much of the world access to factor concentrates remains a primary barri-er to care.
1Haemonetics Corporation, 400 Wood Road, Braintree, Massachusetts, 02184; 2Dana Farber/Boston Children’s Cancer and Blood Disorders Center and Harvard MedicalSchool, 450 Brookline Ave, Dana 3, Boston, Massachusetts, 02215
Disclosures: Dr. Hartmann is a Vice President and the Head of Strategic Programs at Haemonetics. Previously he was an Associate Partner in the global Med-ical Affairs practice at McKinsey & Co., Inc., where he led the hemophilia disease area team at the time of authoring this manuscript. During the last 2 yearswhile at McKinsey, Dr. Hartmann did not work directly on any hemophilia or bleeding disorder projects for products or manufacturers discussed in thisreview.Dr. Croteau has served as a consultant to Bayer, Baxalta, CSL-Behring, Dimension Therapeutics, Emergent Biosciences, Novo Nordisk, Pfizer, and Octapharma.Her institution receives research funding from Baxalta, Dimension Therapeutics, Hoffmann-La Roche and Octapharma.*Correspondence to: S. E. Croteau; E-mail: [email protected] grant sponsor: National Hemophilia Foundation (NHF)-Baxter.Received for publication: 6 July 2016; Revised: 18 August 2016; Accepted: 24 August 2016Am. J. Hematol. 91:1252–1260, 2016.Published online: 26 August 2016 in Wiley Online Library (wileyonlinelibrary.com).DOI: 10.1002/ajh.24543
VC 2016 Wiley Periodicals, Inc.
1252 American Journal of Hematology, Vol. 91, No. 12, December 2016 doi:10.1002/ajh.24543
UPDATES IN CLINICAL TRIALS FOR HEMATOLOGICAL DISEASES AJHAJH

AJH Educational Material
2017 Clinical trials update: Innovations in hemophilia therapy
Jan Hartmann1 and Stacy E. Croteau2*
A surge in therapeutic clinical trials over recent years is paving the way for transformative treatment options forpatients with hemophilia. The introduction of recombinant factor concentrates in the early 1990s facilitated theuse of prophylactic replacement as standard care for hemophilia rather than on-demand treatment. This hasrevolutionized health outcomes for hemophilia patients, enabling participation in physical activities and reducingdebilitating, chronic joint damage. Challenges of prophylactic factor infusion include the frequency of infusionsneeded to maintain factor levels greater than 1%, patient adherence, reliable intravenous access, anddevelopment of neutralizing alloantibodies (“inhibitors”). Novel therapeutics seek to improve upon current factorconcentrates by several different mechanisms: (1) extending the half-life of circulating exogenous factor protein,(2) replacing the gene necessary for production of endogenous factor protein, (3) employing bispecific antibodytechnology to mimic the coagulation function of factor VIII, (4) disrupting anticoagulant proteins, such as tissuefactor pathway inhibitor (TFPI) or antithrombin (AT3) with antibodies, aptamers, or RNA interference technology.Emerging treatment options may reduce the frequency of (extended half-life products) or eliminate (genetherapy) the need for scheduled factor concentrate infusions, or provide a subcutaneous administration option(bispecific antibody, AT3, and TFPI targeting therapies). In addition, the nonfactor replacement strategies providea promising treatment option for patients with inhibitors, presently the greatest unmet medical need inhemophilia. This review highlights current and recently completed clinical trials that are driving a paradigm shiftin our approach to hemophilia care for patients with and without inhibitors.Am. J. Hematol. 91:1252–1260, 2016. VC 2016 Wiley Periodicals, Inc.
! EpidemiologyFactor VIII (FVIII) deficiency (Hemophilia A) and factor IX (FIX) deficiency (Hemophilia B) affect approximately 20,000 individuals in the U.S.and over 400,000 individuals globally. The incidence of these X-linked bleeding disorders is estimated at 1 in 5,000 and 1 in 30,000 male births,respectively, without racial or ethnic predilection [1]. Despite being rare diseases, Hemophilia A and B have a significant impact on patient healthoutcomes and national health economies. Severe hemophilia (factor level <1%) typically presents in male infants with either spontaneous bleedingevents or excessive bleeding/bruising with mild trauma such as circumcision, vaccination, or learning to ambulate. This phenotype can also, rarely,manifest in females as the result of Turner syndrome, skewed lionization, or compound heterozygous variants. In the absence of a family historyto prompt a diagnostic investigation, moderate disease (1–5%) or mild disease (5–50%) may only be diagnosed later in life following a hemostaticchallenge. The bleeding phenotype of “carriers” also warrants consideration. While many females may be asymptomatic, others will have factorlevels in the mild hemophilia range and may have clinically significant bleeding symptoms, such as heavy menstrual bleeding, post-procedure orpostpartum bleeding requiring treatment [2,3].
! Pathophysiology and Current Management of HemophiliaFVIII is a glycoprotein that serves as a co-factor to amplify the rate of FX activation by FIXa (serine protease). The absence or reduction of
FVIII or FIX results in impaired thrombin generation and clot formation. Over 4,000 pathogenic variants in FVIII and FIX genes have been iden-tified. The most common mutation in severe FVIII deficiency is intron 22 inversion; however, nonsense mutations, insertions/deletions, and othervariants also occur and result in absent or reduced functional protein. FIX deficiency more frequently results from point mutations (http://www.factorviii-db.org, http://www.factorix.org) [4].
Without factor replacement, bleed events for patients with hemophilia may be life threatening or result in chronic disability from recur-rent hemarthrosis and intramuscular bleeding [5]. Prophylactic factor concentrate replacement is now standard care for adult andpediatric patients with severe hemophilia [6–8]. Unfortunately, in much of the world access to factor concentrates remains a primary barri-er to care.
1Haemonetics Corporation, 400 Wood Road, Braintree, Massachusetts, 02184; 2Dana Farber/Boston Children’s Cancer and Blood Disorders Center and Harvard MedicalSchool, 450 Brookline Ave, Dana 3, Boston, Massachusetts, 02215
Disclosures: Dr. Hartmann is a Vice President and the Head of Strategic Programs at Haemonetics. Previously he was an Associate Partner in the global Med-ical Affairs practice at McKinsey & Co., Inc., where he led the hemophilia disease area team at the time of authoring this manuscript. During the last 2 yearswhile at McKinsey, Dr. Hartmann did not work directly on any hemophilia or bleeding disorder projects for products or manufacturers discussed in thisreview.Dr. Croteau has served as a consultant to Bayer, Baxalta, CSL-Behring, Dimension Therapeutics, Emergent Biosciences, Novo Nordisk, Pfizer, and Octapharma.Her institution receives research funding from Baxalta, Dimension Therapeutics, Hoffmann-La Roche and Octapharma.*Correspondence to: S. E. Croteau; E-mail: [email protected] grant sponsor: National Hemophilia Foundation (NHF)-Baxter.Received for publication: 6 July 2016; Revised: 18 August 2016; Accepted: 24 August 2016Am. J. Hematol. 91:1252–1260, 2016.Published online: 26 August 2016 in Wiley Online Library (wileyonlinelibrary.com).DOI: 10.1002/ajh.24543
VC 2016 Wiley Periodicals, Inc.
1252 American Journal of Hematology, Vol. 91, No. 12, December 2016 doi:10.1002/ajh.24543
UPDATES IN CLINICAL TRIALS FOR HEMATOLOGICAL DISEASES AJHAJHAJH Educational Material
2017 Clinical trials update: Innovations in hemophilia therapy
Jan Hartmann1 and Stacy E. Croteau2*
A surge in therapeutic clinical trials over recent years is paving the way for transformative treatment options forpatients with hemophilia. The introduction of recombinant factor concentrates in the early 1990s facilitated theuse of prophylactic replacement as standard care for hemophilia rather than on-demand treatment. This hasrevolutionized health outcomes for hemophilia patients, enabling participation in physical activities and reducingdebilitating, chronic joint damage. Challenges of prophylactic factor infusion include the frequency of infusionsneeded to maintain factor levels greater than 1%, patient adherence, reliable intravenous access, anddevelopment of neutralizing alloantibodies (“inhibitors”). Novel therapeutics seek to improve upon current factorconcentrates by several different mechanisms: (1) extending the half-life of circulating exogenous factor protein,(2) replacing the gene necessary for production of endogenous factor protein, (3) employing bispecific antibodytechnology to mimic the coagulation function of factor VIII, (4) disrupting anticoagulant proteins, such as tissuefactor pathway inhibitor (TFPI) or antithrombin (AT3) with antibodies, aptamers, or RNA interference technology.Emerging treatment options may reduce the frequency of (extended half-life products) or eliminate (genetherapy) the need for scheduled factor concentrate infusions, or provide a subcutaneous administration option(bispecific antibody, AT3, and TFPI targeting therapies). In addition, the nonfactor replacement strategies providea promising treatment option for patients with inhibitors, presently the greatest unmet medical need inhemophilia. This review highlights current and recently completed clinical trials that are driving a paradigm shiftin our approach to hemophilia care for patients with and without inhibitors.Am. J. Hematol. 91:1252–1260, 2016. VC 2016 Wiley Periodicals, Inc.
! EpidemiologyFactor VIII (FVIII) deficiency (Hemophilia A) and factor IX (FIX) deficiency (Hemophilia B) affect approximately 20,000 individuals in the U.S.and over 400,000 individuals globally. The incidence of these X-linked bleeding disorders is estimated at 1 in 5,000 and 1 in 30,000 male births,respectively, without racial or ethnic predilection [1]. Despite being rare diseases, Hemophilia A and B have a significant impact on patient healthoutcomes and national health economies. Severe hemophilia (factor level <1%) typically presents in male infants with either spontaneous bleedingevents or excessive bleeding/bruising with mild trauma such as circumcision, vaccination, or learning to ambulate. This phenotype can also, rarely,manifest in females as the result of Turner syndrome, skewed lionization, or compound heterozygous variants. In the absence of a family historyto prompt a diagnostic investigation, moderate disease (1–5%) or mild disease (5–50%) may only be diagnosed later in life following a hemostaticchallenge. The bleeding phenotype of “carriers” also warrants consideration. While many females may be asymptomatic, others will have factorlevels in the mild hemophilia range and may have clinically significant bleeding symptoms, such as heavy menstrual bleeding, post-procedure orpostpartum bleeding requiring treatment [2,3].
! Pathophysiology and Current Management of HemophiliaFVIII is a glycoprotein that serves as a co-factor to amplify the rate of FX activation by FIXa (serine protease). The absence or reduction of
FVIII or FIX results in impaired thrombin generation and clot formation. Over 4,000 pathogenic variants in FVIII and FIX genes have been iden-tified. The most common mutation in severe FVIII deficiency is intron 22 inversion; however, nonsense mutations, insertions/deletions, and othervariants also occur and result in absent or reduced functional protein. FIX deficiency more frequently results from point mutations (http://www.factorviii-db.org, http://www.factorix.org) [4].
Without factor replacement, bleed events for patients with hemophilia may be life threatening or result in chronic disability from recur-rent hemarthrosis and intramuscular bleeding [5]. Prophylactic factor concentrate replacement is now standard care for adult andpediatric patients with severe hemophilia [6–8]. Unfortunately, in much of the world access to factor concentrates remains a primary barri-er to care.
1Haemonetics Corporation, 400 Wood Road, Braintree, Massachusetts, 02184; 2Dana Farber/Boston Children’s Cancer and Blood Disorders Center and Harvard MedicalSchool, 450 Brookline Ave, Dana 3, Boston, Massachusetts, 02215
Disclosures: Dr. Hartmann is a Vice President and the Head of Strategic Programs at Haemonetics. Previously he was an Associate Partner in the global Med-ical Affairs practice at McKinsey & Co., Inc., where he led the hemophilia disease area team at the time of authoring this manuscript. During the last 2 yearswhile at McKinsey, Dr. Hartmann did not work directly on any hemophilia or bleeding disorder projects for products or manufacturers discussed in thisreview.Dr. Croteau has served as a consultant to Bayer, Baxalta, CSL-Behring, Dimension Therapeutics, Emergent Biosciences, Novo Nordisk, Pfizer, and Octapharma.Her institution receives research funding from Baxalta, Dimension Therapeutics, Hoffmann-La Roche and Octapharma.*Correspondence to: S. E. Croteau; E-mail: [email protected] grant sponsor: National Hemophilia Foundation (NHF)-Baxter.Received for publication: 6 July 2016; Revised: 18 August 2016; Accepted: 24 August 2016Am. J. Hematol. 91:1252–1260, 2016.Published online: 26 August 2016 in Wiley Online Library (wileyonlinelibrary.com).DOI: 10.1002/ajh.24543
VC 2016 Wiley Periodicals, Inc.
1252 American Journal of Hematology, Vol. 91, No. 12, December 2016 doi:10.1002/ajh.24543
UPDATES IN CLINICAL TRIALS FOR HEMATOLOGICAL DISEASES AJHAJH
AJH Educational Material
2017 Clinical trials update: Innovations in hemophilia therapy
Jan Hartmann1 and Stacy E. Croteau2*
A surge in therapeutic clinical trials over recent years is paving the way for transformative treatment options forpatients with hemophilia. The introduction of recombinant factor concentrates in the early 1990s facilitated theuse of prophylactic replacement as standard care for hemophilia rather than on-demand treatment. This hasrevolutionized health outcomes for hemophilia patients, enabling participation in physical activities and reducingdebilitating, chronic joint damage. Challenges of prophylactic factor infusion include the frequency of infusionsneeded to maintain factor levels greater than 1%, patient adherence, reliable intravenous access, anddevelopment of neutralizing alloantibodies (“inhibitors”). Novel therapeutics seek to improve upon current factorconcentrates by several different mechanisms: (1) extending the half-life of circulating exogenous factor protein,(2) replacing the gene necessary for production of endogenous factor protein, (3) employing bispecific antibodytechnology to mimic the coagulation function of factor VIII, (4) disrupting anticoagulant proteins, such as tissuefactor pathway inhibitor (TFPI) or antithrombin (AT3) with antibodies, aptamers, or RNA interference technology.Emerging treatment options may reduce the frequency of (extended half-life products) or eliminate (genetherapy) the need for scheduled factor concentrate infusions, or provide a subcutaneous administration option(bispecific antibody, AT3, and TFPI targeting therapies). In addition, the nonfactor replacement strategies providea promising treatment option for patients with inhibitors, presently the greatest unmet medical need inhemophilia. This review highlights current and recently completed clinical trials that are driving a paradigm shiftin our approach to hemophilia care for patients with and without inhibitors.Am. J. Hematol. 91:1252–1260, 2016. VC 2016 Wiley Periodicals, Inc.
! EpidemiologyFactor VIII (FVIII) deficiency (Hemophilia A) and factor IX (FIX) deficiency (Hemophilia B) affect approximately 20,000 individuals in the U.S.and over 400,000 individuals globally. The incidence of these X-linked bleeding disorders is estimated at 1 in 5,000 and 1 in 30,000 male births,respectively, without racial or ethnic predilection [1]. Despite being rare diseases, Hemophilia A and B have a significant impact on patient healthoutcomes and national health economies. Severe hemophilia (factor level <1%) typically presents in male infants with either spontaneous bleedingevents or excessive bleeding/bruising with mild trauma such as circumcision, vaccination, or learning to ambulate. This phenotype can also, rarely,manifest in females as the result of Turner syndrome, skewed lionization, or compound heterozygous variants. In the absence of a family historyto prompt a diagnostic investigation, moderate disease (1–5%) or mild disease (5–50%) may only be diagnosed later in life following a hemostaticchallenge. The bleeding phenotype of “carriers” also warrants consideration. While many females may be asymptomatic, others will have factorlevels in the mild hemophilia range and may have clinically significant bleeding symptoms, such as heavy menstrual bleeding, post-procedure orpostpartum bleeding requiring treatment [2,3].
! Pathophysiology and Current Management of HemophiliaFVIII is a glycoprotein that serves as a co-factor to amplify the rate of FX activation by FIXa (serine protease). The absence or reduction of
FVIII or FIX results in impaired thrombin generation and clot formation. Over 4,000 pathogenic variants in FVIII and FIX genes have been iden-tified. The most common mutation in severe FVIII deficiency is intron 22 inversion; however, nonsense mutations, insertions/deletions, and othervariants also occur and result in absent or reduced functional protein. FIX deficiency more frequently results from point mutations (http://www.factorviii-db.org, http://www.factorix.org) [4].
Without factor replacement, bleed events for patients with hemophilia may be life threatening or result in chronic disability from recur-rent hemarthrosis and intramuscular bleeding [5]. Prophylactic factor concentrate replacement is now standard care for adult andpediatric patients with severe hemophilia [6–8]. Unfortunately, in much of the world access to factor concentrates remains a primary barri-er to care.
1Haemonetics Corporation, 400 Wood Road, Braintree, Massachusetts, 02184; 2Dana Farber/Boston Children’s Cancer and Blood Disorders Center and Harvard MedicalSchool, 450 Brookline Ave, Dana 3, Boston, Massachusetts, 02215
Disclosures: Dr. Hartmann is a Vice President and the Head of Strategic Programs at Haemonetics. Previously he was an Associate Partner in the global Med-ical Affairs practice at McKinsey & Co., Inc., where he led the hemophilia disease area team at the time of authoring this manuscript. During the last 2 yearswhile at McKinsey, Dr. Hartmann did not work directly on any hemophilia or bleeding disorder projects for products or manufacturers discussed in thisreview.Dr. Croteau has served as a consultant to Bayer, Baxalta, CSL-Behring, Dimension Therapeutics, Emergent Biosciences, Novo Nordisk, Pfizer, and Octapharma.Her institution receives research funding from Baxalta, Dimension Therapeutics, Hoffmann-La Roche and Octapharma.*Correspondence to: S. E. Croteau; E-mail: [email protected] grant sponsor: National Hemophilia Foundation (NHF)-Baxter.Received for publication: 6 July 2016; Revised: 18 August 2016; Accepted: 24 August 2016Am. J. Hematol. 91:1252–1260, 2016.Published online: 26 August 2016 in Wiley Online Library (wileyonlinelibrary.com).DOI: 10.1002/ajh.24543
VC 2016 Wiley Periodicals, Inc.
1252 American Journal of Hematology, Vol. 91, No. 12, December 2016 doi:10.1002/ajh.24543
UPDATES IN CLINICAL TRIALS FOR HEMATOLOGICAL DISEASES AJHAJH
" Cell-based approach to gene therapy for hemophiliauses Len=viral vectors and several cell types : liversinusoidal endothelial cells, stem cells derived frombone marrow, blood-outgrowth endothelial cells, andendothelialprogenitorcells
" It requires cytoabla=ve agents to create a niche forhematopoie=cstemcellstransducedexvivo→harm?
" TrialsonlyininmurinemodelsofHAwithinhibitors" Useofplatelet-specificpromotersenablesexpressionof
FVIII within theα-granules of platelets→ delivery atthesiteofhemosta=cneed

Buscar el levante por el poniente… Cristoforo Colombo

AJH Educational Material
2017 Clinical trials update: Innovations in hemophilia therapy
Jan Hartmann1 and Stacy E. Croteau2*
A surge in therapeutic clinical trials over recent years is paving the way for transformative treatment options forpatients with hemophilia. The introduction of recombinant factor concentrates in the early 1990s facilitated theuse of prophylactic replacement as standard care for hemophilia rather than on-demand treatment. This hasrevolutionized health outcomes for hemophilia patients, enabling participation in physical activities and reducingdebilitating, chronic joint damage. Challenges of prophylactic factor infusion include the frequency of infusionsneeded to maintain factor levels greater than 1%, patient adherence, reliable intravenous access, anddevelopment of neutralizing alloantibodies (“inhibitors”). Novel therapeutics seek to improve upon current factorconcentrates by several different mechanisms: (1) extending the half-life of circulating exogenous factor protein,(2) replacing the gene necessary for production of endogenous factor protein, (3) employing bispecific antibodytechnology to mimic the coagulation function of factor VIII, (4) disrupting anticoagulant proteins, such as tissuefactor pathway inhibitor (TFPI) or antithrombin (AT3) with antibodies, aptamers, or RNA interference technology.Emerging treatment options may reduce the frequency of (extended half-life products) or eliminate (genetherapy) the need for scheduled factor concentrate infusions, or provide a subcutaneous administration option(bispecific antibody, AT3, and TFPI targeting therapies). In addition, the nonfactor replacement strategies providea promising treatment option for patients with inhibitors, presently the greatest unmet medical need inhemophilia. This review highlights current and recently completed clinical trials that are driving a paradigm shiftin our approach to hemophilia care for patients with and without inhibitors.Am. J. Hematol. 91:1252–1260, 2016. VC 2016 Wiley Periodicals, Inc.
! EpidemiologyFactor VIII (FVIII) deficiency (Hemophilia A) and factor IX (FIX) deficiency (Hemophilia B) affect approximately 20,000 individuals in the U.S.and over 400,000 individuals globally. The incidence of these X-linked bleeding disorders is estimated at 1 in 5,000 and 1 in 30,000 male births,respectively, without racial or ethnic predilection [1]. Despite being rare diseases, Hemophilia A and B have a significant impact on patient healthoutcomes and national health economies. Severe hemophilia (factor level <1%) typically presents in male infants with either spontaneous bleedingevents or excessive bleeding/bruising with mild trauma such as circumcision, vaccination, or learning to ambulate. This phenotype can also, rarely,manifest in females as the result of Turner syndrome, skewed lionization, or compound heterozygous variants. In the absence of a family historyto prompt a diagnostic investigation, moderate disease (1–5%) or mild disease (5–50%) may only be diagnosed later in life following a hemostaticchallenge. The bleeding phenotype of “carriers” also warrants consideration. While many females may be asymptomatic, others will have factorlevels in the mild hemophilia range and may have clinically significant bleeding symptoms, such as heavy menstrual bleeding, post-procedure orpostpartum bleeding requiring treatment [2,3].
! Pathophysiology and Current Management of HemophiliaFVIII is a glycoprotein that serves as a co-factor to amplify the rate of FX activation by FIXa (serine protease). The absence or reduction of
FVIII or FIX results in impaired thrombin generation and clot formation. Over 4,000 pathogenic variants in FVIII and FIX genes have been iden-tified. The most common mutation in severe FVIII deficiency is intron 22 inversion; however, nonsense mutations, insertions/deletions, and othervariants also occur and result in absent or reduced functional protein. FIX deficiency more frequently results from point mutations (http://www.factorviii-db.org, http://www.factorix.org) [4].
Without factor replacement, bleed events for patients with hemophilia may be life threatening or result in chronic disability from recur-rent hemarthrosis and intramuscular bleeding [5]. Prophylactic factor concentrate replacement is now standard care for adult andpediatric patients with severe hemophilia [6–8]. Unfortunately, in much of the world access to factor concentrates remains a primary barri-er to care.
1Haemonetics Corporation, 400 Wood Road, Braintree, Massachusetts, 02184; 2Dana Farber/Boston Children’s Cancer and Blood Disorders Center and Harvard MedicalSchool, 450 Brookline Ave, Dana 3, Boston, Massachusetts, 02215
Disclosures: Dr. Hartmann is a Vice President and the Head of Strategic Programs at Haemonetics. Previously he was an Associate Partner in the global Med-ical Affairs practice at McKinsey & Co., Inc., where he led the hemophilia disease area team at the time of authoring this manuscript. During the last 2 yearswhile at McKinsey, Dr. Hartmann did not work directly on any hemophilia or bleeding disorder projects for products or manufacturers discussed in thisreview.Dr. Croteau has served as a consultant to Bayer, Baxalta, CSL-Behring, Dimension Therapeutics, Emergent Biosciences, Novo Nordisk, Pfizer, and Octapharma.Her institution receives research funding from Baxalta, Dimension Therapeutics, Hoffmann-La Roche and Octapharma.*Correspondence to: S. E. Croteau; E-mail: [email protected] grant sponsor: National Hemophilia Foundation (NHF)-Baxter.Received for publication: 6 July 2016; Revised: 18 August 2016; Accepted: 24 August 2016Am. J. Hematol. 91:1252–1260, 2016.Published online: 26 August 2016 in Wiley Online Library (wileyonlinelibrary.com).DOI: 10.1002/ajh.24543
VC 2016 Wiley Periodicals, Inc.
1252 American Journal of Hematology, Vol. 91, No. 12, December 2016 doi:10.1002/ajh.24543
UPDATES IN CLINICAL TRIALS FOR HEMATOLOGICAL DISEASES AJHAJHAJH Educational Material
2017 Clinical trials update: Innovations in hemophilia therapy
Jan Hartmann1 and Stacy E. Croteau2*
A surge in therapeutic clinical trials over recent years is paving the way for transformative treatment options forpatients with hemophilia. The introduction of recombinant factor concentrates in the early 1990s facilitated theuse of prophylactic replacement as standard care for hemophilia rather than on-demand treatment. This hasrevolutionized health outcomes for hemophilia patients, enabling participation in physical activities and reducingdebilitating, chronic joint damage. Challenges of prophylactic factor infusion include the frequency of infusionsneeded to maintain factor levels greater than 1%, patient adherence, reliable intravenous access, anddevelopment of neutralizing alloantibodies (“inhibitors”). Novel therapeutics seek to improve upon current factorconcentrates by several different mechanisms: (1) extending the half-life of circulating exogenous factor protein,(2) replacing the gene necessary for production of endogenous factor protein, (3) employing bispecific antibodytechnology to mimic the coagulation function of factor VIII, (4) disrupting anticoagulant proteins, such as tissuefactor pathway inhibitor (TFPI) or antithrombin (AT3) with antibodies, aptamers, or RNA interference technology.Emerging treatment options may reduce the frequency of (extended half-life products) or eliminate (genetherapy) the need for scheduled factor concentrate infusions, or provide a subcutaneous administration option(bispecific antibody, AT3, and TFPI targeting therapies). In addition, the nonfactor replacement strategies providea promising treatment option for patients with inhibitors, presently the greatest unmet medical need inhemophilia. This review highlights current and recently completed clinical trials that are driving a paradigm shiftin our approach to hemophilia care for patients with and without inhibitors.Am. J. Hematol. 91:1252–1260, 2016. VC 2016 Wiley Periodicals, Inc.
! EpidemiologyFactor VIII (FVIII) deficiency (Hemophilia A) and factor IX (FIX) deficiency (Hemophilia B) affect approximately 20,000 individuals in the U.S.and over 400,000 individuals globally. The incidence of these X-linked bleeding disorders is estimated at 1 in 5,000 and 1 in 30,000 male births,respectively, without racial or ethnic predilection [1]. Despite being rare diseases, Hemophilia A and B have a significant impact on patient healthoutcomes and national health economies. Severe hemophilia (factor level <1%) typically presents in male infants with either spontaneous bleedingevents or excessive bleeding/bruising with mild trauma such as circumcision, vaccination, or learning to ambulate. This phenotype can also, rarely,manifest in females as the result of Turner syndrome, skewed lionization, or compound heterozygous variants. In the absence of a family historyto prompt a diagnostic investigation, moderate disease (1–5%) or mild disease (5–50%) may only be diagnosed later in life following a hemostaticchallenge. The bleeding phenotype of “carriers” also warrants consideration. While many females may be asymptomatic, others will have factorlevels in the mild hemophilia range and may have clinically significant bleeding symptoms, such as heavy menstrual bleeding, post-procedure orpostpartum bleeding requiring treatment [2,3].
! Pathophysiology and Current Management of HemophiliaFVIII is a glycoprotein that serves as a co-factor to amplify the rate of FX activation by FIXa (serine protease). The absence or reduction of
FVIII or FIX results in impaired thrombin generation and clot formation. Over 4,000 pathogenic variants in FVIII and FIX genes have been iden-tified. The most common mutation in severe FVIII deficiency is intron 22 inversion; however, nonsense mutations, insertions/deletions, and othervariants also occur and result in absent or reduced functional protein. FIX deficiency more frequently results from point mutations (http://www.factorviii-db.org, http://www.factorix.org) [4].
Without factor replacement, bleed events for patients with hemophilia may be life threatening or result in chronic disability from recur-rent hemarthrosis and intramuscular bleeding [5]. Prophylactic factor concentrate replacement is now standard care for adult andpediatric patients with severe hemophilia [6–8]. Unfortunately, in much of the world access to factor concentrates remains a primary barri-er to care.
1Haemonetics Corporation, 400 Wood Road, Braintree, Massachusetts, 02184; 2Dana Farber/Boston Children’s Cancer and Blood Disorders Center and Harvard MedicalSchool, 450 Brookline Ave, Dana 3, Boston, Massachusetts, 02215
Disclosures: Dr. Hartmann is a Vice President and the Head of Strategic Programs at Haemonetics. Previously he was an Associate Partner in the global Med-ical Affairs practice at McKinsey & Co., Inc., where he led the hemophilia disease area team at the time of authoring this manuscript. During the last 2 yearswhile at McKinsey, Dr. Hartmann did not work directly on any hemophilia or bleeding disorder projects for products or manufacturers discussed in thisreview.Dr. Croteau has served as a consultant to Bayer, Baxalta, CSL-Behring, Dimension Therapeutics, Emergent Biosciences, Novo Nordisk, Pfizer, and Octapharma.Her institution receives research funding from Baxalta, Dimension Therapeutics, Hoffmann-La Roche and Octapharma.*Correspondence to: S. E. Croteau; E-mail: [email protected] grant sponsor: National Hemophilia Foundation (NHF)-Baxter.Received for publication: 6 July 2016; Revised: 18 August 2016; Accepted: 24 August 2016Am. J. Hematol. 91:1252–1260, 2016.Published online: 26 August 2016 in Wiley Online Library (wileyonlinelibrary.com).DOI: 10.1002/ajh.24543
VC 2016 Wiley Periodicals, Inc.
1252 American Journal of Hematology, Vol. 91, No. 12, December 2016 doi:10.1002/ajh.24543
UPDATES IN CLINICAL TRIALS FOR HEMATOLOGICAL DISEASES AJHAJH
AJH Educational Material
2017 Clinical trials update: Innovations in hemophilia therapy
Jan Hartmann1 and Stacy E. Croteau2*
A surge in therapeutic clinical trials over recent years is paving the way for transformative treatment options forpatients with hemophilia. The introduction of recombinant factor concentrates in the early 1990s facilitated theuse of prophylactic replacement as standard care for hemophilia rather than on-demand treatment. This hasrevolutionized health outcomes for hemophilia patients, enabling participation in physical activities and reducingdebilitating, chronic joint damage. Challenges of prophylactic factor infusion include the frequency of infusionsneeded to maintain factor levels greater than 1%, patient adherence, reliable intravenous access, anddevelopment of neutralizing alloantibodies (“inhibitors”). Novel therapeutics seek to improve upon current factorconcentrates by several different mechanisms: (1) extending the half-life of circulating exogenous factor protein,(2) replacing the gene necessary for production of endogenous factor protein, (3) employing bispecific antibodytechnology to mimic the coagulation function of factor VIII, (4) disrupting anticoagulant proteins, such as tissuefactor pathway inhibitor (TFPI) or antithrombin (AT3) with antibodies, aptamers, or RNA interference technology.Emerging treatment options may reduce the frequency of (extended half-life products) or eliminate (genetherapy) the need for scheduled factor concentrate infusions, or provide a subcutaneous administration option(bispecific antibody, AT3, and TFPI targeting therapies). In addition, the nonfactor replacement strategies providea promising treatment option for patients with inhibitors, presently the greatest unmet medical need inhemophilia. This review highlights current and recently completed clinical trials that are driving a paradigm shiftin our approach to hemophilia care for patients with and without inhibitors.Am. J. Hematol. 91:1252–1260, 2016. VC 2016 Wiley Periodicals, Inc.
! EpidemiologyFactor VIII (FVIII) deficiency (Hemophilia A) and factor IX (FIX) deficiency (Hemophilia B) affect approximately 20,000 individuals in the U.S.and over 400,000 individuals globally. The incidence of these X-linked bleeding disorders is estimated at 1 in 5,000 and 1 in 30,000 male births,respectively, without racial or ethnic predilection [1]. Despite being rare diseases, Hemophilia A and B have a significant impact on patient healthoutcomes and national health economies. Severe hemophilia (factor level <1%) typically presents in male infants with either spontaneous bleedingevents or excessive bleeding/bruising with mild trauma such as circumcision, vaccination, or learning to ambulate. This phenotype can also, rarely,manifest in females as the result of Turner syndrome, skewed lionization, or compound heterozygous variants. In the absence of a family historyto prompt a diagnostic investigation, moderate disease (1–5%) or mild disease (5–50%) may only be diagnosed later in life following a hemostaticchallenge. The bleeding phenotype of “carriers” also warrants consideration. While many females may be asymptomatic, others will have factorlevels in the mild hemophilia range and may have clinically significant bleeding symptoms, such as heavy menstrual bleeding, post-procedure orpostpartum bleeding requiring treatment [2,3].
! Pathophysiology and Current Management of HemophiliaFVIII is a glycoprotein that serves as a co-factor to amplify the rate of FX activation by FIXa (serine protease). The absence or reduction of
FVIII or FIX results in impaired thrombin generation and clot formation. Over 4,000 pathogenic variants in FVIII and FIX genes have been iden-tified. The most common mutation in severe FVIII deficiency is intron 22 inversion; however, nonsense mutations, insertions/deletions, and othervariants also occur and result in absent or reduced functional protein. FIX deficiency more frequently results from point mutations (http://www.factorviii-db.org, http://www.factorix.org) [4].
Without factor replacement, bleed events for patients with hemophilia may be life threatening or result in chronic disability from recur-rent hemarthrosis and intramuscular bleeding [5]. Prophylactic factor concentrate replacement is now standard care for adult andpediatric patients with severe hemophilia [6–8]. Unfortunately, in much of the world access to factor concentrates remains a primary barri-er to care.
1Haemonetics Corporation, 400 Wood Road, Braintree, Massachusetts, 02184; 2Dana Farber/Boston Children’s Cancer and Blood Disorders Center and Harvard MedicalSchool, 450 Brookline Ave, Dana 3, Boston, Massachusetts, 02215
Disclosures: Dr. Hartmann is a Vice President and the Head of Strategic Programs at Haemonetics. Previously he was an Associate Partner in the global Med-ical Affairs practice at McKinsey & Co., Inc., where he led the hemophilia disease area team at the time of authoring this manuscript. During the last 2 yearswhile at McKinsey, Dr. Hartmann did not work directly on any hemophilia or bleeding disorder projects for products or manufacturers discussed in thisreview.Dr. Croteau has served as a consultant to Bayer, Baxalta, CSL-Behring, Dimension Therapeutics, Emergent Biosciences, Novo Nordisk, Pfizer, and Octapharma.Her institution receives research funding from Baxalta, Dimension Therapeutics, Hoffmann-La Roche and Octapharma.*Correspondence to: S. E. Croteau; E-mail: [email protected] grant sponsor: National Hemophilia Foundation (NHF)-Baxter.Received for publication: 6 July 2016; Revised: 18 August 2016; Accepted: 24 August 2016Am. J. Hematol. 91:1252–1260, 2016.Published online: 26 August 2016 in Wiley Online Library (wileyonlinelibrary.com).DOI: 10.1002/ajh.24543
VC 2016 Wiley Periodicals, Inc.
1252 American Journal of Hematology, Vol. 91, No. 12, December 2016 doi:10.1002/ajh.24543
UPDATES IN CLINICAL TRIALS FOR HEMATOLOGICAL DISEASES AJHAJH
NonfactorReplacementStrategies:“DisrupTveTherapies”
# Emicizumab# Concizumab# APC-specificserpin
FVIII-specifichuman(CAR)T-regulatorycells

● ahumanizedbispecifican=body to factor IXa(FIXa)andfactorX(FX),termedhBS23
● restoresfactor=vityinmodel# ACE910 (emicizumab) is a
bispecificAbtoFIXaandFXthatmimicsthecofactorfunc=onofFVIII
# In non-human primate model:prolonged half-life and highsubcutaneousbioavailability
(Lillicrap et al Nat Med 2012;18:1460-61)
(hBS23)

● ahumanizedbispecifican=body to factor IXa(FIXa)andfactorX(FX),termedhBS23
● restoresfactor=vityinmodel
(Lillicrap et al Nat Med 2012;18:1460-61)
(hBS23)
subcutaneousemicizumabonceweekly


" Phase 1, mul=center, randomized, double-blind,placebocontrolledtrial
" Escala=ng single i.v. or s.c. doses of concizumabwere administered to 28 healthy volunteers and24hemophiliapa=ents

Results:" Concizumab had a favorable safety profile ajer
singlei.v.ors.c.administra=on" No serious adverse events nor an=-concizumab
an=bodieswerereported" Nonlinearpharmacokine=cswasobserveddueto
target-mediatedclearance." A concentra=on-dependent procoagulant effect
ofconcizumabwasobserved

Analterna=veapproachtohemophiliatreatmentselec=veinhibi=onofAPCTheendogenousinhibitorsofAPCaremembersoftheserpinfamily:proteinCinhibitor(PCI)anda1-an=trypsin(a1AT);however,bothexhibitpoorreac=vityandselec=vityforAPC.WemutatedresiduesinandaroundthescissileP1-P19bondinPCIanda1AT,resul=nginserpinswiththedesiredspecificityprofile.Theleadcandidatewasshowntopromotethrombingenera=oninvitroandtorestorefibrinandplateletdeposi=oninanintravitallaserinjurymodelinhemophiliaBmice.Thepoweroftarge=ngAPCwasfurtherdemonstratedbythecompletenormaliza=onofbleedingajeraseveretailclipinjuryinthesemice.TheseresultsdemonstratethattheproteinCan=coagulantsystemcanbesuccessfullytargetedbyengineeredserpinsandthatadministra=onofsuchagentsiseffec=veatrestoringhemostasisinvivo.
" An alterna=ve approach to hemophilia treatment isselec=veinhibi=onofAPC
" TheendogenousinhibitorsofAPCaremembersoftheserpin family: protein C inhibitor (PCI) and α1-an=trypsin (α1 AT); however, both exhibit poorreac=vityandselec=vityforAPC.
" The Authors mutated residues in and around thescissile P1-P19 bond in PCI and α1 AT, resul=ng inserpinswiththedesiredspecificityprofile.

Analterna=veapproachtohemophiliatreatmentselec=veinhibi=onofAPCTheendogenousinhibitorsofAPCaremembersoftheserpinfamily:proteinCinhibitor(PCI)anda1-an=trypsin(a1AT);however,bothexhibitpoorreac=vityandselec=vityforAPC.WemutatedresiduesinandaroundthescissileP1-P19bondinPCIanda1AT,resul=nginserpinswiththedesiredspecificityprofile.Theleadcandidatewasshowntopromotethrombingenera=oninvitroandtorestorefibrinandplateletdeposi=oninanintravitallaserinjurymodelinhemophiliaBmice.Thepoweroftarge=ngAPCwasfurtherdemonstratedbythecompletenormaliza=onofbleedingajeraseveretailclipinjuryinthesemice.TheseresultsdemonstratethattheproteinCan=coagulantsystemcanbesuccessfullytargetedbyengineeredserpinsandthatadministra=onofsuchagentsiseffec=veatrestoringhemostasisinvivo.

Regular Article
THROMBOSIS AND HEMOSTASIS
FVIII-specific human chimeric antigen receptor T-regulatory cellssuppress T- and B-cell responses to FVIIIJeongheon Yoon,1,* Anja Schmidt,2,* Ai-Hong Zhang,1 Christoph Konigs,2 Yong Chan Kim,1 and David W. Scott1
1Department of Medicine, Uniformed Services University of Health Sciences, Bethesda, MD; and 2Department of Pediatrics, Molecular Hemostasis and
Immunodeficiency, University Hospital Frankfurt, Goethe University, Frankfurt, Germany
Key Points
• Generation and functionalanalysis of FVIII-specifichuman CAR Tregs.
• Specific regulation of FVIIIresponses by engineeredhuman CAR Tregs.
Replacement therapy with factor VIII (FVIII) is used in patients with hemophilia A for
treatment of bleeding episodes or for prophylaxis. A common and serious problem with
this therapy is the patient’s immune response to FVIII, because of a lack of tolerance,
leading to the formation of inhibitory antibodies. Development of tolerogenic therapies,
other than standard immune tolerance induction (ITI), is an unmet goal. We previously
generatedengineeredantigen-specific regulatoryTcells (Tregs), createdby transduction
of a recombinantT-cell receptor (TCR) isolated fromahemophiliaAsubject’sT-cell clone.
The resultingengineeredTcellssuppressedbothT-andB-cell effector responses toFVIII.
In this study, we have engineered an FVIII-specific chimeric antigen receptor (ANS8CAR)
using a FVIII-specific scFv derived from a synthetic phage display library. Transduced ANS8 CAR T cells specific for the A2 domain
proliferated in response to FVIII and ANS8 CAR Tregs were able to suppress the proliferation of FVIII-specific T-effector cells with
specificity for a different FVIII domain in vitro. These data suggest that engineered cells are able to promote bystander suppression.
Importantly, ANS8 CAR-transduced Tregs also were able to suppress the recall antibody response of murine splenocytes from FVIII
knockout mice to FVIII in vitro and in vivo. In conclusion, CAR-transduced Tregs are a promising approach for future tolerogenic
treatment of hemophilia A patients with inhibitors. (Blood. 2017;129(2):238-245)
Introduction
Hemophilia A is an X-linked disorder, in which mutations in thecoagulationFactorVIII (FVIII) gene lead to a loss ofFVIII function andcan result in serious bleeding episodes. Although these episodes can betreated with recombinant or plasma-derived FVIII protein, unfortu-nately,;25% of hemophilia A patients produce inhibitory anti-FVIIIantibodies (inhibitors).1,2 Typically, these patients are treated withrepeated high doses of FVIII in a protocol termed immune toleranceinduction (ITI), a process that is expensive, time-consuming and notentirely effective. The development of effective tolerogenic therapies toprevent, as well as reverse, inhibitor formation is clearly needed.
Recently, regulatoryTcells (Tregs) have beenproposed as a potentialclinical therapy for a variety of adverse immune disorders, ranging fromautoimmune diseases to the development of antidrug antibodies, such asinhibitor formation to FVIII. Treg therapies have already been applied inclinical studies for prevention of graft-versus-host disease (GVHD).3,4
However, polyclonal Tregs encompass many specificities and couldpotentially be globally immunosuppressive. For example, results of aGVHD study suggest an increase in viral reactivation up to 30 days afteradoptive transfer of umbilical cord–derived polyclonal Tregs.5 Thus, theuse of antigen-specific Tregs seems to be preferable for the nextgeneration of Treg therapeutic approaches. Previously, we developed anapproach to render expanded polyclonal Tregs “specific” by transducingthem with a T-cell receptor (TCR) containing the variable genes from a
T-cell clone derived from a hemophilia A patient.6 These Tregs werehighly effective at suppressing both T- and B-cell responses to FVIII.However, TCR-transduced cells remain MHC-restricted. In contrast,chimeric antigen receptors (CARs) containing a single chain variablefragment (scFv) as the binding domain are not major histocompatibilitycomplex (MHC)-restricted and have been used to specifically direct thelytic functionofCD81Tcells against target cells formore thanadecade.7
Most recently,CARshavealsobeenapplied tocreate alloantigen-specificTregs that prevented xenogeneic GVHD in a mouse model.8
Thus, as an alternative to a FVIII-C2-peptide-specific TCR (called17195 TCR),6 we have now used a CAR containing a scFv isolatedfrom a phage library9 (termed ANS8 CAR) that recognizes the A2domain of FVIII. In this report, we characterize these FVIII-specificCAR Tregs and demonstrate their ability to inhibit T- and B-cellresponses to FVIII in vitro and in vivo.
Methods
Human blood samples and cells
Humanblood samples fromhealthy, anonymousmale donors ranging from20 to70 years of age were obtained with written consent from the Department of
Submitted 13 July 2016; accepted 8 November 2016. Prepublished online asBlood First Edition paper, 15 November 2016; DOI 10.1182/blood-2016-07-727834.
*J.Y. and A.S. contributed equally to this work.
The online version of this article contains a data supplement.
There is an Inside Blood Commentary on this article in this issue.
The publication costs of this article were defrayed in part by page chargepayment. Therefore, and solely to indicate this fact, this article is herebymarked “advertisement” in accordance with 18 USC section 1734.
238 BLOOD, 12 JANUARY 2017 x VOLUME 129, NUMBER 2
For personal use only.on May 18, 2017. by guest www.bloodjournal.orgFrom
Regular Article
THROMBOSIS AND HEMOSTASIS
FVIII-specific human chimeric antigen receptor T-regulatory cellssuppress T- and B-cell responses to FVIIIJeongheon Yoon,1,* Anja Schmidt,2,* Ai-Hong Zhang,1 Christoph Konigs,2 Yong Chan Kim,1 and David W. Scott1
1Department of Medicine, Uniformed Services University of Health Sciences, Bethesda, MD; and 2Department of Pediatrics, Molecular Hemostasis and
Immunodeficiency, University Hospital Frankfurt, Goethe University, Frankfurt, Germany
Key Points
• Generation and functionalanalysis of FVIII-specifichuman CAR Tregs.
• Specific regulation of FVIIIresponses by engineeredhuman CAR Tregs.
Replacement therapy with factor VIII (FVIII) is used in patients with hemophilia A for
treatment of bleeding episodes or for prophylaxis. A common and serious problem with
this therapy is the patient’s immune response to FVIII, because of a lack of tolerance,
leading to the formation of inhibitory antibodies. Development of tolerogenic therapies,
other than standard immune tolerance induction (ITI), is an unmet goal. We previously
generatedengineeredantigen-specific regulatoryTcells (Tregs), createdby transduction
of a recombinantT-cell receptor (TCR) isolated fromahemophiliaAsubject’sT-cell clone.
The resultingengineeredTcellssuppressedbothT-andB-cell effector responses toFVIII.
In this study, we have engineered an FVIII-specific chimeric antigen receptor (ANS8CAR)
using a FVIII-specific scFv derived from a synthetic phage display library. Transduced ANS8 CAR T cells specific for the A2 domain
proliferated in response to FVIII and ANS8 CAR Tregs were able to suppress the proliferation of FVIII-specific T-effector cells with
specificity for a different FVIII domain in vitro. These data suggest that engineered cells are able to promote bystander suppression.
Importantly, ANS8 CAR-transduced Tregs also were able to suppress the recall antibody response of murine splenocytes from FVIII
knockout mice to FVIII in vitro and in vivo. In conclusion, CAR-transduced Tregs are a promising approach for future tolerogenic
treatment of hemophilia A patients with inhibitors. (Blood. 2017;129(2):238-245)
Introduction
Hemophilia A is an X-linked disorder, in which mutations in thecoagulationFactorVIII (FVIII) gene lead to a loss ofFVIII function andcan result in serious bleeding episodes. Although these episodes can betreated with recombinant or plasma-derived FVIII protein, unfortu-nately,;25% of hemophilia A patients produce inhibitory anti-FVIIIantibodies (inhibitors).1,2 Typically, these patients are treated withrepeated high doses of FVIII in a protocol termed immune toleranceinduction (ITI), a process that is expensive, time-consuming and notentirely effective. The development of effective tolerogenic therapies toprevent, as well as reverse, inhibitor formation is clearly needed.
Recently, regulatoryTcells (Tregs) have beenproposed as a potentialclinical therapy for a variety of adverse immune disorders, ranging fromautoimmune diseases to the development of antidrug antibodies, such asinhibitor formation to FVIII. Treg therapies have already been applied inclinical studies for prevention of graft-versus-host disease (GVHD).3,4
However, polyclonal Tregs encompass many specificities and couldpotentially be globally immunosuppressive. For example, results of aGVHD study suggest an increase in viral reactivation up to 30 days afteradoptive transfer of umbilical cord–derived polyclonal Tregs.5 Thus, theuse of antigen-specific Tregs seems to be preferable for the nextgeneration of Treg therapeutic approaches. Previously, we developed anapproach to render expanded polyclonal Tregs “specific” by transducingthem with a T-cell receptor (TCR) containing the variable genes from a
T-cell clone derived from a hemophilia A patient.6 These Tregs werehighly effective at suppressing both T- and B-cell responses to FVIII.However, TCR-transduced cells remain MHC-restricted. In contrast,chimeric antigen receptors (CARs) containing a single chain variablefragment (scFv) as the binding domain are not major histocompatibilitycomplex (MHC)-restricted and have been used to specifically direct thelytic functionofCD81Tcells against target cells formore thanadecade.7
Most recently,CARshavealsobeenapplied tocreate alloantigen-specificTregs that prevented xenogeneic GVHD in a mouse model.8
Thus, as an alternative to a FVIII-C2-peptide-specific TCR (called17195 TCR),6 we have now used a CAR containing a scFv isolatedfrom a phage library9 (termed ANS8 CAR) that recognizes the A2domain of FVIII. In this report, we characterize these FVIII-specificCAR Tregs and demonstrate their ability to inhibit T- and B-cellresponses to FVIII in vitro and in vivo.
Methods
Human blood samples and cells
Humanblood samples fromhealthy, anonymousmale donors ranging from20 to70 years of age were obtained with written consent from the Department of
Submitted 13 July 2016; accepted 8 November 2016. Prepublished online asBlood First Edition paper, 15 November 2016; DOI 10.1182/blood-2016-07-727834.
*J.Y. and A.S. contributed equally to this work.
The online version of this article contains a data supplement.
There is an Inside Blood Commentary on this article in this issue.
The publication costs of this article were defrayed in part by page chargepayment. Therefore, and solely to indicate this fact, this article is herebymarked “advertisement” in accordance with 18 USC section 1734.
238 BLOOD, 12 JANUARY 2017 x VOLUME 129, NUMBER 2
For personal use only.on May 18, 2017. by guest www.bloodjournal.orgFrom
" In this study, an FVIII-specific chimeric an=gen receptor (ANS8CAR) was engineered using a FVIII-specific scFv derived from asynthe=cphagedisplaylibrary.
" Transduced ANS8 CAR T cells specific for the A2 domainproliferatedinresponsetoFVIIIandANS8CARTregswereabletosuppress the prolifera=on of FVIII-specific T effector cells withspecificityforadifferentFVIIIdomaininvitro.
" These data suggest that engineered cells are able to promotebystandersuppression
" Importantly, ANS8 CAR-transduced Tregs also were able tosuppresstherecallan=bodyresponseofmurinesplenocytesfromFVIIIknockoutmicetoFVIIIinvitroandinvivo.
" In conclusion, CAR-transduced Tregs are a promising approachfor future tolerogenic treatment of hemophiliaA pa:entswithinhibitors.

Regular Article
THROMBOSIS AND HEMOSTASIS
FVIII-specific human chimeric antigen receptor T-regulatory cellssuppress T- and B-cell responses to FVIIIJeongheon Yoon,1,* Anja Schmidt,2,* Ai-Hong Zhang,1 Christoph Konigs,2 Yong Chan Kim,1 and David W. Scott1
1Department of Medicine, Uniformed Services University of Health Sciences, Bethesda, MD; and 2Department of Pediatrics, Molecular Hemostasis and
Immunodeficiency, University Hospital Frankfurt, Goethe University, Frankfurt, Germany
Key Points
• Generation and functionalanalysis of FVIII-specifichuman CAR Tregs.
• Specific regulation of FVIIIresponses by engineeredhuman CAR Tregs.
Replacement therapy with factor VIII (FVIII) is used in patients with hemophilia A for
treatment of bleeding episodes or for prophylaxis. A common and serious problem with
this therapy is the patient’s immune response to FVIII, because of a lack of tolerance,
leading to the formation of inhibitory antibodies. Development of tolerogenic therapies,
other than standard immune tolerance induction (ITI), is an unmet goal. We previously
generatedengineeredantigen-specific regulatoryTcells (Tregs), createdby transduction
of a recombinantT-cell receptor (TCR) isolated fromahemophiliaAsubject’sT-cell clone.
The resultingengineeredTcellssuppressedbothT-andB-cell effector responses toFVIII.
In this study, we have engineered an FVIII-specific chimeric antigen receptor (ANS8CAR)
using a FVIII-specific scFv derived from a synthetic phage display library. Transduced ANS8 CAR T cells specific for the A2 domain
proliferated in response to FVIII and ANS8 CAR Tregs were able to suppress the proliferation of FVIII-specific T-effector cells with
specificity for a different FVIII domain in vitro. These data suggest that engineered cells are able to promote bystander suppression.
Importantly, ANS8 CAR-transduced Tregs also were able to suppress the recall antibody response of murine splenocytes from FVIII
knockout mice to FVIII in vitro and in vivo. In conclusion, CAR-transduced Tregs are a promising approach for future tolerogenic
treatment of hemophilia A patients with inhibitors. (Blood. 2017;129(2):238-245)
Introduction
Hemophilia A is an X-linked disorder, in which mutations in thecoagulationFactorVIII (FVIII) gene lead to a loss ofFVIII function andcan result in serious bleeding episodes. Although these episodes can betreated with recombinant or plasma-derived FVIII protein, unfortu-nately,;25% of hemophilia A patients produce inhibitory anti-FVIIIantibodies (inhibitors).1,2 Typically, these patients are treated withrepeated high doses of FVIII in a protocol termed immune toleranceinduction (ITI), a process that is expensive, time-consuming and notentirely effective. The development of effective tolerogenic therapies toprevent, as well as reverse, inhibitor formation is clearly needed.
Recently, regulatoryTcells (Tregs) have beenproposed as a potentialclinical therapy for a variety of adverse immune disorders, ranging fromautoimmune diseases to the development of antidrug antibodies, such asinhibitor formation to FVIII. Treg therapies have already been applied inclinical studies for prevention of graft-versus-host disease (GVHD).3,4
However, polyclonal Tregs encompass many specificities and couldpotentially be globally immunosuppressive. For example, results of aGVHD study suggest an increase in viral reactivation up to 30 days afteradoptive transfer of umbilical cord–derived polyclonal Tregs.5 Thus, theuse of antigen-specific Tregs seems to be preferable for the nextgeneration of Treg therapeutic approaches. Previously, we developed anapproach to render expanded polyclonal Tregs “specific” by transducingthem with a T-cell receptor (TCR) containing the variable genes from a
T-cell clone derived from a hemophilia A patient.6 These Tregs werehighly effective at suppressing both T- and B-cell responses to FVIII.However, TCR-transduced cells remain MHC-restricted. In contrast,chimeric antigen receptors (CARs) containing a single chain variablefragment (scFv) as the binding domain are not major histocompatibilitycomplex (MHC)-restricted and have been used to specifically direct thelytic functionofCD81Tcells against target cells formore thanadecade.7
Most recently,CARshavealsobeenapplied tocreate alloantigen-specificTregs that prevented xenogeneic GVHD in a mouse model.8
Thus, as an alternative to a FVIII-C2-peptide-specific TCR (called17195 TCR),6 we have now used a CAR containing a scFv isolatedfrom a phage library9 (termed ANS8 CAR) that recognizes the A2domain of FVIII. In this report, we characterize these FVIII-specificCAR Tregs and demonstrate their ability to inhibit T- and B-cellresponses to FVIII in vitro and in vivo.
Methods
Human blood samples and cells
Humanblood samples fromhealthy, anonymousmale donors ranging from20 to70 years of age were obtained with written consent from the Department of
Submitted 13 July 2016; accepted 8 November 2016. Prepublished online asBlood First Edition paper, 15 November 2016; DOI 10.1182/blood-2016-07-727834.
*J.Y. and A.S. contributed equally to this work.
The online version of this article contains a data supplement.
There is an Inside Blood Commentary on this article in this issue.
The publication costs of this article were defrayed in part by page chargepayment. Therefore, and solely to indicate this fact, this article is herebymarked “advertisement” in accordance with 18 USC section 1734.
238 BLOOD, 12 JANUARY 2017 x VOLUME 129, NUMBER 2
For personal use only.on May 18, 2017. by guest www.bloodjournal.orgFrom
Regular Article
THROMBOSIS AND HEMOSTASIS
FVIII-specific human chimeric antigen receptor T-regulatory cellssuppress T- and B-cell responses to FVIIIJeongheon Yoon,1,* Anja Schmidt,2,* Ai-Hong Zhang,1 Christoph Konigs,2 Yong Chan Kim,1 and David W. Scott1
1Department of Medicine, Uniformed Services University of Health Sciences, Bethesda, MD; and 2Department of Pediatrics, Molecular Hemostasis and
Immunodeficiency, University Hospital Frankfurt, Goethe University, Frankfurt, Germany
Key Points
• Generation and functionalanalysis of FVIII-specifichuman CAR Tregs.
• Specific regulation of FVIIIresponses by engineeredhuman CAR Tregs.
Replacement therapy with factor VIII (FVIII) is used in patients with hemophilia A for
treatment of bleeding episodes or for prophylaxis. A common and serious problem with
this therapy is the patient’s immune response to FVIII, because of a lack of tolerance,
leading to the formation of inhibitory antibodies. Development of tolerogenic therapies,
other than standard immune tolerance induction (ITI), is an unmet goal. We previously
generatedengineeredantigen-specific regulatoryTcells (Tregs), createdby transduction
of a recombinantT-cell receptor (TCR) isolated fromahemophiliaAsubject’sT-cell clone.
The resultingengineeredTcellssuppressedbothT-andB-cell effector responses toFVIII.
In this study, we have engineered an FVIII-specific chimeric antigen receptor (ANS8CAR)
using a FVIII-specific scFv derived from a synthetic phage display library. Transduced ANS8 CAR T cells specific for the A2 domain
proliferated in response to FVIII and ANS8 CAR Tregs were able to suppress the proliferation of FVIII-specific T-effector cells with
specificity for a different FVIII domain in vitro. These data suggest that engineered cells are able to promote bystander suppression.
Importantly, ANS8 CAR-transduced Tregs also were able to suppress the recall antibody response of murine splenocytes from FVIII
knockout mice to FVIII in vitro and in vivo. In conclusion, CAR-transduced Tregs are a promising approach for future tolerogenic
treatment of hemophilia A patients with inhibitors. (Blood. 2017;129(2):238-245)
Introduction
Hemophilia A is an X-linked disorder, in which mutations in thecoagulationFactorVIII (FVIII) gene lead to a loss ofFVIII function andcan result in serious bleeding episodes. Although these episodes can betreated with recombinant or plasma-derived FVIII protein, unfortu-nately,;25% of hemophilia A patients produce inhibitory anti-FVIIIantibodies (inhibitors).1,2 Typically, these patients are treated withrepeated high doses of FVIII in a protocol termed immune toleranceinduction (ITI), a process that is expensive, time-consuming and notentirely effective. The development of effective tolerogenic therapies toprevent, as well as reverse, inhibitor formation is clearly needed.
Recently, regulatoryTcells (Tregs) have beenproposed as a potentialclinical therapy for a variety of adverse immune disorders, ranging fromautoimmune diseases to the development of antidrug antibodies, such asinhibitor formation to FVIII. Treg therapies have already been applied inclinical studies for prevention of graft-versus-host disease (GVHD).3,4
However, polyclonal Tregs encompass many specificities and couldpotentially be globally immunosuppressive. For example, results of aGVHD study suggest an increase in viral reactivation up to 30 days afteradoptive transfer of umbilical cord–derived polyclonal Tregs.5 Thus, theuse of antigen-specific Tregs seems to be preferable for the nextgeneration of Treg therapeutic approaches. Previously, we developed anapproach to render expanded polyclonal Tregs “specific” by transducingthem with a T-cell receptor (TCR) containing the variable genes from a
T-cell clone derived from a hemophilia A patient.6 These Tregs werehighly effective at suppressing both T- and B-cell responses to FVIII.However, TCR-transduced cells remain MHC-restricted. In contrast,chimeric antigen receptors (CARs) containing a single chain variablefragment (scFv) as the binding domain are not major histocompatibilitycomplex (MHC)-restricted and have been used to specifically direct thelytic functionofCD81Tcells against target cells formore thanadecade.7
Most recently,CARshavealsobeenapplied tocreate alloantigen-specificTregs that prevented xenogeneic GVHD in a mouse model.8
Thus, as an alternative to a FVIII-C2-peptide-specific TCR (called17195 TCR),6 we have now used a CAR containing a scFv isolatedfrom a phage library9 (termed ANS8 CAR) that recognizes the A2domain of FVIII. In this report, we characterize these FVIII-specificCAR Tregs and demonstrate their ability to inhibit T- and B-cellresponses to FVIII in vitro and in vivo.
Methods
Human blood samples and cells
Humanblood samples fromhealthy, anonymousmale donors ranging from20 to70 years of age were obtained with written consent from the Department of
Submitted 13 July 2016; accepted 8 November 2016. Prepublished online asBlood First Edition paper, 15 November 2016; DOI 10.1182/blood-2016-07-727834.
*J.Y. and A.S. contributed equally to this work.
The online version of this article contains a data supplement.
There is an Inside Blood Commentary on this article in this issue.
The publication costs of this article were defrayed in part by page chargepayment. Therefore, and solely to indicate this fact, this article is herebymarked “advertisement” in accordance with 18 USC section 1734.
238 BLOOD, 12 JANUARY 2017 x VOLUME 129, NUMBER 2
For personal use only.on May 18, 2017. by guest www.bloodjournal.orgFrom
2weeks after adoptive transfer (data not shown).The results of this in vivoexperiment are in agreementwith our previous6 andcurrent studies,whichdemonstrated effective suppression of FVIII-specific memory responsesby both types of antigen-specific of Tregs in vitro. However, rechallengewithFVIII atday56resulted ina lossof tolerance in theANS8CARgroupas the anti-FVIII antibody development reached the levels of the controlOb2F3 TCR mice. Anti-FVIII antibody levels in the 17195 TCR groupincreased as well. However, they remained significantly lower 1 weekafter the rechallenge, suggesting a different mechanism of action betweenANS8 CAR and 17195 TCR Tregs (Figure 5B). Interestingly, all groupsdeveloped comparable amounts of anti-TNP antibody levels when themicewere rechallenged at day 56with TNP-SRBC, suggesting that Treg-treatedmicewerenot nonspecifically suppressed (supplemental Figure 3).
Discussion
Although polyclonal regulatory T-cell populations have been used inclinical trials to prevent GVHD and treat type I diabetes,5,15-17 thesepolyclonal Tregs could potentially be immunosuppressive. Instead, wepreviously proposed that the use of engineered antigen-specific Tregswould be preferable for future therapeutic strategies in hemophilia Apatientswith inhibitors because theywouldbemore efficacious, bearinga lower risk of global immunosuppression. We previously demon-strated that humanTregs could be engineered to be specific for FVIII bytransducing themwith aTCR recognizing aFVIIIC2domain peptide inthe context of HLA DR1.6 These Tregs (17195 TCR) inhibited theproliferation and cytokine production by C2-specific effector cells, aswell as the production of FVIII-specific antibodies of murine FVIII-
specific memory B cells in vitro. Herein, we demonstrate that humanTregs can be rendered specific for FVIII as well as by transducing themwith a chimeric antigen receptor (CAR), calledANS8CAR, containinga FVIII A2 domain–specific single-chain variable fragment (scFv)isolated from a phage display library. As opposed to TCR-transducedTregs, the ANS8 CARTregs are notMHC-restricted and thus could beused to treat any patient regardless of the MHC background.
ANS8 CAR T-effector cells proliferated in response to a FVIII-specific stimulus, and FVIII-specific stimulation of ANS8 CAR Tregsled to the induction of the Treg activation markers surface LAP andglycoprotein A repetitions predominant (GARP). In addition, Foxp3expression was increased in FVIII-stimulated ANS8 CAR-expressingTregs.Thus, as already shownforTregs transducedwith aFVIII-specificTCR,6 the regulatory phenotype of CAR-transduced Tregs seems to bestabilized by the antigen-specific stimulation, which is important for invitro generation of Treg numbers sufficient for therapeutic approaches.
ANS8 CAR Tregs recognizing an epitope in the FVIII A2 domainsuppressed C2-specific T-effector cell proliferation in the presence ofFVIII as well as proliferation of T-effector cells specific for the MBP inthepresenceofMBPandFVIII. Inaddition,ANS8CARTregspreventedantibody formationof restimulatedFVIII-specific splenocytes against thewhole FVIII molecule in vitro. This demonstrates bystander suppressionand suggests that one could use a single CAR Treg population tocompletely suppress FVIII inhibitor formation. Bystander suppressionhas alreadybeen reported for Tregs.18 Thus,ANS8CARTregs share thissuppressive function with regular Tregs expressing antigen-specificTCRs. As stated before, this bystander suppression is essential fortolerance induction against whole proteins. Conversely, bystandersuppression might be one reason for global immunosuppressive sideeffects ofTreg therapies. Therefore, reducing the number of transfusedTregs by the use of more efficacious antigen-specific cell populationsis of high interest for the generation of safer Treg therapeutic strategies.
A postulated scheme of ANS8 CAR Treg interactions is given inFigure 6. After activation, ANS8 CAR Tregs suppress T-effector cellsin the local milieu (eg, by IL-2 consumption and possibly by secretionof inhibitory cytokines like transforming growth factor-b). Interest-ingly, ANS8 CAR Tregs were optimally activated when FVIII waspresented on PBMCs, suggesting that either signals provided by theloaded PBMCs (acting as antigen-presenting cells) or immobilizationof FVIII are important to effectively deliver CAR-mediated pro-liferation signals, as opposed tominimal activationbyFVIII in solution.This is an important feature because it suggests thatCARTregs functionbest in the local milieu where an immune response is occurring, ratherthan in the bloodstream where their effect would be diluted.
A recent study has shown that the anti-FVIII antibody responsecould be effectively mitigated with in vitro expanded, autologouspolyclonal mouse Tregs.19 Our in vivo data clearly show that boththe FVIII-specific CAR and TCR-engineered Tregs were suppres-sive compared with the nonspecific Ob2F3 TCR Tregs, in terms ofsuppression of anti-FVIII antibody development. Direct dose responsecomparisons between polyclonal Tregs and engineered FVIII-specificTregs have not been done in vivo, although the latter should be moreeffective based on in vitro data. Adoptively transferred human Tregswere not detectable in any group of the mice as analyzed by FACS atday 14 (data not shown), because they were probably rejected by theimmunocompetent animals. However, their suppressive effect lastedfor at least 8 weeks, suggesting that the tolerance to FVIII was inducedrather early after adoptive transfer of FVIII-specific CAR or TCR-engineered human Tregs. The in vivo suppression by engineered TCRTregs was specific, because no significant difference was seen in thelevel of anti-TNP antibody after the challenge with unrelated antigen atday 56. In addition, the transferred Tregs might activate endogenous
T effector
B
?
APC
FVIII
Cytokine MHC
Antibody
Treg
TCR
CAR
Figure 6. Model of FVIII-specific human CAR Treg function. Cartoon depicting
suppressive function of FVIII-specific CAR-engineered human Tregs to FVIII-specificTCR-engineered T-effector cells or antibody-producing B cells in response to FVIII.FVIII-loaded APCs might bring T-effector cells and Tregs into close proximity. Thus,
activated Tregs can inhibit T-effector cell activation in this local milieu (eg, by IL-2consumption). Inhibition of T-effector cells also leads to prevention of FVIII inhibitor
formation as costimulatory signals of T-effector cells are essential for B-cellactivation. In addition, activated Tregs might influence B cells directly by stillunknown mechanisms.
244 YOON et al BLOOD, 12 JANUARY 2017 x VOLUME 129, NUMBER 2
For personal use only.on May 18, 2017. by guest www.bloodjournal.orgFrom

Ed il mare concederà a ogni uomo nuove speranze, come il sonno porta i sogni.
Cristoforo Colombo
ORIGINAL ARTICLE
WFH: Closing the global gap – achieving optimal care
MARK W. SKINNERWorld Federation of Hemophilia, Washington, DC, USA
Summary. For 50 years, the World Federation ofHemophilia (WFH) has been working globally to closethe gap in care and to achieve Treatment for Allpatients, men and women, with haemophilia and otherinherited bleeding disorders, regardless of where theymight live. The WFH estimates that more than one in1000 men and women has a bleeding disorder equatingto 6,900,000 worldwide. To close the gap in carebetween developed and developing nations a continuedfocus on the successful strategies deployed heretoforewill be required. However, in response to the rapidadvances in treatment and emerging therapeuticadvances on the horizon it will also require freshapproaches and renewed strategic thinking. It is difficultto predict what each therapeutic advance on the horizonwill mean for the future, but there is no doubt that weare in a golden age of research and development, whichhas the prospect of revolutionizing treatment onceagain. An improved understanding of ‘‘optimal’’ treat-ment is fundamental to the continued evolution ofglobal care. The challenges of answering governmentand payer demands for evidence-based medicine, andcost justification for the introduction and enhancementof treatment, are ever-present and growing. To sustainand improve care it is critical to build the body ofoutcome data for individual patients, within haemo-philia treatment centers (HTCs), nationally, regionallyand globally. Emerging therapeutic advances (longer
half-life therapies and gene transfer) should not bejustified or brought to market based only on the notionthat they will be economically more affordable,although that may be the case, but rather moreimportantly that they will be therapeutically moreadvantageous. Improvements in treatment adherence,reductions in bleeding frequency (including microhem-orrhages), better management of trough levels, andimproved health outcomes (including quality of life)should be the foremost considerations. As part of a newWFH strategic plan (2012–2014) the WFH has identi-fied several key initiatives for particular emphasis –continuation of the Global Alliance for Progress (GAP)program, a new initiative to address underservedcountries and regions (The Cornerstone Initiative),enhancing health outcomes research and analysis, anda new research mentorship program. Despite ourprogress to date in closing the global gap in care, ourwork is not complete. Too many patients remainundiagnosed and too few receive adequate treatment.This paper will also discuss historical, present andfuture challenges and opportunities to close the gap incare and achieve Treatment for All.
Keywords: global alliance for progress, health outcomesanalysis, optimal care, WFH development model, WFHglobal survey, World federation of hemophilia
The WFH is the cornerstone of global development. For50 years, the WFH has been working globally to closethe gap in care and to achieve Treatment for Allpatients, men and women, with haemophilia and otherinherited bleeding disorders, regardless of where theymight live.
As WFH marks its 50th anniversary, it is appropriateto reflect on the many accomplishments, milestones and
lessons learned. To close the gap in care betweendeveloped and developing nations a continued focus onthe successful strategies deployed heretofore will berequired. However, in response to the rapid advances intreatment and emerging therapeutic advances on thehorizon it will also require fresh approaches andrenewed strategic thinking.
Each year we have moved one step closer to achievingour collective vision of Treatment for All. Over the pastfive decades of the WFH’s history, there has beentremendous progress in our understanding of bleedingdisorders, improvement of treatment, and enhancementof access bringing hope to patients and their familiesthroughout the world. Nonetheless, despite our pro-gress to date in closing the global gap in care, our work
Correspondence: Mark W. Skinner, JD, President, World Federa-tion of Hemophilia, 1155 23rd St NW #3A, Washington, DC20037-3303, USA.Tel.: +1 202 253 8342; fax: +1 202 296 1352;e-mail: [email protected]
Accepted after revision 21 May 2012
Haemophilia (2012), 18 (Suppl. 4), 1–12 DOI: 10.1111/j.1365-2516.2012.02822.x
! 2012 Blackwell Publishing Ltd 1
Lookingjustatpeoplewithhaemophilia,wees:mateonlyabout25%worldwidereceiveatleastminimallyadequatetreatment.ThepercentageisfarlowerforthosewithVWDandtheotherbleedingdisorders.

Non c'è progresso senza giustizia sociale
Jorge Maria Bergoglio