Natural Human Plasmacytoid Dendritic Cells Induce Antigen ...(20). This procedure gave rise to...
14
Clinical Studies Natural Human Plasmacytoid Dendritic Cells Induce Antigen-Specific T-Cell Responses in Melanoma Patients Jurjen Tel 1 , Erik H.J.G. Aarntzen 1,2 , Tetsuro Baba 7 , Gerty Schreibelt 1 , Barbara M. Schulte 1 , Daniel Benitez-Ribas 1 , Otto C. Boerman 5 , Sandra Croockewit 6 , Wim J.G. Oyen 5 , Michelle van Rossum 4 , Gregor Winkels 8 , Pierre G. Coulie 7 , Cornelis J.A. Punt 2 , Carl G. Figdor 1 , and I. Jolanda M. de Vries 1,2,3 Abstract Vaccination against cancer by using dendritic cells has for more than a decade been based on dendritic cells generated ex vivo from monocytes or CD34 þ progenitors. Here, we report on the first clinical study of therapeutic vaccination against cancer using naturally occurring plasmacytoid dendritic cells (pDC). Fifteen patients with metastatic melanoma received intranodal injections of pDCs activated and loaded with tumor antigen-associated peptides ex vivo. In vivo imaging showed that administered pDCs migrated and distributed over multiple lymph nodes. Several patients mounted antivaccine CD4 þ and CD8 þ T-cell responses. Despite the limited number of administered pDCs, an IFN signature was observed after each vaccination. These results indicate that vaccination with naturally occurring pDC is feasible with minimal toxicity and that in patients with metastatic melanoma, it induces favorable immune responses. Cancer Res; 73(3); 1063–75. Ó2012 AACR. Introduction Dendritic cells constitute a family of antigen-presenting cells (APC) defined by their morphology, phenotype, and unique capacity to process exogenously encountered antigens and to present them to na € ve T cells. Following infection or inflammation, dendritic cells undergo a complex process of maturation and migrate to lymph nodes to present antigens and activate T cells. This decisive role in inducing immunity was the rationale for dendritic cell–based immunotherapy, in which dendritic cells loaded with tumor antigens were injected into patients with cancer to stimulate T cells to eradicate tumors (1–3). So far, most dendritic cell–based vaccination studies were conducted in patients with meta- static melanoma because of the immunogenicity of this tumor and the characterization of antigens such as gp100 and tyro- sinase (4, 5). Although numerous vaccination studies showed the immunogenicity of tumor antigen-loaded dendritic cells, the number of objective clinical responses has been limited, hampering its implementation as a novel form of standard treatment (6). Because of the limited number of naturally circulating dendritic cells, virtually all vaccination studies have used dendritic cells differentiated ex vivo from monocytes or CD34 þ progenitors. Recently, we proposed that these "arti- ficial" dendritic cells may be less effective than their natural counterparts that circulate in the blood (7). Two major subsets of natural circulating dendritic cells can be found: plasmacy- toid dendritic cells (pDC) and myeloid dendritic cells. pDCs are the major producers of type I IFN, which is of major importance in combatting viral infections. Freshly iso- lated pDCs have been associated with tolerance or Th2 responses (8, 9), but several groups have now shown that activated human pDCs produced large amounts of type I IFNs and induced Th1 responses (8, 10). Human pDCs induced strong allogeneic T-cell responses (11) and primed CD4 þ and CD8 þ T cells against viruses or tumor antigens (12, 13). Pre- clinical studies showed that antigen-loaded pDCs protected against Leishmania major (14) and induced antitumor re- sponses that inhibited tumor growth (15, 16). Recently, Takagi and colleagues showed that pDCs were crucial for the initiation of inflammation and T-cell immunity (17). Together, these findings prompted us to test the capacity of activated human pDCs to elicit antitumor immune responses in patients. In this first-in-human study, we report on vaccinating pati- ents who have metastatic melanoma, with autologous activat- ed pDCs loaded with tumor-associated peptides. Despite their low abundance in peripheral blood, we succeeded in isolating sufficient numbers (0.3–3 million per vaccination) of highly purified cells to carry out this study. We used the inactivated thick-borne encephalitis virus vaccine as a natural Toll-like receptor (TLR) agonist to activate pDCs and used these Authors' Affiliations: Departments of 1 Tumor Immunology, 2 Medical Oncology, 3 Pediatric Oncology, 4 Dermatology, 5 Nuclear Medicine, and 6 Hematology, Radboud University Nijmegen Medical Centre and Nijmegen Centre for Molecular Life Sciences, Nijmegen, the Netherlands; 7 de Duve Institute, Universit e Catholique de Louvain, Brussels, Belgium; and 8 Milte- nyi Biotec GmbH, Bergisch Gladbach, Germany Note: Supplementary data for this article are available at Cancer Research Online (http://cancerres.aacrjournals.org/). Current address for D. Benitez-Ribas: Department of Gastroenterology, CIBERehd, Hospital Clinic, Barcelona, Spain; and current address for C.J. A. Punt, Department of Medical Oncology, Academic Medical Centre, Amsterdam, the Netherlands. Corresponding Author: I. Jolanda M. de Vries, Department of Tumor Immunology, Radboud University Nijmegen Medical Centre, P.O. Box 9101, 6500 HB Nijmegen, the Netherlands. Phone: 31-24-3617600; Fax: 31-24-3540339; E-mail: [email protected] doi: 10.1158/0008-5472.CAN-12-2583 Ó2012 American Association for Cancer Research. Cancer Research www.aacrjournals.org 1063 on May 24, 2020. © 2013 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from Published OnlineFirst January 23, 2013; DOI: 10.1158/0008-5472.CAN-12-2583
Transcript of Natural Human Plasmacytoid Dendritic Cells Induce Antigen ...(20). This procedure gave rise to...

Clinical Studies
Natural Human Plasmacytoid Dendritic Cells InduceAntigen-Specific T-Cell Responses in Melanoma Patients
Jurjen Tel1, Erik H.J.G. Aarntzen1,2, Tetsuro Baba7, Gerty Schreibelt1, Barbara M. Schulte1,Daniel Benitez-Ribas1, Otto C. Boerman5, Sandra Croockewit6, Wim J.G. Oyen5, Michelle van Rossum4,Gregor Winkels8, Pierre G. Coulie7, Cornelis J.A. Punt2, Carl G. Figdor1, and I. Jolanda M. de Vries1,2,3
AbstractVaccination against cancer by using dendritic cells has for more than a decade been based on dendritic cells
generated ex vivo frommonocytes or CD34þ progenitors. Here, we report on the first clinical study of therapeuticvaccination against cancer using naturally occurring plasmacytoid dendritic cells (pDC). Fifteen patients withmetastaticmelanoma received intranodal injections of pDCs activated and loadedwith tumor antigen-associatedpeptides ex vivo. In vivo imaging showed that administered pDCs migrated and distributed over multiple lymphnodes. Several patients mounted antivaccine CD4þ and CD8þ T-cell responses. Despite the limited number ofadministered pDCs, an IFN signature was observed after each vaccination. These results indicate that vaccinationwith naturally occurring pDC is feasible with minimal toxicity and that in patients with metastatic melanoma, itinduces favorable immune responses. Cancer Res; 73(3); 1063–75. �2012 AACR.
IntroductionDendritic cells constitute a family of antigen-presenting
cells (APC) defined by their morphology, phenotype, andunique capacity to process exogenously encountered antigensand to present them to na€�ve T cells. Following infectionor inflammation, dendritic cells undergo a complex processof maturation andmigrate to lymph nodes to present antigensand activate T cells. This decisive role in inducing immunitywas the rationale for dendritic cell–based immunotherapy,in which dendritic cells loaded with tumor antigens wereinjected into patients with cancer to stimulate T cells toeradicate tumors (1–3). So far, most dendritic cell–basedvaccination studies were conducted in patients with meta-static melanoma because of the immunogenicity of this tumorand the characterization of antigens such as gp100 and tyro-sinase (4, 5). Although numerous vaccination studies showed
the immunogenicity of tumor antigen-loaded dendritic cells,the number of objective clinical responses has been limited,hampering its implementation as a novel form of standardtreatment (6). Because of the limited number of naturallycirculating dendritic cells, virtually all vaccination studies haveused dendritic cells differentiated ex vivo from monocytesor CD34þ progenitors. Recently, we proposed that these "arti-ficial" dendritic cells may be less effective than their naturalcounterparts that circulate in the blood (7). Twomajor subsetsof natural circulating dendritic cells can be found: plasmacy-toid dendritic cells (pDC) and myeloid dendritic cells.
pDCs are the major producers of type I IFN, which is ofmajor importance in combatting viral infections. Freshly iso-lated pDCs have been associated with tolerance or Th2responses (8, 9), but several groups have now shown thatactivated human pDCs produced large amounts of type I IFNsand induced Th1 responses (8, 10). Human pDCs inducedstrong allogeneic T-cell responses (11) and primed CD4þ andCD8þ T cells against viruses or tumor antigens (12, 13). Pre-clinical studies showed that antigen-loaded pDCs protectedagainst Leishmania major (14) and induced antitumor re-sponses that inhibited tumor growth (15, 16). Recently, Takagiand colleagues showed that pDCs were crucial for the initiationof inflammation and T-cell immunity (17). Together, thesefindings prompted us to test the capacity of activated humanpDCs to elicit antitumor immune responses in patients.
In this first-in-human study, we report on vaccinating pati-ents who have metastatic melanoma, with autologous activat-ed pDCs loaded with tumor-associated peptides. Despite theirlow abundance in peripheral blood, we succeeded in isolatingsufficient numbers (0.3–3 million per vaccination) of highlypurified cells to carry out this study. We used the inactivatedthick-borne encephalitis virus vaccine as a natural Toll-likereceptor (TLR) agonist to activate pDCs and used these
Authors' Affiliations: Departments of 1Tumor Immunology, 2MedicalOncology, 3Pediatric Oncology, 4Dermatology, 5Nuclear Medicine, and6Hematology, RadboudUniversity NijmegenMedical Centre andNijmegenCentre for Molecular Life Sciences, Nijmegen, the Netherlands; 7de DuveInstitute, Universit�e Catholique de Louvain, Brussels, Belgium; and 8Milte-nyi Biotec GmbH, Bergisch Gladbach, Germany
Note: Supplementary data for this article are available at Cancer ResearchOnline (http://cancerres.aacrjournals.org/).
Current address for D. Benitez-Ribas: Department of Gastroenterology,CIBERehd, Hospital Clinic, Barcelona, Spain; and current address for C.J.A. Punt, Department of Medical Oncology, Academic Medical Centre,Amsterdam, the Netherlands.
Corresponding Author: I. Jolanda M. de Vries, Department of TumorImmunology, Radboud University Nijmegen Medical Centre, P.O. Box9101, 6500 HB Nijmegen, the Netherlands. Phone: 31-24-3617600; Fax:31-24-3540339; E-mail: [email protected]
doi: 10.1158/0008-5472.CAN-12-2583
�2012 American Association for Cancer Research.
CancerResearch
www.aacrjournals.org 1063
on May 24, 2020. © 2013 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 23, 2013; DOI: 10.1158/0008-5472.CAN-12-2583

antigens as an immunomonitoring tool. We show that theseactivated pDCs were safe to use and induced antigen-specificCD4þ and CD8þ T-cell responses in patients suffering frommelanoma.
Materials and MethodsPatient characteristics and clinical protocol
Sixteen patients with distant metastatic melanoma (ac-cording to the 2001 American Joint Committee on Cancerstaging system; ref. 18) were enrolled in this feasibility study.One patient did not complete the scheduled vaccinations andmonitoring due to rapid progression of disease. Fifteen ofthe patients were considered evaluable. Eligibility criteriaincluded measurable target lesions, HLA-A2.1 phenotype,histologically documented metastatic melanoma expressinggp100 (compulsory) and tyrosinase (noncompulsory), noactive infection or immune suppressive conditions, serumlactate dehydrogenase (LDH) concentration within normallimits (<450 U/L) and World Health Organization (WHO)performance status 0 or 1. Primary endpoint was toxicityrelated to vaccination and immunologic response. The trial,CMO 2004/093, was approved by the local InstitutionalReview Board (Committee on Research involving HumanSubjects Arnhem-Nijmegen) and in accordance with the De-claration of Helsinki. Written informed consent was obtainedfrom all patients. The primary objective of this study wasto generate clinical grade mature pDC preparations and todetermine a safe and effective dosage of the vaccine. Whenthe appropriate dosage of the vaccine was determined, we
evaluated the efficacy of the pDCs to initiate antitumor T-cellresponses in patients with stage IV melanoma. Clinical trialregistration number is NCT01690377.
CliniMACS pDC isolation and immunization schedulePatients were vaccinated with autologous pDCs loaded
with HLA-A2.1-binding tumor peptides derived from the mel-anoma-associated antigens gp100 and tyrosinase. Thefollowing HLA-A2.1–restricted peptides were used: gp100-derived peptides gp100154–162 (KTWGQYWQV) andgp100280–288 (YLEPGPVTA) and tyrosinase-derived peptidetyrosinase369–377 (YMNGTMSQV). The clinical study wasdesigned as a feasibility study. The first patient received 0.3 �106 pDCs per vaccination, patients 2 and 3 received 1.0 � 106
pDCs per vaccination, and patients 4 and 5 received 3 � 106
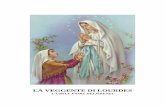
pDCs per injection. Considering the yield from pDC isolation,this is the maximum feasible dose, and was also given topatients 6 to 15. Three intranodal injections were given onceevery 2 weeks followed by a delayed-type hypersensitivity(DTH) challenge (Fig. 1). In the absence of disease progression,patients were eligible for a maximum of 2 maintenance cyclesconsisting of 3 biweekly vaccinations and a DTH challenge,each with a 6-month interval.
pDCs were directly isolated from apheresis productsusing the fully closed immunomagnetic CliniMACS isolationsystem (Miltenyi Biotec). GMP-grade magnetic bead-coupledBDCA4 antibodies were used, following the manufacturer'sguidelines. This procedure resulted in clinically applicablepurified pDCs, which had an average purity of 75% and a yieldbetween 13 � 106 and 33 � 106 (Supplementary Fig. S1).
Figure 1. Schematic overview of thepDC culture protocol andvaccination strategy.
Tel et al.
Cancer Res; 73(3) February 1, 2013 Cancer Research1064
on May 24, 2020. © 2013 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 23, 2013; DOI: 10.1158/0008-5472.CAN-12-2583

Following apheresis and CliniMACS isolation, pDCs werecultured overnight at a concentration of 106 cells/mL inX-VIVO 15 (Cambrex) containing 2% pooled human serum(Sanquin), supplemented with 10 ng/mL recombinant humaninterleukin-3 (rhIL-3; Cellgenix). For the first vaccination,these pDCs were subsequently activated for 6 hours by addi-tion of FSME-IMMUN (1:10 v/v; Baxter AG). During the last3 hours of activation, pDCs were loaded with the melanoma-associated peptides gp100154, gp100280, and tyrosinase (19).For subsequent vaccinations and DTH skin tests, overnightIL-3–cultured pDCs were activated for 3 hours by addition ofFSME-IMMUN (1:10 v/v). Thereafter, these 3-hour activatedpDCs were frozen in X-VIVO 15 medium containing 10%dimethyl sulfoxide (DMSO). Upon subsequent vaccinations/DTH, 3-hour activated pDCs were thawed and activated foran additional 3 hours with FSME-IMMUN (1:10 v/v) andloaded with the melanoma-associated peptides. The pep-tide-loaded pDCs were administered intranodally in a clinic-ally tumor-free lymphnode region under ultrasound guidance(20). This procedure gave rise to mature pDCs meeting thefollowing release criteria; more than 50% viability, IFN-asecretion, high expression of MHC class I, MHC class II, CD83,CD80, CD86, and CCR7.
PhenotypeThe purity of pDCs after CliniMACS isolation and the
phenotype of the pDCs were determined by flow cytometry.The following primary monoclonal antibodies (mAb) andthe appropriate isotype controls were used: anti-CD45-FITC,anti-BDCA2-PE, and anti-CD123-APC (all Miltenyi Biotec);anti-HLA-ABC-PE (W6/32), anti-HLA-DR/DP-FITC (Q5/13),anti-CD80-PE, and CD86-PE (all BD Biosciences Pharmingen);anti-CD83 (Beckman Coulter); and anti-CCR7 (R&D Systems)followed by goat–anti-mouse phycoerythrin (PE).
Cytokine detectionSupernatants were collected from pDC cultures either
directly after 6 hours of stimulation or after 6 hours of stimu-lation followed by a washing step and subsequent reconstitu-tion of cells in fresh medium for an additional 12 hours, andIFN-a production was analyzed with murine monoclonalcapture and horseradish peroxidase-conjugated anti-IFN-aantibodies (BenderMed Systems) using standard ELISAprocedures.To analyze the T-helper cell profile, supernatants were
collected after 2 days of pDC-PBL coculture. Cytokine produc-tion (IL-1b, IL-2, IL-4, IL-5, IL-6, IL-8, IL-10, IL-12 (p70), TNF-a,TNF-b, IFN-g) in the supernatant was analyzed with a humanTh1/Th2 Multiplex kit (BenderMed System) according to themanufacturer's instructions.
111In-oxinate labeling and scintigraphic imagingSix-hour Fr€uhsommer-Meningoenzephalitis (FSME)-acti-
vated pDCs were labeled with 5 MBq 111In-oxinate (GEHealthcare) in 0.1 mol/L Tris–HCl (pH 7.0) for 15 minutesat room temperature as described previously (21, 22). Cellswere washed 3 times with PBS/1%HSA, and the labelingefficiency was calculated as the percentage of the activity
that remained associated with the cell pellet. 111In-labeledpDCs (3 � 106; 4 MBq) in 200 mL saline were injected underultrasound guidance directly into a clinically tumor-freelymph node.
In vivo planar scintigraphic images (256 � 256 matrix, 174and 247 keV 111In photopeaks with 15% energy window) ofthe injection depot and corresponding lymph node basin wereacquired with a gamma camera (Siemens ECAM) equippedwith medium energy collimators, 15 minutes, 24, and 48 hoursafter injection. Migration was quantified by region-of-interestanalysis of the individual nodes visualized on the images andexpressed as the fraction of 111In-labeled dendritic cell thathad migrated from the injection depot to following lymphnodes after 15 minutes, 24, and 48 hours.
Immunomonitoring of patientsBlood samples were obtained before the start of the vacci-
nation regimen and after each individual vaccination. Eachsample was tested for the presence of FSME-specific T cellsby proliferation and 3H-thymidine incorporation, and forthe presence of FSME-specific antibodies in the serum usingan ELISA specific for Tick-borne encephalitis immunoglo-bulin G (IgG; Serion/Virio). Four days after the third vaccina-tion, a DTH skin test was conducted as described previously(23, 24). Monocyte-derived dendritic cells (moDC) pulsedwith gp100 or tyrosinase peptides (1 � 106) and pDCspulsed with gp100 or tyrosinase peptides (0.2 � 106) wereinjected intradermally in the skin of the back of the patientat 4 different sites. The maximum diameter of induration wasmeasured after 48 hours. Punch biopsies (6 mm) were obtain-ed from all DTH sites. Half of the biopsy was cryopreservedand the other half was manually cut and cultured in RPMI-1640 (Gibco-BRL Life Technologies) containing 7% humanserum and IL-2 (100 U/mL, Proleukin). Every 7 days, half ofthe medium was replaced by fresh medium containinghuman serum and IL-2. After 2 to 5 weeks of culturing,T cells were tested for specificity against gp100 and tyro-sinase (19). DTH-derived cells were stained with tetrameric-MHC complexes containing the gp100154–167, gp100280–288,or tyrosinase369–376 peptide (Sanquin) combined with CD8staining as described previously (23). All samples were testedwith HIV77–85-HLA-A2.1-tetramers recognizing the irrelevantHIV-peptide (SLYNTVATL) for background staining.
Mixed lymphocyte-peptide culturesBlood frequencies of antivaccine CD8þ T cells were
estimated using mixed lymphocyte-peptide cultures asdescribed previously (25). Briefly, peripheral blood mono-nuclear cells (PBMC) isolated before and after 1 cycle of3 pDC injections, were thawed and divided in 3 groupsincubated for 1 hour at room temperature in Iscove'smedium (Life Technologies) with 1% human serum and2 mmol/L of the peptides tyrosinase369 (YMDGTMSQV),wild-type gp100154 (KTWGQYWQV), or wild-type gp100280(YLEPGPVVTA). These pulsed cells were then washed,pooled, and distributed at 2 � 105 cells/0.2 mL in round-bottom microwells in Iscove's with 10% human serum,L-arginine (116 mg/L), L-asparagine (36 mg/L), L-glutamine
Human Plasmacytoid Dendritic Cells Enhance Overall Survival in Melanoma Patients
www.aacrjournals.org Cancer Res; 73(3) February 1, 2013 1065
on May 24, 2020. © 2013 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 23, 2013; DOI: 10.1158/0008-5472.CAN-12-2583

(216 mg/L), 1-methyl-L-tryptophan (100 mmol/L), IL-2(20 U/mL), and IL-7 (10 ng/mL). On day 7, 50% of themedium was replaced by fresh medium containing IL-2 andpeptides at 4 mmol/L. Tetramer labeling was conducted onday 14 as described previously (25). Anti-gp100154 T-cellclones were derived that represented either the spontane-ous anti-gp100 T cells present before vaccination in patients2, 5, 6, 10, and 11, or the pDC-induced anti-gp100 T cellspresent after vaccination in patients 1, 4, 8, and 12. Tetra-mer-positive CD8þ T cells were sorted at 1 cell per well andrestimulated weekly with irradiated HLA-A2þ EBV-trans-formed B cells pulsed with the gp100154 peptide at 2 mmol/L,and irradiated allogeneic PBMC as feeder cells, in mediumsupplemented with IL-2 and IL-7. Established T-cell cloneswere stained with the relevant tetramer and their functionalavidity was evaluated by testing their production of IFN-gafter stimulation with HLA-A2þ EBV-B cells pulsed withvarious concentrations (from 10 pmol/L up to 10 mmol/L) ofthe gp100154 peptide.
RNA isolation and qPCRTo determine mRNA expression of IFN and IFN-stimulated
genes, blood was drawn from 1 patient during 1 cycle of 3vaccinations before each vaccination and at 4 and 24 hours aftereach vaccination using PAXgene tubes. RNA isolation wasconducted using PAXgene Blood RNA Kit according to themanufacturer's instructions (Qiagen). RNA isolations fromPBMCs from healthy volunteers were done using the ZR RNAIsolation Kit (Zymo Research) according to manufacturer'sinstructions. RNA was treated with DNase I (amplificationgrade; Invitrogen) and reverse-transcribed into cDNA by usingrandom hexamers and Moloney murine leukemia virus reversetranscriptase (Invitrogen). To exclude genomic DNA conta-mination, we included a "-RT" control in which the reversetranscriptase was replaced with RNase-free water. The -RTcontrol was taken along in the quantitative PCR (qPCR) analy-sis and was used as a cutoff value. cDNA was stored at �20�Cuntil further use. mRNA levels for the genes of interest weredetermined by qPCR with a Bio-Rad CFX apparatus (Bio-Rad)with SYBRGreen (Applied Biosystems). Analysis was done usingBiorad CFX-1.6 software, and expression levels were determin-ed relative to Porphobilinogen deaminase (PBGD) expression.Primer sequences are available on request and were from thePrimer Bank database (26).
Matched historical controlsMatched historical controls were identified from records
of patients with metastatic melanoma from the RadboudUniversity Nijmegen Medical Centre (Nijmegen, the Nether-lands), the Netherlands Cancer Institute—Antoni vanLeeuwenhoek Hospital (Amsterdam, the Netherlands), andUniversity Hospital Essen (Essen, Germany) who hadreceived first-line dacarbazine (DTIC) chemotherapy at850 to 1,000 mg/m2 i.v. at 3 weekly intervals, between March2000 and March 2010. All matched controls were HLA-A�02:01-positive and were required to have received at least3 infusions, a therapy time frame that is consistent with 1cycle of vaccinations.
Historical controls were matched to study subjects, in ratio1:3, primarily forM substage at baseline according to AmericanJoint Committee on Cancer criteria, number of distant metas-tases, number ofmetastatic sites, localization of distantmetas-tases, and baseline serum LDH. These criteria currently rep-resent the most important prognostic factors for survival (27).In case of more than 3 matches for 1 study subject, demo-graphic criteria (age, gender), and systemic salvage treatmentafter progression on DTIC were used to select the closestmatch.
Statistical analysisSignificant differences from controls were determined
according to paired Student t test or by one-way ANOVAanalysis followed by the Tukey post hoc test. Differencesbetween the groups were evaluated using an unpaired t test.Differences between pre- and postvaccination were evaluatedwith a Wilcoxon signed-rank test. Kaplan–Meier probabilityestimates of progression-free survival (PFS) and overall sur-vival (OS) were calculated, statistical differences between thesurvival of the groups were determined with a log-rank test.Statistical significance was defined as P < 0.05. SPSS19.0 wasused for survival analyses.
ResultsVaccination of metastatic melanoma patients withactivated pDCs is safe with minimal side effects
It is of utmost importance that pDCs administered topatients with cancer have an immunostimulatory phenotype(19). Previously, we have shown that the commonly usedpreventive FSME-vaccine induced both IFN-a secretion anda mature pDC phenotype (28). Thus, FSME could be usedas a clinically applicable natural TLR agonist. In this first-in-human study, we vaccinated 15 patients with increasingpDC numbers, ranging from 0.3 to 3 million per vaccination,with 3 vaccinations at biweekly intervals (Fig. 1). Patientcharacteristics are shown in Table 1. The expression ofCD80, CD83, CD86, MHC class I, and II upon FSME-inducedactivation indicated that the generated pDCs were highlymature and capable of providing costimulatory signalsneeded for optimal T-cell activation (Fig. 2A). Furthermore,pDC activation for 6 hours led to the secretion of highlevels of type I IFN (Fig. 2B). In addition, we also washed6-hour activated pDCs and reconstituted the cells in freshmedium. Thereafter, pDCs were maintained for an addition-al 12 hours to show that pDCs have a sustained ability tosecrete IFN-a (Fig. 2B). Thus, all patients received purifiedand activated peptide-loaded pDCs that met the predefinedrelease criteria with the ability to secrete type I IFN in vivo(6). Furthermore, the vaccines were well tolerated andno signs of severe toxicity (common toxicity criteria grade3–4) were observed. Six vaccinated patients developedgrade 1 flu-like symptoms and 1 patient reported grade 2nontreatment–related pain resulting from progressive sub-cutaneous metastasis. In none of the vaccinated patientsdid we detect antibodies to the murine antibody used duringthe isolation procedure (data not shown). We conclude that
Tel et al.
Cancer Res; 73(3) February 1, 2013 Cancer Research1066
on May 24, 2020. © 2013 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 23, 2013; DOI: 10.1158/0008-5472.CAN-12-2583

Tab
le1.
Patient
charac
teris
ticsan
dclinical
andim
mun
olog
icresp
onse
safterpDC
vacc
ination
AntiF
SME
resp
ons
eAntitum
or
resp
ons
e
Patient
Sex
/age
Prior
trea
tmen
tStageat
bas
eline
Siteof
metas
tase
sNum
ber
of
aphe
resis
Injected
pDCs
Num
ber
of
vacc
inations
Tce
llaAbb
CD8þ
Tce
llRes
pons
ePFS
cOSd
Salva
ge
trea
tmen
t
01M/43
SM1b
Lung
,skin
10.3�
106
3þþ
þþþ
PD
<410
RT
02F/45
—M1b
Lymphno
des
,lung
11�
106
3þ
þþ�
PD
<43
CT
03M/62
—M1c
Live
r,lung
11�
106
3þþ
þþþ
SD
636
þCT,
ITe,f
04M/35
—M1c
Live
r,lymphno
des
,es
opha
gus,
omen
tum
13�
106
3�
þþþ
SD
527
CT,
ITe,g
05F/53
SM1c
Live
r,lung
,skin,
spleen
13�
106
3�
þþþ
PD
<45
RT
06M/59
SM1b
Lung
,skin
13�
106
3n.a.
��
PD
<46
RT
07M/43
—M1c
Lymphno
des
,sk
in,tes
tis1
3�
106
3þ
þþ�
PD
45
Non
e
08F/51
—M1b
Lung
13�
106
3þ
þþþ
PD
<413
Non
e
09M/36
—M1b
Lung
,skin
13�
106
3þ
þþ
SD
523
CT,
ITg,h
10M/52
SM1a
Lymphno
des
33�
106
9�
��
SD
728
þS
11M/66
—M1c
Live
r,lymphno
des
,lung
13�
106
3�
þþ�
PD
<412
CT
12F/39
SM1b
Lung
13�
106
3þþ
þþþ
SD
527
þRT,
CT,
ITe
13F/56
SM1b
Lung
13�
106
6þþ
þþþ
SD
1526
þCT,
ITe
14M/69
SM1c
Lung
,skin,
adrena
lgland
13�
106
6þ
þþ�
MR
14þ
24þ
Non
e
15M/67
S,R
T,CT
M1b
Lymphno
des
,lung
,skin
13�
106
3þþ
��
PD
<424
þIT
e
Abbreviations
:CT,
chem
othe
rapy;
IT,im
mun
othe
rapy;
MR,mixed
resp
onse
;OS,ov
erallsu
rvival;PD,prog
ressivedisea
se;PFS
,progres
sion
-freesu
rvival;RT,
radiotherap
y;S,s
urge
ry;S
D,s
table
disea
se.
aNoT-ce
llresp
onse
;þStim
ulationindex
>1<2
;þþ
SI�
2<10
.bNoAbor
<15U/m
L;�
Abtiter
<28
U/m
L;þ
Abtiter
>28
<100
U/m
L;þþ
Abtiter
>100
U/m
L.cPFS
inmon
ths.
dOSin
mon
ths.
eAnti-CTL
A4an
tibod
y.f Akt
inhibito
r.gIfo
sfam
ide-paz
opan
ib.
hMito
gen-ac
tivated
protein/ex
trac
ellularsign
al–regu
latedkina
se(M
EK)inh
ibito
r(AZD62
44).
Human Plasmacytoid Dendritic Cells Enhance Overall Survival in Melanoma Patients
www.aacrjournals.org Cancer Res; 73(3) February 1, 2013 1067
on May 24, 2020. © 2013 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 23, 2013; DOI: 10.1158/0008-5472.CAN-12-2583

it is feasible and safe to administer activated and tumor-peptide–loaded pDCs to patients.
Migration of activated pDCs in vivoFor effective immunization, injected dendritic cells have
to migrate into the T-cell areas of draining lymph nodes topresent antigens to na€�ve T cells. Because of the limitedamount of pDCs available, we opted for intranodal injectionto maximize the number of pDCs in the lymph node. In 3patients, we examined the migration in vivo of activatedpDCs labeled with 111In (21, 29). Forty-eight hours after intra-nodal injection, a significant proportion of 111In-labeledpDCs remained at the injection site and distinct amountswere detected in distant lymph nodes (Fig. 2C). These resultsshowed that the pDCs injected in a single lymph node distri-buted into downstream nodes.
Vaccination with activated pDC induce an IFNsignature in vivo
To verify whether activated pDCs secreted significant quan-tities of type I IFNs in vivo, we investigated in 1 patient theIFN signatures in great detail (multiple time points/3 vaccina-tions). We measured in blood mononuclear cells the expres-sion of type I IFNs genes and of 5 IFN-induced genes in bloodmononuclear cells 1 hour before and 4 and 24 hours after
vaccination, and compared these expression levels with thoseof healthy individuals. Transcription of both IFN-a and IFN-bgenes was clearly induced 4 hours after vaccination anddecreased 20 hours later (Fig. 3A), indicating a temporalsystemic induction of type I IFNs. As expected, we observedincreases in the expression of the IFN-induced genes RIG-I,PKR, OAS-1, OAS-2, and IRF-7 after 4 hours and furtherincreases after 24 hours (Fig. 3B). These results show thatafter each vaccination even small numbers of injected pDCsinduced a systemic type I IFN signature.
Plasmacytoid dendritic cell vaccination leads to CD4þ
T-cell proliferation and antibody productionWe next analyzed the ability of activated pDCs to prime
T-cell responses to the FSME antigens, which served as aninternal control for the tumor-associated antigenic peptides.After 3 pDC vaccinations, FSME-stimulated T-cell proliferationincreased in 9 of 14 tested patients (Fig. 4A and Table 1).Cytokine production experiments carried out in 6 patientsshowedhigher levels of IFN-g , IL-10, and IL-5 after vaccinationsthan before (Fig. 4B and data not shown).
Furthermore, we followed the levels of serum anti-FSMEantibodies after each vaccination. Twelve of 15 tested patientssignificantly increased their anti-FSME IgG titers starting
Figure2. ActivatedpDCsaremature andmigrate todistinct lymphnodes in vivo. A, expression levels of the surfacemoleculesCD80,CD83,CD86,MHCclass I,and class II on pDCs after 6 hours of activation with the FSME-vaccine. Surface receptor expression levels of all molecules of the pDC vaccines depictedin the percentage of positive cells (left) and mean fluorescence intensity (MFI; right) after 6 hours of activation with the FSME-vaccine (n ¼ 15). B, IFN-aproduction by pDCs after 6 hours of cultivation/activation with rhIL-3 or FSME-vaccine or after 6 hours of activation followed by a washing step andreconstitution of pDCs in fresh medium for an additional 12 hours (n ¼ 9; �, P < 0.05; ���, P < 0.001). C, tracking of pDC migration in vivo. Migration andbiodistribution of 111In-labeled pDCs visualized by scintigraphic imaging. Forty-eight hours after administration, 11% (pt 01), 3% (pt 02), and 42%(pt 03) of injected pDCs were distributed over up to 4 distant lymph nodes away from the injection depot.
Tel et al.
Cancer Res; 73(3) February 1, 2013 Cancer Research1068
on May 24, 2020. © 2013 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 23, 2013; DOI: 10.1158/0008-5472.CAN-12-2583

after the second vaccination (Fig. 4C and Table 1). One patient(pt 14) already had anti-FSME antibodies before vaccination.In only 1 of 15 patients neither T cells nor antibodies to
FSME were detected. Thus, the majority of patients developedde novo proliferative and humoral FSME-specific immuneresponses upon vaccination, indicative of a functional immunesystem that can be primed by activated and antigen-loadedpDCs.
Activated pDCs induce tumor antigen-specific CD8þ
T-cell responses in vivoWe used tetramers to detect the presence of tumor
antigen-specific CD8þ T cells in blood, and in biopsies takenfrom skin DTH reactions as described previously (23). Inblood, the proportions of total CD8þ T cells did not changefollowing vaccination (Fig. 5A), and ex vivo tetramer stainingwas negative both before and after vaccination (data notshown). We resorted to an in vitro restimulation of bloodmononuclear cells in limiting dilution conditions over 2weeks with the 3 antigenic peptides, before screening all
microcultures for the presence of CD8þ tetramerþ cells. Thisprocedure allows to estimate the frequencies of blood CD8þ
T cells that recognize a given antigen and proliferate in vitroin response to this antigen. As shown in Fig. 5B, 7 of 15 pati-ents showed a significant increase (�5-fold) of the fre-quency of gp100154-specific CD8þ T cells. To evaluate theaffinity of these antivaccine T cells, we derived anti-gp100154T-cell clones from pre- and postvaccination PBMC andmeasured IFN-g production after a stimulation with variousconcentrations of peptide. The concentration of peptidethat stimulates a half-maximal cytokine production reflectsthe functional avidity of the T cells. As shown in Fig. 5C, 2of 8 postvaccination clones had a higher (>10-fold) func-tional avidity than that of all the other pre- or post vacci-nation clones, suggesting the efficacy of pDCs at priminghigh-affinity T cells.
In the skin, we observed in 10 of 15 patients positive DTHresponses with indurations of up to 22 mm at the sites ofintradermal injection of 0.2 � 106 peptide-loaded activatedpDCs (Supplementary Table S1). Furthermore, we detected
Figure 3. Vaccination with activated pDCs induces an IFN signature.A, the graphs show the IFN-a and IFN-b gene expression levels in theblood relative to PBGD expression at indicated times after each vaccination.B, the graphs show the mRNA expression of indicated IFN-stimulatedgenes determined as in A. Healthy, steady-state expression levels of indicatedgenes in 8 healthy individuals. n.a., not analyzed; n.d., not detected(�, P < 0.05; ��, P < 0.01; ���, P < 0.001).
Human Plasmacytoid Dendritic Cells Enhance Overall Survival in Melanoma Patients
www.aacrjournals.org Cancer Res; 73(3) February 1, 2013 1069
on May 24, 2020. © 2013 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 23, 2013; DOI: 10.1158/0008-5472.CAN-12-2583

anti-gp100154 CD8þ T cells in 1 DTH biopsy obtained after 1
cycle of vaccination (pt 1) and in 1 obtained after 2 cycles(pt 13; Fig. 5D). T cells obtained from biopsies of DTH reac-tions to unloaded pDCs did not proliferate showing the spec-ificity of this response. We conclude that vaccination withsmall numbers of peptide-loaded and activated pDCs caninduce tumor-specific CD8þ T-cell responses in patients withmetastatic melanoma.
Clinical outcome of late-stage melanoma patientsvaccinated with plasmacytoid dendritic cell
Although the patient number does not allow drawing signi-ficant conclusions about the clinical outcome, we did observesome interesting trends. Two patients (pt 13 and 14) showeddurable stable disease and were eligible for 2 additional cyclesconsisting of 3 pDC vaccinations. Patient 14 developed amixedresponse with regression of lung metastases and progressionof a nodal metastasis. Patient 10 had a documented progres-sion but achieved complete remission after surgery andsubsequently received maintenance treatment. To have anindication whether pDC vaccination has an influence on
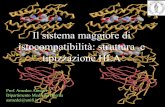
clinical outcome, we compared the clinical outcome of 15pDC-vaccinated patients with the outcome of carefully select-ed matched control patients (n ¼ 72) who received standardDTIC (dacarbazine) chemotherapy as a first-line treatment(Supplementary Table S2). The median PFS in the pDC groupwas 4.0 versus 2.1 months in the control group (notsignificant; Fig. 6A). Although the initial endpoint of this studywas safety and feasibility, the median OS showed a remark-able improvement as compared with matched control pati-ents: 22.0 [95% confidence interval (CI), 1.8–42.2] versus7.6 months (95% CI, 5.8–9.4), P ¼ 0.001. Furthermore, 7 of15 patients were alive, even 2 years after the start of pDCvaccination, compared with 6 of 72 patients treated withstandard chemotherapy (Fig. 6B).
DiscussionAfter almost 15 years of dendritic cell–based immunother-
apy, the clinical efficacy of the ex vivo generated monocyte orCD34þ progenitor derived-dendritic cells is disappointing.Therefore, properly activated naturally occurring dendritic
Figure 4. Activated pDCs induce de novo FSME-specific cellular and humoral immune response in vivo. A, proliferation of anti-FSME blood T cellscollected before and after 3 vaccinations with tumor-peptide loaded pDCs. Proliferation of T cells was measured by 3H-thymidine incorporationand depicted as proliferation in counts per minute (CPM; log scale). B, cytokine production pre- (white bars) and postvaccination (black bars); IFN-g ,IL-10, and IL-5 production by T cells stimulated overnight by FSME-activated pDCs (log scale). The graphs show the cytokine production of T cellsfrom 6 patients. C, FSME-specific IgG detected in the serum of patients before and after the first, second, and third vaccination. The dotted linerepresents the threshold (28 U) for positivity (ns, not significant; ���, P < 0.001).
Tel et al.
Cancer Res; 73(3) February 1, 2013 Cancer Research1070
on May 24, 2020. © 2013 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 23, 2013; DOI: 10.1158/0008-5472.CAN-12-2583

cells might represent the next generation of anticancer cellu-lar therapy to induce tumor-specific immunologic responsesand improve clinical efficacy. In this first clinical study withpDCs in patients with metastatic melanoma, with activatedpDCs injected into lymph nodes, we observed: (i) distribution
of injected pDCs over multiple lymph nodes, (ii) enhancedsystemic secretion of type I IFNs, (iii) de novo T- and B-cellresponses to control antigen, and (iv) induction of tumorantigen-specific CD8þ T cells, including some with high func-tional avidity.
Figure 5. Activated pDCs induce tumor-antigen specific CD8þ T-cell responses in patients. A, proportions of blood CD3þ CD8þ T cells before and after 1cycle of vaccination. B, pDC vaccine-related CD8þ T-cell responses are detected in the blood after mixed lymphocyte-peptide cultures. The graphsshow the blood frequencies of gp100154, gp100280, and tyrosinase tetramerþ CD8þ T cells before and after 1 cycle of vaccination on a log scale.C, functional avidities of anti-gp100154 CD8
þ T-cell clones derived from selected patients before (7 clones) or after (8 clones) 1 cycle of vaccination. Thegraph shows the concentrations of antigenic peptide, pulsed on HLA-A2þ cells, required to obtain 50% of maximal IFN-g production by each ofthe T-cell clones on a log scale. D, pDC vaccine-related CD8þ T-cell responses are detected in biopsies taken from DTH skin tests. Two weeks after thethird pDC injection, a DTH skin test was conducted by injecting intradermally pDCs and moDCs loaded with either the gp100 or the tyrosinase peptides.Biopsies taken 2 days later were cultured for 3 to 4 weeks in low dose IL-2, and proliferating T cells were stained with specific tetramers. Fluorescence-activated cell sorting plots from patients 1 (after 1 vaccination cycle) and 13 (after 2 vaccination cycles) show DTH-infiltrating lymphocytes stained bygp100154 tetramers (ns, not significant; ��, P < 0.01). FITC, fluorescein isothiocyanate.
Human Plasmacytoid Dendritic Cells Enhance Overall Survival in Melanoma Patients
www.aacrjournals.org Cancer Res; 73(3) February 1, 2013 1071
on May 24, 2020. © 2013 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 23, 2013; DOI: 10.1158/0008-5472.CAN-12-2583

pDCs are known to sense viral or self-nucleic acids and tobecome activated to produce type I IFN at sites of inflamma-tion. These IFNs initiate protective immunity through matu-ration of resident myeloid dendritic cells and subsequentactivation of infiltrating T cells and natural killer (NK) cells.In contrast, nonactivated pDCs promote T regulatory cell-mediated immunosuppression (30), and the presence ofpDCs in tumors has been correlatedwith poor clinical outcome(31, 32). We hypothesized that properly activated pDCs,because of their IFN production, might stimulate myeloiddendritic cells and enhance their ability to cross-primeCD8þ T cells, thereby inducing more efficient antitumor T-cellresponses when compared with in vitro generated dendriticcells. This notion is supported by 2 independent studiesshowing in mice that type I IFNs were critical for the induc-tion of antitumor immune responses (33, 34). Therefore, towarrant clinical efficacy, pDCs should secrete type I IFN atthe time of administration. Because previous studies showedthat pDCs produced IFN-a within 12 hours after activationand then became refractory to further stimulation (35–37),isolated pDCs were maintained overnight in IL-3 and subse-quently activated for 6 hours with FSME. Our approachresulted in clinically applicable pDCs with a stimulatory phe-notype and secretion of type I IFNs in vivo. Accordingly,we now show that vaccination with such pDCs indeed inducedan IFN signature based on the upregulated IFN-induced genesin the blood after vaccination, validating our approach.
For an optimal immune response, the injected pDCs shouldmigrate to neighboring lymph nodes and then to T-cell areas.The observed migratory behavior and distribution over mul-tiple lymph nodes of the injected pDCs might be linked tothe expression of CCR7 (Supplementary Fig. S2), the homing
receptor for the chemokines CCL19 and CCL21 that areexpressed by high endothelial venules and stromal cells inthe T-cell areas (30, 38, 39). The pDC migratory behavior isin agreement with previous studies, where although themajority of injected dendritic cells reside at the injectiondepot (22, 29, 40, 41), a substantial fraction of the pDCsmigrated to subsequent lymph nodes. It is important toconsider that the microenvironment influences cell migra-tion (42). Therefore, a high number of pDCs at the injectionsite might affect the microenvironment. For example, pDC-derived IFNs could drive expression of chemokines resultingin the recruitment of immune cells, thereby circumventingthe need for active migration of the pDCs themselves. Unfor-tunately, the clinical protocol did not allow lymph noderesections, to further substantiate this important aspect.
We used FSME as natural TLR agonist to activate pDCs. AsFSME comprises a total inactivated virus, we reasoned thatduring activation pDCs will process FSME-derived antigensand present antigenic peptides on human leukocyte antigen(HLA) molecules. Indeed, we observed cellular as well ashumoral responses against FSME in almost all patients. There-fore, commonly used vaccines are potentially interesting,to serve both as a TLR agonist and as a control antigen. Inaddition, it cannot be excluded that anti-FSME Th1 responsescontribute to the expansion of CD8þ tumor specific T cells, orwhether synthetic CpG oligonucleotides also will be sufficientfor clinical benefit.
We have previously shown that the presence of anti-vaccine CD8þ T cells at sites of vaccine-induced skin DTHreactions was correlated with favorable clinical outcome(23, 43). Several clinical studies in patients with cancer havereported antivaccine T-cell responses in the blood but only
Figure 6. pDC vaccination improves OS. Clinical outcome to pDC vaccination was compared with a group of carefully matched historical controlpatientswho received dacarbazine as first-line treatment. PFS for pDC vaccinationwas 4.0 versus 2.1months in the control group.MedianOSdata showed aremarkable improvement compared with matched control patients; 22.0 versus 7.6 months. Furthermore, the OS of pDC-vaccinated patients wassignificantly improved compared with matched controls. Statistical significance between the survival of the groups was determined by a log-rank test,P ¼ 0.001.
Tel et al.
Cancer Res; 73(3) February 1, 2013 Cancer Research1072
on May 24, 2020. © 2013 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 23, 2013; DOI: 10.1158/0008-5472.CAN-12-2583

in a minority of patients or after prolonged in vitro restimu-lation with antigen (44–47). Here, we observed the specificinduction of tumor specific CD8þ T cells, which indicatesthat even small numbers of pDCs can evoke antigen-specificimmune responses. To verify if this tumor specific T-cellresponse contributed to long-term tumor control, we com-pared the clinical outcome of our patients with that ofcarefully selected controls treated with standard DTIC chemo-therapy. Although it must be emphasized that this study wasnot designed to evaluate clinical outcome, several interestingobservations were made. First, PFS in vaccinated patientswas similar to that of the matched control patients, matchingPFS reported in literature (48–50). Remarkably, the 1- and2-year survival rates were 60% and 45% after pDC vaccinationcompared with 30% and less than 10% of the matched con-trol patients, respectively. To exclude that this discrepancy insurvival might partially be influenced by subsequent salvagetreatments, we carefully matched the total number of differ-ent treatments and the types of salvage treatments for bothcontrol group and the vaccinated patients (SupplementaryTable S1). Second, we detected tumor-specific CD8þ T cells in4 of 6 patients who showed a clinical response (stable diseaseor mixed response) and had a long OS (defined as more than24 months). Therefore, we hypothesize that the improved OSis related to the priming or restimulation of antitumor CD8þ
T cells, which would be in line with our previous findings (23).However, a uniform framework as a reference for immuno-monitoring is mandatory to appreciate immune responses inclinical trials. To date, no monitoring assay that evaluates asingle T-cell function exists that relates to clinical outcome.Most information about CTL frequencies is derived fromcancer germ-line genes such as MAGE (51). These frequenciesare comparable with the here-observed frequencies for differ-entiation antigen-specific T cells. In our previous study, inwhich we compared wild-type peptides and modified peptideson moDCs, increased T-cell frequencies were observed inresponding patients, slightly higher than in this study(0.01%; ref. 52). Third, given the low numbers of CTLs that wedetected, as compared with numbers reported in trials withmonocyte- or CD34þ progenitor-derived dendritic cells, it istempting to speculate that other immune cells from the innatearm play an important role in assisting CTLs. Therefore, itwould be extremely interesting to study the immune cell
repertoire within resected lymph nodes in more detail. Com-parable patterns, no effect on PFS but significantly extendedOS, were recently described for other immunotherapies, espe-cially anti-CTLA4 blockade (49). These findings support thenotion that immunotherapy may act indirectly, rather thanhaving a direct cytotoxic antitumor effect.
The interesting observation about the OS, albeit retrospec-tively, urge for a randomized phase II clinical trial to confirmthe potential of natural pDCs as an anticancer vaccine.
Disclosure of Potential Conflicts of InterestG.Winkels is employed as a Senior ProjectManager inMiltenyi Biotec GmbH.
No potential conflicts of interest were disclosed by the other authors.
Authors' ContributionsConception and design: J. Tel, D. Benitez-Ribas, C.J.A. Punt, C.G. Figdor, I.J.M.de VriesDevelopment ofmethodology:D. Benitez-Ribas, O.C. Boerman, C.J.A. Punt, I.J.M. de VriesAcquisition of data (provided animals, acquired and managed patients,provided facilities, etc.): J. Tel, E.H.J.G. Aarntzen, G. Schreibelt, B.M. Schulte, O.C. Boerman, S. Croockewit, W.J.G. Oyen, M. van Rossum, P.G. Coulie, I.J.M. deVriesAnalysis and interpretation of data (e.g., statistical analysis, biostatistics,computational analysis): J. Tel, E.H.J.G. Aarntzen, T. Baba, G. Schreibelt, B.M.Schulte, O.C. Boerman, W.J.G. Oyen, C.J.A. Punt, I.J.M. de VriesWriting, review, and/or revision of themanuscript: J. Tel, E.H.J.G. Aarntzen,G. Schreibelt, B.M. Schulte, O.C. Boerman, S. Croockewit,W.J.G. Oyen, P.G. Coulie,C.J.A. Punt, C.G. Figdor, I.J.M. de VriesAdministrative, technical, or material support (i.e., reporting or orga-nizing data, constructing databases):T. Baba, G. Schreibelt, G.Winkels, I.J.M.de VriesStudy supervision: C.J.A. Punt, I.J.M. de Vries
AcknowledgmentsThe authors thank Mandy van de Rakt, Tjitske Duiveman-de Boer, Nicole
Scharenborg, Annemiek de Boer, Michel OldeNordkamp, and Jeanette Pots foranalytic support.
Grant SupportThis researchwas supported byNederlandse organisatie voorwetenschappelijk
onderzoek (NWO) Vidi grant 917.76.363 to I.J.M. de Vries, by EU grants Cancer-immunotherapy (LSHC-CT-2006- 518234) and DC-THERA (LSHB-CT-2004-512074), by the Nijmeegs offensief tegen kanker (NOTK) foundation, the Tumorimmunology laboratory (TIL) foundation, and by the Cancer Plan of the BelgianFederal Public Service. C.G. Figdor was awarded with a NWO Spinoza prize.
The costs of publication of this article were defrayed in part by the payment ofpage charges. This article must therefore be hereby marked advertisement inaccordance with 18 U.S.C. Section 1734 solely to indicate this fact.
Received July 2, 2012; revised November 19, 2012; accepted December 2, 2012;published OnlineFirst January 23, 2013.
References1. Banchereau J, Palucka AK. Dendritic cells as therapeutic vaccines
against cancer. Nat Rev Immunol 2005;5:296–306.2. denBrokMH,Nierkens S, Figdor CG, Ruers TJM, AdemaGJ.Dendritic
cells: tools and targets for antitumor vaccination. Expert Rev Vaccines2005;4:699–710.
3. Nestle FO, Farkas A, Conrad C. Dendritic-cell-based thera-peutic vaccination against cancer. Curr Opin Immunol 2005;17:163–9.
4. Bakker AB, Schreurs MW, Tafazzul G, de Boer AJ, Kawakami Y,Adema GJ, et al. Identification of a novel peptide derived fromthe melanocyte-specific gp100 antigen as the dominant epitoperecognized by an HLA-A2.1-restricted anti-melanoma CTL line. IntJ Cancer 1995;62:97–102.
5. Brichard V, Van Pel A,Wolfel T,Wolfel C, De Plaen E, Lethe B, et al. Thetyrosinase gene codes for an antigen recognized by autologouscytolytic T lymphocytes on HLA-A2 melanomas. J Exp Med 1993;178:489–95.
6. Figdor CG, de Vries IJ, Lesterhuis WJ, Melief CJ. Dendritic cellimmunotherapy: mapping the way. Nat Med 2004;10:475–80.
7. Schreibelt G, Benitez-Ribas D, Schuurhuis D, Lambeck AJ, van Hout-Kuijer M, Schaft N, et al. Commonly used prophylactic vaccines as analternative for synthetically produced TLR ligands to mature mono-cyte-derived dendritic cells. Blood 2010;116:564–74.
8. Kadowaki N, Antonenko S, Lau JY, Liu YJ. Natural interferon alpha/beta-producing cells link innate and adaptive immunity. J Exp Med2000;192:219–26.
Human Plasmacytoid Dendritic Cells Enhance Overall Survival in Melanoma Patients
www.aacrjournals.org Cancer Res; 73(3) February 1, 2013 1073
on May 24, 2020. © 2013 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 23, 2013; DOI: 10.1158/0008-5472.CAN-12-2583

9. Farkas L, Kvale EO, Johansen FE, Jahnsen FL, Lund-Johansen F.Plasmacytoid dendritic cells activate allergen-specific TH2 memorycells: modulation by CpG oligodeoxynucleotides. J Allergy Clin Immu-nol 2004;114:436–43.
10. Ito T, Liu YJ, Kadowaki N. Functional diversity and plasticity of humandendritic cell subsets. Int J Hematol 2005;81:188–96.
11. Cella M, Facchetti F, Lanzavecchia A, Colonna M. Plasmacytoiddendritic cells activated by influenza virus and CD40L drive a potentTH1 polarization. Nat Immunol 2000;1:305–10.
12. Fonteneau JF, Gilliet M, Larsson M, Dasilva I, Munz C, Liu YJ, et al.Activation of influenza virus-specific CD4þ and CD8þ T cells: a newrole for plasmacytoid dendritic cells in adaptive immunity. Blood2003;101:3520–6.
13. Salio M, Cella M, Vermi W, Facchetti F, Palmowski MJ, Smith CL, et al.Plasmacytoid dendritic cells prime IFN-gamma-secreting melanoma-specificCD8 lymphocytes and are found in primarymelanoma lesions.Eur J Immunol 2003;33:1052–62.
14. Remer KA, Apetrei C, Schwarz T, Linden C, Moll H. Vaccination withplasmacytoid dendritic cells induces protection against infection withLeishmania major in mice. Eur J Immunol 2007;37:2463–73.
15. Schlecht G, Garcia S, Escriou N, Freitas AA, Leclerc C, Dadaglio G.Murine plasmacytoid dendritic cells induce effector/memory CD8þ T-cell responses in vivo after viral stimulation. Blood 2004;104:1808–15.
16. Salio M, Palmowski MJ, Atzberger A, Hermans IF, Cerundolo V. CpG-matured murine plasmacytoid dendritic cells are capable of in vivopriming of functional CD8 T cell responses to endogenous but notexogenous antigens. J Exp Med 2004;199:567–79.
17. Takagi H, Fukaya T, Eizumi K, Sato Y, Sato K, Shibazaki A, et al.Plasmacytoid dendritic cells are crucial for the initiation of inflamma-tion and T cell immunity in vivo. Immunity 2011;35:958–71.
18. Balch CM, Buzaid AC, Soong SJ, Atkins MB, Cascinelli N, Coit DG,et al. Final version of the American Joint Committee on Cancer stagingsystem for cutaneous melanoma. J Clin Oncol 2001;19:3635–48.
19. de Vries IJ, Lesterhuis WJ, Scharenborg NM, Engelen LP, Ruiter DJ,Gerritsen MJ, et al. Maturation of dendritic cells is a prerequisite forinducing immune responses in advanced melanoma patients. ClinCancer Res 2003;9:5091–100.
20. de Vries IJM, Lesterhuis WJ, Barentsz JO, Verdijk P, van Krieken JH,Boerman OC, et al. Magnetic resonance tracking of dendritic cells inmelanoma patients for monitoring of cellular therapy. Nat Biotechnol2005;23:1407–13.
21. de Vries IJ, Eggert AA, Scharenborg NM, Vissers JL, Lesterhuis WJ,Boerman OC, et al. Phenotypical and functional characterization ofclinical grade dendritic cells. J Immunother 2002;25:429–38.
22. Eggert AAO, Schreurs MWJ, Boerman OC, Oyen WJC, de Boer AJ,Punt CJA, et al. Biodistribution and vaccine efficiency of murinedendritic cells are dependent on the route of administration. CancerRes 1999;59:3340–5.
23. de Vries IJM, Bernsen MR, Lesterhuis WJ, Scharenborg NM, StrijkSP, Gerritsen M-JP, et al. Immunomonitoring tumor-specific T cellsin delayed-type hypersensitivity skin biopsies after dendritic cellvaccination correlates with clinical outcome. J Clin Oncol 2005;23:5779–87.
24. Labtube.tv [Internet]. Sudbury, United Kingdom: Technology Net-works Ltd.; 2011 [cited 2011 Oct 11]. Available from: http://www.labtube.tv/playvideo.aspx?vid¼131825.
25. Karanikas V, Lurquin C, Colau D, van Baren N, De Smet C, Lethe B,et al. Monoclonal anti-MAGE-3 CTL responses in melanoma patientsdisplaying tumor regression after vaccination with a recombinantcanarypox virus. J Immunol 2003;171:4898–904.
26. Wang X, Seed B. A PCR primer bank for quantitative gene expressionanalysis. Nucleic Acids Res 2003;31:e154.
27. BalchCM,Gershenwald JE, SoongSJ, Thompson JF, AtkinsMB, ByrdDR, et al. Final version of 2009 AJCC melanoma staging and classi-fication. J Clin Oncol 2009;27:6199–206.
28. de Vries IJ, Tel J, Benitez-Ribas D, Torensma R, Figdor CG. Prophy-lactic vaccines mimic synthetic CpG oligonucleotides in their ability tomodulate immune responses. Mol Immunol 2011;48:810–7.
29. De Vries IJ, Krooshoop DJ, Scharenborg NM, Lesterhuis WJ, DiepstraJH, Van Muijen GN, et al. Effective migration of antigen-pulsed den-
dritic cells to lymph nodes inmelanoma patients is determined by theirmaturation state. Cancer Res 2003;63:12–7.
30. ConradC,Meller S,GillietM. Plasmacytoid dendritic cells in the skin: tosense or not to sense nucleic acids. Semin Immunol 2009;21:101–9.
31. Treilleux I, Blay JY, Bendriss-Vermare N, Ray-Coquard I, Bachelot T,Guastalla JP, et al. Dendritic cell infiltration and prognosis of earlystage breast cancer. Clin Cancer Res 2004;10:7466–74.
32. Labidi-Galy SI, Sisirak V,MeeusP, GobertM, Treilleux I, Bajard A, et al.Quantitative and functional alterations of plasmacytoid dendritic cellscontribute to immune tolerance in ovarian cancer. Cancer Res2011;71:5423–34.
33. Diamond MS, Kinder M, Matsushita H, Mashayekhi M, Dunn GP,Archambault JM, et al. Type I interferon is selectively required bydendritic cells for immune rejection of tumors. J Exp Med 2011;208:1989–2003.
34. Fuertes MB, Kacha AK, Kline J, Woo SR, Kranz DM, Murphy KM, et al.Host type I IFN signals are required for antitumor CD8þ T cellresponses through CD8{alpha}þ dendritic cells. J Exp Med 2011;208:2005–16.
35. Kadowaki N, Ho S, Antonenko S, Malefyt RW, Kastelein RA, Bazan F,et al. Subsets of human dendritic cell precursors express different toll-like receptors and respond to different microbial antigens. J Exp Med2001;194:863–9.
36. Siegal FP, KadowakiN, ShodellM, Fitzgerald-Bocarsly PA, ShahK,HoS, et al. The nature of the principal type 1 interferon-producing cells inhuman blood. Science 1999;284:1835–7.
37. Cella M, Jarrossay D, Facchetti F, Alebardi O, Nakajima H, Lanzavec-chia A, et al. Plasmacytoid monocytes migrate to inflamed lymphnodes and produce large amounts of type I interferon. Nat Med1999;5:919–23.
38. Penna G, Vulcano M, Sozzani S, Adorini L. Differential migrationbehavior and chemokine production by myeloid and plasmacytoiddendritic cells. Hum Immunol 2002;63:1164–71.
39. YoneyamaH,MatsunoK, ZhangY, Nishiwaki T, KitabatakeM,Ueha S,et al. Evidence for recruitment of plasmacytoid dendritic cell precur-sors to inflamed lymph nodes through high endothelial venules. IntImmunol 2004;16:915–28.
40. MorseMA,ColemanRE, AkabaniG, NiehausN,ColemanD, Lyerly HK.Migration of human dendritic cells after injection in patients withmetastatic malignancies. Cancer Res 1999;59:56–8.
41. Mackensen A, Krause T, Blum U, Uhrmeister P, Mertelsmann R,Lindemann A. Homing of intravenously and intralymphatically injectedhuman dendritic cells generated in vitro from CD34þ hematopoieticprogenitor cells. Cancer Immunol Immunother 1999;48:118–22.
42. GunzerM, Friedl P, NiggemannB,Brocker EB,KampgenE, Zanker KS.Migration of dendritic cells within 3-D collagen lattices is dependent ontissue origin, state of maturation, and matrix structure and is main-tained by proinflammatory cytokines. J Leukoc Biol 2000;67:622–9.
43. LopezMN, PeredaC, Segal G,Munoz L, Aguilera R,Gonzalez FE, et al.Prolonged survival of dendritic cell-vaccinated melanoma patientscorrelates with tumor-specific delayed type IV hypersensitivityresponse and reduction of tumor growth factor {beta}-expressing Tcells. J Clin Oncol 2009;27:945–52.
44. Brossart P, Wirths S, Stuhler G, Reichardt VL, Kanz L, Brugger W.Induction of cytotoxic T-lymphocyte responses in vivo after vaccina-tions with peptide-pulsed dendritic cells. Blood 2000;96:3102–8.
45. Lau R, Wang F, Jeffery G, Marty V, Kuniyoshi J, Bade E, et al. Phase Itrial of intravenous peptide-pulsed dendritic cells in patients withmetastatic melanoma. J Immunotherapy 2001;24:66–78.
46. Speiser DE, Li�enard D, Mika€el JP, Batard P, Rimoldi D, Guillaume P,et al. In vivo activation of melanoma-specific CD8þ T cells by endog-enous tumor antigen and peptide vaccines. A comparison to virus-specific T cells. Eur J Immunol 2002;32:731–41.
47. Valmori D, Dutoit V, Schnuriger V, Quiquerez A-L, Pittet MJ, GuillaumeP, et al. Vaccinationwith amelan-Apeptide selects anoligoclonal T cellpopulation with increased functional avidity and tumor reactivity.J Immunol 2002;168:4231–40.
48. Robert C, Thomas L, Bondarenko I, O'Day S, Weber J, Garbe C, et al.Ipilimumab plus dacarbazine for previously untreated metastatic mel-anoma. N Engl J Med 2011;364:2517–26.
Tel et al.
Cancer Res; 73(3) February 1, 2013 Cancer Research1074
on May 24, 2020. © 2013 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 23, 2013; DOI: 10.1158/0008-5472.CAN-12-2583

49. Hodi FS, O'Day SJ, McDermott DF, Weber RW, Sosman JA, HaanenJB, et al. Improved survival with ipilimumab in patients with metastaticmelanoma. N Engl J Med 2010;363:711–23.
50. Chapman PB, Hauschild A, Robert C, Haanen JB, Ascierto P, Larkin J,et al. Improved survival with vemurafenib in melanoma with BRAFV600E mutation. N Engl J Med 2011;364:2507–16.
51. Lonchay C, van der Bruggen P, Connerotte T, Hanagiri T, Coulie P,Colau D, et al. Correlation between tumor regression and T cell
responses in melanoma patients vaccinated with a MAGE antigen.Proc Natl Acad Sci U S A 2004;101(Suppl 2):14631–8.
52. Lesterhuis WJ, Schreibelt G, Scharenborg NM, Brouwer HM,Gerritsen MJ, Croockewit S, et al. Wild-type and modifiedgp100 peptide-pulsed dendritic cell vaccination of advancedmelanoma patients can lead to long-term clinical responsesindependent of the peptide used. Cancer Immunol Immunother2011;60:249–60.
Human Plasmacytoid Dendritic Cells Enhance Overall Survival in Melanoma Patients
www.aacrjournals.org Cancer Res; 73(3) February 1, 2013 1075
on May 24, 2020. © 2013 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 23, 2013; DOI: 10.1158/0008-5472.CAN-12-2583

2013;73:1063-1075. Published OnlineFirst January 23, 2013.Cancer Res Jurjen Tel, Erik H.J.G. Aarntzen, Tetsuro Baba, et al. Antigen-Specific T-Cell Responses in Melanoma PatientsNatural Human Plasmacytoid Dendritic Cells Induce
Updated version
10.1158/0008-5472.CAN-12-2583doi:
Access the most recent version of this article at:
Material
Supplementary
http://cancerres.aacrjournals.org/content/suppl/2012/12/31/0008-5472.CAN-12-2583.DC1
Access the most recent supplemental material at:
Cited articles
http://cancerres.aacrjournals.org/content/73/3/1063.full#ref-list-1
This article cites 51 articles, 24 of which you can access for free at:
Citing articles
http://cancerres.aacrjournals.org/content/73/3/1063.full#related-urls
This article has been cited by 19 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerres.aacrjournals.org/content/73/3/1063To request permission to re-use all or part of this article, use this link
on May 24, 2020. © 2013 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 23, 2013; DOI: 10.1158/0008-5472.CAN-12-2583