n. 4/2016 OLORE
40
DOLORE AggiornAmenti clinici ❖ n. 4/2016 ISSN 1974-448x Organo ufficiale della Associazione Italiana per lo Studio del Dolore
Transcript of n. 4/2016 OLORE

DOLOREAggiornAmenti clinici
❖ n. 4/2016 ISSN 1974-448x
Organo ufficiale della Associazione Italiana per lo Studio del Dolore
CONGRESSO NAZIONALE
www.aisd.itNH VILLA CARPEGNA
ROMA 8-10 GIUGNO 2017
SAVE
THE DATE • SAVE TH
E DATE • SAVE THE D
ATE
•

◗ 3 ◗
AggiornAmenti clinici
Organo ufficiale della Associazione Italiana per lo Studio del Dolore
Associazione Italiana per lo Studio del Dolore AISDVia Tacito, 7 - 00193 RomaTel. 3396195974 [email protected]
Consiglio Direttivo AISD 2016-2018PresidenteEnrico PolatiPast President Caterina Aurilio
Presidente eletto per il biennio 2018-2020Stefano Coaccioli
VicepresidenteMaria Caterina Pace
SegretarioVittorio Schweiger
TesoriereGiustino Varrassi
ConsiglieriMaurizio EvangelistaDiego M. FornasariFranco MarinangeliFilomena PuntilloAndrea Truini
Direttore ResponsabileGiustino Varrassi
Segreteria ScientificaAntonella Paladini
Coordinamento RedazionaleLorenza Saini
Grafica e impaginazione a cura di Osvaldo Saverino
TRIMESTRALE Prima Reg. Trib. dell’Aquila n. 335/97Seconda Reg. Trib. dell’Aquila n. 571 del 18/12/2007
Copia omaggio riservata ai soci.Il trattamento dei dati personali avviene nel rispettodel D.lgs. 196/03. Per l’informativa completa o peresercitare i diritti di cui all’art. 7 si può scrivere [email protected] i diritti riservati.A causa dei rapidi progressi della scienza medica si raccomanda sempre una verifica indipendente delle diagnosi e dei dosaggi farmacologici riportati.
© Copyright 2017
ISSN 1974-448x
DOLORE
In questo numero
Anno Mondiale contro il dolore 4
IASP Statement on U.S. Travel Restrictions 7
New frontiers in cancer pain management 8
a palliative care perspective
Paracetamol: Is There Still a Place in Pain Management? 10
Opioid Receptor Agonists and Antagonists 13
NSAIDs for Pain Management: Benefits and Risks 17
Adjuvant Analgesics in Chronic Non Cancer Pain 22
NSAID-Opioid Combinations: Rationale and Clinical Efficacy 25
nterventional Pain Management: Pros & Cons 32
L’analgesia ai tempi dei Faraoni 37
Effetti della statistica nella medicina 38

dolore4AggiornAmenti clinici
◗ 4 ◗
Anno mondiale contro dolore
.
Nel mondo si eseguono ognianno più di 300 milioni di inter-venti chirurgici: da interventiminori a operazioni complessesu organi vitali. Il dolore postoperatorio viene consideratocome inevitabile, da sopportaree in effetti il dolore post operato-rio è stato rilevato in circa metàdei pazienti operati in varie inda-gini. Il dolore che si protrae dopo l'interventochirurgico è stato focalizzato come argomen-to di studio sistematico meritevole solo circa25 anni fa, in parte grazie agli sforzi dellaIASP®. Circa 1 paziente su 4 identifica infatti nella chi-rurgia la causa responsabile dell’insorgenzadel dolore cronico di cui soffre. Recenti datiepidemiologici hanno messo in luce come,attualmente, l’incidenza del dolore persisten-te post-operatorio sia inaccettabilmente alta epossa variare in base alla tipologia di interven-to chirurgico. Il dolore cronico si sviluppaapprossimativamente nel 50% dei pazientisottoposti ad amputazioni degli artiinferiori, chirurgia mammaria oncologica etoracotomia.Sfortunatamente, tale problematica nonè limitata solo alla chirurgia maggiore,ma anche procedure chirurgiche considerate
minori, come la riparazione diernia inguinale, sono caratterizza-te da un rischio significativo disviluppare un dolore cronicopost-operatorio (*).Da un po' di tempo la richiestadei pazienti per un più efficacetrattamento del dolore postope-ratorio sostenuto dall'impegnodei medici per tempi di degenza
più brevi e liberi dal dolore, ha trasformatol'approccio al controllo del dolore postopera-torio. Inoltre, tecniche chirurgiche minima-mente invasive e nuovi metodi per la gestionedel dolore post-chirurgico con minori effetticollaterali consentono di effettuare più proce-dure ambulatoriali o con brevi ricoveri, tuttaviail dolore spesso persiste a lungo dopo l'inter-vento chirurgico. Oggi l'approccio al dolore post operatoriodovrebbe essere così concepito:• occorre presupporre che quasi tutto il dolo-
re dopo intervento chirurgico può e deveessere gestito in modo da ottimizzare lafunzionalità fisica ed emotiva;
• valutare l'intensità del dolore a riposo e inazione per personalizzare la terapia del dolo-re rispetto alle esigenze riabilitative;
• identificare in anticipo quei pazienti chepossono richiedere una particolare attenzio-
L’International Association for the Study of Pain(IASP®) ha dedicato il tema dell'anno mondiale contro il dolore post operatorio
* Leggi anche: Dal dolore acuto postoperatorio al dolore persistente postoperatorio: possiamo prevenirlo? di Paolo Scimiaet al Dol agg clinici n. 3 2016. Si legga anche nello stesso numero del periodico: Fattori predittivi del dolore post-operato-rio acuto e cronico di Pasquale Sansone et al.

❖ n. 4 / 2016
ne; ad esempio, a causa di problemi com-portamentali o terapia con oppioidi prece-dente l’intervento;
• integrare il controllo del dolore con altriaspetti della preparazione per il recuperopost operatorio, come attività o nutrizione eassunzione di liquidi;
• adottare un approccio "multimodale" checombina diversi tipi di farmaci e (quandopossibile) l'anestesia locale per ridurre ladipendenza da una sola modalità di tratta-mento; per esempio, gli oppiacei con i loronumerosi effetti collaterali;
• tener conto delle differenze dei pazienti intermini di esperienza e report del dolore,preferenze tra i possibili trattamenti e rispo-sta alla terapia, con attenzione a fattori
come sesso ed etnia;• continuare la valutazione del paziente dopo
la dimissione per riconoscere e trattare ilprima possibile il dolore persistente e altreconseguenze chirurgiche indesiderate;
• prendere atto che la gestione del doloreacuto, post intervento chirurgico, devediventare una sottospecialità medica, vistoil miglioramento di conoscenze e tecnichespecializzate, come, per esempio, l'aneste-sia regionale.
Queste le raccomandazioni per i medici, macosa possono fare i pazienti e le loro famiglieper trarre il massimo beneficio da questirecenti progressi?- Sapere dal chirurgo se la tecnica di interven-
www.aisd.it

dolore4AggiornAmenti clinici
to proposta può generare dolore e, in casoaffermativo, farsi indicare la probabile inten-sità, la durata e come sarà gestito. Alcuneoperazioni comportano infatti un rischio didolore postoperatorio persistente più eleva-to rispetto ad altre.- Richiamare l'attenzione del chirurgo, o di
altri membri del team (anestesista, infer-miere, fisioterapista, farmacista), su aspet-ti rilevanti della propria storia medica osulla situazione attuale, problemi prece-denti di dolore, terapie del dolore in corsoe reazioni avverse ai farmaci.
- Chiedere:- Chi formulerà il mio "piano di terapia
del dolore" (anche se si tratta di unprotocollo standard di provata efficacia neipazienti che già hanno subito la stessaoperazione)?
- Il mio “piano dolore” sarà "multimodale"?Cioè combinerà diversi tipi di farmaci per iltrattamento del dolore e/o anestesialocale, per esempio anestesia epidurale oblocco del nervo in modo da ridurre ladipendenza da un singolo farmaco comela morfina?
- Quali misure saranno adottate nel casoavessi bisogno di un dosaggio di oppioidisuperiore al normale per il controllo delmio dolore (per quei pazienti che hannoricevuto un trattamento con oppioidi primadell'intervento)?
- Chi monitorerà il piano di terapia deldolore e lo regolerà o modificherà, senecessario?
- Quali sono le strategie terapeutiche per ilcontrollo del dolore dopo che sarò dimes-so dall'ospedale?
- Se il dolore persiste dopo dimissione, a chipotrò rivolgermi, giorno e notte, se la tera-pia non riesce ad assicurarmi riposo erecupero, o se l’antidolorifico mi provocaeffetti collaterali inaccettabili, o se il doloreriaffiora o peggiora?
◗ 6 ◗
Raccomandazioni più dettagliate sono tutte disponibili nel sito della IASP:www.iasp-pain.org
01 What the Public Should Know About Pain After Surgery
02 What Health-Care Professionals Should Know About Pain After Surgery
03 Pathophysiology of Acute Postoperative Pain04 Chronic Postsurgical Pain: Definition
and Impact05 Management of Postsurgical Pain in Adults:
Pharmacotherapy and Regional Anesthesia06 Behavioral Techniques including Hypnosis
for Pain After Surgery07 Management of Postsurgical Pain in Children08 Management of Postsurgical Pain in
Older Adults09 Management of Postsurgical Pain in Patients
Treated Preoperatively with Opioids10 Management of Pain Related to Surgery
and Procedures in Patients with Known or Suspected Cancer
11 Pain Management in Critical Care 12 Acupuncture for Acute Pain and Nausea
After Surgery13 Management of Patients First Presenting
with Chronic Pain After Surgery14 Using Outcomes to Improve Care: Real-Time,
Short-Term, and Long-Term.3
❖ n. 4/2016
◗ 7 ◗
Recognizing that scientific progress andmedical advances depend on the freeexchange of ideas among international net-works of diverse health-care professionalsand scientists, IASP joins with scientificsocieties in the United States and worldwidein opposing the recent White House executi-ve order on travel restrictions from certaincountries.For more than 40 years, IASP has convenedinternational meetings of scientists and clini-cians who collaborate to advance learningand discover new and better pain treatments.The U.S. travel restrictions place such colla-borations at great risk.Our member scientists and clinicians live onsix continents, treating patients suffering inpain throughout the developed and develo-ping world-including those in countriesnamed in the restrictive order. As a directconsequence of the order, IASP membersfrom those countries as well as those whohave traveled to them have told us they areunable or reluctant to travel to the UnitedStates for fear of harassment or detention atairports. Others have told us they are prote-sting the travel restrictions by refusing tomeet in the United States.IASP urges a more balanced approach toaccess to the United States that not only pro-vides for security but also protects important
scientific collaborations. We believe the tra-vel restrictions will have a negative effect onthe ability of the United States to attracttalented researchers, clinicians, and studentswhose collaborative work advances scienceand medical care.
- Judith A. Turner, PhD, President (USA)Lars Arendt-Nielsen, Prof., Dr.med., PhD, President-Elect (Denmark)
- Rolf-Detlef Treede, Prof., Dr.med., Past-President (Germany)
- Michael Nicholas, PhD, Secretary (Australia)G. Allen Finley, MD, FRCPC, Treasurer(Canada)
- Matthew R. D’Uva, FASAE, CAE, Executive Director (USA)
3 febbraio 2017More info: www.iasp-pain.org
IASP Statement on U.S. Travel Restrictions
.
Statement of the Executive Committee of the International Association
for the Study of Pain, on behalf of the organization
dolore4AggiornAmenti clinici
◗ 8 ◗
The 12th edition of the Asia-Pacific HospicesCongress is the perfect occasion to include aworkshop on cancer pain and palliative cares.The Fondazione Internazionale Menarini didnot loose such appetizing occasion. In fact,with the help of a very well known internatio-nal Faculty is proposing a WS whose titlereminds the potential audience of the borderline between Cancer Pain andPalliative Care. This border haschanged during the last fewyears, and the hospice is beco-ming the place where to carefor the suffering people thatcannot be cured at home, inhis/her terminal part of life. Theapproach at the moment isquite different than the one per-ceived in the past, when theHospice was a place to avoid,not just for the patients but alsofor the relatives.This behavioral revolution is theeffect of the cultural promotion of the bestcares for the cancer pain, and for the patientswith cancer, in general. It has been enough toopen the discussion on topics that were pre-viously forbidden. Now we are more acquain-ted with the different aspects and all thenecessities of those patients. Hence we aremore ready, at international level, to acceptthe concepts of the terminal care. Part of thiscultural revolution has been the consequen-
ce of a better knowledge of the physiopatho-logy of the disease named cancer, and all itsconsequences, but also of the availability ofnew drugs. All the topic will be discussed bya team of experts that will start discussingwhy the patient with cancer has an extreme-ly high prevalence and incidence of pain.Immediately after, many other clinical pro-
blems will be presented.Between others, in the last fewyears one of the aspects that hasreceived the attention of thescientists is the breakthroughcancer pain (BTcP). Part of theWS will be dedicated to thisaspect.Any Oncologist and Pain Doctor,but also the GeneralPractitioners, should know betterthis difficult part of PainMedicine. This is the reason whyall of us should applaude to thegenerosity of the Menarini
International Foundation, which has showngreat sensibility to accept the proposal toorganize a dedicated WS to this importanttopic. In fact, this is not only important for thebetter cure of the cancer pain patients, butfor their better care in general.
New frontiers in cancer pain management:a palliative care perspectiveJuly 26, 2017 -Suntec City, Singapore
.
Prof. Giustino Varrassi
Responsible for the Scientific Programme

◗ 9 ◗
L’ottobre scorso, dal 13 al 15 ottobre, a Budapest, il Simposio Internazionale “PainManagement: the Science Behind” ha riunito esperti internazionali sul dolore, esperti chehanno costituito le colonne portanti della scienza di base, che ha consentito lo sviluppo orga-nico e armonico delle basi neurofisiologiche e terapeutiche indispensabili per capire e cura-re al meglio il dolore. Presidenti del Comitato Scientifico del Congresso: il prof. CarmeloScarpignato (Università di Parma) e il prof. Giustino Varrassi (Università Ludes, Malta).Al Simposio, promosso dalla Fondazione Internazionale Menarini, con la collaborazionescientifica di EuLAP®, European League against Pain, abbiamo già dato ampio spazio nelnumero precedente di Dolore aggiornamenti clinici. Ora, sottoponiamo all’attenzione deinostri lettori la sintesi di alcune delle relazioni presentate. Ricordiamo che i video di tutti gli interventi sono disponibili online, previa registrazione, nelsito www.fondazione-menarini.it (sezione archivio eventi). Ringraziamo la FondazioneInternazionale Menarini per l’autorizzazione a pubblicare. Nelle pagine seguenti:
• Paracetamol: Is There Still a Place in Pain Management?, Stephan Reichenbach
• Opioid Receptor Agonists and Antagonists,Stephan A. Schug
• NSAIDs for Pain Management: Benefits and Risks,David J. Hunter
• Adjuvant Analgesics in Chronic Non Cancer Pain,Nadine Attal
• NSAID-Opioid Combinations: Rationale and Clinical Efficacy, Carmelo Scarpignato
• Interventional Pain Management: Pros & Cons, Serdar Erdine
dolore4AggiornAmenti clinici
◗ 10 ◗
. Introduction
Paracetamol (or acetaminophen, as it is calledin the USA), is one of the oldest pain killers. Itsnames derive from the chemical name, N-ace-tyl-paraaminophenol.It was introduced to the market in 1955 as anantipyretic and analgesic drug for children, and1 year later, as 500 mg tablets, as an over-the-counter drug in Great Britain. Although disco-vered more than100 years ago, its mechanismof action has not been completely elucidated.Paracetamol is prescribed for the symptomatictreatment of fever and painful conditions suchas postoperative pain, dental pain, dysmenor-rhea, headache, and acute and chronic muscu-loskeletal disease such as osteoarthritis or lowback pain. On the WHO analgesic ladder, which does notdifferentiate among origins of pain, it is inclu-ded in all three steps. It can be combined withother analgesics such as non-steroidal antiinflammatory drugs and either weak or strongopioids.
. Effectiveness of Paracetamol in Acute Painful Conditions
For postoperative painful conditions, a sin-gle oral dose of 1000 mg paracetamol pro-vides pain relief provides at least 50% pain
relief for 4 hours in about 50% of patients,with a number needed to treat (NNT) of 3.6[1]. Similar results were obtained for intra-venous (i.v.) formulations, where at least50% pain relief is achieved in 36% ofpatients, corresponding to a NNT of 5 [2].For the treatment of episodic tension-typeheadache in adults, the NNT for a singleoral dose of 1000 mg paracetamol was 22to be pain free at 2 hours, with no signifi -cant difference after 1 hour [3]. In patientswith migraine, the NNT for paracetamol1000 mg was 12 for pain-free response at2 hours [4]. Data derived from randomizedcontrolled trials comparing paracetamol toplacebo for other acute painful conditionsare scarce.
. Effectiveness of Paracetamol in Acute and Chronic Musculoskeletal Diseases
In 2014, a large randomized placebo con-trolled trial was published in the Lancet,questioning the so far universal endorse-ment of paracetamol for acute low backpain [5].A Cochrane review published in2016 did not fi nd any evidence to supportthe use of paracetamol at 4 g day up to 12weeks [6]. The use of paracetamol was also
.. Paracetamol: Is There Still a Placein Pain Management?
Stephan Reichenbach, MD
Associate Professor of Rheumatology,University Hospital and Head Musculoskeletal Research Group,Institute of Social and Preventive Medicine,University of Bern, Switzerland
❖ n. 4 / 2016
◗ 11 ◗
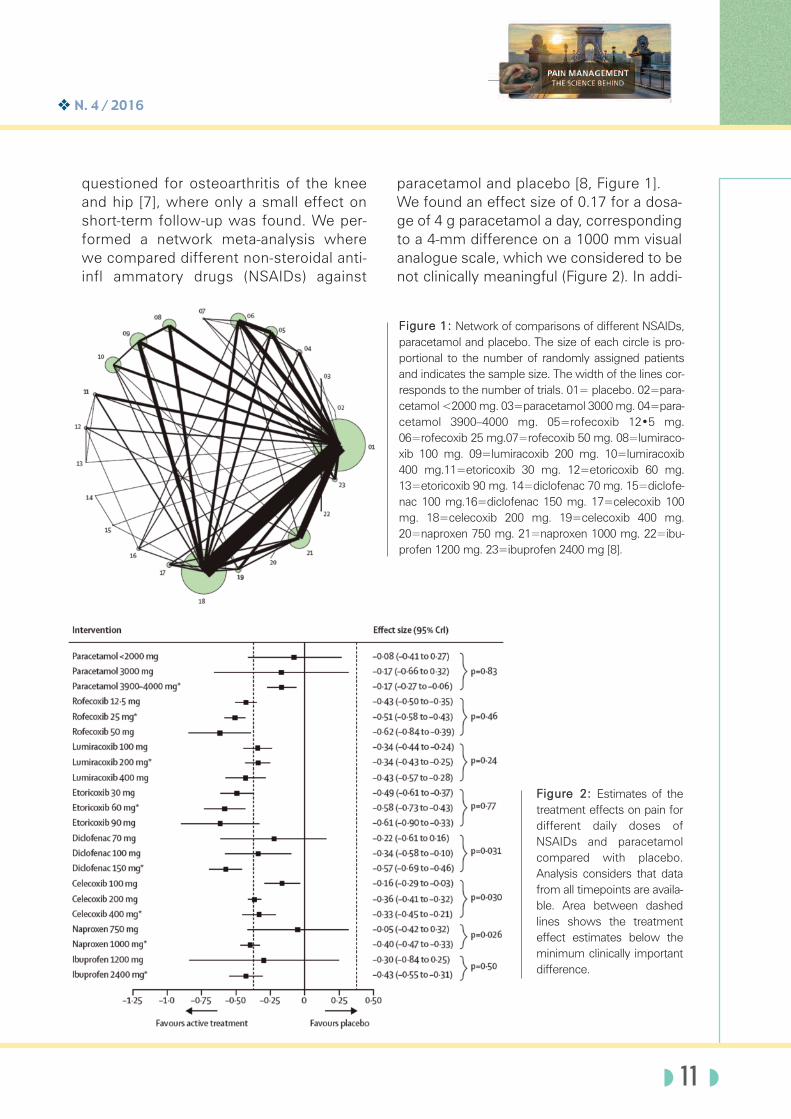
questioned for osteoarthritis of the kneeand hip [7], where only a small effect onshort-term follow-up was found. We per-formed a network meta-analysis wherewe compared different non-steroidal anti-infl ammatory drugs (NSAIDs) against
paracetamol and placebo [8, Figure 1].We found an effect size of 0.17 for a dosa-ge of 4 g paracetamol a day, correspondingto a 4-mm difference on a 1000 mm visualanalogue scale, which we considered to benot clinically meaningful (Figure 2). In addi-
Figure 1: Network of comparisons of different NSAIDs,paracetamol and placebo. The size of each circle is pro-portional to the number of randomly assigned patientsand indicates the sample size. The width of the lines cor-responds to the number of trials. 01= placebo. 02=para-cetamol <2000 mg. 03=paracetamol 3000 mg. 04=para-cetamol 3900–4000 mg. 05=rofecoxib 12•5 mg.06=rofecoxib 25 mg.07=rofecoxib 50 mg. 08=lumiraco-xib 100 mg. 09=lumiracoxib 200 mg. 10=lumiracoxib400 mg.11=etoricoxib 30 mg. 12=etoricoxib 60 mg.13=etoricoxib 90 mg. 14=diclofenac 70 mg. 15=diclofe-nac 100 mg.16=diclofenac 150 mg. 17=celecoxib 100mg. 18=celecoxib 200 mg. 19=celecoxib 400 mg.20=naproxen 750 mg. 21=naproxen 1000 mg. 22=ibu-profen 1200 mg. 23=ibuprofen 2400 mg [8].
Figure 2: Estimates of thetreatment effects on pain fordifferent daily doses ofNSAIDs and paracetamolcompared with placebo.Analysis considers that datafrom all timepoints are availa-ble. Area between dashedlines shows the treatmenteffect estimates below theminimum clinically importantdifference.
dolore4AggiornAmenti clinici
◗
tion, we found no evidence that treatmenteffects varied over time.
. Safety
Data from randomized controlled trialsdemonstrated no increased risk for anyadverse events or serious adverse events [7].However, a recently published meta-analysisof cohort studies suggested a potentiallyincreased risk of cardiovascular, gastrointe-stinal and renal adverse events [9]. The mostfeared complication, though, is that of para-cetamol poisoning, either accidental or inten-tional, leading to liver failure and approxima-
tely 150 deaths per year in the UnitedKingdom [10].
. Conclusions
Evidence from randomized controlled trialsdoes not support the use of paracetamol inacute or chronic musculoskeletal pain suchas low back pain or osteoarthritis.Accordingly, guidelines need to be modifi ed.For the treatment of acute headache andpostoperative pain, there seems to be asmall, clinically questionable effect. The roleof the combination of paracetamol withopioids should be carefully evaluated.
01) Toms L, McQuay HJ, Derry S, Moore RA. Single dose oralparacetamol (acetaminophen) for postoperative pain inadults. Cochrane Database Syst Rev 2008; 4: CD004602.
02) McNicol ED, Ferguson MC, Haroutounian S, Carr DB,Schumann R. Single dose intravenous paracetamol orintravenous propacetamol for postoperative pain.Cochrane Database Syst Rev 2016;5: CD007126.
03) Stephens G, Derry S, Moore RA. Paracetamol (aceta-minophen) for acute treatment of episodic tension-typeheadache in adults. Cochrane Database Syst Rev 2016; 6:CD011889.
04) Derry S, Moore RA. Paracetamol (acetaminophen) with orwithout an antiemetic for acute migraine headaches inadults. Cochrane Database Syst Rev 2013; 4: CD008040.
05) CM, Maher CG, Latimer J, McLachlan AJ, Hancock MJ,Day RO, Lin CW. Effi cacy of paracetamol for acute low-back pain: a double-blind, randomised controlled trial.Lancet 2014; 384: 1586-1596.
06) Saragiotto BT, Machado GC, Ferreira ML, Pinheiro MB,Abdel Shaheed C, Maher CG. Paracetamol for low backpain. Cochrane Database Syst Rev 2016, Issue 6. Art. No.:CD012230.
07) Machado GC, Maher CG, Ferreira PH, Pinheiro MB, LinCW, Day RO, McLachlan AJ, Ferreira ML. Effi cacy andsafety of paracetamol for spinal pain and osteoarthritis:systematic review and metaanalysis of randomised place-bo controlled trials. BMJ 2015; 350: h1225.
08) da Costa BR, Reichenbach S, Keller N, Nartey L, WandelS, Juni P, Trelle S. Effectiveness of nonsteroidalanti-infl ammatory drugs for the treatment of pain in kneeand hip osteoarthritis: a network meta-analysis. Lancet2016; 387: 2093-2105.
09) Roberts E, Delgado Nunes V, Buckner S, Latchem S,Constanti M, Miller P, Doherty M, Zhang W, Birrell F,Porcheret M, Dziedzic K, Bernstein I, Wise E, ConaghanPG. Paracetamol: not as safe as we thought? A -systematic literature review of observational studies. AnnRheum Dis 2016; 75:552-559.
10) Park BK, Dear JW, Antoine DJ. Paracetamol (aceta-minophen) poisoning. Systematic review. BMJ Clin Evid2015; 10: 2101.3
References
Associazione italiana per lo studio del doloredal 1976 impegnata nello studio
e nella cura del dolore
www.aisd.it

Opioid Receptor Agonists and Antagonists
.
Stephan A. Schug, MD(Cgn) FANZCA FFPMANZCA
Professor of Anaesthesiology, Pharmacology and Anaesthesiology Unit, University of Western Australia & Directorof Pain Medicine, Royal Perth Hospital Perth, Australia
.
❖ n. 4 / 2016
◗ 13 ◗
The extract of the poppy seed, opium, isamong the oldest medicines used by humankind. While its pain relieving effects weredescribed as early as 2000 BC, the sedativeeffects and the abuse potential were alsonoticed early; Paracelsus described it as “apotent pain killer”, but to “be used sparingly”.A balancing act between the therapeutic useof opioids and the medical needs for their useon the one hand and their misuse and abuseon the other hand continues. In view of theimportance of opioids, it is impossible toseparate their pharmacology and clinical usefrom the societal issues of their abuse (1).The German pharmacist Friedrich Sertürnerisolated the alkaloid morphine in 1804, butthe unravelling of the basic pharmacology ofopioids primarily took place in the last 40years and continues until today. This under-standing started with the finding of endoge-nous ligands to opioid binding sites in theearly seventies. These substances becameknown as endorphins and encephalins andpermitted understanding the complex interac-tions between opioids and their receptors. Opioid receptors are G protein-coupled recep-tors with seven hydrophobic transmembranedomains ). Three major opioid receptor sub-types, the mu-, delta- and kappa-receptors,have been identified. These receptors arehighly homologous, in particular with regardto transmembrane domains and intracellularloops. By being coupled to inhibitory pro-teins, opioids are inhibiting voltage-depen-dent calcium channels as well as activating
rectifying-potassium channels. Other mole-cular effects include the inhibition of thecyclic adenosine monophosphate pathwayand the activation of phosphorylation casca-des. The overall effect is to inhibit neuronalactivity. It is obvious that mu-receptors mediate allmorphine activities and it might, therefore, beimpossible to separate the beneficial effectsof analgesia from the potential adverseeffects such as respiratory depression, tole-rance and dependence. The discovery ofopioid receptors in the superficial dorsal horn(Laminae I and II) permitted the developmentof the concept of spinal analgesia. Current understanding of analgesic effectprovided by opioids suggests a pre- and post-synaptic effect in the dorsal horn of the spinalcord, as well as supraspinal effects in therostromedial medulla and the peri-aqueductalgrey (2). Here opioids activate so-called OFF-cells and inhibit ON-cells. Overall the resulting effect is analgesia,however, these beneficial effects are accom-panied by adverse effects including thepotentially life-threatening respiratory depres-sion [1]. Nausea and vomiting are disturbingpatients primarily in the acute setting, whileconstipation can be a significant problemwith long-term use and in cancer patients.Other side effects include urinary retention,sedation and cognitive impairment, hallucina-tions and delirium, rigidity, myoclonus andseizures as well as pruritus. Relevant adverse effects of long-term use
dolore4AggiornAmenti clinici
include the development of tolerance,although true tolerance is rarely seen with theuse of opioids in pain settings. Another phar-macological long-term effect is physicaldependence resulting in withdrawal sym-ptoms after abrupt discontinuation or admini-stration of an antagonist. In practical terms,this can be easily overcome by tapering thedose gradually. As outlined before, the issueof addiction or abuse has resulted in most ofthe societal consequences of opioid use.Such abuse is characterised by a behaviouralpattern of compulsive drug use resulting inphysical, psychological and social harm (3).Addiction or abuse were regarded as extre-mely rare in the setting of medical use ofopioids. This continues to seem to be true forthe management of acute and cancer pain.However, the increasing long term use ofopioids, either in patients with increasing sur-vival times after a cancer diagnosis or evenmore pronounced in the setting of chronicnon-malignant pain, has challenged thisassumption. In the latter setting aberrantdrug-taking behaviour has been reported in24% and current substance abuse in 43% ofpatients (4). On the other hand it is alsoimportant to recognise the issue of pseudo-addiction (5). This is defined as behaviourthat is perceived as addiction, but representsabnormal behaviour developing as a directconsequence of inadequate pain manage-ment, usually triggered by insufficient pre-scription of analgesics in settings of extremepain.With regard to use of opioids in specific clini-cal settings, opioids are an essential compo-nent of the management of severe acute painafter trauma and surgery (6). The use ofopioids by titration to effect, ideally by meansof patient-controlled analgesia (PCA), has pro-ven to be highly effective and satisfying forpatients. However, even in this setting, there
is an increasing interest in the use of opioid-sparing techniques; the acute adverse effectsof opioids, in particular with regard togastrointestinal function (nausea, vomiting,constipation), but also sedation and cognitiveimpairment, are delaying recovery after surge-ry and trauma. This is leading to increasedcomplications, impaired rehabilitation, dela-yed discharge and increased hospital costs.The concept of multimodal analgesia, i.e.combining opioids with analgesics with diffe-rent sites or mechanisms of action, has pro-ven to be a useful concept here; most acutepain services worldwide are now utilisingmultimodal analgesia to achieve opioid-spa-ring effects and thereby reduce the relianceon opioids in this setting.Similarly, in cancer pain, opioids are essentialto control severe pain and improve the quali-ty of life of patients (7). The British Hospicemovement, and subsequently the WorldHealth Organisation as outlined in a previouspresentation at this meeting, have aggressi-vely promoted the use of opioids for themanagement of cancer pain. Again in thissetting, there may be advantages of multimo-dal analgesia, but it is impossible to treatsevere cancer pain appropriately without useof opioid analgesics.The positive experiences with the use ofopioids in the setting of acute and even moreso cancer pain by the end of the last centuryhave resulted in the increasing use of opioidsin the management of chronic non-cancerpain. There was a dramatic increase in theuse of opioids in the highly industrialisedcountries of the world, in particular Canada,the United States, Australia and the EuropeanUnion. On the other hand, in about 150 coun-tries of the world, even simple oral morphinefor treatment of appropriate indications suchas cancer, postoperative and trauma pain isrestricted or barely available (8).
◗ 14 ◗
❖ n. 4 / 2016
◗ 15 ◗
From a historical point of view, the world hasswung from the 19th century, when opioidswere pretty much unregulated and, for exam-ple, freely available in the United States, tostrict controls initiated by the HarrisonNarcotic Tax Act in 1914 and further spreadaround the world by the International OpiumConvention, which lead to the SingleConvention on Narcotic Drugs (1). The adhe-rence to this convention is the task of theInternational Narcotics Control Board (INCB).This approach resulted in a time of signciant‘opiophobia’, which made it nearly impossibleto use opioids even in the setting of cancerpain (9). This was successfully overcome by,initially, the British Hospice movement andthen the world Health Organisation with theirpublication of the first Guidelines on CancerPain Relief in 1986. Regrettably, this approachhas not been successful in the whole worldand, therefore, there are now significantdiscrepancies in availability of opioids. Forexample, in 2014 countries like Canada, TheUnited States of America and Australia had anannual per capita consumption of opioidsexpressed in milligram morphine equivalentsin the range of 500-1000 milligrams, whilethese numbers for countries like India,Zambia and Nicaragua were in the range of0.5-1.0 milligrams (10).In retrospect it might have been a mistake toassume that simply transferring the conceptof acute and cancer pain management to thetreatment of chronic non-cancer pain is a validapproach (11). In the setting of chronic non-cancer pain, opioids might be more useful inwell-defined nociceptive conditions such asosteoarthritis or neuropathic pain, wherethere are good data on efficacy. However,even in these settings there are no good dataon long-term efficacy and safety of opioids.This has led to opioids being for example onlythird-line treatment for neuropathic pain
despite proven efficacy, as concerns aboutdiversion, abuse and long-term safety have tobe considered (12). The situation becomeseven more complicated in chronic pain states,which are mainly based on central sensitisa-tion and often multifactorial such as fibro-myalgia, nonspecific chronic low back pain,chronic visceral pain states and headaches(11). It is obvious that in such conditions,which are not only the result of biological, butalso psychological and social issues, opioidscannot overcome suffering, dysfunction, rele-vant psychosocial factors and are actuallyincreasing the dependence on the health caresystem and strengthening passive strategiesof pain management. Therefore, it is not sur-prising that outcome data on use of opioids inthis setting have only limited evidence ofsome short-term efficacy; meta-analysis ofrandomised controlled trials and epidemiolo-gical data suggest only weak evidence for cli-nically significant pain relief and inconclusiveand sometimes even negative effects on fun-ctional outcomes and quality of life. In addi-tion, long-term opioid use, in particular inhigher doses, can result in opioid-inducedhyperalgesia and endocrine consequencessuch as opioid-induced androgen deficiency(OPIAD).The increasing use of opioids in chronic non-malignant pain had significant consequencesnot only for patients not receiving optimalpain management, but also for the societiesin countries, which adopted this approach.This has been exemplified in a paper in theNew England Journal of Medicine in 2010with the disturbing title “A Flood of Opioids, aRising Tide of Deaths” (13). There are now fri-ghtening statistics suggesting that from 1999to 2014 more than 165,000 people in theUnited States died from prescription opioidoverdose with an annual rate of currentlybeyond 14,000 such overdose deaths (14). In
countries such as Canada, the USA, Australiaand the European Union, the use of opioids inthe last 20 years has increased so dramatical-ly that prescription opioids going on to theblack market are now the main source of ille-gal opioid use in these countries.We are now in a situation where opiophobiahas been overcome in many industrialisedcountries and has actually lead to such rela-xed attitudes that opioid use is resulting inincreased mortality and significant societal
problems. In those countries, like the UnitedStates, regulatory authorities are developingnew approaches to the use of opioids such asthe FDA a risk evaluation and mitigation stra-tegy (REMS). On the other hand, the WorldHealth Organisation continues to try to con-vince governments in other countries to makebasic opioids available for patients with can-cer pain. The search for a useful balance bet-ween appropriate use of opioids in pain andprevention of abuse will have to continue.3
dolore4AggiornAmenti clinici
◗ 16 ◗
01. Schug SA. Opioids: Clinical Use. In: McMahon SB,Koltzenburg M, Tracey I, Turk D, editors. Wall & Melzack'sTextbook of Pain. Amsterdam: Elsevier; 2013.
2. Dickenson AH, Kieffer BL. Opioids: Basic Mechanisms. In:McMahon SB, Koltzenburg M, Tracey I, Turk D, editors.Wall & Melzack's Textbook of Pain. Amsterdam: Elsevier;2013.
3. Hojsted J, Sjogren P. Addiction to opioids in chronic painpatients: a literature review. Eur J Pain 2007; 11(5): 490-518.
4. Martell BA, O'Connor PG, Kerns RD, Becker WC, MoralesKH, Kosten TR, et al. Systematic review: opioid treatmentfor chronic back pain: prevalence, efficacy, and associationwith addiction. Ann Intern Med 2007; 146(2): 116-27.
5. Weissman DE, Haddox JD. Opioid pseudoaddiction-aniatrogenic syndrome. Pain 1989; 36(3): 363-6.
6. Schug SA, Palmer GM, Scott DA, Halliwell R, Trinca J.Acute Pain Management: Scientific Evidence. 4th ed.Melbourne: ANZCA & FPM; 2015.
7. Auret K, Schug SA. Pain management for the cancerpatient - current practice and future developments. BestPract Res Clin Anaesthesiol 2013; 27(4): 545-61.
8. Anderson T. The politics of pain. BMJ 2010; 341: c3800.9. Morgan JP. American opiophobia: Customary underutiliza-
tion of opioid analgesics. Advances in Alcohol andSubstance Abuse 1985; 5: 163-73.
10. Pain & Policy Studies Group. Opioid Consumption Data,http://www.painpolicy.wisc.edu/opioid-consumption-data;[accessed 10 August 2016.
11. Freynhagen R, Geisslinger G, Schug SA. Opioids forchronic non-cancer pain. BMJ 2013; 346: f2937.
12. Finnerup NB, Attal N, Haroutounian S, McNicol E, Baron R,Dworkin RH, et al. Pharmacotherapy for neuropathic painin adults: a systematic review and meta-analysis. LancetNeurol 2015; 14(2): 162-73.
13. Okie S. A flood of opioids, a rising tide of deaths. N Engl JMed 2010;363(21):1981-5.
14. Centers for Disease Control and Prevention. InjuryPrevention & Control: Opioid Overdose,http://www.cdc.gov/drugoverdose/index.html; 2016[accessed 10 August 2016.3
References
❖ n. 4 / 2016
◗ 17 ◗
. Rationale underlying importance of analgesics
Pain is the dominant symptom in patientswith osteoarthritis (OA) and a major driver ofclinical decision-making (1). Due to its asso-ciated pain, approximately 80% of patientswith OA have some degree of movementlimitation, 25% are unable to perform majoractivities of daily living (ADL's) and 11%require help with personal care (2). Insights into the mechanisms of pain in OAare emerging and have revealed a complexbio-psychosocial process, in which the sub-chondral bone, inflammatory mediators andsensitization of peripheral and central noci-ceptive pathways play a role in the initiationand perpetuation of pain (3). In addition tothe structural pathology of OA, other factorsmay also influence the perception of painsuch as psychosocial (e.g., social isolation,catastrophizing, coping strategies, mooddisturbances) and environmental factors(e.g., culture and lifestyle) (4). Significant progress has been made in thelast few years to uncover the pathogenesisof the disease and enable the developmentof more effective drugs to alleviate sym-ptoms and minimize structural damage ofthe joint. However, no cure for establisheddisease or efficacious drugs for diseasemodification have been approved or are like-ly to appear in the immediate future (5). On
the other hand, non-pharmacological mea-sures have been associated with positiveoutcomes targeting the main goals of thetreatment of OA: pain relief and improve-ment in joint function. Weight loss and lowimpact exercises can reach improvementsin pain up to 50% (6) and, perhaps moreimportantly, are able to prevent a large num-ber of new cases of knee OA, even whenfocused on people aged 50 years and over.Despite this favorable evidence, the rate ofimplementation of these non-pharmacologi-cal strategies is low and the current care forpatients with knee OA is typically inappro-priate (7). Care is largely focused on themanagement of established disease, asopposed to prevention, and predominantlydirected to surgical replacement of the kneeand palliative therapies with little or noimpact on the protection of joint structures(8). Adequate intervention in a timelyfashion is critical to minimize the conse-quences of knee OA such as functionaldecline and slow further deterioration of thejoint (Table 1).In the context of changing evidence, poly-pharmacy in the elderly and a plethora ofavailable options, drug selection for painrelief in OA has been and will remain a chal-lenge. Every therapeutic decision involvesconsideration of risks versus benefits andfinding a balance between efficacy andtolerability.
NSAIDs for Pain Management: Benefitsand Risks
.
David Hunter, MBBS, MSc, PhD, FRACP
Professor of Medicine and Florance and Cope Chair of Rheumatology,Chair of the Institute of Bone and Joint Research, University of Sydney, Australia

. What should the first-line analgesic be for OA pain?
NSAIDs are often considered to be the pre-ferred first-line drug treatment for osteoar-thritis. They have shown efficacy similar orsuperior to paracetamol (9, 10). Systematicreviews have found NSAIDs are superior forrest pain and overall pain (11). The currentOA Research Society International (OARSI)guidelines suggest topical or oral NSAIDs,depending on the clinical context, as well asconsideration of comorbidities and potentialfor harm (12). Oral NSAIDs have larger effects on paincompared to paracetamol, albeit a higherrisk of renal, gastrointestinal (GI) and cardio-vascular (CV) complications frequently limitstheir use (13). Gastrointestinal toxicity causes over 16.500deaths and hospital admissions per year inthe USA (14). Associated cardiovascular andrenal risks are also a concern. These riskspertain to both non-selective and COX-2-selective NSAIDs, even though COX-2 inhibi-tors have a better safety profile. A meta-ana-lysis of 26 studies comparing the two foundthat COX-2 inhibitors reduced the relativerisk of dyspepsia by 12% and the absoluterisk by 3.7% (15). Other systematic reviewsand meta-analysis also confirm similar fin-dings (16).GI toxicity related to NSAIDs have beenreported by several studies and includessevere complications such as clinicallysignificant ulcers, bleeding and perforation(17). Advanced age is recognized as a majorrisk factor for adverse events related toNSAIDs. For this reason, prescription ofgastroprotective drugs such as proton-pump inhibitors (PPIs) is recommended for
this demographic group as well as forpatients with co-morbidities (18). Combiningan NSAID with a proton pump inhibitor redu-ced the relative risk of dyspepsia by 66%and the absolute risk by 9% compared to anNSAID alone (15). There is no superiority of any particularNSAID over the others but safety profilesdiffer between COX-2 selective and non-selective drugs and should be considered inthe decision of the best NSAIDs type foreach individual patient. COX-2 selectivedrugs have a safer GI profile with lower riskof ulcer complications at short-term but lessclear evidence for long-term safety (16). Onthe other hand, risk of CV harm is lower withnaproxen than with any other non-selectiveor COX-2 selective NSAIDs (16). NSAIDs should be avoided when risks out-weigh benefits such as in patients with mul-tiple comorbidities or with little response tothis type of medication. Particularly in olderpatients, serum creatinine can underestima-te the degree of renal failure and is an unre-liable indicator of glomerular filtration rate.Alternative methods such as theModification of Diet in Renal Disease(MDRD) formula should be used for this pur-pose in this population (19). The treatmentstrategy should be based on the minimumdose and duration necessary to control sym-ptoms and according to prescribing limits.The optimum duration of NSAID therapy isunclear. A meta-analysis of randomizedtrials (16) found no clear association betwe-en the duration of therapy with selective ornon-selective NSAIDs and the risk of cardio-vascular events. One small trial found conti-nuous celecoxib use to be slightly moreeffective than intermittent use on pain andfunction, with similar rates of withdrawalsdue to adverse events (20). No trials havebeen designed to assess serious gastrointe-
dolore4AggiornAmenti clinici
◗ 18 ◗
❖ n. 4 / 2016
stinal or cardiovascular harms associatedwith intermittent dosing strategies. OA painis characterized by marked fluctuations orflares. NSAIDs are effective analgesicagents, but they do not modify the under-lying disease. In light of their well-publicizedtoxicity profiles (especially adverse gastroin-testinal and cardiovascular effects), theirprescription on a long-term daily basis iscounterintuitive and rather they should begiven on an ‘as-needed basis’ at the lowesttherapeutic dose.Topical NSAIDs are a good alternative toalleviate joint pain, with similar efficacy tooral NSAIDs (especially with topical diclofe-nac solution) but no higher systemic sideeffects than placebo, due to the reducedsystemic absorption of topical formulations(5-17 fold lower systemic absorption of topi-cal diclofenac compared to its oral prepara-tion) (21, 22).
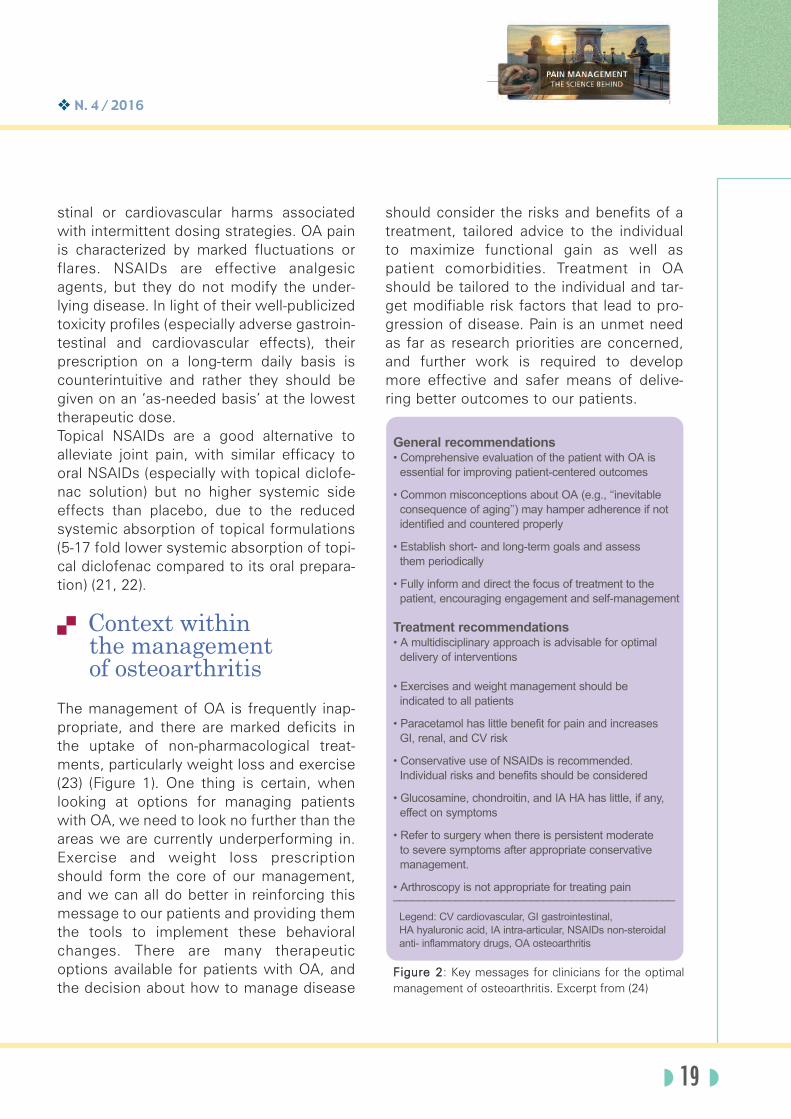
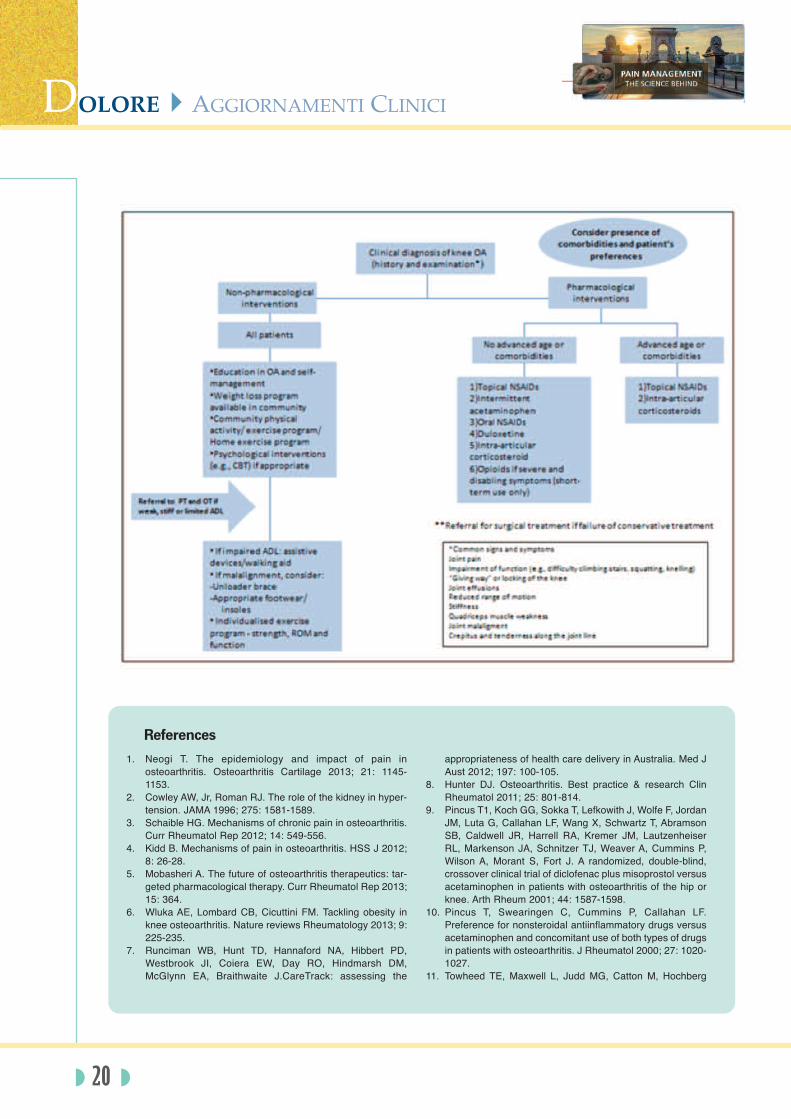
. Context within the management of osteoarthritis
The management of OA is frequently inap-propriate, and there are marked deficits inthe uptake of non-pharmacological treat-ments, particularly weight loss and exercise(23) (Figure 1). One thing is certain, whenlooking at options for managing patientswith OA, we need to look no further than theareas we are currently underperforming in.Exercise and weight loss prescriptionshould form the core of our management,and we can all do better in reinforcing thismessage to our patients and providing themthe tools to implement these behavioralchanges. There are many therapeuticoptions available for patients with OA, andthe decision about how to manage disease
should consider the risks and benefits of atreatment, tailored advice to the individualto maximize functional gain as well aspatient comorbidities. Treatment in OAshould be tailored to the individual and tar-get modifiable risk factors that lead to pro-gression of disease. Pain is an unmet needas far as research priorities are concerned,and further work is required to developmore effective and safer means of delive-ring better outcomes to our patients.
◗ 19 ◗
Figure 2: Key messages for clinicians for the optimalmanagement of osteoarthritis. Excerpt from (24)
General recommendations
• Comprehensive evaluation of the patient with OA is
essential for improving patient-centered outcomes
• Common misconceptions about OA (e.g., ‘‘inevitable
consequence of aging’’) may hamper adherence if not
identified and countered properly
• Establish short- and long-term goals and assess
them periodically
• Fully inform and direct the focus of treatment to the
patient, encouraging engagement and self-management
Treatment recommendations
• A multidisciplinary approach is advisable for optimal
delivery of interventions
• Exercises and weight management should be
indicated to all patients
• Paracetamol has little benefit for pain and increases
GI, renal, and CV risk
• Conservative use of NSAIDs is recommended.
Individual risks and benefits should be considered
• Glucosamine, chondroitin, and IA HA has little, if any,
effect on symptoms
• Refer to surgery when there is persistent moderate
to severe symptoms after appropriate conservative
management.
• Arthroscopy is not appropriate for treating pain_____________________________________________
Legend: CV cardiovascular, GI gastrointestinal,
HA hyaluronic acid, IA intra-articular, NSAIDs non-steroidal
anti- inflammatory drugs, OA osteoarthritis
dolore4AggiornAmenti clinici
◗ 20 ◗
1. Neogi T. The epidemiology and impact of pain inosteoarthritis. Osteoarthritis Cartilage 2013; 21: 1145-1153.
2. Cowley AW, Jr, Roman RJ. The role of the kidney in hyper-tension. JAMA 1996; 275: 1581-1589.
3. Schaible HG. Mechanisms of chronic pain in osteoarthritis.Curr Rheumatol Rep 2012; 14: 549-556.
4. Kidd B. Mechanisms of pain in osteoarthritis. HSS J 2012;8: 26-28.
5. Mobasheri A. The future of osteoarthritis therapeutics: tar-geted pharmacological therapy. Curr Rheumatol Rep 2013;15: 364.
6. Wluka AE, Lombard CB, Cicuttini FM. Tackling obesity inknee osteoarthritis. Nature reviews Rheumatology 2013; 9:225-235.
7. Runciman WB, Hunt TD, Hannaford NA, Hibbert PD,Westbrook JI, Coiera EW, Day RO, Hindmarsh DM,McGlynn EA, Braithwaite J.CareTrack: assessing the
appropriateness of health care delivery in Australia. Med JAust 2012; 197: 100-105.
8. Hunter DJ. Osteoarthritis. Best practice & research ClinRheumatol 2011; 25: 801-814.
9. Pincus T1, Koch GG, Sokka T, Lefkowith J, Wolfe F, JordanJM, Luta G, Callahan LF, Wang X, Schwartz T, AbramsonSB, Caldwell JR, Harrell RA, Kremer JM, LautzenheiserRL, Markenson JA, Schnitzer TJ, Weaver A, Cummins P,Wilson A, Morant S, Fort J. A randomized, double-blind,crossover clinical trial of diclofenac plus misoprostol versusacetaminophen in patients with osteoarthritis of the hip orknee. Arth Rheum 2001; 44: 1587-1598.
10. Pincus T, Swearingen C, Cummins P, Callahan LF.Preference for nonsteroidal antiinflammatory drugs versusacetaminophen and concomitant use of both types of drugsin patients with osteoarthritis. J Rheumatol 2000; 27: 1020-1027.
11. Towheed TE, Maxwell L, Judd MG, Catton M, Hochberg
References

❖ n. 4 / 2016
MC, Wells G. Acetaminophen for osteoarthritis. CochraneDatabase Syst Rev 2006; 1: CD004257.
12. McAlindon TE, Bannuru RR, Sullivan MC, Arden NK,Berenbaum F, Bierma-Zeinstra SM, et al. OARSI guide-lines for the non-surgical management of knee osteoarthri-tis. Osteoarthritis Cartilage 2014; 22: 363-388.
13. Zhang W, Jones A, Doherty M. Does paracetamol (aceta-minophen) reduce the pain of osteoarthritis? A meta-analy-sis of randomised controlled trials. Ann Rheum Dis 2004;63: 901-907.
14. McGettigan P, Henry D, McGettigan P, Henry D.Cardiovascular risk and inhibition of cyclooxygenase: asystematic review of the observational studies of selectiveand nonselective inhibitors of cyclooxygenase 2. JAMA2006; 296: 1633-1644.
15. Spiegel BM, Farid M, Dulai GS, Gralnek IM, Kanwal F,Spiegel BMR. Comparing rates of dyspepsia with Coxibsvs NSAID+PPI: a meta-analysis. Am J Med 2006; 119: 448-436.
16. Chou R, McDonagh MS, Nakamoto E, Griffin J. Analgesicsfor Osteoarthritis: An Update of the 2006 ComparativeEffectiveness Review. AHRQ Comparative EffectivenessReviews. Rockville (MD) 2011.
17. Scarpignato C, Lanas A, Blandizzi C, Lems WF, HermannM, Hunt RH for the International NSAID Consensus Group.Safe prescribing of non-steroidal anti-inflammatory drugsin patients with osteoarthritis--an expert consensusaddressing benefits as well as gastrointestinal and cardio-
vascular risks. BMC Med 2015; 13: 55.18. McAlindon TE, Bannuru RR, Sullivan MC, Arden NK,
Berenbaum F, Bierma-Zeinstra SM, et al. OARSI guide-lines for the non-surgical management of knee osteoarthri-tis. Osteoarthritis Cartilage 2014; 22: 363-388.
19. Fliser D. Assessment of renal function in elderly patients.Curr Opin Nephrol Hypertens 2008; 17: 604-608.
20. Luyten FP1, Geusens P, Malaise M, De Clerck L,Westhovens R, Raeman F, Vander Mijnsbrugge D, MathyL, Hauzeur JP, De Keyser F, Van den Bosch F. A prospec-tive randomised multicentre study comparing continuousand intermittent treatment with celecoxib in patients withosteoarthritis of the knee or hip. Ann Rheum Dis 2007; 66:99-106.
21. Kienzler JL, Gold M, Nollevaux F. Systemic bioavailabilityof topical diclofenac sodium gel 1% versus oral diclofenacsodium in healthy volunteers. J Clin Pharmacol 2010; 50:50-61.
22. Derry S, Moore RA, Rabbie R. Topical NSAIDs for chronicmusculoskeletal pain in adults. Cochrane Database SystRev 2012; 9: CD007400.
23. Basedow M, Esterman A. Assessing appropriateness ofosteoarthritis care using quality indicators: a systematicreview. J EvalClinPract 2015; 21: 782-789.
24. Deveza LA, Hunter DJ. Pain Relief for an OsteoarthriticKnee in the Elderly: A Practical Guide. Drugs Aging 2016;33: 11-20.3
◗ 21 ◗
Dialoghi, riflessioni tra medico e paziente,approfondimenti su esperienze vissute
Scaricalo gratuitamente dai sitiwww.painnursing.itwww.fondazioneprocacci.org
ilMiodolore

Adjuvant analgesics generally refer to medi-cations that are not primarily designed tocontrol pain, but can be used for this purpo-se. Some adjuvant analgesics are useful inseveral painful conditions (antidepressants,antiepileptics), while others are more speci-fic for neuropathic pain (local anesthetics,N-methyl-D-aspartate receptor antagonists).Here, we will briefly review the evidencesupporting the use of major adjuvant analge-sics (Table 1) administered at repeated dosa-ges or as topical/local agents (antidepres-sants, antiepileptics, local anesthetics, cap-saicin, botulinum toxin A) for the treatmentof chronic non cancer pain with particularemphasis on two largely studied conditions:neuropathic pain and fibromyalgia (1-4).
. Antidepressants
The analgesic efficacy of antidepressants isindependent of their antidepressant effect. It isprobably largely mediated by their action ondescending modulatory inhibitory controls, butother mechanisms such as a blockade ofsodium channels and glutamate receptors,and effect on beta2 adrenergic receptors havebeen proposed. Two antidepressant classeshave been found beneficial in neuropathic painor fibromyalgia: tricyclic antidepressants(TCAs) particularly amitriptyline in neuropathicpain and serotonin–norepinephrine reuptake
inhibitors (SNRIs) duloxetine, venlafaxine andmilnacipran (the latter has only been studied infibromyalgia). Somnolence and constipationare the most common side effects of antide-pressants, while dry mouth is more commonwith TCA and nausea is more common withduloxetine. Tertiary amine TCAs (imipramine,amitriptyline, and clomipramine) have a poorerside effect profile with major anticholinergiceffects including postural hypotension and car-diac conduction slowing, sedative side effectsand consequently risk of falls.
. Antiepileptics
Pregabalin and gabapentin In preclinical studies, the analgesic effects ofpregabalin and gabapentin are mainly relatedto a decrease in central sensitization and noci-ceptive transmission through action on thealpha-2-delta subunit of calcium channels.Their efficacy is established in peripheral orcentral NP and to a lesser extent in fibromyal-gia. Extended-release formulations of gaba-pentin (gabapentin extended release or enacar-bil) have similar efficacy and safety in clinicaltrials in NP and can be used BID. Similar effica-cy as compared to antidepressants has beenreported and their efficacy is probably higherwhen combined to antidepressants. Mostcommon side effects include somnolence, diz-ziness and weight gain. These agents have agenerally good safety profile with no drug drug
dolore4AggiornAmenti clinici
◗ 22 ◗
Adjuvant analgesics in chronic non cancer pain
.
Nadine Attal, MD
INSERM U-987, Centre d’Evaluation et de Traitement de la DouleurCHU Ambroise Paré, Boulogne-Billancourt, and Université Versailles Saint-Quentin, Versailles, France
.
❖ n. 4 / 2016
interaction. Other antiepileptics Antiepileptics other than pregabalin and gaba-pentin (e.g. topiramate, oxcarbazepine, carba-mazepine, valproate, zonisamide, lacosamide)have mainly been tested in NP and have weakor inconsistent results, with the notable excep-tion of carbamazepine in trigeminal neuralgia.All the studies of levetiracetam are negative inneuropathic pain.
. Local anesthetics
Lidocaine may reduce ectopic dischargesthrough its sodium channel–blocking proper-ties. The efficacy of lidocaine 5 % patches hasbeen assessed mainly in post-herpetic neural-gia in small duration trials (less than 3 weeks).The therapeutic gain is modest as comparedwith placebo and one large-scale trial using anenriched enrollment design failed to show adifference between lidocaine patches and pla-cebo on the primary outcome measure.However given the excellent safety profile ofthis treatment, particularly in the lack of alterna-tive safe and well tolerated medications, it isstill recommended in peripheral NP especiallyin the elderly.
. Capsaicin cream andhigh concentration patches
Capsaicin activates TRPV1 ligand-gated chan-nels on nociceptive fibers. This causes depola-rization, the initiation of an action potential, andthe transmission of pain signals to the spinalcord. After several days of application, TRPV1-containing sensory axons are desensitized, aprocess also referred to as “defunctionaliza-tion”. Standard capsaicin-containing creams(0.075%) have been found to be moderatelyeffective in post-herpetic neuralgia, but theyrequire many applications per day and cause a
burning sensation for many days before theanalgesic effect starts. The efficacy of a singleapplication of high-concentration capsaicinpatch (8%) for up to 3 months compared to alow concentration patch (0.04%) has beendemonstrated in PHN and HIV neuropathy,more recently in diabetic painful neuropathies.Better results were noted for the 60-min appli-cation in post-herpetic neuralgia and 30-minapplication in HIV-related painful polyneuropa-thy. Common adverse effects include localpain and erythema, but there is a potential riskof blood pressure elevation due to the imme-diate pain caused by the application. The long-term safety of repeated applications in patientshas not been clearly established particularlywith respect to degeneration of epidermalnerve fibers, which may be a concern in pro-gressive neuropathy.
. Botulinum toxin type A
Botulinum toxin type A (BTX-A), a potent neuro-toxin commonly used for the treatment of focalmuscle hyperactivity, may have analgesiceffects independent of its action on muscletone. Several single center randomized control-led trials have reported the long-term efficacyof BTX-A (one single set of subcutaneous injec-tions into the painful area) in peripheral neuro-pathic pain, but one unpublished study (spon-sored by Allergan) was negative (3). We haverecently reported long term efficacy of tworepeated administrations of BTX-A in peripheralneuropathic pain, with enhanced efficacy ofthe second injection (5). In published studies,the onset of efficacy (about 1 week) and dura-tion of effects (3 months) is remarkably similar.
. Emerging drug treatments
A few drugs targeting novel mechanisms ofaction are under clinical development particu-
◗ 23 ◗

larly for the treatment of neuropathic pain.These include for example subtype selectivesodium blocking agents particularly Nav1.7antagonists and novel angiotensin type II anta-gonists.
. Conclusion
Adjuvant analgesics are increasingly used for
chronic non cancer pain, particularly fibromyal-gia and neuropathic pain. Recommendationshave recently been proposed concerning theiruse in these chronic pain conditions (1-4). Newdrug treatments are also being developed andshould contribute to reduce the therapeutic fai-lures which are still a major concern in chronicnon cancer pain.
dolore4AggiornAmenti clinici
◗ 24
1. Attal N, Bouhassira D. Pharmacotherapy of neuropathicpain: which drugs, which treatment algorithms? Pain 2015;156 Suppl 1: S104-14.
2. Finnerup NB, Attal N, Haroutounian S, McNicol E, BaronR, Dworkin RH, Gilron I, Haanpaa M, Hansson, P, JensenTS, Kamerman PR, Lund K, Moore A, Raja SR, Rice ASC,Rowbotham M, Sena E, Siddall P, Smith B, Wallace M.Pharmacotherapy for neuropathic pain in adults: systemat-ic review, meta-analysis and NeuPSIG recommendations.Lancet Neurol 2015; 14(2): 162-173.
3. Macfarlane GJ, Kronisch C, Dean LE, Atzeni F, HäuserW, Fluß E, Choy E, Kosek E, Amris K, Branco J, Dincer F,Leino-Arjas P, Longley K, McCarthy GM, Makri S, Perrot S,Sarzi-Puttini P, Taylor A, Jones GT. EULAR revised recom-
mendations for the management of fibromyalgia. AnnRheum Dis 2016 Jul 4 doi:10.1136/annrheumdis-2016-209724.
4. Nüesch E, Häuser W, Bernardy K, Barth J, Jüni P.Comparative efficacy of pharmacological and non-pharma-cological interventions in fibromyalgia syndrome: networkmeta-analysis. Ann Rheum Dis 2013; 72(6): 955-962.
5. Attal N, de Andrade DC, Adam F, Ranoux D, Teixeira MJ,Galhardoni R, Raicher I, Üçeyler N, Sommer C,Bouhassira D. Safety and efficacy of repeated injections ofbotulinum toxin A in peripheral neuropathic pain (BOT-NEP): a randomised, double-blind, placebo-controlled trial.Lancet Neurol 2016; 15(6): 555-565. 3
References
SEI SOCIO DELL'ASSOCIAZIONE ITALIANA PER LO STUDIO DEL DOLORE?
HAI DIRITTOALL’ABBONAMENTO ONLINE GRATUITOall’European Journal of Pain
www.efic.org

❖ n. 4 / 2016
◗ 25 ◗
NSAID-Opioid Combinations:Rationale and Clinical Efficacy
.
Carmelo Scarpignato, MD, DSc, PharmD (h.c.),
MPH, FRCP (Hon), FACP, FCP, FACG, AGAF
Professor of Clinical Pharmacology, University of Parma, ItalyAssociate Professor of Gastroenterology, University of Nantes, FranceGeneral Secretary, World Organization for EsophagealDiseases (OESO), Paris, FranceGovernor for Italy, American College of Gastroenterology (ACG)
with the cooperation of Anna Bertelé, MDConsultant Physician & Gastroenterologist
Pain is the most common symptom reportedin both the general population and the generalmedical setting [1-3] and pain medications arethe second most prescribed class of drugs(after cardiac–renal drugs), accounting for 12%of all medications prescribed during ambulato-ry offi ce visits in the United States [4].Although pain treatment remains suboptimal,pain medicine research has led to significantpharmacologic, behavioral, and rehabilitationadvances, including the development of neuro-biologic therapies targeted at specific neuralnetworks and systems. Major progress in theunderstanding of opioid pharmacology hasoffered to clinicians a wider range of indica-tions for these drugs, alone or in combinationwith other agents, especially in non-cancerpain [5]. It is difficult to achieve effective pain controlusing a single treatment, for several reasons.Most analgesics cannot be prescribed at unli-mited doses due to the ceiling of effi cacyand/or safety and tolerability concerns, such asliver damage (this is the case of paracetamol,for instance), gastrointestinal (GI) and cardiova-scular (CV) risks [for both non-selective andcyclooxygenase-2 (COX-2) selective non-steroi-dal anti-infl ammatory drugs (NSAIDs)], orsedation, constipation and other effects of
opioid agonists [6]. Combining drugs from dif-ferent classes offers effective analgesia atreduced doses of individual agents, which mayreduce the severity of dose-related adverseevents [7]. Another limitation of single-agentanalgesia is that many patients experiencepain due to multiple causes. It is very unlikelythat any single therapy will be able to targetevery pain mechanism for these patients, so itis logical to combine drugs with differentmechanisms of action. This approach offersincreased effi cacy due to additive or synergi-stic effects without increasing the dose. Theideal combination regimen would both enhan-ce analgesic efficacy and reduce side effectscompared with either treatment alone.
. Currently Available Analgesic Drug Combinations
A number of analgesic drug combinationshave been tested for the management of post-operative pain, including paracetamol withweak, (e.g. tramadol or codeine) or strong, (e.g.morphine or oxycodone) opioids. Besidesbeing less effective than NSAIDs [8, 9], parace-tamol may not be as safe as originally believed,
both from a GI and CV perspective, not to men-tion the well-known hepatotoxicity (especiallyat doses higher than 3 g daily) [10, 11]. Despiteadding codeine to paracetamol producesworthwhile additional pain relief [12], none ofthe available studies found this combination tobe superior to NSAIDs in controlling postopera-tive pain [13]. Combining an effective NSAIDwith weak opioids could represent therefore abetter alternative.
. NSAIDs: Pharmacologyand Clinical Use of Selected Compounds
NSAIDs are very effective drugs [14-15], buttheir use is associated with a broad spectrumof adverse reactions involving the liver, kid-ney, CV system, skin and gut [16]. GI sideeffects are the most common and cover awide clinical spectrum ranging from dyspep-sia, heartburn and abdominal discomfort tomore serious events, such as peptic ulcerwith life-threatening complications of blee-ding and perforation [17,18]. Differentattempts have been made to reduce NSAID-induced gastro-duodenal damage [18]. Theseinclude enteric-coated preparations or solu-ble formulations of NSAIDs to reduce thegastric residence time and thus contact withgastric mucosa, buffered preparations, non-acidic pro-drugs and the development ofenantiomers. The chiral switch of NSAIDsproved to be a rational approach to improveboth effi cacy [19] and safety [20] of this classof drugs.
Ibuprofen is one of the most popular NSAIDs,introduced in the United Kingdom in the 60’sand in the United States in 70’s. Ibuprofen is aracemate. The R(-) isomer is converted in the
body to the more active S(+) isomer afterabsorption in the GI tract. Ex vivo inhibition ofboth COX-1 and COX-2 isoenzymes at the pla-sma concentrations, achieved following inge-stion of 400 mg ibuprofen in dental and otherinfl ammatory pain models, provides evidenceof its main mechanism of action. R(-)-ibuprofeninhibits leucocyte activation, neural activity andspinal transmission, thus contributing to theeffects of racemic ibuprofen in infl ammatorypain [21]. Recent evidence from large-scaleclinical trials with the newer COX-2 selectiveinhibitors, where this NSAID was as a com-parator, has confirmed earlier studies, showingthat ibuprofen has comparable therapeuticbenefi ts with COX-2 selective and non-selecti-ve NSAIDs. Both clinical trials and epidemiolo-gical studies have shown that ibuprofen hasrelatively low risks for GI and hepato-renaladverse effects, compared to other NSAIDs. Ahigher risk of CV events has been reported insome studies, but the risks are in general lowerthan observed with some COX-2 inhibitors (likerofecoxib or etoricoxib) and diclofenac. Thepossibility that ibuprofen may interfere with theanti-platelet effects of aspirin has given rise tocaution on its use in patients that are at CV risk,who take aspirin for primary or secondary pre-vention [22].While inhibition of prostanoid syn-thesis remains an important analgesic mode ofaction for NSAIDs both in the periphery and thecentral nervous system (CNS), other mecha-nisms should be considered [23]. SomeNSAIDs, in addition to their effects on prosta-noid synthesis, also affect the synthesis andactivity of other neuroactive substances, belie-ved to have key roles in processing nocicepti-ve input within the dorsal horn. It has beenargued that these other actions, in conjunctionwith COX inhibition, may synergistically aug-ment the effects of NSAIDs on spinal nocicep-tive processing. When the clinical effi cacy of
dolore4AggiornAmenti clinici
◗ 26 ◗
❖ n. 4 / 2016
NSAIDs in dental pain is plotted against theratio between anti-infl ammatory and analgesicactivities in experimental models, ketoprofenappears to be the most effective analgesicamongst the different NSAIDs [23]. Along thesame lines, a recent meta-analysis of 13 rando-mized controlled trials (RCTs) involving 898patients [24] found that the efficacy of oralketoprofen in relieving moderate to severe painwas significantly better than that achieved withibuprofen and/or diclofenac.
Dexketoprofen trometamol is a water-solublesalt of the active stereoisomer of ketoprofen,one of the most potent COX inhibitors in vitro.The analgesic effi cacy of oral dex-ketoprofentrometamol (10 to 20 mg) is superior to that ofplacebo and similar to that of ibuprofen 400mg in patients with moderate to severe dentalpain. The time to onset of pain relief appears tobe shorter in patients treated with dex-ketopro-fen trometamol than in those treated with ibu-profen. This NSAID is well tolerated, with areported incidence of adverse events similar tothat of placebo [25]. A systematic review of theavailable studies concluded that dex-ketopro-fen is at least as effective as other NSAIDs orparacetamol/opioid combinations [26].
. Opioids: Pharmacologyand Clinical Use of Selected Compounds
Opioid therapy continues to be an important“mainstream” option for the relief of pain,despite continued debate over the effi cacyand safety of utilizing opioids with chronic non-cancer populations. The recognition that opioidtherapy can relieve pain and improve moodand functioning in many patients with chronicpain has led experts on pain to recommend
that such patients not be denied opioids [5].Opioids represent indeed the most effectivepain relieving medications. This has led guide-lines to recommend their use in patients withpersistent moderate-to-severe pain [27-31].Despite these recommendations, manyclinicians without specialist knowledge of painmanagement remain reluctant to prescribeopioids for chronic pain of non-malignantorigin. A systematic review of 34 trials including 4212patients provided information on adverseevents related to opioid use in treating non-cancer pain [32]. Only three side effects occur-red signifi cantly more frequently with opioids:nausea, constipation and somnolence, withexcess rates over placebo of 14%, 9% and6%, respectively. A substantial proportion ofpatients on opioids (22%) withdrew becauseof adverse events. Because most trials wereshort (<4 weeks) and did not titrate the dose,the implications for long-term use in clinicalpractice are less certain. Eisenberg et al. [33]also reported on adverse events in their syste-matic review of opioids for neuropathic pain.Opioid therapy compared to placebo resultedin higher reporting of nausea (33% versus 9%),constipation (33% versus 10%), drowsiness(29% versus 12%), dizziness (21% versus 6%)and vomiting (15% versus 3%). Where repor-ted, more patients on opioids withdrew becau-se of adverse effects (11% versus 4%).
Oxycodone is a semisynthetic opioid analge-sic that acts as an agonist at μ- and κ-opioidreceptors in the CNS and has additional effectson smooth muscle. It is available as immediaterelease and controlled release formulations.Oxycodone has good oral bioavailability andproduces more predictableplasma concentra-tions than morphine, which has a poor andmore variable bioavailability. Oxycodone has
◗ 27 ◗
clinically significant drug interactions withdrugs affecting cytochrome P450 3A enzymes.The efficacy of oxycodone in managing neuro-pathic and somatic pain, both of malignant andnon-malignant origin, has been established in awide range of settings [34]. Side effects arethose common to opioids: mainly nausea, con-stipation and drowsiness. Vomiting, pruritusand dizziness are less common. The intensity ofthese side effects tends to decrease over time.Oxycodone causes somewhat less nausea, hal-lucinations and pruritus than morphine [35].
Tramadol is an analgesic with dual mecha-nisms of action: opioid receptor activation andenhancement of serotonin and norepinephrinetransmission [36]. Although the relative degreeof contribution of each mechanism toward paincontrol is not fully understood, the drug provedto be beneficial in the treatment of a wide rangeof acute and chronic pain syndromes, includingneuropathic pain. Its the analgesic efficacy canfurther be improved by combination with anon-opioid analgesic [37]. Most importantly,tramadol does not induce signifi cant respirato-ry depression or constipation and proved to bean effective and well-tolerated analgesic agentin the perioperative setting [38].
. NSAID-opioid Fixed-dose Combinations
Oxycodone-ibuprofen (5 mg/400 mg) is anoral fi xed-dose combination tablet. It is appro-ved in the US for the short-term (up to 7 days)management of acute, moderate-to-severepain and was the he fi rst fi xed-dose combina-tion (FDC), containing an NSAID and an opioid.A single tablet provided better analgesia thanlowdose oxycodone or ibuprofen, administe-red alone, in most trials and appeared to bemore effective than a single dose of someother fi xed-dose combination analgesics.
While co-administration of ibuprofen and oxy-codone in experimental models producessynergistic analgesia, clinical trials showedonly an additive effect [39]. Onset of pain relief was experienced by 90%of oxycodone/ibuprofen recipients comparedwith 36% of placebo recipients over the 6-hourpost-administration period. The oxycodone/ibu-profen combination was generally well tolera-ted in patients with acute, moderate-to-severepostoperative pain. Nausea, dizziness andsomnolence were the treatment-related adver-se events that occurred most frequently after asingle dose or multiple doses. Most (52%)adverse events that occurred with multipledoses of oxycodone/ibuprofen were of mildseverity.Oxycodone/ibuprofen FDC is therefore aneffective, convenient treatment option for theshort-term management of acute, moderate-to-severe pain [39]. Animal studies have shownthat the combination of dex-ketopropen withtramadol is synergic for the inhibition of noci-ception in different models of infl ammatorypain [40]. Along the same lines, the intra-articu-lar administration of both drugs producedsynergistic antinociceptive effects in the modelof monosodium iodoacetate-induced osteoar-thritis in rats [41]. A dexketoprofen-trama-dol FDC was recently evaluated for its analge-sic activity in acute dental pain. Four differentfixed combinations and as single componentsin comparison to placebo, on moderate tosevere acute pain following impacted thirdmandibular molar tooth extraction. This phaseII study was performed in more than 600patients in 16 clinical sites located in 6European countries. Dexketoprofen trometa-mol 25 mg combined with tramadol hydrochlo-ride 75 mg provided the best analgesia withrapid onset and long (median: 8.1 h) duration(Figure 1). The combination proved to be cost-effective, with a number needed to treat (NNT)of 1.2 (Figure 2). Adverse events were unre-
◗ 28 ◗
dolore4AggiornAmenti clinici

◗ 29 ◗
❖ n. 4 / 2016
Figure 1: Percentage of patients showing response (> 50% max TOTPAR) over 6 h post-dose (Primary Endpoint).Maximum TOTPAR corresponds to the theoretical maximum possible time-weighted sum of the PAR scores, measuredon a 5-point VRS (0=’none’ to 4=’complete’) (from Moore et al. [42]).
Figure 2: NNT for > 50% max TOTPAR compared with placebo over six hours post-dose. Maximum TOTPARcorresponds to the theoretical maximum possible time-weighted sum of the PAR scores, measured on a 5-pointVRS (0=’none’ to 4=’complete’). Bars show 95% confi dence interval of NNT, with colour change as pointestimate (Note that TRAM37.5 was not signifi cantly better than placebo) (from Moore et al. [42]).

markable [42]. Two phase III clinical trials [43, 44]in post-surgical moderate to severe acute pain,have been completed and included some 1200patients in about 80 clinical centers located in 14European and Asian countries. The studies confirmed that the dexketoprofen trometamol 25 mg+ tramadol hydrochloride 75 mg FDC was ableto provide a level of analgesia above the oneachievable by each component alone and pre-sented a safety profi le consistent with what
was previously reported for dexketoprofen tro-metamol and tramadol hydrochloride whenused as single agents [43, 44].In conclusion the US approved ibuprofen-oxy-codone combination and the recently EMAapproved dexketoprofen-tramadol combina-tion are effective analgesic medications andrepresent useful addition to our therapeuticarmamentarium to faith pain.
dolore4AggiornAmenti clinici
◗ 30 ◗
01) Sternbach RA. Survey of pain in the United States: TheNuprin Pain Report. Clin J Pain 1986; 2:49-53.
02) Verhaak PF, Kerssens JJ, Dekker J, Sorbi MJ, Bensing JM.Prevalence of chronic benign pain disorder among adults:a review of the literature. Pain 1998; 77: 231-239.
03) Kroenke K. Patients presenting with somatic complaints:epidemiology, psychiatric comorbidity and management.Int J Methods Psychiatr Res 2003; 12: 34-43.
04) Turk DC. Clinical effectiveness and cost-effectiveness oftreatments for patients with chronic pain. Clin J Pain 2002;18: 355-365.
05) Dubois MY, Gallagher RM, Lippe PM. Pain medicine posi-tion paper. Pain Med 2009; 10: 972-1000.
06) Schug SA, Garrett WR, Gillespie G. Opioid and non-opioidanalgesics. Best Pract Res Clin Anaesthesiol 2003; 17: 91-110
07) Kehlet H, Dahl JB. The value of “multimodal” or “balancedanalgesia” in postoperative pain treatment. Anesth Analg1993; 77: 1048-1056
08) Machado GC, Maher CG, Ferreira PH, Pinheiro MB, LinCW, Day RO, McLachlan AJ, Ferreira ML. Effi cacy andsafety of paracetamol for spinal pain and osteoarthritis:systematic review and metaanalysis of randomised place-bo controlled trials. BMJ 2015; 350: h1225.
09) da Costa BR, Reichenbach S, Keller N, Nartey L, WandelS, Juni P, Trelle S. Effectiveness of nonsteroidalantiinflammatory drugs for the treatment of pain in kneeand hip osteoarthritis: a network meta-analysis. Lancet2016; [Epub ahead of print]
10) Roberts E, Delgado Nunes V, Buckner S, Latchem S,Constanti M, Miller P, Doherty M, Zhang W, Birrell F,Porcheret M, Dziedzic K, Bernstein I, Wise E, ConaghanPG. Paracetamol: not as safe as we thought? A systemat-ic literature review of observational studies. Ann RheumDis 2016; 75:552-559.
11) Scarpignato C, Lanas A, Blandizzi C, Lems WF, HermannM, Hunt RH; International NSAID Consensus Group. Safeprescribing of non-steroidal anti-infl ammatory drugs inpatients with osteoarthritis – an expert consensus address-ing benefi ts as well as gastrointestinal and cardiovascularrisks. BMC Med 2015; 13: 55.
12) Moore A, Collins S, Carroll D, McQuay H. Paracetamol with
and without codeine in acute pain: a quantitativesystematic review. Pain 1997; 70: 193-201.
13) Nauta M, Landsmeer ML, Koren G. Codeine-acetamino-phen versus nonsteroidal anti-inflammatory drugs in thetreatment of post-abdominal surgery pain: a systematicreview of randomized trials. Am J Surg 2009; 198: 256-261.
14) Brooks PM, Day RO. Nonsteroidal anti-inflammatory drugs--differences and similarities. N Engl J Med 1991; 324:1716-25.
15) Tramèr MR, Williams JE, Carroll D, Wiffen PJ, Moore RA,McQuay HJ. Comparing analgesic efficacy of non-steroidalanti-infl ammatory drugs given by different routes in acuteand chronic pain: a qualitative systematic review. ActaAnaesthesiol Scand 1998; 42: 71-79.
16) Aronson JK. Meyler’s Side Effects of Analgesics andAnti-Inflammatory Drugs. Amsterdam: Elsevier; 2009.
17) Lanas A, Hunt R. Prevention of anti-inflammatory drug-induced gastrointestinal damage: benefi ts and risks oftherapeutic strategies. Ann Med 2006; 38: 415-28.
18) Scarpignato C, Hunt RH. Nonsteroidal anti-inflammatorydrug-related injury to the gastrointestinal tract: clinicalpicture, pathogenesis, and prevention. Gastroenterol ClinNorth Am 2010; 39: 433-64.
19) Hardikar MS. Chiral non-steroidal anti-inflammatory drugs –a review. J Indian Med Assoc 2008;106: 615-618.
20) Scarpignato C, Bjarnason I, Bretagne JF, De PouvourvilleG, Garcìa-Rodriguez LA, Goldstein JL, Muller P, Simon B.Working team report: towards a GI safer anti-inflammatorytherapy. GastroenterologyInt 1999; 12: 186-215.
21) Rainsford KD. Ibuprofen: from invention to an OTC thera-peutic mainstay. Int J Clin Pract Suppl. 2013 Jan;(178):9-20. Rainsford KD. Ibuprofen: from invention to an OTCtherapeutic mainstay. IntJ Clin Pract Suppl 2013; 178: 9-20.
22) Rainsford KD. Ibuprofen: pharmacology, efficacy andsafety. Inflammopharmacology 2009; 17:275-342.
23) McCormack K. The spinal actions of nonsteroidalanti-infl ammatory drugs and the dissociation between theiranti-infl ammatory and analgesic effects. Drugs 1994; 47(Suppl 5): 28-45.
24) Sarzi-Puttini P, Atzeni F, Lanata L, Bagnasco M. Efficacy ofketoprofen vs. ibuprofen and diclofenac: a systematic
References
❖ n. 4/2016
◗ 31 ◗
review of the literature and meta-analysis. Clin ExpRheumatol 2013; 31: 731-738.
25) Mauleón D, Artigas R, García ML, Carganico G. Preclinicaland clinical development of dexketoprofen. Drugs 1996; 52(Suppl 5): 24-45.
26) Moore RA, Barden J. Systematic review of dexketoprofenin acute and chronic pain. BMC Clin Pharmacol 2008; 8:11.
27) Chou R, Fanciullo GJ, Fine PG, Adler JA, Ballantyne JC,Davies P, Donovan MI, Fishbain DA, Foley KM, Fudin J,Gilson AM, Kelter A, Mauskop A, O’Connor PG, Passik SD,Pasternak GW, Portenoy RK, Rich BA, Roberts RG, ToddKH, Miaskowski C; American Pain Society-AmericanAcademy of Pain Medicine Opioids Guidelines Panel.Clinical guidelines for the use of chronic opioid therapy inchronic noncancer pain. J Pain 2009; 10: 113-130.
28) Nuckols TK, Anderson L, Popescu I, Diamant AL, Doyle B,Di Capua P, Chou R. Opioid prescribing: a systematicreview and critical appraisal of guidelines for chronic pain.Ann Intern Med 2014; 160:38-47.
29) Cheung CW, Qiu Q, Choi SW, Moore B, Goucke R, Irwin M.Chronic opioid therapy for chronic non-cancer pain: areview and comparison of treatment guidelines. PainPhysician 2014; 17: 401-414.
30) Berna C, Kulich RJ, Rathmell JP. Tapering Long-termOpioid Therapy in Chronic Noncancer Pain: Evidence andRecommendations for Everyday Practice. Mayo Clin Proc2015; 90: 828-842.
31) Brooks A, Kominek C, Pham TC, Fudin J. Exploring the Useof Chronic Opioid Therapy for Chronic Pain: When, How,and for Whom? Med Clin North Am 2016; 100: 81-102.
32) Moore RA, McQuay HJ. Prevalence of opioid adverseevents in chronic non-malignant pain: systematic review ofrandomised trials of oral opioids. Arthritis Res Ther 2005;7: R1046-51.
33) Eisenberg E, McNicol E, Carr DB. Opioids for neuropathicpain. Cochrane Database Syst Rev 2006; 3: CD006146.
34) Riley J, Eisenberg E, Muller-Schwefe G, Drewes AM,Arendt-Nielsen L. Oxycodone: a review of its use in themanagement of pain. Curr Med Res Opin 2008; 24: 175-192.
35) Ordóñez Gallego A, González Barón M, Espinosa Arranz E.Oxycodone: a pharmacological and clinical review. Clin
Transl Oncol 2007; 9: 298-307.36) Reeves RR, Burke RS. Tramadol: basic pharmacology and
emerging concepts. Drugs Today (Barc) 2008; 44: 827-836.
37) Scott LJ, Perry CM. Tramadol: a review of its use inperioperative pain. Drugs. 2000; 60: 139-176.
38) Katz WA. Pharmacology and clinical experience withtramadol in osteoarthritis. Drugs 1996; 52 (Suppl 3): 39-47.
39) Oldfi eld V, Perry CM. Oxycodone/Ibuprofen combinationtablet: a review of its use in the management of acute pain.Drugs 2005; 65: 2337-2354.
40) Miranda HF, Romero MA, Puig MM. Antinociceptive andanti-exudative synergism between dexketoprofen and tra-madol in a model of inflammatory pain in mice. FundamClin Pharmacol 2012; 26: 373-382.
41) Cialdai C, Giuliani S, Valenti C, Tramontana M, Maggi CA.Comparison between oral and intraarticular antinociceptiveeffect of dexketoprofen and tramadol combination inmonosodium iodoacetate- induced osteoarthritis in rats.Eur J Pharmacol 2013; 714: 346-351.
42) Moore RA, Gay-Escoda C, Figueiredo R, Tóth-Bagi Z,Dietrich T, Milleri S, Torres-Lagares D, Hill CM, García-García A, Coulthard P, Wojtowicz A, Matenko D,Peñarrocha-Diago M, Cuadripani S, Pizà-Vallespir B,Guerrero-Bayón C, Bertolotti M, Contini MP, Scartoni S,Nizzardo A, Capriati A, Maggi CA. Dexketoprofen/tramadol:randomised double-blind trial and confirmation of empiricaltheory of combination analgesics in acute pain. JHeadache Pain 2015; 16: 541.
43) Moore RA, McQuay HJ, Tomaszewski J, Raba G, TutunaruD, Lietuviete N, Galad J, Hagymasy L, Melka D, Kotarski J,Rechberger T, Fulesdi B, Nizzardo A, Guerrero-Bayón C,Cuadripani S, Pizà-Vallespir B, Bertolotti M.Dexketoprofen/tramadol 25 mg/75 mg: randomised dou-ble-blind trial in moderate-to-severe acute pain afterabdominal hysterectomy. BMC Anesthesiol 2016; 16: 9.
44) McQuay HJ, Moore RA, Berta A, Gainutdinovs O, FulesdiB, Porvaneckas N, Petronis S, Mitkovic M, Bucsi L,Samson L, Zegunis V, Ankin ML, Bertolotti M, Pizà-Vallespir B, Cuadripani S, Contini MP, Nizzardo A.Randomized clinical trial of dexketoprofen/tramadol 25mg/75 mg in moderate-tosevere pain after total hip arthro-plasty. Br J Anaesth 2016; 116: 269-276.3
Seguici su:
Seguici su:
Seguici su:
www.facebook.com/MedicinaDolore/
Interventional pain management techniques areminimally invasive procedures, including percu-taneous precision needle placement, with pla-cement of drugs in targeted areas or ablation oftargeted nerves and some surgical techniques,such as laser or endoscopic discectomy, intra-thecal infusion pumps and spinal cord stimula-tors, for the diagnosis and management of chro-nic, persistent or intractable pain. The interven-tional pain procedures are indicated when paincannot be relieved by conservative manage-ment or there are unacceptable side effects forother treatments of chronic pain. In the lastthree decades there is a visible increase in thenumber of interventional pain procedures (1).The classification of interventional pain procedu-res are presented in Table 1 (2).Today’s medicine is increasingly based on thebiomedical system. Biomedicine is a failed pro-mise of the late Industrial Age. It does not workwell for most chronic diseases, especially pain.The schism between those providers who fun-ction with a biomedical model and those whoutilize a biopsychosocial model has impaired thedevelopment of pain management. The biome-dical system uses the interventional pain proce-dures in its own way harming the patient (3).On the other hand the biopsychosocial systemaccepts the patient as a human being, as a chro-nic pain patient having a chronic pain disease inits own right.Over the past several decades, some of thechanges have been positive, whereas othershave been deleterious. An interventionalist per-ceives a multidisciplinary or comprehensive pro-
gram as one with interventional techniques asthe primary modality and physical and psycholo-gical applications as secondary components.In contrast, a psychiatrist, rehabilitation specia-list, or surgeon practicing interventional painmanagement may put emphasis on psycholo-gy/psychiatry, physical therapy/functional reha-bilitation or surgical techniques, with multidisci-plinary management provided by secondaryapplication of other modalities, such as interven-tional techniques in this case.There are large gaps and controversies in theliterature describing the interventional procedu-res for pain management. The literature is limi-ted. There is lack of double-blind studies, andthere are problems with randomization. The dia-gnosis are not homogeneous. There are difficul-ties in arranging the appropriate comparisongroups. There are problems with standardizedassessment of treatment outcomes, and agree-ment on the definition of a successful treatmentresponse. The variability in assessed outcomes,particularly how and when pain intensity or disa-bility is measured, is especially problematicsince it precludes combining data acrossstudies with different methods in a meaningfulway. Clinical trials are challenging. Recruiting well-defined patient samples appropriate for and wil-ling to undergo investigation of an interventionalpain procedure is especially difficult. The place-bo response, which is substantial in pain trials ingeneral, may be even larger in response tosham surgery and sham interventions (4). To test and validate a single intervention requires
dolore4AggiornAmenti clinici
◗ 32 ◗
Interventional Pain Management: Pros & Cons.
Serdar Erdine, PhD, FIPP
Chair, Istanbul Pain Institute, Turkey
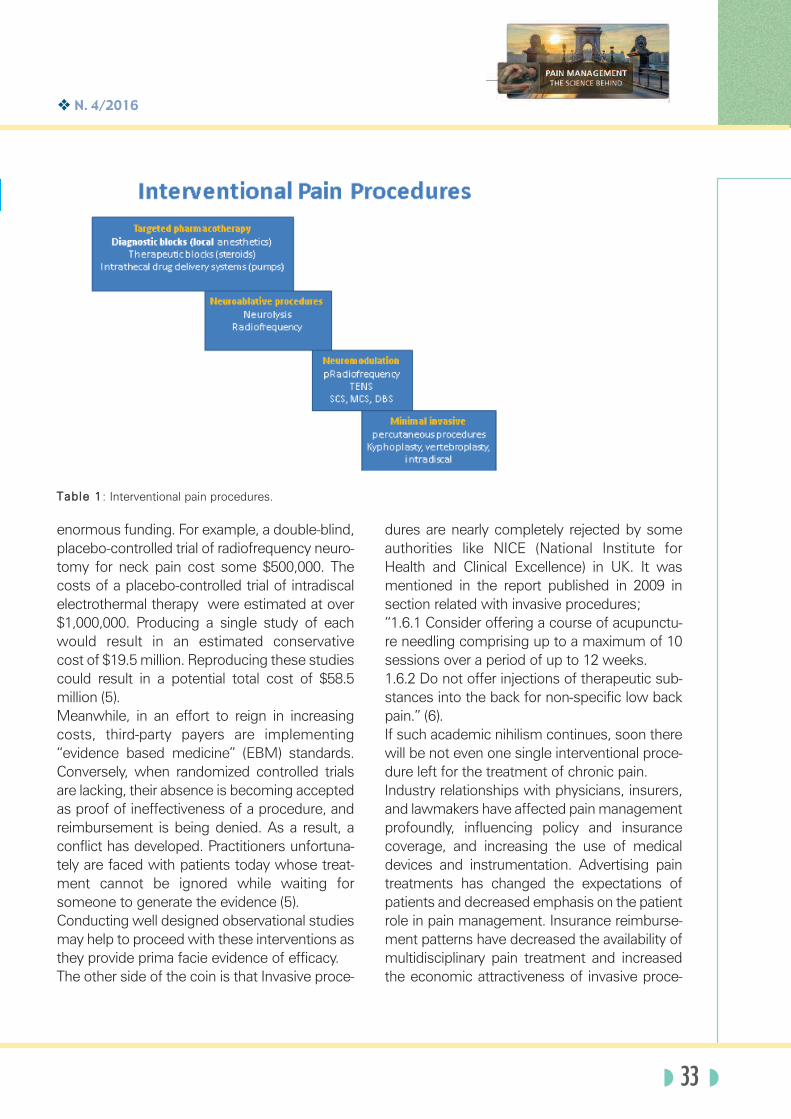
❖ n. 4/2016
◗ 33 ◗
enormous funding. For example, a double-blind,placebo-controlled trial of radiofrequency neuro-tomy for neck pain cost some $500,000. Thecosts of a placebo-controlled trial of intradiscalelectrothermal therapy were estimated at over$1,000,000. Producing a single study of eachwould result in an estimated conservativecost of $19.5 million. Reproducing these studiescould result in a potential total cost of $58.5million (5). Meanwhile, in an effort to reign in increasingcosts, third-party payers are implementing“evidence based medicine” (EBM) standards.Conversely, when randomized controlled trialsare lacking, their absence is becoming acceptedas proof of ineffectiveness of a procedure, andreimbursement is being denied. As a result, aconflict has developed. Practitioners unfortuna-tely are faced with patients today whose treat-ment cannot be ignored while waiting forsomeone to generate the evidence (5).Conducting well designed observational studiesmay help to proceed with these interventions asthey provide prima facie evidence of efficacy.The other side of the coin is that Invasive proce-
dures are nearly completely rejected by someauthorities like NICE (National Institute forHealth and Clinical Excellence) in UK. It wasmentioned in the report published in 2009 insection related with invasive procedures;“1.6.1 Consider offering a course of acupunctu-re needling comprising up to a maximum of 10sessions over a period of up to 12 weeks.1.6.2 Do not offer injections of therapeutic sub-stances into the back for non-specific low backpain.” (6).If such academic nihilism continues, soon therewill be not even one single interventional proce-dure left for the treatment of chronic pain.Industry relationships with physicians, insurers,and lawmakers have affected pain managementprofoundly, influencing policy and insurancecoverage, and increasing the use of medicaldevices and instrumentation. Advertising paintreatments has changed the expectations ofpatients and decreased emphasis on the patientrole in pain management. Insurance reimburse-ment patterns have decreased the availability ofmultidisciplinary pain treatment and increasedthe economic attractiveness of invasive proce-
Table 1: Interventional pain procedures.

dures. Competition among pain medicine prac-titioners has often resulted in a stress on newtechnologies and high-paying procedures, witha reduction in less profitable treatment options(7).Conflicts of interest can create self-serving bia-ses that are unconscious and unintentional, andthat do influence patient care. The growingdemand for therapeutic and diagnostic injec-tions has generated the “injectionists” (8).Another important issue is the misuse andabuse of interventional pain management.Interventional techniques increased significantlyin Medicare beneficiaries from 1997 to 2006:197% increase in IPM service. Exponentialincrease in facet joint and sacroiliac joint injec-tions.” (9) (Figure 1).Lumbosacral injections increased dramaticallyin Medicare population from 1994-2001. Lessthan ½ performed for sciatica or radiculopathy.Professional fees increased from $24 million to$175 million. Costs per injection doubled from$115 to $227. Non-anesthesiologists (especiallyradiologists) increased their percentage of pro-cedures (2).Widespread use of inadequately tested or unne-
cessary pain management diagnostic and treat-ment techniques, decreased use of some treat-ments with well documented effectiveness, andlack of adequate pain education are major con-cerns. The future of interventional pain mana-gement depends on proper understanding ofthe practice of interventional pain management,the appropriate use of interventional techni-ques, the research aimed at elucidating thepathophysiologic basis of pain, the studies vali-dating evidence-based approaches for interven-tional pain management, and the good faitheffort to eliminate fraud and abuse with contai-ned and appropriate utilization.Clinicians may often be applying an acute caremodel to a chronic condition. There are no“magic bullets” for chronic back pain, andexpecting a cure from a drug, injection, or ope-ration is generally wishful thinking. Instead ofmeasuring only technical success (solid bonyfusion or properly placed injection), researchshould clarify a treatment’s safety and its effectson pain, function, and return to work.The practice of pain medicine, involving thosewith chronic pain of cancer and non-cancer ori-gin, more closely resembles that of our surgical
colleagues. The practiceresembles surgical-basedpractices because it isbased on office evaluationand procedure-based tre-atment. It is a new discipli-ne, a subspecialty andeven specialty in the futu-re which required athrough training (10). Painmanagement is an art. It isa science and it is a busi-ness. The business ofpain management influen-ces patients’ attitudestoward pain, their expec-tation for pain relief andcure, and their choices of
dolore4AggiornAmenti clinici
◗ 34 ◗
Figure 1:Increase in physician fees.
❖ n. 4/2016
◗ 35 ◗
1. Manchikanti L, Singh V, Pampati V, Smith HS, JHirsch J.Analysis of Growth of Interventional Techniques inManaging Chronic Pain in the Medicare Population: A 10-Year Evaluation from 1997 to 2006. Pain Physician 2009;12: 9-34.
2. Raj PP, Erdine S. Pain Relieving Procedures. TheIllustrated Guide. Wes Sussex: Wiley Blackwell, 2012.
3. Greenhalgh S. Under the medical gaze. Facts and Fictionsof Chronic Pain. Oakland: University of California Press,2001.
4. Hartrick CT. Quality Assessment in Clinical Trials:Considerations for Outcomes Research in InterventionalPain Medicine, Pain Pract 2008; 8: 433–438.
5. Bogduk N. Proof or Consequences: Who Shall Pay for theEvidence in Pain Medicine? Pain Med 2010; 11: 1–2.
6. NICE (National Institute for Health and ClinicalExcellence). Low back pain. Early management of persist-ent non-specific low back pain. London: 2009.
7. Taylor ML. The Impact of the “Business” of Pain Medicineon Patient Care Pain Medicine. 2011; 12: 763–772.
8. Rathmell JP. The Injectionists (Editorial). RegionalAnesthesia and Pain Medicine 2004; 29: 305-306.
9. Friedly J, Chan L, Deyo R. Increases in lumbrosacral injec-tions in the Medicare population 1994–2001. Spine 2007;32(16): 1754–60.
10. Schatman ME, Lebovits A. On the Transformation of the“Profession” of Pain Medicine to the “Business” of Pain,Medicine: An Introduction to a Special Series, Pain Med2011; 12: 403–405.3
References
treatments. The place of the interventional painmedicine in an optimistic way is, to be a part of amultimodal approach. It can palliate natural cour-se of disease, can facilitate rehabilitation for chro-nic pain and sustain a better balance betweenbenefit and risks especially in comparison withsurgical techniques. Interventional pain manage-ment should adopt a biopsychosocial perspecti-
ve on pain and operate within a framework ofmultidisciplinary pain rehabilitation to improve itseffectiveness.Interventional pain management isprogressing despite diversity. Interventional painmanagement must provide a leading role in thehuman society, which is afflicted by chronic per-sistent pain.
◗ 35 ◗
PAin mAnAgement
Unmet needS in AcUte PAin
BArcelonA 14-16 SePtemBer 2017
Presidents of the Symposium
Carmelo Scarpignato and Giustino Varrassi
Scientific Committee
Eli Alon, Stefano Coaccioli, Stephan Schug, Margarita Puig
Scientific Secretariat
Anna Bertelè, Antonella Paladini
For more information
and for registration:www.fondazione-menarini.it
����������
Scientific Director Prof. Eli Alon
��#'����%�33036.�4239�+%���.��,�'-�%�� �
������ ����������������������������������
�������� �����
The European League Against Pain EULAP®invites you to attend an interdisciplinary paincourse in English in the beautiful city of Zürich, Switzerland.A team of pain specialists including Anaesthesiologists, Neurologists, Rheumatologists, Psychiatrists, Psychologists, Clinical Pharmacologists, Lawyers and others lecture on different aspects of pain.You will learn to understand chronic pain, to develop management strategies, thus to improve patient’s therapy.
�����������������������������e-mail: [email protected]
FACULTY• Eli Alon, Zürich (Anesthesiology)• Mirjam Baechler, Luzern (Chiropractic)• Daniel Bärlocher, Zürich (Psychology)• Florian Brunner, Zürich (Physical Medicine)• Stefano Coaccioli, Terni-Perugia (Rheumatology)• Wolfgang Dumat, Nottwil (Psychology)• Dominik Ettlin, Zürich (Dentistry)• Karin Fattinger, Schaffhausen (Internal Medicine)• Andreas Gantenbein, Zürich (Neurology)• Michael Hartmann, Zürich (Anesthesiology)• Antje Heck, Aarau (Cl. Pharmachology)• Monika Jaquenod, Zürich (Anesthesiology)• Michael Lottan Tel Aviv (Anesthesiology, Lawyer)• Thomas Maier, St. Gallen (Psychiatry)• Chantal Manz, Basel (Pharmacy)• Antonella Palla, Zürich (Neurology)• Sandro Palla, Zürich (Dentistry)• Daniel Richter, Zürich (Lawyer)• Angie Röder, Winterthur (Physiotherapy)• Wilhelm Ruppen, Basel (Anesthesiology)• Peter Sandor, Zürich (Neurology)• David Scheiner, Zürich (Gynecology)• Dagmar Schmid, Basel (Psychiatry)• Kyrill Schwegler, Basel (Psychiatry)• Andreas Siegenthaler, Bern (Anesthesiology)• Giustino Varrassi, L’Aquila, Malta (Anesthesiology)
! ��+�4432/22032/37�"� � ��/���! .��/���%%�&&�032/37032/67�!���&����%"��&%�!��"�� �/���! 032/67033/52��! !�������%"��&%!����$! ���"�� �/��� -033/52034/37� �&!������� ��"�+%�!�!�������! %���$�'! %���!(&�"�� �/��(��
1�* ��
35/52036/37�"�!���&$��&�� &�!����$! ��"�� �"�'� &%�/��$*� !�036/37037/22���������$�!$���$! ���"�� �2�%'���)����.�/���%%�&&�037/22037/67�"�!���� ����%�����"� �� ���/���%%�&&�
1�%���
38/37039/22�($!"�&����"�� �/��� '� ��� �
39/22039/67��$! ���"�� �� ��"%+����&$�����%��%�%/����,����%0�(�%��+�452:/2202:/67!����"')��"�� ���02:/6702;/52���02;/52032/37�$(%&���&*�� �"�'� &�� ��"�+%���� /����,����%
1�%���
32/67033/52��$! ����������"�� �/� ����033/52034/37��� �� �� �%�%�/��!����!��
1�* ��
38/37039/22��+%�!&��$�"+�/��"��%39/22039/67���$!"$��'��/��������%
��($%��+�472:/2202:/67� ���/��%* �%02:/6702;/52� ������$�"+�/��*##� 02;/52032/37�� ��$�"�� �/��*##�
1�%���
32/67033/52�$���$+����������/� ����
33/52034/37�&���%���*�( ������� ��/��!(�
1�* ��
35/52036/37� &�$)� '! ����� ����� &�� ���$)������ ���(���$�$���! �/������ '����%
36/37037/22� &�$)� '! ����� ����� &�� ���$)������ ���(���$�$���! �/������ '����%
37/22037/67�($!�!�(��'! �� �����!$+&����!$�� &�$)� '! ���&��$�"+�/���%'��
1�%���
38/37039/22�%+��!�!�������%"��&%�!����$! ���"�� �&$��&�� &�/���%�!���%
39/22039/67��!%� ��$���$�%�/���!
�����3��%��� ! �"$!��&�!$�� �,�&�! �����#(�$&�$���� ��(-$���/��*�&,�$�� �1�����"($"!%��!��&����%%!���&�! ��%0• To support the cause and interest of pain patients
• To improve the treatment, prevention and rehabilitation of pain patients
• To promote research in the field of pain
• To foster and improve excellence in education of health professionals, with traditional and online educational courses and workshops, giving the participants the opportunity to meet and exchange experiences and ideas
• To foster the publication of updated guidelines, best practices, books and journals
35/52036/37��� �� ����!'! /����,����%036/37037/22(�'�!����"�� �&$��&�� &�/��*��'037/22037/67�$� %�(�&($����%"��&%�!��"�� �/�����%
1�%���
38/37039/22����"���%!$��$%�� ����$! ���"�� �/�������
39/22039/67�������%"��&%�!����$! ���"�� ��/�����'�%0��� �%��+�4602:/2202:/67���$���!�+ �'�%�� ��2�+ ����%�!��"�� ������$%/���) ��%02:/6702;/52��$���&��!�/�����%�� ���"�!��%/���) ��%02;/52032/37��&�!"�+%�!�!�+�!���������� /��� �!%
1�%���
32/67033/52� '��"$�%%� &%/�� ,!���,�"� �%/����� &��! �%&�/�����033/52034/37�($!��"'�%/�� '�"���"'�%/�%&�$!��%�/�����
1�* ��
35/52036/37�!*������"�� �/��!����!��036/37037/22���$!�+������/��!����!��037/22037/67�$&�$!%��!��"�$�"��$����!� &%�/��!����!��
1�%���
Number of participants is limited.Venue: HHootteell ZZüürriicchhbbeerrgg,, Orellistrasse, 21
����� ��������������������
❖ n. 4/2016
◗ 37 ◗
ANALGESIA E SEDAZIONE AI TEMPI DEI FARAONI C. Milani DMD MS1, S. Malgora PhD2, D. Di Pinto3, D. Paradiso3, S. Di Pierro3, A. Barelli MD5, F. La Mura MD MS3
1. Mummy Project, Studio di Odontologia e Antropologia Forense, Torino.
2. Mummy Project, Castello del Buonconsiglio,Trento.
3. Hospice Don Uva, Bisceglie.
4. A.S. Congregazione Ancelle della Divina Provvidenza, Bisceglie.
5. Centro Antiveleni, Ist. Anestesia e Rianimazione, Policlinico Universitario A. Gemelli, Roma.
INTRODUZIONE La pratica della medicina trova in Egitto le più antiche attestazioni (Fig.1), oltre a fonti storiche greche e latine. Nell’antica lingua egizia “sunu” significa “colui che appartiene a chi è ammalato” e che quindi reca su di sé il gravoso incarico di ricondurre il paziente alla guarigione. Tale capacità veniva appresa nelle “case della vita ” situate in prossimità dei templi. Fin dal 2650 a.C., la figura del medico, sia nell'accezione moderna, sia con connotazioni religiose è documentata con specializzazioni e gerarchizzazioni.
Fig.1 – Kom Ombo. Bassorilievo raffigurante strumenti chirurgici.
MATERIALI E METODI: LE FONTI Diversi sono i papiri che documentano pratiche mediche di tipo chirurgico (papiro Smith, papiro Hearst, ecc.) o ricette mediche con fini terapeutici di vario genere (es, papiro di Londra, p. Ebers, p. Chester Beatty, etc.). Il Papiro Smith (Fig.2), ad esempio, uno dei più antichi trattati di traumatologia, ma copia di un documento antecedente, ci tramanda che dopo l’esame del paziente il medico annotava la prognosi:
favorevole : “È un male che curerò” incerta: “È un male che combatterò” infausta: “È un male che non curerò”
e, a seguire, proponevano un’eventuale terapia. In essi è attestato l’uso di medicamenti di origine vegetale o minerale utili a fini analgesici, sedativi o ipnoinducenti. Allo stesso modo pitture murarie e oggetti rinvenuti in corredi funerari raffigurano piante dalle note proprietà psicotrope.
Fig.2 – Papiro Edwin Smith (1500 a.C.), VI-VII foglio, scrittura ieratica. New York Academy of Meicine.
RISULTATI E DISCUSSIONE Molte sono le fonti risalenti all’Egitto antico che fanno riferimento a sostanze dalla funzione sedativa o narcotica: il lattice proveniente da alcune lattughe, il loto, la mandragora e, probabilmente, anche l’uso di componenti del papavero. Il lattucato estratto dai fusti fiorieri della Lactuca Serriola, della L. Sativa, e della L.Virosa, lasciato asciugare, produce una sostanza resinosa dalle proprietà sedative, ipnoinducenti e anafrodisiache, riconosciute anche dalla farmacopea moderna. La Mandragora officinarum la cui radice, contenente iosciamina, atropina e scopolamina, trovava invece impiego come anestetico e sedativo. È raffigurata in pitture murali di varie tombe tebane della XVIII dinastia e le sue bacche sono presenti in cesti rinvenuti nella tomba di Tutankhamon .La ritroviamo nel papiro di Leida (I-383) dove, miscelata al vino, viene prescritta come ipnoinducente. La conoscenza del papavero da Oppio (shepen) pare essere documentato, invece, da rappresentazioni di capsule in monili. Ne sono un esempio un paio di orecchini in oro recanti il cartiglio di Seti II (Fig.3) risalenti alla XIX dinastia: rappresentano la capsula del papavero con la tipica striatura longitudinale. La stessa viene riprodotta in una collana di perline di cornalina (Fig.4) della XVIII dinastia. Tali riscontri non sono, tuttavia, di univoca interpretazione e sono oggetto di discussione, a causa della somiglianza della capsula del papavero con i frutti di alcune specie di ninfea o fiordaliso. Un’anforetta appartenente al corredo funerario di Kha (Fig. 5), architetto della XVIII dinastia sotto il regno di Amenohtep III, è stata più volte oggetto di indagini: nel 1925 il suo contenuto fu sottoposto ad analisi chimiche che individuarono residui di morfina. Tale riscontro non fu confermato da successive analisi con metodologie più moderne (es. gascromatgrafia) e non venne rilevatala presenza né degli alcaloidi dell’oppio, né degli alcaloidi tropanici (es. mandragora, solanacee, ecc.). Il papiro Smith, raccomanda l’uso di fiori di papavero rosso per lenire ascessi e piaghe infette. Il papiro Ebers (1550 a.C., lungh. 20 m. circa) che raccoglie circa 700 ricette mediche e formule rituali di vario genere, prescrive la capsula di papavero per le eruzioni del cuoio capelluto o per calmare le grida del bambino. 1543-1292 a.C.
Fig.4 Orecchini di Sethi II, XIX dinastia (1214-1204 a.C.). Museo del Cairo.
Fig.5 Collana di Cornalina, XVIII dinastia (1214-1204 a.C.). British Museum.
Fig.6 Anforette del corredo di Kha, XVIII dinastia (1405 a.C. circa). Museo Egizio di Torino.
CONCLUSIONI La conoscenza di medicamenti dalla funzione psicotropa, in particolare di tipo alcaloide, è documentata nell’antico Egitto da molteplici reperti archeologici, fonti scritte e iconografiche. Tuttavia, per alcune di queste, le specifiche applicazioni non sono sempre univocamente riconosciute e condivise dagli studiosi.
BIBLIOGRAFIA 1.Bisset G et al. (1994) Was opium known in 18th dynasty ancient
Egypt? An examination of materials from the tomb of the chief royal architect Kha, J. of Ethnopharmacology, vol. 41:99-114.
2.Scandone MG (2006) Una pietra per amica, Pharaon Magazine, Anno II, n. 2, pp. 54-60.
3.Emboden WA (1981) Transcultural use of narcotic water lilies in ancient Egyptian and Maya drug ritual, vol.1:39-83.
4.Muzio I (1925) Su di un olio medicate della tomba di Cha, Atti della Società Liguistica di scienze e lettere, vol.4:249-253.
5.Kamal H (1965) A Dictionary of Pharaonic Medicine, El Cairo National Publishing House.
6.Malgora S. (2008) Ur Sunu. Grandi dottori dell’antico Egitto, Saviolo ed., Vercelli.
La pratica della medicina trova in Egitto le piùantiche attestazioni, oltre a fonti storiche grechee latine. Fin dal 2650 a.C., la figura del medico,sia nell'accezione moderna, sia con connotazio-ni religiose è documentata con specializzazioni egerarchizzazioni. Diversi sono i papiri che docu-mentano pratiche mediche di tipo chirurgico(papiro Smith, papiro Hearst, ecc.) o ricettemediche con fini terapeutici di vario genere (p.es., papiro di Londra, Ebers, Chester Beatty,ecc). In essi è attestato l’uso di medicamenti diorigine vegetale o minerale utili a fini analgesici,sedativi o ipnoinducenti. Allo stesso modo pittu-re murarie e oggetti rinvenuti in corredi funerariraffigurano piante dalle note proprietà psicotro-pe.Molte sono le fonti risalenti all’Egitto antico chefanno riferimento a sostanze dalla funzionesedativa o narcotica: il lattice proveniente daalcune lattughe, il loto, la mandragora e, proba-bilmente, anche l’uso di componenti del papa-vero. Il lattucato estratto dai fusti fiorieri dellaLactuca Serriola, della L. Sativa, e della L. Virosa,lasciato asciugare, produce una sostanza resi-nosa dalle proprietà sedative, ipnoinducenti eanafrodisiache, riconosciute anche dalla farma-copea moderna.La Mandragora officinarum la cui radice, conte-nente iosciamina, atropina e scopolamina, trova-va invece impiego come anestetico e sedativo.È raffigurata in pitture murali di varie tombetebane della XVIII dinastia e le sue bacche sonopresenti in cesti rinvenuti nella tomba di
Tutankhamon. La ritroviamo nel papiro di Leida(I-383)dove, miscelata al vino, viene prescrittacome ipnoinducente. La conoscenza del papavero da oppio (shepen)pare essere documentato, invece, da rappre-sentazioni di capsule in monili: un paio di orec-chini in oro recanti il cartiglio di Seti II (XIX dina-stia, Museo del Cairo), rappresentano la capsuladel papavero con la tipica striatura longitudinale;la stessa si trova in una collana di perline di cor-nalina (XVIII dinastia, BritishMuseum). Taliriscontri non sono, tuttavia, di univoca interpre-tazione e sono oggetto di discussione, a causadella somiglianza della capsula del papavero coni frutti di alcune specie di ninfea o fiordaliso.Un’anforetta appartenente al corredo funerariodell’architetto Kha (Museo Egizio di Torino) èstata più volte oggetto di indagini: nel 1925 ilsuo contenuto fu sottoposto ad analisi chimicheche individuarono residui di morfina. Tale riscon-tro non fu confermato da analisi successive, enon venne rilevatala presenza né degli alcaloididell’oppio, né degli alcaloidi tropanici (p. es.,mandragora, solanacee, ecc.). Il papiro Smith,forse il più antico trattato di traumatologia risa-lente al 1500 a.C. circa, copia di un documentoantecedente, raccomanda l’uso di fiori di papa-vero rosso per lenire ascessi e piaghe infette. Ilpapiro Ebers (1550 a.C., lungh. 20 m. circa) cheraccoglie circa 700 ricette mediche e formulerituali di vario genere, prescrive la capsula dipapavero per le eruzioni del cuoio capelluto oper calmare le grida del bambino.
L’analgesia ai tempi dei Faraoni
.
Chantal Milani 1, S. Malagora2, Dorotea Paradiso 3, Ilaria Ricchitelli 3,
Francesco Barbangelo 4, Fabrizio La Mura 4
1 DMD, MS, Antropologo ed Odontologo Forense – Reparto Investigazioni Scientifiche (R.I.S.) di Roma, Arma dei Carabinieri, Italia
2 PhD – Direttore Mummy Project, curatore sezione egizia Castello Buonconsiglio
3 Infermiere, Centro di Cure Palliative – Hospice Don Uva – Casa della Divina Provvidenza, Bisceglie
4 Servizio di Anestesia, Rianimazione, Terapia del Dolore, Day Surgery – Presidio Ospedaliero di Bisceglie – Trani, ASL BAT

dolore4AggiornAmenti clinici
◗ 38 ◗
Il 24 dicembre u.s. veniva pubblicato un articoloinerente al rapporto fra l’arresto di circolo e l’usodi antinfiammatori non steroidei, FANS (1).Leggiamo una sintesi di questo articolo pubbli-cata online (2). Incuriositi dai toni allarmistici delcomunicato, rispetto ai pericoli da consumo diFANS senza prescrizione medica, siamo risalitialla fonte, per leggere l'articolo originale.L’articolo originale, metodologicamente benfatto, ammette alla fine di avere alcuni bias, peri quali propone anche dei potenziali fattori miti-gativi. Ad esempio, evidenzia che nel fare lo stu-dio non si disponeva dei dati di consumo dei far-maci OTC. Chiarisce, però, che in Danimarca esi-ste solo un FANS OTC. Dallo studio in generaleemergerebbe una associazione significativa frauso di FANS (soprattutto alcuni) e arresto cardia-co. Di fatto, dice lo studio, ben l’11% dei pazien-ti in cui si è verificato un arresto cardiaco extra-ospedaliero, nell’arco dei 10 anni studiati, usavaFANS. Peccato che lo stesso studio non ci dicain che percentuale della popolazione totaledanese ci sia stata la stessa modalità di utilizza-zione di FANS. Infatti, se questa fosse non signi-ficativamente diversa dall’11% renderebbe vanol’intero costrutto scientifico su cui la relazione frauso di FANS e Arresto Cardiaco Extra-ospedalie-ro viene sostenuto. Infatti, se l’uso di FANS, conle stesse modalità, nella popolazione generalefosse pari a quello della popolazione studiata sipotrebbe evincere che l’uso di FANS non è unfattore influente nella insorgenza di arresto car-dio-circolatorio extra ospedaliero.Ancor più pesanti sono le conseguenze di quan-to riferito da DottNet. Dalla lettura di quel report,infatti, sembra emergere che, stando ai dati pro-venienti dalla Danimarca, la vendita di FANS OTCè potenzialmente pericolosissima (peccato che
in quel lavoro non vengono studiati), in quantoassociata con arresto cardiocircolatorio extra-ospedaliero in un numero significativo di casi.In sintesi, sembrerebbe che la lettura più atten-ta e critica di alcuni lavori scientifici sia sempreconsigliabile.Questo e solo questo ci consente di non diffon-dere allarmismi o falsi miti, e di fare un lavorodecisamente più utile per il benessere dei mala-ti, specialmente di quelli con dolore. (G.V.)
1 )h t tps: / /academic .oup.com/eh jcvp/a r t i -cle/3/2/100/2739709/Non-steroidal-anti-inflamma-tory-drug-use-is?searchresult=1.2)https://www.dottnet.it/articolo/20390/studio-con-gli-antidolorifici-aumenta-il-rischio-di-arrestocardiaco/?tag=10318078541&tkg=1&cnt=1
Effetti della statistica nella medicina.

PROGRAMMA Ore 8.30 Apertura della segreteria ed accreditamento dei partecipanti
Ore 9.00 Saluto delle Autorità
I SESSIONE Moderatore: Stefano Coaccioli
Ore 9.20 Le ferite croniche: onerosa realtà Fabrizia Toscanella
Ore 9.40 Eziologia delle lesioni croniche Fabrizia Toscanella
Ore 10.00 Le ferite degli anziani: skin tears e lesioni da decubito Angela Peghetti
Ore 10.20 Lesioni cutanee e delle mucose correlate ai trattamenti radio e chemioterapici Fabio Trippa
Ore 10.40 Discussione
Ore 11.00 Coffee Break
II SESSIONE Moderatori: Giustino Varrassi, Maurizio Evangelista
Ore 11.20 Dolore acuto: fisiopatologia e trattamento Stefano Coaccioli
Ore 11.40 Dolore procedurale: prevenzione e trattamento del dolore attraverso la medicazione Angela Peghetti
Ore 12.00 Ruolo della nutrizione: sostegno nutrizionale e malnutrizionale dell’anziano Giuseppe Fatati
Ore 12.20 Discussione interattiva con televoter
Ore 13.15 Compilazione Questionario ECM
Ore 13.30 Fine Lavori
EDUCAZIONE CONTINUA IN MEDICINA CREDITI ECM ASSEGNATI n. 7,8L’evento ECM n. 3599-189576 è stato accreditato per n. 50 partecipanti pressola Commissione Nazionale per la Formazione Continua per le seguenti figure pro-fessionali:
• MEDICO-CHIRURGO* E INFERMIERE* Discipline di riferimento per la professione di Medico-Chirurgo:Endocrinologia, Malattie Metaboliche e Diabetologia, Medicina Interna, Gastroenterologia,Scienza dell’Alimentazione e Dietetica, Geriatria, Medicina Generale, Oncologia, Pediatria, Psi-chiatria, Chirurgia Generale, Reumatologia, Medicina Fisica e Riabilitazione, Neurologia, Neu-rochirurgia, Ortopedia e Traumatologia, Anestesia e Rianimazione, Dermatologia eVenereologia, Radioterapia
Il corso è gratuito (fino a n. 50 partecipanti) con pre-iscrizione obbligatoria sul sito www.fondazioneprocacci.org e www.viva-voce.it
RESPONSABILESCIENTIFICOProf. Stefano CoaccioliProfessore Associato in Medicina Interna, Università degli Studi di Perugia
SEGRETERIA SCIENTIFICAFondazione Paolo ProcacciVia Tacito, 700193 Romawww.fondazioneprocacci.orgwww.painnursing.it
PROVIDER ECME SEGRETERIAORGANIZZATIVA
ID ECM 3599Via Angelo da Orvieto, 3605018 Orvieto (TR)Tel. 0763 391752 Fax 0763 [email protected]
CON IL PATROCINIO DI
EVENTO REALIZZATO CON IL CONTRIBUTO EDUCAZIONALE NON CONDIZIONANTE DI

Ci sono almeno 6 buoni motivi per diventare socio AISD Associazione Italiana Studio del Dolore4Essere sempre informati sulle ultime ricerche nel campo
della terapia del dolore
4Essere sempre informati su tutte le iniziative riguardanti la terapia del dolore, a livello nazionale ed internazionale
4Partecipare attivamente alle attività dell’associazioneper il progresso della terapia del dolore
4Avere un sito di riferimento dove poter scambiare liberamenteinformazioni con altri soci
4Avere l’iscrizione al Congresso con quota agevolata
4Consultare gratuitamente online “l’European Journal of Pain”
1. Collegati al sito www.aisd.it e vai alla pagina “diventa socio”
2. Riempi il modulo di iscrizione online
3. La quota annuale di (50,00 euro per medici, psicologi e farmacistie 25,00 euro per infermieri e fisioterapisti) può essere versata sul seguente conto bancario:
BANCA DI CREDITO COOPERATIVO DI ROMA
IBAN: IT 44 J 08327 03239 0000 0000 2154
Intestato a: Associazione Italiana per lo studio del dolore (AISD)indicando nella causale: quota iscrizione anno... oppure puoi pagare con carta di credito tramite Paypal, con accesso dal sito www.aisd.it
4. Spedisci la ricevuta di pagamento tramite e-mail a: [email protected]
www.aisd.it
Accedi alla modalità di iscrizione in 4 semplici mosse