Mortalità e morbilita liposuzione
103
Mortalità e morbilità da liposuzione Claudio Melloni Anestesista libero professionista Consulente per Villa Torri,Bologna,Villa Chiara,Bologna,Poliambulatorio Gynepro,Bologna
-
Upload
claudio-melloni -
Category
Health & Medicine
-
view
770 -
download
0
description
mortality and morbidity form liposuction,2008
Transcript of Mortalità e morbilita liposuzione

Mortalità e morbilità da liposuzione
Claudio Melloni
Anestesista libero professionista
Consulente per Villa Torri,Bologna,Villa Chiara,Bologna,Poliambulatorio Gynepro,Bologna

PERUGIA: CONDANNATI MEDICI PER PAZIENTE MORTA DURANTE
LIPOSUZIONE
� PERUGIA, 11 MARZO - Si è concluso con la condanna di tutti gli imputati il processo davanti alla Corte d' Appello di Perugia a 3 medici per la morte di una paziente dopo un intervento di liposuzione.In serata i giudici di secondo grado hanno infatti condannato ADG a 2 anni di reclusione, S A a 1 anno e 4 mesi ed AP a 1 anno di reclusione. Tutti sono stati ritenuti colpevoli di omicidio colposo.Francesca De Tommaso morì nel 1993 dopo essersi sottoposta ad un intervento di liposcultura per eliminare 3 chilogrammi di grasso. I 3 medici erano stati processati in primo grado dal pretore di Ancona che aveva inflitto 2 anni di reclusione a DG ed A ed 1 anno e 4 mesi a P. La sentenza era poi stata parzialmente riformata dalla Corte d' Appello del capoluogo marchigiano e quindi annulla dalla Cassazione che aveva rinviato il processo alla Corte d'Appello di Perugia.

Il chirurgo: «Una disgrazia»Morte dopo la liposuzione. Il dottor P:in tv: «L’intervento era perfettamente riuscito».
� L’autopsia conferma: la giovane commerciante è stata uccisa da un’embolia. Francavilla, tanti mazzi di fiori davanti al negozio di Mariana .
� Articolo di: Il Messaggero, Cronaca, Provincia Chieti, 19-02-2002
FRANCAVILLA — E’ stata una tromboembolia polmonare ad uccidere Mariana Bellomo, la giovane mamma deceduta a Francavilla sabato mattina. A confermarlo è stato l’esame autoptico effettuato dal dottor Armando Colagreco dell’istituto legale di Chieti. Quattro, forse addirittura cinque, gli emboli killer che hanno stroncato la vita di Mariana, 24 anni, madre di una bimba di appena 2 anni. E R P il medico che l’ha operata, va in tv e dice di non sentirsi responsabile: «L’intervento era perfettamente riuscito, ed è stato fatto rispettando tutte le procedure dal punto di vista sanitario».


Chiesto il rinvio a giudizio per C G, il medico fiorentino che operò Bernadette Fontana, uccisa da un'infezione.Morta per liposuzione"Omicidio volontario"
�
FIRENZE - Sapeva che avrebbe potuto uccidere. Sapeva che qualcuno, prima o poi, sarebbe morto a causa sua. Ma il sapere tutto questo non l'ha messa in guardia contro il pericolo che correva, e che avrebbe fatto correre agli altri. Per questo CG, il medico di Firenze che lo scorso anno fece un intervento di liposuzione su una donna che poì morì per un'infezione post-operatoria, è colpevole. Colpevole a tutti gli effetti. Per il pubblico ministero Paolo Canessa che ha condotto l'inchiesta sul caso, si tratta senza ombra di dubbio di omicidio volontario e per questo ne chiede il rinvio a giudizio: se il giudice accoglierà la richiesta del pm, Costanza Greco dovrà rispondere dell'omicidio di Bernadette Fontana, la donna di 48 anni morta per una grave infezione dopo essere passata sotto i ferri del medico fiorentino.

� Ma non è finita qui. La dottoressa G.è anche accusata di lesioni colpose e lesioni volontarie gravi per aver provocato in quello stesso periodo di tempo, fra il 18 e il 20 marzo 1999, analoghe infezioni post-operatorie ad altre due pazienti, L. B., 39 anni, e P. F., 44 anni. Anche loro andarono dalla G.nella speranza di togliersi quei chili di troppo. Ma, dopo essersi sottoposte all'intervento di liposuzione al "Centro servizi Edonè" di Firenze che, tra l'altro, secondo l'accusa, non aveva neanche l'autorizzazione della Regione, se ne sono tornate a casa con un'infezione in eredità.ILpm Canessa è arrivato a contestare il reato di omicidio e di lesioni volontarie al medico dopo aver valutato anche altre ipotesi: la G.infatti inizialmente sembrava avere avuto un comportamento colposo. Ma dopo l'infezione provocata alla prima donna, L.B., la .G non prese precauzioni per evitare anche alle altre pazienti conseguenze disastrose. E continuò a operare senza mascherina chirurgica, a non sterilizzare la sala operatoria, a non prevedere nessuna profilassi antibiotica, utilizzando infine cannule per aspirazione e medicinali non adeguatamente sterilizzati. Per questo alla colpa si è aggiunta nella convinzione degli inquirenti una responsabilità volontaria della G.

By Damon Adams, AMNews staff. March 1, 2004.
� Florida puts limits on office plastic surgery after 8 deaths.
� State officials want to examine surgical logs to see if more rules are needed for such surgery.

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
August 10, 2000, Florida Boardof Medicine
August 10, 2000, Florida Boardof Medicine
90 days moratorium on Officesurgery
90 days moratorium on Officesurgery
..."there is an immediate danger tothe health,safety and welfare of
patients"....
..."there is an immediate danger tothe health,safety and welfare of
patients"....

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
21 luglio 2000,UK.,eadings21 luglio 2000,UK.,eadings
Vietata AG nello studio dentisticoVietata AG nello studio dentistico
18 mesi di tempo per la transizione inambiente ospedaliero.18 mesi di tempo per la transizione inambiente ospedaliero.

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Di che cosa stiamo parlando?
0
50000
100000
150000
200000
250000
300000
350000
400000
2000 2002 2003 2004
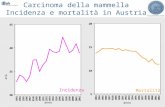
National USA Plastic Surgery StatisticsCosmetic procedure trends.
mastoplast addit
mentoplastica
dermabrasione
otoplastica
blefaroplastica
lift facciale
lift frontale
trap capelli
liposuz
addominoplast

Morello DC,Colon GA, Fredricks S,Iverson RE,Singer R Patient Safety in Accredited Office Surgical Facilities. Plast Reconstr Surg, Volume 99(6).May 1997.1496-1500
� Questionario inviato ai 418 AAAASF,uffici chir accreditati
� Ripetizione del questionario alcune settimane a dopo a chi non aveva risposto
� 241 risposte :57.7 %� (organizzazione curata da una ditta
esterna , Chalana, Inc).

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Eventi dannosi in ufficio
0 10 20 30 40 50
%
eventi resp
probl cardiovasc
probl.attrezz
probl con farmaci
traumi da aghi??
Errori di dosaggio,allergia,IM
Broncospasmo,depressione resp severa,ipossia,fallita o errata intubaz,ostruzione…

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Complicanze della office chirurgia plastica From: Keyes: Plast Reconstr Surg, Volume 113(6).May 2004.1760-1770 Analysis of outpatient surgery center safety using an internet-based quality improvement and peer review program

Keyes GR, Singer R, Iverson RE, McGuire M, Yates J, Gold A, Thompson D.
Analysis of outpatient surgery center safety using an internet-based quality improvement and peer review program.
.Plast Reconstr Surg. 2004 ;113:1760-70. � 411,670 interventi� 2001-2002� 2597 sequele,di cui 1378 significative � 1 sequela/299 procedurs (incidenza 0.33 %) � 7 morti ,1/ 58,810 procedure (0.0017 %.

Aritmie cardiache(2 arresti card.)

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Alterazioni della PA Intraop.

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Trombosi venosa profonda/embolia polmonare:0.004%

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Pneumotorace

Cause di morte durante liposuzione. Grazer F, deJong RH. Fatal outcomes from liposuction: census survey of cosmetic surgeons. Plast Reconstr Surg 2000;105:436-46.
� Embolia polmonare 23%� Perforazione visceri addominali 14,6%� Anestesiologiche 10%� Embolia grassosa 8,5%� Insuff cardioresp 5,4%� Infez massiva 5,4%� Emorragia 4,6%� Sconosciuta o confidenziale 28,5%� Mortalità globale 19,1 per
100.000,ossia 1/5000

Mortalità da liposuzione. Grazer F, deJong RH. Fatal outcomes from liposuction: census survey of cosmetic surgeons. Plast
Reconstr Surg 2000;105:436-46.
sede Morti tot Morti % Sede chir %
office 62 47,7% 45%
Day surg 39 30% 29%
Sala op ospedale
22 17% 26%
sconosciuta 7 5,4%

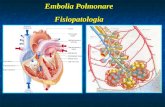
Complicazioni delle liposuzioni per area trattata
Grazer F, deJong RH. Fatal outcomes from liposuction: census survey of cosmetic surgeons. Plast Reconstr Surg 2000;105:436-46.
72
39
3
14
8 6
addome
natiche,estr.infestr sup
dorso sup
dorso inf
testa,collo

Rao,RB,Ely,SF,Hoffman,RS.DEATHS RELATED TO LIPOSUCTION. NEJM;1999;340:1471
� 5 morti dopo liposuzione in tumescenza su 48,527 esaminate dal Office of Chief Medical Examiner of the City of New York tra il 1993 e1998.
� I 5 paz avevano ricevuto lidocaina a dosaggi fra 10 - 40 mg/kg
� Altri farmaci: midazolam,mep,isoflurane� 3 morti improvvise con bradicardia ed ipotensione intraop
inspiegabili .Postmortem lidocaina ematica in 2 paz. era 5.2 e 2 mg/lt
� 1 decesso per sovraccarico idrico� 1 decesso per dvt delle vene del polpaccio e PE dopo
liposuzione delle gambe

Osservazioni sul lavoro di Rao:
� Chirurghi operatori;plastici,1 chir gen� Anestesista sempre presente� Rianimazione sempre effettuata � Quasi tutte procedure combinate di + aree

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)

Teimourian B, Rogers WB A national survey of complications associated with suction lipectomy: a comparative study. Plast
Reconstr Surg. 1989 Oct;84(4):628-31.
Pulmonary embolism in 9
January 1984 -to January 1988 112,756 p rocedures : major liposuction (75,591), dermatolipectomy (10,603),
and abdominoplasty (26,562).

4 anni di Florida MoratoriaAnn Plast Surg. 2006 Jan;56(1):78-81. Office surgery safety and the Florida
moratoria. Clayman MA, Caffee HH.

Mark A. Clayman, M.D. Brent M. Seagle, M.D. Office Surgery Safety: The Myths and Truths behind the Florida Moratoria–-Six Years ofFlorida DataPlastic and Reconstructive Surgery • 2006;118:777-785
� The authors reviewed all office surgical incidents that resulted in death, injury, or hospital transfer in Florida from January of 2000 to January of 2006. Various methods were used to determine board status, office accreditation, and hospital privileges.

Mortalità in Florida,2000-2006,da office surgery
600.000 interventi

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)

Procedure combinate:7/11Addominoplastica:7/11

� Conclusions: There were over 600,000 operations during the study period. The fact that 11 office deaths were reported would suggest that the location in which these procedures were performed was not as much of a factor as the regulators have suggested. The most frequent cause of death after discharge was thromboembolism.

Reduction of Lipoplasty Risks and Mortality: An ASAPS Survey
Charles E. Hughes .A E S T H E T I C S U R G E R Y J O U R N A L ~ M A R C H / A P R I L 2 0 0 1
� lipoplasty morbidity and mortality � performed by members of the American Society for Aesthetic
Plastic Surgery (ASAPS) from September 1, 1998, through August 31, 2000.
� response rate of 53%.
� 94,159 lipoplasty procedures.» 66% of the procedures lipoplasty only
» 20% lipoplasty without abdominoplasty but with one or more additional procedures
» 14% lipoplasty with abdominoplasty, with or without any other procedures..

Mortalità della liposuzione:da Hughes 2001
� liposuzione da sola: 2.1 : 100.000� Liposuzione con altre procedure eccetto
addominoplastica:1 su 7314� Liposuzione con addominoplastica e altre procedure
1:3281
Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)

Complicazioni non fatali della lipoplastica con o senza altri interventi combinati:da Hughees 2001
Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)

I chirurghi plast (ASAPS) che hanno modificato la loro pratica ,in che cosa
l’hanno modificata?
Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)

Rischi della lipoplastica :da Hughes 2001
» PONV :1.02%, 1 per 98 procedures. » 245 major complications,for a rate of 0.2602%.
� Conclusions: The ASAPS survey documents the current safety of lipoplasty when it is performed as an isolated procedure by properly trained surgical specialists adhering to recommended standards of clinical practice. Further studies are needed to examine the factors that increase the risk in combined procedures as well as the effectiveness of prophylactic measures in avoiding complications

Cause della insufficienza rianimativa
� Attrezzature di rianimazione inadeguate� Monitoraggio insufficiente,specie
pulsossimetria� Errore umano� Lento riconoscimento dell’evento� Mancanza di esperienza� Sovradosaggio farmacologico� Inadeguata valutazione preop.� Inadeguata valutaz postop

Linee guida della ASA per la sedazione 1996Practice guidelines for sedation and analgesia by non-anesthesiologists.Anesthesiology 1996; 84:459-471
� Registrazione simultanea dei:» livelli di coscienza» funzione resp» emodinamica » prima,durante la procedura ad intervalli regolari,;nella fase di ripresa e al
momento della dimissione
� Anche la chir maxillo faciale ha poi definito più precisamente I ciriteri per il monitoraggio postop e la dimissione
� Invece di “ segni vitali stabili prima della dimissione”� Ora specificamente raccomanda "determinazione e documentazione della
ossigenazione,ventilazione,circolazione e temperatura stabili prima della dimissione”
� Nel 2000 è stato stabilito che il chirurgo determini che “il paziente è ritornato al suo stato basale fisico e mentale di prima dell’intervento e non è più a rischio di depressione cardiorespiratoria”
� In passato la formula era “il paziente risponde appropriatamente”

Personale aggiuntivo� 1 persona preparata e competente per BLS� (il chirurgo deve essere ALS se somministra sedazione…) � 2 persone con BCLS o equivalente in caso di AG� + recentemente ASA e American Association of Pediatrics (AAP) hanno definito le
quqlifiche :AAPnelle linee guida ultime � Definisce la presenza oltre al chirurgo di una altra persona in caso di sedazione
profonda la cui unica responsabilità sia di osservare costantemente “i segni vitali del paziente,la pervietà delle vie aeree e l’ adeguatzza della ventilazione e per somministrare farmaci”
� Guidelines for Monitoring and Management of Pediatric Patients During and After Sedation for Diagnostic and Therapeutic Procedures. Pediatrics 1992;89:1110-1115
� Nell’ ASA "Statement of Qualifications of Anesthesia Providers in the Office-Based Setting," (1999),è scritto che"ASA believes that anesthesiologist participation in an office-based surgery is optimally desirable as an important anesthesia safety standard and will always support such a standard. It does not oppose however regulatory requirements that, where necessary, speak merely in terms of `physician supervision‘”

Collaborazione su indicazioni per pazienti in ambito OBS/OBA
ASA Committee on Ambulatory Surgical Care � Society for Ambulatory Anesthesia (SAMBA) stanno
sviluppando policies to safeguard the increasing numbers� Anesthesia Patient Safety Foundation� Dipartimenti della salute e società di anestesia locali per
creare dei legami con le società di accreditamento � interazione con American College of Surgeons (ACS).

Practice Advisory for Procedures in the Office-based Surgery Setting, approved by the ASPS Board of Directors in November
of 2001� Elementi da considerare nella scelta della sede
più idonea:� Stress fisiologico:
» Ipotermia» Perdite ematiche intraop» Liposuz di più aree» Durata della procedura
� Misure di tromboprofilassi� problemi di ripresa postop� Qualificazione dei providers� Standard dell’ufficio chirurgico

Ipotermia
� Ne parla il collega Zanello� Hypothermia can be a potentially serious complication of office-based surgery. Both regional and general anesthetics
markedly impair the normal precise regulation of core body temperature. Hypothermia develops because the typical operating room environment is cold; however, it is anesthetic-induced impairment of thermoregulatory responses that contributes the most to this condition. 3 The degree of hypothermia is a significant concern with regard to infection and safety of anesthetic management. Studies indicate that hypothermia may directly impair neutrophil function or impair it indirectly by triggering subcutaneous vasoconstriction and subsequent tissue hypoxia. 4
� Recommendation: The office surgery suite must be equipped so that temperatures can be adequately monitored and adjusted; equipment should be available to warm the patient, including such cutaneous warming devices as Bair Huggers (Augustine Medical, Eden Prairie, Minn.), forced air warming blankets, and intravenous fluids warmers, as necessary. Without such hypothermia prevention measures, the procedures performed should be of short duration (1 to 2 hours) and limited to no more than 20 percent of the body surface area.

Perdite ematiche intraoperatorie
� Possono portare ad una instabilità emodinamica intra e postop
� Possono portare al ricovero� Raccomandazione:
» Se le perdite anticipate sono dell’ordine dei 500 ml o maggiori l’intervento è da attuare solo in strutture ove sangue ed emocomponenti sono prontamente disponibili

Liposuzione combinata con altre procedure
� Multiple procedure effettuate nel corso di un singolo intervento aumentano la probabilità di complicazioni

Comunque la liposuzione ha visto intervenire lo Stato della Florida
� “Liposuction may be performed in combination with another separate surgical procedure during a single level II or level III operation, only in the following circumstances:
� when combined with abdominoplasty, liposuction may not exceed 1000 cc of aspirant;
� when associated with or directly related to another procedure, liposuction may not exceed 1000 cc of aspirant;
� major liposuction (in excess of 1000 cc aspirant), may not be performed in a remote location from any other procedure” (Florida Board of Medicine 64B8–9.009 Rule. Standard of Care for Office Surgery, February 27, 2001).

� Some data support these limitations; however, the data tend to be anecdotal or in studies lacking the level of rigor necessary to establish clear standards of practice. 5
� Recommendation: � The presumed benefits of combining procedures, particularly
liposuction, must be weighed against the possibility of adverse events. It is the position of ASPS that liposuction can be performed safely in the office setting when done in accordance with ASPS recommendations to limit total aspirant (supernatant fat and fluid) to 5000 cc or less. 6 When large-volume liposuction is combined with certain other procedures, such as abdominoplasty, serious complications have arisen. 5,6 Therefore, it is recommended that such combination procedures be avoided.

Durata dell’intervento� Aumenta le complicanze postop e la frequenza di
ricovero ospedaliero:– Mingus
� Interventi che si prolungano > h15 del pomeriggio hanno un aumentata incidenza di ricovero

Prevenzione dei problemi postop
� PONV:tecnica anest,fattori di rischio,profilassi,trattamento
� Giramenti di testa� Confusione � Dolore
postop:prevenzione,trattamento,scorte a casa…..
� Chiare istruzioni

Qualificazioni mediche
� Specializzazione� Partica ospedlaiera nella disciplina� Possibilità di ricovero?

Surgical Facility Standards
� Plastic surgery performed under anesthesia, other than minor local anesthesia and/or minimal oral tranquilization, should be performed in a surgical facility that meets at least one of the following criteria:
� accredited by a national or state-recognized accrediting agency/organization such as the American Association for Accreditation of Ambulatory Surgery Facilities (AAAASF), the Accreditation Association for Ambulatory Health Care (AAAHC), or the Joint Commission on Accreditation of Healthcare Organizations (JCAHO)
� certified to participate in the Medicare program under Title XVIII� licensed by the state in which the facility is located.

Conclusioni
� In ambulatorio non si puo fare di tutto� Selezione dei pazienti� Selezione delle procedure chir;
– Selezione degli operatori………
– Il rischio clinico e le possibili sequele medico legali sono maggiori!

Per chi fosse interessato:� Patient Safety in Office-Based Surgery Facilities: II. Patient
Selection.[COSMETIC SECTION: COSMETIC SPECIAL TOPIC].Iverson, Ronald E. Lynch, Dennis J. ASPS Task Force on Patient Safety in Office-based Surgery Facilities .Plast Reconstr Surg 2004 Apr 15;113(5):1478-90. [59 references]
� American Academy of Dermatology Liposuction Guideline Development Task Force .American Academy of Dermatology Guidelines/Outcomes CommitteeNGC Clearinghouse 2001

FINE

Mortalità nella office surgery Morello DC,Colon GA, Fredricks S,Iverson RE,Singer R Patient Safety in Accredited Office Surgical Facilities. Plast Reconstr Surg, Volume 99(6).May 1997.1496-1500
� 7 casi ( 0.0017 %, 1 / 57,000) � 1 decesso 3 gg dopo lifting facciale e frontale� 2 decessi da occlusione della LAD ,1 durante mastoplast addit.e 1
4 h dopo rinoplastica.� 3 decessi da complicanze intraop:1 /133,558
» ipossia cerebrale durante addominoplastica ,con decesso dopo 11 gg:– Un pnx iperteso durante mastoplastica con decesso 4 h più tardi– Un arresto cardioresp (con decesso più tardi) durante decompressione
tunnel carpale

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Casistica Morello DC,Colon GA, Fredricks S,Iverson RE,Singer R Patient Safety in Accredited Office Surgical Facilities. Plast Reconstr Surg, Volume 99(6).May 1997.1496-1500
� 400,675 interventi in 5 anni (Jan1, 1989 - Dec 31, 1993)» 253,355 estetici (63.2 %) ,147,320 ricostruttive (36.8 %).
� Complicazioni : 1877 (1/ 213 ), 0.47 %» Emorragie(ematomi intra-postop):965 ,1 /415 (0.24 %).» Episodi ipertensivi :414 ,1 /968 0.1 %). » Infezione (infezione maggiore o sepsi ) 350 , 1/1145 (0.09 %).» Ipotensione intra e postop :148 ,1 / 2707 (0.04 %).» Ritorno in sala op entro 24 h: 530 casi, 1/ 756 , (0.13 %, )» Ospedalizzazione precauzionale 126 casi, 1/ 3180 (0.03 %)

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
Incidenza di complicanze a confronto:office based vs day
surg.centers Warner, M. A., Shields, S. E., and Chute, C. G. Major morbidity and mortality within 1 month of ambulatory surgery and anesthesia.J.A.M.A. 270: 1437, 1993 Natof, H. E. Complications associated with ambulatory surgery. J.A.M.A. 244: 1116, 1980
emorragia infezione Trasf in ospedale
mortalità
Morello 0,24% 0.09% 0.03% 0,0017%1/57000
Natof 0.55% 0.74% 0.12% 0
Warner 0,00871/11273
14 MI 7 SNC 5 emb polm 5 insuff resp

Dimensione del problema
� Membership Audit, American Society for Aesthetic Plastic Surgery, Inc., Spring 1993.
� survey of members of the American Society for Aesthetic Plastic Surgery (ASAPS)
� 48.7 % of members perform their aesthetic surgery in an office surgical facility.

Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)
SMG Group: SMG Forecast of Surgical Volume in Hospital/Ambulatory Settings: 1994 2001. Chicago, SMG ‑Marketing Group, 1996
0
2
4
6
8
10
12
14
16
18
20
milio
ni e %
1984 1990 2001
interventi chir
% interventi in OB

Evoluzione della attività sanitaria(USA???)
� Anni 50-70� Gli ospedali posseggono le tecnologie più nuove ed i mezzi più potenti� Un professionista ,da solo, non potrebbe mai permetterselo� Ospedalizzazioni prolungate,prima e dopo l’intervento
� Anni 90-2000-� Contenimento dei costi� Le tecnologie più avanzate costano sempre care,ma sono alla portata,per lo
meno come ingombro….� Enfasi sulla day surgery� Parcelle chirurgiche calanti( e quindi anche anestesiologiche)
� Movimento dei pazienti verso l’ufficio» Si riducono le spese per la struttura» Si riducono le spese per i pazienti » L’office che non sembra un ospedale fa meno paura al paziente?

Ann Plast Surg. 2006 Jan;56(1):78-81. Office surgery safety
and the Florida moratoria. Clayman MA, Caffee HH.� Department of Surgery, Division of Plastic &
Reconstructive Surgery, University of Florida Health Science Center, Gainesville, Florida 32610, USA. [email protected]
� BACKGROUND: Office-based surgery has become an important method of healthcare delivery, but there is controversy about its safety. Since 2000, a series of articles were published in the lay media emphasizing the hazards of office surgery, leading to the Florida Board of Medicine restricting office procedures. OBJECTIVE: The objective of this study was to determine the nature and scope of deaths resulting from office surgery. METHODS: We reviewed the data on mandatory reporting by physicians to a central agency of all office surgical incidents that resulted in death, injury, or hospital transfer in the state of Florida from January 2000 to November 2004. E-mail, Internet, and telephone follow up were used to determine physician's board status, office accreditation, and hospital privileges. We reviewed data on medication interactions, anesthesia, and monitoring. RESULTS: A total of 36 deaths related to office procedures were reported. Only 18 of those were related to surgical procedures that are within the realm of plastic surgery, although surgeons of other specialties did 3 of these. When these 18 were reviewed by type of anesthesia, there were 12 who had general anesthesia, 10 with an anesthesiologist and 2 with a Certified Registered Nurse Anesthetist. Of those 18, 7 died before discharge. Although all 7 of them survived long enough to be transferred to a hospital, we classified them as office deaths. The other 11 died after appropriate discharge. Of the 7 office deaths, one developed bronchospasm during induction by an anesthesiologist. Five were during deep sedation (level III anesthesia) and 4 appeared to be related to excessive sedation and/or inadequate monitoring; the fifth was probably related to illicit drug use and the sixth from a fat embolism. Of the 11 postoperative deaths, 7 were said to be the result of thromboembolism and the others were from unknown causes. CONCLUSION: Although the total number of office operations during the study period is unknown, the fact that 7 deaths were reported would suggest that the location in which these procedures were done was not as much of a factor as the regulators have suggested. However, better patient screening, sedation management, deep vein thrombosis prophylaxis, and clinical judgment may have prevented some, if not most, of these deaths. The most frequent cause of death after discharge was thromboembolism, and some of these might have been prevented with better prophylaxis. More detailed findings and recommendations are presented.
Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)

� 1: Plast Reconstr Surg. 2006 Sep;118(3):777-85; discussion 786-7. Links
� Comment in: Plast Reconstr Surg. 2007 Jun;119(7):2332-3; author reply 2333-4. Office surgery safety: the myths and truths behind the Florida moratoria--six years of Florida data.
� Clayman MA, Seagle BM.� Division of Plastic and Reconstructive
Surgery, University of Florida College of Medicine, USA. [email protected]
� BACKGROUND: Office-based surgery is an important method of health care delivery, and in 2000, the Florida Board of Medicine restricted office procedures. The objective of this study was to analyze the deaths resulting from office procedures in Florida. METHODS: The authors reviewed all office surgical incidents that resulted in death, injury, or hospital transfer in Florida from January of 2000 to January of 2006. Various methods were used to determine board status, office accreditation, and hospital privileges. RESULTS: In 6 years of Florida data, a total of 46 deaths related to office procedures were reported. Twenty of those were surgical procedures that are within the scope of plastic surgery, although non-board-certified plastic surgeons performed nine. Of those 20 related to plastic surgery, 11 died before discharge. Although all 11 survived long enough to be transferred to a hospital, we classified them as office deaths. The other nine died after appropriate discharge. Of the nine, seven deaths were from thromboembolism and the others from unknown causes. Thirty-five deaths were related to non-board-certified plastic surgeons and specialists in other fields. Board-certified plastic surgeons accounted for less than one-fourth of the deaths. There were no deaths from a board-certified plastic surgeon since April of 2004. CONCLUSIONS: There were over 600,000 operations during the study period. The fact that 11 office deaths were reported would suggest that the location in which these procedures were performed was not as much of a factor as the regulators have suggested. The most frequent cause of death after discharge was thromboembolism
Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)

� Dermatol Surg. 2008 Mar;34(3):285-91; discussion 291-2. Epub 2007 Dec 20. Links
� Office surgery incidents: what seven years of Florida data show us.
� Coldiron BM, Healy C, Bene NI.� Department of Dermatology, University
of Cincinnati, Cincinnati, Ohio, USA. [email protected]
� BACKGROUND: In the wake of increased media attention focusing on human error in medicine, numerous state medical boards and legislatures have drafted, and are continuing to draft, regulations aimed at protecting patients undergoing procedures in the office setting. These regulations will have a considerable impact on patient access to medically necessary procedures, and any regulations should be based on good data. This report summarizes 7 years of prospective data from the state of Florida, the best data available on office surgery incidents. OBJECTIVE: The objective was to determine the nature and incidence of hospital transfers and deaths resulting from office procedures. METHODS: This study is a compilation of mandatory reporting by Florida physicians to a central agency of all in-office adverse incidents resulting in death, serious injury, or hospital transfer in the State of Florida from March 2000 to March 2007. Telephone and internet follow-up was conducted to determine reporting physician board certification, hospital privileges, and office accreditation. RESULTS
Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)

Mortalità 2000-2007 nello stato della Florida:dati sulla Office based surgery
� In 7 anni :31 morti e 143 complicazioni degli interventi con trasferimento in ospedale
� 18 morti (58% del totale) e 87 complicanze (61%) da proceduree estetiche
� Liposuzione e liposuzione con addominoplastica o altro intervento cosmetico : 24 complicazioni e 8 decessi

� CONCLUSION: Plastic surgeons were responsible for an inordinate number of deaths and hospital transfers. Requiring physician board certification and physician hospital privileges would not seem to increase safety, because most physicians already have these credentials, and physicians without these credentials were not responsible for a disproportionate share of incidents. These data do not show an emergent hazard to patients from medically necessary office surgery. Liposuction under general anesthesia deserves continued scrutiny because deaths due to this procedure continue to occur and this procedure can be performed with dilute local anesthesia, with which no deaths were reported. Mandatory reporting of office incidents should be strongly supported, as well as reporting of incidents that occur after surgery in the hospital outpatient department and ambulatory surgery center. These data should be available for analysis after protecting patient confidentiality. A national debate needs to occur to determine how many deaths and injuries are acceptable from cosmetic procedures performed under general and intravenous anesthesia.

� Status degli uffici: 38.5% accreditati da una agenzia indipendente, 92.5% dei medici specialisti e 96.6% con privilegi ospedalieri.
� A total of 78% (14/18) of these deaths were in ASA Class 1 patients. Plastic surgeons were responsible for 48% of all deaths (83% of cosmetic surgery deaths) and for 52% of all hospital transfers (83% of cosmetic surgery complications and hospital transfers).

� Thermodynamics, Liposuction, and Metabolism
Kelley D. E. Extract | Full Text | PDF N Engl J Med 2004; 350:2542-2544, Jun 17, 2004. Perspective
Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)

� Metabolic Effects of Liposuction — Yes or No?
Esposito K., Giugliano G., Giugliano D., Arner P., Busetto L., Bassetto F., Nolli M. L., Klein S. Extract | Full Text | PDF N Engl J Med 2004; 351:1354-1357, Sep 23, 2004. Correspondence
Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)

American Academy of Dermatology Liposuction Guideline Development Task Force
American Academy of Dermatology Guidelines/Outcomes CommitteeNGC Clearinghouse 2001
� The guidelines were provided to the entire American Academy of Dermatology membership. Upon request, the guidelines have been sent to credentialing bodies. Finally, the guidelines were provided to state medical boards and/or state legislators
Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)

� Physician qualifications� The physician performing liposuction
has completed residency training or is board certified in a specialty that is recognized by the American Board of Medical Specialties, and that provides education in liposuction and training in cutaneous surgery.
� Level of Evidence: L6Strength of Recommendation: Unanimous Task Force opinion and weak evidence.
� The physician has documented liposuction training in residency or documented training and experience at the surgical table under the supervision of an appropriately trained and experienced liposuction surgeon.
� Strength of Recommendation: Unanimous Task Force opinion.
� In addition to the surgical technique, training includes instruction in fluid and electrolyte balance, potential complications of liposuction, and tumescent anesthesia and other forms of anesthesia employed.
� Strength of Recommendation: Unanimous Task Force opinion.
Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)

� Facility in which the procedure is performed and availability of emergency care
� Liposuction can be performed safely in a physician's office surgical facility, an ambulatory surgical facility, or a hospital operating room.
� Level of Evidence: L6Strength of Recommendation: Unanimous Task Force opinion and weak evidence.
� All liposuction surgeons and designated operating room staff have training in the management of acute cardiac emergencies.
� Strength of Recommendation: Unanimous Task Force opinion.
� Hospital privileges should not be required to perform tumescent liposuction, but a written plan for management of medical emergencies, including possible transfer, should be in place.
� Strength of Recommendation: Unanimous Task Force opinion
Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)

� Preoperative medical and psychosocial evaluation of the patient
� Liposuction is contraindicated in patients with severe cardiovascular disease, severe coagulation disorders, including thrombophilia, and during pregnancy.
� Strength of Recommendation: Unanimous Task Force opinion.
� A thorough medical history that gives special attention to any history of bleeding diathesis, emboli, thrombophlebitis, infectious diseases, poor wound healing, and diabetes mellitus is taken. Patients with a medical history of these conditions receive medical clearance prior to undergoing liposuction. The history also includes prior abdominal surgery and problems from past surgical procedures that may influence complications.
� Level of Evidence: L6Strength of Recommendation: Unanimous Task Force opinion and weak evidence.
� The use of all medications, vitamins, and herbs is documented with particular attention to medications that affect blood clotting (e.g., aspirin, nonsteroidal anti-inflammatory agents, vitamin E, and anticoagulants). Drugs that may interact with lidocaine, epinephrine, or sedative and anesthetic agents are noted.
� Strength of Recommendation: Unanimous Task Force opinion.
� Physical evaluation includes assessment of the general physical health to determine if the patient is a suitable candidate for surgery, and examination of specific sites under consideration for liposuction to check for potential problems.
� Level of Evidence: L6Strength of Recommendation: Unanimous Task Force opinion and weak evidence.
� Psychosocial evaluation includes inquiries about diet and exercise habits; history of weight gain and loss; familial body shape; and evaluation of patient's emotional ability to endure the procedure, their understanding of the limitations of liposuction, and their realistic expectations.
� Level of Evidence: L6Strength of Recommendation: Unanimous Task Force opinion and weak evidence.
� Selection of preoperative laboratory studies to be performed depends on the type and extent of the anticipated liposuction procedure and the conditions revealed in the history and physical examination.
� Strength of Recommendation: Unanimous Task Force opinion.
� If indicated by history, system review, or extent of anticipated liposuction procedure, a complete blood count with quantitative platelet assessment, prothrombin time, partial thromboplastin time, chemistry profile including liver function tests, and a pregnancy test for women of childbearing age is sufficient for most liposuction procedures.
� Strength of Recommendation: Unanimous Task Force opinion.
Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)

� Type of anesthesia employed and perioperative administration of anxiolytics, sedatives, and analgesics
� Lidocaine is the preferred type of local anesthetic.
� Level of Evidence: L6Strength of Recommendation: Unanimous Task Force opinion and weak evidence.
� If a patient takes medications that inhibit the metabolism of lidocaine, the medications should be discontinued before liposuction, or the total dosage of lidocaine should be reduced.
� Strength of Recommendation: Unanimous Task Force opinion.
� The recommended maximum dose of lidocaine is 55 mg/kg for most patients. Recommended lidocaine dosages are dependent upon appropriate epinephrine concentration in the tumescent solution.
� Level of Evidence: L6Strength of Recommendation: Unanimous Task Force opinion and weak evidence.
� The recommended concentration of epinephrine in tumescent solutions is 0.25 mg/L to 1.5 mg/L. The total dosage of epinephrine should be minimized, within these limits, and usually should not exceed 50 micrograms/kg.
� Strength of Recommendation: Unanimous Task Force opinion.
� If the surgeon anticipates that the maximum dose will be exceeded, consideration may be given to dividing the liposuction into separate procedures.
� Strength of Recommendation: Unanimous Task Force opinion.
� Oral anxiolytics, sedatives, or narcotic analgesics at dosages that are not associated with respiratory depression may be used with tumescent liposuction.
� Level of Evidence: L6Strength of Recommendation: Unanimous Task Force opinion and weak evidence.
� Intramuscular anxiolytics, sedatives, or narcotic analgesics may be used with caution with tumescent liposuction, since dose-response can vary widely and may be associated with respiratory depression.
� Strength of Recommendation: Unanimous Task Force opinion.
� Intravascular anxiolytics, sedatives, or narcotic analgesics may be associated with increased risk of morbidity and mortality if not used properly and in a setting such as an accredited surgical facility or hospital operating room and monitored by appropriately trained and credentialed personnel.
� Strength of Recommendation: Unanimous Task Force opinion.
� The use of inhalational (general) anesthesia for tumescent liposuction is not recommended.
� Level of Evidence: L6Strength of Recommendation: Unanimous Task Force opinion and weak evidence.
Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)

� Surgical technique/procedure including the performance of concomitant additional surgery, the size of the cannulae employed, the length of time of the procedure, and the volume of fat extracted per session and by body weight
� Performing liposuction with other procedures should be done with caution, unless all procedures are done under local anesthesia and the recommended dosage for tumescent lidocaine is not exceeded.
� Level of Evidence: L6Strength of Recommendation: Unanimous Task Force opinion and weak evidence.
� The recommended cannula size for liposuction is generally no larger than 4.5 mm in diameter.
� Level of Evidence: L6Strength of Recommendation: Unanimous Task Force opinion and weak evidence.
� The recommended volume of fat removed is in proportion to the fat content and/or size and/or weight of the patient being treated; and the recommended volume of fat removed generally does not exceed 4500 mL in a single operative session.
� Level of Evidence: L6Strength of Recommendation: Unanimous Task Force opinion and weak evidence.
� The dry technique for liposuction is contraindicated.
� Level of Evidence: L6Strength of Recommendation: Unanimous Task Force opinion and weak evidence.
� Liposuction in the treatment of obesity is experimental at this time and is not recommended.
� Level of Evidence: L6Strength of Recommendation: Unanimous Task Force opinion and weak evidence.
Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)

� Type of intra- and postoperative monitoring
� Baseline vital signs, including blood pressure and heart rate, are to be recorded pre- and postoperatively.
� Strength of Recommendation: Unanimous Task Force opinion.
� For procedures removing >100 mL of aspirate, there is the capability of continuous blood pressure monitoring, cardiac monitoring with pulse oximetry, and the availability of supplemental oxygen.
� Level of Evidence: L6Strength of Recommendation: Unanimous Task Force opinion and weak evidence.
� Sedated patients have postoperative monitoring until fully recovered and ready for discharge.
� Strength of Recommendation: Unanimous Task Force opinion.
� A plan for management of medical emergencies is in place.
� Strength of Recommendation: Unanimous Task Force opinion
Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)

� Postoperative compression� Specialized compression garments, binders,
and tape help to reduce bruising, hematomas, seromas, and pain. Anti-phlebitis support hose may be valuable for cases involving the lower legs.
� Strength of Recommendation: Unanimous Task Force opinion.
� The duration of compression is dictated by physician judgment, the location of the surgery, and the rate of recovery.
� Strength of Recommendation: Unanimous Task Force opinion.
Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)

� POTENTIAL HARMS� Rare but serious surgical complications
include:� Mortality � Cerebrovascular accident or transient
ischemic attack � Pulmonary thromboembolism � Fat embolism � Major skin loss � Anesthesia complication � Transfusion complication � Deep vein thrombosis� Subgroups Most Likely to be Harmed:� Patients who have a history of bleeding
diathesis, emboli, thrombophebitis, infectious diseases, poor wound healing, and diabetes mellitus.
� Obese patients and, for abdominal liposuction, patients with history of prior abdominal surgery.
Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)

� The Pursuit of Perfection: The Promise and Perils of Medical Enhancement
Resnik D. B. Extract | Full Text | PDF N Engl J Med 2004; 350:1368, Mar 25, 2004. B
Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)

� Unraveling the Fat Embolism Syndrome
Fabian T. C. Extract | Full Text N Engl J Med 1993; 329:961-963, Sep 23, 1993. Editorials
Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)

American Society of Plastic Surgeons - Practice advisory on liposuction,2004 Apr
� Iverson RE, Lynch DJ. Practice advisory on liposuction. Plast Reconstr Surg 2004 Apr 15;113(5):1478-90. [59 references] PubMed
� GUIDELINE COMMITTEE� American Society of Plastic Surgeons
(ASPS) Committee on Patient Safety� NGC Clearinghouse

� Comparative Outcomes Analysis of Procedures Performed in Physician Offices and Ambulatory Surgery Centers Hector Vila, Jr, MD; Roy Soto, MD; Alan B. Cantor, PhD; David Mackey, MD
� Arch Surg. 2003;138:991-995. � Hypothesis This study compared
outcomes to determine whether patient safety is similar in Florida ambulatory surgery centers and offices. Data Sources All adverse incident reports to the Florida Board of Medicine for procedure dates April 1, 2000, to April 1, 2002 were reviewed. The numbers of office procedures performed during a 4-month period were used to estimate the total number of procedures. Ambulatory surgery death summaries, adverse incident data, and volumes of procedures for 2000 were procured from
the Florida Agency for Health Care Administration.
� Study Selection/Data Extraction Adverse incident reports were reviewed by multiple parties; only reports that involved an office surgical procedure and resulted in injury or death were included in the outcomes calculation. Reports were extracted independently by multiple reviewers.
� Data Synthesis Adverse incidents occurred at a rate of 66 and 5.3 per 100 000 procedures in offices and ambulatory surgery centers, respectively. The death rate per 100 000 procedures performed was 9.2 in offices and 0.78 in ambulatory surgery centers. The relative risks for injuries and deaths for office procedures vs ambulatory surgery centers were 12.4 (95% confidence interval, 9.5-16.2) and 11.8 (95% confidence interval, 5.8-24.1), respectively.
� Conclusions In this review of surgical procedures performed in offices and ambulatory surgery centers in Florida during a recent 2-year period, there was an approximately 10-fold increased risk of adverse incidents and death in the office setting. If all office procedures had been performed in ambulatory surgery
centers, approximately 43 injuries and 6 deaths per year could have been prevented.
Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)

� 2003 Update: Outcomes Analysis of Procedures Performed in Florida Physician Offices and Ambulatory Surgery Centers Hector Vila, Jr., M.D., Roy G. Soto, M.D., Rafael V. Miguel, M.D., David C. Mackey, M.D.Anesthesiology / Interdisciplinary Oncology, H. Lee Moffitt Cancer Center and Research Institute; University of South Florida, Tampa, Florida. Introduction: Driven by media reports of office surgery deaths, in 2000, the Florida Board of Medicine enacted strict regulations for office surgery that included mandatory reporting of adverse incidents. Based on 2000 to 2002 data, we have previously reported a 12 fold higher risk for procedures performed in the office compared to the ambulatory surgery center. Many of the deaths occurred in unaccredited offices and in the absence of an anesthesiologist. This report compares the third year of outcomes data to prior years and also compares differences in anesthesia providers and facility accreditation.
Methods: All adverse incident reports filed from April 2002 through March 2003 were obtained from the Florida Board of Medicine and reviewed. Only reports associated with surgical procedures were included in the analysis. The number of injuries and deaths for the 12-month period were summarized and compared to similar data from the 24 months prior. Data on the number of office facilities that were accredited or passed Florida department of health inspection were also obtained by special request.
Results: There were 2 procedure related deaths and 18 injuries reported to the Florida Board of Medicine for the 12 month study period. There were 13 procedure related deaths and 93 injuries reported during the previous 24 months. During the study period 86% of the 350 registered offices met the inspected/accreditation requirement while only 56% of the registered offices had met this requirement before. Also, in April 2002 Florida instituted a requirement of an anesthesiologist for all deep sedation or general anesthetics. This requirement was met during the study period and was not met during the previous 24 months.
Discussion: The number of injuries and deaths in Florida offices was less during the last year than in the previous two-year period. This decrease in the number of adverse outcomes coincided with the implementation of the anesthesiologist requirement and an increase in the number of office facilities accredited or inspected. Data on the number of procedures performed in offices was not available for the study period, however the number of registered offices did not change significantly.
Anesthesiology 2003; 99: A1364
Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)

FINE
Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)

� Results: In 6 years of Florida data, a total of 46 deaths related to office procedures were reported. Twenty of those were surgical procedures that are within the scope of plastic surgery, although non–board-certified plastic surgeons performed nine. Of those 20 related to plastic surgery, 11 died before discharge.
� Although all 11 survived long enough to be transferred to a hospital, we classified
� them as office deaths. The other nine died after appropriate discharge. Of the nine, seven deaths were from thromboembolism and the others from unknown causes.
Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)

� Thirty-five deaths were related to non–board-certified plastic surgeons and specialists in other fields. Board-certified plastic surgeons accounted for less than one-fourth of the deaths. There were no deaths from a board-certified plastic surgeon since April of 2004.
Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)

Durata dell’intervento� In the selection of a plastic surgery procedure for the office setting, there are few prospective
data and mostly conflicting opinions on the importance of surgery duration alone as a predictor of adverse outcomes. Most plastic surgery procedures typically performed in an ambulatory setting take longer than 1 hour to complete. These procedures include face lifts, rhinoplasties, breast reductions, mastopexies, liposuctions, and abdominoplasties. It is not uncommon for several plastic surgery procedures to be performed during the same operative period, increasing the total duration of the surgery. In some studies, the duration of surgery does seem to correlate with adverse outcomes. In the anesthesia literature, Mingus et al. 7 suggest that any procedures extending beyond 1 hour correlate with a higher rate of postoperative admission. This may be a direct function of the procedure or it may relate to the procedure being more extensive than initially anticipated.
� Fogarty et al. 8 compared three categories of reconstructive plastic surgery that often last longer than 6 hours: head and neck, breast reconstruction, and upper and lower limb surgery. Despite having a similar mean duration of surgery, the differences in postoperative complications among the three groups suggest that the duration of surgery alone is not a major determinant of postoperative morbidity and that the type of surgery performed and the patient’s general health are more important predictors of outcomes. More extended procedures are likelier to produce postoperative nausea, vomiting, bleeding, and excessive pain, warranting overnight stay. 2,9,10 Several studies indicate that patients whose surgical procedure ended after 3 pm have a higher incidence of unanticipated admission than those whose surgery ended earlier. 9
� Recommendation: It is important to schedule long procedures sufficiently early in the day to allow for adequate recovery time before discharge. 7 If possible, the surgery should be completed by 3 pm to allow adequate time for recovery and discharge. Ideally, the overall duration of the procedure(s) should be completed within 6 hours. Although many plastic surgery procedures have proved safe in the office setting, attention to patient selection, intraoperative management, and postoperative care is of particular importance when procedures of longer duration are to be performed in the office setting. 2,10,11

� REf 7 e 8 di IVerson e AFPS task forcePatient Safety in Office-Based Surgery Facilities: I. Procedures in the Office-Based Surgery Setting
� [COSMETIC SECTION: COSMETIC SPECIAL TOPIC]
� Iverson, Ronald E. M.D.; and the ASPS Task Force on Patient Safety in Office-based Surgery Facilities

Misure di tromboprofilassi� Identificazione dei fattori di rischio e classificazione dei pazienti a
seconda della entità del rischio � Fattori genetici o acqusiti� Sindrome antifosfoilipidi� Omocistinemia� Contraccettivi recenti o terapia sostitutiva ormonale postmenopausa� Storia di dvt� Anamnesi ed esame obbiettivo� .� Risk Rating for Thrombosis or Embolism� * Low-risk: Patients who face uncomplicated surgery and have no risk
factors. These patients are usually under 40 years of age, although older patients undergoing short procedures may qualify.
� * Moderate-risk: Patients 40 years and older who have no additional risk factors but who face procedures longer than 30 minutes. Patients who use oral contraceptives or are on postmenopausal replacement therapy are also at moderate or greater risk.
� * High-risk: Patients over 40 years of age with at least one risk factor who face procedures over 30 minutes or longer under general anesthesia and/or have other risk factors.
� .

Tromboprofilassi a seconda della stratificazione del rischio
� * Low-risk: Comfortable positioning on the operating table with the knees slightly flexed. Constriction of the extremities and external pressure should be avoided.
� * Moderate-risk: In addition to the recommendations for low-risk patients, intermittent pneumatic compression devices of the calf or ankle and frequent alteration of the operating room table are recommended. The devices should be in place before the induction of general anesthesia, and their use should
be continued until the patient is awake and moving in the recovery unit.� * High-risk: In addition to all recommendations for low-risk and moderate-
risk patients, both a hematology consultation and preoperative/postoperative
pharmacologic antithrombotic therapy should be considered.
Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)

Problemi potenziali postoperatori che portano al ricovero ospedaliero non
programmato� Giramento di testa� Dolore� Nausea e vomito� Levin et al. 13 found that 9.5 percent of unplanned hospital
admissions resulted primarily from dizziness, pain, and nausea/vomiting. In their study, these symptoms were not correlated with the patient’s age.
� Dolore:correlato a :� Tipo di liposuzione� BMI� Estensione della procedura� Durata della procedura:>120 min + dolore

� Absence of an Effect of Liposuction on Insulin Action and Risk Factors for Coronary Heart Disease
Klein S., Fontana L., Young V. L., Coggan A. R., Kilo C., Patterson B. W., Mohammed B. S. Abstract | Full Text | PDF N Engl J Med 2004; 350:2549-2557, Jun 17, 2004. Original Articles
� ook Reviews

� 1: N Engl J Med. 2004 Jun 17;350(25):2549-57. Links
� Comment in: N Engl J Med. 2004 Jun 17;350(25):2542-4. N Engl J Med. 2004 Sep 23;351(13):1354-7; author reply 1354-7. N Engl J Med. 2004 Sep 23;351(13):1354-7; author reply 1354-7. N Engl J Med. 2004 Sep 23;351(13):1354-7; author reply 1354-7. Absence of an effect of liposuction on insulin action and risk factors for coronary heart disease.
� Klein S, Fontana L, Young VL, Coggan AR, Kilo C, Patterson BW, Mohammed BS.
� Center for Human Nutrition, Washington University School of Medicine, St. Louis 63110, USA.
� BACKGROUND: Liposuction has been proposed as a potential treatment for the metabolic complications of obesity. We evaluated the effect of large-volume abdominal liposuction on metabolic risk factors for coronary heart disease in women with abdominal obesity. METHODS: We evaluated the insulin sensitivity of liver, skeletal muscle, and adipose tissue (with a euglycemic-hyperinsulinemic clamp procedure and isotope-tracer infusions) as well as levels of inflammatory mediators and other risk factors for coronary heart disease in 15 obese women before and 10 to 12 weeks after abdominal liposuction. Eight of the women had normal glucose tolerance (mean [+/-SD] body-mass index, 35.1+/-2.4), and seven had type 2 diabetes (body-mass index, 39.9+/-5.6). RESULTS: Liposuction decreased the volume of subcutaneous abdominal adipose tissue by 44 percent in the subjects with normal glucose tolerance and 28 percent in those with diabetes; those with normal oral glucose tolerance lost 9.1+/-3.7 kg of fat (18+/-3 percent decrease in total fat, P=0.002), and those with type 2 diabetes lost 10.5+/-3.3 kg of fat (19+/-2 percent decrease in total fat, P<0.001). Liposuction did not significantly alter the insulin sensitivity of muscle, liver, or adipose tissue (assessed by the stimulation of glucose disposal, the suppression of glucose production, and the suppression of lipolysis, respectively); did not significantly alter plasma concentrations of C-reactive protein, interleukin-6, tumor necrosis factor alpha, and adiponectin; and did not significantly affect other risk factors for coronary heart disease (blood pressure and plasma glucose, insulin, and lipid concentrations) in either group. CONCLUSIONS: Abdominal liposuction does not significantly improve obesity-associated metabolic abnormalities. Decreasing adipose tissue mass alone will not achieve the metabolic benefits of weight loss. Copyright 2004 Massachusetts Medical Society
Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)

� Losing Weight — An Ill-Fated New Year's Resolution
Kassirer J. P., Angell M. Extract | Full Text N Engl J Med 1998; 338:52-54, Jan 1, 1998.
�
Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)

� Edito rials Deaths Related to LiposuctionRao R. B., Ely S. F., Hoffman R. S. Abstract | Full Text | PDF N Engl J Med 1999; 340:1471-1475, May 13, 1999. Original Articles
� Deaths Related to LiposuctionGinsberg M. M., Gresham L., Vermeulen C., Serra M., Roujeau J.-C., Talmor M., Barie P. S., Klein J. A., Rigel D. S., Wheeland R. G., Schnur P., Penn J., Fodor P. B., Rao R. B., Ely S. F., Hoffman R. S. Extract | Full Text N Engl J Med 1999; 341:1000-1003, Sep 23, 1999. Correspondence
Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)

� 1: N Engl J Med. 1999 May 13;340(19):1471-5. Links
� Comment in: N Engl J Med. 1999 Sep 23;341(13):1000-1; author reply 1002-3. N Engl J Med. 1999 Sep 23;341(13):1000; author reply 1002-3. N Engl J Med. 1999 Sep 23;341(13):1001-2; author reply 1002-3. N Engl J Med. 1999 Sep 23;341(13):1001; author reply 1002-3. N Engl J Med. 1999 Sep 23;341(13):1001; author reply 1002-3. N Engl J Med. 1999 Sep 23;341(13):1002-3. Deaths related to liposuction.
� Rao RB, Ely SF, Hoffman RS.� New York City Poison Control Center,
Department of Surgery-Emergency Medicine, New York University Medical Center, NY 10016, USA. [email protected]
� BACKGROUND: The technique of tumescent liposuction involves the subcutaneous infusion of a solution containing lidocaine, followed by the aspiration of fat through microcannulas. Although the recommended doses of lidocaine are as high as 55 mg per kilogram of body weight, few safety data are available. Since reporting of adverse events associated with tumescent liposuction is not mandatory, the incidence of complications and deaths is unknown. METHODS: We identified 5 deaths after tumescent liposuction among 48,527 deaths referred to the Office of Chief Medical Examiner of New York City between 1993 and 1998. The patients' records and postmortem examination results were reviewed to identify common contributory factors. RESULTS: The five patients had received lidocaine in doses ranging from 10 to 40 mg per kilogram. Other drugs, such as midazolam, were also administered. Three patients died as a result of precipitous intraoperative hypotension and bradycardia with no definitively identified cause. Postmortem blood lidocaine concentrations in two of the patients were 5.2 and 2 mg per liter. One patient died of fluid overload, and one died of deep venous thrombosis of calf veins with pulmonary thromboembolism after tumescent liposuction of the legs. CONCLUSIONS: Tumescent liposuction can be fatal, perhaps in part because of lidocaine toxicity or lidocaine-related drug interactions
Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)

� : Dermatol Surg. 2002 Aug;28(8):710-2; discussion 713. Links
� Office surgical incidents: 19 months of Florida data.
� Coldiron B.� [email protected]� BACKGROUND: In 1999-2000 a series
of sensational articles were published in the lay media emphasizing the hazards of office surgery. Since then 31 state medical boards or legislatures have, or are in the process of drafting regulations restricting office procedures. OBJECTIVE: To determine the nature, incidence and scope of injuries and deaths resulting from office procedures. METHODS: Mandatory reporting by physicians to a neutral central agency of all office surgical incidents that resulted in death, serious injury, or transfer to a hospital in the State of Florida from February 2000 to September 2001. Telephone and Internet follow up to determine reporting physician board status, hospital privilege status, and office accreditation status. RESULTS: In 19 months there were 43 procedure related-complications and eight deaths. Liposuction under general anesthesia was the single most common cause of incidents and deaths. There were no injuries or deaths reported with liposuction with tumescent anesthesia. 50% of offices reporting incidents or deaths were accredited by an independent accrediting agency. There were no incidents or deaths reported due to the anesthesia when using conscious sedation anesthesia, or intramuscular sedation or analgesia 98% of physicians reporting incidents or deaths had hospital privileges and were board certified. Anesthesiologists or nurse anesthetists provided all general anesthesia, and deep sedation. There were no physicians performing procedures outside their scope of specialty training. CONCLUSION: Liposuction under general anesthesia deserves closer scrutiny. Office accreditation is not associated with fewer patient injuries and deaths. Restrictions on tumescent liposuction, conscious sedation and intramuscular sedation and analgesia would not yield any saved lives or fewer injuries since these modes of anesthesia resulted in no injuries or deaths. Board certification and hospital privilege requirements for office practice would have very little effect since the vast majority of reporting physicians already had these credentials. These data do not show an emergent hazard to patients from office surgery This data strongly contradicts the lay media portrayal of the dangers of office procedures. Mandatory reporting of office incidents should be strongly supported, and this data should be available for analysis after protecting patient confidentiality
Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)

� Dermatol Surg. 2005 Jul;31(7 Pt 1):733-43; discussion 743. Links
� Erratum in: Dermatol Surg. 2005 Sep;31(9 Pt 1):1158. Review of the liposuction, abdominoplasty, and face-lift mortality and morbidity risk literature.
� Yoho RA, Romaine JJ, O'Neil D.� Department of Dermatology, Martin
Luther King-Drew Medical Center, Los Angeles, California, USA. [email protected]
� BACKGROUND: The statistical discrepancies that exist in the mortality and morbidity risk literature are such that surgeons and patients cannot accurately assess the true risk rates associated with plastic surgery procedures. OBJECTIVES AND METHODS: To review any relevant literature published to date in which the risk rates from liposuction, abdominoplasty, and rhytidectomy are cited and to reassess these figures alongside those published for both elective and emergency general surgeries. RESULTS AND CONCLUSION: Despite the lack of reliable, comprehensive reporting of deaths and complications resulting from cosmetic surgeries, published data demonstrate that the risks associated with liposuction and rhytidectomy compare favorably with those from most general surgical procedures. In contrast, the morbidity and mortality rates from abdominoplasty remain unacceptably high. A significant lack of literature documenting cosmetic breast implant surgery and blepharoplasty risks is observed, which should be of concern to both patients and physicians. Liposuction and face-lift surgery data generally show that surgical centers are statistically safer than hospital operating rooms, although the data have not been standardized for the patients' American Society of Anesthesiologists (ASA) risk class, the health of the patient prior to surgery. General anesthesia may carry a risk roughly equivalent to or perhaps greater than cosmetic surgery, although, again, ASA class variables confound clear comparison between studies. Recent anesthesia literature refutes the many claims that general anesthesia risks are now remote: a landmark study that surveyed the entire scholarly literature showed a mortality rate of 1 in 13,000, roughly similar to overall cosmetic surgery mortality risks. Moreover, a prolonged operating time has been repeatedly implicated in other surgical literature to be related to morbidity and mortality. The latter certainly has relevance to cosmetic surgery.
Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)

� Teimourian B, Rogers W. A national survey of complications associated with suction lipectomy: a comparative study. Plast Reconstr Surg 1989; 84:628-631.
� 2. Grazer F, De Jong R. Fatal outcomes from liposuction: census survey of cosmetic surgeons. Plast Reconstr Surg 2000;105:436-446.
� 3. Teimourian B, Adham M. A national survey of complications associated with suction lipectomy: what we did then and what we do now. Plast Reconstr Surg 2000;105:1881-1883.
� 4. Schorge JO, Goldhaber SZ, Duska LR, Goodman A, Feldman S. Clinically significant venous thromboembolism after gynecologic surgery. J Reprod Med 1999;44:669-673.
� 5. Turpie AG, Gallus AS, Hoek JA. A synthetic pentasaccharide for the prevention of deep-vein thrombosis after total hip replacement. N Engl J Med 2001;344:619-625.
� 6. Florida Moratorium on Office Surgery. AM News. September 4, 2000.
� 7. Jewell M. The patient’s right to self-determination: complexities of informed consent. Aesthetic Surg J 2000;20:133-134.

� Plast Reconstr Surg. 1989 Oct;84(4):628-31. Links
� A national survey of complications associated with suction lipectomy: a comparative study.
� Teimourian B, Rogers WB 3rd.� Department of Surgery, Suburban
Hospital, Bethesda, Md.� In March of 1988, a survey form was
sent to all 2695 U.S. and Canadian members of the American Society of Plastic and Reconstructive Surgeons. Nine-hundred and thirty-five members responded, for a response rate of 34.7 percent. The purpose of the survey was to ascertain the total number of major liposuction, dermatolipectomy, and abdominoplasty procedures performed from January of 1984 to January of 1988 and to compare nine specific complications that are associated with these three procedures. The 935 surgeons reported a total of 112,756 procedures performed: major liposuction (75,591), dermatolipectomy (10,603), and abdominoplasty (26,562). Nine major complications were surveyed: mortality, myocardial infarction, cerebrovascular accident or transient ischemic attack, pulmonary thromboembolism, fat embolism, major skin loss, anesthesia complication, transfusion complications, and deep venous thrombosis. The findings in this survey showed, when comparing these three procedures and the nine types of complications, that the complication rate for major suction lipectomy was 0.1 percent, for dermatolipectomy 0.9 percent, and for abdominoplasty 2.0 percent. Fat emboli did not prove to be a significant factor associated with any of the three procedures. However, of the 15 reported deaths (major liposuction 2, dermatolipectomy 2, and abdominoplasty 11), pulmonary thromboembolism was the causative factor in 9 deaths (60 percent). Based on these analyzed data, we feel that major suction lipectomy has a low complication rate and is a reasonably safe procedure.
Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)

� complication rate for major suction lipectomy was 0.1 percent, for dermatolipectomy 0.9 percent, and for abdominoplasty 2.0 percent. Fat emboli did not prove to be a significant factor associated with any of the three procedures. However, of the 15 reported deaths (major liposuction 2, dermatolipectomy 2, and abdominoplasty 11), pulmonary thromboembolism was the causative factor in 9 deaths (60 percent).
Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)

� 1: Plast Reconstr Surg. 2006 May;117(6):1797-808. Links
� Erratum in: Plast Reconstr Surg. 2007 Jan;119(1):426-7. Comment in: Plast Reconstr Surg. 2007 Jan;119(1):426-7. Abdominoplasty and abdominal contour surgery: a national plastic surgery survey.
� Matarasso A, Swift RW, Rankin M.� [email protected]� BACKGROUND: According to the
American Society for Aesthetic Plastic Surgery's 2004 Cosmetic Surgery National Data Bank, during the last 7 years, the number of abdominoplasty procedures performed has increased 344 percent. A national report on abdominoplasty has not been since 1977. Grazer and Goldwyn's study reflects the preliposuction era of abdominal contouring surgery. The purpose of this study was to assess current trends in abdominal contouring techniques and associated procedures and the incidence of their complications. METHODS: The study was designed as a descriptive correlation survey evaluating the frequency of various abdominal contour techniques and complications among 3300 randomly chosen members of the American Society of Plastic Surgeons. There were 497 respondents, for a response rate of 15 percent. RESULTS: A total of 20,029 procedures were reported in the survey; 35 percent (n = 7010) were liposuction of the abdomen, 10 percent (n = 2003) were limited abdominoplasties, and 55 percent (n = 11,016) were full abdominoplasties. Survey data covered the plastic surgeon's demographics, techniques, and incidence of complications during a 12-month period. CONCLUSIONS: The authors report the largest series of local and systemic complication rates and compare them with those of previously published abdominoplasty surveys. With respect to full abdominoplasty, lower complication rates for deep vein thrombosis (0.04 percent) and pulmonary embolus (0.02 percent) were seen. No deaths were reported. There was no correlation between a surgeon's years in practice and complication rates, in concordance with the earlier study by Grazer and Goldwyn. Despite more extensive abdominal contouring techniques and the addition of liposuction to abdominal contouring, the local and systemic complication rates coincided with previous complication rates, as outlined in other studies.
Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)

� Plast Reconstr Surg. 2006 Jul;118(1):207-12; discussion 213-4. Links
� Is it safe to combine abdominoplasty with elective breast surgery? A review of 151 consecutive cases.
� Stevens WG, Cohen R, Vath SD, Stoker DA, Hirsch EM.
� Marina Plastic Surgery Associates and the Keck School of Medicine of University of Southern California, USA. [email protected]
� BACKGROUND: This study was designed to evaluate and compare the complication rates of patients having abdominoplasty without breast surgery with the rates of those having abdominoplasty with various types of elective breast surgery, including breast augmentation, breast reduction, mastopexy, and mastopexy combined with simultaneous augmentation. METHODS: The data collected represent a retrospective chart review of consecutive abdominoplasty procedures performed at a single outpatient facility by the senior surgeon (W.G.S.) over a 15-year period (1989 to 2004). Two groups were compared: patients who underwent abdominoplasty without breast surgery and those who had abdominoplasty with breast surgery. The second group was subdivided by the various types of breast procedures noted above. The minor complications assessed included seromas, hematomas, infections, and small (<5 cm) wound breakdowns. Major complications evaluated included large (>5 cm) flap necrosis, need for blood transfusion, deep vein thrombosis, pulmonary embolus, myocardial infarction, and death. Additional data compiled included age, sex, tobacco use, body mass index, past medical history, American Society of Anesthesiologists physical status level, and operative times. RESULTS: Of the 415 abdominoplasty procedures, 264 (group 1) did not include simultaneous breast surgery. One hundred fifty-one procedures (group 2) involved simultaneous breast surgery, representing 36 percent of the total. Group 2 was further subdivided into those who had breast augmentation surgery (group 2A, n = 50), those who had breast reduction surgery (group 2B, n = 31), those who had mastopexy surgery (group 2C, n = 28), and those who had simultaneous mastopexy and breast augmentation surgery (group 2D, n = 42). Removal and replacement of implants and capsulectomy/capsulotomy procedures were included in the augmentation group (group 2A). There were no major complications, including flap necrosis (open wound >5 cm), blood transfusions, deep vein thrombosis, pulmonary embolus, myocardial infarction, or death. No patients required hospitalization. No statistically significant associations with complications were noted between groups 1 and 2 (chi-square, 0.0045; p > 0.95, not significant). Furthermore, when subdivided by type of breast surgery, no statistically significant associations were noted among subgroups: group 1 versus 2A (chi-square, 0.96; p > 0.05, not significant), group 1 versus 2B (chi-square, 0.032; p > 0.9, not significant), group 1 versus 2C (chi-square, 0.003; p > 0.975, not significant), and group 1 versus 2D (chi-square, 0.83; p > 0.5, not significant). CONCLUSION: The results of this retrospective review indicate that combining elective breast surgery with abdominoplasty does not appear to significantly increase the number of major or minor complications.
Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)

PRATO Liposuzione, Nas sequestrano studio non autorizzato
� PRATO, 18 OTTOBRE 2002 - Un locale utilizzato per interventi chirurgici di liposuzione è stato sequestrato dai carabinieri del Nas di Firenze in uno studio medico di Prato. Il locale - che era stato affittato da un chirurgo di Pisa - non avrebbe avuto alcuna autorizzazione per gli interventi di quel tipo. I carabinieri hanno sequestrato anche tutte le apparecchiature e le attrezzature e hanno denunciato il medico e il rappresentante legale dello studio per esercizio medico in locali non autorizzati.

� In an attempt to crack down on problems with office-based surgeries, the Florida Board of Medicine has imposed a 90-day ban on combination abdominoplasty and liposuction procedures.
� The board is responding to media reports and concerns about the deaths of eight patients during office surgeries since the summer of 2002. Three of those deaths involved combination liposuction and abdominoplasty.
� The moratorium went into effect Feb. 11. It requires that liposuction and abdominoplasty procedures performed on the same patient in an office setting be separated by 14 days. Board officials said the combination of procedures increases the risks of a deadly blood clot.
� In 2000, patient deaths prompted the medical board to issue a 90-day ban on office surgeries that required general anesthesia or heavy sedation. That led to new safety standards for office surgery, including accrediting of offices, mandatory reporting of adverse incidents and credentialing of surgeons.
� But board Chair Lisa Tucker, MD, said the current regulations might not be enough to protect patients. Board officials said they would evaluate office surgery logs to determine if stricter measures are needed.
� "This rule doesn't close anybody down," said Larry McPherson Jr., board executive director. "This is a very limited restriction
Servizio di Anestesia e Rianimazione Ospedale di Faenza(RA)