Me e t i n g d e l l e n e u r o s c i e n z e t o s c a n ...€¦ · AI P E R CO R SI I NTE R DI...
31
Il contributo della stimolazione transcranica alle neuroscienze: una riflessione SIMPOSIO CONGIUNTO SNO/SIN–SINC (Società Italiana di Neurofisiologia Clinica) Massimo Cincotta S.C. di Neurologia, Firenze - Azienda USL Toscana Centro Discussant Simone Rossi Dip.to di Scienze Mediche Chirurgiche e Neuroscienze - Università di Siena Societ à dei Neurologi, Neurochirurghi e Neuroradiologi Ospedalieri Meet ing del l e neur oscienze t oscane DALLA EPIDEMIOLOGIA AI PERCORSI INTERDISCIPLINARI 6-8 apr ile 2017 GROSSETO
Transcript of Me e t i n g d e l l e n e u r o s c i e n z e t o s c a n ...€¦ · AI P E R CO R SI I NTE R DI...

Il contributo della stimolazione transcranica
alle neuroscienze: una riflessione
SIMPOSIO CONGIUNTO
SNO/SIN–SINC (Società Italiana di Neurofisiologia Clinica)
Massimo Cincotta S.C. di Neurologia, Firenze - Azienda USL Toscana Centro
Discussant Simone Rossi Dip.to di Scienze Mediche Chirurgiche e Neuroscienze - Università di Siena
6-8 aprile 2017 GROSSETO
HOTEL CONFERENCE CENTRE
FATTORIA LA PRINCIPINAS.P. 158 delle Collacchie, 465
58100 Principina Terra (GR)
Sono stati concessi i patrocini di:
Società dei Neurologi,Neurochirurghi eNeuroradiologi Ospedalier i
Meet ing del l e neur oscienze t oscane
Comune di Grosseto
Ordine dei Medici Chirurghi
e degli Odontoiatri
DALLA EPIDEMIOLOGIA AI PERCORSI INTERDISCIPLINARI
Pr o g r aMM
a
6-8 aprile 2017 GROSSETO
HOTEL CONFERENCE CENTRE
FATTORIA LA PRINCIPINAS.P. 158 delle Collacchie, 465
58100 Principina Terra (GR)
Sono stati concessi i patrocini di:
Società dei Neurologi,Neurochirurghi eNeuroradiologi Ospedalier i
Meet ing del l e neur oscienze t oscane
Comune di Grosseto
Ordine dei Medici Chirurghi
e degli Odontoiatri
DALLA EPIDEMIOLOGIA AI PERCORSI INTERDISCIPLINARI
Pr o g r aMM
a

Potenziali evocati motori (MEP)
da stimolazione elettrica transcranica
Stimolazione
corticale

Cenni storici D ’ Arsonval (1896) Electromagnetic fields may also elicit phosphenes
Thompson SP. 1910. A physiological effect of an alternating magnetic field. Proc R Soc Lond B B82:396-399.
Dunlap K. 1911. Visual sensations from the alternating magnetic field. Science 33:68-71.
Magnusson CE & Stevens HC. 1911. Visual sensations created by a magnetic field. Am J Physiol 29:124-136.
Barker AT, Jalinous R, Freeston IL. Non-invasive magnetic stimulation of human motor cortex. Lancet 1985;1:1106–7.

Coil focale e coil circolare

Principali applicazioni
della stimolazione magnetica transcranica
• Studio della conduzione nervosa cortico-spinale
• Studio dei meccanismi eccitatori ed inibitori corticali
• Interferenza con le funzioni corticali
• Modulazione dei meccanismi eccitatori ed inibitori corticali
• Studio della neuroplasticità
• Studio delle connessioni cortico-corticali

Stimolazione magnetica transcranica
PubMed: transcranial magnetic stimulation
0
200
400
600
800
1000
1200
1400
PubMed: transcranial magnetic stimulation


Potenziali evocati motori
da stimolazione magnetica transcranica:
mielopatia cervicale spondiloartrosica

Valutazione dei fenomeni eccitatori ed inibitori della
corteccia motoria primaria (M1) mediante TMS
• Soglia motoria (RMT, AMT)
• Ampiezza e curva di reclutamento del MEP
• Periodo silente corticale (CSP)
• Periodo silente ipsilaterale (ISP)
• Inibizione intracorticale da impulsi appaiati a breve intervallo interstimolo (SICI)
• Facilitazione intracorticale (ICF)
• Inibizione intracorticale da impulsi appaiati a lungo intervallo interstimolo (LICI)
• Inibizione transcallosale del MEP da impulsi appaiati
• Inibizione afferente a breve latenza (SAI)
• Inibizione afferente a lunga latenza (LAI)

Stimolazione magnetica
transcranica (TMS)






Nature © Macmillan Publishers Ltd 1997
letters to nature
182 NATURE|VOL 389| 11 SEPTEMBER1997
somatosensory information in sighted mammalsoccursat corticalassociation sites2. It is possible that connections between parietaland visual association areasmediate thetransfer of somatosensoryinformation to the occipital cortex in blind subjects22. If so, whatoperations does the occipital cortex perform with the tactileinformation?In our experiment, speech wasnot affected bystimu-lation of anysite, and errorswerenot corrected when subjectsweregiven achanceto restate their choice after theend of stimulation.This indicates that errorswerenot dueto interferencewith speech(output), but todisruption of discrimination processing.TMSovercontralateral sensorimotor cortex and over parietal sites was rela-tively lesseffectivein inducingerrorsthan over mid-occipital areas(Fig. 2). Therefore, arrival of somatosensory information in pri-marysomatosensorycortex (input) wasrelativelysparedbyTMSinblind subjects. Becauseprimary input (somatosensory) and output(speech) werespared, theeffectsof mid-occipital TMSarethoughtto be related to interference with more complex discriminativeoperations performed by the occipital cortex in the blind. Theoccasional induction of complex sensations (phantom or extradots) with occipital TMSsupportsthis interpretation. Stimulationof sensorimotor regions that resulted in jerking of contralateralhand muscles (each TMS train produced 12:206 4:43 motor
evoked potentials in theSVRand 12:406 3:38 in theEBBgroups)did not induce sensations of missing or extra dots in any of thesubjectstested.
In theSVRgroup, therewasasignificant effect of stimulated scalpposition ontheerror rate.Stimulation of theoccipital cortexdidnotaffect identification of embossedRoman lettersor induceabnormalsomatosensory perceptions. This result, in combination with thedecreaseof occipital activity on positron emission tomography insubjectsperformingasimilar task1,suggeststhat sighted individualsdo not normally use the occipital cortex for identification ofembossed Roman letters as the blind do for Braille and Romanletter reading. Stimulation of the contralateral sensorimotorcortex induced more errors than in the control conditionðP# 0:001;OR¼2:95;CI ¼ð1:95;4:48ÞÞ. Because the ability tointerfere with a task is likely to depend on how well learned thetask is, the hand movements induced by stimulation of the con-tralateral sensorimotor cortex may haveexerted amoredisruptiveeffect in theless-trained sighted readersthan in thehighly trainedblind readers. Alternatively, sighted subjectsmay havespent moretimethan blind subjects in somatosensory processing, making thetask moresusceptible to disruption by TMSover thecontralateralsensorimotor cortex.
Thefinding that theoccipital cortex isan important componentof the network involved in Braille reading supports the idea thatperceptionsaredynamicallydeterminedbythecharacteristicsof thesensory inputs rather than only by the brain region that receivesthose inputs, at least in thecaseof early blindness2,7. Theseresultsshowthat cross-modal plasticityasidentified electrophysiologicallyor by neuroimaging techniques in humans may be involved infunctional compensation. M. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Methods
Subjects. StudyprotocolswereapprovedbytheInstitutional ReviewBoardsof
theNational Instituteof Neurological DisordersandStrokeand theUniversity
of Valencia, and TMSwas used under a USFood and Drug Administration
investigational deviceexemption. Subjectsgavetheir written informed consent
for thestudy. Blind subjectshad normal brain magnetic resonanceimagesand
no progressiveneurological disease. Sighted volunteers had normal neurolo-
gical examinationsand visual acuity better than 20/40.
Stimulation technique. Each train of TMSwastriggered bythereadingfinger
crossing a laser beam (Fig. 1b) and had a fixed frequency of 10Hz and a
duration of 3s. TMSwasdeliveredwith amagnetoelectricstimulator (Cadwell
Laboratories, Kennewick, WA) and an 8-shaped23 water-cooled coil, each loop
of which was7cm in diameter. Thecoil washeld tangentially to thescalp with
the intersection of both loops oriented sagittally. The stimulus intensity
(normalized across subjects) was 10% above the minimal output of the
stimulator required to induce a 50-mV electromyographic response from a
relaxed muscle (first dorsal interosseous) involved in theBraille reading task
when thestimuluswasapplied over theprimary motor cortex.
Positions stimulated. SeeFig. 1a. In theblindsubjects(EBB, seeTable1),TMS
wasdelivered randomly to threeoccipital positions(midline, contralateral and
ipsilateral to thereadingfinger, overlyingBrodmann areas17, 18 and 19; Oz,
O1 and O2 of the international 10–20 system of electrode placement), two
parietal positions (contralateral and ipsilateral, approximately overlying
Brodmann area 7; P3 and P4), a midfrontal position (Fz) and to the
contralateral sensorimotor area(overlyingBrodmannareas4,3,1and2)24.Asa
control condition, TMS was also delivered into the air (the sound of the
stimulator was as loud as in actual brain stimulation, but no stimulation
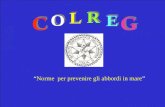
Figure 2 Error rates (mean 6 s:e:) for stimulation of different positions in the four
groups studied. Missing bars indicate that stimulation at that position was not
performed in that specific group (see Methods). Black bars indicate error rates
induced by stimulation of the mid-occipital position, and grey bars the error rates
induced by stimulation of the contralateral sensorimotor cortex. In both groups of
early blind subjects, stimulation of the mid-occipital position induced more errors
in reading Braille and Roman letters than stimulation of any other position,
whereas in the sighted volunteers stimulation of the contralateral primary sen-
sorimotor region induced more errors than stimulation of any other position.
Asterisks indicate scalp positions where significantly more errors occurred than
control (air, marked with arrows). S-M, sensorimotor cortex; contra, contralateral;
ipsi, ipsilateral. Asterisk, P , 0:001.
Table 2 Number of letters read in 3 s
5 Braille letters
EBB
3 Roman letters
SVR
3 Roman letters
EBR
Unstimulated
trials
Stimulated
trials
Unstimulated
trials
Stimulated
trials
Unstimulated
trials
Stimulated
trials.............................................................................................................................................................................
Mean 3.80 3.73 2.38 2.44 2.80 2.86
S.d. 0.83 1.10 0.49 0.62 0.40 0.34.............................................................................................................................................................................



2013

Quartarone et al., 2006
Protocolli di stimolazione transcranica off-line


In the late 1700s to early 1800s,
Giovanni Aldini (Galvani’s
nephew) reported experiments
using galvanization to treat
psychosis and depression
Stimolazione elettrica transcranica (tES)

Guidelines
Evidence-based guidelines on the therapeutic use of transcranial direct
current stimulation (tDCS)
Jean-Pascal Lefaucheur a,b,⇑, Andrea Antal c, Samar S. Ayachea,b, David H. Benninger d, Jérôme Brunelin e,
Filippo Cogiamanian f,g, Maria Cotelli h, Dirk De Ridder i,j, Roberta Ferrucci f,g, Berthold Langguth k,
Paola Marangolo l,m, Veit Myliusn,o, Michael A. Nitschep,q, Frank Padberg r, Ulrich Palm r,
Emmanuel Poulet e,s, Alberto Priori f,g,t, Simone Rossi u, Martin Schecklmann k, Sven Vannestev,w,
Ulf Ziemann x, Luis Garcia-Larrea y,1, Walter Paulusc,1
aDepartment of Physiology, Henri Mondor Hospital, Assistance Publique–Hôpitaux deParis,Créteil, FrancebEA4391, NerveExcitability and Therapeutic Team (ENT), Faculty of Medicine, ParisEst Créteil University, Créteil, FrancecDepartment of Clinical Neurophysiology, University Medical Center, Georg-August University, Göttingen, GermanydDepartment of Clinical Neurosciences, Section of Neurology, CentreHospitalier Universitaire Vaudois, Lausanne, SwitzerlandePsyR2 Team, U1028, INSERM and UMR5292, CNRS, Center for Neuroscience Research of Lyon (CRNL), CH LeVinatier, Lyon-1 University, Bron, Francef Clinica Neurologica III, Dipartimento di Scienzedella Salute, Azienda Ospedaliera Santi Paolo eCarlo,Università degli Studi di Milano, Milano, ItalygIRCCSFondazione OspedaleMaggiorePoliclinico, Milano, ItalyhNeuropsychology Unit, IRCCSFondazione Istituto Centro San Giovanni di Dio Fatebenefratelli, Brescia, Italyi Brai2n, Tinnitus Research Initiative Clinic of Antwerp, Sint Augustinus Hospital, Wilrijk, Belgiumj Department of Surgical Sciences, Section of Neurosurgery, Dunedin School of Medicine, University of Otago, Dunedin, New ZealandkDepartment of Psychiatry and Psychotherapy, University of Regensburg, Regensburg, Germanyl Dipartimento di Studi Umanistici, University Federico II, Naples, Italym IRCCSFondazione Santa Lucia, Rome, ItalynDepartment of Neurology, Section Pain and Neuromodulation, University of Marburg, Marburg, GermanyoDepartment of Neurology, Center for Neurorehabilitation, Valens, SwitzerlandpDepartment of Psychology and Neurosciences, Leibniz Research Centre for Working Environment and Human Factors, Dortmund, GermanyqDepartment of Neurology, University Medical Hospital Bergmannsheil, Bochum, Germanyr Department of Psychiatry and Psychotherapy, Ludwig Maximilian University, Munich, GermanysDepartment of Emergency Psychiatry, Edouard Herriot Hospital, HospicesCivilsdeLyon, Lyon, Francet Dipartimento di Fisiopatologia Medico-Chirurgica edei Trapianti, Università degli Studi di Milano, Milano, ItalyuUnit of Neurology and Clinical Neurophysiology, Brain Investigation & Neuromodulation Lab, Department of Neuroscience, and Human Physiology Section, Siena University, Siena,
ItalyvDepartment of Translational Neuroscience, Faculty of Medicine, University of Antwerp, Edegem, BelgiumwLaboratory for Auditory and Integrative Neuroscience, School of Behavioral and Brain Sciences, TheUniversity of Texas, Dallas, TX, USAxDepartment of Neurology & Stroke, and Hertie Institute for Clinical Brain Research, Eberhard KarlsUniversity, Tübingen, GermanyyNeuroPain Team, U1028, INSERM, Center for Neuroscience Research of Lyon (CRNL), Lyon-1 University, Bron, France
a r t i c l e i n f o
Articlehistory:
Accepted 20 October 2016
Available online 29 October 2016
h i g h l i g h t s
Agroup of European experts reviewed current evidencefor therapeutic efficacy of tDCS.
Level Bevidence (probableefficacy) was found for fibromyalgia, depression and craving.
The therapeutic relevance of tDCSneeds to be further explored in theseand other indications.
http://dx.doi.org/10.1016/j.clinph.2016.10.087
1388-2457/Ó2016 International Federation of Clinical Neurophysiology. Published by Elsevier Ireland Ltd. All rights reserved.
Abbreviations: AD, Alzheimer’s disease; ARAT, action research arm test; BDI, Beck Depression Inventory; BI, Barthel Index; DC, direct current; DLPFC, dorsolateral
prefrontal cortex; EEG, electroencephalography; ERP, event-related potentials; FMA, Fugl-Meyer assessment; fMRI, functional magnetic resonance imaging; GABA, gamma-
aminobutyric acid; HDRS, Hamilton Depression Rating Scale; JTT, Jebsen–Taylor hand function test; M1, primary motor cortex; MADRS, Montgomery–Asberg depression
rating scale; MCS, minimally conscious state; MEP, motor evoked potential; NMDA, N-methyl D-aspartate; OMCASS, Orgogozo MCA scale; PANSS, positive and negative
symptomsscale; PD,Parkinson’sdisease; PES, peripheral electrical stimulation; RCT, randomized controlled trial; rTMS, repetitive transcranial magnetic stimulation; SANS,
Scalefor theAssessment of NegativeSymptoms; tACS, transcranial alternating current stimulation; tDCS, transcranial direct current stimulation; TMS, transcranial magnetic
stimulation; tRNS, transcranial random noise stimulation; tsDCS, transcutaneous spinal direct current stimulation; UPDRS, unified Parkinson’s disease rating scale; V1,
primary visual cortex; VAS, visual analogue scale; VRT, virtual reality training; VS, vegetative state.⇑ Correspondingauthor at: ServicePhysiologie,ExplorationsFonctionnelles,Hôpital Henri Mondor,51avenuedeLattredeTassigny,94010Créteil cedex,France. Fax: +331
4981 4660.
E-mail address: [email protected] (J.-P. Lefaucheur).1 Equal contribution.
Clinical Neurophysiology 128 (2017) 56–92
Contents lists available at ScienceDirect
Clinical Neurophysiology
journal homepage: www.elsevier.com/locate/cl inphKeywords:
Cortex
Indication
Neurological disease
Neuromodulation
Noninvasive brain stimulation
Psychiatric disease
tDCS
Treatment
a b s t r a c t
Agroup of European expertswascommissioned by theEuropean Chapter of theInternational Federation
of Clinical Neurophysiology to gather knowledgeabout thestateof theart of the therapeutic useof tran-
scranial direct current stimulation (tDCS) from studies published up until September 2016, regarding
pain,Parkinson’sdisease,other movement disorders, motor stroke,poststrokeaphasia,multiplesclerosis,
epilepsy, consciousness disorders, Alzheimer’sdisease, tinnitus, depression, schizophrenia, and craving/
addiction. Theevidence-based analysis included only studiesbased on repeated tDCSsessionswith sham
tDCScontrol procedure; 25 patients or more having received active treatment was required for Class I,
while a lower number of 10–24 patients was accepted for Class II studies. Current evidence does not
allow makingany recommendation of Level A (definiteefficacy) for any indication. Level Brecommenda-
tion (probableefficacy) isproposed for: (i) anodal tDCSof the left primary motor cortex (M1) (with right
orbitofrontal cathode) in fibromyalgia; (ii) anodal tDCSof the left dorsolateral prefrontal cortex (DLPFC)
(with right orbitofrontal cathode) in major depressive episodewithout drug resistance; (iii) anodal tDCS
of theright DLPFC(with left DLPFCcathode) in addiction/craving. Level Crecommendation (possibleeffi-
cacy) is proposed for anodal tDCSof the left M1 (or contralateral to pain side, with right orbitofrontal
cathode) in chronic lower limb neuropathicpain secondary to spinal cord lesion. Conversely, Level Brec-
ommendation (probable inefficacy) isconferred on theabsenceof clinical effectsof: (i) anodal tDCSof the
left temporal cortex (with right orbitofrontal cathode) in tinnitus; (ii) anodal tDCSof theleft DLPFC(with
right orbitofrontal cathode) in drug-resistant major depressiveepisode. It remainstobeclarifiedwhether
the probable or possible therapeutic effects of tDCSare clinically meaningful and how to optimally per-
form tDCSin atherapeutic setting. In addition, theeasy management and low cost of tDCSdevicesallow
at homeuseby thepatient,but thismight raiseethical and legal concernswith regard topotential misuse
or overuse. Wemust becareful toavoid inappropriateapplicationsof thistechniqueby ensuring rigorous
training of the professionals and education of the patients.
Ó2016 International Federation of Clinical Neurophysiology. Published by Elsevier Ireland Ltd. All rights
reserved.
Contents
1. Principles and mechanisms of action of transcranial direct current stimulation. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 58
2. Clinical applications of tDCS: literature data analysis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 59
3. Pain . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 60
4. Parkinson’s disease. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 63
4.1. tDCSeffects on motor symptoms. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 63
4.2. tDCSeffects on nonmotor symptoms. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 63
4.3. Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 64
5. Other movement disorders . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 64
6. Motor stroke. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 65
7. Aphasia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 68
8. Multiple sclerosis. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 69
9. Epilepsy. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 71
10. Disorders of consciousness . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 72
11. Alzheimer’s disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 72
12. Tinnitus. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 72
13. Depression . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 74
13.1. Antidepressant effects. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 75
13.2. Cognitive effects . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 76
14. Schizophrenia. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 76
15. Substance abuse, addiction and craving. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 78
16. Other psychiatric disorders . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 79
17. At-home do-it-yourself DCSand neural enhancement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 80
18. Perspectives of targets other than cortical (cerebellum and spinal cord). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 80
18.1. Cerebellar tDCS. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 80
18.2. Transcutaneous spinal direct current stimulation. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 81
19. Perspectives of treatment by transcranial electrical stimulation methods other than tDCS(tACS, tRNS) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 81
20. Summary of recommendations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 82
Conflict of interest. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 83
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 83
J.-P. Lefaucheur et al./Clinical Neurophysiology 128 (2017) 56–92 57
Guidelines
Evidence-based guidelines on the therapeutic use of transcranial direct
current st imulat ion (tDCS)
Jean-Pascal Lefaucheur a,b,⇑, Andrea Antal c, Samar S. Ayache a,b, David H. Benninger d, Jérôme Brunelin e,
Fil ippo Cogiamanian f,g, Maria Cotelli h, Dirk De Ridder i,j, Roberta Ferrucci f,g, Berthold Langguth k,
Paola Marangolo l,m, Veit Mylius n,o, Michael A. Nitsche p,q, Frank Padberg r, Ulrich Palm r,
Emmanuel Poulet e,s, Alberto Priori f,g,t, Simone Rossi u, Mart in Schecklmann k, Sven Vanneste v,w,
Ulf Ziemann x, Luis Garcia-Larrea y,1, Walter Paulusc,1
aDepartment of Physiology, Henri Mondor Hospital, Assistance Publique – Hôpitaux deParis, Créteil, FrancebEA4391, Nerve Excitability and Therapeutic Team (ENT), Faculty of Medicine, Paris Est Créteil University, Créteil, FrancecDepartment of Clinical Neurophysiology, University Medical Center, Georg-August University, Göttingen, GermanydDepartment of Clinical Neurosciences, Section of Neurology, Centre Hospitalier Universitaire Vaudois, Lausanne, SwitzerlandePsyR2 Team, U 1028, INSERM and UMR5292, CNRS, Center for Neuroscience Research of Lyon (CRNL), CH Le Vinatier, Lyon-1 University, Bron, Francef Clinica Neurologica III, Dipartimento di Scienze della Salute, Azienda Ospedaliera Santi Paolo eCarlo, Università degli Studi di Milano, Milano, Italyg IRCCSFondazione Ospedale Maggiore Policlinico, Milano, ItalyhNeuropsychology Unit, IRCCSFondazione Istituto Centro San Giovanni di Dio Fatebenefratelli, Brescia, Italyi Brai2n, Tinnitus Research Initiative Clinic of Antwerp, Sint Augustinus Hospital, Wilrijk, Belgiumj Department of Surgical Sciences, Section of Neurosurgery, Dunedin School of Medicine, University of Otago, Dunedin, New Zealandk Department of Psychiatry and Psychotherapy, University of Regensburg, Regensburg, Germanyl Dipartimento di Studi Umanistici, University Federico II, Naples, Italym IRCCSFondazione Santa Lucia, Rome, ItalynDepartment of Neurology, Section Pain and Neuromodulation, University of Marburg, Marburg, GermanyoDepartment of Neurology, Center for Neurorehabilitation, Valens, SwitzerlandpDepartment of Psychology and Neurosciences, Leibniz Research Centre for Working Environment and Human Factors, Dortmund, GermanyqDepartment of Neurology, University Medical Hospital Bergmannsheil, Bochum, Germanyr Department of Psychiatry and Psychotherapy, Ludwig Maximilian University, Munich, GermanysDepartment of Emergency Psychiatry, Edouard Herriot Hospital, Hospices Civils de Lyon, Lyon, Francet Dipartimento di Fisiopatologia Medico-Chirurgica edei Trapianti, Università degli Studi di Milano, Milano, ItalyuUnit of Neurology and Clinical Neurophysiology, Brain Investigation & Neuromodulation Lab, Department of Neuroscience, and Human Physiology Section, Siena University, Siena,
Italyv Department of Translational Neuroscience, Faculty of Medicine, University of Antwerp, Edegem, Belgiumw Laboratory for Auditory and Integrative Neuroscience, School of Behavioral and Brain Sciences, TheUniversity of Texas, Dallas, TX, USAx Department of Neurology & Stroke, and Hertie Institute for Clinical Brain Research, Eberhard Karls University, Tübingen, Germanyy NeuroPain Team, U 1028, INSERM, Center for Neuroscience Research of Lyon (CRNL), Lyon-1 University, Bron, France
a r t i c l e i n f o
Article history:
Accepted 20 October 2016
Available online 29 October 2016
h i g h l i g h t s
A group of European experts reviewed current evidence for therapeutic efficacy of tDCS.
Level Bevidence (probable efficacy) was found for fibromyalgia, depression and craving.
The therapeutic relevance of tDCSneeds to be further explored in these and other indications.
http://dx.doi.org/10.1016/j.clinph.2016.10.087
1388-2457/Ó 2016 International Federation of Clinical Neurophysiology. Published by Elsevier Ireland Ltd. All rights reserved.
Abbreviations: AD, Alzheimer’s disease; ARAT, action research arm test; BDI, Beck Depression Inventory; BI, Barthel Index; DC, direct current; DLPFC, dorsolateral
prefrontal cortex; EEG, electroencephalography; ERP, event-related potentials; FMA, Fugl-Meyer assessment; fMRI, functional magnetic resonance imaging; GABA, gamma-
aminobutyric acid; HDRS, Hamilton Depression Rating Scale; JTT, Jebsen–Taylor hand function test; M1, primary motor cortex; MADRS, Montgomery–Asberg depression
rating scale; MCS, minimally conscious state; MEP, motor evoked potential; NMDA, N-methyl D-aspartate; OMCASS, Orgogozo MCA scale; PANSS, positive and negative
symptoms scale; PD,Parkinson’s disease; PES, peripheral electrical stimulation; RCT, randomized controlled trial; rTMS, repetitive transcranial magnetic stimulation; SANS,
Scale for the Assessment of Negative Symptoms; tACS, transcranial alternating current stimulation; tDCS, transcranial direct current stimulation; TMS, transcranial magnetic
stimulation; tRNS, transcranial random noise stimulation; tsDCS, transcutaneous spinal direct current stimulation; UPDRS, unified Parkinson’s disease rating scale; V1,
primary visual cortex; VAS, visual analogue scale; VRT, virtual reality training; VS, vegetative state.⇑ Corresponding author at: ServicePhysiologie, ExplorationsFonctionnelles,Hôpital Henri Mondor, 51 avenuedeLattredeTassigny, 94010Créteil cedex, France. Fax: +33 1
4981 4660.
E-mail address: [email protected] (J.-P. Lefaucheur).1 Equal contribution.
Clinical Neurophysiology 128 (2017) 56–92
Contents lists available at ScienceDirect
Clinical Neurophysiology
journal homepage: www.elsevier.com/locate/cl inph


Recommendation:
Necessary conditions: Given this situation, the IFCN recommends that for any use of tES in the
treatment of a medical indication (at home or in the clinic) this should be done with a medical grade
device or consumer device (CE mark) and under supervision of a medical provider and trained
personnel. In the United States, devices having been approved for Over-The-Counter (Non-
Prescription) by the governing regulatory agency may also be used by law.
Necessary and sufficient conditions: In medical applications, a necessary and sufficient condition is
the use of protocols, which have demonstrated in peer-reviewed clinical trials to be both safe and
efficacious. The manufacturer should have this information in the user manual, based on clinical
evaluations. In non-medical applications, efficacy and safety should also be standard, including
home-use. Many scientific investigations have shown both positive and negative results for
circumscribed cognitive processes in special investigations. As many ‘home-applied’ protocols have
not been formally tested, and many sensitive parameters have not been carefully reproduced,
stimulation may switch positive into negative results.
Thus, the IFCN warns against the use of DIY devices and methods unless they have shown
both efficacy and safety.

Grazie
dell’attenzione!

• The utility of a neurophysiological technique is helping difficult differential diagnosis
• VS/MCS: misdiagnosis in 40% of cases, even in qualified Centers
• TMS/EEG differentiates VS/MCS with a sensitivity of 94.7%

Local and Distant Responses (Cortical Reactivity & Connectivity)
Santarnecchi & Rossi 2016

PLOS One, 2014
Absence of EEG responses expecially in axonal damage

• rTMS is complementary to traditional neuroimaging (causality)
rTMS produces errors

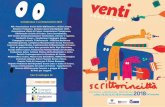
SMA rTMS Trial ~ results
Supplementary motor area stimulation for Parkinson
disease:
a randomized controlled study. Neurology 2013;80:1–6
10
20
30
0 5 10 15 20
1Hz10 HzSham
Intervention
Week
UP
DR
S p
art
III
sco
re
10
20
30
0 5 10 15 20
1Hz10 HzSham
Intervention
Week
UP
DR
S p
art
III
sco
re
*
8 weeks
6.8
UPDRS
points
rTMS for therapy: The case of Parkinson’s Disease
Problems:
Costs/efficacy
Sustainability