
LEGGERE I NUMERI DEL CANCRO -...
41
LEGGERE I NUMERI DEL CANCRO Seconda Università di Napoli Paolo Chiodini
Transcript of LEGGERE I NUMERI DEL CANCRO -...

LEGGERE I NUMERI DEL CANCRO
Seconda Università di Napoli Paolo Chiodini
Paolo Chiodini – Parma AIOM – 19 Giugno 2015
OUTLINE
RELATIVO E ASSOLUTO (efficacia trattamenti)
VELOCITÀ (analisi intermedie)
SINTESI (revisioni sistematiche)
DATI MANCANTI (publication bias)
SOPRAVVIVENZA E DIAGNOSI (lead time bias)
SFORTUNA (caso e tumore)
Paolo Chiodini – Parma AIOM – 19 Giugno 2015
RELATIVO E ASSOLUTO (efficacia trattamenti)
Paolo Chiodini – Parma AIOM – 19 Giugno 2015
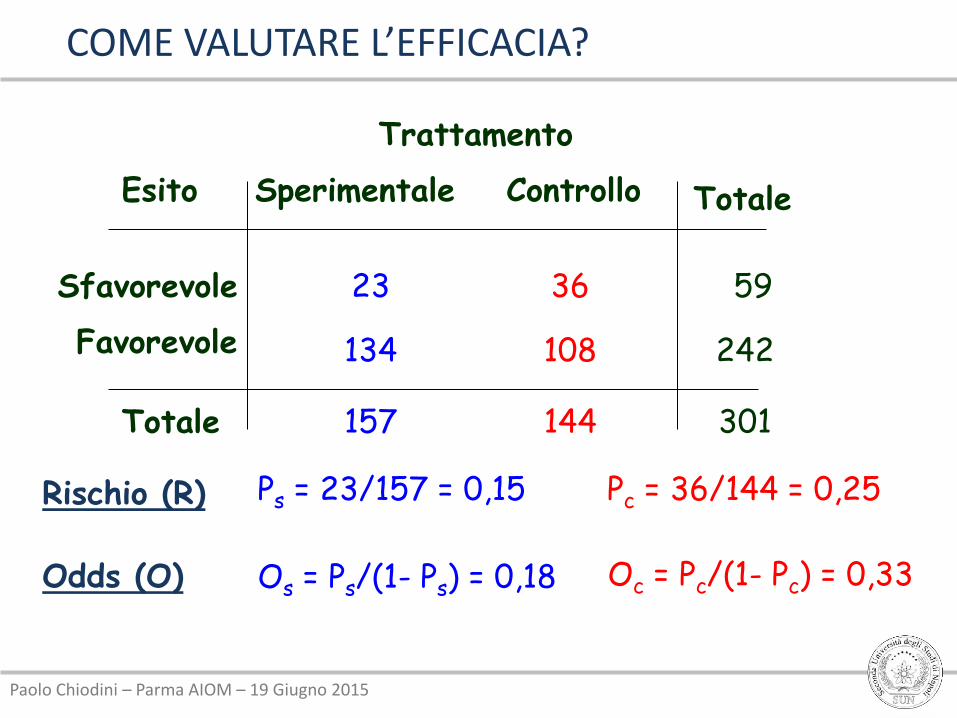
Esito
Sfavorevole
Trattamento
Sperimentale Controllo
Totale
Totale
23 36
134 108
157 144
59
242
301
Favorevole
Rischio (R) Ps = 23/157 = 0,15 Pc = 36/144 = 0,25
Odds (O) Os = Ps/(1- Ps) = 0,18 Oc = Pc/(1- Pc) = 0,33
COME VALUTARE L’EFFICACIA?
Paolo Chiodini – Parma AIOM – 19 Giugno 2015
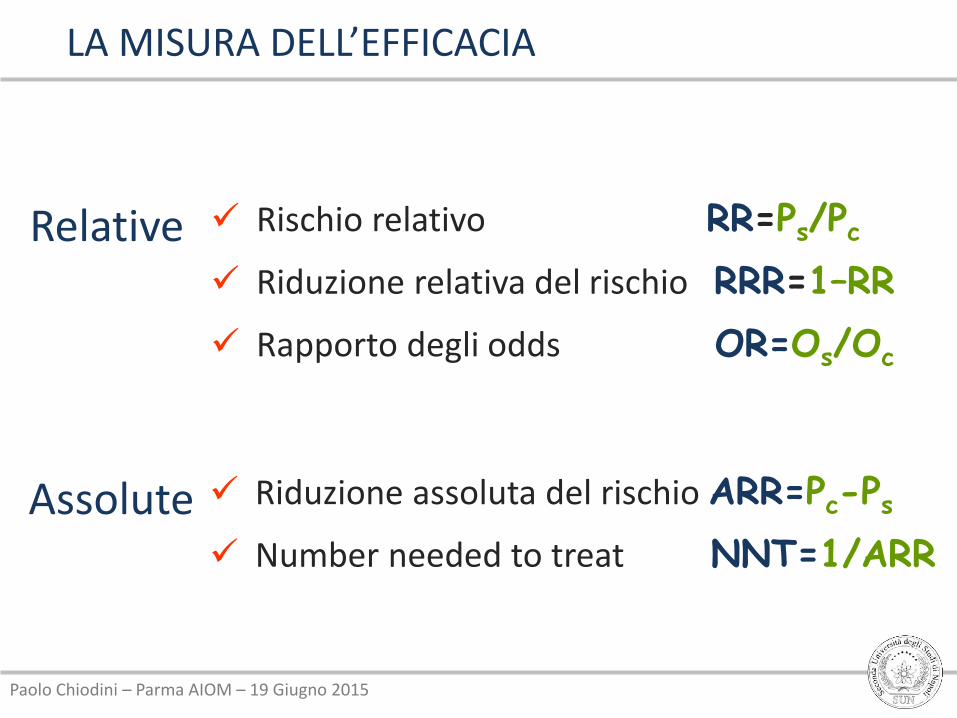
Relative Rischio relativo RR=Ps/Pc
Riduzione relativa del rischio RRR=1–RR
Rapporto degli odds OR=Os/Oc
Assolute Riduzione assoluta del rischio ARR=Pc-Ps
Number needed to treat NNT=1/ARR
LA MISURA DELL’EFFICACIA
Paolo Chiodini – Parma AIOM – 19 Giugno 2015
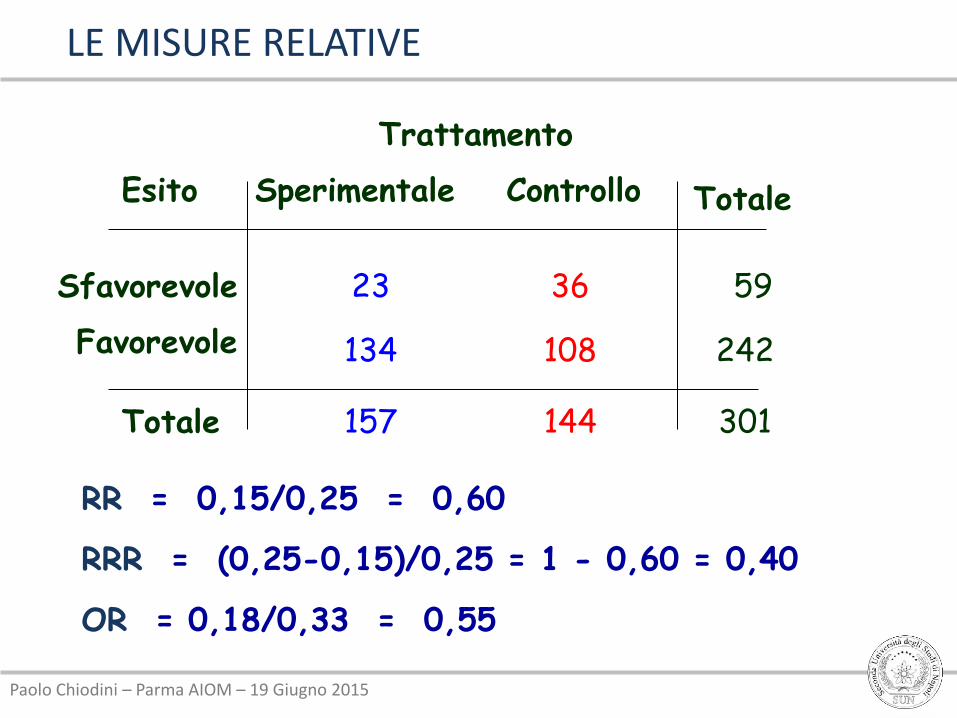
RR = 0,15/0,25 = 0,60
RRR = (0,25-0,15)/0,25 = 1 - 0,60 = 0,40
OR = 0,18/0,33 = 0,55
LE MISURE RELATIVE
Esito
Sfavorevole
Trattamento
Sperimentale Controllo
Totale
Totale
23 36
134 108
157 144
59
242
301
Favorevole
Paolo Chiodini – Parma AIOM – 19 Giugno 2015
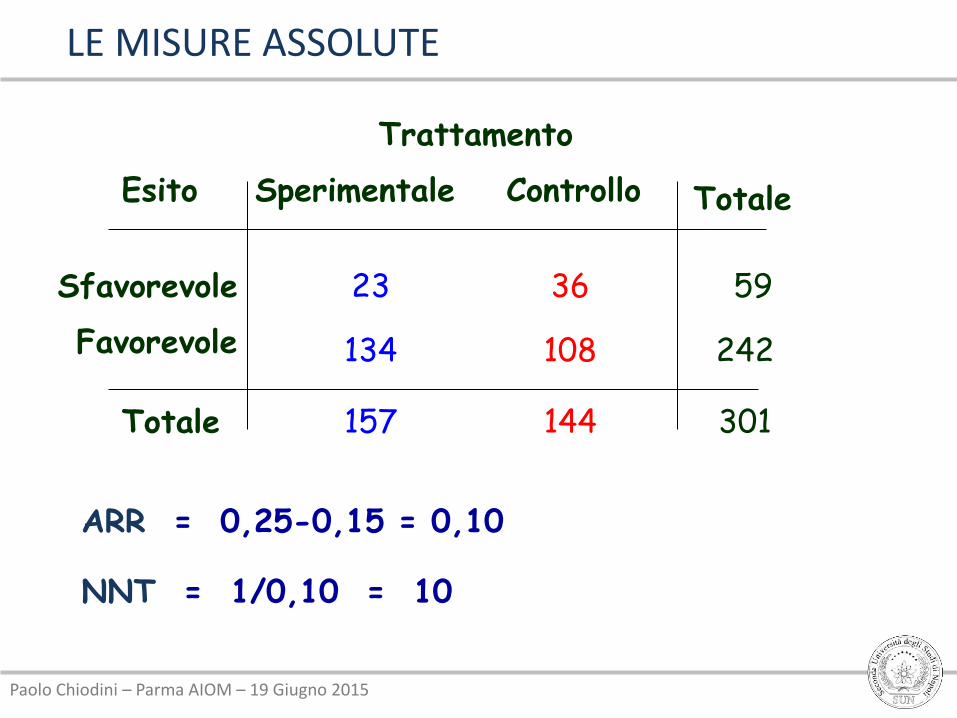
ARR = 0,25-0,15 = 0,10
NNT = 1/0,10 = 10
Esito
Sfavorevole
Trattamento
Sperimentale Controllo
Totale
Totale
23 36
134 108
157 144
59
242
301
Favorevole
LE MISURE ASSOLUTE
Paolo Chiodini – Parma AIOM – 19 Giugno 2015
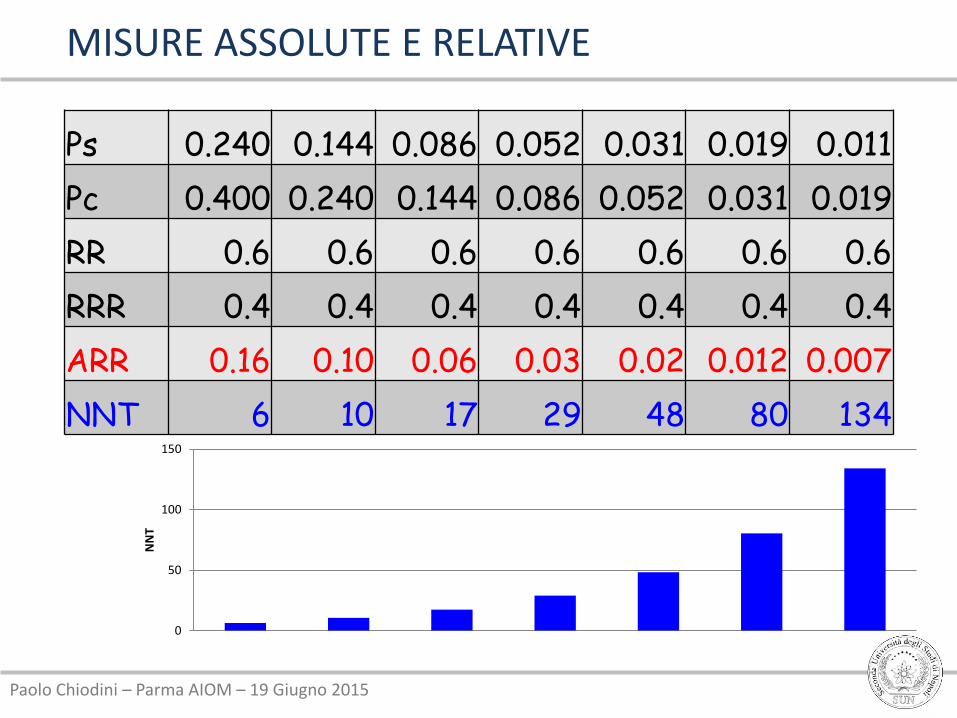
MISURE ASSOLUTE E RELATIVE
Ps 0.240 0.144 0.086 0.052 0.031 0.019 0.011
Pc 0.400 0.240 0.144 0.086 0.052 0.031 0.019
RR 0.6 0.6 0.6 0.6 0.6 0.6 0.6
RRR 0.4 0.4 0.4 0.4 0.4 0.4 0.4
ARR 0.16 0.10 0.06 0.03 0.02 0.012 0.007
NNT 6 10 17 29 48 80 134
0
50
100
150
NN
T
Paolo Chiodini – Parma AIOM – 19 Giugno 2015
0 20 40 60 80 100
RRR
ARR
NNT
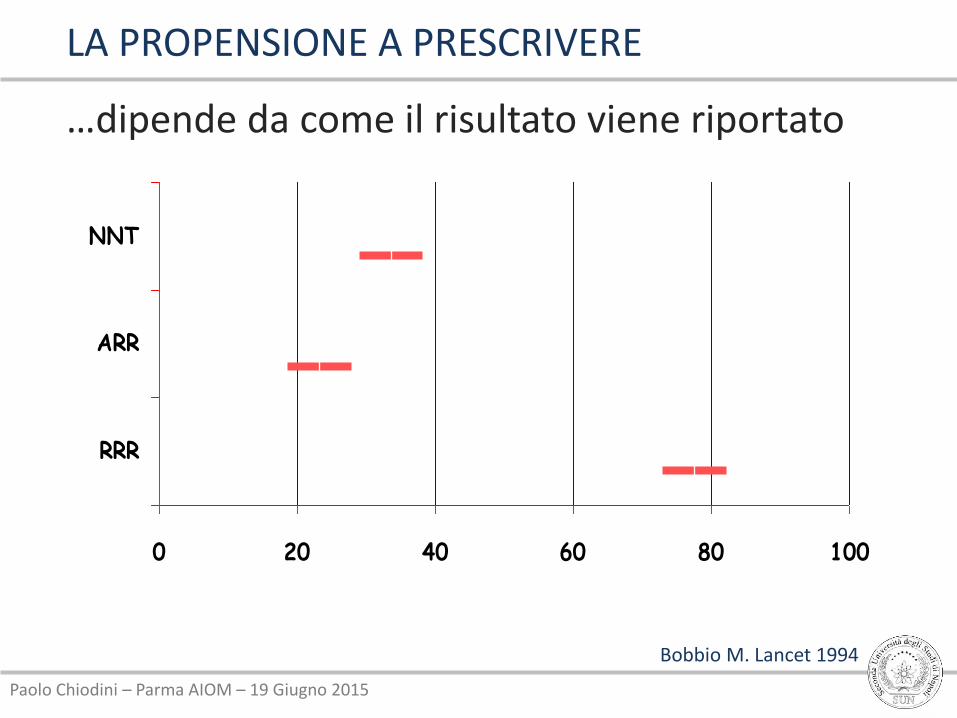
Bobbio M. Lancet 1994
LA PROPENSIONE A PRESCRIVERE
…dipende da come il risultato viene riportato
Paolo Chiodini – Parma AIOM – 19 Giugno 2015
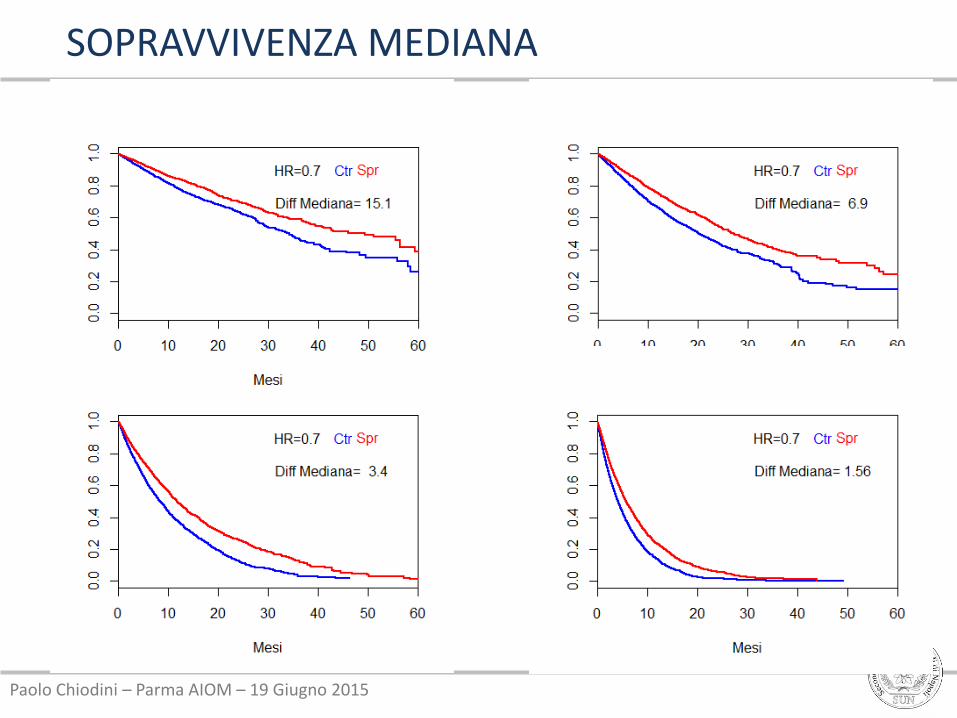
SOPRAVVIVENZA MEDIANA

Paolo Chiodini – Parma AIOM – 19 Giugno 2015
VELOCITÀ (analisi intermedie)
Paolo Chiodini – Parma AIOM – 19 Giugno 2015
Permettono di individuare precocemente differenze rilevanti e inattese fra i gruppi confrontati (efficacia, sicurezza, fattibilità)
Possono ridurre potenzialmente il numero di soggetti esposti ad un trattamenti inferiore
Anticipano la disponibilità di un trattamento superiore
Evitano il coinvolgimento inutile di pazienti in uno studio che non può raggiungere gli obiettivi prefissati
Risparmio di tempo e risorse
LE ANALISI INTERMEDIE
Paolo Chiodini – Parma AIOM – 19 Giugno 2015
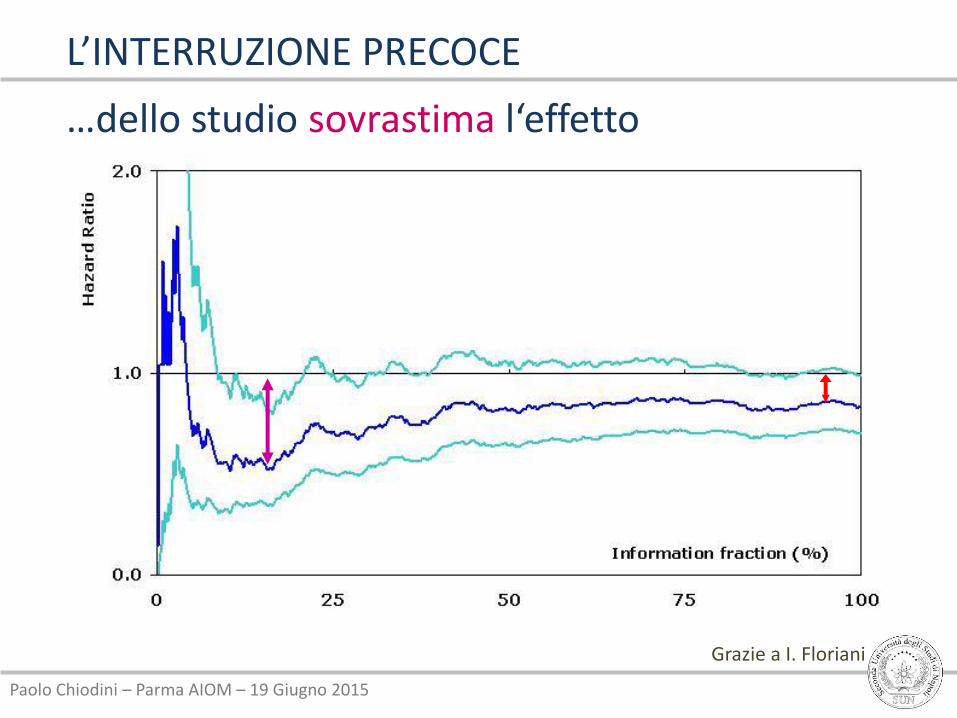
Grazie a I. Floriani
L’INTERRUZIONE PRECOCE
…dello studio sovrastima l‘effetto
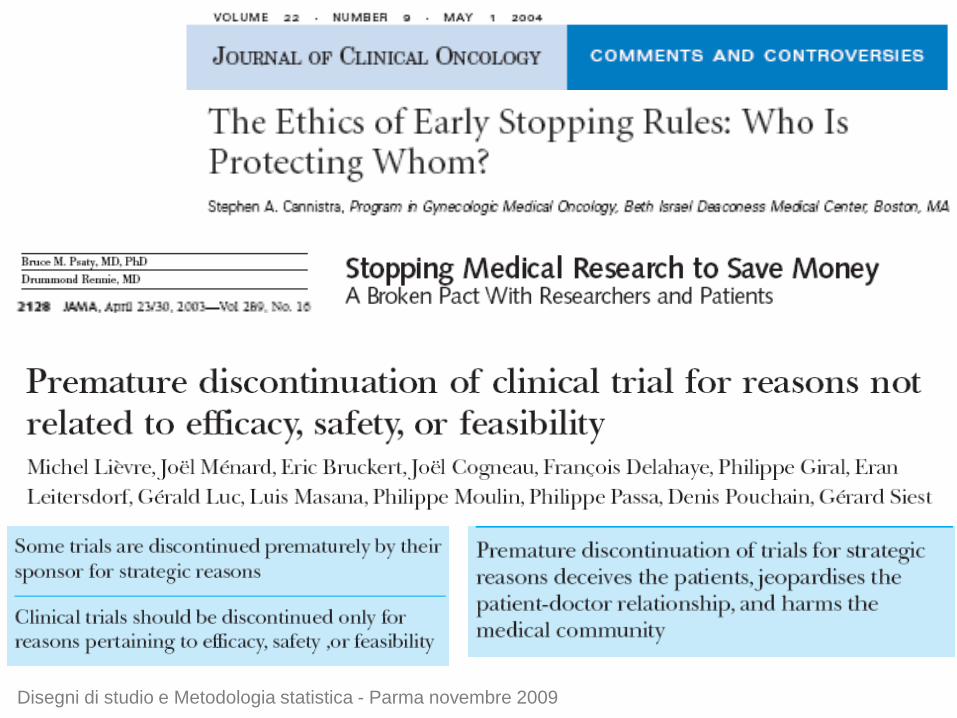
Disegni di studio e Metodologia statistica - Parma novembre 2009
5_Piano di analisi
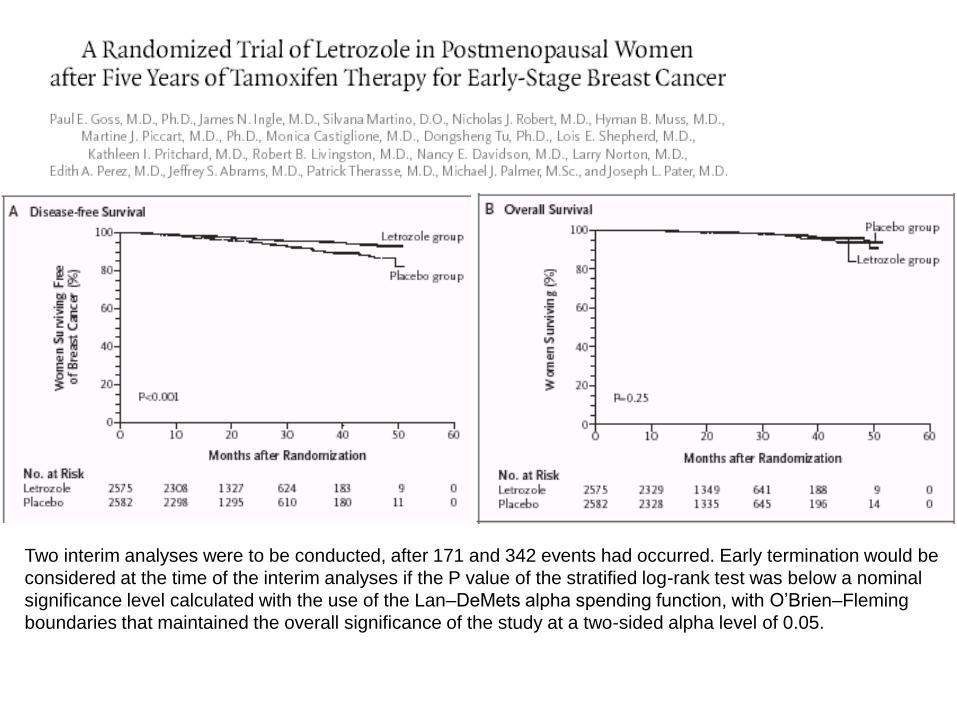
Two interim analyses were to be conducted, after 171 and 342 events had occurred. Early termination would be
considered at the time of the interim analyses if the P value of the stratified log-rank test was below a nominal
significance level calculated with the use of the Lan–DeMets alpha spending function, with O’Brien–Fleming
boundaries that maintained the overall significance of the study at a two-sided alpha level of 0.05.

We conducted a double-blind, placebo-controlled trial to test the
effectiveness of five years of letrozole therapy in postmenopausal
women with breast cancer who have completed five years of tamoxifen
therapy. The primary end point was disease-free survival.
A total of 5187 women were enrolled (median follow-up, 2.4 years). At
the first interim analysis, there were 207 local or metastatic recurrences
of breast cancer or new primary cancers in the contralateral breast —
75 in the letrozole group and 132 in the placebo group — with estimated
four-year disease-free survival rates of 93 percent and 87 percent,
respectively, in the two groups (P = 0.00008 for the comparison of
disease-free survival).
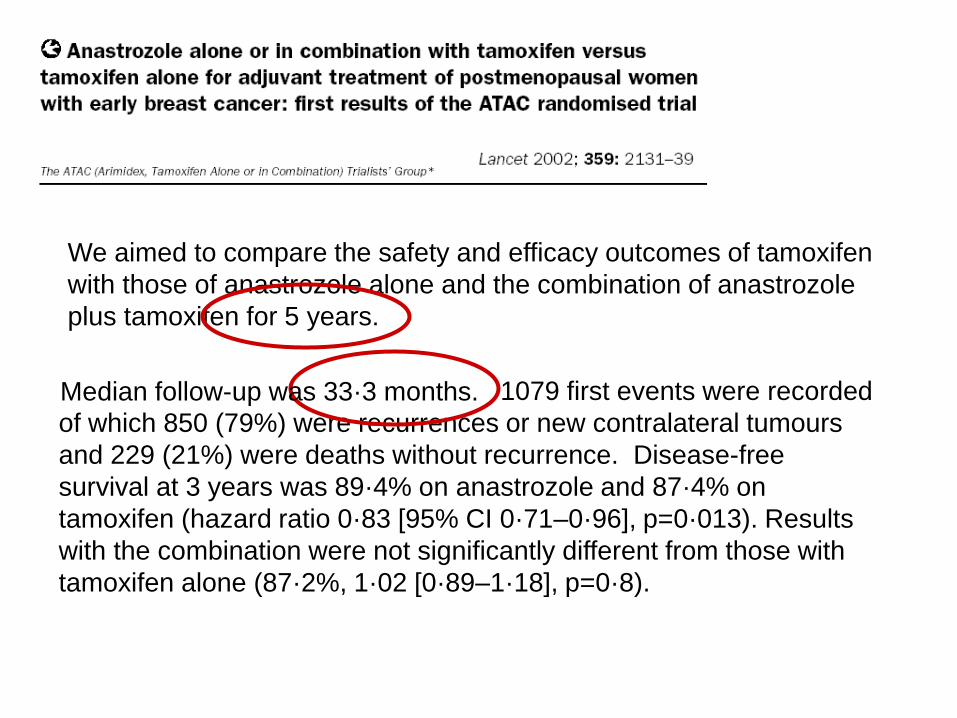
We aimed to compare the safety and efficacy outcomes of tamoxifen
with those of anastrozole alone and the combination of anastrozole
plus tamoxifen for 5 years.
1079 first events were recorded
of which 850 (79%) were recurrences or new contralateral tumours
and 229 (21%) were deaths without recurrence. Disease-free
survival at 3 years was 89·4% on anastrozole and 87·4% on
tamoxifen (hazard ratio 0·83 [95% CI 0·71–0·96], p=0·013). Results
with the combination were not significantly different from those with
tamoxifen alone (87·2%, 1·02 [0·89–1·18], p=0·8).
Median follow-up was 33·3 months.
Paolo Chiodini – Parma AIOM – 19 Giugno 2015
SINTESI (revisioni sistematiche)
Paolo Chiodini – Parma AIOM – 19 Giugno 2015
“It is surely a great criticism of our profession that we have not organised a critical summary, by specialty or subspecialty, adapted periodically, of all relevant randomised controlled trials.” (Archie Cochrane, 1979)
ARCHIE COCHRANE
Paolo Chiodini – Parma AIOM – 19 Giugno 2015
3. Valutare criticamente le evidenze reperite per determinarne la validità e l’utilità
Come valutare la qualità degli studi?
Come sintetizzare le evidenze?
Come valutare l’efficacia e la sicurezza?
Come valutare l’eterogeneità fra gli studi?
LA SINTESI DELLE INFORMAZIONI
Paolo Chiodini – Parma AIOM – 19 Giugno 2015
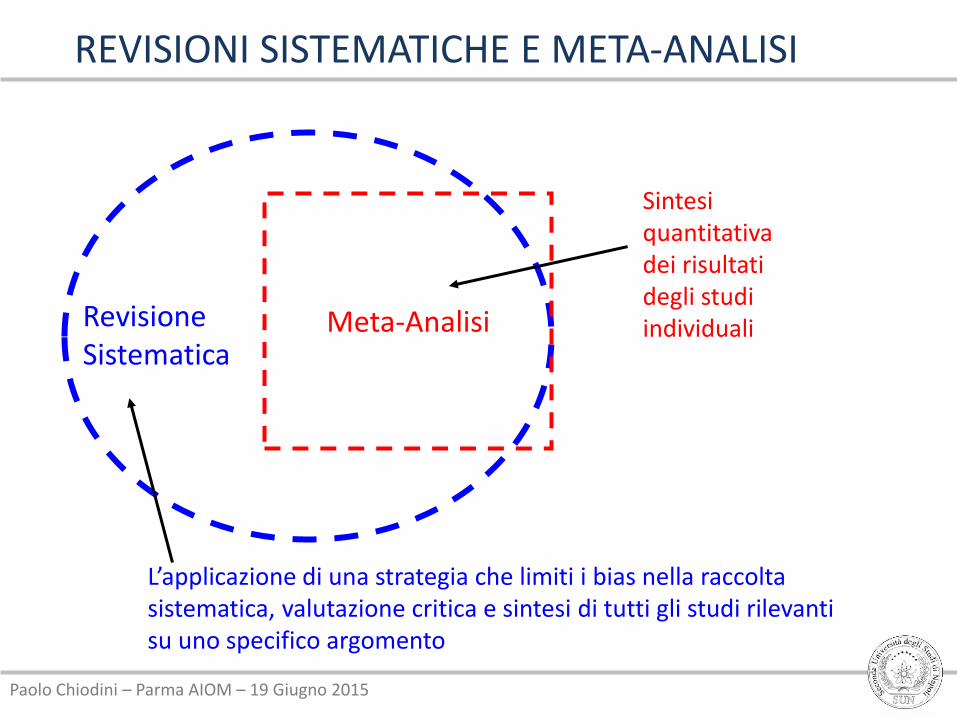
REVISIONI SISTEMATICHE E META-ANALISI
Meta-Analisi Revisione Sistematica
Sintesi quantitativa dei risultati degli studi individuali
L’applicazione di una strategia che limiti i bias nella raccolta sistematica, valutazione critica e sintesi di tutti gli studi rilevanti su uno specifico argomento
Paolo Chiodini – Parma AIOM – 19 Giugno 2015
dipende dalla selezione degli studi valutati
dipende dalla qualità degli studi primari
dipende dalla coerenza degli studi valutati
LE QUALITÀ DELLE REVISIONI SISTEMATICHE
… e soprattutto dei suoi risultati
Paolo Chiodini – Parma AIOM – 19 Giugno 2015
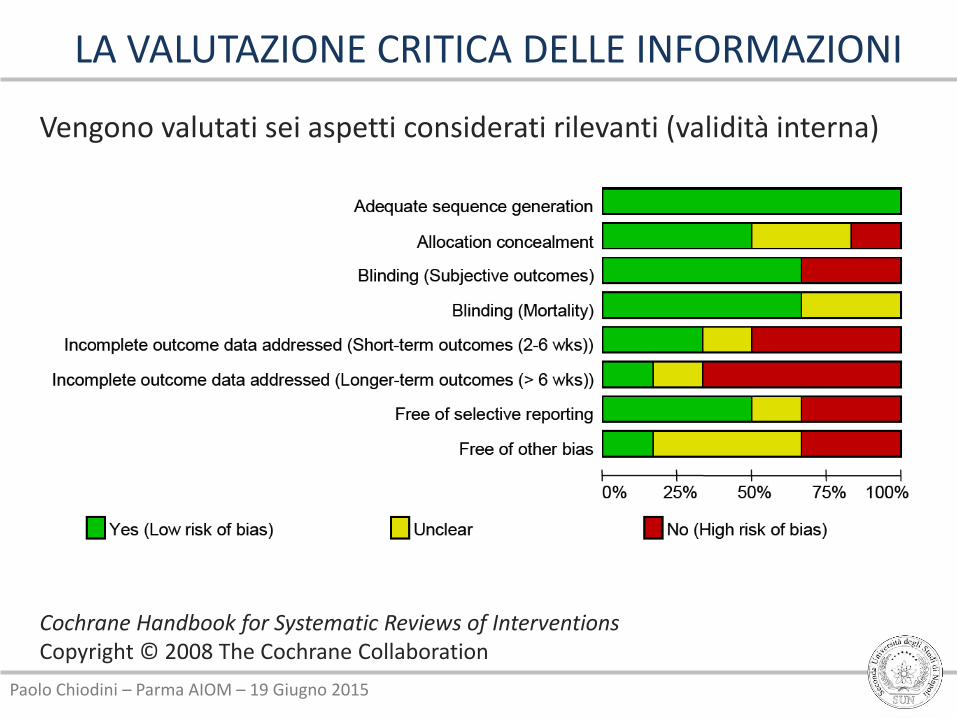
Cochrane Handbook for Systematic Reviews of Interventions Copyright © 2008 The Cochrane Collaboration
Vengono valutati sei aspetti considerati rilevanti (validità interna)
LA VALUTAZIONE CRITICA DELLE INFORMAZIONI
Paolo Chiodini – Parma AIOM – 19 Giugno 2015
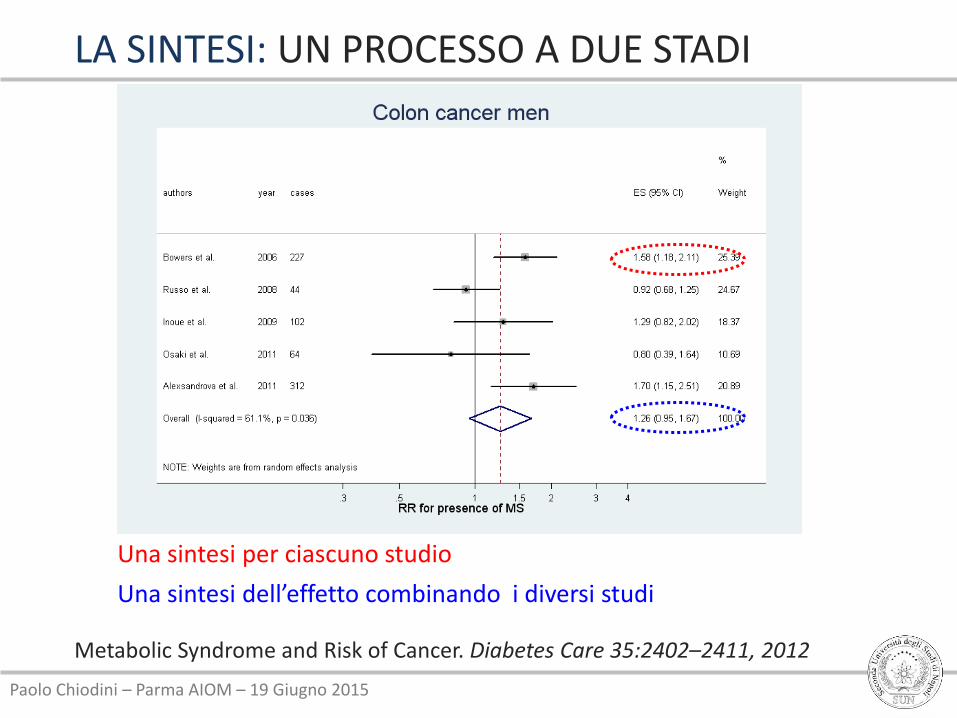
LA SINTESI: UN PROCESSO A DUE STADI
Una sintesi per ciascuno studio
Una sintesi dell’effetto combinando i diversi studi
Metabolic Syndrome and Risk of Cancer. Diabetes Care 35:2402–2411, 2012

Paolo Chiodini – Parma AIOM – 19 Giugno 2015
• Una certa variabilità tra le stime degli studi dovuta al campionamento è attesa
• Domanda: questa variabilità è consistente o più grande con quella attesa dovuta al campionamento?
• Cosa intendiamo con eterogeneità:
• I risultati degli studi hanno segno diverso (+ o -)
• I risultati degli studi sono nella stessa direzione, ma con differente grandezza
LA SINTESI: ETEROGENEITÀ
Paolo Chiodini – Parma AIOM – 19 Giugno 2015
ETEROGENEITÀ: COSA EVITARE?
Paolo Chiodini – Parma AIOM – 19 Giugno 2015
DATI MANCANTI (publication bias)

Paolo Chiodini – Parma AIOM – 19 Giugno 2015
PUBLICATION BIAS
Paolo Chiodini – Parma AIOM – 19 Giugno 2015
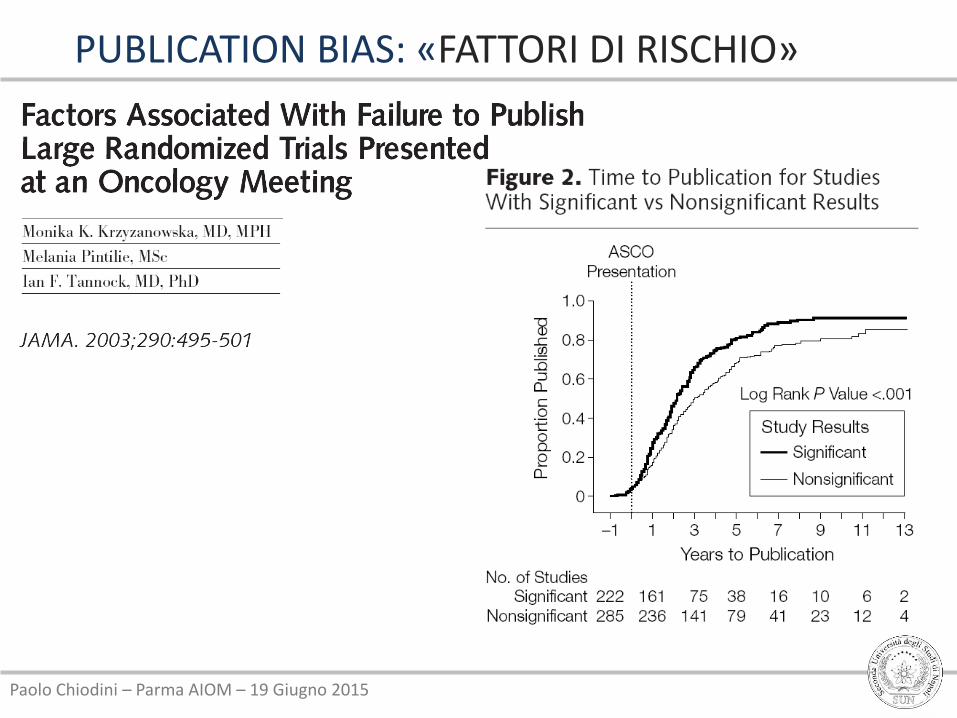
PUBLICATION BIAS: «FATTORI DI RISCHIO»
Paolo Chiodini – Parma AIOM – 19 Giugno 2015
SOPRAVVIVENZA E DIAGNOSI (lead time bias)

Paolo Chiodini – Parma AIOM – 19 Giugno 2015
La diagnosi precoce di malattia non modifica la
sopravvivenza (benefit time nullo)
B C D
B C D
I casi diagnosticati allo screening hanno una sopravvivenza più elevata anche in assenza di qualsiasi efficacia dell’intervento
LEAD TIME BIAS (ANTICIPAZIONE DIAGNOSTICA)

Paolo Chiodini – Parma AIOM – 19 Giugno 2015
DATI REGISTI TUMORI
Differenza di sopravvivenza di quasi il 10% a 5 anni
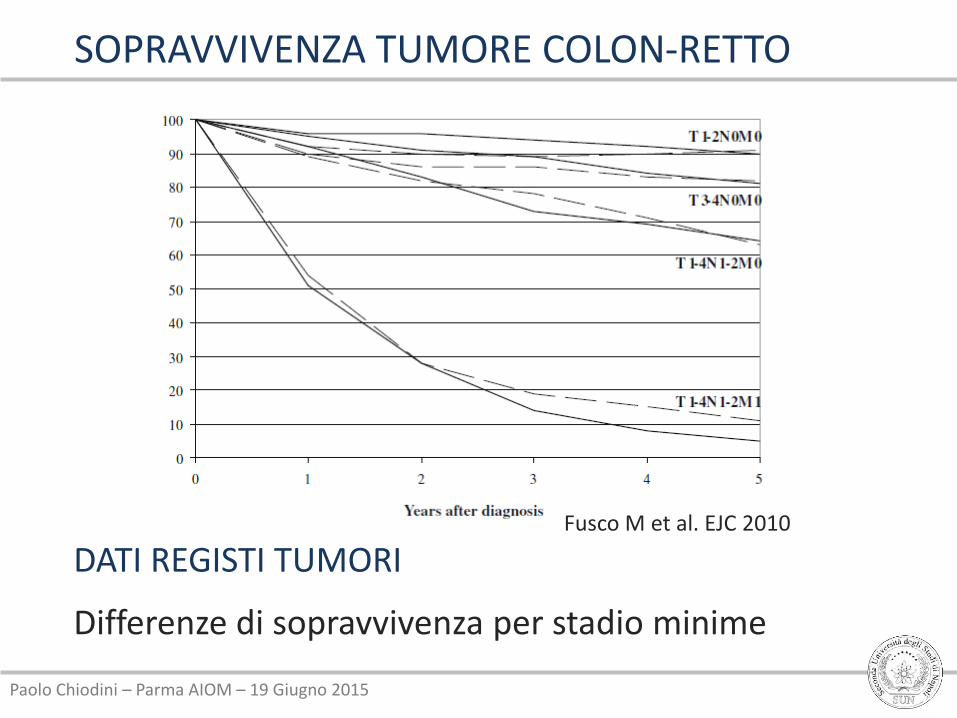
SOPRAVVIVENZA TUMORE COLON-RETTO
Fusco M et al. EJC 2010

Paolo Chiodini – Parma AIOM – 19 Giugno 2015
INCIDENZA TUMORE COLON-RETTO
Fusco M et al. EJC 2010
DATI REGISTI TUMORI
Maggiore incidenza a Modena dopo i 55 anni
Paolo Chiodini – Parma AIOM – 19 Giugno 2015
DATI REGISTI TUMORI
Differenze di sopravvivenza per stadio minime
SOPRAVVIVENZA TUMORE COLON-RETTO
Fusco M et al. EJC 2010
Paolo Chiodini – Parma AIOM – 19 Giugno 2015
SFORTUNA (caso e tumore)

Paolo Chiodini – Parma AIOM – 19 Giugno 2015
DAI DETERMINANTI DELLA SALUTE…
Paolo Chiodini – Parma AIOM – 19 Giugno 2015
…AL CASO
Paolo Chiodini – Parma AIOM – 19 Giugno 2015
...only a third of the variation in cancer
risk among tissues is attributable to
environmental factors or inherited
predispositions. The majority is due to
“bad luck,” that is, random mutations
arising during DNA replication in normal,
noncancerous stem cells.
Science 2 Jan 2015
Paolo Chiodini – Parma AIOM – 19 Giugno 2015
Science 13 Feb 2015
Epidemiologia & Prevenzione Marzo-aprile 2015
Paolo Chiodini – Parma AIOM – 19 Giugno 2015
LA RICERCA CHE NON SERVE
New York Times, 27 April 1997