Le linee guida Sincope 2018 della Società Europea di ...tigulliocardio.com/2018/Ungar.pdf · –...
28
Andrea Ungar, MD, PhD, FESC Syncope Unit, Hypertension Centre Geriatric and Intensive care Medicine University of Florence, Italy Le linee guida Sincope 2018 della Società Europea di Cardiologia La Syncope Unit Multidisciplinare
Transcript of Le linee guida Sincope 2018 della Società Europea di ...tigulliocardio.com/2018/Ungar.pdf · –...
Andrea Ungar, MD, PhD, FESC
Syncope Unit, Hypertension CentreGeriatric and Intensive care Medicine
University of Florence, Italy
Le linee guida Sincope 2018 della Società Europea di Cardiologia
La Syncope Unit Multidisciplinare

www.escardio.org/guidelines2
NEW / REVISED CLINICAL SETTINGS AND TESTS:• Tilt testing: concepts of hypotensive
susceptibility• Increased role of prolonged ECG monitoring• Video recording in suspected syncope• “Syncope without prodrome, normal ECG and
normal heart” (adenosine sensitive syncope)• Neurological causes: “ictal asystole”
NEW / REVISED INDICATIONS FOR TREATMENT:• Reflex syncope: algorithms for selection of
appropriate therapy based on age, severity of syncope and clinical forms• Reflex syncope: algorithms for selection of
best candidates for pacemaker therapy• Patients at risk of SCD: definition of
unexplained syncope and indication for ICD• Implantable loop recorder as alternative to
ICD, in selected cases
(OUT-PATIENT) SYNCOPE MANAGEMENT UNIT:• Structure: staff, equipment, and procedures• Tests and assessments• Access and referrals• Role of the Clinical Nurse Specialist• Outcome and quality indicators
MANAGEMENT IN EMERGENCY DEPARTMENT:• List of low-risk and high-risk features• Risk stratification flowchart• Management in ED Observation Unit and/or fast-track to Syncope Unit • Restricted admission criteria• Limited usefulness of risk stratification scores
2018NEW/REVISED
CONCEPTSin management
of syncope


www.escardio.org/guidelines
Organizational aspects: Syncope Unit
�The syncope unit should take the lead in service delivery for syncope, and in education and training of healthcare professionals who encounter syncope.
�The syncope unit should be led by a clinician with specific knowledge of TLOC and additional necessary team members (i.e. clinical nurse specialist) depending on the local model of service delivery.
4
Key components - 1
2018 ESC Guidelines on Syncope – Michele brignole & Angel MoyaEHJ Doi:10.1093/eurheartj/ehy037

www.escardio.org/guidelines
Organizational aspects: Syncope Unit
� The syncope unit should provide minimum core treatments for reflex syncope and OH, and treatments or preferential access for cardiac syncope, falls, psychogenic pseudosyncope, and epilepsy.
� Referrals should be directly from family practitioners, EDs, in-hospital and out-hospital services, or self-referral depending on the risk stratification of referrals. Fast-track access, with a separate waiting list and scheduled follow-up visits, should be recommended.
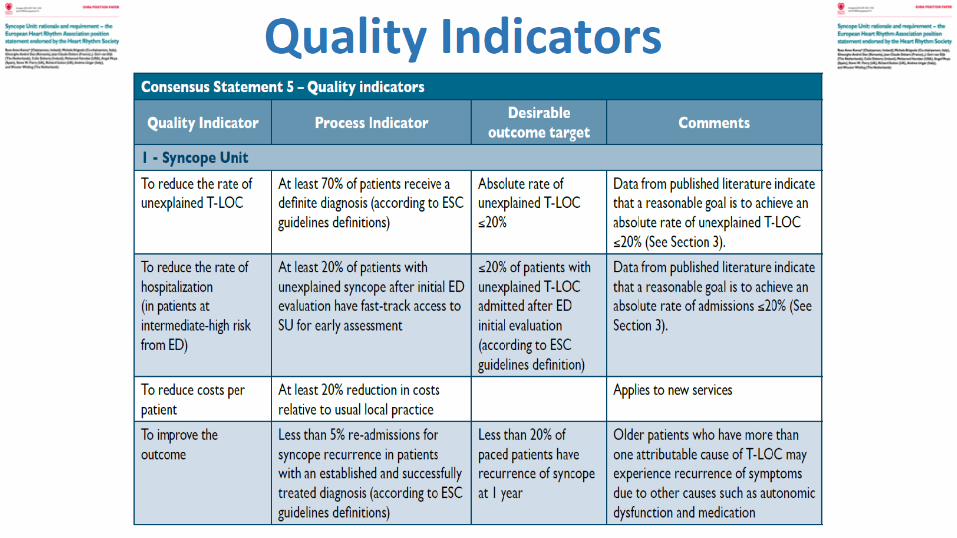
� Syncope units should employ quality indicators, process indicators, and desirable outcome targets.
5
Key components - 2
2018 ESC Guidelines on Syncope – Michele brignole & Angel MoyaEHJ Doi:10.1093/eurheartj/ehy037

www.escardio.org/guidelines
Staffing of an SU is composed of:1. One or more physicians of any specialty who are syncope specialists.2. A team comprised of professionals who will advance the care of
syncope patients.Equipment:
1. Essential Equipment/tests:– 12-lead ECG and 3-lead ECG monitoring,– non-invasive beat-to-beat blood pressure monitor,– tilt-table,– Holter monitors,– external loop recorders,– follow-up of implantable loop recorders (*),– 24-hour blood pressure monitoring,– Basic autonomic function tests.
2018 ESC Guidelines on Syncope – Michele brignole & Angel MoyaEHJ Doi:10.1093/eurheartj/ehy037
Organizational aspects: Structure of the SU
6
2. Established procedures for:– Echocardiography– Electrophysiological
studies– Stress test– Neuroimaging tests
3. Specialists’ consultancies (cardiology, neurology, internal medicine, geriatric,psychology), when needed
www.escardio.org/guidelines
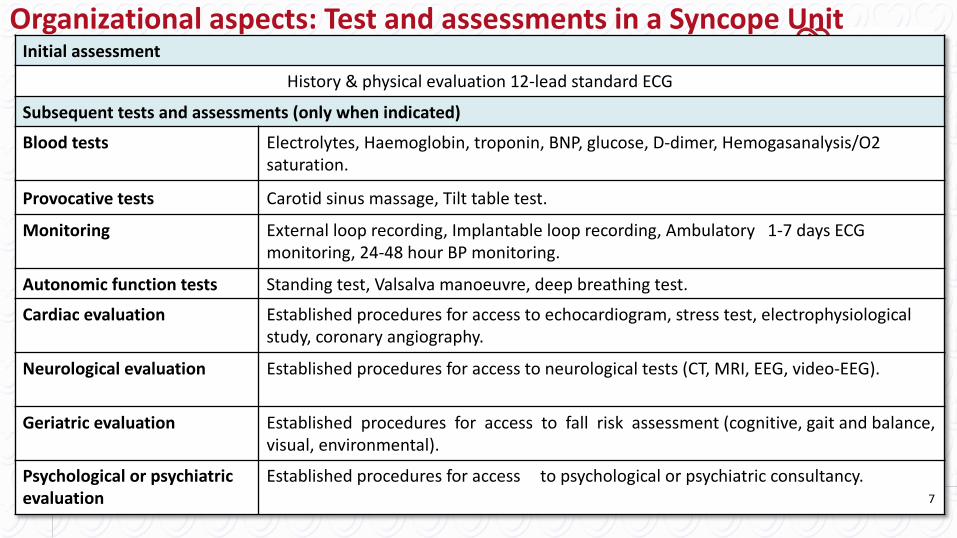
Initial assessment
History & physical evaluation 12-lead standard ECG
Subsequent tests and assessments (only when indicated)
Blood tests Electrolytes, Haemoglobin, troponin, BNP, glucose, D-dimer, Hemogasanalysis/O2 saturation.
Provocative tests Carotid sinus massage, Tilt table test.
Monitoring External loop recording, Implantable loop recording, Ambulatory 1-7 days ECG monitoring, 24-48 hour BP monitoring.
Autonomic function tests Standing test, Valsalva manoeuvre, deep breathing test.Cardiac evaluation Established procedures for access to echocardiogram, stress test, electrophysiological
study, coronary angiography.
Neurological evaluation Established procedures for access to neurological tests (CT, MRI, EEG, video-EEG).
Geriatric evaluation Established procedures for access to fall risk assessment (cognitive, gait and balance, visual, environmental).
Psychological or psychiatric evaluation
Established procedures for access to psychological or psychiatric consultancy.
Organizational aspects: Test and assessments in a Syncope Unit
7

www.escardio.org/guidelines9
Procedure or test SUPhysician
SU Staff Non-SU personnel
History taking xStructured history taking (e.g., application of software technologies) x12-lead ECG xBlood tests xEchocardiogram and imaging xCarotid sinus massage xActive standing test xTilt table test (x) xBasic autonomic function test xECG monitoring (Holter, ELR): administration and interpretation x xImplantable loop recorder x (x)Remote monitoring xOthers: stress test, electrophysiological study, angiograms xNeurological tests (CT, MRI, EEG, video-EEG) xPacemaker and ICD implantation, catheter ablation xPatient’s education, biofeedback training. and instructions x x
Final report and clinic note xCommunication with patients, referring physicians x xFollow-up x x
Organizational aspects: Role of physician and staff in a SU
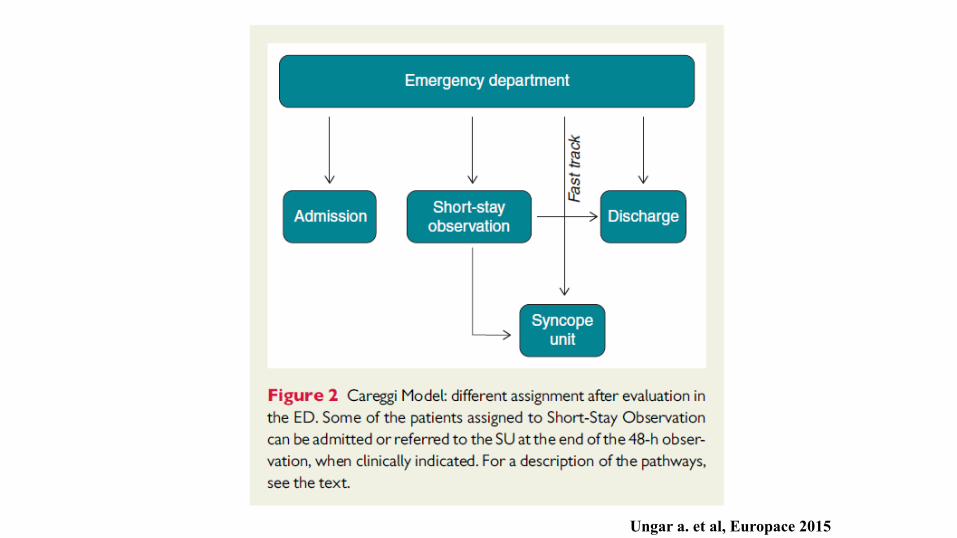
Ungar a. et al, Europace 2015

Assessment of a novel management pathway for patients referred to the Emergency Department for
syncope: results in a Tertiary Hospital
(Careggi Hospital - Florence, Italy)
Ungar a et al, 2015
ED295 patients
Admitted85 pz(29%)
Short stay60 pt(20%)
Syncope UnitFast Track
58 pt(21%)
Discharded92 pt(31%)

Ungar a et al, 2015

Destination related to ED “suspected” diagnosis
SYNCOPE Admission
n=85
Short – stay observation
n=60
SyncopeUnit
n=58
Discharge
n=80
Refusal
n=12
Cardiac 17 (60.7*) 5 (17.9*) 3 (10.7*) 0 3 (10.7*)
Neurally-mediate 13 (10,1*) 26 (20.2*) 20 (15.5*) 67 (51.9*) 3 (2.3*)
Pseudosyncope 11 (39.3*) 9 (32.1*) 2 (7.1*) 3 (10.7*) 3(10.7*)
Unexplained 44 (40.0*) 20 (18.2*) 33 (30.0*) 10 (9.1*) 3 (2.7*)
* % destination related to the diagnosis Ungar a et al, 2015

0.1
.2.3
.4.5
0 5 10 15Months of follow-up
Ricovero OBIFast Track NienteRifiuta
Estimated hospital re-admission according to multivariable Cox model-destino
New admissions related to ED destination
1 month
12 months
Ungar a et al, 2015
Admitted
Refusal
Discharged
Short stay obs
Syncope Unit

Ungar a et al, 2015
No patients sent to Syncope Unit
was dead within one year
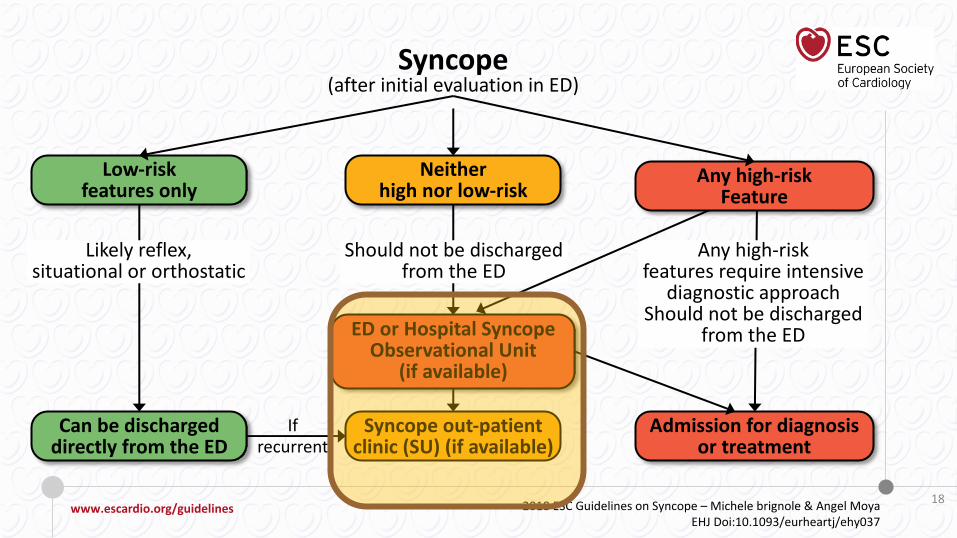
www.escardio.org/guidelines
Should not be discharged
from the ED
Any high-risk
features require intensive
diagnostic approach
Should not be discharged
from the ED
Low-riskfeatures only
Can be dischargeddirectly from the ED
Neitherhigh nor low-risk
Syncope out-patientclinic (SU) (if available)
ED or Hospital SyncopeObservational Unit
(if available)
Any high-riskFeature
Admission for diagnosisor treatment
Syncope(after initial evaluation in ED)
Likely reflex,
situational or orthostatic
If
recurrent
2018 ESC Guidelines on Syncope – Michele brignole & Angel Moya
EHJ Doi:10.1093/eurheartj/ehy037
18





2015
Syncope Unit: 69
20092011
2013
GIMSI - Syncope Unit Ceritication
www.gimsi.it
Syncope Unit: 21 Syncope Unit: 47 Syncope Unit: 71
2017
Syncope Unit: 73

57
67
21
Geriatrics
Internal Medicine
Emergency dptNeurology
Cardiology
GIMSI 2017 Certificated Syncope Unit(Total = 73)
www.gimsi.it



Grazie per l’attenzione
Le linee guida Sincope 2018 della Società Europea di Cardiologia
La Syncope Unit Multidisciplinare