LE COMPLICANZE OSSEE DEI TRATTAMENTI … Metabolismo Minerale 2 PTH SANGUE PTH Ca - P Ca - P CT ....
50
LE COMPLICANZE OSSEE DEI LE COMPLICANZE OSSEE DEI TRATTAMENTI FARMACOLOGICI TRATTAMENTI FARMACOLOGICI ADIUVANTI ADIUVANTI LE COMPLICANZE OSSEE DEI LE COMPLICANZE OSSEE DEI TRATTAMENTI FARMACOLOGICI TRATTAMENTI FARMACOLOGICI ADIUVANTI ADIUVANTI ADIUVANTI ADIUVANTI ADIUVANTI ADIUVANTI G.C. Isaia G.C. Isaia Torino, 10 Torino, 10 Giugno 2014 Giugno 2014 A.O.U. A.O.U. CITTA CITTA’ DELLA SALUTE E DELLA SCIENZA DI TORINO ’ DELLA SALUTE E DELLA SCIENZA DI TORINO S.C. GERIATRIA E MALATTIE METABOLICHE DELL’OSSO S.C. GERIATRIA E MALATTIE METABOLICHE DELL’OSSO Centro di Riferimento Regionale per le Malattie Metaboliche dell’osso Centro di Riferimento Regionale per le Malattie Metaboliche dell’osso
Transcript of LE COMPLICANZE OSSEE DEI TRATTAMENTI … Metabolismo Minerale 2 PTH SANGUE PTH Ca - P Ca - P CT ....

LE COMPLICANZE OSSEE DEI LE COMPLICANZE OSSEE DEI TRATTAMENTI FARMACOLOGICI TRATTAMENTI FARMACOLOGICI
ADIUVANTIADIUVANTI
LE COMPLICANZE OSSEE DEI LE COMPLICANZE OSSEE DEI TRATTAMENTI FARMACOLOGICI TRATTAMENTI FARMACOLOGICI
ADIUVANTIADIUVANTITRATTAMENTI FARMACOLOGICI TRATTAMENTI FARMACOLOGICI
ADIUVANTIADIUVANTITRATTAMENTI FARMACOLOGICI TRATTAMENTI FARMACOLOGICI
ADIUVANTIADIUVANTI
G.C. Isaia G.C. Isaia
Torino, 10 Torino, 10 Giugno 2014Giugno 2014
A.O.U.A.O.U. CITTACITTA’ DELLA SALUTE E DELLA SCIENZA DI TORINO ’ DELLA SALUTE E DELLA SCIENZA DI TORINO S.C. GERIATRIA E MALATTIE METABOLICHE DELL’OSSO S.C. GERIATRIA E MALATTIE METABOLICHE DELL’OSSO Centro di Riferimento Regionale per le Malattie Metaboliche dell’ossoCentro di Riferimento Regionale per le Malattie Metaboliche dell’osso

Dichiarazione di conflitto di interessiDichiarazione di conflitto di interessi
Aziende Farmaceutiche che hanno erogato finanziamenti per
ricerca,formazione, sperimentazioni o consulenze (2012-2014)
- Eli Lilly
- Nycomed
- Amgen
- Abiogen- Abiogen
- Novartis
- Sigma Tau
- Servier Italia
- IFB Stroeder
- Merck Sharp Dhome
- SPA Società Prodotti Antibiotici
- Italfarmaco
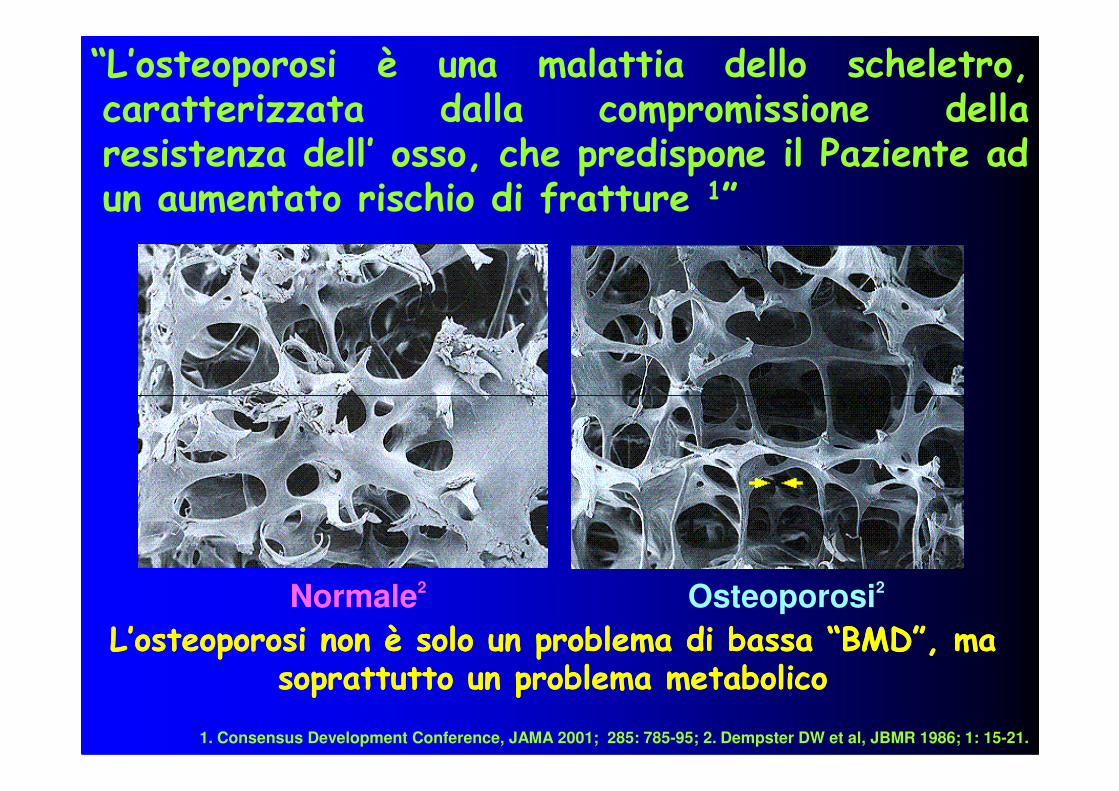
“L’osteoporosi è una malattia dello scheletro,caratterizzata dalla compromissione dellaresistenza dell’ osso, che predispone il Paziente adun aumentato rischio di fratture 1”
Normale2 Osteoporosi2
1. Consensus Development Conference, JAMA 2001; 285: 785-95; 2. Dempster DW et al, JBMR 1986; 1: 15-21.
L’osteoporosi non è solo un problema di bassa “BMD”, ma L’osteoporosi non è solo un problema di bassa “BMD”, ma soprattutto un problema metabolico soprattutto un problema metabolico
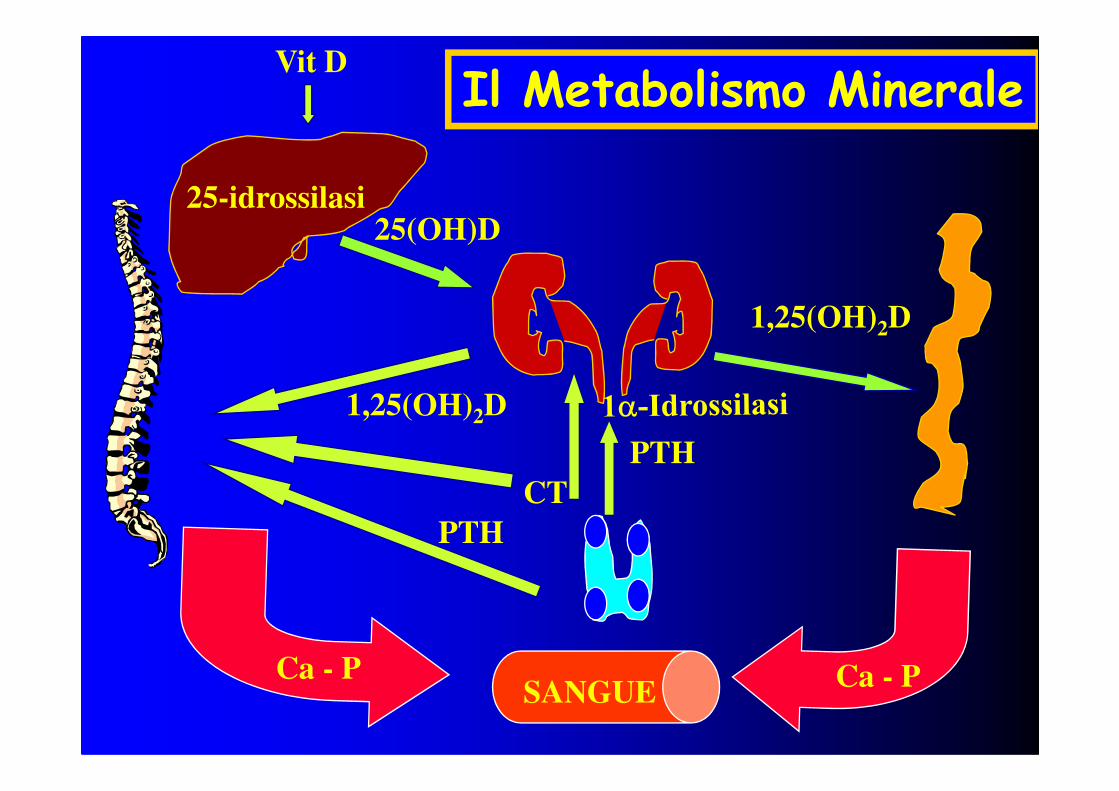
Vit D
25-idrossilasi
1,25(OH) D
25(OH)D
1,25(OH)2D
Il Metabolismo Minerale
1,25(OH)2D
PTH
SANGUE
PTH
Ca - P Ca - P
CT
Apoptosi
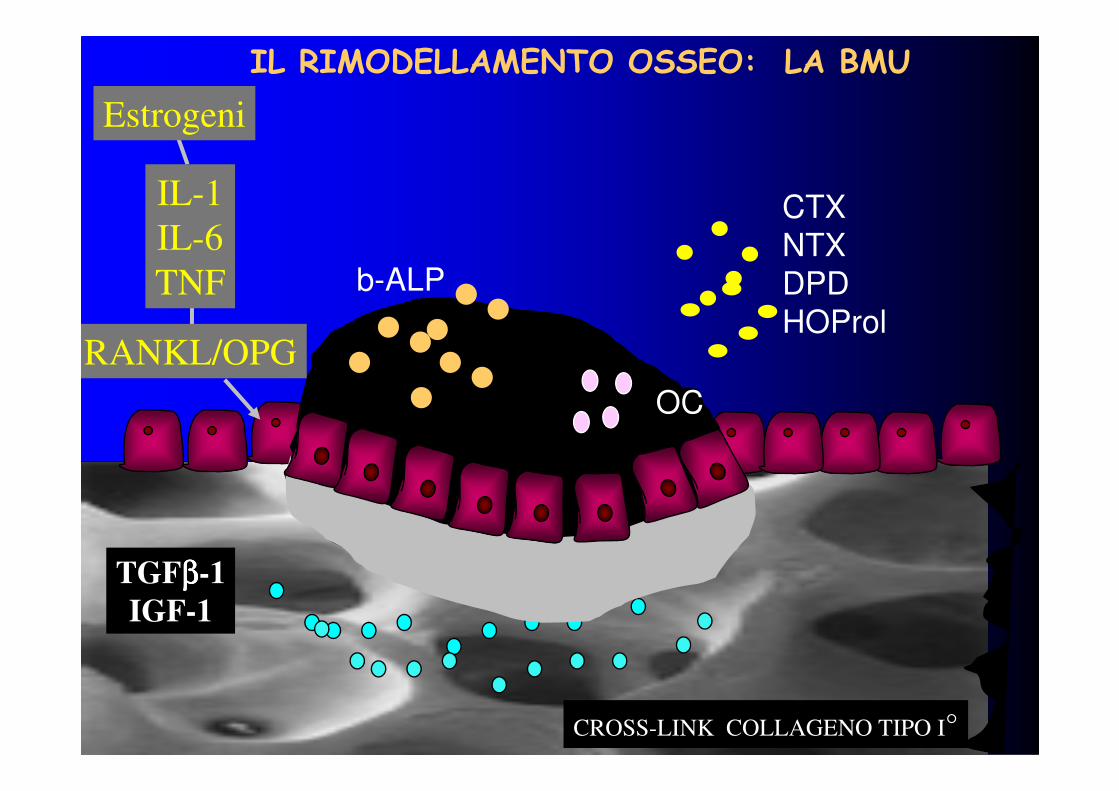
CTX
NTX
DPD
HOProl
b-ALP
OC
IL RIMODELLAMENTO OSSEO: LA BMU
Estrogeni
IL-1
IL-6
TNF
RANKL/OPG
TGFββββ-1
IGF-1
CROSS-LINK COLLAGENO TIPO I°
OC
• La maggiore sopravvivenza conseguente alle moderneterapie antitumorali conferisce una notevole rilevanzaagli effetti collaterali, immediati o tardivi, da essecausati, che spesso sono assai evidenti a livello osseo.
TESSUTO OSSEO E TERAPIE ANTITUMORALI
causati, che spesso sono assai evidenti a livello osseo.
•Gli studi prospettici sull’incidenza delle fratture inquesti pazienti sono difficilmente ottenibili a causadell’eterogeneità e della complessità dei protocolli(farmaci sostituiti ovvero discontinuati), della difficoltàdi ottenere popolazioni omogenee e numerose, deiproblemi etici frequentemente presenti.
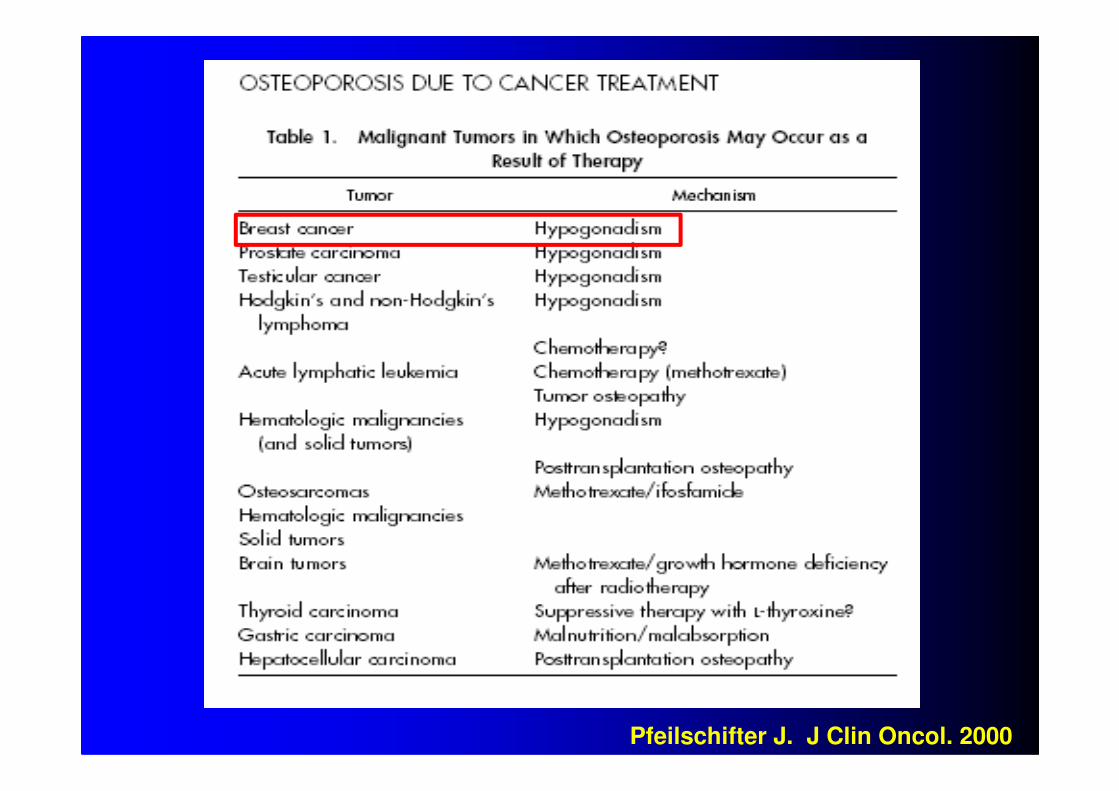
Pfeilschifter J. J Clin Oncol. 2000
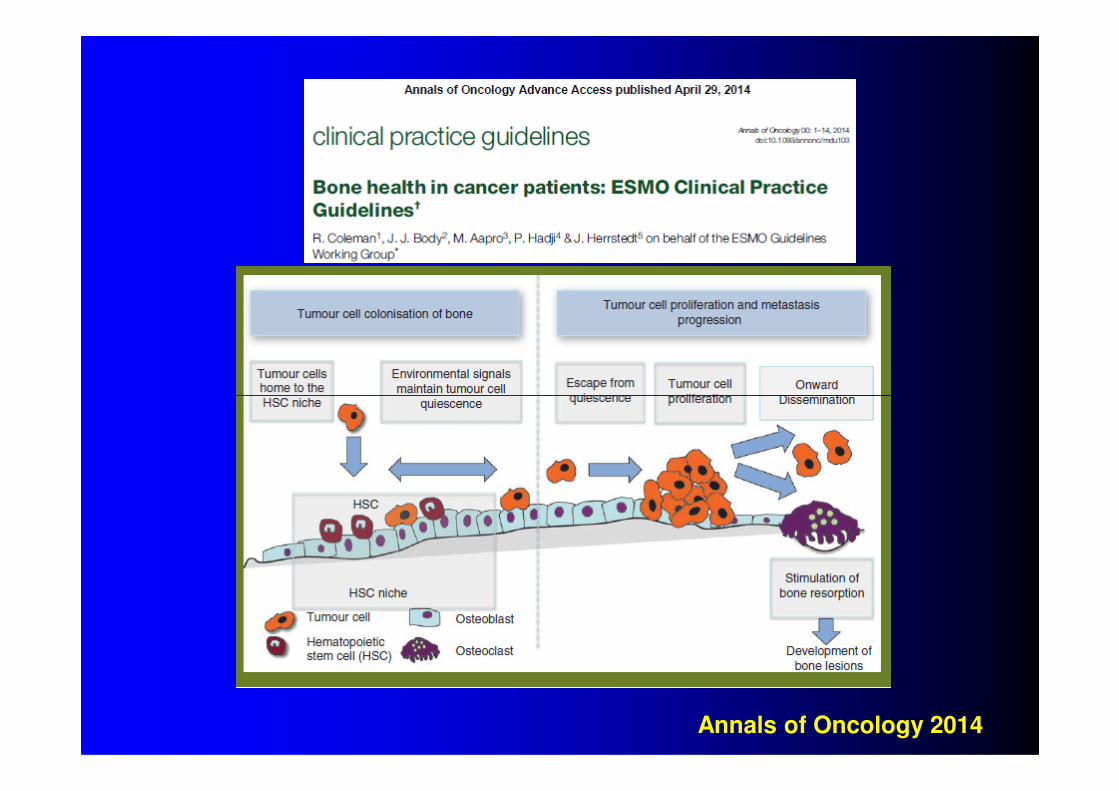
Annals of Oncology 2014
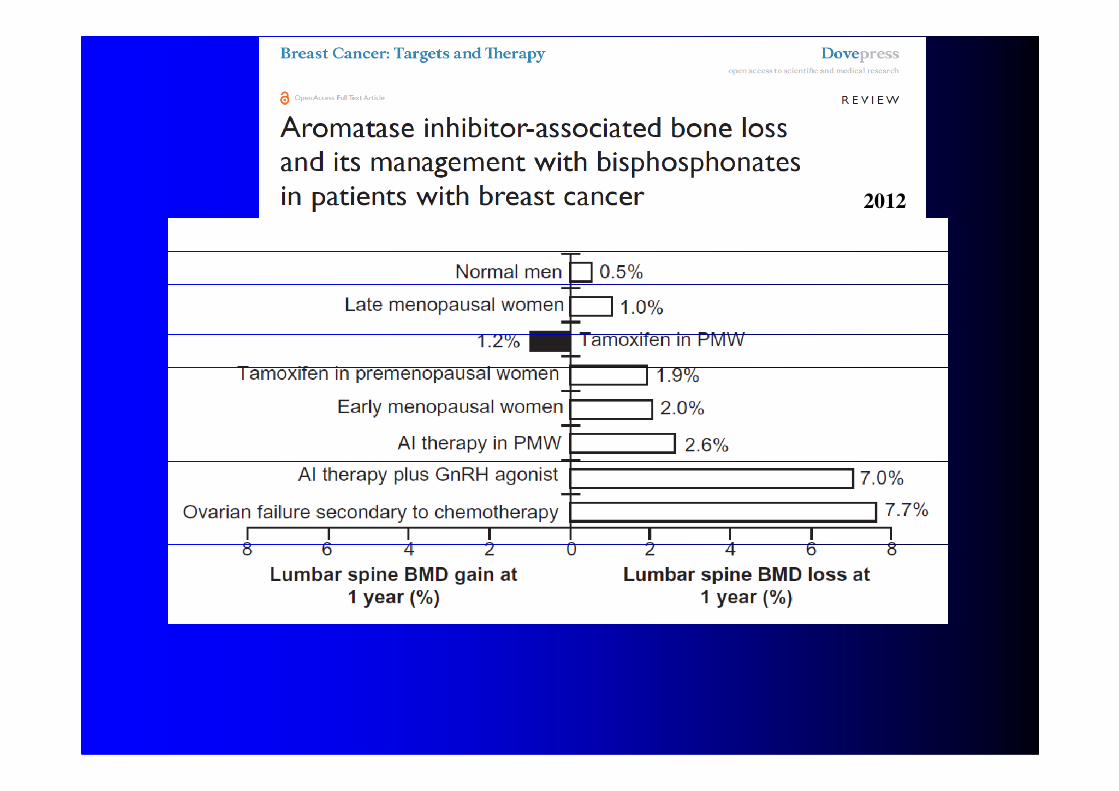
2012
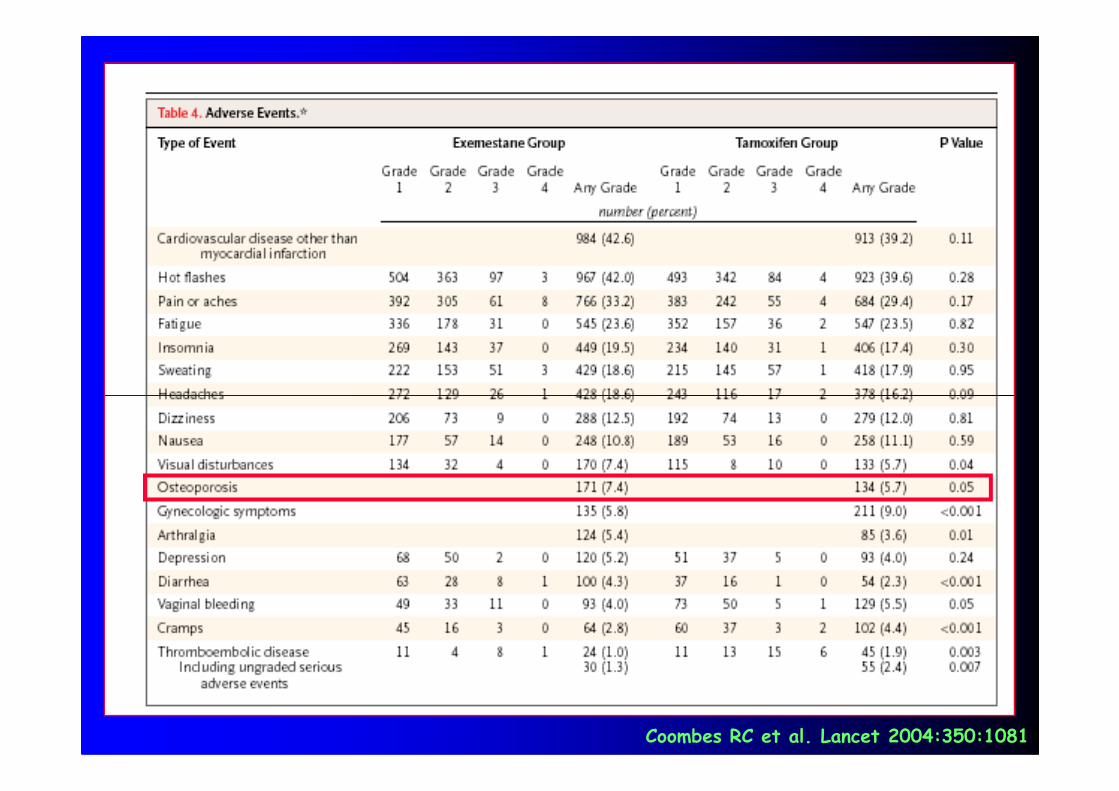
Coombes RC et al. Lancet 2004:350:1081
• Tamoxifene
• GnRH Agonisti
• Inibitori dell’aromatasi
CARCINOMA DELLA MAMMELLA TERAPIE SPECIFICHE AD EFFETTO SULL’OSSO
• Inibitori dell’aromatasi
• Tamoxifene
• GnRH Agonisti
• Inibitori dell’aromatasi
CARCINOMA DELLA MAMMELLA TERAPIE SPECIFICHE AD EFFETTO SULL’OSSO
• Inibitori dell’aromatasi
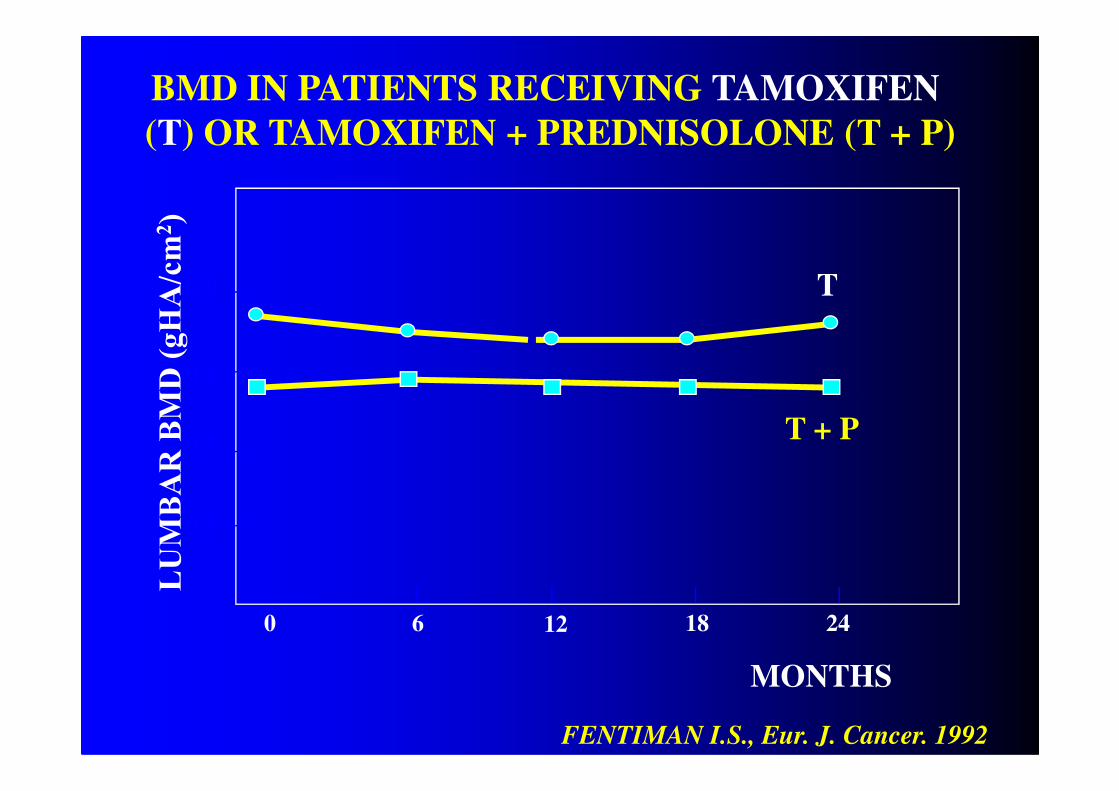
• Nelle donne in postmenopausa il trattamentocon Tamoxifene si associa ad un mantenimentodella densità minerale ossea a livello lombare.
TAMOXIFENE ED OSSO
della densità minerale ossea a livello lombare.• Resta da definire se questo effetto siaccompagni ad una riduzione del rischio difrattura.
N. Engl. J. Med. 1992; 326:852-856
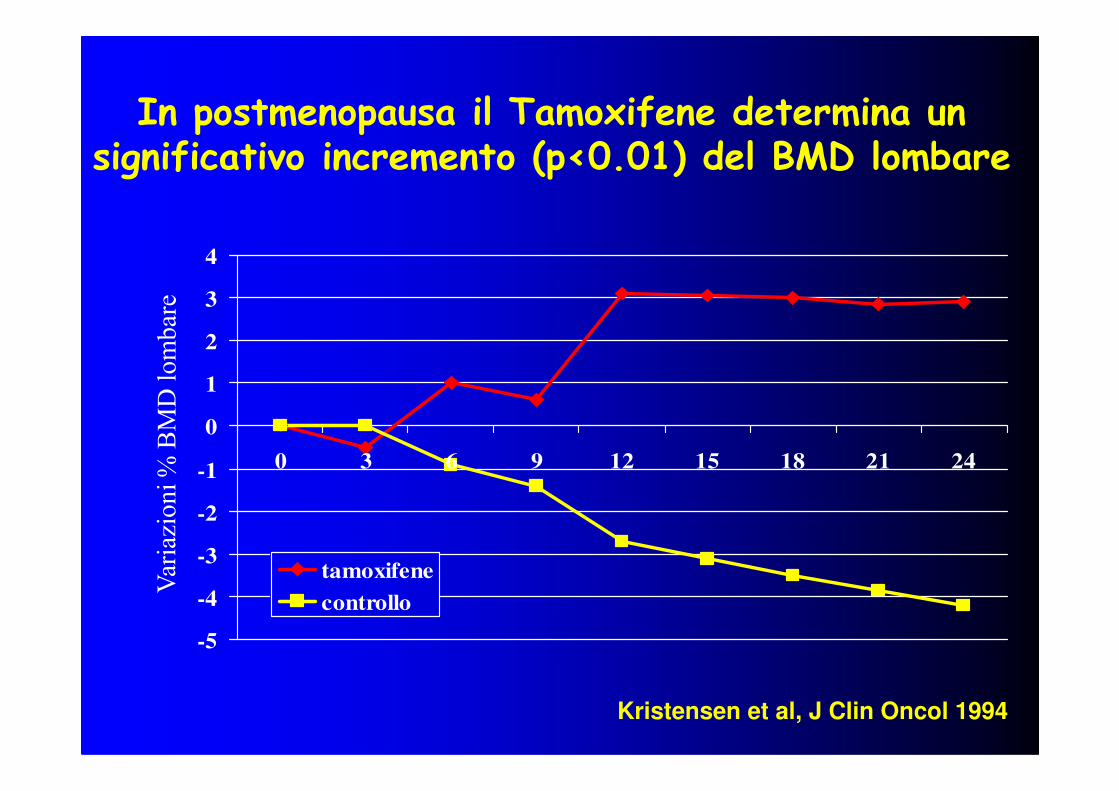
In postmenopausa il Tamoxifene determina un significativo incremento (p<0.01) del BMD lombare
1
2
3
4
-5
-4
-3
-2
-1
0
1
0 3 6 9 12 15 18 21 24
tamoxifene
controllo
Kristensen et al, J Clin Oncol 1994
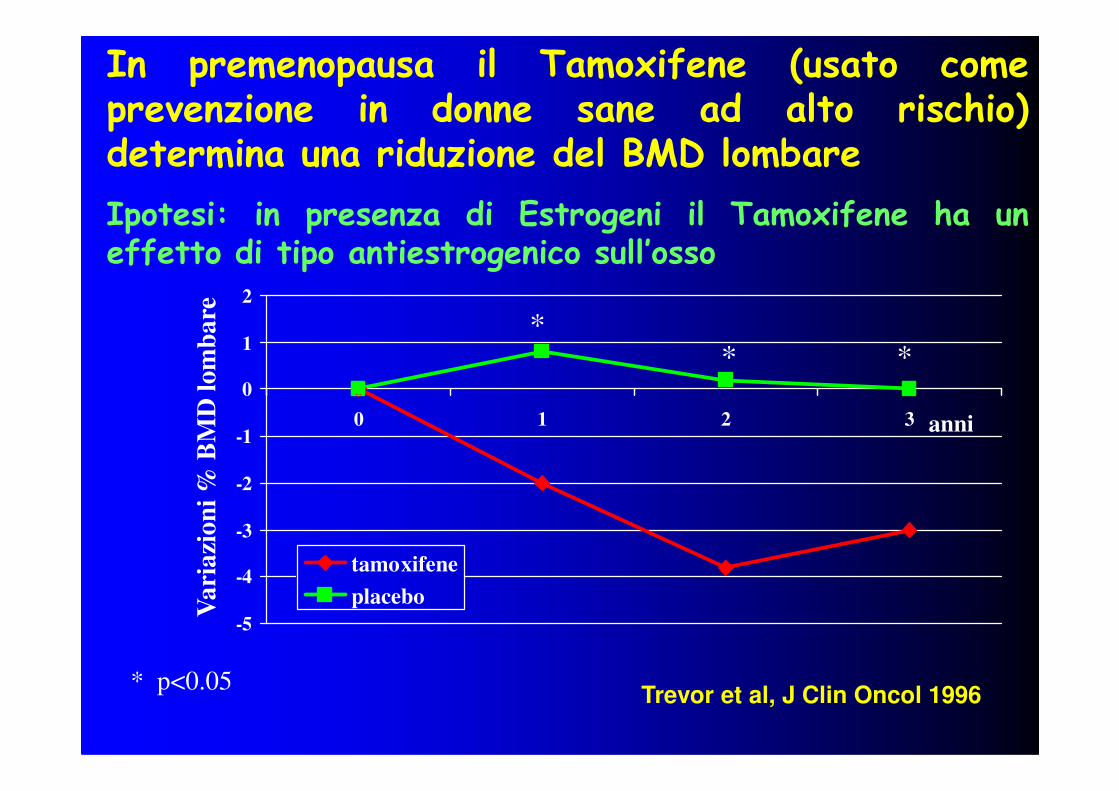
In premenopausa il Tamoxifene (usato comeprevenzione in donne sane ad alto rischio)determina una riduzione del BMD lombare
Ipotesi: in presenza di Estrogeni il Tamoxifene ha uneffetto di tipo antiestrogenico sull’osso
0
1
2
Va
ria
zio
ni
% B
MD
lo
mb
are
** *
-5
-4
-3
-2
-1
0
0 1 2 3
tamoxifene
placebo
Va
ria
zio
ni
% B
MD
lo
mb
are
Trevor et al, J Clin Oncol 1996
anni
* p<0.05
• Tamoxifene
• GnRH Agonisti
• Inibitori dell’aromatasi
CARCINOMA DELLA MAMMELLA TERAPIE SPECIFICHE AD EFFETTO SULL’OSSO
• Inibitori dell’aromatasi
Riduzione degli estrogeni circolanti
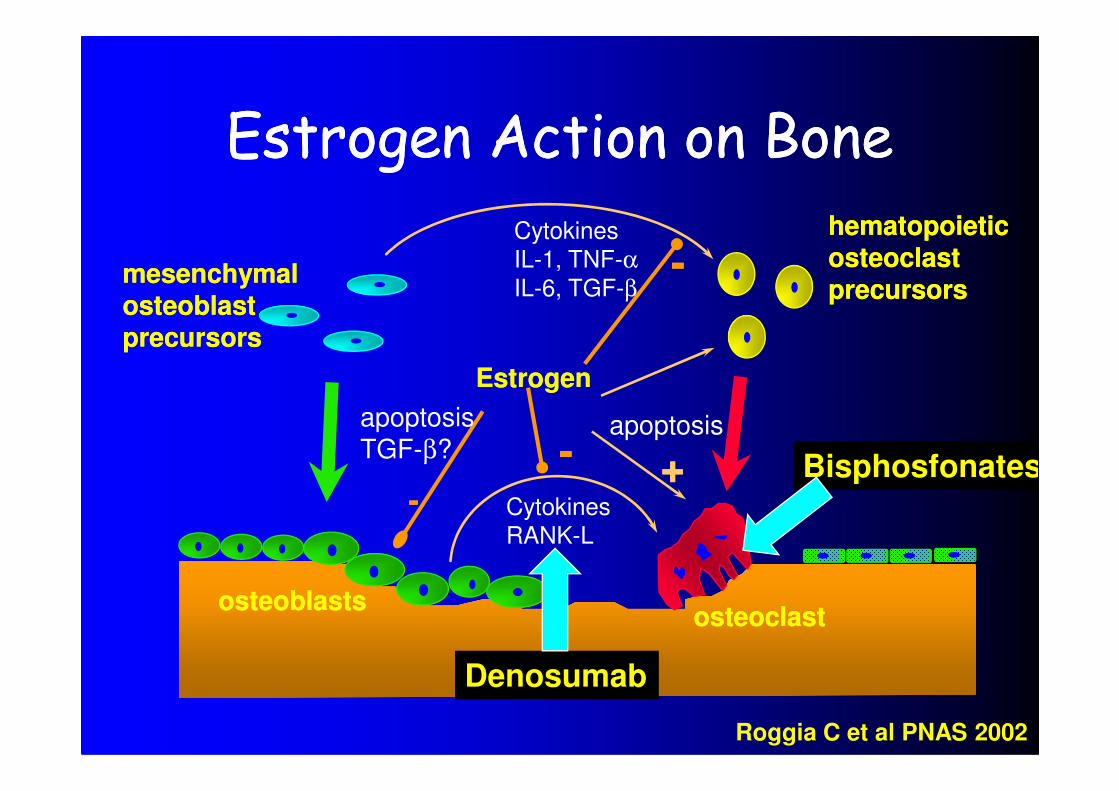
Estrogen Action on BoneEstrogen Action on Bone
EstrogenEstrogen
Cytokines
IL-1, TNF-αIL-6, TGF-β
--mesenchymalmesenchymalosteoblastosteoblastprecursorsprecursors
hematopoietichematopoieticosteoclastosteoclastprecursorsprecursors
Cytokines
RANK-L
--
apoptosisTGF-β? -- ++
apoptosis
osteoblastsosteoblastsosteoclastosteoclast
Roggia C et al PNAS 2002
Bisphosfonates
Denosumab
The RANKL/RANK/OPG Pathway is The RANKL/RANK/OPG Pathway is Involved in Regulating Bone RemodellingInvolved in Regulating Bone Remodelling
RANK Ligand (RANKL)
- Member of the TNF superfamily
– Signalling protein expressed by osteoblasts/bone lining cells
– Binds to RANK and promotes osteoclast formation, function and survival
RANKRANK
– Receptor expressed by osteoclasts and their precursors
– Activated by RANK Ligand binding
Osteoprotegerin (OPG)
– Protein secreted by osteoblasts/bone lining cells
– Natural inhibitor of RANK Ligand
– Blocks RANK Ligand signalling to balance bone remodelling
Kostenuik PJ. Curr Opin Pharmacol 2005;5:618-625; Boyle WJ, et al. Nature 2003;423:337-342;Kostenuik PJ, et al. Curr Pharm Des 2001;7:613-635.
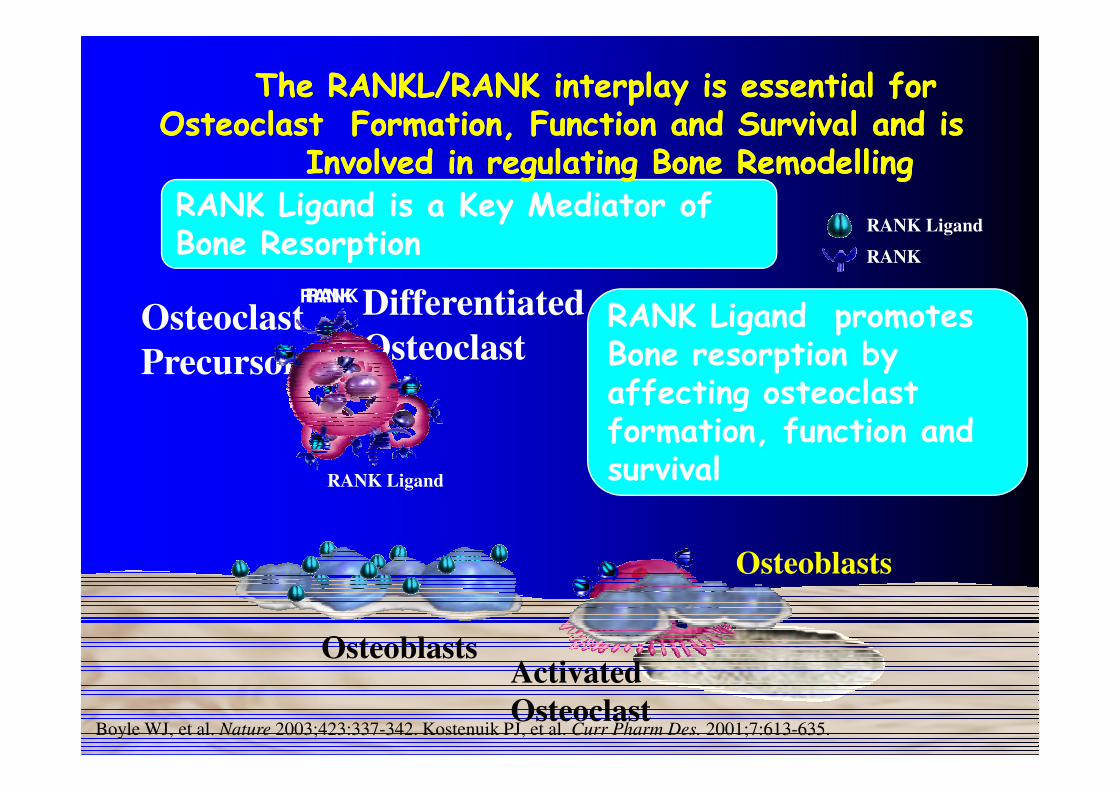
RANK Ligand is a Key Mediator of Bone Resorption
RANK Ligand
RANK
Differentiated
Osteoclast
The RANKL/RANK interplay is essential for The RANKL/RANK interplay is essential for OsteoclastOsteoclast Formation, Function and Survival and is Formation, Function and Survival and is
Involved in regulating Bone RemodellingInvolved in regulating Bone Remodelling
Osteoclast
Precursors
RANKRANK
RANK Ligand promotes Bone resorption by affecting osteoclast
Boyle WJ, et al. Nature 2003;423:337-342. Kostenuik PJ, et al. Curr Pharm Des. 2001;7:613-635.
Osteoblasts
Osteoblasts
RANK Ligand
Activated
Osteoclast
affecting osteoclast formation, function and survival
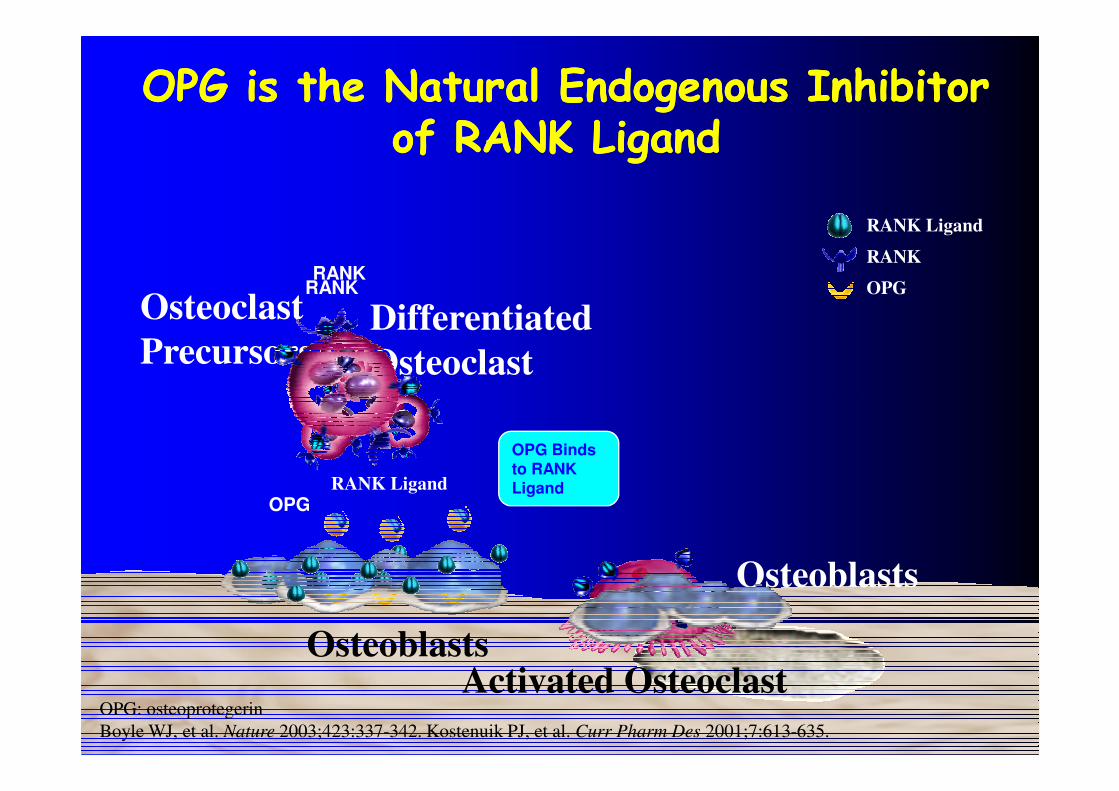
RANK Ligand
RANK
OPG
Differentiated
Osteoclast
OPG is the Natural Endogenous Inhibitor OPG is the Natural Endogenous Inhibitor of RANK Ligandof RANK Ligand
Osteoclast
Precursors
RANKRANK
OPG: osteoprotegerin
Boyle WJ, et al. Nature 2003;423:337-342. Kostenuik PJ, et al. Curr Pharm Des 2001;7:613-635.
Osteoblasts
OPG Binds to RANK Ligand
OPG
Osteoblasts
RANK Ligand
Activated Osteoclast
OsteoclastPrecursors
RANK Ligand
RANK
OPG
RANK
DifferentiatedOsteoclasts
RANK
Imbalanced Resorption
and Formation
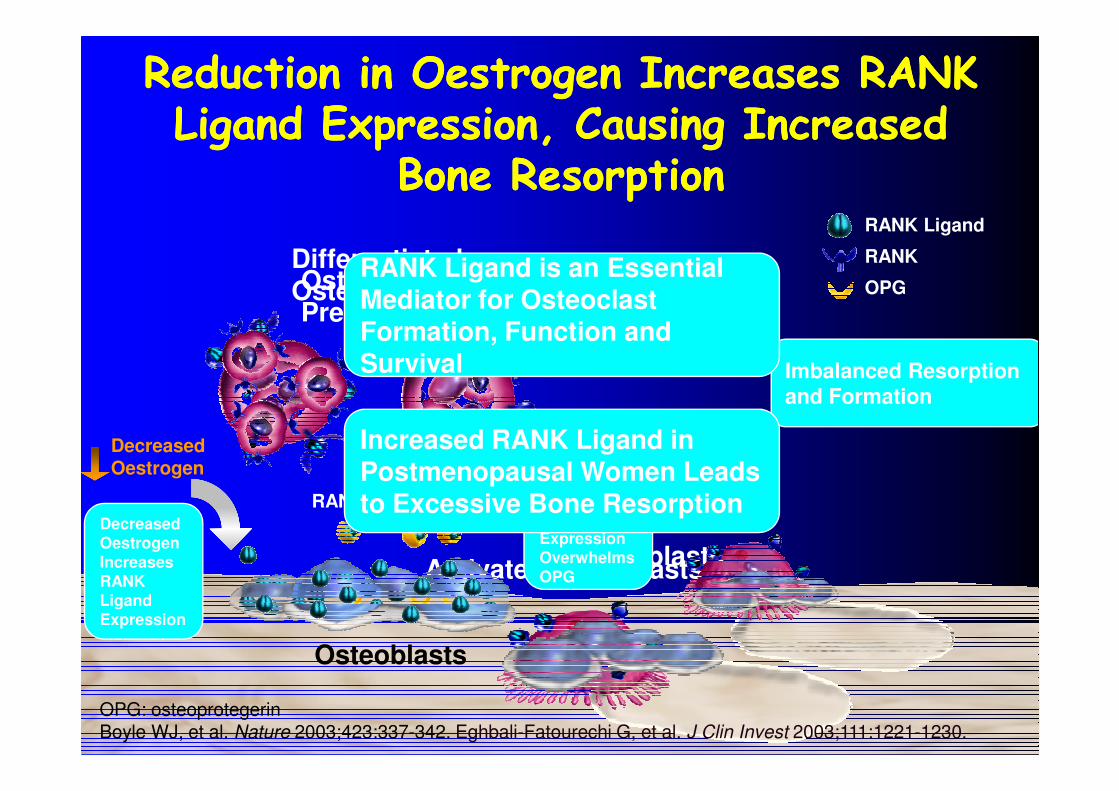
Reduction in Oestrogen Increases RANK Reduction in Oestrogen Increases RANK Ligand Expression, Causing Increased Ligand Expression, Causing Increased
Bone Bone ResorptionResorption
RANK Ligand is an Essential Mediator for Osteoclast Formation, Function and Survival
Activated Osteoclasts
RANK Ligand
Decreased Oestrogen
OPGDecreased Oestrogen Increases RANK Ligand Expression
Osteoblasts
Excess RANK LigandExpression Overwhelms OPG
Osteoblasts
and Formation
Increased RANK Ligand in Postmenopausal Women Leads to Excessive Bone Resorption
OPG: osteoprotegerinBoyle WJ, et al. Nature 2003;423:337-342. Eghbali-Fatourechi G, et al. J Clin Invest 2003;111:1221-1230.
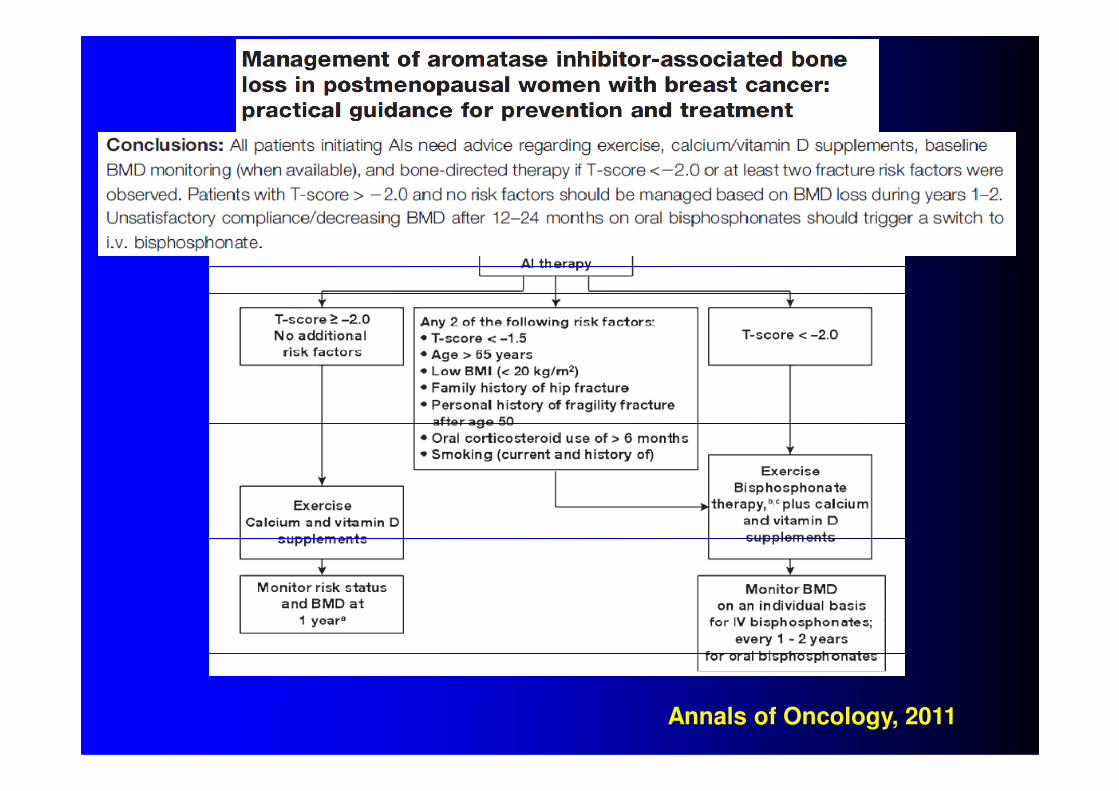
Annals of Oncology, 2011
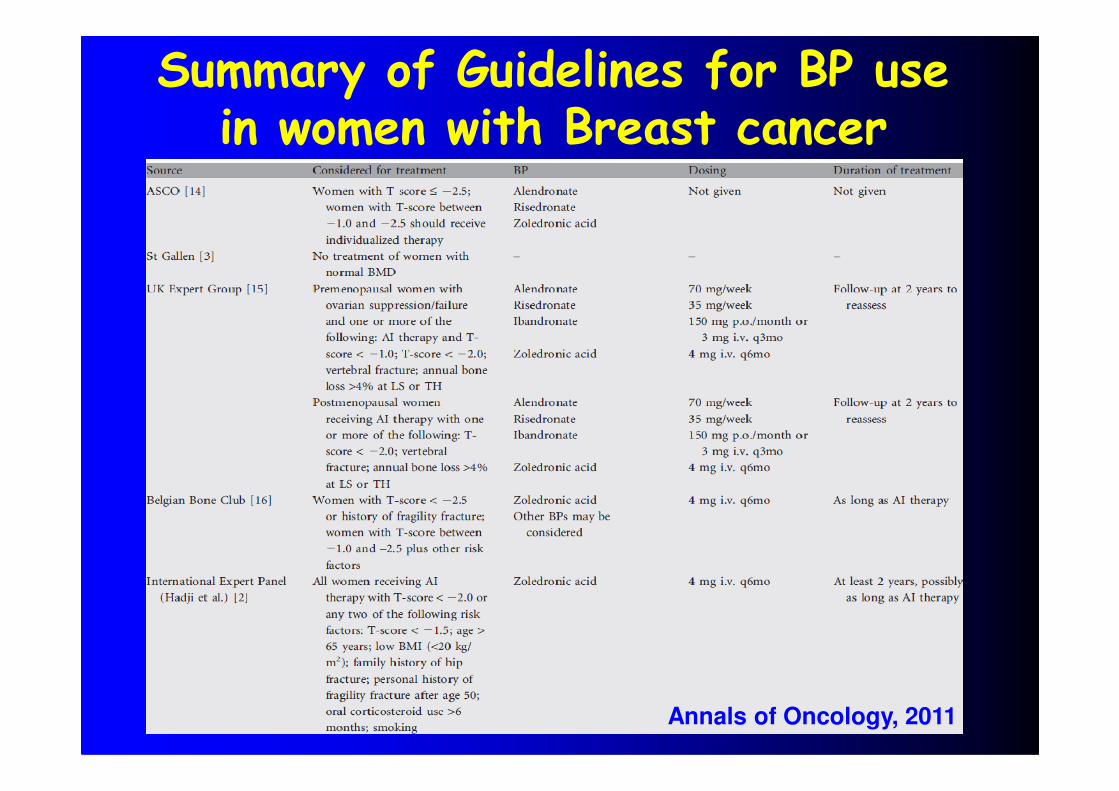
Summary of Guidelines for BP use in women with Breast cancer
Annals of Oncology, 2011
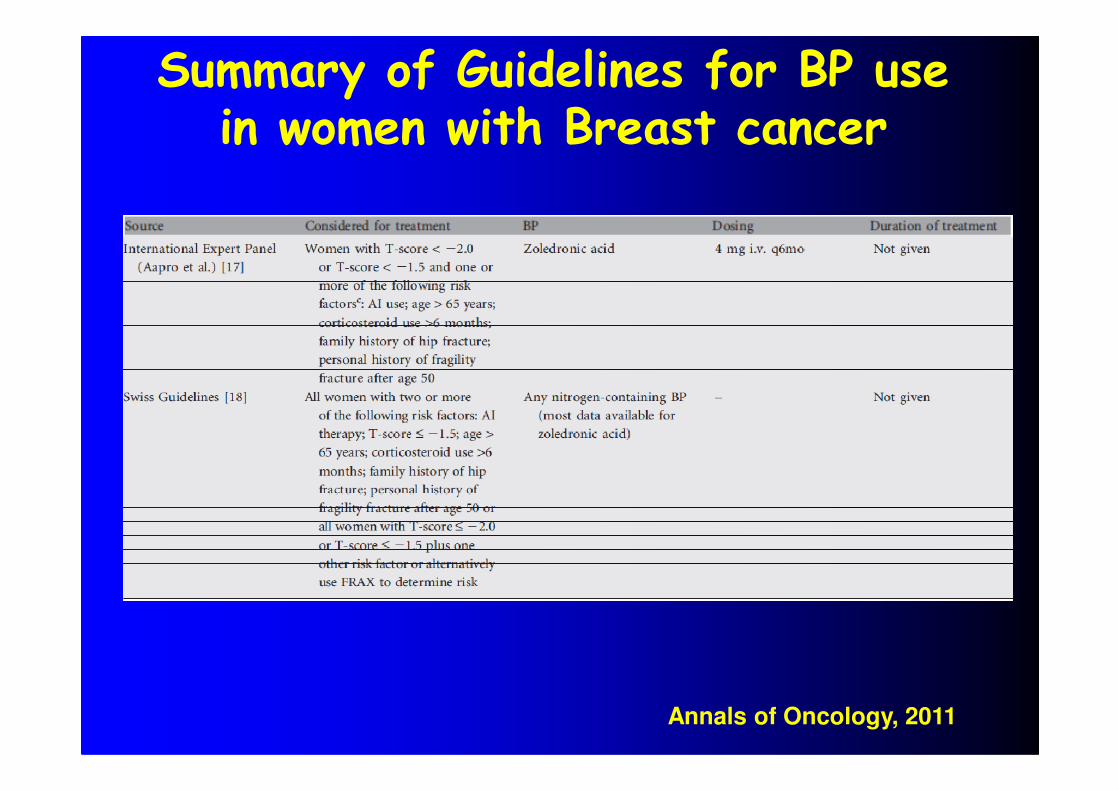
Summary of Guidelines for BP use in women with Breast cancer
Annals of Oncology, 2011
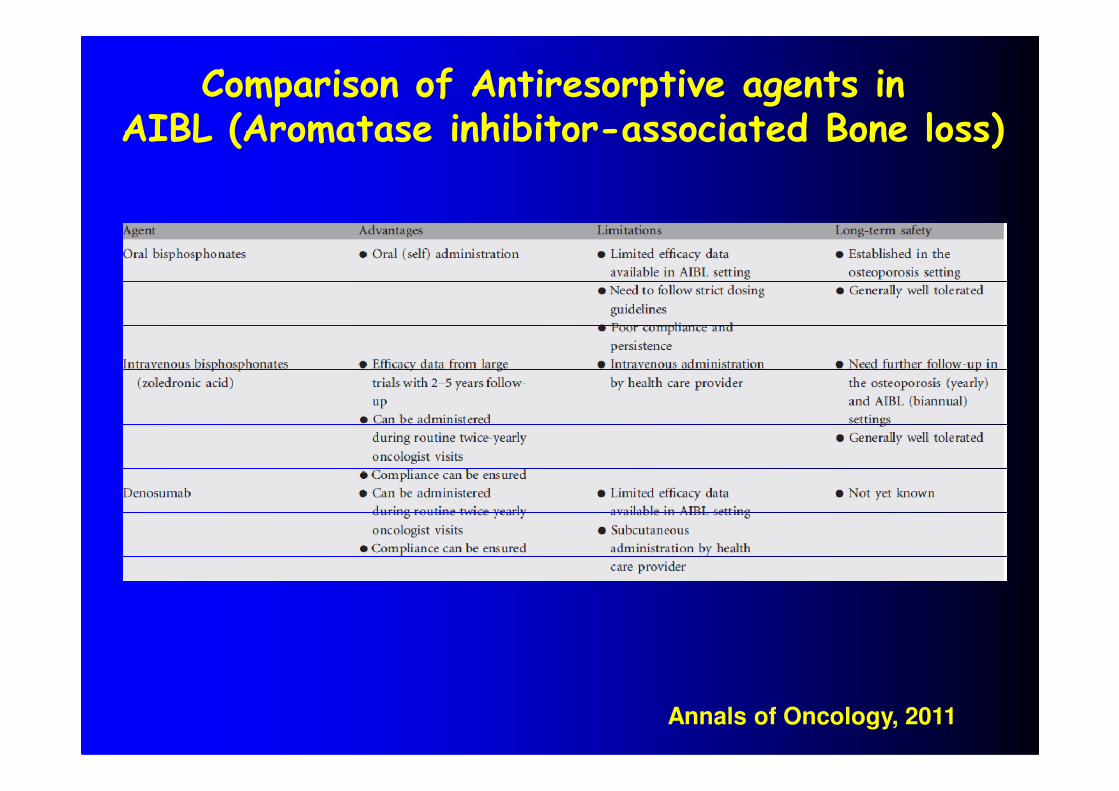
Comparison of Antiresorptive agents in AIBL (Aromatase inhibitor-associated Bone loss)
Annals of Oncology, 2011
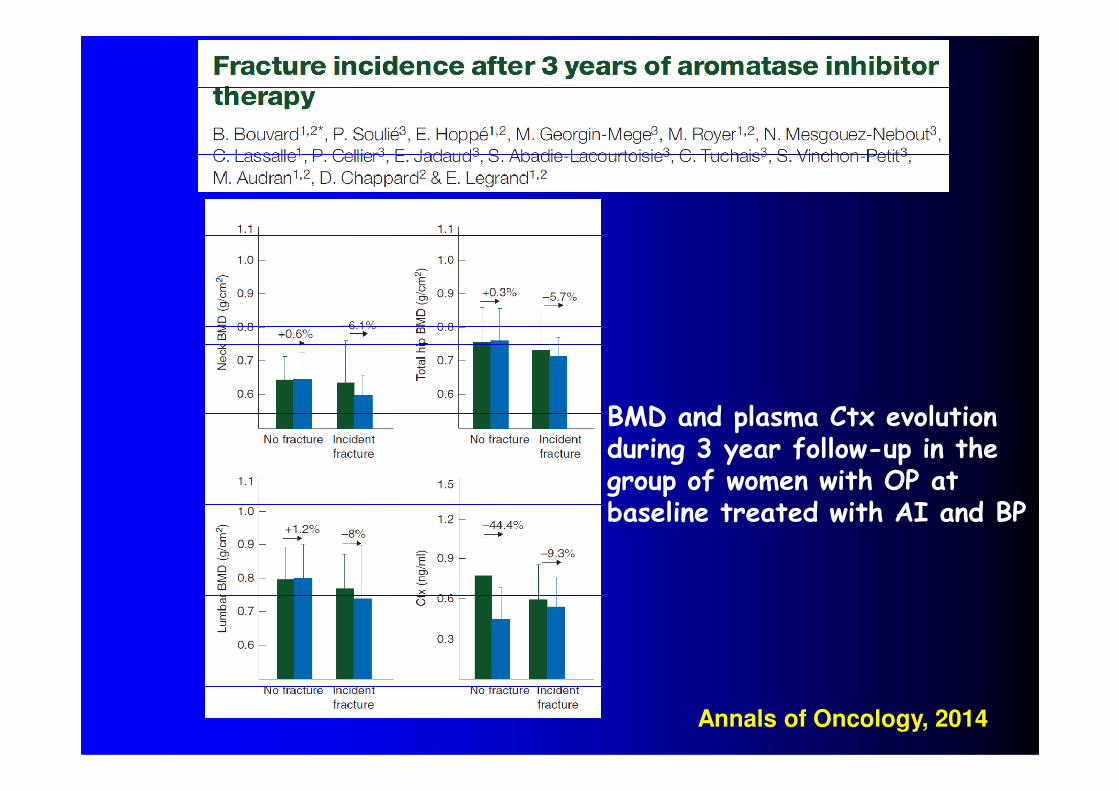
Annals of Oncology, 2014
BMD and plasma Ctx evolutionduring 3 year follow-up in the group of women with OP atbaseline treated with AI and BP
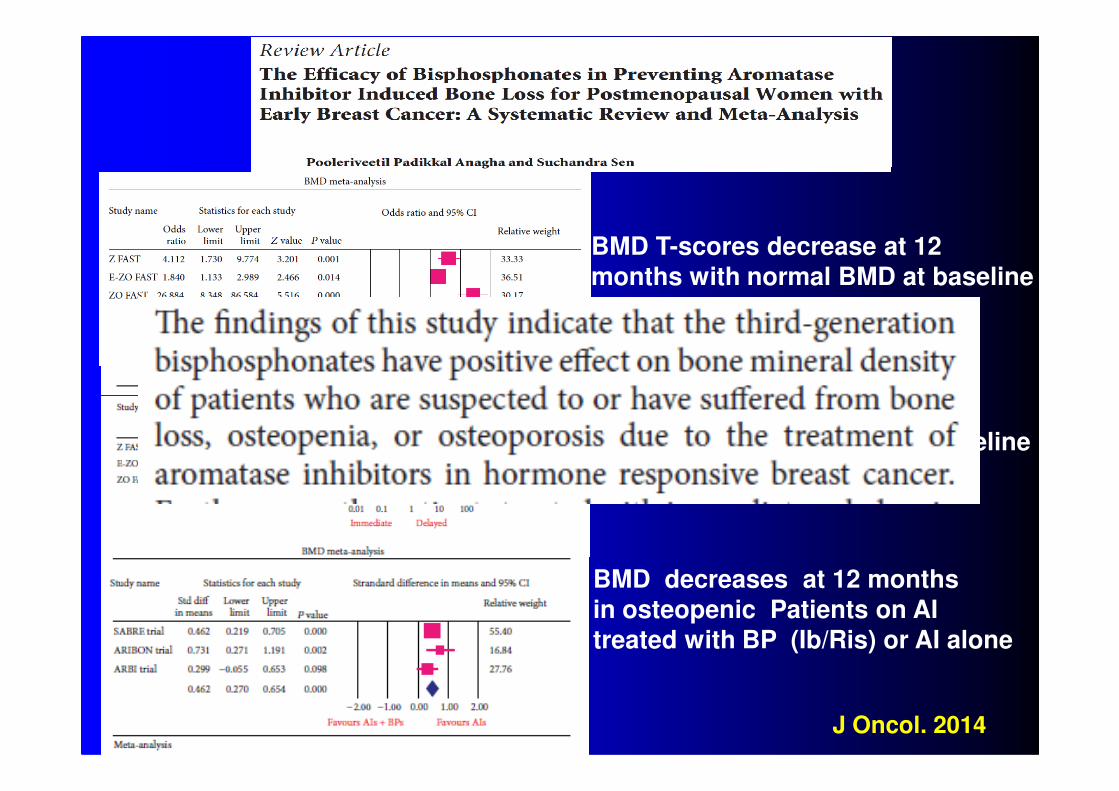
BMD T-scores decrease at 12
months with normal BMD at baseline
BMD T-scores decrease at 12
months with Osteopenia at baseline
BMD decreases at 12 months
in osteopenic Patients on AI
treated with BP (Ib/Ris) or AI alone
J Oncol. 2014
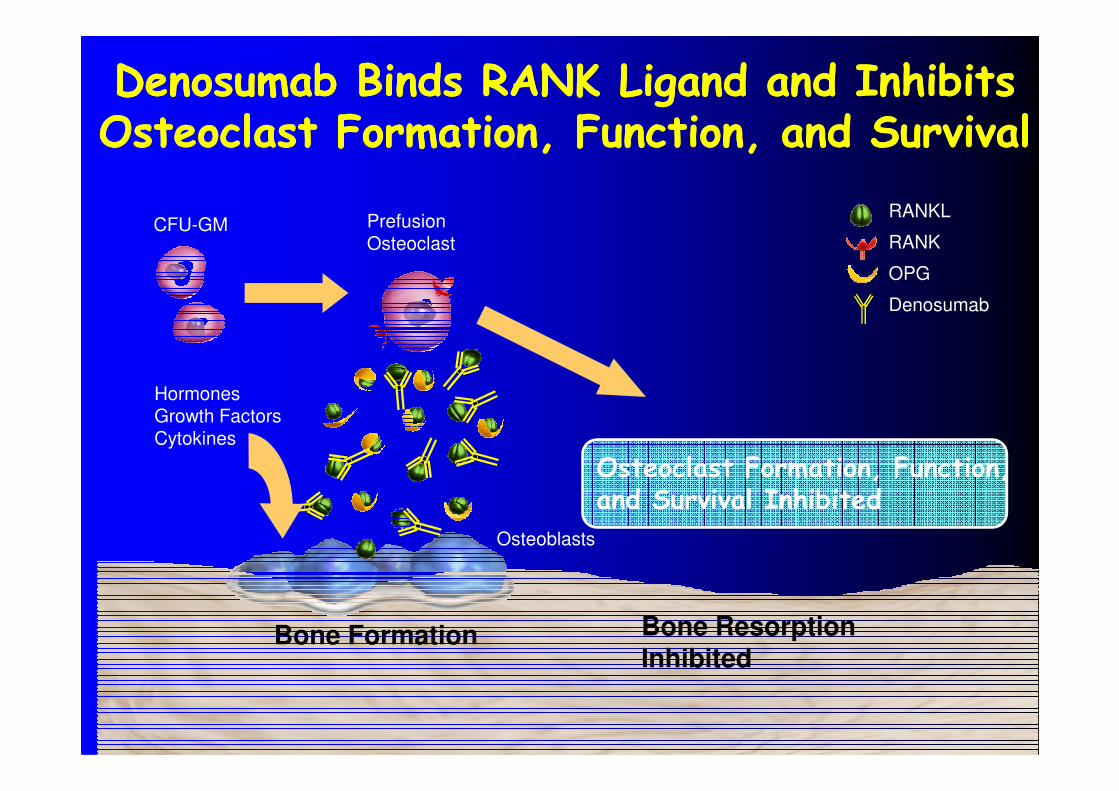
Denosumab Binds RANK Ligand and Inhibits Denosumab Binds RANK Ligand and Inhibits Osteoclast Formation, Function, and SurvivalOsteoclast Formation, Function, and Survival
RANKL
RANK
OPG
Denosumab
CFU-GM PrefusionOsteoclast
Hormones
Bone Formation Bone Resorption Inhibited
Osteoclast Formation, Function, and Survival Inhibited
Osteoblasts
HormonesGrowth FactorsCytokines
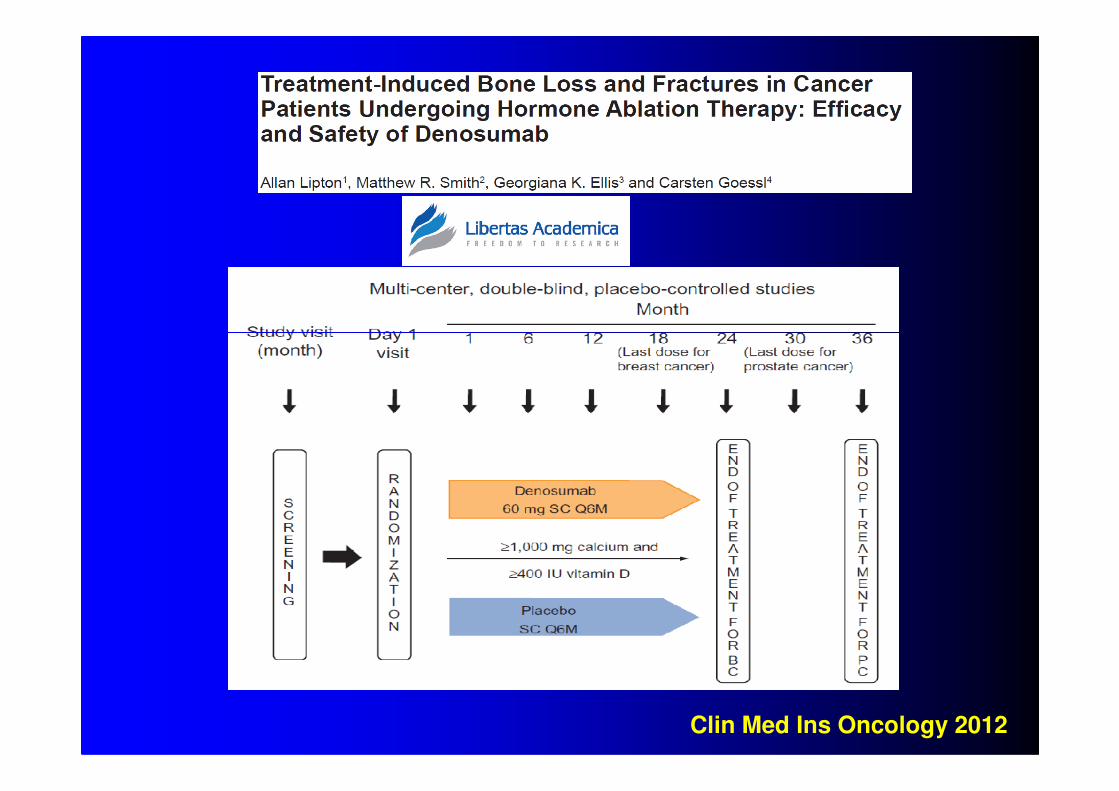
Clin Med Ins Oncology 2012
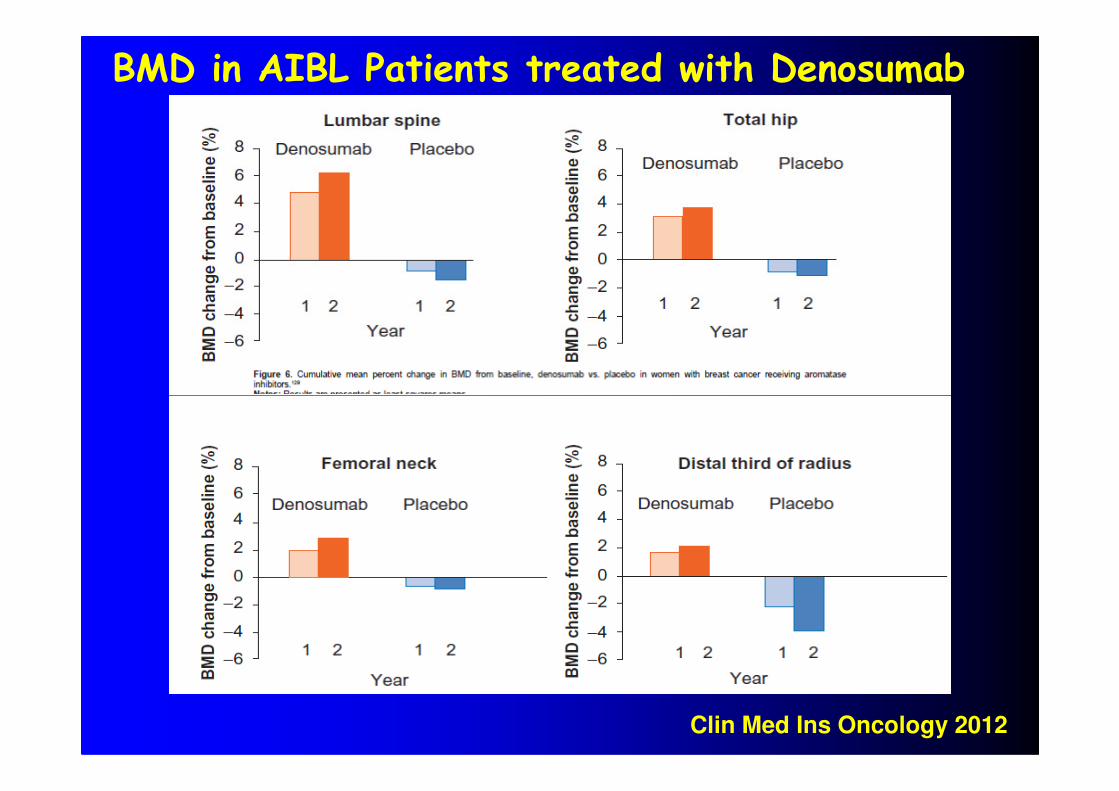
BMD in AIBL Patients treated with Denosumab
Clin Med Ins Oncology 2012
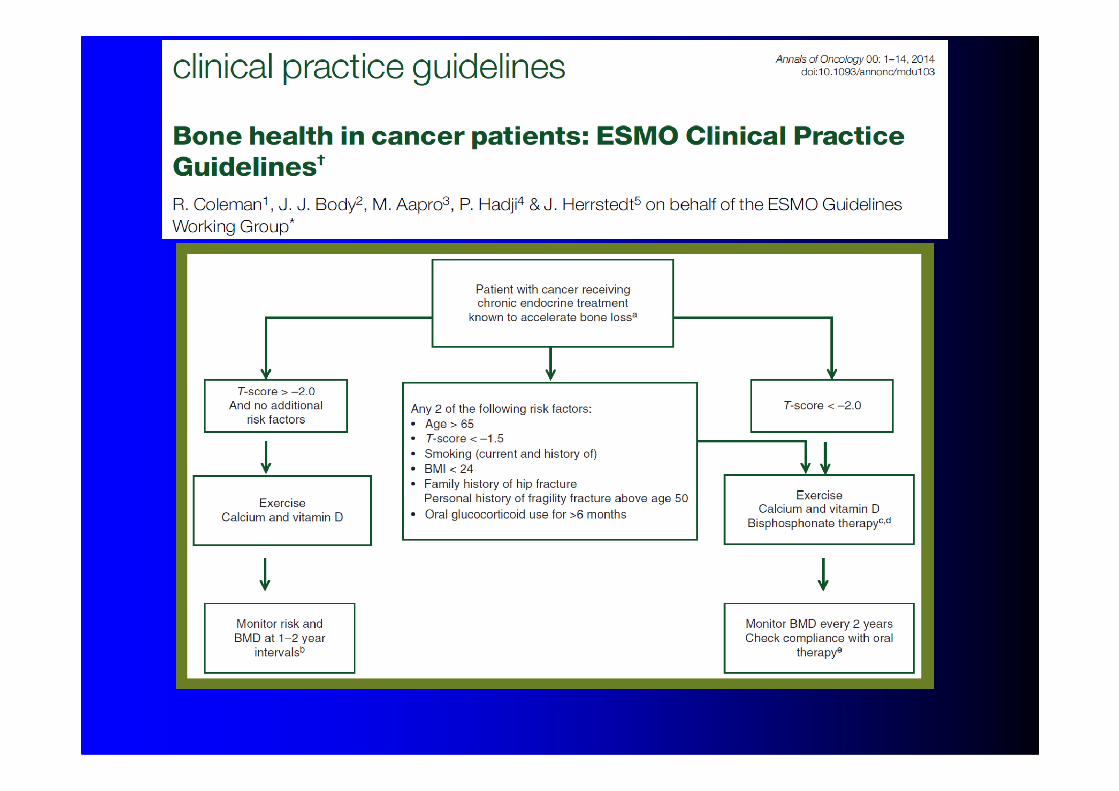
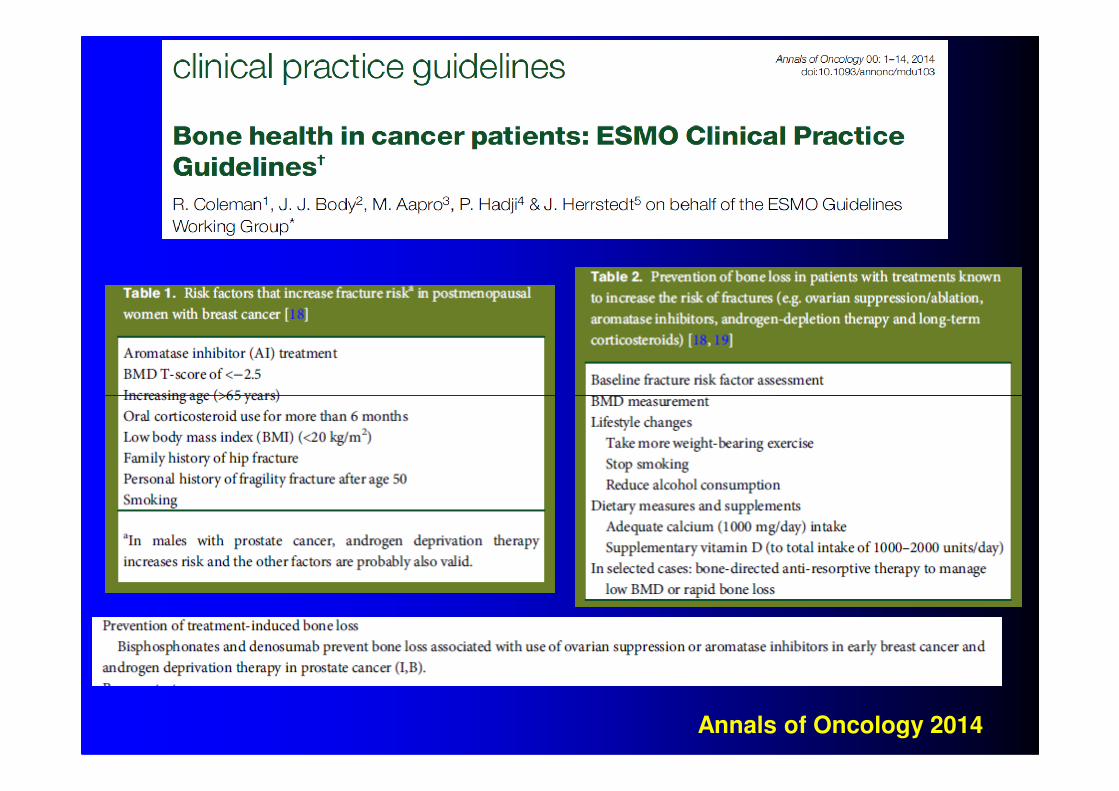
Annals of Oncology 2014
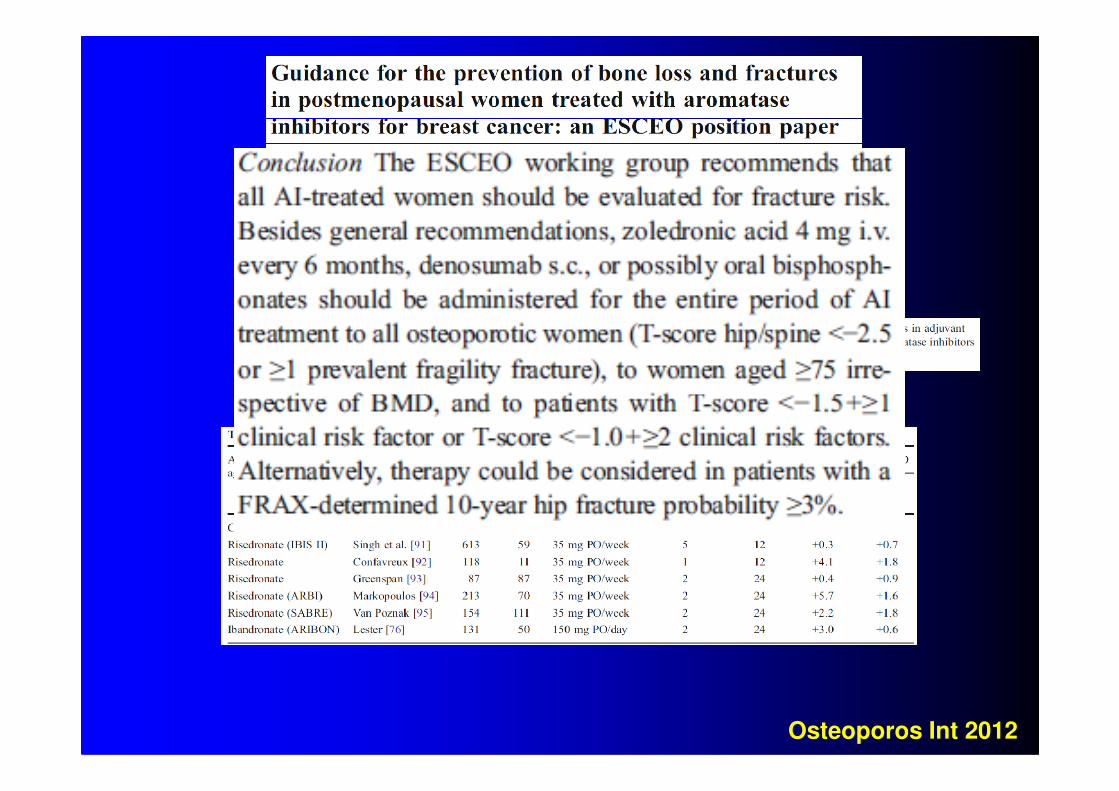
Osteoporos Int 2012
CONCLUSIONS� AILS is both preventable and treatable.
A lack of awarness of the potential long-termadverse effect of tumor treatment on theskeleton may lead to chronic pain, disability anda decrease in Quality of life in many Patients.
� The challenge is to make the assessment of� The challenge is to make the assessment ofthe risk of Osteoporosis an integral part of thefollow-up of cancer Patients whose therapyregimens predispose to skeletal damage, so thattherapy be initiated before fractured occur.
� There are emerging data showing that the use ofBone targeting treatments (BP or Denosumab)can reduce metastasis to bone.



Grazie dell’attenzione
0.9
0.8
T
BMD IN PATIENTS RECEIVING TAMOXIFEN
(T) OR TAMOXIFEN + PREDNISOLONE (T + P)
0 12 24
0.7
0.6
186
MONTHS
T + P
FENTIMAN I.S., Eur. J. Cancer. 1992
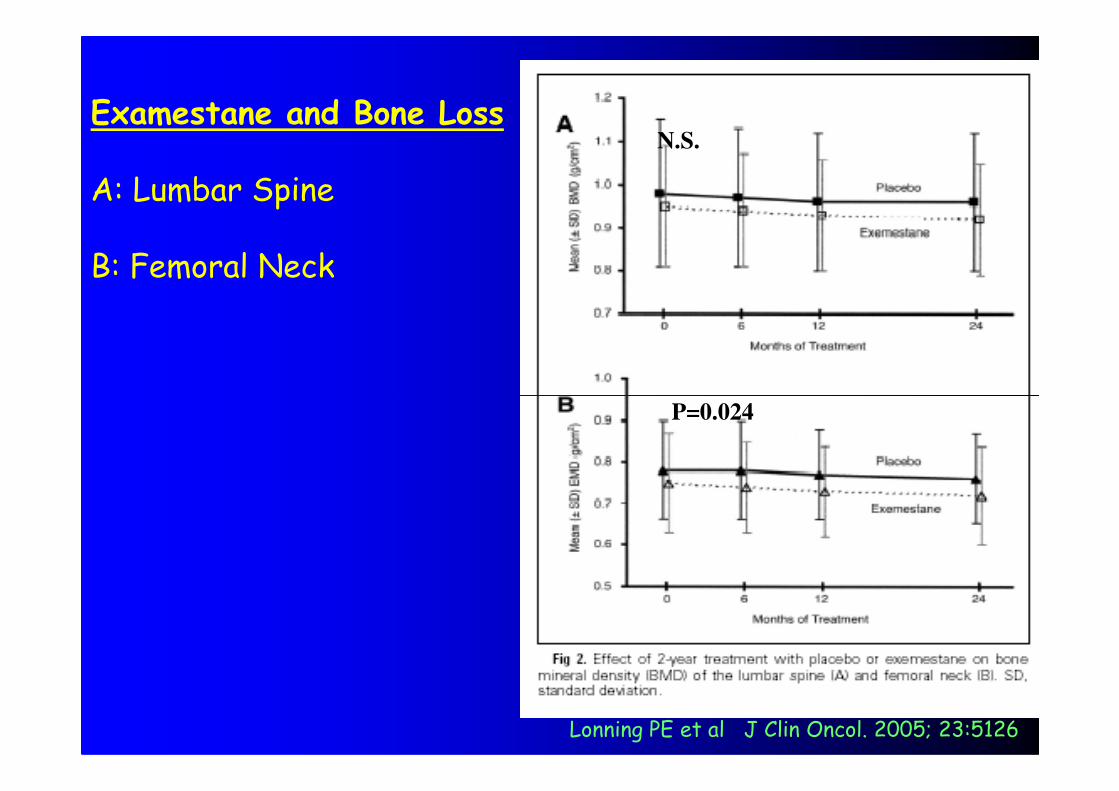
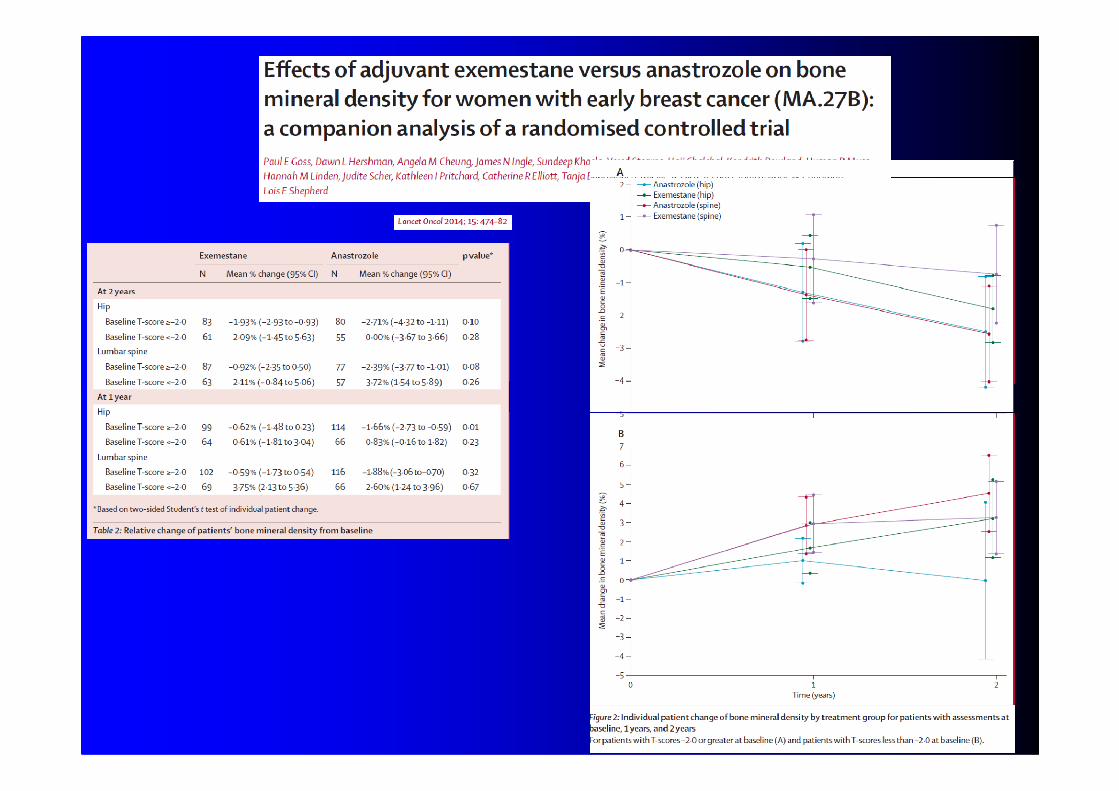
N.S. Examestane and Bone Loss
A: Lumbar Spine
B: Femoral Neck
Lonning PE et al J Clin Oncol. 2005; 23:5126
P=0.024
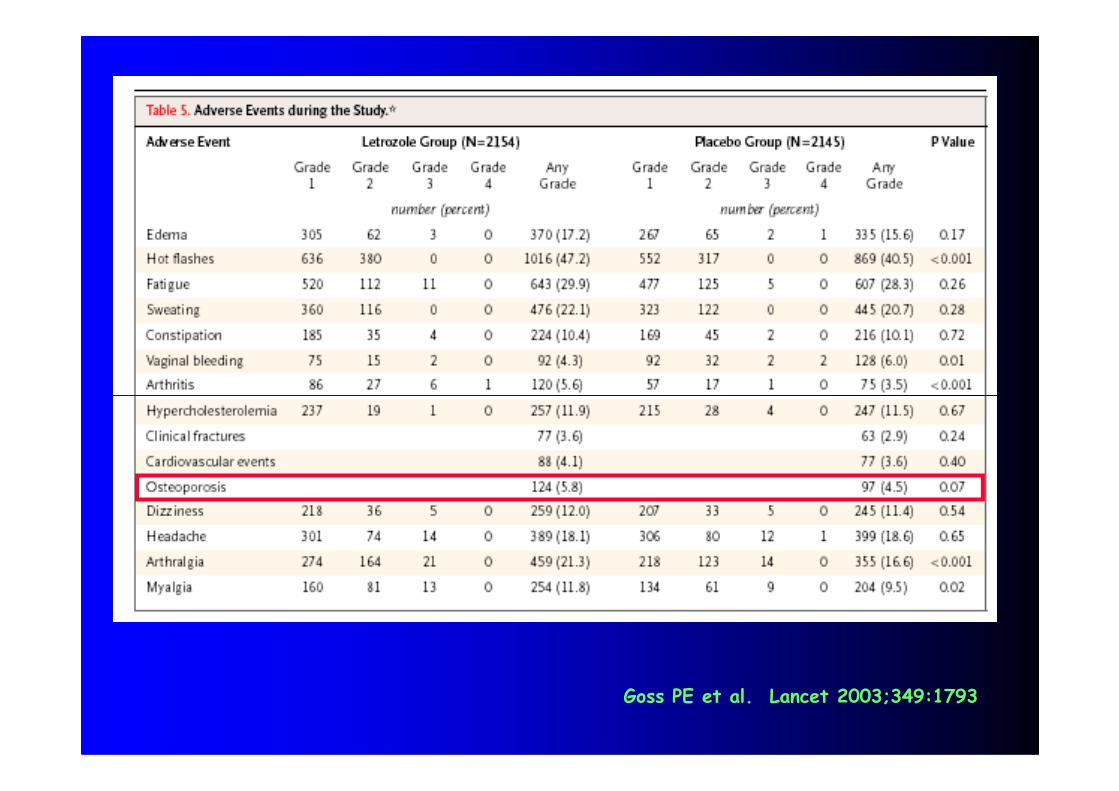
Goss PE et al. Lancet 2003;349:1793
•Tamoxifene
•GnRH Agonisti
•Effetti ormono-dipendenti
TERAPIE ANTITUMORALI AD EFFETTO SULL’OSSO
•Effetti non ormono-dipendenti
•Glucocorticoidi
•Inibitori dell’aromatasi
QUALE MANAGEMENT ?
Raccomandazioni per lo screening e la diagnosi•La DXA è considerata la modalità standard perindividuare precocemente riduzioni del BMD che èopportuno valutare prima di iniziare il trattamento edopo la sospensione dei farmaci.
•Evitare di giungere alla diagnosi di OP in fase avanzatao quando è già presente la frattura, poiché i miglioririsultati del trattamento sono ottenuti in fase precoce.risultati del trattamento sono ottenuti in fase precoce.
•Nel paziente in trattamento antineoplastico lacomparsa/presenza di dolore osseo,fratture patologiche,pronunciata riduzione in altezza, captazioni anomale allascintigrafia ossea non devono far pensare solo asecondarietà, ma anche a possibili fratture daosteoporosi secondaria.
•Considerare e correggere anche altri fattori di rischio,come deficit di vitamina D, malnutrizione ecc.
Prevenzione e trattamento (1)•HRT:L’OP da chemioterapici può essere prevenuta,soprattutto nelle donne ipogonadiche con tumori nonormono-dipendenti, nelle quali vi è l’indicazione assolutaalla terapia ormonale sostitutiva immediata e di lungadurata. L’HRT risulta più efficace se iniziata almomento della menopausa o entro i 3 anni successivi,anche se mancano studi prospettici sulla prevenzioneanche se mancano studi prospettici sulla prevenzionedelle fratture in queste pazienti
•Supplementazione con Calcio e Vitamina D: (500-1000mg di calcio e 700 UI di Vitamina D) da istituire intutti i pazienti a meno di chiare controindicazioni comeipercalcemia ed ipercalciuria•Raloxifene: in attesa dei dati riguardo all’utilizzocome antitumorale (Studio STAR). Utilizzo approvatoper l’osteoporosi postmenopausale

BisfosfonatiIndicati nei tumori ormono-dipendenti (mammario e prostatico).Hanno un effetto favorevole in presenza di MTS scheletriche.
a) Alendronato: 10 mg aumenta la BMD, riduce l’incidenza difratture vertebrali e non da osteoporosi postmenopausale e GIOP
b) Etidronato: aumenta la massa ossea, riduce l’incidenza difratture vertebrali, previene la perdita di BMD indotta da GC
Prevenzione e trattamento (2)
fratture vertebrali, previene la perdita di BMD indotta da GC
c) Pamidronato (30-60 mg e.v. ogni 3 mesi): aumenta la BMDnell’OP postmenopausale e nella GIOP. Indicato nell’ipercalcemianeoplastica, nelle MTS ossee osteolitiche da ca mammario e mieloma
D) Zoledronato (4 mg q 6 mesi) contrasta la perdita ossea indottada Letrozolo. Sono in corso studi sulla prevenzione delle fratture.
d) Risedronato (5 mg):riduce le fratture vertebrali in OPpostmenopausale e GIOP
e) Clodronato (800 mg): riduce le fratture vertebrali in OPpostmenopausale e mantiene il BMD
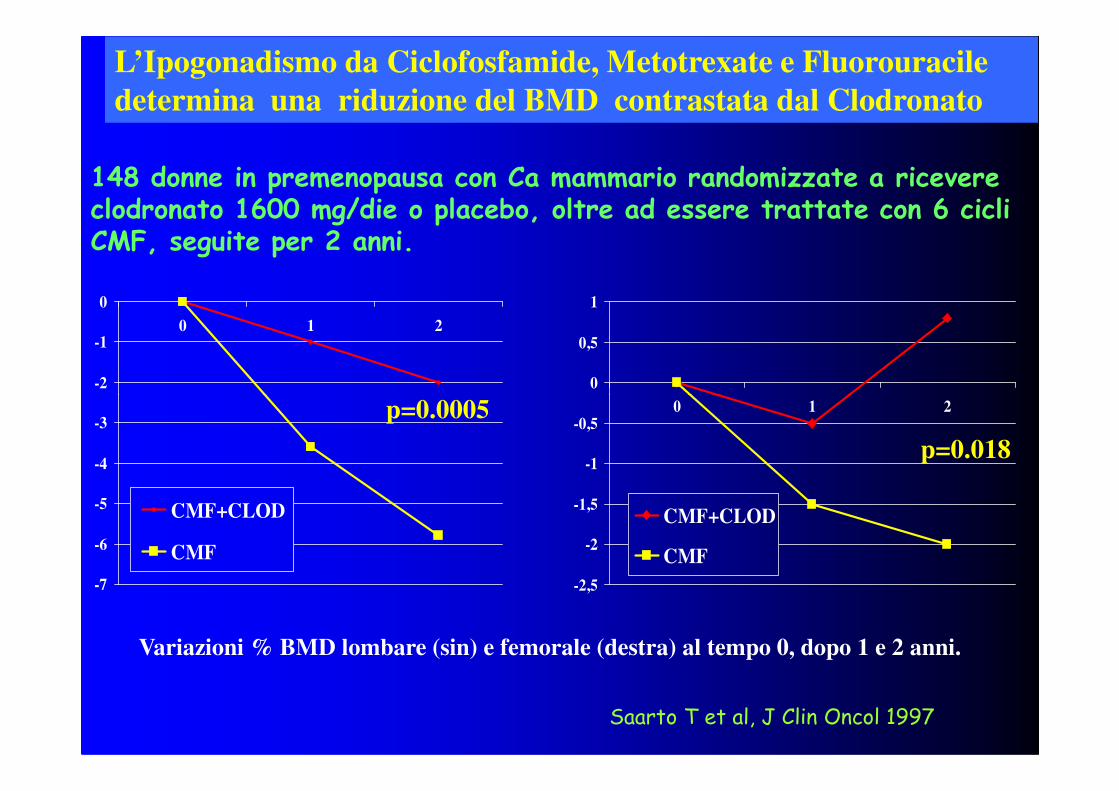
L’Ipogonadismo da Ciclofosfamide, Metotrexate e Fluorouracile
determina una riduzione del BMD contrastata dal Clodronato
148 donne in premenopausa con Ca mammario randomizzate a ricevere clodronato 1600 mg/die o placebo, oltre ad essere trattate con 6 cicli CMF, seguite per 2 anni.
-2
-1
0
0 1 2
0
0,5
1
p=0.0005
-7
-6
-5
-4
-3
CMF+CLOD
CMF
Variazioni % BMD lombare (sin) e femorale (destra) al tempo 0, dopo 1 e 2 anni.
-2,5
-2
-1,5
-1
-0,50 1 2
CMF+CLOD
CMF
Saarto T et al, J Clin Oncol 1997
p=0.0005
p=0.018
-1
0
1
2
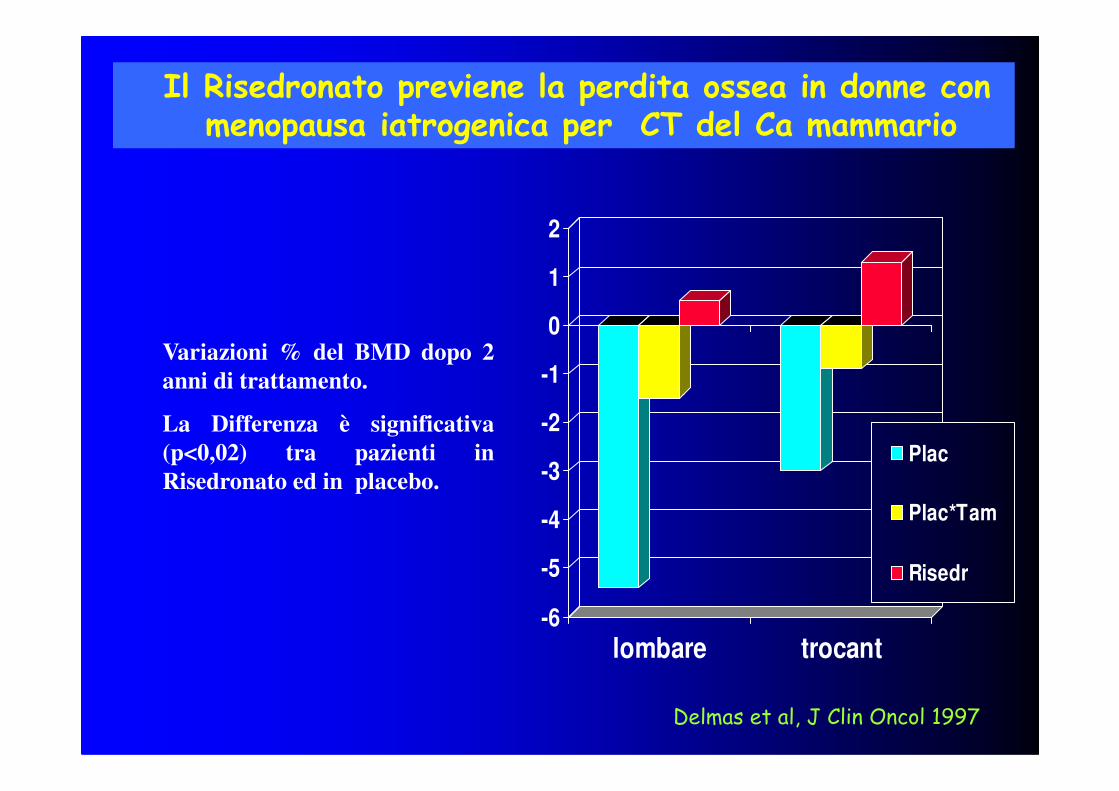
Variazioni % del BMD dopo 2
anni di trattamento.
Il Risedronato previene la perdita ossea in donne con menopausa iatrogenica per CT del Ca mammario
-6
-5
-4
-3
-2
lombare trocant
Plac
Plac*Tam
Risedr
Delmas et al, J Clin Oncol 1997
La Differenza è significativa
(p<0,02) tra pazienti in
Risedronato ed in placebo.
RRAANNDDOOMMIIZZEE
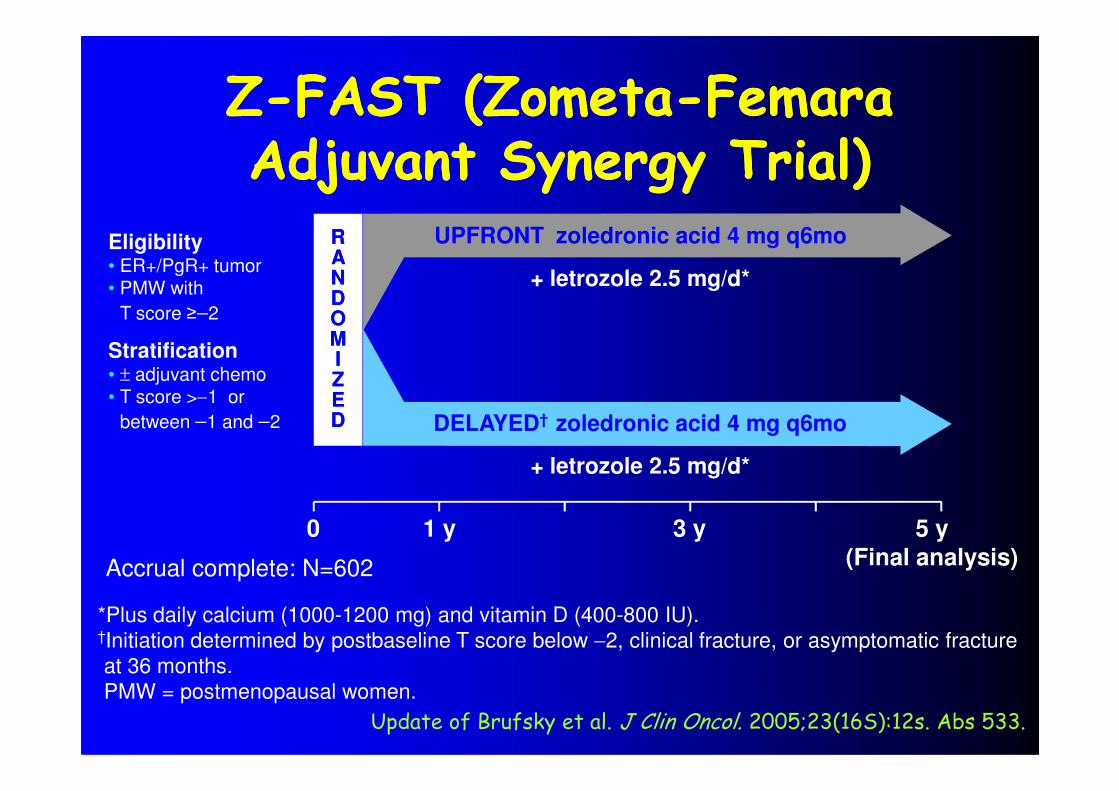
Eligibility• ER+/PgR+ tumor• PMW with
T score ≥−2
Stratification• ± adjuvant chemo• T score >−1 or
ZZ--FAST (ZometaFAST (Zometa--FemaraFemaraAdjuvant Synergy Trial)Adjuvant Synergy Trial)
UPFRONT zoledronic acid 4 mg q6mo
+ letrozole 2.5 mg/d*
0 5 y
(Final analysis)
EEDD
3 y1 y
• T score >−1 or
between −1 and −2
+ letrozole 2.5 mg/d*
DELAYED† zoledronic acid 4 mg q6mo
Accrual complete: N=602
*Plus daily calcium (1000-1200 mg) and vitamin D (400-800 IU).†Initiation determined by postbaseline T score below −2, clinical fracture, or asymptomatic fracture
at 36 months.
PMW = postmenopausal women.
Update of Brufsky et al. J Clin Oncol. 2005;23(16S):12s. Abs 533.
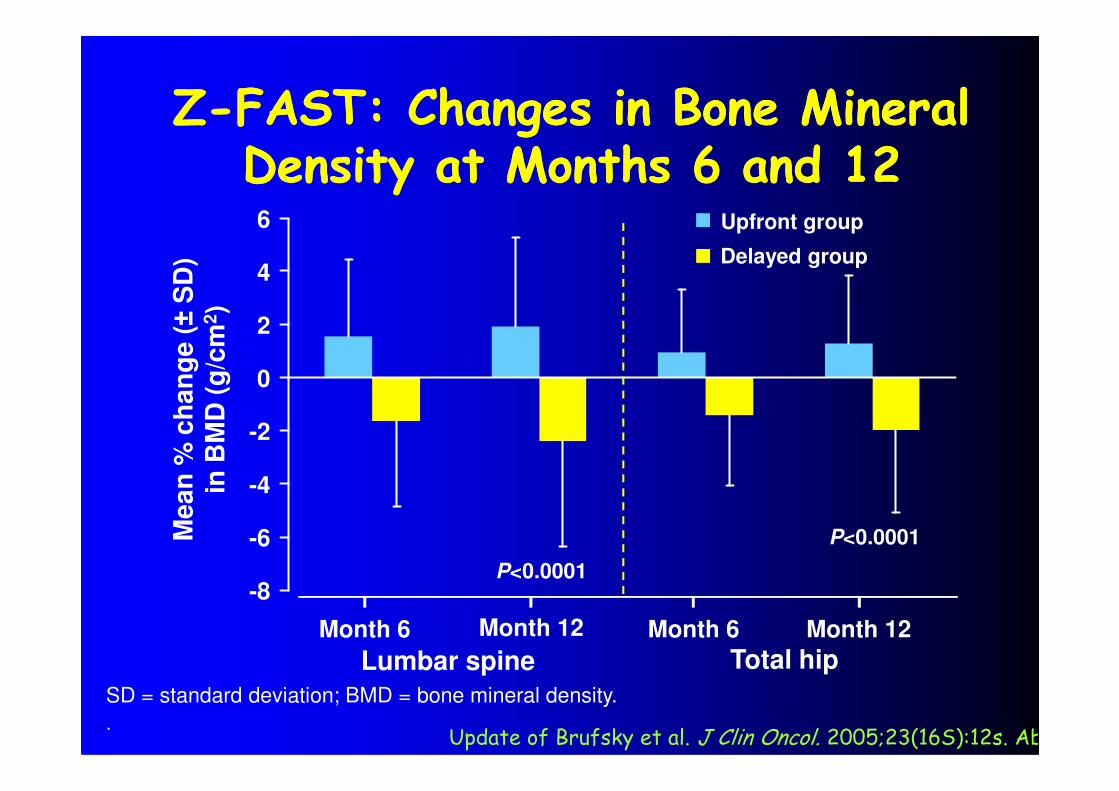
ZZ--FAST: Changes in Bone Mineral FAST: Changes in Bone Mineral Density at Months 6 and 12Density at Months 6 and 12
0
2
4
6
Me
an
% c
ha
ng
e (±
SD
)in
BM
D (
g/c
m2)
Upfront group
Delayed group
Lumbar spine Total hip
P<0.0001
P<0.0001
Month 6 Month 12 Month 6 Month 12
SD = standard deviation; BMD = bone mineral density.
.
-8
-6
-4
-2
Me
an
% c
ha
ng
e (
in B
MD
(g
/cm
Update of Brufsky et al. J Clin Oncol. 2005;23(16S):12s. Ab
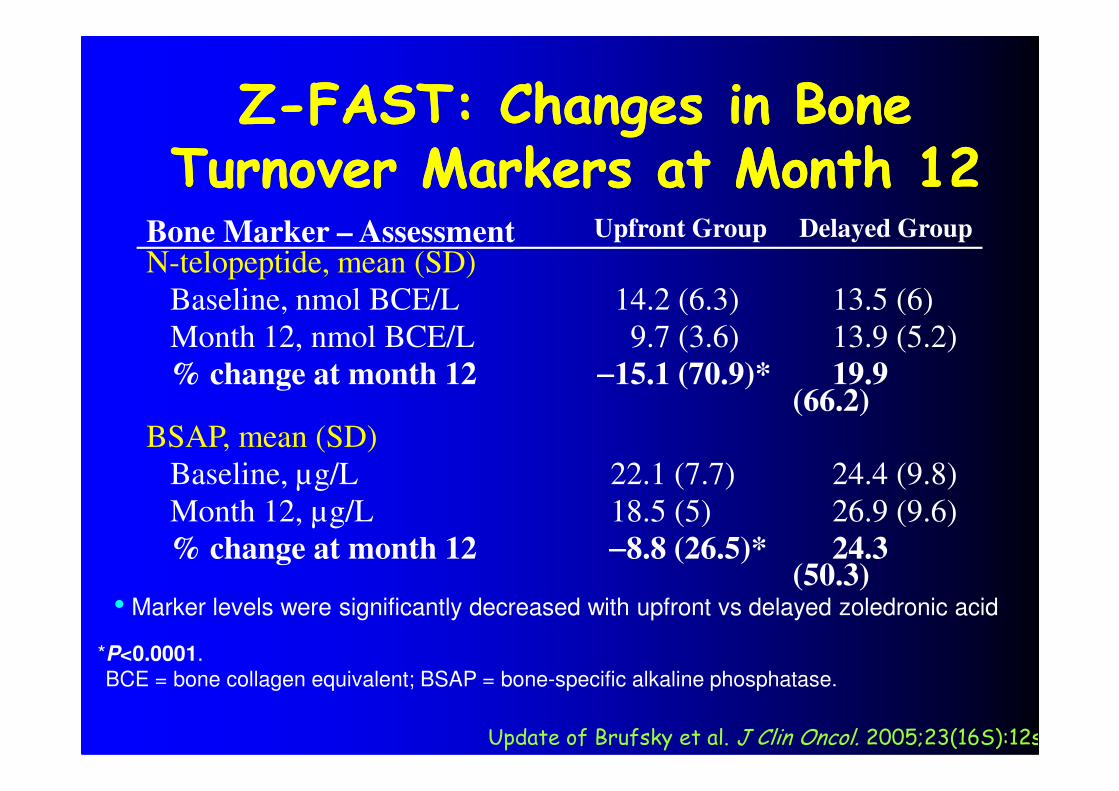
ZZ--FAST: Changes in Bone FAST: Changes in Bone Turnover Markers at Month 12Turnover Markers at Month 12
13.5 (6)
13.9 (5.2)
19.9 (66.2)
14.2 (6.3)
9.7 (3.6)
−−−−15.1 (70.9)*
N-telopeptide, mean (SD)
Baseline, nmol BCE/L
Month 12, nmol BCE/L
% change at month 12
Delayed GroupUpfront GroupBone Marker – Assessment
(66.2)
24.4 (9.8)
26.9 (9.6)
24.3 (50.3)
22.1 (7.7)
18.5 (5)
−−−−8.8 (26.5)*
BSAP, mean (SD)
Baseline, µg/L
Month 12, µg/L
% change at month 12
*P<0.0001.
BCE = bone collagen equivalent; BSAP = bone-specific alkaline phosphatase.
• Marker levels were significantly decreased with upfront vs delayed zoledronic acid
Update of Brufsky et al. J Clin Oncol. 2005;23(16S):12s