Somministrazione di insulina sottocutanea in adulti con Diabete di ...
Gianluca PerseghinDipartimento di Medicina e Chirurgia
Università degli Studi di Milano Bicocca
Dipartimento di Medicina Interna e RiabilitazionePoliclinico di Monza, Monza
Le associazioni insulina/GLP1-RA
Dichiarazione di Conflitto di InteressiHonorarium as a speaker in Scientific EventsSigma-Tau Alleanza Lilly/BI ServierNovartis AstraZeneca BMS BITakeda Janssen MundipharmaEli-Lilly Sanofi-Aventis Menarini Diag BayerMSD Novo Nordisk Roche Diag
Grant supportNovo Nordisk (Investigator-Initiated-Study Grant) Kellogg (Investigator-Initiated-Study Grant)
AstraZeneca, Lilly, Sanofi, Novo Nordisk, Sigma-Tau, Menarini Diag(Travel grants)
Scientific advisory boardsAstraZeneca, Lilly, Sanofi
Quando ?
Programma DIA Pavia2019
Nuovi farmaci
Nuove insuline
Associazioniinsulina/GLP1-RA
Il bisogno clinicoRCTs demonstrate that many patients do not achieveglycaemic control despite a treat-to-target approach
1 2 3 4
20 weeks 24 weeks 52 weeks
Glargine
NPH
Detemir
a
aHbA1c responders
Il bisogno clinicoReal world data in clinical practice show that many patients do
not achieve glycaemic target after basal insulin initiation
Patients achieving glycaemic target (%)
2-year retrospective cohort study of basal insulin initiation in the US (n=14,458)1
Baseline HbA1c: 8.6%
3-year retrospective audit of basal insulin initiation in the UK (n=516)2
Baseline HbA1c: 9.3%
Curtis & Lage. J Med Econ 2014;17:21–31 Dale et al. Prim Care Diabetes 2010;4:85–9
Grafico1
Category 1
Category 2
Series 1
29
29
Sheet1
Series 1Column1Column2
Category 129
Category 229
Barriers to traditionalbasal insulin intensification
Diabetologist’s fear ofhypoglycaemia
Diabetologist’s and patients’ fear about weight gain
Peyrot et al. Diabet Med 2012;29:682–9Peyrot et al. Curr Med Res Opin 2009;25:1985–93Davidson et al. Endocr Pract 2011;17:395–403Meneghini et al. Endocr Pract 2011;17:727–36
Rubin et al. Diabetes Educ 2009;35:1014–22Vijan et al. J Gen Intern Med 2005;20:479–82
Donnelly et al. QJM 2007;100:345–50
Diabetologist’s and patients’ inertia
Quando la “basalizzazione”non è sufficiente ?
Considerare l’aggiunta di insulina rapida sePPG > 180 mg/dl.
Inzucchi S et al, Diabetes Care 2015
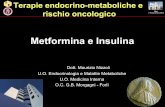
Come ?Add-on a pazienti già
basalizzati rispetto allaottimizzazione della
titolazione
Subjects with T2DM
(N=557)IGlar + metformin
(n=279)
IDegLira + metformin(n=278)
IDegLiraStarting dose:16 dose steps
Maximum dose:50 dose steps
IGlarStarting dose:Pre-trial dose
Maximum dose:None
Randomized 1:1Open label
0 27
Inclusion criteria•T2DM
•Metformin + IGlar (20–50 units)•HbA1c 7–10%•Age ≥18 years•BMI ≤40 kg/m2
–2 26
ScreeningVisit 1
randomizationVisit 2
End of trialVisit 28
Follow-up Visit 29
Week
Mean FPGa Dose change
mmol/L mg/dL dose steps/units
90 +2aAdjustments performed twice weekly based on mean of three preceding fasting self-measured
blood glucose values obtained prior to dosing adjustment days
DUAL V
NN9068-3952; IDegLira vs. IGlar. BMI, body mass index; FPG, fasting plasma glucose
Dual V - resultsLingvay I et al JAMA, 2016
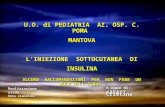
Lixilan: Study Design and EndpointsOpen label, 1:1 randomized, 2-arm parallel-group, 24-week treatment trial
Patients with:● T2DM≥ 1 year● Stable dose of
metformin ≥ 1.5g/d● 7 ≤HbA1c ≤10%
Objectives
Primary:- Non-inferiority of LixiLan
over Lantus® on HbA1c change at Week 24
- Once shown, superiority tested
Study design
Lantus® + Metformin
24W
LixiLan + Metformin
Daily dose adjusted to FPG target (80 to 100mg/dL) Secondary:
- Superiority of LixiLan over Lantus® on:• Postprandial glucose• Body weight• % of patients with HbA1c < 7%
and no weight gain at week 30 and/or documented hypoglycemia
• Insulin dose
(Maximum dose = 60U/30µg)
(No upper limit)
2U Lantus/ 1µg Lixisenatide ratio
5 6 7 8 9 10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
10
12
14
16
18
20
22
24
26
28
30
32
34
36
38
40
42
44
46
48
50
52
54
56
58
60
Lixilan: Efficacy Results
Aroda VR et al Diabetes Care 2016
Results - summary
Conclusioni 1
Come ?Add-on a pazienti già
basalizzativs analogo rapido
Quando la “basalizzazione”non è sufficiente ?
Considerare l’aggiunta di insulina rapida sePPG > 180 mg/dl.
Inzucchi S et al, Diabetes Care 2015
Billings LK et al,Diabetes Care 2018
Conclusioni 2
In pazienti non controllati con la terapia insulinica basale, la combinazione precostituita LIRA + insulina degludec non è inferiore alla terapia multi-iniettiva in termini di riduzione della HbA1c, con risultati migliori in termini di rischio di ipoglicemia e di aumento del peso
Se non vi piaceassociazione
precostituita fissa?
Award 9Pozzilli P et al DOM, 2018
Key inclusion criteria• Treatment with insulin glargine once daily (+/- metformin) for at least 3 months prior to
study entry• A1C ≥7.0% and ≤10.5%• Required glargine dose increase at randomization per the treat-to-target algorithm• Body mass index ≤45 kg/m2
aPatients continued prestudy regimens; did not change antihyperglycemia medications used or their doses, except when allowed per protocol. Stabilization Period = Weeks 0 to 4 w/ restricted insulin dose adjustments. Glargine Titration Period = Weeks 4 to 28 w/ unrestricted insulin dose adjustments.
Week -3 0 12Randomization
Dulaglutide 1.5 mg + Titrated Basal Insulin Glargine (+/- Metformin)
28
Insulin Glargine Titration Period
Primary/Final Time Point
Treatment Period
Screening/Lead-ina Placebo + Titrated Basal Insulin Glargine (+/- Metformin)
4
Stabilization Period
Award 9Pozzilli P et al DOM, 2018
Il paziente in GLP1-RA
Un paradigma da “sfatare”
?
La scelta di raccomandare solo alcuni farmaci in aggiunta alla metformina è dettata da:
• Efficacia sulla HbA1c• Tollerabilità• Sicurezza• Effetti di protezione cardiovascolare nei pazienti a rischio
Cortesia Edoardo Mannucci SID Rimini 2018
Davies MJ et al Diabetes Care, 2018
Goals of Care
Prevent complicationsOptimize QoL
Davies MJ et al Diabetes Care, 2018
Key messagges
Davies MJ et al Diabetes Care, 2018
Davies MJ et al Diabetes Care, 2018
Intensificazione con iniettivi
Davies MJ et al Diabetes Care, 2018
Davies MJ et al Diabetes Care, 2018
What if the patients is in primary prevention ?
Davies MJ et al Diabetes Care, 2018
What if the patients is in primary prevention ?
Dual III – resultsLinjawi S et al Diabetes Ther, 2017
Anyway, what is the best strategy ?
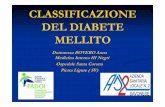
DUAL™ I: study design
Patients with type 2 diabetes
(n= 1663)
0 26 weeks
Randomised 2:1:1Open label
Titrate to targetFPG 4–5 mmol/L
Starting dose:10 dose steps/units
Dose adjustments (2-0-2) twice
weekly Liraglutide 1.8 mg + Met ± pio (n=415)
IDeg + Met ± pio (n=414)
IDegLira + Met ± pio (n=834)
Inclusion criteria• Type 2 diabetes • Insulin-naïve treated with
Met ± pio• HbA1c 7.0–10.0%• BMI ≤40 kg/m2• Age ≥18 years*
Mean fasting PG Dose change
mmol/L dose steps or U
5.0 +2
Titration algorithm: IDegLira and IDeg
FPG, fasting plasma glucose; IDeg, insulin degludec; IDegLira, insulin degludec/liraglutide combination; Met, metformin; pio, pioglitazone*Singapore, age ≥21 years; FPG, self-measured using a glucometer which was calibrated to convert blood glucose measurements to plasma glucose values; liraglutide starting dose: 0.6 mg, dose escalated by 0.6 mg/week
Gough SC et al Lancet Diabetes Endocrinol, 2014
DUAL™ I: HbA1c over time
Time (weeks)
HbA
1c(%
)
0.0
−1.91%* 6.4%
*p
DUAL™ I: percentage of patients to target
IDegLira (n=833)
IDeg (n=413)
Liraglutide (n=414)p
Conclusioni 3
Conclusioni finaliLa terapia di associazione GLP1-RA con insulina basale in associazione fissa o estemporanea è sicura ed efficace in pazienti
1) già «basalizzati» rispetto ad una ottimizzazione della titolazione, nei quali è superiore
2) già «basalizzati» rispetto alla strategia basal-bolus, nei quali non è inferiore
3) Nei pazienti in OHA naive alla terapia insulinica/iniettiva rispetto alla basalizzazione e/o GLP1-RA
Con effetti favorevoli sia rispetto al rischio di ipoglicemia che di massa corporea
Diapositiva numero 1Diapositiva numero 2Quando ?�Programma DIA Pavia�2019�Il bisogno clinico�RCTs demonstrate that many patients do not achieve�glycaemic control despite a treat-to-target approachIl bisogno clinico�Real world data in clinical practice show that many patients do not achieve glycaemic target after basal insulin initiationBarriers to traditional�basal insulin intensificationQuando la “basalizzazione”�non è sufficiente ?Diapositiva numero 9DUAL VDual V - resultsLixilan: Study Design and EndpointsLixilan: Efficacy ResultsDiapositiva numero 14Diapositiva numero 15Diapositiva numero 16Quando la “basalizzazione”�non è sufficiente ?Diapositiva numero 18Diapositiva numero 19Diapositiva numero 20Diapositiva numero 21Diapositiva numero 22Il paziente in GLP1-RA��Un paradigma da “sfatare”�?�Diapositiva numero 24Diapositiva numero 25Diapositiva numero 26Diapositiva numero 27Diapositiva numero 28Diapositiva numero 29Diapositiva numero 30Diapositiva numero 31Diapositiva numero 32Diapositiva numero 33Dual III – results�Linjawi S et al Diabetes Ther, 2017Diapositiva numero 35DUAL™ I: study designDUAL™ I: HbA1c over timeDUAL™ I: percentage of patients to targetDiapositiva numero 39Diapositiva numero 40