La RCP di Qualità - Formazione In Emergenza Sanitaria¹ RCP + HQ - RCP = Maggiore Sopravvivenza
121
Linee Guida ILCOR 2010 La RCP di Qualità
Transcript of La RCP di Qualità - Formazione In Emergenza Sanitaria¹ RCP + HQ - RCP = Maggiore Sopravvivenza
Linee Guida ILCOR 2010
La RCP di Qualità
CPR
New Guidelines 2010

18 Ottobre 2010
Quanti
dimessi vivi
senza esiti
neurologici
permanenti
invalidanti?
Quante
persone
coscienti
recuperate
alla vita?
Quali orizzonti
Attuativi ?
Con le ultime linee guida ILCOR 2005 si sono
evidenziati parametri clinici di miglioramento
con criterio di significatività statistica?
La letteratura internazionale evidenzia come,
ancora oggi, la RCP venga effettuata poco e
male
JAMA 2005
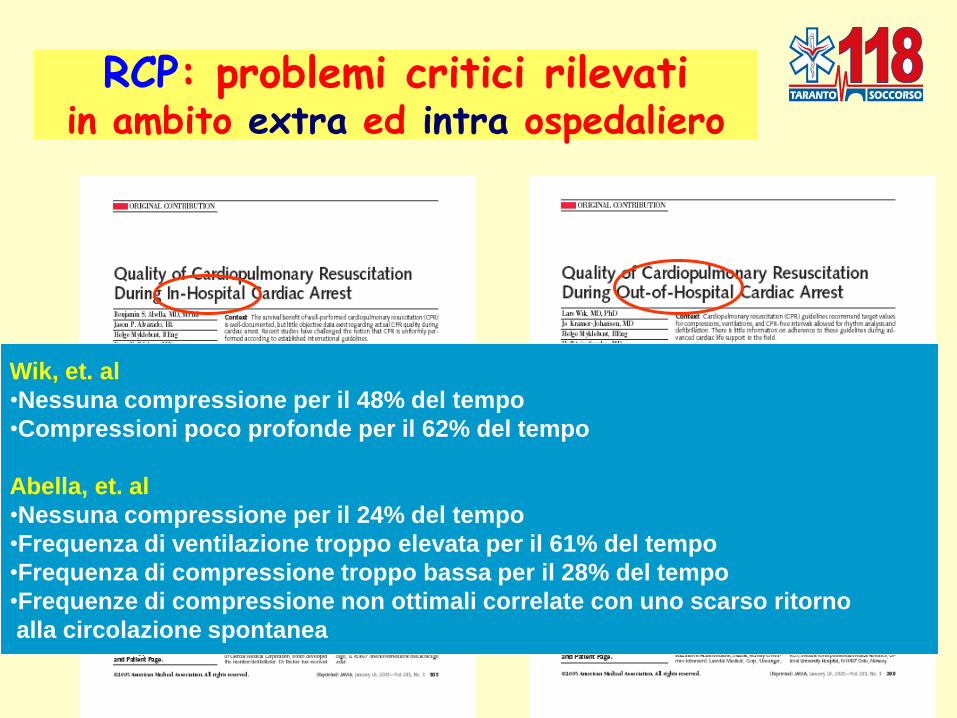
RCP: problemi critici rilevati in ambito extra ed intra ospedaliero
Wik, et. al
•Nessuna compressione per il 48% del tempo
•Compressioni poco profonde per il 62% del tempo
Abella, et. al
•Nessuna compressione per il 24% del tempo
•Frequenza di ventilazione troppo elevata per il 61% del tempo
•Frequenza di compressione troppo bassa per il 28% del tempo
•Frequenze di compressione non ottimali correlate con uno scarso ritorno
alla circolazione spontanea
CPR was inconsistent and often did not meet published guideline recommendations…

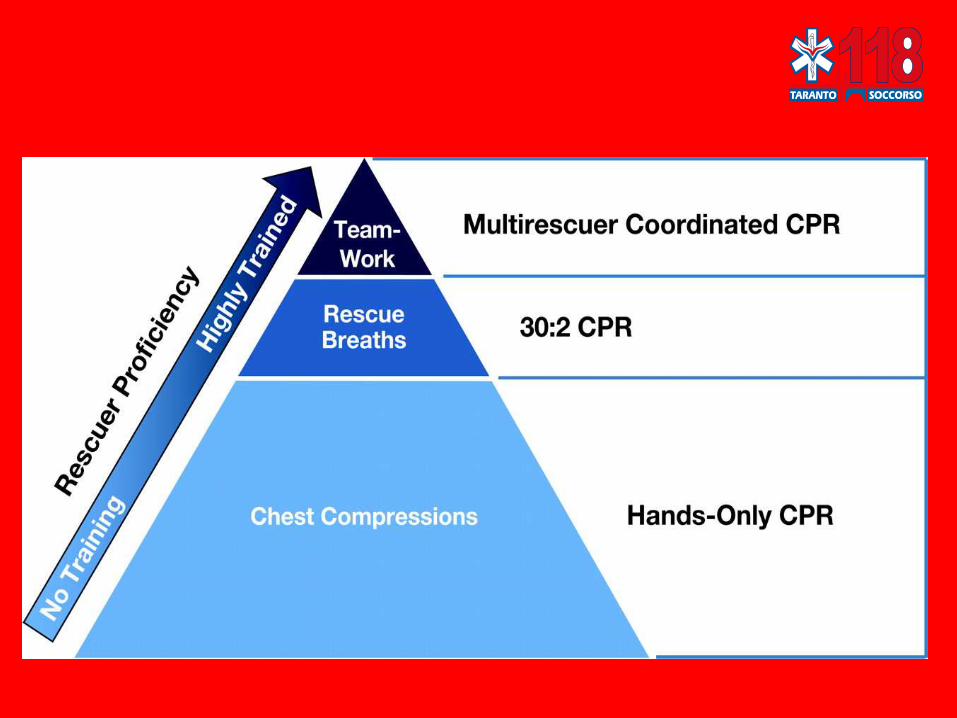
E’ indispensabile una rianimazione
di “alta qualità”
di qualità”…
deve essere:
Eseguita immediatamente
Eseguita correttamente
RCP
Interrotta il meno possibile
Abbinata nel momento giusto
alla defibrillazione
ILCOR 2005

di qualità”…
deve essere:
Eseguita immediatamente
Eseguita correttamente
RCP
Interrotta il meno possibile
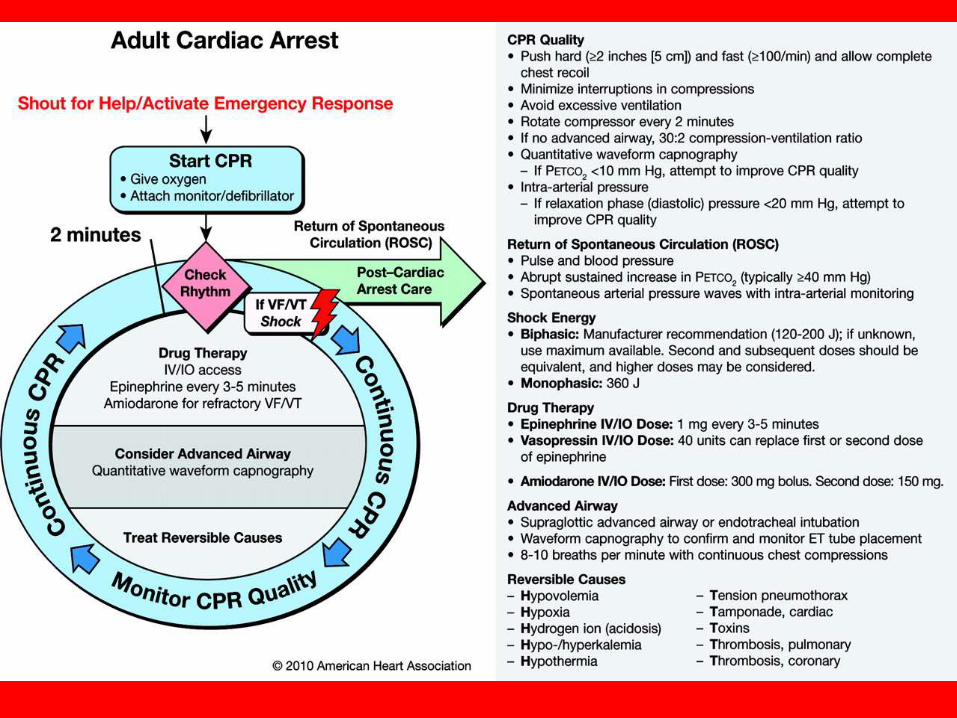
ILCOR 2010
Comprimi con forza ( 5 cm, non > 6)
Comprimi velocemente (almeno 100 compressioni/min, non > 120)
Rilascia completamente il torace tra le compressioni
Evita una eccessiva ventilazione del paziente

RCP
Eseguita immediatamente
Per produrre risultati statisticamente significativi la
RCP deve essere immediata
Eseguita correttamente
Interrotta il meno possibile
Ottobre 2007
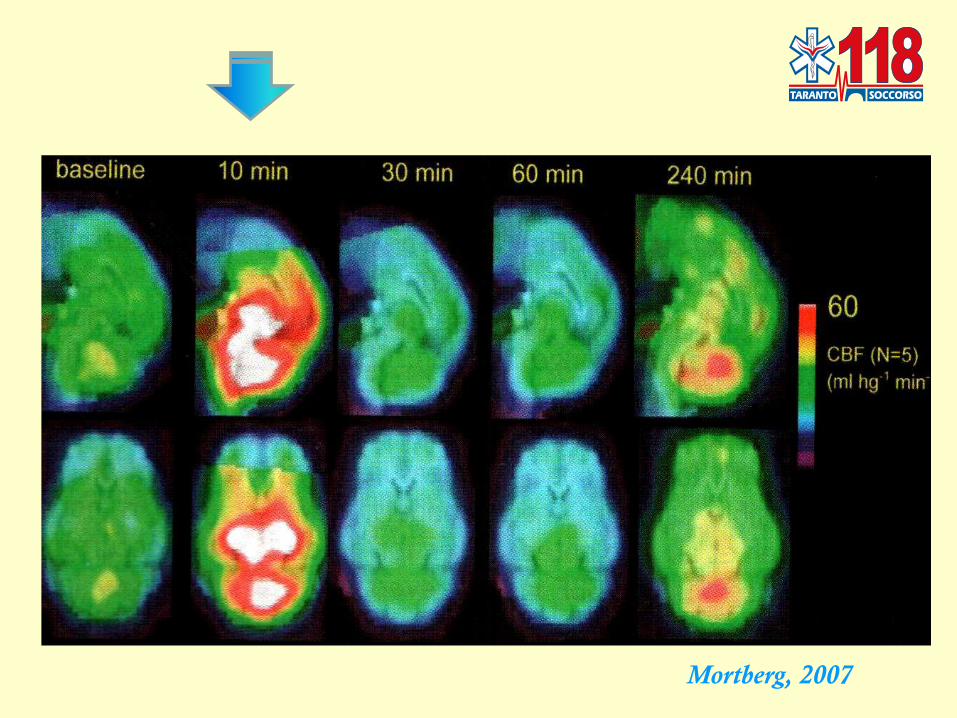
Mortberg, 2007
Maggio 2008
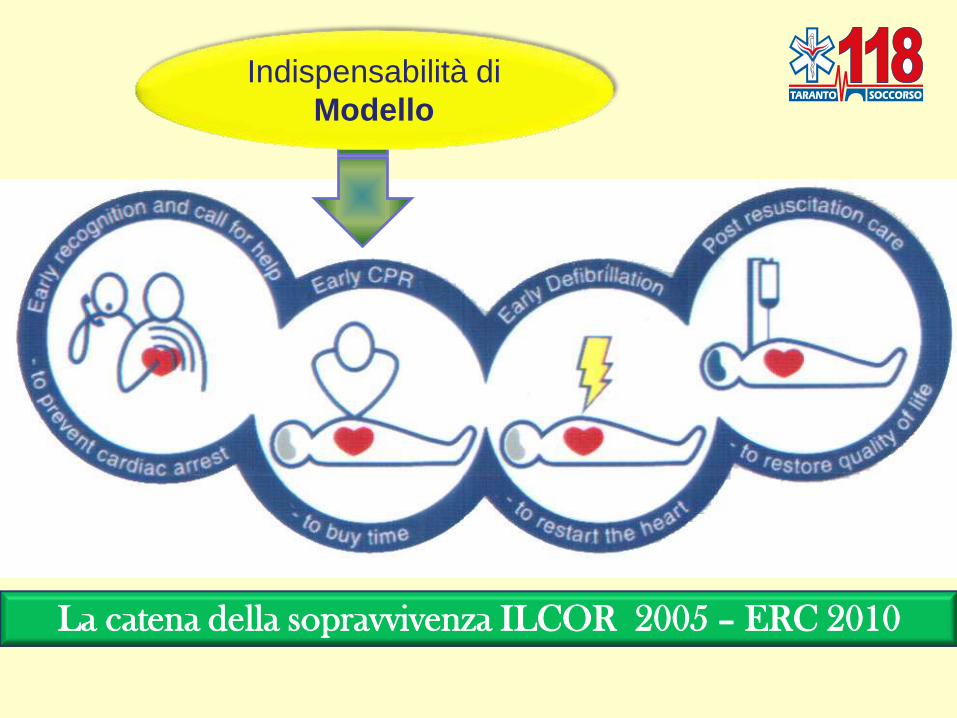
Indispensabilità di
Modello
La catena della sopravvivenza ILCOR 2005 – ERC 2010

La catena della sopravvivenza ILCOR 2005 – ERC 2010

La catena della sopravvivenza AHA 2010
Taranto Sera, mercoledì 5 settembre 2007
Taranto Sera, mercoledì 5 settembre 2007
93.000
Firme

23 Ottobre 2008 – Camera dei Deputati - Roma

23 Ottobre 2008 – Camera dei Deputati - Roma

23 Ottobre 2008 – Senato della Repubblica - Roma

Quale evoluzione?
Progredire attraverso le evidenze
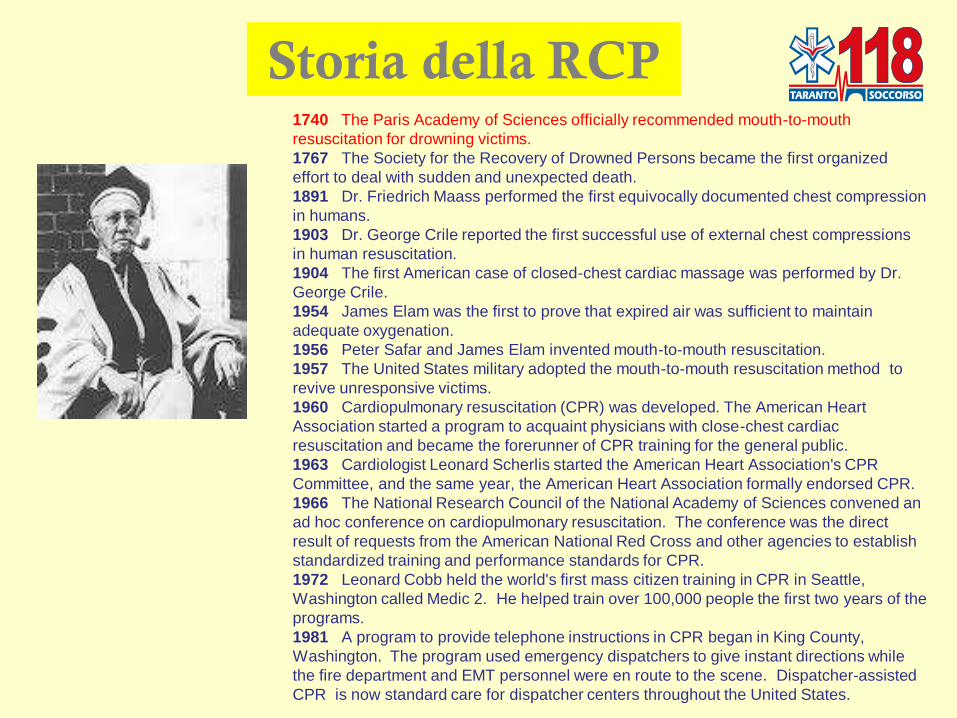
Storia della RCP 1740 The Paris Academy of Sciences officially recommended mouth-to-mouth
resuscitation for drowning victims.
1767 The Society for the Recovery of Drowned Persons became the first organized
effort to deal with sudden and unexpected death.
1891 Dr. Friedrich Maass performed the first equivocally documented chest compression
in humans.
1903 Dr. George Crile reported the first successful use of external chest compressions
in human resuscitation.
1904 The first American case of closed-chest cardiac massage was performed by Dr.
George Crile.
1954 James Elam was the first to prove that expired air was sufficient to maintain
adequate oxygenation.
1956 Peter Safar and James Elam invented mouth-to-mouth resuscitation.
1957 The United States military adopted the mouth-to-mouth resuscitation method to
revive unresponsive victims.
1960 Cardiopulmonary resuscitation (CPR) was developed. The American Heart
Association started a program to acquaint physicians with close-chest cardiac
resuscitation and became the forerunner of CPR training for the general public.
1963 Cardiologist Leonard Scherlis started the American Heart Association's CPR
Committee, and the same year, the American Heart Association formally endorsed CPR.
1966 The National Research Council of the National Academy of Sciences convened an
ad hoc conference on cardiopulmonary resuscitation. The conference was the direct
result of requests from the American National Red Cross and other agencies to establish
standardized training and performance standards for CPR.
1972 Leonard Cobb held the world's first mass citizen training in CPR in Seattle,
Washington called Medic 2. He helped train over 100,000 people the first two years of the
programs.
1981 A program to provide telephone instructions in CPR began in King County,
Washington. The program used emergency dispatchers to give instant directions while
the fire department and EMT personnel were en route to the scene. Dispatcher-assisted
CPR is now standard care for dispatcher centers throughout the United States.
•

Evidenza post
ILCOR 2005
Importanza
delle
compressioni
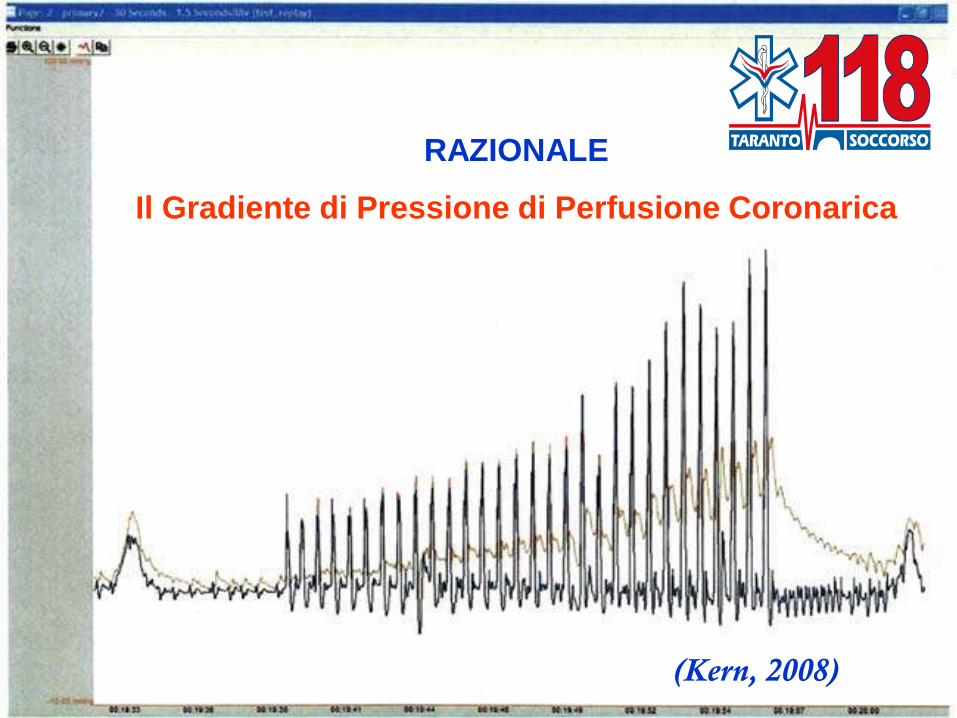
RAZIONALE
Il Gradiente di Pressione di Perfusione Coronarica
(Kern, 2008)
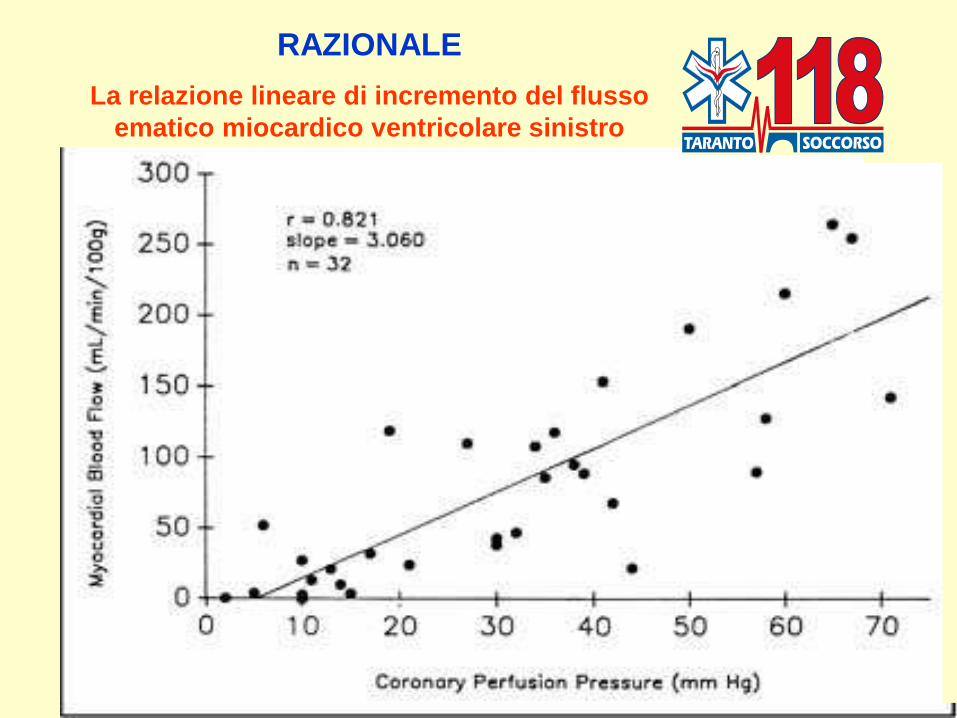
RAZIONALE
La relazione lineare di incremento del flusso
ematico miocardico ventricolare sinistro
Metodologia
di RCP
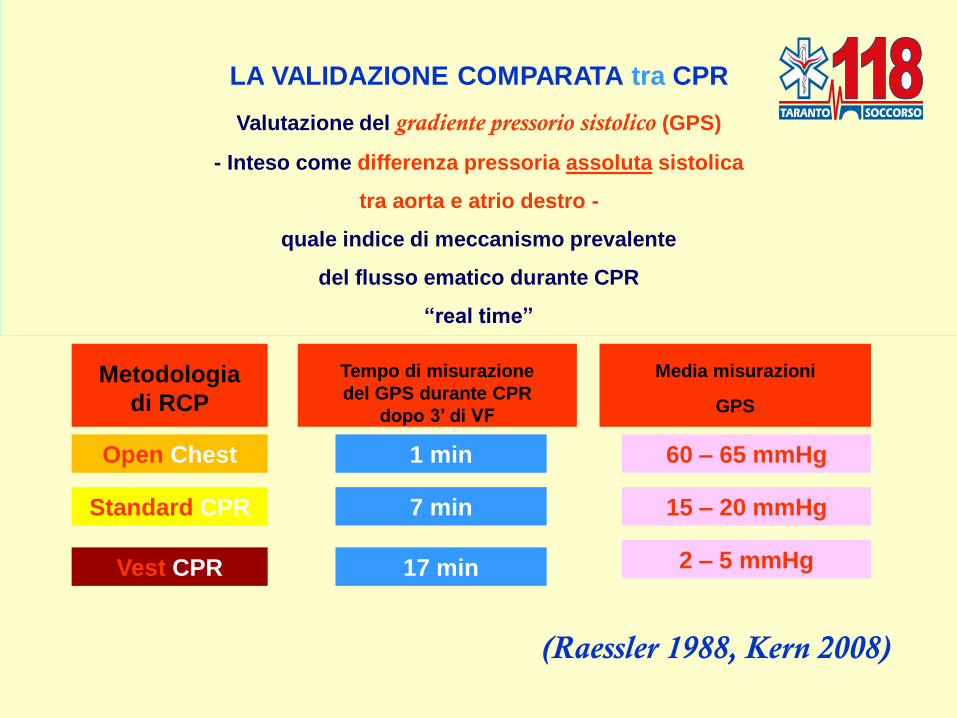
LA VALIDAZIONE COMPARATA tra CPR
Valutazione del gradiente pressorio sistolico (GPS)
- Inteso come differenza pressoria assoluta sistolica
tra aorta e atrio destro -
quale indice di meccanismo prevalente
del flusso ematico durante CPR
“real time”
Open Chest
Standard CPR
Vest CPR
Tempo di misurazione
del GPS durante CPR
dopo 3’ di VF
1 min
7 min
17 min
Media misurazioni
GPS
60 – 65 mmHg
15 – 20 mmHg
2 – 5 mmHg
(Raessler 1988, Kern 2008)
COMPRESSIONI
> Quantità
> Qualità
L’ESIGENZA CONCRETA
SUL CAMPO
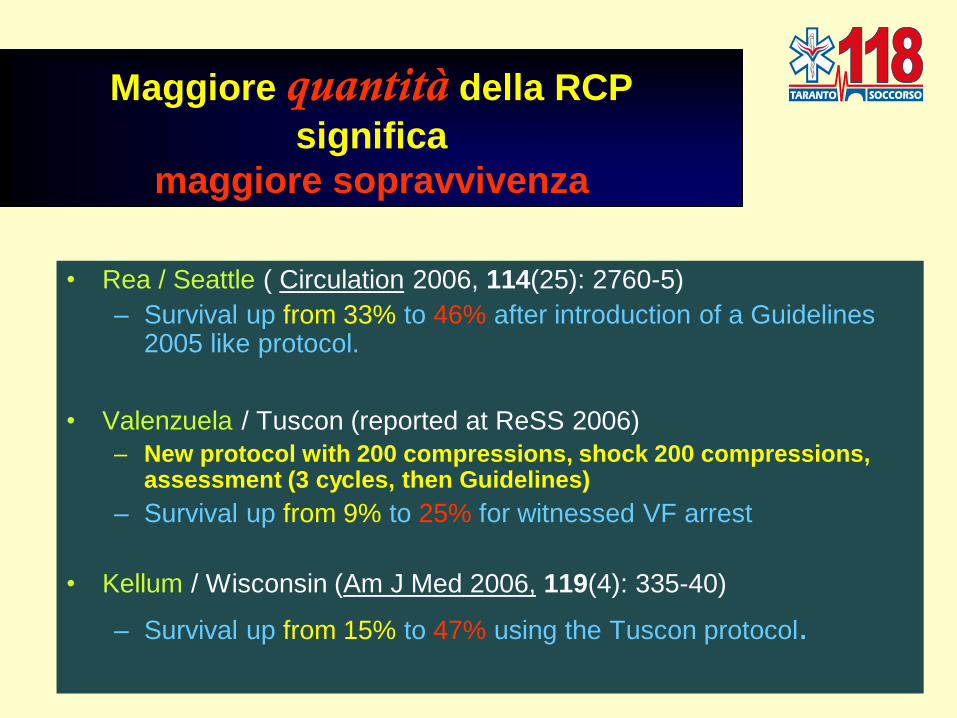
• Rea / Seattle ( Circulation 2006, 114(25): 2760-5)
– Survival up from 33% to 46% after introduction of a Guidelines 2005 like protocol.
• Valenzuela / Tuscon (reported at ReSS 2006)
– New protocol with 200 compressions, shock 200 compressions, assessment (3 cycles, then Guidelines)
– Survival up from 9% to 25% for witnessed VF arrest
• Kellum / Wisconsin (Am J Med 2006, 119(4): 335-40)
– Survival up from 15% to 47% using the Tuscon protocol.
Maggiore quantità della RCP
significa
maggiore sopravvivenza

Van Hoeyweghen. Resuscitation 1993. 3306 patients. Bystander CPR
Good Quality 16% survival Poor Quality 4 % survival
Wik. Resuscitation 1994. 334 patients. Bystander CPR
Good Quality 23% survival Poor Quality 1 % survival
Ko. Resuscitation 2005. 52 patients of witnessed VF arrest. EMS CPR
Good Quality 53% survival Poor Quality 8 % survival
Gallagher. Jama 1995. 2071 patients. Bystander CPR
Good CPR improved discharge rate OR 3.9
Maggiore qualità della RCP
significa
maggiore sopravvivenza

Più RCP
(maggiore Quantità)
+
RCP di Qualità
(maggiore Qualità)
=
Maggiore
Sopravvivenza
RCP di Qualita’: l’Essenziale
Più RCP + HQ - RCP = Maggiore Sopravvivenza
• Comprimi con energia e profondamente (Press Hard)
• Comprimi velocemente (Press Fast)
• Riduci al minimo le interruzioni tra le compressioni
• Rilascia totalmente la pressione tra le compressioni
• Evita l’iperventilazione

Evidenza post ILCOR 2005:
la sopravvivenza sta aumentando
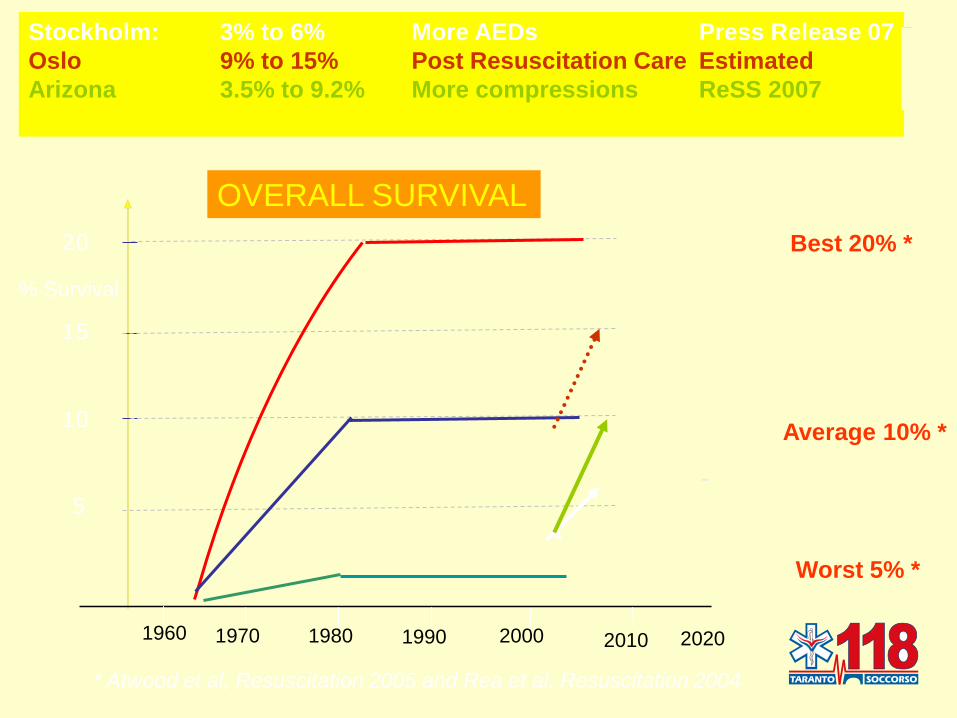
* Atwood et al, Resuscitation 2005 and Rea et al, Resuscitation 2004
Stockholm: 3% to 6% More AEDs Press Release 07
Oslo 9% to 15% Post Resuscitation Care Estimated
Arizona 3.5% to 9.2% More compressions ReSS 2007
% Survival
5
10
15
1970 1980 1990 2000 2010 2020 1960
-
20
Worst 5% *
Average 10% *
Best 20% *
OVERALL SURVIVAL
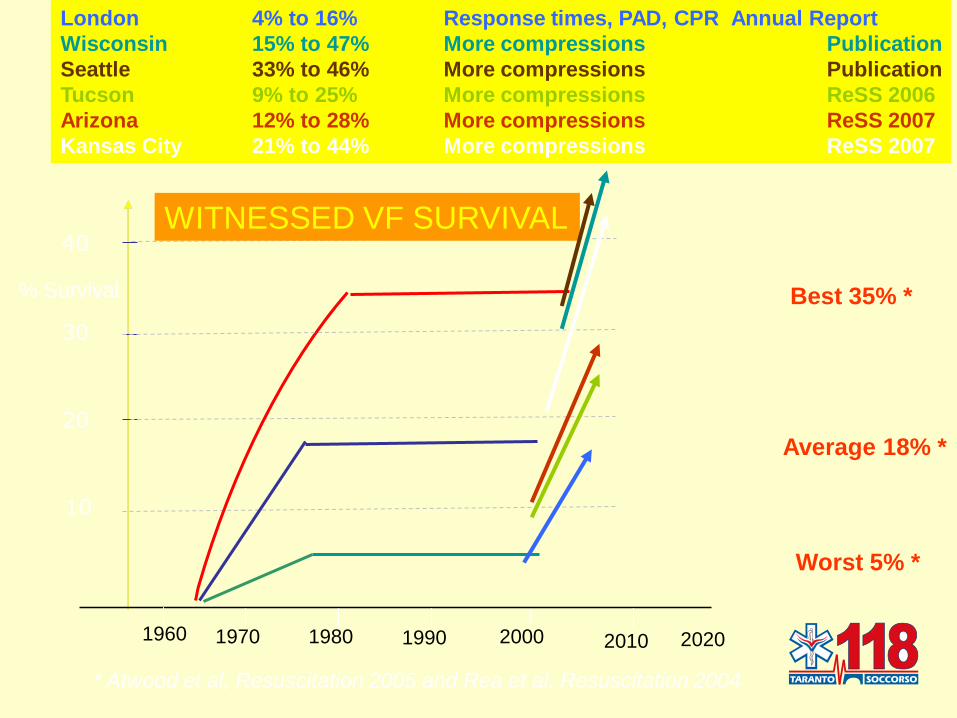
* Atwood et al, Resuscitation 2005 and Rea et al, Resuscitation 2004
London 4% to 16% Response times, PAD, CPR Annual Report
Wisconsin 15% to 47% More compressions Publication
Seattle 33% to 46% More compressions Publication
Tucson 9% to 25% More compressions ReSS 2006
Arizona 12% to 28% More compressions ReSS 2007
Kansas City 21% to 44% More compressions ReSS 2007
% Survival
10
20
30
1970 1980 1990 2000 2010 2020 1960
40
Worst 5% *
Average 18% *
Best 35% *
WITNESSED VF SURVIVAL
Minimal Chest Compression
Interruption Bobrow et al. Arizona (AHA ReSS 2007 & JAMA March 2008)
MICR objectives:
Immediate pre-shock chest compression
Delay or eliminate Endotracheal intubation
Minimize Positive Pressure Ventilation
Decrease the time to intravenous Epinephrine
Two metropolitan cities in Arizona: EMS trained to MICR protocol (one training)
Treatment intervention: 600 continuous chest compressions, only interrupted for
shocks every 200 compressions.
Patients had some ventilation (BVM or oro-pharyngeal airway)
61 % of patient after training met all 4 MIRC criteria.
2460 patients, MICR protocol compliance, survival was 9.1% vs 3.8% earlier; CI: 95%
528 patients witnessed VF + MICR protocol 28.4% vs 11.9% earlier; CI: 95%
More chest compression
Less defibrillation and ventilation
Garza et al. Kansas City
Treatment intervention: • minimizing interruptions of chest compression
• using a 50:2 compression\ ventilation ratio
• Chest compression prior to defibrillation
• deemphasizing and delaying intubation
Result: Survival doubled for VF witnessed arrests
From 21.3% to 44.3% (p<0.01)
(presume vs previous Guidelines, 5: 1)
Why do Chest compressions aid delayed defibrillation? Douglas Chamberlain, Michael Frenneaux, Stig Steen, Andrew Smith,
Resuscitation 2008, Commentary
• Haemodynamic factors as important as the Metabolic factors in Cardiac arrest
• Support the Three Phase model (Weisfeldt, Abella; JAMA 2002) – The Electrical Phase … (0-4 min.)
– The Circulatory Phase (4-10 min.)
– The Metabolic Phase (> 10 min.)
• Changes in the size and shape of the ventricles are the most important reason for the
narrow window of opportunity for defibrillation alone and for the value of
compressions in extending this period.
– Dilatation of Right Ventricle during Cardiac Arrest leading intra-pericardial pressure to increase rapidly.
– Coronary artery pressure is negative first minutes of chest compressions because peak Right Atrial
pressure exceeds peak Aortic pressure
– Brief periods of Chest compressions can unlikely improve outcome, > 90 seconds of continues
chests compressions can improve outcome.
• AHA guidelines recommend healthcare professionals should continue compressions during
charging of a defibrillator, but — controversially — the ERC guidelines do not. We believe that
the European position should be reconsidered as a matter of urgency.
D. Chaimberlain et al. Resuscitation 2008
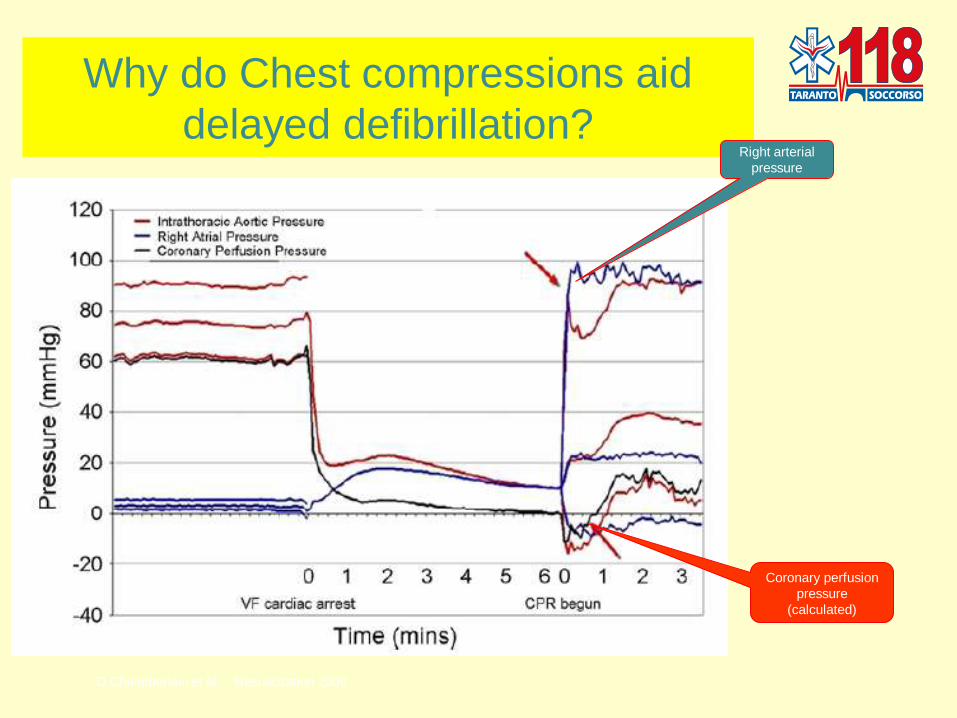
Why do Chest compressions aid
delayed defibrillation?
D.Chaimberlain et al. Resuscitation 2008
Coronary perfusion
pressure
(calculated)
Right arterial
pressure
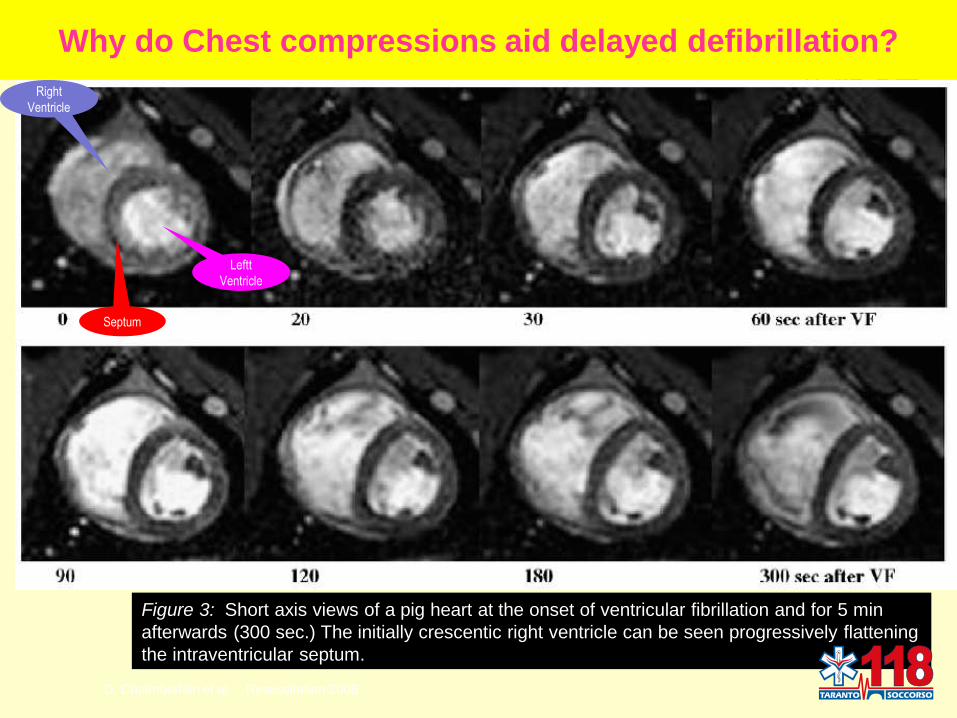
Why do Chest compressions aid delayed defibrillation?
D. Chaimberlain et al. Resuscitation 2008
Figure 3: Short axis views of a pig heart at the onset of ventricular fibrillation and for 5 min
afterwards (300 sec.) The initially crescentic right ventricle can be seen progressively flattening
the intraventricular septum.
Right
Ventricle
Leftt
Ventricle
Septum
The Challenge of CPR Quality:
Improvement in the real world Leary & Abella, Resuscitation March 2008, Editorial
• CPR Quality vary significant in clinical practice.
• Long intervals between CPR performances & trainings
• Inadequate training strategies.
• Discomfort w/CPR.
• Rescuer fatigue.
• Difficult to recognize performance error.
• Compression depth decline over time.
• Need more research on
– Time management.
– Human factors.
– Leadership quality.
• New technology may play important roles.
• CPR Quality is likely to be required for effective pharmalogic interventions.
• Need agreement on how CPR quality to be reported and compared.

Quali novità ?
2010

Bobrow 2008, Mirza 2008, Berdowsky 2009
A
B
C
C
A
B
?
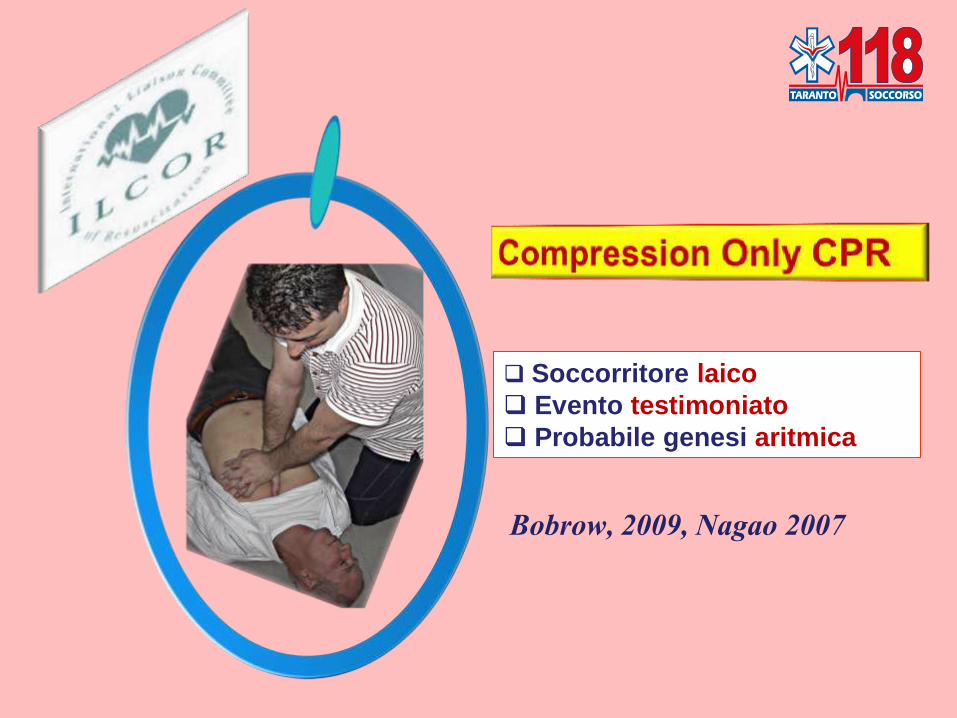
Soccorritore laico
Evento testimoniato
Probabile genesi aritmica
Bobrow, 2009, Nagao 2007

Soccorritore addestrato
Evento testimoniato
Probabile genesi aritmica
Kellum 2006, Heidenreich 2006

Soccorritore addestrato
Evento non testimoniato
Probabile genesi asfittica
Qualunque arresto dopo 6 –
8 minuti
Kelley 2006, Williams 2006
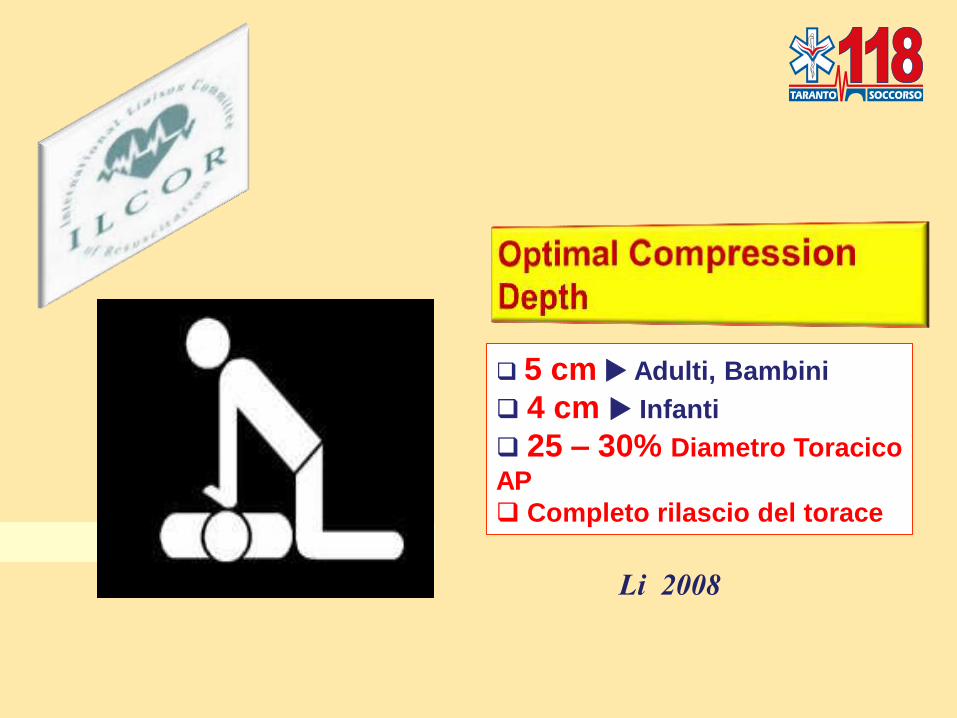
5 cm Adulti, Bambini
4 cm Infanti
25 – 30% Diametro Toracico
AP
Completo rilascio del torace
Li 2008
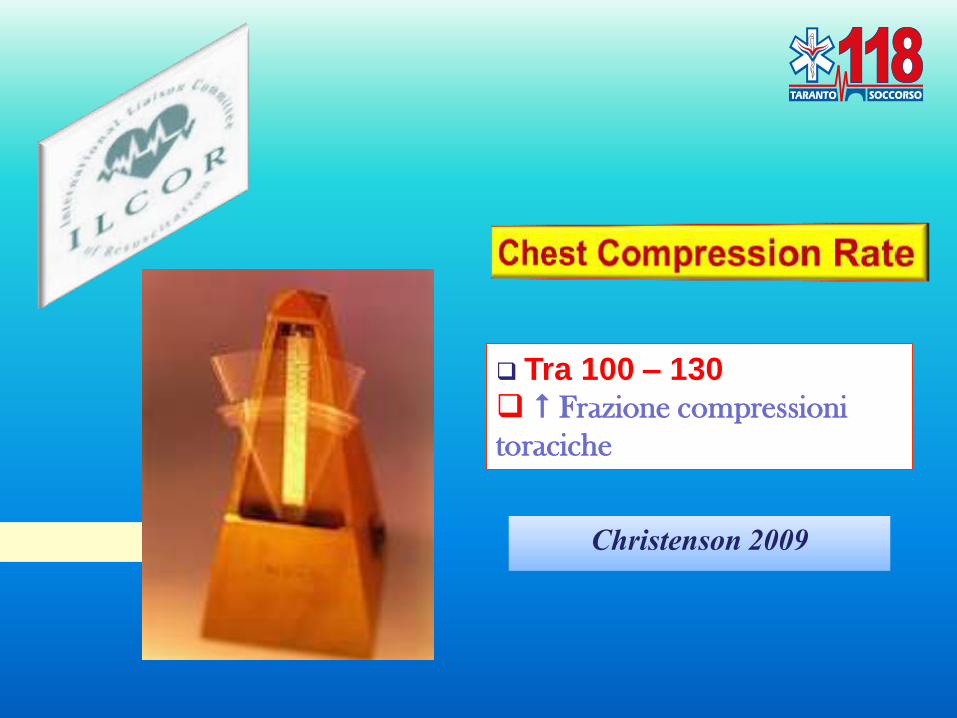
Tra 100 – 130 Frazione compressioni
toraciche
Christenson 2009
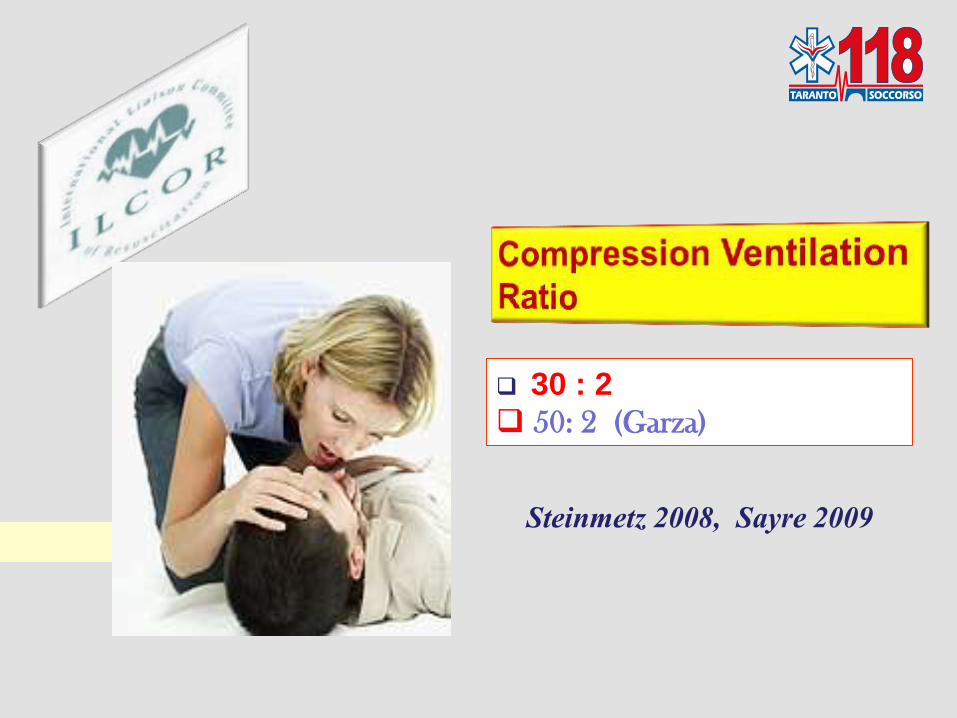
30 : 2 50: 2 (Garza)
Steinmetz 2008, Sayre 2009
Support the Three Phase model (Weisfeldt, Abella;
JAMA 2002)
The Electrical Phase … (0-4 min.)
The Circulatory Phase (4-10 min.)
The Metabolic Phase (> 10 min.)
Evidenze in equilibrio
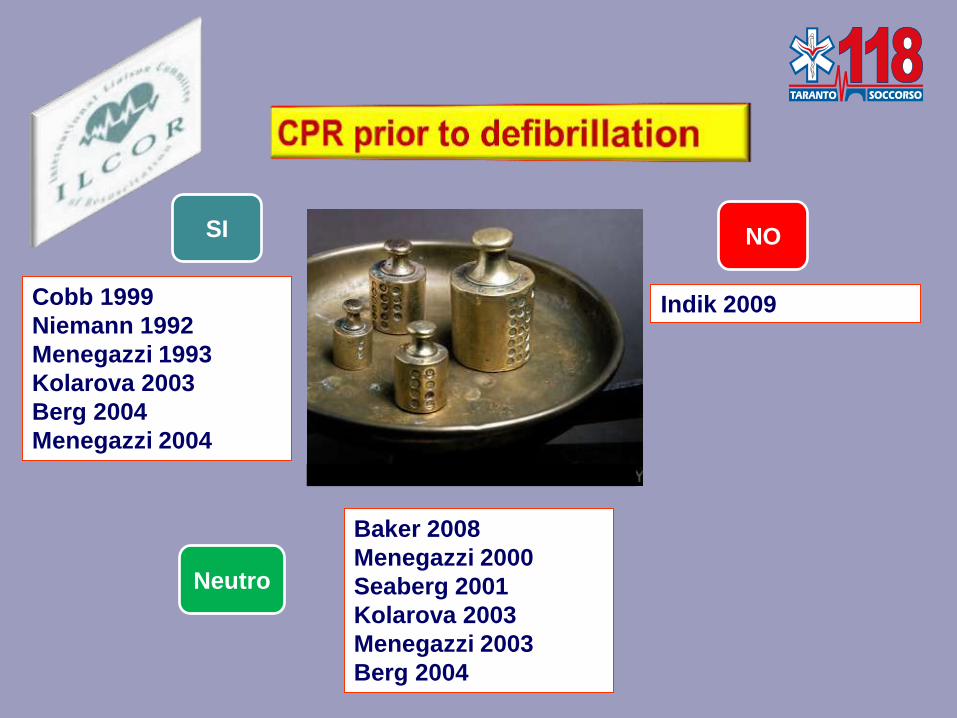
Cobb 1999
Niemann 1992
Menegazzi 1993
Kolarova 2003
Berg 2004
Menegazzi 2004
Indik 2009
Baker 2008
Menegazzi 2000
Seaberg 2001
Kolarova 2003
Menegazzi 2003
Berg 2004
SI NO
Neutro
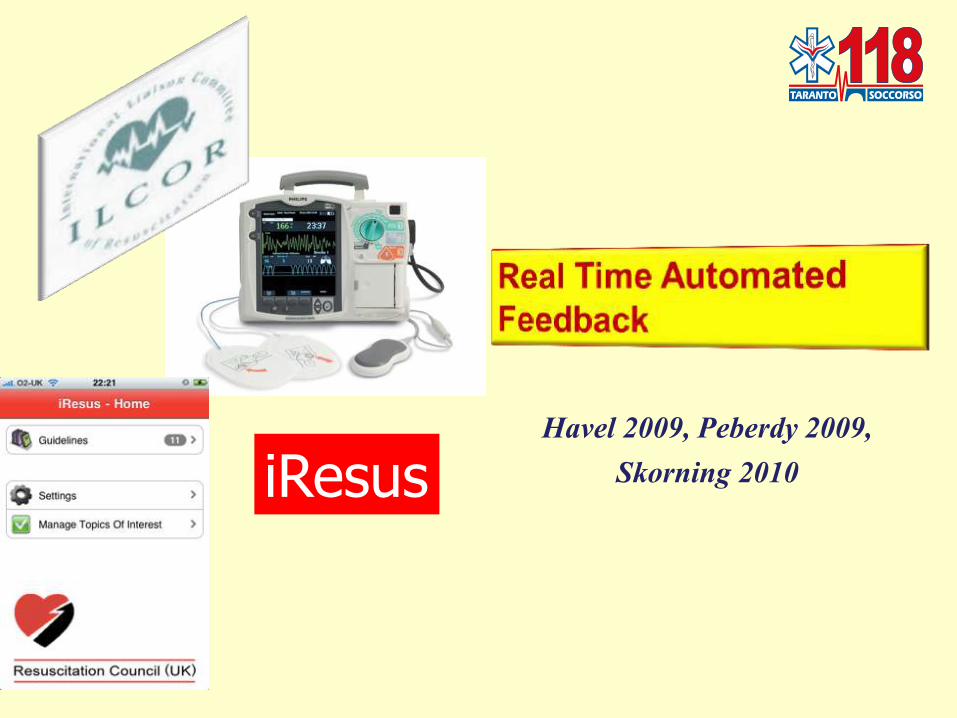
Havel 2009, Peberdy 2009, Skorning 2010 iResus

“However, there are no studies to date that
demonstrate a significant improvement in
patient survival related to the use of CPR
feedback devices during actual cardiac arrest
events.”
Circulation, November 2, 2010, Part 5, S697

RCP
ILCOR 2005
La nostra
esperienza
attuale

REKEDA Study
Resuscitation Key Data
Studio Sull’ArreSto CArdiACo
Improvviso
Preospedaliero
Sistema 118 - Taranto Direttore
Dr Mario Balzanelli

Arresto Cardiaco Improvviso
Preospedaliero
Totale Arresti Cardiaci Improvvisi (ACI)
Provincia di Taranto
considerati dallo studio nel periodo
Agosto 2006 – Ottobre 2010
919

Arresto Cardiaco Improvviso
Preospedaliero
Incidenza annuale
Arresti Cardiaci Improvvisi
Provincia di Taranto calcolata su periodo
Agosto 2006 – Ottobre 2010
0,36 /1000 abitanti

Arresto Cardiaco Improvviso
Preospedaliero
Totale Rianimazioni
tentate
Agosto 2006 – Ottobre 2010
578
62.8% degli ACI totali
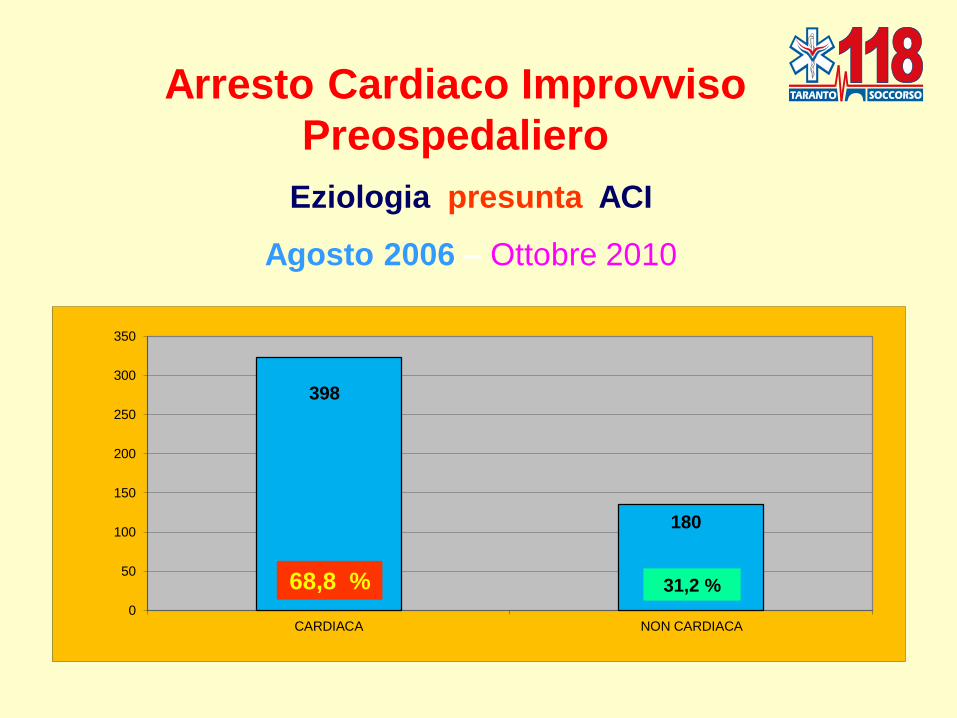
Arresto Cardiaco Improvviso
Preospedaliero
Eziologia presunta ACI
Agosto 2006 – Ottobre 2010
398
180
0
50
100
150
200
250
300
350
CARDIACA NON CARDIACA
68,8 % 31,2 %

Arresto Cardiaco Improvviso
Preospedaliero
Totale ACI Testimoniati – non Testimoniati
Agosto 2006 – Ottobre 2010
357
221
0
50
100
150
200
250
300
350
TESTIMONIATI NON TESTIMONIATI
61,7% 38,3 %
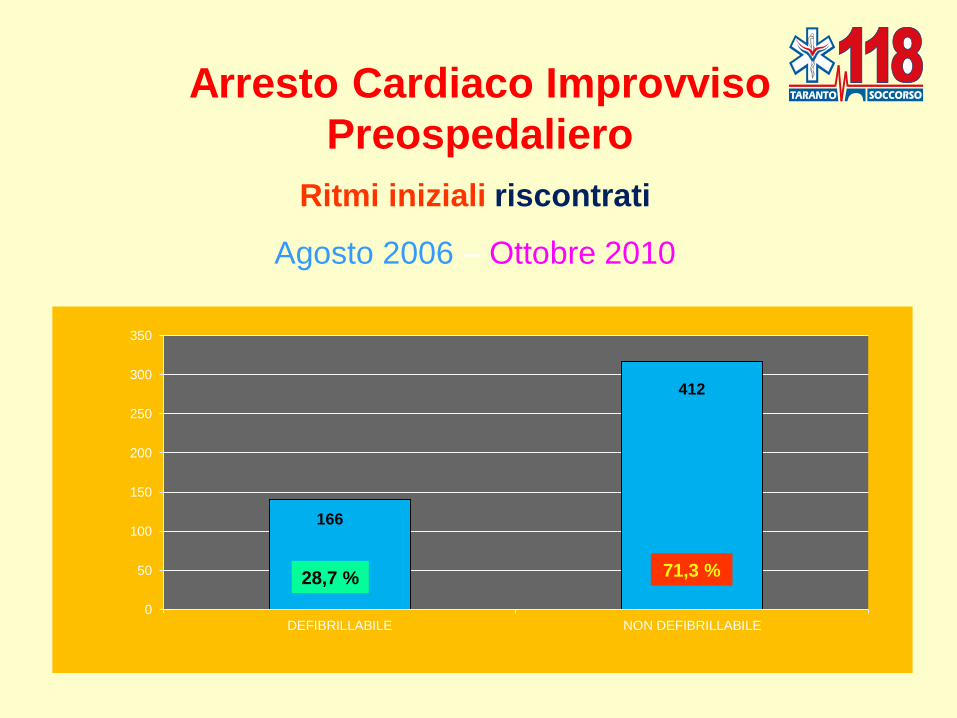
Ritmi iniziali riscontrati
Agosto 2006 – Ottobre 2010
Arresto Cardiaco Improvviso
Preospedaliero
0
50
100
150
200
250
300
350
DEFIBRILLABILE NON DEFIBRILLABILE
166
412
28,7 % 71,3 %
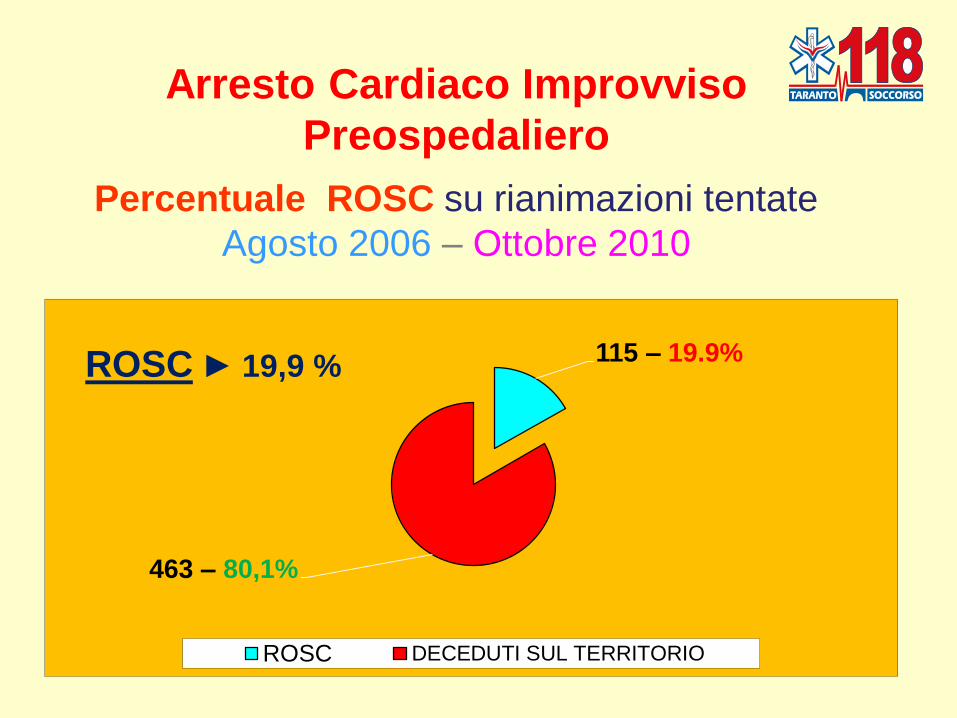
Arresto Cardiaco Improvviso
Preospedaliero
Percentuale ROSC su rianimazioni tentate
Agosto 2006 – Ottobre 2010
115 – 19.9%
463 – 80,1%
ROSC DECEDUTI SUL TERRITORIO
ROSC ► 19,9 %

Arresto Cardiaco Improvviso
Preospedaliero
Tempi medi di arrivo su ROSC per periodo
Agosto 2006 - Ottobre 2010
0
2
4
6
8
10
12
8.14
9.7 10.5
8.1
9.8

9.24 min
Arresto Cardiaco Improvviso
Preospedaliero documentati
Tempi medio di arrivo su totale ROSC
periodo AGOSTO 2006 – OTTOBRE 2010

Arresto Cardiaco Improvviso
Preospedaliero
Dimessi vivi senza esiti neurologici invalidanti
sui ROSC
PERIODO
AGOSTO 2006 – OTTOBRE 2010
48
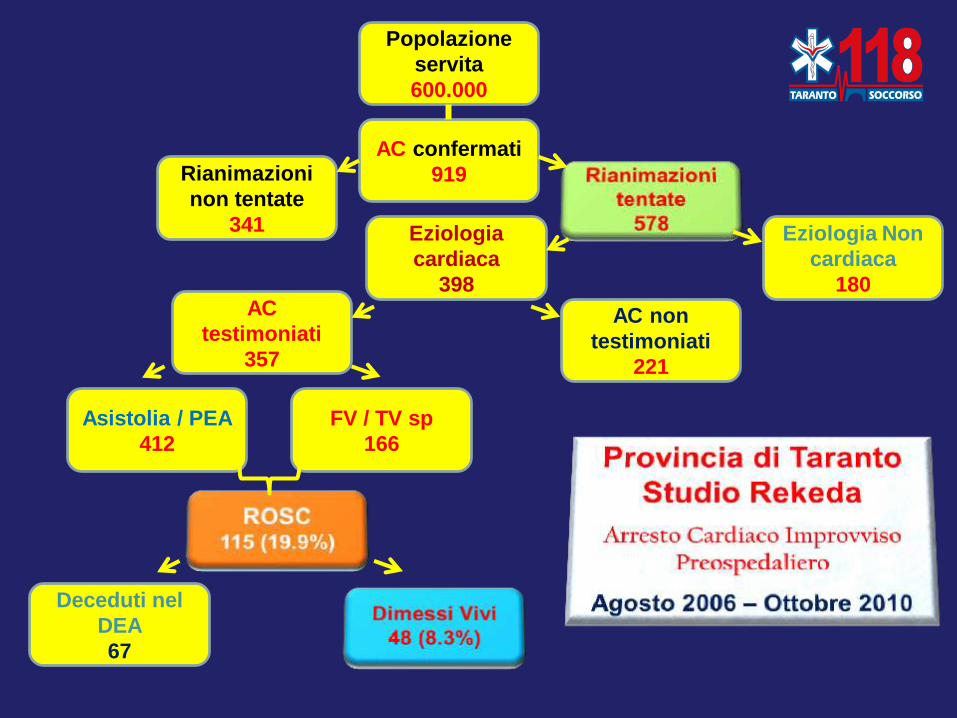
Popolazione
servita
600.000
AC confermati
919 Rianimazioni
non tentate
341 Eziologia
cardiaca
398
Eziologia Non
cardiaca
180 AC
testimoniati
357
AC non
testimoniati
221
Asistolia / PEA
412
FV / TV sp
166
Deceduti nel
DEA
67
48 Pazienti dimessi vivi
SU 115 rosc
Su totale rianimazioni documentate

RCP di Qualità
La nostra
esperienza
nuova
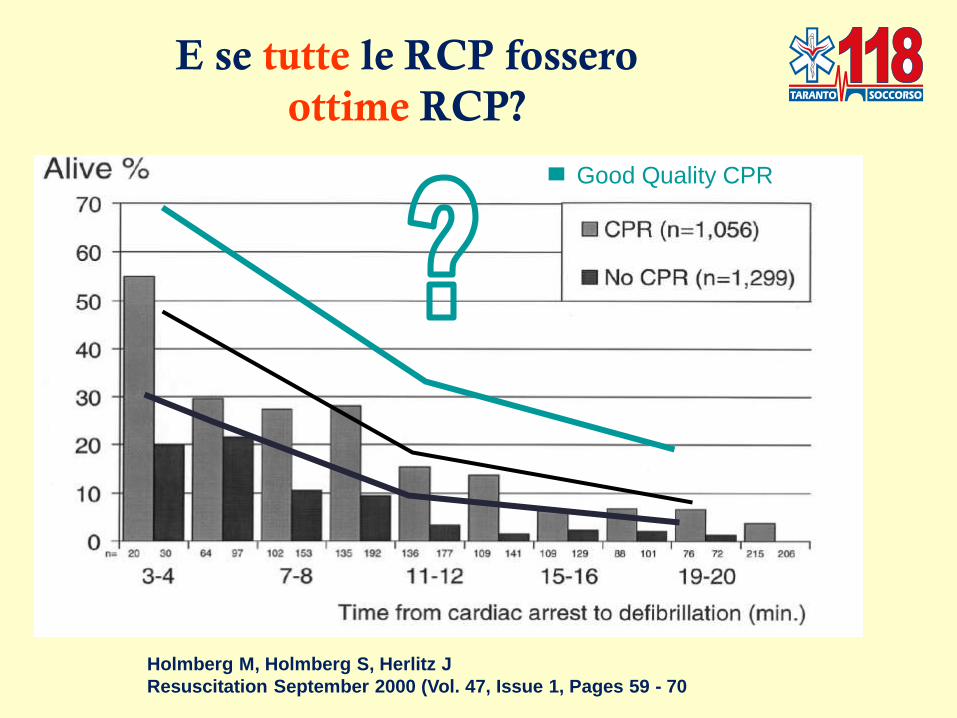
E se tutte le RCP fossero
ottime RCP?
Holmberg M, Holmberg S, Herlitz J
Resuscitation September 2000 (Vol. 47, Issue 1, Pages 59 - 70
▄ Good Quality CPR
Settembre 2007
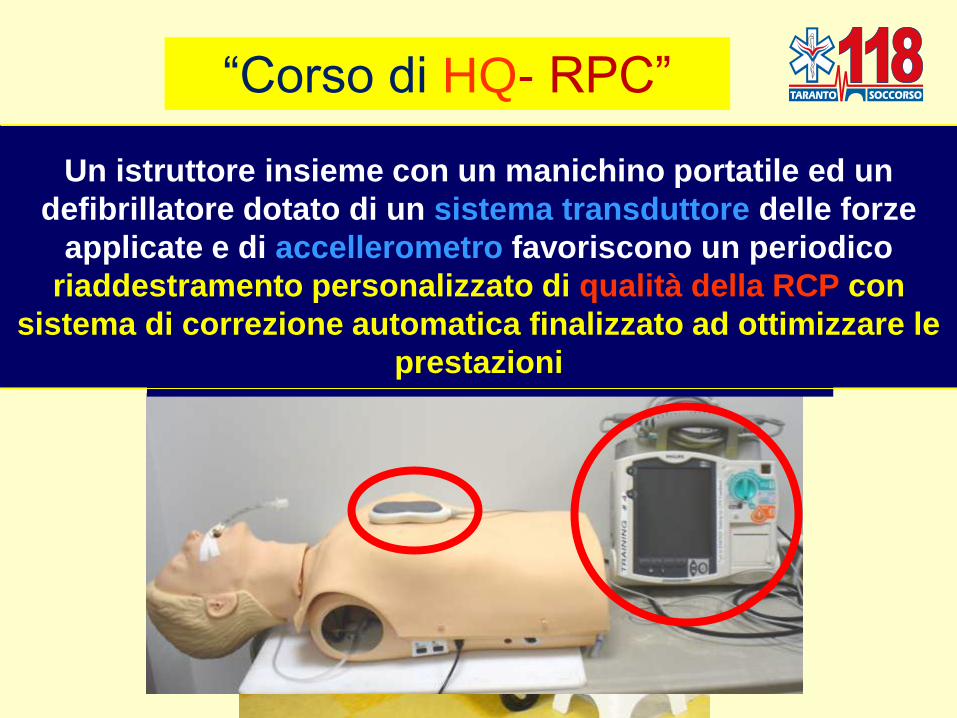
―Corso di HQ- RPC‖
Un istruttore insieme con un manichino portatile ed
un defibrillatore dotato di un sistema transduttore
delle forze applicate e di accellerometro favorisce un
riaddestramento personalizzato di qualità della RCP
con sistema di correzione automatica finalizzato ad
Un istruttore insieme con un manichino portatile ed un
defibrillatore dotato di un sistema transduttore delle forze
applicate e di accellerometro favoriscono un periodico
riaddestramento personalizzato di qualità della RCP con
sistema di correzione automatica finalizzato ad ottimizzare le
prestazioni

Misurazione della Compressione
Cosa fa il sensore… • Rileva il movimento utilizzando un accelerometro • Rileva la forza utilizzando un trasduttore di forza
Sensore di Compressione

Misurazione della Compressione
• La frequenza di compressione è una media mobile delle ultime 5 compressioni • La profondità da raggiungere è di 4 ÷ 5 cm indicati dalle linee • Il rilascio incompleto (“Appoggiarsi”) è indicato da un “*” sulla linea d’onda

Misurazione della Compressione
Sensore di Compressione
Misurazioni:
• Profondità della compressione • Frequenza delle Compressioni • Appoggiarsi (rilascio incompleto) • Duty Cycle (durata) • Periodo di Assenza del flusso (timer di inattività) Placca adesiva del Sensore
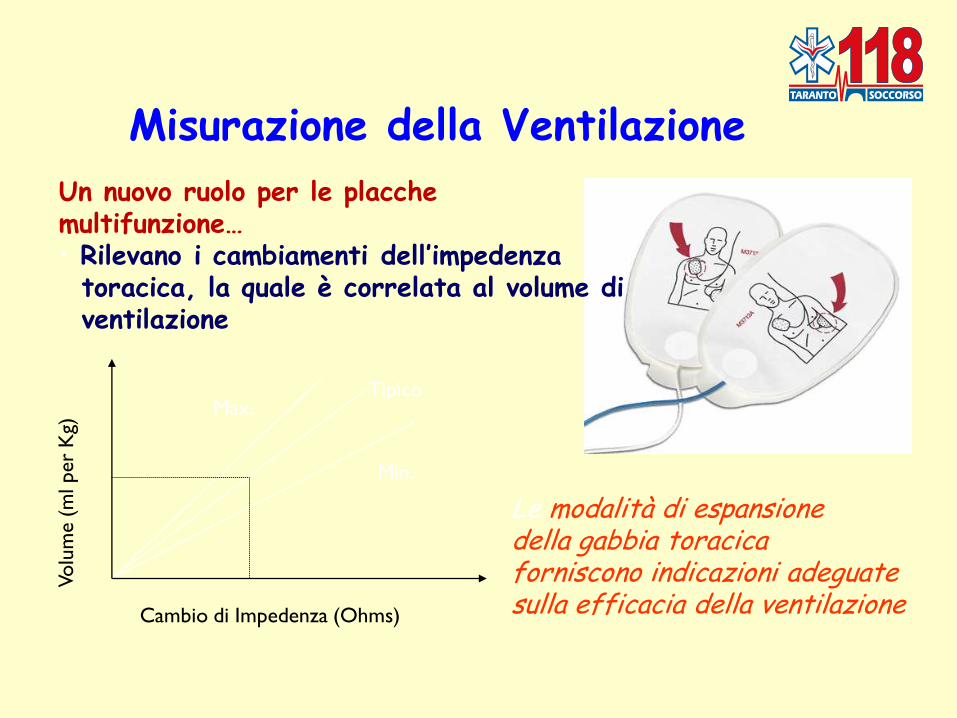
Misurazione della Ventilazione
Un nuovo ruolo per le placche multifunzione… • Rilevano i cambiamenti dell’impedenza toracica, la quale è correlata al volume di ventilazione
Min.
Max. Tipico
Cambio di Impedenza (Ohms)
Volu
me (
ml per
Kg)
Le modalità di espansione della gabbia toracica forniscono indicazioni adeguate sulla efficacia della ventilazione

Misurazione della Ventilazione
• La frequenza di ventilazione è una media mobile delle ultime 4 ventilazioni • L’icona del volume di ventilazione mostra 0, 1/3, 2/3 oppure 1+ del volume obiettivo • Timer di inattività -- “30 Secondi senza ventilazione”
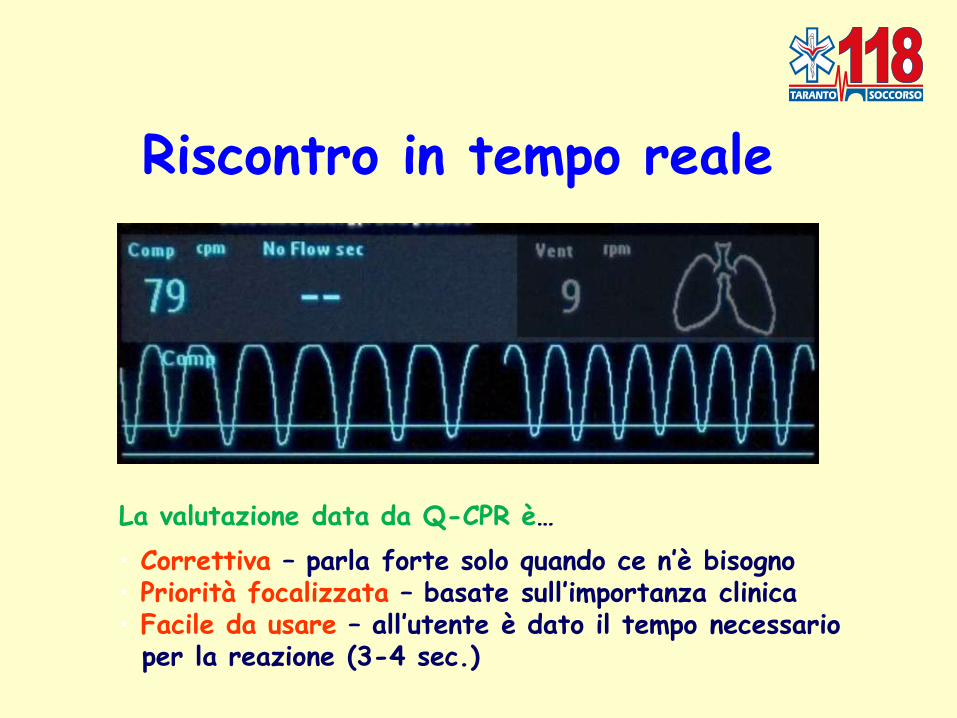
Riscontro in tempo reale
La valutazione data da Q-CPR è…
• Correttiva – parla forte solo quando ce n’è bisogno • Priorità focalizzata – basate sull’importanza clinica • Facile da usare – all’utente è dato il tempo necessario per la reazione (3-4 sec.)
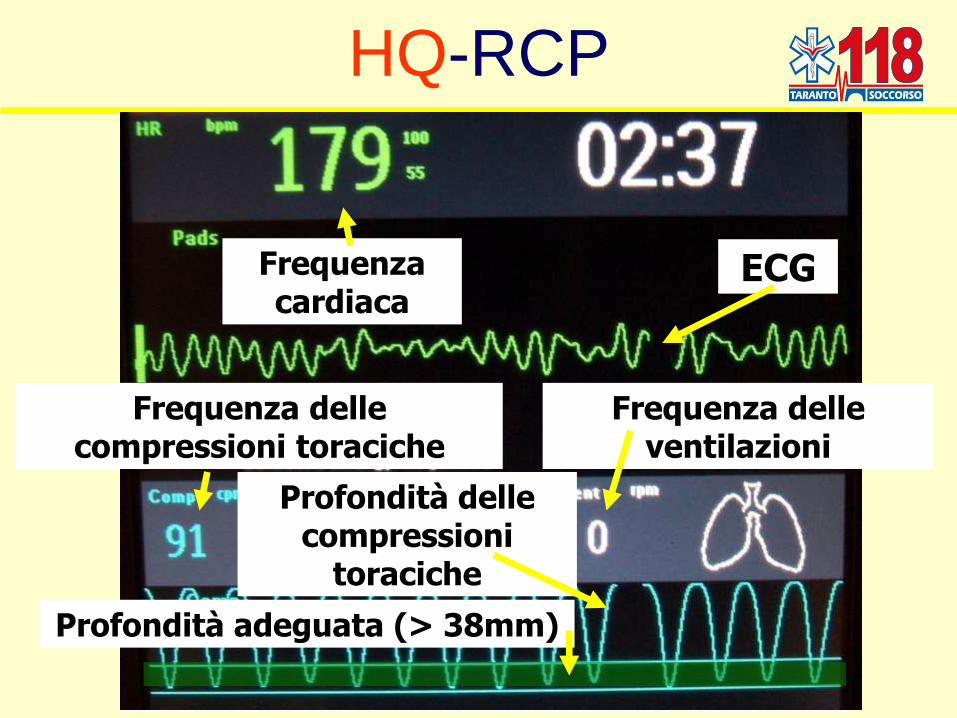
HQ-RCP
Frequenza delle compressioni toraciche
Frequenza delle ventilazioni
Frequenza cardiaca
ECG
Profondità delle compressioni
toraciche
Profondità adeguata (> 38mm)
RICERCA

SI COLMA
LA DIFFERENZA TRA
VIRTUALE
Aula
Perfezionamento
continuo
della didattica
REALE
Paziente
Perfezionamento
continuo
della gestione clinica
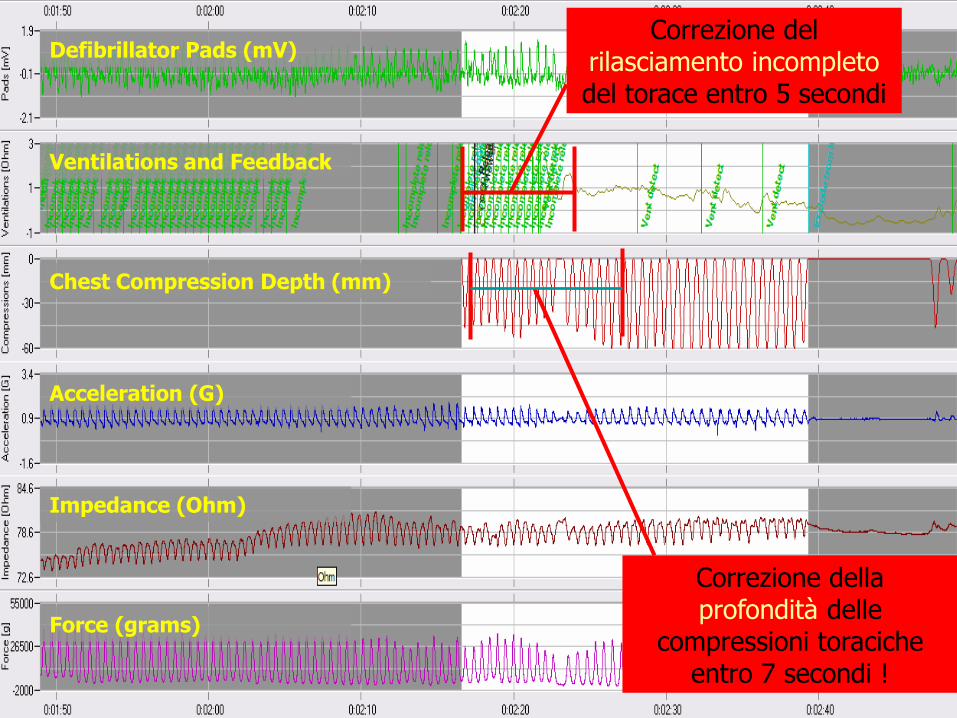
Correzione del rilasciamento incompleto del torace entro 5 secondi
Correzione della profondità delle
compressioni toraciche entro 7 secondi !
Defibrillator Pads (mV)
Ventilations and Feedback
Chest Compression Depth (mm)
Acceleration (G)
Impedance (Ohm)
Force (grams)

5° CONGRESSO
NAZIONALE
Società Italiana
Sistema 118
Presidente: Dott. Pietro Golino
Responsabile Centrale Operativa 118 di
Cagliari
Vice Presidente: Dott. Piero Delogu
Responsabile Centrale Operativa 118 di
Sassari
Cagliari
12 - 14 ottobre 2007
• Durata: 5 ore
• Rapporto docente / discenti ► 1 / 15
• Teoria: 1 ora
• Addestramento: 2 ore e 45 minuti
• Pausa: 30 minuti
• Verifica: 45 minuti
Corso di HQ - RCP
HQ - CPR
Gennaio 2008 –
Dicembre 2009 ►
200 operatori
Operatori addestrati
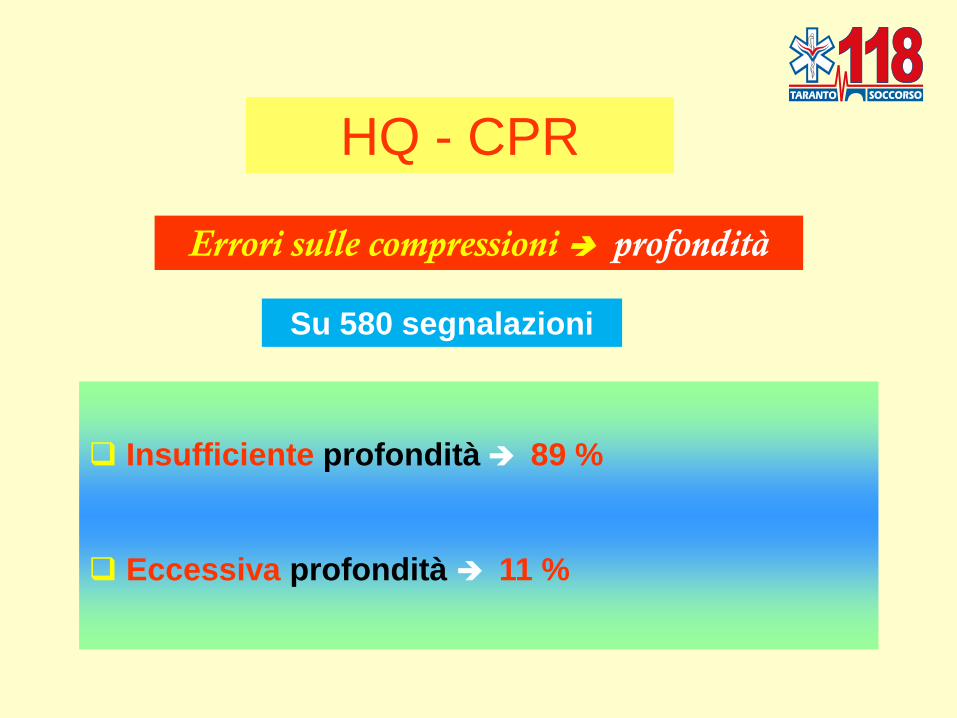
HQ - CPR
Errori sulle compressioni profondità
Insufficiente profondità 89 %
Eccessiva profondità 11 %
Su 580 segnalazioni
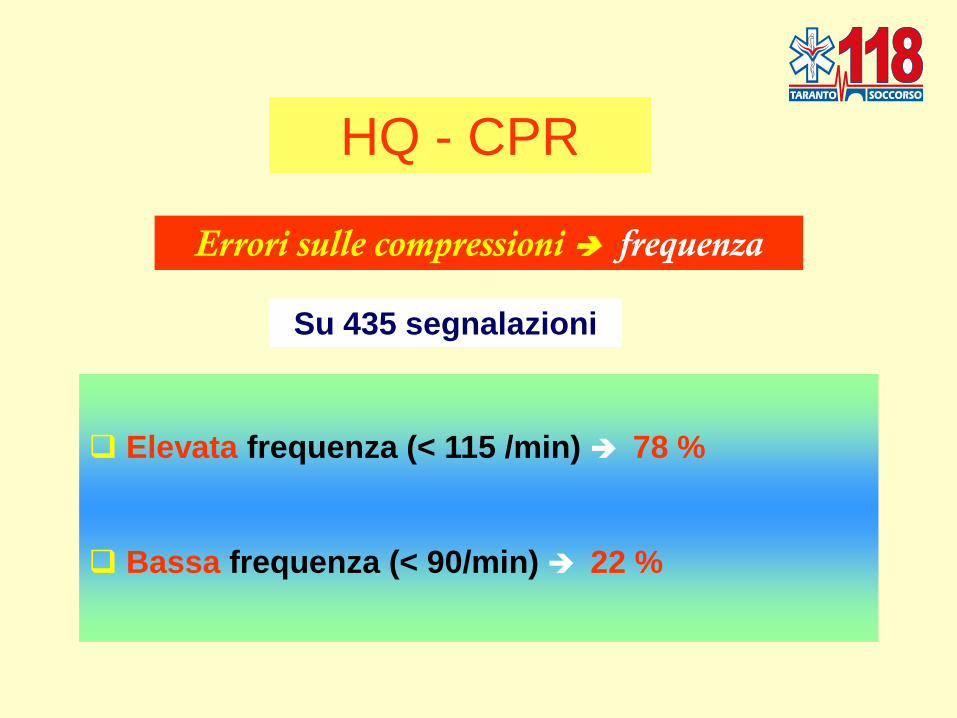
HQ - CPR
Errori sulle compressioni frequenza
Elevata frequenza (< 115 /min) 78 %
Bassa frequenza (< 90/min) 22 %
Su 435 segnalazioni
HQ - CPR
Errori sulle ventilazioni volume di ventilazione
Insufficiente 77 %
Eccessiva 23 %
Su 220 segnalazioni

Media percentuale di miglioramento
sulla esecuzione delle compressioni toraciche
alla ripetizione del corso
38% Alla 2^ sessione
Alla 3^ sessione 74%
Alla 4^ sessione 94%

Media percentuale di miglioramento
sulla esecuzione delle ventilazioni
alla ripetizione del corso
69 % Alla 2^ sessione
Alla 3^ sessione 100 %
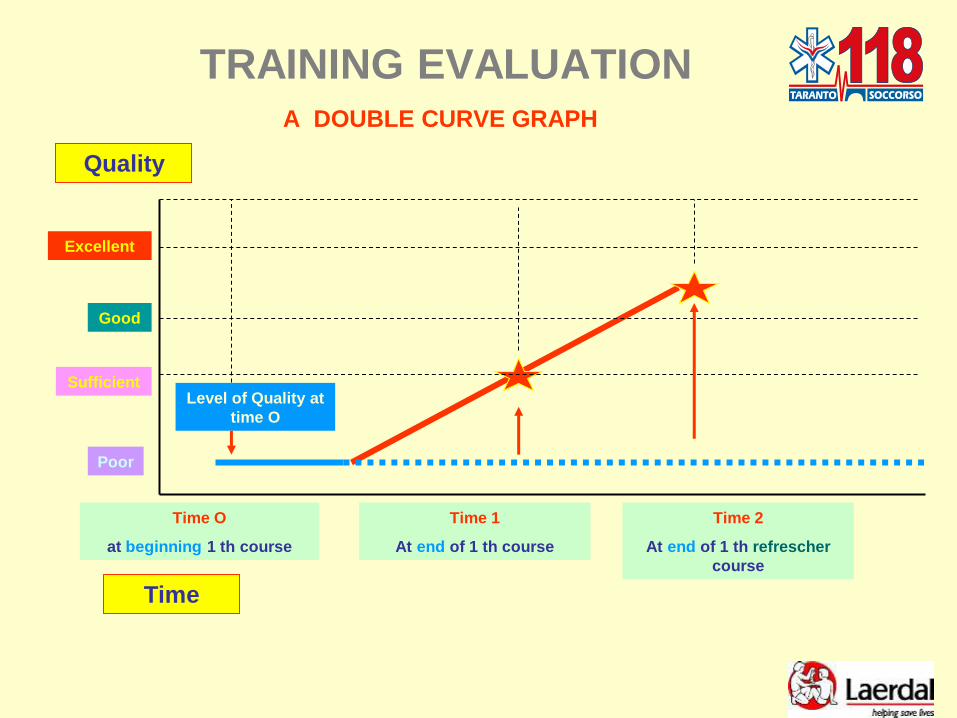
TRAINING EVALUATION A DOUBLE CURVE GRAPH
Time
Quality
Time O
at beginning 1 th course
Time 1
At end of 1 th course
Level of Quality at
time O
Poor
Good
Excellent
Sufficient
Time 2
At end of 1 th refrescher
course

E sul paziente ?
Pur con limitazioni prospettiche e doverose cautele valutative:
- Primi due anni di sperimentazione HQ - CPR in fase didattica
- Mancata sperimentazione HQ - CPR sulla scena
- Differente peso statistico del campione schede anno 2008 - 2010 (n° 301) rispetto periodo anni 2006 – 2007 (n° 277)

Primi risultati incoraggianti
a partire dalla fase di avvio
dei corsi di HQ - RCP

Nel periodo gennaio 2008 – ottobre 2010
rispetto al periodo
agosto 2006 – dicembre 2007

ROSC su rianimazioni tentate + 7 %
Dimessi vivi su rianimazioni tentate + 3,5 %
Dimessi vivi su ROSC + 2,8 %

Dimessi vivi / ROSC pre HQ-
CPR (18/ 45) 40% (agosto 2006- anno 2007)
Dimessi vivi / ROSC post
HQ-CPR (30/ 70) 42.8% (anno 2008 - anno 2009 - anno 2010 )
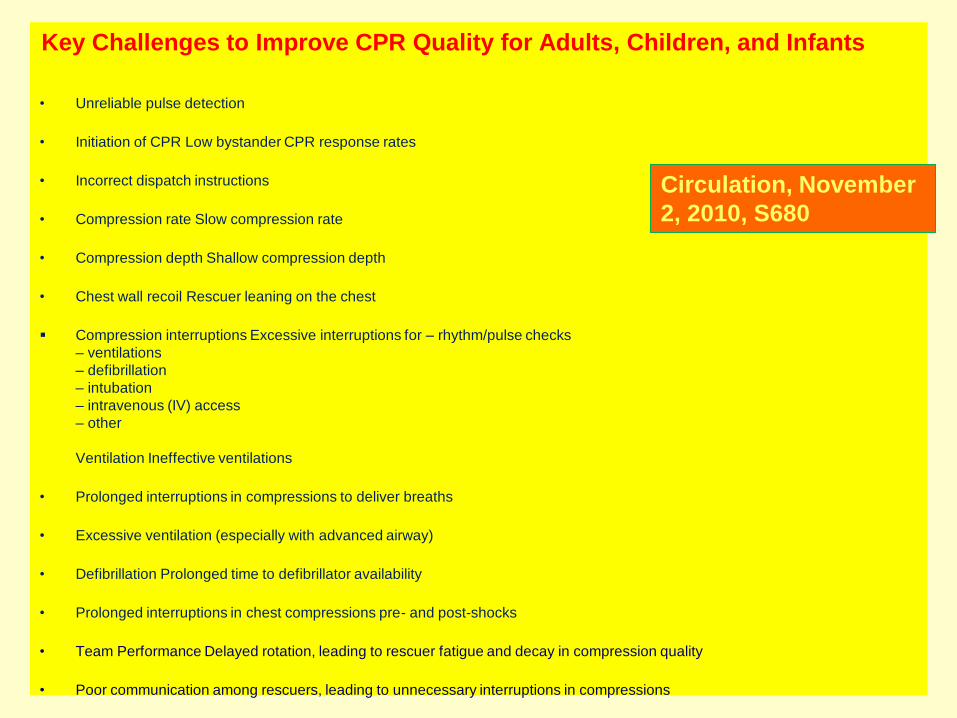
Key Challenges to Improve CPR Quality for Adults, Children, and Infants
• Unreliable pulse detection
• Initiation of CPR Low bystander CPR response rates
• Incorrect dispatch instructions
• Compression rate Slow compression rate
• Compression depth Shallow compression depth
• Chest wall recoil Rescuer leaning on the chest
Compression interruptions Excessive interruptions for – rhythm/pulse checks
– ventilations
– defibrillation
– intubation
– intravenous (IV) access
– other
Ventilation Ineffective ventilations
• Prolonged interruptions in compressions to deliver breaths
• Excessive ventilation (especially with advanced airway)
• Defibrillation Prolonged time to defibrillator availability
• Prolonged interruptions in chest compressions pre- and post-shocks
• Team Performance Delayed rotation, leading to rescuer fatigue and decay in compression quality
• Poor communication among rescuers, leading to unnecessary interruptions in compressions
Circulation, November
2, 2010, S680

HQ – CPR una risorsa
indispensabile per il pieno
recupero delle funzioni
neurologiche del paziente e,
quindi, non solo della sua
vita quanto, più ancora,
della sua qualità di vita.
Oltre la sopravvivenza,
per una vita ancora vera



Grazie