
LA NUTRIZIONE ARTIFICIALE DOMICILIARE: LUCI E...
32
LA NUTRIZIONE ARTIFICIALE DOMICILIARE: LUCI E OMBRE PAOLO COTOGNI SC Terapia del Dolore e Cure Palliative Dipartimento di Anestesia e Rianimazione AOU Città della Salute e della Scienza Università di Torino
Transcript of LA NUTRIZIONE ARTIFICIALE DOMICILIARE: LUCI E...

LA NUTRIZIONE ARTIFICIALE
DOMICILIARE:
LUCI E OMBRE
PAOLO COTOGNI
SC Terapia del Dolore e Cure Palliative
Dipartimento di Anestesia e Rianimazione
AOU Città della Salute e della Scienza
Università di Torino

2

3
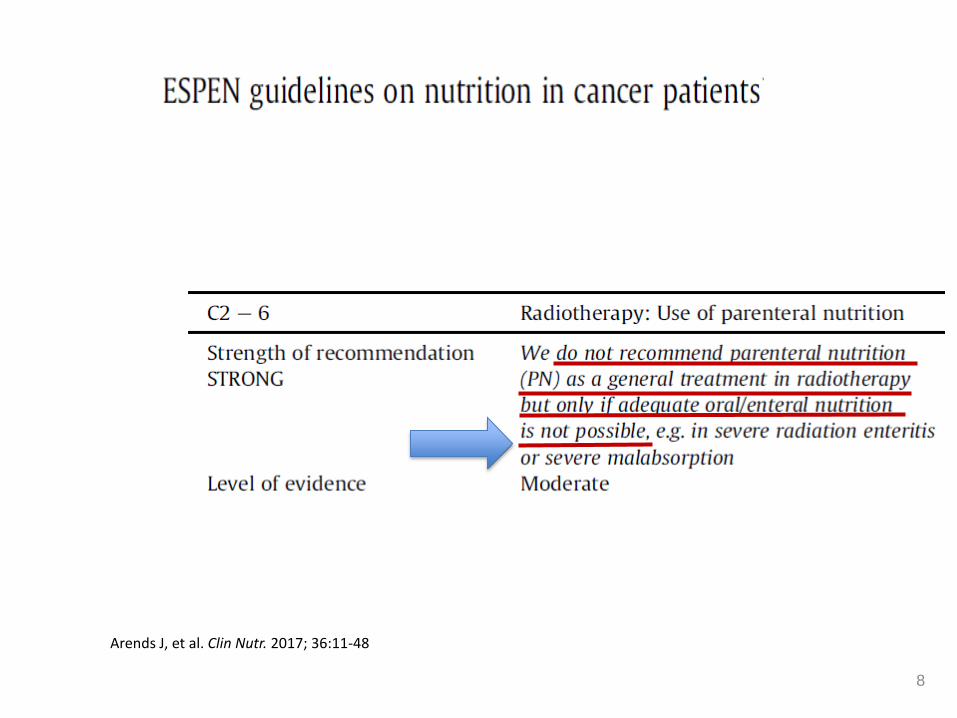
Arends J, et al. Clin Nutr. 2017; 36:11-48

Arends J, et al. Clin Nutr. 2017; 36:11-48
4
VS.
5
Old Misunderstanding
EN PN
Cotogni P. Ann Palliat Med. 2016;5(1):42-9.

Worthington P. et al. JPEN J Parenter Enteral Nutr. 2017.
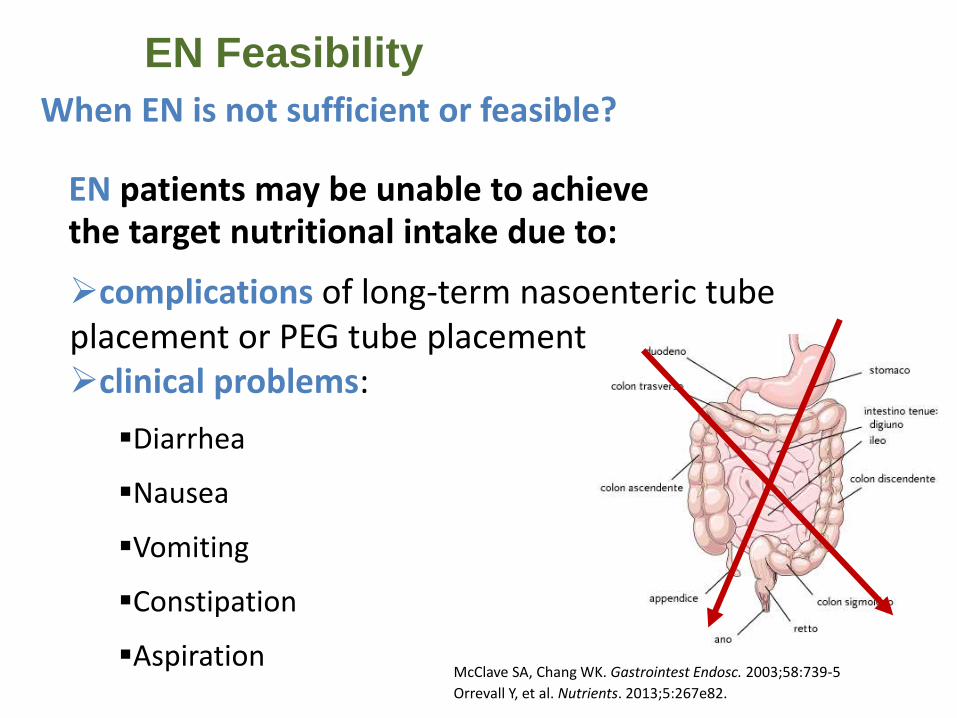
EN Feasibility
When EN is not sufficient or feasible?
EN patients may be unable to achieve the target nutritional intake due to:
complications of long-term nasoenteric tube placement or PEG tube placement clinical problems:
Diarrhea
Nausea
Vomiting
Constipation
Aspiration McClave SA, Chang WK. Gastrointest Endosc. 2003;58:739-5
Orrevall Y, et al. Nutrients. 2013;5:267e82.
8
Arends J, et al. Clin Nutr. 2017; 36:11-48
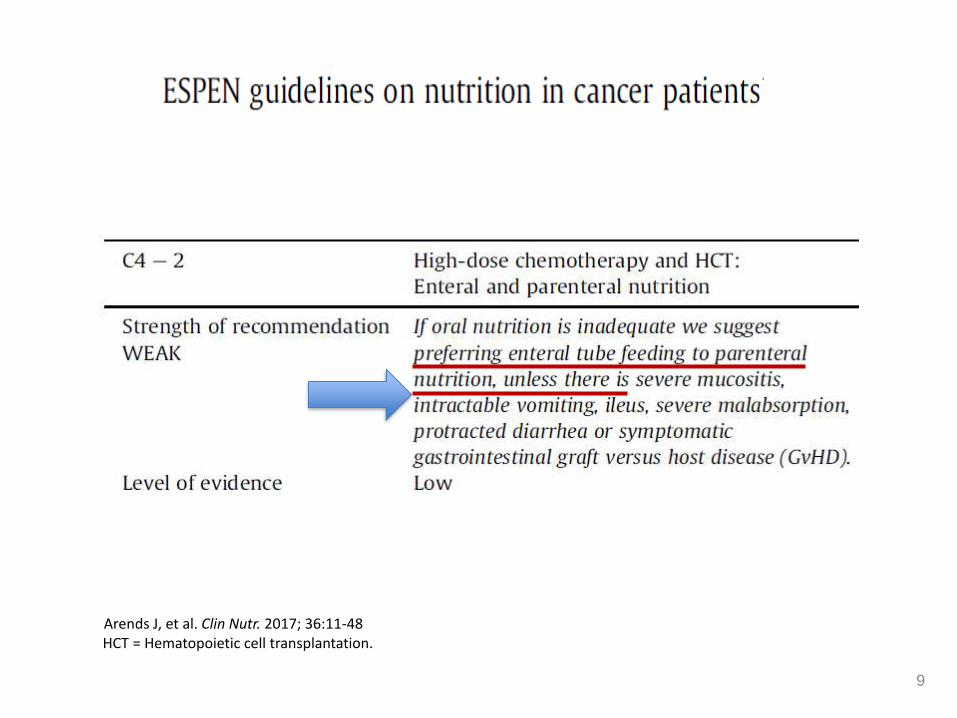
HCT = Hematopoietic cell transplantation.
9
Arends J, et al. Clin Nutr. 2017; 36:11-48

Nutrition Support
during Chemotherapy
• “If patients develop GI toxicity
from chemotherapy or radiation
therapy, short-term PN is usually
better tolerated (and more efficient)
than EN to restore the intestinal
function and prevent nutritional
deterioration.”
Bozzetti F, et al. Clin Nutr. 2009;28:445-54 (ESPEN Guidelines).
10

Disease State (n)
% of Patients with
Nutrition Support
% of Malnourished Patients with
Nutrition Support
% of Non-Malnourished Patients with
Nutrition Support
% Receiving Oral
Supplements
% Receiving Enteral
Nutrition
% Receiving Parenteral Nutrition
Blood (377) 34.5 44.5 29.3 20.3 9.5 16.2
Head and Neck (366) 63.7 76.5 51.3 36.4 40.4 6.1
Lung (247) 42.9 55.4 32.6 38.8 11.1 8.1
Breast (229) 14.8 34.0 9.89 12.3 5.2 4.1
Colon/Rectum (191) 30.4 41.3 23.3 21.5 5.8 10.9
Esophagus/Stomach (103) 65.0 77.4 46.3 47.8 25.8 19.6
Uterus/Ovaries (87) 32.2 41.0 25.0 14.7 6.8 21.3
Prostate (72) 13.9 40.0 9.7 13.0 1.5 4.5
Pancreas (42) 66.7 78.6 42.9 55.0 6.3 24.3
Kidney/Bladder (29) 41.4 66.7 14.3 28.6 15.4 7.7
Others (160) 31.9 52.2 23.7 19.1 10.6 10.2
TOTAL (1903) 39.8 57.6 28.4 24.2 13.8 9.6
Adapted from Hébuterne X, et al. JPEN J Parenter Enteral Nutr 2014;38:196-204 11
Prevalence of Malnutrition and Current
Use of Nutrition Nutrition Support
Volume 38 Number 2
Original Communication

12
Is There a Benefit?
Bozzetti F, et al. Clin Nutr. 2009;28:445-54 (ESPEN Guidelines).
PN may contribute to the maintenance or improvement of quality of life (QoL) in advanced cancer patients

13

Cotogni P, et al., Cancer Medicine; 2017, in press.

15
Volume 37 Number 3
Original Communication
Medium-term VADs Long-term VADs
Total PICC Hohn Tunneled Port
No of VADs 65 107 45 72 289
Local Infection, No. 2 2 2 3 9
No./1000 Catheter-Days 0.17 9.19 0.26 0.14 0.17
No./1000 HPN-Days 0.24 0.26 0.39 0.34 0.30
CRBSI, No. 0a 9 5 4b,c 18
No./1000 Catheter-Days 0 0.87 0.64 0.19 0.35
No./1000 HPN-Days 0 1.17 0.97 0.45 0.60
Risk Factors for CRBSI,
P-value
Use During HPN ― <.001 <.001 <.001
Previous VAD ― NS <.05 <.05
No Ultrasound-Guidance ― <.04 NS NS
Securement by Suture ― <.05 NS ―
Infraclavicular Exit Site ― <.01 ― ―
Cuff <2 cm from Exit Site ― ― <.05 ―
Infectious Complications
CRBSI=catheter-related bloodstream infection; HPN=home parenteral nutrition; NS=not significant; PICC=peripherally inserted central catheter; VAD=venous access device; — = not applicable. aP<.01 vs Hohn catheter and tunneled Groshong catheter; bP<.01 vs Hohn catheter; cP<.05 vs tunneled Groshong catheter.
Cotogni P, et al. JPEN J Parenter Enteral Nutr. 2013;37:375-383.
Catheter-Related Complications in Cancer Patients on Home Parenteral Nutrition: A Prospective Study
of Over 51,000 Catheter Days
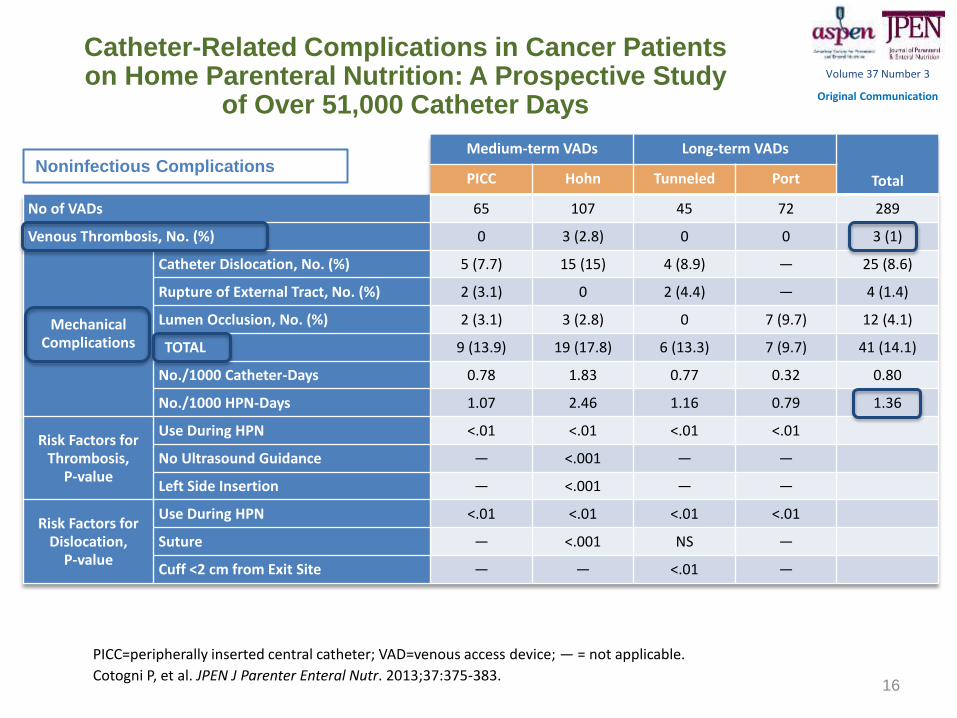
Medium-term VADs Long-term VADs
Total PICC Hohn Tunneled Port
No of VADs 65 107 45 72 289
Venous Thrombosis, No. (%) 0 3 (2.8) 0 0 3 (1)
Mechanical Complications
Catheter Dislocation, No. (%) 5 (7.7) 15 (15) 4 (8.9) ― 25 (8.6)
Rupture of External Tract, No. (%) 2 (3.1) 0 2 (4.4) ― 4 (1.4)
Lumen Occlusion, No. (%) 2 (3.1) 3 (2.8) 0 7 (9.7) 12 (4.1)
TOTAL 9 (13.9) 19 (17.8) 6 (13.3) 7 (9.7) 41 (14.1)
No./1000 Catheter-Days 0.78 1.83 0.77 0.32 0.80
No./1000 HPN-Days 1.07 2.46 1.16 0.79 1.36
Risk Factors for Thrombosis,
P-value
Use During HPN <.01 <.01 <.01 <.01
No Ultrasound Guidance ― <.001 ― ―
Left Side Insertion ― <.001 ― ―
Risk Factors for Dislocation,
P-value
Use During HPN <.01 <.01 <.01 <.01
Suture ― <.001 NS ―
Cuff <2 cm from Exit Site ― ― <.01 ―
16
Noninfectious Complications
Volume 37 Number 3
Original Communication
PICC=peripherally inserted central catheter; VAD=venous access device; — = not applicable.
Cotogni P, et al. JPEN J Parenter Enteral Nutr. 2013;37:375-383.
Catheter-Related Complications in Cancer Patients on Home Parenteral Nutrition: A Prospective Study
of Over 51,000 Catheter Days
12
Cotogni P, et al. JPEN J Parenter Enteral Nutr. 2013;37:375-83. 17
Catheter-Related Complications in Cancer Patients on Home Parenteral Nutrition: A Prospective Study
of Over 51,000 Catheter Days
Volume 37 Number 3
Original Communication
CONCLUSIONS
• If accurately managed, HPN can be safely provided for most cancer patients, even in an advanced stage, without expecting a relevant incidence of catheter-related complications
• Therefore, concerns about the risks should not still have influence on the decision to feed or not a cancer patient when HPN is clinically indicated

18
Is There an EBM?
Bozzetti F, et al. Clin Nutr. 2009;28:445-54 (ESPEN Guidelines).
• It would have been ethically unacceptable to
have a non-PN control arm
• So, any prospectively controlled evidence of
potential benefit
is denied
RCT EBM
19
Should This Patient Continue PN or
Start PN at Home?

20
How to Intervene?
Kumpf VJ, Tillman EM. Nutr Clin Pract. 2012;27(6):749-57.

21 Dreesen M, et al. Support Care Cancer. 2013;21:1373-81.
How to Intervene?

“… HAN should be prescribed and regularly monitored using defined protocols shared between oncologists and clinical nutrition specialists.”
How to Intervene?

Worthington P. et al. JPEN J Parenter Enteral Nutr. 2017.
How to Intervene?

Worthington P. et al. JPEN J Parenter Enteral Nutr. 2017.
How to Intervene?

25
Is There the Indication for HPN in
Patients With No Further Treatments?
Bozzetti F, et al. Clin Nutr. 2009;28:445-54 (ESPEN Guidelines).
Yes “It is not a contraindication for HPN that oncologic treatment has been stopped.”

of death due to malnutrition
26
Arends J, et al. Clin Nutr. 2017; 36:11-48

27 Hoda D. Cancer 2005;103:863-8.
Daanish Hoda
Oncology, Mayo Clinic Rochester Cancer 2005;103:863-8.
©2005 American Cancer Society
28
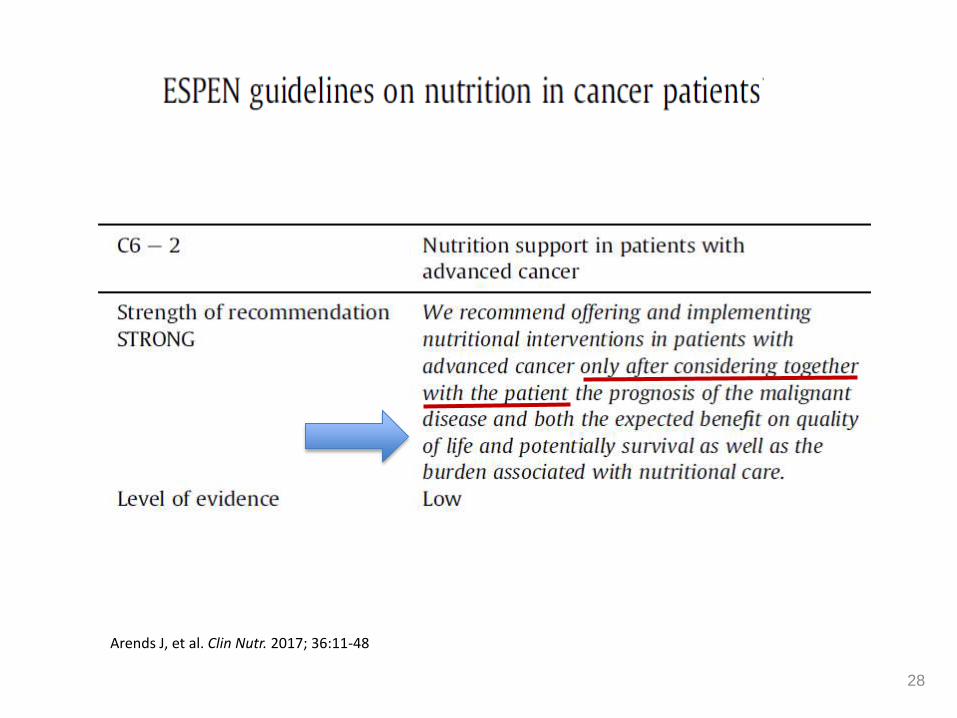
Arends J, et al. Clin Nutr. 2017; 36:11-48
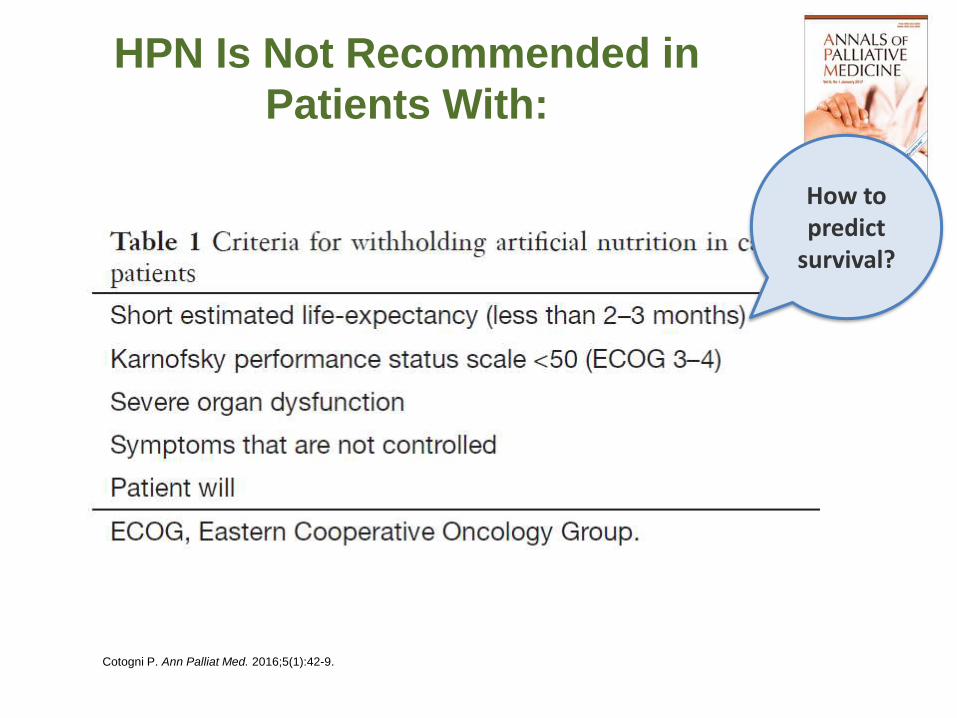
Cotogni P. Ann Palliat Med. 2016;5(1):42-9.
HPN Is Not Recommended in
Patients With:
How to predict
survival?

30
Development and Validation of a Nomogram
to Predict Survival in Incurable Cachectic
Cancer Patients on Home Parenteral Nutrition
Cox modeling based nomogram for predicting 3-, 6-month and median overall survival
Adapted from Bozzetti F, et al. Ann Oncol. 2015;26(11):2335-40.

LA NUTRIZIONE
ARTIFICIALE
DOMICILIARE:
più LUCI che OMBRE















![CENTRI DI RIFERIMENTO DEFINITIVO[1] - … CENTRO DI RIFERIMENTO REGIONALE PER LA NUTRIZIONE ARTIFICIALE DOMICILIARE RESPONSABILE: PROF. FRANCO CONTALDO UBICAZIONE: EDIFICIO 1 IV PIANO](https://static.fdocumenti.com/doc/165x107/5c66272c09d3f2c14e8ba675/centri-di-riferimento-definitivo1-centro-di-riferimento-regionale-per-la-nutrizione.jpg)
