La misura del grasso intra-epatico, uno specchio della...
55
La sfida della Cura della Salute nel Terzo Millennio • Curare la Salute della Persona nella Sua Unicità e Complessità • Evolvere dalla cura impersonale e tardiva della lesione alla cura personalizzata della salute per prevenire la lesione La misura del grasso intra-epatico, uno specchio della salute e corretto stile di vita personale Prof. Ferruccio Bonino UPMC Institute for Health Chianciano Terme Fondazione Italiana Fegato
Transcript of La misura del grasso intra-epatico, uno specchio della...
La sfida della Cura della Salute nel Terzo Millennio
• Curare la Salute della Persona nella Sua Unicità e Complessità• Evolvere dalla cura impersonale e tardiva della lesione alla cura personalizzata della salute per
prevenire la lesione
La misura del grasso intra-epatico, uno specchio della
salute e corretto stile di vita personale
Prof. Ferruccio BoninoUPMC Institute for Health
Chianciano Terme Fondazione Italiana Fegato
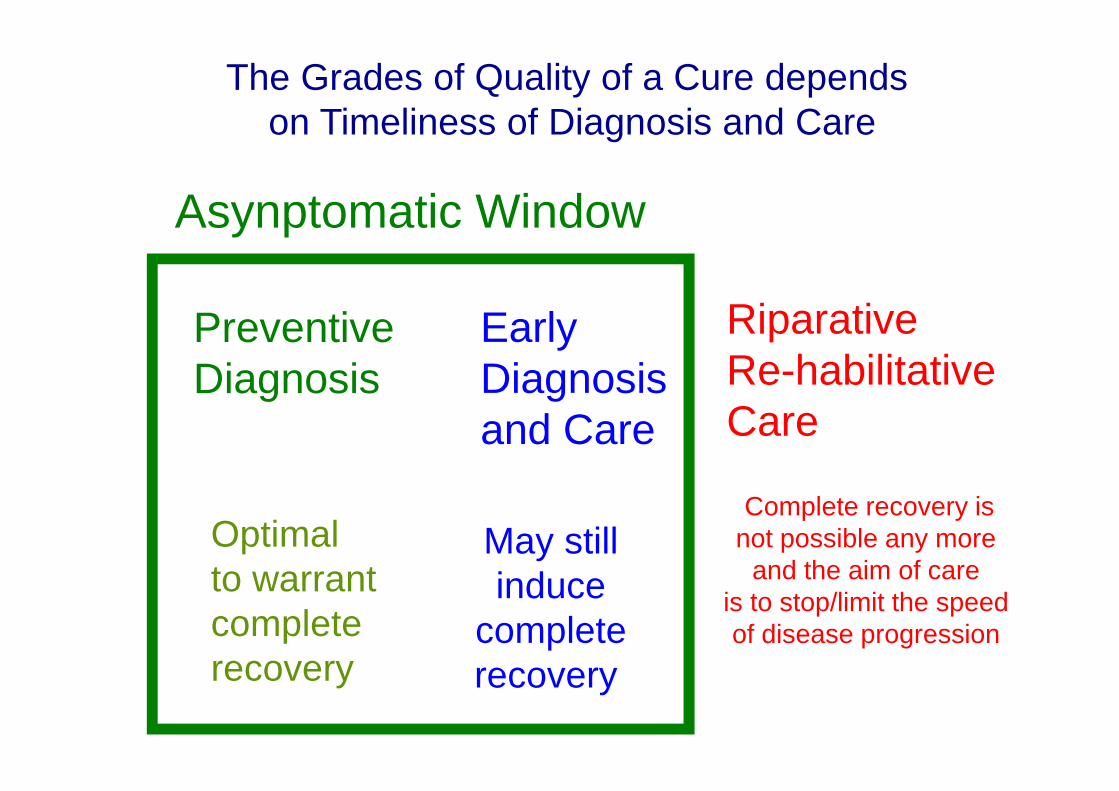
The Grades of Quality of a Cure depends on Timeliness of Diagnosis and Care
PreventiveDiagnosis
EarlyDiagnosisand Care
RiparativeRe-habilitativeCare
Optimalto warrantcomplete recovery
May stillinduce
complete recovery
Complete recovery isnot possible any more
and the aim of care is to stop/limit the speedof disease progression
Asynptomatic Window
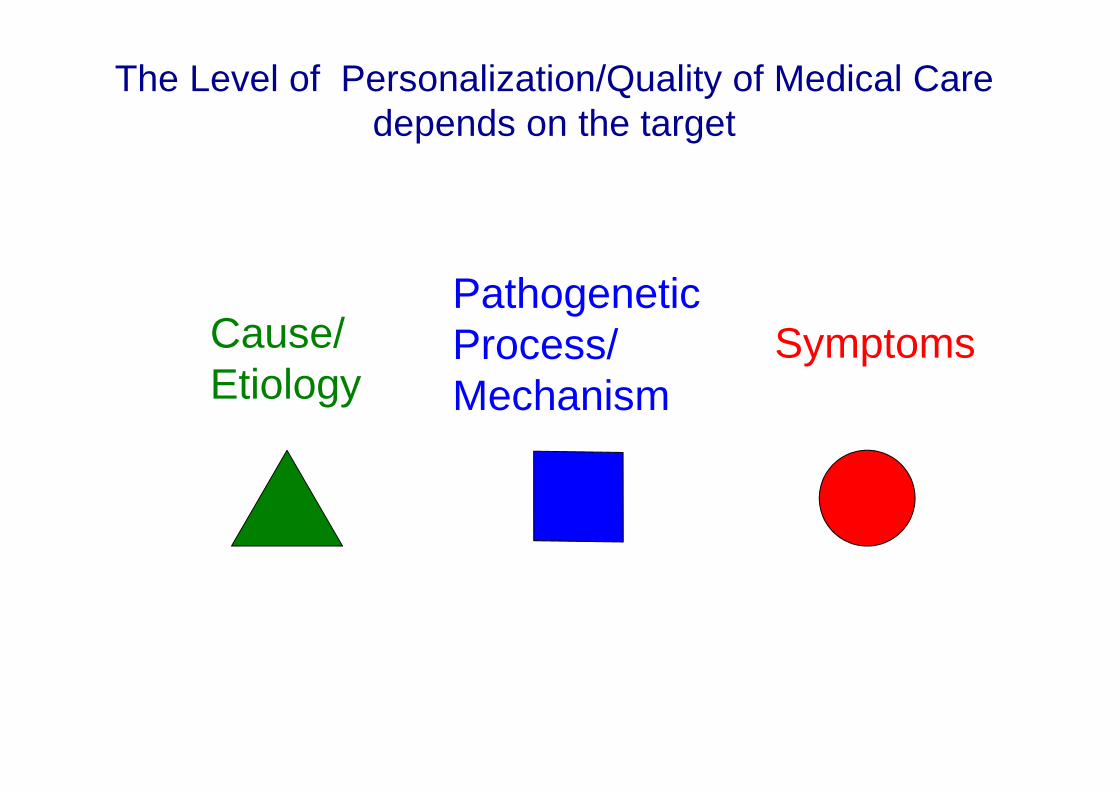
Cause/Etiology
PathogeneticProcess/Mechanism
Symptoms
The Level of Personalization/Quality of Medical Caredepends on the target


24.1%23.7%
31.8%
27.4%
13.5%
30.5%
Younossi et al. Hepatology, 2016
Worldwide prevalence of NAFLD

P
R
E
V
A
L
E
N
Z
A
Fegato Grasso – Studio DionysosPREVALENZA NELLA POPOLAZIONE GENERALE IN ITALIA: NAFLD = 25-30 % ; NASH = 2-3 %
Bellentani et al., Ann.Int.Med., 2000

NAFLD
NASH
Epatite
Rischio di Morte
age50 70 90
Malattie
Cardiovascolari
Metaboliche (Diabete)
Neoplastiche
Neurodegenerative
Malattie Suddette
Epatopatia
Epatopatia

Non alcoholic fatty liver disease (NAFLD) is a major independent risk factorassociated with overweight and inadequate life style
and the most sensitive biomarker in the asymptomatic subjectof the risk of death for cardiovascular diseases, type 2 diabetes
The prevalence of NAFLD in the general population is about 30 %, but it is 3 times higher in T2DM and 100% in obese patients with T2DM
The early identification of NASLD is mandatory to prevent thesediseases and their progression.
Among patho-physiologic mechanisms leading to NAFLD, common with T2DM are liver and muscle insulin resistance, however, it is mainly adipose tissue insulinresistance that results in increased hepatic de novo lipogenesis, inflammation, and lipotoxicity.
Although genetics predispose to NAFLD, an unhealthy lifestyle, includinghigh-fat/high-sugar diets and low physical activity, increases the risk. In addition, alterations in gut microbiota and environmental chemical agents, acting as endocrine disruptors play a role.
Saponaro C, Gaggini M, Gstaldelli A NAFLD and T2DM common pathophysiologic mechanims Curr Diab Rep. 2015;15(6):607

TG
GLP-1
Insulin
Lipolysis
FFA
Irisin
InflammationOxidative stress
AdiponectinLeptin
VLDL
VLDL
VLDL
VLDL
VLDL
Ghrelin
Acylated/deacylated
Ghrelin
Acylated/deacylated
Ghrelin
anti-inflammatory properties
WAT BAT Thermogenesis
FFA
DNL
β-oxidation FC
Lipogenesis
Glucose
Glucagon
Endothelial dysfunctionAtherosclerosis
GLP-1
GlycogenolysisGNG
SeP
Insulin Resistance
GNGGlycogenolysis
Inflammation
Glucotoxicity
VLDL
LDL
Hepatic IRSeP
Exercise / Insulin Resistance
Petta S, Gastaldelli A, Rebelos E, Bugianesi E, Messa P, Miele L, Svegliati-Baroni G, Valenti L, Bonino F. Pathophysiology of Non Alcoholic Fatty Liver Disease. Int J Mol Sci. 2016 Dec 11;17(12). pii: E2082.

Putative mechanisms linking NAFLD and extra-hepatic cancers
Mechanism Effects Extra-Hepatic Site Insulin resistance
↑ IGF-1 axis Proliferative and anti-apoptotic effects
Prostate/colorectal/lung/Breast cancers, Barrett’s esophagus, esophageal adenocarcinoma
Dysfunctional adipose tissue
↓ adiponectin/caspase activation ↓ adiponectin/TNF-α ↑ leptin/MAPK ↑ resistin/NF-κB
Anti-apoptotic effects Proliferation and angiogenesis Invasiveness, motility, lamellipodia formation
Gastrointestinal and extra-intestinal cancer Gastrointestinal and extra-intestinal cancer Colon/breast cancer, Barrett’s esophagus, esophageal adenocarcinoma Breast/gastrointestinal and non-small cell lung cancers
Inflammation IL-6/JAK/STAT3 and IL-6/MAPK TNF-α/Wnt/β-catenin
Proliferation Angiogenesis, differentiation and metastasis development
Renal/gastric/colorectal cancers Colorectal cancer
Gut microbiota MAMPs/TLRs Inflammasome-derived IL-18
Inflammation Anti-apoptotic effects
Colon cancer Colon cancer
IGF-1,insulingrowthfactor-1;IL,interleukin;MAMPs,microorganism-associated
molecularpatterns;MAPK,mitogen-activatedproteinkinase;NF-κB,nuclearfactor-κB;
STAT3,signaltransducerandactivatoroftranscription3;TLRs,toll-likereceptors;TNF-
α,tumornecrosisfactor-α.
Sanna C. et al. Int J Mol Sci. 2016 May; 17(5): 717

Libro Bianco dell’Associazione Italiana per lo Studio del Fegato-http://www.webaisf.org/media/13891/ libro-bianco-aisf-2011.pdf
Petta S, Valenti L, Bugianesi E, Targher G, Bellentani S, Bonino FSpecial Interest Group on Personalised Hepatology of the Italian Association for the Study of the Liver (AISF) A "systems medicine"approach to the study of non-alcoholicfatty liver disease. Dig Liver Dis. 2016 Mar;48(3):333-42.
European Association for the Study of the Liver (EASL), Association for the Studyof Diabetes (EASD), European Association for the Study of Obesity (EASO) ClinicalPractice Guidelines for the management of non-alcoholic fatty liver disease.J Hepatol. 2016 Jun;64(6):1388-402. doi: 10.1016/j.jhep.2015.11.004.
AISF POSITION PAPER ON NON ALCOHOLIC FATTY LIVER DISEASE (NAFLD): UPDATES AND FUTURE DIRECTIONS. Lonardo A, Nascimbeni F, Targher G,Bernardi M, Bonino F, Bugianesi E, Casini A, Gastaldelli A,Marchesini G, Marra F,Miele L, Morisco F, Petta S, Piscaglia F, Svegliati-Baroni GL, Valenti L, Bellentani S Dig Liver Dis. 2017 in press.

Is Liver Biopsy a Gold Standard? It is not.1/50.000
Steatosis Score: 65%
Steatosis Score: 15%
Steatosis is not
homogeneously
distributed in at least 30%
of cases;
Biopsy is invasive and
unsuitable
for tight monitoring
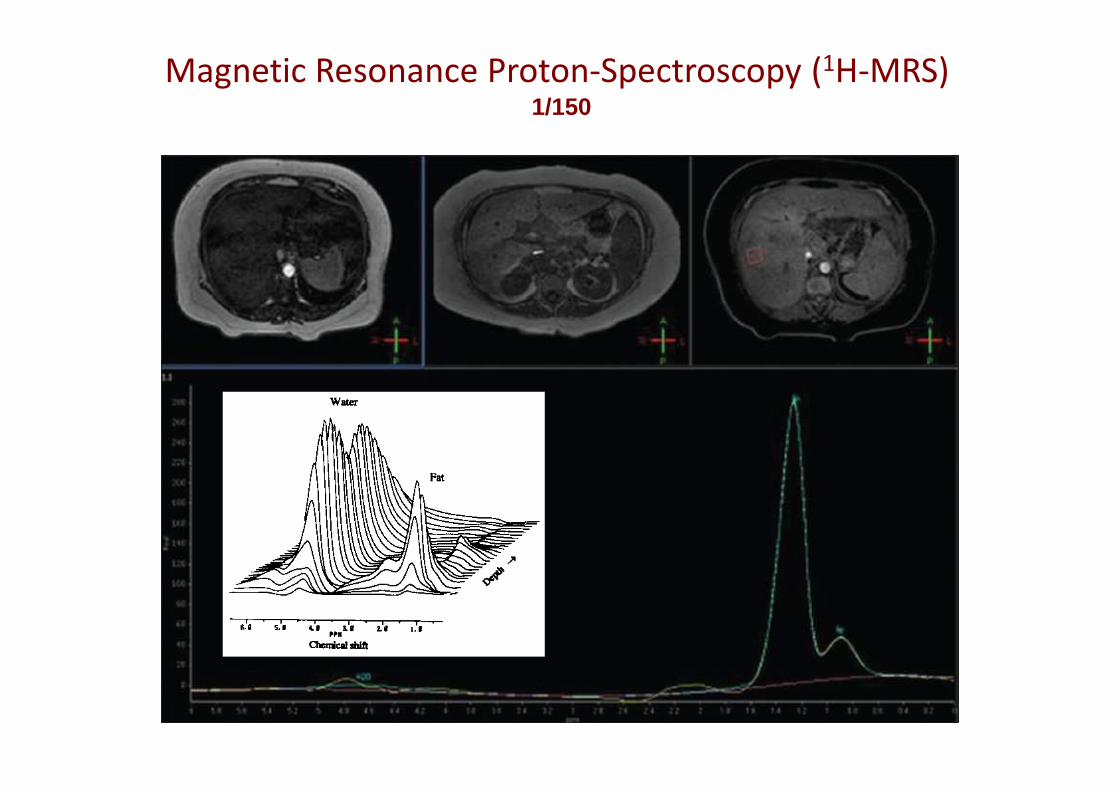
Magnetic Resonance Proton-Spectroscopy (1H-MRS) 1/150


Sonographic hepatic-renal ratio as indicator of hepatic steatosis: comparison with 1H
magnetic resonance spectroscopy
Metabolism Clinical and Experimental 58 (2009) 1724–1730

Castera L. et al Sem Liver Dis, 2015; Tapper EB, Afdahl NH. Curr Opin Gastroenterol , 2015
Liver Stiffness (LS)
7 8.7 10.3kPa
F0-F1 F2 F3 F4
Mild Sign Severe Cirrhosis
Matavir
Fibrosis
Congestion
Infiammation
Fibrosis
Bonino F et al Antivir Ther. 2010;


Castera L. Sem Liver Dis, 2015; Tapper EB and Afdahl NH. Curr OpinGastroenterol , 2015
Controlled Attenuation Parameter (CAP)
215 250 300 dB/m
S0 S1 S2 S3
<10%10-32% 33-66% >66%
Steatosis
% hepatocyteswith steatosis
86% 88% 87%Accuracy
measures the US attenuation rate by liver fat at 3.5 MHz frequ ency

Karlas T et al. Individual patient data meta-
analysis of controlled attenuation parameter
(CAP) technology for assessing steatosis.
J Hepatol. 2016 Dec 28. pii: S0168-
8278(16)30755-3. doi:
10.1016/j.jhep.2016.12.022.
The ultrasound based controlled attenuation
parameter (CAP) can be used to assess
steatosis, but factors such as the underlying
disease, BMI and diabetes must be taken into
accountUltrasound in Medicine & Biology 2010 61;36:1825-35

Figure 2
Imajo K et al Gastroenterology 2016 150, 626-637.e7DOI: (10.1053/j.gastro.2015.11.048)
Relationship between steatosis assessed by MRI-based PDFF and TE-based CAP

IngegneriFrancesco Faita (CNR – IFC)Nicole Di Lascio (SSSUP S. Anna)Nicola Martini (FTGM)
BiologiCinzia Avigo (CNR-IFC)
MediciMaurizia Rossana Brunetto (Università di Pisa, Epatologia AOUP)Filippo Oliveri, Barbara Coco, Antonio Salvati (Epato logia AOUP)Dante Chiappino (FTGM)Lorenzo Ghiadoni ( Università di Pisa, Medicina Urgenza AOUP)Rosa Maria Bruno (Medicina 1 AOUP)Ferruccio Bonino ( Università di Pisa, UPMC Institute for Health)
Steatometer: development of a software applicable to common US instruments for a reliable operator-indepen dentnon-invasive measure of liver fat
Progetto Ricerca Finalizzata 2013 CNR/SDN/Università di Pisa-Epatologia AOUP)
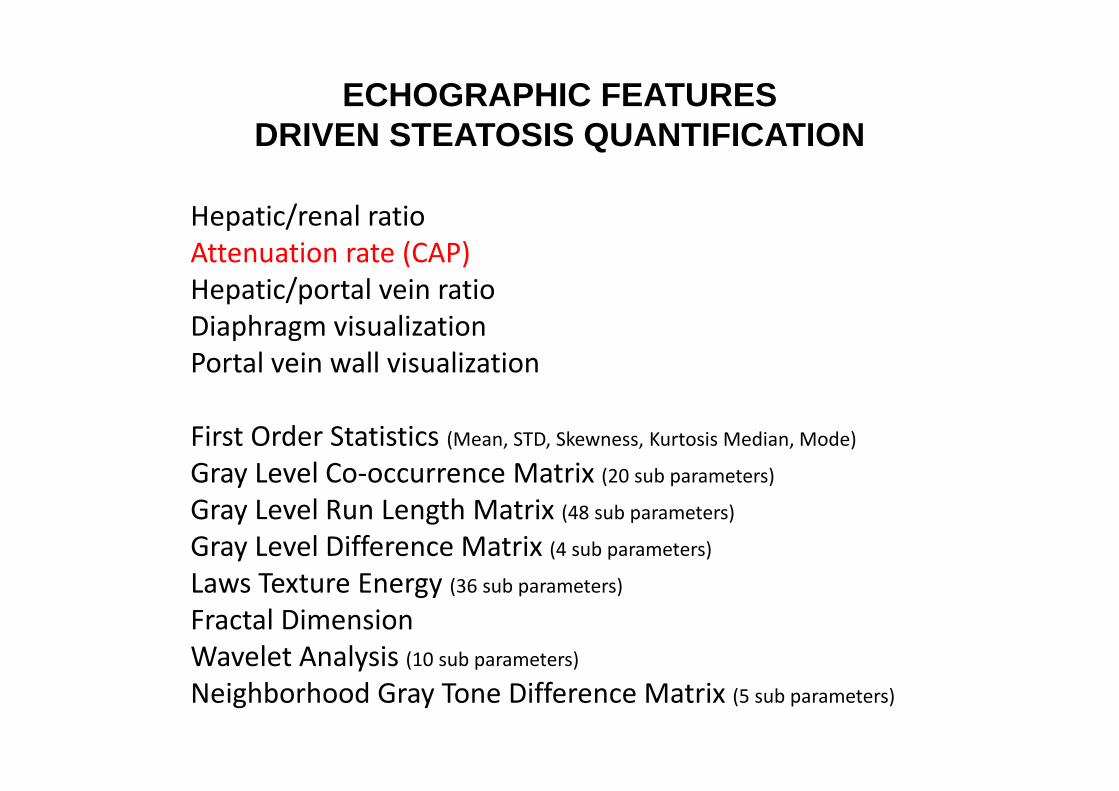
ECHOGRAPHIC FEATURESDRIVEN STEATOSIS QUANTIFICATION
Hepatic/renal ratio
Attenuation rate (CAP)
Hepatic/portal vein ratio
Diaphragm visualization
Portal vein wall visualization
First Order Statistics (Mean, STD, Skewness, Kurtosis Median, Mode)
Gray Level Co-occurrence Matrix (20 sub parameters)
Gray Level Run Length Matrix (48 sub parameters)
Gray Level Difference Matrix (4 sub parameters)
Laws Texture Energy (36 sub parameters)
Fractal Dimension
Wavelet Analysis (10 sub parameters)
Neighborhood Gray Tone Difference Matrix (5 sub parameters)

Clinical decision support system (CDSS)
CDSSSelected features(US + Biomarkers)
Steatosis score
Semi-autonomous diagnosis procedure
Selection of classifier: Bayesian with Gaussian model, k Nearest Neighbours,random forests and support vector machine
Learning phase
Liver RadarChart Status


Weighted linear combination:
US steato-grading =����1∙H/R ratio + ����2∙ attenuation rate +
����3∙ H/PV ratio – ����4∙diaphragm visualization -����5∙portal vein wall visualization
COMPARISON WITH MRS DATA

US-Steatometer
Best Accuracy, AUC, Sensitivity, Specificity and Youden index for > 5% liver fat content

Analysis of the inter/intra-operator/inter-session variabilities
Calculation of the Variability Coefficient for single parameters of the Steatometer Score obtained repeating the US analysis in 10 subjects at one hour time interval and changing operator
HR-ratio � VC = 4.75%HPV-ratio � VC = 7.22%AR � VC = 10.09%DV � VC = 10.8%HPV-wall � 4.96%Overall Steatometer Index � VC=7.50%

E’ necessario quindi un approccio di Medicina Sistematica per la Prototipizzazione dei Soggetti a Rischio e una
Adeguata Personalizzazione della Cura

Lee Kaplan, M.D., director of the Obesity, Metabolism, and Nutrition Instituteat Massachusetts General Hospital, tells the Times that there are at least59 types of obese subjects
1 2 3
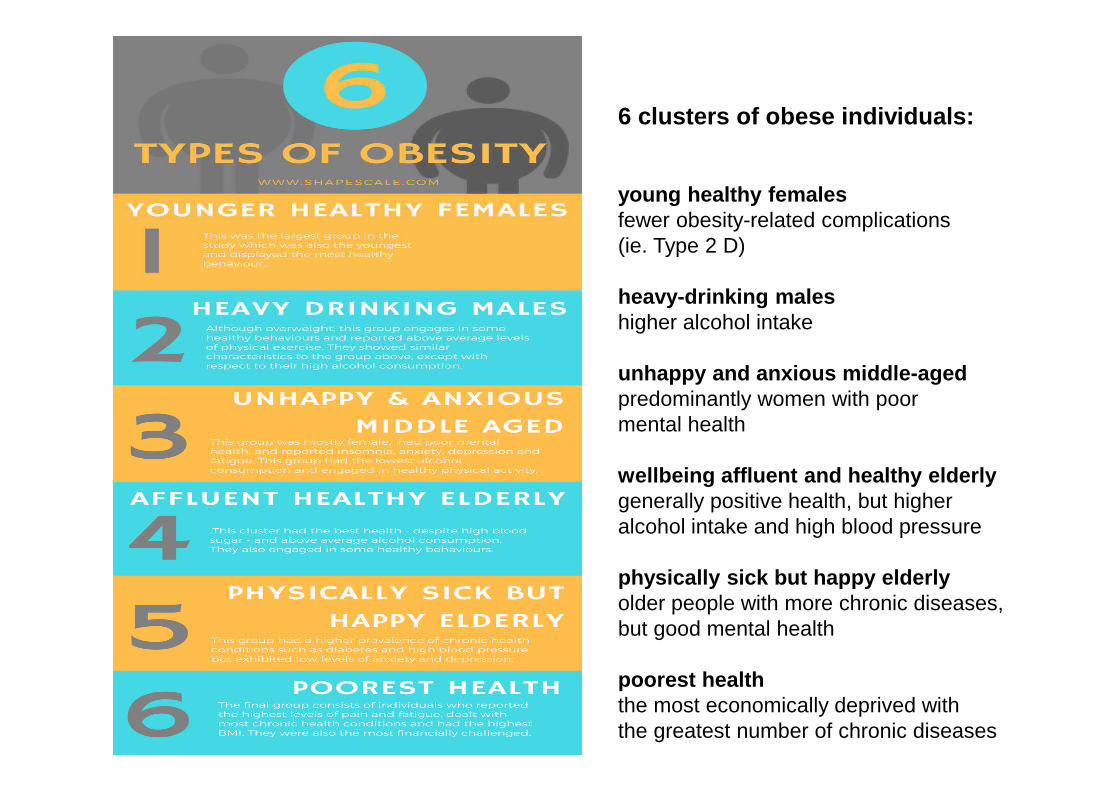
6 clusters of obese individuals:
young healthy femalesfewer obesity-related complications(ie. Type 2 D)
heavy-drinking maleshigher alcohol intake
unhappy and anxious middle-agedpredominantly women with poormental health
wellbeing affluent and healthy elderlygenerally positive health, but higheralcohol intake and high blood pressure
physically sick but happy elderlyolder people with more chronic diseases, but good mental health
poorest healththe most economically deprived with the greatest number of chronic diseases
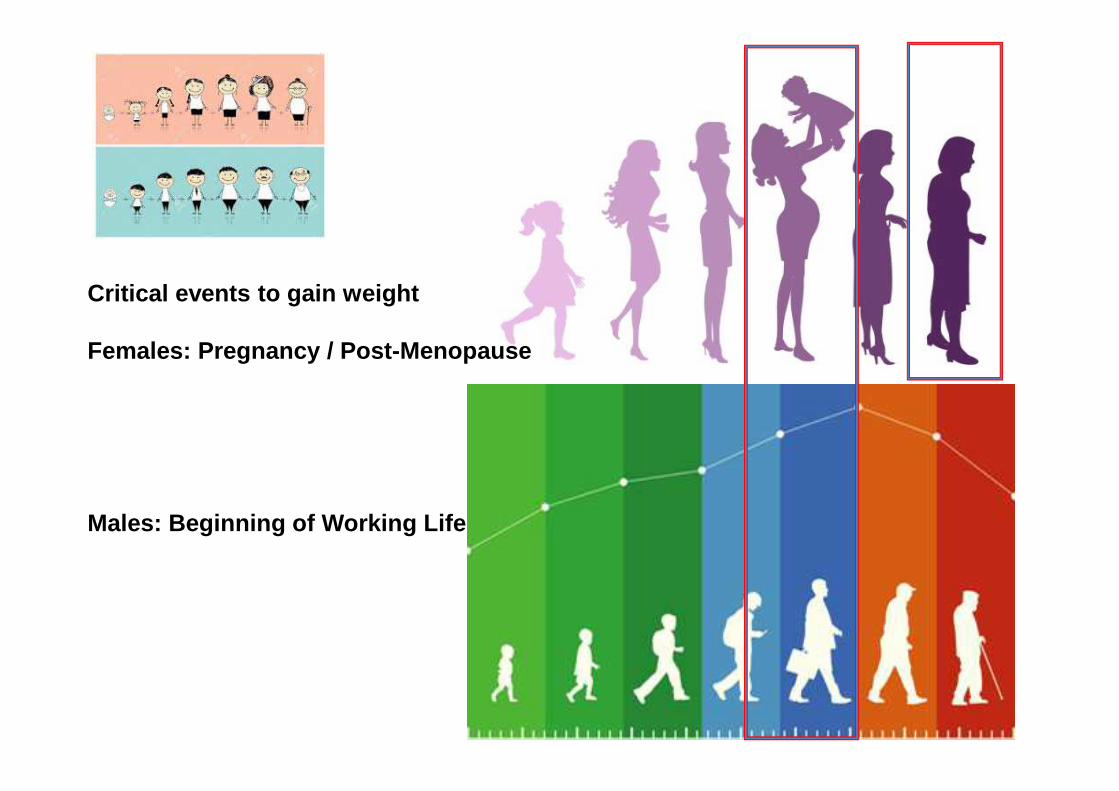
Critical events to gain weight
Females: Pregnancy / Post-Menopause
Males: Beginning of Working Life

Preventiva Precoce Tardiva
Timing/Efficacia della Cura

1 2 3O
Target of Bariatric Surgery and
Non-reversible GI Modifications
Targets of ReversibleGI Modifications

Major Negative Prognostic Factorsto be taken into account
for personal care
Hypoventilation SyndromeOSAS
Inflammation (NASH) Gut Microbiota Rehabilitation
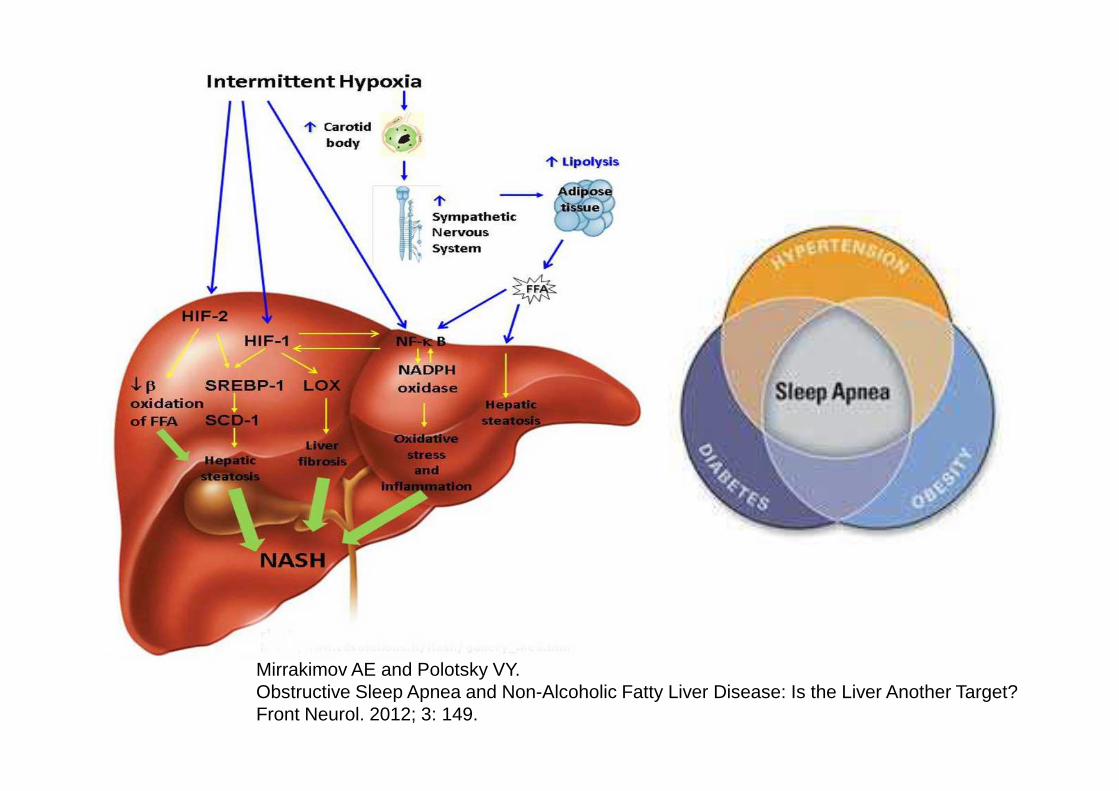
Mirrakimov AE and Polotsky VY. Obstructive Sleep Apnea and Non-Alcoholic Fatty Liver Disease: Is the Liver Another Target?Front Neurol. 2012; 3: 149.
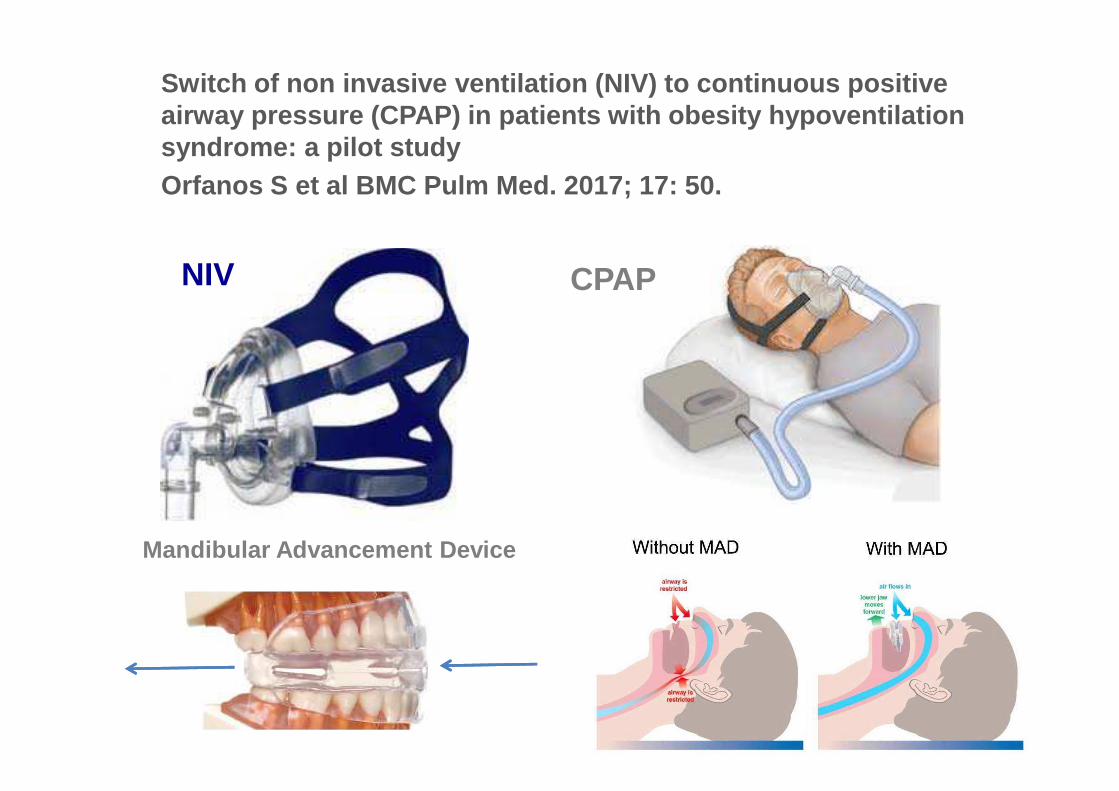
Switch of non invasive ventilation (NIV) to continu ous positive airway pressure (CPAP) in patients with obesity hyp oventilation syndrome: a pilot studyOrfanos S et al BMC Pulm Med. 2017; 17: 50.
NIV CPAP
Mandibular Advancement Device



Lin and Zhang BMC Immunology (2017) 18:2
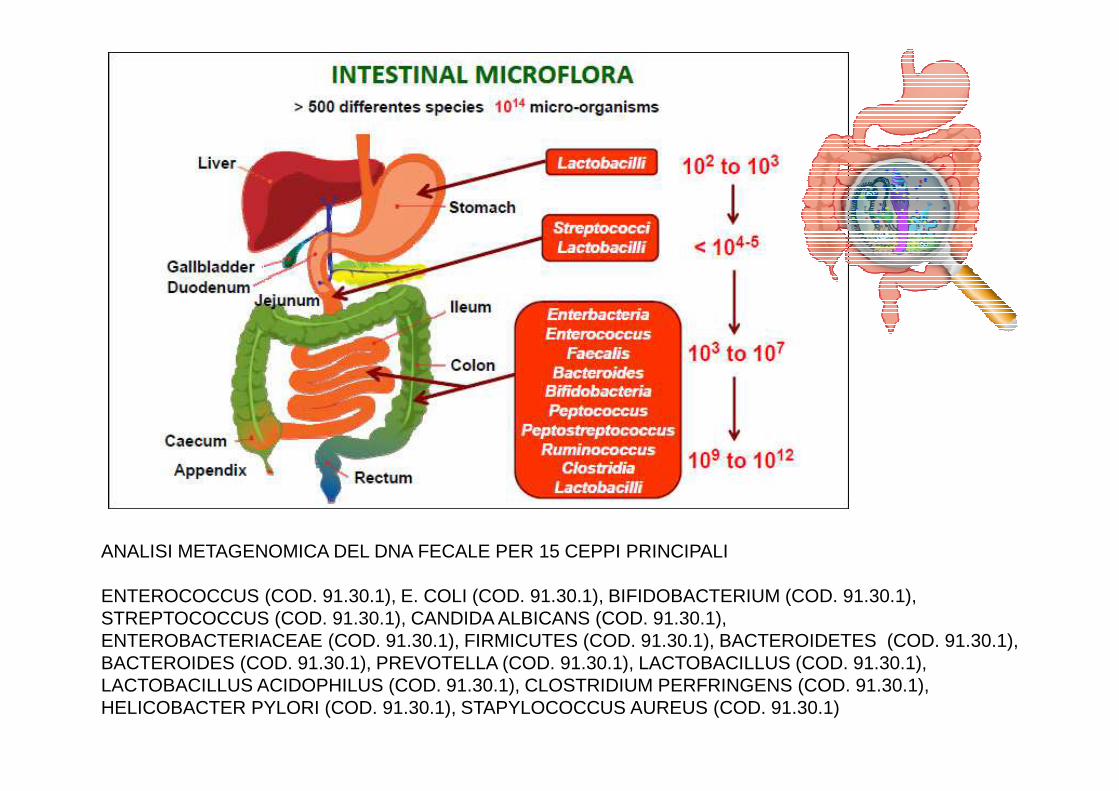
ANALISI METAGENOMICA DEL DNA FECALE PER 15 CEPPI PRINCIPALI
ENTEROCOCCUS (COD. 91.30.1), E. COLI (COD. 91.30.1), BIFIDOBACTERIUM (COD. 91.30.1), STREPTOCOCCUS (COD. 91.30.1), CANDIDA ALBICANS (COD. 91.30.1), ENTEROBACTERIACEAE (COD. 91.30.1), FIRMICUTES (COD. 91.30.1), BACTEROIDETES (COD. 91.30.1), BACTEROIDES (COD. 91.30.1), PREVOTELLA (COD. 91.30.1), LACTOBACILLUS (COD. 91.30.1), LACTOBACILLUS ACIDOPHILUS (COD. 91.30.1), CLOSTRIDIUM PERFRINGENS (COD. 91.30.1), HELICOBACTER PYLORI (COD. 91.30.1), STAPYLOCOCCUS AUREUS (COD. 91.30.1)
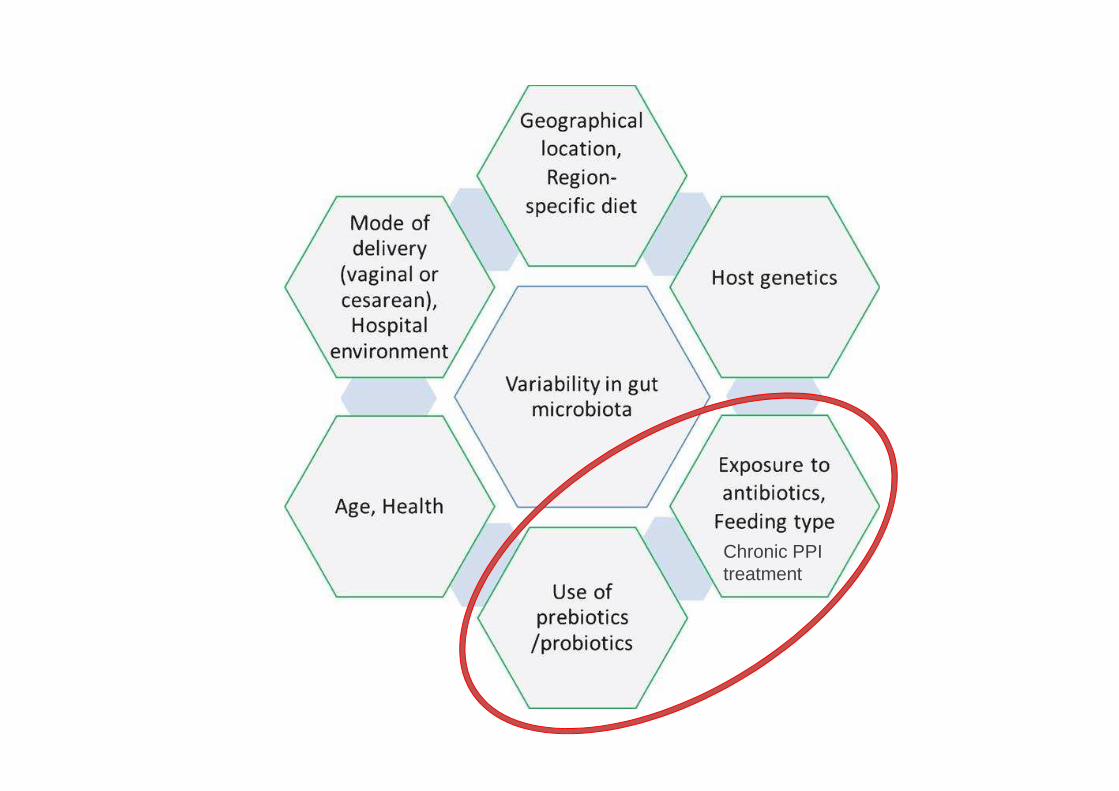
Chronic PPItreatment

La prevenzione abbinata all’appropriata personalizzazione prescrittiva rappresenta la più efficace spending review sanitaria
• Spesa farmaceutica Annuale totale circa 28 miliardi di euro, di cui il 75% rimborsato dal SSN
• I PPI sono circa l’11% della spesa = 3,0 miliardi euro di cui 80% inappropriati, quindi
• Con 2,4 miliardi risparmiati si eradica l’infezione da HCV e si copre la spesa per i farmaci oncologici innovativi
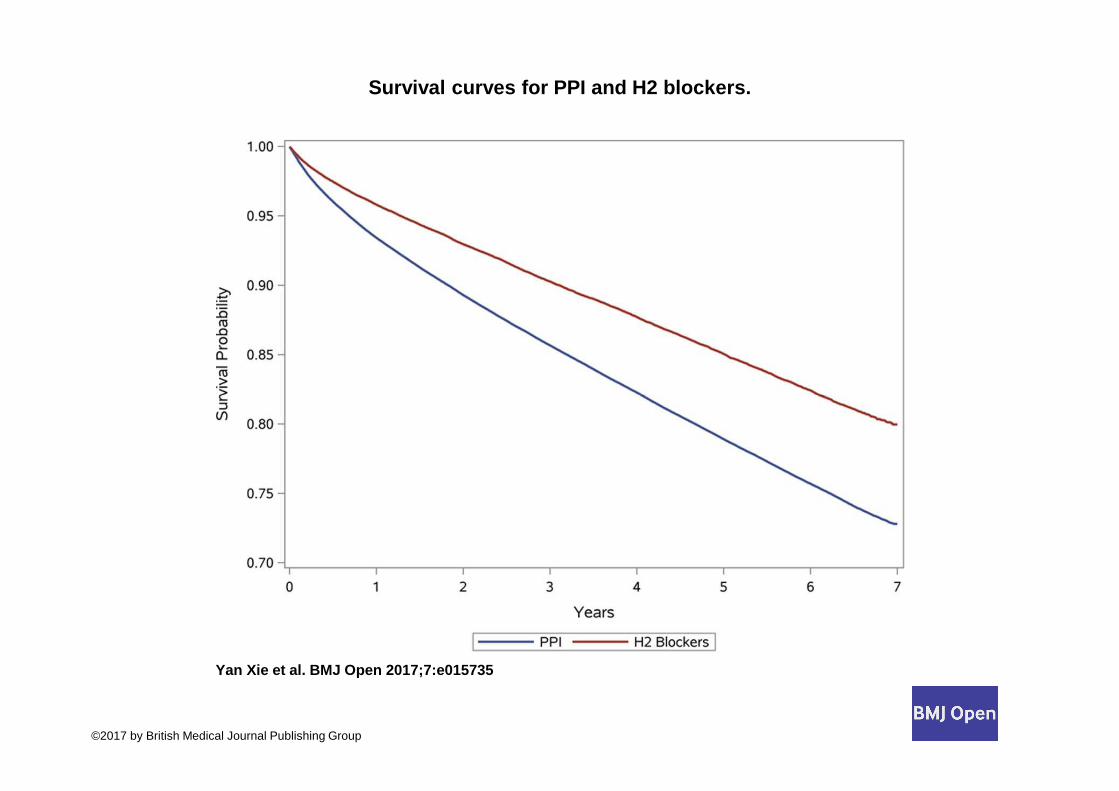
Survival curves for PPI and H2 blockers.
Yan Xie et al. BMJ Open 2017;7:e015735
©2017 by British Medical Journal Publishing Group

Duration of PPI exposure and risk of death among ne w PPI users (n=166 098).
Yan Xie et al. BMJ Open 2017;7:e015735
©2017 by British Medical Journal Publishing Group

Personalized HealthAssessment & Care
AgeGeneticsLiver
FatContent
100%
50%
0%0%Exercise
Life Style
FoodOtherRisk
Factors

The Impact of Genetics
• PNPLA3 patatin like phospholipase domain containing 3 http://www.ncbi.nlm.nih.gov/gene/80339
• TM6SF2 transmembrane 6 superfamilymember 2
• http://www.ncbi.nlm.nih.gov/gene/53345

InternistaEndocrinologo, Epatologo,..
Dietologo/Nutrizionista
Psicologo/PsichiatraFisioterapistaTrainer Sportivo
Specialista OperativoEndoscopista, Chirurgo
MMG/Supervisore
Briefings Periodici
Team Work Obbligatorio

Il percorso del paziente è riferibile a quello dell’ auto condotta dal guidatore per un determinato segmento di percorso (diagnostico-terapeutico). Il guidatore è accompagnato da 3-4 colleghi che lo consigliano sul percorso e che a loro volta si alternano alla guida.
Il paziente-autoè direttamentepartecipe, attore e autore del percorso di cura
Cars – Disney-Pixar
Casati S, Monti P, Bonino F From actors to authors: a first account about the involvement of patients In the informed consent governance of a major italian translational research hospitalJ Ambul Care Management. 2010 Jul-Sep;33(3):231-40.

Normale Grasso
La misura del grasso intra -epatico manometro dell’efficacia della cura nel singolo pazi ente
ColesteroloHDL
ALT/ASTGGT
Glicemia Insulina

Fine II – Inizio I Secolo A.C. Il fegato indice di salute generale
per l’ aruspice
Fine XX – Inizio XXI Secolo D.C.Il nostro fegato specchio
di salute individuale
Ritorno al Futuro: il fegato specchio di salute nella storia come nella pratica clinica
Il Fegato Specchio della Salute

Hepatology UnitUniversity Hospital of Pisa, Italy
Director Prof. Maurizia Rossana Brunetto
Medical Doctors
Barbara CocoPiero ColombattoFilippo OliveriVeronica RomagnoliAntonio SalvatiGabriele RiccoRiccardo GattaiLidia Surace
Nurses
Antonella CristofaniSimonetta Ferretti (part-time)Simona GiannettiTeresa Crisponi Barbara ZucchelliElena Centi
Arianna Del Chicca
Biologists
Daniela CavalloneFrancesco MoriconiPierpaola Tannorella
Bio-Physics – EngineersLuigi CivitanoFrancesco FaitaRanieri Bizzarri
Administrative Personel

Seo SW, Gottesman RF, Clark JM, Hernaez R, Chang Y, Kim C, Ha KH, Guallar E, Lazo M
Non alcoholic fatty liver disease is associated with cognitive function in adults

Reduced brain activity in female patients with non alco holic fatty liver diseaseas measured by near infrared spectroscopy
Takahashi A et Al. 2017
European Association for the Study of the Liver (EASL), Association for the Studyof Diabetes (EASD), European Association for the Study of Obesity (EASO) ClinicalPractice Guidelines for the management of non-alcoholic fatty liver disease .J Hepatol. 2016 Jun;64(6):1388-402. doi: 10.1016/j.jhep.2015.11.004.
Petta S, Valenti L, Bugianesi E, Targher G, Bellentani S, Bonino FSpecial Interest Group on Personalised Hepatology of AISF A "systems medicine"approach to the study of non-alcoholicfatty liver disease. Dig Liver Dis. 2016 Mar;48(3):333-42.
AISF POSITION PAPER ON NONALCOHOLIC FATTY LIVER DISEASE (NAFLD): UPDATES AND FUTURE DIRECTIONS. Lonardo A, Nascimbeni F, Targher G,Bernardi M, Bonino F, Bugianesi E, Casini A, Gastaldelli A,Marchesini G, Marra F,Miele L, Morisco F, Petta S, Piscaglia F, Svegliati-Baroni GL, Valenti L, Bellentani S Dig Liver Dis. 2017 in press.