Influence of body adiposity on structural characteristics of skeletal muscle in men and women
9
Influence of body adiposity on structural characteristics of skeletal muscle in men and women Claudio L. Lafortuna, Daniele Tresoldi and Giovanna Rizzo Istituto di Bioimmagini e Fisiologia Molecolare del Consiglio Nazionale delle Ricerche, Segrate, Milan, Italy Summary Correspondence Claudio L. Lafortuna, Istituito di Bioimmagini e Fisiologia Molecolare del C.N.R., via Cervi, 93, I-20090 Segrate, Milan, Italy E-mail: [email protected] Accepted for publication Received 10 April 2013; accepted 31 May 2013 Key words ageing; computed tomography imaging; muscle quality; muscle quantity; overweight and obesity The structure of skeletal muscle (SM) can be characterized by quantitative (size) and qualitative (composition) attributes, which are disparately reported to be influenced by body adiposity. This study tests the hypothesis that body adiposity exerts a sys- tematic influence on these muscle characteristics and evaluates the possible func- tional implications for movements. Lower limb SM volume (VSM) and attenuation (ATTSM), an inverse measure of lipid infiltration in muscle, were determined with computed tomography in 21 men (BMI = 21–36 kg m 2 ; age = 31–71 years.) and 18 women (BMI = 19–35 kg m 2 ; age = 32–76 years.). After adjusting for age, a multivariate regression analysis revealed that body adiposity positively corre- lated (P<0 05–0 001) with absolute VSM and cross-sectional area (CSA) in both genders, while VSM per unit body mass (VSM/BM) decreased with adiposity (P<0 001) in women and was constant in men. ATTSM was higher in men (P<0 05) and decreased (P<0 05) with adiposity in both genders. The product of ATTSM by average muscle CSA (predictor of maximal strength) and by VSM/BM (predictor of maximal dynamic performance) was lower in women (P<0 001) and was reduced by age in both genders (P<0 05–0 01), while obesity had a negative effect (P<0 001) only on the predictor of performance. In conclusion, body adipos- ity significantly increases SM size and reduces ATTSM. Structural indicators account- ing for both quantitative and qualitative characteristics of SM may be useful predictors of the effects of obesity on motor function at different ages. With rising body adiposity and advancing age, women appear mostly affected by the decline of SM features relevant for motor performance. Introduction Specific motor functional capabilities are intrinsically related to the dimensions of involved skeletal muscle (SM) (Maughan et al., 1983; Fukunaga et al., 2001). Several common conditions like body adiposity and ageing, beside inactivity, bed resting/ disuse and chronic illness influence structural properties of SM with effects on the inherent capability of strength and power generation due to a relative or absolute variation in muscle vol- ume (Doherty, 2003; Lafortuna et al., 2005; Evans 2010). Due to the recent surge of obesity epidemics with its asso- ciated complications as well as the rising prevalence of obesity in older adults (Flegal et al., 2002), the negative effects of adi- posity excess on SM characteristics and performance in the ages of life have gained a relevant clinical impact. In fact, an important role is played by the restriction of the individual’s work capacity in the accomplishment of basic daily activities concurring to a good quality of life, as well as in the decline of the functional status and overall increased risk of disability (Janssen et al., 2002; Walter et al., 2009). Under these perspectives, the understanding of the effects of body adiposity on muscle size and composition during life may have a relevant clinical importance. While the effects of ageing processes per se on muscle mass and functions are well established (see Doherty, 2003; for a review), the effects of increased adiposity on muscle characteristics are still unde- fined, estimation of SM in obese or overweight individuals being mostly based on indirect evaluation of fat-free or lean soft tissue mass, in spite of the considerable functional limita- tions associated with body mass excess. In this condition, the disproportionately augmented mass of fat tissue put muscles at disadvantage during the execution of everyday life activities as well as during specific exercise movements. In fact, body mass excess imposes a burden limiting most motor capabili- ties with a particularly disabling effect in women, who are inherently endowed with a reduced amount of SM (Evers Clin Physiol Funct Imaging (2014) 34, pp47–55 doi: 10.1111/cpf.12062 47 © 2013 Scandinavian Society of Clinical Physiology and Nuclear Medicine. Published by John Wiley & Sons Ltd 34, 1, 47–55
Transcript of Influence of body adiposity on structural characteristics of skeletal muscle in men and women

Influence of body adiposity on structural characteristicsof skeletal muscle in men and womenClaudio L. Lafortuna, Daniele Tresoldi and Giovanna Rizzo
Istituto di Bioimmagini e Fisiologia Molecolare del Consiglio Nazionale delle Ricerche, Segrate, Milan, Italy
Summary
CorrespondenceClaudio L. Lafortuna, Istituito di Bioimmagini
e Fisiologia Molecolare del C.N.R., via Cervi,
93, I-20090 Segrate, Milan, Italy
E-mail: [email protected]
Accepted for publicationReceived 10 April 2013;
accepted 31 May 2013
Key words
ageing; computed tomography imaging; muscle
quality; muscle quantity; overweight and obesity
The structure of skeletal muscle (SM) can be characterized by quantitative (size) andqualitative (composition) attributes, which are disparately reported to be influencedby body adiposity. This study tests the hypothesis that body adiposity exerts a sys-tematic influence on these muscle characteristics and evaluates the possible func-tional implications for movements. Lower limb SM volume (VSM) and attenuation(ATTSM), an inverse measure of lipid infiltration in muscle, were determined withcomputed tomography in 21 men (BMI = 21–36 kg m�2; age = 31–71 years.)and 18 women (BMI = 19–35 kg m�2; age = 32–76 years.). After adjusting forage, a multivariate regression analysis revealed that body adiposity positively corre-lated (P<0�05–0�001) with absolute VSM and cross-sectional area (CSA) in bothgenders, while VSM per unit body mass (VSM/BM) decreased with adiposity(P<0�001) in women and was constant in men. ATTSM was higher in men(P<0�05) and decreased (P<0�05) with adiposity in both genders. The product ofATTSM by average muscle CSA (predictor of maximal strength) and by VSM/BM(predictor of maximal dynamic performance) was lower in women (P<0�001) andwas reduced by age in both genders (P<0�05–0�01), while obesity had a negativeeffect (P<0�001) only on the predictor of performance. In conclusion, body adipos-ity significantly increases SM size and reduces ATTSM. Structural indicators account-ing for both quantitative and qualitative characteristics of SM may be usefulpredictors of the effects of obesity on motor function at different ages. With risingbody adiposity and advancing age, women appear mostly affected by the decline ofSM features relevant for motor performance.
Introduction
Specific motor functional capabilities are intrinsically related to
the dimensions of involved skeletal muscle (SM) (Maughan
et al., 1983; Fukunaga et al., 2001). Several common conditions
like body adiposity and ageing, beside inactivity, bed resting/
disuse and chronic illness influence structural properties of SM
with effects on the inherent capability of strength and power
generation due to a relative or absolute variation in muscle vol-
ume (Doherty, 2003; Lafortuna et al., 2005; Evans 2010).
Due to the recent surge of obesity epidemics with its asso-
ciated complications as well as the rising prevalence of obesity
in older adults (Flegal et al., 2002), the negative effects of adi-
posity excess on SM characteristics and performance in the
ages of life have gained a relevant clinical impact. In fact, an
important role is played by the restriction of the individual’s
work capacity in the accomplishment of basic daily activities
concurring to a good quality of life, as well as in the decline
of the functional status and overall increased risk of disability
(Janssen et al., 2002; Walter et al., 2009).
Under these perspectives, the understanding of the effects
of body adiposity on muscle size and composition during life
may have a relevant clinical importance. While the effects of
ageing processes per se on muscle mass and functions are well
established (see Doherty, 2003; for a review), the effects of
increased adiposity on muscle characteristics are still unde-
fined, estimation of SM in obese or overweight individuals
being mostly based on indirect evaluation of fat-free or lean
soft tissue mass, in spite of the considerable functional limita-
tions associated with body mass excess. In this condition, the
disproportionately augmented mass of fat tissue put muscles
at disadvantage during the execution of everyday life activities
as well as during specific exercise movements. In fact, body
mass excess imposes a burden limiting most motor capabili-
ties with a particularly disabling effect in women, who are
inherently endowed with a reduced amount of SM (Evers
Clin Physiol Funct Imaging (2014) 34, pp47–55 doi: 10.1111/cpf.12062
47© 2013 Scandinavian Society of Clinical Physiology and Nuclear Medicine. Published by John Wiley & Sons Ltd 34, 1, 47–55

Larsson & Mattsson, 2001; Lafortuna, 2013). In spite of this,
several studies have evidenced a preservation or even an
increase in muscle strength in obese individuals during move-
ments of different body segments and under different condi-
tions (Hulens et al., 2001; Lafortuna et al., 2005), which was
no longer apparent when fat-free mass was accounted for,
suggesting that also the mass of involved muscles was aug-
mented in the condition of overweight/obesity.
Indeed, SM can be characterized by quantitative (size) and
qualitative (composition) structural attributes which concur in
determining functional performance and possibly impairment.
Abundant evidence supports a robust association between
muscle size and strength production on a general context
(Maughan et al., 1983; Fukunaga et al., 2001). On the other
side, disparate investigations have pointed out that also
changes in skeletal muscle composition due to a degree of fat
infiltration, such as observed in obesity, are associated with
reductions in muscle performance (Goodpaster et al., 2001;
Visser et al., 2005; Hilton et al., 2008). In spite of the apparent
effects of obesity on muscle size and composition, studies
exploring the variation in muscle dimension and fat infiltra-
tion are mainly focused on the contrast between groups of
persons in a specific condition and investigations on the sys-
tematic effect of the degree of body adiposity on trends of SM
characteristics are hardly available.
Methods based on different mathematical modelling of
body composition and using different principles of measure-
ments have been devised to achieve an indirect estimate of
total or regional SM mass (Janssen et al., 2000; Kim et al.,
2002). On the contrary, imaging techniques, such as com-
puted tomography (CT) and magnetic resonance imaging, can
provide a direct measurement of muscle tissue (Mitsiopoulos
et al., 1998; Ross et al., 2000). A major advantage of imaging
techniques is the tomographic visualization of body tissues,
which enables the volume reconstruction of total and regional
SM mass and avoids the approximation entailed in the use of
mathematical models and predictive equations. Moreover, SM
quality, related to adipose infiltration within the muscle, can
be studied with CT using voxel information about tissue atten-
uation (Goodpaster et al., 2000a).
Therefore, to test the hypothesis that body adiposity exerts
a direct influence on muscular characteristics and to evaluate
whether these changes may have functional implications for
movements, we determined volume and attenuation of the
lower limb SM from total CT images in a sample of individu-
als of both genders within a wide span of adiposity and age.
Subjects and methods
Subjects
Total body CT scans obtained in 39 subjects [21 males (mean
age � SD: 50�5 � 13�0 year, range: 31–71 year); 18 females
(mean age: 55�0 � 12�1 year, range: 32–76 year, P: not
significant)] were retrospectively analysed for lower limb
imaging. All subjects were undergoing a follow-up protocol
for melanoma diagnosed >24 months prior to the CT study
presently considered, and all were negative for a recurrence of
regional or distance disease thereafter, as assessed with repeated
routine total body clinical imaging (CT-Positron Emission
Tomography scans). Informed consent had been obtained from
all patients prior to the examinations in accordance with the
institutional ethics guidelines for clinical testing, and the pres-
ent analysis was anonymously conducted. For all patients, body
mass (males: mean, 80�4 � 12�1 kg, range, 60–120 kg;
females: mean, 64�5 � 12�4 kg, range, 49–90 kg, P<0�001)and height (males: mean, 1�75 � 0�06 m, range, 1�62–1�86 m; females: mean, 1�59 � 0�05 m, range, 1�50–1�67 m,
P<0�001) were obtained at the moment of examination and
body mass index (BMI) subsequently calculated (males: mean,
26�2 � 3�5 kg m�2, range, 21�4–35�9 kg m�2; females:
mean, 25�7 � 4�7 kg m�2, range, 19�0–34�7 kg m�2, p: not
significant). Waist circumference (WC) was determined from
the CT slice at mid-distance between iliac crest and rib cage,
according to the WHO criteria (World Health Organization,
1987). As an indicator of body adiposity, WC was expressed as
a ratio (WCr) with the values considered by the International
Diabetes Federation (Alberti et al., 2006) as the cut-off for cen-
tral obesity in Europids (i.e. 94 cm for males and 80 cm for
females). Average values of WCr were 1�02 � 0�12 (range
0�82–1�30) in men, and 1�10 � 0�17 (range 0�84–1�37) in
women, P: not significant. In both genders, a significant corre-
lation was found through linear regression between BMI and
WCr (men: BMI = 26�6 WCr–1�03, R2 = 0�811, P<0�001;women: BMI = 26�4 WCr–3�44, R2 = 0�877, P < 0�001).
Imaging technique
In all participant subjects, CT images were acquired by a Phi-
lips Gemini GXL tomograph (Philips Healthcare, Best, the
Netherlands) and consisted in a series of contiguous trans
axial slices, imaged as 512 9 512 voxel matrices with 5-mm
slice thickness and 1�17-mm pixel size.
A body segment comprised between the most cranial bor-
der of iliac crest and the apex of lateral malleolus was consid-
ered for image analysis in all subjects, and included buttock,
thigh and calf. The true anatomical length of the entire seg-
ment (LS) was calculated by accounting for knee and hip
angles possibly detected on CT images of the study, due to
occasional slight flexion spontaneously assumed by patients
during the examination. Slices were automatically processed
by a segmentation algorithm based on fuzzy c-mean approach
(Goldszal & Pham, 2000), using the public domain software
package (McAuliffe et al., 2001) Medical Image Processing,
Analysis and Visualization – MIPAV (Center for Information
Technology, National Institutes of health, available at http://
mipav.cit.nih.gov [last access 14 June 2013]).
After segmentation, voxels belonging to SM, adipose tissue
and bone were labelled with a component-specific numerical
values and could thus be discriminated. From the segmented
© 2013 Scandinavian Society of Clinical Physiology and Nuclear Medicine. Published by John Wiley & Sons Ltd 34, 1, 47–55
Adiposity and human leg muscle features, C. L. Lafortuna et al.48

images, volumes of the different tissues were automatically
calculated as the sum of the voxels belonging to the specific
component multiplied by the voxel size. Volume rendering of
segmented images was achieved by means of a dedicated
commercial software (Amira v.4; Mercury Computer Systems,
Chelmsford, MA, USA) to visualize the three-dimensional
aspect of the lower limb tissue components. The volume of
SM (VSM) included all muscles with at least one insertion on
bone segments belonging to the lower limb, with exclusion
of ileus–psoas muscle. VSM was also expressed per unit limb
length (VSM/Ls), representing the ideal average muscle cross
section throughout lower limbs, and per unit body mass
(VSM/BM), representing the amount of muscle theoretically
available to support each unit of body load. Adipose tissue
volume was established by analysing slices representing the
true appendicular segment of lower limb, that is, ranging
from malleoli to a horizontal plane tangential to ischiatic
tuberosity, and included both subcutaneous and intermuscular
fat. Bone tissue comprised femur, patella, tibia and fibula. An
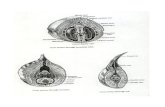
example of mid-thigh CT imaging, tissue segmentation and
whole limb tissue rendering representative of calculated
volumes is available in Fig. 1, for a typical male subject.
From the slices at mid-thigh, the mean CT attenuation coef-
ficient value for SM (ATTSM), which corresponds to the reci-
procal of lipid infiltration practically denoting the amount of
contractile elements within the muscle, was determined by
averaging the Hounsfield units intensity in voxels belonging
to the segmented muscle area.
To take into account the interaction between quantity and
quality of SM, the product VSM/Ls 9 ATTSM [related to mus-
cle section area, and expected to predict the strength capability
of the muscle (Maughan et al., 1983)] and VSM/BM 9 ATT-
SM [related to muscles volume relative to body mass, and
expected to predict the actual power performance (Lafortuna
et al., 2002)] were considered in the analysis.
Statistical methods
All values are given as means � SD. Significance of differences
between males and females was assessed with a Student’s t-test
for unpaired data. Regression line equations were calculated
with the least-square method and the differences between
regression lines were tested using conventional regression
equation comparison methods (Zar, 1984). The independent
effect of age and adiposity on muscle volume, cross-sectional
area and composition was evaluated by bivariate regression
analysis performed in men and women, separately. Multivari-
ate analysis of variance was performed to assess the indepen-
dent effect of gender, degree of adiposity and age on variables
combining size and composition of SM, in the whole sample.
P values <0�05 were considered statistically significant.
Results
The average values of VSM, mid-thigh muscle cross-sectional
area (CSASM) and ATTSM in lower limbs are presented in
Table 1, along with the values of adipose tissue and bone vol-
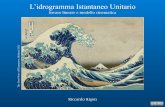
ume, while lower limb regional distribution of average cross-
section area of SM, adipose tissue and bone in the subjects
taking part in the study is shown in Fig. 2, for males and
females. As expected, the size of limb segments was smaller in
women, due to a significantly lower volume of SM and bone
and in spite of a significantly larger adipose tissue volume.
Therefore, the total volume of lower limbs was significantly
smaller in women than in men (21�6 L � 4�6 versus
25�0 L � 4�9, P<0�05). Similar gender differences in the tis-
sues of lower limbs were detected also when expressing the
values per unit body mass (P<0�001 for all tissues) and per
unit limb length (P<0�001 for all tissues). As shown in
Table 1, also average ATTSM was significantly lower in
women.
(a) (c)
(b)
Figure 1 Mid-thigh CT imaging (A), tissuesegmentation (B; light grey: skeletal muscle;dark grey: adipose tissue; white: bone; black:background) and whole limb tissue rendering(C) representative of calculated volumes in atypical male subject (age: 40 y; body massindex: 24�1 kg/m2).
© 2013 Scandinavian Society of Clinical Physiology and Nuclear Medicine. Published by John Wiley & Sons Ltd 34, 1, 47–55
Adiposity and human leg muscle features, C. L. Lafortuna et al. 49

The independent effect of body adiposity, as represented by
WCr, and age on lower limb SM characteristics was assessed
by means of a multiple linear regression analysis and the
resulting coefficients are presented in Table 2. In both gen-
ders, the analysis revealed that body adiposity and age had an
opposite independent effect on SM dimensional variables
(VSM, VSM/Ls and CSASM), while only body adiposity had a
negative effect on SM composition (i.e. on ATTSM), especially
in women. Moreover, in women, adiposity influenced nega-
tively also VSM/BM, representing the amount of lower limb
SM which functionally contributes to body mass support and
movement, whereas no effect was detected in males.
Therefore, in the individual subjects, high body adiposity
and advanced age had opposite effects on lower limb SM size,
with important differences among genders. In Fig. 3, the
value of VSM adjusted for age and expressed in both absolute
terms (panel A) or normalized by unit limb length (panel B)
is plotted as a function of body adiposity. Statistical compari-
son of regression lines obtained in men and women revealed
significantly different slopes (VSM: t = 4�09, P<0�001; VSM/
Ls: t = 4�40; P < 0�001), while similar trends between the
genders were observed for the decrease in both VSM and
VSM/Ls as a function of age (data not shown). Also VSM/BM
was similarly decreased by age in both genders, but it was
significantly reduced in women by body adiposity while unaf-
fected in men, as it can be appreciated from Fig. 4.
To explore the interaction between the changes in SM quan-
tity and quality and the impact for the overweight/obesity
0
100
200
300
400
500
600
700
–40 –20 0 20 40 60 80 100
CSA (
cm2)
Total Skeletal muscle Adipose tissue Bone
Men
Thigh
Calf
Buttocks
Knee Trochanter Ankle
0
100
200
300
400
500
600
700
–40 –20 0 20 40 60 80 100
CSA (
cm2)
Relative limb appendicular length (%)
Total Skeletal muscle Adipose tissue Bone
Women
Calf Thigh Buttocks
Trochanter Ankle Knee
Figure 2 Spatial distribution of cross-sectional area (CSA) of skeletal muscle, adiposetissue, bone and total tissue along the lowerlimb, expressed as relative appendicular length(from ischiatic tuberosity to malleoli) in men(upper panel) and women (lower panel).
Table 1 Average values (� SD) of skeletal muscle volume (VSM),mid-thigh muscle cross-sectional area (CSASM) and attenuation(ATTSM), together with volumes of adipose tissue (VAT) and bone(VBO) measured in lower limbs of the subjects taking part in the study.
Males (n = 21) Females (n = 18)
LS (cm) 97�5 � 4�6 87�1 � 3�3***VSM (L) 15�83 � 2�11 10�34 � 1�21***CSASM (cm2) 144�1 � 23�6 101�8 � 13�8***ATTSM (HU) 46�33 � 3�62 43�57 � 4�15*VAT (L) 6�84 � 3�09 9�48 � 3�94*VBO (L) 2�11 � 0�22 1�39 � 0�17***
LS denotes the length of lower limb segment considered for analysis(comprised between the most cranial border of iliac crest and theapex of lateral malleolus). CSASM was determined on right limbs. Adi-pose tissue volume was assessed in the appendicular segment of lowerlimb (comprised between a horizontal plane tangential to ischiatictuberosity and the apex of lateral malleolus); bone volume includesfemur, patella, tibia and fibula (see Methods for further details). Sig-nificance of differences between males and females is assessed with aStudent’s t-test for unpaired data.*P<0�05.***P<0�001.
© 2013 Scandinavian Society of Clinical Physiology and Nuclear Medicine. Published by John Wiley & Sons Ltd 34, 1, 47–55
Adiposity and human leg muscle features, C. L. Lafortuna et al.50

condition, the product VSM/Ls 9 ATTSM (accounting for aver-
age muscle section area) and VSM/BM 9 ATTSM (accounting
for average muscles volume relative to body mass) were consid-
ered. These variables were analysed with a multivariate analysis
of variance after stratifying the whole sample for gender, for
BMI (normal weight, NW, with BMI ≤ 25 kg m�2; overweight
and obese, OW&OB, with BMI > 25 kg m�2) and for age
(younger and older, using the median age (i.e. 53 year.) as a
cut-off). The average values for men and women and for the
different strata of adiposity and age are shown in Table 3 along
with the results of the multivariate analysis. It appears that
VSM/BM 9 ATTSM (expected to predict the individual’s maxi-
mal power performance) is negatively affected by female gen-
der, overweight/obesity and advancing age, whereas VSM/
Ls 9 ATTSM (expected to predict strength maximal capability)
Table 2 Coefficients from multiple linear regression analysis model-ling the independent effect of age and body adiposity (as representedby WCr) on lower limb skeletal muscle characteristics in men andwomen taking part in the study: volume in absolute terms (VSM) orrelative to anatomical length (VSM/LS) and body mass (VSM/BM);mid-thigh cross-sectional area (CSASM) and attenuation (ATTSM).
Coefficient T P Multiple R2
Males (n = 21)VSM (L)Constant 4�960 2�361 0�030 0�759Body adiposity 15�622 7�062 <0�001Age �0�106 �5�178 <0�001
VSM/LS (cm2)Constant 58�60 2�336 0�031 0�658Body adiposity 146�9 5�561 <0�001Age �0�967 �3�959 <0�001
VSM/BM (cm3 kg�1)Constant 260�0 9�504 <0�001 0�305Body adiposity �41�48 �1�440 0�167Age �0�439 �1�650 0�116
CSASM (cm2)Constant 41�80 1�359 0�191 0�587Body adiposity 152�4 4�704 <0�001Age �1�067 �3�563 0�002
ATTSM (HU)Constant 63�803 11�00 <0�001 0�338Body adiposity �14�40 �2�287 0�035Age �0�054 �0�922 0�369
Females (n = 18)VSM (L)Constant 9�915 5�363 <0�001 0�393Body adiposity 3�067 2�051 0�058Age �0�054 �2�652 0�018
VSM/LS (cm2)Constant 110�0 6�034 <0�001 0�425Body adiposity 34�80 2�359 0�016Age �0�543 �2�711 0�025
VSM/BM (cm3 kg�1)Constant 312�5 16�00 <0�001 0�824Body adiposity �124�1 �8�041 <0�001Age �0�217 �1�036 0�316
CSASM (cm2)Constant 111�9 5�213 <0�001 0�376Body adiposity 24�35 1�402 0�181Age �0�672 �2�854 0�012
ATTSM (HU)Constant 60�153 9�625 <0�001 0�339Body adiposity �11�14 �2�529 0�023Age �0�081 �1�130 0�276
R = 0·683P < 0·001
R = 0·214P = 0·05
0
5
10
15
20
25
0·65 0·85 1·05 1·25 1·45
SM
volu
me
(l)
Men
Women
(a)
R = 0·602P < 0·001
R = 0·275P < 0·05
80
100
120
140
160
180
200
220
0·65 0·85 1·05 1·25 1·45
Body adiposity (WCr)
SM
volu
me
per
lim
b len
gth
(cm
2)
Men
Women
(b)
2
2
2
2
Figure 3 The relationship between lower limb skeletal muscle vol-ume and body adiposity. Muscle volume is adjusted for age andexpressed in absolute terms (panel A) or normalized by unit limblength (panel B). Regression lines through the data are also shown.Men (filled circles); women (open circles).
R = 0·039P = 0·392
R = 0·725P < 0·001
0·05
0·10
0·15
0·20
0·25
0·30
0·65 0·85 1·05 1·25 1·45
Body adiposity (WCr)
SM
volu
me
per
BM
(l kg
–1) Men
Women 2
2
Figure 4 The ratio between lower limb skeletal muscle and bodymass (BM) is plotted against body adiposity. Regression lines throughthe data are also shown. Men (filled circles); women (open circles).
© 2013 Scandinavian Society of Clinical Physiology and Nuclear Medicine. Published by John Wiley & Sons Ltd 34, 1, 47–55
Adiposity and human leg muscle features, C. L. Lafortuna et al. 51

is reduced by effect of female gender and advancing age but not
by the degree of body adiposity.
Discussion
The purpose of the study was to assess the effect of body adi-
posity on the characteristics of SM determined with CT imag-
ing and to evaluate the possible functional implications for
movement execution.
Well-grounded evidences indicate that CT imaging is a reli-
able reference method to estimate appendicular skeletal muscle
size and composition, and regional tissue distribution (Mitsio-
poulos et al., 1998; Goodpaster et al., 2000b). Using a correla-
tion approach in a sample of men and women within a
relatively wide range of adiposity (from normal weight to
obesity) and ages (from young adulthood to older age), this
study quantified the (age-independent) influence of body adi-
posity on SM characteristics, which consisted in a gender-spe-
cific positive linear effect on muscle size counterbalanced by a
significant decrease in muscle tissue density.
Although the loss of SM size with advancing age, also pres-
ently detected, is widely known (Doherty, 2003), the effect
of body adiposity on SM quantity and quality has been fairly
less well explored systematically.
Body adiposity and muscle size
The rise of BMI in the continuum from normal weight to
obesity was associated with a progressive increase in absolute
and relative lower limb volume and cross-sectional area of
SM, with a different trend in the two genders. Such a finding
can be viewed as the result of an adaptive muscle response to
increased body mass which acts as a chronic training load
during everyday motor activity. Accordingly, previous studies
detected a gender-related increase also in the amount of fat-
free mass (FFM) as a function of the degree of body adipos-
ity (Hulens et al., 2001; Lafortuna et al., 2005). Indeed, SM is
an adaptable tissue actively responding to mechanical loading,
besides to growth factors and nutrients, and is finely
regulated by a complex and not completely understood cellu-
lar signalling network ultimately controlling muscle protein
synthesis and sarcomere addition (Miyazaki & Esser, 2009).
Unfortunately, at present, no study has been performed to
detect the involvement of any regulatory process possibly
controlling the muscle response to the obesity-related
mechanical overload.
From present results, it can be established that overall leg
muscle volume increases on average by about 2�4 kg every
five BMI units in man and about 1�3 kg in women, when
variations due to age are accounted for.
We detected that women have in general less SM in lower
limbs and more adipose tissue than men, even when adjusted
for the different body size, as a reflection of a gender-related
difference in body composition. Moreover, men and women
seem also to undergo different changes in body composition
along with the increase in body adiposity. Due to the lower
enlargement of SM volume with raising adiposity, in women
of the present study, the ratio VSM/BM (which represents the
amount of the movement actuator in lower limbs available
per unit body mass) decreases considerably as a function of
BMI, with important functional implications, as discussed
below. Similar gender-related trends in the variation in FFM/
BM with the degree of body adiposity have also been reported
previously (Lafortuna et al., 2005).
This raises the hypothesis that different mechanisms may
intervene in men and women to regulate muscle size as a func-
tion of body adiposity. Because no information concerning
lifestyle of the subjects participant to the present study was
available, the role of a different attitude to leisure time physical
activity between genders could not be excluded (Mart�ınez-
Gonz�alez et al., 2001). Nevertheless, it has been observed that
even a prolonged heavy strength training stimulus induces a
significantly greater increase in muscle volume in males than in
females (Ivey et al., 2000). Beside a possible role of the higher
levels of masculine testosterone, several gender-related differ-
ences in the regulation of growth hormone, as differences in
body composition and fat distribution (Roelen et al., 1997),
and in leptin plasma concentration (Llopis et al., 1998), may
participate in determining such as a gender-dependent
response of muscle mass to the increase in body adiposity.
Among the anatomical parameters investigated in the study,
there are important determinants of muscle performance in
static conditions and during movements.
Several investigations report in obesity a maintained or aug-
mented capacity of maximal isometric and isotonic strength
production and higher leg absolute power output (Miyatake
et al., 2000; Hulens et al., 2001; Lafortuna et al., 2002). Inter-
estingly, in obese subjects, the stronger muscle groups, in
comparison with normal weight persons, were those mainly
involved in movements against the force of gravity (Lafortuna
Table 3 Mean values (� SD) of the product of muscle attenuation(ATTSM) by VSM/Ls and by VSM/MB for the different strata of gen-der, body mass index (BMI) and age, and results of multivariate anal-ysis of variance.
VSM/LS 3 ATTSM(cm2 3 HU)
VSM/BM 3 ATTSM(L kg�1 3 HU)
GenderMen 21 7412 � 988 Men 21 9�07 � 1�21Women 18 5150 � 556 Women 18 7�16 � 1�45
ObesityNW 18 6535 � 1430 NW 18 8�94 � 1�47OW&OB 21 6163 � 1376 OW&OB 21 7�55 � 1�50
AgeYounger 20 6863 � 1460 Younger 20 8�61 � 1�66Older 19 5847 � 1150 Older 19 7�74 � 1�51
Effects df F-ratio P Effects df F-ratio PGender 1 70�29 <0�001 Gender 1 26�66 <0�001Obesity 1 0�782 = 0�383 Obesity 1 20�93 <0�001Age 1 9�424 <0�01 Age 1 5�246 <0�05
© 2013 Scandinavian Society of Clinical Physiology and Nuclear Medicine. Published by John Wiley & Sons Ltd 34, 1, 47–55
Adiposity and human leg muscle features, C. L. Lafortuna et al.52

et al., 2005), possibly reflecting the gravity-related nature of
the obesity overload. Nonetheless, as detectable with functional
tests (Lafortuna et al., 2002; Sartorio et al., 2004), obese sub-
jects have markedly reduced capabilities in tasks requiring the
development of explosive anaerobic power, such as climbing
stairs or executing vertical jumps with maximal effort. In fact,
the actual determinant of these performances is the power out-
put per unit body mass, which is notably decreased in persons
with excess of body mass (Lafortuna et al., 2002), due to the
disproportionate increase in fat mass relative to contractile ele-
ments which determine a low muscle to body mass ratio.
Body adiposity and muscle fat infiltration
Present results also reveal a significant reduction in ATTSM
detected through the Hounsfield Units scale of CT imaging for
the effect of body adiposity in both genders, on average
women presenting a lower value of ATTSM than men. Indeed,
attenuation characteristics of tissues in vivo, depending from
their density and electron per unit mass (Bushberg et al.,
1994), provide the basis for differentiating fat and muscle on
CT images and to assess the lipid content in muscle. Due to
the widely lower attenuation coefficient of fat, the interindi-
vidual variation in ATTSM has been shown to reflect the
degree of lipid infiltration (Goodpaster et al., 2000a). By
means of a quantitative evaluation of ATTSM, several investi-
gations detected a higher degree of such infiltration within
muscles in obesity and older age (Kelley et al., 1991; Ryan &
Nicklas, 1999) and found it to be associated with reduced
motor performances (Goodpaster et al., 2001; Visser et al.,
2005; Hilton et al., 2008), along with an increased metabolic
risk (Kelley et al., 1991; Goodpaster et al., 1997; Ryan & Nicklas,
1999). Hence, although muscle size is known to be the
major predictor of force production on a general contest
(Maughan et al., 1983; Fukunaga et al., 2001), qualitative
attributes related to muscle composition may be important in
determining the association between muscle mass and its
function.
Functional considerations
In practice, the structural gender-dependent changes associated
with body adiposity are expected to combine with the effects
induced by advancing age, and likely determine a complex sit-
uation for muscle functionality.
Thus, in older obese adults, the combination of increased
body adiposity reducing the relative size of lower limb SM
per unit body mass (and hence power) and advancing age
reducing the size of SM (and hence strength) produces a con-
dition with potentially very serious consequences on health
and disability (Jensen & Hsiao, 2010), especially for women
who are inherently provided with a smaller volume of muscle
with lower density and responding to adiposity overload with
a minor increase. In view of the rising number of obese older
individuals (Flegal et al., 2002), the detailed knowledge of the
concomitant effects induced on muscles by obesity and ageing
could be relevant for the appropriate identification, prevention
and treatment of this motor frailty.
To characterize the functional implications for movements
deriving from the different variations in muscular size and
composition, we devised an index integrating the trends in
leg muscle characteristics presently observed. Thus, ATTSM
(denoting the amount of contractile elements within the mus-
cle) was combined with VSM/Ls, representing the average
muscle section area in the lower limb and related to muscle
strength (VSM/Ls 9 ATTSM), and with VSM/BM, indicating
the average volume of lower limb muscle per unit body mass
and related to muscle explosive performance (VSM/BM
9 ATTSM). According with functional observations reporting
a decline of specific power output with a preserving of
strength capabilities in obesity (Hulens et al., 2001; Lafortuna
et al., 2002, 2005), the index denoting dynamic performance
results significantly reduced by female gender, overweight/
obesity condition and older age, while the strength index is
decreased by female gender and older age, but not by adipos-
ity excess. Thus, the concomitance of obesity and older age in
females appears to involve a particularly unfavourable condi-
tion for muscle structural characteristics expected to produce a
functional derangement of dynamic performance. As also
experimentally evidenced (Lafortuna et al., 2004), older
women with high degree of obesity are prone to suffer from
major dysfunctions in movements which may interfere with
everyday locomotor abilities and even lead towards thresholds
for impaired mobility. Nonetheless, although consistent with
functional observations, the physiological representativeness of
these structural indices should be carefully evaluated and
further investigation seems to be necessary.
In conclusion, this study revealed in this sample of subjects
that while advancing age had a negative effect on quantitative
attributes of lower limb SM, raising body adiposity had a
positive influence on these, but were also accompanied by
unfavourable qualitative changes represented by a reduction in
muscle density. Moreover, as the enlargement of SM size
under the effect of increasing body adiposity was notably less
prominent in females, who also have a lower muscle density,
overweight/obese women (especially in older age) experience
a conspicuous decrease in lower limb SM volume available for
sustaining body movements and appear to be more damaged
than men by the obesity-related imbalance between the
amount of contractile elements and body mass.
Although a previous diagnosis of melanoma common to all
participants to the study unlikely affected the characteristics of
SM presently investigated, our findings cannot be considered
as the outcome of a population-based investigation and gen-
eral conclusions should be drawn with some caution.
Nevertheless, implications deriving from these results may
have a potential clinical impact on the formulation of physical
activity protocols using exercise as an intervention tool for
treating body mass excess and contrasting motor disabilities of
overweight/obese individuals at different ages of life.
© 2013 Scandinavian Society of Clinical Physiology and Nuclear Medicine. Published by John Wiley & Sons Ltd 34, 1, 47–55
Adiposity and human leg muscle features, C. L. Lafortuna et al. 53

Acknowledgments
The authors gratefully thank Dr Luigi Gianolli, Department of
Nuclear Medicine, Scientific Institute San Raffaele, Milano,
Italy, for providing patient and CT data.
Funding
Partially financed by the project Platform for International Col-
laborative Knowledge on Food Improvement Based on Ecolog-
ical Resources (PICKFIBER), Grant No. 0120R1/21,
(subproject in the miniprogramme Innovation 4 Welfare),
funded by INTERREG IVC Programme.
Conflict of interest
The authors declare that there is no conflict of interest that
could be perceived as prejudicing the impartiality of the
reported information.
References
Alberti KG, Zimmet P, Shaw J. Metabolic syn-drome – a new world-wide definition. A
consensus statement from the InternationalDiabetes Federation. Diabet Med (2006); 23:
469–480.Bushberg JT, Seibert JA, Leidholdt EMJ, Boone
JM. X-ray computed tomography. In: TheEssentials of Medical Imaging. (ed. Passano, WM)
(1994), pp. 239–289. Williams & Wilkins,Baltimore, MD.
Doherty TJ. Invited review: aging and sarco-penia. J Appl Physiol (2003); 95: 1717–1727.
Evans WJ. Skeletal muscle loss: cachexia, sar-copenia, and inactivity. Am J Clin Nutr
(2010); 91: 1123S–1127S.
Evers Larsson U, Mattsson E. Functional lim-itations linked to high body mass index,
age and current pain in obese women.Int J Obes Relat Metab Disord (2001); 25:
893–899.Flegal KM, Carroll MD, Ogden CL, Johnson
CL. Prevalence and trends in obesity amongUS adults, 1999–2000. JAMA (2002); 288:
1723–1727.Fukunaga T, Miyatani M, Tachi M, Kouzaki
M, Kawakami Y, Kanehisa H. Muscle vol-ume is a major determinant of joint torque
in humans. Acta Physiol Scand (2001); 172:249–255.
Goldszal AF, Pham DL. Volumetric segmenta-tion. In: Handbook of Medical Imaging: Processing
and Analysis. (ed. Bankman, IN) (2000), pp.185–194. Academic Press, London, UK.
Goodpaster BH, Thaete FL, Simoneau JA, Kel-ley DE. Subcutaneous abdominal fat and
thigh muscle composition predict insulinsensitivity independently of visceral fat. Dia-
betes (1997); 46: 1579–1585.Goodpaster BH, Kelley DE, Thaete FL, He J,
Ross R. Skeletal muscle attenuation deter-mined by computed tomography is associ-
ated with skeletal muscle lipid content. JAppl Physiol (2000a); 89: 104–110.
Goodpaster BH, Thaete FL, Kelley DE. Com-position of skeletal muscle evaluated with
computed tomography. Ann N Y Acad Sci(2000b); 904: 18–24.
Goodpaster BH, Carlson CL, Visser M, KelleyDE, Scherzinger A, Harris TB, Stamm E,
Newman AB. Attenuation of skeletal muscleand strength in the elderly: the health ABC
study. J Appl Physiol (2001); 90: 2157–2165.Hilton TN, Tuttle LJ, Bohnert KL, Mueller MJ,
Sinacore DR. Excessive adipose tissue infil-tration in skeletal muscle in individuals
with obesity, diabetes mellitus, and periph-
eral neuropathy: association with perfor-mance and function. Phys Ther (2008); 88:
1336–1344.Hulens M, Vansant G, Lysens R, Claessens AL,
Muls E, Brumagne S. Study of differences inperipheral muscle strength of lean versus
obese women: an allometric approach. Int JObes Relat Metab Disord (2001); 25: 676–681.
Ivey FM, Roth SM, Ferrell RE, Tracy BL,Lemmer JT, Hurlbut DE, Martel GF, Siegel
EL, Fozard JL, Jeffrey Metter E, Fleg JL,Hurley BF. Effects of age, gender, and myo-
statin genotype on the hypertrophicresponse to heavy resistance strength train-
ing. J Gerontol A Biol Sci Med Sci (2000); 55:M641–M648.
Janssen I, Heymsfield SB, Baumgartner RN,Ross R. Estimation of skeletal muscle mass
by bioelectrical impedance analysis. J ApplPhysiol (2000): 89: 465–471.
Janssen I, Heymsfield SB, Ross R. Low relativeskeletal muscle mass (sarcopenia) in older
persons is associated with functionalimpairment and physical disability. J Am Ge-
riatr Soc (2002); 50: 889–896.Jensen GL, Hsiao PY. Obesity in older adults:
relationship to functional limitation. CurrOpin Clin Nutr Metab Care (2010); 13: 46–51.
Kelley DE, Slasky BS, Janosky J. Skeletal mus-cle density: effects of obesity and non-insu-
lin-dependent diabetes mellitus. Am J ClinNutr (1991); 54: 509–515.
Kim J, Wang Z, Heymsfield SB, Baumgartner
RN, Gallagher D. Total-body skeletal musclemass: estimation by a new dual-energy X-
ray absorptiometry method. Am J Clin Nutr(2002); 76: 378–383.
Lafortuna CL. Physiological bases of physicallimitations during exercise. In: Disabling Obes-
ity (eds Capodaglio, P, Faintuch, J, Liuzzi,
A) (2013) Springer-Verlag, Berlin, Heidel-berg. DOI: 10.1007/978-3-642-35972-
9_2.Lafortuna CL, Fumagalli E, Vangeli V,
Sartorio A. Lower limb alactic anaerobicpower output assessed with different tech-
niques in morbid obesity. J Endocrinol Invest(2002); 25: 134–141.
Lafortuna CL, Agosti F, Marinone PG, Marazzi
N, Sartorio A. The relationship betweenbody composition and muscle power out-
put in men and women with obesity. JEndocrinol Invest (2004); 27: 854–861.
Lafortuna CL, Maffiuletti NA, Agosti F, Sarto-rio A. Gender variations of body composi-
tion, muscle strength and power output inmorbid obesity. Int J Obes (Lond) (2005); 29:
833–841.Llopis MA, Granada ML, Cuatrecasas G, Form-
iguera X, S�anchez-Planell L, Sanmart�ı A,Alastru�e A, Rull M, Corominas A, Foz M.
Growth hormone-binding protein directlydepends on serum leptin levels in adults
with different nutritional status. J Clin Endo-crinol Metab (1998); 83: 2006–2011.
Mart�ınez-Gonz�alez MA, Varo JJ, Santos JL, DeIrala J, Gibney M, Kearney J, Mart�ınez JA.
Prevalence of physical activity during leisuretime in the European Union. Med Sci Sports
Exerc (2001); 33: 1142–1146.Maughan RJ, Watson JS, Weir J. Strength and
cross-sectional area of human skeletal mus-cle. J Physiol (1983); 338: 37–49.
McAuliffe MJ, Lalonde FM, McGarry D, Gan-dler W, Csaky K, Trus BL. Medical image
processing, analysis and visualization inclinical research. In: Computer-Based Medical
System, 2001 (CBMS 2001), Proceedings of the14th IEEE Symposium on Computer-Based Medical
Systems, 26–27 Jul 2001, pp. 381–386.Bethesda, MD. Available at http://ieeexpl
ore.ieee.org/xpl/mostRecentIssue.jsp?punum
ber=7489Mitsiopoulos N, Baumgartner RN, Heymsfield
SB, Lyons W, Gallagher D, Ross R. Cadavervalidation of skeletal muscle measurement
by magnetic resonance imaging and com-puterized tomography. J Appl Physiol (1998);
85: 115–122.
54 Adiposity and human leg muscle features, C. L. Lafortuna et al.
© 2013 Scandinavian Society of Clinical Physiology and Nuclear Medicine. Published by John Wiley & Sons Ltd 34, 1, 47–55

Miyatake N, Fujii M, Nishikawa H, Wada J,
Shikata K, Makino H, Kimura I. Clinicalevaluation of muscle strength in 20–79-
years-old obese Japanese. Diabetes Res ClinPract (2000); 48: 15–21.
Miyazaki M, Esser KA. Cellular mechanismsregulating protein synthesis and skeletal
muscle hypertrophy in animals. J Appl Physiol(2009); 106: 1367–1373.
Roelen CA, Koppeschaar HP, de Vries WR,Snel YE, Doerga ME, Zelissen PM, Thijssen
JH, Blankenstein MA. Visceral adipose tis-sue is associated with circulating high
affinity growth hormone-binding protein.J Clin Endocrinol Metab (1997); 82: 760–
764.Ross R, Goodpaster B, Kelley D, Boada F.
Magnetic resonance imaging in human
body composition research. From quantita-
tive to qualitative tissue measurement. AnnN Y Acad Sci (2000); 904: 12–17.
Ryan AS, Nicklas BJ. Age-related changes infat deposition in mid-thigh muscle in
women: relationships with metabolic car-diovascular disease risk factors. Int J Obes Relat
Metab Disord (1999); 23: 126–132.Sartorio A, Proietti M, Marinone PG, Agosti F,
Adorni F, Lafortuna CL. Influence of gen-der, age and BMI on lower limb muscular
power output in a large population of obesemen and women. Int J Obes Relat Metab Disord
(2004); 28: 91–98.Visser M, Goodpaster BH, Kritchevsky SB,
Newman AB, Nevitt M, Rubin SM, Simon-sick EM, Harris TB. Muscle mass, muscle
strength, and muscle fat infiltration as
predictors of incident mobility limita-
tions in well-functioning older persons. JGerontol A Biol Sci Med Sci (2005); 60: 324–
333.Walter S, Kunst A, Mackenbach J, Hofman A,
Tiemeier H. Mortality and disability: theeffect of overweight and obesity. Int J Obes
(Lond) (2009); 33: 1410–1418.World Health Organization. Measuring obesity
- Classification and description of anthropo-metric data. Report on a WHO consultation
on the epidemiology of obesity. EUR/ICP/NUT 125. (1987). WHO regional office for
Europe, Warsaw.Zar JH. Biostatistical Analysis (1984). Prentice-
Hall International Editions, Englewood Cliff,NJ.
© 2013 Scandinavian Society of Clinical Physiology and Nuclear Medicine. Published by John Wiley & Sons Ltd 34, 1, 47–55
Adiposity and human leg muscle features, C. L. Lafortuna et al. 55