Il dilemma troponine nei percorsi ospedalieri di diagnosi ... · e cura »Dott.ssa Daria BROGI...
63
Il dilemma troponine nei percorsi ospedalieri di diagnosi e cura »Dott.ssa Daria BROGI Cardiologia, Lucca Ospedale San Luca Conflitti di Interesse: nessuno Lucca 27 Novembre 2014
Transcript of Il dilemma troponine nei percorsi ospedalieri di diagnosi ... · e cura »Dott.ssa Daria BROGI...
Il dilemma troponine nei
percorsi ospedalieri di diagnosi
e cura
»Dott.ssa Daria BROGI
Cardiologia, Lucca
Ospedale San Luca
Conflitti di Interesse: nessuno
Lucca 27 Novembre 2014
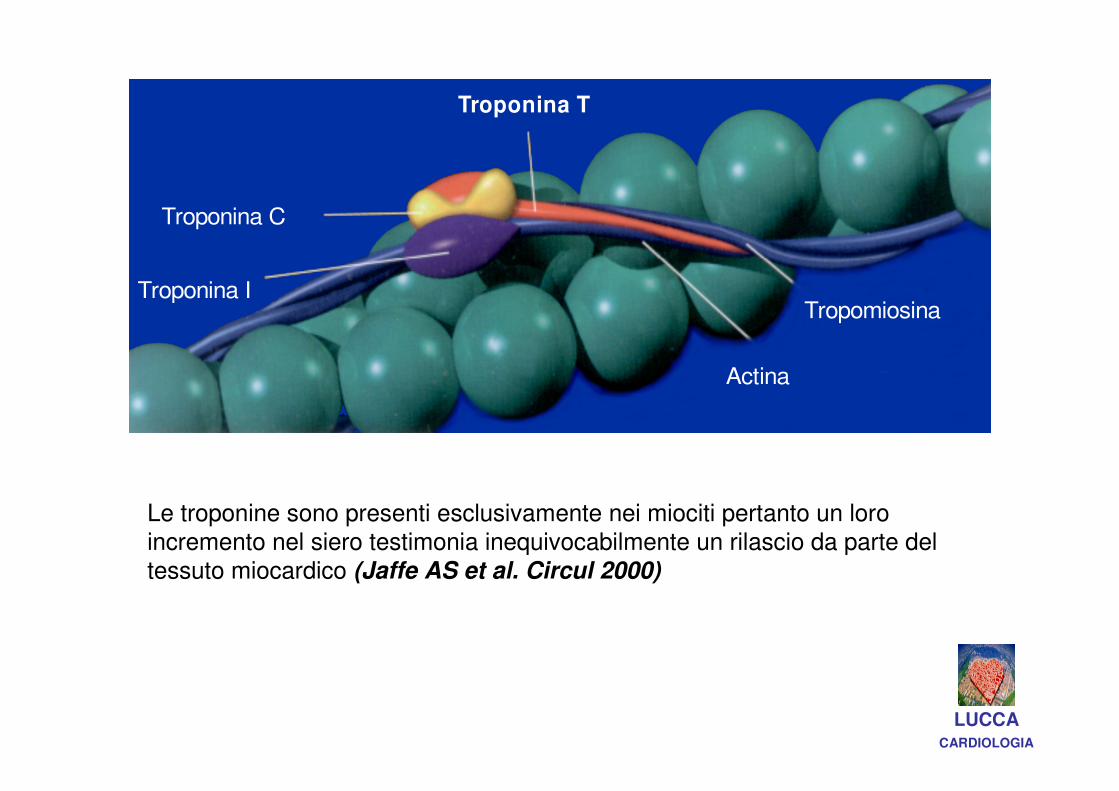
Actina
Tropomiosina
Troponina T
Troponina C
Troponina I
Le troponine sono presenti esclusivamente nei miociti pertanto un loro incremento nel siero testimonia inequivocabilmente un rilascio da parte del
tessuto miocardico (Jaffe AS et al. Circul 2000)
LUCCACARDIOLOGIA
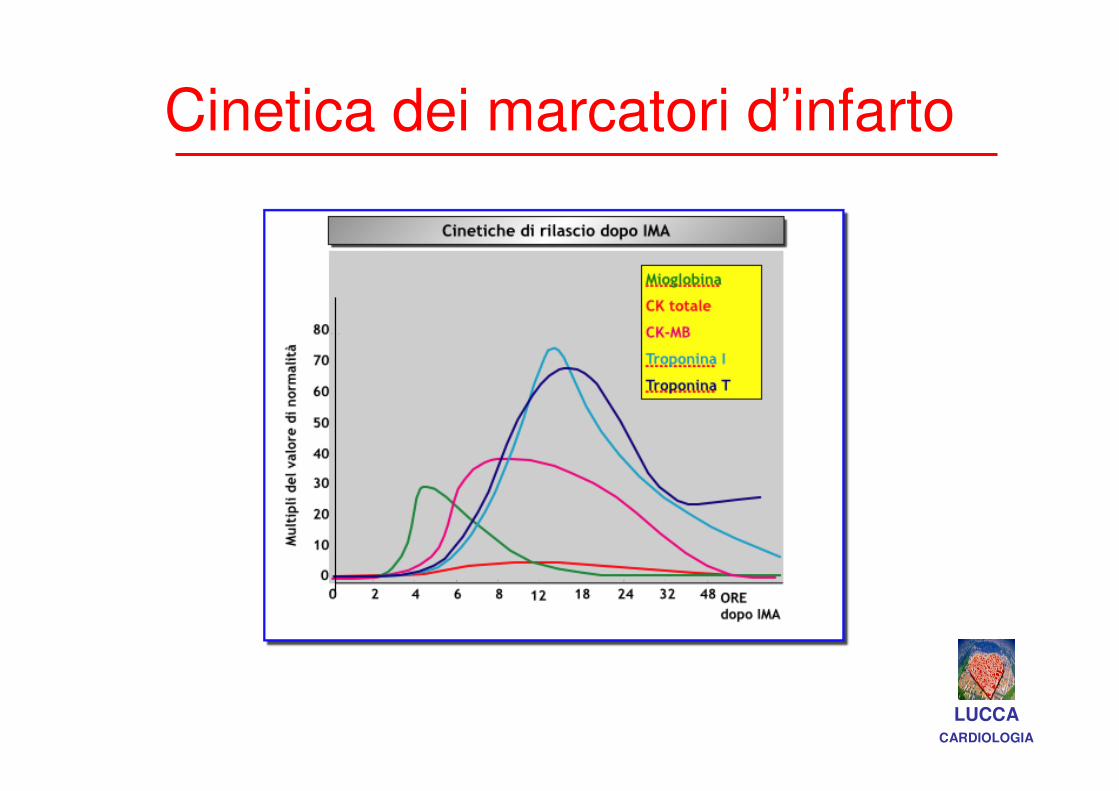
Cinetica dei marcatori d’infarto
LUCCACARDIOLOGIA
Editorial It’s Time for a Change to a Troponin Standard
Allan S. Jaffe, MD; Jan Ravkilde, MD, DMSc; Robert Roberts, MD; Ulf Naslund, MD,
PhD; Fred S. Apple, PhD; Marcello Galvani, MD; Hugo Katus, MD, PhD
Circulation 2000;102:1216-1220
We recommend for the preferred markers (cTnI and cTnT) and for CK-MB that the upper limit be defined as the 99th percentile.
This information should be available from peer-reviewed information published for each of these assays, along with an acceptable level (<10%) of analytical variability in precision at this level of detection.
LUCCACARDIOLOGIA
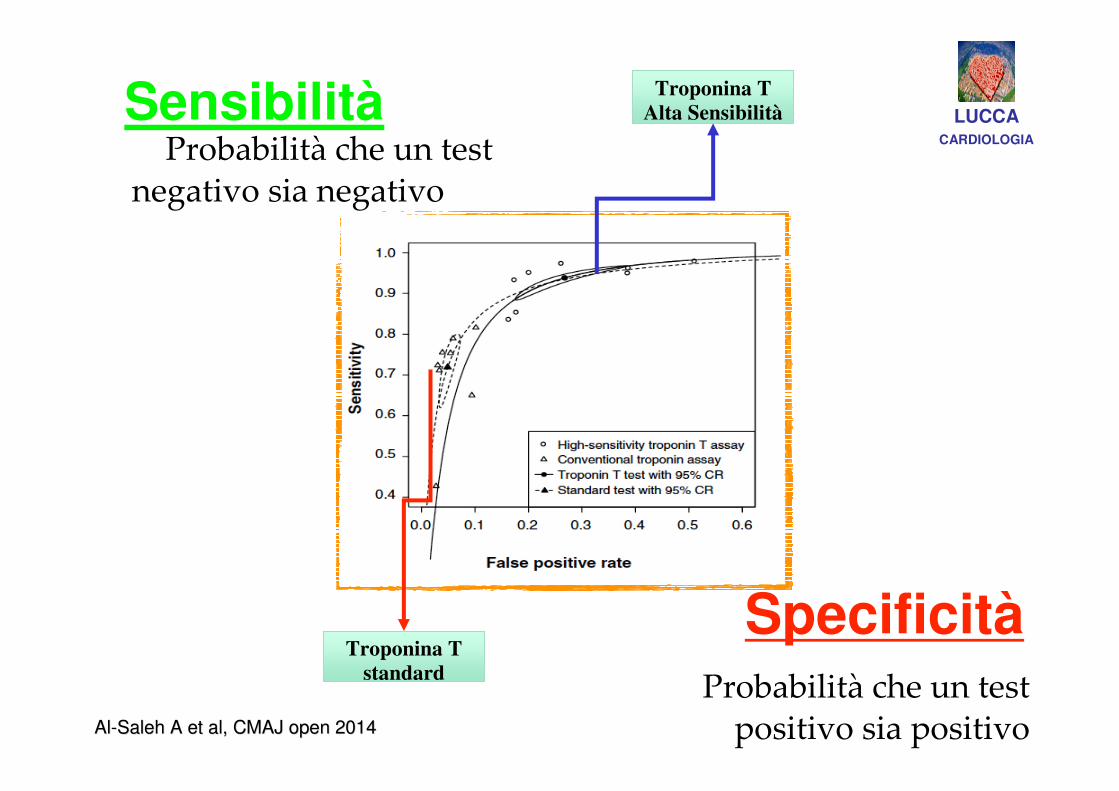
SensibilitàProbabilità che un test
negativo sia negativo sia negativo
SpecificitàProbabilità che un test
positivo sia positivo
Troponina T standard
Troponina T Alta Sensibilità LUCCA
CARDIOLOGIA
AlAl--Saleh A et al, CMAJ open 2014Saleh A et al, CMAJ open 2014
SensibilitàCapacità di
identificare i sani
LUCCACARDIOLOGIA
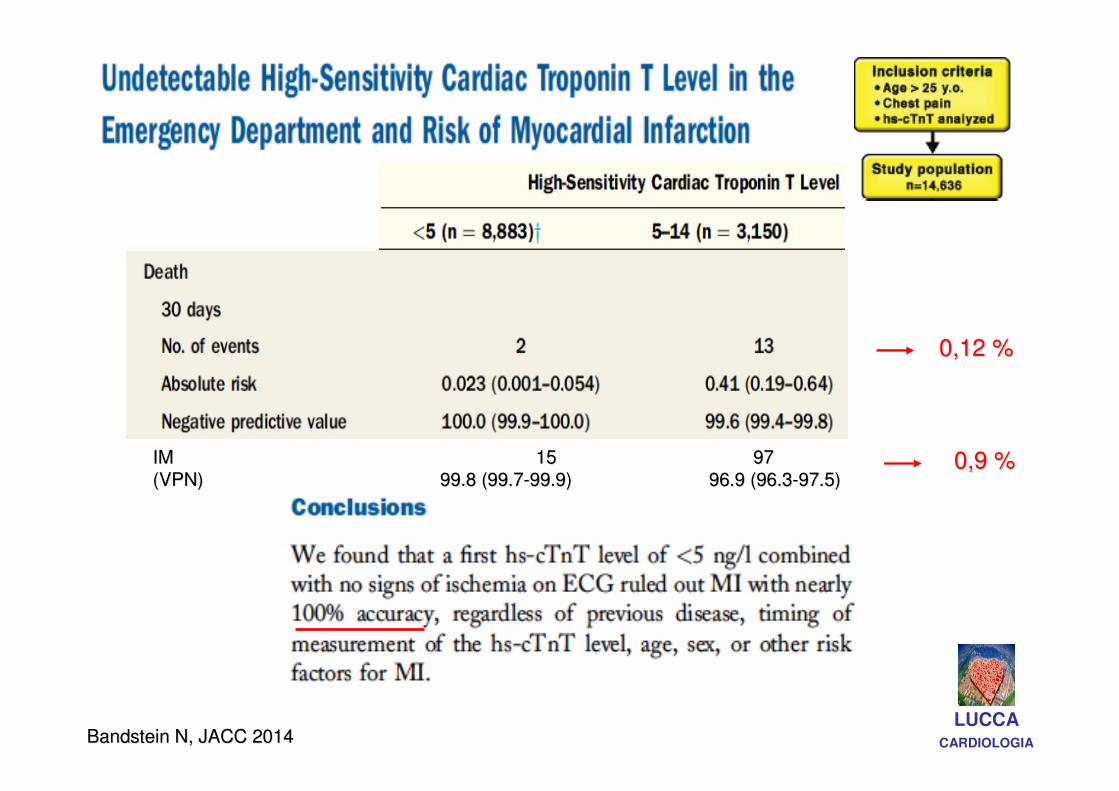
Bandstein N, JACC 2014Bandstein N, JACC 2014LUCCA
CARDIOLOGIA
0,12 %0,12 %
0,9 %0,9 %IMIM 1515 9797
(VPN)(VPN) 99.8 (99.799.8 (99.7--99.9)99.9) 96.9 (96.396.9 (96.3--97.5)97.5)
SensibilitàCapacità di
identificare i sani
Specificità
Capacità di
identificare i malati
LUCCACARDIOLOGIA
DILEMMA troponine!!DILEMMA troponine!!
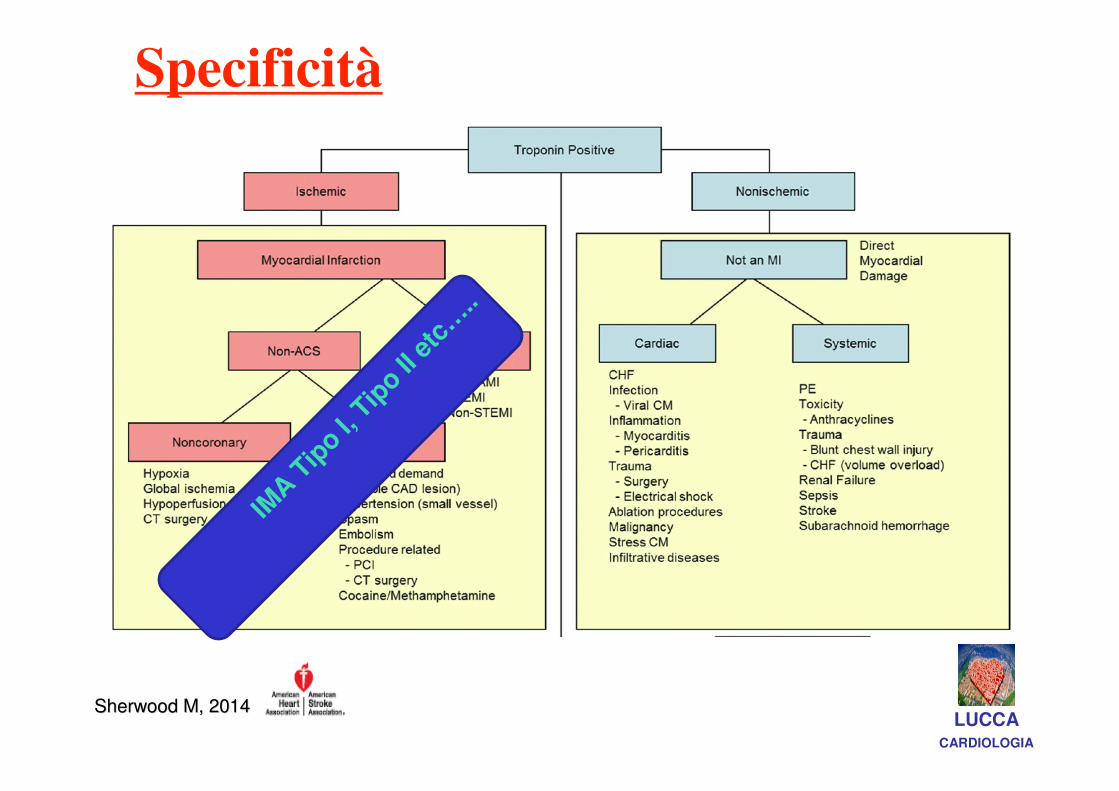
Specificità
Capacità di
identificare i malati
IMA
Tip
o I, T
ipo II
etc
…..
Sherwood M, 2014Sherwood M, 2014LUCCA
CARDIOLOGIA

20051980
Cardiac Biomarkers
Giannitsis E, et al. Clin Chem 2010;56:254-261 LUCCACARDIOLOGIA
Early Diagnosis of Myocardial InfarctionEarly Diagnosis of Myocardial Infarction
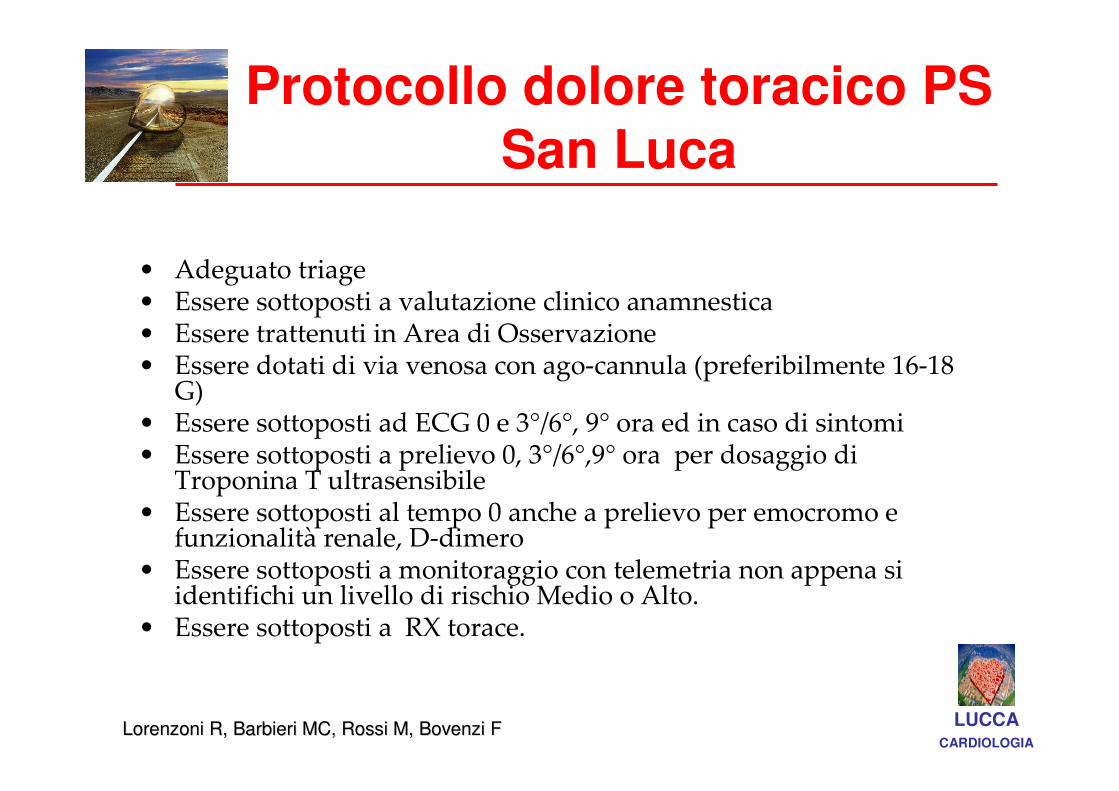
Protocollo dolore toracico PS San Luca
• Adeguato triage• Essere sottoposti a valutazione clinico anamnestica • Essere trattenuti in Area di Osservazione • Essere dotati di via venosa con ago-cannula (preferibilmente 16-18
G)• Essere sottoposti ad ECG 0 e 3°/6°, 9° ora ed in caso di sintomi• Essere sottoposti a prelievo 0, 3°/6°,9° ora per dosaggio di
Troponina T ultrasensibile• Essere sottoposti al tempo 0 anche a prelievo per emocromo e
funzionalità renale, D-dimero• Essere sottoposti a monitoraggio con telemetria non appena si
identifichi un livello di rischio Medio o Alto.• Essere sottoposti a RX torace.
LUCCACARDIOLOGIA
Lorenzoni R, Barbieri MC, Rossi M, Bovenzi FLorenzoni R, Barbieri MC, Rossi M, Bovenzi F
..ma avere
una Ferrari non vuol
dire saperla guidare!
LUCCACARDIOLOGIA
“overdiagnosisof acute coronary syndromes because of the increased sensitivity
of the high-sensitivity troponin test???”
“an assay that is very sensitive but has low specificity may lead to unnecessary
Investigations”.
……..APPROPRIATEZZA..APPROPRIATEZZA……..
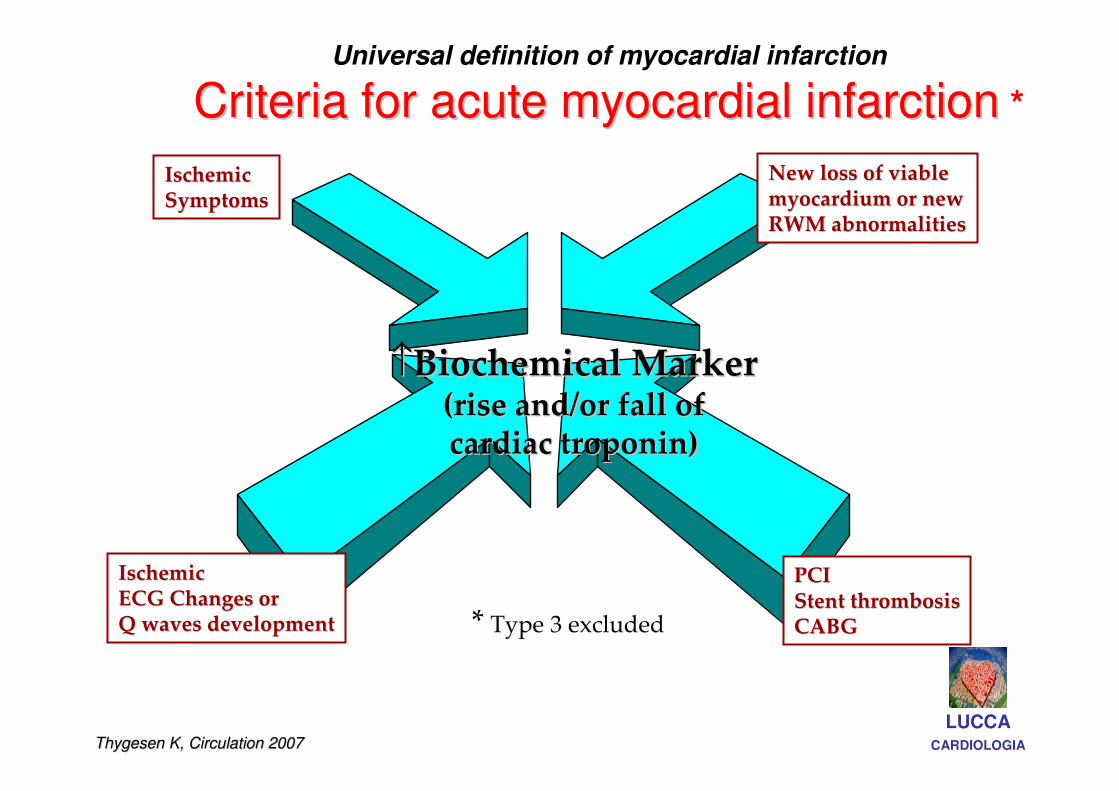
Universal definition of myocardial infarction
Criteria for acute myocardial infarctionCriteria for acute myocardial infarction *
↑↑Biochemical MarkerBiochemical Marker(rise and/or fall of(rise and/or fall ofcardiac troponin)cardiac troponin)
Ischemic Ischemic SymptomsSymptoms
New loss of viable New loss of viable myocardium or newmyocardium or newRWM abnormalitiesRWM abnormalities
Ischemic Ischemic ECG Changes orECG Changes orQ waves developmentQ waves development
PCIPCIStent thrombosisStent thrombosisCABGCABG* Type 3 excluded
LUCCACARDIOLOGIAThygesen K, Circulation 2007Thygesen K, Circulation 2007
Turno di guardiaTurno di guardia
Nei tre mesi successivi l’entrata in vigore della metodica us, in collaborazione con i
colleghi del PS del nostro dipartimento, abbiamo osservato che:
• Tn primo esame richiesto in PS (più dell’emocromo!)
• Richiesta per dolore toracico (48%), dispnea (12%), dolore addominale (6,3%),
sincope (5%), tachicardia (5%), crisi ipertensiva ( 1%), distrurbi neurologici (1,1%),
traumi toracici (1%), febbre 0,6%, altro (confusione mentale,vomito…) 20%
• Elevata nel 44% dei casi
Brogi D, Scannavacca ABrogi D, Scannavacca A
““astute physician must be able to astute physician must be able to interpretinterpret cTn as a cTn as a
dynamic marker of myocardial damage, using clinical dynamic marker of myocardial damage, using clinical
acumen to determine the source of significance of any acumen to determine the source of significance of any
reported c Tn increasereported c Tn increase”” vs vs ……frequently considered a frequently considered a
clinical confounder ??clinical confounder ??
Kelley, Clin Chemistry 2009Kelley, Clin Chemistry 2009
LUCCACARDIOLOGIA
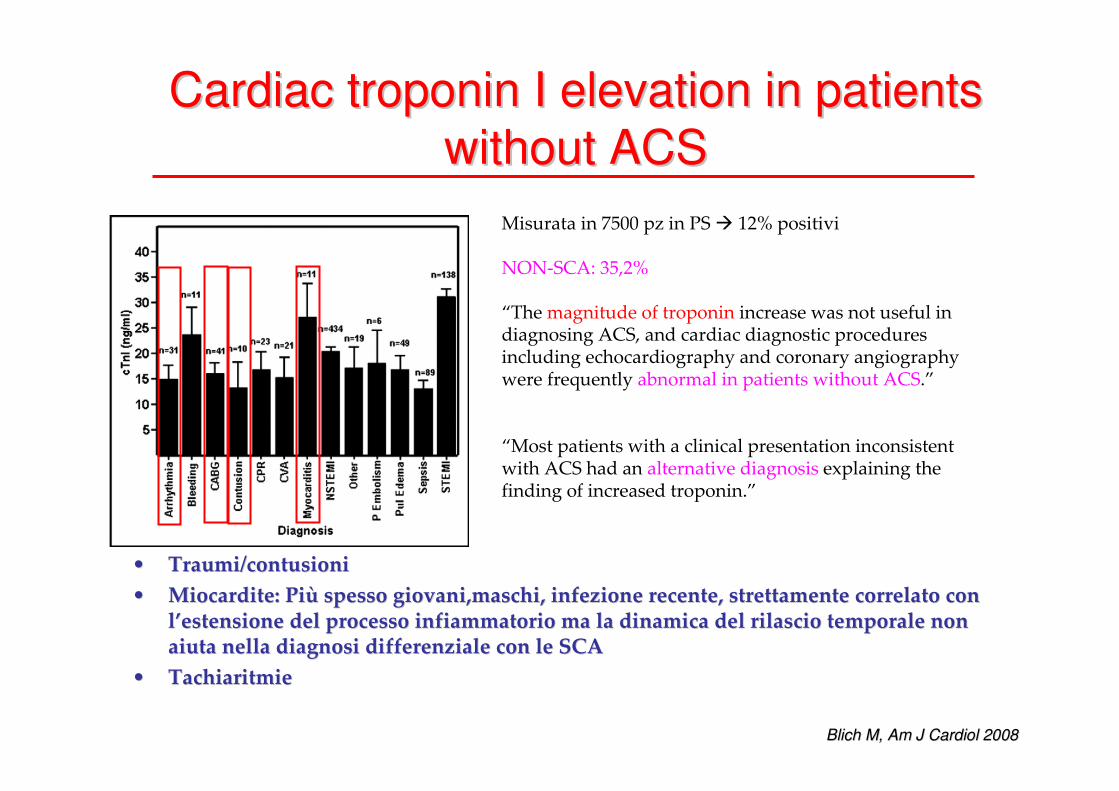
Cardiac troponin I elevation in patients Cardiac troponin I elevation in patients
without ACSwithout ACS
Blich M, Am J Cardiol 2008Blich M, Am J Cardiol 2008
Misurata in 7500 pz in PS � 12% positivi
NON-SCA: 35,2%
“The magnitude of troponin increase was not useful in diagnosing ACS, and cardiac diagnostic proceduresincluding echocardiography and coronary angiographywere frequently abnormal in patients without ACS.”
“Most patients with a clinical presentation inconsistent with ACS had an alternative diagnosis explaining the finding of increased troponin.”
•• Traumi/contusioniTraumi/contusioni
•• Miocardite: PiMiocardite: Piùù spesso giovani,maschi, infezione recente, strettamente correlatspesso giovani,maschi, infezione recente, strettamente correlato con o con ll’’estensione del processo infiammatorio ma la dinamica del rilasciestensione del processo infiammatorio ma la dinamica del rilascio temporale non o temporale non aiuta nella diagnosi differenziale con le SCAaiuta nella diagnosi differenziale con le SCA
•• TachiaritmieTachiaritmie
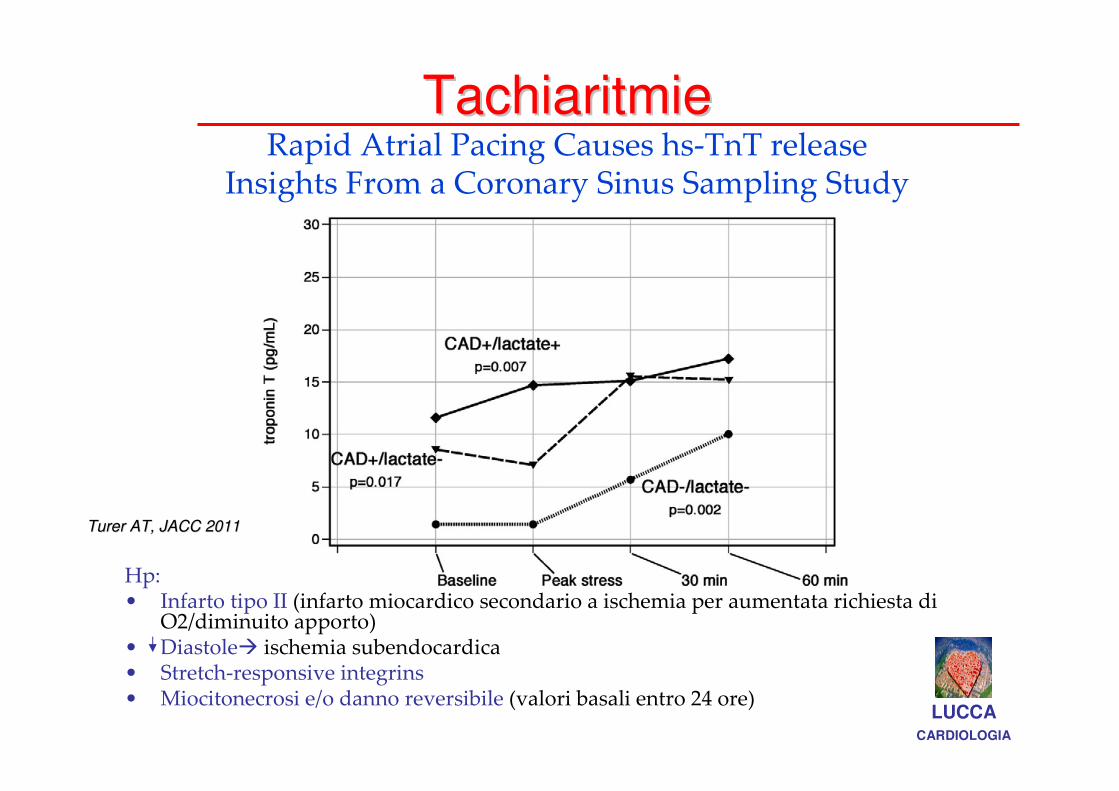
TachiaritmieTachiaritmieRapid Atrial Pacing Causes hs-TnT release
Insights From a Coronary Sinus Sampling Study
Hp:• Infarto tipo II (infarto miocardico secondario a ischemia per aumentata richiesta di
O2/diminuito apporto)• Diastole� ischemia subendocardica • Stretch-responsive integrins• Miocitonecrosi e/o danno reversibile (valori basali entro 24 ore)
LUCCACARDIOLOGIA
Turer AT, JACC 2011Turer AT, JACC 2011
Eur Heart J 2011;32:404Eur Heart J 2011;32:404--1111
Discrimination of type 2 MI is challenging!
LUCCACARDIOLOGIA

Malattie DellMalattie Dell’’App.RespiratorioApp.Respiratorio
Embolia PolmonareEmbolia Polmonare
�� Strain acuto del ventricolo destro secondario allStrain acuto del ventricolo destro secondario all’’incremento incremento della resistenza arteriosa polmonaredella resistenza arteriosa polmonare (Meyer T et al, JACC 2000)(Meyer T et al, JACC 2000)
�� Ipossiemia secondaria al mismatch perfusioneIpossiemia secondaria al mismatch perfusione--ventilazioneventilazione(Agewell S et al, Eur Heart J 2011)(Agewell S et al, Eur Heart J 2011)
�� Ipoperfusione come conseguenza del basso output e flusso Ipoperfusione come conseguenza del basso output e flusso coronarico ridottocoronarico ridotto (Agewell S et al, Eur Heart J 2011)(Agewell S et al, Eur Heart J 2011)
BPCO BPCO -- ARDSARDS
� Infiammazione ed incremento neutrofili, anemia (Brekke PH et al, BMC (Brekke PH et al, BMC
Pulmonary Medicine 2009) Pulmonary Medicine 2009)
� Ipossiemia, tachicardia (Kelley WE,Clinical Chem 2009)(Kelley WE,Clinical Chem 2009)
� Danno ossidativo vascolare (Brekke PH et al, BMC Pulmonary Medicine 2009)(Brekke PH et al, BMC Pulmonary Medicine 2009)
Cinetica del Cinetica del rilasciorilascio diversa dalle SCAdiversa dalle SCA LUCCACARDIOLOGIA
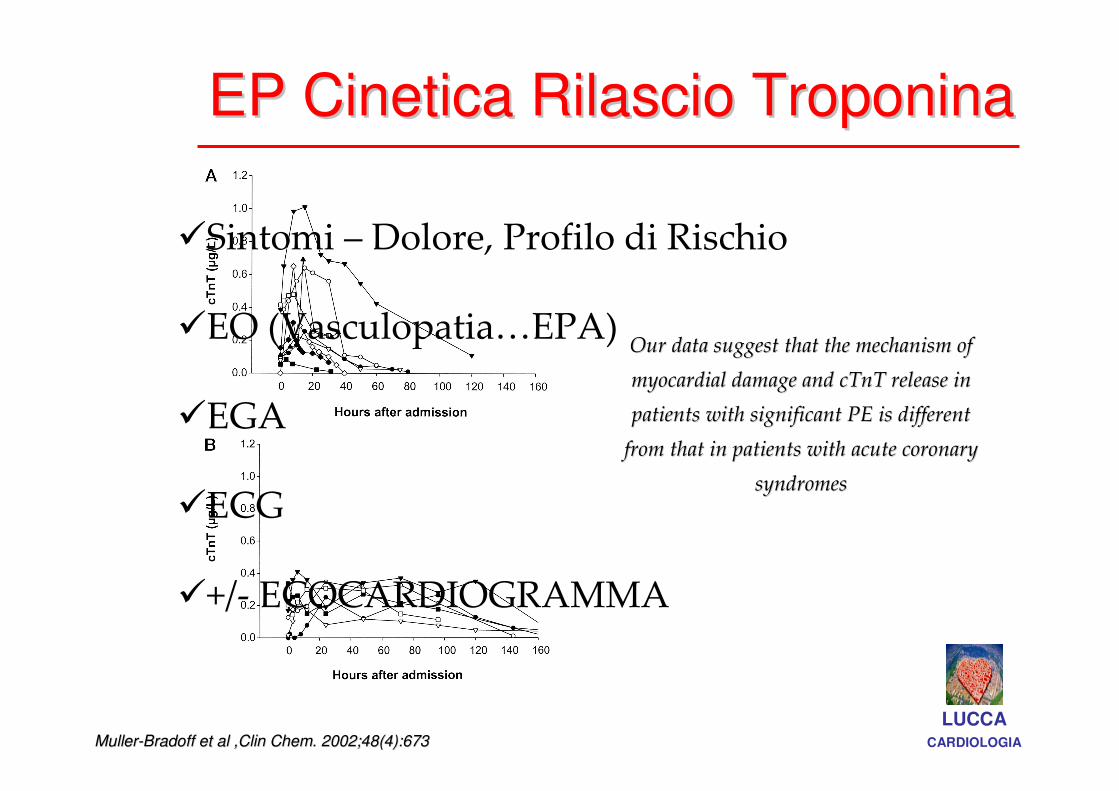
EP Cinetica Rilascio TroponinaEP Cinetica Rilascio Troponina
MullerMuller--Bradoff et al ,Clin Chem. 2002;48(4):673Bradoff et al ,Clin Chem. 2002;48(4):673
Our data suggest that the mechanism of Our data suggest that the mechanism of
myocardial damage and cTnT release in myocardial damage and cTnT release in
patients with significant PE is different patients with significant PE is different
from that in patients with acute coronary from that in patients with acute coronary
syndromessyndromes
LUCCACARDIOLOGIA
�Sintomi – Dolore, Profilo di Rischio
�EO (Vasculopatia…EPA)
�EGA
�ECG
�+/- ECOCARDIOGRAMMA
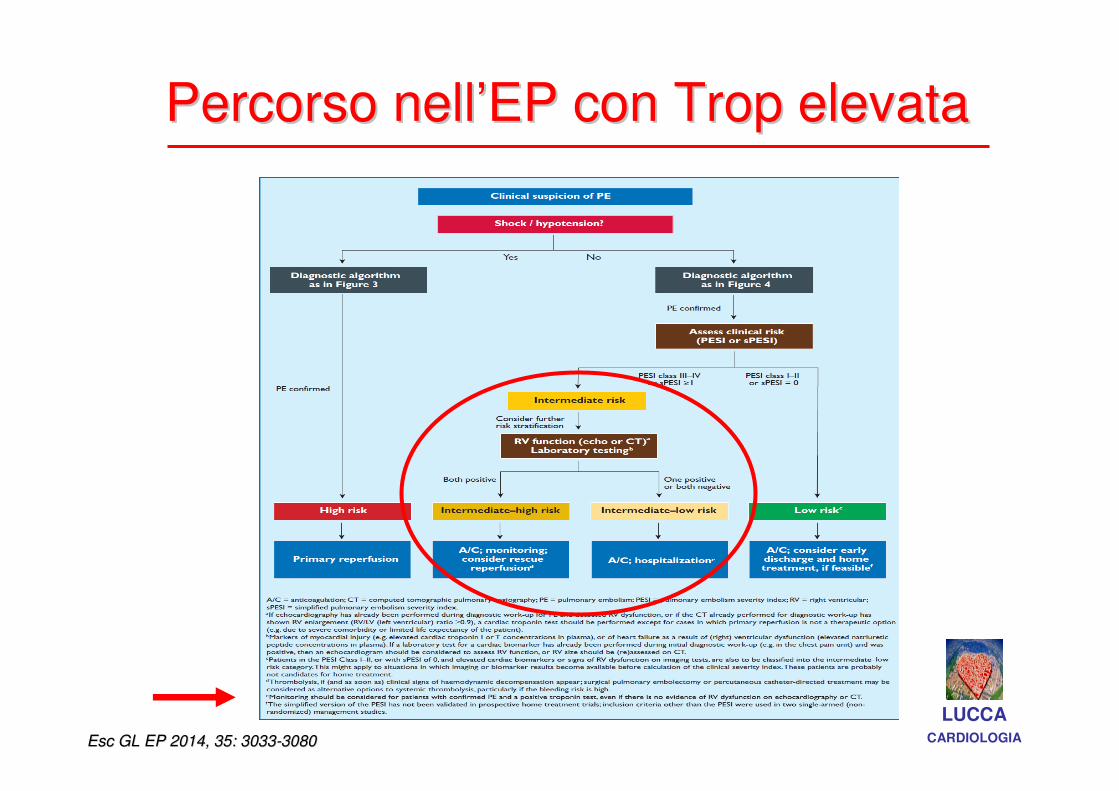
Percorso nellPercorso nell’’EP con Trop elevataEP con Trop elevata
LUCCACARDIOLOGIAEsc GL EP 2014, 35: 3033Esc GL EP 2014, 35: 3033--30803080
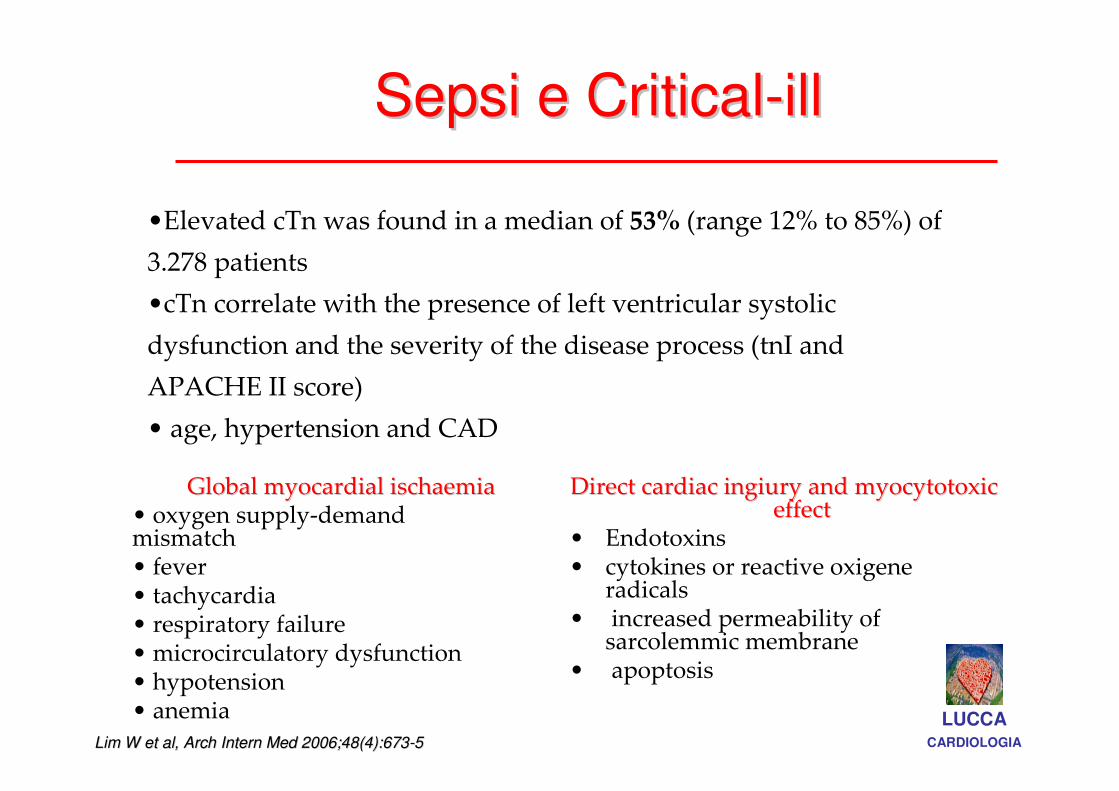
Sepsi e CriticalSepsi e Critical--illill
Lim W et al, Arch Intern Med 2006;48(4):673Lim W et al, Arch Intern Med 2006;48(4):673--5 5
Direct cardiac ingiury and myocytotoxic Direct cardiac ingiury and myocytotoxic effecteffect
• Endotoxins• cytokines or reactive oxigene
radicals• increased permeability of
sarcolemmic membrane• apoptosis
•Elevated cTn was found in a median of 53% (range 12% to 85%) of
3.278 patients
•cTn correlate with the presence of left ventricular systolic
dysfunction and the severity of the disease process (tnI and
APACHE II score)
• age, hypertension and CAD
Global myocardial ischaemiaGlobal myocardial ischaemia• oxygen supply-demand mismatch• fever• tachycardia • respiratory failure• microcirculatory dysfunction• hypotension• anemia LUCCA
CARDIOLOGIA
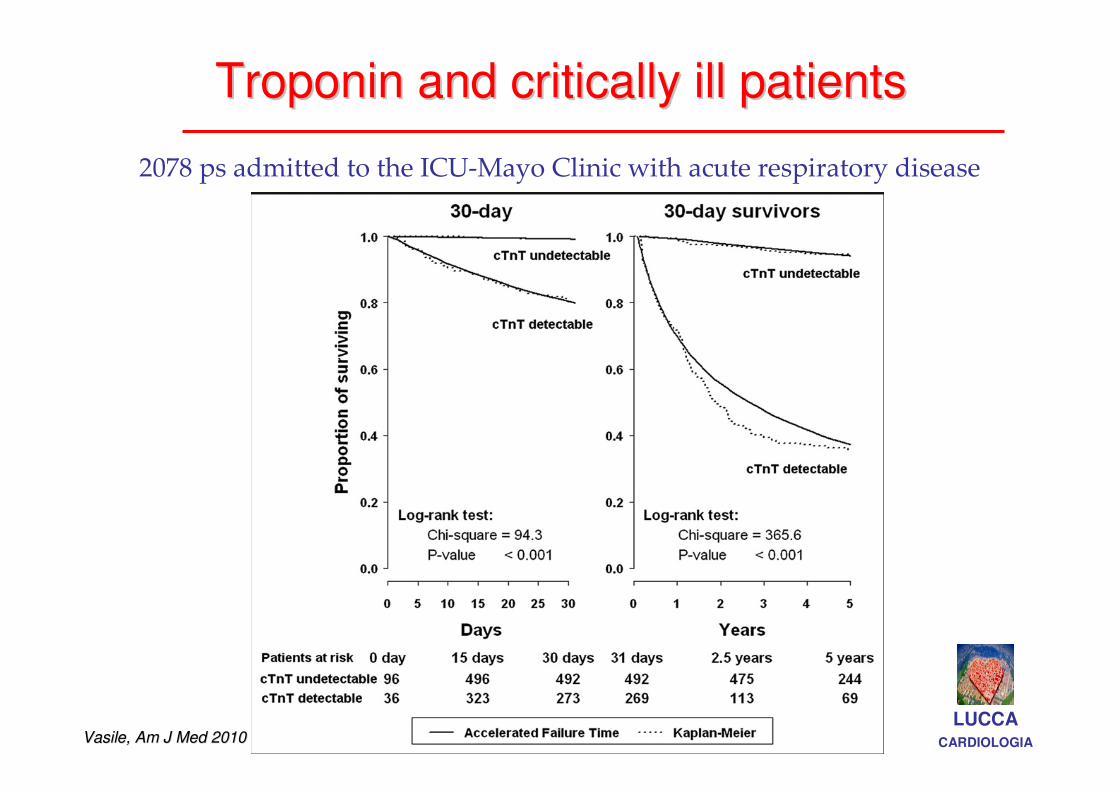
Troponin and critically ill patientsTroponin and critically ill patients
2078 ps admitted to the ICU-Mayo Clinic with acute respiratory disease
LUCCACARDIOLOGIAVasile, Am J Med 2010Vasile, Am J Med 2010
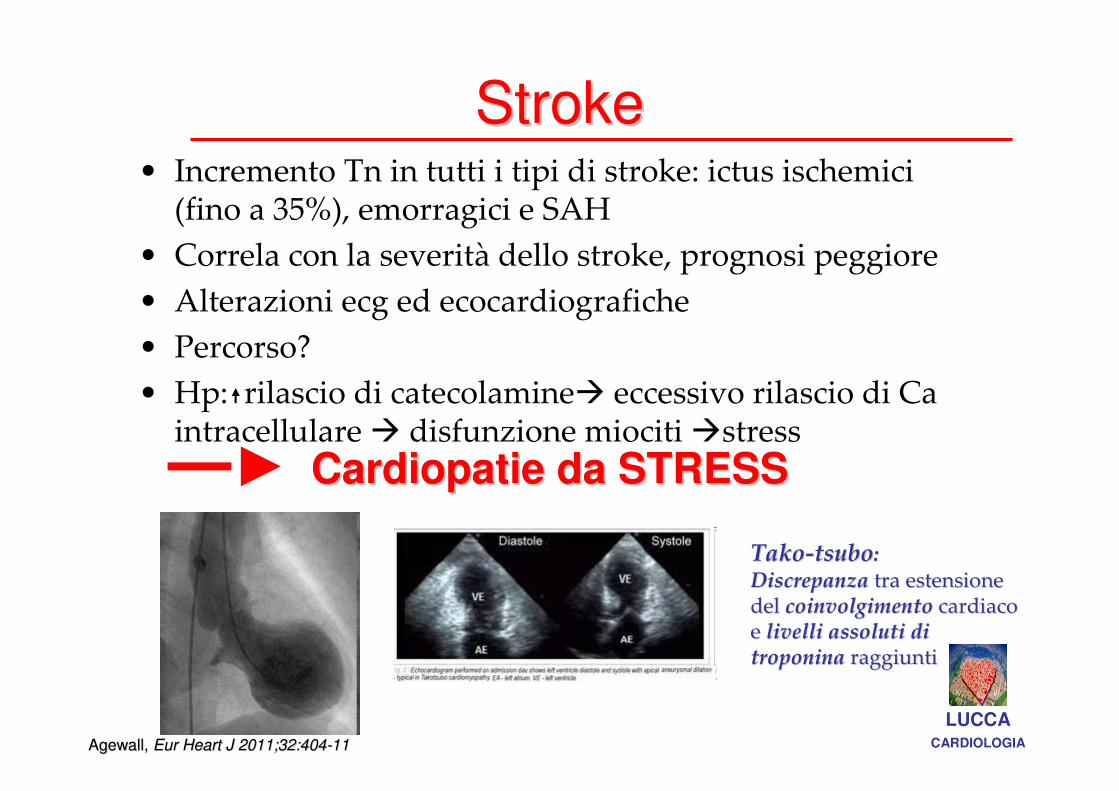
StrokeStroke• Incremento Tn in tutti i tipi di stroke: ictus ischemici
(fino a 35%), emorragici e SAH
• Correla con la severità dello stroke, prognosi peggiore
• Alterazioni ecg ed ecocardiografiche
• Percorso?
• Hp: rilascio di catecolamine� eccessivo rilascio di Ca intracellulare � disfunzione miociti �stress
Cardiopatie da STRESSCardiopatie da STRESS
TakoTako--tsubotsubo::DiscrepanzaDiscrepanza tra estensione tra estensione del del coinvolgimentocoinvolgimento cardiaco cardiaco e e livelli assoluti di livelli assoluti di troponinatroponina raggiuntiraggiunti
LUCCACARDIOLOGIAAgewall, Agewall, Eur Heart J 2011;32:404Eur Heart J 2011;32:404--1111
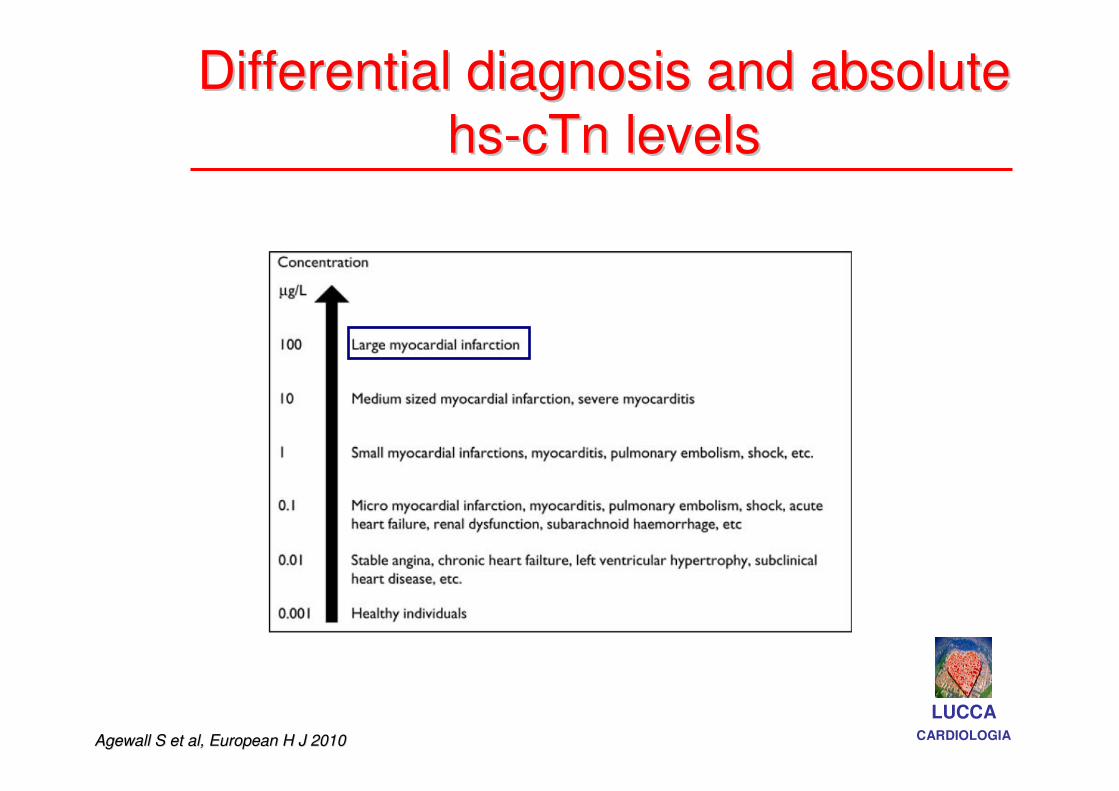
Differential diagnosis and absolute Differential diagnosis and absolute
hshs--cTn levelscTn levels
Agewall S et al, European H J 2010Agewall S et al, European H J 2010
LUCCACARDIOLOGIA
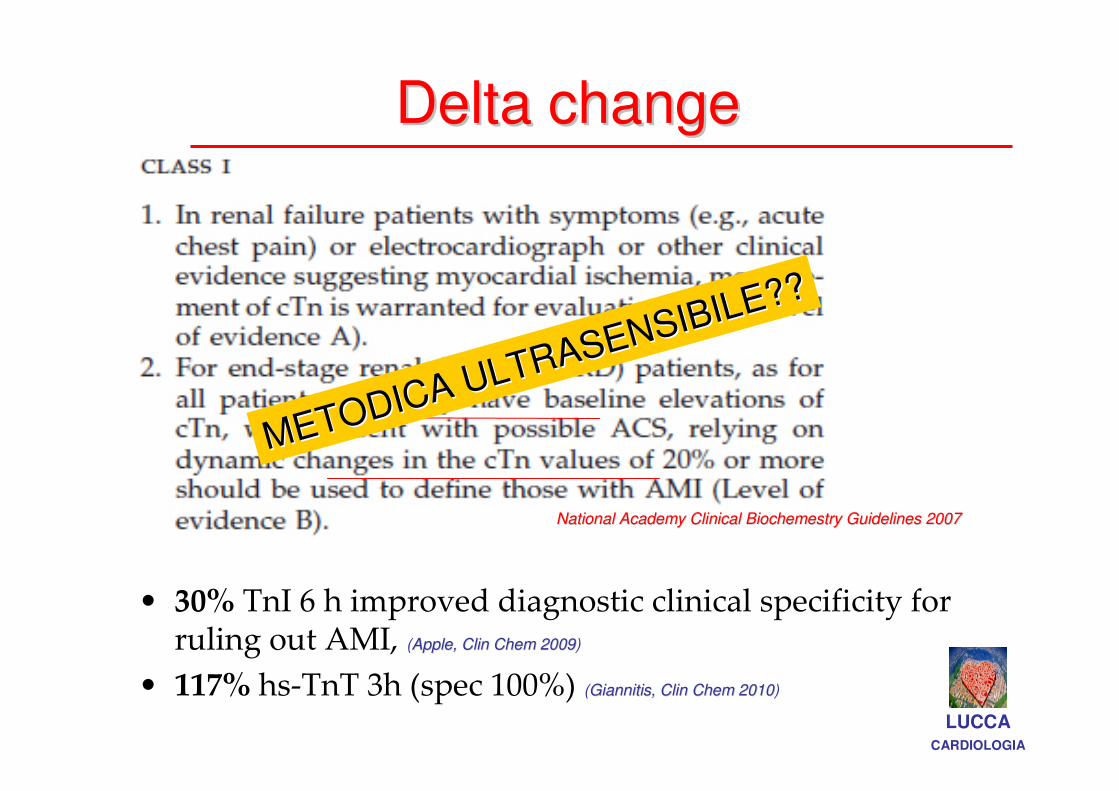
Delta changeDelta change
• 30% TnI 6 h improved diagnostic clinical specificity for ruling out AMI, (Apple, Clin Chem 2009Apple, Clin Chem 2009)
• 117% hs-TnT 3h (spec 100%) (Giannitis, Clin Chem 2010Giannitis, Clin Chem 2010)
National Academy Clinical Biochemestry Guidelines 2007National Academy Clinical Biochemestry Guidelines 2007
LUCCACARDIOLOGIA
METODICA ULTRASENSIBILE??
METODICA ULTRASENSIBILE??
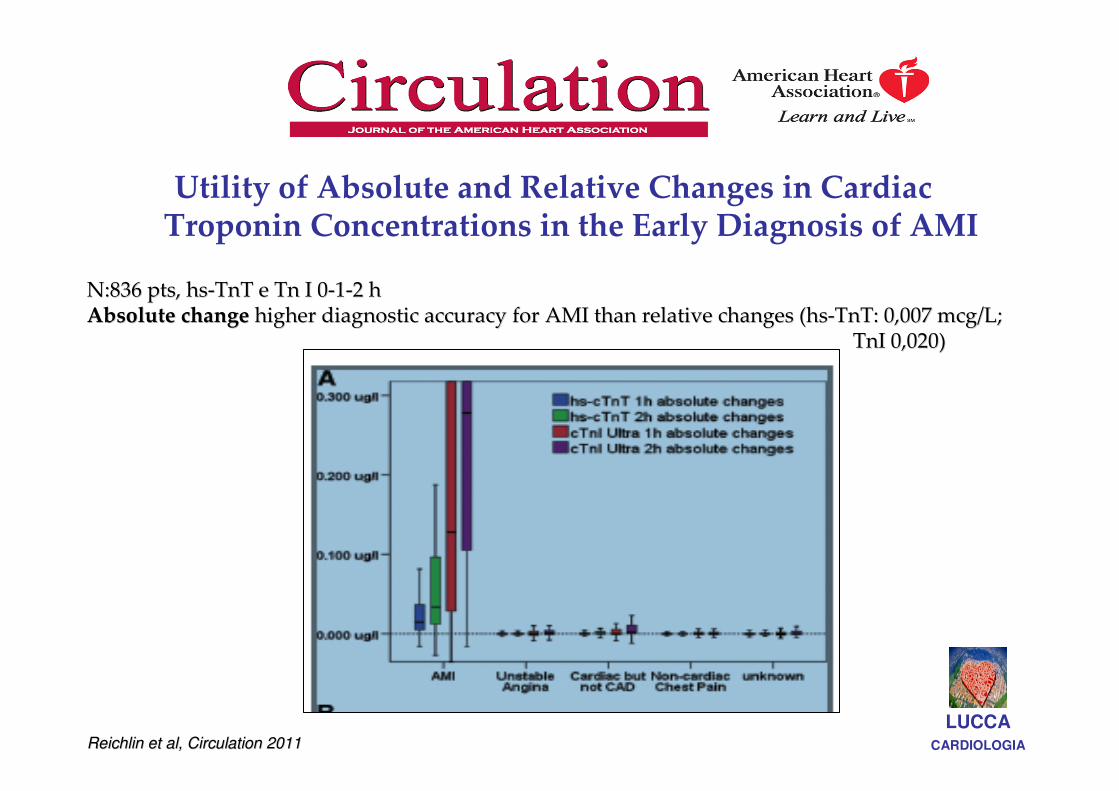
Utility of Absolute and Relative Changes in Cardiac Troponin Concentrations in the Early Diagnosis of AMI
LUCCACARDIOLOGIA
N:836 pts, hsN:836 pts, hs--TnT e Tn I 0TnT e Tn I 0--11--2 h2 hAbsolute changeAbsolute change higher diagnostic accuracy for AMI than relative changes (hshigher diagnostic accuracy for AMI than relative changes (hs--TnT: 0,007 mcg/L; TnT: 0,007 mcg/L;
TnI 0,020)TnI 0,020)
Reichlin et al, Circulation 2011Reichlin et al, Circulation 2011
Acute vs chronic Tn elevationAcute vs chronic Tn elevation
LUCCACARDIOLOGIAApple et al ,Clin Chem 2009Apple et al ,Clin Chem 2009
……A A risingrising Tn pattern would be indicative ofTn pattern would be indicative ofan an acuteacute process, process,
whereas a whereas a static patternstatic patternwould be indicative of would be indicative of
a a chronic processchronic process……
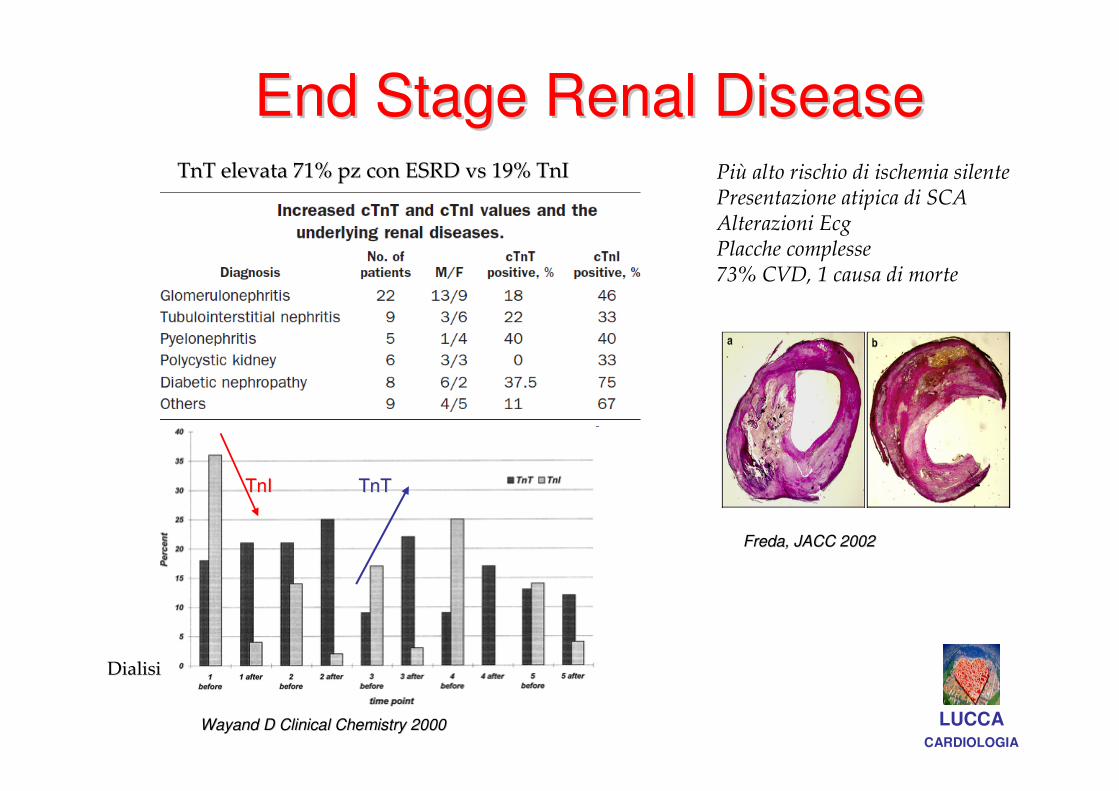
End Stage Renal DiseaseEnd Stage Renal Disease
LUCCACARDIOLOGIA
Wayand D Clinical Chemistry 2000Wayand D Clinical Chemistry 2000
Più alto rischio di ischemia silentePresentazione atipica di SCA Alterazioni EcgPlacche complesse73% CVD, 1 causa di morte
TnT elevata 71% pz con ESRD vs 19% TnITnT elevata 71% pz con ESRD vs 19% TnI
Freda, JACC 2002Freda, JACC 2002
TnITnI TnTTnT
DialisiDialisi
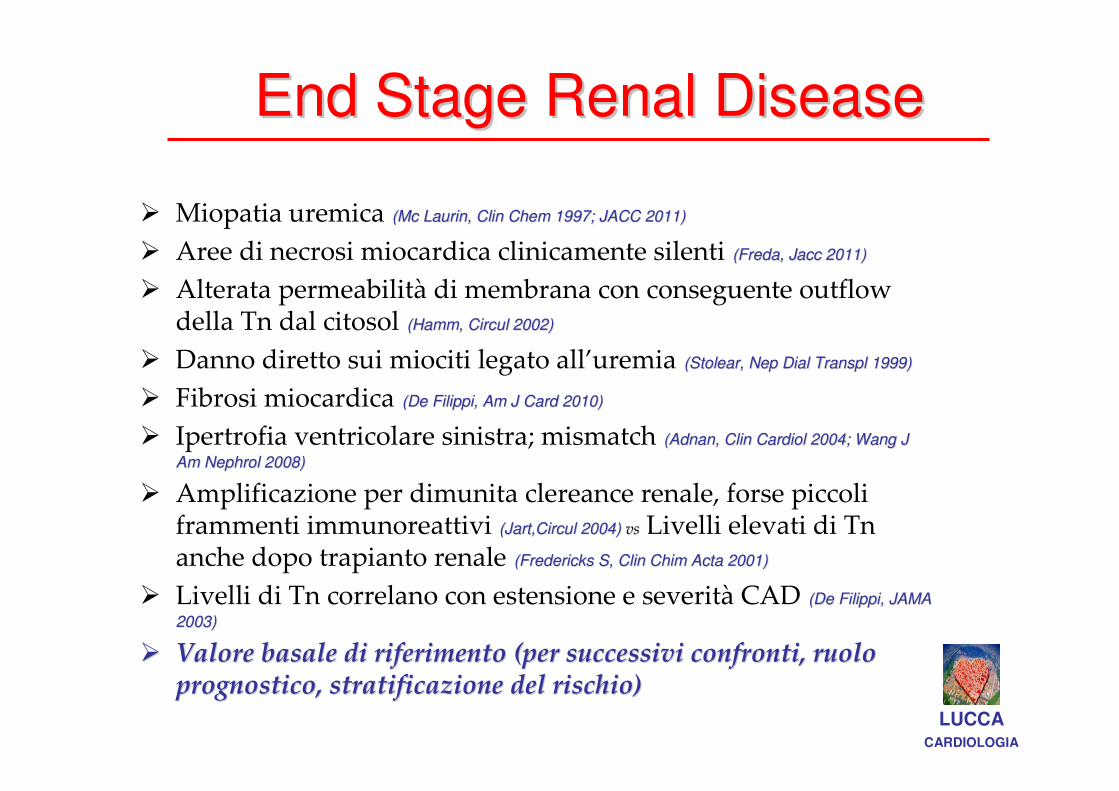
End Stage Renal DiseaseEnd Stage Renal Disease
LUCCACARDIOLOGIA
� Miopatia uremica (Mc Laurin, Clin Chem 1997; JACC 2011)(Mc Laurin, Clin Chem 1997; JACC 2011)
� Aree di necrosi miocardica clinicamente silenti (Freda, Jacc 2011)(Freda, Jacc 2011)
� Alterata permeabilità di membrana con conseguente outflow della Tn dal citosol (Hamm, Circul 2002)(Hamm, Circul 2002)
� Danno diretto sui miociti legato all’uremia (Stolear, Nep Dial Transpl 1999)(Stolear, Nep Dial Transpl 1999)
� Fibrosi miocardica (De Filippi, Am J Card 2010)(De Filippi, Am J Card 2010)
� Ipertrofia ventricolare sinistra; mismatch (Adnan, Clin Cardiol 2004; Wang J (Adnan, Clin Cardiol 2004; Wang J
Am Nephrol 2008) Am Nephrol 2008)
� Amplificazione per dimunita clereance renale, forse piccoli frammenti immunoreattivi (Jart,Circul 2004) (Jart,Circul 2004) vsvs Livelli elevati di Tn anche dopo trapianto renale (Fredericks S, Clin Chim Acta 2001)(Fredericks S, Clin Chim Acta 2001)
� Livelli di Tn correlano con estensione e severità CAD (De Filippi, JAMA (De Filippi, JAMA
2003)2003)
�� Valore basale di riferimento (per successivi confronti, ruolo Valore basale di riferimento (per successivi confronti, ruolo prognostico, stratificazione del rischio)prognostico, stratificazione del rischio)
LUCCACARDIOLOGIA
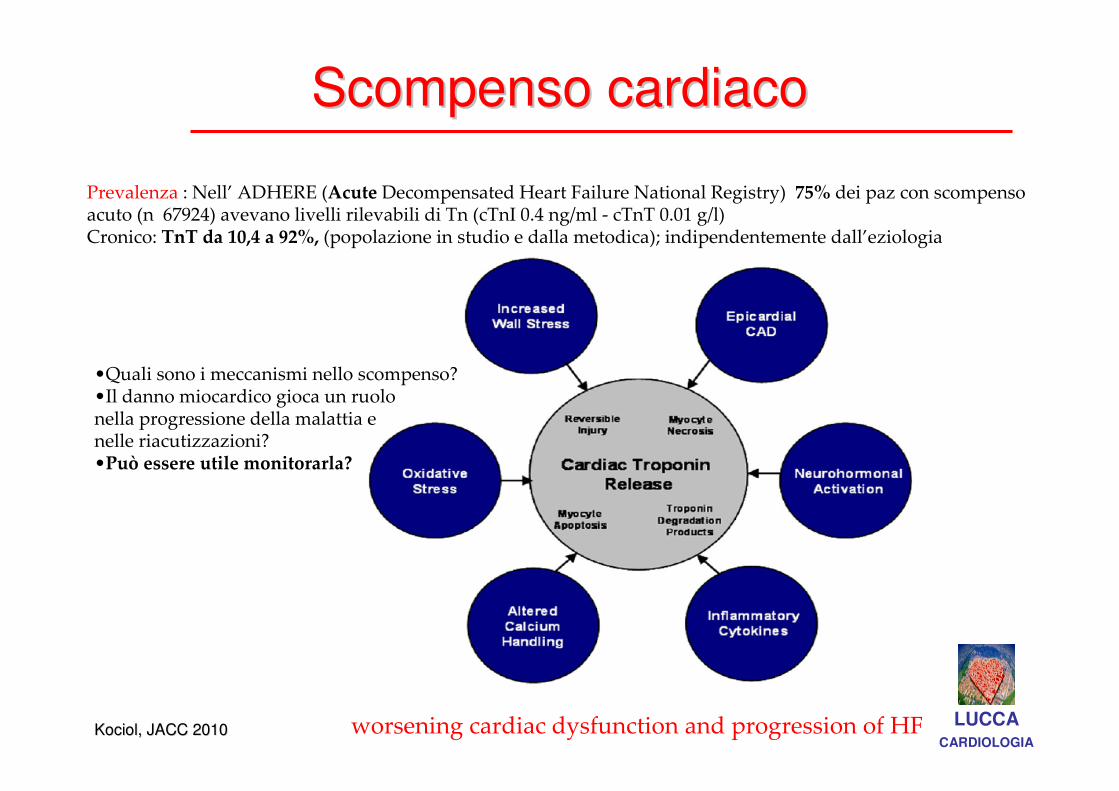
•Quali sono i meccanismi nello scompenso? •Il danno miocardico gioca un ruolo nella progressione della malattia enelle riacutizzazioni?•Può essere utile monitorarla?
Prevalenza : Nell’ ADHERE (Acute Decompensated Heart Failure National Registry) 75% dei paz con scompenso acuto (n 67924) avevano livelli rilevabili di Tn (cTnI 0.4 ng/ml - cTnT 0.01 g/l)Cronico: TnT da 10,4 a 92%, (popolazione in studio e dalla metodica); indipendentemente dall’eziologia
worsening cardiac dysfunction and progression of HFKociol, JACC 2010Kociol, JACC 2010
Scompenso cardiacoScompenso cardiaco
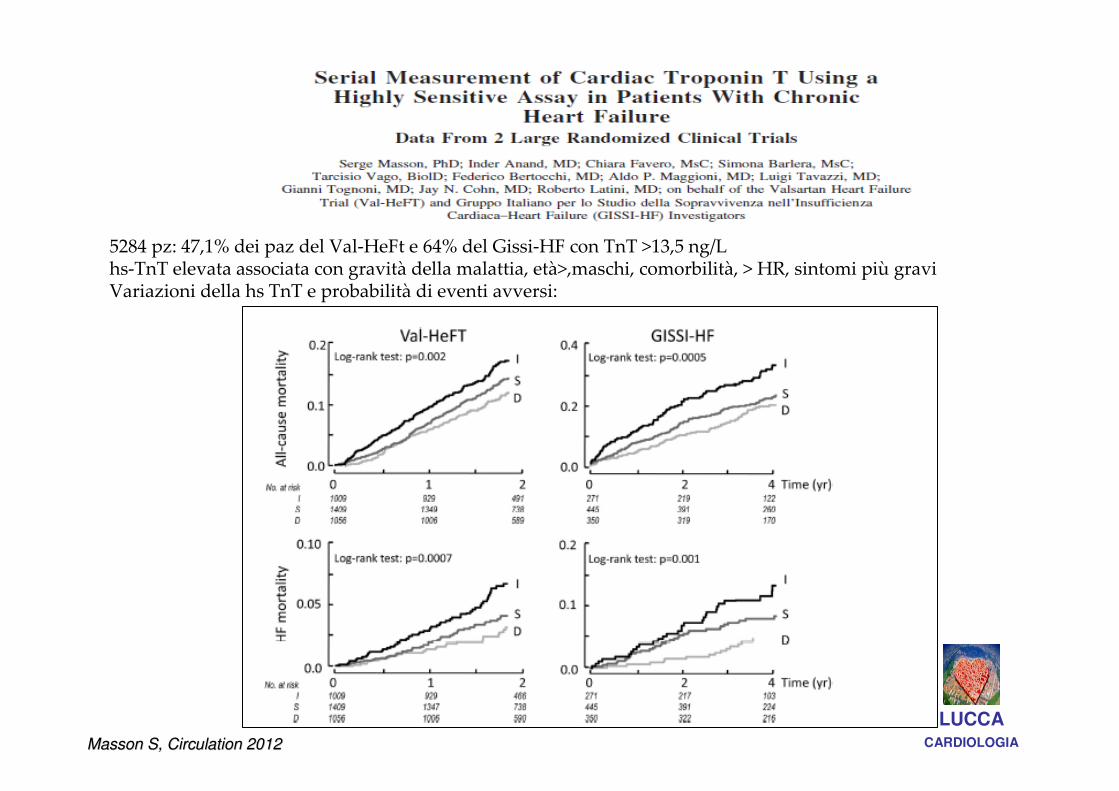
LUCCACARDIOLOGIAMasson S, Circulation 2012Masson S, Circulation 2012
5284 pz: 47,1% dei paz del Val-HeFt e 64% del Gissi-HF con TnT >13,5 ng/Lhs-TnT elevata associata con gravità della malattia, età>,maschi, comorbilità, > HR, sintomi più gravi Variazioni della hs TnT e probabilità di eventi avversi:
LUCCACARDIOLOGIA
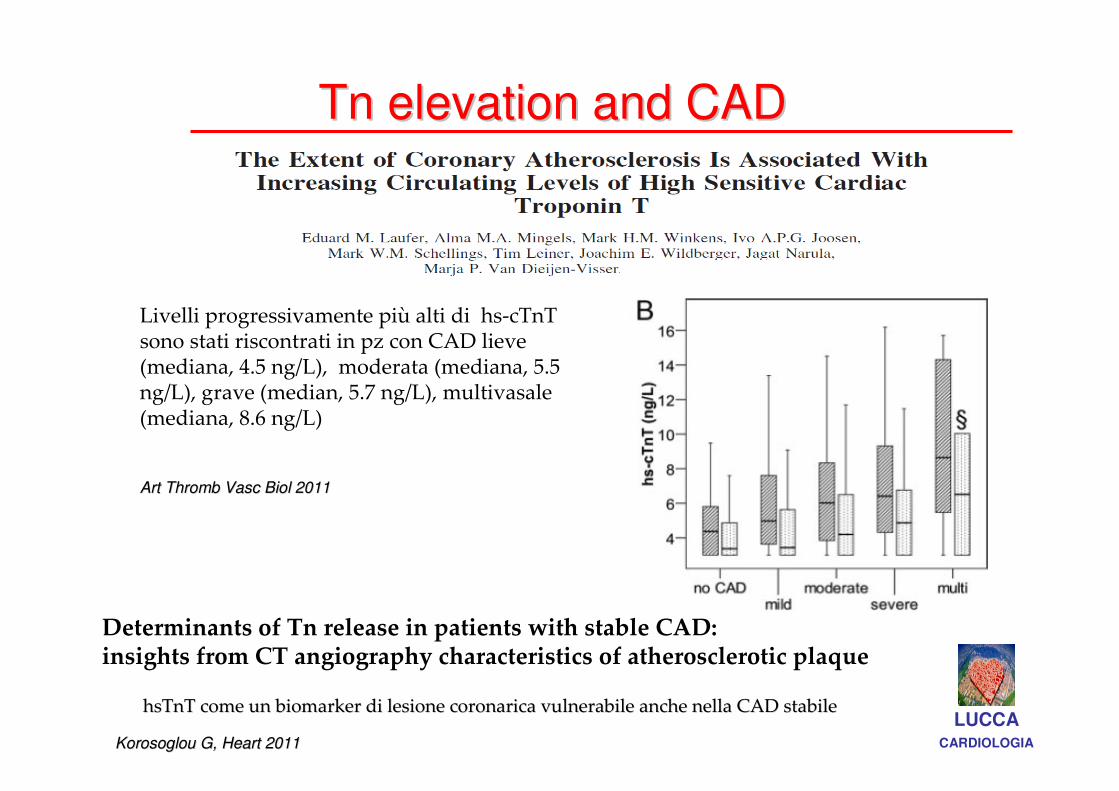
Livelli progressivamente più alti di hs-cTnT sono stati riscontrati in pz con CAD lieve (mediana, 4.5 ng/L), moderata (mediana, 5.5 ng/L), grave (median, 5.7 ng/L), multivasale (mediana, 8.6 ng/L)
Tn elevation and CADTn elevation and CAD
Art Thromb Vasc Biol 2011Art Thromb Vasc Biol 2011
Determinants of Tn release in patients with stable CAD: insights from CT angiography characteristics of atherosclerotic plaque
hsTnT come un biomarker di lesione coronarica vulnerabile anche hsTnT come un biomarker di lesione coronarica vulnerabile anche nella CAD stabilenella CAD stabile
Korosoglou G, Heart 2011Korosoglou G, Heart 2011
LUCCACARDIOLOGIA
..
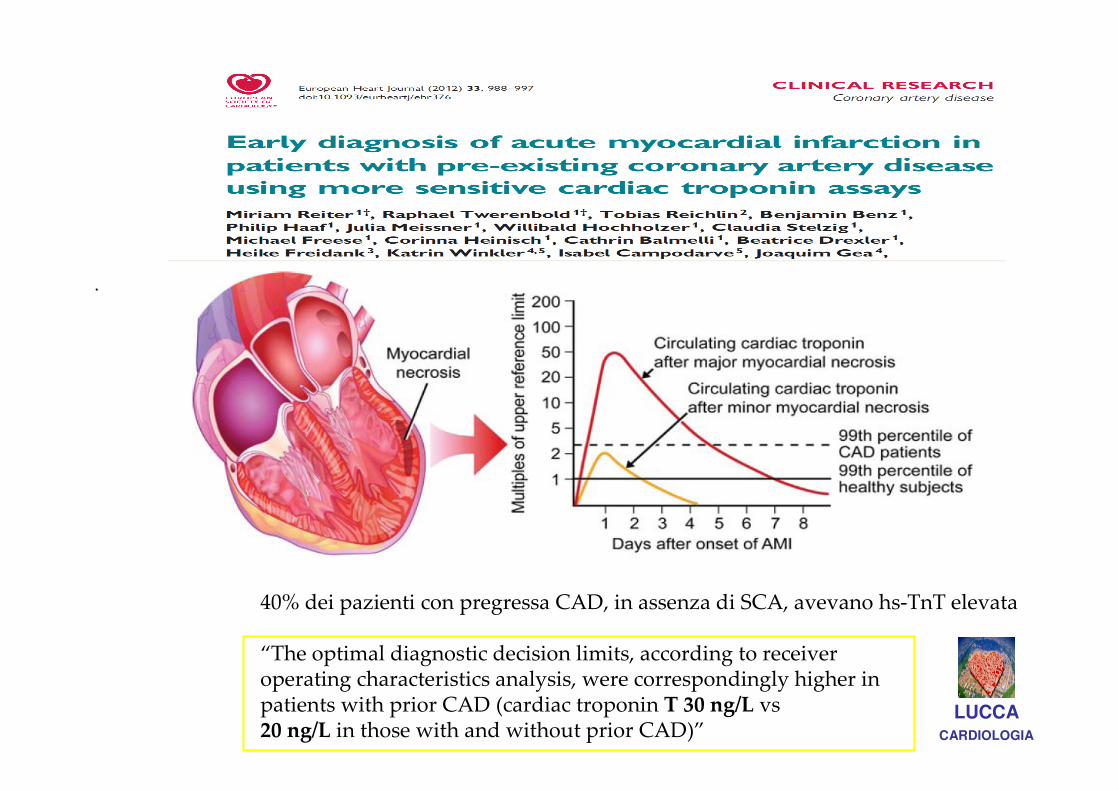
40% dei pazienti con pregressa CAD, in assenza di SCA, avevano hs-TnT elevata
“The optimal diagnostic decision limits, according to receiveroperating characteristics analysis, were correspondingly higher inpatients with prior CAD (cardiac troponin T 30 ng/L vs20 ng/L in those with and without prior CAD)”
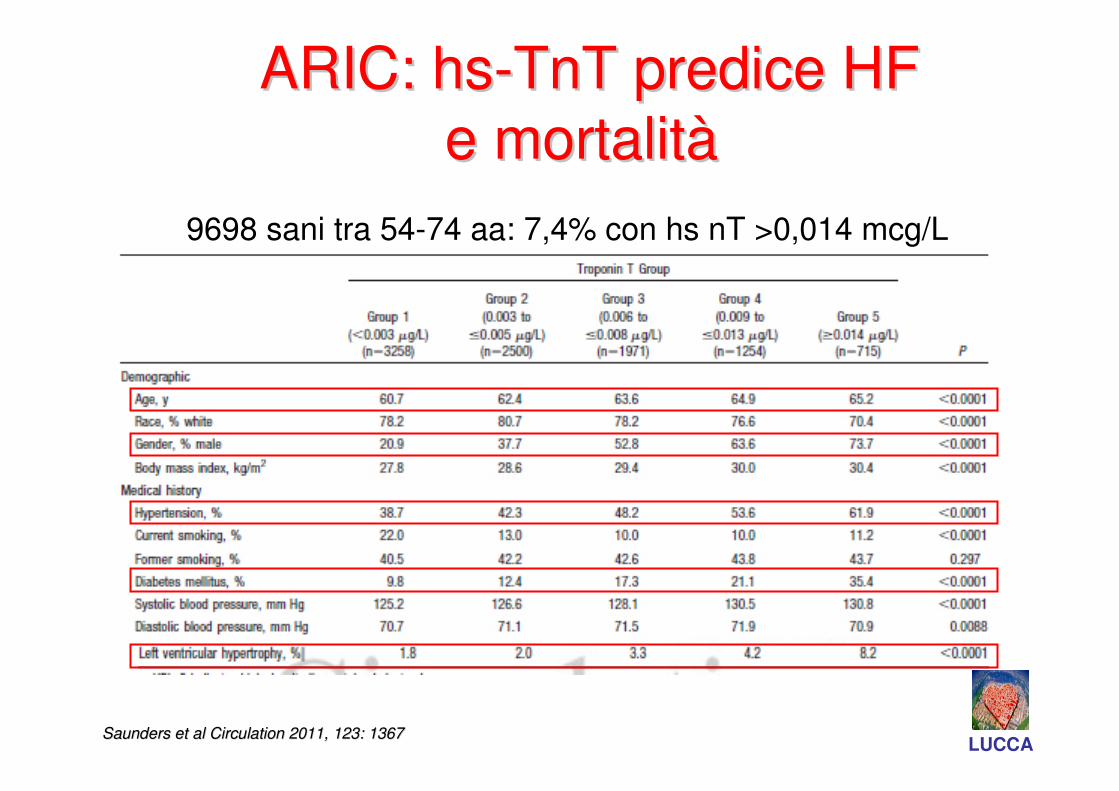
9698 sani tra 54-74 aa: 7,4% con hs nT >0,014 mcg/L
Saunders et al Circulation 2011, 123: 1367Saunders et al Circulation 2011, 123: 1367
ARIC: hsARIC: hs--TnT predice HF TnT predice HF
e mortalite mortalitàà
LUCCA
• Le Tn-hs consentono la diagnosi/esclusione rapida di IM
• Rising and/or falling differenzia un danno
acuto dal cronico
• Variazione assolute vs relative, quale valore? Questione non risolta!
LUCCACARDIOLOGIA
CONCLUSIONICONCLUSIONI
• Trop elevata non SCA: necessario recupero
della clinica La valutazione clinica è mandatoria
per interpretare il risultato
• Il significato diagnostico della Tn nel paziente
che giunge al PS senza sintomatologia specifica
rimane da determinare (percorso?)
• Non essere spaventati ma …
Twerenbold R et al Eur Heart J (2012) 33(5): 579-586 LUCCACARDIOLOGIA
CONCLUSIONICONCLUSIONI

Necessità di interazioni tra vari specialisti: appropriatezza /specificità
Amiloidosi CardiacaAmiloidosi Cardiaca……!!
LUCCACARDIOLOGIAGRAZIE PER LGRAZIE PER L’’ATTENZIONE!!!!ATTENZIONE!!!!


SCASCA NonNon--SCASCA
LUCCACARDIOLOGIA
Aumento Troponina = Ischemia
Interpretazione del risultatoInterpretazione del risultato
LUCCACARDIOLOGIA
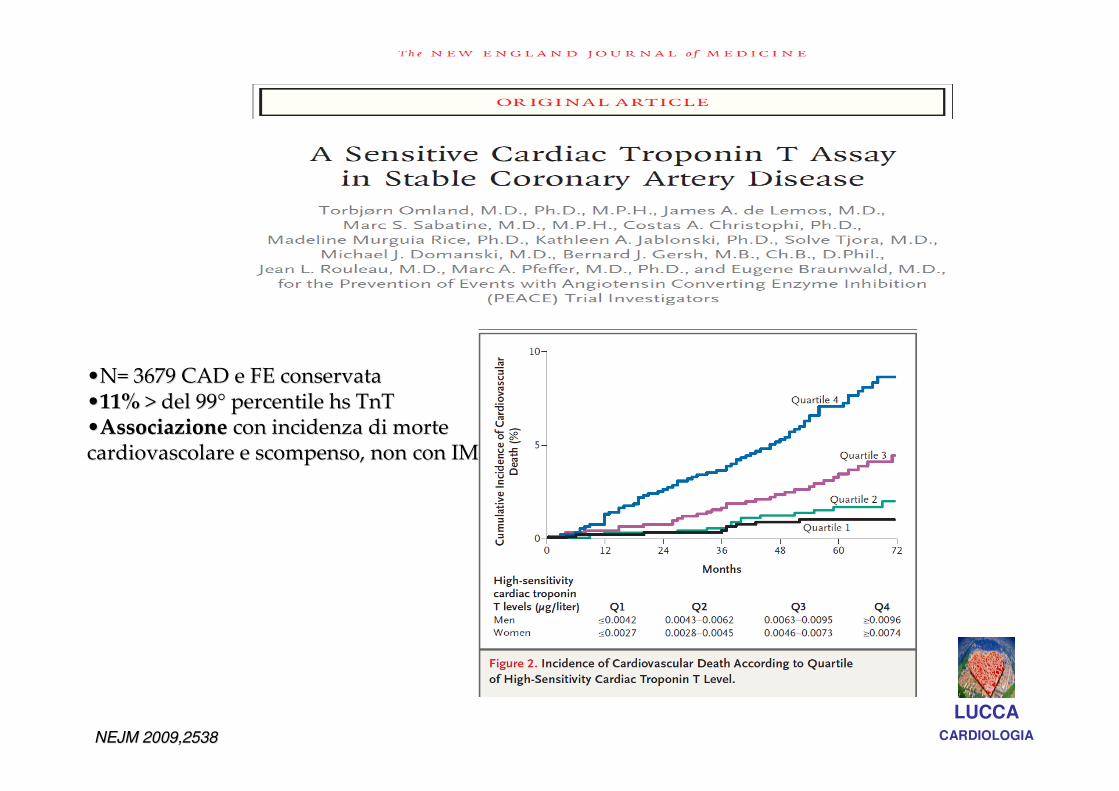
••N= 3679 CAD e FE conservataN= 3679 CAD e FE conservata••11%11% > del 99> del 99°° percentile hs TnTpercentile hs TnT••Associazione Associazione con incidenza di morte con incidenza di morte cardiovascolare e scompenso, non con IMcardiovascolare e scompenso, non con IM
NEJM 2009,2538NEJM 2009,2538
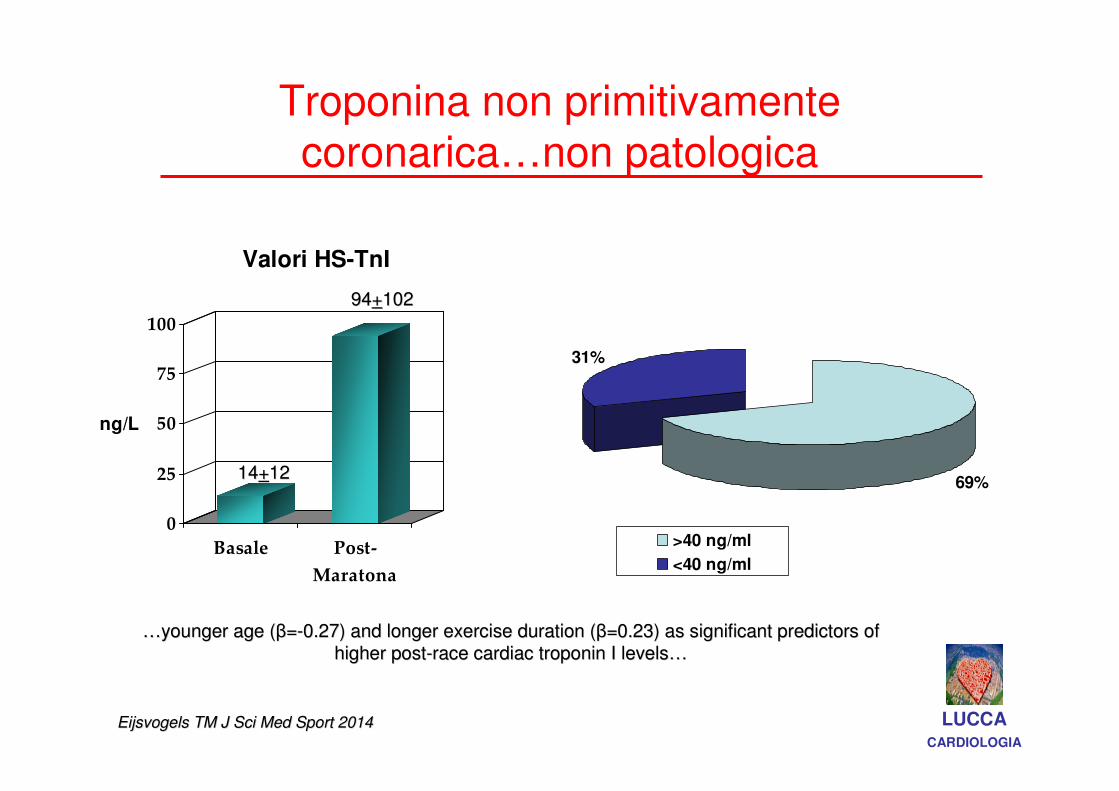
Troponina non primitivamente coronarica…non patologica
0
25
50
75
100
ng/L
Basale Post-
Maratona
Valori HS-TnI
LUCCACARDIOLOGIA
1414++1212
9494++102102
69%
31%
>40 ng/ml
<40 ng/ml
Eijsvogels TM J Sci Med Sport 2014 Eijsvogels TM J Sci Med Sport 2014
……younger age (younger age (ββ==--0.27) and longer exercise duration (0.27) and longer exercise duration (ββ=0.23) as significant predictors of =0.23) as significant predictors of
higher posthigher post--race cardiac troponin I levelsrace cardiac troponin I levels……
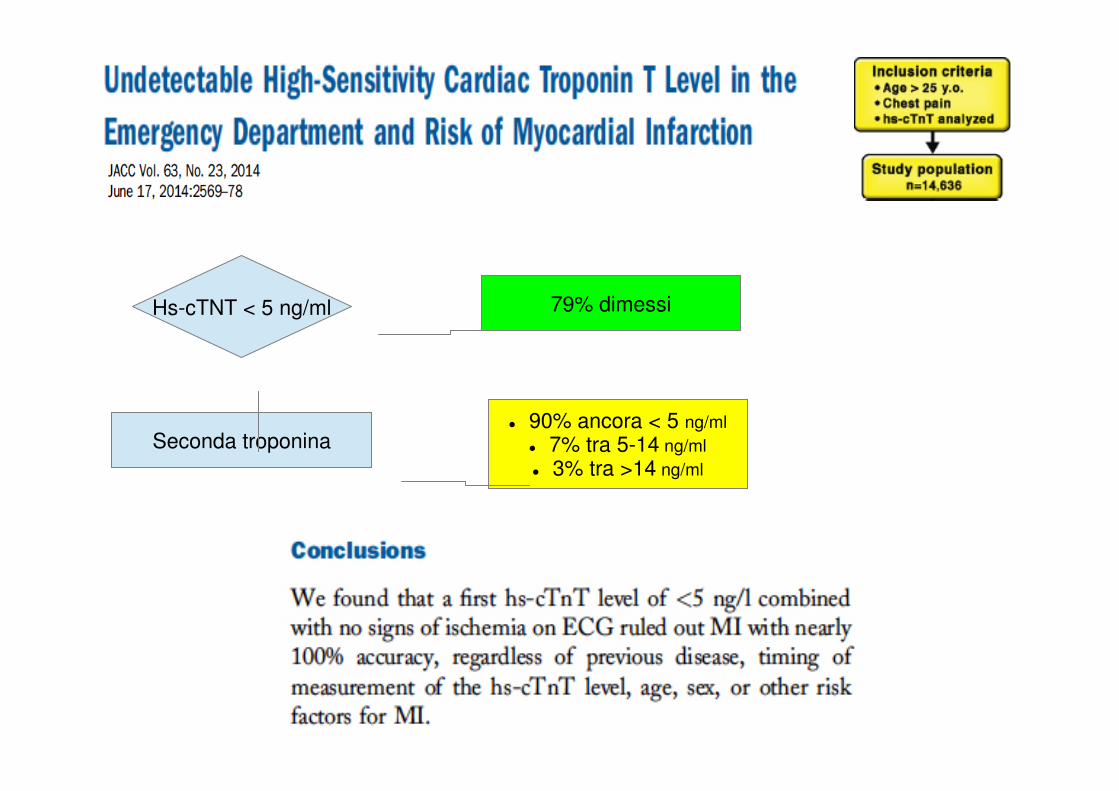
Hs-cTNT < 5 ng/ml
Seconda troponina
79% dimessi
� 90% ancora < 5 ng/ml
� 7% tra 5-14 ng/ml
� 3% tra >14 ng/ml
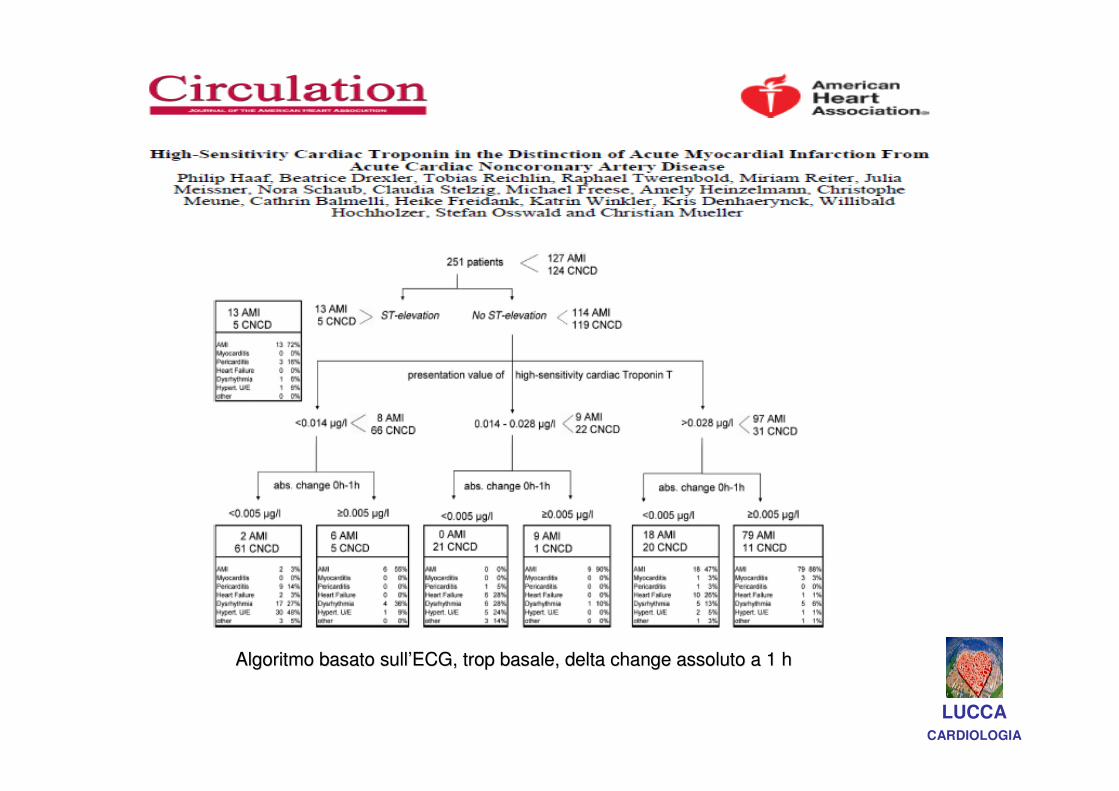
Algoritmo basato sullAlgoritmo basato sull’’ECG, trop basale, delta change assoluto a 1 hECG, trop basale, delta change assoluto a 1 h
LUCCACARDIOLOGIA
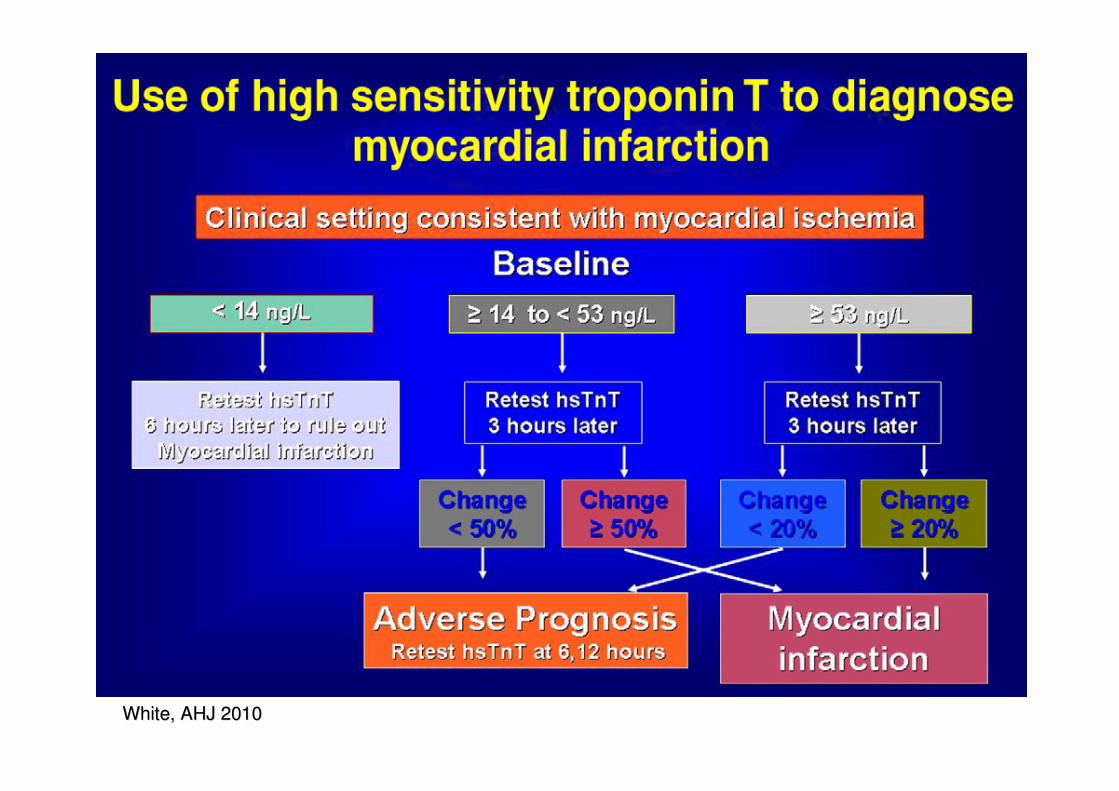
White, AHJ 2010White, AHJ 2010
JACC, 2013JACC, 2013 LUCCACARDIOLOGIA
PREMESSEPREMESSE
IPOTESIIPOTESI
Eur Heart J. 2010 Sep;31(18):2197-204. LUCCACARDIOLOGIA
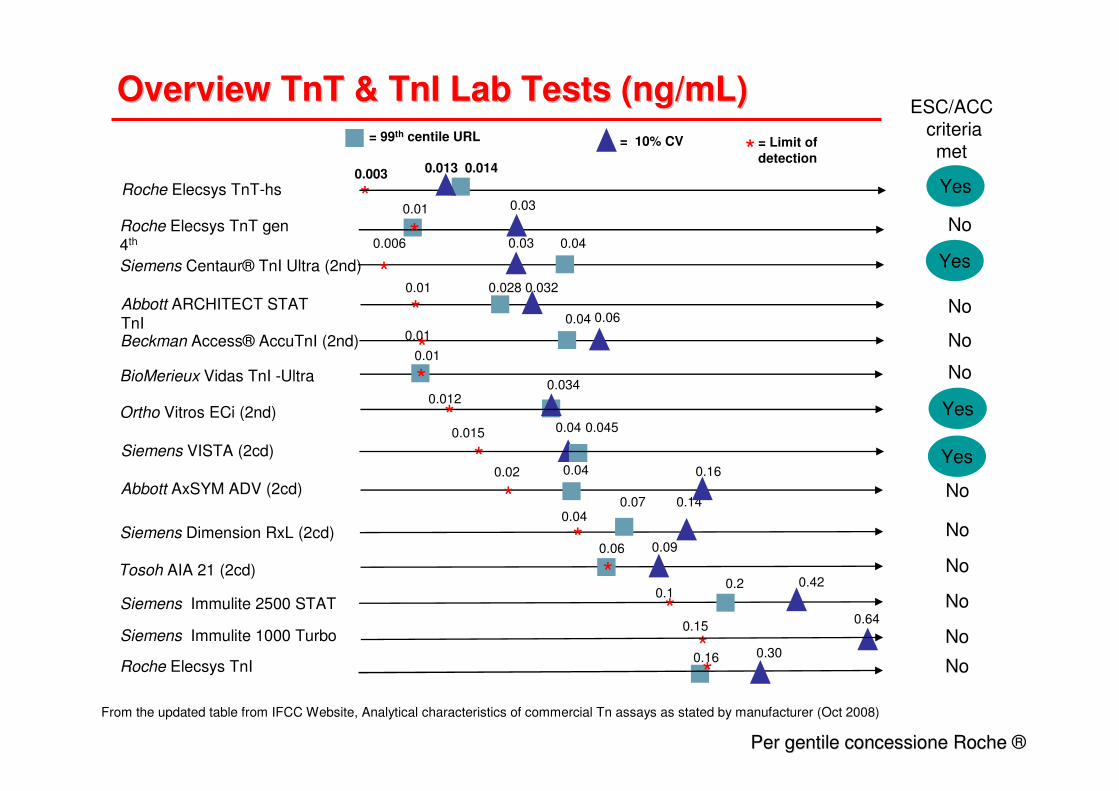
Overview TnT & TnI Lab Tests (ng/mL)Overview TnT & TnI Lab Tests (ng/mL)
Roche Elecsys TnT gen 4th
Siemens Centaur® TnI Ultra (2nd)
Abbott ARCHITECT STAT TnIBeckman Access® AccuTnI (2nd)
Siemens Immulite 2500 STAT
Siemens Immulite 1000 Turbo
= 99th centile URL = 10% CV
Siemens VISTA (2cd)
ESC/ACCcriteria met
No
No
No
No
No
* = Limit of detection
From the updated table from IFCC Website, Analytical characteristics of commercial Tn assays as stated by manufacturer (Oct 2008)
Ortho Vitros ECi (2nd)
No
Roche Elecsys TnT-hs
Siemens Dimension RxL (2cd) No
BioMerieux Vidas TnI -Ultra
No
Abbott AxSYM ADV (2cd)
NoTosoh AIA 21 (2cd)
0.013 0.014
Yes
Yes
Yes
Yes
NoRoche Elecsys TnI*
0.040.03
0.028 0.032
0.04 0.06
0.034
0.03
0.150.64
0.045
0.14
0.01
*
*0.01
*
0.006
*0.01
*0.012
*0.04
*0.003
0.2 0.420.1
*
*0.015
0.07
0.04
0.01
*
*0.02 0.04 0.16
0.06
*0.09
0.16 0.30
*
Per gentile concessione Roche Per gentile concessione Roche ®
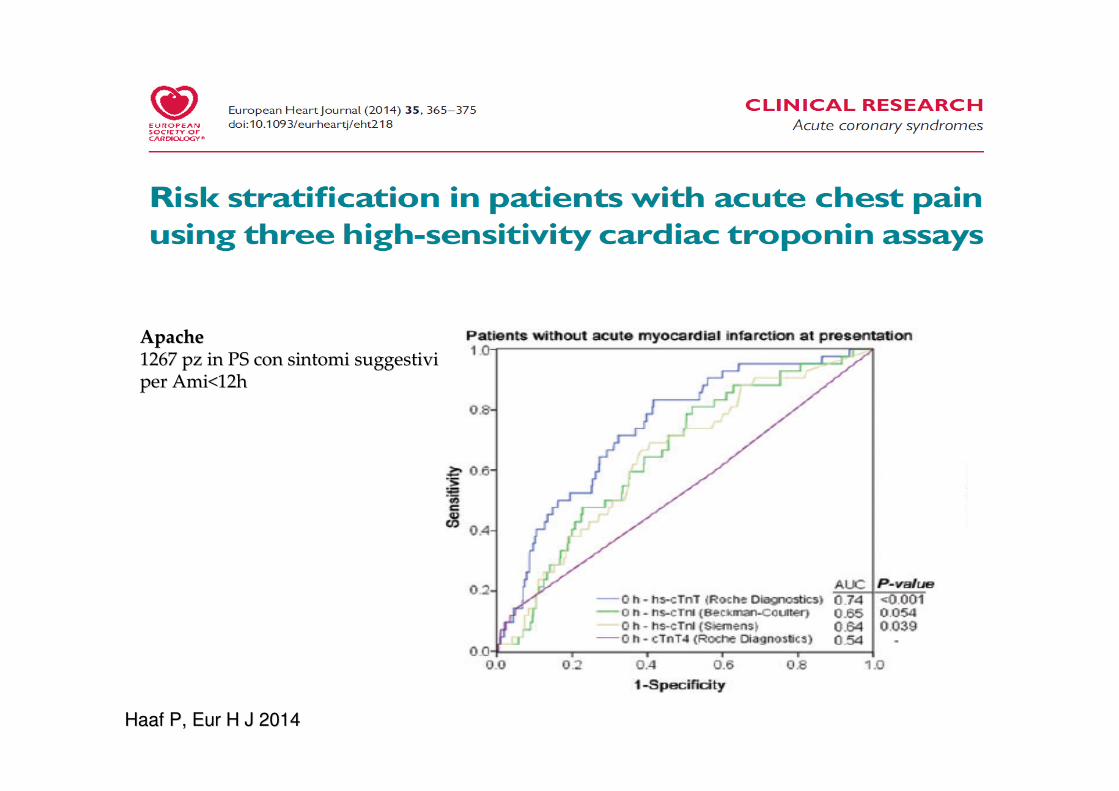
ApacheApache1267 pz in PS con sintomi suggestivi1267 pz in PS con sintomi suggestiviper Ami<12hper Ami<12h
Haaf P, Eur H J 2014Haaf P, Eur H J 2014
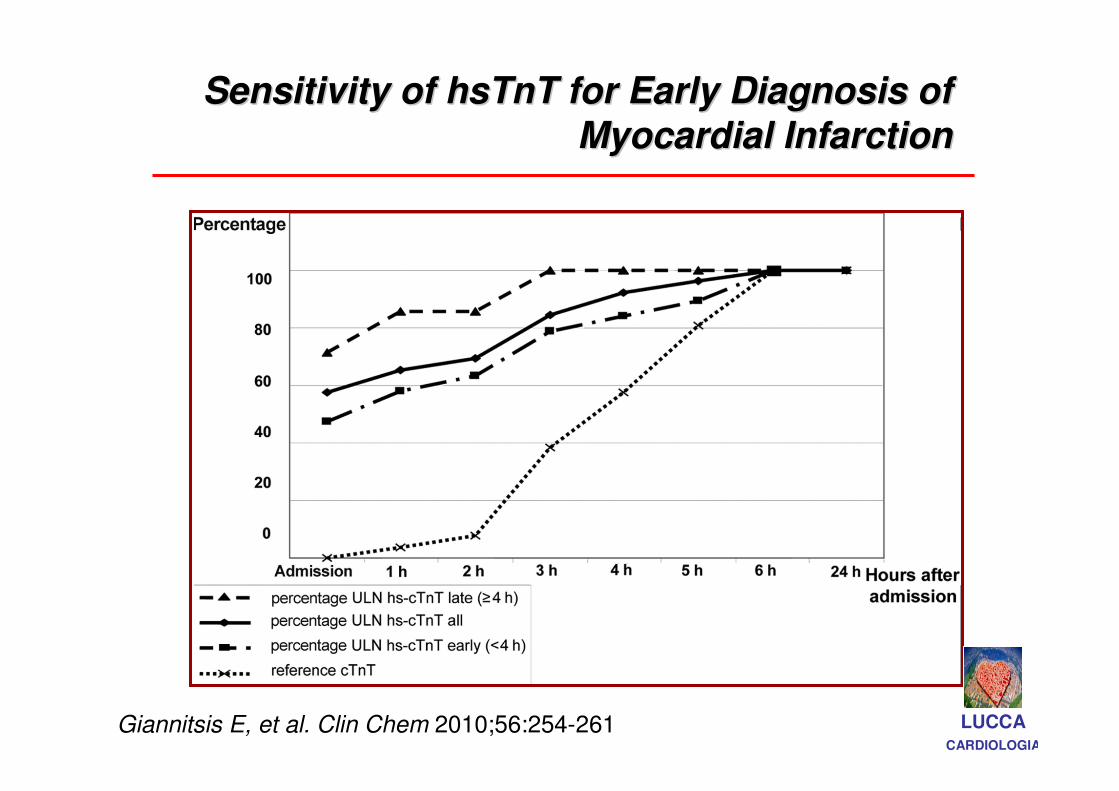
Sensitivity of hsTnT for Early Diagnosis of Sensitivity of hsTnT for Early Diagnosis of
Myocardial InfarctionMyocardial Infarction
Giannitsis E, et al. Clin Chem 2010;56:254-261 LUCCACARDIOLOGIA
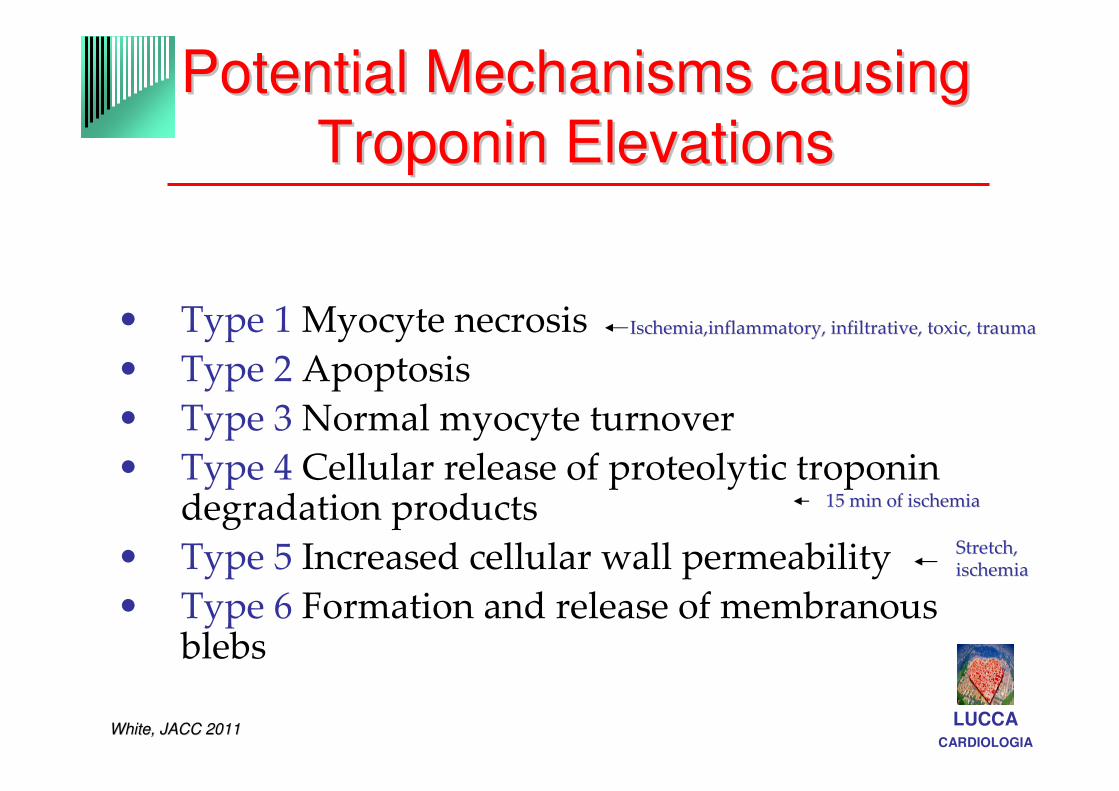
Potential Mechanisms causing Potential Mechanisms causing
Troponin ElevationsTroponin Elevations
• Type 1 Myocyte necrosis
• Type 2 Apoptosis
• Type 3 Normal myocyte turnover
• Type 4 Cellular release of proteolytic troponin degradation products
• Type 5 Increased cellular wall permeability
• Type 6 Formation and release of membranous blebs
LUCCACARDIOLOGIA
White, JACC 2011White, JACC 2011
Stretch,Stretch,ischemiaischemia
Ischemia,inflammatory, infiltrative, toxic, traumaIschemia,inflammatory, infiltrative, toxic, trauma
15 min of ischemia15 min of ischemia
• Minimi incrementi
• Precocemente
• Pochi falsi positivi
LUCCACARDIOLOGIA
Troponinosi: i veri …falsi positivi!
•presenza di anticorpi eterofili (Fitzmaurice et al Clin Chem 1998)
• fattore reumatoide (Dasgupta A et al Am J Clin Pathol 1999)
• incompleta separazione del siero (Nosanchuk JS et al Clin Chem 1999)
• emolisi (Agewall S ,Eur Heart J 2011)
• bilirubina (Dasgupta A. et al J.Clin. Lab. Anal. 2001)
Role of troponin in pz with CKD
and suspected SCA
• 31500 PZ!!!!!
• “ we found low quality or insufficient evidence for the utility of Trop assays for diagnosis and managment of ACS and for prognostic value of elevated Trop levels for ACS in Pz with CKD”
• “our findings do not refute utility of Trop testing in pz with CKD and ACS: equally effective in diagnosis ACS in Pz with CKD and those with normal renal function”
• …it depends on the pretest probability of disease…
Johns Hopkins University, Annals Int Med 2014Johns Hopkins University, Annals Int Med 2014
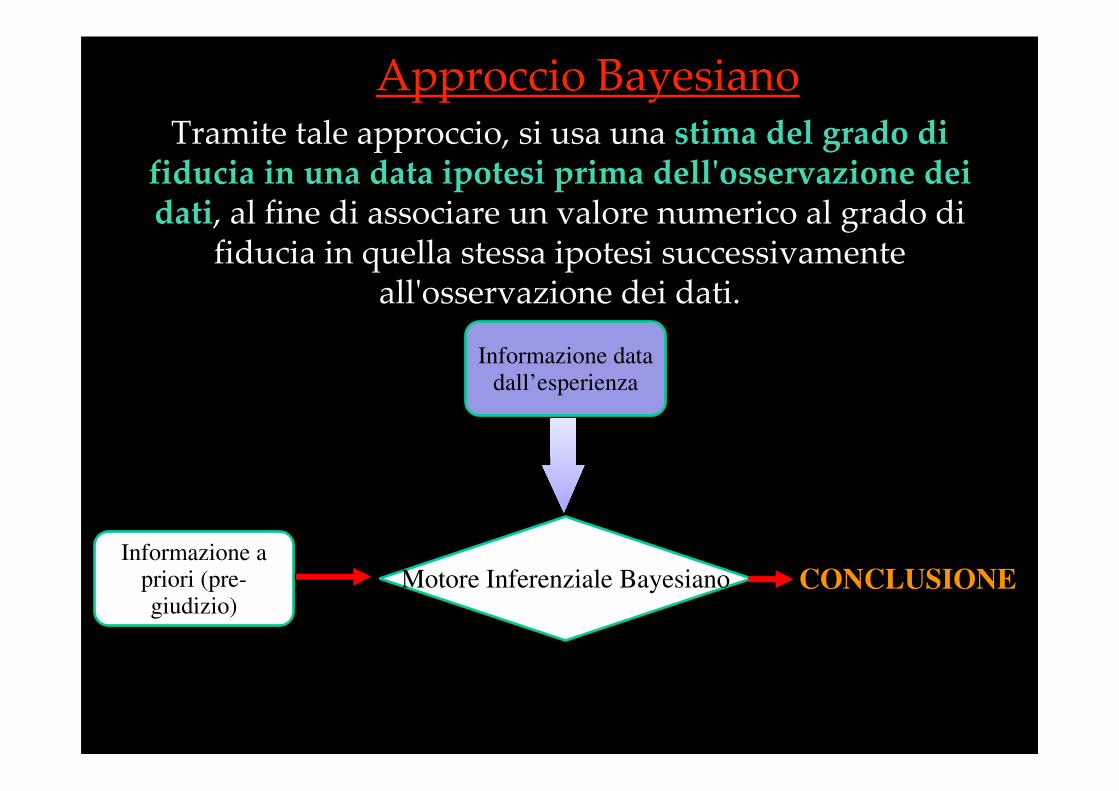
Approccio BayesianoTramite tale approccio, si usa una stima del grado di
fiducia in una data ipotesi prima dell'osservazione dei dati, al fine di associare un valore numerico al grado di
fiducia in quella stessa ipotesi successivamente all'osservazione dei dati.
Informazione a priori (pre-giudizio)
Informazione data dall’esperienza
Motore Inferenziale Bayesiano CONCLUSIONE
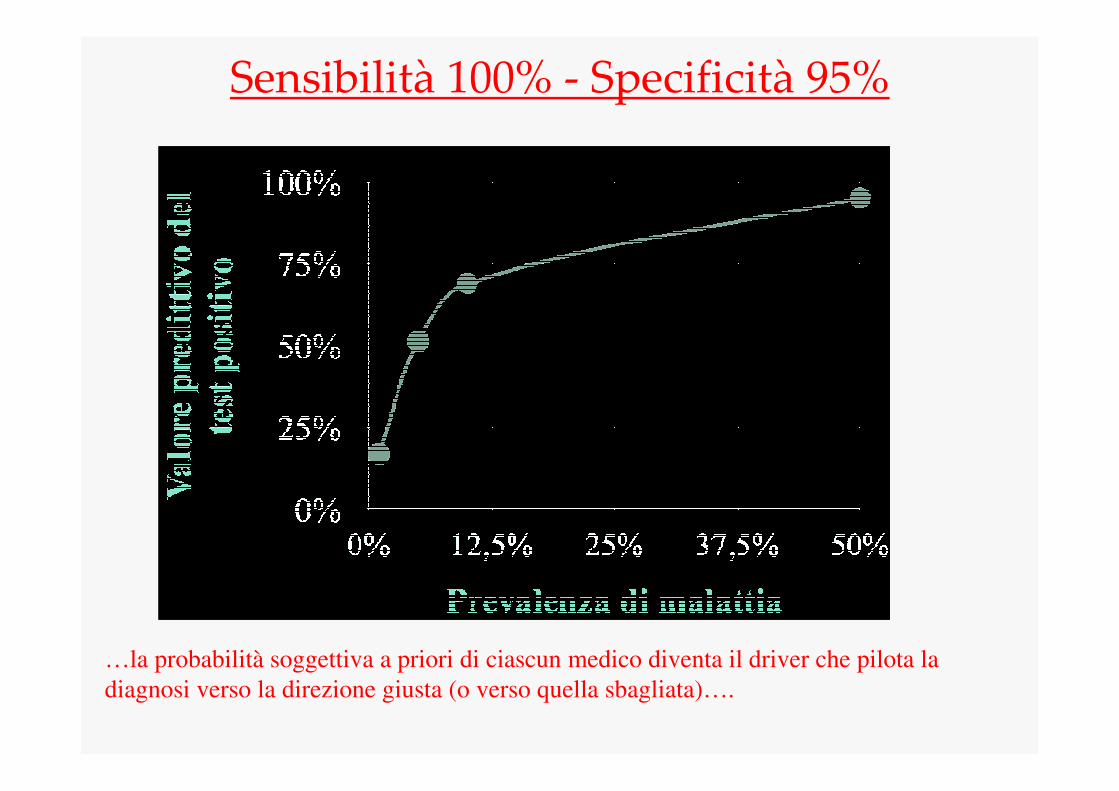
Sensibilità 100% - Specificità 95%
…la probabilità soggettiva a priori di ciascun medico diventa il driver che pilota la
diagnosi verso la direzione giusta (o verso quella sbagliata)….
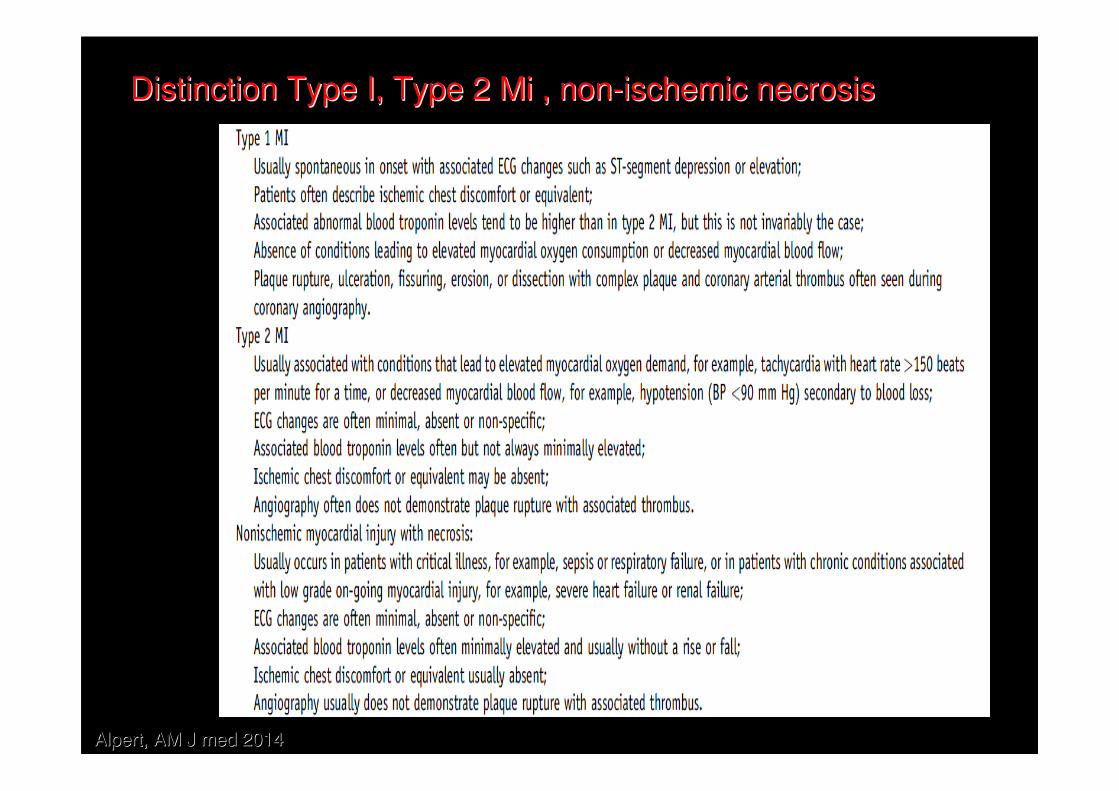
Distinction Type I, Type 2 Mi , nonDistinction Type I, Type 2 Mi , non--ischemic necrosisischemic necrosis
Alpert, AM J med 2014Alpert, AM J med 2014
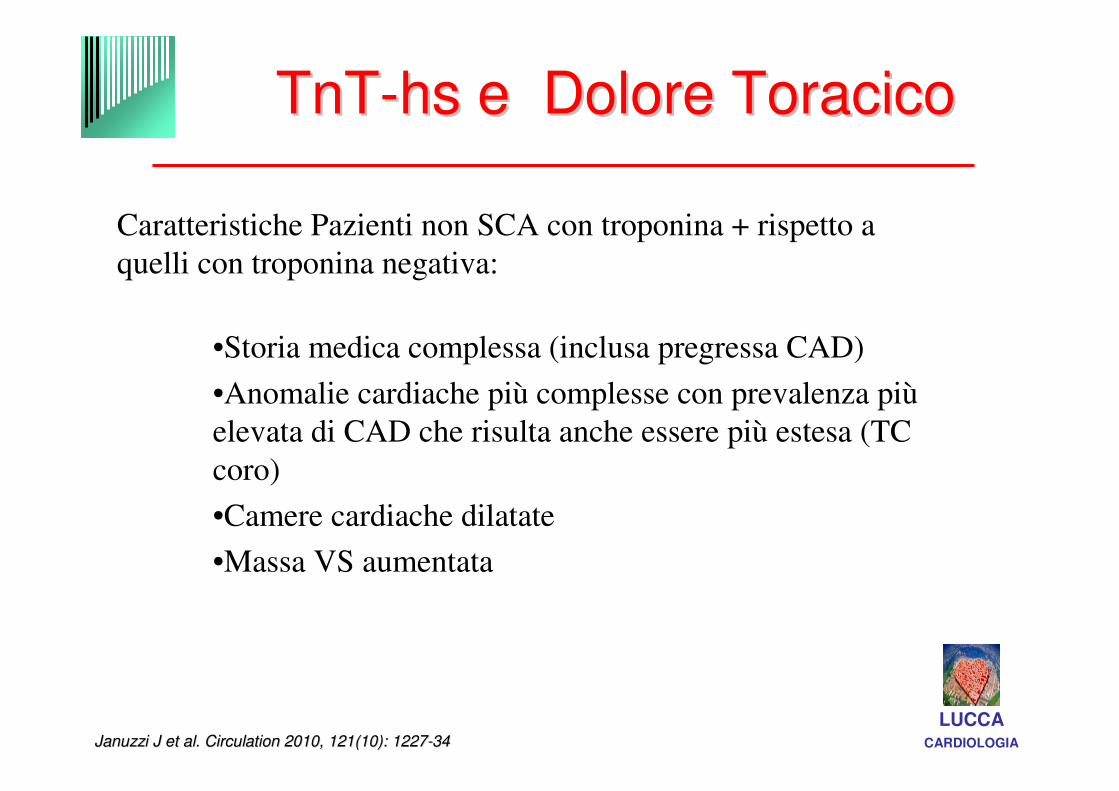
TnTTnT--hs e Dolore Toracicohs e Dolore Toracico
Januzzi J et al. Circulation 2010, 121Januzzi J et al. Circulation 2010, 121(10): 1227(10): 1227--3434
Caratteristiche Pazienti non SCA con troponina + rispetto a
quelli con troponina negativa:
•Storia medica complessa (inclusa pregressa CAD)
•Anomalie cardiache più complesse con prevalenza più
elevata di CAD che risulta anche essere più estesa (TC
coro)
•Camere cardiache dilatate
•Massa VS aumentata
LUCCACARDIOLOGIA
How Low Can You Go
if You Can See the Rise?• First, it is very likely from a large body of data that the way to make the
distinction between those with acute heart disease and this modest number of patients with structural heart disease who have increases is by looking for rising values
• There will, of course, be doubters. Sometimes the timing will not allow this analysis to be done, and when using cardiac troponin T, there are occasional patients with ST-segment elevation myocardial infarction who have a double peaked curve;
• The increases that are structural are modest, so patients who have substantial increases in troponin (decided on an assay-by-assay basis) will not need to be evaluated by assessing change over time, and those at high risk will be admitted regardless of changes.
• the increased sensitivity will cause complaints from clinicians who are frustrated by their inability to find an etiology for an increased troponin value and blame the assays. But there are multiple advantages to more sensitive assays
• Riferimento dallas study per aumenti cronici
Jaffe Jacc 2006Jaffe Jacc 2006
Making it More SensitiveThe New Era of Troponin Use
• Accordingly, the established diagnostic troponin
• cutoff representing the 99th percentile of a
reference population should only be applied in
patients with suspected acute coronary
syndrome, whereas in other clinical settings,
• individual thresholds or categories must be
established.
• In the current issue of Circulation, Saunders et
al5 now
Keller, circulation 2011Keller, circulation 2011
Delta change: 50 come da ehj 2012
• a definition of rise and or fall is required to distinguish “normal,” or chronic background troponin levels from acute changes.
• The Universal definition of MI group recommended a 20% change from the baseline value to be diagnostic reinfarction with the current troponin assays. (ERDS)
Clin Chim Acta. 2010 Jun 3;411(11-12):812-7. High-sensitive cardiac troponin I (hs-cTnI) values in patients with
stable cardiovascular disease: an initial foray.Schulz O, Reinicke M, Berghoefer GH, Bensch R, Kraemer J, Schimke
I, Jaffe AS.
Stable cardiovascular patients have detectable hs-cTnI concentrations irrespective of their underlying disease. In this heterogeneous group of patients with diverse etiologies for cardiac disease, values were not helpful in distinguishing the etiology of the elevations or in predicting prognosis.
Livelli aumentati di troponina sono frequentemente associati a patologie non
primitivamente coronariche
L’ischemia secondaria (IMA di tipo II) è un meccanismo frequente in molte
condizioni ma non è il solo e la sua discriminazione da altre noxae patogene è
spesso complessa
Alcune peculiarità debbono essere sottolineate nelle patologie che si associano al
rilascio di Tn non in corso di sindrome coronarica acuta:
• Presentazione clinica�Contestualizzare del dato di laboratorio
• Andamento temporale del rilascio � Evoluzione clinico/strumentale
• La presenza di fattori confondenti
LUCCACARDIOLOGIA
CONCLUSIONICONCLUSIONI
C’è almeno una malattia in ogni organo capace di causare l’incremento della troponina…
…i ricercatori hanno rilevato la troponina elevata anche in un corpo mummificato di circa 3000 anni fa…..suggerendo una
morte cardiaca improvvisa (!!!)…
LUCCACARDIOLOGIA
Heart 2011;97:940-946
GRAZIE PER LGRAZIE PER L’’ATTENZIONE!!!!ATTENZIONE!!!! LUCCACARDIOLOGIA