III Sessione Carcinoma della mammella -...
67
III Sessione Carcinoma della mammella Novità nel trattamento della malattia avanzata G. Ricciardi Università degli Studi di Messina
Transcript of III Sessione Carcinoma della mammella -...

III Sessione
Carcinoma della
mammella
Novità nel
trattamento della
malattia avanzata
G. Ricciardi
Università degli Studi di Messina
OUTLINE
New insight in to HR-positive/HER2-negative MBC
Emerging Therapeutic options in HER2-positive MBC
Brain Metastases and HER2 disease
Triple Negative Breast Cancer
Other

OUTLINE
New insight in to HR-positive/HER2-negative MBC
Emerging Therapeutic options in HER2-positive MBC
Brain Metastases and HER2 disease
Triple Negative Breast Cancer
Other
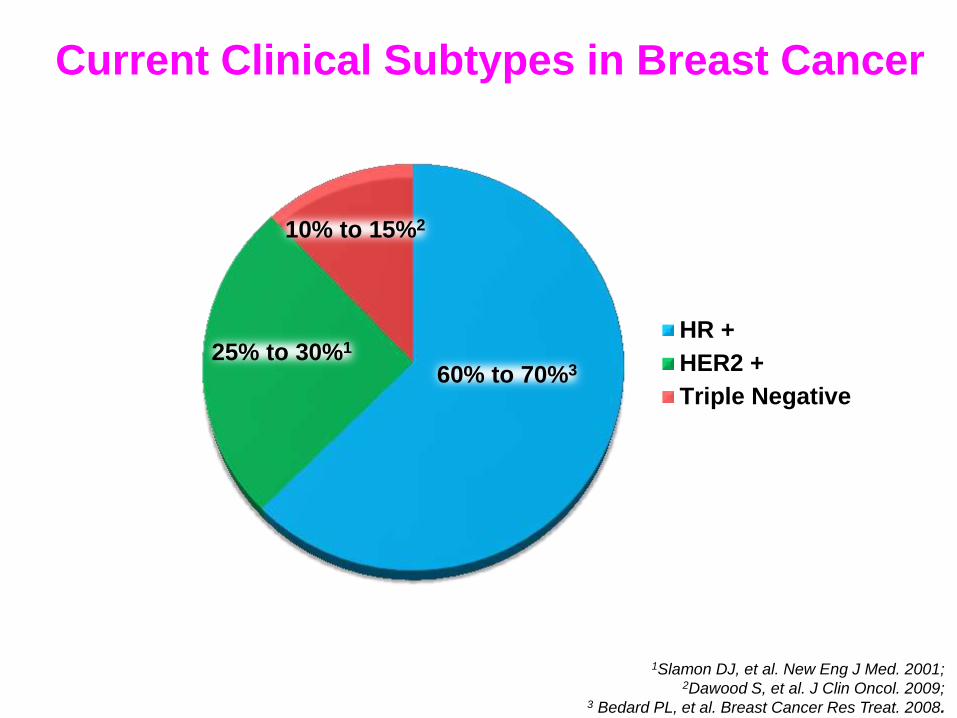
HR +
HER2 +
Triple Negative
10% to 15%2
25% to 30%1
60% to 70%3
1Slamon DJ, et al. New Eng J Med. 2001; 2Dawood S, et al. J Clin Oncol. 2009;
3 Bedard PL, et al. Breast Cancer Res Treat. 2008.
Current Clinical Subtypes in Breast Cancer
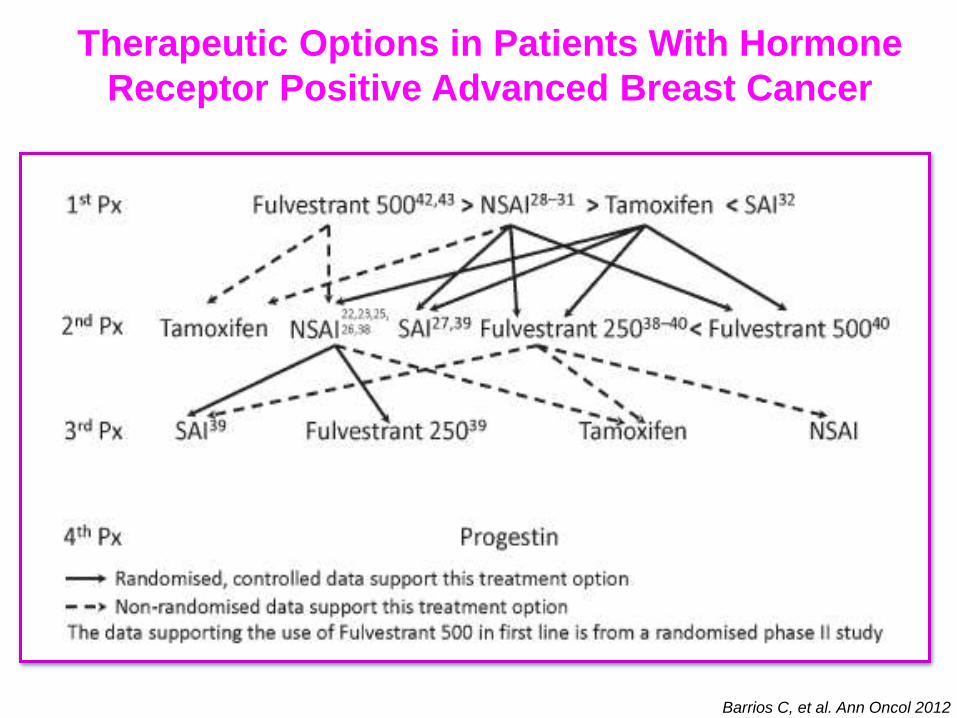
Barrios C, et al. Ann Oncol 2012
Therapeutic Options in Patients With Hormone
Receptor Positive Advanced Breast Cancer
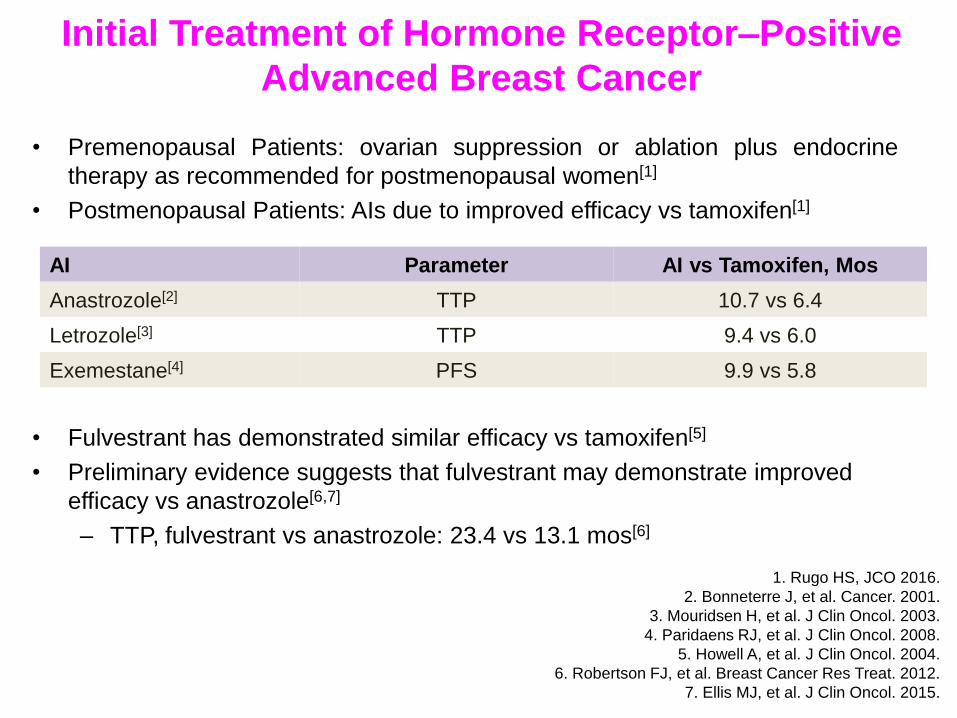
Initial Treatment of Hormone Receptor–Positive
Advanced Breast Cancer
• Premenopausal Patients: ovarian suppression or ablation plus endocrine
therapy as recommended for postmenopausal women[1]
• Postmenopausal Patients: AIs due to improved efficacy vs tamoxifen[1]
• Fulvestrant has demonstrated similar efficacy vs tamoxifen[5]
• Preliminary evidence suggests that fulvestrant may demonstrate improved
efficacy vs anastrozole[6,7]
– TTP, fulvestrant vs anastrozole: 23.4 vs 13.1 mos[6]
AI Parameter AI vs Tamoxifen, Mos
Anastrozole[2] TTP 10.7 vs 6.4
Letrozole[3] TTP 9.4 vs 6.0
Exemestane[4] PFS 9.9 vs 5.8
1. Rugo HS, JCO 2016.
2. Bonneterre J, et al. Cancer. 2001.
3. Mouridsen H, et al. J Clin Oncol. 2003.
4. Paridaens RJ, et al. J Clin Oncol. 2008.
5. Howell A, et al. J Clin Oncol. 2004.
6. Robertson FJ, et al. Breast Cancer Res Treat. 2012.
7. Ellis MJ, et al. J Clin Oncol. 2015.
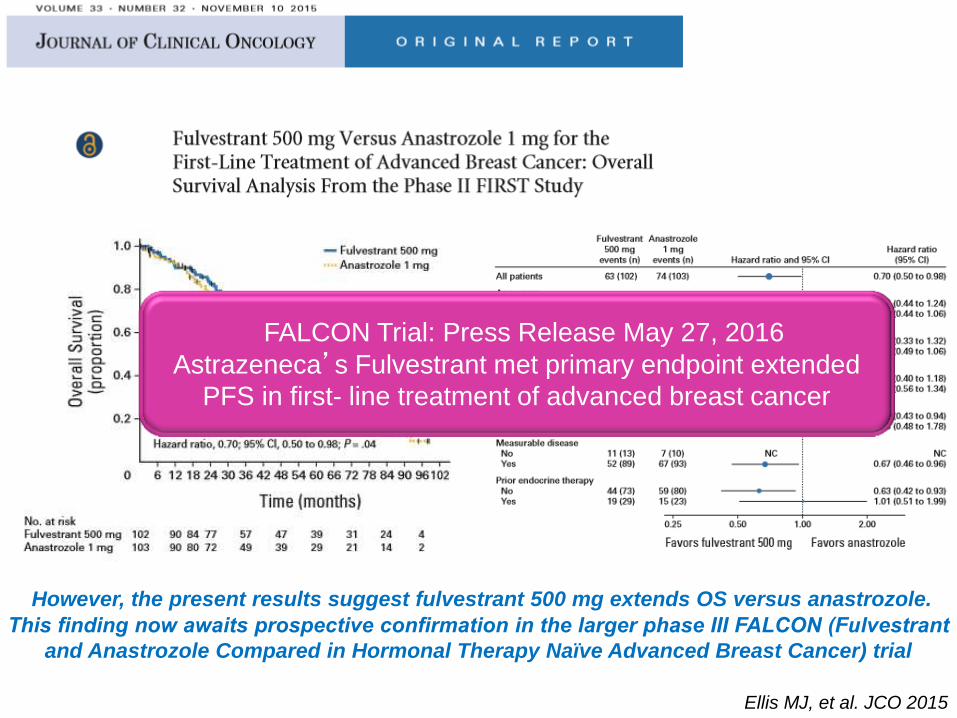
However, the present results suggest fulvestrant 500 mg extends OS versus anastrozole.
This finding now awaits prospective confirmation in the larger phase III FALCON (Fulvestrant
and Anastrozole Compared in Hormonal Therapy Naïve Advanced Breast Cancer) trial
Ellis MJ, et al. JCO 2015
FALCON Trial: Press Release May 27, 2016
Astrazeneca’s Fulvestrant met primary endpoint extended
PFS in first- line treatment of advanced breast cancer
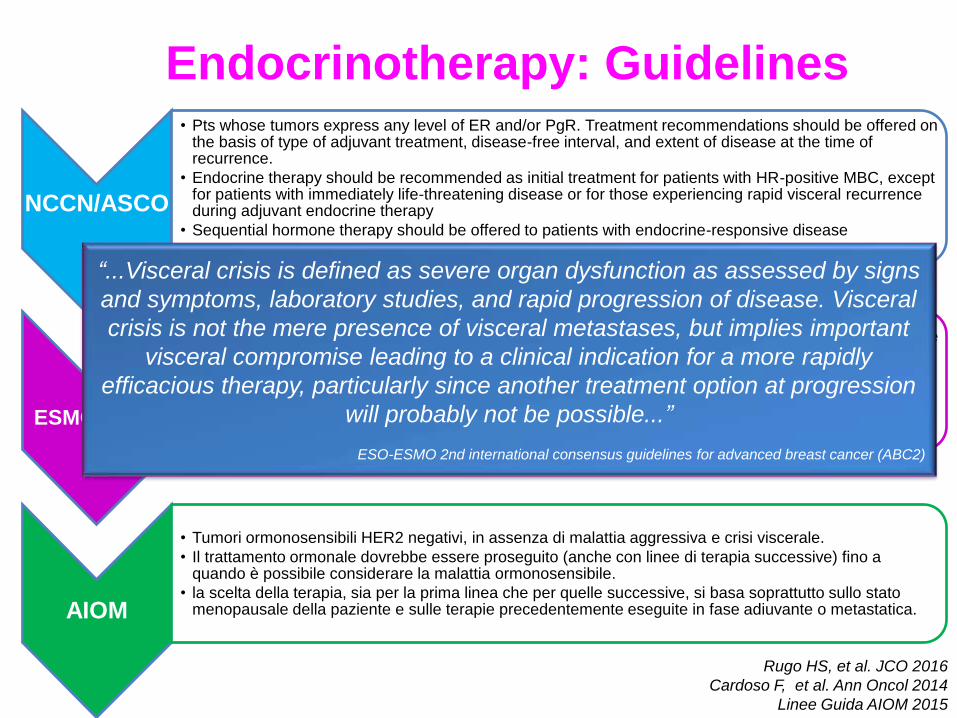
Endocrinotherapy: Guidelines
NCCN/ASCO
• Pts whose tumors express any level of ER and/or PgR. Treatment recommendations should be offered on the basis of type of adjuvant treatment, disease-free interval, and extent of disease at the time of recurrence.
• Endocrine therapy should be recommended as initial treatment for patients with HR-positive MBC, except for patients with immediately life-threatening disease or for those experiencing rapid visceral recurrence during adjuvant endocrine therapy
• Sequential hormone therapy should be offered to patients with endocrine-responsive disease
• Treatment should be administered until there is unequivocal evidence of disease progression.
ESMO/ABC2
• the preferential use of endocrine therapy, even in the presence of visceral metastases,until clear evidence of endocrine resistance.
• Chemotherapy should be reserved for cases of rapidly progressive disease or proven endocrine resistance.
• Endocrine treatment after CT(maintenance ET)to maintain benefit is a reasonable option,althought his approach has not been assessed in randomized trials.
AIOM
• Tumori ormonosensibili HER2 negativi, in assenza di malattia aggressiva e crisi viscerale.
• Il trattamento ormonale dovrebbe essere proseguito (anche con linee di terapia successive) fino a quando è possibile considerare la malattia ormonosensibile.
• la scelta della terapia, sia per la prima linea che per quelle successive, si basa soprattutto sullo stato menopausale della paziente e sulle terapie precedentemente eseguite in fase adiuvante o metastatica.
Rugo HS, et al. JCO 2016
Cardoso F, et al. Ann Oncol 2014
Linee Guida AIOM 2015
“...Visceral crisis is defined as severe organ dysfunction as assessed by signs
and symptoms, laboratory studies, and rapid progression of disease. Visceral
crisis is not the mere presence of visceral metastases, but implies important
visceral compromise leading to a clinical indication for a more rapidly
efficacious therapy, particularly since another treatment option at progression
will probably not be possible...”
ESO-ESMO 2nd international consensus guidelines for advanced breast cancer (ABC2)

About 50% of hormone receptor-positive breast cancers are de novo
resistant to endocrine therapy. This intrinsic resistance occurs de novo at
the initial exposure to endocrine therapy. However, 25% of ER+/PgR+
tumors, 66% of ER+/PgR- tumors and 55% of ER-/PgR+ tumors fail to
respond to tamoxifen or develop early resistance to tamoxifen for reason
that are unclear.
1.Gant M. Expert Rev. Anticancer Ther. 2012).
2.Moy B et al. Clin. Cancer Res. 2006
Almost all patients with advanced disease will develop
acquired resistance to endocrine therapies. That acquired
resistance manifests over time after an initial response to
endocrine therapy.
The mechanisms of de novo and acquired resistance are likely
similar, but are not completely understood.
The Problem in ER+HER2 neg Breast Cancer
Is Endocrine Therapy Resistance
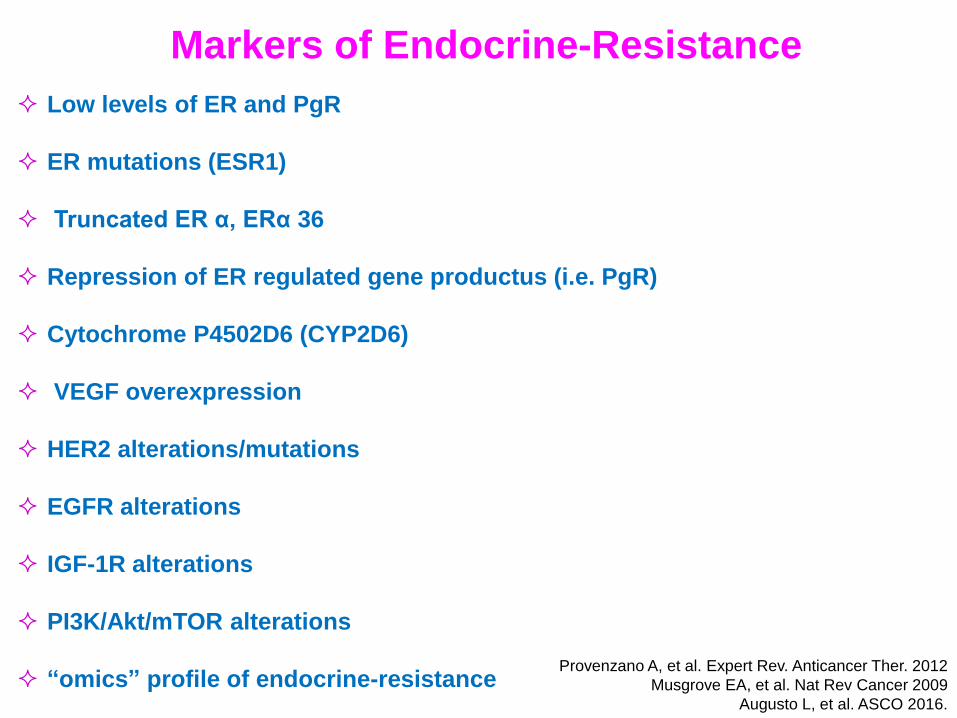
Low levels of ER and PgR
ER mutations (ESR1)
Truncated ER α, ERα 36
Repression of ER regulated gene productus (i.e. PgR)
Cytochrome P4502D6 (CYP2D6)
VEGF overexpression
HER2 alterations/mutations
EGFR alterations
IGF-1R alterations
PI3K/Akt/mTOR alterations
“omics” profile of endocrine-resistance Provenzano A, et al. Expert Rev. Anticancer Ther. 2012
Musgrove EA, et al. Nat Rev Cancer 2009
Augusto L, et al. ASCO 2016.
Markers of Endocrine-Resistance
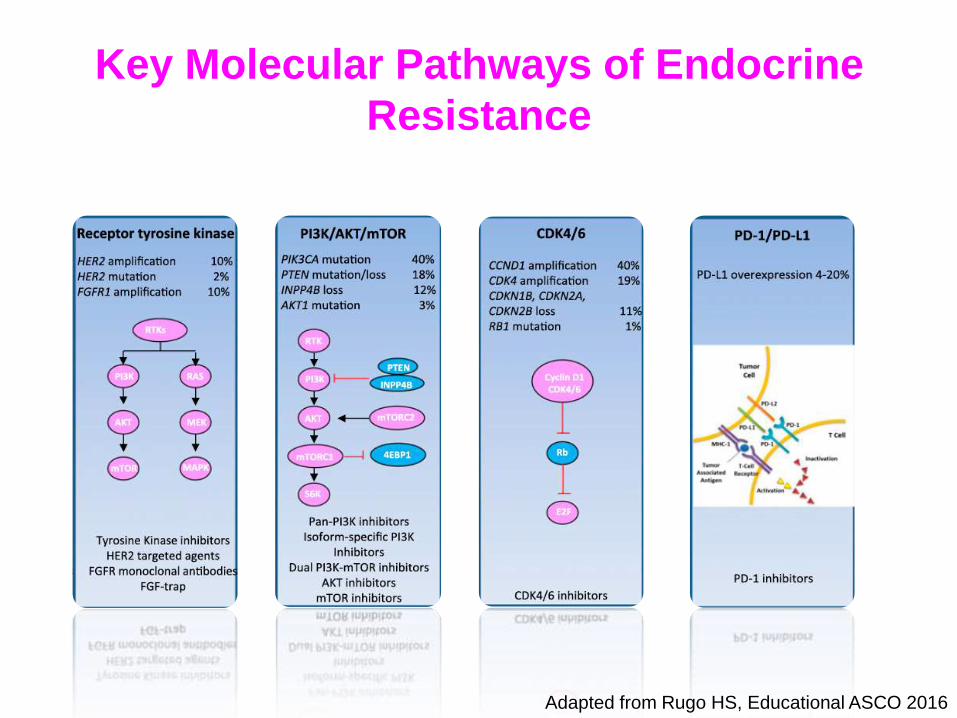
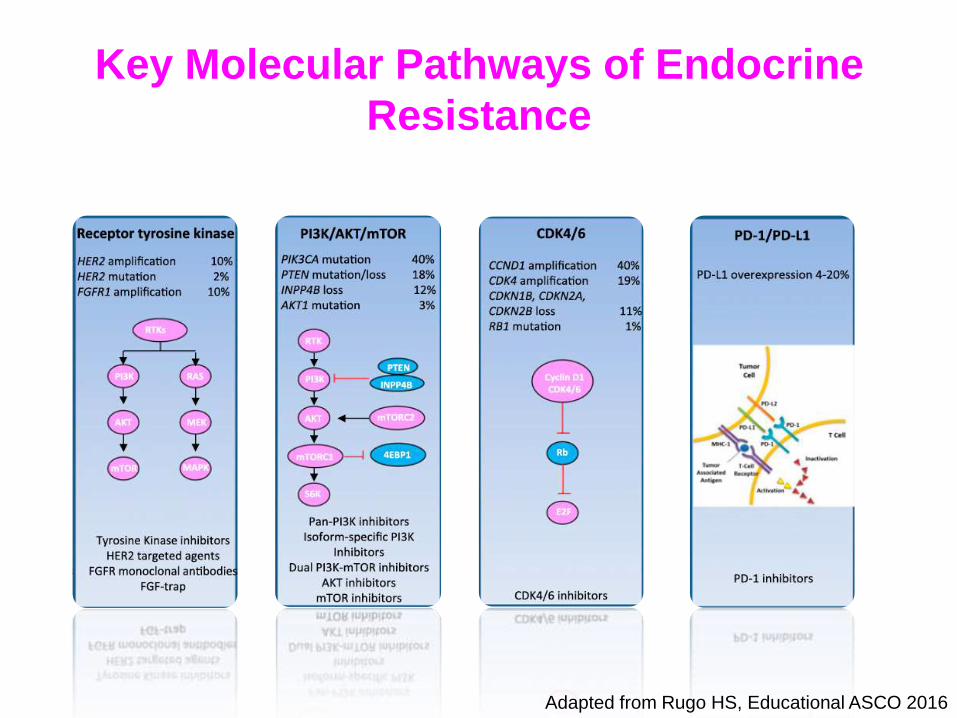
Key Molecular Pathways of Endocrine
Resistance
Adapted from Rugo HS, Educational ASCO 2016
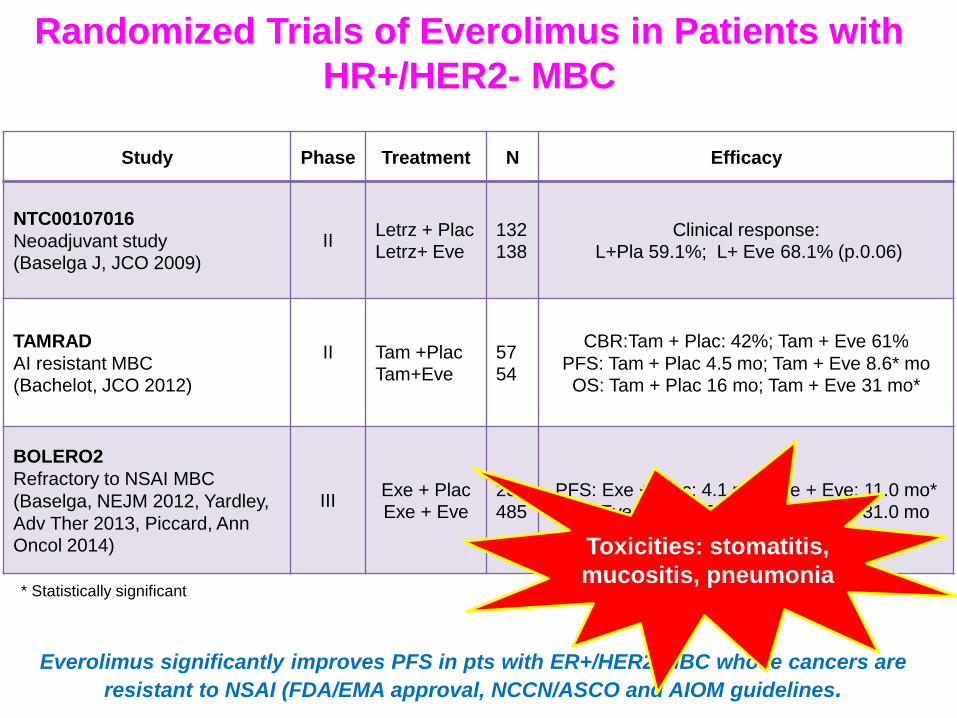
Study Phase Treatment N Efficacy
NTC00107016
Neoadjuvant study (Baselga J, JCO 2009)
II Letrz + Plac Letrz+ Eve
132 138
Clinical response: L+Pla 59.1%; L+ Eve 68.1% (p.0.06)
TAMRAD
AI resistant MBC (Bachelot, JCO 2012)
II
Tam +Plac Tam+Eve
57 54
CBR:Tam + Plac: 42%; Tam + Eve 61%
PFS: Tam + Plac 4.5 mo; Tam + Eve 8.6* mo OS: Tam + Plac 16 mo; Tam + Eve 31 mo*
BOLERO2
Refractory to NSAI MBC
(Baselga, NEJM 2012, Yardley,
Adv Ther 2013, Piccard, Ann Oncol 2014)
III Exe + Plac Exe + Eve
239 485
PFS: Exe + Plac: 4.1 mo; Exe + Eve: 11.0 mo* OS: Eve+ Plac: 26.6 mo; Exe + Eve 31.0 mo
Randomized Trials of Everolimus in Patients with
HR+/HER2- MBC
Everolimus significantly improves PFS in pts with ER+/HER2-MBC whose cancers are
resistant to NSAI (FDA/EMA approval, NCCN/ASCO and AIOM guidelines.
* Statistically significant
Toxicities: stomatitis,
mucositis, pneumonia
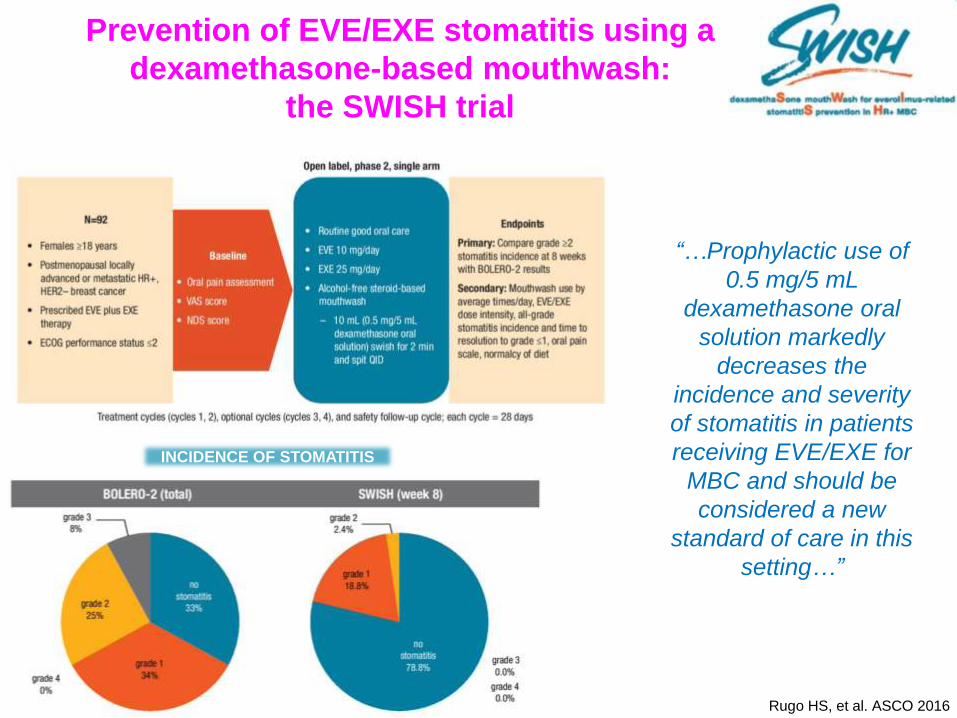
Prevention of EVE/EXE stomatitis using a
dexamethasone-based mouthwash:
the SWISH trial
Rugo HS, et al. ASCO 2016
INCIDENCE OF STOMATITIS
“…Prophylactic use of
0.5 mg/5 mL
dexamethasone oral
solution markedly
decreases the
incidence and severity
of stomatitis in patients
receiving EVE/EXE for
MBC and should be
considered a new
standard of care in this
setting…”
…can you predict who benefit from mTOR
inhibitors in the clinic…

•The cfDNA analysis suggest that pts with harboring PI3KCA activating mutations derive a similar PFS
benefit from everolimus compared to pts without PI3KCA mutations. •This analysis support the previous observation that everolimus efficacy was indipendent of PI3KCA.
•Limitation of this analysis included the evaluation of only 3 PI3KCA and relatively small samples size for
muation Site-specific subgroups.
Moynahan ME, et al. ASCO 2016
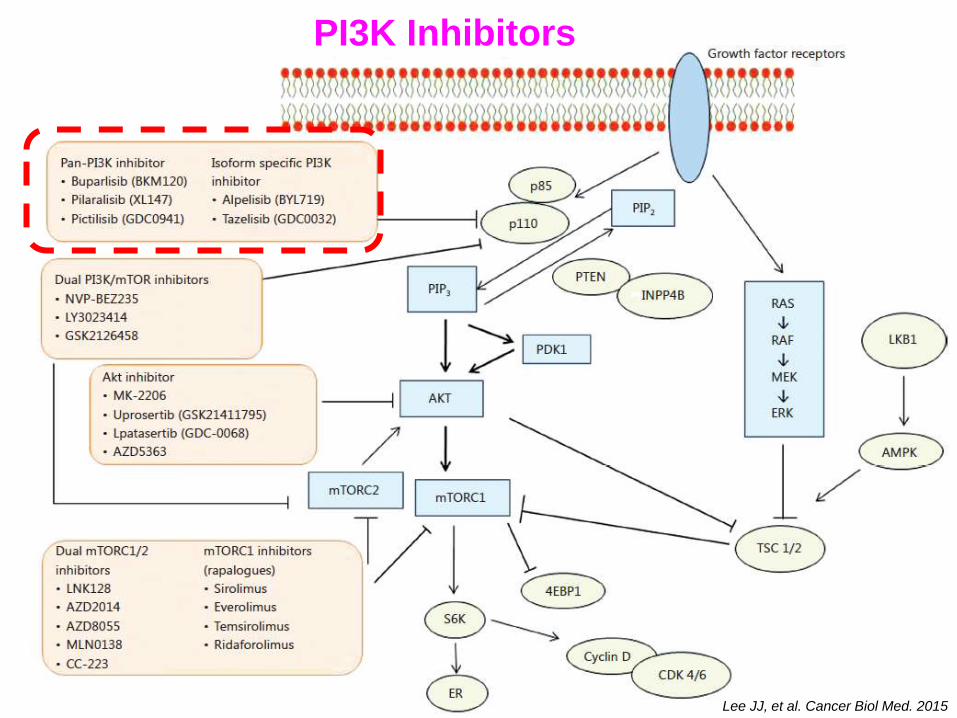
Lee JJ, et al. Cancer Biol Med. 2015
PI3K Inhibitors
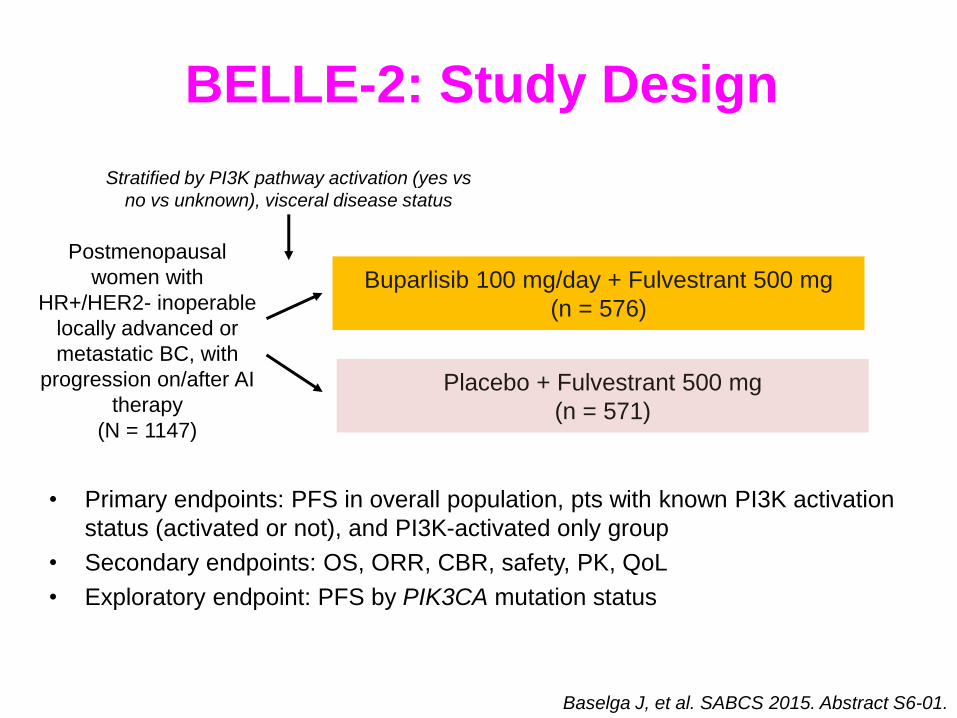
BELLE-2: Study Design
• Primary endpoints: PFS in overall population, pts with known PI3K activation
status (activated or not), and PI3K-activated only group
• Secondary endpoints: OS, ORR, CBR, safety, PK, QoL
• Exploratory endpoint: PFS by PIK3CA mutation status
Postmenopausal
women with
HR+/HER2- inoperable
locally advanced or
metastatic BC, with
progression on/after AI
therapy
(N = 1147)
Buparlisib 100 mg/day + Fulvestrant 500 mg
(n = 576)
Placebo + Fulvestrant 500 mg
(n = 571)
Baselga J, et al. SABCS 2015. Abstract S6-01.
Stratified by PI3K pathway activation (yes vs
no vs unknown), visceral disease status
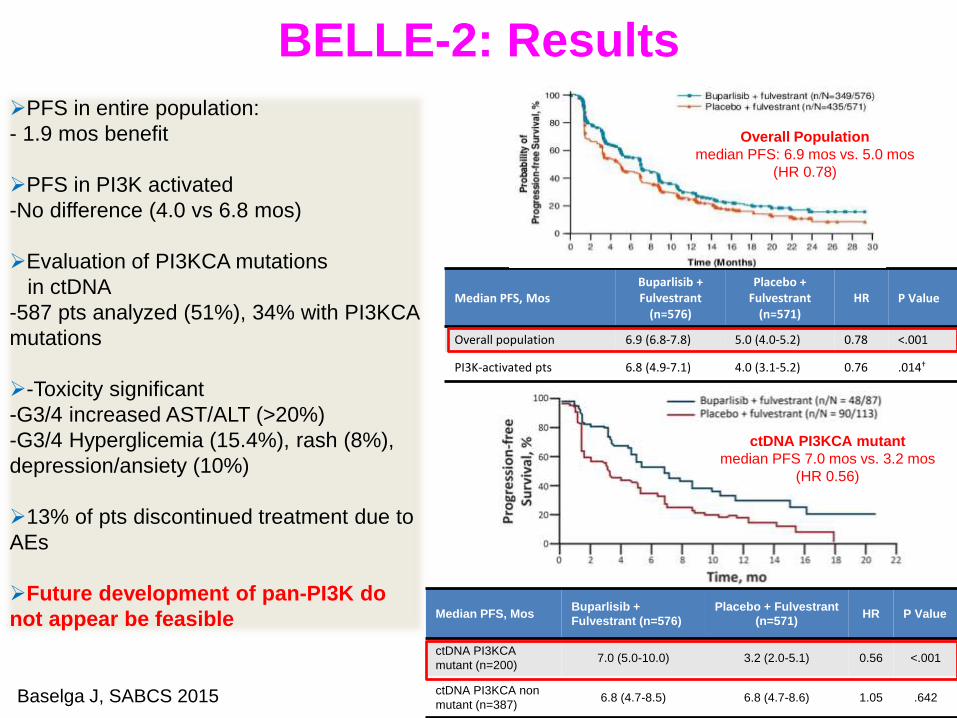
BELLE-2: Results
Median PFS, Mos
Buparlisib + Fulvestrant
(n=576)
Placebo + Fulvestrant
(n=571) HR P Value
Overall population 6.9 (6.8-7.8) 5.0 (4.0-5.2) 0.78 <.001
PI3K-activated pts 6.8 (4.9-7.1) 4.0 (3.1-5.2) 0.76 .014†
PFS in entire population:
- 1.9 mos benefit
PFS in PI3K activated
-No difference (4.0 vs 6.8 mos)
Evaluation of PI3KCA mutations
in ctDNA
-587 pts analyzed (51%), 34% with PI3KCA
mutations
-Toxicity significant
-G3/4 increased AST/ALT (>20%)
-G3/4 Hyperglicemia (15.4%), rash (8%),
depression/ansiety (10%)
13% of pts discontinued treatment due to
AEs
Future development of pan-PI3K do
not appear be feasible Median PFS, Mos Buparlisib +
Fulvestrant (n=576)
Placebo + Fulvestrant
(n=571) HR P Value
ctDNA PI3KCA
mutant (n=200) 7.0 (5.0-10.0) 3.2 (2.0-5.1) 0.56 <.001
ctDNA PI3KCA non
mutant (n=387) 6.8 (4.7-8.5) 6.8 (4.7-8.6) 1.05 .642
ctDNA PI3KCA mutant
median PFS 7.0 mos vs. 3.2 mos
(HR 0.56)
Overall Population
median PFS: 6.9 mos vs. 5.0 mos
(HR 0.78)
Baselga J, SABCS 2015

Key Molecular Pathways of Endocrine
Resistance
Adapted from Rugo HS, Educational ASCO 2016
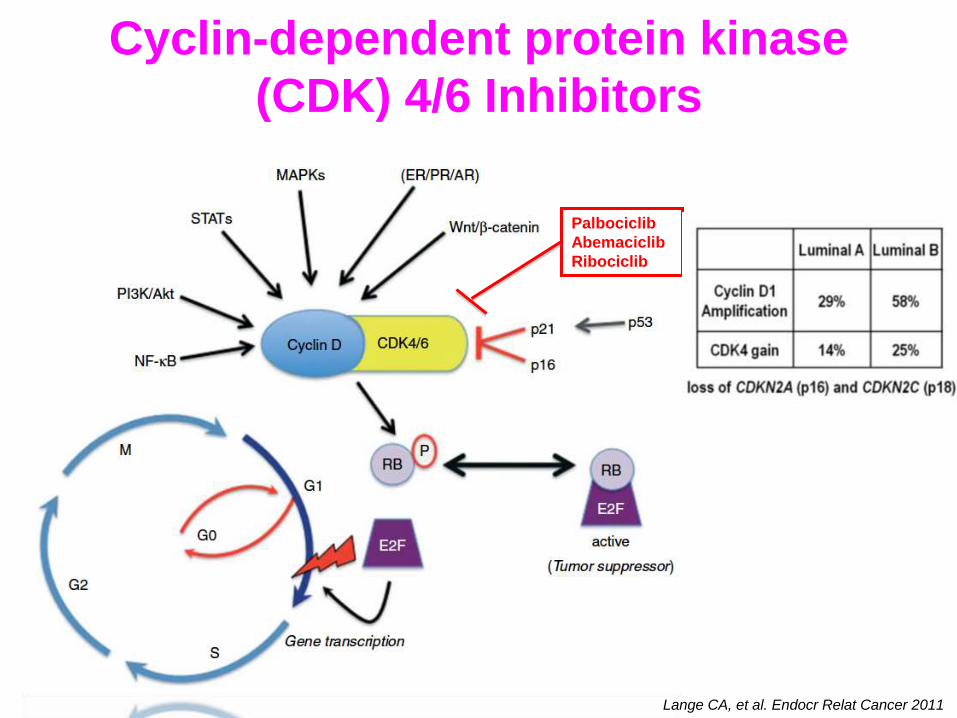
Cyclin-dependent protein kinase
(CDK) 4/6 Inhibitors
Lange CA, et al. Endocr Relat Cancer 2011
Palbociclib
Abemaciclib
Ribociclib
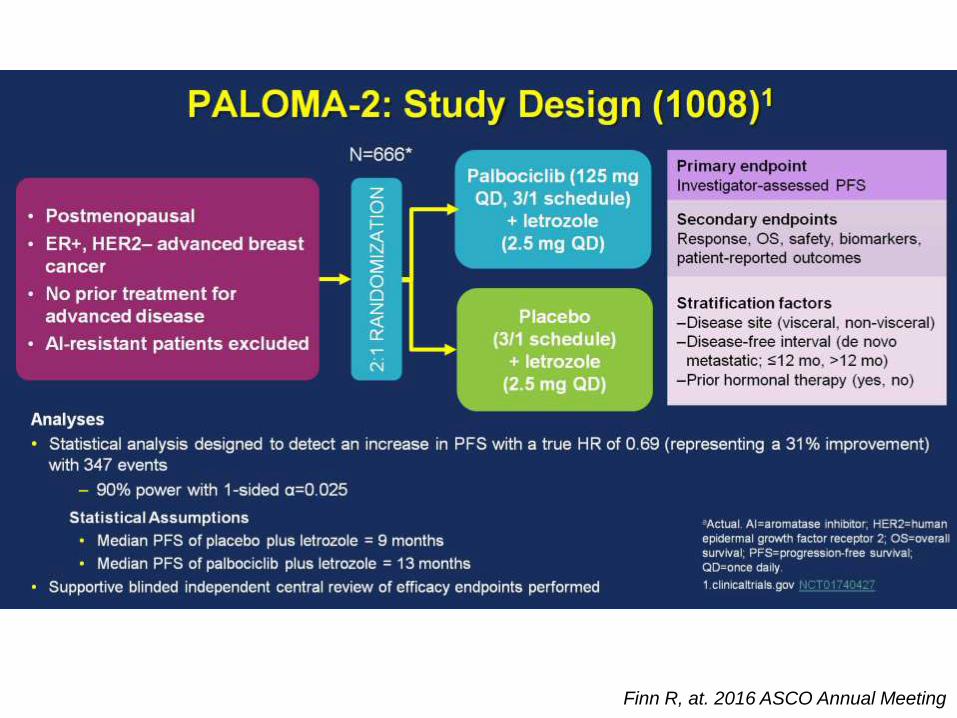
Slide 6
Finn R, at. 2016 ASCO Annual Meeting

PFS: Blinded Independent Central Review<br />Confirms PFS Advantage Observed Using Investigator Assessment
PALOMA-2: Efficacy
“…PALOMA-2 expands and confirms the significant clinical benefit and safety of P+L in ER+/HER2–
ABC pts who had not received prior systemic therapy for their advanced disease…”
Finn R, et al. 2016 ASCO Annual Meeting
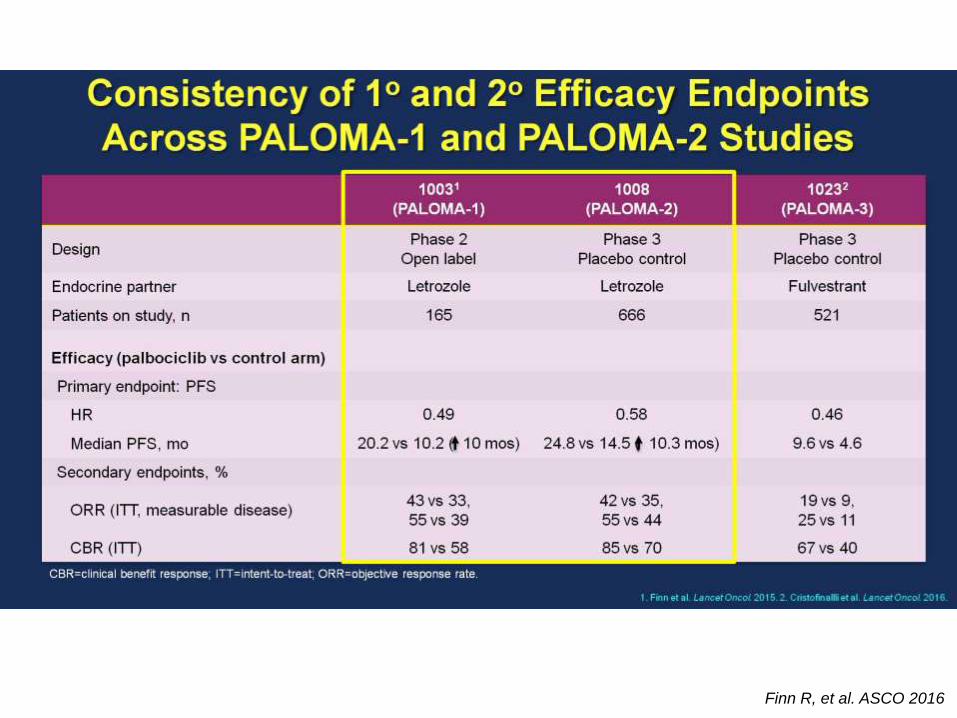
Consistency of 1o and 2o Efficacy Endpoints Across PALOMA-1 and PALOMA-2 Studies
Finn R, et al. ASCO 2016
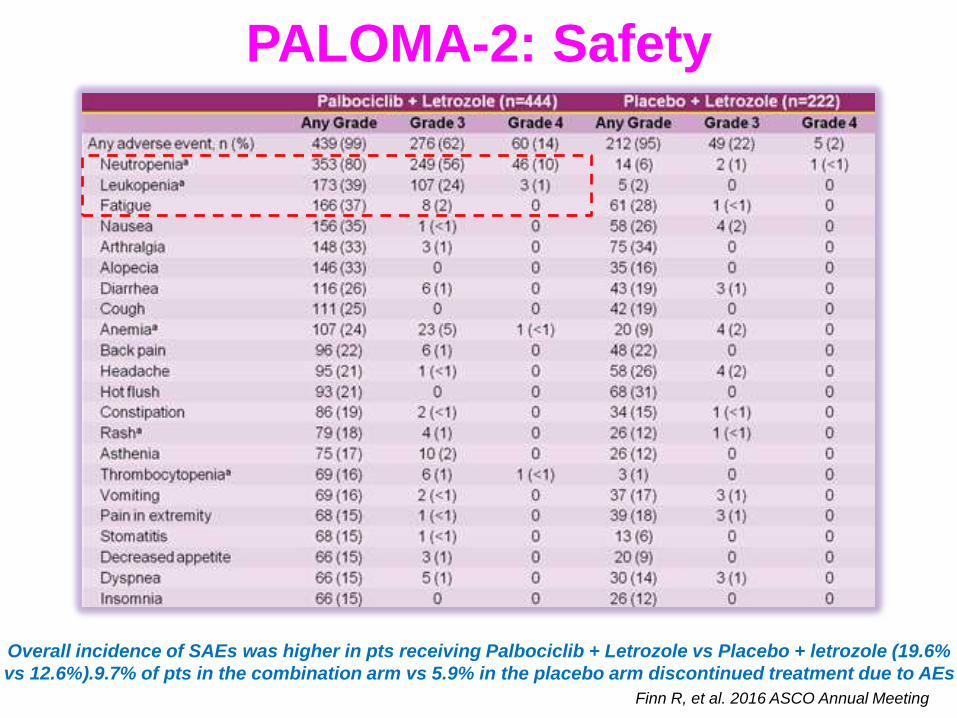
PALOMA-2: Safety
Overall incidence of SAEs was higher in pts receiving Palbociclib + Letrozole vs Placebo + letrozole (19.6%
vs 12.6%).9.7% of pts in the combination arm vs 5.9% in the placebo arm discontinued treatment due to AEs
Finn R, et al. 2016 ASCO Annual Meeting
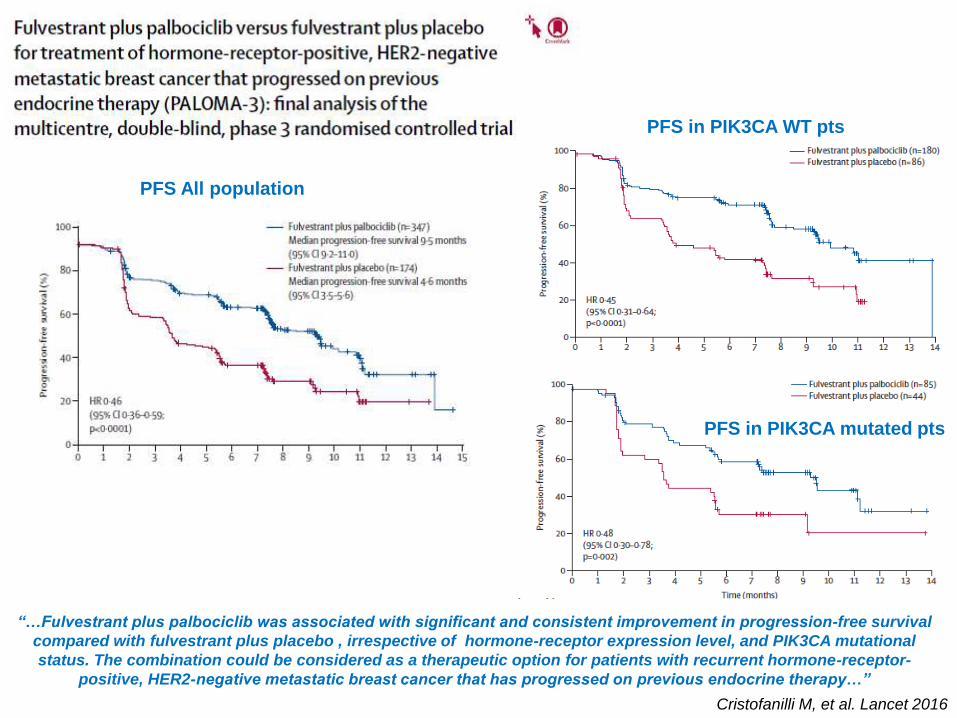
PFS All population
Cristofanilli M, et al. Lancet 2016
“…Fulvestrant plus palbociclib was associated with significant and consistent improvement in progression-free survival
compared with fulvestrant plus placebo , irrespective of hormone-receptor expression level, and PIK3CA mutational
status. The combination could be considered as a therapeutic option for patients with recurrent hormone-receptor-
positive, HER2-negative metastatic breast cancer that has progressed on previous endocrine therapy…”
PFS in PIK3CA WT pts
PFS in PIK3CA mutated pts
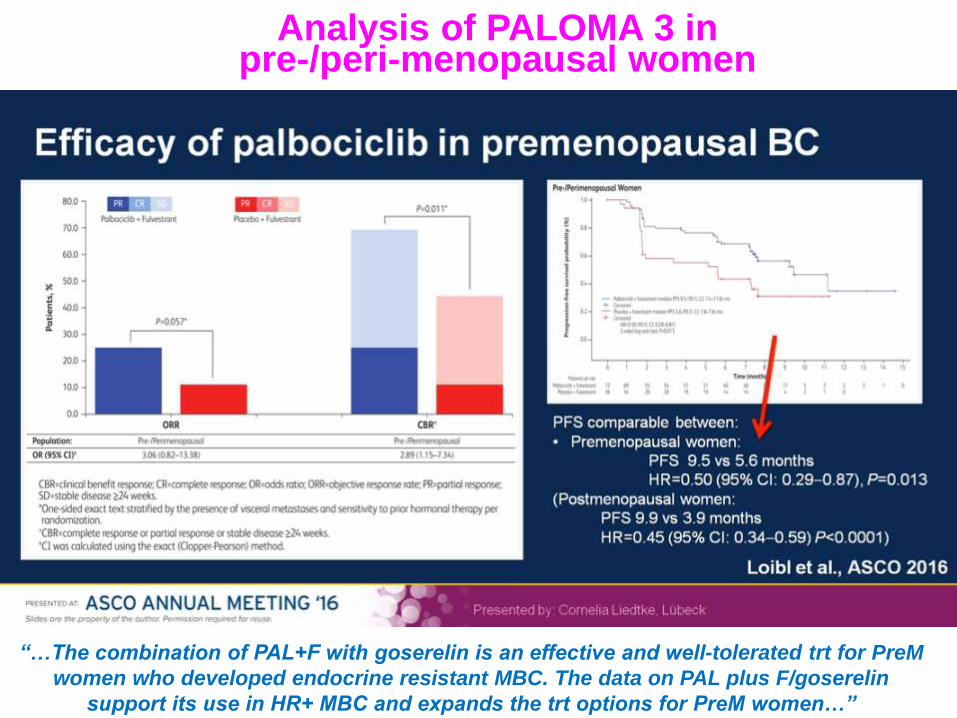
Analysis of PALOMA 3 in pre-/peri-menopausal women
“…The combination of PAL+F with goserelin is an effective and well-tolerated trt for PreM
women who developed endocrine resistant MBC. The data on PAL plus F/goserelin
support its use in HR+ MBC and expands the trt options for PreM women…”
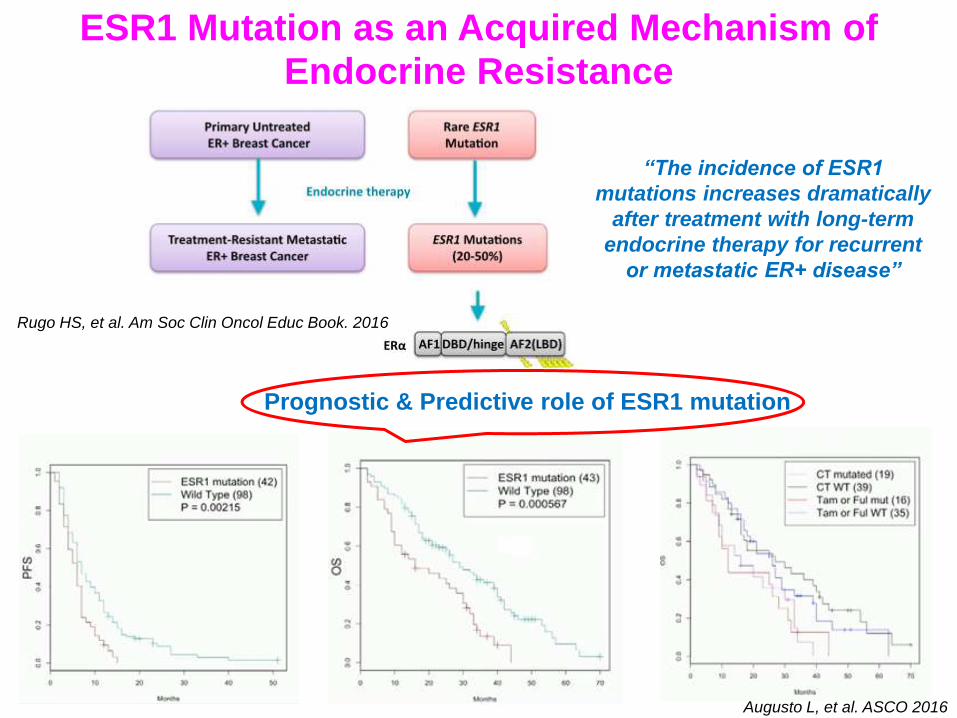
ESR1 Mutation as an Acquired Mechanism of Endocrine Resistance
“The incidence of ESR1
mutations increases dramatically
after treatment with long-term
endocrine therapy for recurrent
or metastatic ER+ disease”
Prognostic & Predictive role of ESR1 mutation
Rugo HS, et al. Am Soc Clin Oncol Educ Book. 2016
Augusto L, et al. ASCO 2016
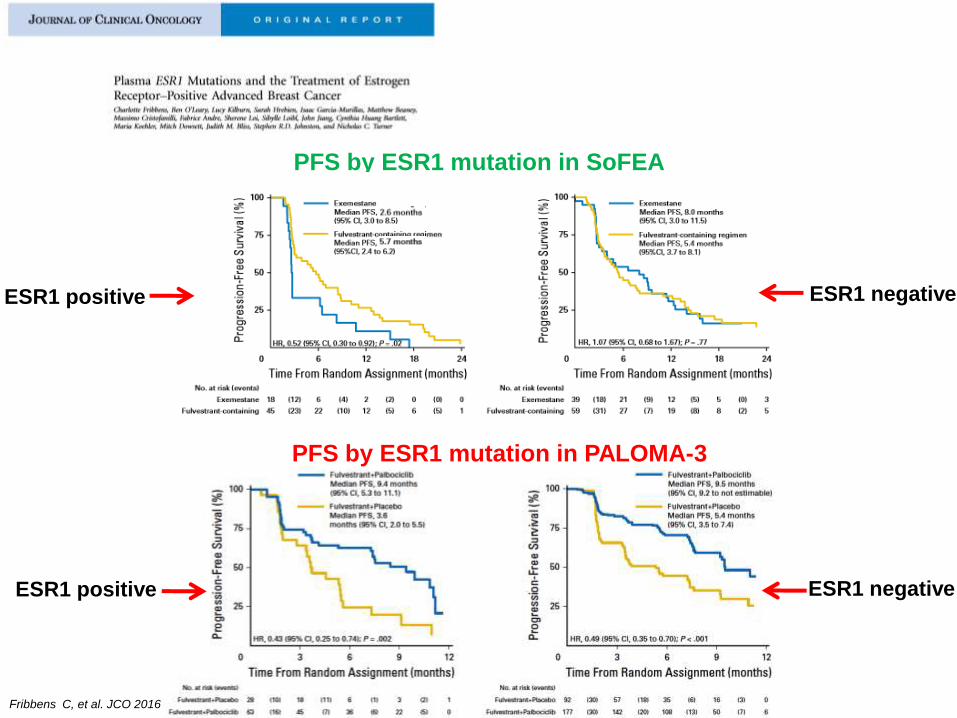
PFS by ESR1 mutation in SoFEA
PFS by ESR1 mutation in PALOMA-3
ESR1 positive
ESR1 positive
ESR1 negative
ESR1 negative
Fribbens C, et al. JCO 2016
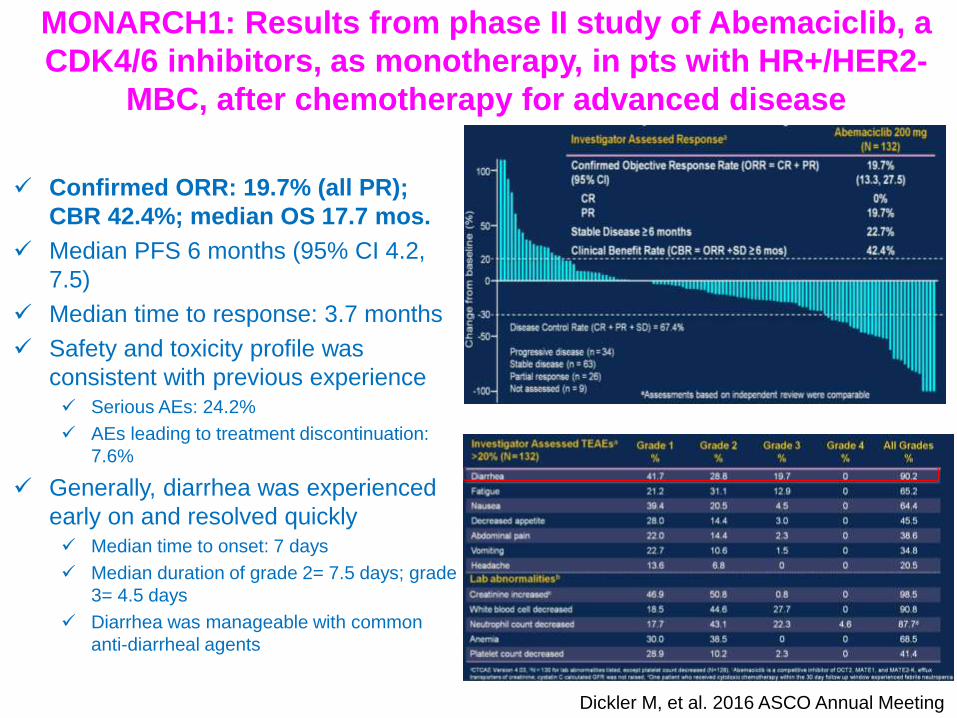
MONARCH1: Results from phase II study of Abemaciclib, a
CDK4/6 inhibitors, as monotherapy, in pts with HR+/HER2-
MBC, after chemotherapy for advanced disease
Confirmed ORR: 19.7% (all PR);
CBR 42.4%; median OS 17.7 mos.
Median PFS 6 months (95% CI 4.2,
7.5)
Median time to response: 3.7 months
Safety and toxicity profile was
consistent with previous experience Serious AEs: 24.2%
AEs leading to treatment discontinuation:
7.6%
Generally, diarrhea was experienced
early on and resolved quickly Median time to onset: 7 days
Median duration of grade 2= 7.5 days; grade
3= 4.5 days
Diarrhea was manageable with common
anti-diarrheal agents
Dickler M, et al. 2016 ASCO Annual Meeting
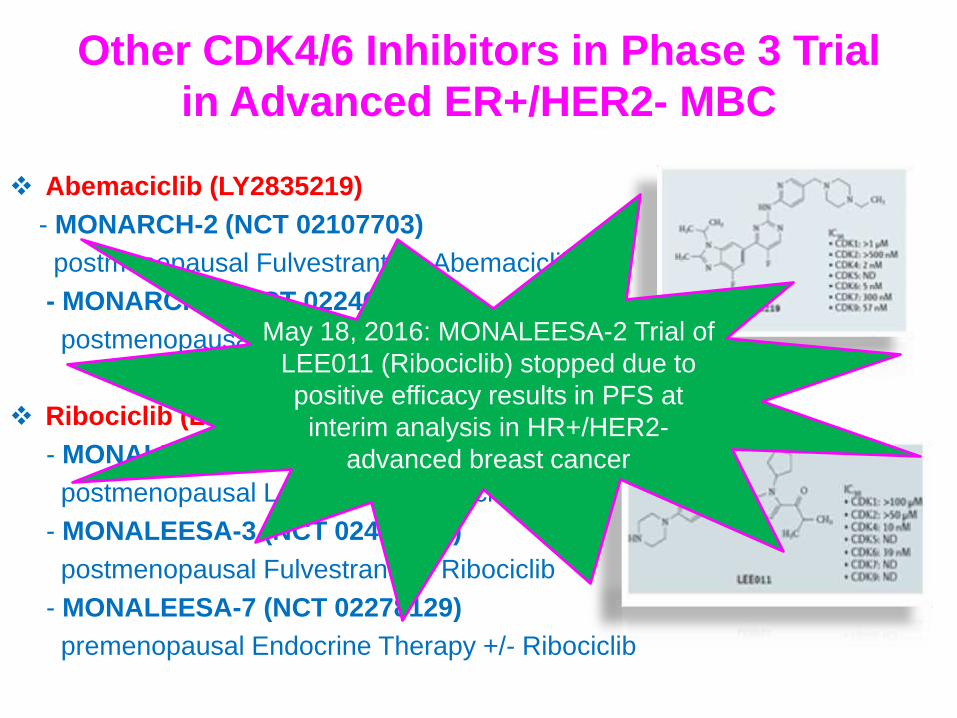
Other CDK4/6 Inhibitors in Phase 3 Trial
in Advanced ER+/HER2- MBC
Abemaciclib (LY2835219)
- MONARCH-2 (NCT 02107703)
postmenopausal Fulvestrant +/- Abemaciclib
- MONARCH-3 (NCT 02246621)
postmenopausal NSAI +/- Abemaciclib
Ribociclib (LEE 011)
- MONALEESA-2 (NCT 01958021)
postmenopausal Letrozolo +/- Ribociclib
- MONALEESA-3 (NCT 02422615)
postmenopausal Fulvestrant +/- Ribociclib
- MONALEESA-7 (NCT 02278129)
premenopausal Endocrine Therapy +/- Ribociclib
May 18, 2016: MONALEESA-2 Trial of
LEE011 (Ribociclib) stopped due to
positive efficacy results in PFS at
interim analysis in HR+/HER2-
advanced breast cancer
Key Molecular Pathways of Endocrine
Resistance
Adapted from Rugo HS, Educational ASCO 2016
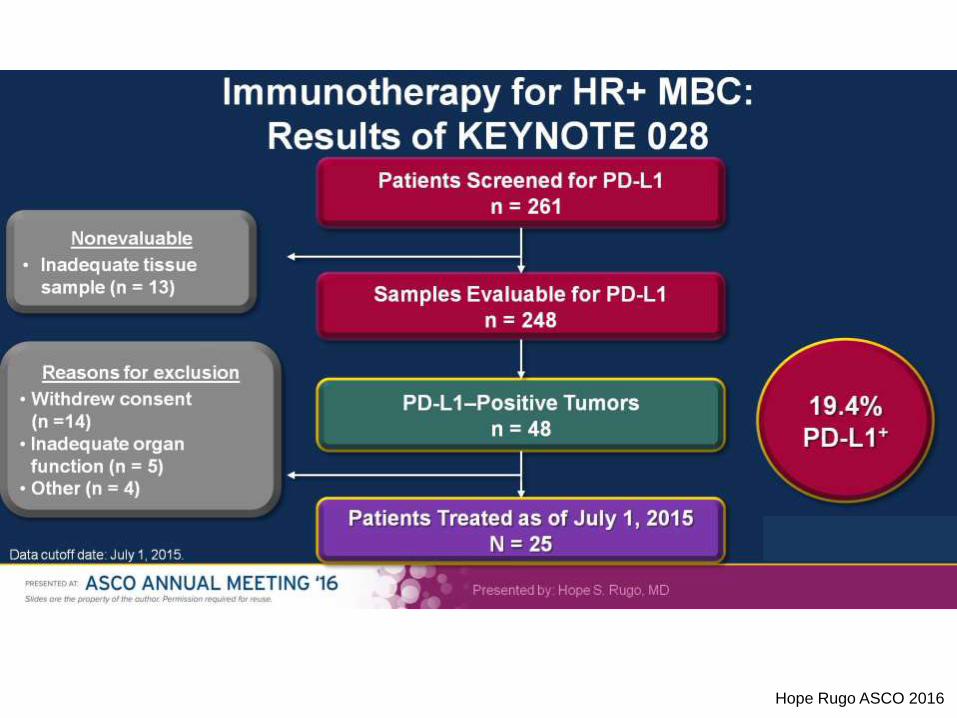
Immunotherapy for HR+ MBC: <br />Results of KEYNOTE 028
Hope Rugo ASCO 2016
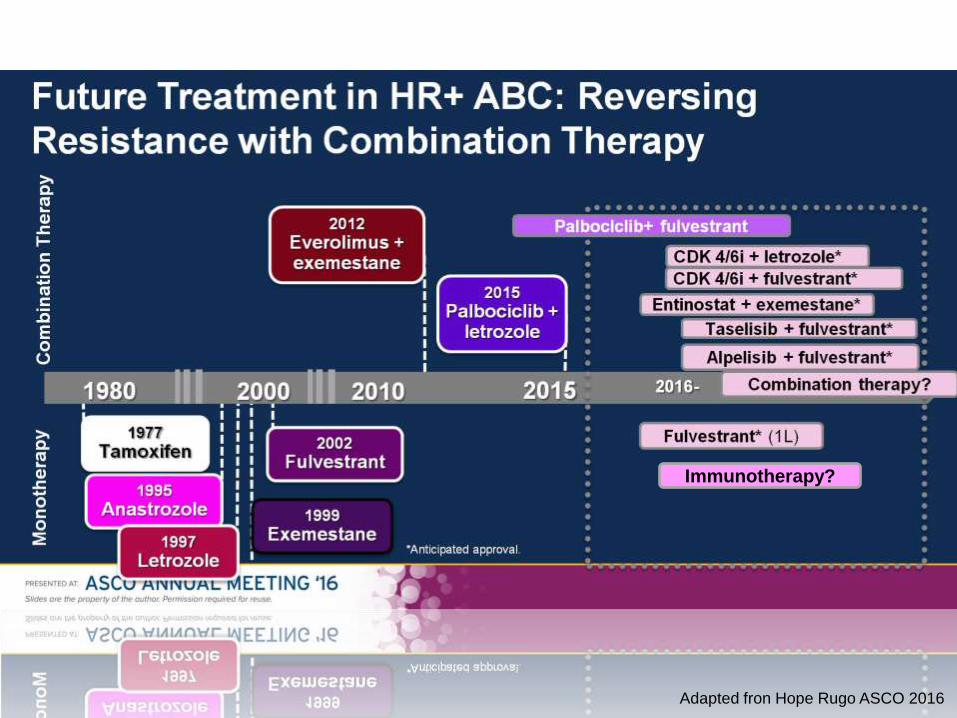
Future Treatment in HR+ ABC: Reversing Resistance with Combination Therapy
Adapted fron Hope Rugo ASCO 2016
Immunotherapy?

OUTLINE
New insight in to HR-positive/HER2-negative MBC
Emerging Therapeutic options in HER2-positive MBC
Brain Metastases and HER2 disease
Triple Negative Breast Cancer
Other

Overview of improvements in OS brought
by anti HER2 agents
1 Slamon D, et al. NEJM 2001; 2 Cameron D, et al. Oncologist 2010; 3 Geyer CE, et al. NEJM 2006; 4 Baselga J, et al. NEJM 2012; 5 Swain SM, et al.
NEJM 2015; 6 Verma S, et al. NEJM 2012; 7 Krop IE, et al. Lancet Oncol 2014; 8Wildiers H, et al. SABCS 2015.
CHT
0 10 20 30 40 50 60
20,3
CHT + H 25,1
CAPE 14,88
CAPE + LAP 17,25
D + H 40,8
D + H + P 56,5
Slamon D, 2001 [1]
Cameron D, 2011 [2,3]
CLEOPATRA [4,5]
TPC 25,1
T-DM1 30,9 EMILIA [6]
CAPE + LAP 15,8
T-DM1 22,7 TH3RESA [7,8]
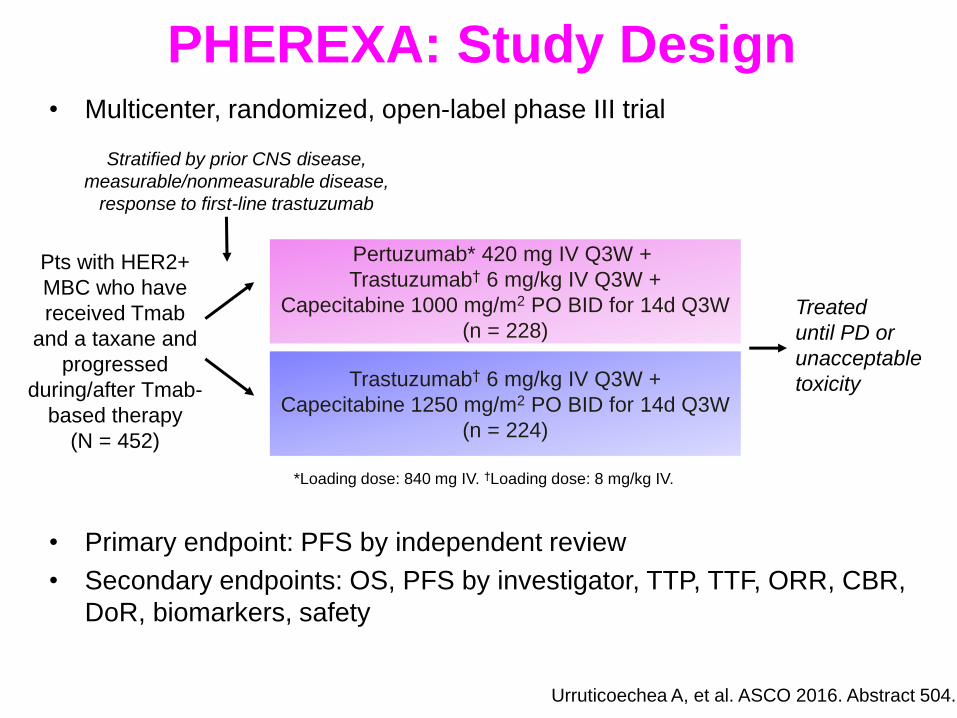
PHEREXA: Study Design • Multicenter, randomized, open-label phase III trial
• Primary endpoint: PFS by independent review
• Secondary endpoints: OS, PFS by investigator, TTP, TTF, ORR, CBR,
DoR, biomarkers, safety
Urruticoechea A, et al. ASCO 2016. Abstract 504.
Stratified by prior CNS disease,
measurable/nonmeasurable disease,
response to first-line trastuzumab
Pts with HER2+
MBC who have
received Tmab
and a taxane and
progressed
during/after Tmab-
based therapy
(N = 452)
Pertuzumab* 420 mg IV Q3W +
Trastuzumab† 6 mg/kg IV Q3W +
Capecitabine 1000 mg/m2 PO BID for 14d Q3W
(n = 228)
Trastuzumab† 6 mg/kg IV Q3W +
Capecitabine 1250 mg/m2 PO BID for 14d Q3W
(n = 224)
Treated
until PD or
unacceptable
toxicity
*Loading dose: 840 mg IV. †Loading dose: 8 mg/kg IV.
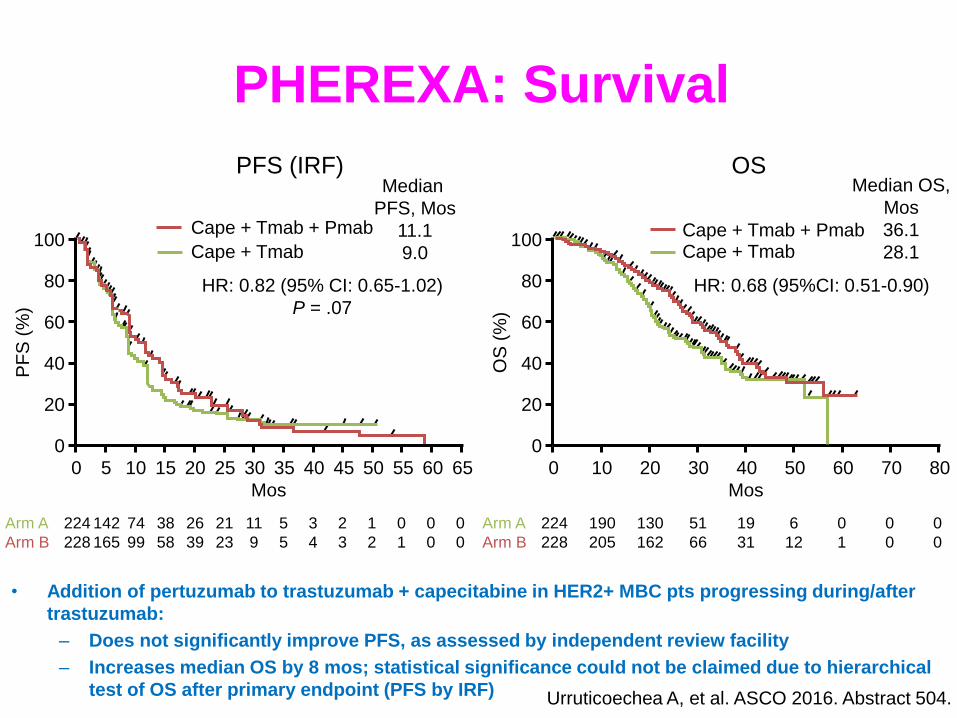
PHEREXA: Survival
Urruticoechea A, et al. ASCO 2016. Abstract 504.
PFS (IRF) OS
Cape + Tmab + Pmab
Cape + Tmab
Median
PFS, Mos
11.1
9.0 100
80
60
40
20
0
PF
S (
%)
Mos
0 65 5 10 15 20 25 30 35 40 45 50 55 60
Arm A
Arm B
224
228
142
165
74
99
38
58
26
39
21
23
11
9
5
5
3
4
2
3
1
2
0
1
0
0
0
0
Cape + Tmab + Pmab Cape + Tmab
Median OS,
Mos
36.1
28.1 100
80
60
40
20
0
OS
(%
) Mos
0 80 10 20 30 40 50 60 70
Arm A
Arm B
224
228
190
205
130
162
51
66
19
31
6
12
0
1
0
0
0
0
HR: 0.82 (95% CI: 0.65-1.02)
P = .07
HR: 0.68 (95%CI: 0.51-0.90)
• Addition of pertuzumab to trastuzumab + capecitabine in HER2+ MBC pts progressing during/after
trastuzumab:
– Does not significantly improve PFS, as assessed by independent review facility
– Increases median OS by 8 mos; statistical significance could not be claimed due to hierarchical
test of OS after primary endpoint (PFS by IRF)
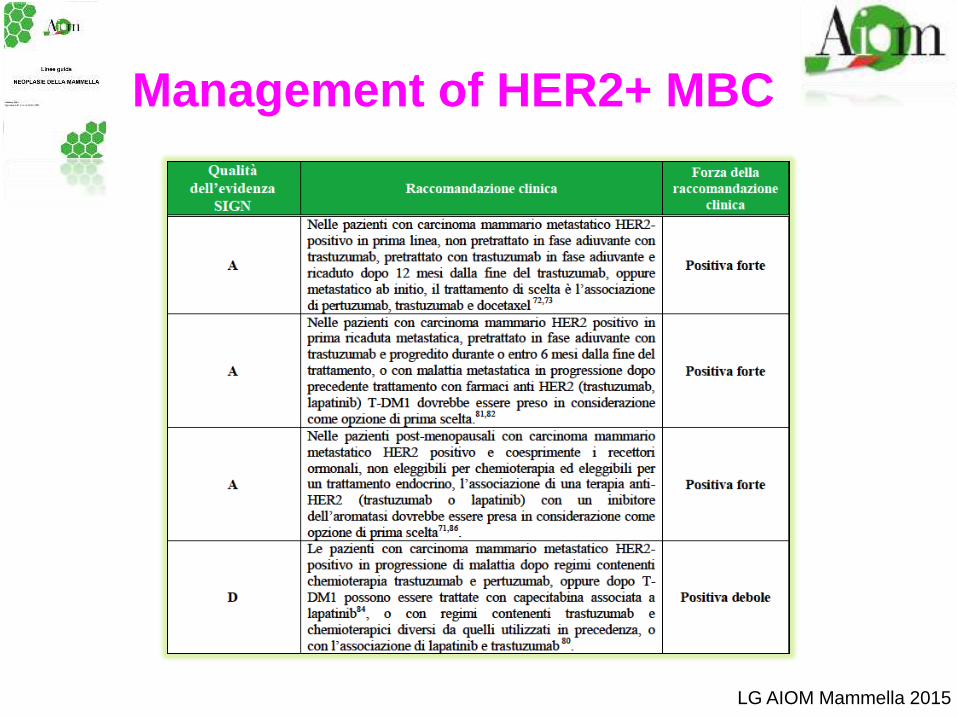
Management of HER2+ MBC
LG AIOM Mammella 2015

Neratinib: pan-HER inhibitor in
HER2-positive MBC
STUDY Phase Drug(s) Population ORR PFS OS
Burstein, 2010 [1] II Neratinib
HER2+MBC
with and without
prior
trastuzumab
40%
22.3 weeks in
prior T and
39.6 in non
prior T
N. R.
Martin M, 2013 [2] II
Neratinib
vs.
Lap-Cape
HER2+ MBC,
prior
trastuzumab
29%
vs.
41%
4.5 mos
vs.
6.8 mos
19.7 mos
vs.
23.6 mos
Saura C, 2014 [3] I/II Neratinib + Cape
HER2+ MBC,
prior
trastuzumab
and lapatinib
64% (no prior
lapatinib)
57% (prior
lapatinib)
9.27 mos (no
prior lapatinib)
8.26 mos (prior
lapatinib)
N.R.
TBCRC 022 [4] II Neratinib HER2+, BMs 8%* 1.9 mos N.R.
NEfERT-T [5] II
Neratinib-Tax
vs.
H-Tax
HER2+, 1st line
74.8%
vs.
77.6%
12.9 mos
vs. 12.9 mos N.R
1 Burstein HJ, JCO 2010; 2Martin M, et al. Eur J Cancer 2013; 3Saura C, et al. JCO 2014; 4Freedman RA, et al. JCO 2016; 5Awada A, et al. JAMA Oncol 2016
* Intracranial ORR
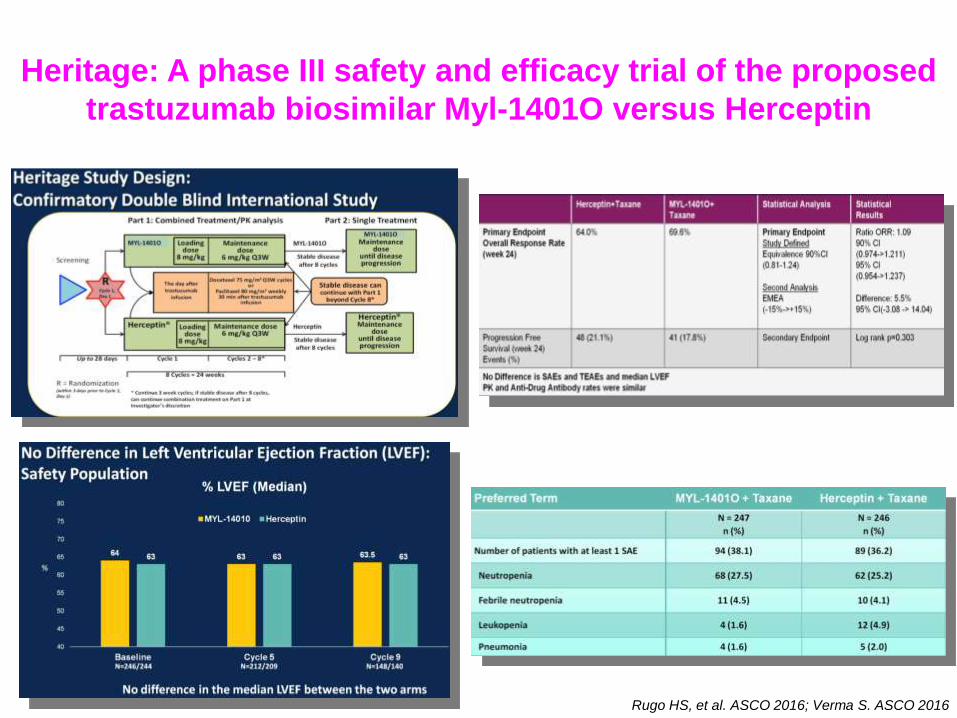
Heritage: A phase III safety and efficacy trial of the proposed
trastuzumab biosimilar Myl-1401O versus Herceptin
Rugo HS, et al. ASCO 2016; Verma S. ASCO 2016

OUTLINE
New insight in to HR-positive/HER2-negative MBC
Emerging Therapeutic options in HER2-positive MBC
Brain Metastases and HER2 disease
Triple Negative Breast Cancer
Other
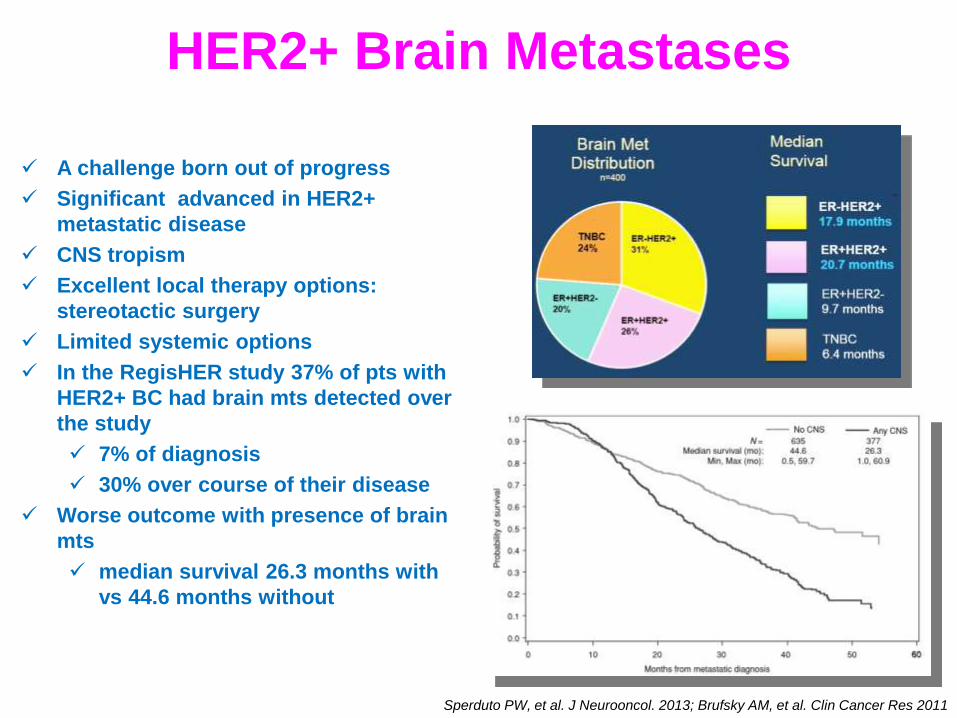
HER2+ Brain Metastases
A challenge born out of progress
Significant advanced in HER2+
metastatic disease
CNS tropism
Excellent local therapy options:
stereotactic surgery
Limited systemic options
In the RegisHER study 37% of pts with
HER2+ BC had brain mts detected over
the study
7% of diagnosis
30% over course of their disease
Worse outcome with presence of brain
mts
median survival 26.3 months with
vs 44.6 months without
Sperduto PW, et al. J Neurooncol. 2013; Brufsky AM, et al. Clin Cancer Res 2011
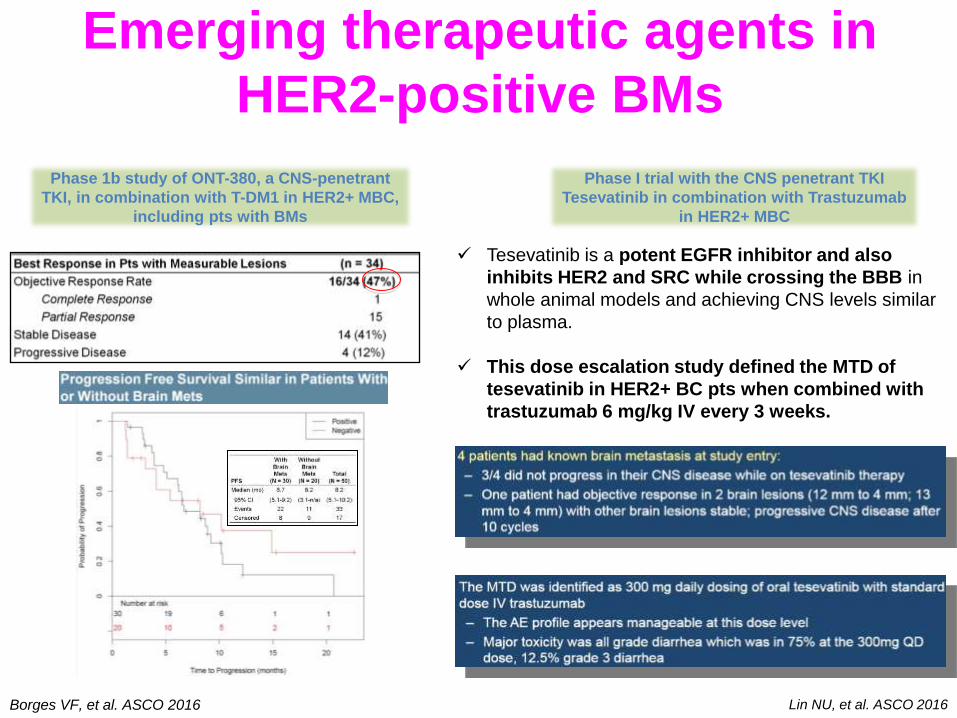
Emerging therapeutic agents in
HER2-positive BMs
Borges VF, et al. ASCO 2016
Phase 1b study of ONT-380, a CNS-penetrant
TKI, in combination with T-DM1 in HER2+ MBC,
including pts with BMs
Phase I trial with the CNS penetrant TKI
Tesevatinib in combination with Trastuzumab
in HER2+ MBC
Lin NU, et al. ASCO 2016
Tesevatinib is a potent EGFR inhibitor and also
inhibits HER2 and SRC while crossing the BBB in
whole animal models and achieving CNS levels similar
to plasma.
This dose escalation study defined the MTD of
tesevatinib in HER2+ BC pts when combined with
trastuzumab 6 mg/kg IV every 3 weeks.
OUTLINE
New insight in to HR-positive/HER2-negative MBC
Emerging Therapeutic options in HER2-positive MBC
Brain Metastases and HER2 disease
Triple Negative Breast Cancer
Other

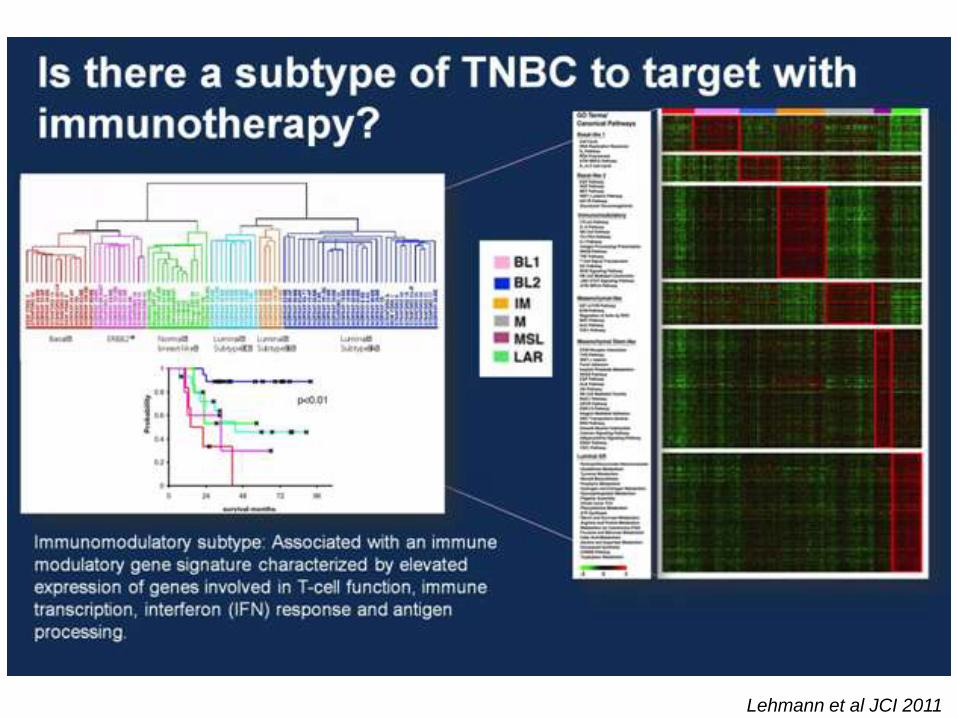
Basal-like 1: cell cycle,
DNA repair and
proliferation genes
Basal-like 2: Growth factor
signaling (EGFR, MET, Wnt,
IGF1R)
IM: immune cell
processes (medullary
breast cancer)
M: Cell motility and
differentiation, EMT
processes
MSL: similar to M but
growth factor signaling, low
levels of proliferation genes
(metaplastic cancers)
LAR: Androgen receptor
and downstream genes,
luminal features Lehmann et al JCI 2011
New classification of TNBC

Pathways, Targets and Emerging
Targeted Agents in TNBC
Mayer IA, et al. Clin Cancer Res 2014: Lehmann BD JCI 2011
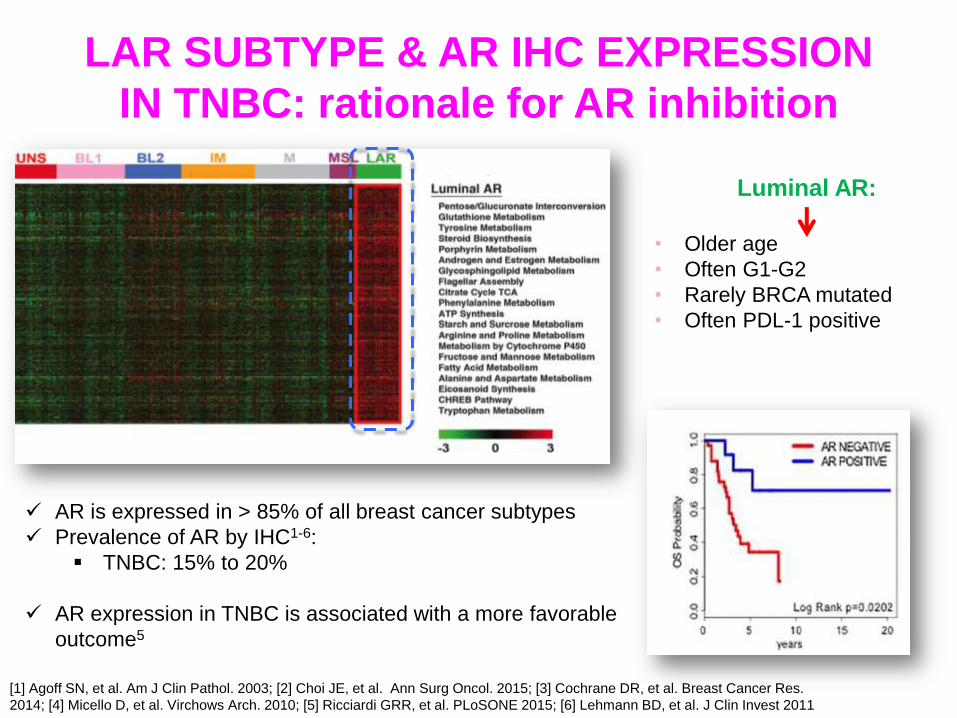
LAR SUBTYPE & AR IHC EXPRESSION
IN TNBC: rationale for AR inhibition
[1] Agoff SN, et al. Am J Clin Pathol. 2003; [2] Choi JE, et al. Ann Surg Oncol. 2015; [3] Cochrane DR, et al. Breast Cancer Res.
2014; [4] Micello D, et al. Virchows Arch. 2010; [5] Ricciardi GRR, et al. PLoSONE 2015; [6] Lehmann BD, et al. J Clin Invest 2011
AR is expressed in > 85% of all breast cancer subtypes
Prevalence of AR by IHC1-6:
TNBC: 15% to 20%
AR expression in TNBC is associated with a more favorable
outcome5
Luminal AR:
• Older age
• Often G1-G2
• Rarely BRCA mutated
• Often PDL-1 positive
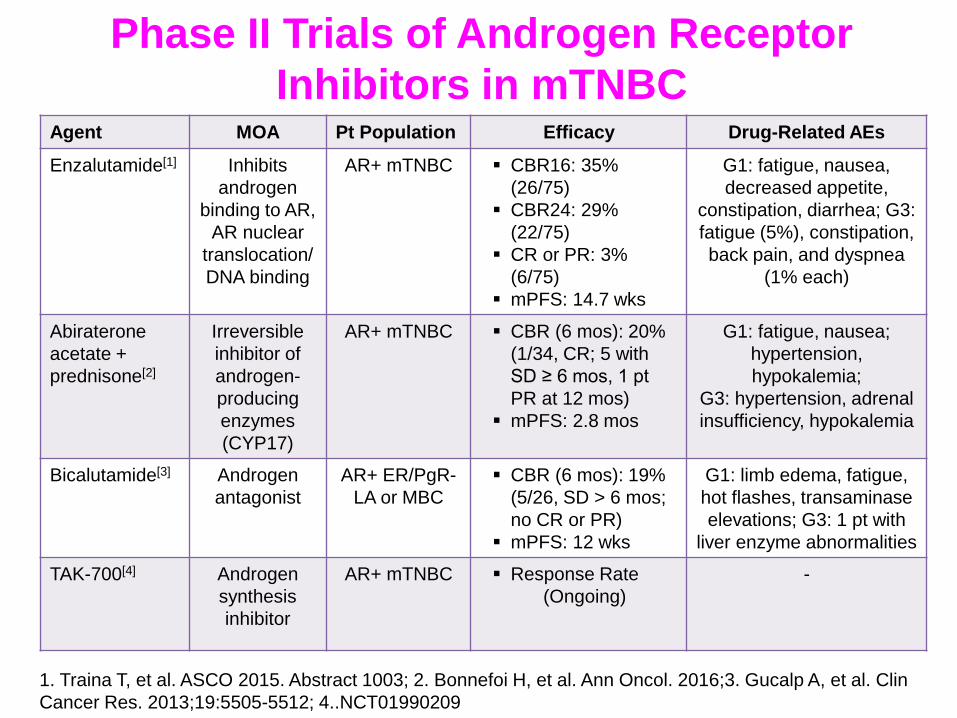
Agent MOA Pt Population Efficacy Drug-Related AEs
Enzalutamide[1] Inhibits
androgen
binding to AR,
AR nuclear
translocation/
DNA binding
AR+ mTNBC CBR16: 35%
(26/75)
CBR24: 29%
(22/75)
CR or PR: 3%
(6/75)
mPFS: 14.7 wks
G1: fatigue, nausea,
decreased appetite,
constipation, diarrhea; G3:
fatigue (5%), constipation,
back pain, and dyspnea
(1% each)
Abiraterone
acetate +
prednisone[2]
Irreversible
inhibitor of
androgen-
producing
enzymes
(CYP17)
AR+ mTNBC CBR (6 mos): 20%
(1/34, CR; 5 with
SD ≥ 6 mos, 1 pt
PR at 12 mos)
mPFS: 2.8 mos
G1: fatigue, nausea;
hypertension,
hypokalemia;
G3: hypertension, adrenal
insufficiency, hypokalemia
Bicalutamide[3] Androgen
antagonist
AR+ ER/PgR-
LA or MBC
CBR (6 mos): 19%
(5/26, SD > 6 mos;
no CR or PR)
mPFS: 12 wks
G1: limb edema, fatigue,
hot flashes, transaminase
elevations; G3: 1 pt with
liver enzyme abnormalities
TAK-700[4]
Androgen
synthesis
inhibitor
AR+ mTNBC
Response Rate
(Ongoing)
-
Phase II Trials of Androgen Receptor
Inhibitors in mTNBC
1. Traina T, et al. ASCO 2015. Abstract 1003; 2. Bonnefoi H, et al. Ann Oncol. 2016;3. Gucalp A, et al. Clin
Cancer Res. 2013;19:5505-5512; 4..NCT01990209
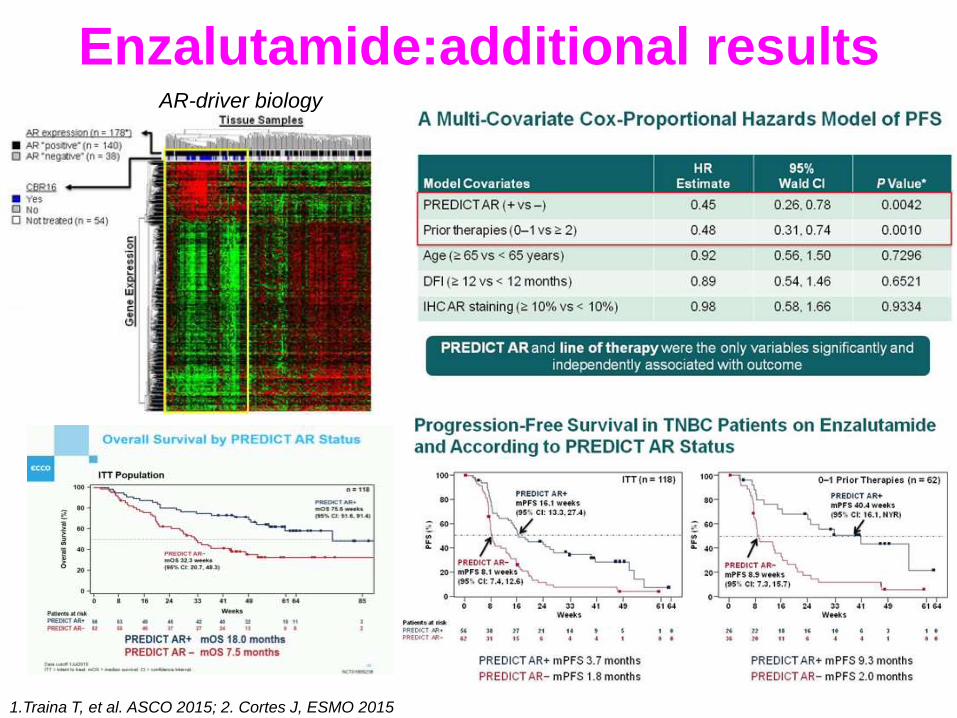
Enzalutamide:additional results AR-driver biology
1.Traina T, et al. ASCO 2015; 2. Cortes J, ESMO 2015
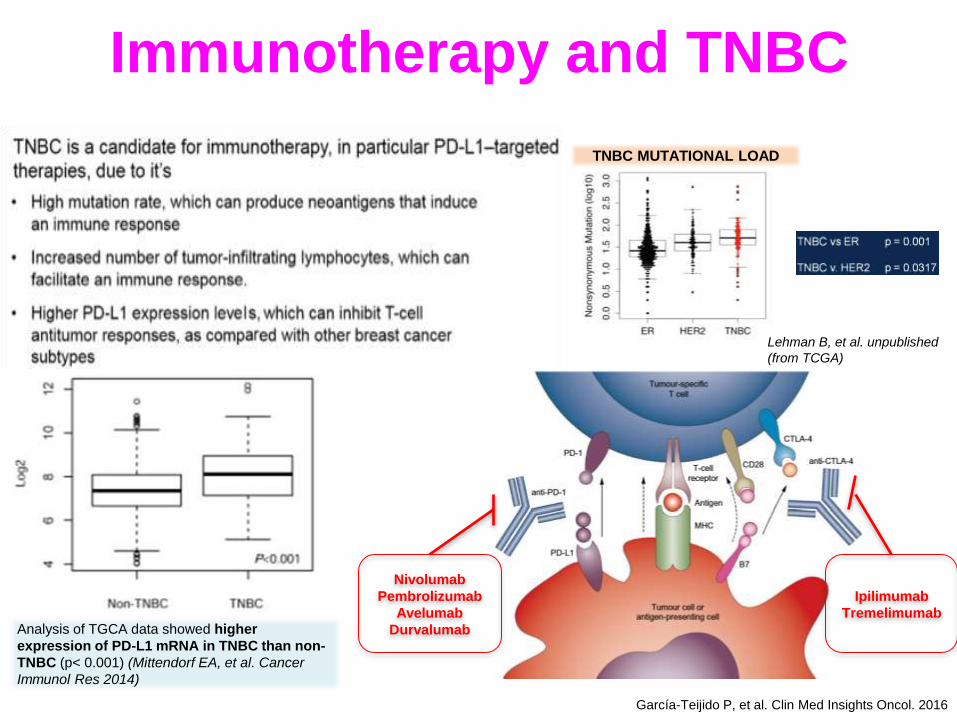
Immunotherapy and TNBC
Analysis of TGCA data showed higher
expression of PD-L1 mRNA in TNBC than non-
TNBC (p< 0.001) (Mittendorf EA, et al. Cancer
Immunol Res 2014)
Lehman B, et al. unpublished
(from TCGA)
TNBC MUTATIONAL LOAD
García-Teijido P, et al. Clin Med Insights Oncol. 2016
Nivolumab
Pembrolizumab
Avelumab
Durvalumab
Ipilimumab
Tremelimumab
Lehmann et al JCI 2011
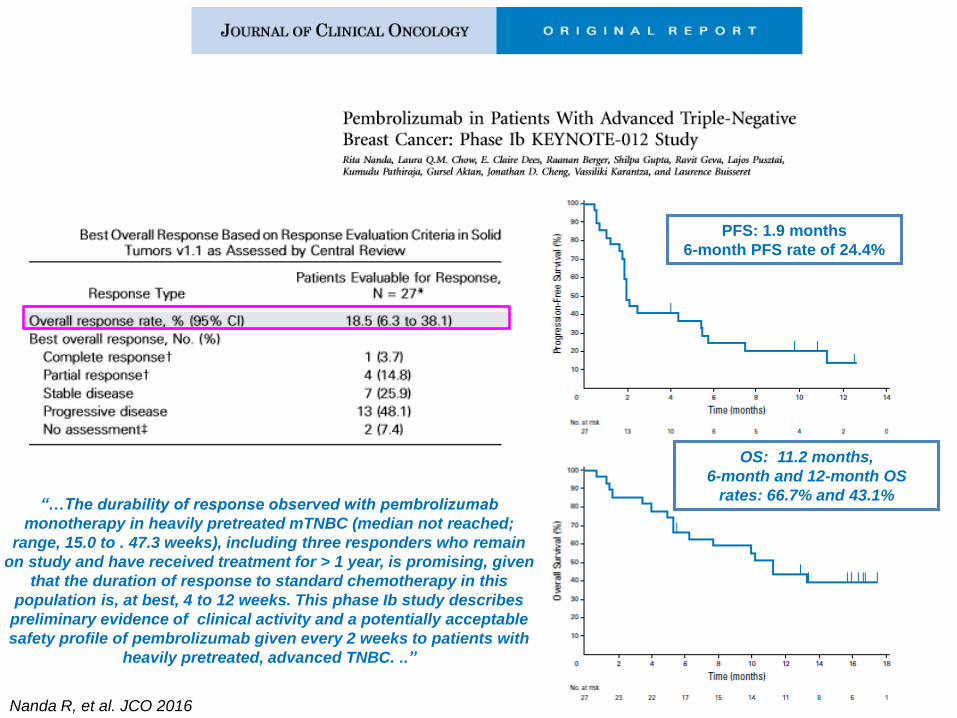
“…The durability of response observed with pembrolizumab
monotherapy in heavily pretreated mTNBC (median not reached;
range, 15.0 to . 47.3 weeks), including three responders who remain
on study and have received treatment for > 1 year, is promising, given
that the duration of response to standard chemotherapy in this
population is, at best, 4 to 12 weeks. This phase Ib study describes
preliminary evidence of clinical activity and a potentially acceptable
safety profile of pembrolizumab given every 2 weeks to patients with
heavily pretreated, advanced TNBC. ..”
PFS: 1.9 months
6-month PFS rate of 24.4%
OS: 11.2 months,
6-month and 12-month OS
rates: 66.7% and 43.1%
Nanda R, et al. JCO 2016

Atezolizumab + nab-paclitaxel in
TNBC: a phase Ib trial
Adams S, et al. ASCO 2016
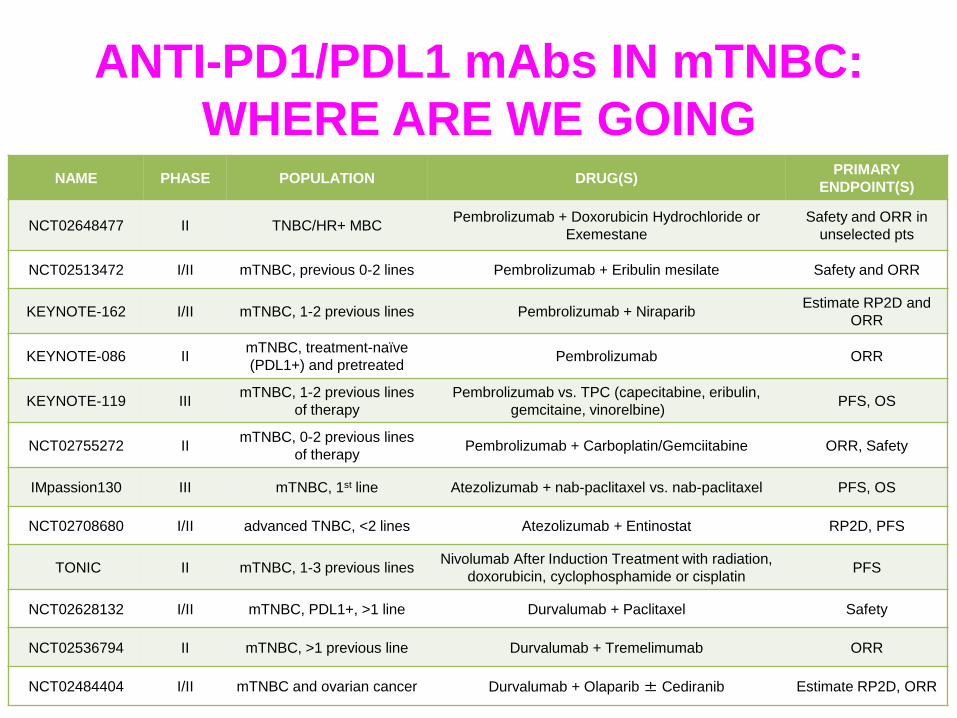
ANTI-PD1/PDL1 mAbs IN mTNBC:
WHERE ARE WE GOING NAME PHASE POPULATION DRUG(S)
PRIMARY
ENDPOINT(S)
NCT02648477 II TNBC/HR+ MBC Pembrolizumab + Doxorubicin Hydrochloride or
Exemestane
Safety and ORR in
unselected pts
NCT02513472 I/II mTNBC, previous 0-2 lines Pembrolizumab + Eribulin mesilate Safety and ORR
KEYNOTE-162 I/II mTNBC, 1-2 previous lines Pembrolizumab + Niraparib Estimate RP2D and
ORR
KEYNOTE-086 II mTNBC, treatment-naïve
(PDL1+) and pretreated Pembrolizumab ORR
KEYNOTE-119 III mTNBC, 1-2 previous lines
of therapy
Pembrolizumab vs. TPC (capecitabine, eribulin,
gemcitaine, vinorelbine) PFS, OS
NCT02755272 II mTNBC, 0-2 previous lines
of therapy Pembrolizumab + Carboplatin/Gemciitabine ORR, Safety
IMpassion130 III mTNBC, 1st line Atezolizumab + nab-paclitaxel vs. nab-paclitaxel PFS, OS
NCT02708680 I/II advanced TNBC, <2 lines Atezolizumab + Entinostat RP2D, PFS
TONIC II mTNBC, 1-3 previous lines Nivolumab After Induction Treatment with radiation,
doxorubicin, cyclophosphamide or cisplatin PFS
NCT02628132 I/II mTNBC, PDL1+, >1 line Durvalumab + Paclitaxel Safety
NCT02536794 II mTNBC, >1 previous line Durvalumab + Tremelimumab ORR
NCT02484404 I/II mTNBC and ovarian cancer Durvalumab + Olaparib ± Cediranib Estimate RP2D, ORR

LG AIOM Mammella 2015
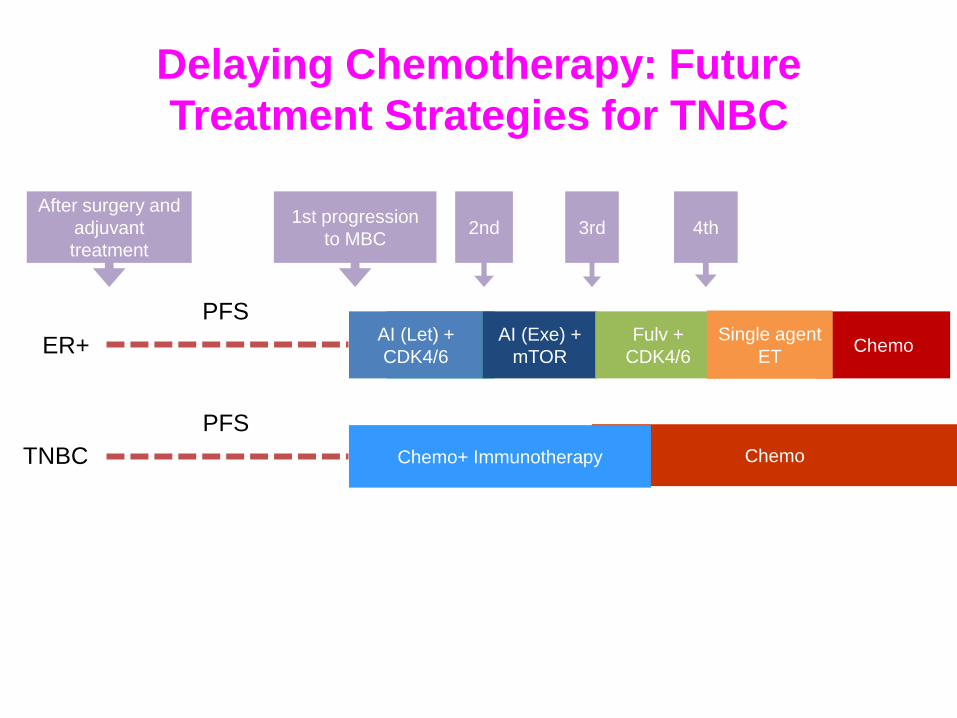
AI AI (Let) +
CDK4/6
AI (Exe) +
mTOR Chemo
Fulv +
CDK4/6
After surgery and
adjuvant
treatment
1st progression
to MBC 2nd 3rd 4th
ER+
TNBC
PFS
PFS
Single agent
ET
Chemo Chemo+ Immunotherapy
Delaying Chemotherapy: Future
Treatment Strategies for TNBC
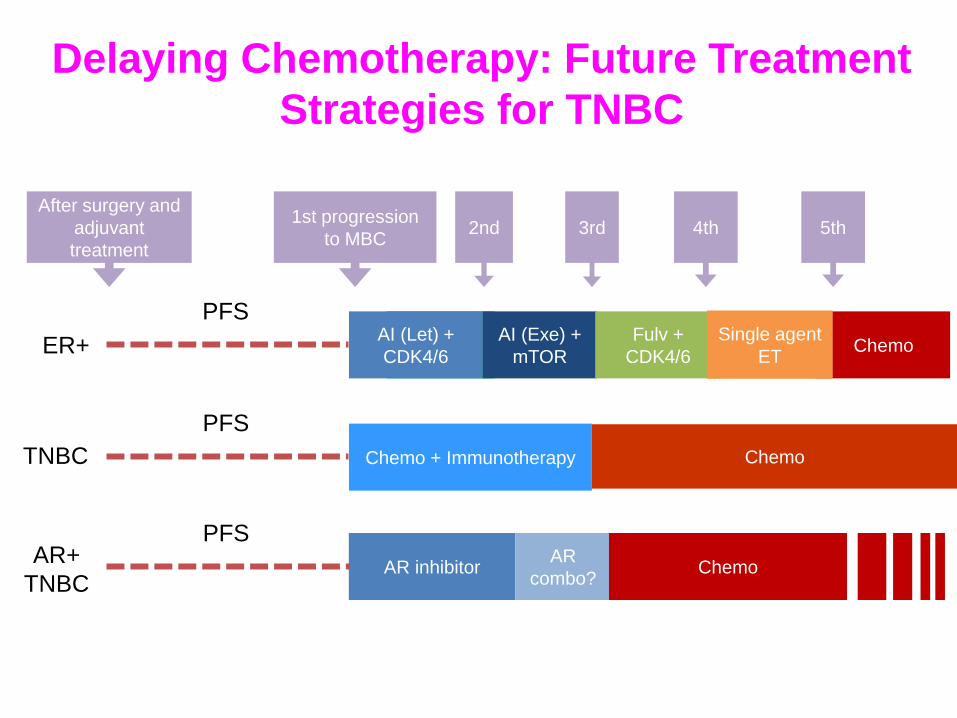
Delaying Chemotherapy: Future Treatment
Strategies for TNBC
AR inhibitor AR
combo? Chemo
AR+
TNBC
AI AI (Let) +
CDK4/6
AI (Exe) +
mTOR Chemo
Fulv +
CDK4/6 ER+
PFS Single agent
ET
5th
PFS
After surgery and
adjuvant
treatment
1st progression
to MBC 2nd 3rd 4th
TNBC
PFS
Chemo + Immunotherapy Chemo
OUTLINE
New insight in to HR-positive/HER2-negative MBC
Emerging Therapeutic options in HER2-positive MBC
Brain Metastases and HER2 disease
Triple Negative Breast Cancer
Others
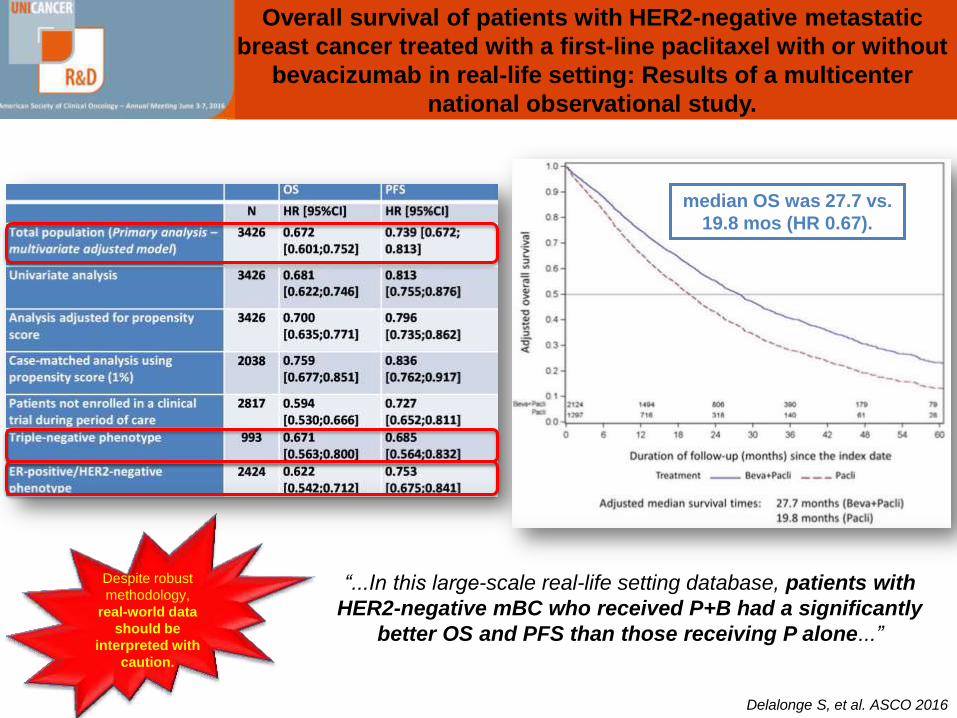
Overall survival of patients with HER2-negative metastatic
breast cancer treated with a first-line paclitaxel with or without
bevacizumab in real-life setting: Results of a multicenter
national observational study.
Delalonge S, et al. ASCO 2016
“...In this large-scale real-life setting database, patients with
HER2-negative mBC who received P+B had a significantly
better OS and PFS than those receiving P alone...”
median OS was 27.7 vs.
19.8 mos (HR 0.67).
Despite robust
methodology,
real-world data
should be
interpreted with
caution.
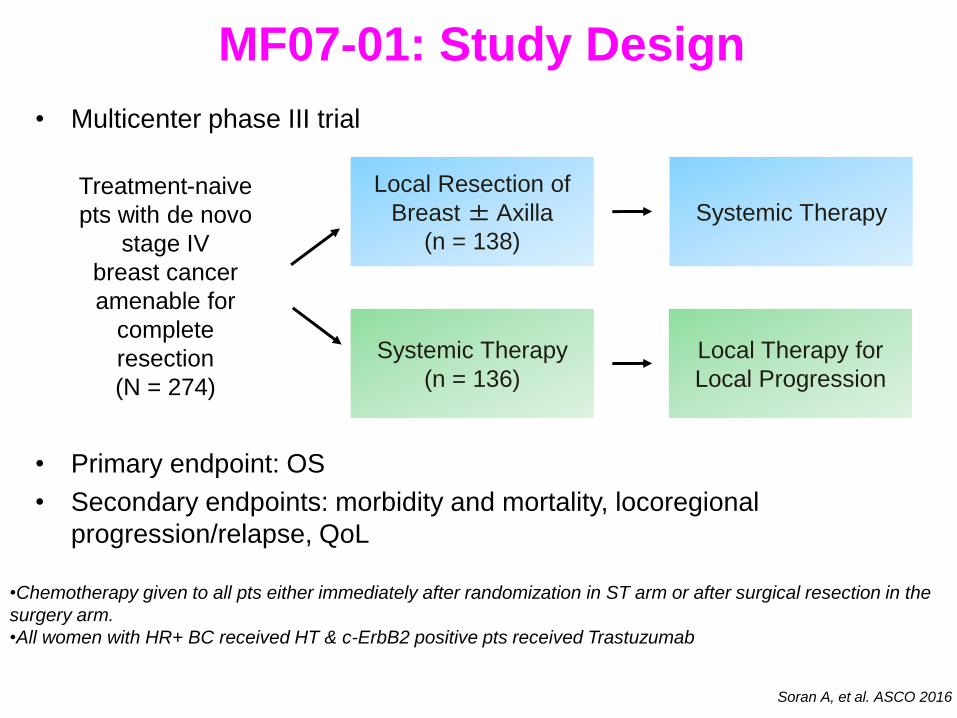
MF07-01: Study Design
• Multicenter phase III trial
• Primary endpoint: OS
• Secondary endpoints: morbidity and mortality, locoregional
progression/relapse, QoL
Treatment-naive
pts with de novo
stage IV
breast cancer
amenable for
complete
resection
(N = 274)
Local Resection of
Breast ± Axilla
(n = 138)
Systemic Therapy
(n = 136)
Local Therapy for
Local Progression
Systemic Therapy
•Chemotherapy given to all pts either immediately after randomization in ST arm or after surgical resection in the
surgery arm.
•All women with HR+ BC received HT & c-ErbB2 positive pts received Trastuzumab
Soran A, et al. ASCO 2016
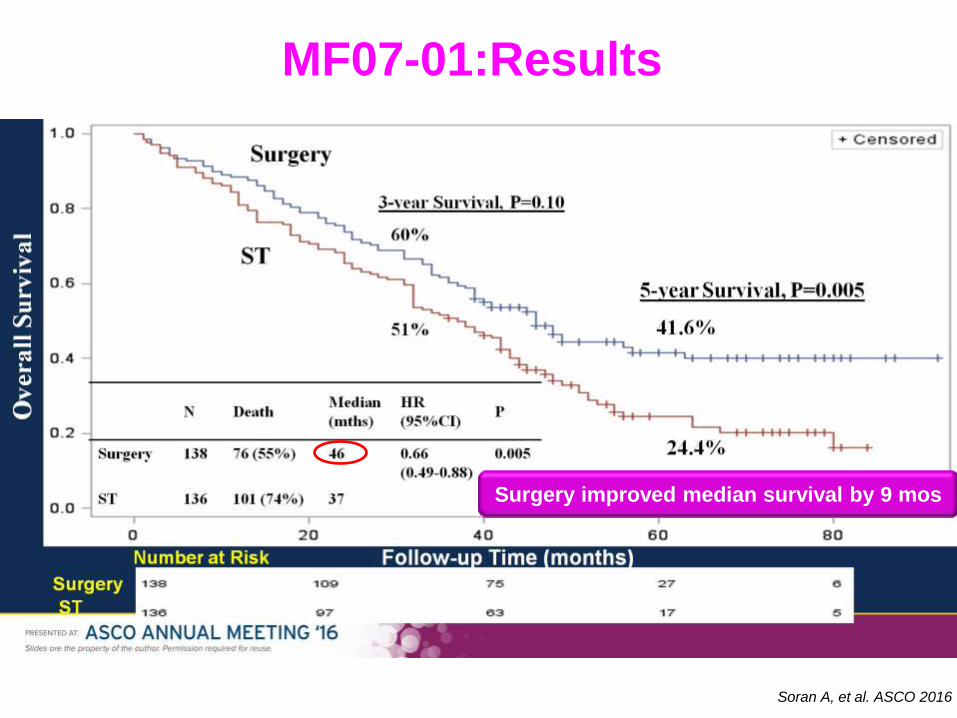
Slide 13
Surgery improved median survival by 9 mos
MF07-01:Results
Soran A, et al. ASCO 2016
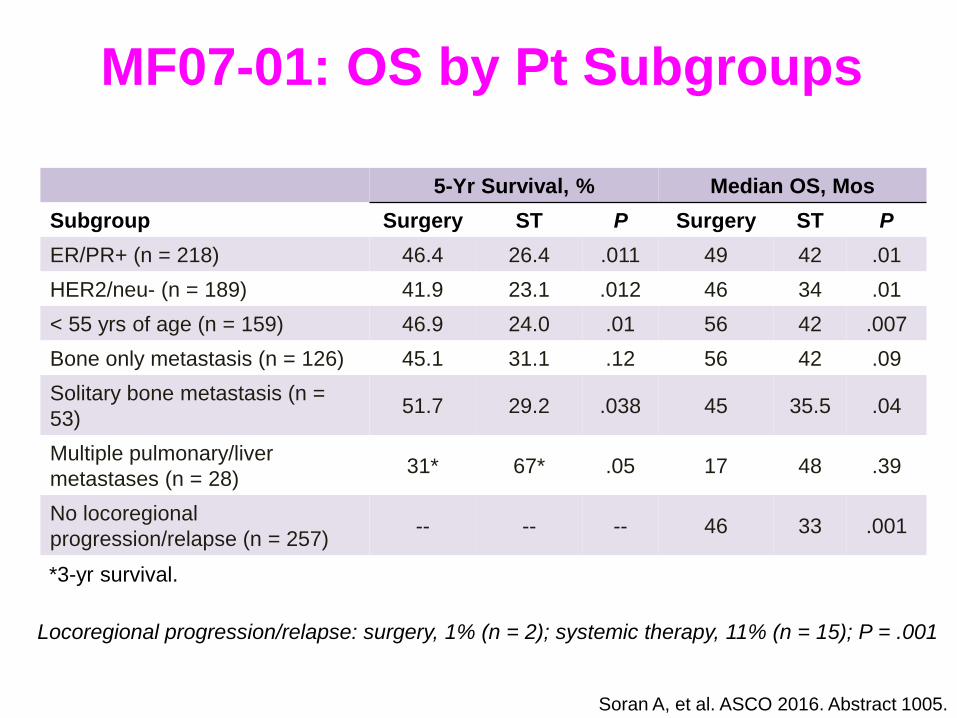
MF07-01: OS by Pt Subgroups
Locoregional progression/relapse: surgery, 1% (n = 2); systemic therapy, 11% (n = 15); P = .001
5-Yr Survival, % Median OS, Mos
Subgroup Surgery ST P Surgery ST P
ER/PR+ (n = 218) 46.4 26.4 .011 49 42 .01
HER2/neu- (n = 189) 41.9 23.1 .012 46 34 .01
< 55 yrs of age (n = 159) 46.9 24.0 .01 56 42 .007
Bone only metastasis (n = 126) 45.1 31.1 .12 56 42 .09
Solitary bone metastasis (n =
53) 51.7 29.2 .038 45 35.5 .04
Multiple pulmonary/liver
metastases (n = 28) 31* 67* .05 17 48 .39
No locoregional
progression/relapse (n = 257) -- -- -- 46 33 .001
Soran A, et al. ASCO 2016. Abstract 1005.
*3-yr survival.

LG AIOM Mammella 2015



Grazie!