Harmonization of contemporary-sensitive troponin I immunoassays: calibration may only be a part of...
7
Riv Ital Med Lab DOI 10.1007/s13631-014-0053-3 ARTICOLO ORIGINALE Harmonization of contemporary-sensitive troponin I immunoassays: calibration may only be a part of the problem Armonizzazione dei metodi contemporanei per la determinazione della troponina I: la calibrazione rappresenta solo una parte del problema Giuseppe Lippi · Gian Luca Salvagno · Giorgio Da Rin · Davide Giavarina Ricevuto: 4 dicembre 2013 / Accettato: 31 dicembre 2013 © Springer-Verlag Italia 2014 Summary Background. Standardization of cardiac tro- ponin I (cTnI) immunoassays remains an unmet target and comparability of current commercial methods is modest. We hence planned a study to investigate whether realignment of cTnI data by means of reference samples may improve comparability among different cTnI methods. Methods. Seventy six routine serum samples were collected in one center, centrifuged, aliquoted and shipped to partic- ipant centers, along with four additional reference serum samples with defined cTnI concentrations. The centers per- formed blind measurement of thawed aliquots and refer- ence samples using four widespread contemporary-sensitive immunoassays (Ortho-Clinical Diagnostics Vitros cTnI ES, Beckman Coulter DXI 800 AccuTnI, Siemens Healthcare Diagnostics Dimension Vista cTnI and Abbott Diagnostics Architect STAT cTnI). Test results were analyzed as pro- G. Lippi (B ) UO Diagnostica Ematochimica, Azienda Ospedaliero-Universitaria di Parma, Via Gramsci 14, 43126 Parma, Italy e-mail: [email protected] G. Lippi Laboratory of Clinical Chemistry and Hematology, Academic Hospital of Parma, Parma, Italy G.L. Salvagno Laboratory of Clinical Chemistry and Hematology, Academic Hospital of Verona, Verona, Italy G. Da Rin Service of Laboratory Medicine, Hospital of Bassano del Grappa, Bassano del Grappa (VI), Italy D. Giavarina Laboratory of Clinical Chemistry and Hematology, San Bortolo Hospital, Vicenza, Italy vided by the centers, and also after data alignment by means of polynomial regression parameters obtained on reference sera. Results. In five out of six circumstances the Deming fit im- proved after harmonization. The median inter-assay vari- ability increased from 22% to 53% after alignment with polynomial regression parameters. A reduction of bias was observed in half of the circumstances, whereas in the re- maining the bias increased. After harmonization, the agree- ment at diagnostic thresholds decreased in 4 out of 6 cir- cumstances. Conclusions. These results show that calibration may only be a minor contributor of inter-assay variability of commer- cial cTnI immunoassays. Harmonization by means of refer- ence sera was also counterproductive for improving meth- ods agreement around a diagnostic threshold. Keywords Myocardial infarction · Troponin · Immunoassays · Harmonization Riassunto Premesse. La standardizzazione del dosaggio della troponina cardiaca I (cTnI) rimane un obiettivo irri- solto e la confrontabilità dei metodi commerciali contempo- ranei è modesta. È stato quindi pianificato uno studio per ve- rificare se il riallineamento dei risultati mediante campioni di riferimento può migliorare la confrontabilità tra i diversi metodi. Metodi. Settantasei campioni di siero sono stati raccolti in un unico centro, centrifugati, aliquotati e spediti agli altri centri partecipanti, insieme a quattro campioni di siero di riferimento con concentrazioni note di cTnI. I centri hanno eseguito la determinazione in cieco delle aliquote scongela- te e dei campioni di riferimento, utilizzando quattro tra i più diffusi metodi immunochimici contemporanei per la deter- minazione di cTnI (Ortho-Clinical Diagnostics Vitros cTnI
Transcript of Harmonization of contemporary-sensitive troponin I immunoassays: calibration may only be a part of...

Riv Ital Med LabDOI 10.1007/s13631-014-0053-3
A RT I C O L O O R I G I NA L E
Harmonization of contemporary-sensitive troponin Iimmunoassays: calibration may only be a part of the problem
Armonizzazione dei metodi contemporanei per la determinazione dellatroponina I: la calibrazione rappresenta solo una parte del problema
Giuseppe Lippi · Gian Luca Salvagno · Giorgio Da Rin ·Davide Giavarina
Ricevuto: 4 dicembre 2013 / Accettato: 31 dicembre 2013© Springer-Verlag Italia 2014
Summary Background. Standardization of cardiac tro-ponin I (cTnI) immunoassays remains an unmet target andcomparability of current commercial methods is modest. Wehence planned a study to investigate whether realignmentof cTnI data by means of reference samples may improvecomparability among different cTnI methods.Methods. Seventy six routine serum samples were collectedin one center, centrifuged, aliquoted and shipped to partic-ipant centers, along with four additional reference serumsamples with defined cTnI concentrations. The centers per-formed blind measurement of thawed aliquots and refer-ence samples using four widespread contemporary-sensitiveimmunoassays (Ortho-Clinical Diagnostics Vitros cTnI ES,Beckman Coulter DXI 800 AccuTnI, Siemens HealthcareDiagnostics Dimension Vista cTnI and Abbott DiagnosticsArchitect STAT cTnI). Test results were analyzed as pro-
G. Lippi (B)UO Diagnostica Ematochimica, AziendaOspedaliero-Universitaria di Parma, Via Gramsci 14,43126 Parma, Italye-mail: [email protected]
G. LippiLaboratory of Clinical Chemistry and Hematology, AcademicHospital of Parma, Parma, Italy
G.L. SalvagnoLaboratory of Clinical Chemistry and Hematology, AcademicHospital of Verona, Verona, Italy
G. Da RinService of Laboratory Medicine, Hospital of Bassano del Grappa,Bassano del Grappa (VI), Italy
D. GiavarinaLaboratory of Clinical Chemistry and Hematology, San BortoloHospital, Vicenza, Italy
vided by the centers, and also after data alignment by meansof polynomial regression parameters obtained on referencesera.Results. In five out of six circumstances the Deming fit im-proved after harmonization. The median inter-assay vari-ability increased from 22% to 53% after alignment withpolynomial regression parameters. A reduction of bias wasobserved in half of the circumstances, whereas in the re-maining the bias increased. After harmonization, the agree-ment at diagnostic thresholds decreased in 4 out of 6 cir-cumstances.Conclusions. These results show that calibration may onlybe a minor contributor of inter-assay variability of commer-cial cTnI immunoassays. Harmonization by means of refer-ence sera was also counterproductive for improving meth-ods agreement around a diagnostic threshold.
Keywords Myocardial infarction · Troponin ·Immunoassays · Harmonization
Riassunto Premesse. La standardizzazione del dosaggiodella troponina cardiaca I (cTnI) rimane un obiettivo irri-solto e la confrontabilità dei metodi commerciali contempo-ranei è modesta. È stato quindi pianificato uno studio per ve-rificare se il riallineamento dei risultati mediante campionidi riferimento può migliorare la confrontabilità tra i diversimetodi.Metodi. Settantasei campioni di siero sono stati raccolti inun unico centro, centrifugati, aliquotati e spediti agli altricentri partecipanti, insieme a quattro campioni di siero diriferimento con concentrazioni note di cTnI. I centri hannoeseguito la determinazione in cieco delle aliquote scongela-te e dei campioni di riferimento, utilizzando quattro tra i piùdiffusi metodi immunochimici contemporanei per la deter-minazione di cTnI (Ortho-Clinical Diagnostics Vitros cTnI

Riv Ital Med Lab
ES, Beckman Coulter DXI 800 AccuTnI, Siemens Healthca-re Diagnostics Dimension Vista cTnI ed Abbott DiagnosticsArchitect STAT cTnI). I risultati sono stati analizzati primae dopo riallineamento con parametri ottenuti da regressionipolinomiali sui valori dei sieri di riferimento.Risultati. In cinque circostanze su sei i parametri della re-gressione di Deming sono migliorati dopo armonizzazione.La variabilità tra i diversi metodi è però aumentata da 22%a 53% dopo allineamento mediante parametri delle regres-sioni polinomiali. Una riduzione del bias è stata ottenutasolo nella metà delle circostanze, mentre nelle rimanenti ilbias è aumentato. Dopo armonizzazione, la concordanza allasoglia diagnostica è diminuita in 4 circostanze su 6.Conclusioni. I risultati ottenuti in questo studio dimostranoche la calibrazione sembra rappresentare solo un parte del-la variabilità nei risultati ottenibili con metodi commercialicontemporanei per la determinazione di cTnI. Paradossal-mente, l’armonizzazione mediante sieri di riferimento ha de-terminato una peggiore concordanza dei valori in relazionealla soglia diagnostica.
Parole chiave Infarto del miocardio · Troponina · MetodiImmunochimici · Armonizzazione
Introduction
Ischemic heart disease is the worldwide leading cause ofdeath and disability [1]. Several efforts have been made inthe past decades for improving the diagnostic approach ofpatients with acute myocardial infarction (AMI), which haveled to the identification of cardiospecific troponins (cTns) asthe biochemical gold standards for identifying cardiac in-jury. The measurements of cTn has hence become the main-stay for diagnosing an episode of AMI, especially of nonST-elevation MI (NSTEMI) [2, 3].
The commercial availability of a single method for mea-suring cardiac troponin T (cTnT) does not pose major prob-lems of standardization, rather understandably [4]. There areinstead several biological and analytical issues that chal-lenge the harmonization of the various cardiac troponinI (cTnI) immunoassays existing on the market. cTnI is ahighly heterogeneous protein, physiologically bound to thetroponin complex which also include cTnT and troponin C(TnC). The free soluble pool of cTnI is typically low, usu-ally lower than 6% of the total intracellular content [5].During ischemic myocardiocyte injury, increased produc-tion of reactive oxygen species and active release of pro-teases (especially from leukocytes) occur, both events pro-moting a complex series of degradation processes of thewhole troponin complex and of the single protein moieties.When the cTns are released into the circulation as a result of
plasma membrane injury, additional modifications may oc-cur, including oxidation, reduction, phosphorylation, furtherdegradation and fragmentations by proteases in blood [6].All these events involve different epitopes on the proteinsand may hence generate a heterogeneous impairment of theimmunoreactivity according to the specific targets of the an-tibodies in the various immunoassays. An additional sourceof bias is represented by the differential renal clearance ofcomplexes and protein fragments generated upon myocar-diocyte injury, which may contain different epitopes andmay hence generate heterogeneous and time-dependent im-munoreactive responses [6].
As regards a genuine analytical perspective, the lead-ing issue that challenge the standardization of cTnI is rep-resented by the use of different cocktails of antibodies indifferent immunoassays. Despite the well known recom-mendation of the IFCC Working Group on Standardizationof Troponin I to select antibodies that should specificallyreact with the more stable domains of the molecule [7],the different commercial methods contain a heterogeneousmix of antibodies, with only partial overlap as recently de-scribed by Apple et al [8]. The lack of a reference materialis another important drawback. Several efforts have beenmade over the past decade, culminated in the generationof SRM 2921, i.e., a native cTnICT ternary complex [9].Unfortunately, this serum-based reference material encoun-tered several problems of stability and its use was provento be mostly unsuitable with commercial methods [10]. Thelack of a reference method is another important drawback,which may hamper the generation of secondary referencematerials even if the primary standard had become avail-able [10].
Despite these important issues, harmonization of cTnIimmunoassay remains a foremost target for laboratorymedicine. Cardiology units and cath labs are increasinglyorganized according to a typical “hub and spoke” model,where optimal patient management is coordinated withinregional myocardial infarction networks [11, 12]. It is henceclear that all clinical laboratories included in a regionalnetwork should harmonize measurements, in order to al-low serial monitoring of patients, as currently advocatedby all national and supranational guidelines [1–3]. Sev-eral lines of evidence attest, however, that this remainsan unmet target and that the comparability of the currentcommercial cTnI methods is modest, at best. In particu-lar, we recently showed that a significant bias still existsamong contemporary-sensitive cTnI immunoassays, whichhas been mostly attributed to random variation of data, thatwould finally make the objective of harmonization a virtu-ally unreachable perspective [13]. To provide further sup-port to the hypothesis that harmonization of contemporary-sensitive cTnI immunoassays cannot be simply achieved byusing reference materials, we carried out a specific study to

Riv Ital Med Lab
Table 1 Deming fit amongcTnI methods before (roundbrackets) and after (squarebrackets) data alignment withpolynomial regressionparameters
cTnI, cardiac troponin I
DXI 800 AccuTnI Dimension Vista cTnI Architect STAT cTnI
Vitros cTnI ES (y = 1.05x + 0.01)
[y = 1.02x + 0.03](y = 1.33x − 0.01)
[y = 0.97x + 0.04](y = 0.97x + 0.05)
[y = 1.05x + 0.05]DXI 800 AccuTnI – (y = 1.27x − 0.02)
[y = 0.96x + 0.02](y = 0.92x + 0.05)
[y = 1.03x + 0.02]Dimension Vista cTnI – – (y = 0.73x + 0.06)
[y = 1.08x]
investigate whether or not the realignment of data by meansof reference samples may improve comparability among dif-ferent cTnI methods.
Materials and methods
Sample collection and shipment
Sample collection was centralized in one center (i.e., Aca-demic Hospital of Verona, Italy) and consisted in all serumspecimens referred to the stat section of the laboratory witha urgent request for troponin testing over an entire work-ing day. All samples were separated by centrifugation ac-cording to local procedures and then divided 5 in aliquotsof 0.5 mL each. A first aliquot was employed for rou-tine assessment of cardiospecific troponin according to thetest request, whereas the remaining four were immediatelyfrozen at −70 °C. After one week of storage, the aliquotswere conveyed to the other centers, with strict observationof transportation requirements (i.e., controlled conditionsof temperature and humidity). The mean time of sampletransportation to the laboratories was 85 min (range: 61–109 min). The aliquots were kept stored at −70 °C until allcenters had received the shipment, in order to allow simulta-neous testing. Before starting the analyses, the aliquots wereleft to thaw at room temperature and were then centrifuged.Four additional reference serum samples with cTnI concen-trations of 0.01, 0.05, 0.93 and 4.34 µg/L (values obtained induplicate with Vitros cTnI ES, Ortho-Clinical Diagnostics,Rochester, NY, USA), were prepared exactly as the routinespecimens and included in the shipment.
Sample analysis
The participant centers were asked to perform a blind mea-surement of thawed aliquots and reference samples, and pro-vide results to the reference center. This study included fourwidespread contemporary-sensitive immunoassays, sincethe delayed commercial availability of high-sensitivity cTnIimmunoassays on the European market still makes these
method virtually unavailable to routine clinical laboratories.The reference center (Parma) used Vitros cTnI ES [limit ofdetection (LOD): 0.003 µg/L; value with 10% coefficient ofvariation (CV): 0.028 µg/L; 99th percentile of the upper ref-erence limit (URL): 0.021 µg/L] [14], and DXI 800 AccuTnI(Beckman Coulter, Brea CA, USA; LOD: 0.011 µg/L; valuewith 10% CV: 0.058 µg/L; 99th percentile URL: 0.034 µg/L)[15]. Other two centers (Vicenza and Bassano del Grappa)used respectively Dimension Vista cTnI (Siemens Health-care Diagnostics, Tarrytown, NY, USA; LOD: 0.015 µg/L;value with 10% CV: 0.036 µg/L; 99th percentile URL:0.022 µg/L) [16], and Architect STAT cTnI (Abbott Diag-nostics, Lake Forest, IL, USA; LOD: 0.010 µg/L; value with10% CV: 0.076 µg/L; 99th percentile URL: 0.020 µg/L)[17].
Statistical analysis
Data obtained with the four cTnI contemporary-sensitive as-says were analyzed as provided by the centers, and also afterharmonization. In brief, the data obtained on four referenceserum samples were used for comparing results between anarbitrary reference assay (Vitros cTnI ES) with those ob-tained with the other three methods. Specifically, the arbi-trary reference method was used for alignment by servingas the abscissa in polynomial analysis for regressing sam-ple 1 through 4 results with each of the other three cTnIsystems, which served as respective ordinate values, as sug-gested by Christenson et al [18]. The coefficients of the poly-nomial curves were then used to realign the original valuesobtained with DXI 800 AccuTnI, Dimension Vista cTnI andArchitect STAT cTnI, and the relative cut-off values werealso realigned to a common threshold (i.e., that of the arbi-trary reference method; 0.021 µg/L). The statistical analysiswas then performed using Analyse-it for Microsoft Excel(Analyse-it Software Ltd, Leeds, UK), and included Dem-ing fit, Bland & Altman plots (with t-statistics) and kappaagreement. Since this study used pre-existing samples andresults did not change the clinical management, ethical per-mission and informed consent were unnecessary accordingto our local ethical committee. The study was however per-

Riv Ital Med Lab
Fig. 1 Bland & Altman Plots of values obtained with Vitros cTnI ES, DXI 800 AccuTnI, Dimension Vista cTnI and Architect STAT cTnI, beforedata alignment with polynomial regression parameters
formed in accordance with the Declaration of Helsinki andunder the terms of all relevant local legislations.
Results
Seventy six samples were collected throughout the studyperiod and finally included in this experimental investiga-tion. The polynomial curves generated by data correlation
of reference sera obtained with the arbitrary reference as-say (Vitros cTnI ES) and the other three methods (DXI 800AccuTnI, Dimension Vista cTnI and Architect STAT cTnI),generated the following equations (r = 1.00 for all):
◦ Vitros cTnI ES = −0.054∗[DXI 800 AccuTnI]2 +1.22∗[DXI 800 AccuTnI] − 0.001;
◦ Vitros cTnI ES = −0.068∗[Dimension Vista cTnI]2 +1.13∗[Dimension Vista cTnI] + 0.006;

Riv Ital Med Lab
Fig. 2 Bland & Altman Plots of values obtained with Vitros cTnI ES, DXI 800 AccuTnI, Dimension Vista cTnI and Architect STAT cTnI, afterdata alignment with polynomial regression parameters
◦ Vitros cTnI ES = 0.011∗[Architect STAT cTnI]2 +1.034∗[Architect STAT cTnI] − 0.003.
The Deming fit among values of routine samples ob-tained with the four cTnI methods, before and after harmo-nization, is shown in Table 1. As predictable, in five out ofsix circumstances method comparison improved after dataadjustment. The original median inter-assay variability (i.e.,CV) was 22.2% (IQR, 22.0–59.9%), but further increased to
52.9% (IQR, 2.3–57.0%) after alignment with polynomialregression parameters. The absolute bias among methods,before (Fig. 1) and after harmonization (Fig. 2), is shownin Table 2. Interestingly, a reduction of bias was observedin half of the circumstances, whereas in the remaining halfthe absolute value of the bias among methods paradoxi-cally increased. The agreement of methods at the diagnosticthresholds is shown in Table 3. In only two out of six cir-
Riv Ital Med Lab
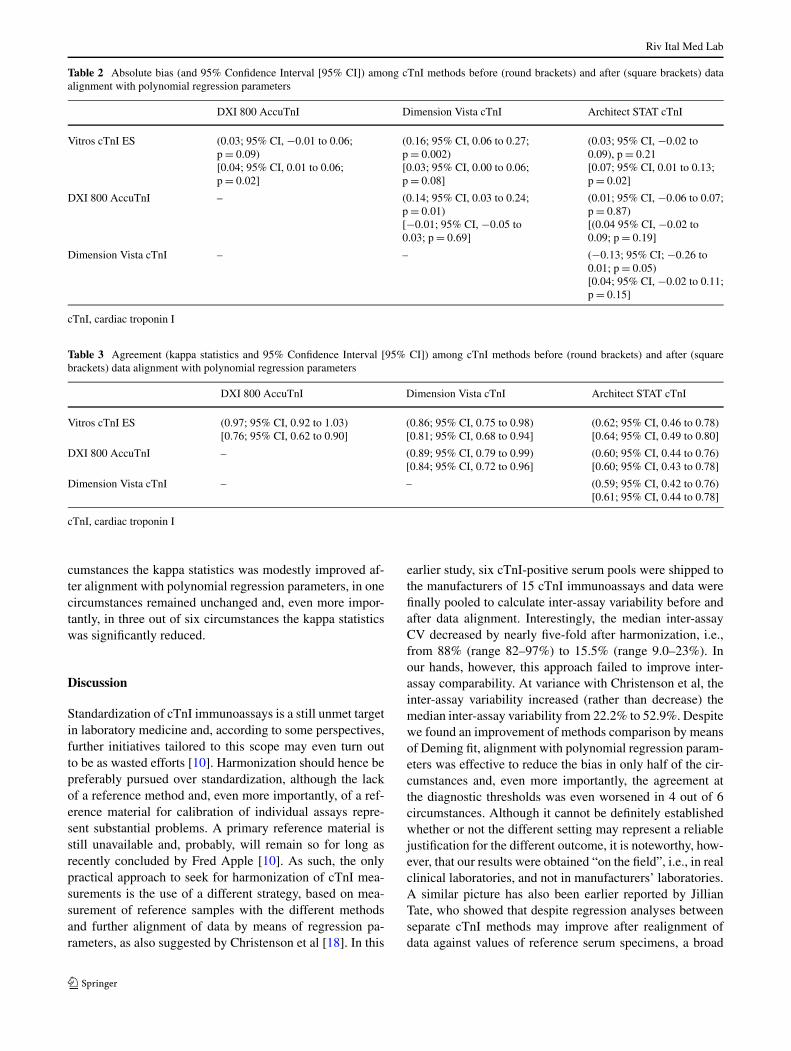
Table 2 Absolute bias (and 95% Confidence Interval [95% CI]) among cTnI methods before (round brackets) and after (square brackets) dataalignment with polynomial regression parameters
DXI 800 AccuTnI Dimension Vista cTnI Architect STAT cTnI
Vitros cTnI ES (0.03; 95% CI, −0.01 to 0.06;p = 0.09)[0.04; 95% CI, 0.01 to 0.06;p = 0.02]
(0.16; 95% CI, 0.06 to 0.27;p = 0.002)[0.03; 95% CI, 0.00 to 0.06;p = 0.08]
(0.03; 95% CI, −0.02 to0.09), p = 0.21[0.07; 95% CI, 0.01 to 0.13;p = 0.02]
DXI 800 AccuTnI – (0.14; 95% CI, 0.03 to 0.24;p = 0.01)[−0.01; 95% CI, −0.05 to0.03; p = 0.69]
(0.01; 95% CI, −0.06 to 0.07;p = 0.87)[(0.04 95% CI, −0.02 to0.09; p = 0.19]
Dimension Vista cTnI – – (−0.13; 95% CI; −0.26 to0.01; p = 0.05)[0.04; 95% CI, −0.02 to 0.11;p = 0.15]
cTnI, cardiac troponin I
Table 3 Agreement (kappa statistics and 95% Confidence Interval [95% CI]) among cTnI methods before (round brackets) and after (squarebrackets) data alignment with polynomial regression parameters
DXI 800 AccuTnI Dimension Vista cTnI Architect STAT cTnI
Vitros cTnI ES (0.97; 95% CI, 0.92 to 1.03)[0.76; 95% CI, 0.62 to 0.90]
(0.86; 95% CI, 0.75 to 0.98)[0.81; 95% CI, 0.68 to 0.94]
(0.62; 95% CI, 0.46 to 0.78)[0.64; 95% CI, 0.49 to 0.80]
DXI 800 AccuTnI – (0.89; 95% CI, 0.79 to 0.99)[0.84; 95% CI, 0.72 to 0.96]
(0.60; 95% CI, 0.44 to 0.76)[0.60; 95% CI, 0.43 to 0.78]
Dimension Vista cTnI – – (0.59; 95% CI, 0.42 to 0.76)[0.61; 95% CI, 0.44 to 0.78]
cTnI, cardiac troponin I
cumstances the kappa statistics was modestly improved af-ter alignment with polynomial regression parameters, in onecircumstances remained unchanged and, even more impor-tantly, in three out of six circumstances the kappa statisticswas significantly reduced.
Discussion
Standardization of cTnI immunoassays is a still unmet targetin laboratory medicine and, according to some perspectives,further initiatives tailored to this scope may even turn outto be as wasted efforts [10]. Harmonization should hence bepreferably pursued over standardization, although the lackof a reference method and, even more importantly, of a ref-erence material for calibration of individual assays repre-sent substantial problems. A primary reference material isstill unavailable and, probably, will remain so for long asrecently concluded by Fred Apple [10]. As such, the onlypractical approach to seek for harmonization of cTnI mea-surements is the use of a different strategy, based on mea-surement of reference samples with the different methodsand further alignment of data by means of regression pa-rameters, as also suggested by Christenson et al [18]. In this
earlier study, six cTnI-positive serum pools were shipped tothe manufacturers of 15 cTnI immunoassays and data werefinally pooled to calculate inter-assay variability before andafter data alignment. Interestingly, the median inter-assayCV decreased by nearly five-fold after harmonization, i.e.,from 88% (range 82–97%) to 15.5% (range 9.0–23%). Inour hands, however, this approach failed to improve inter-assay comparability. At variance with Christenson et al, theinter-assay variability increased (rather than decrease) themedian inter-assay variability from 22.2% to 52.9%. Despitewe found an improvement of methods comparison by meansof Deming fit, alignment with polynomial regression param-eters was effective to reduce the bias in only half of the cir-cumstances and, even more importantly, the agreement atthe diagnostic thresholds was even worsened in 4 out of 6circumstances. Although it cannot be definitely establishedwhether or not the different setting may represent a reliablejustification for the different outcome, it is noteworthy, how-ever, that our results were obtained “on the field”, i.e., in realclinical laboratories, and not in manufacturers’ laboratories.A similar picture has also been earlier reported by JillianTate, who showed that despite regression analyses betweenseparate cTnI methods may improve after realignment ofdata against values of reference serum specimens, a broad

Riv Ital Med Lab
heterogeneity of inter-assay variation was still present, withsome patient samples displaying CV of 55% or greater, abias which was ultimately attributed to method differencesin immunoreactivity [19].
We believe that our results may have some meaningfulimplications. First, it seems reasonable to conclude that cal-ibration may only be a (minor) contributor of inter-assayvariability of cTnI, whereas the largest part of the bias maybe attributable to the peculiar cocktails of antibodies thatspecifically characterize the different methods. In the caseof our study, in fact, there was a large heterogeneity of cap-ture (C) and detection (D) monoclonal antibodies across thedifferent methods (i.e., C: 24–40 and 41–49, D: 87–91 forVitros cTnI ES; C: 41–49; D: 24–40 for DXI 800 AccuTnI,C: 27–32; D: 41–56 for Dimension Vista cTnI, and C: 87–91and 24–40; D: 41–49 for Architect STAT cTnI [8]. In a worldof limited resources, where selection of cTnI immunoas-says may be influenced by a variety of extra-analytical as-pects (cost, laboratory automation, organization, among oth-ers) [20], this represents indeed a substantial problem. Inan era where recombinant standards are increasingly beingproduced and validated in tandem with certified immunoas-says [21, 22], it is not so unrealistic to advocate that thein vitro diagnostic companies may use common recombi-nant peptides to develop their next generation cTnI mono-clonal antibodies, directed against identical epitopes on themolecule. The IFCC Working Group on Standardization ofTroponin I has already identified those protein moieties thatare more suitable to be targeted [7]. A second important im-plication of this study is the evidence that harmonization notonly was unproductive to enhance the agreement of methodsaround a diagnostic threshold but, paradoxically, this strat-egy even reduced the accordance. This can be probably in-terpreted as a consequence of the large efforts placed by invitro diagnostic companies on alignment of individual cTnIimmunoassays over recent years, in spite of persisting lackof reference material and reference methods.
Conflict of interest None.
References
1. Lippi G, Franchini M, Cervellin G (2013) Diagnosis and manage-ment of ischemic heart disease. Semin Thromb Hemost 39:202–213
2. Lackner KJ (2013) Laboratory diagnostics of myocardialinfarction—troponins and beyond. Clin Chem Lab Med 51:83–89
3. Casagranda I, Cavazza M, Clerico A et al (2013) Proposal forthe use in emergency departments of cardiac troponins measured
with the latest generation methods in patients with suspected acutecoronary syndrome without persistent ST-segment elevation. ClinChem Lab Med 51:1727–1737
4. Franzini M, Masotti S, Prontera C et al (2014) Clinical implica-tions of a recent adjustment to the high-sensitivity cardiac troponinT assay: some results. Clin Chem Lab Med 52:e21–e23
5. Lippi G, Targher G, Franchini M, Plebani M (2009) Genetic andbiochemical heterogeneity of cardiac troponins: clinical and labo-ratory implications. Clin Chem Lab Med 47:1183–1194
6. Lippi G, Cervellin G (2012) Degradation of troponin I in serumor plasma: mechanisms, and analytical and clinical implications.Semin Thromb Hemost 38:222–229
7. Panteghini M, Bunk DM, Christenson RH et al, IFCC Work-ing Group on Standardization of Troponin I (2008) Standardiza-tion of troponin I measurements: an update. Clin Chem Lab Med46:1501–1506
8. Apple FS, Ler R, Murakami MM (2012) Determination of 19 car-diac troponin I and T assay 99th percentile values from a commonpresumably healthy population. Clin Chem 58:1574–1581
9. He HJ, Lowenthal MS, Cole KD et al (2011) An immunoprecipita-tion coupled with fluorescent Western blot analysis for the charac-terization of a model secondary serum cardiac troponin I referencematerial. Clin Chim Acta 412:107–111
10. Apple FS (2012) Counterpoint: standardization of cardiac tro-ponin I assays will not occur in my lifetime. Clin Chem 58:169–171
11. Nobilio L, Ugolini C (2003) Selective referrals in a ‘hub andspoke’ institutional setting: the case of coronary angioplasty pro-cedures. Health Policy 63:95–107
12. Birkemeyer R, Dauch A, Müller A et al (2013) Short term costeffectiveness of a regional myocardial infarction network. HealthEcon Rev 3:10
13. Salvagno GL, Giavarina D, Meneghello M et al (2014) Mul-ticenter comparison of four contemporary-sensitive troponinimmunoassays. Journal of Medical Biochemistry. doi:10.2478/jomb-2014-0015
14. Zaninotto M, Vernocchi A, Di Serio F et al (2012) Assay perfor-mance improved, but which “scorecard” designation for vitros tro-ponin I? Clin Chim Acta 413:826–828
15. Zaninotto M, Mion MM, Novello E et al (2009) Precision per-formance at low levels and 99th percentile concentration of theaccess AccuTnl assay on two different platforms. Clin Chem LabMed 47:367–371
16. Arrebola MM, Lillo JA, Diez De Los Ríos MJ et al (2010) Ana-lytical performance of a sensitive assay for cardiac troponin I withloci technology. Clin Biochem 43:998–1002
17. La’ulu SL, Roberts WL (2010) Performance characteristics of fivecardiac troponin I assays. Clin Chim Acta 411:1095–1101
18. Christenson RH, Duh SH, Apple FS et al (2006) Toward standard-ization of cardiac troponin I measurements part II: assessing com-mutability of candidate reference materials and harmonization ofcardiac troponin I assays. Clin Chem 52:1685–1692
19. Tate JR (2008) Troponin revisited 2008: assay performance. ClinChem Lab Med 46:1489–1500
20. Lippi G, Cervellin G (2013) Choosing troponin immunoassays ina world of limited resources. J Am Coll Cardiol 62:647–648
21. Bidlingmaier M (2008) Problems with GH assays and strategiestoward standardization. Eur J Endocrinol 159(Suppl 1):S41–S44
22. Chapman MD, Briza P (2012) Molecular approaches to allergenstandardization. Curr Allergy Asthma Rep 12:478–484