«Focus on: La Sincope» - Home Page - Sito AcEMC 2017/Ungar.pdf · recommended by 2009 ESC...
75
«Focus on: La Sincope» (in attesa delle linee guida ESC 2018) Syncope Unit. Geriatria e Terapia Intensiva Geriatrica Università degli Studi di Firenze e Azienda Ospedaliero Universitaria Careggi - Firenze Andrea Ungar, MD, PhD, FESC
Transcript of «Focus on: La Sincope» - Home Page - Sito AcEMC 2017/Ungar.pdf · recommended by 2009 ESC...
«Focus on: La Sincope»(in attesa delle linee guida ESC 2018)
Syncope Unit. Geriatria e Terapia Intensiva Geriatrica
Università degli Studi di Firenze e Azienda Ospedaliero Universitaria Careggi - Firenze
Andrea Ungar, MD, PhD, FESC
«La Sincope»
Definizione e fisiopatologia
Definizione
La sincope è una perdita di coscienza transitoria dovuta ad ipoperfusione cerebrale globale, caratterizzata da
rapida insorgenza, breve durata,
recupero completo e spontaneo
2009 ESC guidelines
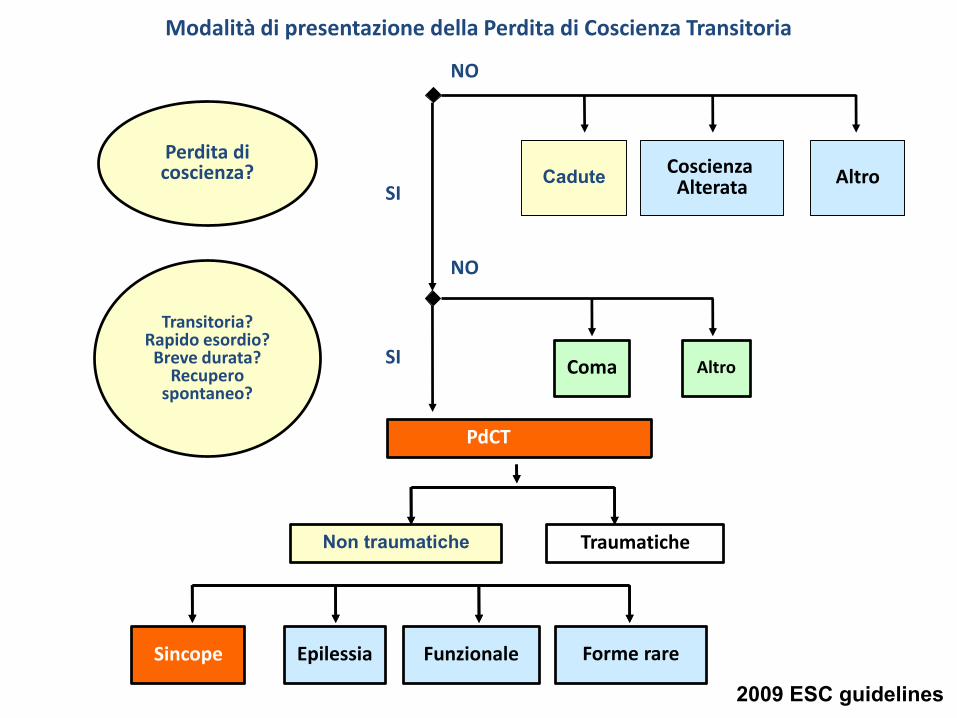
Perdita di coscienza?
NO
Cadute
Modalità di presentazione della Perdita di Coscienza Transitoria
Coscienza Alterata Altro
SI
Transitoria?Rapido esordio?
Breve durata?Recupero
spontaneo?
Coma Altro
NO
PdCT
SI
Sincope Epilessia Funzionale Forme rare
Non traumatiche Traumatiche
2009 ESC guidelines
Il meccanismo fisiopatologico
sottostante la sincope è una ipoperfusione cerebrale globale
transitoria
Poligono del Willis
In condizioni di normale
funzionamento del poligono
del Willis, la causa della
sincope è per definizione
“extracranica”

«La Sincope»
Inquadramento, stratificazione e gestione
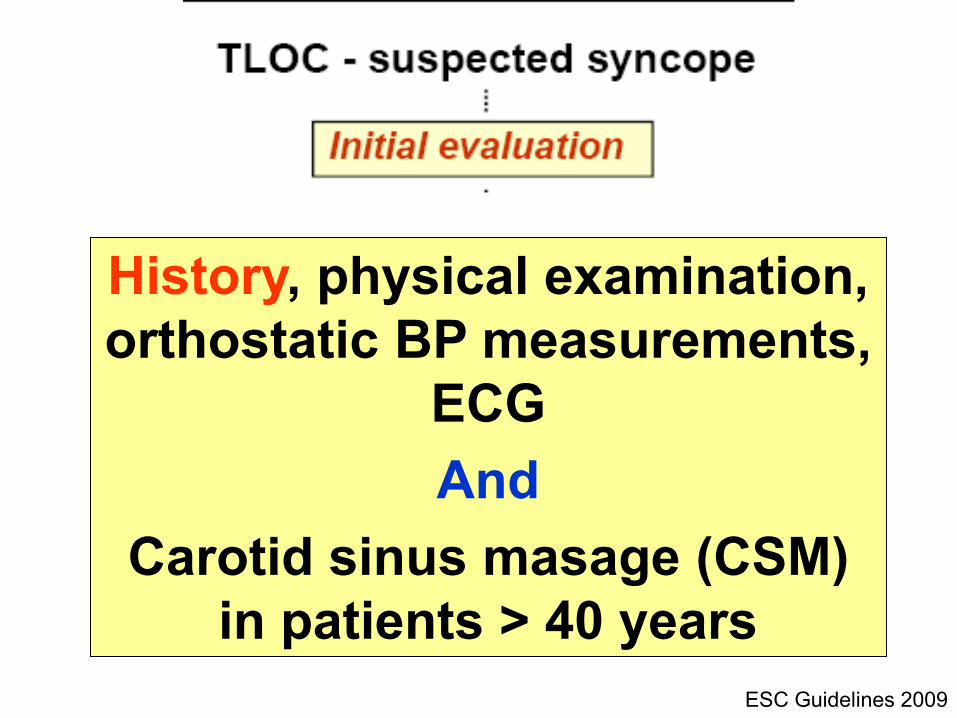
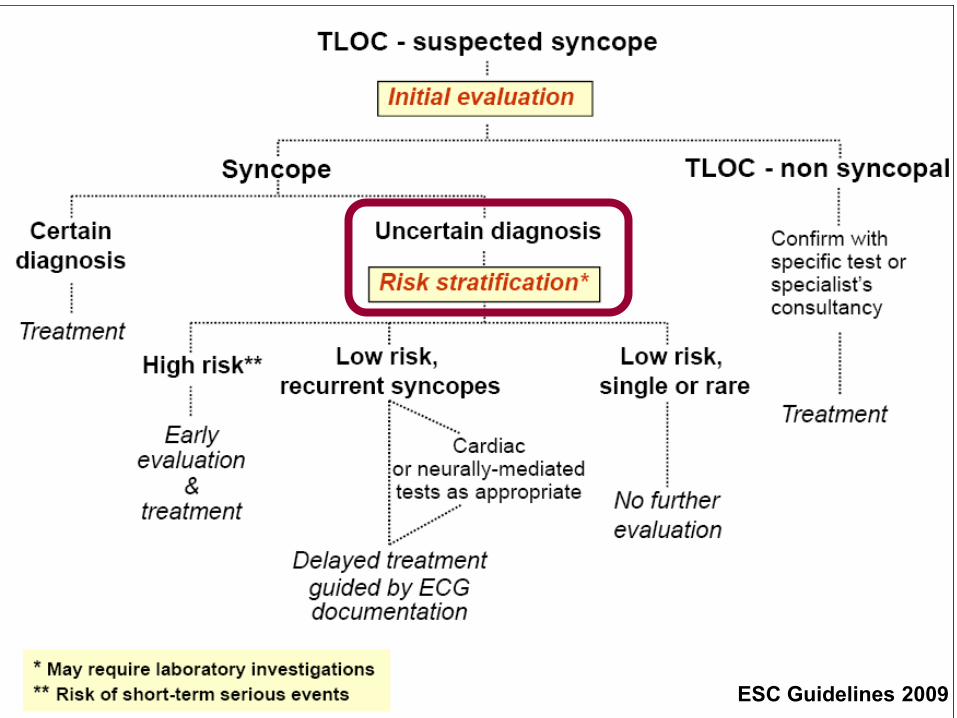
ESC Guidelines 2009
History, physical examination,
orthostatic BP measurements,
ECG
And
Carotid sinus masage (CSM)
in patients > 40 years
ESC Guidelines 2009
Eur Heart J 2010
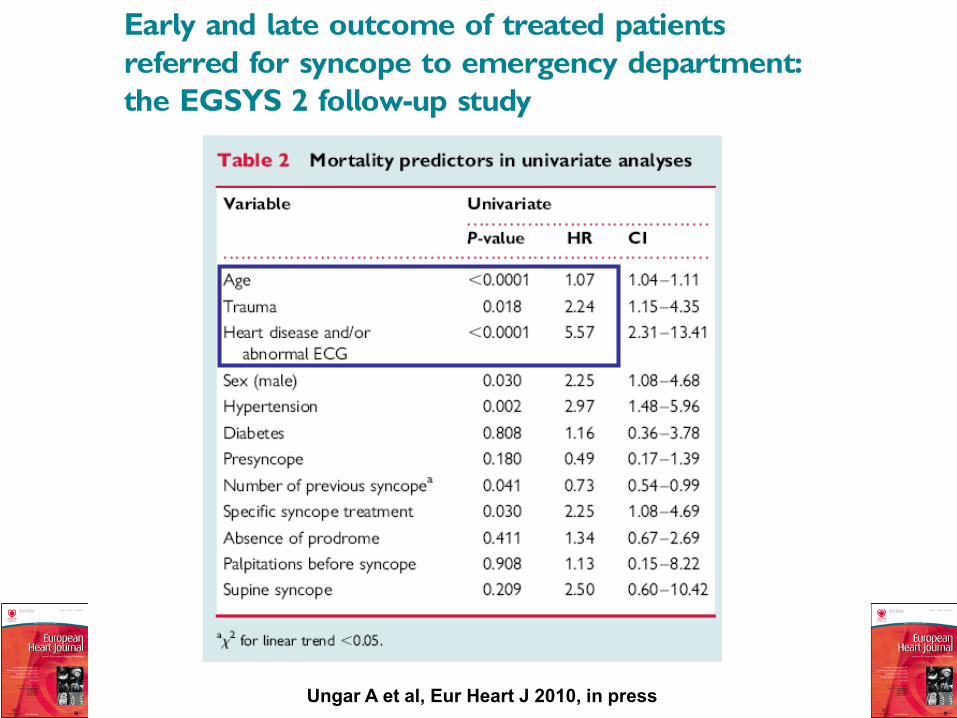
Ungar A et al, Eur Heart J 2010, in press
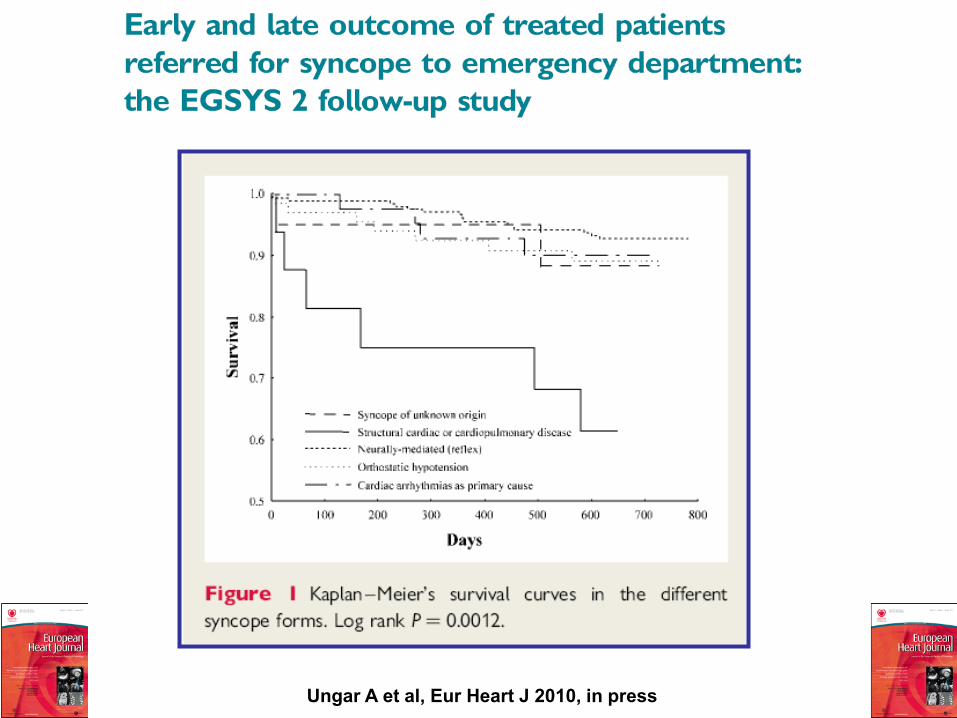
Ungar A et al, Eur Heart J 2010, in press
Long term mortality
Syncope in those with structural heart disease
triples probability of death [OR 3.0 (95% CI 1–10)].
The outcome of arrhythmic syncope, instead, is
more favourable and not different from the
syncope forms usually considered as benign such
as neurally mediated and orthostatic hypotension
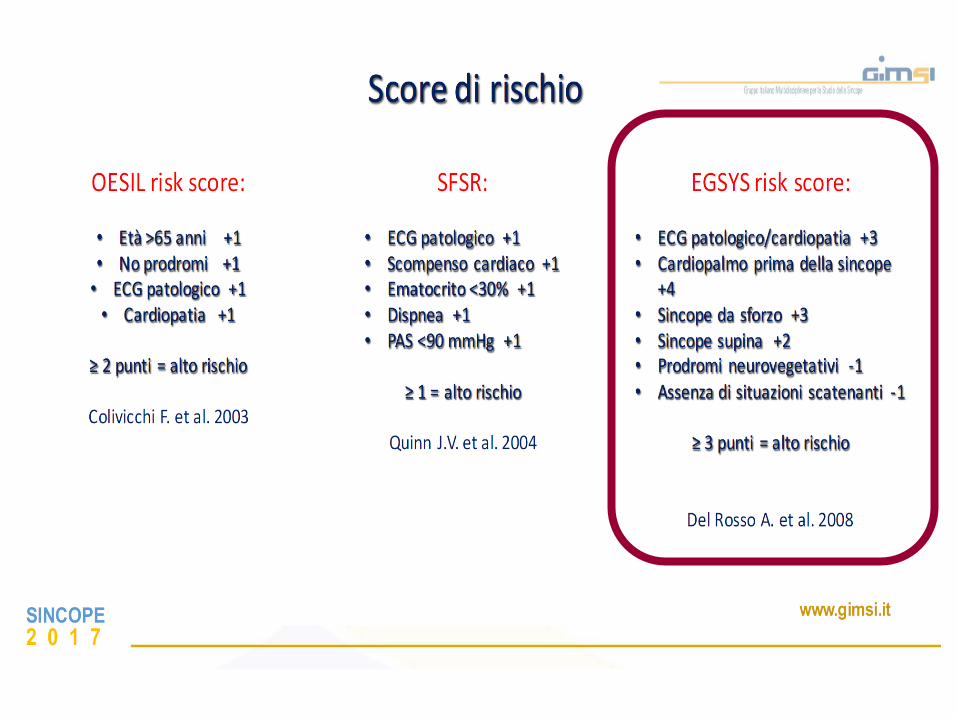
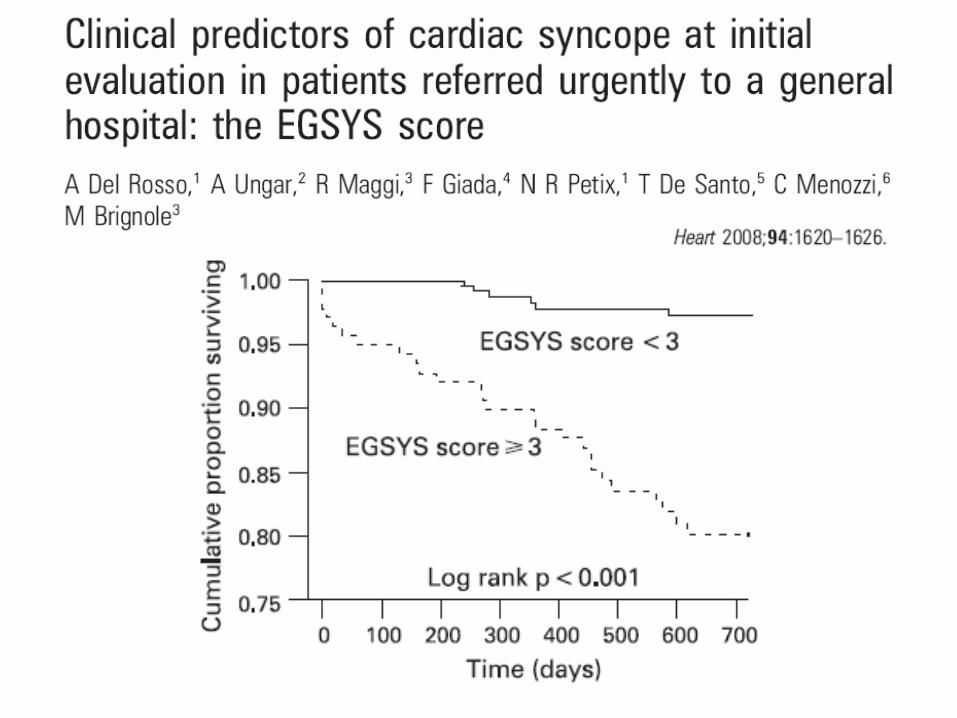
EGSYS score < 3: cardiac syncope is unlikely
EGSYS score > 3: cardiac syncope is probable
Specificity 69%
Sensitivity 95%
SINCOPE2 0 1 7
www.gimsi.it
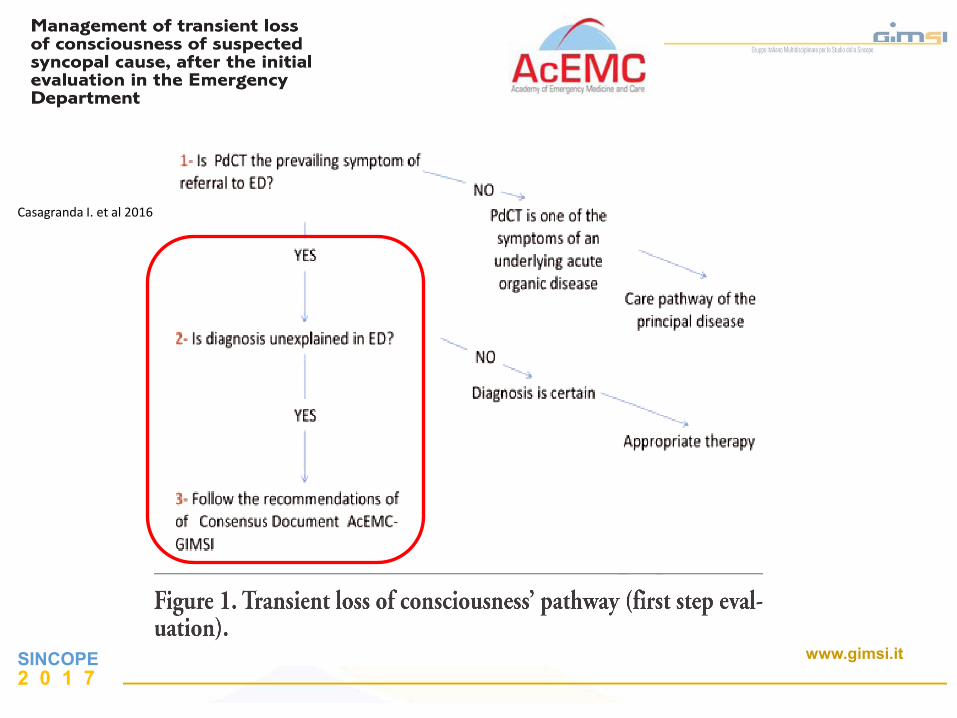
Casagranda I. et al 2016
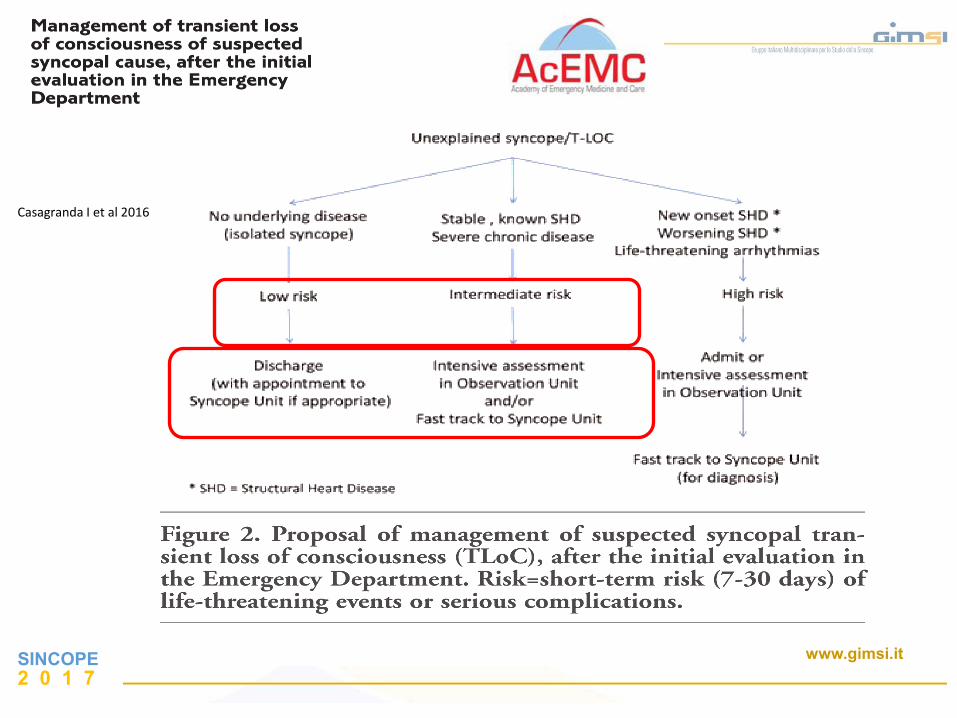
Casagranda I et al 2016
SINCOPE2 0 1 7
www.gimsi.it
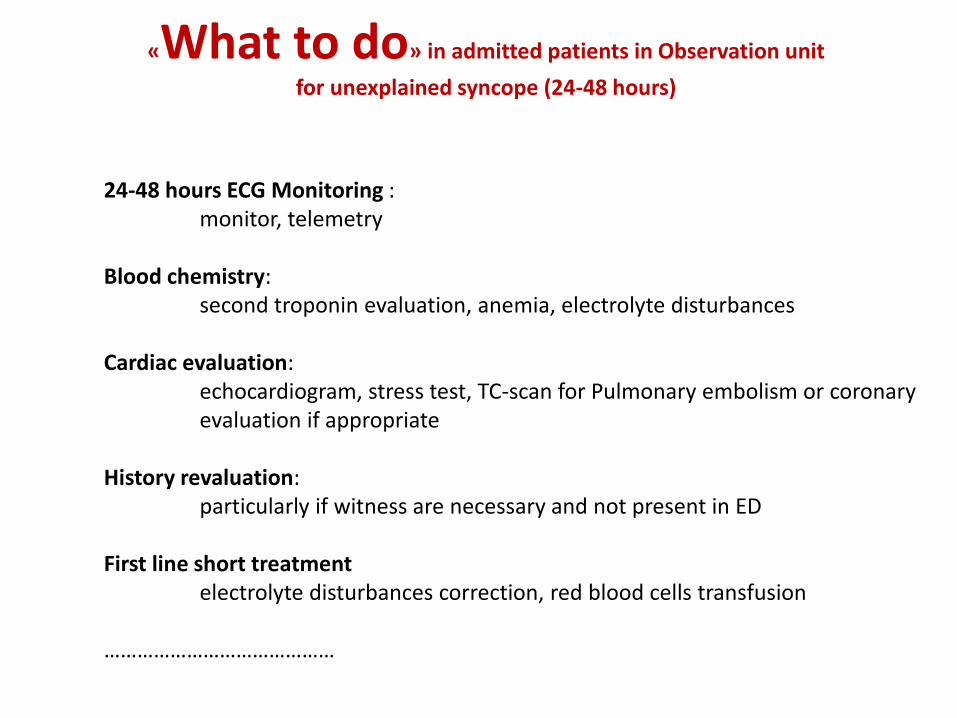
«What to do» in admitted patients in Observation unit
for unexplained syncope (24-48 hours)
24-48 hours ECG Monitoring :monitor, telemetry
Blood chemistry:second troponin evaluation, anemia, electrolyte disturbances
Cardiac evaluation:echocardiogram, stress test, TC-scan for Pulmonary embolism or coronary evaluation if appropriate
History revaluation:particularly if witness are necessary and not present in ED
First line short treatmentelectrolyte disturbances correction, red blood cells transfusion
……………………………………
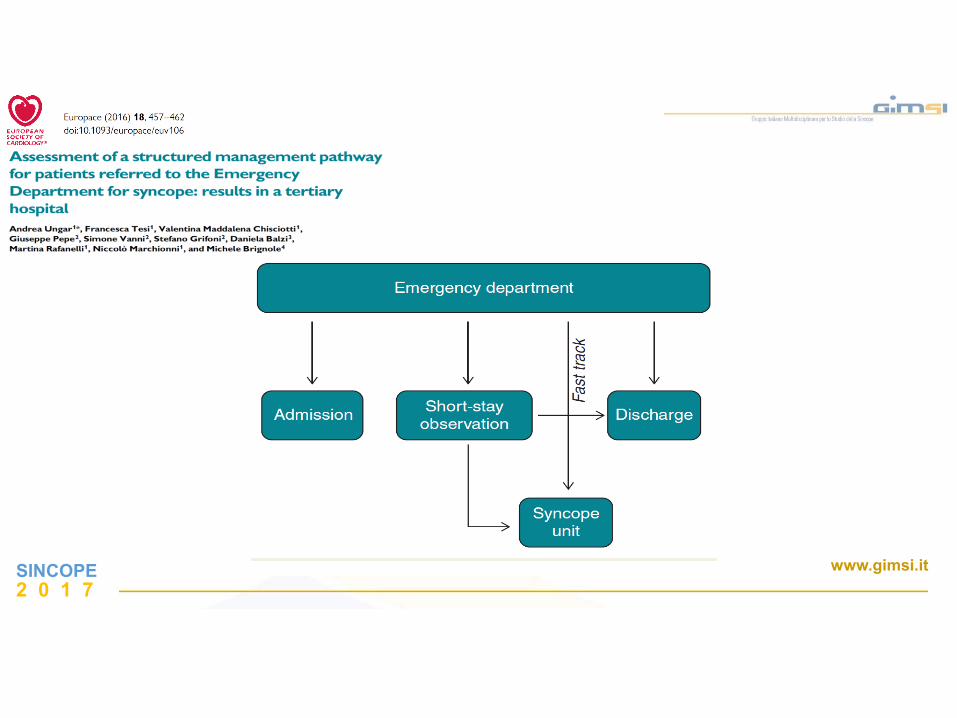
Assessment of a novel management
pathway for patients referred to the
Emergency Department for syncope: results
in a Tertiary Hospital
(Careggi Hospital - Florence, Italy)
Ungar a et al, Europace 2015
SINCOPE2 0 1 7
www.gimsi.it
Consecutive patients referred to the EDof Careggi Hospital for T-LOC in whichsyncope was suspected as the maindiagnosis, from 1 January to 30 June2010
SINCOPE2 0 1 7
www.gimsi.it
Consecutive patients referred to the EDof Careggi Hospital for T-LOC in whichsyncope was suspected as the maindiagnosis, from 1 January to 30 June2010
SINCOPE2 0 1 7
www.gimsi.it
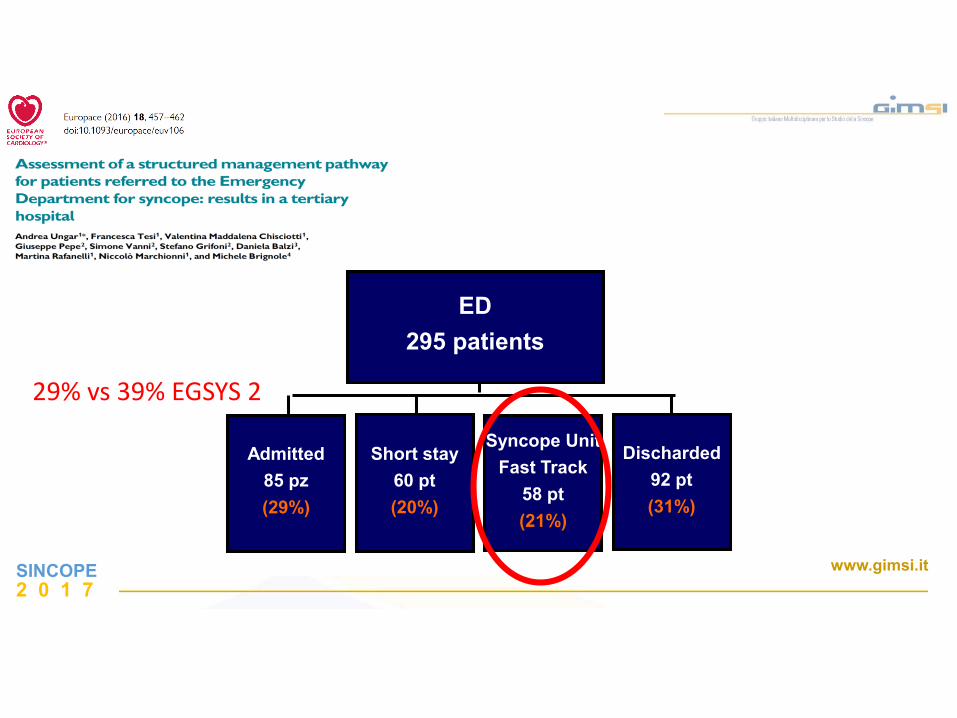
ED
295 patients
Admitted
85 pz
(29%)
Short stay
60 pt
(20%)
Syncope Unit
Fast Track
58 pt
(21%)
Discharded
92 pt
(31%)
29% vs 39% EGSYS 2
SINCOPE2 0 1 7
www.gimsi.it
0.1
.2.3
.4.5
0 5 10 15Months of follow-up
Ricovero OBI
Fast Track Niente
Rifiuta
Estimated hospital re-admission according to multivariable Cox model-destino
New admissions related to ED destination
1 month 12 months
Follow-up
Admission Short stay observation Syncope Unit DimissionRefusal
No patients sent to Syncope Unit
was dead within one year
Our outcomes prove the safety of the model
recommended by 2009 ESC guidelines
Ungar a et al, Europace 2015
SINCOPE2 0 1 7
www.gimsi.it
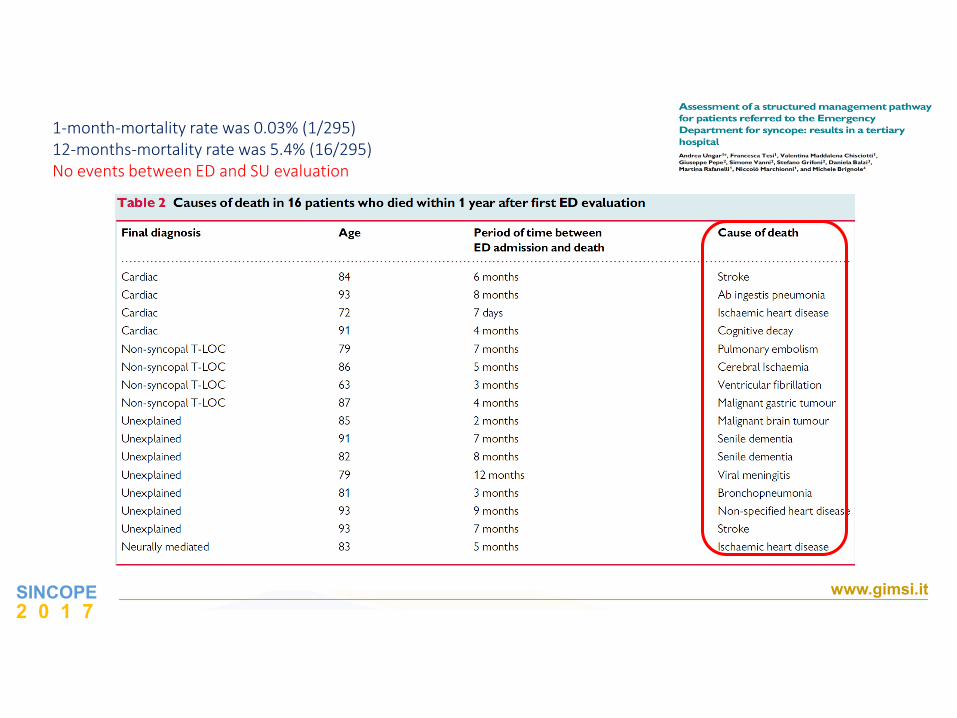
1-month-mortality rate was 0.03% (1/295)12-months-mortality rate was 5.4% (16/295)No events between ED and SU evaluation
SINCOPE2 0 1 7
www.gimsi.it
SINCOPE2 0 1 7
www.gimsi.it
Kenny R.A. et al. 2015
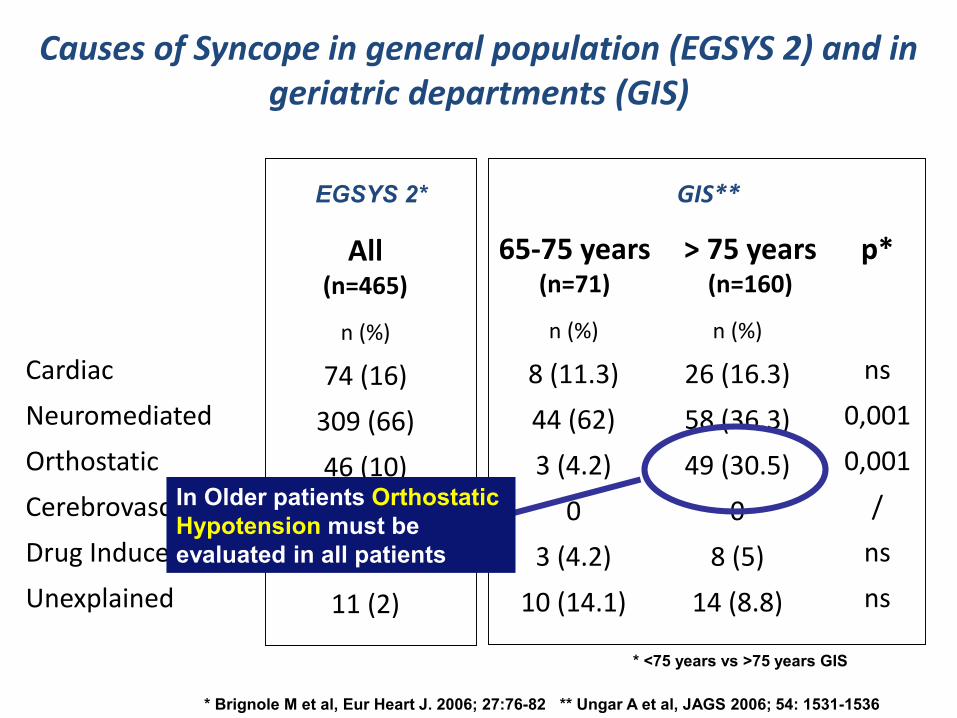
Causes of Syncope in general population (EGSYS 2) and in geriatric departments (GIS)
Cardiac
Neuromediated
Orthostatic
Cerebrovascular
Drug Induced
Unexplained
n (%)
8 (11.3)
44 (62)
3 (4.2)
0
3 (4.2)
10 (14.1)
n (%)
26 (16.3)
58 (36.3)
49 (30.5)
0
8 (5)
14 (8.8)
ns
0,001
0,001
/
ns
ns
65-75 years(n=71)
> 75 years(n=160)
p*
n (%)
74 (16)
309 (66)
46 (10)
0 (0)
2 (0)
11 (2)
All(n=465)
GIS**
* <75 years vs >75 years GIS
* Brignole M et al, Eur Heart J. 2006; 27:76-82 ** Ungar A et al, JAGS 2006; 54: 1531-1536
EGSYS 2*
In Older patients Orthostatic
Hypotension must be
evaluated in all patients
Gruppo Italiano Sincope (GIS) - SIGG
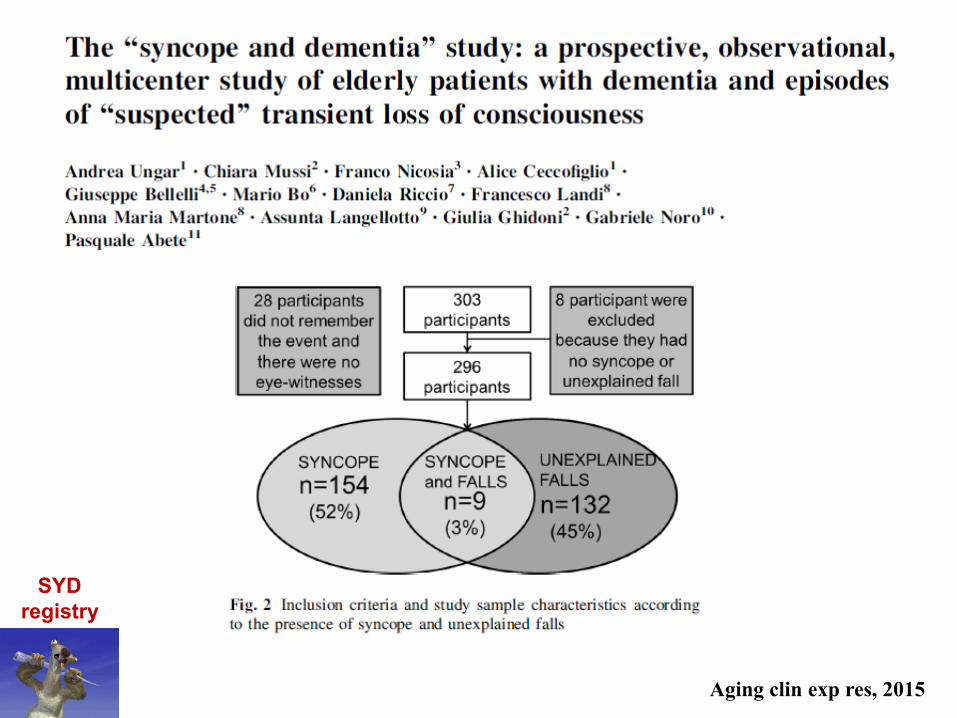
Syncope and Dementia, a GIS Registry
SYD Registry
We enrolled patients with Syncope and Unexplained falls
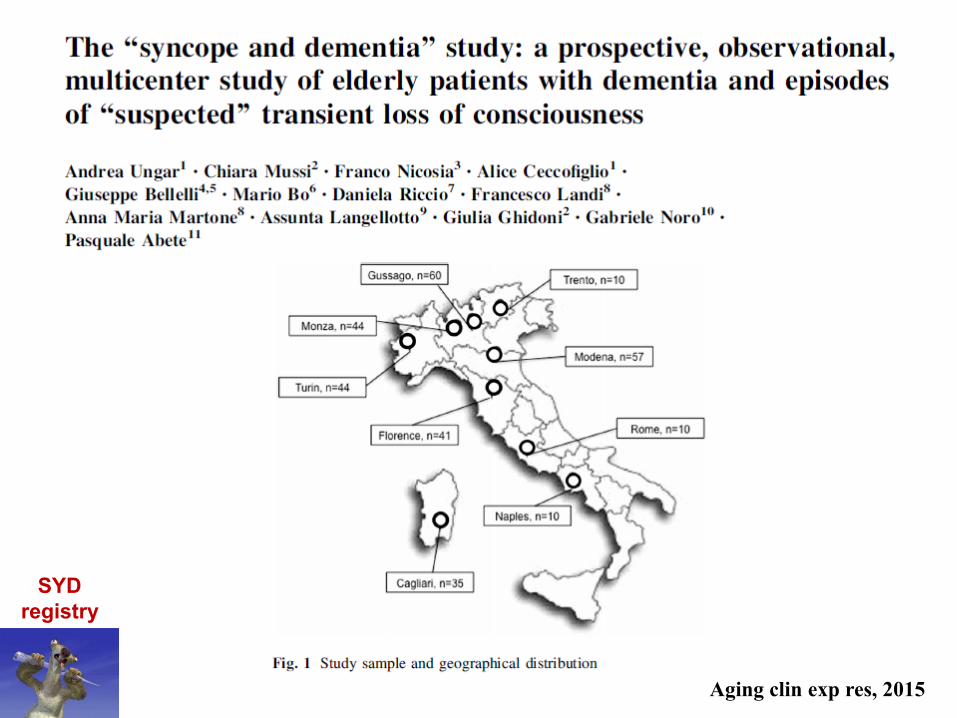
Aging clin exp res, 2015
SYD
registry
Aging clin exp res, 2015
SYD
registry
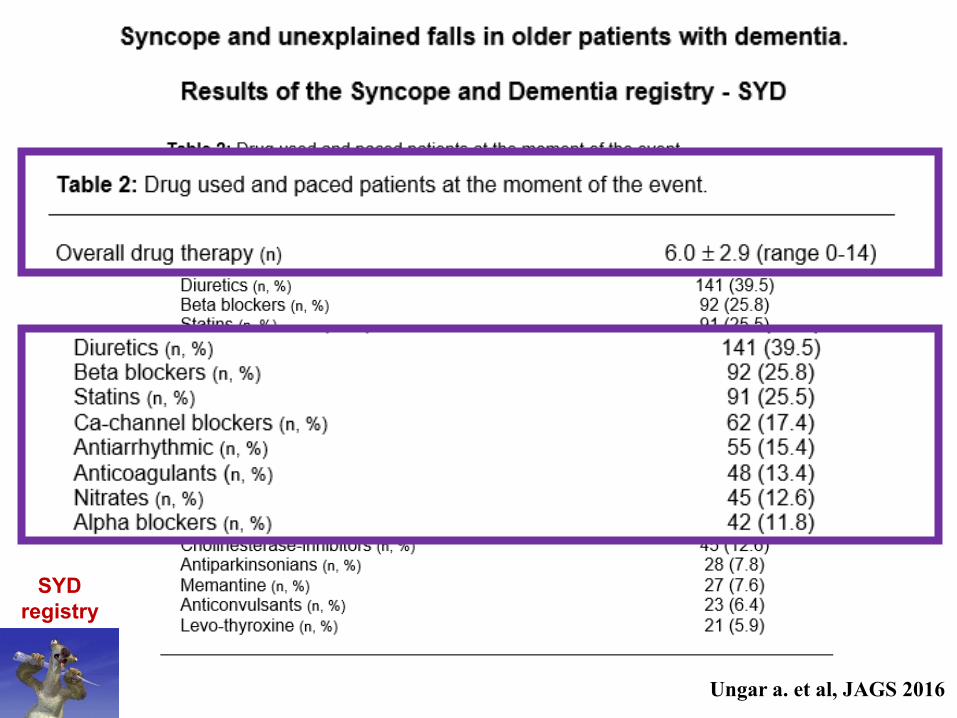
Ungar a. et al, JAGS 2016
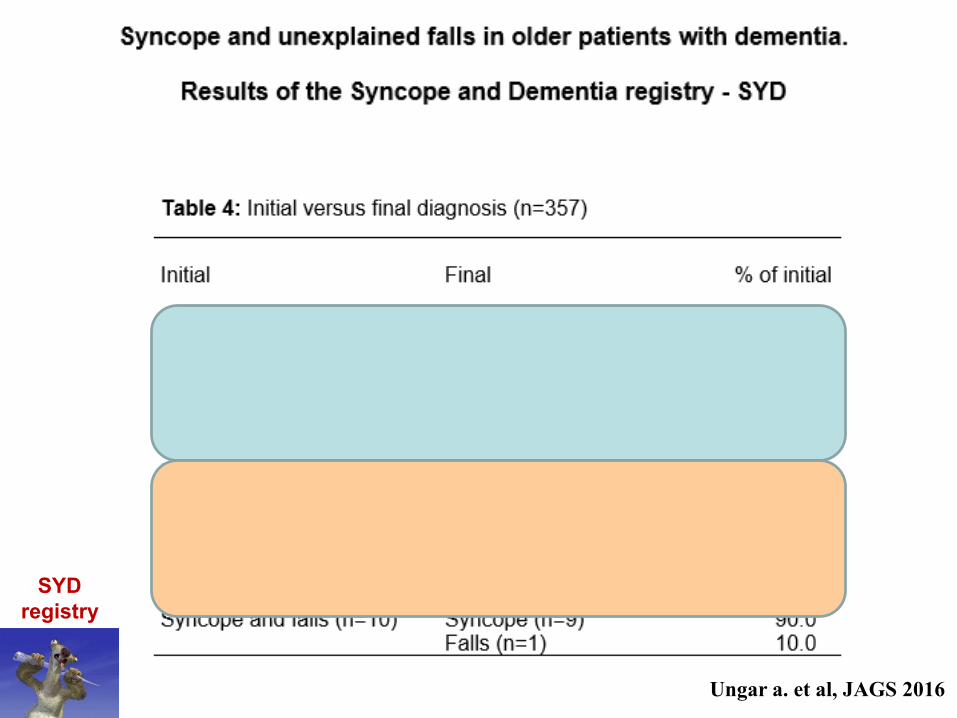
SYD
registry
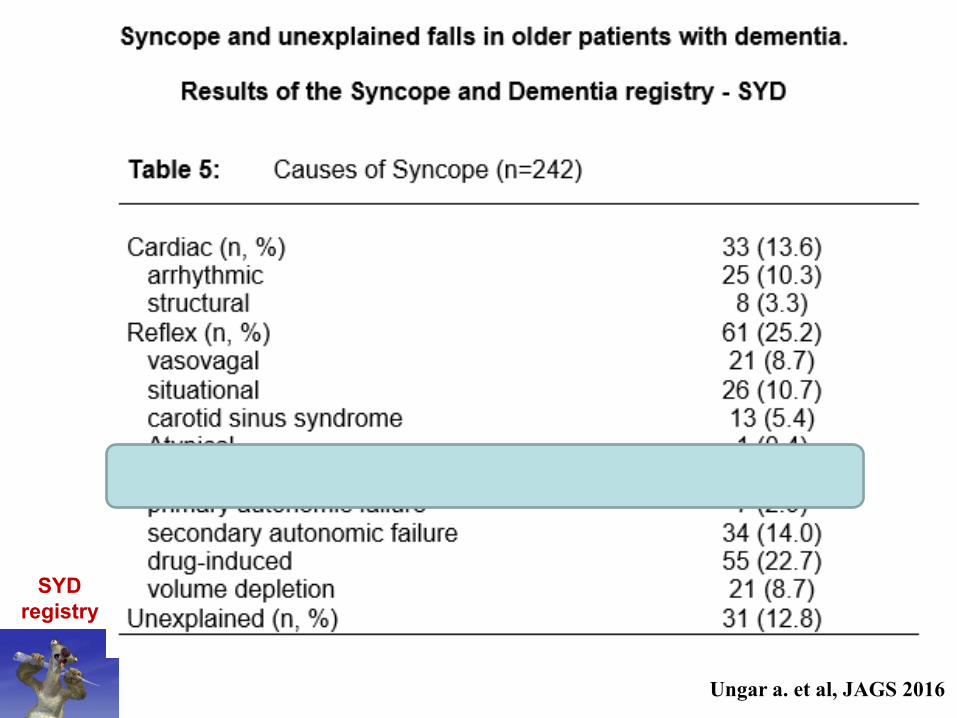
Ungar a. et al, JAGS 2016
SYD
registry
Ungar a. et al, JAGS 2016
SYD
registry
www.gimsi.it
STOP-VDStop vasodepressor drugs in reflex syncope
A randomized controlled trial
Bolzano, 20 febbraio 2016
Diana SolariFrancesca TesiMatthias UnterhuberGermano GaggioliAndrea UngarMarco TomainoMichele Brignole
From the Syncope Units of:
Ospedali del Tigullio, Lavagna
University of Firenze
Ospedale Generale, Bolzano
Ospedale Villa Scassi, Genova
A trial sponsored by GIMSI
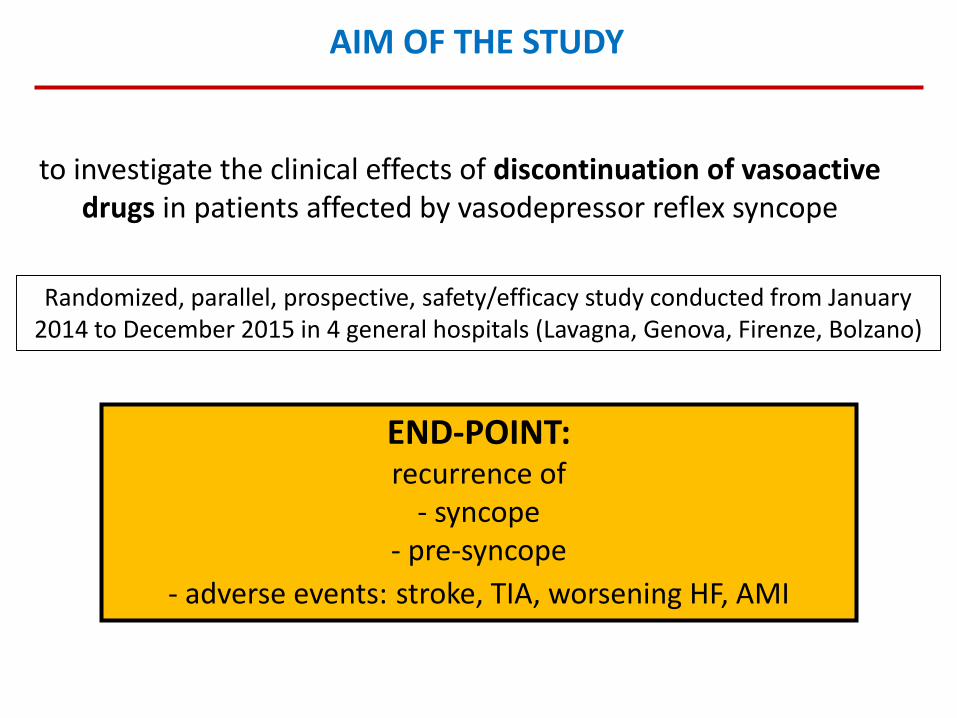
AIM OF THE STUDY
to investigate the clinical effects of discontinuation of vasoactive drugs in patients affected by vasodepressor reflex syncope
Randomized, parallel, prospective, safety/efficacy study conducted from January 2014 to December 2015 in 4 general hospitals (Lavagna, Genova, Firenze, Bolzano)
END-POINT: recurrence of
- syncope - pre-syncope
- adverse events: stroke, TIA, worsening HF, AMI
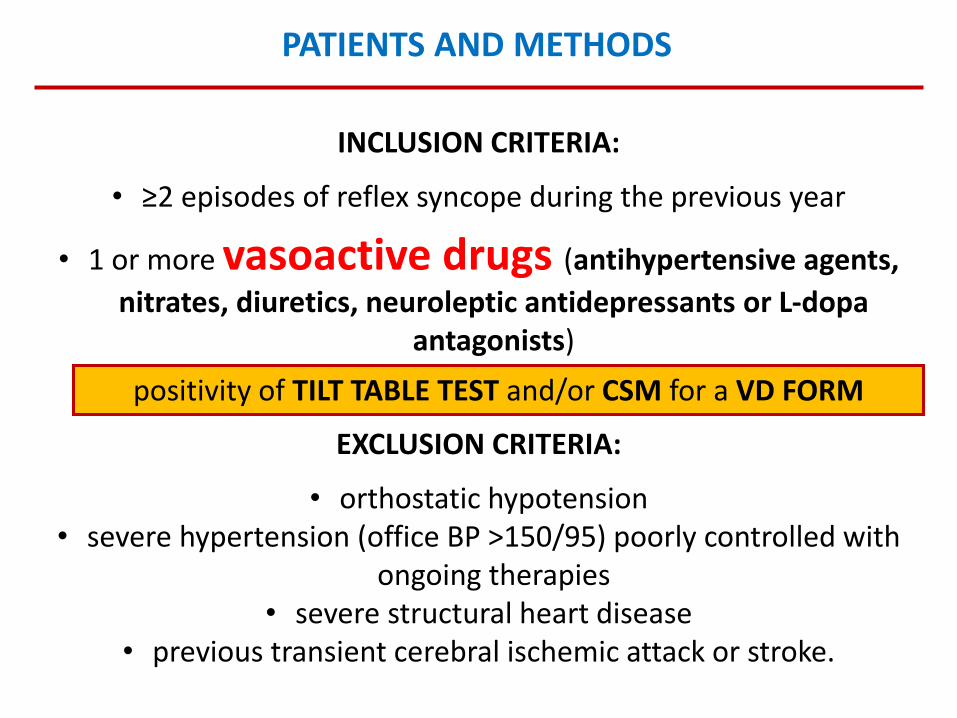
PATIENTS AND METHODS
INCLUSION CRITERIA:
• ≥2 episodes of reflex syncope during the previous year
• 1 or more vasoactive drugs (antihypertensive agents,
nitrates, diuretics, neuroleptic antidepressants or L-dopa antagonists)
positivity of TILT TABLE TEST and/or CSM for a VD FORM
EXCLUSION CRITERIA:
• orthostatic hypotension• severe hypertension (office BP >150/95) poorly controlled with
ongoing therapies• severe structural heart disease
• previous transient cerebral ischemic attack or stroke.
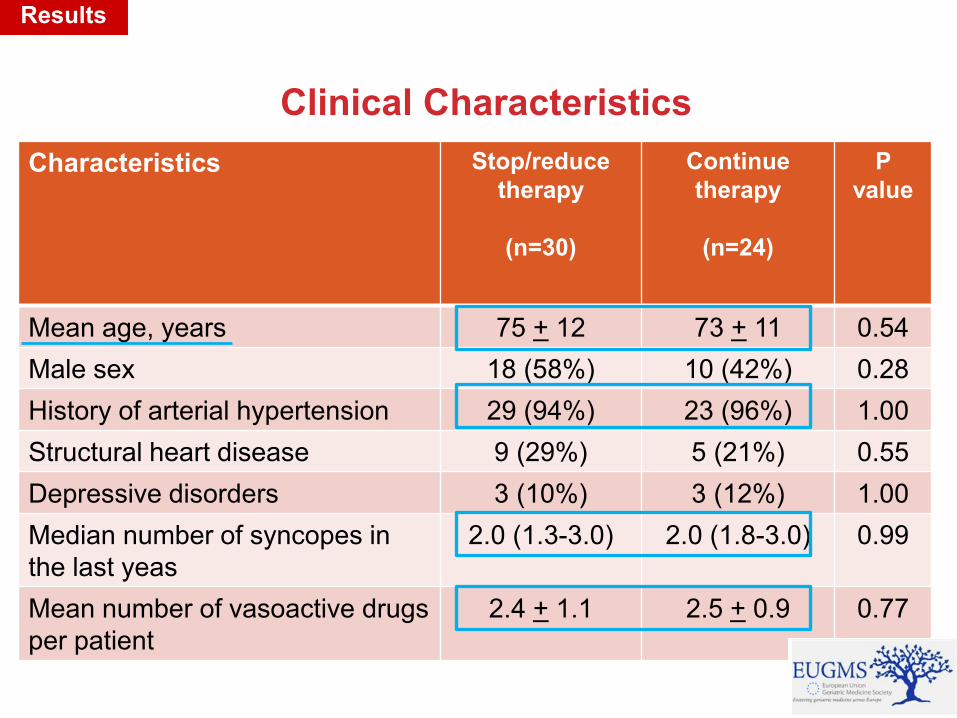
Clinical Characteristics
Results
Characteristics Stop/reduce
therapy
(n=30)
Continue
therapy
(n=24)
P
value
Mean age, years 75 + 12 73 + 11 0.54
Male sex 18 (58%) 10 (42%) 0.28
History of arterial hypertension 29 (94%) 23 (96%) 1.00
Structural heart disease 9 (29%) 5 (21%) 0.55
Depressive disorders 3 (10%) 3 (12%) 1.00
Median number of syncopes in
the last yeas
2.0 (1.3-3.0) 2.0 (1.8-3.0) 0.99
Mean number of vasoactive drugs
per patient
2.4 + 1.1 2.5 + 0.9 0.77
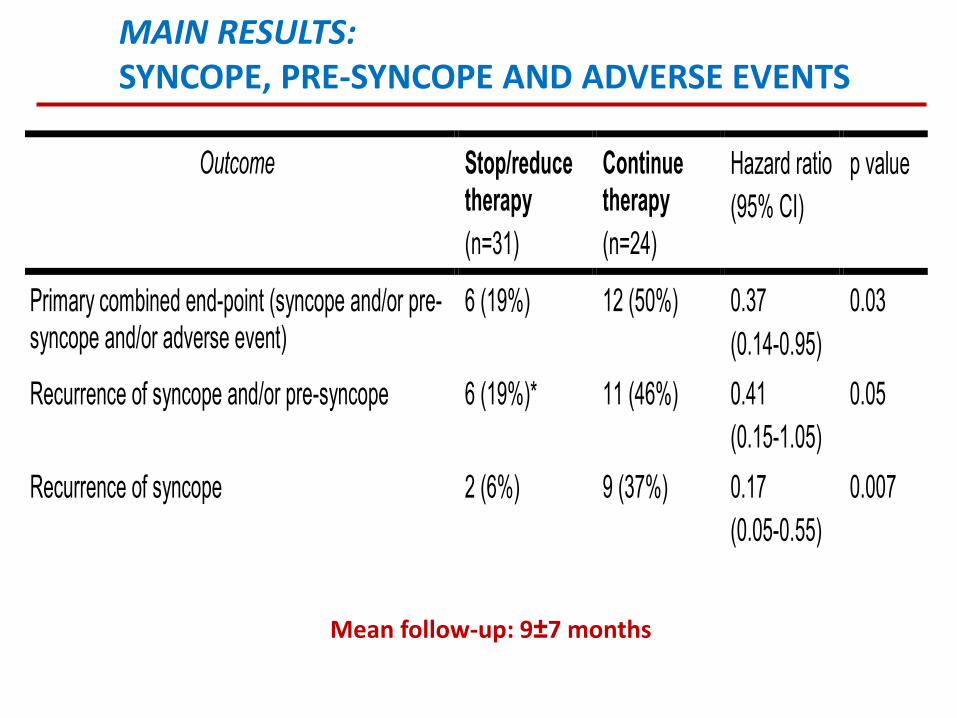
MAIN RESULTS: SYNCOPE, PRE-SYNCOPE AND ADVERSE EVENTS
Outcome Stop/reduce therapy
(n=31)
Continue therapy
(n=24)
Hazard ratio
(95% CI)
p value
Primary combined end-point (syncope and/or pre-syncope and/or adverse event)
6 (19%) 12 (50%) 0.37
(0.14-0.95)
0.03
Recurrence of syncope and/or pre-syncope 6 (19%)*
11 (46%) 0.41
(0.15-1.05)
0.05
Recurrence of syncope 2 (6%) 9 (37%) 0.17
(0.05-0.55)
0.007
Assessment at 1 month:
- Office supine SBP, mmHg 141±13 128±14 0.001
- Office standing SBP, mmHg 133±13 122±15 0.006
- Home daily SBP (average of 30-day measurements)
141±15 133±16 0.06
- SSS-OI Questionnaire: total score (score 0-70) 7.2±8.8 13.1±10.6 0,04
Mean follow-up: 9±7 months
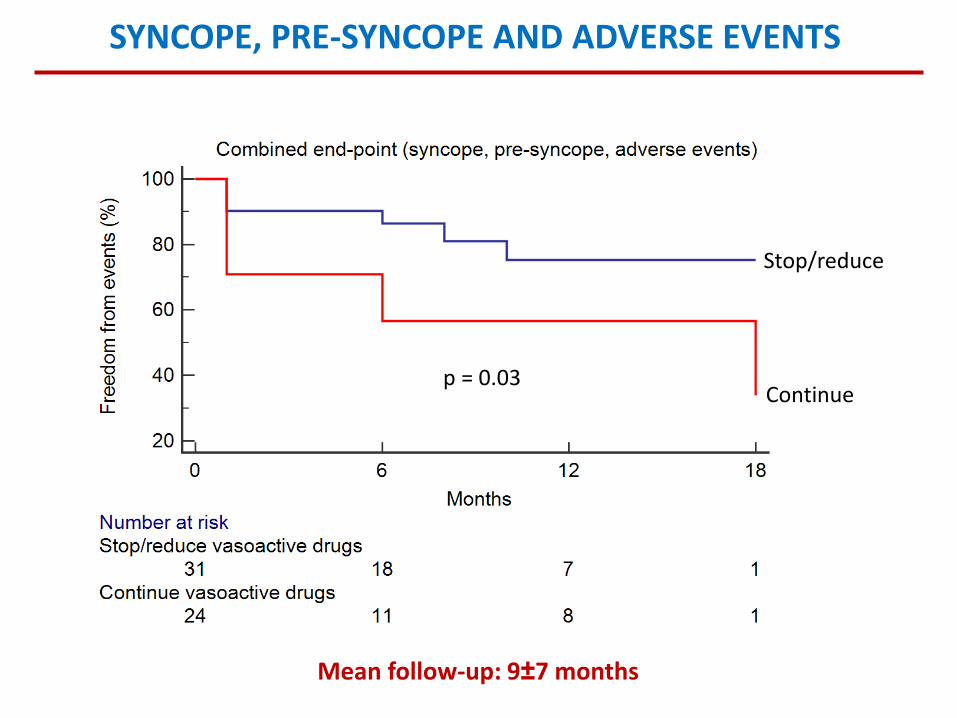
p = 0.03
Stop/reduce
Continue
SYNCOPE, PRE-SYNCOPE AND ADVERSE EVENTS
Mean follow-up: 9±7 months
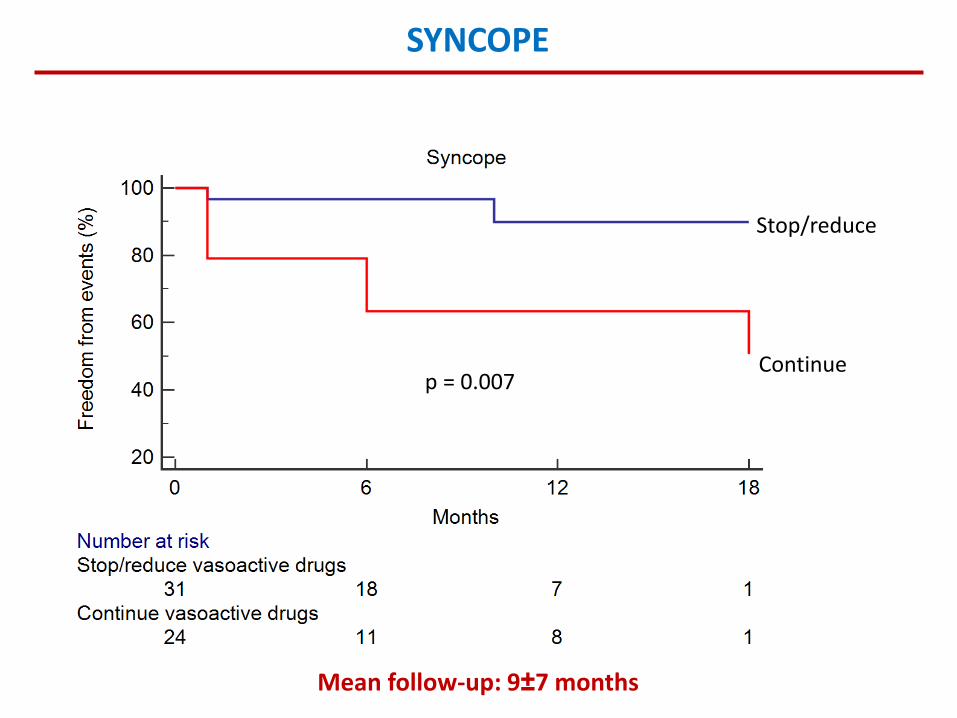
p = 0.007
Stop/reduce
Continue
SYNCOPE
Mean follow-up: 9±7 months

«La Sincope»
Il monitoraggio
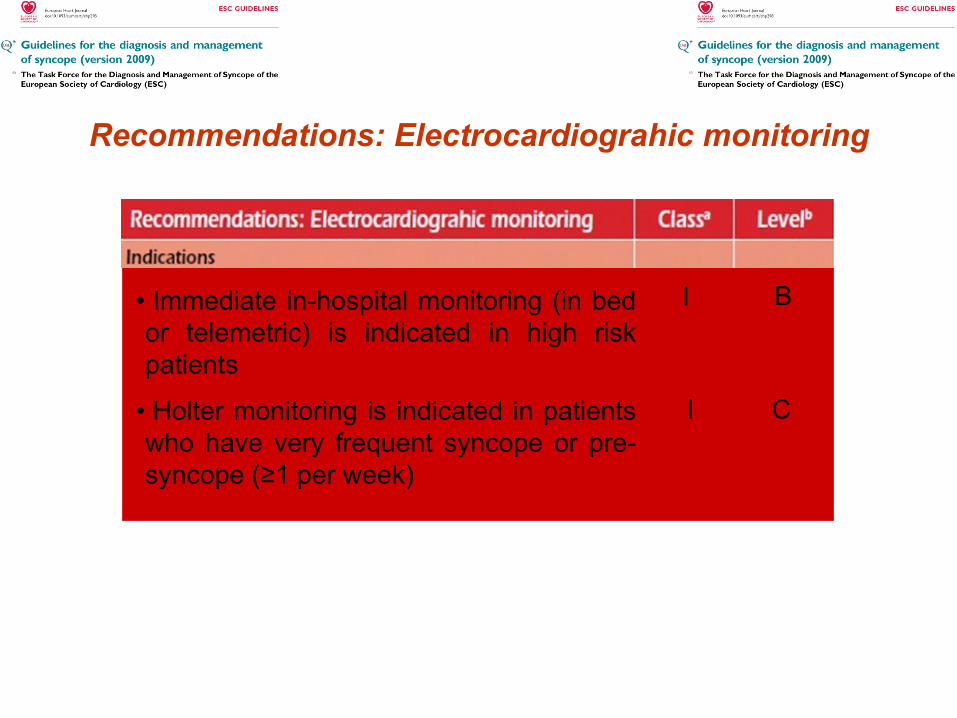
Recommendations: Electrocardiograhic monitoring
I B• Immediate in-hospital monitoring (in bed
or telemetric) is indicated in high risk
patients
• Holter monitoring is indicated in patients
who have very frequent syncope or pre-
syncope (≥1 per week)
I C


Recommendations: Electrocardiograhic monitoring
• Il monitoraggio è diagnostico se vi è una correlazione
tra sintomo e aritmia
• In assenza di correlazione sono diagnostici un blocco
atrioventricolare avanzato, una pausa ventricolare > 3
secondi, o una tachicardia atriale ad elevata frequenza
• Le altre aritmie asintomatiche non hanno rilievo
diagnostico
• La bradicardia sinusale in assenza di sintomi non è
indicativa della causa di sincope
• La presincope non è diagnostica

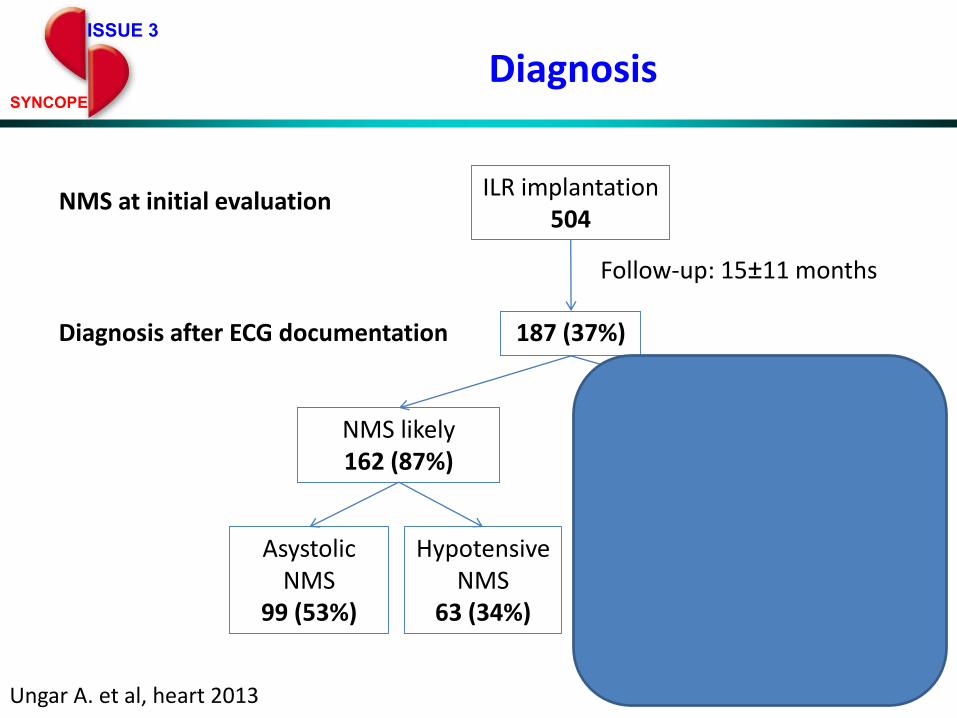
NMS at initial evaluationILR implantation
504
Diagnosis after ECG documentation
Follow-up: 15±11 months
187 (37%)
Hypotensive NMS
63 (34%)
Asystolic NMS
99 (53%)
Intrinsic cardiac
arrhythmias21 (11%)
Non-arrhythmic
T-LOC4 (2%)
NMS likely 162 (87%)
NMS excluded25 (13%)
ISSUE 3
SYNCOPE
Diagnosis
Ungar A. et al, heart 2013
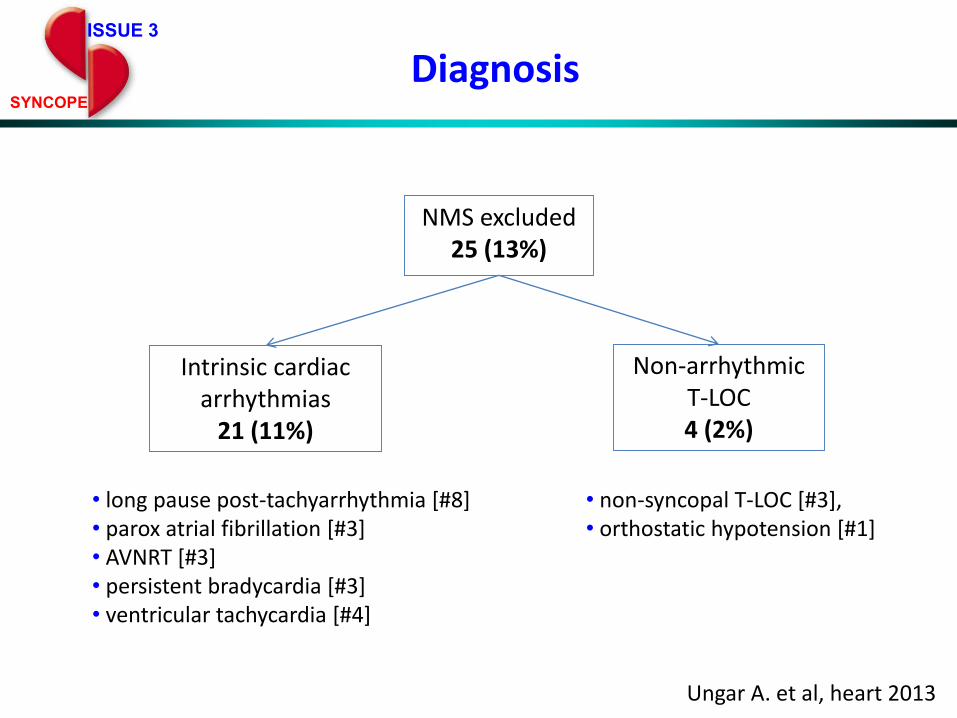
ISSUE 3
SYNCOPE
Diagnosis
Intrinsic cardiac arrhythmias
21 (11%)
Non-arrhythmic T-LOC4 (2%)
NMS excluded25 (13%)
• long pause post-tachyarrhythmia [#8]• parox atrial fibrillation [#3]• AVNRT [#3] • persistent bradycardia [#3]• ventricular tachycardia [#4]
• non-syncopal T-LOC [#3], • orthostatic hypotension [#1]
Ungar A. et al, heart 2013
«La Sincope»
Due peculiarità:1. Le cadute non spiegate
Le cadute
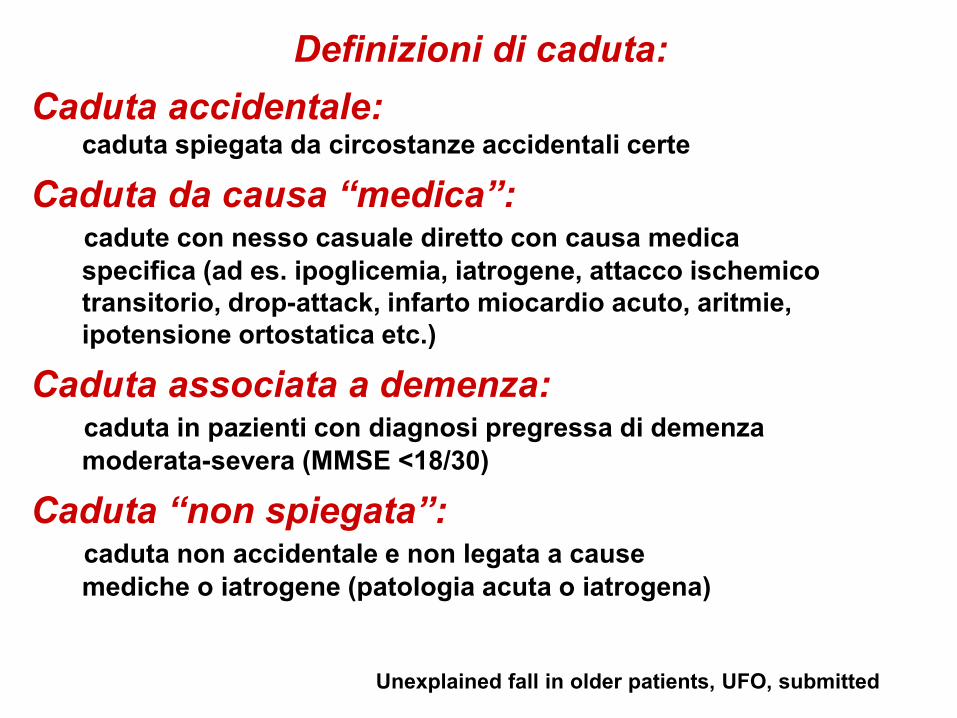
Definizioni di caduta:
Caduta accidentale:caduta spiegata da circostanze accidentali certe
Caduta da causa “medica”:cadute con nesso casuale diretto con causa medica
specifica (ad es. ipoglicemia, iatrogene, attacco ischemico
transitorio, drop-attack, infarto miocardio acuto, aritmie,
ipotensione ortostatica etc.)
Caduta associata a demenza:caduta in pazienti con diagnosi pregressa di demenza
moderata-severa (MMSE <18/30)
Caduta “non spiegata”:caduta non accidentale e non legata a cause
mediche o iatrogene (patologia acuta o iatrogena)
Unexplained fall in older patients, UFO, submitted
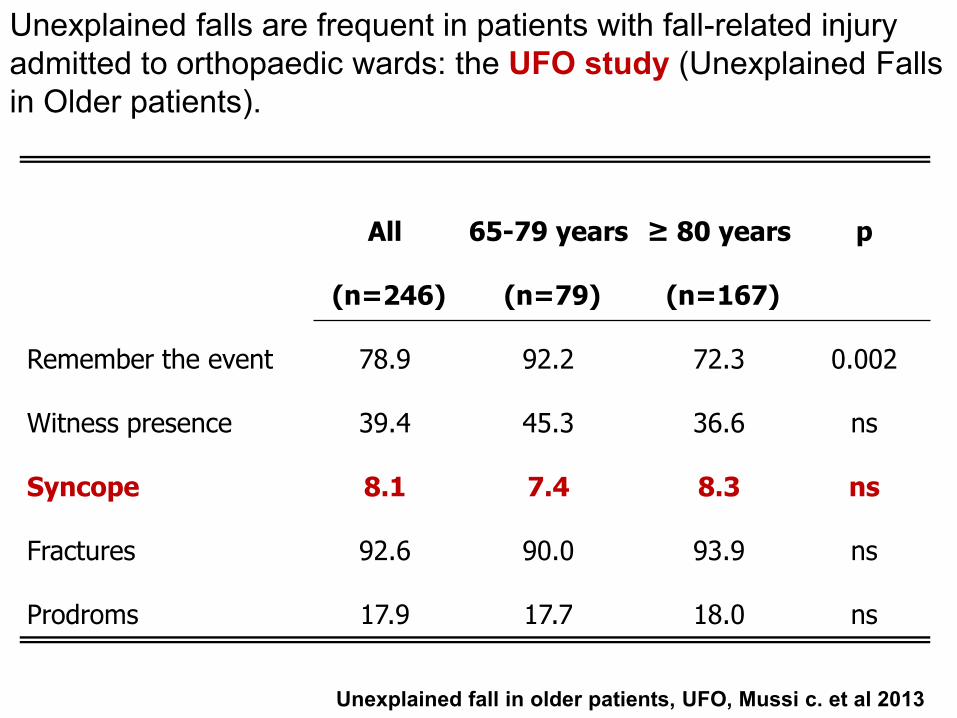
Unexplained falls are frequent in patients with fall-related injury
admitted to orthopaedic wards: the UFO study (Unexplained Falls
in Older patients).
All
(n=246)
65-79 years
(n=79)
≥ 80 years
(n=167)
p
Remember the event 78.9 92.2 72.3 0.002
Witness presence 39.4 45.3 36.6 ns
Syncope 8.1 7.4 8.3 ns
Fractures 92.6 90.0 93.9 ns
Prodroms 17.9 17.7 18.0 ns
Unexplained fall in older patients, UFO, Mussi c. et al 2013
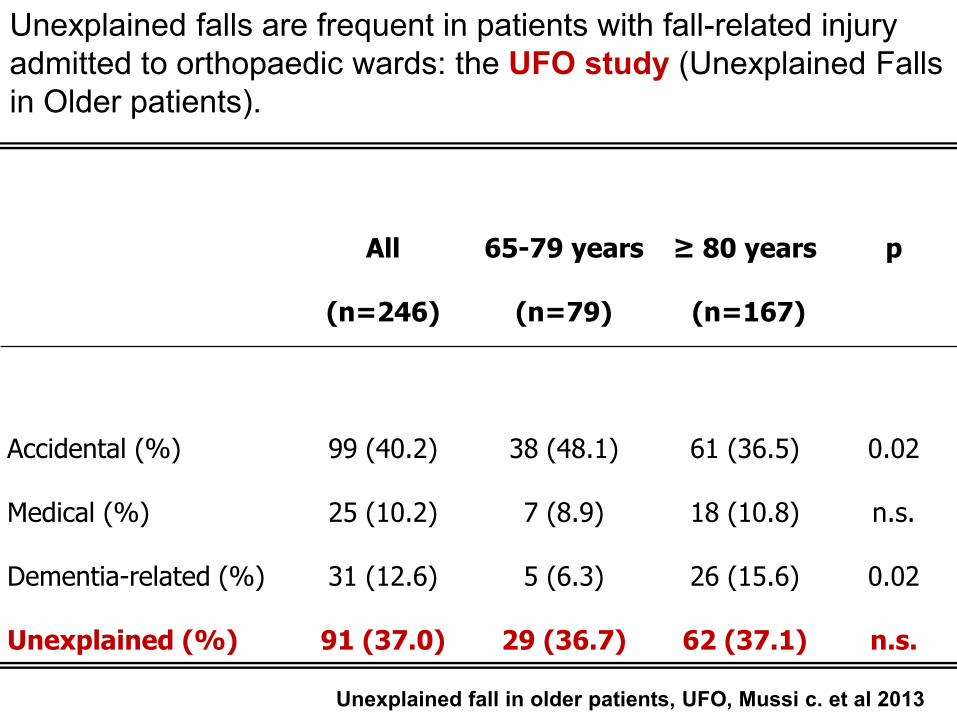
Unexplained falls are frequent in patients with fall-related injury
admitted to orthopaedic wards: the UFO study (Unexplained Falls
in Older patients).
All
(n=246)
65-79 years
(n=79)
≥ 80 years
(n=167)
p
Accidental (%) 99 (40.2) 38 (48.1) 61 (36.5) 0.02
Medical (%) 25 (10.2) 7 (8.9) 18 (10.8) n.s.
Dementia-related (%) 31 (12.6) 5 (6.3) 26 (15.6) 0.02
Unexplained (%) 91 (37.0) 29 (36.7) 62 (37.1) n.s.
Unexplained fall in older patients, UFO, Mussi c. et al 2013
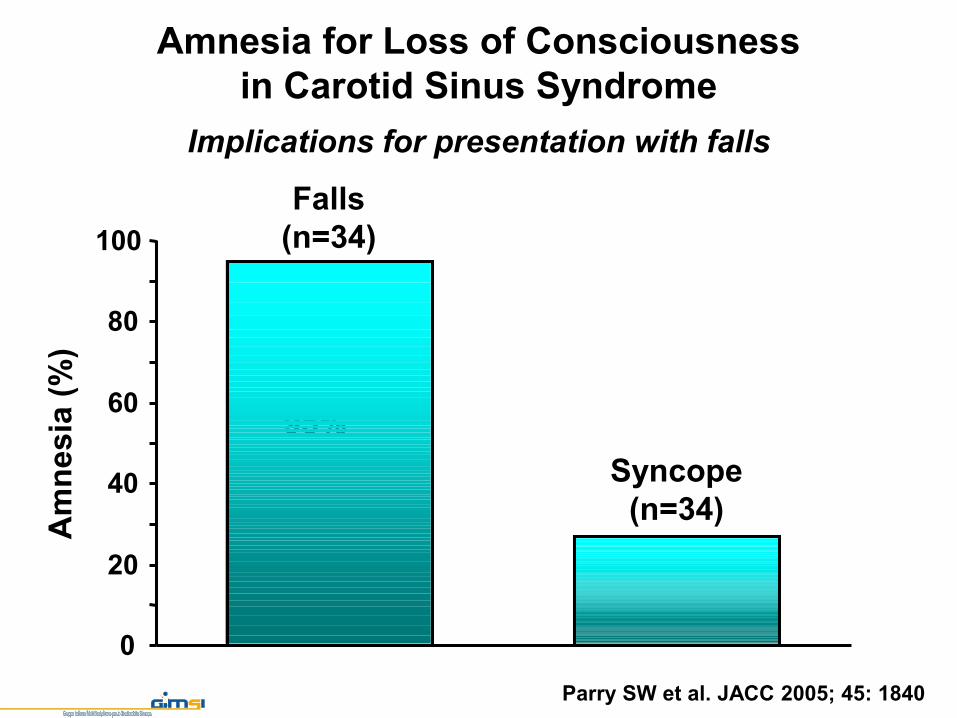
Amnesia for Loss of Consciousness
in Carotid Sinus Syndrome
Implications for presentation with falls
Parry SW et al. JACC 2005; 45: 1840
Falls
(n=34)
Syncope
(n=34)
Am
nesia
(%
)
95%
27%
0
20
40
60
80
100
Caduta accidentale …….

… o caduta non spiegata???
Sincope, Demenza, “Dizziness”,
Ipotensione ortostatica, Aritmie …
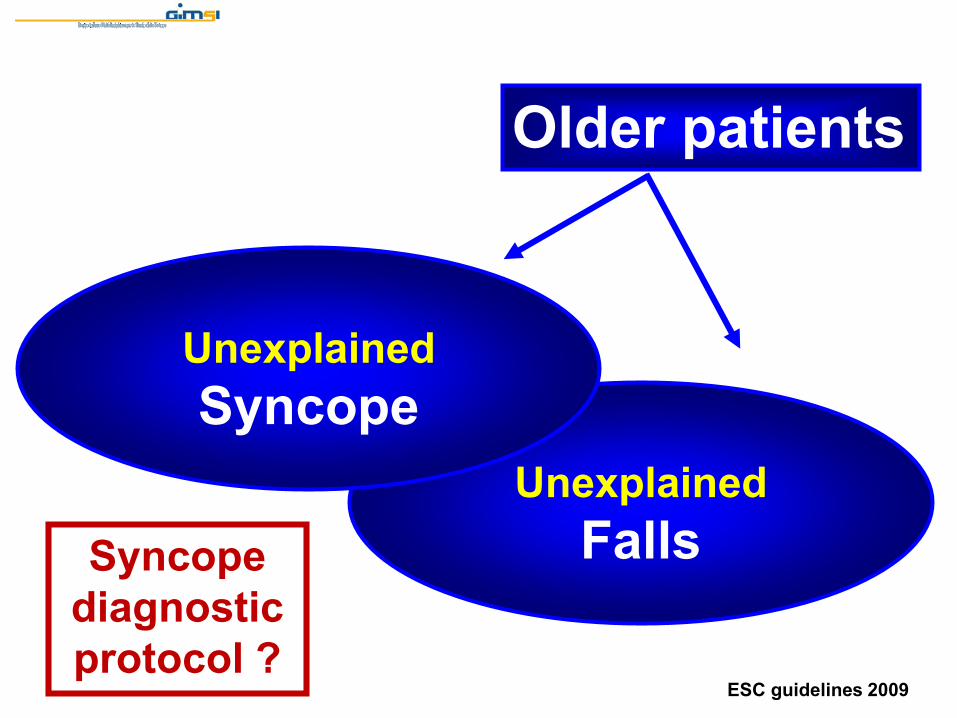
Unexplained
Falls
Unexplained
Syncope
Older patients
Syncope
diagnostic
protocol ?ESC guidelines 2009
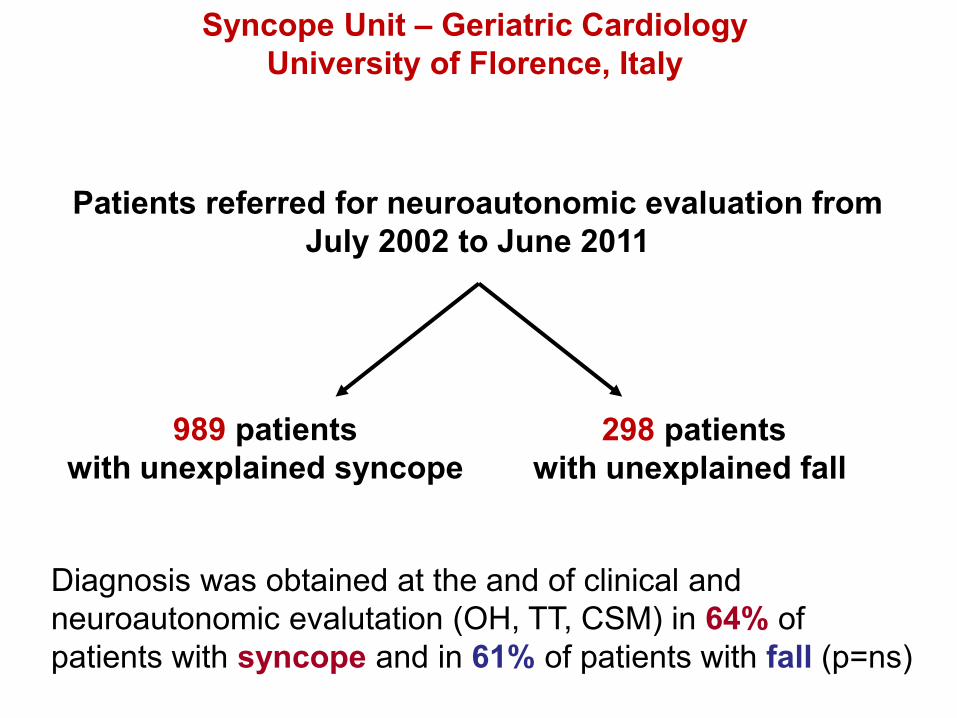
Syncope Unit – Geriatric Cardiology
University of Florence, Italy
Patients referred for neuroautonomic evaluation from
July 2002 to June 2011
989 patients
with unexplained syncope
298 patients
with unexplained fall
Diagnosis was obtained at the and of clinical and
neuroautonomic evalutation (OH, TT, CSM) in 64% of
patients with syncope and in 61% of patients with fall (p=ns)
0
4000
8000
12000
Pati
en
ts (
n)
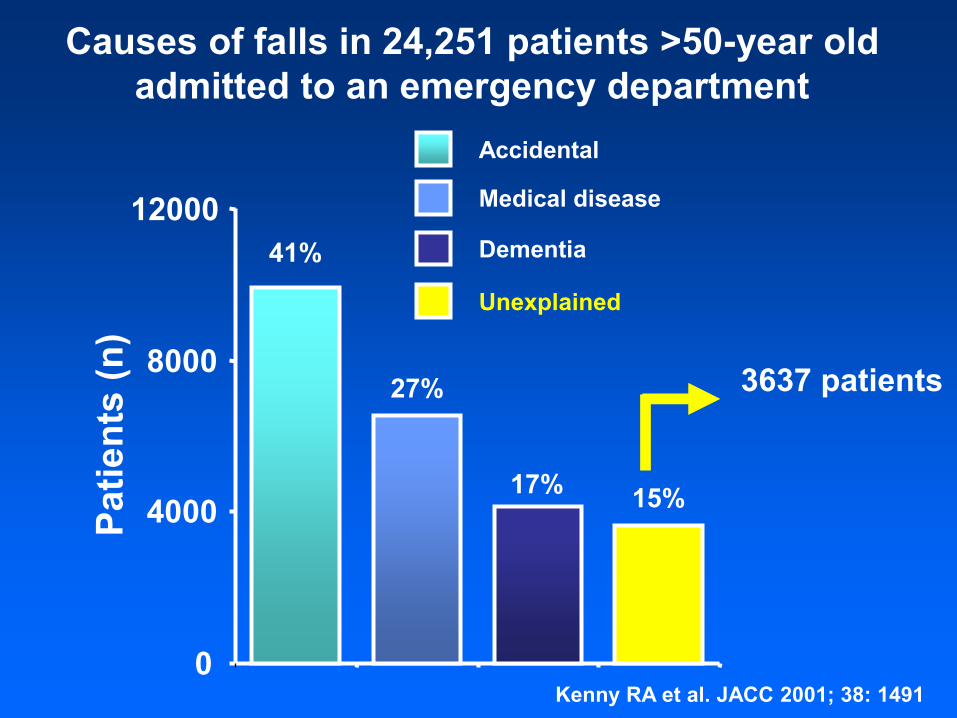
Causes of falls in 24,251 patients >50-year old
admitted to an emergency department
Kenny RA et al. JACC 2001; 38: 1491
Accidental
41%
Medical disease
27%
Dementia
17%
Unexplained
15%
3637 patients
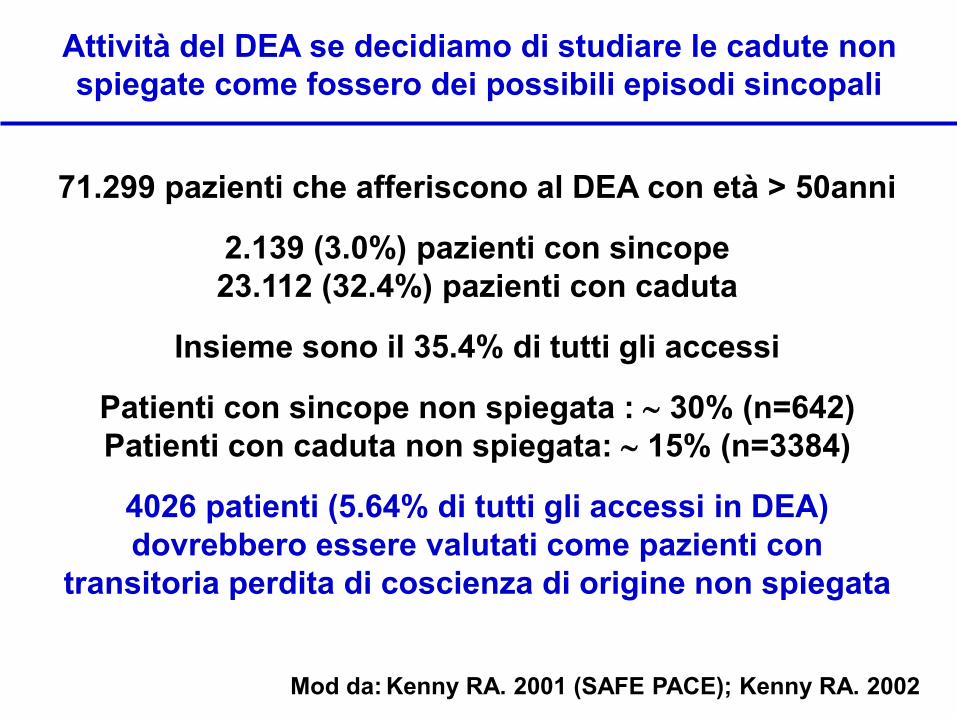
Attività del DEA se decidiamo di studiare le cadute non
spiegate come fossero dei possibili episodi sincopali
71.299 pazienti che afferiscono al DEA con età > 50anni
2.139 (3.0%) pazienti con sincope
23.112 (32.4%) pazienti con caduta
Insieme sono il 35.4% di tutti gli accessi
Patienti con sincope non spiegata : 30% (n=642)
Patienti con caduta non spiegata: 15% (n=3384)
4026 patienti (5.64% di tutti gli accessi in DEA)
dovrebbero essere valutati come pazienti con
transitoria perdita di coscienza di origine non spiegata
Mod da: Kenny RA. 2001 (SAFE PACE); Kenny RA. 2002
Attività del DEA se decidiamo di studiare le cadute non
spiegate come fossero dei possibili episodi sincopali
Abbiamo bisogno di
Syncope and Falls Unit
per valutare questi
pazienti
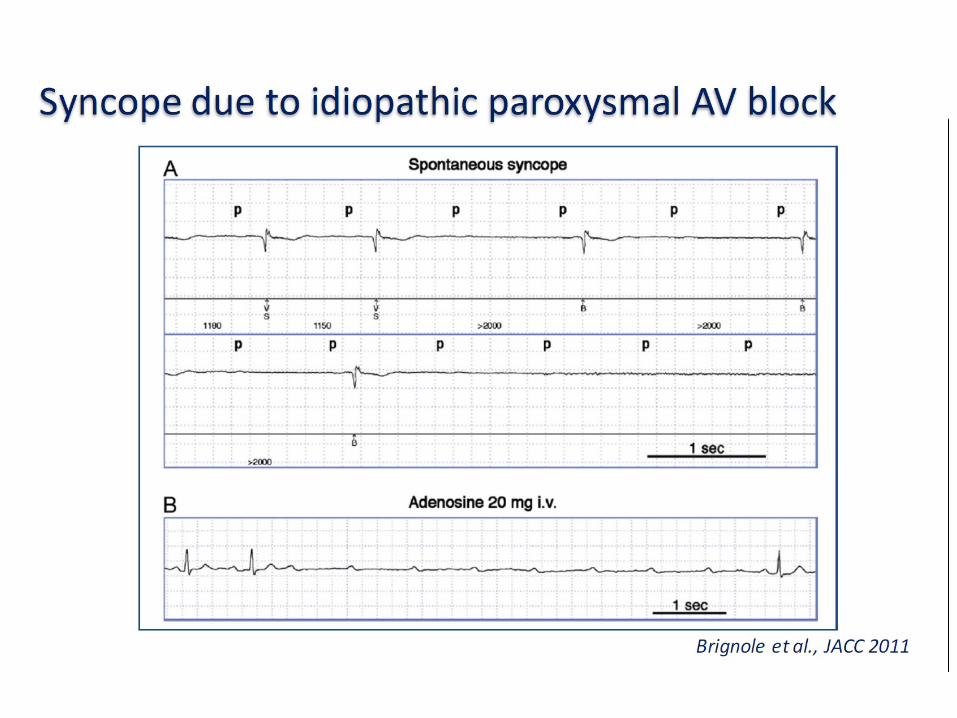
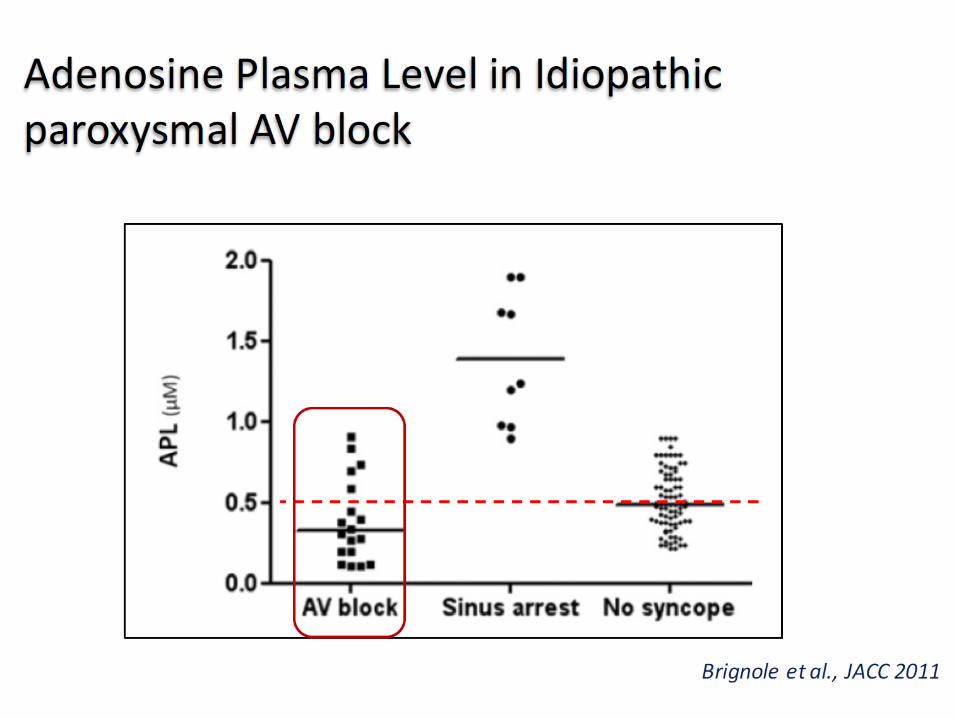
«La Sincope»
Due peculiarità:2. La sincope adenosino-
mediata
«La Sincope»
Grazie per la vostra attenzione