Linee Guida a confronto - Sito AcEMC 2017/Bellone.pdf · LA VENTILAZIONE NON INVASIVA nello...
45
LA VENTILAZIONE NON INVASIVA nello SCOMPENSO CARDIACO ACUTO: Linee Guida a confronto Andrea Bellone UOC di Pronto Soccorso- MURG Ospedale di Niguarda, Milano
Transcript of Linee Guida a confronto - Sito AcEMC 2017/Bellone.pdf · LA VENTILAZIONE NON INVASIVA nello...
LA VENTILAZIONE NON INVASIVA
nello SCOMPENSO CARDIACO ACUTO:
Linee Guida a confronto
Andrea Bellone
UOC di Pronto Soccorso- MURG
Ospedale di Niguarda, Milano

DEFINIZIONE
Rapida comparsa o peggioramento di
sintomi/segni compatibili con scompenso
cardiaco
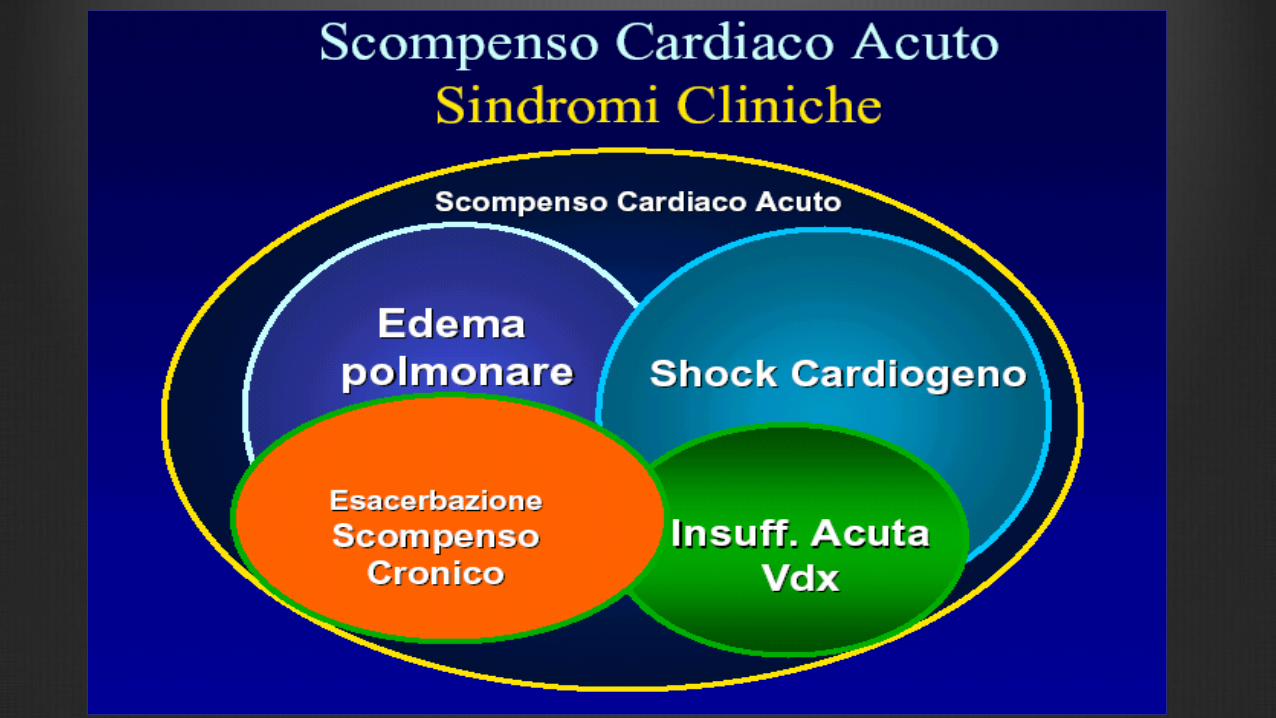
SCOMPENSO CARDIACO ACUTO
6/7/2011
6/7/2011
Scompenso
cardiaco
ipertensivo
LINEE GUIDA ESC 2016
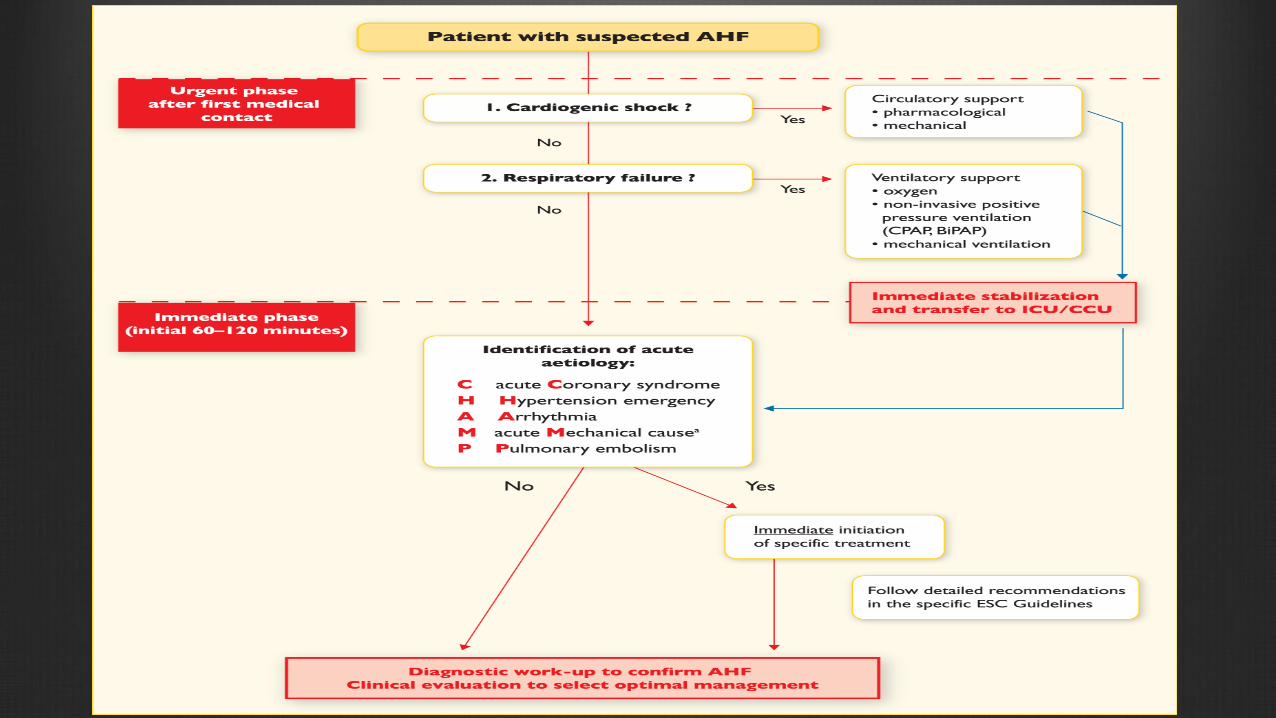
Recommendations (ESC 2016, EHJ)
Non-invasive positive pressure ventilation (CPAP, BiPAP) should be
considered in patients with respiratory distress (respiratory rate >25
breaths/min, SpO2 <90%) and started as soon as possible in order to
decrease respiratory distress and reduce the rate of mechanical
endotracheal intubation.
Non-invasive positive pressure ventilation can reduce blood pressure
and should be used with caution in hypotensive patients.
Blood pressure should be monitored regularly when this treatment is
used. IIa B
.
IOT (Esc 2016, EHJ)
Respiratory failure, leading to
•hypoxaemia (PaO2 <60 mmHg, 8.0 kPa)
•hypercapnia (PaCO2 >50 mmHg, 6.65kPa)
•acidosis (pH <7.35)
cannot be managed non-invasively
INDICAZIONI ALLA NIV
Indicazioni alla NIV (mandatorie)
•BPCO riacutizzata con pH < 7.35 e PaCO2>50 mmHg
•EPA cardiogeno e segni clinici/strumentali di EPA
•Svezzamento dalla VMI in pazienti BPCO
•Pazienti immunocompromessi e polmonite
Controindicazioni assolute
•Respiratory arrest
•Inable to fit mask
(Nava et Hill, Lancet 2009)
Controindicazioni relative
• Coma or confusion
• Inability to protect the airway
• Significant comorbility
• Vomiting
• Haemodynamic instability
• Orofacial abnormalities
• Obstructed bowel
• Recent abdominal surgery

REAL LIFE
TUTTI I PAZIENTI CHE GIUNGONO IN PS CON DISTRESS
RESPIRATORIO VENGONO IMMEDIATAMENTE AVVIATI ALLA NIV
NIV E IPOTENSIONE

NIV e IPOTENSIONE (real life)
• Non utilizzare NIV in pazienti ipotesi-ipoperfusi.
• Alternare cicli di NIV e vasodilatatori/diuretici
se pazienti ipotesi ma congesti.
• In corso di EPA diastolico il volume telediastolico
ventricolare sinistro non è ridotto e pertanto la NIV
indicata.
What is the role of noninvasive
ventilation in diastolic heart failure?Intensive Care Medicine 2005.
R Agarwal, D Gupta
“Caution must be used with CPAP because
patients with DHF are sensitive to the right
and left ventricular preload reduction and
may develop hypotension or several prerenal
azotemia”
The role of CPAP in ACPE with
preserved LVSF(Bellone A, Vettorello M, Etteri
M et al, Am J Emerg Medic 2009)
Patients: 36 patients were included in the study
(18 affected by DHF and 18 by SHF)
Interventions: All patients underwent a
morphologic echocardiographic investigation
shortly before CPAP
Resolution time did not differ significantly
between the 2 groups of patients
All patients improved vital signs and gas
exchange after CPAP
One patient of DHF group required
endotracheal intubation
No patient died
Results
NIV e IOT
IOT (Esc 2016, EHJ)
Respiratory failure, leading to
•hypoxaemia (PaO2 <60 mmHg, 8.0 kPa)
•hypercapnia (PaCO2 >50 mmHg, 6.65kPa)
•acidosis (pH <7.35)
cannot be managed non-invasively
24
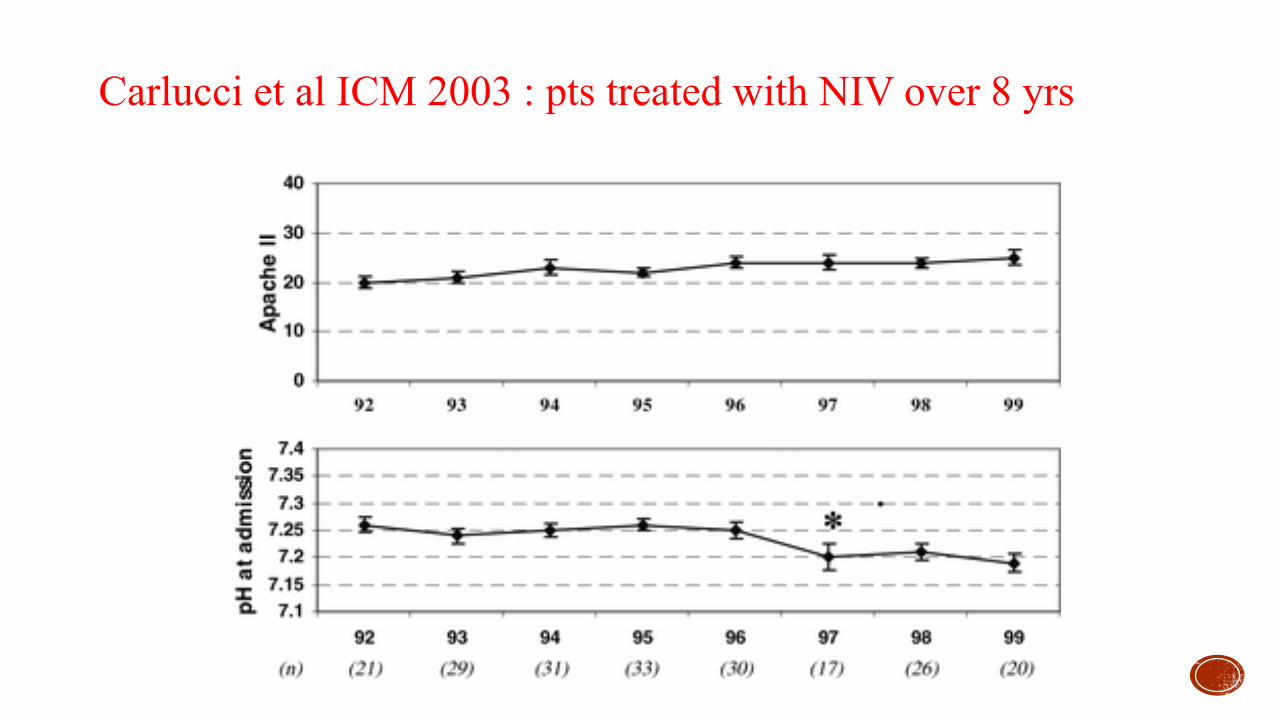
Carlucci et al ICM 2003 : pts treated with NIV over 8 yrs
Quando IOT
• Fallimento NIV/impossibilità alla protesi ventilatoria
• GASPING/arresto respiratorio
• Coma ipercapnico con depressione dei centri respiratori
• Piu’ di 3 controindicazioni relative
REAL LIFE
Il quesito è SE intubare non
QUANDO
L’Equivoco o il pregiudizio

• CPAP/BPAP migliorano gli scambi gassosi e la dispnea
• CPAP/BPAP non riducono la mortalità né il ricorso
all’intubazione rispetto ad O2 standard
(Gray et al NEJM 2008)
NIV e MORTALITA’

Limiti dello Studio
• Pazienti poco “compromessi”:
- pH 7.35 con PaO2 media = 98 mmHg
- tasso di intubazione del 3%
• Il 15% dei pazienti in O2 terapia (causa fallimento) è
“entrato” nel gruppo CPAP/BPAP ma l'outcome
favorevole è stato attribuito al braccio di randomizzazione
originario

Limite degli studi clinici randomizzati
- Il campione valutato non è mai omogeneo
- Nel contesto di una sindrome clinica esistono differenti
fenotipi clinici con differente prognosi e terapia
EFFETTI FAVOREVOLI della NIV in corso di EPA
•La NIV “riduce” i tempi di risoluzione dell'edema
•La NIV “migliora” gli scambi gassosi e “riduce” il distress
respiratorio
•La NIV “riduce” il ritorno venoso e la pressione transmurale
del ventricolo sinistro
•La NIV aumenta la CFR
NPPV in addition to standard medical care is an
effective and safe intervention for the treatment of adult
patients with acute cardiogenic pulmonary oedema.
The evidence to date on the potential benefit of NPPV
in reducing mortality is entirely derived from small-
trials.
Vital et al, Cochrane 2013 (Review)
Conclusioni
1) - Sempre piu’ linee guida e real life non sono in sintonia
2) - Sempre piu’ sono utili metanalisi e review rispetto a linee guida standard
3) - Protocolli-linee guida hanno consentito il superamento della medicina empirica e autoreferenziata ma sono strumenti a disposizione del quesito clinico-diagnostico-terapeutico
4) -LA NIV nell’EPA è una metodica sicura ed efficace

Grazie

NIV e MORTALITA'
Gray et al NEJM 2008:
- CPAP/BPAP migliorano gli scambi gassosi e la
dispnea
- CPAP/BPAP non riducono la mortalità né il ricorso
all'IOT rispetto ad O2 standard
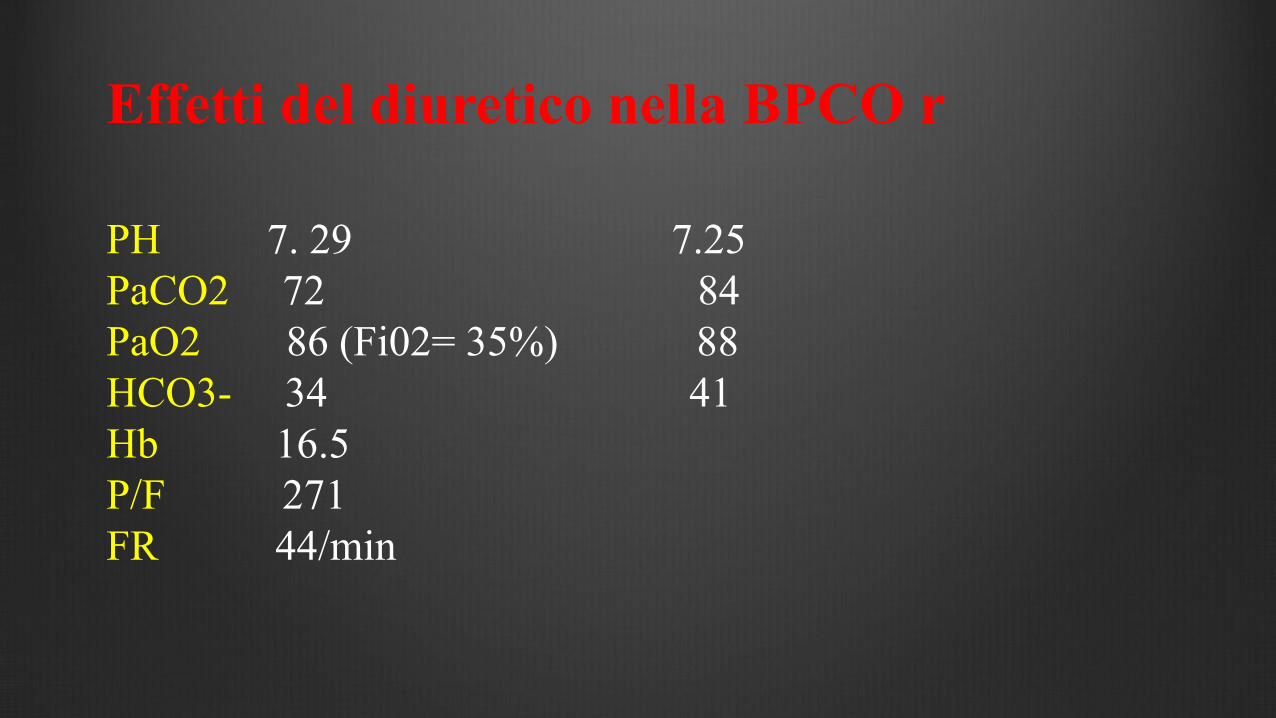
Effetti del diuretico nella BPCO r
PH 7. 29 7.25
PaCO2 72 84
PaO2 86 (Fi02= 35%) 88
HCO3- 34 41
Hb 16.5
P/F 271
FR 44/min
Impatto prognostico sfavorevole
-Aumentano i bicarbonati ematici
-Inibizione centri respiratori
-Aumenta la CO2 ematica
-Deplezione di volume
Indicazioni per NIV/CPAP in PS
-BPCO riacutizzata con pH<7.35, PaCO2>50mmHg, FR>25/min
-Insufficienza respiratoria ipossiemica e distress respiratorio
-EPA (segni clinici e distress respiratorio)

PINK PUFFERS BLUE BLOATERS
<20% BMI >28%
Absent EDEMA Present
>60 mmHg PaO2 <55 mmHg
<40 mmHg PaCO2 >45 mmHg
++++ Dyspnea ++
Absent Ht > 45 Present
Absent APH Present ???
V/Q
Perfusion Deficit ventilarory
Nella vita reale………….
Abbiamo selezionato correttamente i pazienti da
sottoporre a VNI ?
-Indicazione a IOT
-Indicazione a NIV
-Indicazione a O2+farmaci
-Indicazione a NIV palliativa
-Sedazione terminale
- GCS < 11
- APACHE II > 29
- RR > 30/min
- pH < 7.25
Have a predicted risk of failure > 70%
A pH < 7.25 after 2 hours NIV greatly increase the risk ( > 90%)
(Confalonieri et al, ERJ 2005)
Failure risk for NIV
Quando O2+farmaci
-Ph < 7.2 + distress respiratorio + sensorio alterato + condizioni generali compromesse (cachessia)
-Assenza di miglioramento dopo 2 ore di NIV e terapia
-Comorbilità severa
-Prognosi sfavorevole (IV stadio cronicità, pregressa IOT, O2LT/VMD, condizioni generali scadute/disordine cognitivo)

Prognosi sfavorevole
Svezzamento difficile
Comorbilità
Almeno 3 ricoveri/anno nei 3 anni precedenti
Malnutrizione/Ridotta autonomia/Disturbo cognitivo
Quando NIV palliativa
Palliative NIV can either be administered to offer a chance for survival or to alleviate the symptoms of respiratory distress in dying patients
(Intens Care Medic 2011)