EVOLUZIONE DELLA MALATTIA DI PARKINSON 13.11$all... · • Peggioramento della bradicinesia •...
21
EVOLUZIONE DELLA MALATTIA DI PARKINSON Dr. Massimo Moleri Direttore U.O. NEUROLOGIA CDC S. FRANCESCO
Transcript of EVOLUZIONE DELLA MALATTIA DI PARKINSON 13.11$all... · • Peggioramento della bradicinesia •...

EVOLUZIONE DELLA MALATTIA
DI PARKINSON
Dr. Massimo Moleri
Direttore U.O. NEUROLOGIA
CDC S. FRANCESCO

• L’evoluzione della malattia dipende da più
fattori:
• La progressione del processo degenerativo
• L’associazione di sintomi non motori
• La ridotta efficacia e le complicanze della
terapia nel tempo
Malattia di Parkinson: stadiazione clinica (Hoehn e Yahr)
• Stadio 1 m. unilaterale
• Stadio 1.5 m. unilaterale con coinvolgimento
assiale
• Stadio 2 m. bilaterale senza problemi di
equilibrio
• Stadio 2.5 m. bilaterale con recupero di
equilibrio dopo pull test
• Stadio 3 disabilitá lieve moderata con
qualche problema di equilibrio
• Stadio 4 disabilitá marcata. pz cammina.
• Stadio 5 pz. in sedia a rotelle o a letto

Malattia di Parkinson: evoluzione
clinica
Periodo Sintomi Durata
Preclinico Non evidenti Pochi o diversi anni
Prodromico Non specifici Mesi o anni
Sintomatico Parkinsoniani Finché é in vita
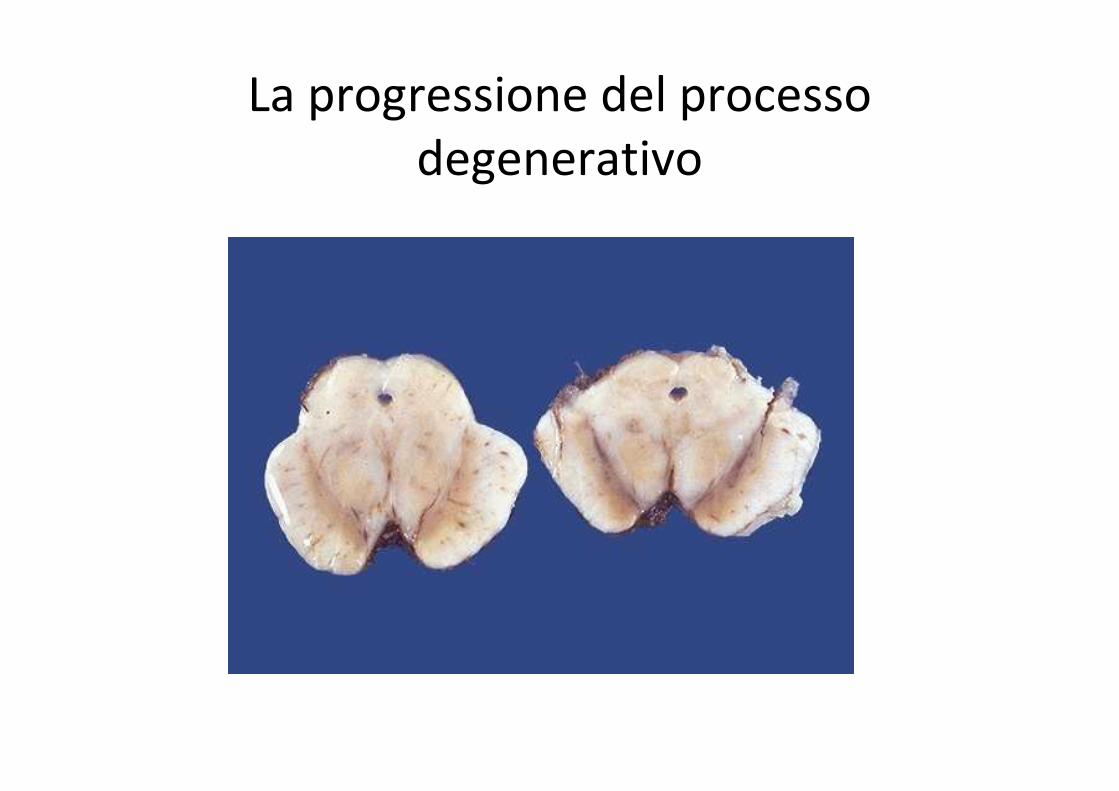
La progressione del processo
degenerativo

SPECT: 123I-FP-CIT
Controllo Tr. essenziale
SPECT in un soggetto
controllo, in un soggetto con
TE ed in uno con MP. Notare
la progressiva riduzione di
captazione a carico del
putamen
MP stadio I MP stadio II MP stadio III MP stadio IV

SEGNI MOTORI DELL’EVOLUZIONE
• Peggioramento della bradicinesia
• Aumento dell’ipertono
• Disturbi dell’equilibrio
• Deficit della deambulazione
• Ipofonia
• Disfagia
• Allettamento

� Complessivamente correlati alla durata ed alla gravità della malattia (Hely et et al, 2005)
� Impatto sulla qualità della vita dei pazienti(Schrag et al., 2000; Global Parkinson’s Disease Survey Steering Committee, 2002)
� Impatto sui costi assistenziali (Aarsland et al., 2000; Findley et al. 2003)
� Possono precedere l’insorgenza dei disturbi motori
I disturbi non motori nella malattia di Parkinson

� Il sintomo più frequente è costituito dalle allucinazioni, prevalentemente visive (Cummings, 1991)
� Più rari i deliri, prevalentemente persecutori (Factor et al, 1995)
� Gli stati confusionali ( delirium) sono associati a patologie concomitanti, all’etàavanzata o al trattamento con farmaci anticolinergici (Cummings, 1991)
Sintomi psicotici e malattia di Parkinson

Depressione vs gravitàdella malattia di Parkinson


Demenze e Parkinson
• Demenze con segni “parkinsoniani”
• Parkinson demenza
• Demenza a corpi di Lewy

Neurology
A 10-year study of the incidence of and factors predicting
dementia in Parkinson’s disease T. A. Hughes,, MD et al
• The association of age at onset of PD with incident dementia
was of only borderline significance. Multivariate analysis
found that age at entry into the study and severity of motor
symptoms were significant predictors of dementia but
duration of PD and age at onset of PD were not.
• CONCLUSIONS: Dementia in PD is likely to reflect interaction
of the neuropathology of the basal ganglia and age-related
pathology. The findings do not support the division of PD into
early and late-onset cases.
[The German Study on the Epidemiology of Parkinson's Disease with Dementia
(GEPAD): more than Parkinson]. Von Reichmann H, Deuschl G, Riedel O, Spottke A, Förstl H, Henn F, Heuser I, Oertel W, Riederer P, Trenkwalder C, Dodel R,
Wittchen HU
MMW Fortschr Med Apr 2010; 152 Suppl 1() :1-6
•
• Abstract
It is unknown, how frequently Parkinson's disease (PD) is complicated by
dementia, depression and other neuropsychiatric conditions. An epidemiologic
characterisation of the situation in specialised neurologic settings is lacking. The
Geman Study on the Epidemiology of Parkinson's Disease with Dementia (GEPAD)
isa national representative epidemiological study of n=1449 PD patients in n=315
office-based neurological settings, designed to estimate the prevalence of
dementia, depression and other neuropsychiatric conditions in patients with PD of
all stages by using standardized clinical assessments. RESULTS: 28.6% met
DSM-IV criteria for dementia. 33.6% met criteria for depression and 61%
additionally had other clinically significant psychopathological syndromes. Only
29.4% had no neuropsychiatric conditions. GEPAD reveals for the first time
comprehensively that the neuropsychiatric burden of PD patients in all stages and
even early stages is considerable, posing challenging questions for research and
clinical management.
Arch Neurol. 2005 Aug;62(8):1265-9.
Prognosis of Parkinson disease: risk of dementia and mortality: the Rotterdam Study.de Lau LM, Schipper CM, Hofman A, Koudstaal PJ, Breteler MM.
• Abstract
• BACKGROUND: Most prognostic studies on Parkinson disease have been hospital based or
have applied register-based case-finding methods. Potential under-representation of mild
cases may have given biased results.
• OBJECTIVE: To evaluate whether Parkinson disease is associated with an increased risk of
dementia and death.
• SETTING: General population.
• PARTICIPANTS: A total of 6969 participants, including 99 prevalent and 67 incident cases of
Parkinson disease.
• MAIN OUTCOME MEASURES: Incident dementia and death. Adjusted hazard ratios were
calculated through Cox proportional hazards regression analysis.
• CONCLUSIONS: Especially patients with Parkinson disease who carry an APOE epsilon2 allele
have an increased risk of developing dementia ( rischio aumentato 13 volte rispetto ai non
Parkinsoniani) Increased mortality risk in Parkinson disease is dependent on disease duration
and is only modest in the absence of dementia

Sono presenti in circa:
� il 50 % dei pazienti trattati con levodopa per almeno 5 anni (Poewe et al., 1988; Rascol et al, 2000)
� il 70 % dei pazienti trattati con levodopa per almeno 9 anni (Ahlskog and Muenter, 2001)
� la totalità dei pazienti con malattia ad esordio giovanile (Golbe, 1991)
Sono correlate alla dose di levodopa e, in pazienti con malattia ad esordio recente, dopo soli 9 mesi di terapia alla posologia di 200 mg x 3/die sono state
riscontrate nel 16-20 % dei casi (ELLDOPA study, 2004)
Fluttuazioni motorie e discinesie
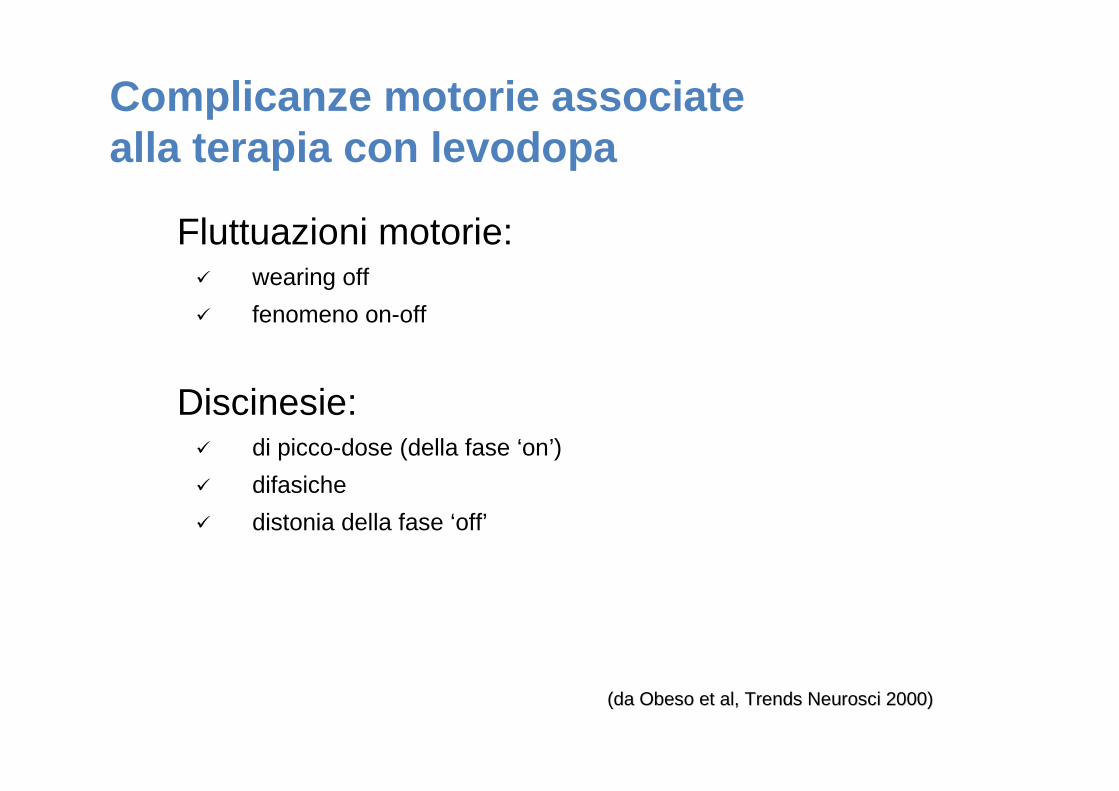
Fluttuazioni motorie:� wearing off
� fenomeno on-off
Discinesie:� di picco-dose (della fase ‘on’)
� difasiche
� distonia della fase ‘off’
Complicanze motorie associate alla terapia con levodopa
(da Obeso et al, (da Obeso et al, Trends NeurosciTrends Neurosci 2000)2000)

Tempo� Discinesie
�� Blocchi motori
Con
cent
razi
one
levo
dopa
Restringimento progressivo della finestra terapeutica per la somministrazione orale di levodopa

Disturbi motori che non rispondono alla terapia dopaminergica
Freezing della marcia e disturbi assiali in genere


GESTIONE DELL’EVOLUZIONE
• Neuroprotezione (rasagilina)
• Utilizzo dopaminoagonisti (fasi precoci)
• Entacapone
• DBS
• apomorfina s.c. o infusione continua
• Duodopa
• Antipsicotici atipici (dist. Psicotici e discinesie)
• Inib. Acetilcolinesterasi (demenze)