Epidemiologia e prevenzione - Gruppo Fides · • Indicazioni delle precauzioni da contatto •...
25
1 Paolo Durando Dipartimento di Scienze della Salute Scuola di Scienze Mediche e Farmaceutiche IRCCS AOU San Martino-IST, Università degli Studi di Genova Gruppo Tecnico Regionale per il Controllo delle Infezioni Correlate all’Assistenza Società Italiana Multidisciplinare per la Prevenzione delle Infezioni nelle Organizzazioni Sanitarie (SIMPIOS) – Sezione Liguria I Sessione: Le infezioni nosocomiali: quale gestione nelle strutture residenziali assistite? Epidemiologia e prevenzione Host Microrganisms Environment (setting, procedures, HCWs behaviour) HEALTH CARE-ASSOCIATED INFECTIONS THE RESULT OF A DINAMIC INTERACTION Prevalenza di Infezioni Correlate all’Assistenza (ICA): studi italiani pubblicati fra il 2000 e oggi 88 Ospedali 18667 Pazienti arruolati 10 Ospedali 1315 Pazienti arruolati 59 Ospedali 9467 Pazienti arruolati 15 Ospedali 2165 Pazienti arruolati 51 Ospedali 9609 Pazienti arruolati 25 Ospedali 3176 Pazienti arruolati 912 Pazienti arruolati % 21 Ospedali 6352 Pazienti arruolati
Transcript of Epidemiologia e prevenzione - Gruppo Fides · • Indicazioni delle precauzioni da contatto •...
1
Paolo Durando
Dipartimento di Scienze della SaluteScuola di Scienze Mediche e Farmaceutiche
IRCCS AOU San Martino-IST, Università degli Studi di GenovaGruppo Tecnico Regionale per il Controllo delle Infezioni Correlate all’Assistenza
Società Italiana Multidisciplinare per la Prevenzione delle Infezioni nelle Organizzazioni Sanitarie (SIMPIOS) – Sezione Liguria
I Sessione:
Le infezioni nosocomiali: quale gestione nelle strutture residenziali assistite?
Epidemiologia e prevenzione
Host
Microrganisms Environment(setting, procedures,
HCWs behaviour)
HEALTH CARE-ASSOCIATED INFECTIONSTHE RESULT OF A DINAMIC INTERACTION
Prevalenza di Infezioni Correlate all’Assistenza (ICA): studi italiani pubblicati fra il 2000 e oggi
88 Ospedali18667 Pazienti
arruolati
10 Ospedali1315 Pazienti
arruolati
59 Ospedali9467 Pazienti
arruolati
15 Ospedali2165 Pazienti
arruolati
51 Ospedali9609 Pazienti
arruolati
25 Ospedali3176 Pazienti
arruolati
912 Pazientiarruolati
%
21 Ospedali6352 Pazienti
arruolati

2
Infection control and quality health care:current challenges and future perspectives
Pittet D, AJIC 2005
, A/H1N1, MERS-CoV, Ebola…
Resistance in Enterobacteriaceae:impact and ability of
different β-lactamases
Livermore DM, K J Intern Med 2012Cosgrove SE et al, Arch Int Med 2002
3
MultiDrug Resistance of Gram-Negative Bacilli (MDR-GNB): an important clinical and public health issue
Emergence of resistance to multiple antimicrobial agents in pathogenic GNB has become a significant
public health threat, having a significant impact on morbidity, mortality (risk estimated nearly 2-3 times)
and on LOS and health-related costs.
The greater problem is for empirical theraphy, where growing resistance increases the risk that the
antimicrobial used will prove inactive: in particular, highly-resistant Gram-negative bacteria e.g.
multidrug-resistant carbapenemase-producing Klebsiella pneumoniae and Acinetobacter spp. can be
resistant to all currently available antimicrobial agents or remain susceptible only to older, potentially
more toxic agents like the polymyxins, leaving limited and suboptimal options for treatment.
Antibiotic treatment options for multidrug-resistant GNB are often very limited and finding an appropriate
drug is an increasing challenge since very few new antibiotics are expected to enter the market as the
older classes lose their efficacy
Testing and evaluation of antibiotic lead substances should identify epidemiologically frequent and
clinically relevant resistance mechanisms, as a basis for recommended hygiene measures in patient
care.
Magiorakos AP et al, Clin Microbiol Infect 2012; de Kraker ME et al, J Antimicrob Chemother 2011; ECDC 2011;MMWR 2009; Roberts RR et al, Clin Infect Dis 2009; Falagas ME et al Clin Infect Dis 2008, Pitout JDD Lancet Infect Dis 2008
Antimicrobial resistance data from invasive isolates (blood and cerebrospinal fluid) reported to EARS-Net by 29 EU/EEA countries in
2012 (data referring to 2011), and on trend analyses of EARSS/EARS-Net data reported by the participating countries during the
period 2008 to 2011
2009
2010
Klebsiella pneumoniae. Percentage (%) of invasive isolates with resistanceto carbapenems, by country, EU/EEA countries, 2009-2013.
European Centre for Disease Prevention and Control. Antimicrobial resistance surveillance in Europe. Annual Report of the European Antimicrobial Resistance Surveillance Network (EARS-Net). 2009-2013.
2013
2012
2011
Dramatic increase in Carbapenem-ResistantKlebsiella Pneumoniae in Italy (I)

4
Dramatic increase in Carbapenem-ResistantKlebsiella Pneumoniae in Italy (II)
Escherichia coli: trends of invasive isolates with combined resistance (resistant to fluoroquinolones, third generation cephalosporins and
aminoglycosides), by country, EU/EEA countries, 2008–2011
A trend analysis showed increasingtrends for Greece, Cyprus, Hungaryand Italy (p < 0.01)
EARS-Net collects data on invasivebacterial isolates, which likelycorrespond to a fraction of the totalnumber of infections.
Increasing reports of community casessuggest that dissemination ofcarbapenem-resistant K. pneumoniaehas penetrated into the community.
Good surveillance and infection controlmeasures are urgently needed tocontain this spread.
The rise of carbapenem resistance in Europe:just the tip of the iceberg?
Magiorakos et al.Antimicrobial Res Infect Control 2013

5
The results highlight the emergence of carbapenemase-producing K. pneumoniae strains in different hospitals and wards and the urgent need for infection control, antibiotic stewardship
programmes and utilization of a surveillance and prevention system
Results (II)
Multivariate analysis adjustedfor appropriate treatment,combination therapy andinfectious-source removal,showed the following asindependent risk factors formortality:
Univariate analysis of risk factors for in-hospital mortality among 91 patients infected by carbapenem-resistant Klebsiella
pneumoniae (CR-KP)
BackgroundFrom January 2007 to May 2010, the five ICUs of the San MartinoUniversity Hospital, Genoa, Italy, experienced sequential outbreaks of A.baumannii infection.
Aims
(i) to study the population structure of A. baumannii and identify the spread of epidemic clones in the San Martino hospital;
(ii) to compare characterization data obtained using different molecularapproaches and evaluate their utility in molecular investigation;
(iii) to study the emergence of antimicrobial resistance.

6
Cases of infections caused by A. baumannii among ICUs and other wards by the most frequently found genotypes of carbapenem-resistant A. baumannii
In ICUs, 27 (50.9%) and 26 (49.1%) patients were colonized and infected, respectively.
The mean age for colonized and infected patients was 68.5 and 56.2 years, respectively.
• BSI: 53.8%• VAP: 19.2%• Complicated skin and soft tissue infections: 11.5% • meningitis or urinary tract infection: 7.7%
Among infected patients admitted in ICUs, the fatality rate was 33.3%.
6 Epidemic clusters of A. baumannii
Antimicrobial susceptibility patterns of Acinetobacter baumannii isolates belonging to the most frequently found genotypes:
ST4, ST118, ST95
Most A. baumannii isolates were multidrug-resistant.
The majority of the strains typed were resistant to ampicillin-sulbactam,piperacillin-tazobactam, broad spectrum cephems and fluoroquinolones, butsusceptible to colistin.
This pattern may have contributed to the rapid and successful spread.

7
Geographical distribution of
Clostridium difficile PCR ribotypes in
European countries with more than
five typable isolates, November, 2008
Rybotypes 018, 056, 027 are
usually associated with complicated disease outcome

8
Con legge regionale n. 2/2011 è stata costituitol'IRCCS AOU San Martino – IST di Genova, aseguito dell'accorpamento dell’AOU SanMartino e dell'Istituto Scientifico Tumori. Ilnuovo Istituto è stato costituito dal 1°settembre 2011, a seguito del riconoscimentodel carattere scientifico per la disciplina diOncologia, con conseguente estinzione dei duepregressi enti.
L'Istituto è costituito da 6 Dipartimenti adAttività Integrata:
Dipartimento di Chirurgia generale,specialistica e oncologica
Dipartimento di Neuroscienze edOrgani di senso
Dipartimento di Medicina InternaGenerale e Specialistica
Dipartimento di Emergenza edAccettazione
Dipartimento delle TerapieOncologiche Integrate
Dipartimento della Diagnostica, dellapatologia e delle cure ad altacomplessità tecnologica
Ospedale di riferimento regionale per acuti Numero di posti letto ordinari (anno 2013): circa 1200 Numero di ricoveri ordinari (anno 2013): circa 45.000 Numero di accessi totali (anno 2013): circa 90.000 Giornate di degenza (media 2011 – 2013): 473.810
HAI surveillance and control activities atI.R.C.C.S. AOU San Martino – IST Genoa, Italy
Laboratory surveillance of alert microrganisms for all hospital wards
Point-prevalence surveys
Carbapenemase-producing Enterobacteriacee (CPE)-BSI passive surveillance
CPE-Colonization Screening in patients and hospital wards at higher risk
Active surveillance of environmental cleaning and decontamination procedures
Active surveillance of health-care workers adherence and compliance with HAIprevention measures (i.e. hand hygiene, perioperative antimicrobial prophylaxis)
Antimicrobial stewardship
SORVEGLIANZA DEI MICRORGANISMI SENTINELLA
ANALISI DATI 2012-2013
Valutazione semestrale prevista nel 2014
IRCCS Azienda Ospedaliera Universitaria San Martino ‐ ISTIstituto Nazionale per la Ricerca sul CancroLargo Rosanna Benzi, 10 16132 GENOVA

9
FLUSSO INFORMATIVONel momento in cui il Laboratorio referta un esame ed inserisce i dati nelprogramma di Laboratorio, il dato viene rilevato dal sistema informatico“Controllo infezioni ospedaliere” che, in automatico, invia una mail allaDirezione Sanitaria e al Team ICA.Contemporaneamente il referto è leggibile presso l’U.O. di interesse suLaboWeb.
L’U.O. Igiene ed Epidemiologia Ospedaliera invia, via fax, il modulo “SCHEDA DI SEGNALAZIONE DIISOLAMENTO DI MICRORGANISMO SENTINELLA” MODAZHEP_0044 all’U.O. di pertinenza. In talemodulo è riportato:Indicazione della U.O. (Padiglione, CdC, fax)• Data, nome del paziente, microrganismo isolato, sede di isolamento• Indicazioni delle precauzioni da contatto• Consulenza infettivologo• Data e firma di chi segnala• Data e firma del ricevente.
Il fax datato e firmato dal ricevente, dovrà essere inserito dal Medico di reparto nella cartella clinica delpaziente.L’U.O. provvede ad attuare le misure specifiche previste dalle procedure:- LGAZHEP_0002 “RACCOMANDAZIONI PER LE MISURE DI ISOLAMENTO IN OSPEDALE”- IOAZHEP_0044 “GESTIONE E SORVEGLIANZA PAZIENTI COLONIZZATI/INFETTI DA MICRORGANISMISENTINELLA”
Primi Isolamenti dei Principali Microrganismi Alert
* Trattandosi di un patogeno endemico la sorveglianza è stata sospesa a marzo 2013
* 608

10
Studio di prevalenza delle infezioni correlate all’assistenza all’interno dell’I.R.C.C.S. S. Martino – IST
Gennaio - Febbraio 2014
Complessivamente sono stati inclusi nello studio 956 pazienti ricoverati in 74 reparti ospedalieriafferenti a 5 Dipartimenti ad Attività Integrata.
Perc
entu
ale
di p
azie
nti
Anni
63,9%34,4%1,7%

11
Perc
entu
ale
di p
azie
nti
Perc
entu
ale
di p
azie
nti
Analisi multivariata: principali ICA (overall e per singolalocalizzazione) e valutazione dei fattori di rischio associati
Durando P et al., J Hosp Infect 2009
12
Durata della degenza (giorni)
TotaleIRCCS(n=956)
MED(n=556)
SUR(n=236)
RHB(n=50)
ICU(n=43)
PSY(n=30)
GO(n=27)
PED(n=14)
Media 12,9 12,1 10,3 27,9 29,0 11,8 3,2 5,9
Mediana 7 8 6 22 20 7 3 4
IQR 3-16 4 – 15,5 2 - 12 10 - 38 10 - 39 2 - 13 1 - 6 2 – 7
Range 0-139 1 - 129 0 - 139 1 - 102 2 - 103 0 - 133 0 - 7 0 - 17
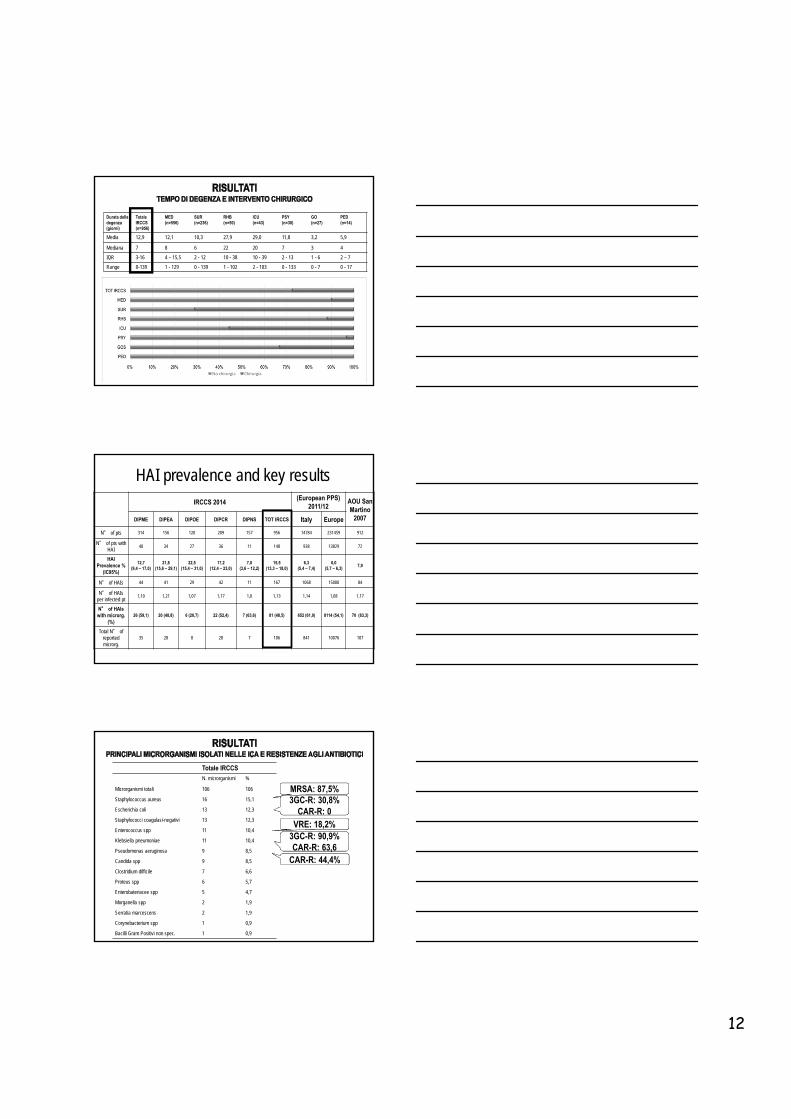
HAI prevalence and key resultsIRCCS 2014
(European PPS) 2011/12
AOU San Martino
2007DIPME DIPEA DIPOE DIPCR DIPNS TOT IRCCS Italy Europe
N° of pts 314 156 120 209 157 956 14784 231459 912
N° of pts withHAI
40 34 27 36 11 148 938 13829 72
HAI Prevalence %
(IC95%)
12,7(9,4 – 17,0)
21,8(15,6 – 29,1)
22,5(15,4 – 31,0)
17,2(12,4 – 23,0)
7,0(3,6 – 12,2)
15,5(13,3 – 18,0)
6,3(5,4 – 7,4)
6,0 (5,7 – 6,3)
7,9
N° of HAIs 44 41 29 42 11 167 1068 15000 84
N° of HAIsper infected pt
1,10 1,21 1,07 1,17 1,0 1,13 1,14 1,08 1,17
N° of HAIswith microrg.
(%)26 (59,1) 20 (48,8) 6 (20,7) 22 (52,4) 7 (63,6) 81 (48,5) 652 (61,0) 8114 (54,1) 70 (83,3)
Total N° ofreportedmicrorg.
35 28 8 28 7 106 841 10076 107
Totale IRCCSN. microrganismi %
Microrganismi totali 106 106
Staphylococcus aureus 16 15,1
Escherichia coli 13 12,3
Staphylococci coagulasi-negativi 13 12,3
Enterococcus spp 11 10,4
Klebsiella pneumoniae 11 10,4
Pseudomonas aeruginosa 9 8,5
Candida spp 9 8,5
Clostridium difficile 7 6,6
Proteus spp 6 5,7
Enterobateriacee spp 5 4,7
Morganella spp 2 1,9
Serratia marcescens 2 1,9
Corynebacterium spp 1 0,9
Bacilli Gram Positivi non spec. 1 0,9
MRSA: 87,5%3GC-R: 30,8%
CAR-R: 0VRE: 18,2%
,3GC-R: 90,9%CAR-R: 63,6
CAR-R: 44,4%

13
IRCCS 2014
UA1D1 UA1D2TOT
UA1DHAND1 HAND4
TOTHAND
TOTICU
N HAIs Rel % N HAIs Rel % N HAIs Rel % N HAIs Rel % N HAIs Rel % N HAIs Rel % N HAIs Rel %
Day of HAI onset
Day 1 – 2 0 - 0 - 0 - 1 16,7 0 - 1 6,7 1 3,6
Day 3 - 4 2 18,2 0 - 2 15,4 0 - 0 - 0 - 2 7,1
Day 5 – 7 2 18,2 0 - 2 15,4 0 - 1 11,1 1 6,7 3 10,7
Day 8 - 14 1 9,1 0 - 1 7,7 2 33,3 2 22,2 4 26,6 5 17,9
Day 15 - 21 2 18,2 0 - 2 15,4 1 16,7 2 22,2 3 20 5 17,9
> Day 21 4 16,4 2 100 6 46,2 2 33,3 4 44,5 6 40 12 42,9
HAIs with onset during currenthospitalization in ICUs
Patients with positive culture for carpapenem-resistantKlebsiella pneumoniae (any site, only first isolate) at I.R.C.C.S.
San Martino – IST Genoa, Italy (years 2008-2013)
June 2012: mandatory screening

14
Mortalità per tutte le cause a 30 giorni: analisi univariataN Pazienti/totale (%) OR CI95% P-value
Sopravvissuti (n=298) Deceduti (n=164)Caratteristiche demograficheSesso (M/F) 188/291 (64,60%) 103/291 (35,40%) 0,99 0,67 - 1,47 0,95Età40< 33/41 (80,49%) 8/41 (19,51%) ref40-49 29/32 (90,63%) 3/32 (9,38%) 0,43 0,10 - 1,76 0,2450-59 40/56 (71,43%) 16/56 (28,57%) 1,65 0,63 - 4,33 0,3160-69 71/112 (63,39%) 41/112 (36,61%) 2,38 1,01 - 5,64 0,0570-79 89/156 (57,05%) 67/156 (42,95%) 3,11 1,35 - 7,16 0,008≥80 36/65 (55,38%) 29/65 (44,62%) 3,32 1,33 - 8,29 0,01Condizioni di comorbositàNeoplasia 83/134 (61,94%) 51/134 (38,06%) 1,16 0,77 - 1,77 0,46Infezioni 89/149 (59,73%) 60/149 (40,27%) 1,35 0,91 - 2,03 0,14Intervento chirurgico 163/244 (66,80%) 81/244 (33,20%) 0,81 0,55-1,18 0,27Charlson comorbidity index0 18/22 (81,82%) 4/22 (18,18%) ref1-2 30/35 (85,71%) 5/35 (14,29%) 0,75 0,18 - 3,16 0,703 32/37 (86,49%) 5/37 (13,51%) 0,70 0,17 - 3,0 0,634 41/63 (65,08%) 22/63 (34,92%) 2,41 0,73 - 8,02 0,15≥5 177/305 (58,03%) 128/305 (41,97%) 3,25 1,08 - 9,85 0,04Pattern di resistenzaResistenza ai carbapenemi 191/317 (60,25%) 126/317 (39,75%) 1,86 1,2-2,86 0,005Area specialistica di insorgenzaICU 142/237 (59,92%) 95/237 (40,08%) 3,43 1,71 - 6,89 0,0005MED 84/138 (60,87%) 54/138 (39,13%) 3,31 1,59 - 6,88 0,001RHB 18/22 (81,82%) 4/22 (18,18%) 1,20 0,34 - 4,25 0,78SUR 58/69 (84,06%) 11/69 (15,94%) ref
Mortalità per tutte le cause in pazienti affetti
da BSI da CRKP a 30 giorni 39,75%
Mortalità per tutte le cause in pazienti affetti
da BSI da CSKP a 30 giorni 26,21%
Stimare l’incidenza delle infezioni da Clostridium difficile acquisitedurante il ricovero presso l’IRCCS San Martino – IST di Genova
Stimare la mortalità da tutte le cause nei 30 giorni successiviall’infezione da Clostridium difficile
Descrivere le caratteristiche demografiche e cliniche dei pazienti coninfezione da Clostridium difficile acquisite durante il ricovero pressol’IRCCS San Martino – IST di Genova
Descrivere i fattori di rischio correlati alla mortalità da tutte le causenei 30 giorni successivi all’infezione da Clostridium difficile
Studio retrospettivo basato sulla definizione di caso del NationalHealth Safety Network (NHSN) di Laboratory Identified Event (LabIDEvent):« A case of CDI is defined as a positive laboratory test result (nonduplicative) for C. difficile toxin A and/or B, or a toxin-producing C.difficile organism detected by culture or other laboratory meansperformed on a stool sample»
Incident (new case) CDI Assay: AnyLabID Event from a specimenobtained >8 weeks after the mostrecent LabID Event (or with noprevious LabID Event documented)for that patient.
Recurrent CDI Assay: Any LabIDEvent from a specimen obtained >2weeks and ≤8 weeks after the mostrecent LabID Event for that patient.

15
Sulla base delle tempistiche della diagnosi di CDI e della storia clinicadel paziente, le CDI sono state ulteriormente categorizzate comeprescritto dal NHSN
Healthcare Facility–Onset (HO):CDI identified >3 days after admissionto the facility (i.e., on or after day 4)
Community-Onset Healthcare Facility–Associated (CO-HCFA): Community onsetCDI identified from a patient who wasdischarged from the facility ≤4 weeks prior tocurrent date of stool specimen collection
Community-Onset (CO): CDIidentified as an outpatient or aninpatient ≤3 days after admissionto the facility (i.e., before or ondays 1, 2, or 3 of admission).
3282 stool specimens tested(from April 2010 to August 2014)
450 positive specimens (13,7%)
374 patients
Correction for duplicate positivitesand CDI recurrences
348 patients
Excluded 26 community onset or community onset healthcare facilityassociated CDI patients
Totale Test
Totale positivi Nuovi casi totali(>56 giorni)
Recidive(≤56; >14 giorni)
Duplicati(< 14 giorni)
Healthcare Facility onsetHO-CDI (nuovi casi)
2010A 277 24 (8,7%) 21 2 1 192011 442 38 (8,6%) 35 1 2 32
2012 678 82 (12,1%) 75 6 1 742013 1122 164 (14,6%) 134 15 15 1272014B 813 142 (17,5%) 109 11 22 96A i dati iniziano dal 1/4/2010B i dati arrivano fino al 31/8/2014C Healthcare Facility-Onset (HO): CDI identified > 3 days after admission to the facility (or after day 4)
0
0,05
0,1
0,15
0,2
0,25
0,3
0,35
0,4
0,45
0,5
0,55
0,6
0,65
apr-1
0
giu-
10
ago-
10
ott-1
0
dic-
10
feb-
11
apr-1
1
giu-
11
ago-
11
ott-1
1
dic-
11
feb-
12
apr-1
2
giu-
12
ago-
12
ott-1
2
dic-
12
feb-
13
apr-1
3
giu-
13
ago-
13
ott-1
3
dic-
13
feb-
14
apr-1
4
giu-
14
ago-
14
+3 Standard Deviation
+2 Standard Deviation
+1 Standard Deviation
Meanper 1
000
patie
ntda
ys
Hospital Onset – Clostridium difficile Infection (HO-CDI) incidence atI.R.C.C.S. San Martino – IST Genoa, 2010 – 2014
2010 2011 2012 2013 2014N° Hosp.
daysIncidence (x 1000 pd)
N° Hosp. days
Incidence (x 1000 pd)
N° Hosp. days
Incidence (x 1000 pd)
N° Hosp. days
Incidence (x 1000 pd)
N° Hosp. days
Incidence (x 1000 pd)
Tot IRCCS 19 351450 0,05 32 485309 0,07 74 475438 0,16 127 460683 0,28 96 298006 0,32
MED 9 187399 0,05 24 250474 0,10 54 240704 0,22 53 223616 0,24 59 152190 0,39
SUR 3 93908 0,03 1 130901 0,01 1 123733 0,01 5 117828 0,04 6 73923 0,08
ICU 3 12613 0,24 0 18521 0,00 3 16451 0,18 4 14940 0,27 1 10387 0,10
RHB 4 17669 0,23 7 33423 0,21 15 45487 0,33 65 62927 1,03 30 34347 0,87

16
29,4
17,7
72,7
18,7
0
10
20
30
40
50
60
70
80
Area medica Area chirurgica Area terapia intensiva Area riabilitativa elungo-degenza
%
p value = 0,0005
A steady stream of new antibiotics aimed at MDR Gram-negative bacteriawould be welcome, but this alone might make a relatively modest impacton clinical outcomes.
Much more effective would be innovative approaches to reducing thelikelihood of colonization and subsequent infection, thereby reducing boththe need to use antibiotics at all and the constant pressure leading tomultiple antibiotic resistance.
Such strategies are likely to be more effective in the long term thanrelying on a pipeline of antibiotics that will only ever have a limitedlifespan.
It is not antibiotic resistance genes that kill people, it is bacteria…
Cohen J, Antimicrob Chemother 2013
Strategie per il controllo delle infezioni
Misure generali Sorveglianza Precauzioni standard Misure aggiuntive (isolamento, ecc.)
Antibiotico profilassi e terapia
Misure specifiche (Immunoprofilassi)
Specificamente dirette contro: Infezioni del Tratto Urinario Infezioni del Sito Chirurgico Infezioni Respiratorie (es., VAPs) Sepsi (es., CR-BSIs) ……
17
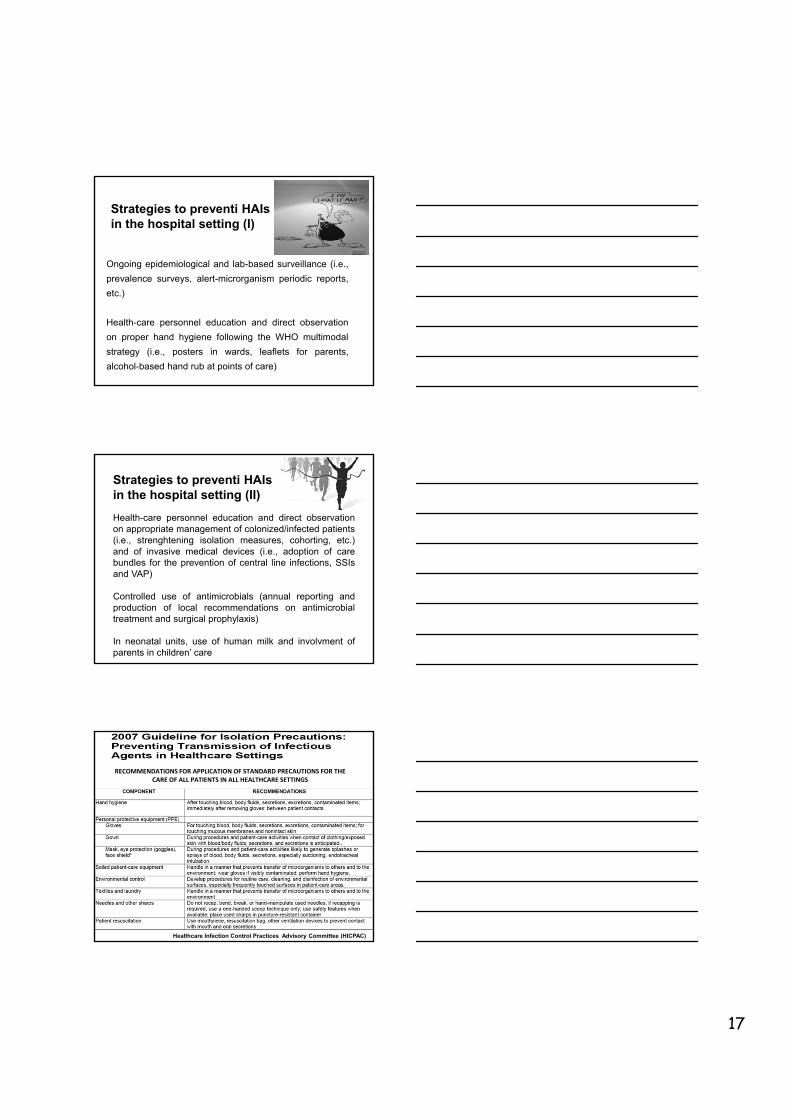
Strategies to preventi HAIs in the hospital setting (I)
Ongoing epidemiological and lab-based surveillance (i.e.,
prevalence surveys, alert-microrganism periodic reports,
etc.)
Health-care personnel education and direct observation
on proper hand hygiene following the WHO multimodal
strategy (i.e., posters in wards, leaflets for parents,
alcohol-based hand rub at points of care)
Strategies to preventi HAIs in the hospital setting (II)
Health-care personnel education and direct observationon appropriate management of colonized/infected patients(i.e., strenghtening isolation measures, cohorting, etc.)and of invasive medical devices (i.e., adoption of carebundles for the prevention of central line infections, SSIsand VAP)
Controlled use of antimicrobials (annual reporting andproduction of local recommendations on antimicrobialtreatment and surgical prophylaxis)
In neonatal units, use of human milk and involvment ofparents in children’ care
RECOMMENDATIONS FOR APPLICATION OF STANDARD PRECAUTIONS FOR THE CARE OF ALL PATIENTS IN ALL HEALTHCARE SETTINGS
51
Healthcare Infection Control Practices Advisory Committee (HICPAC)

18
RECOMMENDATIONS FOR APPLICATION OF STANDARD PRECAUTIONS FOR THE CARE OF ALL PATIENTS IN ALL HEALTHCARE SETTINGS
52Healthcare Infection Control Practices Advisory Committee (HICPAC)
Impatto della promozione dell’igiene delle mani Negli ultimi 30 anni, oltre 20 studi hanno dimostrato l’efficacia nel ridurre le ICPA
Year Hospital setting
Increase of hand hygiene compliance Reduction of HCAI rates Follow-up Reference
1989 Adult ICU From 14% to 73% (before pt contact)
HCAI rates: from 33% to 10% 6 years Conly et al
2000 Hospital-wide From 48% to 66% HCAI prevalence: from 16.9% to 9.5% 8 years Pittet et al
2004 NICU From 43% to 80% HCAI incidence: from 15.1 to 10.7/1000 patient-days 2 years Won et al
2005 Adult ICUs From 23.1% to 64.5% HCAI incidence: from 47.5 to 27.9/1000 patient-days 21 months Rosenthal et al
2005 Hospital-wide From 62% to 81% Significant reduction in rotavirus infections 4 years Zerr et al
2007 Neonatal unit From 42% to 55% HCAI incidence: overall from 11 to 8.2 infections/1000 patient-days) and in very low birth weight neonates from 15.5 to 8.8 infections /1000 patient-days
27 months Pessoa-Silva et al
2007 Neurosurgery NA SSI rates: from 8.3% to 3.8% 2 years Thu et al
2008 1) 6 pilot health-care facilities2) all public health-care facilities in Victoria (Aus)
1) from 21% to 48%2) from 20% to 53%
MRSA bacteraemia: 1) from 0.05 to 0.02/100 patient-discharges per month; 2) from 0.03 to 0.01/100 patient-discharges per month
1) 2 years2) 1 year
Grayson et al
2008 NICU NA HCAI incidence: from 4.1 to 1.2/1000 patient-days 18 months Capretti et al
Author Year Sector Compliance
Preston 1981 General Wards
ICU
16%
30%
Albert 1981 ICU
ICU
41%
28%
Larson 1983 Hospital-wide 45%
Donowitz 1987 Neonatal ICU 30
Graham 1990 ICU 32
Dubbert 1990 ICU 81
Pettinger 1991 Surgical ICU 51
Larson 1992 Neonatal Unit 29
Doebbeling 1992 ICU 40
Zimakoff 1993 ICU 40
Meengs 1994 Emergency Room 32
Pittet 1999 Hospital-wide 48
Compliance per l’igiene delle maniin diverse strutture sanitarie
<40%Pittet and Boyce. Lancet Infectious Diseases 2001
19
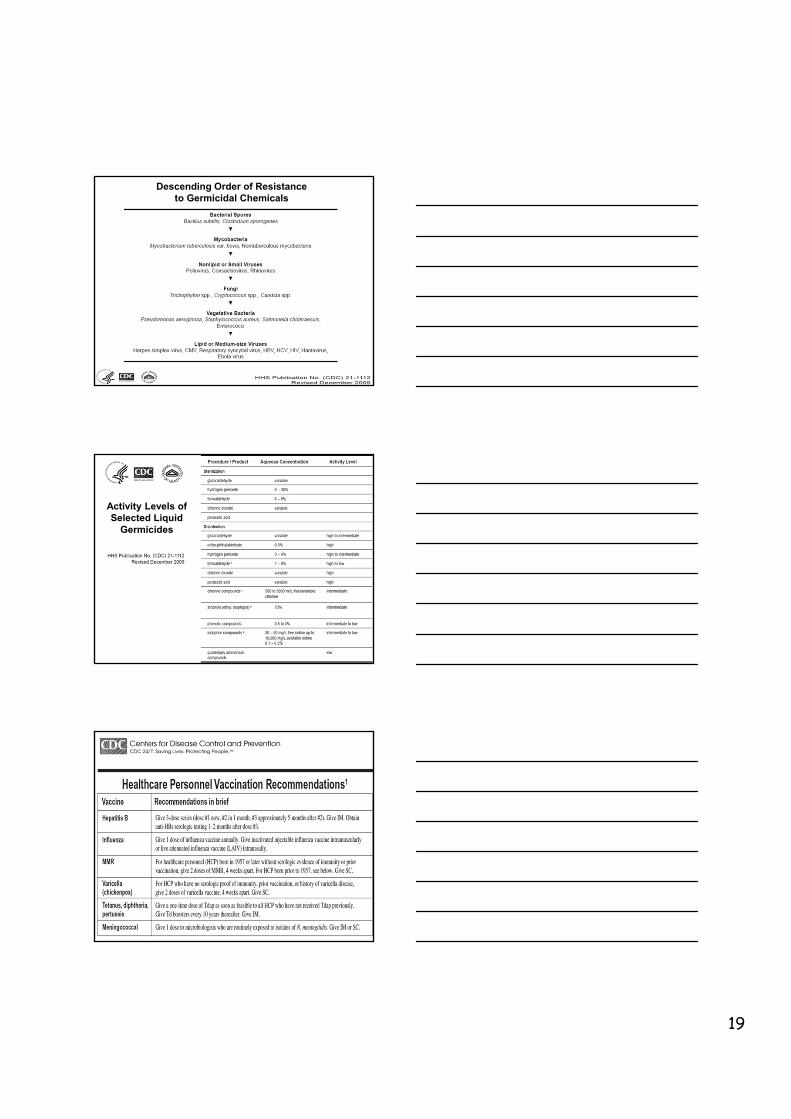
Descending Order of Resistanceto Germicidal Chemicals
Activity Levels of Selected Liquid
Germicides
20

21

22
2013
Early recognition of CDI
Hand hygiene
Implementation of Contact Precautions for CDI pts.
Environmental controls
Antimicrobial stewardship
Healthcare personnel education
Patient education
Administrative support

23
“Efficacy, Immunogenicity, and SafetyStudy of Clostridium difficile Toxoid
Vaccine in Subjects at Risk for C. difficile Infection”
H-030-014 Study
Ambulatorio Prevenzione Malattie Trasmissibili,Vaccinazioni e Sperimentazioni Cliniche
Dipartimento di Scienze della SaluteScuola di Scienze Mediche e Farmaceutiche
Università degli Studi di GenovaIRCCS AOU San Martino-IST di Genova
Noi operatori sanitari seguiamo le linee guida e raccomandazioni internazionali e nazionali
per la prevenzione del rischio infettivo nei nostri reparti?
24
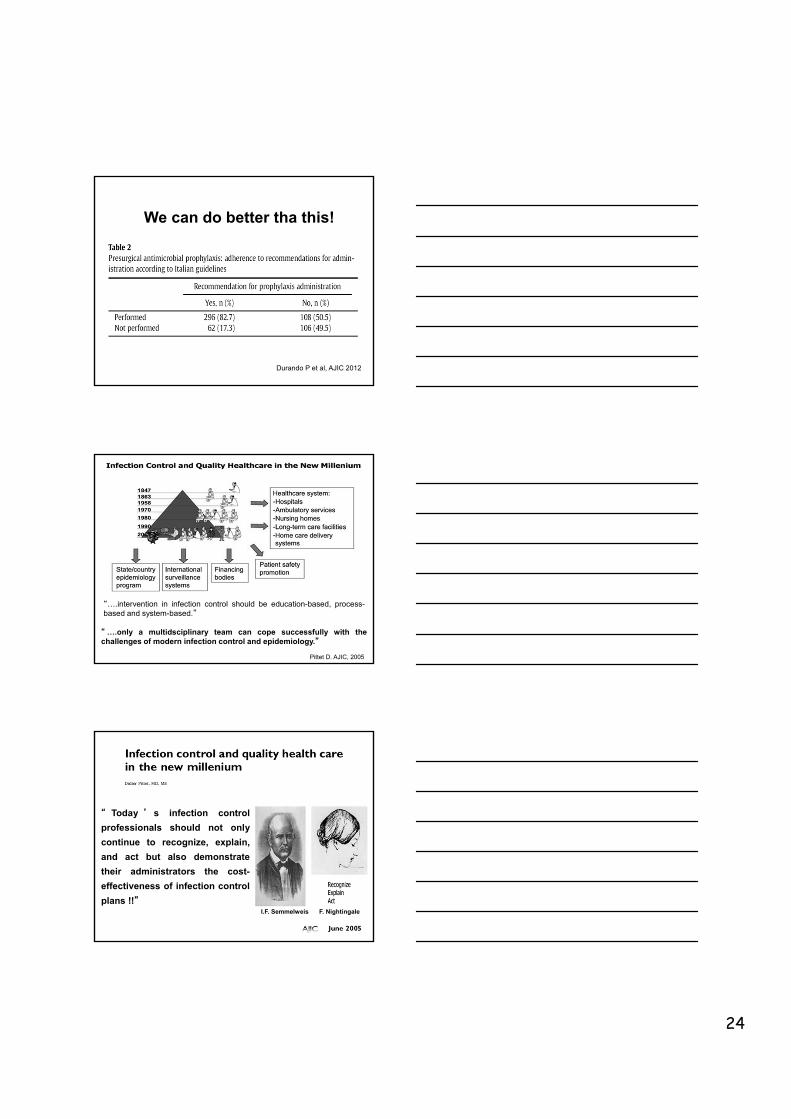
Durando P et al, AJIC 2012
We can do better tha this!
“ ….only a multidsciplinary team can cope successfully with thechallenges of modern infection control and epidemiology.”
Pittet D. AJIC, 2005
“….intervention in infection control should be education-based, process-based and system-based.”
“ Today ’ s infection control
professionals should not only
continue to recognize, explain,
and act but also demonstrate
their administrators the cost-
effectiveness of infection control
plans !!”I.F. Semmelweis F. Nightingale

25
Società scientifiche e gruppi di lavoro sulle
infezioni correlate all’assistenza
Gruppo Italiano di Studio di Igiene Ospedaliera (GISIO)
http://www.simpios.it/
Società Italiana Multidisciplinare per la Prevenzione delle Infezioni
nelle Organizzazioni Sanitarie
http://www.societaitalianaigiene.org/
GRAZIE!!!