della Provincia di Lecco Trattamento dello shock...
54
Data: 3 aprile 2014 Evento: Tigullio Titolo: Cardiogenic shock Autore: Stefano Savonitto Azienda Ospedaliera della Provincia di Lecco Trattamento dello shock cardiogeno Mancanza di mezzi o mancanza di stoffa? Stefano Savonitto Divisione di Cardiologia Ospedale A. Manzoni Lecco
Transcript of della Provincia di Lecco Trattamento dello shock...
Data: 3 aprile 2014
Evento: Tigullio
Titolo: Cardiogenic shock Autore: Stefano Savonitto
Azienda Ospedaliera della Provincia di Lecco
Trattamento dello shock cardiogeno Mancanza di mezzi o mancanza di stoffa?
Stefano Savonitto Divisione di Cardiologia
Ospedale A. Manzoni Lecco
Data: 3 aprile 2014
Evento: Tigullio
Titolo: Cardiogenic shock Autore: Stefano Savonitto
Azienda Ospedaliera della Provincia di Lecco
Trattamento dello shock cardiogeno Mancanza di mezzi o mancanza di stoffa?
Stefano Savonitto Divisione di Cardiologia
Ospedale A. Manzoni Lecco
Data: 3 aprile 2014
Evento: Tigullio
Titolo: Cardiogenic shock Autore: Stefano Savonitto
Azienda Ospedaliera della Provincia di Lecco
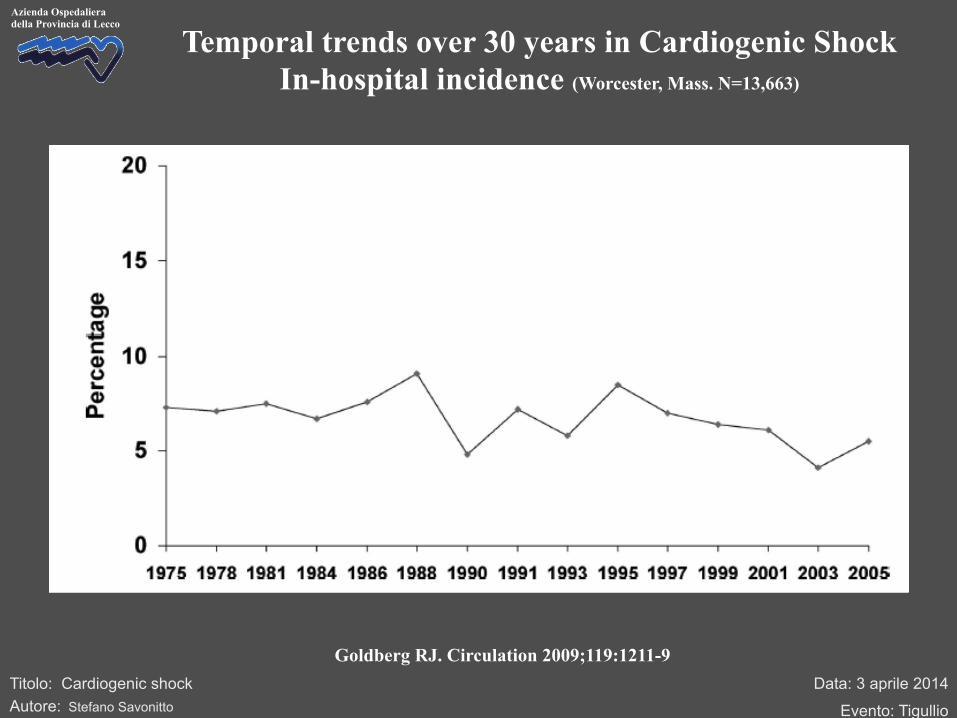
Temporal trends over 30 years in Cardiogenic Shock In-hospital incidence (Worcester, Mass. N=13,663)
Goldberg RJ. Circulation 2009;119:1211-9

Data: 3 aprile 2014
Evento: Tigullio
Titolo: Cardiogenic shock Autore: Stefano Savonitto
Azienda Ospedaliera della Provincia di Lecco
Goldberg RJ. Circulation 2009;119:1211-9
Temporal trends over 30 years in Cardiogenic Shock In-hospital incidence (Worcester, Mass. N=13,663)

Data: 3 aprile 2014
Evento: Tigullio
Titolo: Cardiogenic shock Autore: Stefano Savonitto
Azienda Ospedaliera della Provincia di Lecco In-hospital Mortality
Aissaoui N. Eur Heart J 2012; 33:2535–2543
USIK 1995, USIC 2000, FAST-MI France National Registry
1995 2000 2005
90 80 70 60 50 40 30 20 10 0
Dea
th a
t 30
days
(%)
8.7 (7.5-10.0) 4.2
(3.4-5.1) 3.6
(3.0-4.4)
51 (44-59)
63 (56-70)
70 (62-77)
Shock No Shock

Data: 3 aprile 2014
Evento: Tigullio
Titolo: Cardiogenic shock Autore: Stefano Savonitto
Azienda Ospedaliera della Provincia di Lecco Temporal trends over 10 years:
PCI, CABG and fibrinolytic therapy
Jeger . Ann Int Med 2008;149:618-626
Registry of 1977 patients with cardiogenic shock
Data: 3 aprile 2014
Evento: Tigullio
Titolo: Cardiogenic shock Autore: Stefano Savonitto
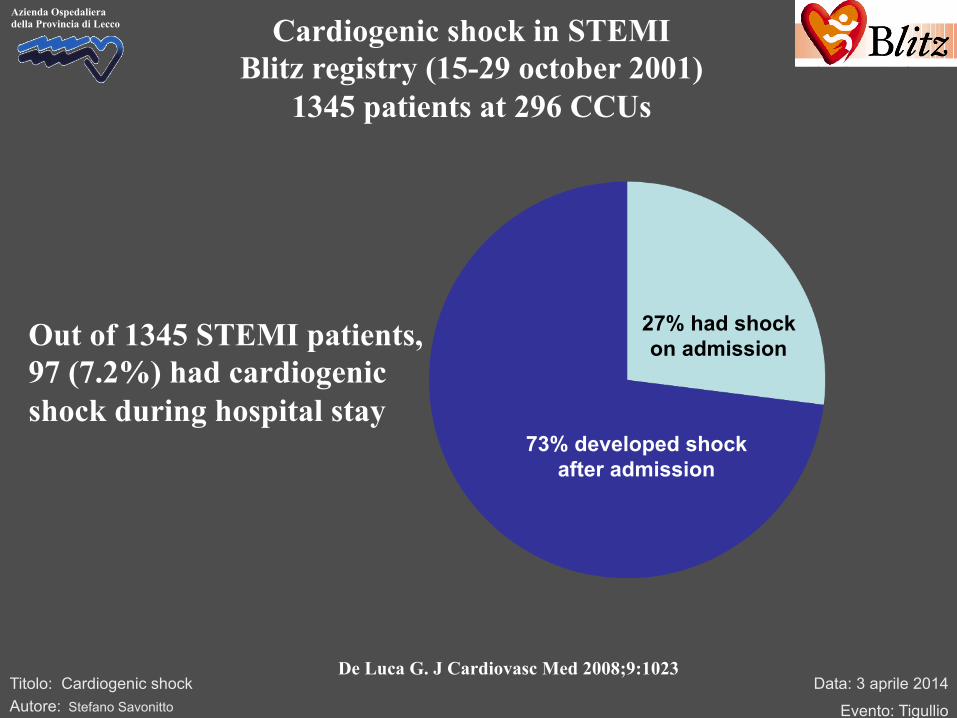
Azienda Ospedaliera della Provincia di Lecco Cardiogenic shock in STEMI
Blitz registry (15-29 october 2001) 1345 patients at 296 CCUs
De Luca G. J Cardiovasc Med 2008;9:1023
73% developed shock after admission
27% had shock on admission Out of 1345 STEMI patients,
97 (7.2%) had cardiogenic shock during hospital stay
Data: 3 aprile 2014
Evento: Tigullio
Titolo: Cardiogenic shock Autore: Stefano Savonitto
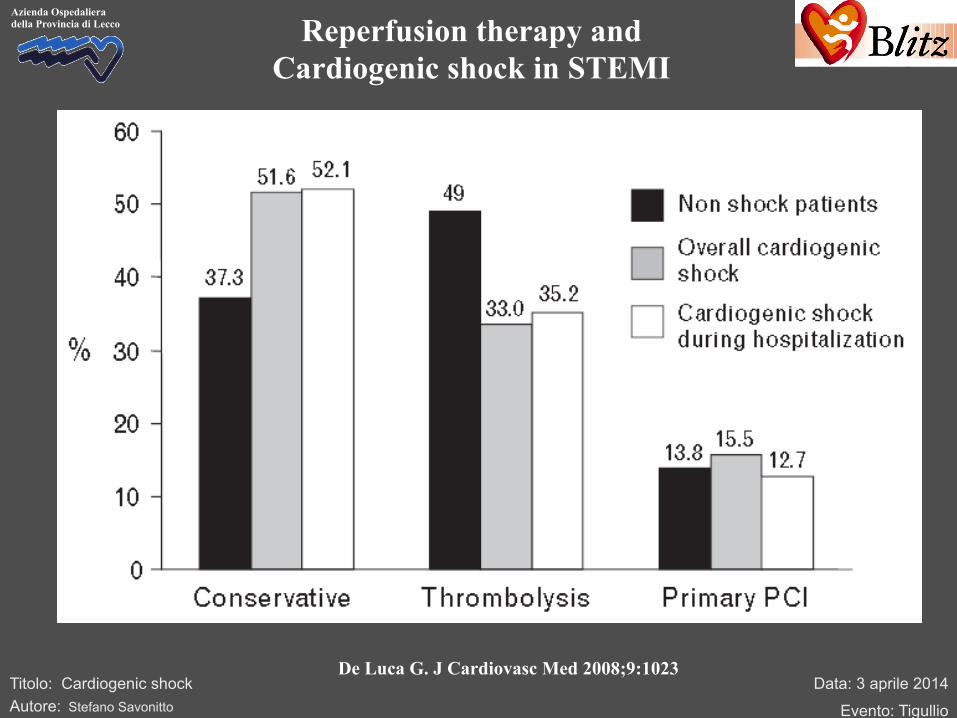
Azienda Ospedaliera della Provincia di Lecco Reperfusion therapy and
Cardiogenic shock in STEMI
De Luca G. J Cardiovasc Med 2008;9:1023
Data: 3 aprile 2014
Evento: Tigullio
Titolo: Cardiogenic shock Autore: Stefano Savonitto
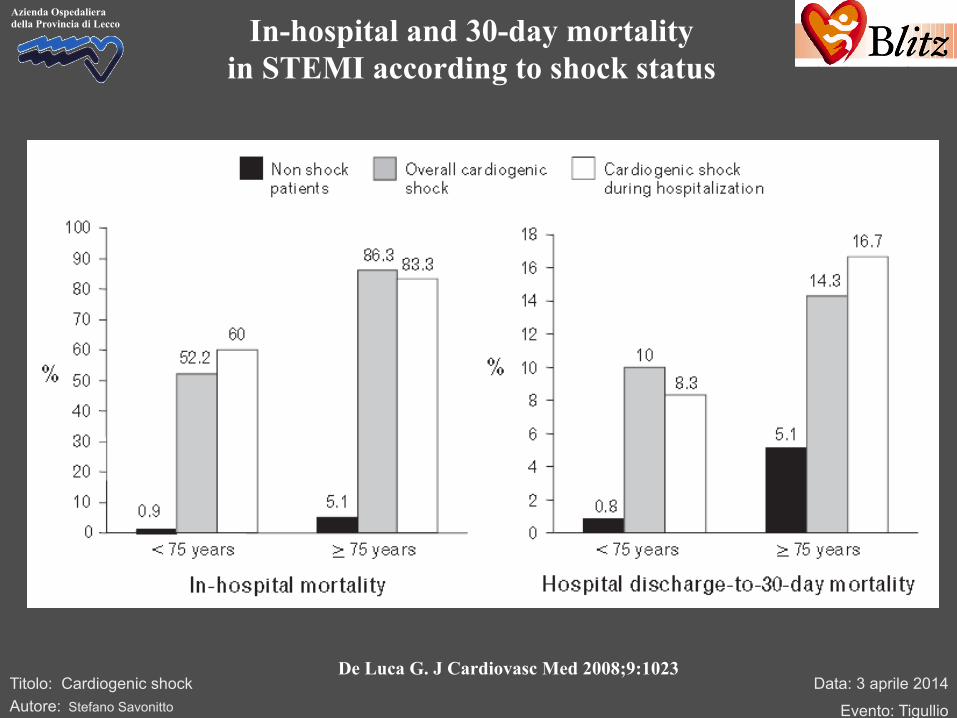
Azienda Ospedaliera della Provincia di Lecco In-hospital and 30-day mortality
in STEMI according to shock status
De Luca G. J Cardiovasc Med 2008;9:1023

Data: 3 aprile 2014
Evento: Tigullio
Titolo: Cardiogenic shock Autore: Stefano Savonitto
Azienda Ospedaliera della Provincia di Lecco Predictors of postadmission
cardiogenic shock in STEMI patients
1 2 3 4 5 6 7 8 9 10
Killip class >1 at entry
SBP at entry (continuous)
Age (continuous)
Unsuccesful reperfusion
Diabetes
38.3 39
22.3 23
21.5 22
11.4 12
5.2 6
Χ2 % Predictive information
De Luca G. J Cardiovasc Med 2008;9:1023

Data: 3 aprile 2014
Evento: Tigullio
Titolo: Cardiogenic shock Autore: Stefano Savonitto
Azienda Ospedaliera della Provincia di Lecco Early and late mortality in
cardiogenic shock patients >65 y.o.
Bagai A. Am Heart J 2013;166:298
N=40,655
N=2001
Landmark after 6 months
Data: 3 aprile 2014
Evento: Tigullio
Titolo: Cardiogenic shock Autore: Stefano Savonitto
Azienda Ospedaliera della Provincia di Lecco
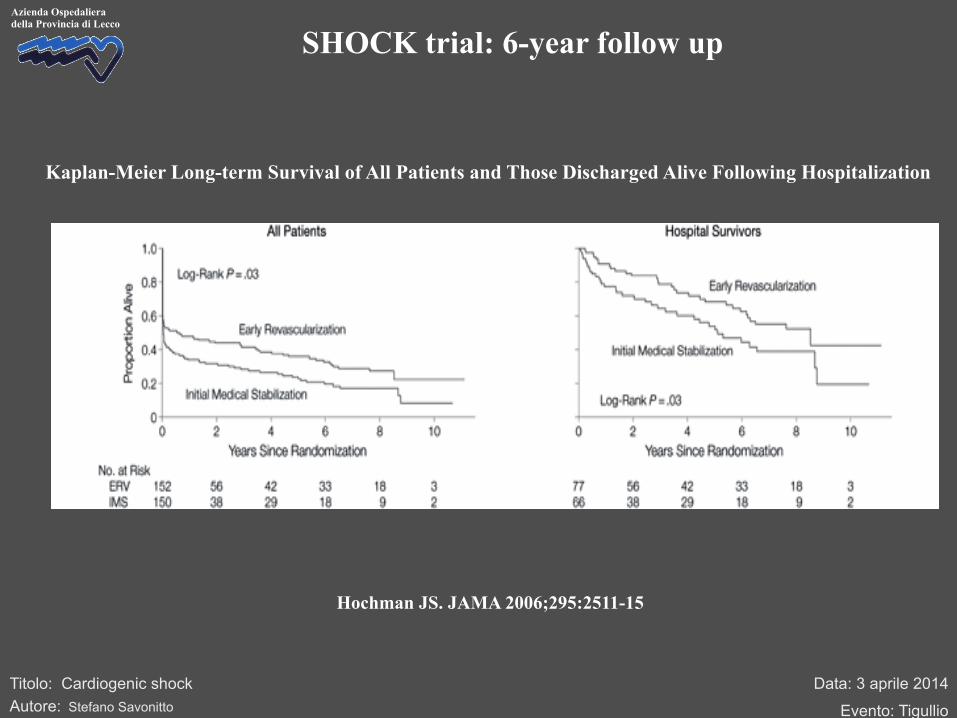
Hochman JS. JAMA 2006;295:2511-15
Kaplan-Meier Long-term Survival of All Patients and Those Discharged Alive Following Hospitalization
SHOCK trial: 6-year follow up
Data: 3 aprile 2014
Evento: Tigullio
Titolo: Cardiogenic shock Autore: Stefano Savonitto
Azienda Ospedaliera della Provincia di Lecco
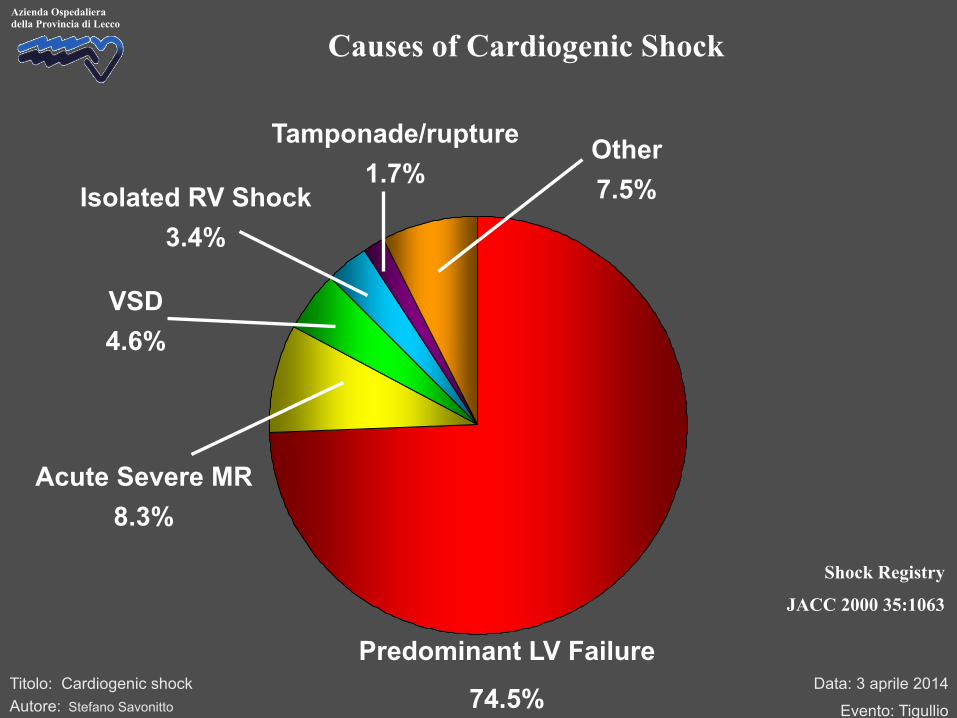
Causes of Cardiogenic Shock
Predominant LV Failure
74.5%
Acute Severe MR 8.3%
VSD 4.6%
Isolated RV Shock 3.4%
Tamponade/rupture 1.7%
Other 7.5%
Shock Registry
JACC 2000 35:1063
Data: 3 aprile 2014
Evento: Tigullio
Titolo: Cardiogenic shock Autore: Stefano Savonitto
Azienda Ospedaliera della Provincia di Lecco
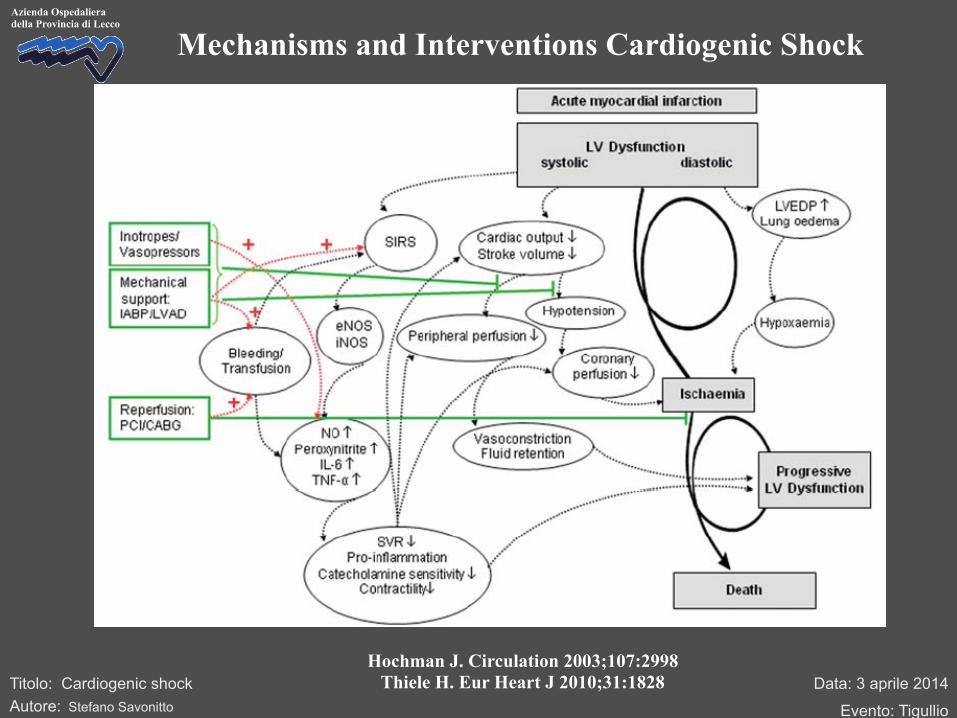
Hochman J. Circulation 2003;107:2998 Thiele H. Eur Heart J 2010;31:1828
Mechanisms and Interventions Cardiogenic Shock

Data: 3 aprile 2014
Evento: Tigullio
Titolo: Cardiogenic shock Autore: Stefano Savonitto
Azienda Ospedaliera della Provincia di Lecco
Revascularization – SHOCK trial
Overall 30-Day Survival in the Study
Hochman J. N Engl J Med 1999;341:625-634
HR 0.83 (0.67-1.04). P=0.11

Data: 3 aprile 2014
Evento: Tigullio
Titolo: Cardiogenic shock Autore: Stefano Savonitto
Azienda Ospedaliera della Provincia di Lecco
47%50%
53%56%
63%66%
0%
10%
20%
30%
40%
50%
60%
70%
30 days (n=302) 6 months (n=301) 12 months (n=299)
Mor
talit
y (%
)ERVIMS
85% of survivors NYHA Class I/II at 12 months
Hochman J. JAMA 2000;285:190
p=0.11 p=0.03
Revascularization – SHOCK trial

Data: 3 aprile 2014
Evento: Tigullio
Titolo: Cardiogenic shock Autore: Stefano Savonitto
Azienda Ospedaliera della Provincia di Lecco Emergency revascularisation in the Elderly
SHOCK Trial
41%
75%
57%53%
0%
10%
20%
30%
40%
50%
60%
70%
80%
<75 years (n=246) >75 years (n=56)
30-d
ay M
orta
lity
(%)
ERVIMS
• >75 years ERV vs IMS baseline characteristics – LVEF 28% vs 36% p=0.051 – Anterior MI 63% vs 41% p=0.18 – Female 54% vs 31% p=0.11
p=0.01
p=0.01
Hochman J. NEJM 1999;341:625
Data: 3 aprile 2014
Evento: Tigullio
Titolo: Cardiogenic shock Autore: Stefano Savonitto
Azienda Ospedaliera della Provincia di Lecco
Trial n/N n/N Relative Risk
95% CI Relative Risk 95% CI
0 0.5 1 2 3
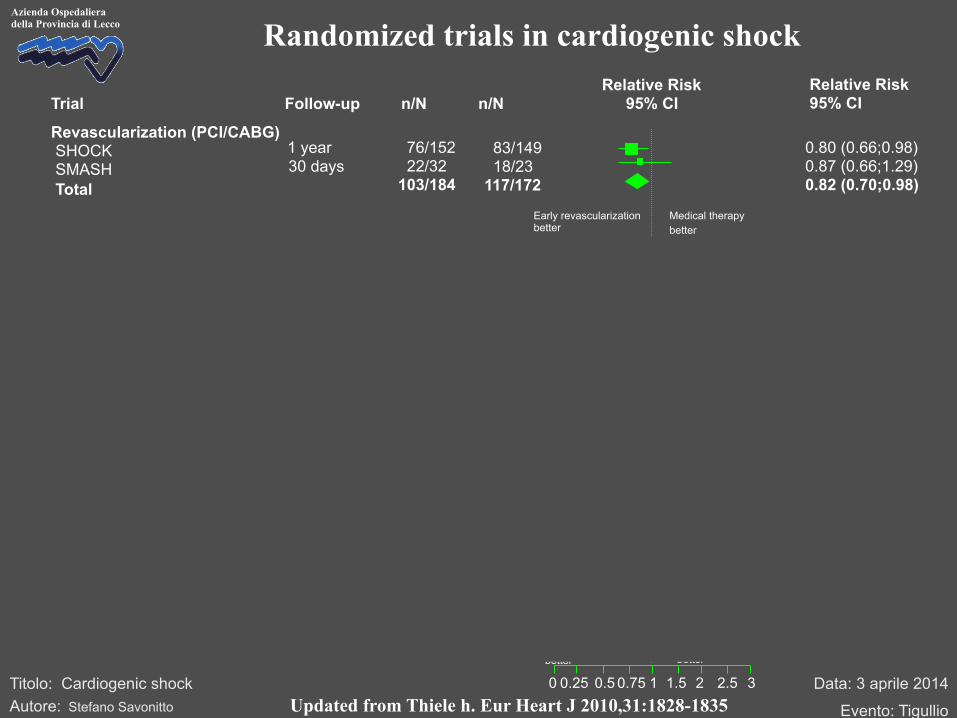
Randomized trials in cardiogenic shock
Follow-up
Revascularization (PCI/CABG) SHOCK SMASH Total
76/152 22/32 103/184
83/149 18/23 117/172
0.80 (0.66;0.98) 0.87 (0.66;1.29) 0.82 (0.70;0.98)
1 year 30 days
Early revascularization better
Medical therapy better
0.75 1.5 2.5 0.25
Noradrenaline better
0.75 (0.55;0.93) 64/145 50/135 28 days Dopamine better
Catecholamines SOAP II (CS subgroup)
In-hospital 15/40 13/40 1.15 (0.59;2.27) Up-stream abciximab better
Standard therapy better
Glycoprotein IIb/IIIa-Inhibitors PRAGUE-7
97/201 24/59 4/15 125/275
30 days 30 days 30 days
76/180 7/20 10/15 93/215
1.14 (0.91;1.45) 1.16 (0.59;2.69) 0.40 (0.13;1.05) 1.05 (0.85;1.29)
NO synthase inhibition better
Placebo better
NO synthase inhibitors TRIUMPH SHOCK-2 Cotter et al Total
30 days 1-year
7/19 155/299 126/319
6/21 152/296 129/319
IABP better
Standard therapy better
1.28 (0.45;3.72) 1.02 (0.88;1.19) 1.02 (0.88;1.19)
IABP IABP-SHOCK I IABP-SHOCK II Total
30 days 30 days 30 days
9/21 9/19 6/13 24/53
9/20 5/14 6/13 20/47
0.95 (0.48;1.90) 1.33 (0.57-3.10) 1.00 (0.44-2.29) 1.06 (0.68-1.66)
LVAD better
IABP better
LVAD Thiele et al Burkhoff et al Seyfarth et al Total
Updated from Thiele h. Eur Heart J 2010,31:1828-1835
Data: 3 aprile 2014
Evento: Tigullio
Titolo: Cardiogenic shock Autore: Stefano Savonitto
Azienda Ospedaliera della Provincia di Lecco
“The panel believes that all accessible vessels should be treated in patients with cardiogenic shock”
“Current Recommendations:- 1-2 vessel disease: PCI IRA 3VD: PCI IRA + staged complete revascularisation Early MV PCI may be warranted if shock persists despite IRA PCI”

Data: 3 aprile 2014
Evento: Tigullio
Titolo: Cardiogenic shock Autore: Stefano Savonitto
Azienda Ospedaliera della Provincia di Lecco Single vessel or Multivessel PCI? SHOCK Trial
• 81% of PCI patients multivessel disease
• 85% PCI IRA only; 23% complete revascularisation
80%
46%45%
54%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
1-y
ear
mo
rtal
ity
(%)
MV PCISV PCI
p<0.01
Shock Trial Shock Registry
p=NS

Data: 3 aprile 2014
Evento: Tigullio
Titolo: Cardiogenic shock Autore: Stefano Savonitto
Azienda Ospedaliera della Provincia di Lecco
Webb et al. J Am Coll Cardiol 2003;42:1380-1386. van der Schaaf et al. Am J Cardiol 2010;105:955-959.
Cavender et al. Am J Cardiol 2009;104:507-513. Bauer et al. Am J Cardiol 2012;109:941-6.
Zeymer et al. Clin Res Cardiol 2012;101 (Suppl):117.
Evidence from registries: Multivessel PCI or culprit lesion PCI only
(endpoint death)
N=74 p<0.05
N=161 p=n.s.
N=3087 p<0.05 N=336
p=n.s.
N=735 p<0.05

Data: 3 aprile 2014
Evento: Tigullio
Titolo: Cardiogenic shock Autore: Stefano Savonitto
Azienda Ospedaliera della Provincia di Lecco
France
Germany
Austria
Lithuania
Sweden
Switzerland
Netherlands
PI: Holger Thiele National coordinators Kurt Huber (Austria) Stefan James (Sweden) Gilles Montalescot (France) Marko Noc (Slovenia) Keith Oldroyd (UK) Jan Piek (Netherlands) Stefano Savonitto (Italy) Pranas Serpitis (Lithuania) Janina Stepinska (Poland) Holger Thiele (Germany) Stephan Windecker (Switzerland)
Poland
Slovenia
Italy
UK
CULPRIT-SHOCK project
Data: 3 aprile 2014
Evento: Tigullio
Titolo: Cardiogenic shock Autore: Stefano Savonitto
Azienda Ospedaliera della Provincia di Lecco
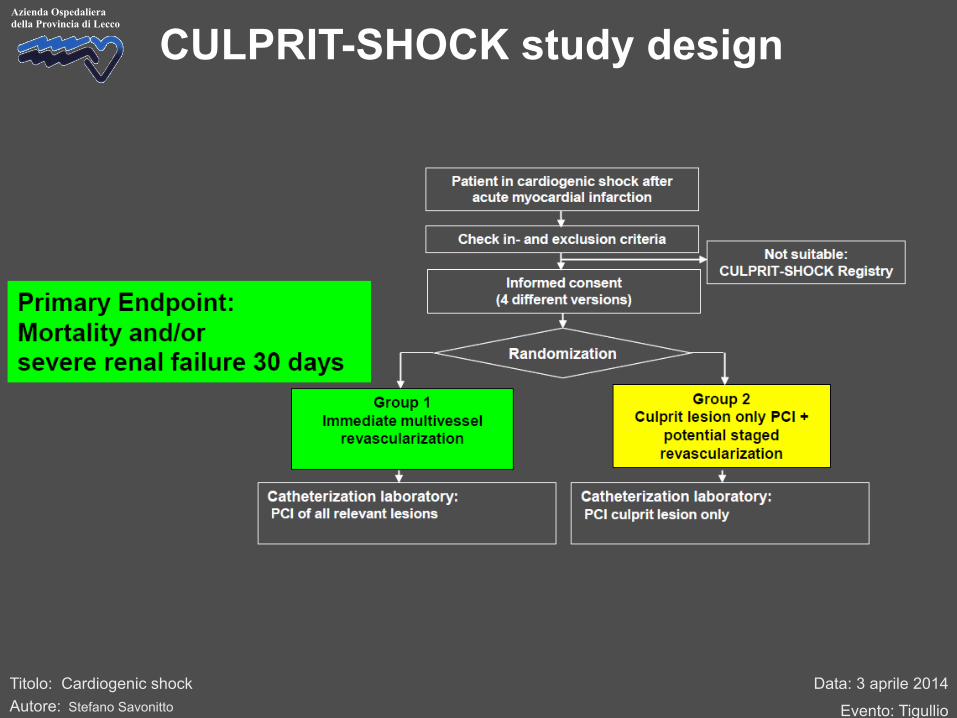
CULPRIT-SHOCK study design

Data: 3 aprile 2014
Evento: Tigullio
Titolo: Cardiogenic shock Autore: Stefano Savonitto
Azienda Ospedaliera della Provincia di Lecco
Inclusion criteria
1. Planned early revascularization by PCI 2. Multivessel CAD [>70% stenosis in > 2 major vessels (≥2 mm diameter)] with identifiable
culprit 3. SBP <90 mmHg for >30‘ or catecholamines required to maintain BP >90 mmHg 4. Signs of pulmonary congestion 5. Signs of impaired organ perfusion with at least one of the following criteria
a) Altered mental status b) Cold, clammy skin and extremities c) Oliguria with urine output <30 ml/h d) Serum-lactate >2.0 mmol/l
6. Informed consent Exclusion critieria
• Single vessel disease • Need for primary urgent bypass surgery (to be determined after diagnostic
angiography) • Mechanical cause of cardiogenic shock • Onset of shock >12 h • Resuscitation >30 minutes • No intrinsic heart action • Cerebral deficit with fixed dilated pupils (not drug-induced) • Massive pulmonary embolism • Age >90 years • Shock of other cause (bradycardia, sepsis, hypovolemia, etc.) • Other severe concomitant disease with limited life expectancy <6 months

Data: 3 aprile 2014
Evento: Tigullio
Titolo: Cardiogenic shock Autore: Stefano Savonitto
Azienda Ospedaliera della Provincia di Lecco Stunned myocardium in STEMI patients
as a cause of cardiogenic shock
Matsusaki M. Circulation 1983;68:170

Data: 3 aprile 2014
Evento: Tigullio
Titolo: Cardiogenic shock Autore: Stefano Savonitto
Azienda Ospedaliera della Provincia di Lecco
To support myocardium during recovery
Stunned myocardium in STEMI patients as a cause of cardiogenic shock
Matsusaki M. Circulation 1983;68:170

Data: 3 aprile 2014
Evento: Tigullio
Titolo: Cardiogenic shock Autore: Stefano Savonitto
Azienda Ospedaliera della Provincia di Lecco
Catecholamine effects
Overgaard & Dzavik. Circulation 2008;118:1047-56

Data: 3 aprile 2014
Evento: Tigullio
Titolo: Cardiogenic shock Autore: Stefano Savonitto
Azienda Ospedaliera della Provincia di Lecco
Inotropic agents: dosage and recommendations
Da: Savonitto S (editor). Manuale di Terapia Cardiovascolare, 3° edizione, Pensiero Scientifico 2010

Data: 3 aprile 2014
Evento: Tigullio
Titolo: Cardiogenic shock Autore: Stefano Savonitto
Azienda Ospedaliera della Provincia di Lecco Catecholamines in shock (all kinds of shock)
De Backer D. NEJM 2010;362:779-89

Data: 3 aprile 2014
Evento: Tigullio
Titolo: Cardiogenic shock Autore: Stefano Savonitto
Azienda Ospedaliera della Provincia di Lecco Catecholamines in cardiogenic shock
De Backer D. NEJM 2010;362:779-89
“The exact cause of the increased mortality with dopamine in patients with CS could not be determined, but the early difference in the rate of death suggests that the higher heart rate with dopamine may have contributed to the occurrence of ischemic events”
Titrated up to 20 mcg/kg

Data: 3 aprile 2014
Evento: Tigullio
Titolo: Cardiogenic shock Autore: Stefano Savonitto
Azienda Ospedaliera della Provincia di Lecco
Christopher B. Overgaard and Vladimír DzavíkDisease
Inotropes and Vasopressors : Review of Physiology and Clinical Use in Cardiovascular
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 2008 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/CIRCULATIONAHA.107.728840
2008;118:1047-1056Circulation.
http://circ.ahajournals.org/content/118/10/1047World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer this process is available in the
click Request Permissions in the middle column of the Web page under Services. Further information aboutOffice. Once the online version of the published article for which permission is being requested is located,
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the EditorialCirculationin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
at UNIV DE MODENA BIBLIO CENTRAL on October 23, 2012http://circ.ahajournals.org/Downloaded from
Close observation is essential to monitor for exacerbation ofhypotension and atrial arrhythmias, which can profoundlyworsen hemodynamics.
BradyarrhythmiasOwing to their chronotropic effects, !-adrenergic agonistscan be useful for transient emergency treatment of bradyar-rhythmias if atropine is ineffective.53 The use of the!-agonists dobutamine, dopamine, or isoproterenol can sta-bilize the patient to allow time for a temporary pacemaker tobe inserted. These agents are also useful under the samecircumstances to treat bradycardia-induced torsade despointes. Finally, isoproterenol has also been used to suppressthe trigger for ventricular fibrillation in patients with theBrugada syndrome who do not wish to have cardioverter-defibrillator implantation to prevent sudden cardiac death.72
Adjuvant IssuesPatient Monitoring During Parenteral Inotropicand Vasopressor TherapyPatients requiring treatment with inotropes and vasopressorsgenerally require monitoring in an intensive care or step-down setting because of the potential for development oflife-threatening arrhythmias.
Invasive Blood Pressure MonitoringIn shock, continuous blood pressure monitoring with anarterial line is essential both to monitor the status of theunderlying illness and because inotropes and vasopressorshave the potential to induce life-threatening hypotension orhypertension. Chronic HF patients undergoing hemodynamictailoring with a low-dose !-agonist or PDI can usually bemonitored noninvasively.
Pulmonary Artery Catheter UseConsensus on pulmonary artery catheter use during treatmentwith inotropic therapy is lacking. Although this tool can behelpful diagnostically, its routine use has never been shown toimprove outcomes.73 This may reflect an absence of effectiveevidence-based therapies to be used in response to pulmonaryartery catheter data in the treatment of critically ill patients.74
In the ESCAPE trial (Evaluation Study of Congestive HeartFailure and Pulmonary Artery Catheterization Effectiveness),which examined pulmonary artery catheter use in patientswith severe HF, catheter insertion was deemed safe but wasnot associated with improved rates of mortality or hospital-ization.75 Inotropic titration with pulmonary artery catheterdata in isolation can result in inappropriate stimulation of CO,thus negatively impacting prognosis in heterogeneous inten-sive care unit patient populations.76 Titration of inotropictherapy should be guided by the adequacy of end-organperfusion, based on multiple clinical parameters.
Goals of Inotropic and Vasopressor TherapyThe use of inotropes and vasopressors has not been shown inrandomized, controlled studies to ultimately lead to improvedpatient outcomes, at least in part because no clinical trialshave been conducted with study size and power adequate totest their effect on improving survival. In the absence of suchdata, the definitive goals of therapy must be considered of
primary importance, and the role of inotropic therapy shouldbe kept in a supportive context to allow treatment of theunderlying disorder. Such therapy includes prompt percuta-neous or surgical revascularization and the institution ofmechanical support (intra-aortic balloon counterpulsation orLV assist device) to improve coronary perfusion, CO, or both.
Conclusions and RecommendationsIn conclusion, inotropes and vasopressors play an essentialrole in the supportive care of a number of important cardio-vascular disease processes. To date, prospective examinationof their impact on clinical outcomes in randomized trials hasbeen minimal, despite their widespread use in cardiovascularillness. However, the recently published TRIUMPH (Tilargi-nine Acetate Injection in a Randomized International Study inUnstable MI Patients With Cardiogenic Shock) internationalrandomized trial of NG-monomethyl L-arginine in cardiogenicshock has shown that such trials are not only feasible butnecessary to validate findings of smaller studies.77,78 A betterunderstanding of the physiology and important adverse ef-fects of these medications should lead to directed clinical use,with realistic therapeutic goals. The following broad recom-mendations can be made:
Smaller combined doses of inotropes and vasopressors maybe advantageous over a single agent used at higher doses toavoid dose-related adverse effects.
The use of vasopressin at low to moderate doses may allowcatecholamine sparing, and it may be particularly useful insettings of catecholamine hyposensitivity and after pro-longed critical illness.
In cardiogenic shock complicating AMI, current guidelinesbased on expert opinion recommend dopamine or dobuta-mine as first-line agents with moderate hypotension (sys-tolic blood pressure 70 to 100 mm Hg) and norepinephrineas the preferred therapy for severe hypotension (systolicblood pressure !70 mm Hg).
Routine inotropic use is not recommended for end-stage HF.When such use is essential, every effort should be made toeither reinstitute stable oral therapy as quickly as possibleor use destination therapy such as cardiac transplantationor LV assist device support.
Large randomized trials focusing on clinical outcomes areneeded to better assess the clinical efficacy of these agents.
AcknowledgmentsWe would like to thank Uchewnwa Genus for her assistance duringthe preparation of this article.
DisclosuresDr Overgaard is supported by a Heart and Stroke Foundation ofCanada (HSFC)/AstraZeneca Canada Inc fellowship award. DrDzavík is supported in part by the Brompton Funds (Toronto,Canada) Professorship in Interventional Cardiology. Dr Dzavík hasreceived research funding from Arginox Inc and speaker’s honorariafrom Datascope Inc.
References1. Abel JJ, Taveau RD. On the decomposition products of epinephrine
hydrate. J Biol Chem. 1905;1:1–32.2. Barger G, Dale HH. Chemical structure and sympathomimetic action of
amines. J Physiol. 1910;41:19–59.
1054 Circulation September 2, 2008
at UNIV DE MODENA BIBLIO CENTRAL on October 23, 2012http://circ.ahajournals.org/Downloaded from
diastolic relaxation (lusitropy), thus reducing preload, after-load, and SVR.
Milrinone is the PDI most commonly used for cardiovas-cular indications (Table). In its parenteral form, it has a longerhalf-life (2 to 4 hours) than many other inotropic medications.This drug is particularly useful if adrenergic receptors aredownregulated or desensitized in the setting of chronic HF, orafter chronic !-agonist administration. Amrinone is used lessoften because of important side effects, which include dose-related thrombocytopenia.
VasopressinIsolated in 1951,16 the nonapeptide vasopressin or “antidi-uretic hormone” is stored primarily in granules in the poste-rior pituitary gland and is released after increased plasmaosmolality or hypotension, as well as pain, nausea, andhypoxia. Vasopressin is synthesized to a lesser degree by theheart in response to elevated cardiac wall stress17 and by theadrenal gland in response to increased catecholamine secre-tion.18 It exerts its circulatory effects through V1 (V1a invascular smooth muscle, V1b in the pituitary gland) and V2
receptors (renal collecting duct system; Table). V1a stimula-tion mediates constriction of vascular smooth muscle,whereas V2 receptors mediate water reabsorption by enhanc-ing renal collecting duct permeability.
Vasopressin causes less direct coronary and cerebral vaso-constriction than catecholamines and has a neutral or inhib-itory impact on CO, depending on its dose-dependent in-crease in SVR and the reflexive increase in vagal tone. Avasopressin-modulated increase in vascular sensitivity tonorepinephrine further augments its pressor effects. The agentmay also directly influence mechanisms involved in thepathogenesis of vasodilation, through inhibition of ATP-ac-tivated potassium channels,19 attenuation of nitric oxideproduction,20 and reversal of adrenergic receptor downregu-lation.21 The pressor effects of vasopressin are relativelypreserved during hypoxic and acidotic conditions, whichcommonly develop during shock of any origin.
Calcium-Sensitizing AgentsCalcium sensitizers are a recently developed class ofinotropic agents, levosimendan being the most well known(Table).22 These agents have a dual mechanism of action thatincludes calcium sensitization of contractile proteins and theopening of ATP-dependent potassium (K!) channels.Calcium-dependent binding to troponin C enhances ventric-ular contractility without increasing intracellular Ca2! con-centration or compromising diastolic relaxation, which mayfavorably impact myocardial energetics relative to traditionalinotropic therapies. The opening of K! channels on vascularsmooth muscle leads to arteriolar and venous vasodilationand may confer a degree of myocardial protection duringischemia.23 The combination of improved contractile perfor-mance and vasodilation is particularly beneficial during acuteand chronic HF states, for which levosimendan is being usedwith increasing frequency in some countries.
Evidence for Use of Inotropes andVasopressors in Cardiovascular Disease
Cardiogenic Shock Complicating AcuteMyocardial InfarctionInotropes and vasopressors are used routinely in the setting ofcardiogenic shock complicating acute myocardial infarction(AMI). These agents all increase myocardial oxygen con-sumption and can cause ventricular arrhythmias, contraction-band necrosis, and infarct expansion. However, critical hy-potension itself compromises myocardial perfusion, leadingto elevated left ventricular (LV) filling pressures, increasedmyocardial oxygen requirements, and further reduction in thecoronary perfusion gradient. Thus, hemodynamic benefitsusually outweigh specific risks of inotropic therapy whenused as a bridge to more definitive treatment measures.
Inotropic agents may improve mitochondrial function innoninfarcted myocardium that has become deranged duringAMI complicated by shock.24 However, free cytosolic Ca2!,which is significantly elevated in postischemic cardiac myo-cytes, is further increased with the administration of dopa-mine, which leads to activation of proteolytic enzymes,proapoptotic signal cascades, mitochondrial damage, andeventual membrane disruption and necrosis.25 Thus, thelowest possible doses of inotropic and pressor agents shouldbe used to adequately support vital tissue perfusion whilelimiting adverse consequences, some of which may not beimmediately apparent.
The American College of Cardiology/American HeartAssociation guidelines for management of hypotension com-plicating AMI suggest the use of dobutamine as a first-lineagent if systolic blood pressure ranges between 70 and100 mm Hg in the absence of signs and symptoms of shock.Dopamine is suggested in patients who have the same systolicblood pressure in the presence of symptoms of shock.26
However, definitive evidence supporting use of specificagents in this setting is lacking. Moderate doses of theseagents maximize inotropy and avoid excessive "1-adrenergicstimulation that can result in end-organ ischemia. The delib-erate combination of dopamine and dobutamine at a dose of7.5 #g ! kg"1 ! min"1 each was shown to improve hemody-namics and limit important side effects compared with eitherindividual agent administered at 15 #g ! kg"1 ! min"1.27 Mod-erate doses of combinations of medications may potentiallybe more effective than maximal doses of any individualagent.
When response to a medium dose of dopamine or dopa-mine/dobutamine in combination is inadequate, or the pa-tient’s presenting systolic blood pressure is #70 mm Hg, theuse of norepinephrine has been recommended.26 With anantithrombotic effect in addition to its pressor qualities,norepinephrine may be the optimal choice under these con-ditions compared with epinephrine, which can exacerbatelactic acidosis and promote thrombosis in coronaryvasculature.28
During early shock, endogenous vasopressin levels areelevated significantly to help maintain end-organ perfusion.29
As the shock state progresses, however, plasma vasopressinlevels fall dramatically, which contributes to a loss of
Overgaard and Dzavík Inotropes, Vasopressors, and Cardiovascular Disease 1051
at UNIV DE MODENA BIBLIO CENTRAL on October 23, 2012http://circ.ahajournals.org/Downloaded from

Data: 3 aprile 2014
Evento: Tigullio
Titolo: Cardiogenic shock Autore: Stefano Savonitto
Azienda Ospedaliera della Provincia di Lecco IABP History
History: 1962 Animal studies
Moulopoulos et al, Am Heart J 1962;63:669-675 1968 1. clinical description in shock
Kantrowitz et al, JAMA 1968;203:135-140 1973 Hemodynamic effects in shock,
Mortality unchanged Scheidt et al, NEJM 1973;288:979-984
> 40 years > 1 Million patients treated, low complication
rate, Benchmark registry Ferguson et al, JACC 2001;38:1456-1462

Data: 3 aprile 2014
Evento: Tigullio
Titolo: Cardiogenic shock Autore: Stefano Savonitto
Azienda Ospedaliera della Provincia di Lecco
Thiele H. Eur Heart J 2010,31:1828-1835
IABP use in cardiogenic shock studies
Data: 3 aprile 2014
Evento: Tigullio
Titolo: Cardiogenic shock Autore: Stefano Savonitto
Azienda Ospedaliera della Provincia di Lecco
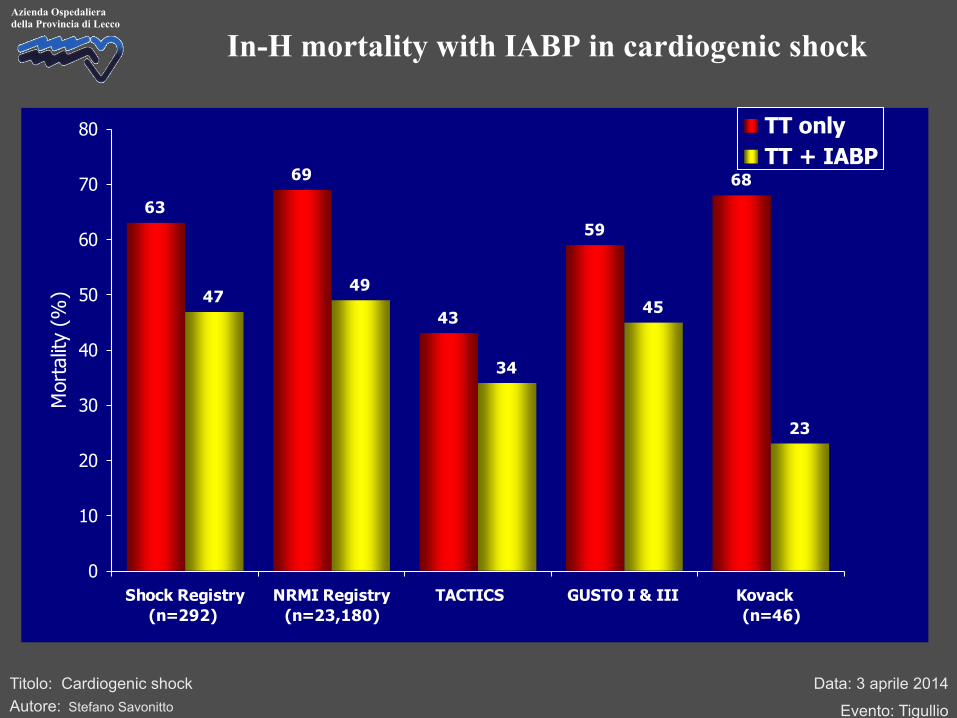
In-H mortality with IABP in cardiogenic shock
63
69
43
59
68
4749
34
45
23
0
10
20
30
40
50
60
70
80
Shock Registry(n=292)
NRMI Registry(n=23,180)
TACTICS GUSTO I & III Kovack (n=46)
Mor
talit
y (%
)
TT onlyTT + IABP

Data: 3 aprile 2014
Evento: Tigullio
Titolo: Cardiogenic shock Autore: Stefano Savonitto
Azienda Ospedaliera della Provincia di Lecco
IABP in Cardiogenic Shock Primary PCI
67
49
4246
0
10
20
30
40
50
60
70
80
Thrombolysis only Thrombolysis + IABP Primary PCI only Primary PCI + IABP
In-h
ospi
tal M
orta
lity
(%)
Retrospective analysis of 23,180 patients from NRMI database
7268 treated by IABP

Data: 3 aprile 2014
Evento: Tigullio
Titolo: Cardiogenic shock Autore: Stefano Savonitto
Azienda Ospedaliera della Provincia di Lecco
Sjauw et al. Eur Heart J 2009;30:459-468
Mortality IABP vs no IABP - Metaanalysis
-1 -0.5 0.5 1 0
No IABP better IABP better
30-day mortality Risk difference
IABP n/N
No IABP n/N
Trial
-0.18 (-0.20 to -0.16) Total
Thrombolysis Stomel
Kovack
Bengtson Waksman
GUSTO-1 SHOCK registry
NRMI-2 TT
28/51
10/27 48/99 11/20
30/62 220/439
1068/2180
1415/2878
10/13 13/19
58/101 17/21
146/248 300/417
2346/3501
2890/4320
-0.11 (-0.13 to -0.09) Total 2488/5146 3332/5283
Total 1049/2234 0.06 (0.03 to 0.10)
Primary PCI NRMI-2 PCI AMC CS
956/2035
93/199 401/955
26/93 427/1048
-0.29 (-0,47 to -0.12)
No reperfusion
24/34
24/34
15/15
15/15
Moloupoulos
Total

Data: 3 aprile 2014
Evento: Tigullio
Titolo: Cardiogenic shock Autore: Stefano Savonitto
Azienda Ospedaliera della Provincia di Lecco
Thiele H. N Engl J Med 2012;367:1287-96
Trial flow and treatment
Data: 3 aprile 2014
Evento: Tigullio
Titolo: Cardiogenic shock Autore: Stefano Savonitto
Azienda Ospedaliera della Provincia di Lecco
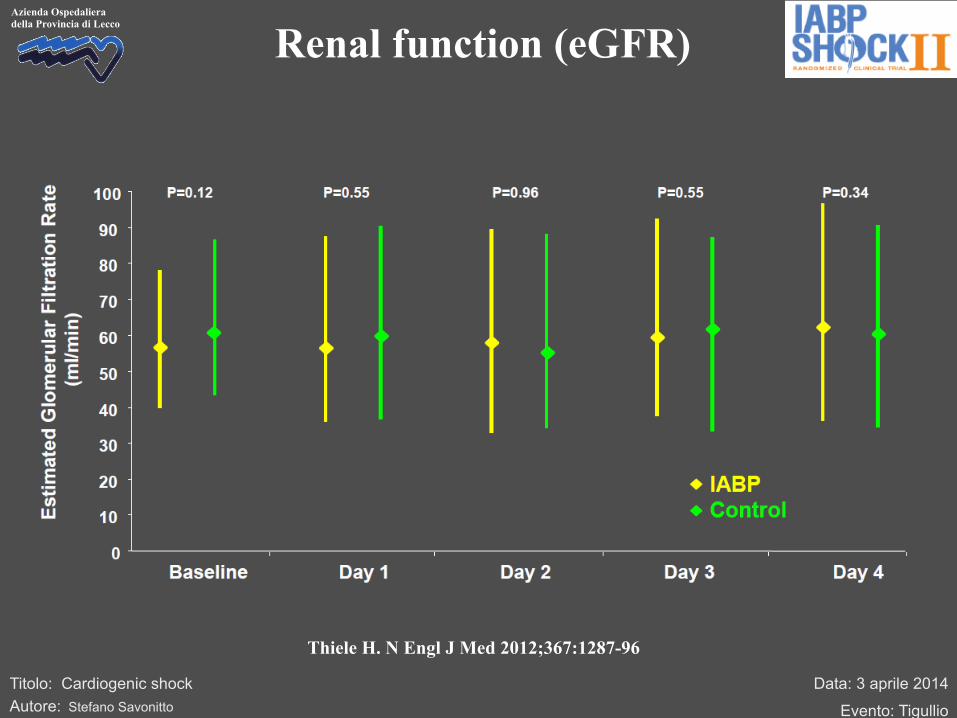
Thiele H. N Engl J Med 2012;367:1287-96
Renal function (eGFR)
Data: 3 aprile 2014
Evento: Tigullio
Titolo: Cardiogenic shock Autore: Stefano Savonitto
Azienda Ospedaliera della Provincia di Lecco
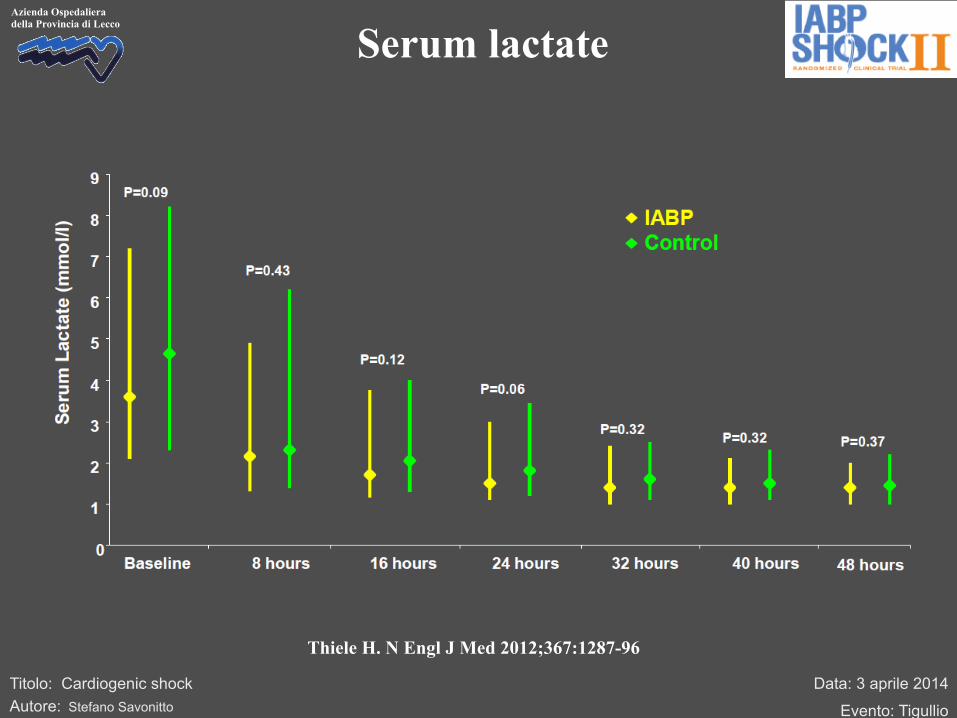
Thiele H. N Engl J Med 2012;367:1287-96
Serum lactate
Data: 3 aprile 2014
Evento: Tigullio
Titolo: Cardiogenic shock Autore: Stefano Savonitto
Azienda Ospedaliera della Provincia di Lecco
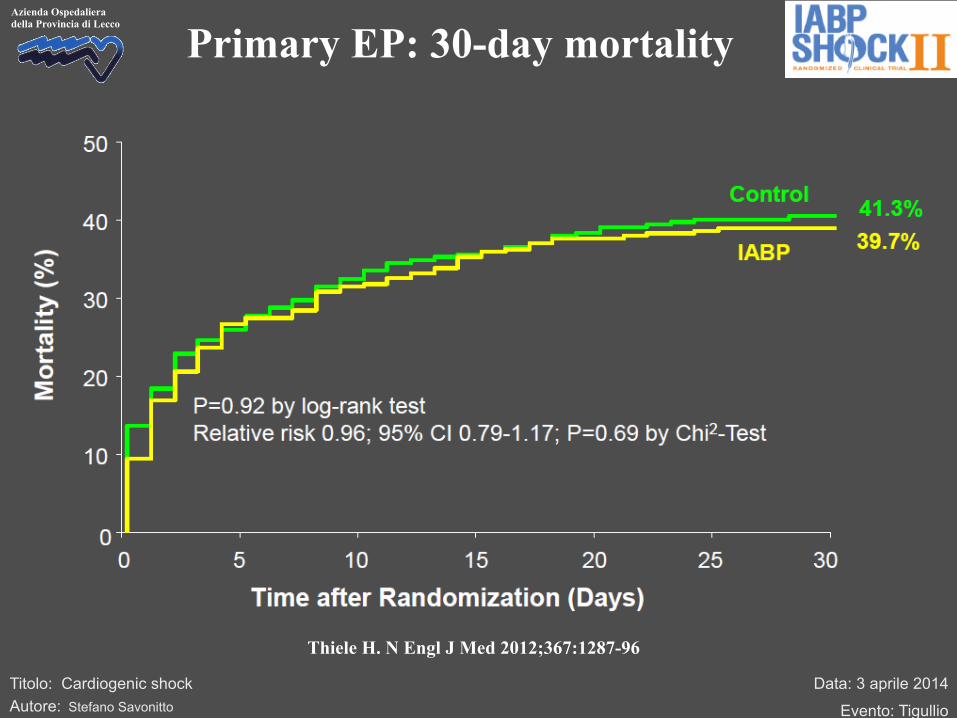
Thiele H. N Engl J Med 2012;367:1287-96
Primary EP: 30-day mortality

Data: 3 aprile 2014
Evento: Tigullio
Titolo: Cardiogenic shock Autore: Stefano Savonitto
Azienda Ospedaliera della Provincia di Lecco
Thiele H. N Engl J Med 2012;367:1287-96
Primary EP: 30-day mortality
Data: 3 aprile 2014
Evento: Tigullio
Titolo: Cardiogenic shock Autore: Stefano Savonitto
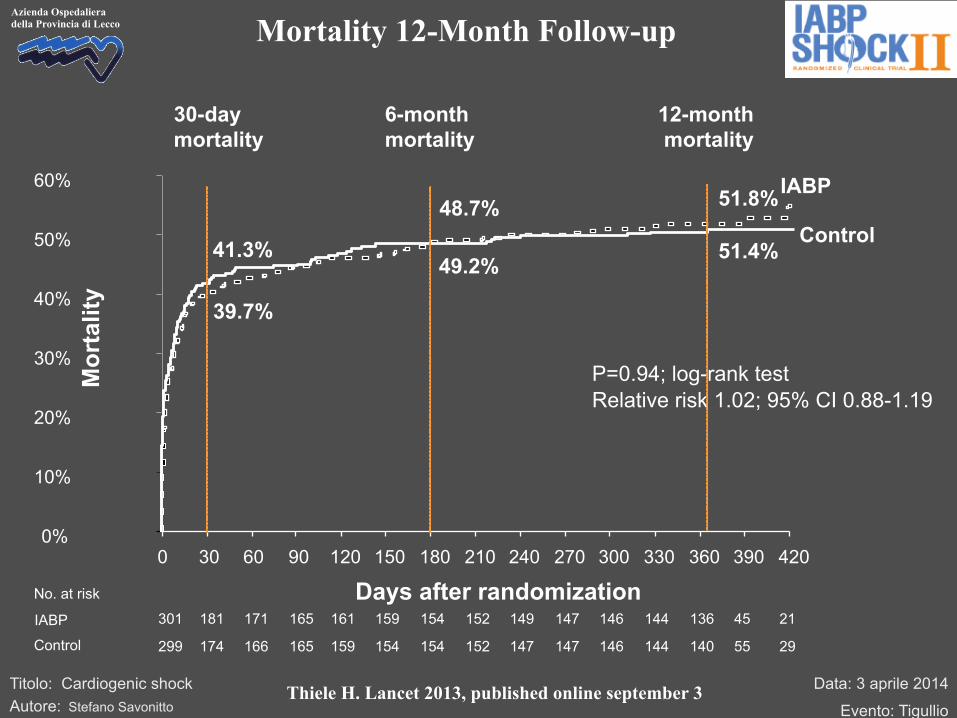
Azienda Ospedaliera della Provincia di Lecco Mortality 12-Month Follow-up
Control
IABP
0%
10%
20%
30%
40%
50%
60%
0 30 60 90 120 150 180 210 240 270 300 330 360 390 420
Mor
talit
y
Days after randomization
P=0.94; log-rank test Relative risk 1.02; 95% CI 0.88-1.19
12-month mortality
49.2%
48.7%
6-month mortality
30-day mortality
41.3%
39.7%
51.8%
51.4%
301 181 171 165 161 159 154 152 149 147 146 144 136 45 21 299 174 166 165 159 154 154 152 147 147 146 144 140 55 29
No. at risk IABP Control
Thiele H. Lancet 2013, published online september 3

Data: 3 aprile 2014
Evento: Tigullio
Titolo: Cardiogenic shock Autore: Stefano Savonitto
Azienda Ospedaliera della Provincia di Lecco Subgroups (12-Month Mortality)
0 0.5 1 1.5 2 2.5
186 409
Baseline Variable N 12-Month Mortality n (%)
IABP Control Relative Risk
(95% CI) P-Value for Interaction
Female Male
Age <50 years Age 50-75 years Age >75 years
Diabetes No diabetes
History of hypertension No history of hypertension
STEMI/LBBB NSTEMI
Anterior STEMI Non-anterior STEMI
Previous infarction No previous infarction
Hypothermia No hypothermia
70 332 193
195 396
410 180
414 181
216 198
131 463
223 372
1.06 (0.76-1.47) 1.00 (0.81-1.20)
0.71 (0.49-1.02) 1.07 (0.88-1.31) 0.96 (0.64-1.43)
0.90 (0.65-1.24) 1.04 (0.86-1.26)
1.14 (0.92-1.41) 0.76 (0.59-0.98)
1.01 (0.83-1.23) 1.00 (0.72-1.37)
0.93 (0.72-1.21) 1.12 (0.84-1.51)
1.27 (0.86-1.89) 0.95 (0.79-1.14)
0.93 (0.70-1.24) 1.10 (0.87-1.31)
0.72
0.13
0.45
0.02
0.94
0.36
0.20
0.43
IABP better Control better
Blood pressure <80 mmHg Blood pressure ≥80 mmHg
168 427
1.07 (0.76-1.51) 1.00 (0.82-1.20)
0.73
57 (57.6) 98 (49.0)
9 (25.0) 75 (48.4) 71 (65.7)
57 (54.3) 95 (50.0)
122 (57.6) 29 (35.4)
102 (50.5) 53 (54.6)
53 (47.0) 49 (55.1)
44 (62.0) 111 (49.0)
55 (53.0) 100 (51.3)
48 (55.2) 104 (49.8)
16 (47.1) 79 (44.6) 57 (67.1)
53 (59.0) 99 (48.1)
102 (51.5) 50 (51.0)
106 (50.0) 46 (54.8)
52 (50.5) 54 (49.5)
31 (51.7) 121 (51.3)
67 (56.3) 85 (48.0)
47 (58.0) 108 (49.5)
48 (55.2) 104 (49.8)
Thiele H. Lancet 2013, published online september 3

Data: 3 aprile 2014
Evento: Tigullio
Titolo: Cardiogenic shock Autore: Stefano Savonitto
Azienda Ospedaliera della Provincia di Lecco
Predictors of 1-year mortality in IABP-SHOCK II
Thiele H. Lancet 2013, published online september 3
Data: 3 aprile 2014
Evento: Tigullio
Titolo: Cardiogenic shock Autore: Stefano Savonitto
Azienda Ospedaliera della Provincia di Lecco
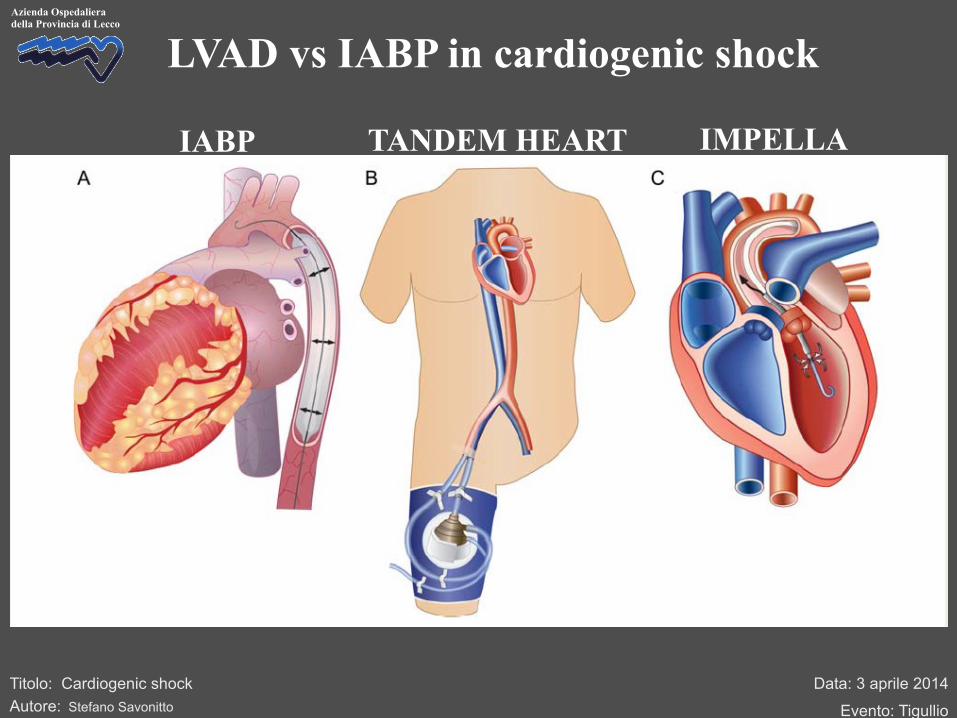
LVAD vs IABP in cardiogenic shock
IABP TANDEM HEART IMPELLA
Data: 3 aprile 2014
Evento: Tigullio
Titolo: Cardiogenic shock Autore: Stefano Savonitto
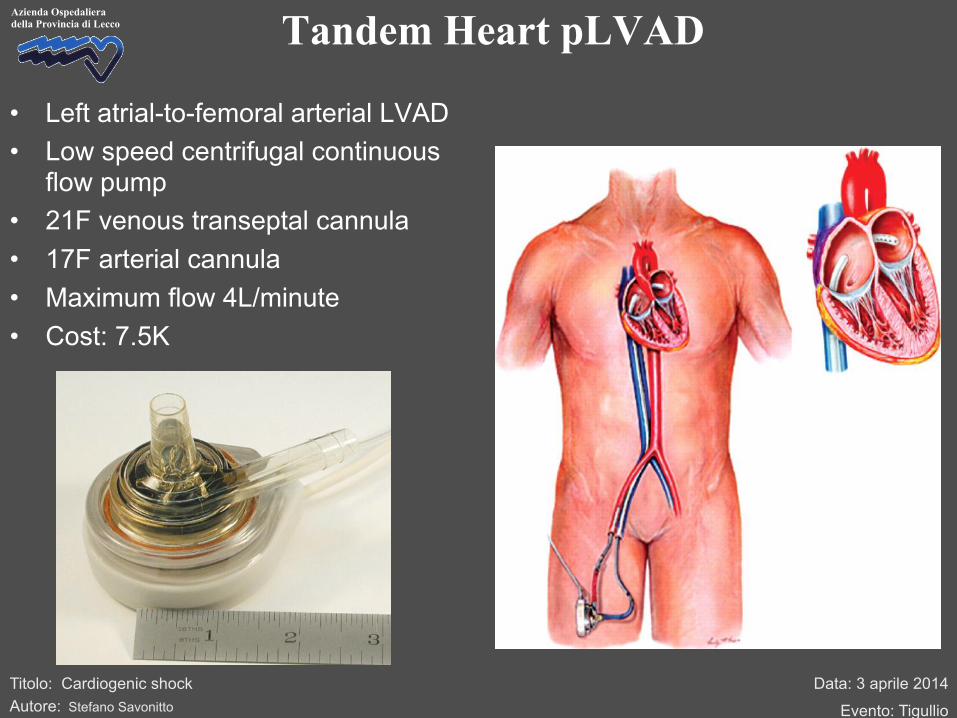
Azienda Ospedaliera della Provincia di Lecco Tandem Heart pLVAD
• Left atrial-to-femoral arterial LVAD • Low speed centrifugal continuous
flow pump • 21F venous transeptal cannula • 17F arterial cannula • Maximum flow 4L/minute • Cost: 7.5K

Data: 3 aprile 2014
Evento: Tigullio
Titolo: Cardiogenic shock Autore: Stefano Savonitto
Azienda Ospedaliera della Provincia di Lecco Tandem Heart Outcome Data
42%
47%45%
36%
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
Thiele (n=41) Burkhoff (n=33)
30 d
ay m
orta
lity
(%)
Tandem HeartIABP
Improved haemodynamic parameters
Increase in bleeding, limb ischaemia, and sepsis
Thiele EHJ 2005;26:1276. Burkhoff AHJ 2006;152:e1
p=NS
Data: 3 aprile 2014
Evento: Tigullio
Titolo: Cardiogenic shock Autore: Stefano Savonitto
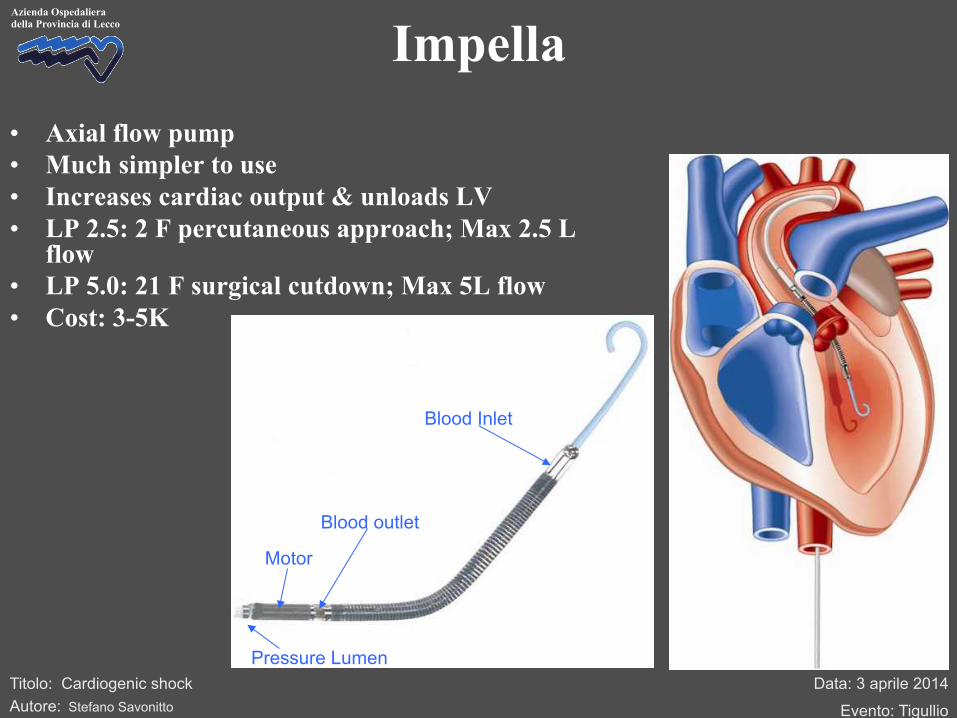
Azienda Ospedaliera della Provincia di Lecco Impella • Axial flow pump • Much simpler to use • Increases cardiac output & unloads LV • LP 2.5: 2 F percutaneous approach; Max 2.5 L
flow • LP 5.0: 21 F surgical cutdown; Max 5L flow • Cost: 3-5K
Pressure Lumen
Motor
Blood outlet
Blood Inlet

Data: 3 aprile 2014
Evento: Tigullio
Titolo: Cardiogenic shock Autore: Stefano Savonitto
Azienda Ospedaliera della Provincia di Lecco
Impella outcome data
• 1 RCT of Impella 2.5 in AMI Cardiogenic Shock
• ISAR-SHOCK
– 26 patient RCT Impella vs IABP – ↑ Cardiac Index, ↑ MAP (by 10mmHg) vs
IABP – Complications ≤ IABP
– No difference in mortality
Data: 3 aprile 2014
Evento: Tigullio
Titolo: Cardiogenic shock Autore: Stefano Savonitto
Azienda Ospedaliera della Provincia di Lecco
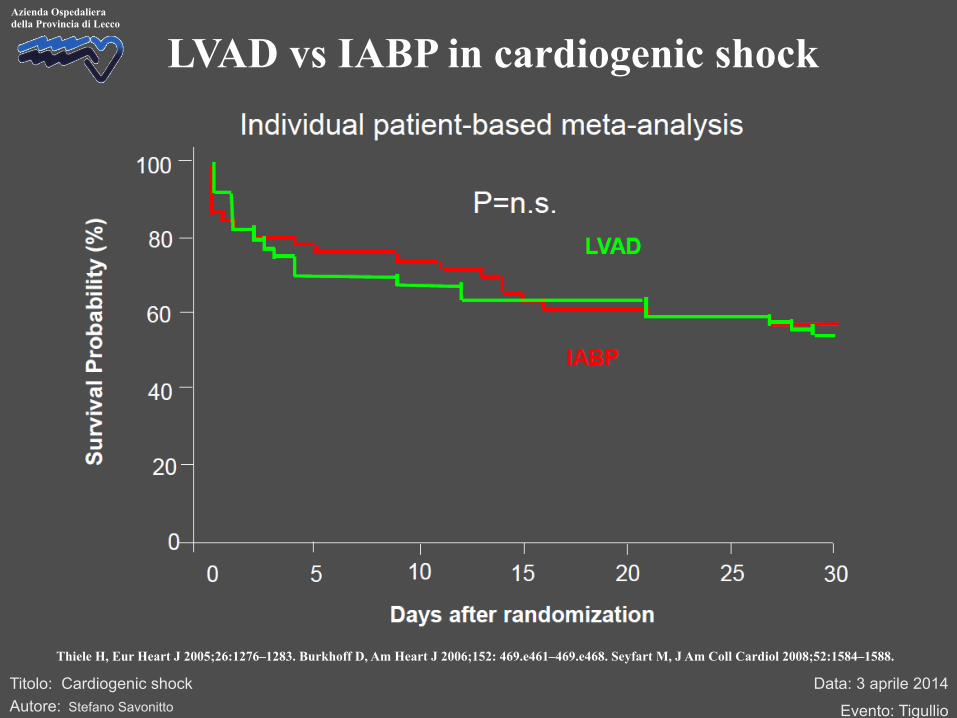
LVAD vs IABP in cardiogenic shock
Thiele H, Eur Heart J 2005;26:1276–1283. Burkhoff D, Am Heart J 2006;152: 469.e461–469.e468. Seyfart M, J Am Coll Cardiol 2008;52:1584–1588.

Data: 3 aprile 2014
Evento: Tigullio
Titolo: Cardiogenic shock Autore: Stefano Savonitto
Azienda Ospedaliera della Provincia di Lecco
Trial n/N n/N Relative Risk
95% CI Relative Risk 95% CI
0 0.5 1 2 3
Randomized trials in cardiogenic shock Follow-up
Revascularization (PCI/CABG) SHOCK SMASH Total
76/152 22/32 103/184
83/149 18/23 117/172
0.80 (0.66;0.98) 0.87 (0.66;1.29) 0.82 (0.70;0.98)
1 year 30 days
Early revascularization better
Medical therapy better
0.75 1.5 2.5 0.25
Noradrenaline better
0.75 (0.55;0.93) 64/145 50/135 28 days Dopamine better
Catecholamines SOAP II (CS subgroup)
In-hospital 15/40 13/40 1.15 (0.59;2.27) Up-stream abciximab better
Standard therapy better
Glycoprotein IIb/IIIa-Inhibitors PRAGUE-7
97/201 24/59 4/15 125/275
30 days 30 days 30 days
76/180 7/20 10/15 93/215
1.14 (0.91;1.45) 1.16 (0.59;2.69) 0.40 (0.13;1.05) 1.05 (0.85;1.29)
NO synthase inhibition better
Placebo better
NO synthase inhibitors TRIUMPH SHOCK-2 Cotter et al Total
30 days 1-year
7/19 155/299 126/319
6/21 152/296 129/319
IABP better
Standard therapy better
1.28 (0.45;3.72) 1.02 (0.88;1.19) 1.02 (0.88;1.19)
IABP IABP-SHOCK I IABP-SHOCK II Total
30 days 30 days 30 days
9/21 9/19 6/13 24/53
9/20 5/14 6/13 20/47
0.95 (0.48;1.90) 1.33 (0.57-3.10) 1.00 (0.44-2.29) 1.06 (0.68-1.66)
LVAD better
IABP better
LVAD Thiele et al Burkhoff et al Seyfarth et al Total
Updated from Thiele H. Eur Heart J 2010,31:1828-1835

Data: 3 aprile 2014
Evento: Tigullio
Titolo: Cardiogenic shock Autore: Stefano Savonitto
Azienda Ospedaliera della Provincia di Lecco
Thiele H. Eur Heart J 2010;31:1828-1835
Potential treatment algorithm in cardiogenic shock

Data: 3 aprile 2014
Evento: Tigullio
Titolo: Cardiogenic shock Autore: Stefano Savonitto
Azienda Ospedaliera della Provincia di Lecco
Miglioramento (Lattati/SVO2/QU)
Rivalutazione dopo 2 h
Adeguamento terapeutico
IABP
Continua terapia medica
Non miglioramento (Lattati/SVO2/QU)
Rivalutazione dopo 1 h
Non miglioramento
(Lattati/SVO2/QU) Miglioramento
(Lattati/SVO2/QU)
MCA: ECMO/VAD Continua terapia medica + IABP
Monitoraggio avanzato
Adrenalina >0,05γ/Kg/min + altro inotropo >6 PVC< 12 mmHg VAM se indicata
Swan-Ganz ECO
In presenza di indicatori clinici e strumentali di ipoperfusione da SBP/SC
Danno miocardico reversibile? NO: comincia a considerare MCA urgente SI: valuta trend
Flow Chart Operativa “De Gasperis 2006
Se indicazione a MCA
NO indicazione a MCA
Contattare: Cardiologo UCC Cardiologo C2 AR UCICT Cardiochirurgo
Data: 3 aprile 2014
Evento: Tigullio
Titolo: Cardiogenic shock Autore: Stefano Savonitto
Azienda Ospedaliera della Provincia di Lecco
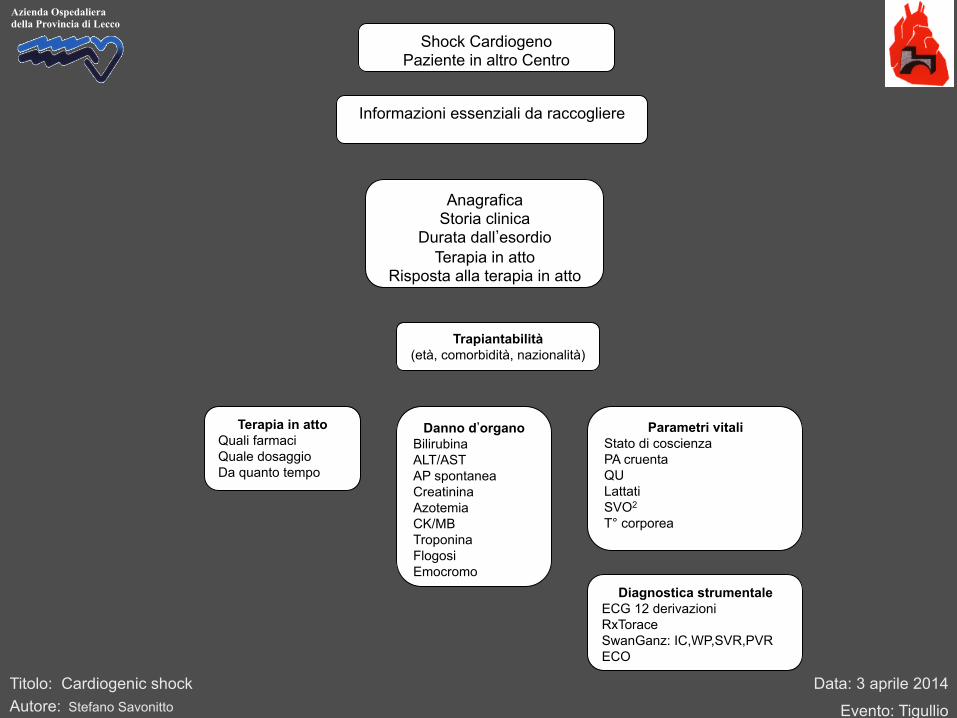
Shock Cardiogeno
Paziente in altro Centro
Terapia in atto Quali farmaci Quale dosaggio Da quanto tempo
Parametri vitali Stato di coscienza PA cruenta QU Lattati SVO2 T° corporea
Informazioni essenziali da raccogliere
Danno d’organo Bilirubina ALT/AST AP spontanea Creatinina Azotemia CK/MB Troponina Flogosi Emocromo
Trapiantabilità (età, comorbidità, nazionalità)
Anagrafica
Storia clinica
Durata dall’esordio
Terapia in atto
Risposta alla terapia in atto
Diagnostica strumentale ECG 12 derivazioni RxTorace SwanGanz: IC,WP,SVR,PVR ECO