Cattedra di Oncologia Medica Università di Palermopacs.unica.it/pacs/oncologiamedica1/2-81.pdf ·...
36
Chemioterapia nei Chemioterapia nei Tumori dell’Anziano: Tumori dell’Anziano: Rischi e Benefici Rischi e Benefici I. I. Carreca Carreca Cattedra di Oncologia Medica Cattedra di Oncologia Medica Università di Palermo Università di Palermo Innovazioni Terapeutiche Innovazioni Terapeutiche In Oncologia Medica In Oncologia Medica Policlinico Universitario Policlinico Universitario Cagliari Cagliari - - 24 Giugno 2005 24 Giugno 2005
Transcript of Cattedra di Oncologia Medica Università di Palermopacs.unica.it/pacs/oncologiamedica1/2-81.pdf ·...

Chemioterapia neiChemioterapia neiTumori dell’Anziano:Tumori dell’Anziano:
Rischi e BeneficiRischi e Benefici
I. I. CarrecaCarrecaCattedra di Oncologia MedicaCattedra di Oncologia Medica
Università di PalermoUniversità di Palermo
Innovazioni TerapeuticheInnovazioni TerapeuticheIn Oncologia MedicaIn Oncologia Medica
Policlinico UniversitarioPoliclinico UniversitarioCagliari Cagliari -- 24 Giugno 200524 Giugno 2005

Invecchiamento della popolazioneInvecchiamento della popolazione
••Riduzione del rischio di morte a tutte le etRiduzione del rischio di morte a tutte le etàà
••Riduzione della natalitRiduzione della natalitàà
••Invecchiamento della Invecchiamento della ““babybaby--boom generationboom generation”” del dopoguerradel dopoguerra
••Aumento Aumento % popolazione >65aa% popolazione >65aa: 18,2% (10.527.600/57.844.000): 18,2% (10.527.600/57.844.000)
••Aumento della Aumento della vita mediavita media: 77 M: 77 M; 83 F; 83 F
••Aumento dellAumento dell’’indice di vecchiaiaindice di vecchiaia: 127,1: 127,1
••Aumento dellAumento dell’’indice di dipendenza strutturale degli anzianiindice di dipendenza strutturale degli anziani: 27,1: 27,1
Fonte: ISTAT, Stime per l’anno 2001Fonte: ISTAT, Stime per l’anno 2001

Incidenza delle neoplasie Incidenza delle neoplasie ITALIA 2000 ITALIA 2000
proiezione per sesso ed etàproiezione per sesso ed età
((VerdecchiaVerdecchia etet al.al. EJC 2001)EJC 2001)
0
500
1000
1500
2000
2500
3000
3500
4000
Uomini Donne
25-29aa30-34aa35-39aa40-44aa45-49aa50-54aa55-59aa60-64aa65-69aa70-74aa75-79aa80-84aa
Frequenza per 100.000Frequenza per 100.000

Cancer risk increases with ageCancer risk increases with age
1,4
7,73
24,48
1,7
8,08
13,38
MaleFemale
30
25
20
15
10
5
00–39 40–59 60–74
Age (years)
Cum
ulat
ive
risk
in
Euro
pean
Uni
on (%
)
Ferlay J, et al. Eucan IARC CancerBase. Lyon:IARC Press; 1999. Updated September 29, 2000.

Incidenza neoplasie nell’anzianoIncidenza neoplasie nell’anzianoSedi più frequentiSedi più frequenti
Polmone
Prostata
Colon-retto
Vescica
Altri
Polmone
Mammella
Colon-retto
Utero
AltriUomini Donne
18,2
35,811,3
28,2
6,5
Età 65-74 aa
34,9
136,4
17,3
28,4
Fonte: Fonte: NCI SEER Program e NPCRNCI SEER Program e NPCR

Incidenza neoplasie nell’anzianoIncidenza neoplasie nell’anzianoSedi più frequentiSedi più frequenti
Polmone
Prostata
Colon-retto
Vescica
Altri
Polmone
Mammella
Colon-retto
Utero
Altri
Età>75 aa
Uomini Donne
31,6 40
14,5
16,9
28,38,7
18,7
13,2
23,5
4,6
Fonte: Fonte: NCI SEER Program e NPCRNCI SEER Program e NPCR
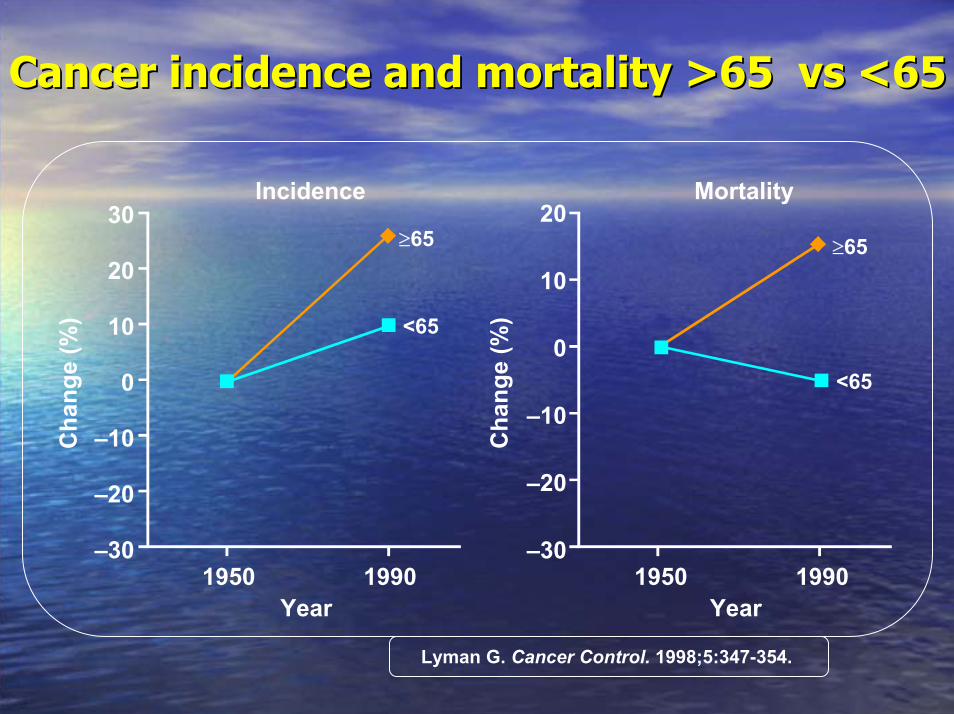
Cancer incidence and mortality >65 vs <65Cancer incidence and mortality >65 vs <65
30
20
10
0
–10
–20
–30
20
10
0
–10
–20
–30
Cha
nge
(%)
1950 1990 1950 1990Year Year
Cha
nge
(%)
Incidence Mortality
≥65
<65
<65
≥65
Lyman G. Cancer Control. 1998;5:347-354.

Cancer incidence and mortality are Cancer incidence and mortality are increased in the elderly (>65 years)increased in the elderly (>65 years)
IncidenceIncidence MortalityMortality
OvarianOvarian BreastBreast NHLNHL LungLung ColorectalColorectal OvarianOvarian BreastBreast NHLNHL LungLung ColorectalColorectal
Over 65Over 65Under 65Under 65
NHL = non-Hodgkin’s lymphoma
Cas
es (%
)C
ases
(%)
0
20
40
60
80
100
Ferlay J, et al. Eucan IARC CancerBase. Lyon:IARC Press; 1999. Updated September 29, 2000.

Comorbidity Comorbidity Prevalence in Cancer Patients by AgePrevalence in Cancer Patients by Age
0%
10%
20%
30%
40%
50%
60%
Perc
ent
55-59 60-64 65-69 70-74 75-79 80-84 85+Age Group
Hypertension
Previous malignancy
Arthritis
High severity heart disease
Stroke/TIA
COPD
Diabetes
Heart disease, moderate
Yancik R, Wesley M, Ries L, Havlik R, Edwards B, Yates, J, Effect of Age and Comorbidity in
Cancer Patients, JAMA, 2001, Vol 285, No.7, 885-892

Physiological AgingPhysiological Aging--related Changesrelated Changes(20 to 80 yrs)(20 to 80 yrs)
test changeBody weight/fat + 35%
Plasmatic volume - 8%Albumine - 10%globulins - 10%
Total body water - 17%Extracellular fluids - 40%
Cardiac electric stym/velocity - 20%Cardiac capacity - 40%Ejection fraction - 35%
Vital capacity - 60%glomerular filtration - 50%
Renal/GI ematic circulation - 40%

Aging affects chemotherapy Aging affects chemotherapy toxicity and effectivenesstoxicity and effectiveness
•• Pharmacokinetic changes that increase toxicityPharmacokinetic changes that increase toxicity–– decreased volume of distribution (Vd)decreased volume of distribution (Vd)–– decreased decreased glomerular glomerular filtration rate (GFR)filtration rate (GFR)–– decreased hepatic metabolismdecreased hepatic metabolism–– decreased intestinal absorptiondecreased intestinal absorption
•• Pharmacodynamic Pharmacodynamic changes that limit effectivenesschanges that limit effectiveness–– increased expression of increased expression of multidrug multidrug resistance (MDR) generesistance (MDR) gene–– decreased apoptosisdecreased apoptosis–– increased tumour anoxiaincreased tumour anoxia–– decreased cell proliferationdecreased cell proliferation
Balducci L et Al.., Oncologist. 2000;5:224-237.

Anemia: Anemia: AnAn IndipendentIndipendent RiskRisk FactorFactor forfor DeathDeath
•• MortalityMortality riskrisk isis significantlysignificantly increasedincreased in in individualsindividuals agedaged >75 >75 yearsyears withwith anemiaanemia11
•• ThisThis increasedincreased riskrisk isis indipendentindipendent of of diseasesdiseases at at baselinebaseline, or , or functionalfunctionalimpairmentimpairment11
•• OtherOther data indicate data indicate thatthat mortalitymortality isis alsoalsoincreasedincreased in in elderlyelderly individualsindividuals >65 years>65 years22
1. Izaks G, et al JAMA. 1999;281:1714 - 17172. Ania B, et al. J Am Geriatr Soc 1997;45:825-831

Bone Marrow CompositionBone Marrow Composition
CellularityCellularity
•• 30% fat 30% fat -- youngyoung•• 50% fat 50% fat -- normalnormal•• 70% fat 70% fat -- elderlyelderly

Le fasi della Le fasi della mucositemucosite oraleorale1. Infiammazione 1. Infiammazione 2. Ulcerazione/Infezione2. Ulcerazione/Infezione3. Danno epiteliale3. Danno epiteliale

Effect of Treatment Methods onEffect of Treatment Methods onTotal Fatigue ScoreTotal Fatigue Score
Chemotherapy Radiationtherapy
Hormonal therapy
Chemotherapy + radiation
therapy
54.5
43.5
32.5
21.5
10.5
0
Total fatigue score
Woo, Oncol. Nursing Forum, 1998

Undertreatment Undertreatment in elderly patientsin elderly patients
•• Aggressive lymphomaAggressive lymphoma–– older patients less likely to be treated for cure,older patients less likely to be treated for cure,
less likely to survive for 5 yearsless likely to survive for 5 years
•• Breast cancerBreast cancer–– older women less likely to be invited into clinical trialsolder women less likely to be invited into clinical trials
•• Stage III colon cancer Stage III colon cancer –– older patients less likely to receive chemotherapyolder patients less likely to receive chemotherapy
•• Lung cancerLung cancer–– older patients receive delay in diagnosis and less older patients receive delay in diagnosis and less
aggressive treatmentaggressive treatmentChen C, et al. Leuk Lymphoma. 2000;38:327-334.
Kemeny M, et al. Proc Am Soc Clin Oncol. 2000; 19:602a, Abstract 237I.Mahoney T, et al. Arch Surg. 2000;135:182-185.
Peake M. Presentation at 96th International Conference of Am Thoracic Soc, Toronto, May 2000.

Likelihood of receiving fullLikelihood of receiving full--dose dose chemotherapy decreases with agechemotherapy decreases with age
Patients receiving <85% of planned doseadjuvant CMF (every 4 weeks) for breast cancer75
50
25
0
Patie
nts
(%)
<65 (n = 223) ≥65 (n = 76)
35.4
51.9P <0.001
Age (years)
Crivellari D, et al. J Clin Oncol. 2000;18:1412-1422.


To TreatTo Treatoror
Not To TreatNot To Treat
ELDERLY ELDERLY PATIENTSPATIENTS
??

FrialtyFrialty: : CriteriaCriteria
• Age > 85 years
• Dependence in one or more ADL
• Presence of three or more comorbidities
• Presence of one or more geriatric syndromes

Tools for Tools for Assessement Assessement of Frailtyof Frailty
Variabili per la definizionePeso, perdita di peso e BMI
CES-D scale per spossatezzaMinnesota Leisure Time Kcal/sett.)
Camminare per 15 piedi (ca. 5 metri)Forza della stretta di mano con dinamometro
Variabili di controlloesame records clinici secondo algoritmi
indicatori biochimici e strumentalidi patologia (ECG, Doppler TSA, …)
MMSEDigit Symbol Substitution testADL, IADL, 16 mobility tasks
Abitudine al fumo

Comprehensive geriatric assessment Comprehensive geriatric assessment reveals stages of agingreveals stages of aging
•• Group 1Group 1–– functionallyfunctionally independent, no serious independent, no serious comorbiditycomorbidity–– standard cancer treatmentstandard cancer treatment
•• Group 2Group 2–– partially dependent, partially dependent, ≤≤2 2 comorbid comorbid conditionsconditions–– modified cancer treatmentmodified cancer treatment
•• Group 3Group 3–– dependent,dependent, ≥≥3 3 comorbid comorbid conditions, any geriatric conditions, any geriatric
syndromesyndrome–– palliative treatmentpalliative treatment
Balducci L, et al. Oncologist. 2000;5:224-237.

Older women with breast cancer Older women with breast cancer benefit from adjuvant chemotherapybenefit from adjuvant chemotherapy
22
14
18
8
Age 50–59 years (n = 3,411)Age 60–69 years (n = 3,413)
Recurrence Mortality
*P = NA
*P <0.00001
*P = 0.0005
*P = 0.05
Ris
k re
duct
ion
(%)
25
20
15
10
5
0NA = not available*Two-sided statistical analysis of risk for patients receiving adjuvant chemotherapy compared with those receiving no chemotherapy
Early Breast Cancer Trialists’ Collaborative Group. Lancet. 1998;352:930-942.

Chemotherapy yields comparable outcomes in Chemotherapy yields comparable outcomes in younger and older patients with lung canceryounger and older patients with lung cancer
36 34
<70 ≥70
Med
ian
surv
ival
(wee
ks)
60
50
40
30
20
10
0
52
42
Age (years) Age (years)
n = 488 n = 86
n = 110
n = 25
Cisplatin + paclitaxel or etoposide1 Carboplatin + paclitaxel2
60
50
40
30
20
10
034–84 ≥70
Med
ian
surv
ival
(wee
ks)
1Langer C, et al. Proc Am Soc Clin Oncol. 2000;19:489a. Abstract 1912.2Rosvold E, et al. Proc Am Soc Clin Oncol. 1999;18:478a. Abstract 1846.

Classification by staging group Classification by staging group increases with ageincreases with age
Age (years)
Patie
nts
(%)
Group 3Group 2Group 1
100
80
60
40
20
070 80 90
Balducci L, et al. Oncologist. 2000;5:224-237.

When to use primary prophylaxis?When to use primary prophylaxis?ASCO recommendationsASCO recommendations
Administer chemotherapywithout CSF support
Yes
Yes
No
No
Consider chemotherapy with CSFsupport in first and subsequent cycles
*eg, history of febrile neutropenia with similar doses, previous chemo/radiotherapyASCO = American Society of Clinical Oncology - CSF = colony-stimulating factor
Is the chemotherapy regimen associatedwith a ≥40% risk of febrile neutropenia*?
Is the patient at high risk forinfectious complications?*
Ozer H, et al. J Clin Oncol. 2000;18:3558-3585.

When to use secondary prophylaxis?When to use secondary prophylaxis?ASCO recommendationsASCO recommendations
Yes
Yes
No
No
Dose reduction/delay innext cycle if appropriate
Continue chemotherapycycles as planned
Did the patient experience febrileor prolonged neutropenia
during the previous cycle?
Will dose reduction/delaycompromise treatment goal?
Administer chemotherapy withCSF support in subsequent cycles
Ozer H, et al. J Clin Oncol. 2000;18:3558-3585.

Factors guiding cancer managementFactors guiding cancer managementin elderly patientsin elderly patients
Disease factorsDisease factorscellular typecellular typestagingstaging
Patient factorsPatient factorsoverall fitnessoverall fitnesscomorbiditiescomorbiditiesfunctional statusfunctional statusmental statusmental statusfamily/social supportfamily/social support
Decision if and how to treat
Balducci L, et al. Oncology. 2000;14:221-227.

Guidelines for the Management of the Guidelines for the Management of the Older Cancer PatientOlder Cancer Patient(NCCN ’03,’04,’05): CHEMOTHERAPY(NCCN ’03,’04,’05): CHEMOTHERAPY
•• ADJUST FIRST DOSE OF CHEMOTHERAPY TO ADJUST FIRST DOSE OF CHEMOTHERAPY TO RENAL FUNCTION FOR PATIENTS AGED 65+ RENAL FUNCTION FOR PATIENTS AGED 65+
•• PROPHILACTIC GROWTH FACTORS FOR PROPHILACTIC GROWTH FACTORS FOR PATIENTS AGED 65+ RECEIVING MODERATELY PATIENTS AGED 65+ RECEIVING MODERATELY TOXIC REGIMENS (CHOP, CA, FEC 100) AND FOR TOXIC REGIMENS (CHOP, CA, FEC 100) AND FOR INDUCTION AND CONSOLIDATION OF AMLINDUCTION AND CONSOLIDATION OF AML
•• MAINTAIN HB MAINTAIN HB >> 12 GM/DL12 GM/DL



Management of elderly cancer patientsManagement of elderly cancer patients
Life-prolongingtreatment Palliation
Assessment
Group 1 Group 2 Group 3
Life expectancy
>Cancer <Cancer
Treatmenttolerance
Yes No
Balducci L, et al. Oncologist. 2000;5:224-237.

Targeted prescription of medicines:Targeted prescription of medicines:
applied applied pharmacogeneticspharmacogenetics
informed physician diagnosisinformed physician diagnosisSavings: time, money & Savings: time, money &
illness illness
drug d
drug a
drug c
drug b
diagnostic
todaytodayempirical prescriptionempirical prescription
“mass market”“mass market”
individual physician experienceindividual physician experienceCCost: time, money & wellost: time, money & well--
beingbeing
drug b
drug c
drug a
trial trial & &
switchswitch
futurefuturerational prescriptionrational prescription
“individualized”“individualized”
definedefine&&
treattreatdrug d

In In clinicalclinical practice…practice…....
•• Selezione della paziente mediante valutazioneSelezione della paziente mediante valutazionegeriatricageriatrica completa.completa.•• Adattamento della dose iniziale ( funzionalità renaleAdattamento della dose iniziale ( funzionalità renalee cardiaca ).e cardiaca ).•• Mantenimento dei livelli di Mantenimento dei livelli di HbHb > 12g/dL con > 12g/dL con EpoEpo•• Attuazione tempestiva di adeguata idratazione perAttuazione tempestiva di adeguata idratazione percontrollare la controllare la mucositemucosite..•• In età In età >> 65 anni uso profilattico dei CSF per tossicità65 anni uso profilattico dei CSF per tossicitàematologicaematologica moderatamoderata--intensa.intensa.

ConclusionsConclusions
•• Age is not a contraindication to fullAge is not a contraindication to full--dose dose therapytherapy
•• Main limiting factors Main limiting factors –– poor overall health and functionpoor overall health and function–– presence of presence of comorbiditiescomorbidities
•• Elderly are more susceptible to Elderly are more susceptible to myelotoxicitymyelotoxicity
•• In elderly with good performance status,In elderly with good performance status,equal treatment yields equal benefitequal treatment yields equal benefit
•• Prophylactic use of GProphylactic use of G--CSF helps maintainCSF helps maintainchemotherapy dose intensitychemotherapy dose intensity

Associazione Italiana per la RicercaAssociazione Italiana per la RicercaIn Oncologia e negli Anziani In Oncologia e negli Anziani -- AIRONAAIRONAWork in Work in progress…progress…Portale di InformazionePortale di Informazionee Divulgazione Scientifica:e Divulgazione Scientifica:
--News in Oncologia News in Oncologia GeriatricaGeriatrica--Informazioni per pazienti e “Informazioni per pazienti e “caregiverscaregivers””--Iniziative ScientificoIniziative Scientifico--CulturaliCulturali