





Le lingue
Pagine
Legale

Integrazione tra terapia chirurgica e terapia medica.Nefrectomia nel ca metastaticoNefrectomia nel ca metastatico
Cinzia Ortega M.D.Medical Oncology I
Fondazione del Piemonte per l’Oncologia

SCUOLA DI URONCOLOGIA: TUMORE del RENE
Integrazione tra terapia chirurgica e terapia medica.Nefrectomia nel ca metastaticoNefrectomia nel ca metastatico
Cinzia Ortega M.D.Medical Oncology I
Fondazione del Piemonte per l’Oncologia
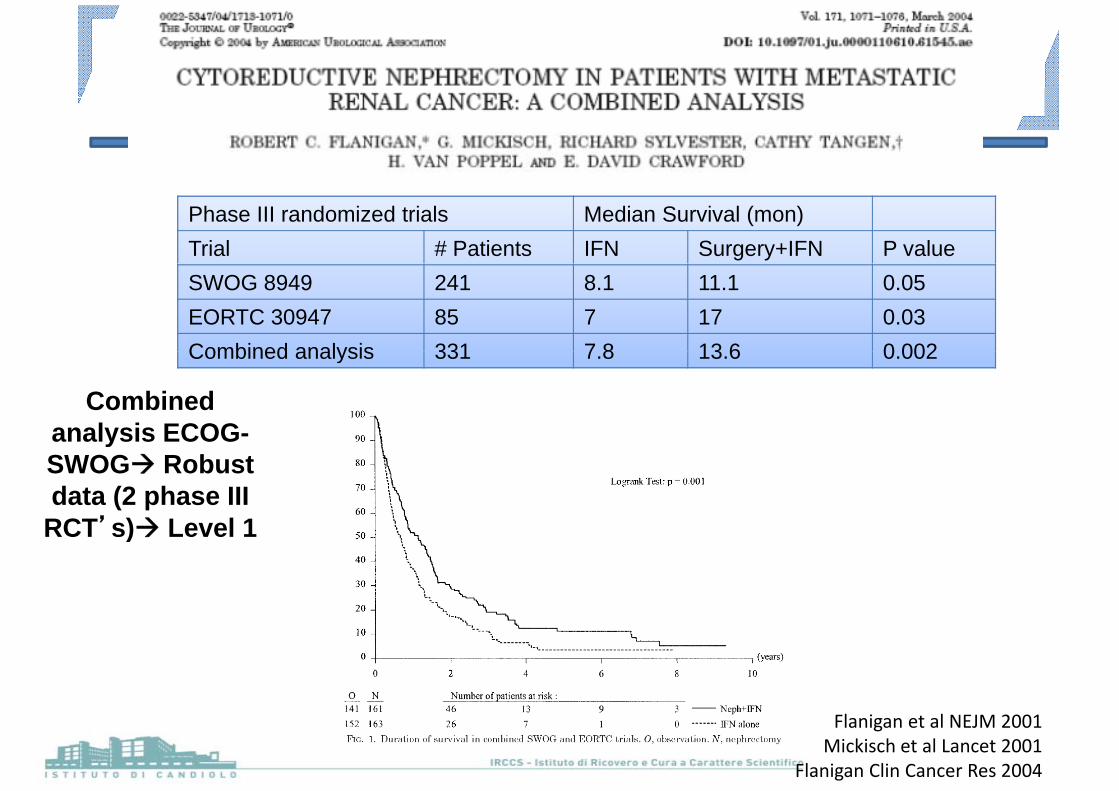
Phase III randomized trials Median Survival (mon)Trial # Patients IFN Surgery+IFN P valueSWOG 8949 241 8.1 11.1 0.05EORTC 30947 85 7 17 0.03Combined analysis 331 7 8 13 6 0 002Combined analysis 331 7.8 13.6 0.002
Combined analysis ECOG-analysis ECOGSWOG Robust data (2 phase III
RCT’s) Level 1RCT s) Level 1
Flanigan et al NEJM 2001Mickisch et al Lancet 2001
Flanigan Clin Cancer Res 2004
2009: In the era of targeted therapies is cytoreductive nephrectomy still necessary?
We now have “better” systemic therapies treating all tumor sites
Why delay administration of systemic treatment that improves PFS and survival?
Responses now seen in primary tumor (20‐30% tumor srinkage)srinkage)Consider possible perioperative complications of surgery
Di i d i t ti i dDisease progression during postoperative recovery period may preclude systemic therapy
Cytoreductive nephrectomy is not for everyone patients’selection
Theoretical concernsTheoretical concerns
Angiogenesis (VEGF) plays a primary role in wound healing
Possible delay of wound healing Dehiscence/anastomotic y gdisruption
Antiangiogenic agents inhibit repair and regenerationAntiangiogenic agents inhibit repair and regeneration of the vasculature
P ibl i ti Bl di /Th b iPossible perioperative Bleeding/Thrombosis
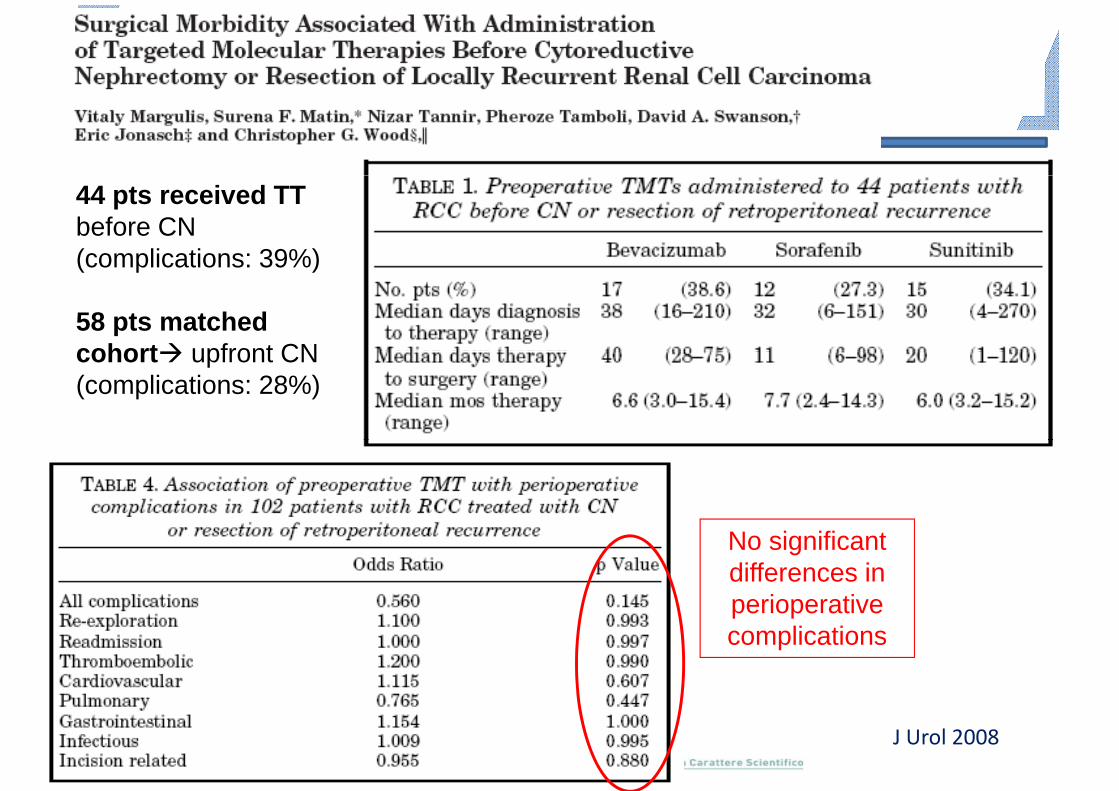
44 pts received TT before CN (complications: 39%)(complications: 39%)
58 pts matched cohort upfront CNcohort upfront CN(complications: 28%)
No significant differences in perioperative p pcomplications
J Urol 2008
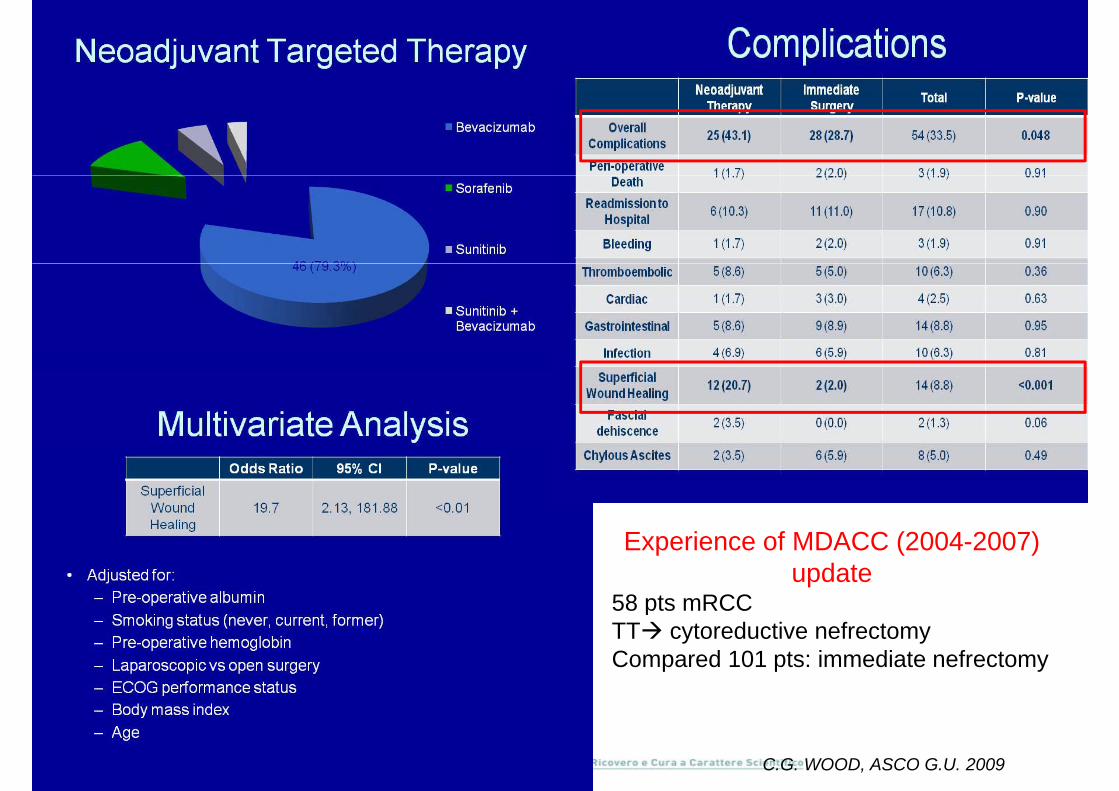
Experience of MDACC (2004-2007) update
58 pts mRCCpTT cytoreductive nefrectomyCompared 101 pts: immediate nefrectomy
C.G. WOOD, ASCO G.U. 2009

Risk of postoperative disease progression
TT after
Retrospective, 23/498 pts T4NxM1/
TT after surgery
16/23 clear cell ;
9/23 sarcomatoid features
Median OS: 6.8 mos3/23 postoperative complications3/23 postoperative complications5/23 progressed after nephrectomy
no systemic therapyno systemic therapy
Urology 2007
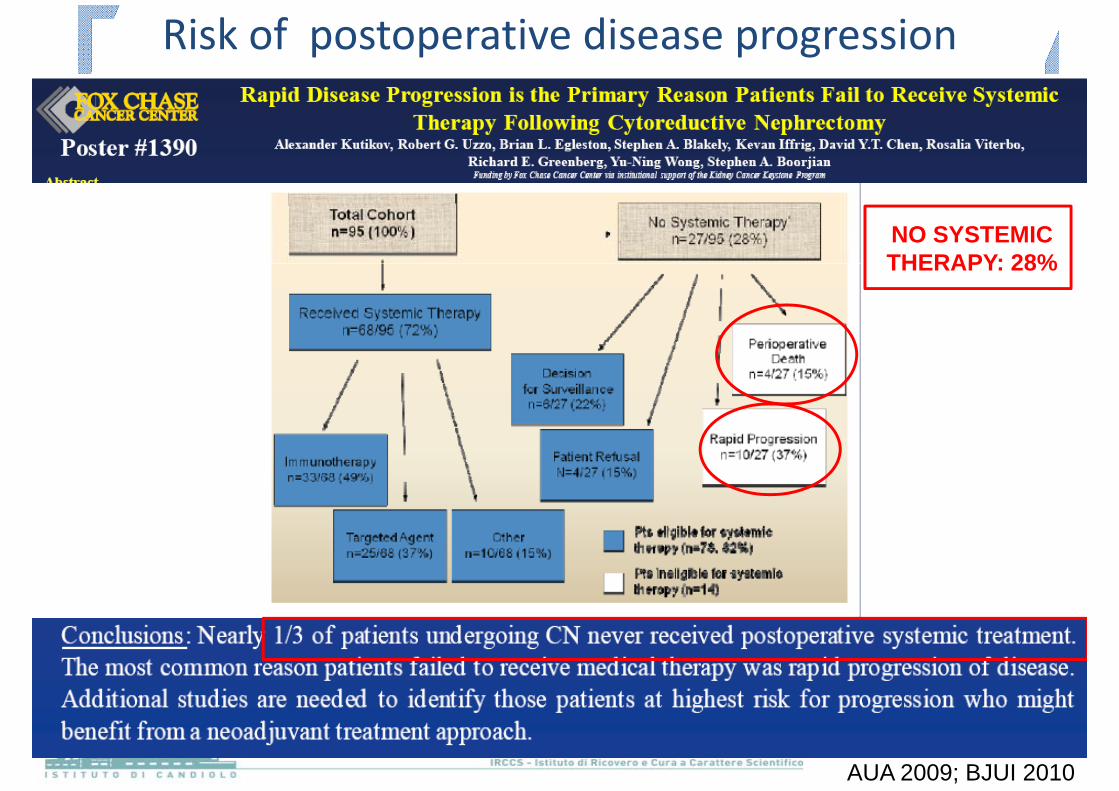
Risk of postoperative disease progression
NO SYSTEMIC THERAPY: 28%THERAPY: 28%
AUA 2009; BJUI 2010
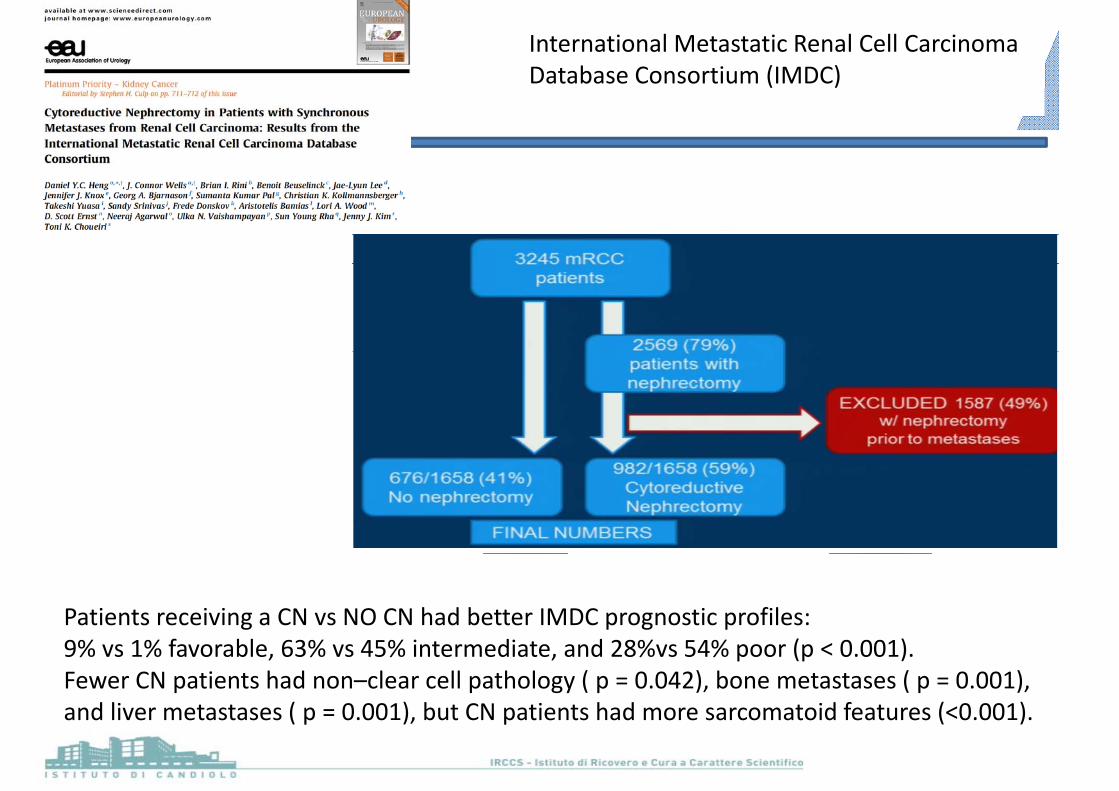
International Metastatic Renal Cell Carcinoma Database Consortium (IMDC)
Patients receiving a CN vs NO CN had better IMDC prognostic profiles:Patients receiving a CN vs NO CN had better IMDC prognostic profiles: 9% vs 1% favorable, 63% vs 45% intermediate, and 28%vs 54% poor (p < 0.001). Fewer CN patients had non–clear cell pathology ( p = 0.042), bone metastases ( p = 0.001), d l ( ) b h d d f ( )and liver metastases ( p = 0.001), but CN patients had more sarcomatoid features (<0.001).
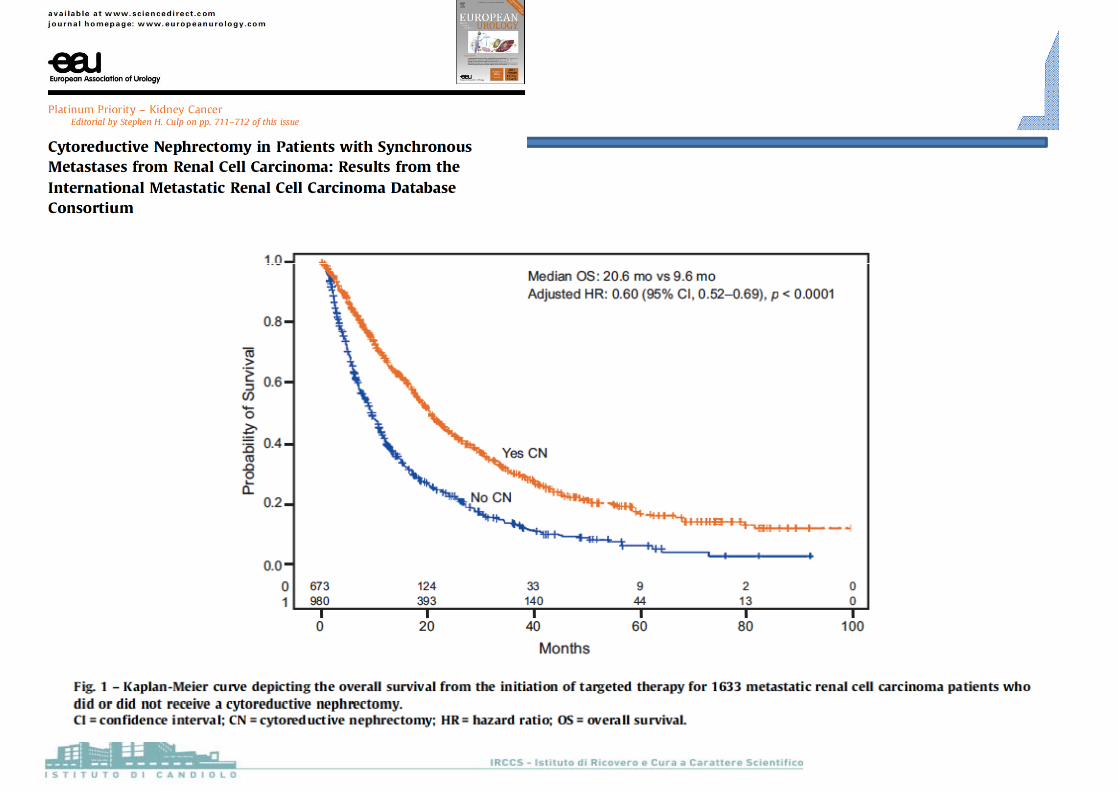
Heng, Eur Urol 2014
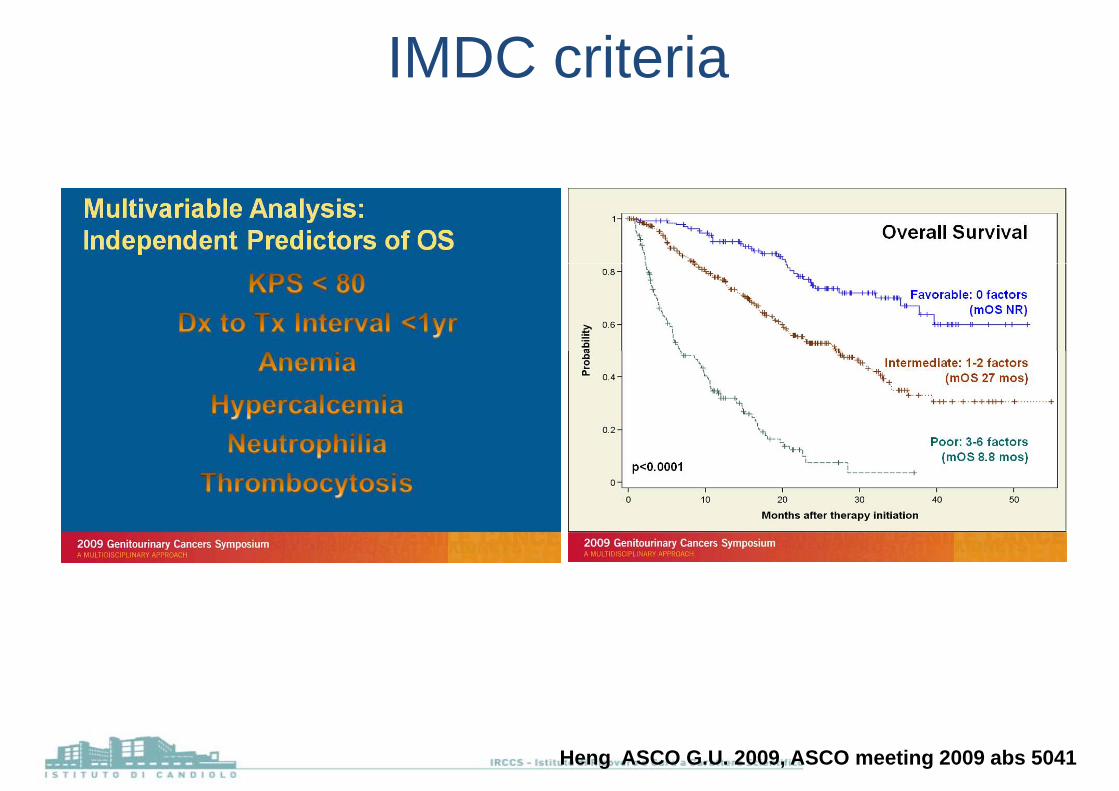
IMDC criteria
Heng ASCO G.U. 2009, ASCO meeting 2009 abs 5041
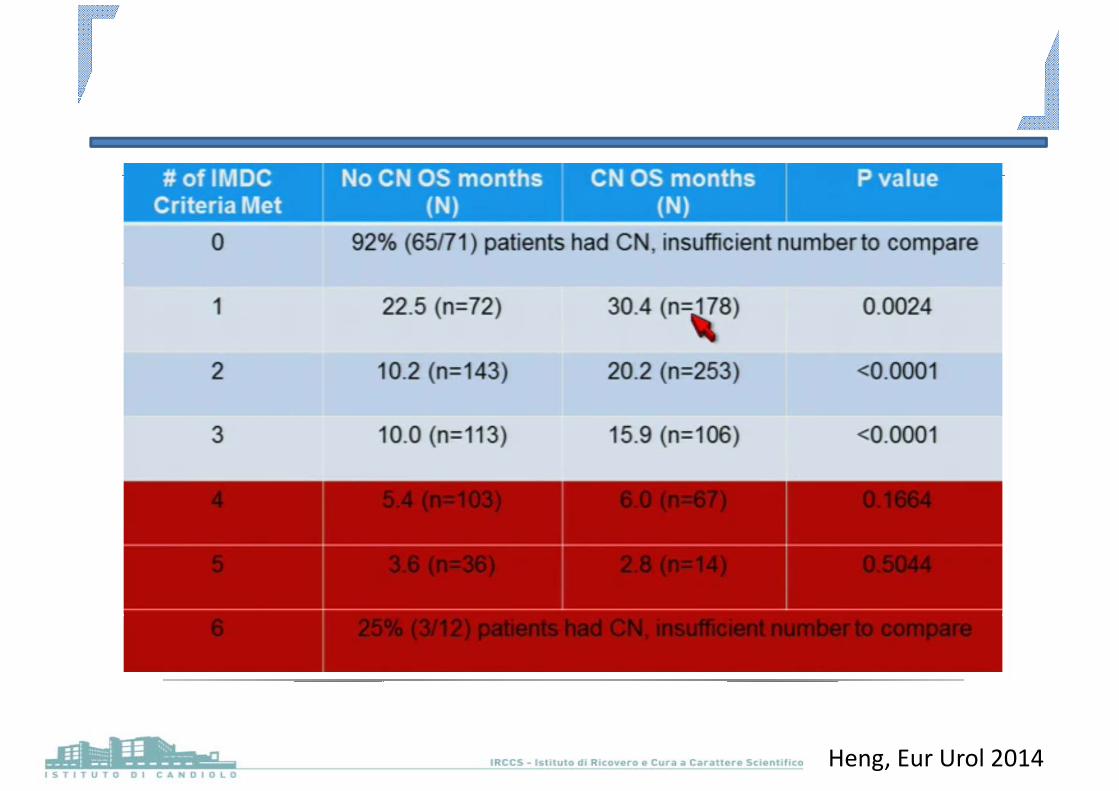
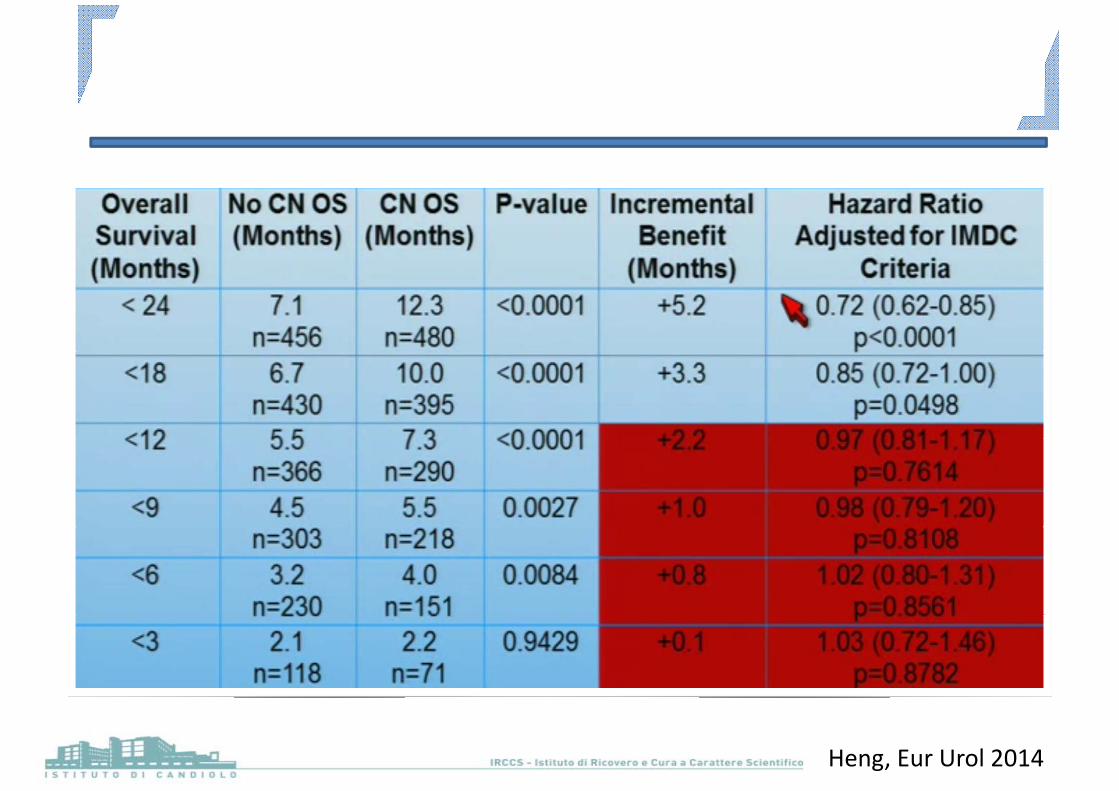
Heng, Eur Urol 2014
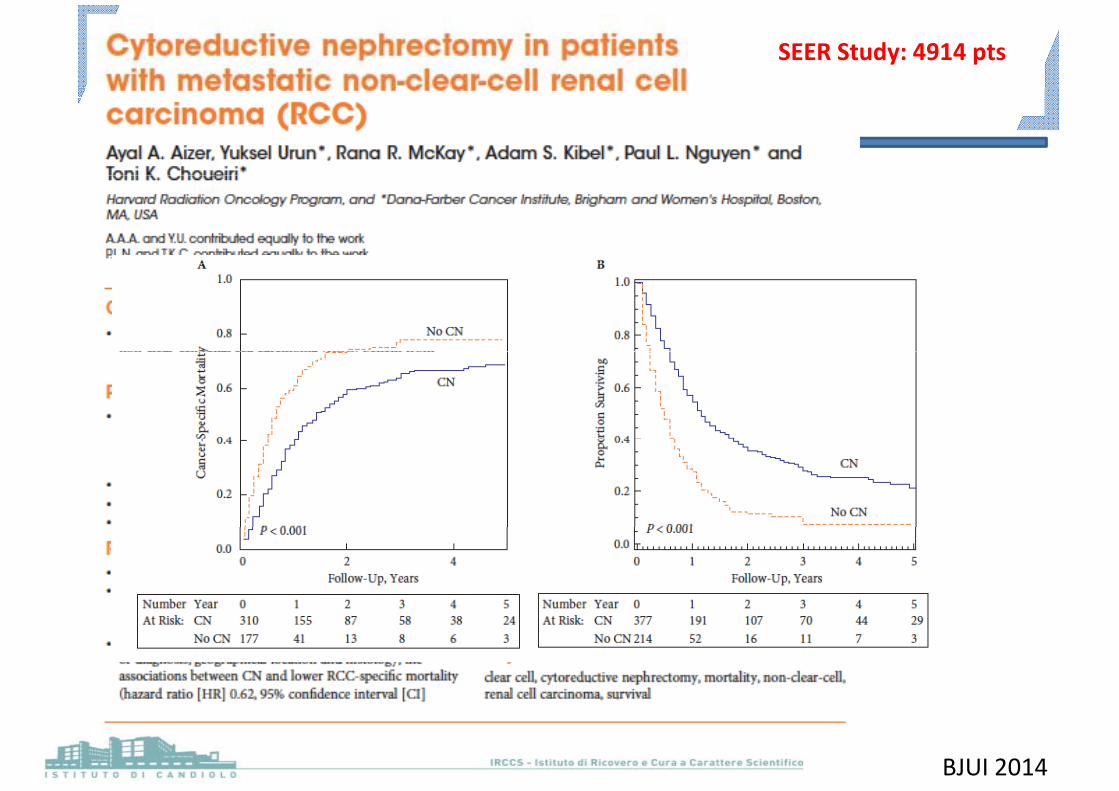
SEER Study: 4914 pts
BJUI 2014
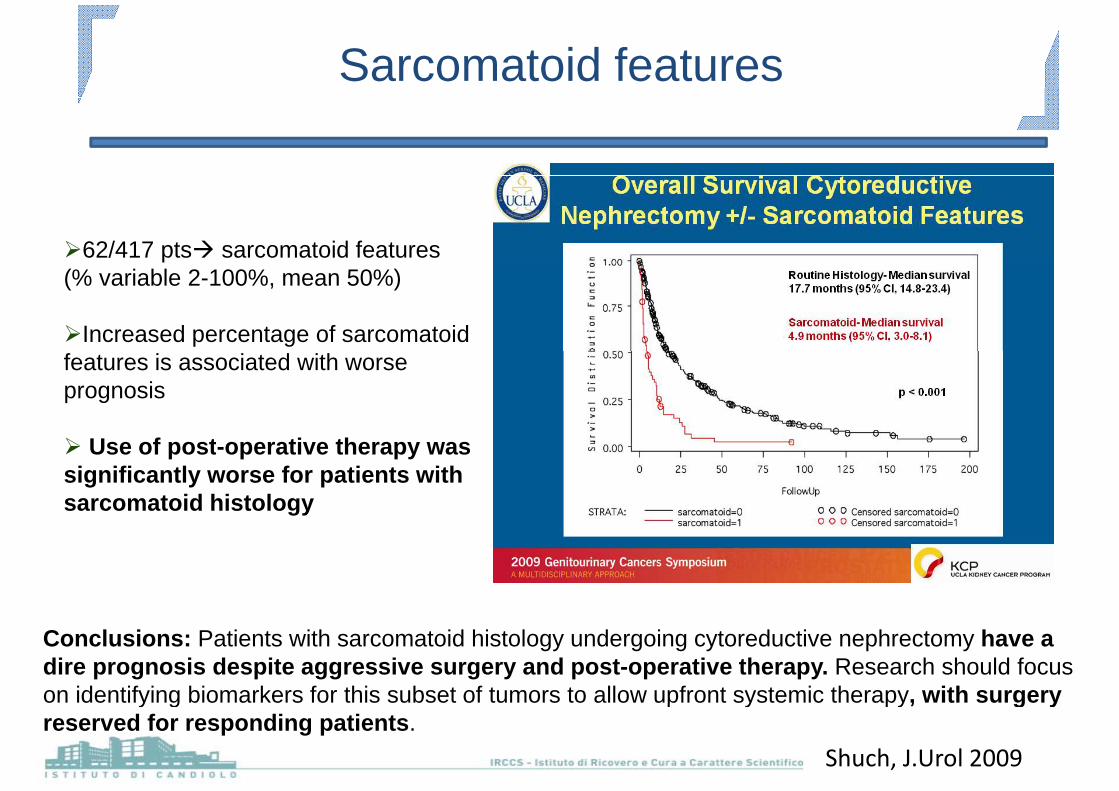
Sarcomatoid features
62/417 pts sarcomatoid features(% variable 2-100%, mean 50%)
Increased percentage of sarcomatoid features is associated with worse prognosis
U f t ti thUse of post-operative therapy was significantly worse for patients with sarcomatoid histology
Conclusions: Patients with sarcomatoid histology undergoing cytoreductive nephrectomy have a dire prognosis despite aggressive surgery and post-operative therapy. Research should focus on identifying biomarkers for this subset of tumors to allow upfront systemic therapy, with surgery o de y g b o a e s o s subse o u o s o a o up o sys e c e apy, t su ge yreserved for responding patients.
Shuch, J.Urol 2009
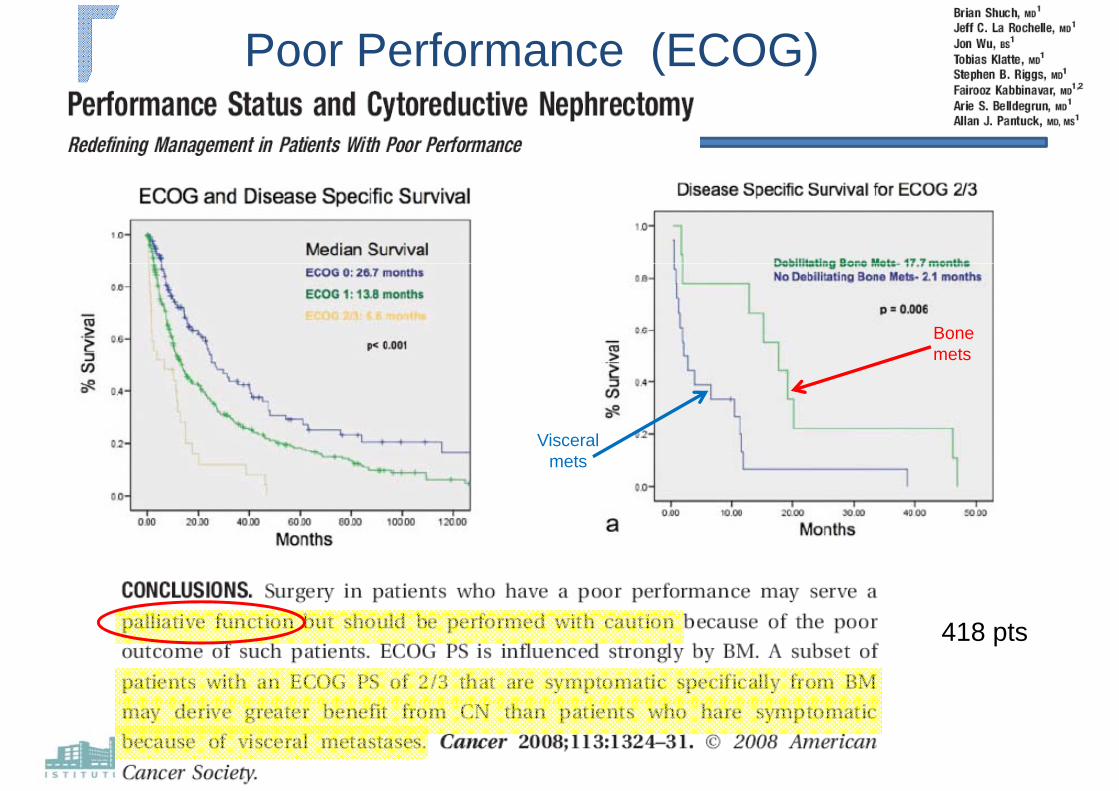
Poor Performance (ECOG)
Bone metsmets
VisceralVisceral mets
418 pts
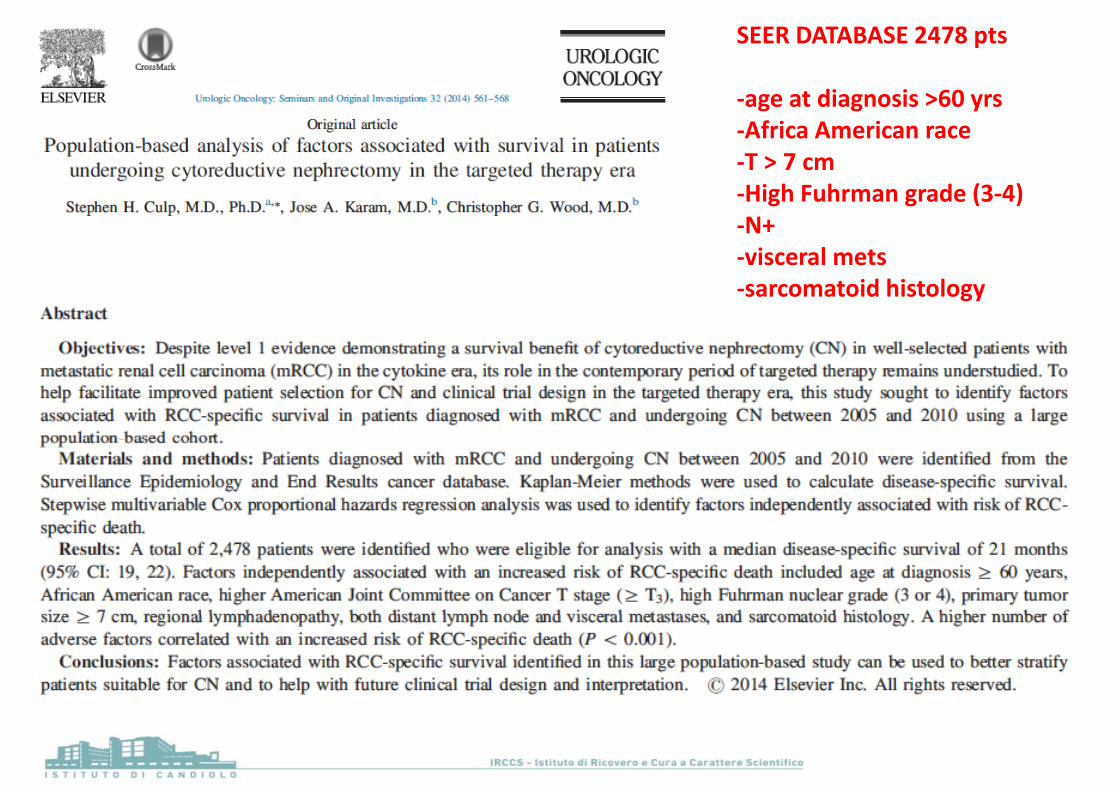
SEER DATABASE 2478 pts
‐age at diagnosis >60 yrs‐Africa American race‐T > 7 cm‐High Fuhrman grade (3‐4)‐N+‐visceral metsvisceral mets‐sarcomatoid histology
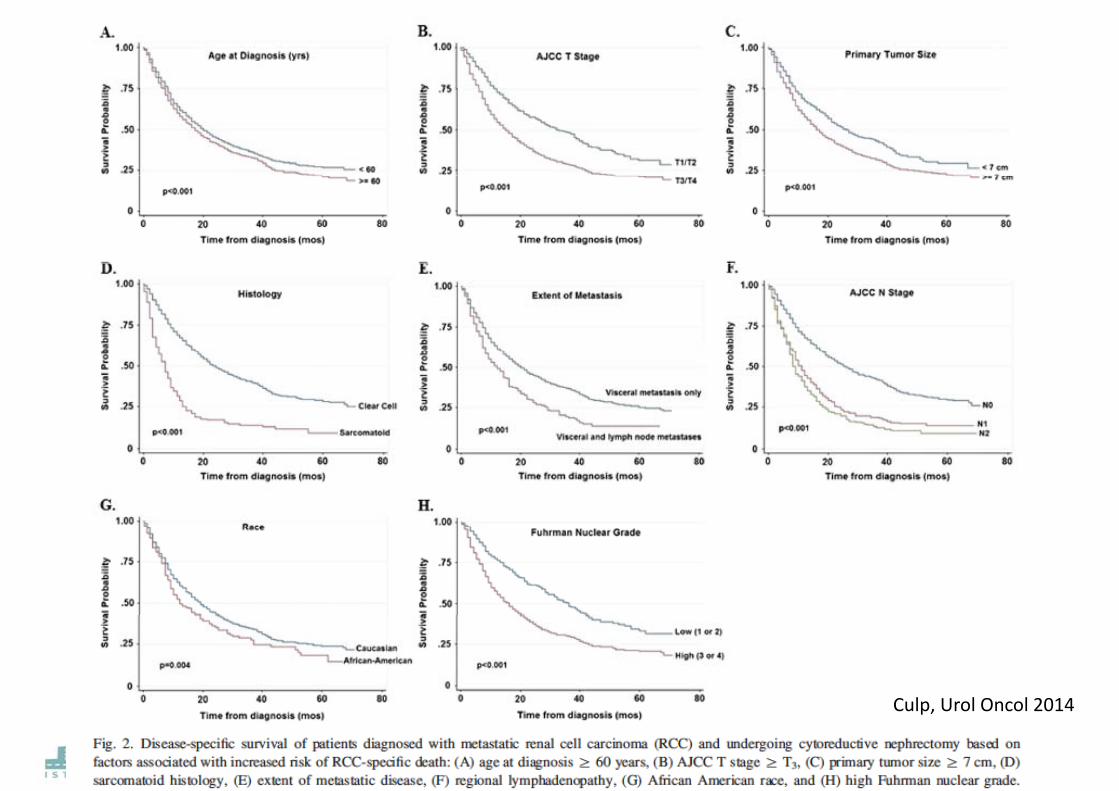
Culp Urol Oncol 2014Culp, Urol Oncol 2014
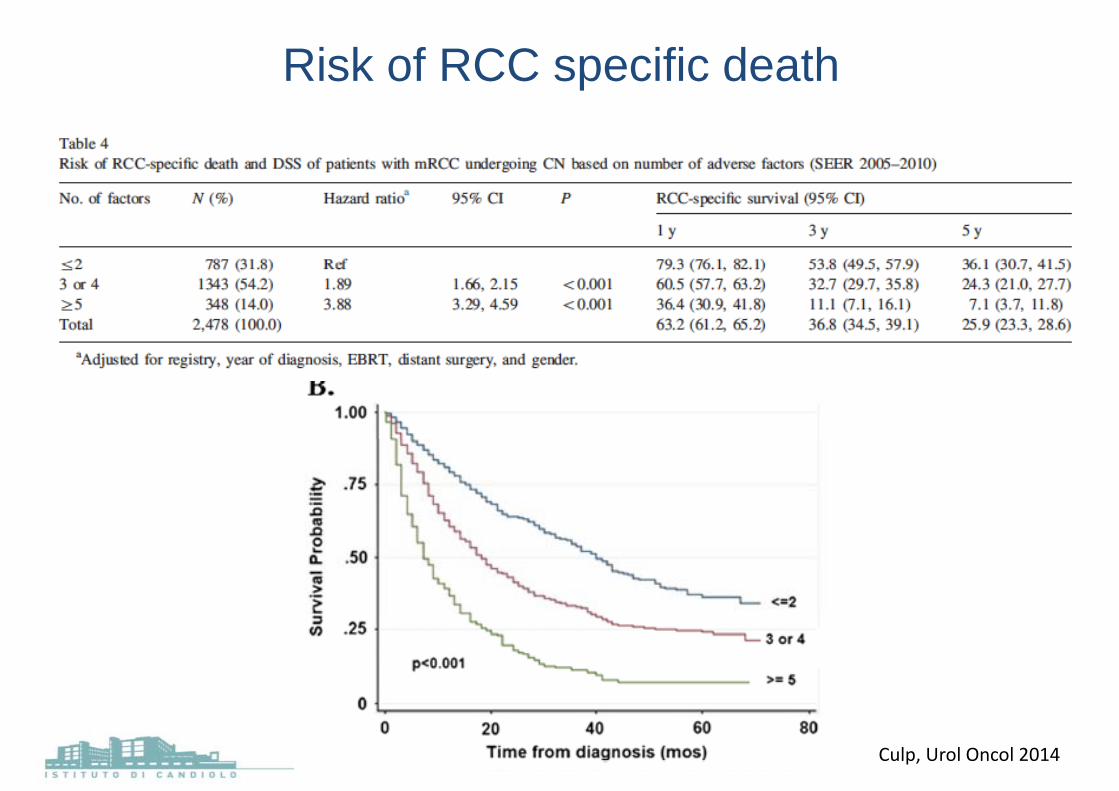
Risk of RCC specific death p
Culp, Urol Oncol 2014
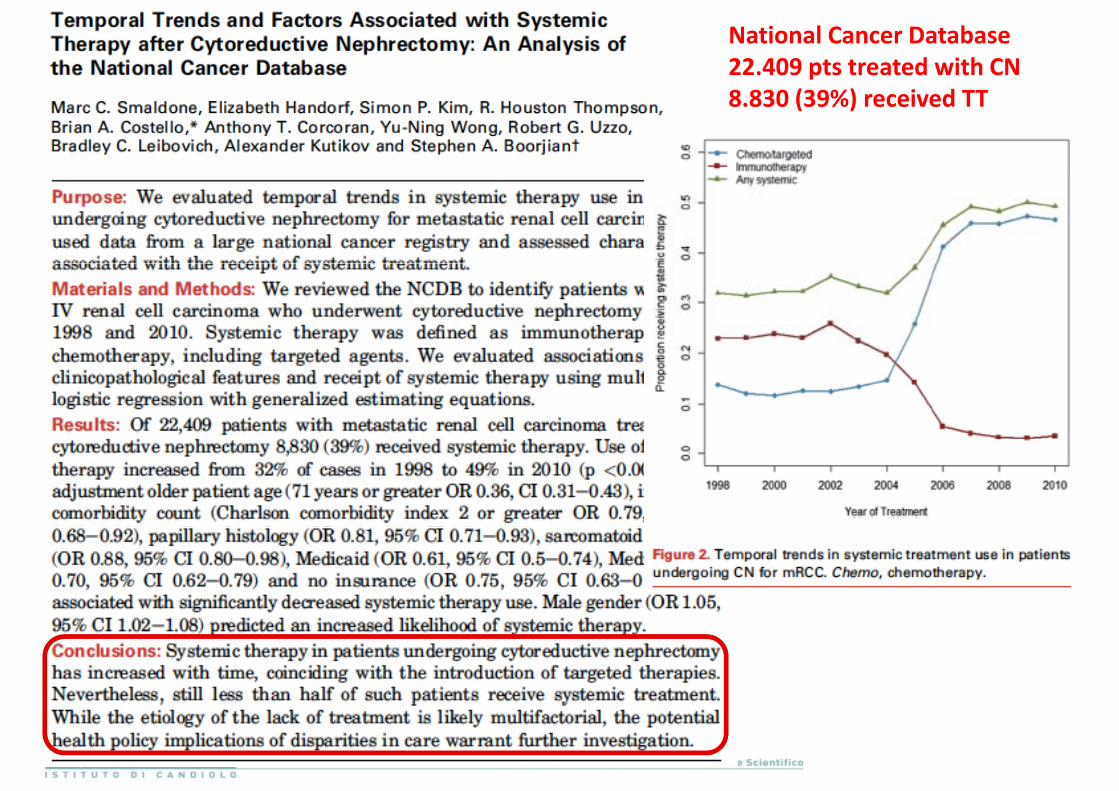
National Cancer Database22.409 pts treated with CN 8.830 (39%) received TT
INSURANCEINSURANCE DATABASE610 pts
2004 20102004‐2010
Urology 2015
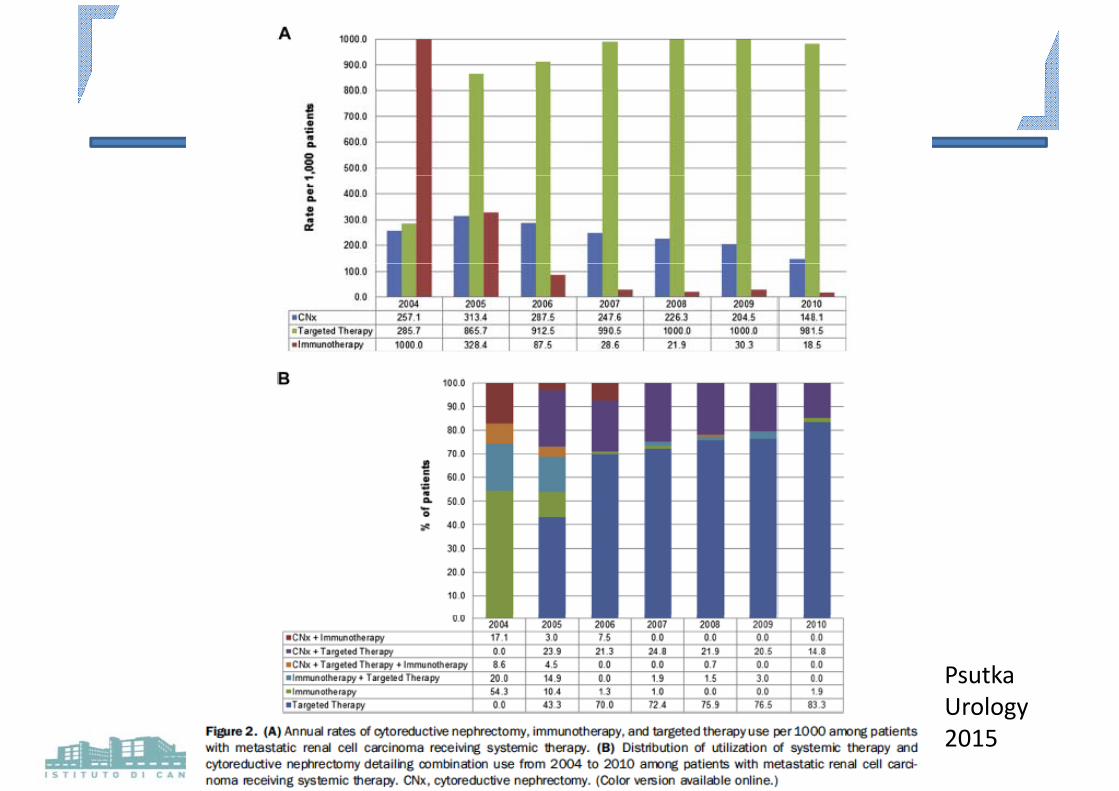
PsutkaUrologyUrology 2015
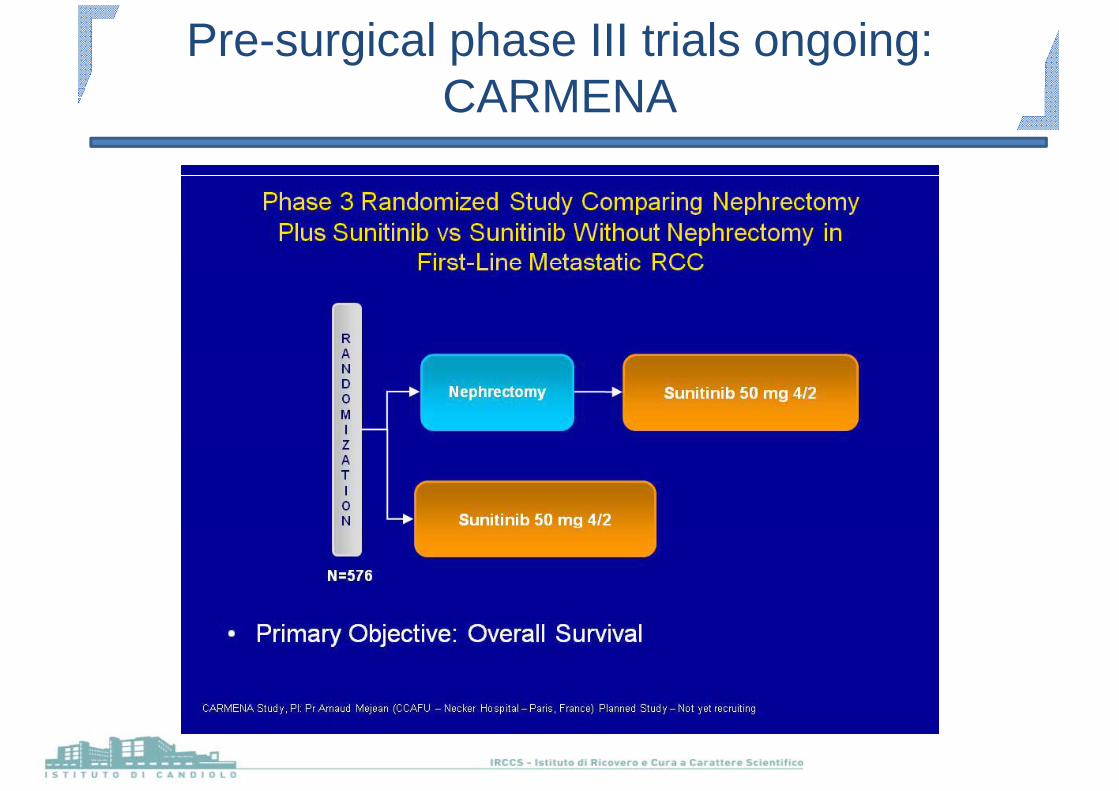
Pre-surgical phase III trials ongoing: CARMENACARMENA
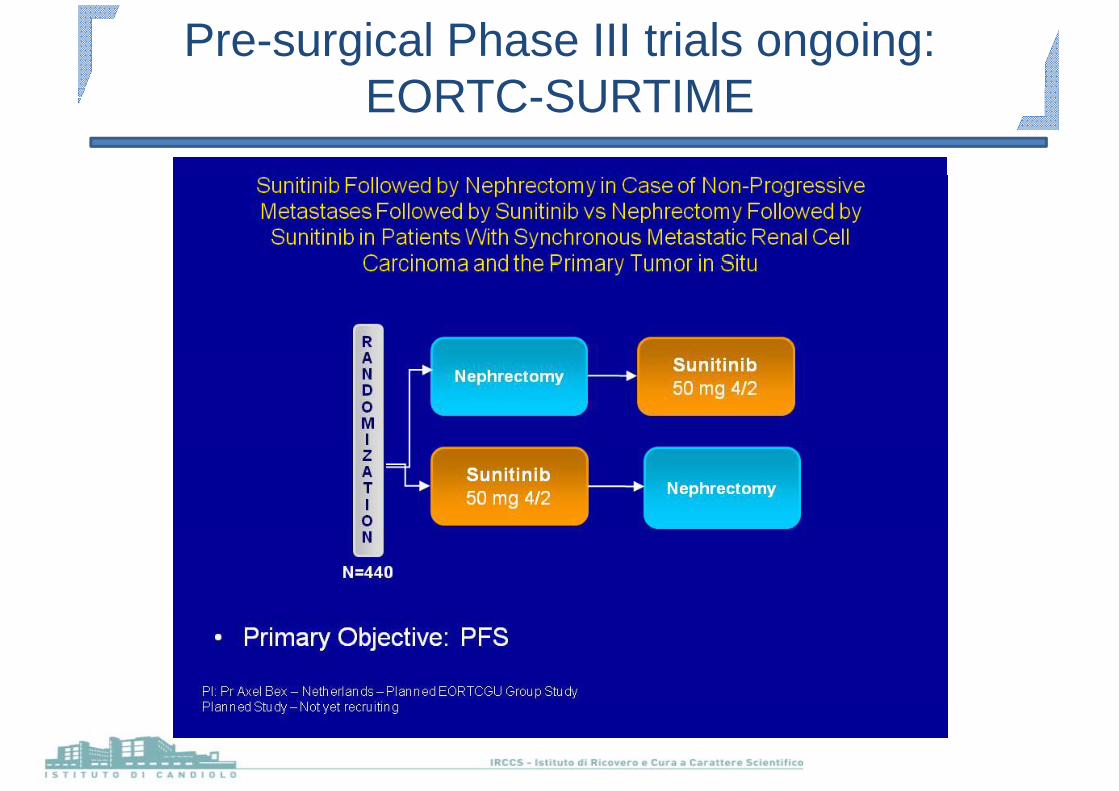
Pre-surgical Phase III trials ongoing: EORTC SURTIMEEORTC-SURTIME
ConclusionsConclusions
Pre‐surgical sistemic therapy has the advantage of: ‐early treatment of metastases‐downsizing of the primary‐effective ‘litmus test’ for the selection of patients for CN based on response to TMT.
h l f h l ( d )The results of two ongoing phase III trials (CARMENA and SURTIME) will address much of the controversy on the role of CN and the ti i f t i thtiming of systemic therapy
There seems to be an important role for CN in the era of TT mostlyThere seems to be an important role for CN in the era of TT, mostly in patients with favorable risk and where a high percentage of tumor burden can be removed by cytoreductive surgerytumor burden can be removed by cytoreductive surgery.

[email protected]@ircc.itg @g @
Top Related