






Le lingue
Pagine
Legale


Dott. Maurizio Miglino
Ospedale policlinico San Martino
Divisione Clinica Ematologica
Città Genova
Problemi aperti nella terapia di MDS/LAM
dell’anziano.
Problemi aperti nella terapia di MDS/LAM
dell’anziano.
- Quale è la miglior terapia di prima linea.
- Cosa fare nei casi ad alto rischio.
- Cosa fare in caso di fallimento della terapia ipometilante.- Cosa fare in caso di fallimento della terapia ipometilante.

Diagnosi di MDS/LMA >
65 aa
Definizione fenotipo
biologico
FLT3 ITD o TKD Mutazioni di IDH 1 o 2 Altri pazienti
(mutazioni p53 ?)
Pazienti non elegibili
≤ 70 aa
Midstaurina
> 70 aa
Quizartinib
Inibitori specifici + AZA Venetoclax + AZA Leucocitosici
Decitabina
citopenici
AZA


With Number of Subjects at Risk
Product-Limit Survival Estimate
0.6
0.8
1.0
Pro
babili
ty
Mediana e range della durata del follow up dalla data di inizio aza alla data ultimo fu o decesso
Analysis Variable : time_osN Minimum Maximum 25th Pctl 50th Pctl 75th Pctl
129 0 82.6973684 8.2565789 19.5723684 42.6973684
405 155 50 15 5At Risk
0 20 40 60 80
time_os
0.0
0.2
0.4
Surv
ival P
95% Hall-Wellner BandCensored

AML CON CITOGENETICA SFAVOREVOLE
Dohner H Blood 2017

Impact of TP53 in Hematologic CancerFrequenza e tipologia di mutazione TP53
nei tumori ematologiciAML: la mutazione di TP 53 si associa al
cariotipo complesso
Stengel A et al Leukemia 2017
Nella fascia di età 60-80, la mutazione TP53 si riscontra in media nel 15% dei casi
La mutazione TP53 in AML è associata a prognosi sfavorevole

N° PZ TOTALI 46
OS mediana
OS rate a 1 anno
OS rate a 2 anni
8,4 mesi
43%
30%
N° di cicli mediano 3,5 (1-20)
ORR 51%
Follow up mediano: 6.4 mesi
DECITABINE DATA IN REAL LIFE DECITABINE DATA IN REAL LIFE
ORR
- CR
- PR
- HI
51%
32%
5,5%
13,6%
ORR, Kariotype
- Normal
- Intermediate
- Adverse
47,3%
77%
21,4%
Durata mediana della risposta 5,3m (1-18)
Tempo mediano alla miglior risposta 3,5 m (1-8,5)
Borlenghi et al. Poster presented at EHA 2017.
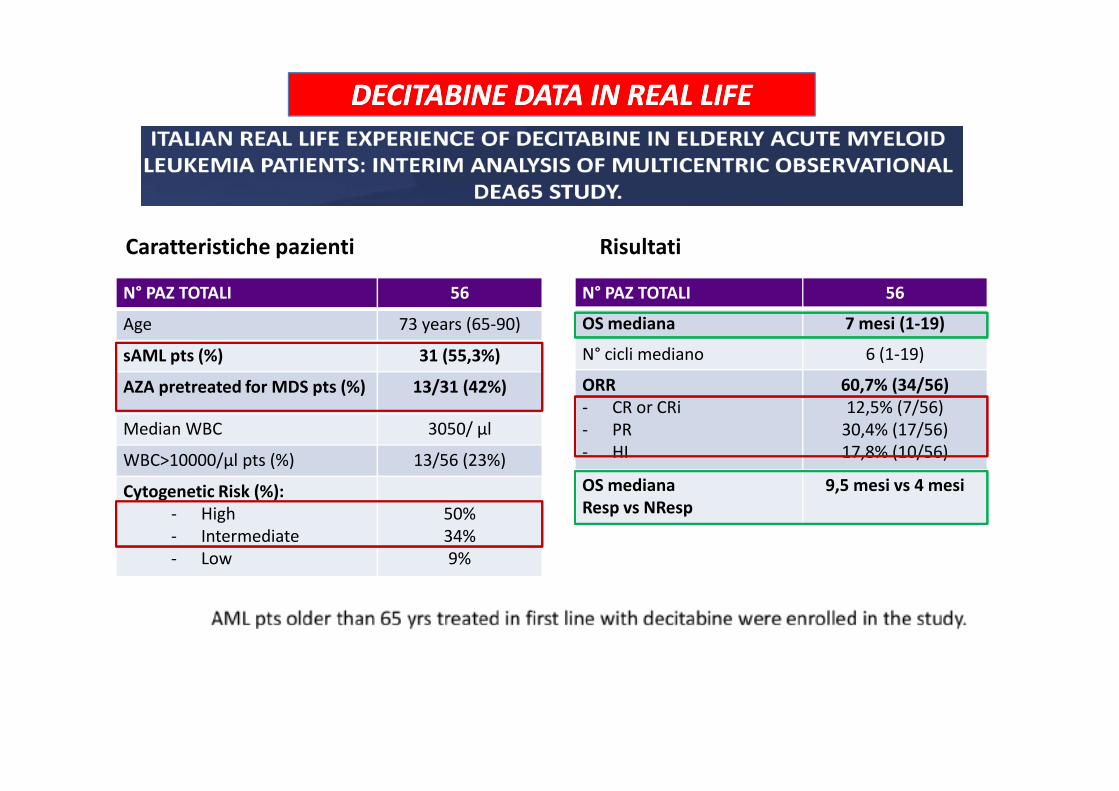
N° PAZ TOTALI 56
Age 73 years (65-90)
sAML pts (%) 31 (55,3%)
AZA pretreated for MDS pts (%) 13/31 (42%)
N° PAZ TOTALI 56
OS mediana 7 mesi (1-19)
N° cicli mediano 6 (1-19)
ORR
- CR or CRi
60,7% (34/56)
12,5% (7/56)
Caratteristiche pazienti Risultati
DECITABINE DATA IN REAL LIFE DECITABINE DATA IN REAL LIFE
Aprile et al. Poster presented at EHA 2017.
AZA pretreated for MDS pts (%) 13/31 (42%)
Median WBC 3050/ µl
WBC>10000/µl pts (%) 13/56 (23%)
Cytogenetic Risk (%):
- High
- Intermediate
- Low
50%
34%
9%
- CR or CRi
- PR
- HI
12,5% (7/56)
30,4% (17/56)
17,8% (10/56)
OS mediana
Resp vs NResp
9,5 mesi vs 4 mesi

DECITABINE DATA IN REAL LIFE DECITABINE DATA IN REAL LIFE
Aprile et al. Poster presented at EHA 2017.
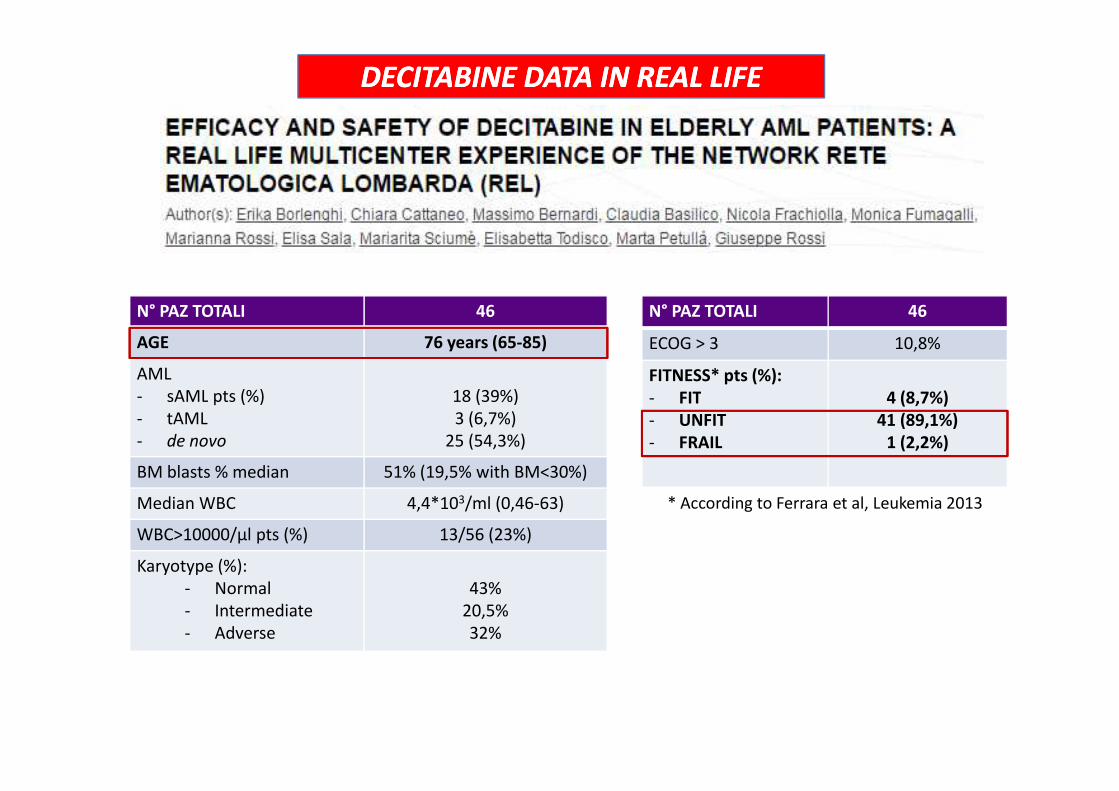
N° PAZ TOTALI 46
AGE 76 years (65-85)
AML
- sAML pts (%) 18 (39%)
N° PAZ TOTALI 46
ECOG > 3 10,8%
FITNESS* pts (%):
- FIT 4 (8,7%)
DECITABINE DATA IN REAL LIFE DECITABINE DATA IN REAL LIFE
Borlenghi et al. Poster presented at EHA 2017.
- sAML pts (%)
- tAML
- de novo
18 (39%)
3 (6,7%)
25 (54,3%)
BM blasts % median 51% (19,5% with BM<30%)
Median WBC 4,4*103/ml (0,46-63)
WBC>10000/µl pts (%) 13/56 (23%)
Karyotype (%):
- Normal
- Intermediate
- Adverse
43%
20,5%
32%
- FIT
- UNFIT
- FRAIL
4 (8,7%)
41 (89,1%)
1 (2,2%)
* According to Ferrara et al, Leukemia 2013

Transfusion independence induced by decitabine is associated with increased
survival benefit, even in the absence of CR
All RBC trasfusion-independent patients RBC trasfusion-independent pts without CR
He et al., 2014. Leukemia & Lymphoma
Median OS12.1 months vs 6.5 months (p=0.0001)
Median OS 9.8 months vs 6.4 months (p=0.021)

Time to AZA discontinuation (TTD) (tutte le cause)
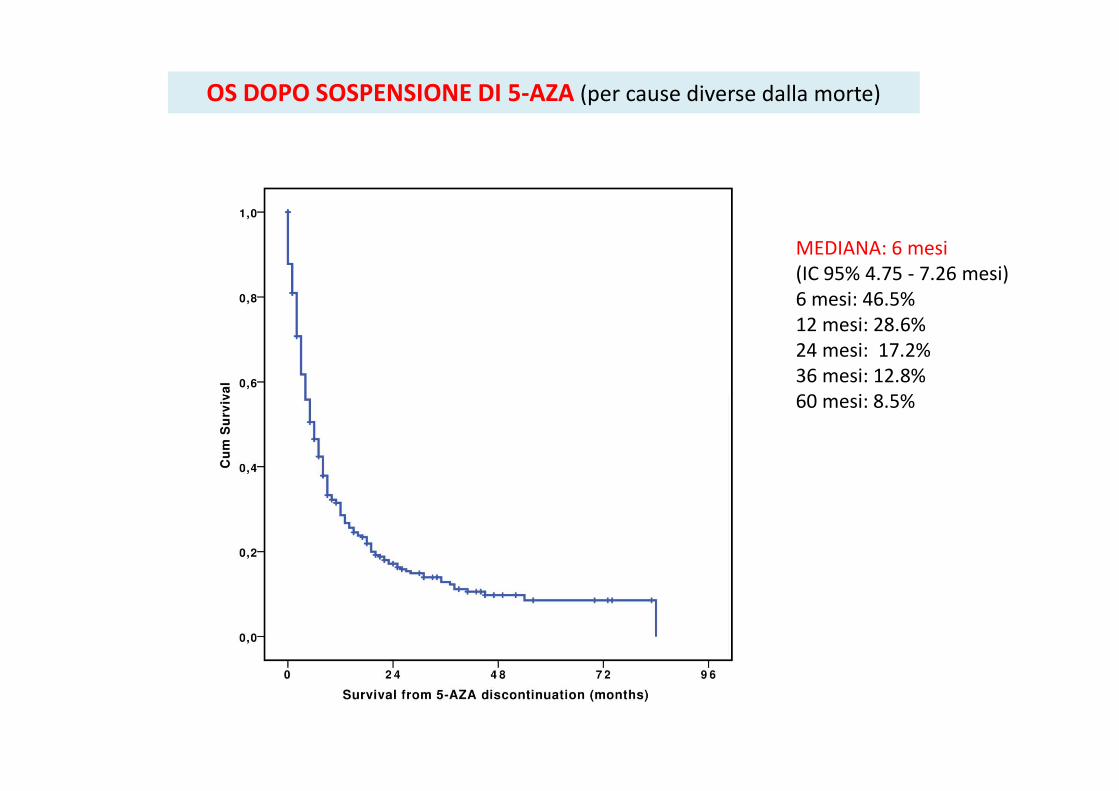
MEDIANA: 6 mesi
(IC 95% 4.75 - 7.26 mesi)
6 mesi: 46.5%
12 mesi: 28.6%
24 mesi: 17.2%
36 mesi: 12.8%
60 mesi: 8.5%
OS DOPO SOSPENSIONE DI 5-AZA (per cause diverse dalla morte)
60 mesi: 8.5%

Decitabine in R/R AML patients
10-day or 5-day schedule

10-day cycles of decitabine 20 mg/m2.
Treatment cycles repeated if there was stable
disease or response with ongoing cycles of
decitabine 20 mg/m2 for 3–5 days every 4–6
weeks as tolerated until progression.
5-day cycles of decitabine 20 mg/m2daily
combined with 1 dose of gemtuzumab
ozogamicin (GO) 3 mg/m2 on day 5.
Treatment cycles repeated if there was stable
disease or response.
45 patients 57 patients
Ritchie EK, et al. Leuk Lymphoma. 2013
102 R/R
patients

Characteristic
Patients (n=102)
Median age (years) 66 (range: 21–88)
Male/female (%) 52/48
Median number of prior therapies 2 (range: 1–5)
Prior anthracycline/ara-C induction (%) 57
Prior low-intensity induction (%) 39
Decitabine single-agent salvage (%) 59
Decitabine + GO salvage (%) 41
ECOG PS 0/1/2/3/unknown (%) 25/49/19/7/1
Cytogenetics: adverse/intermediate (%) 30/70
Baseline bilirubin ≤ 1.3 / > 1.3 mg/dL (%) 92/8
Baseline creatinine ≤ 1.3 / > 1.3 mg/dL (%) 81/19
Ritchie EK, et al. Leuk Lymphoma. 2013
• CR among 102 R/R pts = 16(15.7%)• Median OS among R/R pts: 177.0 days (95% CI=148.0-206.0 days)
• achievement of CR vs NR was a predictor of improved OS (P<0.0001)
� Single-agent decitabine showed a trend for improved OS vs decitabine + GO (median
OS: 209.0 vs 107.0 days, respectively, P=0.13)

Khan et al., Leukemia & Lymphoma 2017
34 pts with R/R AML
13(39%) with t/s AML
25(74%) with Intermediate/Poor Risk
75% treated with 10 days schedule

Decitabina è un Farmaco sicuro ed efficace in pazienti conLAM/High Risk MDS non candidabili a CT intensiva.
Caratteristiche biologiche ad impatto prognosticosfavorevole (TP53m, cariotipo complesso e monosomiale,s/tAML) beneficiano del meccanismo d’azione di
19
sfavorevole (TP53m, cariotipo complesso e monosomiale,s/tAML) beneficiano del meccanismo d’azione diDecitabina.
La schedula 10 giorni impiegata sia in 1a linea sia nel pzR/R ha un impatto positivo sull’ outcome.




Top Related