
TROMBOEMBOLISMO VENOSO: TERAPIE CONSOLIDATE E … 2016/20 mattina/Testa.pdf · TRATTAMENTO DELLA...
78
TROMBOEMBOLISMO VENOSO: TERAPIE CONSOLIDATE E NUOVE PROSPETTIVE Sophie Testa Centro Emostasi e Trombosi A.O. Istituti Ospitalieri di Cremona
Transcript of TROMBOEMBOLISMO VENOSO: TERAPIE CONSOLIDATE E … 2016/20 mattina/Testa.pdf · TRATTAMENTO DELLA...
TROMBOEMBOLISMO VENOSO: TERAPIE CONSOLIDATE E NUOVE
PROSPETTIVE
Sophie Testa Centro Emostasi e Trombosi
A.O. Istituti Ospitalieri di Cremona
PUNTI DI DISCUSSIONE
• Epidemiologia del Tromboembolismo Venoso (TEV)
• I farmaci anticoagulanti
• Terapia “classica” e “innovativa” delle diverse fasi del
trattamento del TEV:
- la fase acuta
- la fase a lungo termine
- la fase estesa = “profilassi delle recidive”
• La durata ottimale del trattamento anticoagulante
• La gestione del paziente
• Informazioni recenti dalla realtà italiana (il registro START)
= “trattamento attivo”
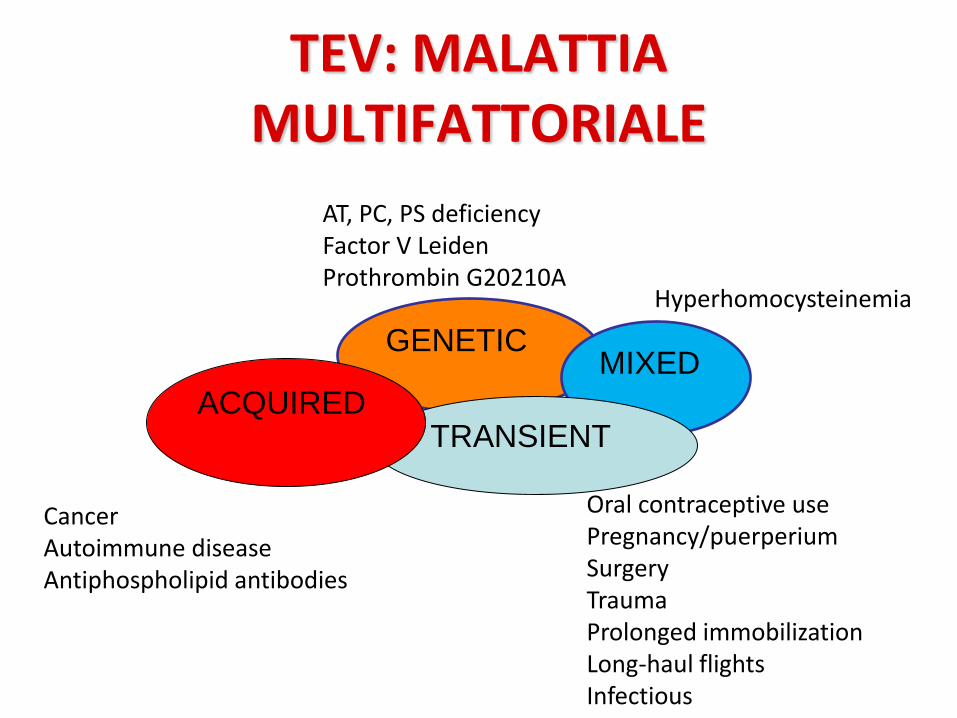
TEV: MALATTIA MULTIFATTORIALE
GENETIC MIXED
TRANSIENT ACQUIRED
AT, PC, PS deficiency Factor V Leiden Prothrombin G20210A
Hyperhomocysteinemia
Oral contraceptive use Pregnancy/puerperium Surgery Trauma Prolonged immobilization Long-haul flights Infectious
Cancer Autoimmune disease Antiphospholipid antibodies
EPIDEMIOLOGIA
• Terza patologia cardiovascolare dopo IMA e STROKE
• Incidenza TEV nel mondo occidentale: 1 caso ogni 1000 soggetti all’anno
• 600.000/anno casi di TEV in Italia
• 2/3 casi sono TVP; 1/3 casi sono EP
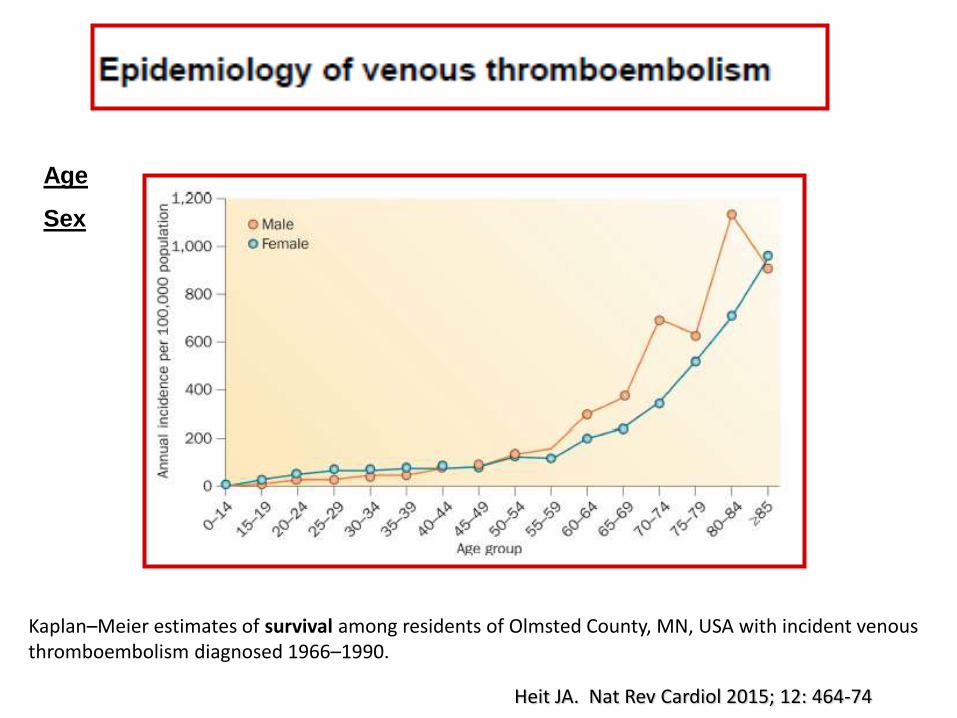
Heit JA. Nat Rev Cardiol 2015; 12: 464-74
Kaplan–Meier estimates of survival among residents of Olmsted County, MN, USA with incident venous thromboembolism diagnosed 1966–1990.
Age
Sex
Heit JA. Nat Rev Cardiol 2015; 12: 464-74
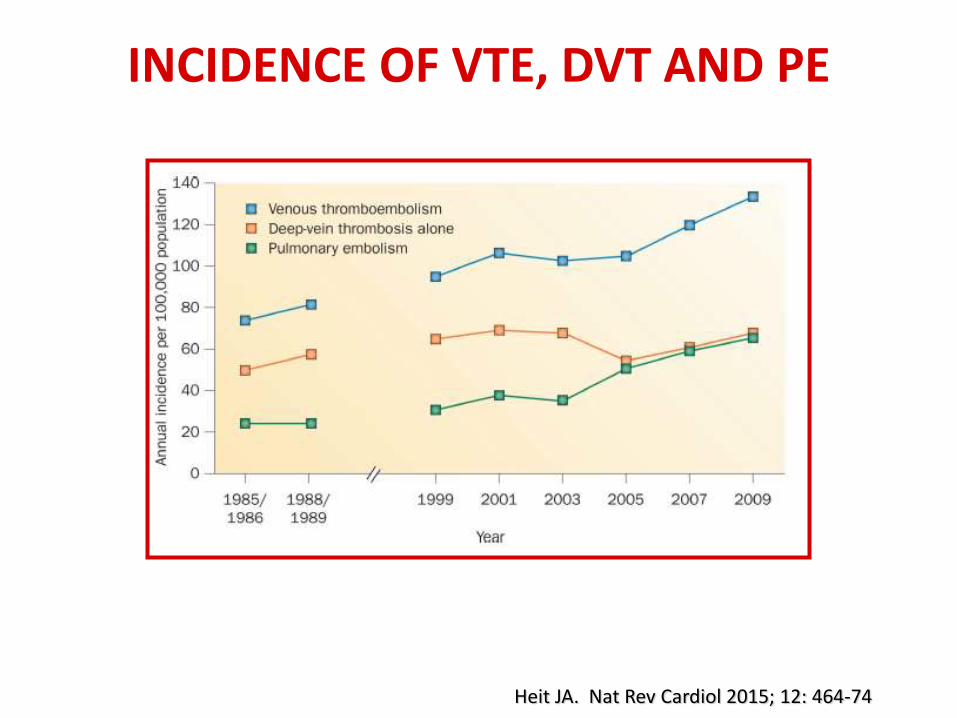
INCIDENCE OF VTE, DVT AND PE
Heit JA. Nat Rev Cardiol 2015; 12: 464-74
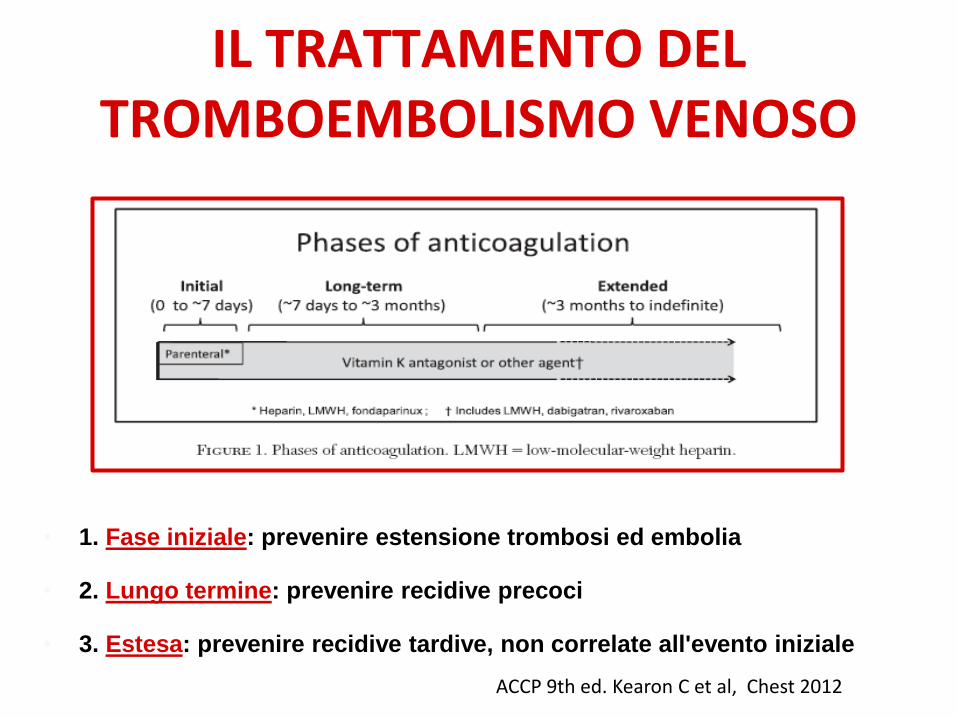
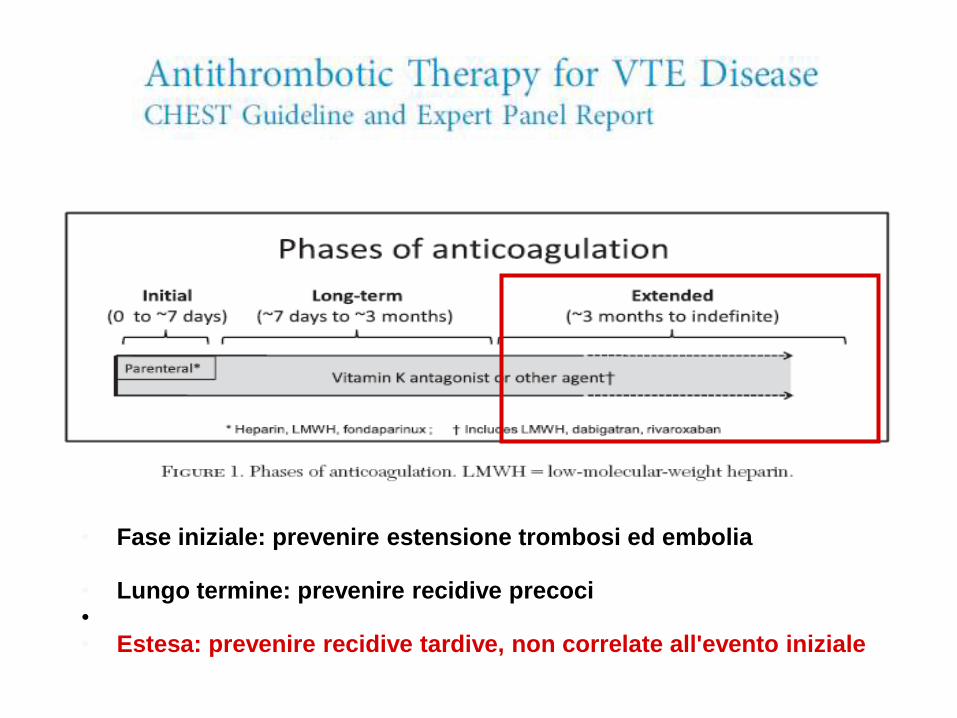
IL TRATTAMENTO DEL TROMBOEMBOLISMO VENOSO
• 1. Fase iniziale: prevenire estensione trombosi ed embolia
• 2. Lungo termine: prevenire recidive precoci
• 3. Estesa: prevenire recidive tardive, non correlate all'evento iniziale
ACCP 9th ed. Kearon C et al, Chest 2012
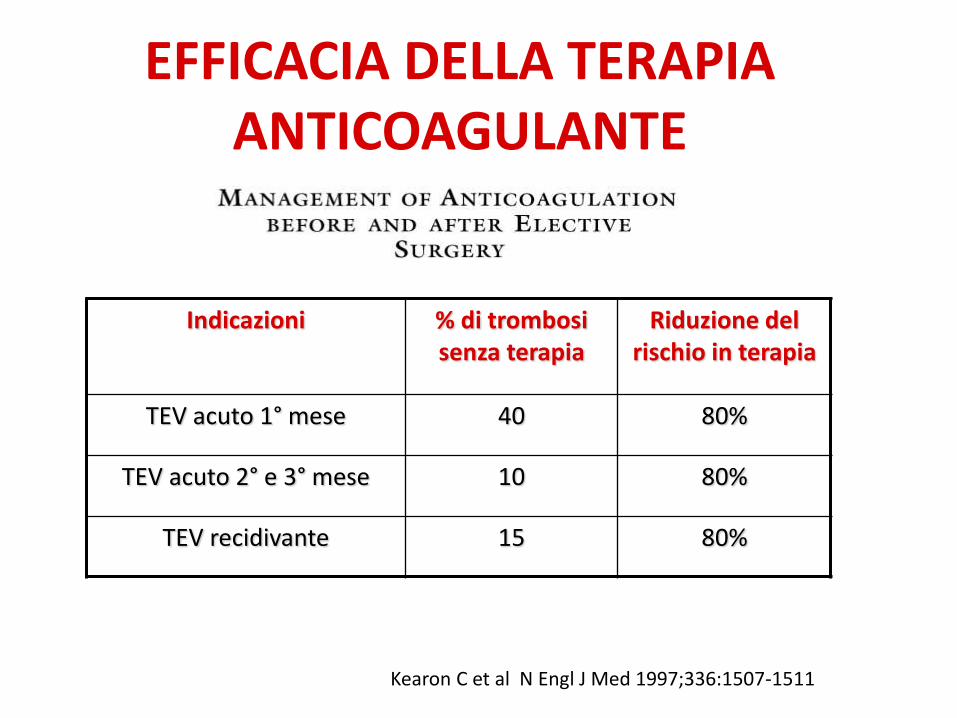
EFFICACIA DELLA TERAPIA ANTICOAGULANTE
Indicazioni % di trombosi senza terapia
Riduzione del rischio in terapia
TEV acuto 1° mese 40 80%
TEV acuto 2° e 3° mese 10 80%
TEV recidivante 15 80%
Kearon C et al N Engl J Med 1997;336:1507-1511
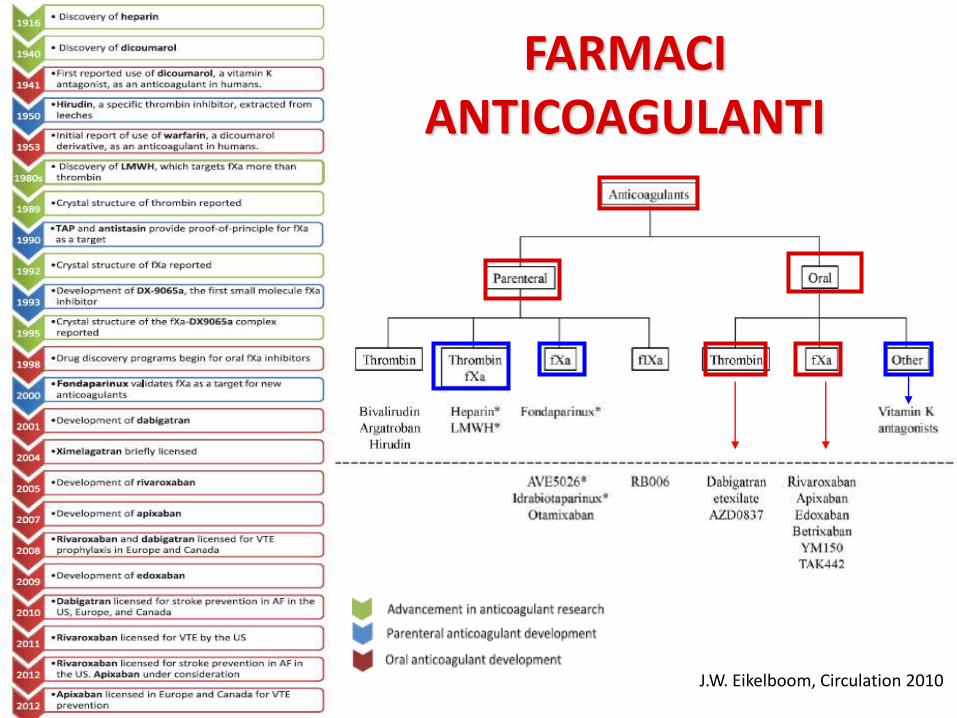
FARMACI ANTICOAGULANTI
J.W. Eikelboom, Circulation 2010
GLI ANTICOAGULANTI ORALI "NUOVI” O "DIRETTI”:
un po’ di acronimi, per confondere le idee…
DOAC (Direct Oral AntiCoagulants)
NOAC o NOA (New Oral AntiCoagulants, Non-VKA Oral AntiCoagulants),
...anche nella variante italiana NAO
…e, ultimo arrivato: TSOACs (Target-Specific
Oral AntiCoagulants)
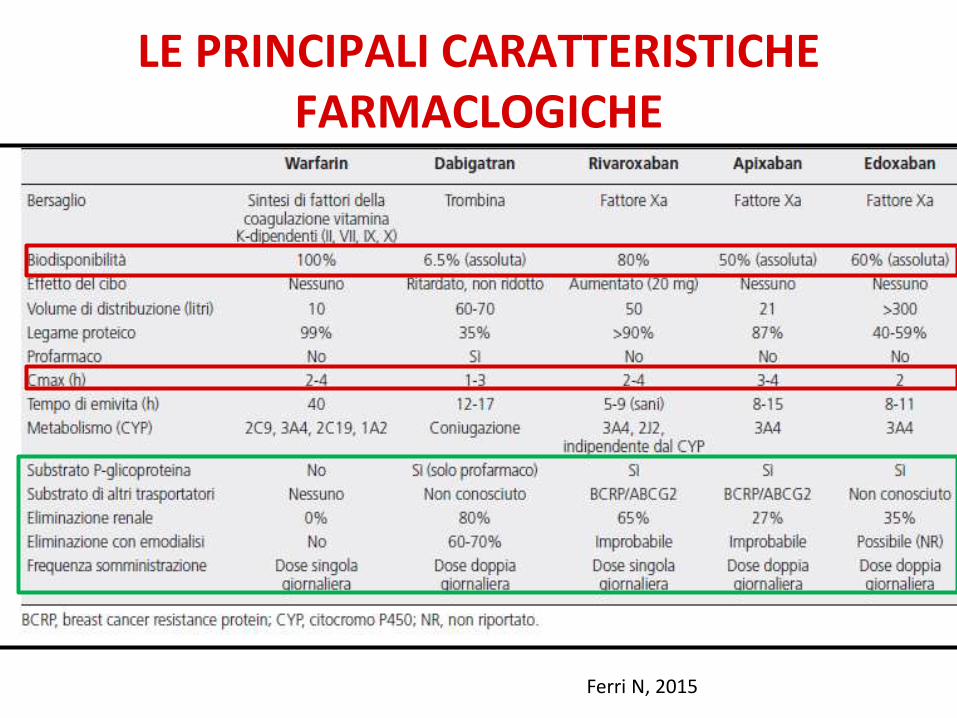
LE PRINCIPALI CARATTERISTICHE FARMACLOGICHE
Ferri N, 2015
DOAC Studi di farmacologia hanno mostrato che la risposta anticoagulante
e’ prevedibile in condizioni cliniche “standard”
Da ciò è derivato:
1) Somministrazione a dosaggio fisso giornaliero
2) La non indicazione al monitoraggio di laboratorio routinario
3) E inizialmente la “non necessità” di antidoti per la breve
emivita…
Diversa percezione delle necessità sanitarie dei pazienti in
trattamento cronico con DOAC
DOAC: ASPETTI DI FARMACOLOGIA
• Esiste ampia variabilita’ intra/inter individuale
• Modificazioni farmacocinetiche e farmacodinamiche
in relazione a: interazioni farmacologiche, insuff.
renale, insuff. epatica, eta’, peso.
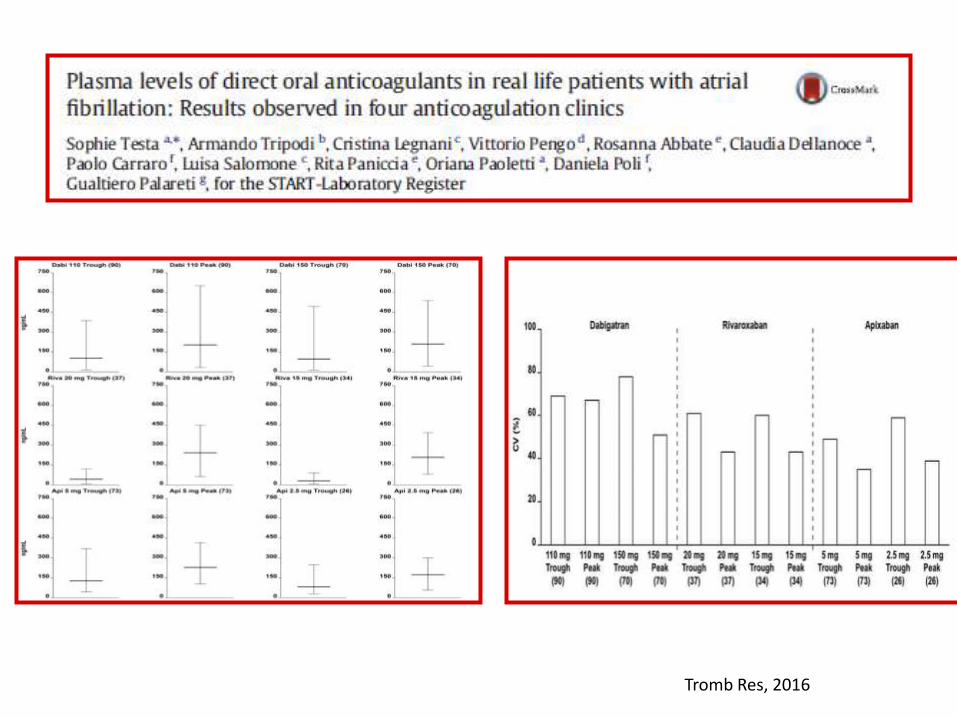
Tromb Res, 2016
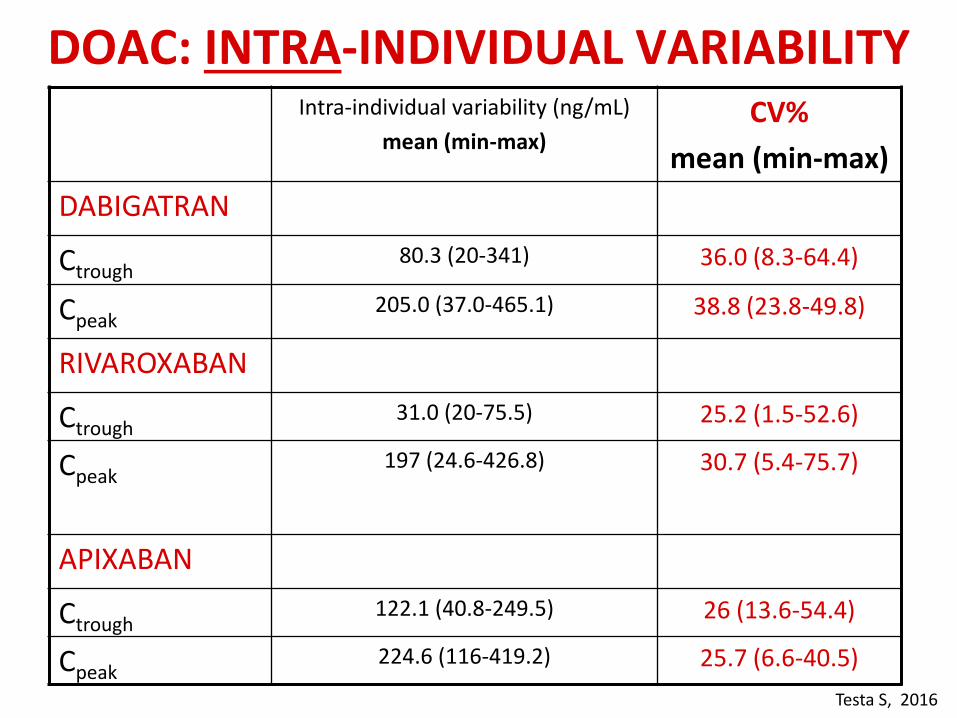
DOAC: INTRA-INDIVIDUAL VARIABILITY Intra-individual variability (ng/mL)
mean (min-max) CV%
mean (min-max)
DABIGATRAN
Ctrough 80.3 (20-341) 36.0 (8.3-64.4)
Cpeak 205.0 (37.0-465.1) 38.8 (23.8-49.8)
RIVAROXABAN
Ctrough 31.0 (20-75.5) 25.2 (1.5-52.6)
Cpeak
197 (24.6-426.8) 30.7 (5.4-75.7)
APIXABAN
Ctrough 122.1 (40.8-249.5) 26 (13.6-54.4)
Cpeak 224.6 (116-419.2) 25.7 (6.6-40.5)
Testa S, 2016
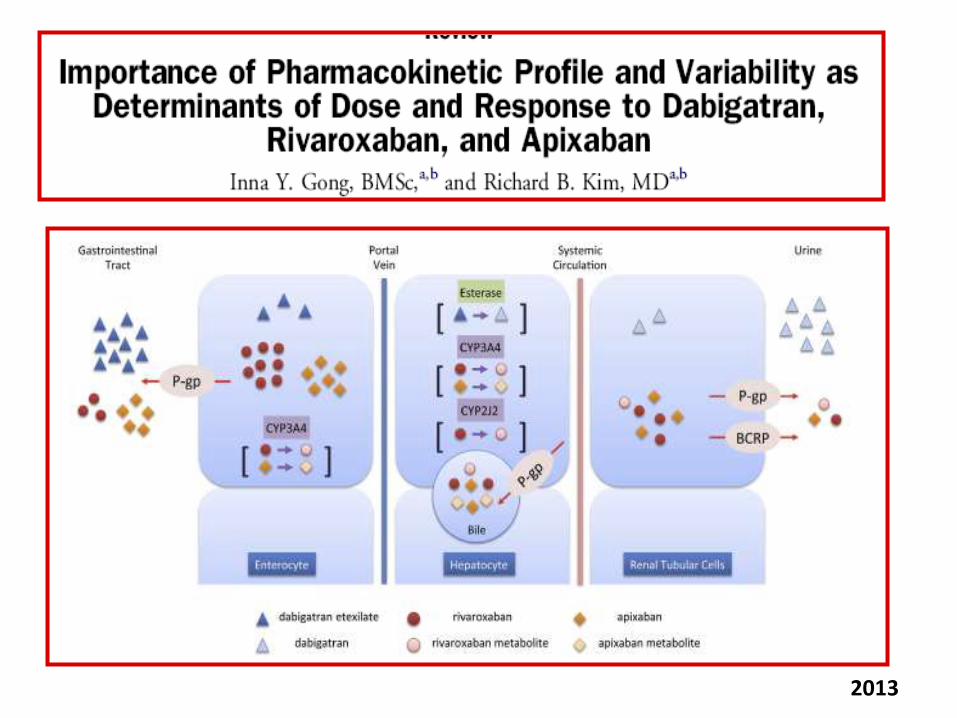
2013
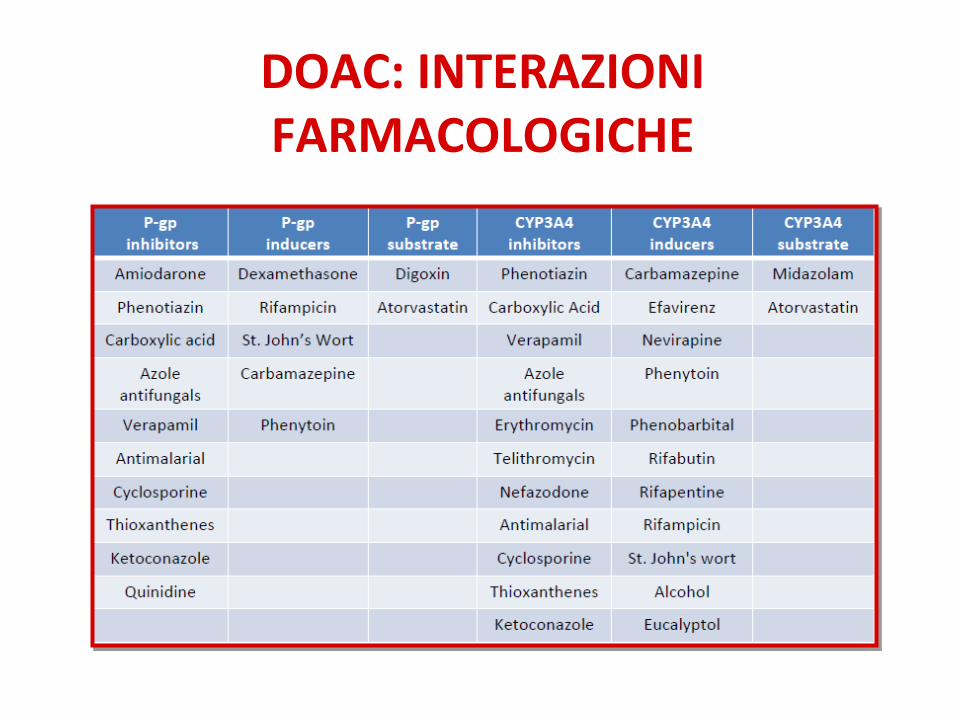
DOAC: INTERAZIONI FARMACOLOGICHE
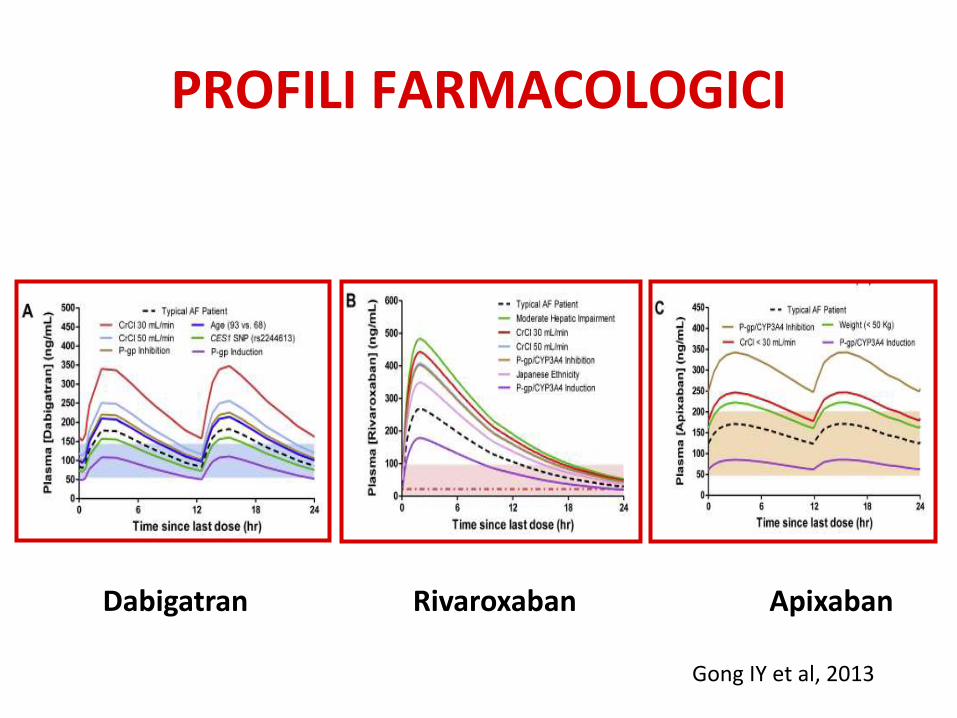
PROFILI FARMACOLOGICI
Dabigatran Rivaroxaban Apixaban
Gong IY et al, 2013
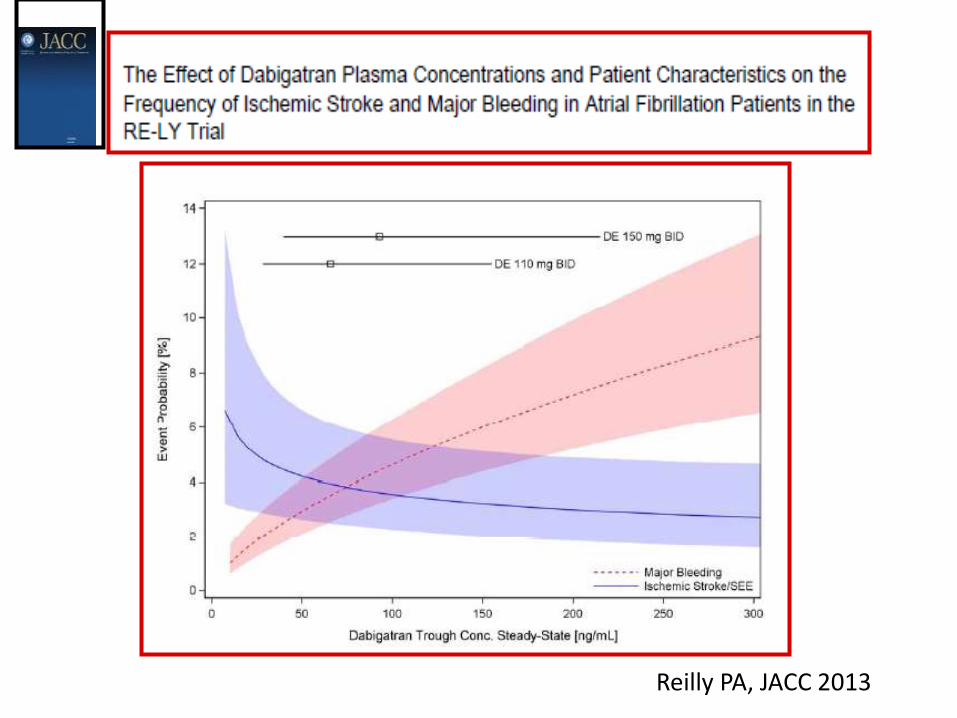
Reilly PA, JACC 2013
• Perioperative management • Patients presenting in emergency with adverse events
(Thrombosis, Bleeding) • Immediate reverse of anticoagulation • Renal Disease • Liver Disease • Suspicion or known interaction with other drugs • Elderly patients • Under/over weight
QUANDO PUO’ ESSERE UTILE IL DOSAGGIO
DELL’ATTIVITA’ ANTICOAGULANTE DEI DOAC?
JTH, 2011
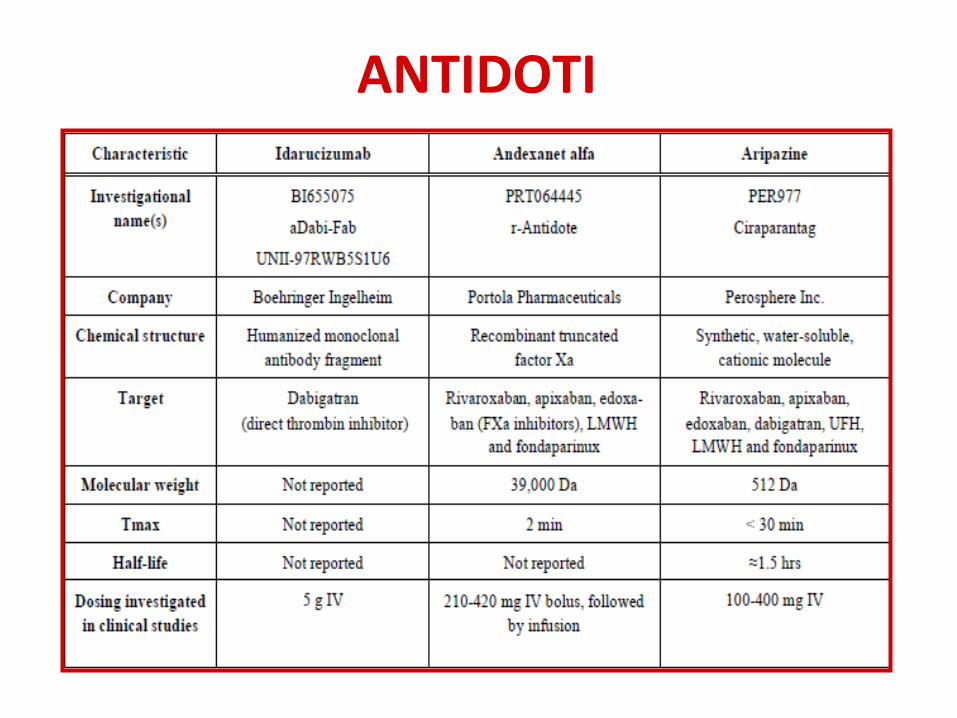
ANTIDOTI
Pollack et al, N Engl J Med 2015
• Idarucizumab rapidly (within few minutes) and completely
reversed the anticoagulant effect of dabigatran in 88 to 98%
of the patients who had had elevated clotting times at
baseline
• One thrombotic event (1%) occurred within 72 hours after
idarucizumab administration in a patient in whom
anticoagulation had not been reinitiated
• Dati convincenti rispetto alla normalizzazione dell’effetto anticoagulante di idarucizumab
• Non possibili conclusioni rispetto ai benefici clinici per mancanza di un gruppo di controllo
• La misura dell’attività di dabigatran è stata centralizzata e non utilizzata per gestire il reverse
• In circa ¼ dei pazienti trattati con antidoto il dTT era normale (assenza di farmaco)
• Pertanto è utile avere la disponibilità IN TEMPO REALE di TEST SPECIFICI per la misura dell’effetto anticoagulante che possa guidare l’utilizzo degli antidoti per evitare un loro sovrautilizzo e consumo inutile di risorse
BAUER , N Engl J Med 2015

VTE: LA TERAPIA
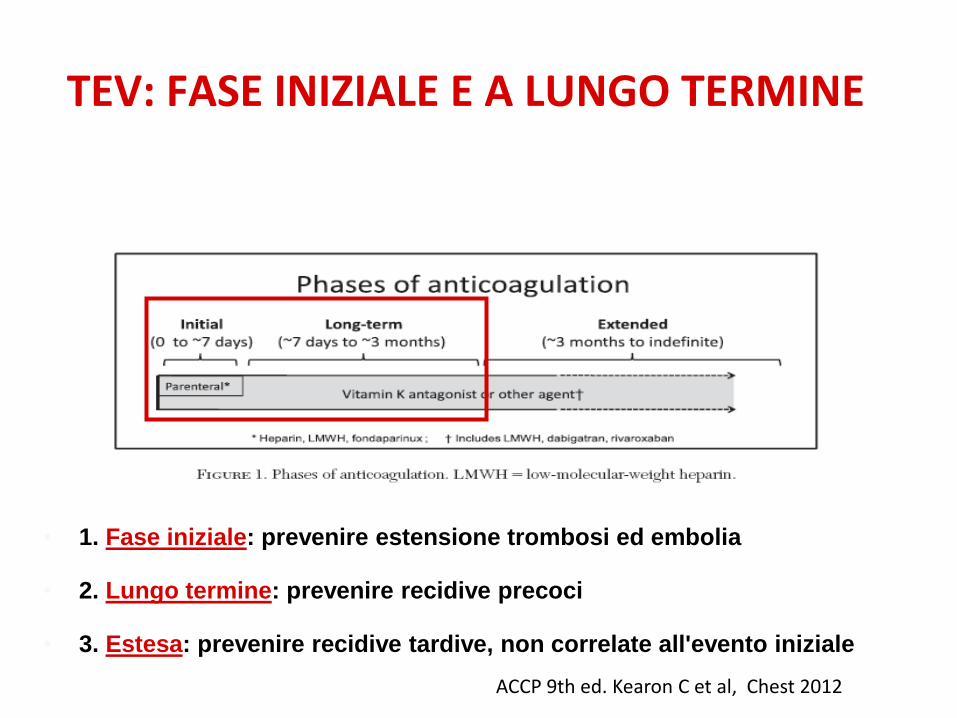
TEV: FASE INIZIALE E A LUNGO TERMINE
• 1. Fase iniziale: prevenire estensione trombosi ed embolia
• 2. Lungo termine: prevenire recidive precoci
• 3. Estesa: prevenire recidive tardive, non correlate all'evento iniziale
ACCP 9th ed. Kearon C et al, Chest 2012
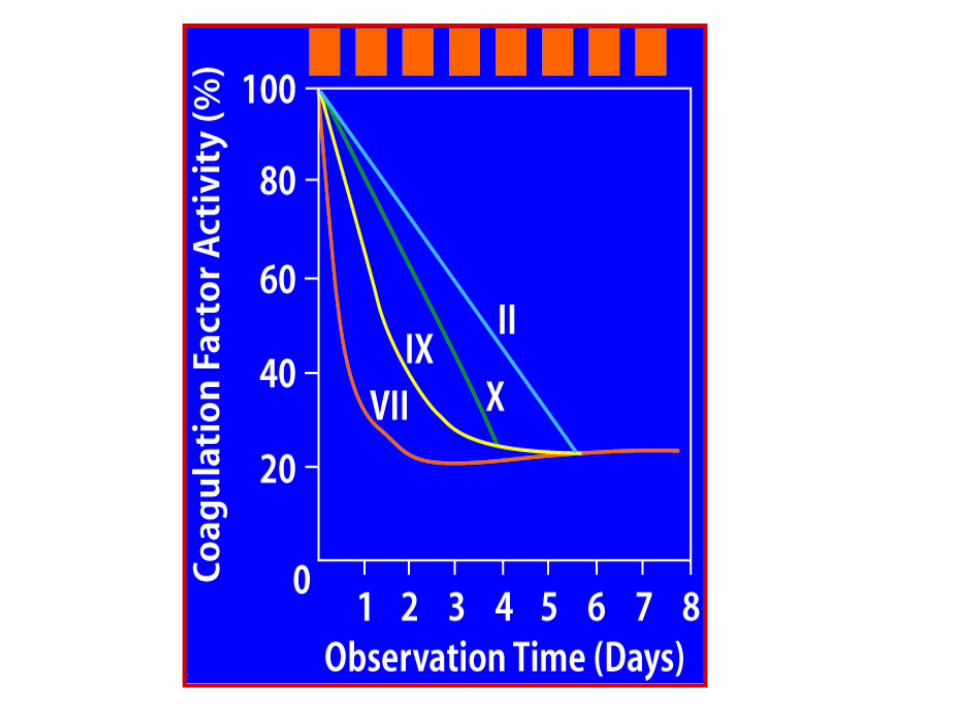
VTE: “TERAPIA CLASSICA”
• LMWH (from 115 to 200 U/kg/d, depending on the
molecule) for at least 5 days; alternatives are UH or
fondaparinux
• VKA (warfarin or acenocoumarol) from the first day,
for at least 3-6 months
• LMWH should not be stopped earlier than 48 hours
from INR at target (INR 2.5, range 2.0-3.0)
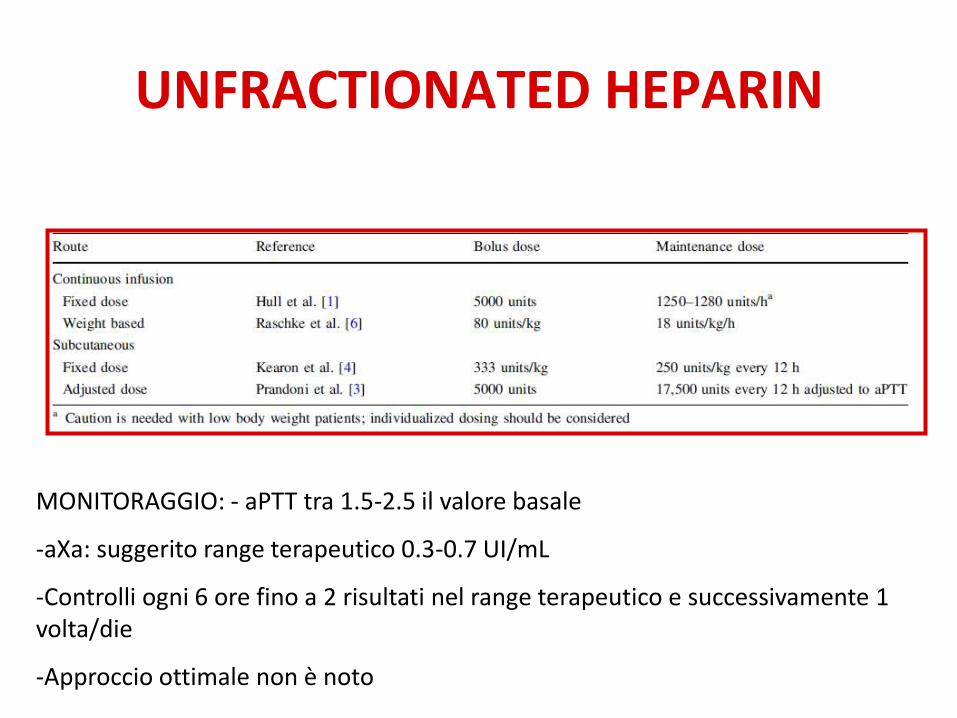
UNFRACTIONATED HEPARIN
MONITORAGGIO: - aPTT tra 1.5-2.5 il valore basale
-aXa: suggerito range terapeutico 0.3-0.7 UI/mL
-Controlli ogni 6 ore fino a 2 risultati nel range terapeutico e successivamente 1 volta/die
-Approccio ottimale non è noto
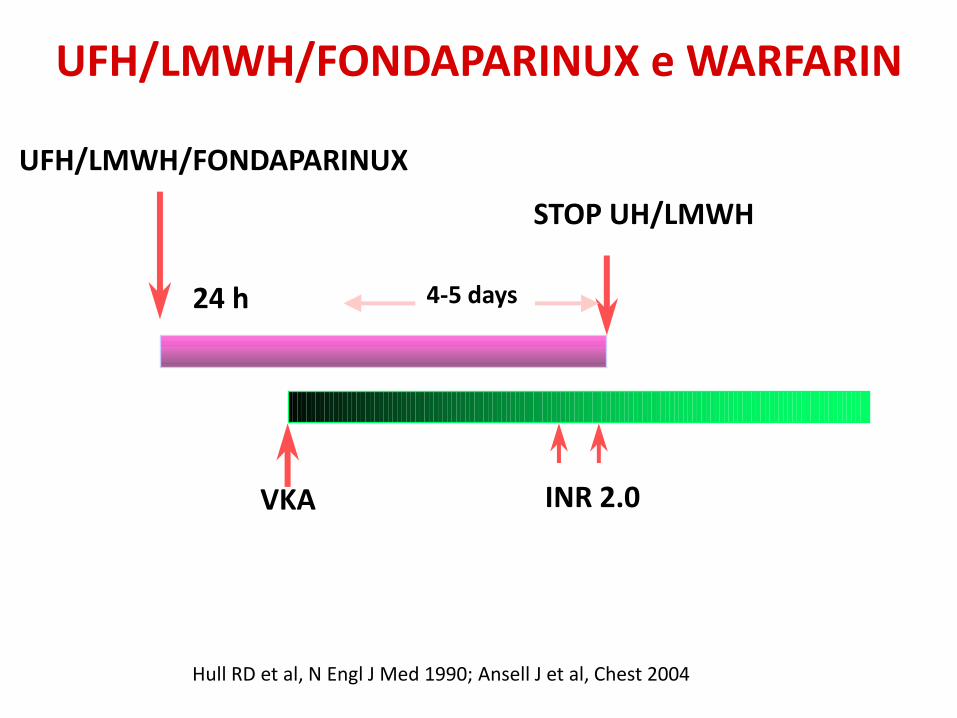
UFH/LMWH/FONDAPARINUX
STOP UH/LMWH
24 h 4-5 days
VKA INR 2.0
UFH/LMWH/FONDAPARINUX e WARFARIN
Hull RD et al, N Engl J Med 1990; Ansell J et al, Chest 2004
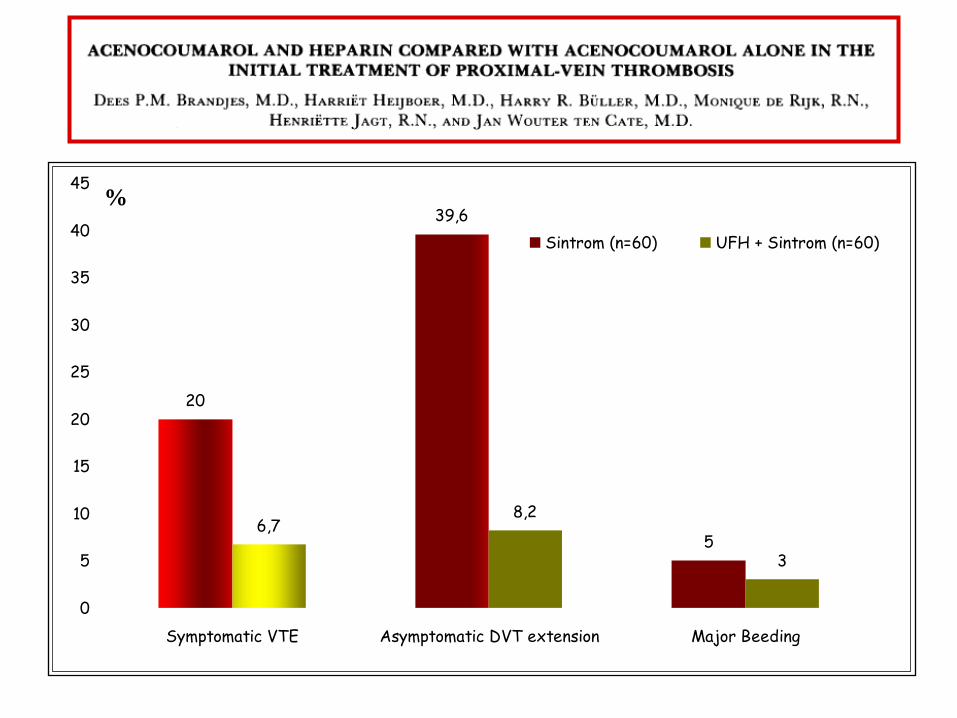
20
39,6
56,7
8,2
3
0
5
10
15
20
25
30
35
40
45
Symptomatic VTE Asymptomatic DVT extension Major Beeding
Sintrom (n=60) UFH + Sintrom (n=60)
%
WHEN VKA SHOULD BE DELAYED OR AVOIDED
• Contraindications to VKA (pregnancy, liver disease…)
• Low compliance (check !)
• Active bleeding
• Surgery/Invasive procedures
• Overt cancer
LMWH/FONDAPARINUX COME UNICO TRATTAMENTO DELLA TROMBOSI
VENOSA ACUTA
• Paziente con neoplasia attiva (LMWH per 3-6 mesi)
• Paziente con trombosi venosa superficiale (per 6 settimane circa)
• TEV ricorrente in corso di terapia con VKA (con INR in range terapeutico) o con DOAC (pz complianti)
• TEV in gravidanza (solo LMWH)
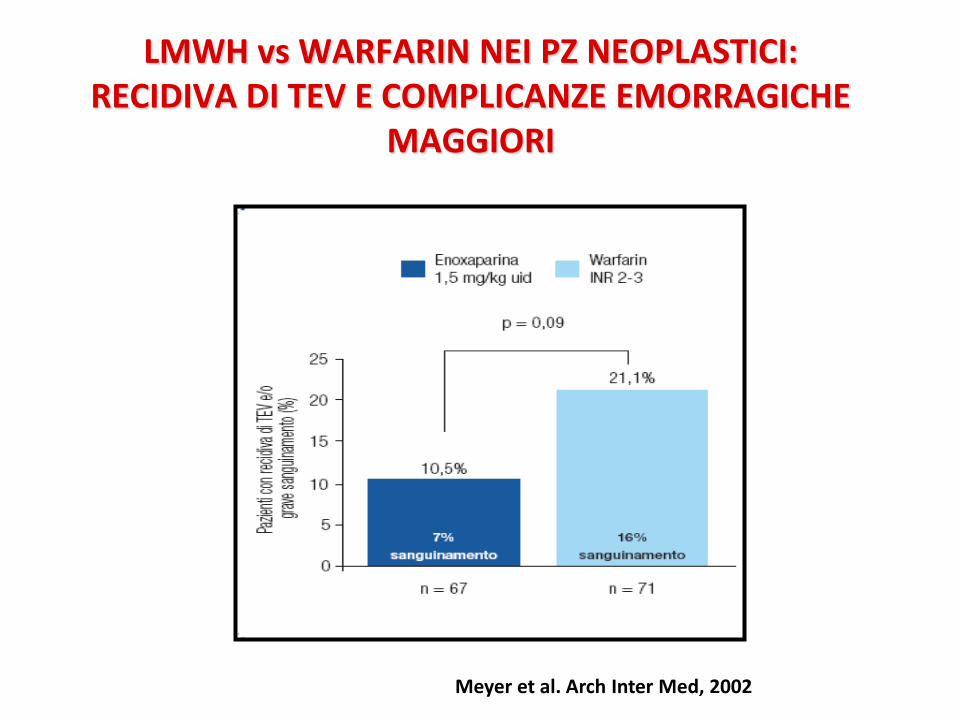
LMWH vs WARFARIN NEI PZ NEOPLASTICI: RECIDIVA DI TEV E COMPLICANZE EMORRAGICHE
MAGGIORI
Meyer et al. Arch Inter Med, 2002
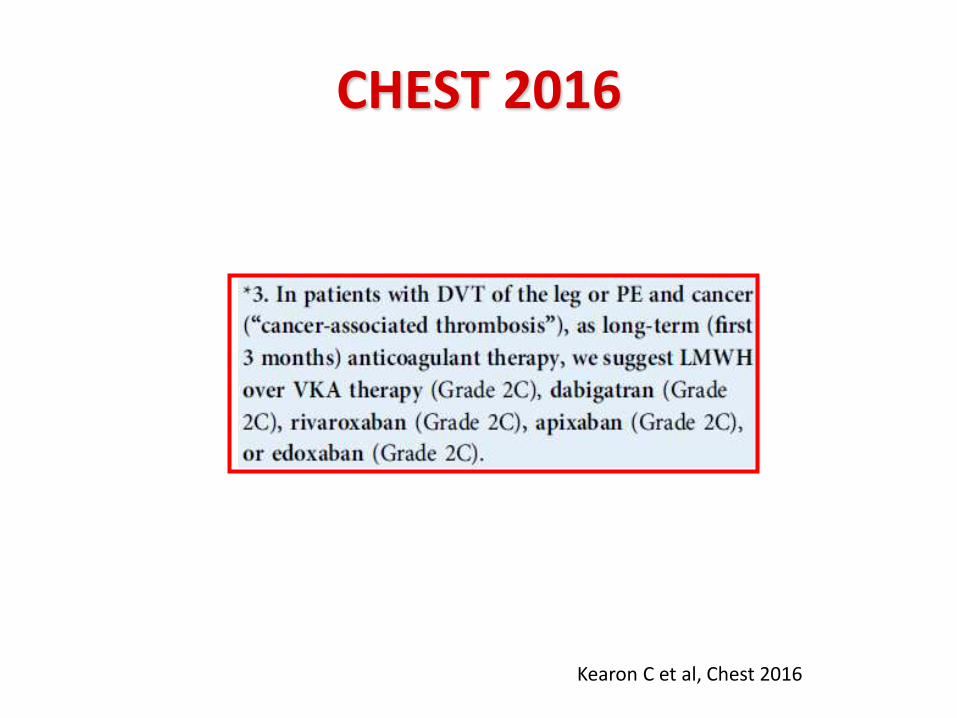
CHEST 2016
Kearon C et al, Chest 2016
• In patients with high suspicion of VTE start treatment (LMWH) while waiting for diagnostic confirmation/exclusion
• In patients with PE, evaluate the risk/benefit ratio of a more aggressive approach:
– In patients hemodinamically unstable: prefer thrombolysis
– In all the other patients, prefer anticoagulant treatment

LE TERAPIE “INNOVATIVE”:
I DOAC
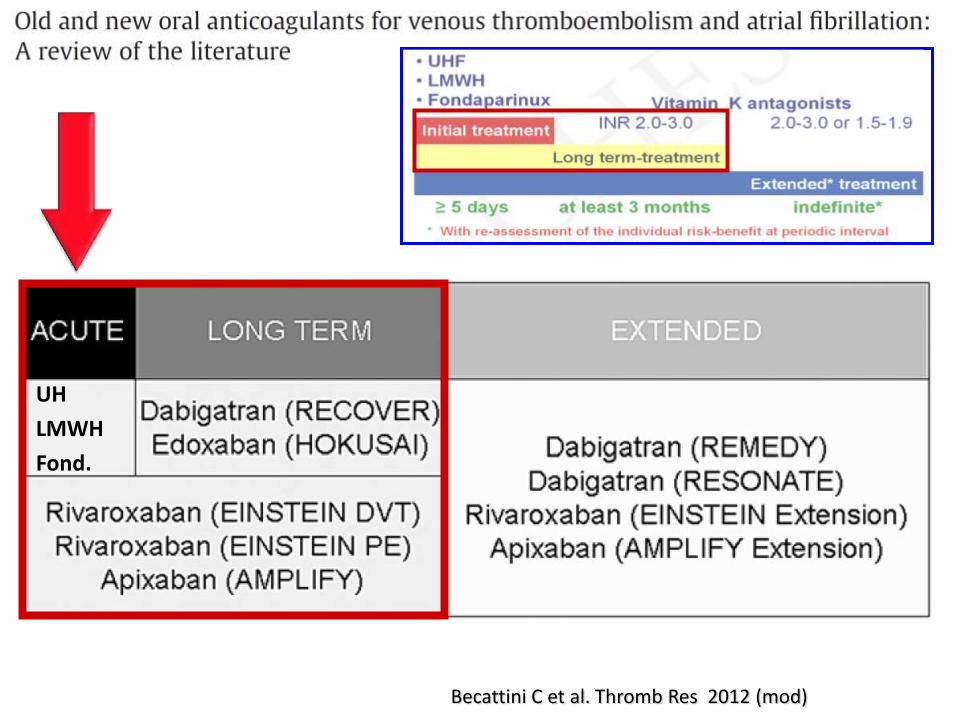
Becattini C et al. Thromb Res 2012 (mod)
UH
LMWH
Fond.
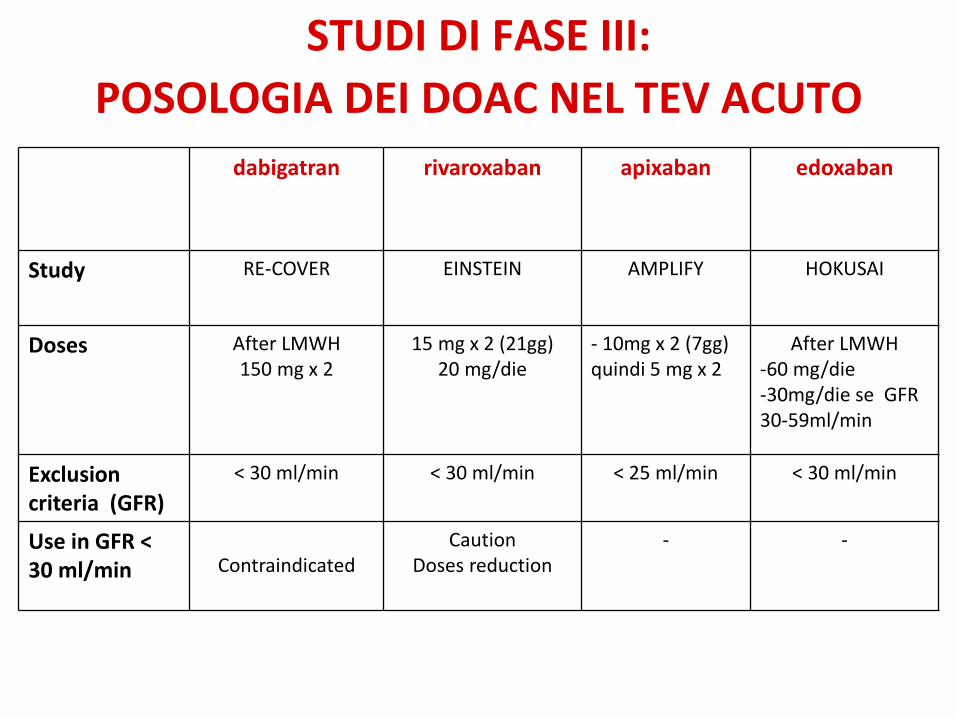
STUDI DI FASE III:
POSOLOGIA DEI DOAC NEL TEV ACUTO dabigatran rivaroxaban apixaban edoxaban
Study RE-COVER EINSTEIN AMPLIFY HOKUSAI
Doses After LMWH 150 mg x 2
15 mg x 2 (21gg) 20 mg/die
- 10mg x 2 (7gg) quindi 5 mg x 2
After LMWH -60 mg/die -30mg/die se GFR 30-59ml/min
Exclusion criteria (GFR)
< 30 ml/min < 30 ml/min < 25 ml/min < 30 ml/min
Use in GFR < 30 ml/min
Contraindicated
Caution Doses reduction
- -
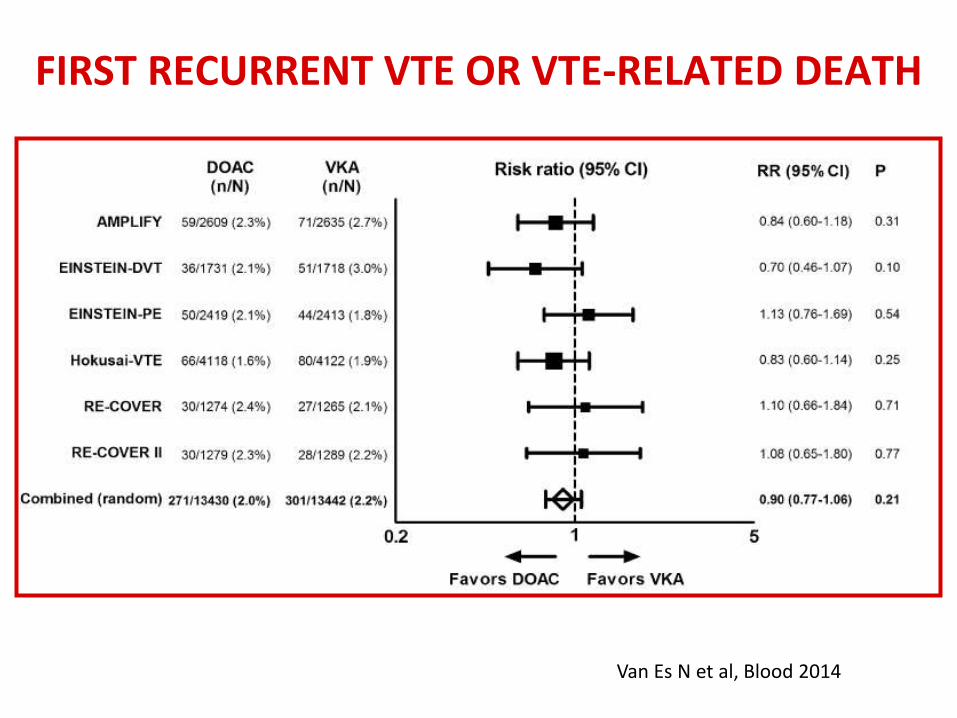
Van Es N et al, Blood 2014
FIRST RECURRENT VTE OR VTE-RELATED DEATH
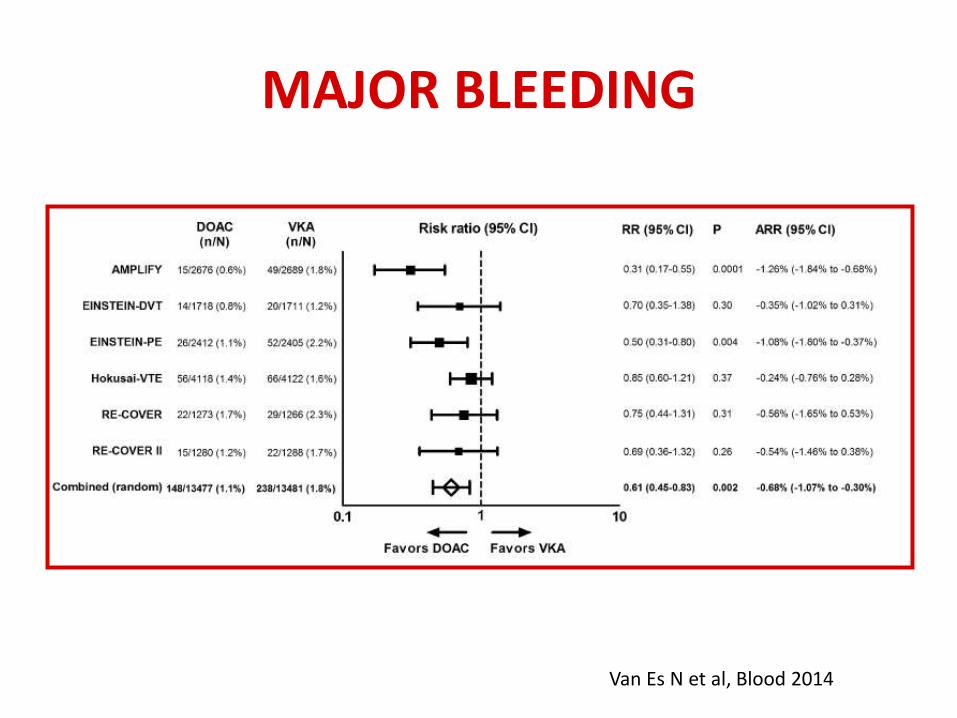
MAJOR BLEEDING
Van Es N et al, Blood 2014
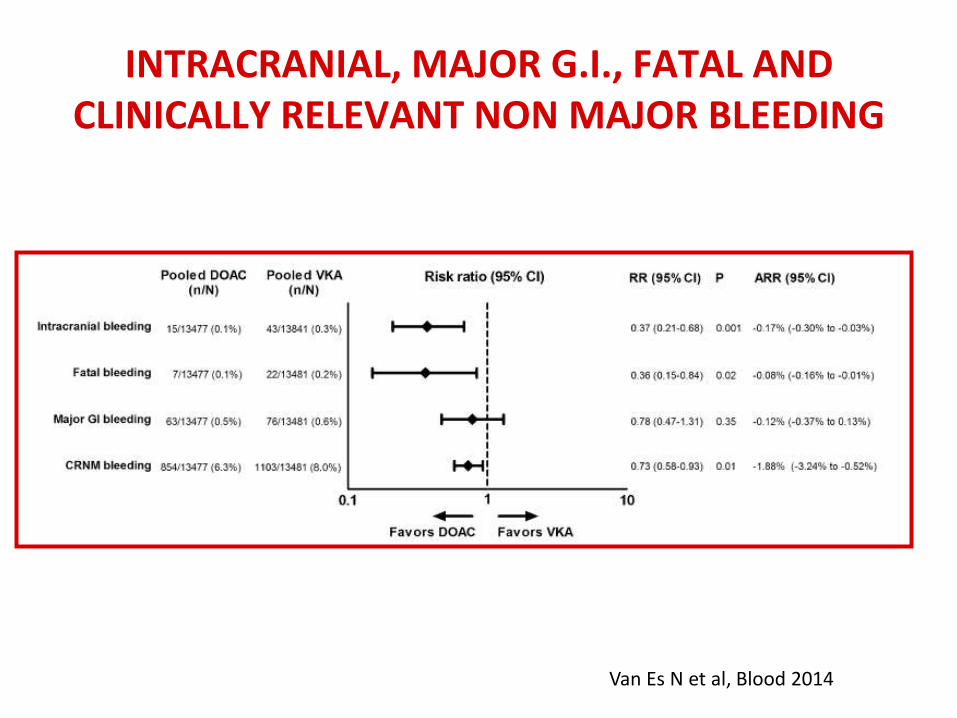
INTRACRANIAL, MAJOR G.I., FATAL AND CLINICALLY RELEVANT NON MAJOR BLEEDING
Van Es N et al, Blood 2014
Blood 2014
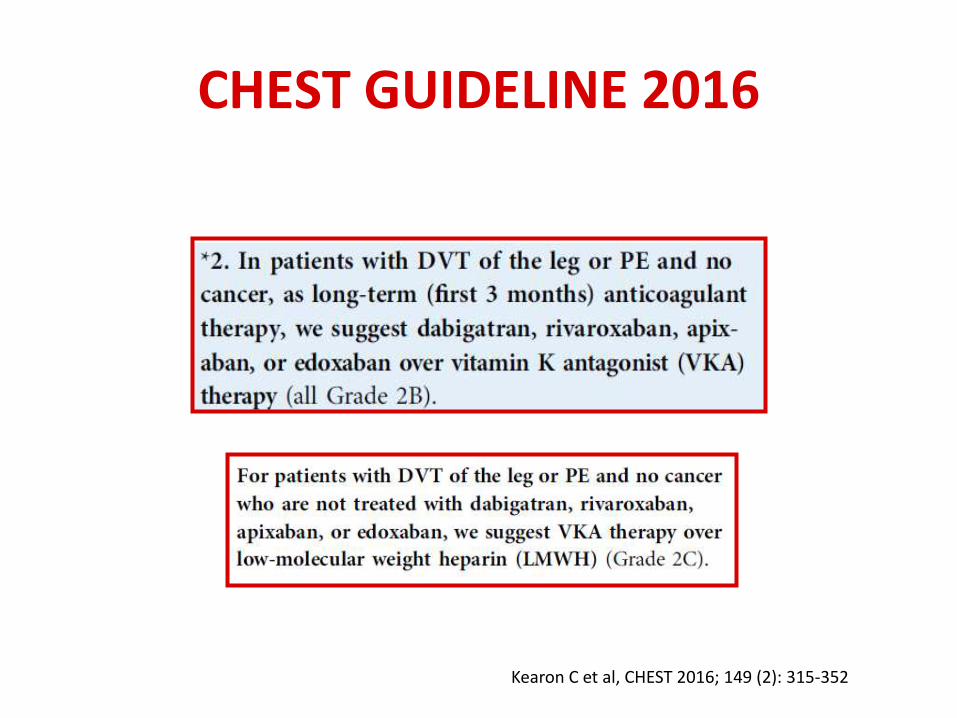
CHEST GUIDELINE 2016
Kearon C et al, CHEST 2016; 149 (2): 315-352
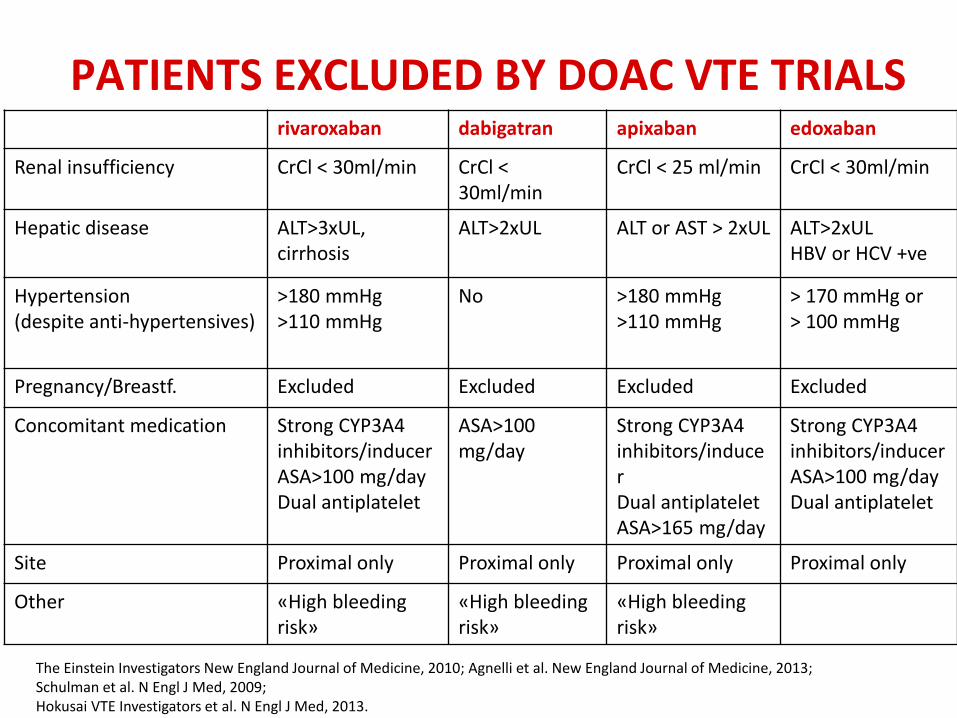
PATIENTS EXCLUDED BY DOAC VTE TRIALS rivaroxaban dabigatran apixaban edoxaban
Renal insufficiency CrCl < 30ml/min CrCl < 30ml/min
CrCl < 25 ml/min CrCl < 30ml/min
Hepatic disease ALT>3xUL, cirrhosis
ALT>2xUL ALT or AST > 2xUL ALT>2xUL HBV or HCV +ve
Hypertension (despite anti-hypertensives)
>180 mmHg >110 mmHg
No >180 mmHg >110 mmHg
> 170 mmHg or > 100 mmHg
Pregnancy/Breastf. Excluded Excluded Excluded Excluded
Concomitant medication Strong CYP3A4 inhibitors/inducer ASA>100 mg/day Dual antiplatelet
ASA>100 mg/day
Strong CYP3A4 inhibitors/inducer Dual antiplatelet ASA>165 mg/day
Strong CYP3A4 inhibitors/inducer ASA>100 mg/day Dual antiplatelet
Site Proximal only Proximal only Proximal only Proximal only
Other «High bleeding risk»
«High bleeding risk»
«High bleeding risk»
The Einstein Investigators New England Journal of Medicine, 2010; Agnelli et al. New England Journal of Medicine, 2013; Schulman et al. N Engl J Med, 2009; Hokusai VTE Investigators et al. N Engl J Med, 2013.

TEV DA NON TRATTARE CON DOAC • Insufficienza renale grave • Child Plugh C (Xarelto: Child-Plugh B e C) • In caso di trattamenti con farmaci fortemente interferenti • Embolie polmonari emodinamicamente instabili • Possibili indicazioni a trombolisi o manovre invasive • Recente chirurgia • Piastrinopenie • Gravidanza • Allattamento • Paziente non compliante
• TEV e cancro attivo (1° scelta LMWH) • TVS (fondaparinux, LMWH) • Trombosi in sedi inusuali
In corso studi
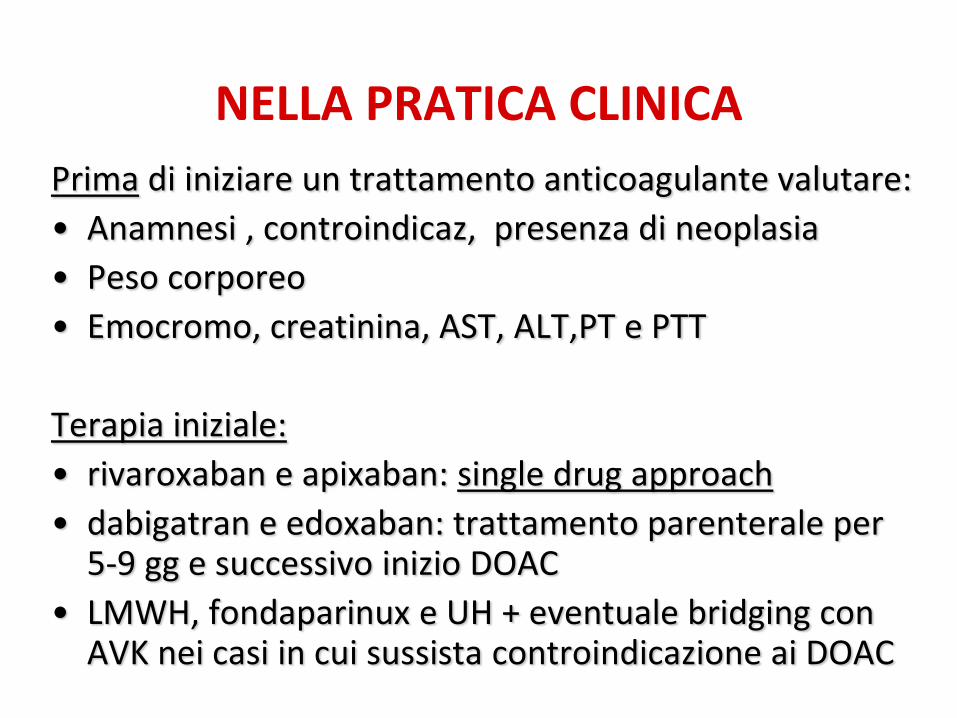
NELLA PRATICA CLINICA
Prima di iniziare un trattamento anticoagulante valutare:
• Anamnesi , controindicaz, presenza di neoplasia
• Peso corporeo
• Emocromo, creatinina, AST, ALT,PT e PTT
Terapia iniziale:
• rivaroxaban e apixaban: single drug approach
• dabigatran e edoxaban: trattamento parenterale per 5-9 gg e successivo inizio DOAC
• LMWH, fondaparinux e UH + eventuale bridging con AVK nei casi in cui sussista controindicazione ai DOAC

TERAPIA DEL TEV
UTILE
- Posizione antideclive degli arti
- Calze elastiche *
- Ecografia prima della sospensione del trattamento
- Ricerca delle cause (trombofilia/cancro)
INUTILE
• Immobilità
• Terapia antibiotica
• FANS
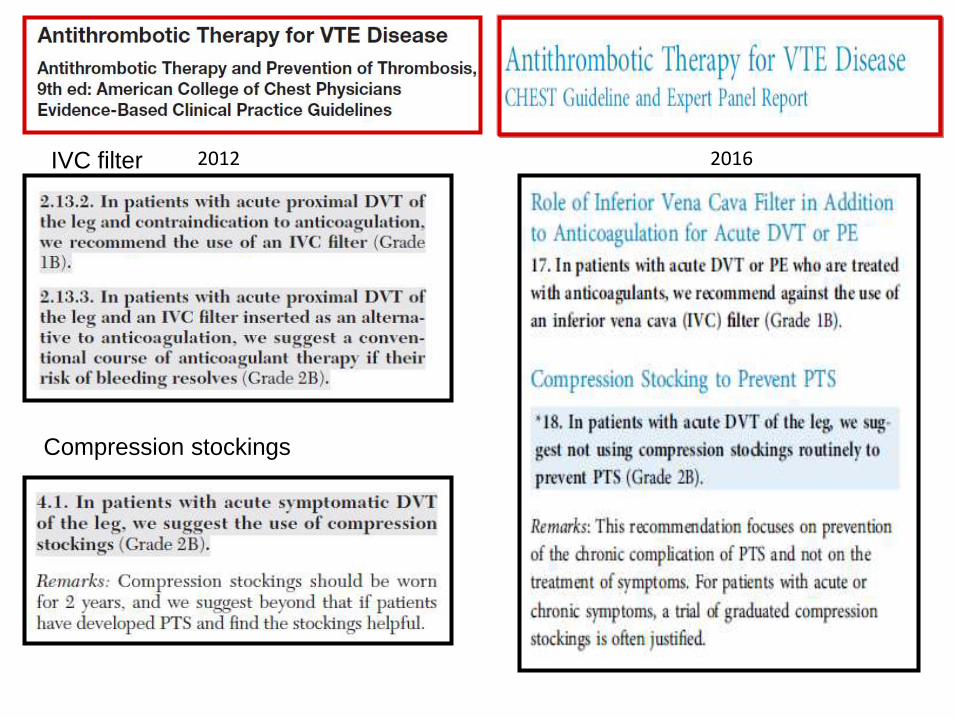
2012 2016 IVC filter
Compression stockings
TEV: TERAPIA DELLA “FASE ESTESA”
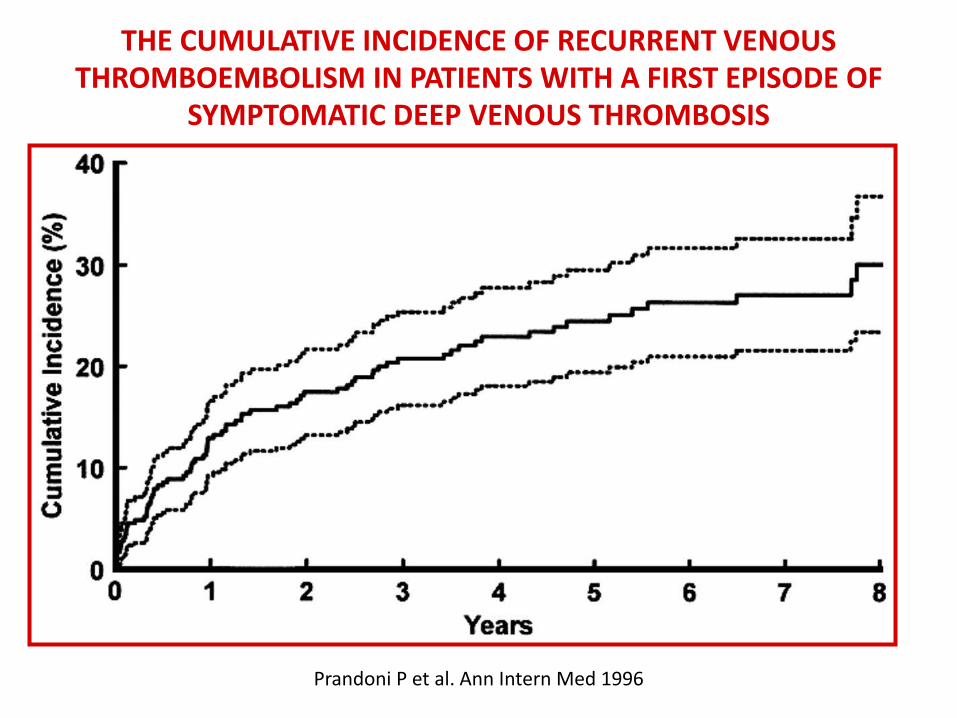
Prandoni P et al. Ann Intern Med 1996
THE CUMULATIVE INCIDENCE OF RECURRENT VENOUS THROMBOEMBOLISM IN PATIENTS WITH A FIRST EPISODE OF
SYMPTOMATIC DEEP VENOUS THROMBOSIS
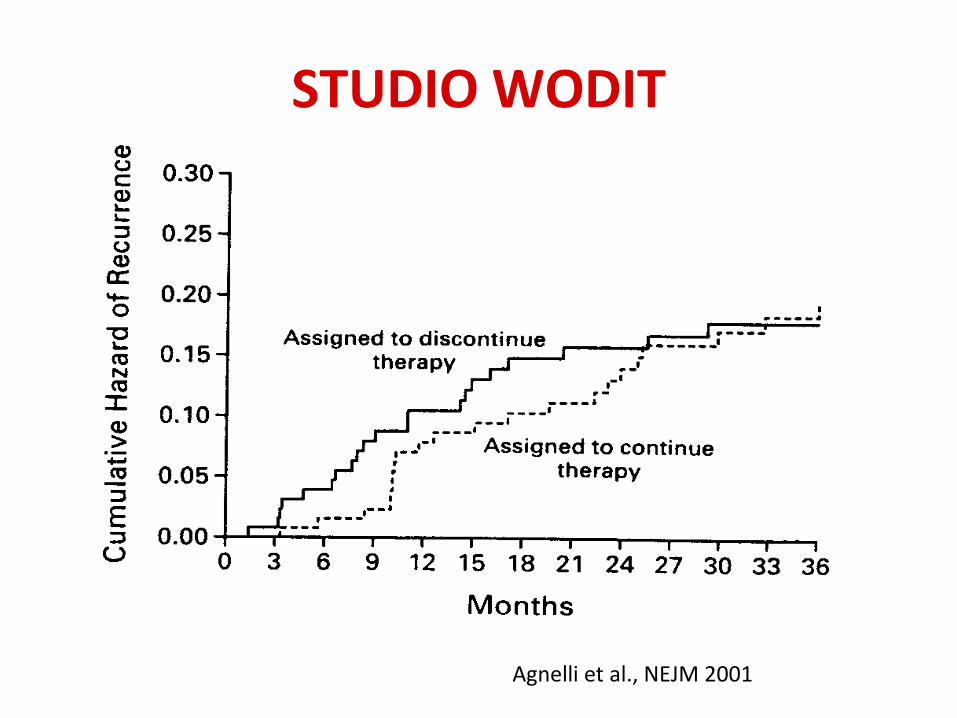
Agnelli et al., NEJM 2001
STUDIO WODIT
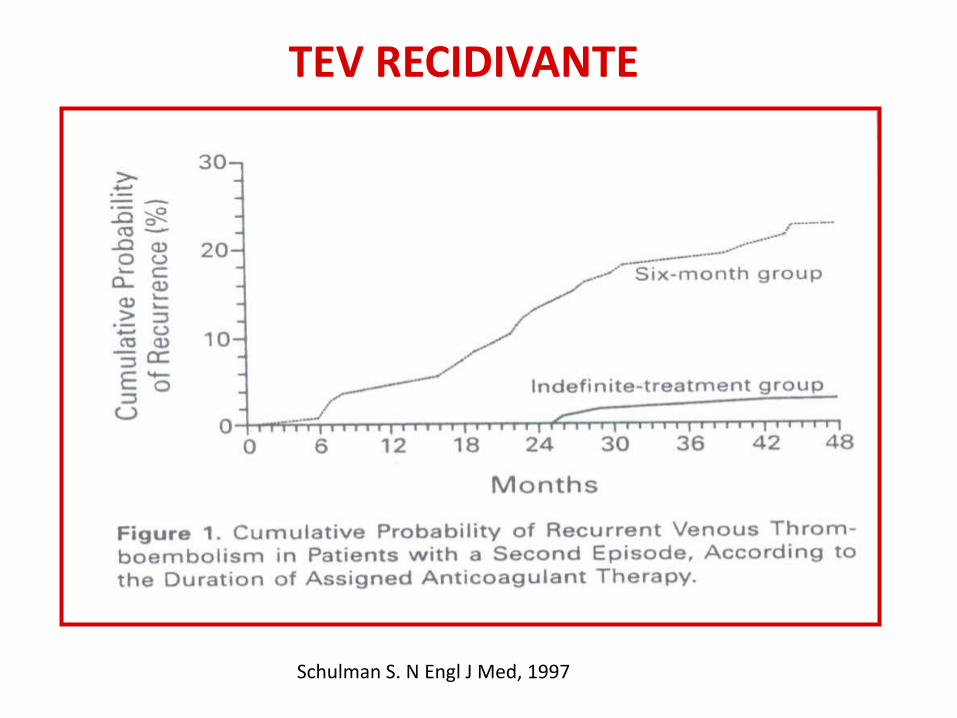
Schulman S. N Engl J Med, 1997
TEV RECIDIVANTE
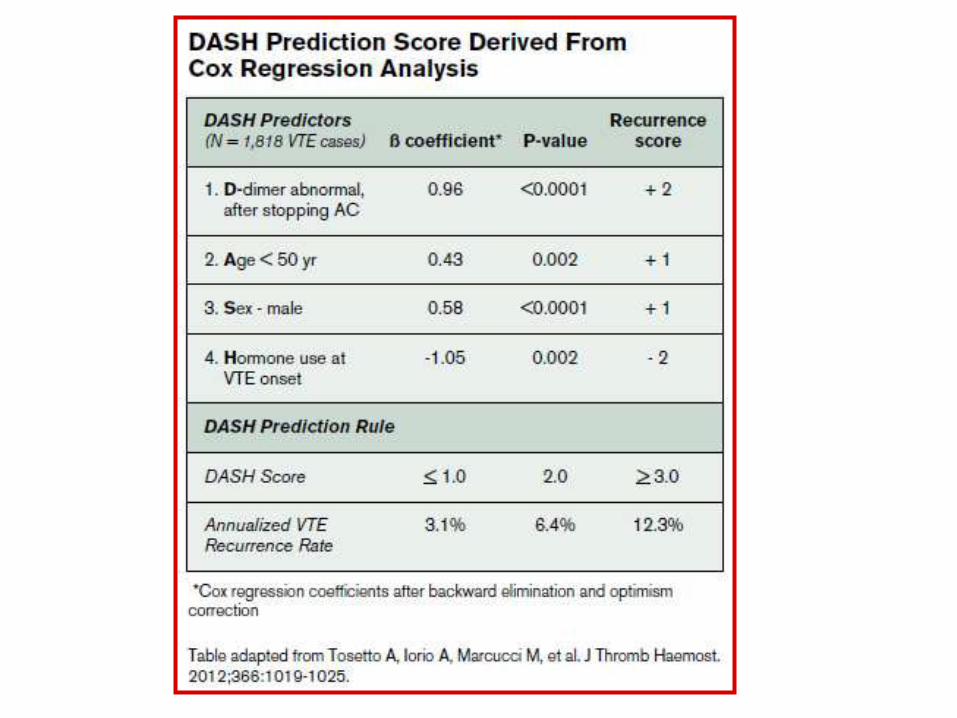
TEV E RISCHIO DI RECIDIVA
1. Caratteristiche e trattamento efficace del primo
episodio
2. Caratteristiche intrinseche del paziente
- Maschi > Femmine
- Tumore (mal. flogistiche croniche)
- Trombofilia ( PC, PS, AT, omozigosi FV e FII, doppie
eterozigosi, LAC)
- Persistenza di residuo trombotico
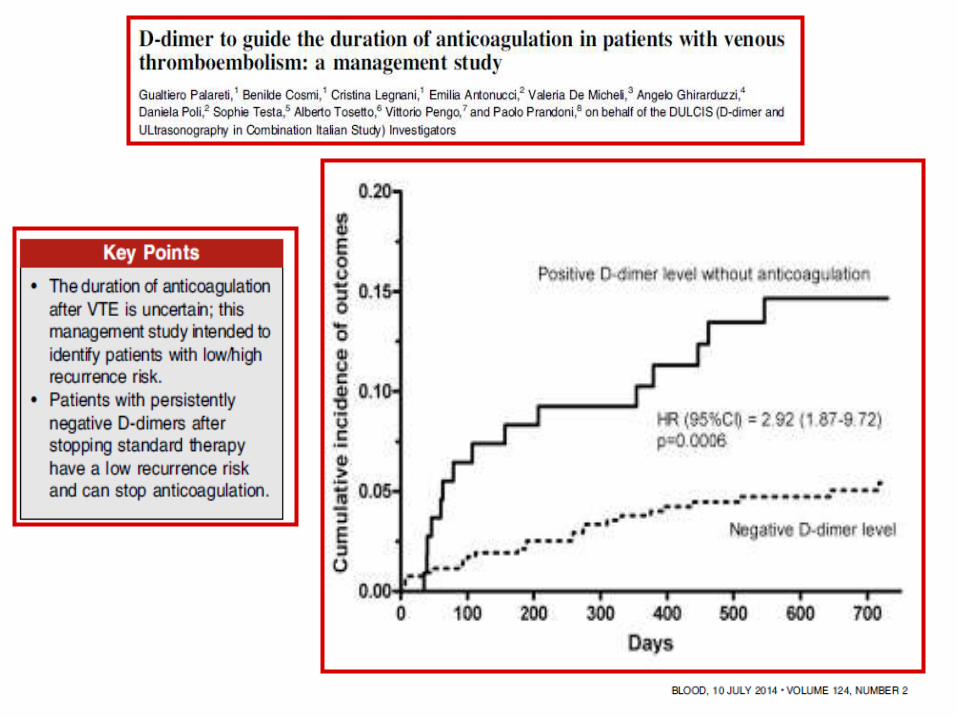
- D-dimeri alterati dopo sospensione TAO
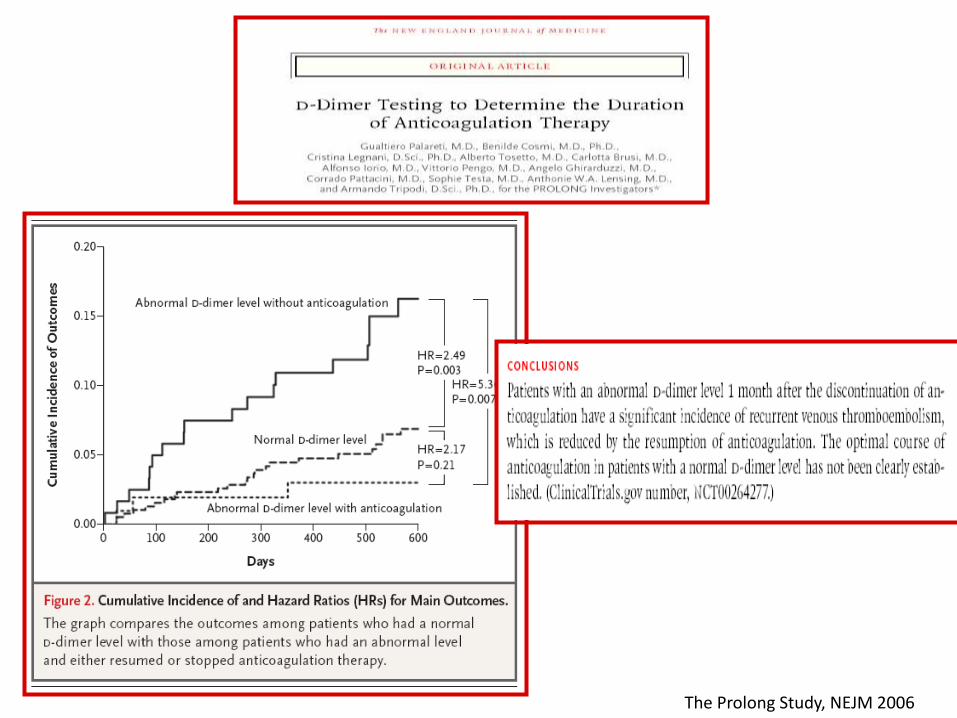
The Prolong Study, NEJM 2006
• Fase iniziale: prevenire estensione trombosi ed embolia
• Lungo termine: prevenire recidive precoci • • Estesa: prevenire recidive tardive, non correlate all'evento iniziale
2013
2013
2010
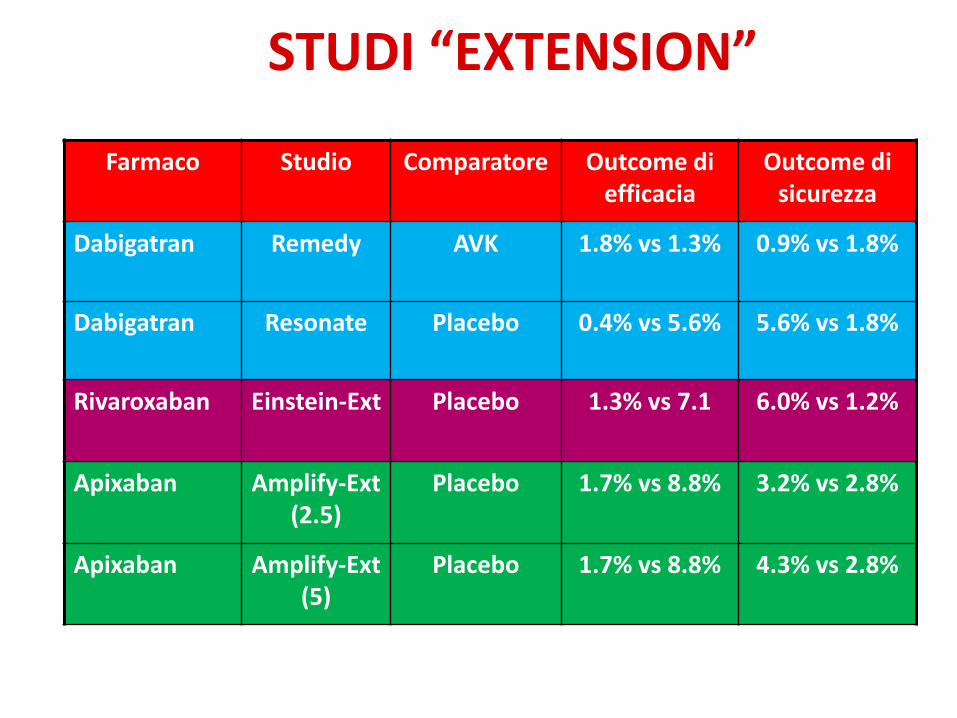
STUDI “EXTENSION”
Farmaco Studio Comparatore Outcome di efficacia
Outcome di sicurezza
Dabigatran Remedy AVK 1.8% vs 1.3% 0.9% vs 1.8%
Dabigatran Resonate Placebo 0.4% vs 5.6% 5.6% vs 1.8%
Rivaroxaban Einstein-Ext Placebo 1.3% vs 7.1 6.0% vs 1.2%
Apixaban Amplify-Ext (2.5)
Placebo 1.7% vs 8.8% 3.2% vs 2.8%
Apixaban Amplify-Ext (5)
Placebo 1.7% vs 8.8% 4.3% vs 2.8%
Conclusions
•Extended anticoagulation with apixaban at either a treatment dose (5 mg) or a prophylactic dose (2,5 mg) reduced the risk of venous thromboembolism without increasing the rate of major bleeding.
•The AMPLIFY-EXT trial has shown that apixaban may be as safe as aspirin or even placebo.
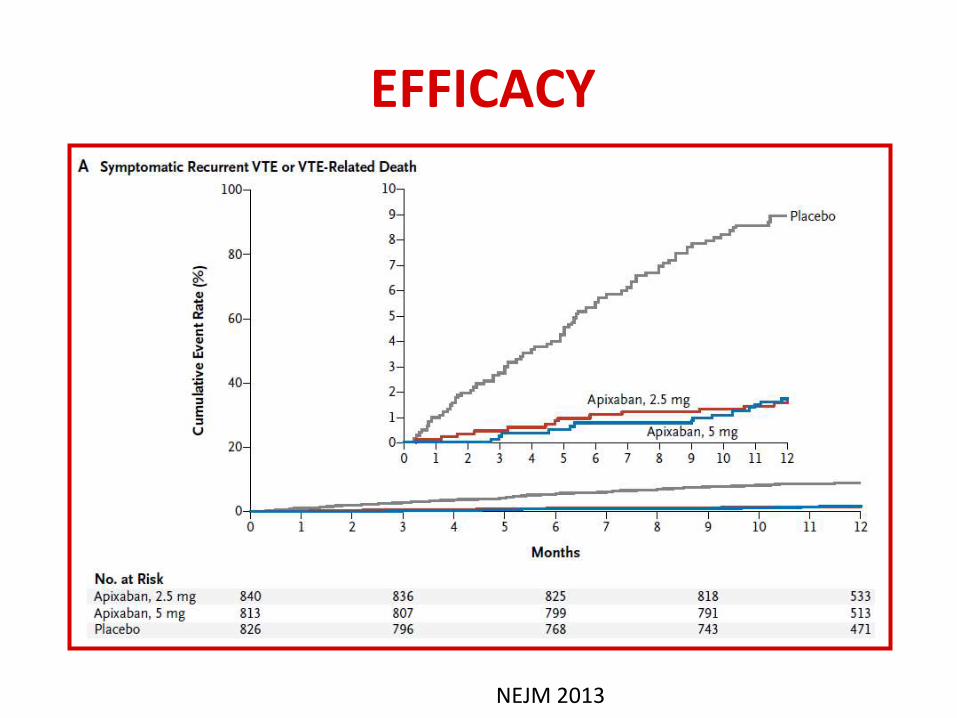
EFFICACY
NEJM 2013
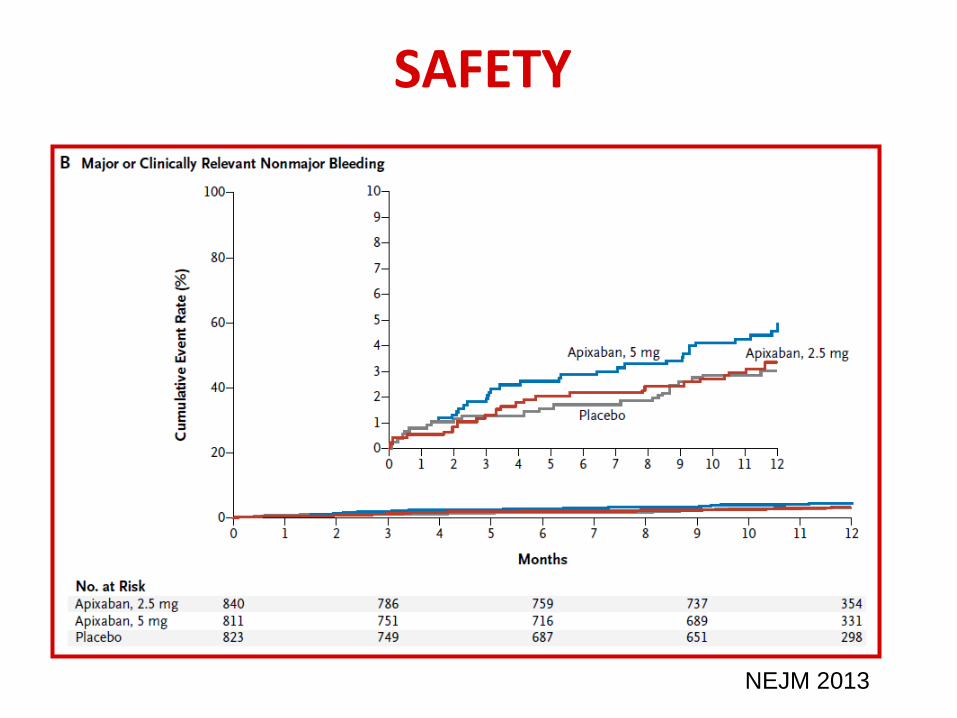
SAFETY
NEJM 2013
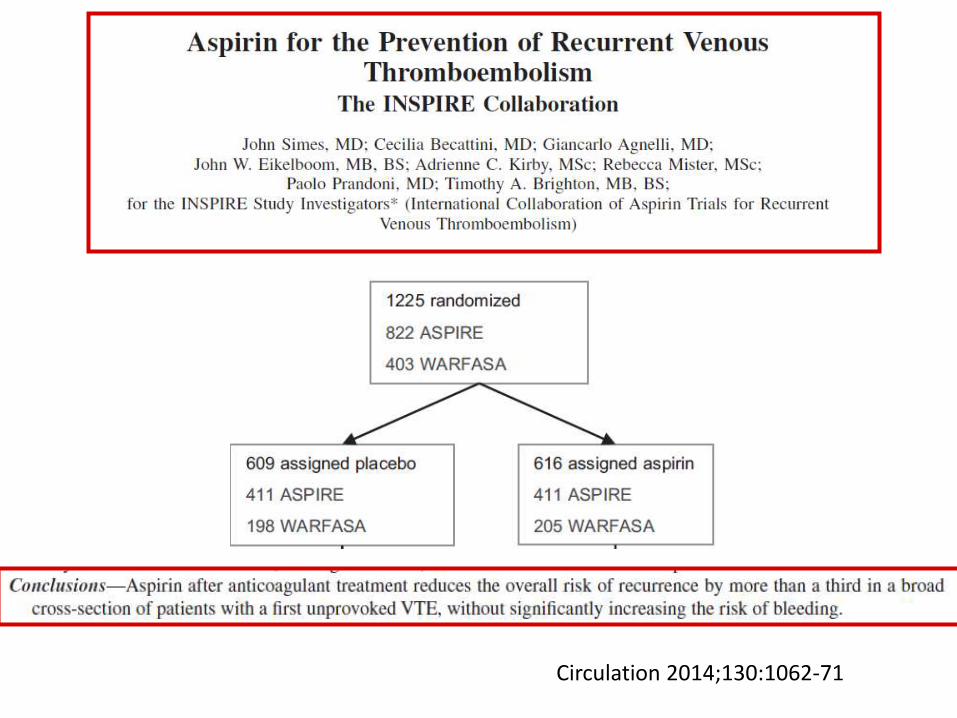
Circulation 2014;130:1062-71
Based on indirect comparison, we expect the net benefit of extended anticoagulant therapy in patients with unprovoked VTE to be substantially greater than the benefits of extended aspirin therapy. Consequently, we do not consider aspirin a reasonable alternative to anticoagulant therapy in patients who want extended therapy.
CHEST 2016; 149(2):315-352
E NEL “MONDO REALE”?
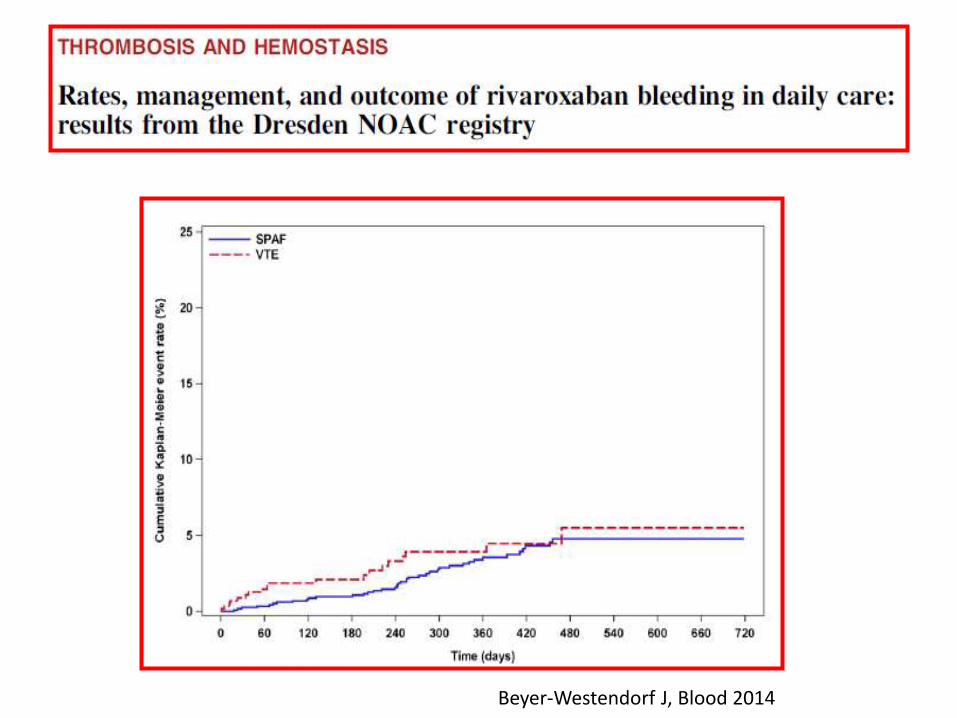
Beyer-Westendorf J, Blood 2014
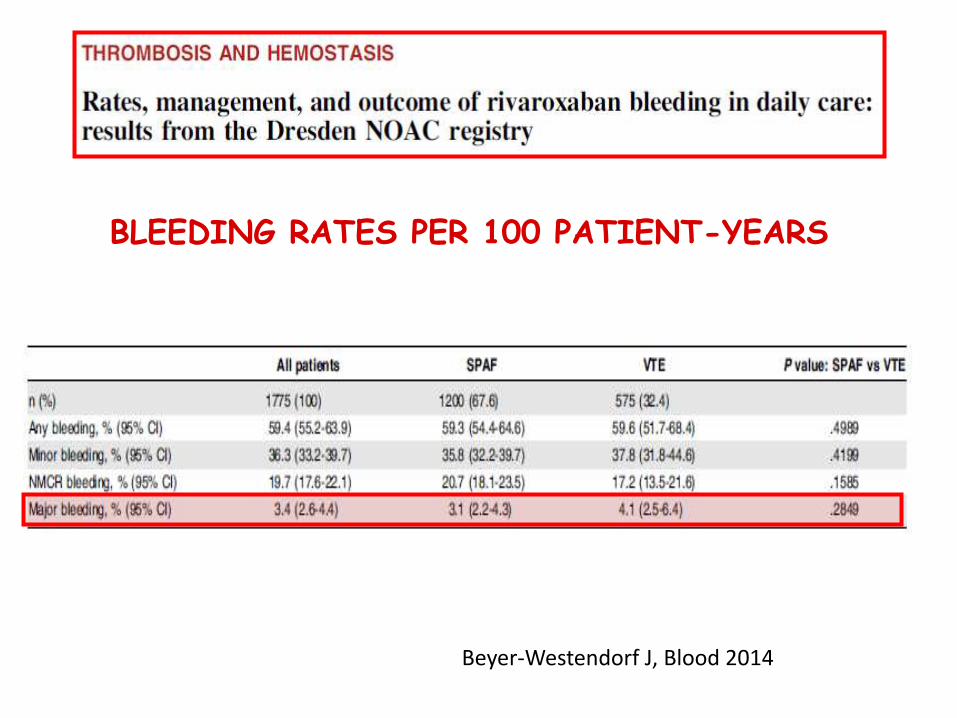
BLEEDING RATES PER 100 PATIENT-YEARS
Beyer-Westendorf J, Blood 2014

http://www.start-register.org
9980patients
75% with fup
133 events
727 patients
40% with fup
Start
laboratorio
593 patients
Start oncology.........
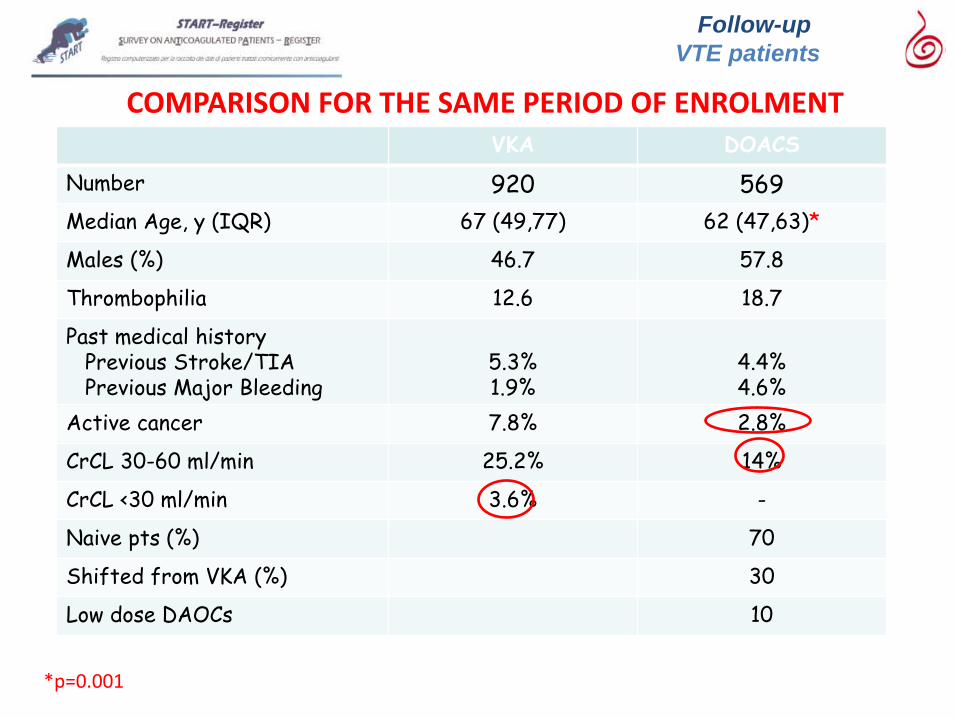
Follow-up
VTE patients
VKA DOACS
Number 920 569
Median Age, y (IQR) 67 (49,77) 62 (47,63)*
Males (%) 46.7 57.8
Thrombophilia 12.6 18.7
Past medical history Previous Stroke/TIA Previous Major Bleeding
5.3% 1.9%
4.4% 4.6%
Active cancer 7.8% 2.8%
CrCL 30-60 ml/min 25.2% 14%
CrCL <30 ml/min 3.6% -
Naive pts (%) 70
Shifted from VKA (%) 30
Low dose DAOCs 10
*p=0.001
COMPARISON FOR THE SAME PERIOD OF ENROLMENT
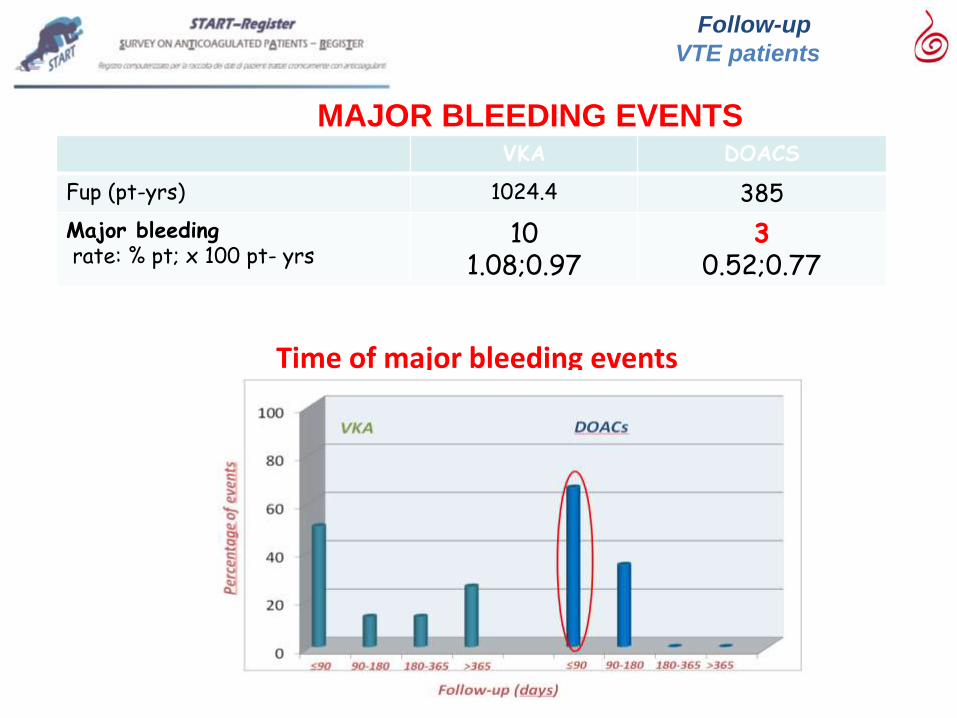
VKA DOACS
Fup (pt-yrs) 1024.4 385
Major bleeding rate: % pt; x 100 pt- yrs
10 1.08;0.97
3 0.52;0.77
MAJOR BLEEDING EVENTS
Follow-up
VTE patients
Time of major bleeding events
VKA DOACs
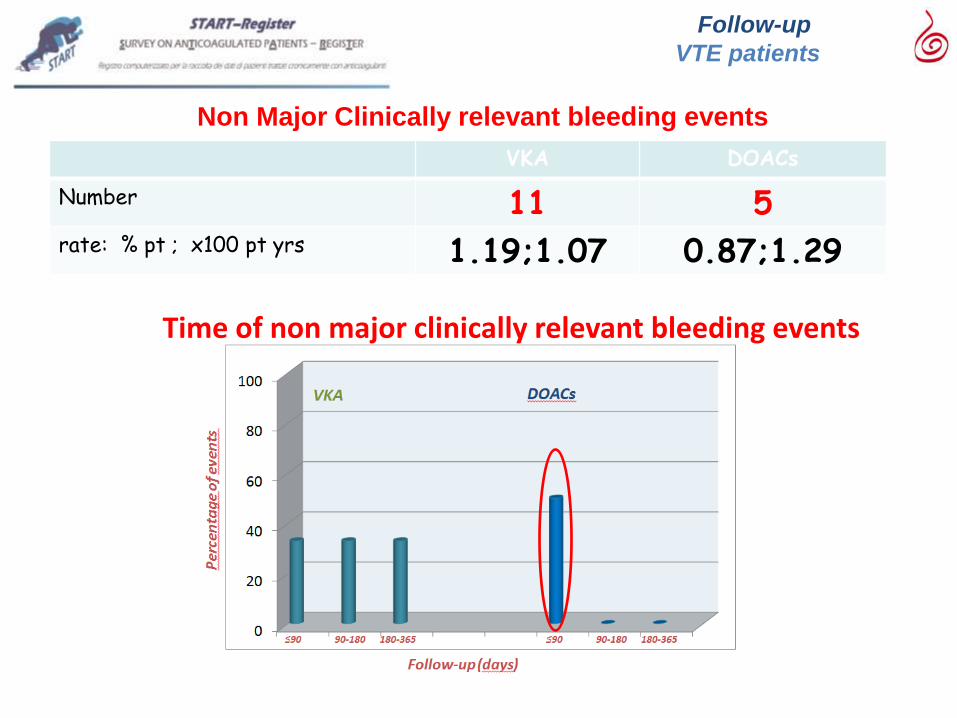
Number 11 5 rate: % pt ; x100 pt yrs 1.19;1.07 0.87;1.29
Non Major Clinically relevant bleeding events
Follow-up
VTE patients
Time of non major clinically relevant bleeding events
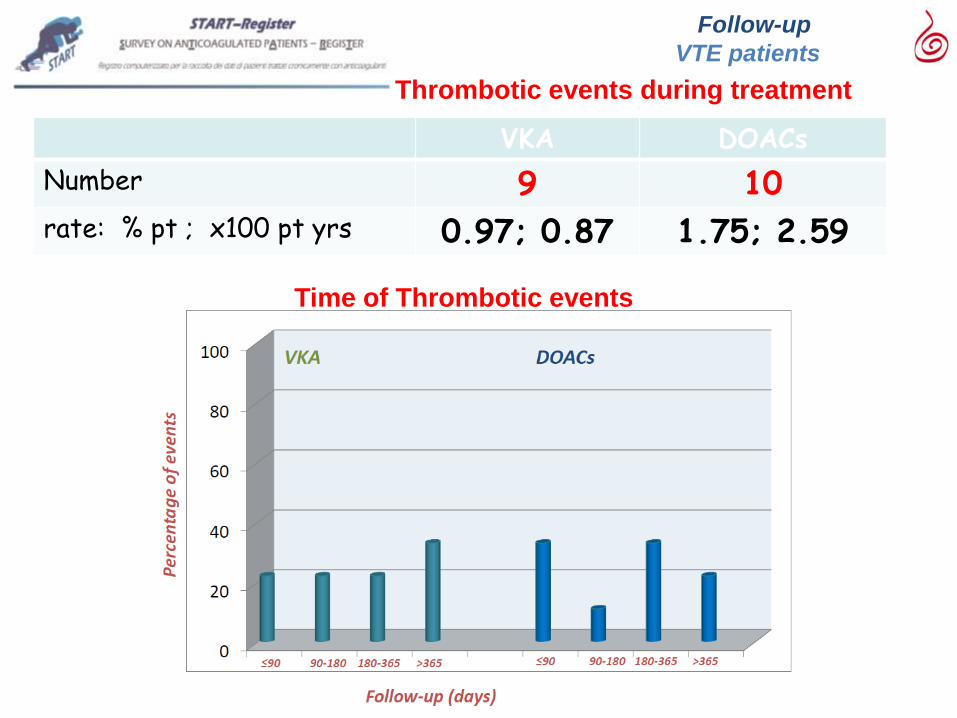
VKA DOACs
Number 9 10 rate: % pt ; x100 pt yrs 0.97; 0.87 1.75; 2.59
Thrombotic events during treatment
Follow-up
VTE patients
Time of Thrombotic events
TROMBOEMBOLISMO VENOSO
• Ottimizzare la scelta del farmaco anticoagulante più idoneo per il
singolo paziente
• Valutare i fattori di rischio individuali
• Effettuare il follow up clinico/di laboratorio e strumentale
• Definire la durata ottimale del trattamento anticoagulante nel
TEV, bilanciando il rischio tromboembolico ed il rischio
emorragico

FATTORI DA CONSIDERARE NELLA SCELTA DEL
FARMACO PER IL TRATTAMENTO DEL TEV
Kearon C et al, Chest 2016
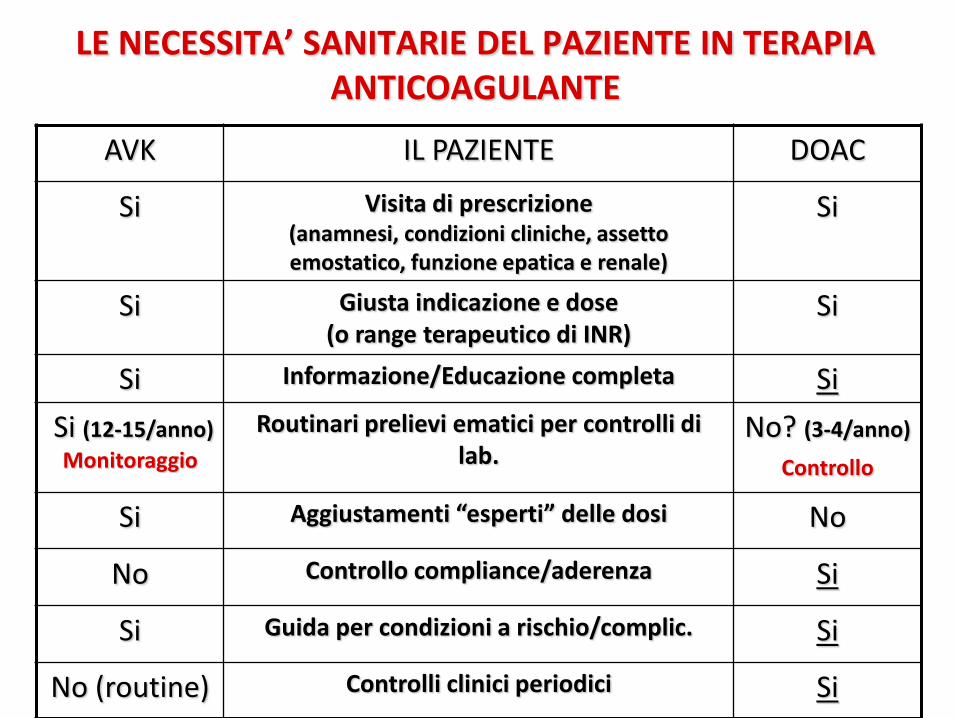
LE NECESSITA’ SANITARIE DEL PAZIENTE IN TERAPIA ANTICOAGULANTE
AVK IL PAZIENTE DOAC
Si Visita di prescrizione (anamnesi, condizioni cliniche, assetto emostatico, funzione epatica e renale)
Si
Si Giusta indicazione e dose (o range terapeutico di INR)
Si
Si Informazione/Educazione completa Si
Si (12-15/anno)
Monitoraggio
Routinari prelievi ematici per controlli di lab.
No? (3-4/anno)
Controllo
Si Aggiustamenti “esperti” delle dosi No
No Controllo compliance/aderenza Si
Si Guida per condizioni a rischio/complic. Si
No (routine) Controlli clinici periodici Si
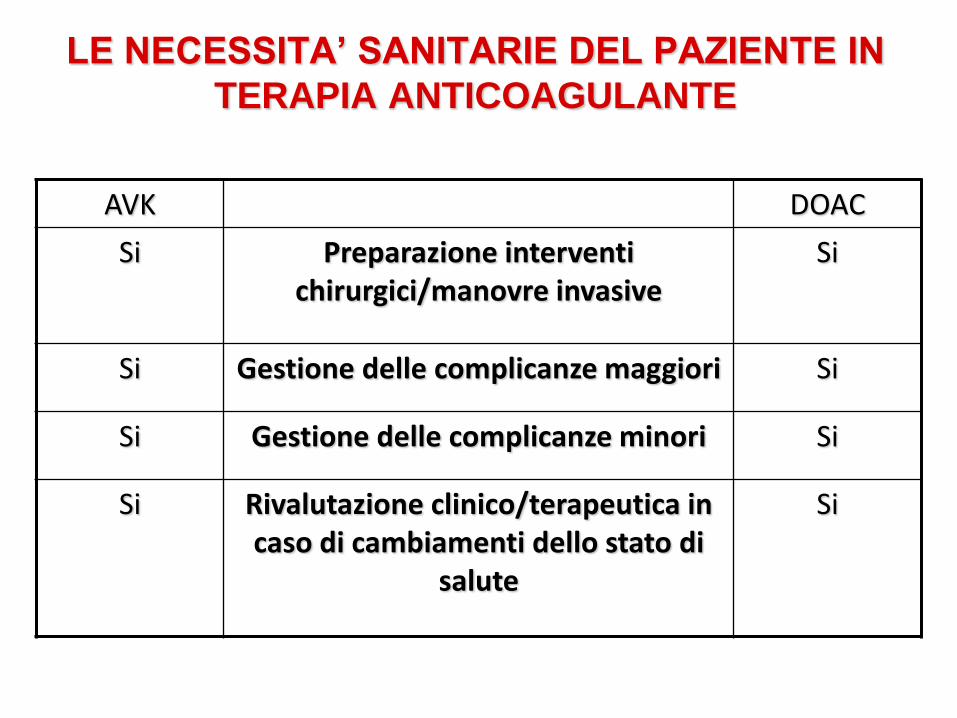
LE NECESSITA’ SANITARIE DEL PAZIENTE IN
TERAPIA ANTICOAGULANTE
AVK DOAC
Si Preparazione interventi chirurgici/manovre invasive
Si
Si Gestione delle complicanze maggiori Si
Si Gestione delle complicanze minori Si
Si Rivalutazione clinico/terapeutica in caso di cambiamenti dello stato di
salute
Si
CONCLUSIONI
• L’introduzione dei DOAC nella pratica clinica ha ampliato le opzioni
terapeutiche per il trattamento del TEV
• I DOAC rappresentano oggi la 1° scelta di trattamento, previa
valutazione delle controindicazioni
• La scelta del trattamento deve basarsi:
1. conoscenza delle singole molecole
2. condizioni cliniche del singolo paziente
• Il paziente affetto da tromboembolismo venoso ha specifiche
necessità sanitarie, non solo rappresentate dalla scelta del farmaco
(Il Piano Terapeutico rappresenta una procedura amministrativa e non
può/deve essere considerato una modalità gestionale sanitaria)


















