Sindrome metabolica/Dia bete - unisalute.it · Sindrome metabolica/Dia bete Giulio Marchesini...
19
Sindrome metabolica/Dia bete Giulio Marchesini “Alma Mater Studiorum” Università di Bologna
Transcript of Sindrome metabolica/Dia bete - unisalute.it · Sindrome metabolica/Dia bete Giulio Marchesini...

Sindrome
metabolica/Dia
bete
Giulio Marchesini
“Alma Mater Studiorum” Università
di Bologna
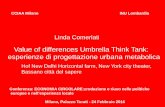
Criteria for Metabolic Syndrome
Grundy, Circulation 2005
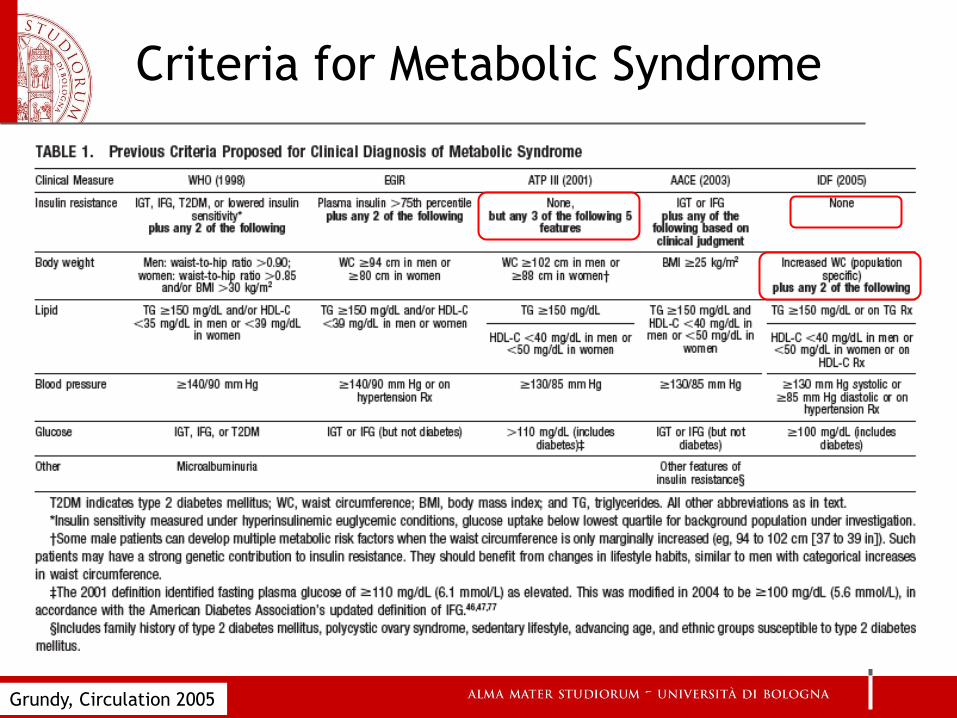
Maison, Diabetes Care 2001
Ely Study: a prospective
cohort established in 1990
Central role of obesity
Factor analysis on changes
in the parameters of MS
• Axis are Factors of MS
• Changes in BMI, WHR and
Fasting insulin are
central to the 3
independent factors in
the entire cohort
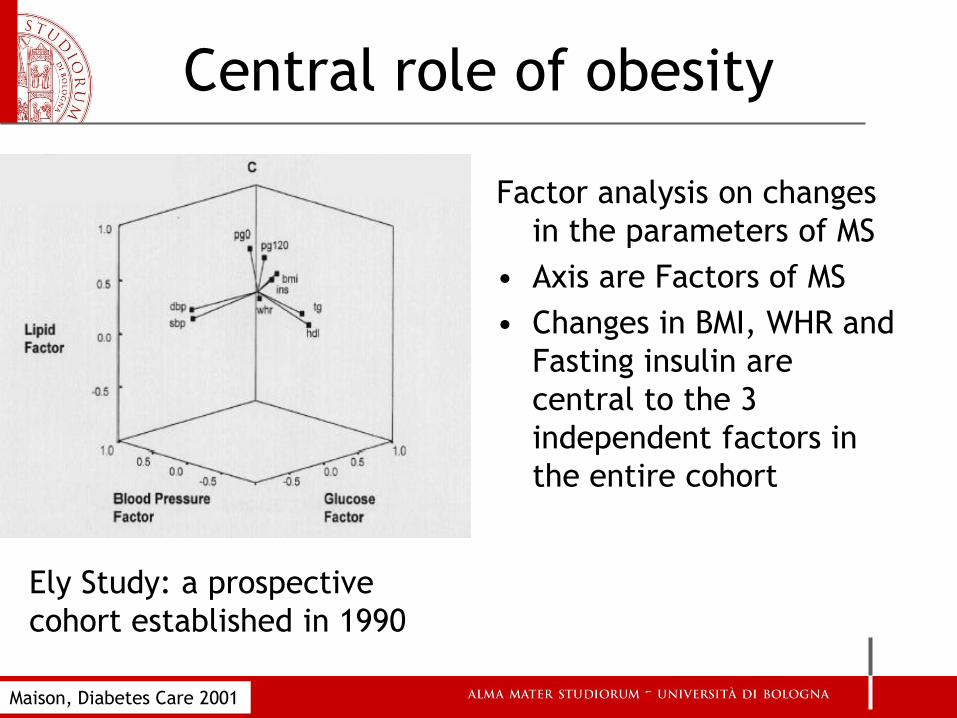
Abdominal obesity predicts the
metabolic syndrome
>30 <30
<102 cm (men)
<88 cm (women)
>102 cm (men)
>88 cm (women)
Body mass index (kg/m2)
8-y
ear
incid
ence o
f
meta
bolic s
yndro
me
Han; Obes Res 2002
33
20
20
10
0
10
20
30
40
San Antonio Heart
Study:
628 non-Hispanic
whites and 1,340
Mexican
Americans
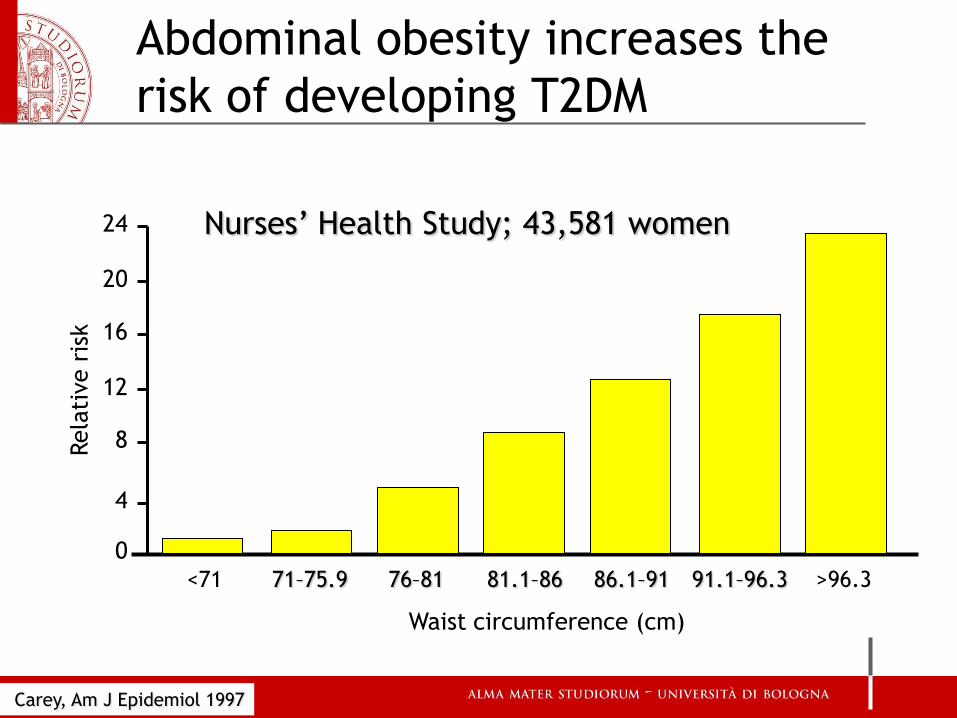
Abdominal obesity increases the
risk of developing T2DM
<71 71–75.9 76–81 81.1–86 86.1–91 91.1–96.3 >96.3
24
20
16
12
8
4
0
Rela
tive r
isk
Waist circumference (cm)
Nurses’ Health Study; 43,581 women
Carey, Am J Epidemiol 1997
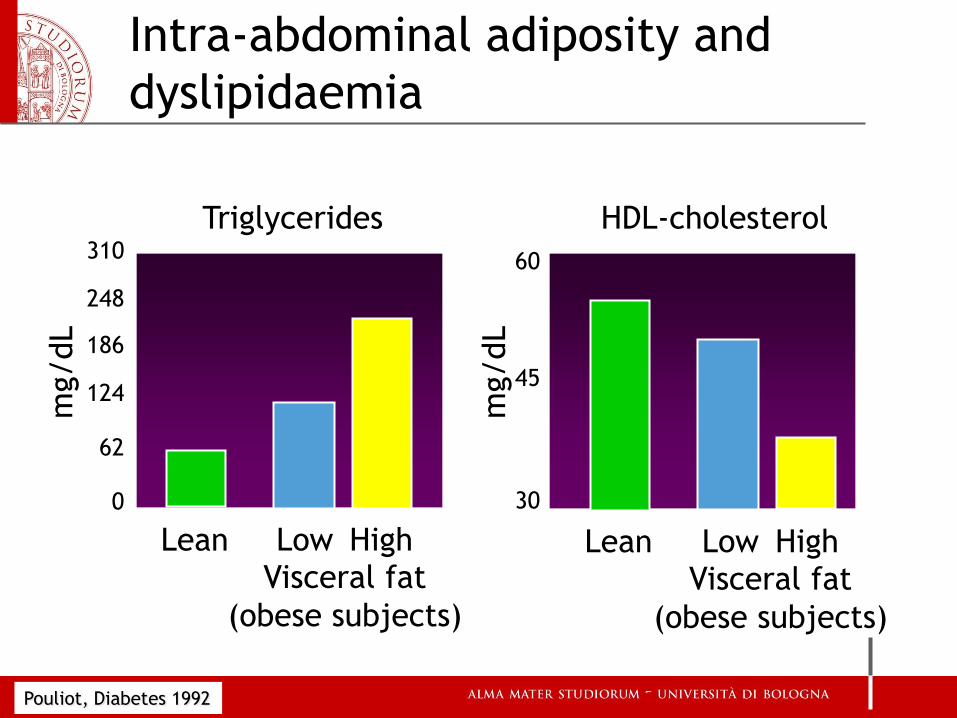
Intra-abdominal adiposity and
dyslipidaemia
Pouliot, Diabetes 1992
310
248
186
124
62
0
60
45
30 m
g/dL
mg/dL
Triglycerides
Lean
HDL-cholesterol
Visceral fat
(obese subjects)
Low High Lean Visceral fat
(obese subjects)
Low High

Abdominal obesity predicts the
risk of CV events Adju
sted r
ela
tive r
isk
1 1 1
1.17 1.16 1.14
1.29 1.27
1.35
0.8
1
1.2
1.4
CVD death MI All-cause deaths
Tertile 1
Tertile 2 Tertile 3
Men Women <95
95–103 >103
<87
87–98 >98
Waist
circ. (cm):
Adjusted for BMI, age, smoking, sex, CVD, disease, DM, HDL-C, total-C
Dagenais, Am Heart J 2005

Come fare lo screening ?
Quale test di screening ?
• Peso
• BMI (peso/altezza2)
• Circonferenza vita
• Rapporto vita/fianchi
• Circonferenza vita/altezza
• (Circonferenza collo)
• (circonferenza polso)
Screening x DM2
L’OMS ha definito criteri che
rendono un test di screening
raccomandabile:
•Test semplice da eseguire,
•Test facile da interpretare,
•Test di elevata accuratezza
diagnostica,
•Test con favorevole rapporto
costo/beneficio.
Holland. WHO European Centre for Health
Policy: Screening in Europe, 2006
Elementi PRO screening
• Il DM2 presenta una lunga fase asintomatica (malattia diagnosticata
solo se ricercata con screening).
• Sono disponibili test di screening non invasivi, semplici e poco
costosi.
• La percentuale di DM2 non diagnosticato varia fra il 30 e il 50% dei
casi di diabete tipo 2 e nella fase pre-clinica si sviluppano le
complicanze.
• Un compenso glicemico ottimale fin dalle prime fasi della malattia
e la correzione dei fattori di rischio CV associati riducono
l’incidenza e la progressione delle complicanze.
• Le complicanze acute e croniche del DM2 hanno un grave impatto
sulla qualità di vita dell’individuo, nonché sulla salute pubblica.
• Nel corso dello screening possono essere identificati soggetti con
IGT e IFG nei quali interventi sullo stile di vita
prevengono/ritardano lo sviluppo della malattia conclamata.
Elementi CONTRO screening
• La prevalenza della malattia non è elevata.
• Alla diagnosi di diabete può far seguito la comparsa di
depressione.
• Dispendio di tempo ed energia da parte del paziente per
eseguire test aggiuntivi necessari a confermare la diagnosi
e per le visite di follow-up.
• Possibili effetti avversi del trattamento.
• Incremento dei costi, almeno iniziali, derivanti dal
trattamento anticipato della malattia rispetto alla sua
naturale evoluzione.
• Carenza di evidenze sulla maggior efficacia di interventi
messi in atto nella fase pre-clinica della malattia rispetto
a quelli instaurati dopo la diagnosi clinica.
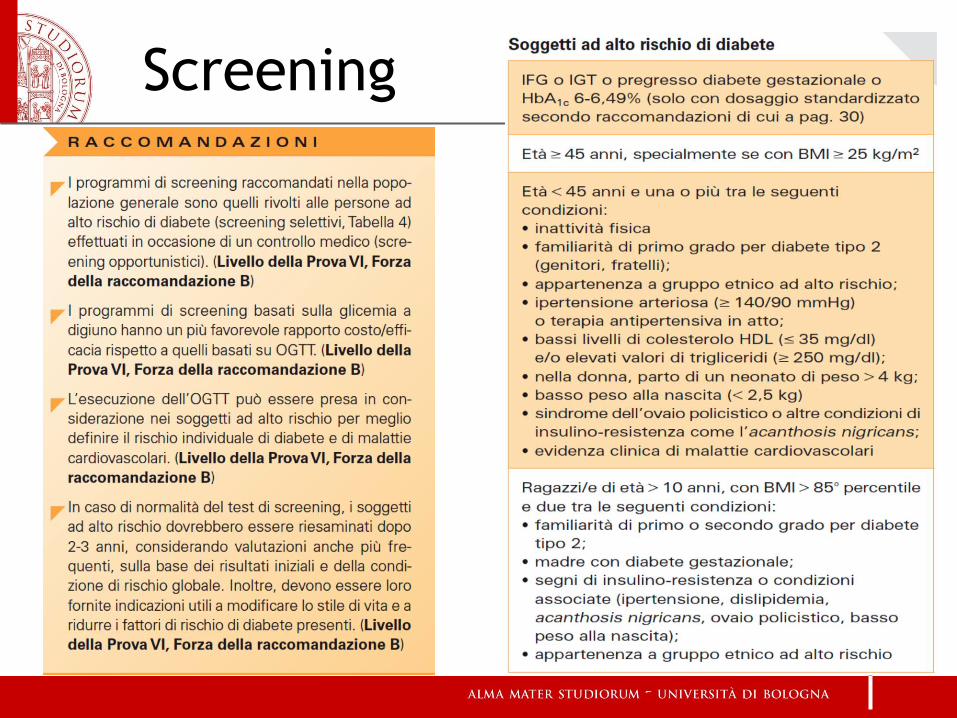
Screening
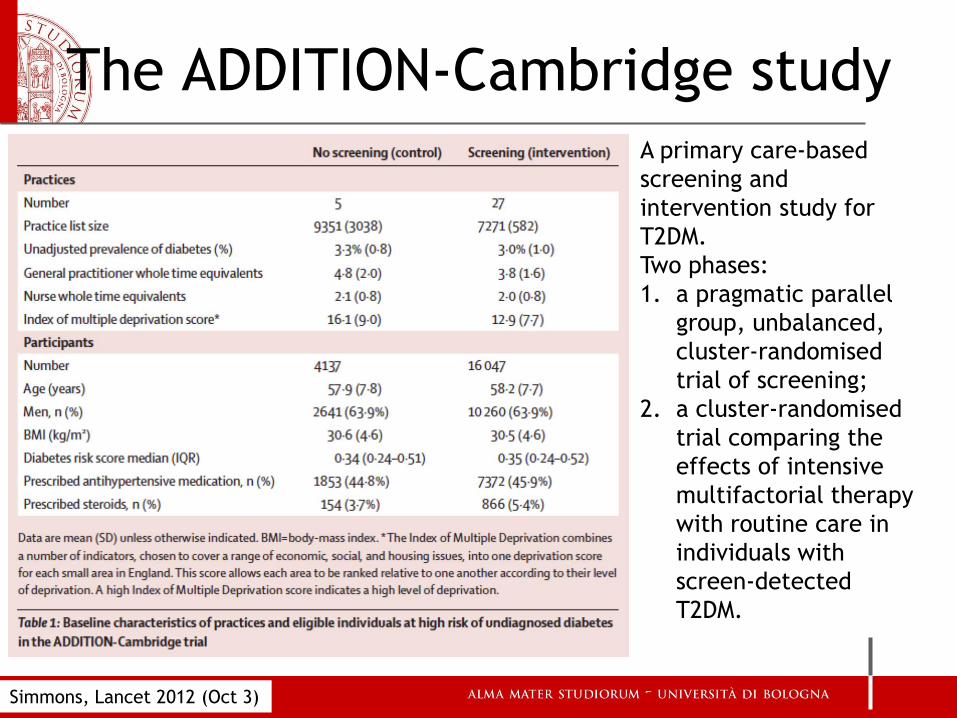
The ADDITION-Cambridge study A primary care-based
screening and
intervention study for
T2DM.
Two phases:
1. a pragmatic parallel
group, unbalanced,
cluster-randomised
trial of screening;
2. a cluster-randomised
trial comparing the
effects of intensive
multifactorial therapy
with routine care in
individuals with
screen-detected
T2DM.
Simmons, Lancet 2012 (Oct 3)

The ADDITION-Cambridge study
Simmons, Lancet 2012 (Oct 3)
Of 16 047 high-risk individuals in screening practices, 15 089 (94%) were
invited for screening during 2001–06, 11 737 (73%) attended, and 466 (3%)
were diagnosed with diabetes. 4137 control individuals were followed up.
During 184 057 person-years of follow up (median duration 9.6 years [IQR
8.9–9.9]), there were 1532 deaths in the screening practices and 377 in
control practices (mortality hazard ratio [HR] 1.06, 95% CI 0.90–1.25).

The ADDITION-Cambridge study
Simmons, Lancet 2012 (Oct 3)
In this large UK sample, screening for type 2 diabetes in patients at increased risk
was not associated with a reduction in all-cause, cardiovascular, or diabetes-related
mortality within 10 years. The benefits of screening might be smaller than expected.
The SWEETHEART registry
• 2,767 pts presenting with STEMI or NSTEMI
• Those without known DM had an OGTT at day 4 after
admission.
• Female pts. have higher rates of known and newly-
diagnosed DM (30.2 and 19.7% compared with 23.1 and
15.3 in males)
• 3-Year mortality rates with known DM not different
between males and females (35.4% and 30.0).
• Mortality in newly-diagnosed DM much higher in
females (30.5% vs. 21.8).
Tschoepe, Diabetologia 2012
CAD as risk for DM
• 506 consecutive non-DM patients undergoing coronary
angiography for suspected CAD (significant CAD, 293
cases)
• Follow up, 7.5 years (3795 patient-years)
• 107 incident cases of DM (21.1%, 2.8% per year)
• Patients with significant CAD had a 33% increased risk
of incident DM at follow-up
Conclusion: The presence of CAD indicates an increased
risk of DM. Repeated screening and targeted programs
are warranted to prevent diabetes
Saely, Diabetologia 2012
Impatto delle Malattie croniche non
trasmissibili (CNCD) sui Sistemi Sanitari
Le CNCD avranno un effetto devastante sui Sistemi Sanitari,
orientati oggi prevalentemente alla cura, non alla
promozione della salute
Il diabete potrebbe diventare la pandemia del 21* secolo
Occorrono interventi sistematici sulla popolazione
“ The lives of far too many people in the
world are being blighted and cut short by
chronic disease such as heart disease ,
stroke, cancer, chronic respiratory disease
and diabetes”
LEE Jong-wook
Director-General,
World Health Organization