Servizio di Endocrinologia Osp. «Sacro Cuore – Don ... · (PCOS), hypogonadism, hypothalamic...
32
V Corso Aggiornamento Ame in Endocrinologia Clinica AGRIGENTO 20/22 MARZO 2014 Museo Archeologico Servizio di Endocrinologia Osp. «Sacro Cuore – Don Calabria» Negrar – Verona AGGIORNAMENTI su PATOLOGIA SURRENALICA Lino Furlani
Transcript of Servizio di Endocrinologia Osp. «Sacro Cuore – Don ... · (PCOS), hypogonadism, hypothalamic...

V Corso Aggiornamento Ame
in Endocrinologia Clinica
AGRIGENTO 20/22 MARZO 2014Museo Archeologico
Servizio di Endocrinologia Osp. «Sacro Cuore – Don Calabria»
Negrar – Verona
AGGIORNAMENTI su PATOLOGIA SURRENALICA Lino Furlani

• Ipercortisolismo – Approccio clinico – screening di laboratorio
– Cenni di terapia farmacologica
• Ipertensione resistente – Approccio clinico e screening di laboratorio
nell’Iperaldosteronismo Primitivo
Di cosa parleremo ?


and relatively young women and men, and patients with
hypertension resistant to treatment [5–7]. As such, theEuropean Society of Endocrinology recommends investi-
gation for Cushing’s disease in patients presenting these
features at an unusual (young) age [8].The heterogeneity of Cushing’s disease, the overlapping
of signs and symptoms with those of other disorders, the
need for differential diagnosis, the variety of biochemicaltests and imaging techniques available for diagnosis, and
questions surrounding how to better define response andremission all contribute to the challenges physicians face in
optimizing patient management, despite ongoing advances
in diagnosis and treatment. Thus, a multidisciplinary teamof neurosurgeons, endocrinologists, and radiation oncolo-
gists, as well as an individualized patient approach, is
recommended for the management of Cushing’s disease[9–19].
The first-line treatment for Cushing’s disease is trans-
sphenoidal surgery (TSS) to remove the adenoma, butinitial surgery frequently fails [2, 13]. Although radio-
therapy is an option if initial TSS is unsuccessful, the
effects of radiotherapy may only become apparent aftermany years [20] and the intervention may be followed by
side effects, such as pituitary deficiency or failure, as well
as damage to the optic nerve because of the frequent needof traditional approaches [21, 22]. Medical therapy can also
be useful in cases of surgical failure, but some of the drugs
in use have limited effects or are not approved for use intreating Cushing’s disease [13, 23]. Pasireotide (Signifor!;
Novartis AG, Basel, Switzerland), the first pituitary-direc-
ted medical therapy, was recently approved in the Euro-pean Union and in the US for treating adult patients with
Cushing’s disease for whom surgery is not an option or for
whom surgery has failed. Its long-term effectiveness intreating the symptoms of Cushing’s disease has been
shown in phase III trials [24, 25]. This state-of-the-art
review aims to provide an overview of the most recentscientific research and clinical information regarding
Cushing’s syndrome, with an overall focus on Cushing’s
disease.
Pathophysiology and etiology of Cushing’s disease
Corticotrophic adenomas secreting ACTH are the most
common cause of endogenous Cushing’s syndrome,accounting for approximately 70 % of cases [2]. The
increased ACTH secreted by the tumor acts on the adrenal
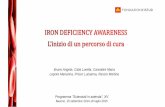
glands to stimulate increased cortisol production, which inturn leads to the variety of signs and symptoms of Cush-
ing’s disease (Fig. 1). In most cases, the tumors are benign
and slow growing. Microadenomas (B10 mm in diameter)are found in [90 % of cases, whereas macroadenomas
([10 mm in diameter) are less common (\10 % of cases).As discussed below, the size of the tumor can influence
treatment outcomes.
The biochemical relationships involved in the hypo-thalamus—pituitary—adrenal axis are such that hypercor-
tisolism leading to Cushing’s syndrome can also be caused
by extrapituitary tumors that secrete ACTH or CRH,adrenal adenomas or carcinomas, and adrenal hyperplasia
or dysplasia [2]. Furthermore, several genetic alterations
have also been identified as contributing to sporadic cor-ticotropinoma formation, including alterations to
PRKAR1A (encoding a cAMP-dependent protein kinase A
subunit), PDE11A (encoding a cyclic nucleotide signaltransducer), and PDE8B (encoding a cyclic nucleotide
phosphodiesterase) [26, 27]. Finally, aberrant stimulation
of steroidogenesis in ACTH-independent macronodularadrenal hyperplasia and in some unilateral adenomas can
be driven by ectopic receptors such as those for glucose-
dependent insulinotropic peptide or gastric inhibitorypolypeptide, b-adrenergic receptors, serotonin, and proba-
bly angiotensin II receptor. However, it can also result
Fig. 1 Signs and symptoms of Cushing’s disease
Endocrine
123
• A chi proporre accertamenti ?
• Quali ?
• Cenni di Terapia Farmacologica

Caso clinico
Daniela, di anni 48 AP: familiarità per ICTUS CEREBRI ed IPERTENSIONE ARTERIOSA; IPERTESA da 8 anni. IPERCOLESTEROLEMIA. DIABETE tipo 2. OBESA 1 grado. Terapia: ACEI + DIURETICO; IPOCOLESTEROLEMIZZANTE; ANTIAGGREGANTE; DIETA + METFORMINA Negli ultimi 10 anni aumenta di peso con accentuazione negli ultimi due anni; adotta una dieta ipocalorica che riesce a farLe perdere significativamente peso Nell’ultimo anno per controllare efficacemente la PA associa all’ACE Inibitore anche il diuretico. ECOCOLORDOPPLER TSA (2013): note diffuse di ateromasia di parete; bilateralmente, al bulbo e all’origine della C.I., placca realizzante stenosi del 30% a destra e del 40% a sinistra

Caso clinico
Es. Obiettivo:
- PA 130/85 con fc 68 bpm, regolare;
- peso 70,5 Kg, altezza 150 cm, BMI 31,3 Kg/m2
- Facies «piena», non striae rubrae, non gibbosità, non
ecchimosi, non segni di iperandrogenismo.
In una paziente con queste caratteristiche
avreste avviato uno screening per Cushing ?

Screening negli obesi?

9
CLINICS 2010;65(1):9-13
CLINICAL SCIENCE
Division of Endocrinology and Metabolism, Department of Internal Medicine, Cerrahpasa Medical Faculty - Sivas, Turkey.Email: [email protected]: 90 216 4623114Received for publication on September 11, 2009 Accepted for publication on October 08, 2009
SCREENING FOR CUSHING’S SYNDROME IN OBESE PATIENTS
Ozay Tiryakioglu, Serdal Ugurlu, Serap Yalin, Sibel Yirmibescik, Erkan Caglar, Demet Ozgil Yetkin, Pinar Kadioglu
doi: 10.1590/S1807-59322010000100003
Tiryakioglu O, Ugurlu S, Yalin S, Yirmibescik S, Caglar E, Yetkin DO et al. Screening for Cushing’s Syndrome in obese patients. Clinics. 2010;65(1):9-13.
OBJECTIVES: The aim of this study was to examine the frequency of Cushing’s syndrome (CS) in obese patients devoid of specific clinical symptoms of Cushing’s syndrome. METHODS: A total of 150 obese patients (129 female, 21 male; mean age 44.41 ± 13.34 yr; mean BMI 35.76 ± 7.13) were in-cluded in the study. As a first screening step, we measured 24-h urinary free cortisol (UFC). An overnight 1-mg dexamethasone suppression test was also performed on all patients. Urinary free cortisol levels above 100 µg/24 h were considered to be abnormal. Suppression of serum cortisol <1.8 µg/dL after administration of 1 mg dexamethasone was the cut-off point for normal suppression. The suppression of the serum cortisol levels failed in all of the patients. RESULTS: Measured laboratory values were as follows: ACTH, median level 28 pg/ml, interquartile range (IQR) 14-59 pg/ml; fasting glucose, 100 (91-113) mg/dL; insulin, 15.7 (7.57-24.45) mU/ml; fT4, 1.17 (1.05-1.4) ng/dL; TSH, 1.70 (0.91-2.90) mIU/L; total cholesterol, 209 (170.5-250) mg/dL; LDL-c, 136 (97.7-163) mg/dL; HDL-c, 44 (37.25-50.75) mg/dL; VLDL-c, 24 (17-36) mg/dL; triglycerides, 120.5 (86-165) mg/dL. The median UFC level of the patients was 30 µg/24 h (IQR 16-103). High levels of UFC (>100 µg/24 h) were recorded in 37 patients (24%). Cushing’s syndrome was diagnosed in 14 of the 150 patients (9.33%). Etiologic reasons for Cushing’s syndrome were pituitary microadenoma (9 patients), adrenocortical adenoma (3 patients), and adrenocortical carcinoma (1 patient). CONCLUSION: A significant proportion (9.33%) of patients with simple obesity were found to have Cushing’s syndrome. These findings argue that obese patients should be routinely screened for Cushing’s syndrome.
KEYWORDS: Cushing’s syndrome. Obesity. Screening. Cortisol. Adrenocorticorticotropic hormone.
INTRODUCTION
Obesity is the most common metabolic problem in industrialized countries. In the USA, 32% of adults are classified as overweight, and 22.5% of these individuals are obese.1 Both overweight and obese subjects are at an increased risk for cardiovascular diseases,2 some types of cancer,3 diabetes4, and even premature death.5 Obesity is often accompanied by other chronic disorders including
hypertension, osteoarthritis, bile stones, and dyslipidemia.6-12 In addition to these physical disorders, obesity is commonly associated with psychological and psycho-social problems.10
Obesity can coexist with diverse physical disorders, and physicians should first focus on the differential diagnosis of possible underlying disorders before initiating any management procedure. Obesity is a prominent feature of endocrine diseases including hypothyroidism, insulin-excess syndromes, polycystic ovary syndrome (PCOS), hypogonadism, hypothalamic disease/injury, growth hormone deficiency, leptin deficiency or leptin receptor defects, pseudohypoparathyroidism, and Cushing’s syndrome (CS).11,12
Diagnosis of CS is primarily based on the signs and 9
CLINICS 2010;65(1):9-13
CLINICAL SCIENCE
Division of Endocrinology and Metabolism, Department of Internal Medicine, Cerrahpasa Medical Faculty - Sivas, Turkey.Email: [email protected]: 90 216 4623114Received for publication on September 11, 2009 Accepted for publication on October 08, 2009
SCREENING FOR CUSHING’S SYNDROME IN OBESE PATIENTS
Ozay Tiryakioglu, Serdal Ugurlu, Serap Yalin, Sibel Yirmibescik, Erkan Caglar, Demet Ozgil Yetkin, Pinar Kadioglu
doi: 10.1590/S1807-59322010000100003
Tiryakioglu O, Ugurlu S, Yalin S, Yirmibescik S, Caglar E, Yetkin DO et al. Screening for Cushing’s Syndrome in obese patients. Clinics. 2010;65(1):9-13.
OBJECTIVES: The aim of this study was to examine the frequency of Cushing’s syndrome (CS) in obese patients devoid of specific clinical symptoms of Cushing’s syndrome. METHODS: A total of 150 obese patients (129 female, 21 male; mean age 44.41 ± 13.34 yr; mean BMI 35.76 ± 7.13) were in-cluded in the study. As a first screening step, we measured 24-h urinary free cortisol (UFC). An overnight 1-mg dexamethasone suppression test was also performed on all patients. Urinary free cortisol levels above 100 µg/24 h were considered to be abnormal. Suppression of serum cortisol <1.8 µg/dL after administration of 1 mg dexamethasone was the cut-off point for normal suppression. The suppression of the serum cortisol levels failed in all of the patients. RESULTS: Measured laboratory values were as follows: ACTH, median level 28 pg/ml, interquartile range (IQR) 14-59 pg/ml; fasting glucose, 100 (91-113) mg/dL; insulin, 15.7 (7.57-24.45) mU/ml; fT4, 1.17 (1.05-1.4) ng/dL; TSH, 1.70 (0.91-2.90) mIU/L; total cholesterol, 209 (170.5-250) mg/dL; LDL-c, 136 (97.7-163) mg/dL; HDL-c, 44 (37.25-50.75) mg/dL; VLDL-c, 24 (17-36) mg/dL; triglycerides, 120.5 (86-165) mg/dL. The median UFC level of the patients was 30 µg/24 h (IQR 16-103). High levels of UFC (>100 µg/24 h) were recorded in 37 patients (24%). Cushing’s syndrome was diagnosed in 14 of the 150 patients (9.33%). Etiologic reasons for Cushing’s syndrome were pituitary microadenoma (9 patients), adrenocortical adenoma (3 patients), and adrenocortical carcinoma (1 patient). CONCLUSION: A significant proportion (9.33%) of patients with simple obesity were found to have Cushing’s syndrome. These findings argue that obese patients should be routinely screened for Cushing’s syndrome.
KEYWORDS: Cushing’s syndrome. Obesity. Screening. Cortisol. Adrenocorticorticotropic hormone.
INTRODUCTION
Obesity is the most common metabolic problem in industrialized countries. In the USA, 32% of adults are classified as overweight, and 22.5% of these individuals are obese.1 Both overweight and obese subjects are at an increased risk for cardiovascular diseases,2 some types of cancer,3 diabetes4, and even premature death.5 Obesity is often accompanied by other chronic disorders including
hypertension, osteoarthritis, bile stones, and dyslipidemia.6-12 In addition to these physical disorders, obesity is commonly associated with psychological and psycho-social problems.10
Obesity can coexist with diverse physical disorders, and physicians should first focus on the differential diagnosis of possible underlying disorders before initiating any management procedure. Obesity is a prominent feature of endocrine diseases including hypothyroidism, insulin-excess syndromes, polycystic ovary syndrome (PCOS), hypogonadism, hypothalamic disease/injury, growth hormone deficiency, leptin deficiency or leptin receptor defects, pseudohypoparathyroidism, and Cushing’s syndrome (CS).11,12
Diagnosis of CS is primarily based on the signs and
9
CL
INIC
S 20
10;6
5(1)
:9-1
3
CLI
NIC
AL
SC
IEN
CE
Div
isio
n of
End
ocri
nolo
gy a
nd M
etab
olis
m, D
epar
tmen
t of I
nter
nal M
edic
ine,
C
erra
hpas
a M
edic
al F
acul
ty -
Siva
s, T
urke
y.E
mai
l: k
adio
glup
@ya
hoo.
com
Tel:
90
216
4623
114
Rec
eive
d fo
r pu
blic
atio
n on
Sep
tem
ber
11, 2
009
Acc
epte
d fo
r pu
blic
atio
n on
Oct
ober
08,
200
9
SC
RE
EN
ING
FO
R C
US
HIN
G’S
SY
ND
RO
ME
IN O
BE
SE
PA
TIE
NTS
Oza
y T
irya
kiog
lu, S
erda
l Ugu
rlu,
Ser
ap Y
alin
, Sib
el Y
irm
ibes
cik,
Erk
an C
agla
r, D
emet
Ozg
il Y
etki
n, P
inar
Kad
iogl
u
doi:
10.
1590
/S18
07-5
9322
0100
0010
0003
Tiry
akio
glu
O, U
gurl
u S,
Yal
in S
, Yir
mib
esci
k S,
Cag
lar
E, Y
etki
n D
O e
t al.
Scre
enin
g fo
r C
ushi
ng’s
Syn
drom
e in
obe
se
patie
nts.
Clin
ics.
201
0;65
(1):
9-13
.
OB
JEC
TIV
ES:
The
aim
of
this
stu
dy w
as t
o ex
amin
e th
e fr
eque
ncy
of C
ushi
ng’s
syn
drom
e (C
S) i
n ob
ese
patie
nts
devo
id o
f sp
ecifi
c cl
inic
al s
ympt
oms
of C
ushi
ng’s
syn
drom
e.
ME
TH
OD
S: A
tota
l of
150
obes
e pa
tient
s (1
29 f
emal
e, 2
1 m
ale;
mea
n ag
e 44
.41
± 13
.34
yr; m
ean
BM
I 35
.76
± 7.
13)
wer
e in
-cl
uded
in th
e st
udy.
As
a fir
st s
cree
ning
ste
p, w
e m
easu
red
24-h
uri
nary
fre
e co
rtis
ol (
UFC
). A
n ov
erni
ght 1
-mg
dexa
met
haso
ne
supp
ress
ion
test
was
als
o pe
rfor
med
on
all p
atie
nts.
Uri
nary
free
cor
tisol
leve
ls a
bove
100
µg/
24 h
wer
e co
nsid
ered
to b
e ab
norm
al.
Supp
ress
ion
of se
rum
cor
tisol
<1.
8 µg
/dL
aft
er a
dmin
istr
atio
n of
1 m
g de
xam
etha
sone
was
the
cut-
off p
oint
for n
orm
al su
ppre
ssio
n.
The
sup
pres
sion
of t
he s
erum
cor
tisol
leve
ls fa
iled
in a
ll of
the
patie
nts.
R
ESU
LTS:
Mea
sure
d la
bora
tory
val
ues
wer
e as
fol
low
s: A
CT
H, m
edia
n le
vel 2
8 pg
/ml,
inte
rqua
rtile
ran
ge (
IQR
) 14
-59
pg/m
l; fa
stin
g gl
ucos
e, 1
00 (9
1-11
3) m
g/dL
; ins
ulin
, 15.
7 (7
.57-
24.4
5) m
U/m
l; fT
4, 1.
17 (1
.05-
1.4)
ng/
dL; T
SH, 1
.70
(0.9
1-2.
90) m
IU/L
; to
tal c
hole
ster
ol, 2
09 (
170.
5-25
0) m
g/dL
; LD
L-c
, 136
(97
.7-1
63)
mg/
dL; H
DL
-c, 4
4 (3
7.25
-50.
75)
mg/
dL; V
LD
L-c
, 24
(17-
36)
mg/
dL; t
rigl
ycer
ides
, 120
.5 (
86-1
65)
mg/
dL. T
he m
edia
n U
FC le
vel o
f th
e pa
tient
s w
as 3
0 µg
/24
h (I
QR
16-
103)
. Hig
h le
vels
of
UFC
(>1
00 µ
g/24
h)
wer
e re
cord
ed in
37
patie
nts
(24%
). C
ushi
ng’s
syn
drom
e w
as d
iagn
osed
in 1
4 of
the
150
patie
nts
(9.3
3%).
Etio
logi
c re
ason
s fo
r C
ushi
ng’s
syn
drom
e w
ere
pitu
itary
mic
road
enom
a (9
pat
ient
s),
adre
noco
rtic
al a
deno
ma
(3 p
atie
nts)
, an
d ad
reno
cort
ical
car
cino
ma
(1 p
atie
nt).
CO
NC
LU
SIO
N: A
sig
nific
ant p
ropo
rtio
n (9
.33%
) of p
atie
nts
with
sim
ple
obes
ity w
ere
foun
d to
hav
e C
ushi
ng’s
syn
drom
e. T
hese
fin
ding
s ar
gue
that
obe
se p
atie
nts
shou
ld b
e ro
utin
ely
scre
ened
for C
ushi
ng’s
syn
drom
e.
KE
YW
OR
DS:
Cus
hing
’s s
yndr
ome.
Obe
sity
. Scr
eeni
ng. C
ortis
ol. A
dren
ocor
ticor
ticot
ropi
c ho
rmon
e.
INT
RO
DU
CT
ION
Obe
sity
is
the
mos
t co
mm
on m
etab
olic
pro
blem
in
indu
stri
aliz
ed c
ount
ries
. In
the
USA
, 32
% o
f ad
ults
are
cl
assi
fied
as o
verw
eigh
t, an
d 22
.5%
of
thes
e in
divi
dual
s ar
e ob
ese.
1 B
oth
over
wei
ght
and
obes
e su
bjec
ts a
re a
t an
in
crea
sed
risk
for
car
diov
ascu
lar
dise
ases
,2 so
me
type
s of
ca
ncer
,3 di
abet
es4 ,
and
even
pre
mat
ure
deat
h.5
Obe
sity
is
ofte
n ac
com
pani
ed b
y ot
her
chro
nic
diso
rder
s in
clud
ing
hype
rten
sion
, ost
eoar
thri
tis, b
ile s
tone
s, a
nd d
yslip
idem
ia.6-
12
In a
dditi
on to
thes
e ph
ysic
al d
isor
ders
, obe
sity
is c
omm
only
as
soci
ated
with
psy
chol
ogic
al a
nd p
sych
o-so
cial
pro
blem
s.10
Obe
sity
can
coe
xist
wit
h di
vers
e ph
ysic
al d
isor
ders
, an
d ph
ysic
ians
sho
uld
firs
t fo
cus
on t
he d
iffe
rent
ial
diag
nosi
s of
pos
sibl
e un
derl
ying
dis
orde
rs b
efor
e in
itiat
ing
any
man
agem
ent
proc
edur
e. O
besi
ty i
s a
prom
inen
t fe
atur
e of
end
ocri
ne d
isea
ses
incl
udin
g hy
poth
yroi
dism
, in
suli
n-ex
cess
syn
drom
es,
poly
cyst
ic o
vary
syn
drom
e (P
CO
S),
hyp
ogon
adis
m,
hypo
thal
amic
dis
ease
/inj
ury,
gr
owth
hor
mon
e de
fici
ency
, le
ptin
def
icie
ncy
or l
epti
n re
cept
or d
efec
ts, p
seud
ohyp
opar
athy
roid
ism
, and
Cus
hing
’s
synd
rom
e (C
S).11
,12
Dia
gnos
is o
f C
S is
pri
mar
ily b
ased
on
the
sign
s an
d
11
CLINICS 2010;65(1):9-13 Screening Cushing’s Syndrome in Obesity Tiryakioglu O et al.
Table 2 - Laboratory findings in the study patients
Simple obesity
Cushing’s syndrome
p
ACTH (pg/ml) 25.7 [15-51]
35 [13.5-94.5]
0.43
Cortisol (µg/dL) 10.2 [7.8-14.8]
9.4 [8.1-13.5]
0.88
Glucose (mg/dL) 99 [91-113]
100 [93.5-114]
0.91
Insulin (mU/ml) 14.7 [7.4-24.2]
18.9 [14.9-28.5]
0.07
f T4 (ng/dL) 1.2 [1.07-1.4]
1.1 [1.04-1.63]
0.56
TSH (mIU/L) 1.64 [0.9-2.8]
1.78 [1.6-4.2]
0.25
Cholesterol (mg/dL) 203 [172-249]
238.5[178.-264]
0.24
LDL-c (mg/dL) 129 [97-159]
168 [122-168]
0.15
HDL-c (mg/dL) 44 [37.5-50.5]
46 [29-66]
0.72
VLDL-c (mg/dL) 24 [17-33]
38 [16.2-50]
0.2
Triglyceride (mg/dL) 120 [86-161]
208[89.8-251]
0.15
Urine cortisol (µg/24 h) 28 [15-92.5]
74 [27-133]
0.02
DMST cortisol (µg/dL) 0.88 [0.7-1.15]
3.35 [2.5-6.5]
< 0.0001
HOMA-R(mg/dl x mU/ml)
4.02[1.91-6.59]
4.66[4.38-9.08]
0.06
Values are medians and interquartile ranges.DMST: 1-mg dexamethasone suppression test
Table 3 - Etiologies of the 14 patients diagnosed with Cush-ing’s syndrome
N %
Pituitary adenoma 9 64.28
Surrenal cortex adenoma 3 21.42
Surrenal cortex carcinoma 1 7.15
Declined further evaluation 1 7.15
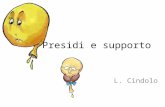
Figure 1 - Twenty-four-hour free cortisol levels in patients with Cushing’s syndrome and simple obesity
Figure 2 - The comparison of the 1-mg dexamethasone suppression test results for both groups
We compared the group of 14 obese patients with CS to the remaining group of 136 patients with simple obesity. There was no significant difference in levels of ACTH (p=0.43) or basal cortisol (p=0.88) between the CS group and the group of simple obese patients without CS. However, 24-h UFC excretion (Figure 1) and morning cortisol levels following administration of 1 mg DMS (Figure 2) were significantly more elevated in obese patients with CS than in simple obese patients without CS.
There were no significant differences between the groups
in mean values for serum lipids, glucose, BMI, systolic blood pressure, or waist-to-hip ratio. Diastolic pressure was higher in patients with CS (p=0.02). Although higher HOMA-R values were recorded in patients with CS (median, 4.66 mg/dL x mU/ml; IQR, 1.38-9.08) compared to simple obese patients (median, 4.02 mg/dL x mU/ml; IQR, 1.91-6.59), the difference between the two groups narrowly failed to achieve statistical significance (p=0.06).
DISCUSSION
Here, we report on 150 obese patients screened for CS. A diagnosis of CS was established in 14 patients (9.33%). This finding confirms the need to evaluate patients with simple obesity for CS despite the absence of other signs or symptoms of the disorder.
This conclusion is supported by several previous studies. Obesity is a frequent clinical sign of CS, and adipose tissues in CS patients typically have a central distribution. Obese patients with CS may live without any evident metabolic disorder associated with CS. However,
11
CLINICS 2010;65(1):9-13 Screening Cushing’s Syndrome in Obesity Tiryakioglu O et al.
Table 2 - Laboratory findings in the study patients
Simple obesity
Cushing’s syndrome
p
ACTH (pg/ml) 25.7 [15-51]
35 [13.5-94.5]
0.43
Cortisol (µg/dL) 10.2 [7.8-14.8]
9.4 [8.1-13.5]
0.88
Glucose (mg/dL) 99 [91-113]
100 [93.5-114]
0.91
Insulin (mU/ml) 14.7 [7.4-24.2]
18.9 [14.9-28.5]
0.07
f T4 (ng/dL) 1.2 [1.07-1.4]
1.1 [1.04-1.63]
0.56
TSH (mIU/L) 1.64 [0.9-2.8]
1.78 [1.6-4.2]
0.25
Cholesterol (mg/dL) 203 [172-249]
238.5[178.-264]
0.24
LDL-c (mg/dL) 129 [97-159]
168 [122-168]
0.15
HDL-c (mg/dL) 44 [37.5-50.5]
46 [29-66]
0.72
VLDL-c (mg/dL) 24 [17-33]
38 [16.2-50]
0.2
Triglyceride (mg/dL) 120 [86-161]
208[89.8-251]
0.15
Urine cortisol (µg/24 h) 28 [15-92.5]
74 [27-133]
0.02
DMST cortisol (µg/dL) 0.88 [0.7-1.15]
3.35 [2.5-6.5]
< 0.0001
HOMA-R(mg/dl x mU/ml)
4.02[1.91-6.59]
4.66[4.38-9.08]
0.06
Values are medians and interquartile ranges.DMST: 1-mg dexamethasone suppression test
Table 3 - Etiologies of the 14 patients diagnosed with Cush-ing’s syndrome
N %
Pituitary adenoma 9 64.28
Surrenal cortex adenoma 3 21.42
Surrenal cortex carcinoma 1 7.15
Declined further evaluation 1 7.15
Figure 1 - Twenty-four-hour free cortisol levels in patients with Cushing’s syndrome and simple obesity
Figure 2 - The comparison of the 1-mg dexamethasone suppression test results for both groups
We compared the group of 14 obese patients with CS to the remaining group of 136 patients with simple obesity. There was no significant difference in levels of ACTH (p=0.43) or basal cortisol (p=0.88) between the CS group and the group of simple obese patients without CS. However, 24-h UFC excretion (Figure 1) and morning cortisol levels following administration of 1 mg DMS (Figure 2) were significantly more elevated in obese patients with CS than in simple obese patients without CS.
There were no significant differences between the groups
in mean values for serum lipids, glucose, BMI, systolic blood pressure, or waist-to-hip ratio. Diastolic pressure was higher in patients with CS (p=0.02). Although higher HOMA-R values were recorded in patients with CS (median, 4.66 mg/dL x mU/ml; IQR, 1.38-9.08) compared to simple obese patients (median, 4.02 mg/dL x mU/ml; IQR, 1.91-6.59), the difference between the two groups narrowly failed to achieve statistical significance (p=0.06).
DISCUSSION
Here, we report on 150 obese patients screened for CS. A diagnosis of CS was established in 14 patients (9.33%). This finding confirms the need to evaluate patients with simple obesity for CS despite the absence of other signs or symptoms of the disorder.
This conclusion is supported by several previous studies. Obesity is a frequent clinical sign of CS, and adipose tissues in CS patients typically have a central distribution. Obese patients with CS may live without any evident metabolic disorder associated with CS. However,
11
CLINICS 2010;65(1):9-13 Screening Cushing’s Syndrome in Obesity Tiryakioglu O et al.
Table 2 - Laboratory findings in the study patients
Simple obesity
Cushing’s syndrome
p
ACTH (pg/ml) 25.7 [15-51]
35 [13.5-94.5]
0.43
Cortisol (µg/dL) 10.2 [7.8-14.8]
9.4 [8.1-13.5]
0.88
Glucose (mg/dL) 99 [91-113]
100 [93.5-114]
0.91
Insulin (mU/ml) 14.7 [7.4-24.2]
18.9 [14.9-28.5]
0.07
f T4 (ng/dL) 1.2 [1.07-1.4]
1.1 [1.04-1.63]
0.56
TSH (mIU/L) 1.64 [0.9-2.8]
1.78 [1.6-4.2]
0.25
Cholesterol (mg/dL) 203 [172-249]
238.5[178.-264]
0.24
LDL-c (mg/dL) 129 [97-159]
168 [122-168]
0.15
HDL-c (mg/dL) 44 [37.5-50.5]
46 [29-66]
0.72
VLDL-c (mg/dL) 24 [17-33]
38 [16.2-50]
0.2
Triglyceride (mg/dL) 120 [86-161]
208[89.8-251]
0.15
Urine cortisol (µg/24 h) 28 [15-92.5]
74 [27-133]
0.02
DMST cortisol (µg/dL) 0.88 [0.7-1.15]
3.35 [2.5-6.5]
< 0.0001
HOMA-R(mg/dl x mU/ml)
4.02[1.91-6.59]
4.66[4.38-9.08]
0.06
Values are medians and interquartile ranges.DMST: 1-mg dexamethasone suppression test
Table 3 - Etiologies of the 14 patients diagnosed with Cush-ing’s syndrome
N %
Pituitary adenoma 9 64.28
Surrenal cortex adenoma 3 21.42
Surrenal cortex carcinoma 1 7.15
Declined further evaluation 1 7.15
Figure 1 - Twenty-four-hour free cortisol levels in patients with Cushing’s syndrome and simple obesity
Figure 2 - The comparison of the 1-mg dexamethasone suppression test results for both groups
We compared the group of 14 obese patients with CS to the remaining group of 136 patients with simple obesity. There was no significant difference in levels of ACTH (p=0.43) or basal cortisol (p=0.88) between the CS group and the group of simple obese patients without CS. However, 24-h UFC excretion (Figure 1) and morning cortisol levels following administration of 1 mg DMS (Figure 2) were significantly more elevated in obese patients with CS than in simple obese patients without CS.
There were no significant differences between the groups
in mean values for serum lipids, glucose, BMI, systolic blood pressure, or waist-to-hip ratio. Diastolic pressure was higher in patients with CS (p=0.02). Although higher HOMA-R values were recorded in patients with CS (median, 4.66 mg/dL x mU/ml; IQR, 1.38-9.08) compared to simple obese patients (median, 4.02 mg/dL x mU/ml; IQR, 1.91-6.59), the difference between the two groups narrowly failed to achieve statistical significance (p=0.06).
DISCUSSION
Here, we report on 150 obese patients screened for CS. A diagnosis of CS was established in 14 patients (9.33%). This finding confirms the need to evaluate patients with simple obesity for CS despite the absence of other signs or symptoms of the disorder.
This conclusion is supported by several previous studies. Obesity is a frequent clinical sign of CS, and adipose tissues in CS patients typically have a central distribution. Obese patients with CS may live without any evident metabolic disorder associated with CS. However,
11
CLINICS 2010;65(1):9-13 Screening Cushing’s Syndrome in Obesity Tiryakioglu O et al.
Table 2 - Laboratory findings in the study patients
Simple obesity
Cushing’s syndrome
p
ACTH (pg/ml) 25.7 [15-51]
35 [13.5-94.5]
0.43
Cortisol (µg/dL) 10.2 [7.8-14.8]
9.4 [8.1-13.5]
0.88
Glucose (mg/dL) 99 [91-113]
100 [93.5-114]
0.91
Insulin (mU/ml) 14.7 [7.4-24.2]
18.9 [14.9-28.5]
0.07
f T4 (ng/dL) 1.2 [1.07-1.4]
1.1 [1.04-1.63]
0.56
TSH (mIU/L) 1.64 [0.9-2.8]
1.78 [1.6-4.2]
0.25
Cholesterol (mg/dL) 203 [172-249]
238.5[178.-264]
0.24
LDL-c (mg/dL) 129 [97-159]
168 [122-168]
0.15
HDL-c (mg/dL) 44 [37.5-50.5]
46 [29-66]
0.72
VLDL-c (mg/dL) 24 [17-33]
38 [16.2-50]
0.2
Triglyceride (mg/dL) 120 [86-161]
208[89.8-251]
0.15
Urine cortisol (µg/24 h) 28 [15-92.5]
74 [27-133]
0.02
DMST cortisol (µg/dL) 0.88 [0.7-1.15]
3.35 [2.5-6.5]
< 0.0001
HOMA-R(mg/dl x mU/ml)
4.02[1.91-6.59]
4.66[4.38-9.08]
0.06
Values are medians and interquartile ranges.DMST: 1-mg dexamethasone suppression test
Table 3 - Etiologies of the 14 patients diagnosed with Cush-ing’s syndrome
N %
Pituitary adenoma 9 64.28
Surrenal cortex adenoma 3 21.42
Surrenal cortex carcinoma 1 7.15
Declined further evaluation 1 7.15
Figure 1 - Twenty-four-hour free cortisol levels in patients with Cushing’s syndrome and simple obesity
Figure 2 - The comparison of the 1-mg dexamethasone suppression test results for both groups
We compared the group of 14 obese patients with CS to the remaining group of 136 patients with simple obesity. There was no significant difference in levels of ACTH (p=0.43) or basal cortisol (p=0.88) between the CS group and the group of simple obese patients without CS. However, 24-h UFC excretion (Figure 1) and morning cortisol levels following administration of 1 mg DMS (Figure 2) were significantly more elevated in obese patients with CS than in simple obese patients without CS.
There were no significant differences between the groups
in mean values for serum lipids, glucose, BMI, systolic blood pressure, or waist-to-hip ratio. Diastolic pressure was higher in patients with CS (p=0.02). Although higher HOMA-R values were recorded in patients with CS (median, 4.66 mg/dL x mU/ml; IQR, 1.38-9.08) compared to simple obese patients (median, 4.02 mg/dL x mU/ml; IQR, 1.91-6.59), the difference between the two groups narrowly failed to achieve statistical significance (p=0.06).
DISCUSSION
Here, we report on 150 obese patients screened for CS. A diagnosis of CS was established in 14 patients (9.33%). This finding confirms the need to evaluate patients with simple obesity for CS despite the absence of other signs or symptoms of the disorder.
This conclusion is supported by several previous studies. Obesity is a frequent clinical sign of CS, and adipose tissues in CS patients typically have a central distribution. Obese patients with CS may live without any evident metabolic disorder associated with CS. However,
9
CLINICS 2010;65(1):9-13
CLINICAL SCIENCE
Division of Endocrinology and Metabolism, Department of Internal Medicine, Cerrahpasa Medical Faculty - Sivas, Turkey.Email: [email protected]: 90 216 4623114Received for publication on September 11, 2009 Accepted for publication on October 08, 2009
SCREENING FOR CUSHING’S SYNDROME IN OBESE PATIENTS
Ozay Tiryakioglu, Serdal Ugurlu, Serap Yalin, Sibel Yirmibescik, Erkan Caglar, Demet Ozgil Yetkin, Pinar Kadioglu
doi: 10.1590/S1807-59322010000100003
Tiryakioglu O, Ugurlu S, Yalin S, Yirmibescik S, Caglar E, Yetkin DO et al. Screening for Cushing’s Syndrome in obese patients. Clinics. 2010;65(1):9-13.
OBJECTIVES: The aim of this study was to examine the frequency of Cushing’s syndrome (CS) in obese patients devoid of specific clinical symptoms of Cushing’s syndrome. METHODS: A total of 150 obese patients (129 female, 21 male; mean age 44.41 ± 13.34 yr; mean BMI 35.76 ± 7.13) were in-cluded in the study. As a first screening step, we measured 24-h urinary free cortisol (UFC). An overnight 1-mg dexamethasone suppression test was also performed on all patients. Urinary free cortisol levels above 100 µg/24 h were considered to be abnormal. Suppression of serum cortisol <1.8 µg/dL after administration of 1 mg dexamethasone was the cut-off point for normal suppression. The suppression of the serum cortisol levels failed in all of the patients. RESULTS: Measured laboratory values were as follows: ACTH, median level 28 pg/ml, interquartile range (IQR) 14-59 pg/ml; fasting glucose, 100 (91-113) mg/dL; insulin, 15.7 (7.57-24.45) mU/ml; fT4, 1.17 (1.05-1.4) ng/dL; TSH, 1.70 (0.91-2.90) mIU/L; total cholesterol, 209 (170.5-250) mg/dL; LDL-c, 136 (97.7-163) mg/dL; HDL-c, 44 (37.25-50.75) mg/dL; VLDL-c, 24 (17-36) mg/dL; triglycerides, 120.5 (86-165) mg/dL. The median UFC level of the patients was 30 µg/24 h (IQR 16-103). High levels of UFC (>100 µg/24 h) were recorded in 37 patients (24%). Cushing’s syndrome was diagnosed in 14 of the 150 patients (9.33%). Etiologic reasons for Cushing’s syndrome were pituitary microadenoma (9 patients), adrenocortical adenoma (3 patients), and adrenocortical carcinoma (1 patient). CONCLUSION: A significant proportion (9.33%) of patients with simple obesity were found to have Cushing’s syndrome. These findings argue that obese patients should be routinely screened for Cushing’s syndrome.
KEYWORDS: Cushing’s syndrome. Obesity. Screening. Cortisol. Adrenocorticorticotropic hormone.
INTRODUCTION
Obesity is the most common metabolic problem in industrialized countries. In the USA, 32% of adults are classified as overweight, and 22.5% of these individuals are obese.1 Both overweight and obese subjects are at an increased risk for cardiovascular diseases,2 some types of cancer,3 diabetes4, and even premature death.5 Obesity is often accompanied by other chronic disorders including
hypertension, osteoarthritis, bile stones, and dyslipidemia.6-12 In addition to these physical disorders, obesity is commonly associated with psychological and psycho-social problems.10
Obesity can coexist with diverse physical disorders, and physicians should first focus on the differential diagnosis of possible underlying disorders before initiating any management procedure. Obesity is a prominent feature of endocrine diseases including hypothyroidism, insulin-excess syndromes, polycystic ovary syndrome (PCOS), hypogonadism, hypothalamic disease/injury, growth hormone deficiency, leptin deficiency or leptin receptor defects, pseudohypoparathyroidism, and Cushing’s syndrome (CS).11,12
Diagnosis of CS is primarily based on the signs and
DSMZ 1 mg CLU
10
CLINICS 2010;65(1):9-13Screening Cushing’s Syndrome in Obesity Tiryakioglu O et al.
symptoms of the disorder. Nevertheless, a significant number of CS patients present only with simple obesity13-14 or with type 2 diabetes mellitus and poor glycemic control.15-17 Metabolic syndrome may also indicate the presence of CS. Patients without specific clinical features of CS have been referred to as sub-clinical Cushing’s syndrome (SCS)15 patients, and the diagnosis of SCS affords a considerable challenge to the physician.
We accordingly set out to determine the frequency of CS in patients presenting with simple obesity in the absence of other specific signs or symptoms indicative of CS.
PATIENTS AND METHODS
This study included 150 consecutive simple obese patients (129 female, 21 male, mean age: 44.41 ± 13.34 yr, body mass index (BMI) > 25 kg/m2) who were followed and treated at the Endocrinology Metabolism outpatient clinic at Cerrahpasa Medical Faculty between June 2003 and June 2004. Written informed consent was obtained from all patients before commencement of the study. Review of patient medical history was used to exclude subjects in which the dexamethasone suppression test could be biased either by medication (including exogenous glucocorticoid intake) or by other factors known to influence the test (including drug use, alcoholism, obvious depression, or pregnancy). None of the patients had nephropathy (creatinine clearance <30 ml/min), acute illness, or sleep disorders.
All patients in our study had simple obesity; none of them had diabetes mellitus. Since the patients had simple obesity, careful examinations did not reveal hirsutism, buffalo hump, easy bruising, or any other manifestations suggestive of CS suggestive manifestations.
Clinical characteristics recorded included BMI and anthropometric measurements. Morning blood samples following fasting (12 h) were drawn from an antecubital vein for determination of the concentrations of adrenocorticorticotropic hormone (ACTH) (N: 0-46 pg/ml), cortisol (N: 5-28 µg/dL), glucose, insulin (N: 0-20 µIU/L), serum lipids (total cholesterol, LDL, HDL, VLDL-cholesterol, and triglyceride), free thyroxin (fT4) (N: 0.93-1.77 ng/dL), and thyrotropin (TSH) (N: 0.15-3.7 IU/ml). Urine (24 h) was collected from each subject in order to perform urinary free cortisol (UFC) measurements. Patients whose 24-h UFC excretion exceeded 100µg/dL were defined as abnormal. All patients subsequently underwent a 1-mg overnight dexamethasone suppression test (DMS). Suppression of serum cortisol to <1.8 µg/dL after dexamethasone administration was the cut-off point for normal suppression without consideration of 24-h UFC. Measurement of serum ACTH levels and an 8-mg DMS
were performed as second-step investigations in all patients who failed to achieve serum cortisol suppression <1.8 µg/dL after administration of 1 mg DMS. Complementary imaging studies, magnetic resonance imaging (MRI) of the sella, cavernous sinus sampling, and abdominal computed tomography (CT) were performed when the results of the second-step evaluations were consistent with ACTH-dependent or ACT-independent CS.
Insulin, cortisol, fT4, TSH, and ACTH were assessed by radioimmunoassay (RIA) using a Packard Riastar gamma counter (Perkin-Elmer, Waltham, MA, USA) and commercial assay kits. Other biochemical laboratory tests were measured with an Olympus AU 600 autoanalyser (Olympus, Tokyo, Japan). Insulin resistance was assessed using the homeostasis model assessment ratio (HOMA-R) formula (18).
Calculations were done with SPSS software (version 10; SPSS Inc, Chicago, IL, USA), and differences in the values of the variables between the groups were evaluated by the Mann-Whitney U test. The degree of the correlation between parameters was evaluated by regression analysis. A value of p<0.05 was considered to be statistically significant.
RESULTS
We analyzed a series of patients presenting with simple obesity for the presence of sub-clinical CS. The clinical characteristics and laboratory findings for these patients are summarized in Tables 1 and 2.
In 37 patients (24%), 24-h UFC excretion exceeded the cut-off point (median, 30; interquartile range (IQR), 16-103 µg/24 h). Fourteen patients had unsuppressed cortisol levels as indicated by the 1-mg dexamethasone suppression test. Complementary imaging studies were performed on these 14 CS patients, which revealed pituitary microadenoma in 9 patients, adrenal adenoma in 3 patients, and adrenal carcinoma in 1 patient. Histological diagnosis was obtained in 13 patients; one patient declined to undergo surgical intervention for definitive diagnosis (Table 3).
Table 1 - Summary of physical examination findings in the patient group
(Mean ± SD) (n=150)
BMI (kg/m2) 35.76 ± 7.13
Waist (cm) 104.07 ± 15.77
Waist-to-hip ratio 0.98 ± 0.92
Systolic blood pressure (mm/Hg) 135.13 ± 20.49
Diastolic blood pressure (mm/Hg) 87.23 ± 13.03
9
CLINICS 2010;65(1):9-13
CLINICAL SCIENCE
Division of Endocrinology and Metabolism, Department of Internal Medicine, Cerrahpasa Medical Faculty - Sivas, Turkey.Email: [email protected]: 90 216 4623114Received for publication on September 11, 2009 Accepted for publication on October 08, 2009
SCREENING FOR CUSHING’S SYNDROME IN OBESE PATIENTS
Ozay Tiryakioglu, Serdal Ugurlu, Serap Yalin, Sibel Yirmibescik, Erkan Caglar, Demet Ozgil Yetkin, Pinar Kadioglu
doi: 10.1590/S1807-59322010000100003
Tiryakioglu O, Ugurlu S, Yalin S, Yirmibescik S, Caglar E, Yetkin DO et al. Screening for Cushing’s Syndrome in obese patients. Clinics. 2010;65(1):9-13.
OBJECTIVES: The aim of this study was to examine the frequency of Cushing’s syndrome (CS) in obese patients devoid of specific clinical symptoms of Cushing’s syndrome. METHODS: A total of 150 obese patients (129 female, 21 male; mean age 44.41 ± 13.34 yr; mean BMI 35.76 ± 7.13) were in-cluded in the study. As a first screening step, we measured 24-h urinary free cortisol (UFC). An overnight 1-mg dexamethasone suppression test was also performed on all patients. Urinary free cortisol levels above 100 µg/24 h were considered to be abnormal. Suppression of serum cortisol <1.8 µg/dL after administration of 1 mg dexamethasone was the cut-off point for normal suppression. The suppression of the serum cortisol levels failed in all of the patients. RESULTS: Measured laboratory values were as follows: ACTH, median level 28 pg/ml, interquartile range (IQR) 14-59 pg/ml; fasting glucose, 100 (91-113) mg/dL; insulin, 15.7 (7.57-24.45) mU/ml; fT4, 1.17 (1.05-1.4) ng/dL; TSH, 1.70 (0.91-2.90) mIU/L; total cholesterol, 209 (170.5-250) mg/dL; LDL-c, 136 (97.7-163) mg/dL; HDL-c, 44 (37.25-50.75) mg/dL; VLDL-c, 24 (17-36) mg/dL; triglycerides, 120.5 (86-165) mg/dL. The median UFC level of the patients was 30 µg/24 h (IQR 16-103). High levels of UFC (>100 µg/24 h) were recorded in 37 patients (24%). Cushing’s syndrome was diagnosed in 14 of the 150 patients (9.33%). Etiologic reasons for Cushing’s syndrome were pituitary microadenoma (9 patients), adrenocortical adenoma (3 patients), and adrenocortical carcinoma (1 patient). CONCLUSION: A significant proportion (9.33%) of patients with simple obesity were found to have Cushing’s syndrome. These findings argue that obese patients should be routinely screened for Cushing’s syndrome.
KEYWORDS: Cushing’s syndrome. Obesity. Screening. Cortisol. Adrenocorticorticotropic hormone.
INTRODUCTION
Obesity is the most common metabolic problem in industrialized countries. In the USA, 32% of adults are classified as overweight, and 22.5% of these individuals are obese.1 Both overweight and obese subjects are at an increased risk for cardiovascular diseases,2 some types of cancer,3 diabetes4, and even premature death.5 Obesity is often accompanied by other chronic disorders including
hypertension, osteoarthritis, bile stones, and dyslipidemia.6-12 In addition to these physical disorders, obesity is commonly associated with psychological and psycho-social problems.10
Obesity can coexist with diverse physical disorders, and physicians should first focus on the differential diagnosis of possible underlying disorders before initiating any management procedure. Obesity is a prominent feature of endocrine diseases including hypothyroidism, insulin-excess syndromes, polycystic ovary syndrome (PCOS), hypogonadism, hypothalamic disease/injury, growth hormone deficiency, leptin deficiency or leptin receptor defects, pseudohypoparathyroidism, and Cushing’s syndrome (CS).11,12
Diagnosis of CS is primarily based on the signs and
150 sogge)

Hindawi Publishing CorporationISRN EndocrinologyVolume 2013, Article ID 321063, 4 pageshttp://dx.doi.org/10.1155/2013/321063
Clinical StudyRoutine Screening for Cushing’s Syndrome Is NotRequired in Patients Presenting with Obesity
Serap Baydur Sahin,1 Hacer Sezgin,2 Teslime Ayaz,3 Emine Uslu Gur,3 and Kadir Ilkkilic3
1 Department of Endocrinology and Metabolism Disease, Recep Tayyip Erdogan University Medical School, 53020 Rize, Turkey2Department of Family Medicine, Recep Tayyip Erdogan University Medical School, Rize, Turkey3Department of Internal Medicine, Recep Tayyip Erdogan University Medical School, Rize, Turkey
Correspondence should be addressed to Hacer Sezgin; [email protected]
Received 7May 2013; Accepted 2 June 2013
Academic Editors: C.-H. Anderwald, C. Bizzarri, C. N. Mowa, and G. F. Wagner
Copyright © 2013 Serap Baydur Sahin et al. This is an open access article distributed under the Creative Commons AttributionLicense, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properlycited.
Background. Cushing’s syndrome (CS) is a relatively unusual condition that resembles many of the phenotypic features of obesity.Our aimwas to evaluate the frequency of CS in obese patients.Materials andMethods.This study included 354 consecutive patients(87.9% female, age 37.8 ± 13.4 years) who presented with simple obesity. All the patients were evaluated for the clinical signs of CS.Lipid parameters, fasting glucose (FPG) and insulin, 75 gr oral glucose tolerance test, basal cortisol and ACTHweremeasured. 1mgovernight DST was performed. Results.The mean weight of the patients was 102.4 ± 20.1 kg and BMI 40 ± 7.35 kg/m2. 34.5% of thepatients were hypertensive. 36.2% of the patients had central obesity, 72% dorsocervical fat accumulation, 28.8% abdominal striaeand 23.2% acne. 49.4% of the women had hirsutism. 46.5% had prediabetes and 12.0% had type 2 diabetes, 72.6% had dyslipidemia.The mean cortisol and ACTH levels were as follows: 9.28 ± 3.53 !g/dL and 17.02 ± 10.43 pg/mL. Seven patients failed to suppressplasma cortisol to less than 1.8 !g/dL. Biochemical confirmation testswere performed in these patients and 2of themwere diagnosedglucocorticoid-secreting adrenal adenoma. Conclusions. Routine screening for CS in obese patients is not required.
1. Introduction
Cushing’s syndrome (CS) is considered a contributing factorto the development of obesity. On the other hand, obesityitself might share the symptoms and signs of CS such as hir-sutism, menstrual abnormalities, acne, dorsocervical fat pad(buffalo hump), supraclavicular fullness, glucose intolerance,and hypertension. Physicians may be called upon to excludeCS in obese patients, who are increasingly present in the gen-eral population. Early recognition of CS can reduce the mor-bidity and mortality [1].
The diagnosis of CS is often a challenge for clinicians dueto the variable pattern and the nonspecificity of clinical man-ifestations.The diagnosis can be difficult particularly in statesof mild or cyclical or periodical hypercortisolism [2–4]. Thesuspicion of CS arises in the presence of concomitant recentweight gain, impaired glucose tolerance, and high blood pres-sure [3]. Several studies reported a 1–5% prevalence of unsus-pected CS in patients with poorly controlled type 2 diabetes
and/or hypertension [5–8]. However, there are only few stud-ies on the prevalence of CS in obese patients [9–13].We there-fore aimed to evaluate the frequency of CS in patients whopresent with obesity.
The 1mg overnight dexamethasone-suppression test(DST) is the most frequently used screening tool for CS [14].Because it is easy to perform and has low cost it is used as afirst-line screening test in outpatient screening. However, thelack of suppression after 1mg overnight DST may be seen in2–8%of the obese individuals [10, 11, 14]. Our second aimwasto reevaluate the validity of the 1mg overnight dexametha-sone suppression test as a CS screening test in obese patients.
2. Patients and Methods
This study included 354 consecutive patients with a bodymass index (BMI) >30 kg/m2 who were admitted to ourendocrine outpatient because of simple obesity betweenNovember 2012 and May 2013. Patients were excluded from
Hindawi Publishing CorporationISRN EndocrinologyVolume 2013, Article ID 321063, 4 pageshttp://dx.doi.org/10.1155/2013/321063
Clinical StudyRoutine Screening for Cushing’s Syndrome Is NotRequired in Patients Presenting with Obesity
Serap Baydur Sahin,1 Hacer Sezgin,2 Teslime Ayaz,3 Emine Uslu Gur,3 and Kadir Ilkkilic3
1 Department of Endocrinology and Metabolism Disease, Recep Tayyip Erdogan University Medical School, 53020 Rize, Turkey2Department of Family Medicine, Recep Tayyip Erdogan University Medical School, Rize, Turkey3Department of Internal Medicine, Recep Tayyip Erdogan University Medical School, Rize, Turkey
Correspondence should be addressed to Hacer Sezgin; [email protected]
Received 7May 2013; Accepted 2 June 2013
Academic Editors: C.-H. Anderwald, C. Bizzarri, C. N. Mowa, and G. F. Wagner
Copyright © 2013 Serap Baydur Sahin et al. This is an open access article distributed under the Creative Commons AttributionLicense, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properlycited.
Background. Cushing’s syndrome (CS) is a relatively unusual condition that resembles many of the phenotypic features of obesity.Our aimwas to evaluate the frequency of CS in obese patients.Materials andMethods.This study included 354 consecutive patients(87.9% female, age 37.8 ± 13.4 years) who presented with simple obesity. All the patients were evaluated for the clinical signs of CS.Lipid parameters, fasting glucose (FPG) and insulin, 75 gr oral glucose tolerance test, basal cortisol and ACTHweremeasured. 1mgovernight DST was performed. Results.The mean weight of the patients was 102.4 ± 20.1 kg and BMI 40 ± 7.35 kg/m2. 34.5% of thepatients were hypertensive. 36.2% of the patients had central obesity, 72% dorsocervical fat accumulation, 28.8% abdominal striaeand 23.2% acne. 49.4% of the women had hirsutism. 46.5% had prediabetes and 12.0% had type 2 diabetes, 72.6% had dyslipidemia.The mean cortisol and ACTH levels were as follows: 9.28 ± 3.53 !g/dL and 17.02 ± 10.43 pg/mL. Seven patients failed to suppressplasma cortisol to less than 1.8 !g/dL. Biochemical confirmation testswere performed in these patients and 2of themwere diagnosedglucocorticoid-secreting adrenal adenoma. Conclusions. Routine screening for CS in obese patients is not required.
1. Introduction
Cushing’s syndrome (CS) is considered a contributing factorto the development of obesity. On the other hand, obesityitself might share the symptoms and signs of CS such as hir-sutism, menstrual abnormalities, acne, dorsocervical fat pad(buffalo hump), supraclavicular fullness, glucose intolerance,and hypertension. Physicians may be called upon to excludeCS in obese patients, who are increasingly present in the gen-eral population. Early recognition of CS can reduce the mor-bidity and mortality [1].
The diagnosis of CS is often a challenge for clinicians dueto the variable pattern and the nonspecificity of clinical man-ifestations.The diagnosis can be difficult particularly in statesof mild or cyclical or periodical hypercortisolism [2–4]. Thesuspicion of CS arises in the presence of concomitant recentweight gain, impaired glucose tolerance, and high blood pres-sure [3]. Several studies reported a 1–5% prevalence of unsus-pected CS in patients with poorly controlled type 2 diabetes
and/or hypertension [5–8]. However, there are only few stud-ies on the prevalence of CS in obese patients [9–13].We there-fore aimed to evaluate the frequency of CS in patients whopresent with obesity.
The 1mg overnight dexamethasone-suppression test(DST) is the most frequently used screening tool for CS [14].Because it is easy to perform and has low cost it is used as afirst-line screening test in outpatient screening. However, thelack of suppression after 1mg overnight DST may be seen in2–8%of the obese individuals [10, 11, 14]. Our second aimwasto reevaluate the validity of the 1mg overnight dexametha-sone suppression test as a CS screening test in obese patients.
2. Patients and Methods
This study included 354 consecutive patients with a bodymass index (BMI) >30 kg/m2 who were admitted to ourendocrine outpatient because of simple obesity betweenNovember 2012 and May 2013. Patients were excluded from
N° Sogge) 354 Test DST 1 mg (> 1,8 mcg/dl) 7 (2%) Test DST 2 mg in 2 gg (> 1,8 mcg/dl) 2 (0,6%) Nei 2 sogge): -‐ UFC nella norma -‐ ACTH < 5 pg/ml -‐ “elevated midnight CorPsol”
DIAGNOSI: Adenoma Surrenalico
ISRN Endocrinology 3
24-hour urinary free cortisol levels were in normal range.One of the patients was a 39-year-old woman and physicalexamination revealed central obesity (BMI = 40 kg/m2), abuffalo hump, moon facies, and supraclavicular fullness. Shehad no muscle weakness, no facial plethora, and abdominalstriae. She had menstrual irregularities and prediabetes.Computed tomography (CT) scanning of the adrenals identi-fied the cortical adenomameasuring 38mmon the right side.She underwent a right laparoscopic adrenalectomy.The otherpatient was a 76-year-old, postmenopausal woman who hadcentral obesity (BMI = 35 kg/m2), a 15-year history of type2 diabetes mellitus, and a 20-year history of hypertension.The patient was being treated with insulin (glycosylatedhemoglobin [HbA1c] was 7%), and her hypertension wasbeing controlled with an angiotensin-converting enzymeinhibitor. Computed tomography (CT) scan of the abdomendetected a low-density adrenal mass measuring 3 cm on theright side. She declined to undergo surgical intervention.
4. Discussion
Among 354 people who were obese, two patients (0.5%) werediagnosed with Cushing’s syndrome. The false positive ratefor the 1mg overnight dexamethasone-suppression test was1.4%, even when using a cut-off serum cortisol of 1.8!g/dL.
The suspicion of CS depends largely on individual clinicaljudgment and personal practice. The patients do not alwayspresent a clear Cushing phenotype. They can have only themild signs of hypercortisolism, such as facial fullness and cen-tral obesity. It may be difficult to decide whether these signsmay be attributable to an underlying occult hypercortisolismor are manifestations of the obesity. In our study, the symp-toms or signs for CS, such as facial fullness, dorsocervical fataccumulation, and hirsutism were present in a major propor-tion of the population.
Screening for Cushing’s syndrome is recommended inpatients with multiple and progressive clinical features (facialplethora, easy bruising, striae, and proximal myopathy),patients with unusual features for age (e.g., osteoporosis,hypertension, and type 2 diabetes), and patients with adrenalincidentaloma by the Endocrine Society guidelines [16].Early recognition of patients with CS, particularly those withmilder forms, is important to prevent the long-term physicalconsequences and increased mortality that may occur whenthe disease is left untreated [17]. Therefore we screened theobese patients for CS who have not a clear Cushing pheno-type. In our study population, which includesmorbidly obesepatients in major proportion, mean age of the patients wasyoung and also the prevalence of glucose intolerance and hy-pertension was high.
The reported prevalence of CS among the obese patientsvaries widely between the different studies, ranging from0.6% to 9.4% [10, 11, 13, 14].This heterogeneity may be due tothe different inclusion criteria as well as the different cut-offvalues to define cortisol suppression after the 1mgDST. Jank-ovic et al. screened 433 morbidly obese patients and foundthe prevalence of CS below 0.6% [13]. They used the 1mg-DST for screening CS, but defined the cut-off value as 3 !g/dL
differently from our study. In the other three studies, CS wasscreened in a small number of patients [10, 11, 14]. Tiryakiogluet al. demonstrated a high prevalence of CS in the obese pop-ulation despite the absence of other signs or symptoms of thedisorder (9.4%). The cutoff value for the 1mg DST was1.8 !g/dL [10].
Some studies evaluated the prevalence of occult CS inoverweight and obese patients with uncontrolled diabetesand it was found to be 0–9.4% indifferent studies [5, 15, 18, 19].In all the studies, the first screening step was performed withthe 1mgDST, but the cutoff values for the suppression of cor-tisol were different (from 1.8 to 5!g/dL).
The 1mg overnight dexamethasone suppression test isproved to be a simple, sensitive, and highly specific screeningtest for Cushing’s syndrome. Serum cortisol after overnight1mgDST above 50 nmol/L (18 ng/mL or 1.8mg/dL) is consid-ered to be suggestive of Cushing’s syndrome [16]. 24 h urinecortisol, 1mgovernightDST andmidnight cortisol, and com-bined strategies based on these tests have similar accuracy [16,20]. 2mg 48 h dexamethasone suppression test is considereda second-line test because it is not often simple to carry out inan outpatient [16].
The lack of suppression after 1mg overnight DST may beseen in the obese individuals.The ratio of false positive 1mgDST results in obese populationwas as follows in the differentstudies: 8%[11] and 2.3%[12]. In our study, this ratiowas 1.4%.Our results suggest that even in the obese population, 1mgovernight DST is a sensitive and specific screening test forCushing’s syndrome.
In conclusion, the present data do not supportwidespreadscreening of obese patients for Cushing’s syndrome. Wesuggest that examination for hypercortisolism should only beperformed in obese patients with a cushingoid appearanceand hypertension or glucose intolerance or dyslipidaemia.
References
[1] J. Etxabe and J. A. Vazquez, “Morbidity and mortality in Cush-ing’s disease: an epidemiological approach,”Clinical Endocrinol-ogy, vol. 40, no. 4, pp. 479–484, 1994.
[2] A. B. Atkinson, D. R. McCance, L. Kennedy, and B. Sheridan,“Cyclical Cushing’s syndrome first diagnosed after pituitary sur-gery: a trap for the unwary,” Clinical Endocrinology, vol. 36, no.3, pp. 297–300, 1992.
[3] G. Arnaldi, T. Mancini, B. Kola et al., “Cyclical Cushing’s syn-drome in a patientwith a bronchial neuroendocrine tumor (typ-ical carcinoid) expressing ghrelin and growth hormone secret-agogue receptors,” Journal of Clinical Endocrinology andMetab-olism, vol. 88, no. 12, pp. 5834–5840, 2003.
[4] D. F. Gunther, I. Bourdeau, L. Matyakhina et al., “Cyclical cush-ing syndrome presenting in infancy: an early form of primarypigmented nodular adrenocortical disease, or a new entity?”Journal of Clinical Endocrinology and Metabolism, vol. 89, no.7, pp. 3173–3182, 2004.
[5] B. Catargi, V. Rigalleau, A. Poussin et al., “Occult Cushing’s syn-drome in type-2 diabetes,” Journal of Clinical Endocrinology andMetabolism, vol. 88, no. 12, pp. 5808–5813, 2003.
[6] G. Reimondo, A. Pia, B. Allasino et al., “Screening of Cushing’ssyndrome in adult patients with newly diagnosed diabetes mel-litus,” Clinical Endocrinology, vol. 67, no. 2, pp. 225–229, 2007.

Screening of Cushing’s Syndrome in Outpatients withType 2 Diabetes: Results of a Prospective MulticentricStudy in Italy
Massimo Terzolo, Giuseppe Reimondo, Iacopo Chiodini, Roberto Castello,Roberta Giordano, Enrica Ciccarelli, Paolo Limone, Claudio Crivellaro,Irma Martinelli, Marcella Montini, Olga Disoteo, Bruno Ambrosi, Roberto Lanzi,Maura Arosio, Sanzio Senni, Antonio Balestrieri, Erica Solaroli, Bruno Madeo,Raffaella De Giovanni, Felice Strollo, Rodolfo Battista, Alessandro Scorsone,Vito A. Giagulli, Daniela Collura, Aldo Scillitani, Renato Cozzi,Marco Faustini-Fustini, Anna Pia, Roberta Rinaldi, Barbara Allasino, Giulia Peraga,Francesco Tassone, Piernicola Garofalo, Enrico Papini, and Giorgio Borretta*
Context: Cushing’s syndrome may remain unrecognized among patients referred for metabolicsyndrome; thus, a proactive screening has been suggested in certain patient populations withfeatures of the disorder. However, conflicting data have been reported on the prevalence ofCushing’s syndrome in patients with type 2 diabetes.
Objective: Our aim was to evaluate the prevalence of unsuspected Cushing’s syndrome amongoutpatients with type 2 diabetes.
Design and Setting: This was a cross-sectional prospective study in 24 diabetes clinics across Italy.
Patients: Between June 2006 and April 2008, 813 patients with known type 2 diabetes withoutclinically overt hypercortisolism were evaluated. Follow-up of the study was closed in September2010. Patients were not selected for characteristics conferring a higher pretest probability ofhypercortisolism. Patients underwent a first screening step with the 1-mg overnight dexametha-sone suppression test.
Results: Forty patients failed to suppress serum cortisol less than 5.0 !g/dl (138 nmol/liter) andunderwent a standard 2-d, 2-mg dexamethasone suppression test, after which six patients (0.6%of the overall series) failed to suppress cortisol less than 1.8 !g/dl (50 nmol/liter), receiving adefinitive diagnosis of Cushing’s syndrome that was adrenal dependent in five patients. Fourpatients were cured, being able to discontinue, or reduce, the glucose-lowering agents.
Conclusions: The present data do not support widespread screening of patients with type 2 dia-betes for Cushing’s syndrome; however, the disorder is less rare than previously thought whenconsidering epidemiology of type 2 diabetes. Our results support a case-finding approach in pa-tients with uncontrolled diabetes and hypertension despite appropriate treatment. (J Clin Endo-crinol Metab 97: 3467–3475, 2012)
Subtle clinical presentations of Cushing’s syndrome,characterized by a paucity of signs and symptoms
due to mild cortisol hypersecretion, are increasinglyfound in clinical practice. In parallel, the metabolicsyndrome epidemic is leading to a boost in the numberof patients with a Cushingoid phenotype, who could
be potentially candidate to be tested for hypercortiso-lism (1).
The Endocrine Society guidelines for the diagnosis ofCushing’s syndrome recommended against widespreadtesting for the condition, unless in patients with unusualfeatures for age or multiple and progressive features, par-
ISSN Print 0021-972X ISSN Online 1945-7197Printed in U.S.A.Copyright © 2012 by The Endocrine Societydoi: 10.1210/jc.2012-1323 Received February 5, 2012. Accepted June 18, 2012.First Published Online July 5, 2012
*Author affiliations are shown at the bottom of the next pageAbbreviations: BMI, Body mass index; CT, computerized tomography; DST, dexametha-sone suppression test; HbA1c, glycosylated hemoglobin; HPA, hypothalamus-pituitary-adrenal; MRI, magnetic resonance imaging.
O R I G I N A L A R T I C L E
E n d o c r i n e C a r e
J Clin Endocrinol Metab, October 2012, 97(10):3467–3475 jcem.endojournals.org 3467
The Endocrine Society. Downloaded from press.endocrine.org by [${individualUser.displayName}] on 18 March 2014. at 05:28 For personal use only. No other uses without permission. . All rights reserved.
small numbers, we cannot definitively prove thatscreening of Cushing’s syndrome results in a more fa-vorable outcome of the patients who were diagnosedwith the condition. However, it is noteworthy that allthe treated patients were able to discontinue, or reduce,medications for diabetes after remission of hypercorti-solism despite that hypercortisolism was rather mildcompared with that usually observed in patients withadrenal-dependent Cushing. Weight loss after surgerywas key to the improved patient outcome.
In conclusion, the results of the present study do notsupport the application of a wide-scale screening of Cush-ing’s syndrome in patients with type 2 diabetes, unlessmore efficient screening procedures will become available.The frequency of Cushing’s syndrome in an unselectedpatient population was low compared with the number offalse-positive results to make a routine screening strategyapplicable in practice.
Considering the epidemic of type 2 diabetes in the West-ern world, however, the present data suggest that Cushing’ssyndrome is less rare than previously thought (although notfrequent enough to warrant systematic screening). This isplausible because the available epidemiological data tookinto account only diagnoses made in hospitalized patients,thus considering only the most severe and clinically obviouscases (31–34).
Our results may influence clinical practice supporting acase-finding approach in patients selected for uncon-trolled diabetes despite appropriate treatment and resis-tant hypertension. The frequency of definitive Cushing’ssyndrome was indeed of 5.1% among patients withHbA1c greater than 9.0% despite intensive treatment andthe levels of blood pressure not at target despite threedrugs. A diagnosis of type 2 diabetes younger than 50 yrof age is another factor that should raise suspicion, recall-ing the value of features unusual for age to suspect Cushing(2) because type 2 diabetes usually occurs in older patients(35), although age at diagnosis of type 2 diabetes is shiftingamong a younger population (36). In addition, the lack offamily history of diabetes, which was absent in our pa-tients with definitive Cushing, should be considered toselect patients for screening. However, we should ac-knowledge the limit of the small number of patients withdefinitive Cushing to provide clear-cut recommendations.Moreover, we know from the literature that a concomi-tant presence of one or more features among central obe-sity, osteoporosis, or polycystic ovary syndrome furtherincreases the probability of the condition and may promptappropriate work-up (1, 2, 23).
The patients found to have occult Cushing’s syndromeshould be referred to endocrinologists with specific ex-pertise to ensure a prompt treatment of the condition that
may have a beneficial impact on health outcomes. It ispertinent to consider the fact that adrenal adenoma is theleading cause of occult Cushing’s syndrome and the factthat laparoscopic adrenalectomy has become a safe andrelatively inexpensive procedure, causing limited discom-fort to the patient (29, 30, 37), and makes the search forthe condition more attractive. Because patients with occultCushing’s syndrome have a milder clinical phenotype,physicians involved in the management of diabetes shouldraise their level of awareness for the condition. The knowl-edge and experience of the physician is key in this context;thus, the present data suggest that a specific educationalpolicy may lead to an improved care of patients with type2 diabetes.
Acknowledgments
The funding source had no role in the design and conduct of thestudy, collection, management, analysis, and interpretation ofthe data; and preparation, review, or approval of the manuscript.All of the authors had full access to all of the data in the study andtake responsibility for the integrity of the data and the accuracyof the data analysis.
Address all correspondence and requests for reprints to: M.Terzolo, M.D., Medicina Interna I, Azienda Ospedaliera Uni-versitaria San Luigi Gonzaga, Regione Gonzole, 10, 10043Orbassano, Italy. E-mail: [email protected].
This work was supported by a grant from the Piedmont Re-gion, “Progetti di Ricerca Sanitaria Finalizzata-Bando 2008.”
Disclosure Summary: None of the authors has any financialrelationship relevant to the present work.
References
1. Raff H, Findling JW 2003 A physiologic approach to diagnosis of theCushing syndrome. Ann Intern Med 138:980–991
2. Nieman LK, Biller BM, Findling JW, Newell-Price J, Savage MO,Stewart PM, Montori VM 2008 The diagnosis of Cushing’s syn-drome: an Endocrine Society clinical practice guideline. J Clin En-docrinol Metab 93:1526–1540
3. Leibowitz G, Tsur A, Chayen SD, Salameh M, Raz I, Cesari E, GrossDJ 1996 Pre-clinical Cushing’s syndrome: an unexpected frequentcause of poor glycaemic control in obese diabetic patients. Clin En-docrinol 44:717–722
4. Catargi B, Rigalleau V, Poussin A, Ronci-Chaix N, Bex V, VergnotV, Gin H, Roger P, Tabarin A 2003 Occult Cushing’s syndrome intype-2 diabetes. J Clin Endocrinol Metab 88:5808–5813
5. Chiodini I, Torlontano M, Scillitani A, Arosio M, Bacci S, Di LemboS, Epaminonda P, Augello G, Enrini R, Ambrosi B, Adda G, Tris-chitta V 2005 Association of subclinical hypercortisolism with type2 diabetes mellitus: a case-control study in hospitalized patients. EurJ Endocrinol 153:837–844
6. Boscaro M, Barzon L, Fallo F, Sonino N 2001 Cushing’s syndrome.Lancet 357:783–791
7. Chiodini I 2011 Clinical review: diagnosis and treatment of sub-clinical hypercortisolism. J Clin Endocrinol Metab 96:1223–1236
8. Bray GA 2001 An approach to the classification and evaluation of
3474 Terzolo et al. Cushing’s Syndrome and Type 2 Diabetes J Clin Endocrinol Metab, October 2012, 97(10):3467–3475
The Endocrine Society. Downloaded from press.endocrine.org by [${individualUser.displayName}] on 18 March 2014. at 05:28 For personal use only. No other uses without permission. . All rights reserved.
Materials and protocolsThe study flow chart is outlined in Fig. 1. All subjects under-
went in an outpatient setting a first screening step by using theovernight 1-mg dexamethasone suppression test (DST) (1 mgdexamethasone administered orally at 2300 h and blood sampledrawing on the following morning at 0800 h for determinationof serum cortisol concentration. Patients who failed to suppressserum cortisol less than 5.0 !g/dl (138 nmol/liter) were offereda second-step evaluation by undergoing a standard 2-d, 2-mgDST 3–6 months after baseline evaluation (0.5 mg dexametha-sone administered orally at 0600, 1200, 1800, and 2400 h andblood sample drawing on the following morning at 0800 h forcortisol determination). A cortisol concentration greaterthan 1.8 !g/dl (50 nmol/liter) was considered abnormal andprompted further evaluation to confirm diagnosis of Cushing’ssyndrome and determine its cause according to a standardizedprotocol (11). Briefly, evaluation should include three 24-h urinecollections for urinary free cortisol measurement and blooddrawing at 0800 h for the determination of plasma ACTH con-centration. An ACTH concentration should provide guidancefor radiological evaluation [pituitary magnetic resonance imag-
ing (MRI) or adrenal computerized tomography (CT)]; in doubt-ful cases, with ACTH concentration between 10 and 20 pg/ml(2.2 and 4.4 pmol/liter), the CRH stimulation test should beperformed to ascertain ACTH dependency (12). Specific treat-ment was pursued in the patients with a definitive diagnosis ofCushing’s syndrome who were followed up for at least 24months after surgery. The hormonal variables were determinedin a single reference laboratory for each participating center us-ing commercially available reagents.
Statistical analysisSample size analysis was done based on the results of previous
studies. It was calculated that approximately 381 patients shouldbe studied to provide an 80% chance (beta) of detecting a prev-alence rate of Cushing’s syndrome of 1%, taking 0.05 as the levelof significance (alpha). Rates and proportions were calculatedfor categorical data and means and SD for continuous data. Nor-mality of data was assessed by the Kolmogorov-Smirnov test. Forcontinuous variables, differences were analyzed by means of thetwo-tailed Student’s t test when data were normally distributed
FIG. 1. Flow-chart of the study.
J Clin Endocrinol Metab, October 2012, 97(10):3467–3475 jcem.endojournals.org 3469
The Endocrine Society. Downloaded from press.endocrine.org by [${individualUser.displayName}] on 18 March 2014. at 05:28 For personal use only. No other uses without permission. . All rights reserved.
0,7 %
5 %

Long-Term Follow-Up in Adrenal Incidentalomas: AnItalian Multicenter Study
Valentina Morelli, Giuseppe Reimondo, Roberta Giordano, Silvia Della Casa,Caterina Policola, Serena Palmieri, Antonio S. Salcuni, Alessia Dolci,Marco Mendola, Maura Arosio, Bruno Ambrosi, Alfredo Scillitani, Ezio Ghigo,Paolo Beck-Peccoz, Massimo Terzolo, and Iacopo Chiodini
Department of Clinical Sciences and Community Health (V.M., S.P., A.D., M.A., P.B.-P., I.C.), Universityof Milan, 20122 Milan, Italy; Unit of Endocrinology and Diabetology (V.M., S.P., P.B.-P., I.C.),Fondazione IRCCS Cà Granda-Ospedale Maggiore Policlinico, 20122 Milan, Italy; Division of InternalMedicine I (G.R., M.T.), Ospedale San Luigi, 10043 Orbassano, Italy; Department of Biological andClinical Sciences (G.R., R.G., M.T.), University of Turin, 10124 Turin, Italy; Catholic University (S.D.C.,C.P.), Unit of Endocrinology and Metabolism, 00168 Rome, Italy; Unit of Endocrinology (A.S.S., A.S.),Ospedale “Casa Sollievo della Sofferenza,” IRCCS, 71013 San Giovanni Rotondo, Foggia, Italy; Unit ofEndocrine Diseases and Diabetology (A.D., M.A.), Ospedale San Giuseppe, Gruppo Multimedica, 20123Milan, Italy; Department of Biomedical Sciences for Health (M.M., B.A.), University of Milan, Unit ofEndocrinology and Diabetology, IRCCS Policlinico San Donato, 20097 San Donato Milanese, Milan, Italy;and Division of Endocrinology, Diabetology, and Metabolism (E.G.), Department of Medical Sciences,University of Turin, 10124 Turin, Italy
Context: The long-term consequences of subclinical hypercortisolism (SH) in patients with adrenalincidentalomas (AIs) are unknown.
Setting and Patients: In this retrospective multicentric study, 206 AI patients with a !5-year fol-low-up (median, 72.3 mo; range, 60–186 mo) were enrolled.
Intervention and Main Outcome Measures: Adrenocortical function, adenoma size, metabolicchanges, and incident cardiovascular events (CVEs) were assessed. We diagnosed SH in 11.6% ofpatients in the presence of cortisol after a 1 mg-dexamethasone suppression test !5 "g/dL (138nmol/L) or at least two of the following: low ACTH, increased urinary free cortisol, and 1 mg-dexamethasone suppression test !3 "g/dL (83 nmol/L).
Results: At baseline, age and the prevalence of CVEs and type 2 diabetes mellitus were higher inpatients with SH than in patients without SH (62.2 " 11 y vs 58.5 " 10 y; 20.5 vs 6%; and 33.3 vs16.8%, respectively; P # .05). SH and type 2 diabetes mellitus were associated with prevalent CVEs(odds ratio [OR], 3.1; 95% confidence interval [CI], 1.1–9.0; and OR, 2.0; 95% CI, 1.2–3.3, respec-tively), regardless of age. At the end of the follow-up, SH was diagnosed in 15 patients who werewithout SH at baseline. An adenoma size !2.4 cm was associated with the risk of developing SH(sensitivity, 73.3%; specificity, 60.5%; P $ .014). Weight, glycemic, lipidic, and blood pressurecontrol worsened in 26, 25, 13, and 34% of patients, respectively. A new CVE occurred in 22 patients.SH was associated with the worsening of at least two metabolic parameters (OR, 3.32; 95% CI,1.6–6.9) and with incident CVEs (OR, 2.7; 95% CI, 1.0–7.1), regardless of age and follow-up.
Conclusion: SH is associated with the risk of incident CVEs. Besides the clinical follow-up, in patientswith an AI !2.4 cm, a long-term biochemical follow-up is also required because of the risk of SHdevelopment. (J Clin Endocrinol Metab 99: 827–834, 2014)
ISSN Print 0021-972X ISSN Online 1945-7197Printed in U.S.A.Copyright © 2014 by the Endocrine SocietyReceived September 18, 2013. Accepted December 18, 2013.First Published Online January 7, 2014
Abbreviations: AH, arterial hypertension; AI, adrenal incidentaloma; BMI, body mass index;CI, confidence interval; CT, computed tomography; CVE, cardiovascular event; DL, dys-lipidemia; 1 mg-DST, 1 mg-dexamethasone suppression test; HPA, hypothalamic-pituitary-adrenal; LDL, low-density lipoprotein; OB, obesity; OR, odds ratio; ROC, receiver operatingcharacteristic; SH, subclinical hypercortisolism; SN, sensitivity; SP, specificity; T2DM, type2 diabetes mellitus; UFC, urinary free cortisol; ULN, upper limit of normal.
O R I G I N A L A R T I C L E
E n d o c r i n e C a r e
doi: 10.1210/jc.2013-3527 J Clin Endocrinol Metab, March 2014, 99(3):827–834 jcem.endojournals.org 827
The Endocrine Society. Downloaded from press.endocrine.org by [Lino Furlani] on 16 March 2014. at 12:54 For personal use only. No other uses without permission. . All rights reserved.
Long-Term Follow-Up in Adrenal Incidentalomas: AnItalian Multicenter Study
Valentina Morelli, Giuseppe Reimondo, Roberta Giordano, Silvia Della Casa,Caterina Policola, Serena Palmieri, Antonio S. Salcuni, Alessia Dolci,Marco Mendola, Maura Arosio, Bruno Ambrosi, Alfredo Scillitani, Ezio Ghigo,Paolo Beck-Peccoz, Massimo Terzolo, and Iacopo Chiodini
Department of Clinical Sciences and Community Health (V.M., S.P., A.D., M.A., P.B.-P., I.C.), Universityof Milan, 20122 Milan, Italy; Unit of Endocrinology and Diabetology (V.M., S.P., P.B.-P., I.C.),Fondazione IRCCS Cà Granda-Ospedale Maggiore Policlinico, 20122 Milan, Italy; Division of InternalMedicine I (G.R., M.T.), Ospedale San Luigi, 10043 Orbassano, Italy; Department of Biological andClinical Sciences (G.R., R.G., M.T.), University of Turin, 10124 Turin, Italy; Catholic University (S.D.C.,C.P.), Unit of Endocrinology and Metabolism, 00168 Rome, Italy; Unit of Endocrinology (A.S.S., A.S.),Ospedale “Casa Sollievo della Sofferenza,” IRCCS, 71013 San Giovanni Rotondo, Foggia, Italy; Unit ofEndocrine Diseases and Diabetology (A.D., M.A.), Ospedale San Giuseppe, Gruppo Multimedica, 20123Milan, Italy; Department of Biomedical Sciences for Health (M.M., B.A.), University of Milan, Unit ofEndocrinology and Diabetology, IRCCS Policlinico San Donato, 20097 San Donato Milanese, Milan, Italy;and Division of Endocrinology, Diabetology, and Metabolism (E.G.), Department of Medical Sciences,University of Turin, 10124 Turin, Italy
Context: The long-term consequences of subclinical hypercortisolism (SH) in patients with adrenalincidentalomas (AIs) are unknown.
Setting and Patients: In this retrospective multicentric study, 206 AI patients with a !5-year fol-low-up (median, 72.3 mo; range, 60–186 mo) were enrolled.
Intervention and Main Outcome Measures: Adrenocortical function, adenoma size, metabolicchanges, and incident cardiovascular events (CVEs) were assessed. We diagnosed SH in 11.6% ofpatients in the presence of cortisol after a 1 mg-dexamethasone suppression test !5 "g/dL (138nmol/L) or at least two of the following: low ACTH, increased urinary free cortisol, and 1 mg-dexamethasone suppression test !3 "g/dL (83 nmol/L).
Results: At baseline, age and the prevalence of CVEs and type 2 diabetes mellitus were higher inpatients with SH than in patients without SH (62.2 " 11 y vs 58.5 " 10 y; 20.5 vs 6%; and 33.3 vs16.8%, respectively; P # .05). SH and type 2 diabetes mellitus were associated with prevalent CVEs(odds ratio [OR], 3.1; 95% confidence interval [CI], 1.1–9.0; and OR, 2.0; 95% CI, 1.2–3.3, respec-tively), regardless of age. At the end of the follow-up, SH was diagnosed in 15 patients who werewithout SH at baseline. An adenoma size !2.4 cm was associated with the risk of developing SH(sensitivity, 73.3%; specificity, 60.5%; P $ .014). Weight, glycemic, lipidic, and blood pressurecontrol worsened in 26, 25, 13, and 34% of patients, respectively. A new CVE occurred in 22 patients.SH was associated with the worsening of at least two metabolic parameters (OR, 3.32; 95% CI,1.6–6.9) and with incident CVEs (OR, 2.7; 95% CI, 1.0–7.1), regardless of age and follow-up.
Conclusion: SH is associated with the risk of incident CVEs. Besides the clinical follow-up, in patientswith an AI !2.4 cm, a long-term biochemical follow-up is also required because of the risk of SHdevelopment. (J Clin Endocrinol Metab 99: 827–834, 2014)
ISSN Print 0021-972X ISSN Online 1945-7197Printed in U.S.A.Copyright © 2014 by the Endocrine SocietyReceived September 18, 2013. Accepted December 18, 2013.First Published Online January 7, 2014
Abbreviations: AH, arterial hypertension; AI, adrenal incidentaloma; BMI, body mass index;CI, confidence interval; CT, computed tomography; CVE, cardiovascular event; DL, dys-lipidemia; 1 mg-DST, 1 mg-dexamethasone suppression test; HPA, hypothalamic-pituitary-adrenal; LDL, low-density lipoprotein; OB, obesity; OR, odds ratio; ROC, receiver operatingcharacteristic; SH, subclinical hypercortisolism; SN, sensitivity; SP, specificity; T2DM, type2 diabetes mellitus; UFC, urinary free cortisol; ULN, upper limit of normal.
O R I G I N A L A R T I C L E
E n d o c r i n e C a r e
doi: 10.1210/jc.2013-3527 J Clin Endocrinol Metab, March 2014, 99(3):827–834 jcem.endojournals.org 827
The Endocrine Society. Downloaded from press.endocrine.org by [Lino Furlani] on 16 March 2014. at 12:54 For personal use only. No other uses without permission. . All rights reserved.
Long-Term Follow-Up in Adrenal Incidentalomas: AnItalian Multicenter Study
Valentina Morelli, Giuseppe Reimondo, Roberta Giordano, Silvia Della Casa,Caterina Policola, Serena Palmieri, Antonio S. Salcuni, Alessia Dolci,Marco Mendola, Maura Arosio, Bruno Ambrosi, Alfredo Scillitani, Ezio Ghigo,Paolo Beck-Peccoz, Massimo Terzolo, and Iacopo Chiodini
Department of Clinical Sciences and Community Health (V.M., S.P., A.D., M.A., P.B.-P., I.C.), Universityof Milan, 20122 Milan, Italy; Unit of Endocrinology and Diabetology (V.M., S.P., P.B.-P., I.C.),Fondazione IRCCS Cà Granda-Ospedale Maggiore Policlinico, 20122 Milan, Italy; Division of InternalMedicine I (G.R., M.T.), Ospedale San Luigi, 10043 Orbassano, Italy; Department of Biological andClinical Sciences (G.R., R.G., M.T.), University of Turin, 10124 Turin, Italy; Catholic University (S.D.C.,C.P.), Unit of Endocrinology and Metabolism, 00168 Rome, Italy; Unit of Endocrinology (A.S.S., A.S.),Ospedale “Casa Sollievo della Sofferenza,” IRCCS, 71013 San Giovanni Rotondo, Foggia, Italy; Unit ofEndocrine Diseases and Diabetology (A.D., M.A.), Ospedale San Giuseppe, Gruppo Multimedica, 20123Milan, Italy; Department of Biomedical Sciences for Health (M.M., B.A.), University of Milan, Unit ofEndocrinology and Diabetology, IRCCS Policlinico San Donato, 20097 San Donato Milanese, Milan, Italy;and Division of Endocrinology, Diabetology, and Metabolism (E.G.), Department of Medical Sciences,University of Turin, 10124 Turin, Italy
Context: The long-term consequences of subclinical hypercortisolism (SH) in patients with adrenalincidentalomas (AIs) are unknown.
Setting and Patients: In this retrospective multicentric study, 206 AI patients with a !5-year fol-low-up (median, 72.3 mo; range, 60–186 mo) were enrolled.
Intervention and Main Outcome Measures: Adrenocortical function, adenoma size, metabolicchanges, and incident cardiovascular events (CVEs) were assessed. We diagnosed SH in 11.6% ofpatients in the presence of cortisol after a 1 mg-dexamethasone suppression test !5 "g/dL (138nmol/L) or at least two of the following: low ACTH, increased urinary free cortisol, and 1 mg-dexamethasone suppression test !3 "g/dL (83 nmol/L).
Results: At baseline, age and the prevalence of CVEs and type 2 diabetes mellitus were higher inpatients with SH than in patients without SH (62.2 " 11 y vs 58.5 " 10 y; 20.5 vs 6%; and 33.3 vs16.8%, respectively; P # .05). SH and type 2 diabetes mellitus were associated with prevalent CVEs(odds ratio [OR], 3.1; 95% confidence interval [CI], 1.1–9.0; and OR, 2.0; 95% CI, 1.2–3.3, respec-tively), regardless of age. At the end of the follow-up, SH was diagnosed in 15 patients who werewithout SH at baseline. An adenoma size !2.4 cm was associated with the risk of developing SH(sensitivity, 73.3%; specificity, 60.5%; P $ .014). Weight, glycemic, lipidic, and blood pressurecontrol worsened in 26, 25, 13, and 34% of patients, respectively. A new CVE occurred in 22 patients.SH was associated with the worsening of at least two metabolic parameters (OR, 3.32; 95% CI,1.6–6.9) and with incident CVEs (OR, 2.7; 95% CI, 1.0–7.1), regardless of age and follow-up.
Conclusion: SH is associated with the risk of incident CVEs. Besides the clinical follow-up, in patientswith an AI !2.4 cm, a long-term biochemical follow-up is also required because of the risk of SHdevelopment. (J Clin Endocrinol Metab 99: 827–834, 2014)
ISSN Print 0021-972X ISSN Online 1945-7197Printed in U.S.A.Copyright © 2014 by the Endocrine SocietyReceived September 18, 2013. Accepted December 18, 2013.First Published Online January 7, 2014
Abbreviations: AH, arterial hypertension; AI, adrenal incidentaloma; BMI, body mass index;CI, confidence interval; CT, computed tomography; CVE, cardiovascular event; DL, dys-lipidemia; 1 mg-DST, 1 mg-dexamethasone suppression test; HPA, hypothalamic-pituitary-adrenal; LDL, low-density lipoprotein; OB, obesity; OR, odds ratio; ROC, receiver operatingcharacteristic; SH, subclinical hypercortisolism; SN, sensitivity; SP, specificity; T2DM, type2 diabetes mellitus; UFC, urinary free cortisol; ULN, upper limit of normal.
O R I G I N A L A R T I C L E
E n d o c r i n e C a r e
doi: 10.1210/jc.2013-3527 J Clin Endocrinol Metab, March 2014, 99(3):827–834 jcem.endojournals.org 827
The Endocrine Society. Downloaded from press.endocrine.org by [Lino Furlani] on 16 March 2014. at 12:54 For personal use only. No other uses without permission. . All rights reserved.
www.associazionemediciendocrinologi.it ame news marzo 2014
2/2
Risultati simili emergono da un recente studio longitudinale di Di Dalmazi et al su 198 pazienti con AI con un follow-up medio di 7.5 anni, che mostra un peggioramento della funzione surrenalica nel 12% dei pazienti durante il follow-up e un aumento del rischio di sviluppo di nuovi eventi cardiovascolari nei pazienti con IS (stabile o peggiorato) rispetto a quelli senza IS stabili nel tempo (HR 3.01, IC95% 1.04-8.7). Inoltre nei pazienti con IS stabile viene riportato un aumento della mortalità per tutte le cause, associata all’età (HR 1.06, IC95% 1.01-1.12, p = 0.06), e ai livelli di cortisolemia dopo 1mg-DST (HR 1.10, IC95% 1.01-1.19, p = 0.04) e una minor sopravvivenza per eventi cardiovascolari (78.4% vs 97.5%, p = 0.02), rispetto ai pazienti senza IS. Non è stata osservata alcuna differenza per mortalità da neoplasia maligna. In conclusione: a. l’IS espone il paziente con AI al rischio di sviluppare nuovi ECV e di aumentata mortalità. Questi fattori
sembrano associati ai livelli di cortisolemia dopo 1mg-DST; b. i pazienti con un adenoma > 2.4 cm mostrano un rischio maggiore di sviluppare IS, per cui è necessario
eseguire oltre al follow-up clinico, atto a valutare la comparsa di fattori di rischio cardiovascolare come DMT2 e ipertensione arteriosa, anche un follow-up biochimico di lunga durata.
Bibliografia 1. Morelli V, Reimondo G, Giordano R, et al. Long-term follow-up in adrenal incidentalomas: an Italian
Multicenter Study. J Clin Endocrinol Metab 2014, DOI: http://dx.doi.org/10.1210/jc.2013-3527. 2. Di Dalmazi G, Vicennati V, Garelli S, et al. Cardiovascular events and mortality in patients with adrenal
incidentalomas that are either non-secreting or associated with intermediate phenotype or subclinical Cushing's syndrome: a 15-year retrospective study. Lancet Diabetes Endocrinol 2014, doi: 10.1016/S2213-8587(13)70211-0.
3. Reimondo G. Incidentaloma surrenalico e ipercortisolismo subclinico. Endowiki.

THE
ENDO
CRIN
E SO
CIET
Y’S
CLIN
ICAL
GUI
DELI
NES
4
SUMMARY OF RECOMMENDATIONS
3.0. DIAGNOSIS OF CUSHING’S SYNDROME
Who should be tested3.1. We recommend obtaining a thorough drug history toexclude excessive exogenous glucocorticoid exposure leadingto iatrogenic Cushing’s syndrome before conductingbiochemical testing (1| ).
3.2. We recommend testing for Cushing’s syndrome in thefollowing groups:• Patients with unusual features for age (e.g. osteoporosis,
hypertension) (Table 1) (1| )• Patients with multiple and progressive features,
particularly those who are more predictive of Cushing’ssyndrome (Table 1) (1| )
• Children with decreasing height percentile and increasingweight (1| )
• Patients with adrenal incidentaloma compatible withadenoma (1| ).
3.3. We recommend against widespread testing for Cushing’ssyndrome in any other patient group (1| ).
Initial testing3.4. For the initial testing for Cushing’s syndrome, werecommend one of the following tests based on its suitabilityfor a given patient (Fig. 1) (1| ):
3.4.1. Urine free cortisol (UFC; at least two measurements)3.4.2. Late-night salivary cortisol (two measurements)3.4.3. 1-mg overnight dexamethasone suppression test
(DST)3.4.4. Longer low-dose DST (2 mg/d for 48 h)
3.5. We recommend against the use of the following to test forCushing’s syndrome (1| ):• Random serum cortisol or plasma ACTH levels• Urinary 17-ketosteroids• Insulin tolerance test• Loperamide test• Tests designed to determine the cause of Cushing’s
syndrome (e.g. pituitary and adrenal imaging, 8 mg DST).
3.6. In individuals with normal test results in whom thepretest probability is high (patients with clinical featuressuggestive of Cushing’s syndrome and adrenal incidentalomaor suspected cyclic hypercortisolism), we recommend furtherevaluation by an endocrinologist to confirm or exclude thediagnosis (1| ).
3.7. In other individuals with normal test results (in whomCushing’s syndrome is very unlikely), we suggest reevaluationin 6 months if signs or symptoms progress (2| ).
3.8. In individuals with at least one abnormal test result (forwhom the results could be falsely positive or indicateCushing’s syndrome), we recommend further evaluation by anendocrinologist to confirm or exclude the diagnosis(1| ).
Subsequent evaluation3.9. For the subsequent evaluation of abnormal initial testresults, we recommend performing another recommended test(Fig. 1, 1| ).
3.9.1. We suggest the additional use of the dexamethasone-CRH test or the midnight serum cortisol test in specificsituations (Fig. 1, 1| ).
3.9.2. We suggest against the use of the desmopressintest, except in research studies, until additional data validateits utility (2| ).
3.9.3. We recommend against any further testing forCushing’s syndrome in individuals with concordantly negativeresults on two different tests (except in patients suspected ofhaving the very rare case of cyclical disease) (1| ).
3.9.4. We recommend tests to establish the cause ofCushing’s syndrome in patients with concordantly positiveresults from two different tests, provided there is no concernregarding possible non-Cushing’s hypercortisolism (Table 2)(1| ).
3.9.5. We suggest further evaluation and follow-up forthe few patients with concordantly negative results who aresuspected of having cyclical disease and also for patients withdiscordant results, especially if the pretest probability ofCushing’s syndrome is high (2| ).
4.0. SPECIAL POPULATIONS/CONSIDERATIONS
4.1. Pregnancy: We recommend the use of UFC and againstthe use of dexamethasone testing in the initial evaluation ofpregnant women (1| ).
4.2. Epilepsy: We recommend against the use ofdexamethasone testing in patients receiving antiepilepticdrugs known to enhance dexamethasone clearance andrecommend instead measurements of nonsuppressed cortisolin blood, saliva, or urine (1| ).
4.3. Renal failure: We suggest using the 1-mg overnight DSTrather than UFC for initial testing for Cushing’s syndrome inpatients with severe renal failure (2| ).
4.4. Cyclic Cushing’s syndrome: We suggest use of UFC ormidnight salivary cortisol tests rather than DSTs in patientssuspected of having cyclic Cushing’s syndrome (2| ).
4.5. Adrenal incidentaloma: We suggest use of the 1-mg DSTor late-night cortisol test, rather than UFC, in patientssuspected of having mild Cushing’s syndrome (2| ).
The Diagnosis of Cushing’s Syndrome:
An Endocrine Society Clinical Practice Guideline
GUIDELINESCLINICAL T h e E n d o c r i n e S o c i e t y ’ s
Authors: Lynnette K. Nieman, Beverly M. K. Biller, James W. Findling, John Newell-Price, Martin O. Savage,Paul M. Stewart, and Victor M. Montori
Affiliations: Program on Reproductive and Adult Endocrinology (L.K.N.), National Institute of Child Health andHuman Development, National Institutes of Health, Bethesda, Maryland 20892; NeuroendocrineUnit/Massachusetts General Hospital (B.M.K.B.), Boston, Massachusetts 02114; Medical College of Wisconsin(J.W.F.), Milwaukee, Wisconsin 53226; University of Sheffield (J.N.-P.), Sheffield S102JF, United Kingdom;William Harvey Research Institute, Queen Mary, University of London (M.O.S.), London EC1M6BQ, UnitedKingdom; University of Birmingham (P.M.S.), Birmingham B15 2TT, United Kingdom; and Mayo Clinic(V.M.M.), Rochester, Minnesota 55905
Co-Sponsoring Association: European Society of Endocrinology
Disclaimer Statement: Clinical practice guidelines are developed to be of assistance to physicians by providingguidance and recommendations for particular areas of practice. The guidelines should not be considered inclusiveof all proper approaches or methods, or exclusive of others. The guidelines cannot guarantee any specific outcome,nor do they establish a standard of care. The guidelines are not intended to dictate the treatment of a particularpatient. Treatment decisions must be made based on the independent judgment of health care providers and eachpatient's individual circumstances.
The Endocrine Society makes no warranty, express or implied, regarding the guidelines and specificallyexcludes any warranties of merchantability and fitness for a particular use or purpose. The Endocrine Society shallnot be liable for direct, indirect, special, incidental, or consequential damages related to the use of the informationcontained herein.
First published in the Journal of Clinical Endocrinology & Metabolism, May 2008, 93(5):1526–1540
© The Endocrine Society, 2008
Commercial Reprint InformationFor information on reprint requests of more than 101 and commercial reprints contact:
Heather EdwardsReprint Sales SpecialistCadmus Professional Communications
Phone: 410.691.6214Fax: 410.684.2789 Email: [email protected]
Single Reprint InformationFor information on reprints of 100 and fewer, complete the guideline order form and return using one of thefollowing methods:
Mail: The Endocrine Societyc/o Bank of AmericaP.O. Box 630721Baltimore, MD 21263-0736
Fax: 301.941.0257Email: [email protected]
Questions & CorrespondencesThe Endocrine SocietyAttn: Government & Public Affairs Department8401 Connecticut Avenue, Suite 900Chevy Chase, MD 20815
Phone: 301.941.0200Email: [email protected]: www.endo-society.org
For more information on The Endocrine Society’s Clinical Practice Guidelines or to download the completeversion of this guideline, visit http://www.endo-society.org/publications/guidelines/index.cfm.
MMTD07
Diabete Ppo 2 in giovane età

The Diagnosis of Cushing’s Syndrome:
An Endocrine Society Clinical Practice Guideline
GUIDELINESCLINICAL T h e E n d o c r i n e S o c i e t y ’ s
Authors: Lynnette K. Nieman, Beverly M. K. Biller, James W. Findling, John Newell-Price, Martin O. Savage,Paul M. Stewart, and Victor M. Montori
Affiliations: Program on Reproductive and Adult Endocrinology (L.K.N.), National Institute of Child Health andHuman Development, National Institutes of Health, Bethesda, Maryland 20892; NeuroendocrineUnit/Massachusetts General Hospital (B.M.K.B.), Boston, Massachusetts 02114; Medical College of Wisconsin(J.W.F.), Milwaukee, Wisconsin 53226; University of Sheffield (J.N.-P.), Sheffield S102JF, United Kingdom;William Harvey Research Institute, Queen Mary, University of London (M.O.S.), London EC1M6BQ, UnitedKingdom; University of Birmingham (P.M.S.), Birmingham B15 2TT, United Kingdom; and Mayo Clinic(V.M.M.), Rochester, Minnesota 55905
Co-Sponsoring Association: European Society of Endocrinology
Disclaimer Statement: Clinical practice guidelines are developed to be of assistance to physicians by providingguidance and recommendations for particular areas of practice. The guidelines should not be considered inclusiveof all proper approaches or methods, or exclusive of others. The guidelines cannot guarantee any specific outcome,nor do they establish a standard of care. The guidelines are not intended to dictate the treatment of a particularpatient. Treatment decisions must be made based on the independent judgment of health care providers and eachpatient's individual circumstances.
The Endocrine Society makes no warranty, express or implied, regarding the guidelines and specificallyexcludes any warranties of merchantability and fitness for a particular use or purpose. The Endocrine Society shallnot be liable for direct, indirect, special, incidental, or consequential damages related to the use of the informationcontained herein.
First published in the Journal of Clinical Endocrinology & Metabolism, May 2008, 93(5):1526–1540
© The Endocrine Society, 2008
Commercial Reprint InformationFor information on reprint requests of more than 101 and commercial reprints contact:
Heather EdwardsReprint Sales SpecialistCadmus Professional Communications
Phone: 410.691.6214Fax: 410.684.2789 Email: [email protected]
Single Reprint InformationFor information on reprints of 100 and fewer, complete the guideline order form and return using one of thefollowing methods:
Mail: The Endocrine Societyc/o Bank of AmericaP.O. Box 630721Baltimore, MD 21263-0736
Fax: 301.941.0257Email: [email protected]
Questions & CorrespondencesThe Endocrine SocietyAttn: Government & Public Affairs Department8401 Connecticut Avenue, Suite 900Chevy Chase, MD 20815
Phone: 301.941.0200Email: [email protected]: www.endo-society.org
For more information on The Endocrine Society’s Clinical Practice Guidelines or to download the completeversion of this guideline, visit http://www.endo-society.org/publications/guidelines/index.cfm.
MMTD07
but that are also common in the general population,such as obesity, depression, diabetes, hypertension, ormenstrual irregularity. As a result, there is an overlapin the clinical presentation of individuals with andwithout the disorder (Table 1). We encouragecaregivers to consider Cushing’s syndrome as asecondary cause of these conditions, particularly ifadditional features of the disorder are present. (seeWho should be tested below.) If Cushing’s syndrome isnot considered, the diagnosis is all too often delayed.
In addition, overactivity of the hypothalamic-pituitary-adrenal (HPA) axis occurs without true Cushing’s
syndrome, so that there is an overlap betweenphysiological and pathophysiological causes ofhypercortisolism (Table 2). Thus, certain psychiatricdisorders (depression, anxiety disorder, obsessive-compulsive disorder), poorly controlled diabetesmellitus, and alcoholism can be associated with mildhypercortisolism and may produce test results suggestiveof Cushing’s syndrome, including abnormaldexamethasone suppressibility and mildly elevated UFC(9). Circulating cortisol concentrations are usuallynormal (or slightly reduced) in obesity, but severeobesity can raise UFC. It is thought that higher braincenters stimulate CRH release in these conditions, with
THE
ENDO
CRIN
E SO
CIET
Y’S
CLIN
ICAL
GUI
DELI
NES
6
TABLE 1. Overlapping conditions and clinical features of Cushing’s syndromea
Symptoms Signs Overlapping conditions
Features that best discriminate Cushing’s syndrome; most do not have a high sensitivity
Easy bruising
Facial plethora
Proximal myopathy (or proximal muscle weakness)
Striae (especially if reddish purple and >1 cm wide)
In children, weight gain with decreasing growth velocity
Cushing’s syndrome features in the general population that are common and/or less discriminatory
Depression Dorsocervical fat pad (“buffalo hump”) Hypertensionb
Fatigue Facial fullness Incidental adrenal mass
Weight gain Obesity Vertebral osteoporosisb
Back pain Supraclavicular fullness Polycystic ovary syndrome
Changes in appetite Thin skinb Type 2 diabetesb
Decreased concentration Peripheral edema Hypokalemia
Decreased libido Acne Kidney stones
Impaired memory Hirsutism or female balding Unusual infections(especially short term)
Insomnia Poor skin healing
Irritability
Menstrual abnormalities
In children, slow growth In children, abnormal genital virilization
In children, short stature
In children, pseudoprecocious puberty or delayed puberty
a Features are listed in random order.b Cushing’s syndrome is more likely if onset of the feature is at a younger age.

OSPEDALE CLASSIFICATO "SACRO CUORE - DON CALABRIA"37024 - NEGRAR (Verona) - Tel 045/601.3111 - Fax 045/7500480
U.O.S. di ENDOCRINOLOGIA
Responsabile: Dr Lino Furlani
Tel. 601.3712 (Dr Furlani) - 601.3711 (Dr Dellera, Dr Guerriero) - 601.3750 (Day Hospital) - 601.3310 (Degenze)
Fax 045 6013727 e mail: [email protected]
Sig.ra FEZZARDI Laura, n. 01/09/1972
Negrar, 18/11/2005
Test CRH
Tempi ACTH(ng/L)
Cortisolo(nmol/L)
ACTH%
Cortisolo%
Base 51 27615’ 128 384 15130’ 24 572 107
60’ 36 448
Note: ………………………………………………………………………………………………………...
………………………………………………………………………………………………………………..
………………………………………………………………………………………………………………..
………………………………………………………………………………………………………………..
………………………………………………………………………………………………………………..
Basali DST 1 mg DST 2 mg DST 8 mg vn
ACTH h.8 ng/L 53 CORTISOLO h 8:00 nmol/L 574 652 534 399 171-536
CORTISOLO h.18.00 nmol/L 497 64-340
CLU nmol/d 2358 465 150-1100
Caso clinico

Caso clinico
Cateterismo seni petrosi

Quali esami di screening?

body temperature in daylight hours (particularly earlymorning – for example, with vigorous exercise) or de-crease body temperature in the evening (that is, throughenvironmental or pharmacological manipulations).
Clinical studies of young people with major depressivedisordersMonitoring the 24-hour sleep-wake and activity cycleA key aspect of those studies that focus on disruptionsof sleep-wake cycles and circadian rhythms is the cap-acity to integrate a number of new detailed objectivemeasures (Table 2). These complement extended self-report measures of daily fluctuations in sleep, mood, en-ergy or physical activity. They include extended periodsof actigraphy (for example, typically at least two weeks),as well as 24- to 72-hour assays of body temperatureand 24-hour fluctuations in cortisol or melatonin (in-cluding under controlled environmental parameters,such as light exposure). Even though actigraphy mea-sures are indirect and somewhat more variable (at leastin the short term) than other circadian markers, be-cause of other behavioral and homeostatic influences,they have consistently been found to correlate withthe circadian rhythm of endogenous melatonin and bodytemperature [242-249]. Other new technologies, such assmart phone applications, permit home monitoring ofextended periods of sleep-wake cycle behavior andpatterns of physical activity.Within the research environment, the introduction of dir-
ect ecological monitoring systems [250,251] continues toprovide important new insights into the daily patterns ofphysical activity, daytime resting, eating and other key so-cial behaviors, alongside data related to subjective energy ormood levels. These types of studies have the capacity to
reveal important longitudinal associations between daytimeactivity, sleep-wake cycle timing and mood and other psy-chological and neuropsychological variables.
Markedly delayed sleep phase in young people withdepressionWhen the various sleep-wake technologies are applied inyounger subjects in the early phases of major mood dis-orders, a quite different pattern of sleep and circadianrhythms emerges in comparison to young persons with-out mood disorders or middle-aged subjects with mooddisorders. Our own studies highlight two key aspects inyoung persons with mood disorders, namely: (a) the pre-dominance of delayed sleep phase (that is, not only go-ing to bed later, but also rising later) [123] rather thanthe more characteristic pattern of phase advance thathas traditionally been linked with more severe forms ofdepression in mid and later-life; and, (b) a late dim lightmelatonin onset (DLMO) compared to values classicallyfound in young healthy persons [42,212]. This delayedpattern of the sleep-wake cycle and endogenous circa-dian rhythms is most marked in those with bipolar thanunipolar phenotypes [123,212]. Importantly, longitudinalprospective studies are needed to identify sleep-wakeor circadian predictors of mood disorders early in thecourse of illness. Notably, promising findings in youthhave highlighted the predictive value of sleep problemsand specific polysomnographic (PSG) markers for the fu-ture development of mood disorders [252-255] and thetransition from unipolar to bipolar depression [256].Such technologies can also be applied in older subjects
with late-life depressive or early neurodegenerative dis-orders. Here, our data shows that greater nocturnalwakefulness as measured by actigraphic monitoring
Figure 3 The normal synchronous relationships between sleep and daytime activity and cortisol, melatonin and body temperature.
Hickie et al. BMC Medicine 2013, 11:79 Page 11 of 27http://www.biomedcentral.com/1741-7015/11/79
30 mcg/dl
0 mcg/dl
536
CorPsolo sierico nmol/L
Cortisolo ritmo circadiano


www.associazionemediciendocrinologi.it Breaking news nr. 9 - marzo 2014
PLENADREN PRESCRIVIBILE DA OGGI IN FASCIA H
Responsabile Editoriale Vincenzo Toscano
Commissione Farmaci AME Raffaele Volpe (Coordinatore) ([email protected] ) Agostino Paoletta, Agostino Specchio, Davide De Brasi, Enrica Ciccarelli
A cura di: Renato Cozzi 1/1
Avevamo già comunicato (AME Breaking News n 3/2014) la pubblicazione sulla G.U. del 28/12/2013 n°
303 della determina AIFA su regime di rimborsabilità e prezzo di vendita del medicinale per uso umano
Plenadren (idrocortisone).
Il medicinale era stato inserito (G.U. 18/05/2012 n° 115) nell'elenco dei farmaci erogabili a totale carico
del Servizio Sanitario Nazionale, ai sensi della legge 648/96.
Da oggi, 3 marzo 2014, il farmaco Plenadren è disponibile in Italia per la prescrizione in fascia H.
Indicazioni terapeutiche: trattamento dell'insufficienza surrenalica negli adulti.
Classe di rimborsabilità: H.
Classificazione ai fini della fornitura: medicinale soggetto a prescrizione medica limitativa, vendibile al
pubblico su prescrizione di centri ospedalieri o di specialisti endocrinologi (RRL).
Allegato: testo GU
www.associazionemediciendocrinologi.it Breaking news nr. 9 - marzo 2014
PLENADREN PRESCRIVIBILE DA OGGI IN FASCIA H
Responsabile Editoriale Vincenzo Toscano
Commissione Farmaci AME Raffaele Volpe (Coordinatore) ([email protected] ) Agostino Paoletta, Agostino Specchio, Davide De Brasi, Enrica Ciccarelli
A cura di: Renato Cozzi 1/1
Avevamo già comunicato (AME Breaking News n 3/2014) la pubblicazione sulla G.U. del 28/12/2013 n°
303 della determina AIFA su regime di rimborsabilità e prezzo di vendita del medicinale per uso umano
Plenadren (idrocortisone).
Il medicinale era stato inserito (G.U. 18/05/2012 n° 115) nell'elenco dei farmaci erogabili a totale carico
del Servizio Sanitario Nazionale, ai sensi della legge 648/96.
Da oggi, 3 marzo 2014, il farmaco Plenadren è disponibile in Italia per la prescrizione in fascia H.
Indicazioni terapeutiche: trattamento dell'insufficienza surrenalica negli adulti.
Classe di rimborsabilità: H.
Classificazione ai fini della fornitura: medicinale soggetto a prescrizione medica limitativa, vendibile al
pubblico su prescrizione di centri ospedalieri o di specialisti endocrinologi (RRL).
Allegato: testo GU
www.associazionemediciendocrinologi.it Breaking news nr. 9 - marzo 2014
PLENADREN PRESCRIVIBILE DA OGGI IN FASCIA H
Responsabile Editoriale Vincenzo Toscano
Commissione Farmaci AME Raffaele Volpe (Coordinatore) ([email protected] ) Agostino Paoletta, Agostino Specchio, Davide De Brasi, Enrica Ciccarelli
A cura di: Renato Cozzi 1/1
Avevamo già comunicato (AME Breaking News n 3/2014) la pubblicazione sulla G.U. del 28/12/2013 n°
303 della determina AIFA su regime di rimborsabilità e prezzo di vendita del medicinale per uso umano
Plenadren (idrocortisone).
Il medicinale era stato inserito (G.U. 18/05/2012 n° 115) nell'elenco dei farmaci erogabili a totale carico
del Servizio Sanitario Nazionale, ai sensi della legge 648/96.
Da oggi, 3 marzo 2014, il farmaco Plenadren è disponibile in Italia per la prescrizione in fascia H.
Indicazioni terapeutiche: trattamento dell'insufficienza surrenalica negli adulti.
Classe di rimborsabilità: H.
Classificazione ai fini della fornitura: medicinale soggetto a prescrizione medica limitativa, vendibile al
pubblico su prescrizione di centri ospedalieri o di specialisti endocrinologi (RRL).
Allegato: testo GU
www.associazionemediciendocrinologi.it
ame news farmaci luglio 2012
2/3
Concentrazione media di cortisolo sierico osservata nell’arco delle 24 ore in seguito alla somministrazione di dosi singole e multiple in pazienti con insufficienza surrenalica primaria (n=62) dopo la somministrazione orale di Plenadren, dato una volta al giorno, e di idrocortisone, dato tre volte al giorno (come da scheda tecnica)
In uno studio recentemente pubblicato (Johannsson G, et al. Improved cortisol exposure-time profile and outcome in patients with adrenal insufficiency: a prospective randomized trial of a novel hydrocortisone dual-release formulation. J Clin Endocrinol Metab 2012, 97: 473-81) è stato paragonato il profilo giornaliero delle concentrazioni circolanti di cortisolo, l’outcome metabolico e la QoL nei pazienti addisoniani trattati con la formulazione a rilascio modificato rispetto a quelli trattati con la formulazione classica. Si è potuto dimostrare che la somministrazione di Plenadren rispetto alla formulazione convenzionale otteneva: x media giornaliera delle concentrazioni di cortisolo più bassa; x livelli di cortisolo dopo la somministrazione mattutina più alti; x riduzione ponderale, miglior compenso pressorio e glicemico, miglioramento degli indici di anabolismo osseo
e miglioramento della QoL. Gli effetti collaterali erano di lieve entità con entrambi i trattamenti. Le dosi sostitutive orali di Plenadren devono essere personalizzate secondo la risposta clinica: x la dose di mantenimento comune è di 20–30 mg/die, somministrata una volta sola al mattino; x nei pazienti in cui si riscontri ancora una produzione endogena di cortisolo potrebbe essere sufficiente una
dose inferiore; x la più alta dose di mantenimento studiata è di 40 mg/die.

0
5
10
15
20
25
30
1 4 7 10 13 16 19 22 25 28 31 34 37 40 43 46 49 52 55 58 61 64
CORTISOLO SIERICO h8 -‐ variabilità
cortisolo (µg/dl)
prelievi multipli mattutini
Variabilità individuale 2-13% tra prelievi
Courtesy of Terzolo

7,5 mcg/dl
5 mcg/dl
1,8 mcg/dl

Findling et Raff; JCEM 2006, 91(10):3746 Kidambi et Al; EJE (2007) 157 725–731
0,15 mcg/dl 0,15 – 0,3 mcg/dl > 0,3 mcg/dl
CORTISOLO SALIVARE

Differentiating between Cushing’s diseaseand pseudo-Cushing’s syndrome: comparisonof four testsR A Alwani*, L W Schmit Jongbloed*, F H de Jong, A J van der Lely,
W W de Herder and R A Feelders
Division of Endocrinology, Room H555, Department of Internal Medicine, Erasmus Medical Centre, PO Box 2040,
3000 CA Rotterdam, The Netherlands*(R A Alwani and L W Schmit Jongbloed contributed equally to this work)
Correspondence
should be addressed
to R A Alwani
Abstract
Objective: To evaluate the diagnostic performance of four different tests in order to differentiate between Cushing’s disease
(CD) and pseudo-Cushing’s syndrome (PCS).
Methods: In this prospective study, a total of 73 patients with clinical features of hypercortisolism and insufficient suppression
of serum cortisol after 1 mg overnight dexamethasone and/or an elevated excretion of cortisol in 24-h urine samples were
included. The circadian rhythm of serum cortisol levels as well as midnight serum cortisol (MserC) levels were assessed in all
73 patients. Late-night salivary cortisol (LNSC) concentrations were obtained in 44 patients. The dexamethasone–CRH
(Dex–CRH) test was performed in 54 patients.
Results: Fifty-three patients were diagnosed with CD and subsequently treated. Twenty patients were classified as having
PSC. Serum cortisol circadian rhythm: the diurnal rhythmicity of cortisol secretion was retained in PCS. A cortisol
midnight:morning ratio of O0.67 is highly suggestive of CD (positive predictive value (PPV) 100% and negative predictive
value (NPV) 73%). MserC concentration O243 nmol/l has a PPV of 98% in predicting true CD (NPV 95%). LNSC level
O9.3 nmol/l predicted CD in 94% of patients (NPV 100%). Dex–CRH test: after 2 days of dexamethasone suppression, a
CRH-stimulated cortisol level O87 nmol/l (TZ15 min) resulted in a PPV of 100% and an NPV of 90%.
Conclusion: The Dex–CRH test as well as a single measurement of cortisol in serum or saliva at late (mid-) night demonstrated
high diagnostic accuracy in differentiating PCS from true CD.
European Journal of
Endocrinology
(2014) 170, 477–486
Introduction
Cushing’s disease (CD) is caused by an adrenocortico-
tropin (ACTH)-secreting pituitary adenoma leading to
chronic overproduction of cortisol. This results in a clinical
phenotype with features like a full plethoric face, central
obesity, and muscle and skin atrophy. The diagnosis can
be difficult due to gradual development of symptoms and
due to overlap with features of metabolic syndrome (1).
In addition, it can be challenging to differentiate cases
with mild ACTH-dependent hypercortisolism from
conditions that are accompanied by (physiologic) over-
activity of the hypothalamic–pituitary–adrenal axis
referred to as pseudo-Cushing’s syndrome (PCS). PCS can
present with a similar clinical phenotype and is associated
with chronic alcoholism, psychiatric disorders, severe
obesity, poorly controlled diabetes, and extreme physical
stress. Treatment of these underlying conditions will lead
EuropeanJournalofEndocrinology
Clinical StudyR A Alwani, L W SchmitJongbloed and others
Differentiating CS and PCS 170 :4 477–486
www.eje-online.org ! 2014 European Society of EndocrinologyDOI: 10.1530/EJE-13-0702 Printed in Great Britain
Published by Bioscientifica Ltd.
Laboratory assays
Serum and urinary cortisol and plasma ACTH were
measured using chemiluminescence-based immunoassays
(Immulite 2000, Siemens, Los Angeles, CA, USA; inter- and
intra-assay coefficients of variation, respectively below 15
and 7% for cortisol and below 6.5 and 5.5% for ACTH).
Urinary cortisol was measured without prior solvent
extraction. Although this may be a less accurate method,
the upper limit of normal of this in-house assay was
carefully determined according to cortisol secretion rate in
healthy controls (18). Salivary cortisol was measured using
a commercial kit (Salivary Cortisol ELISA SLV-2930, DRG
Instruments GmbH, Marburg, Germany).
Statistical analysis
Mean and S.E.M. were calculated for continuous data and
presented as meanGS.E.M. Proportions were calculated for
categorical data. We considered a P value of !0.05 to be
statistically significant. The two-tailed Student’s t-test was
usedwhen continuous datawere normally distributed. The
Mann–WhitneyU testwasusedwhencontinuousdatawere
not normally distributed. Sensitivity, specificity, positive
predictive value (PPV), andnegative predictive value (NPV)
were calculated for each test using standard methods. PPV
was defined as the proportion of patients that are correctly
diagnosed with CD. NPV was defined as the proportion of
patients that are correctly diagnosed with PCS. Receiver
operating characteristic (ROC) curves were used for each
test to determine the area under the curve (AUC) and to
define the cut-off value with the best diagnostic per-
formance by minimizing the absolute difference between
the highest PPV and highest NPV (diagnostic accuracy of
the test). The leave-one-out cross validation method was
used to see if a combination of the MserC measurement
with the Dex–CRH test would further increase the
discriminatory power to distinguish patients with true
CD from patients with PCS. Statistical analysis and
graphing were performed with the commercially available
software packages GraphPad Prism, version 3.0 (GraphPad
Software, San Diego, CA, USA) and MedCalc, version 9.64
(MedCalc Software, Ostend, Belgium).
Results
Cortisol circadian rhythm
The dynamics of cortisol secretion in serum were
investigated in 52 patients with CD and in 19 patients
with PCS. Patients with CD had higher mean cortisol
values at all time points compared with patients with PCS.
Also, patients with CD showed a relatively flat cortisol
pattern throughout the day, whereas patients with PCS
retained a diurnal rhythmicity of cortisol secretion
(Table 1 and Fig. 2). ROC curve analysis (Fig. 2) showed
a cortisol midnight:morning ratio of 0.67 to have the
highest discriminating capacity between the diagnoses of
CD and PCS (PPV 100%, NPV 73%, and AUCZ0.969). The
cortisol midnight:morning ratio was O0.67 in 45 patients
with CD (sensitivity 87%), whereas all patients with PCS
noted a ratio of %0.67 (specificity 100%).
The serum cortisol late afternoon:morning ratio
(cortisol 1700 h:cortisol 0900 h) and the analysis of the
circadian rhythm in salivary cortisol and plasma ACTH
did not improve discrimination between groups and are
therefore not shown.
Midnight serum cortisol
MserC concentrations were obtained in 53 patients with
CD and 20 patients with PCS. Mean MserC levels were
significantly higher in patients with CD (577 nmol/lG43)
than in patients with PCS (141 nmol/lG13) (P!0.001).
800
Cortisol midnight:morningratio
100
80
60
40Sen
sitiv
ity
20
0
100
80
60
40Sen
sitiv
ity
20
0
0 20 40100-Specificity
Midnight serum cortisol
60 80 100
0 20 40100-Specificity
60 80 100
CD
PCS
600h 1200h 1800h 2400h
700
600
500
400
300
Cor
tisol
(nm
ol/l)
200
100
0
Figure 2
(Left) Mean cortisol levels in serum throughout the day of
52 patients with Cushing’s disease (CD) and 19 patients with
pseudo-Cushing’s syndrome (PCS). (Right, top) Receiver
operating characteristic (ROC) curve of the cortisol midnight:
morning ratio in serum. Optimal cut-off valueZ0.67. Area
under ROC curve (AUC)Z0.969 (sensitivity 87%, specificity
100%, positive predictive value (PPV) 100%, and negative
predictive value (NPV) 73%). (Right, bottom) ROC curve of the
midnight serum cortisol concentration. Optimal cut-off
valueZ243 nmol/l. AUCZ0.994 (sensitivity 98%, specificity
95%, PPV 98%, and NPV 95%).
European
JournalofEndocrinology
Clinical Study R A Alwani, L W SchmitJongbloed and others
Differentiating CS and PCS 170 :4 480
www.eje-online.org
lower diagnostic performance of the test (PPV 80–86%
and NPV 92–100%) and proposed different threshold
values for the 15-min post-CRH cortisol concentration
(44–110 nmol/l) (13, 14, 15, 17). These findings are
confirmed in the present survey, as we found an optimal
threshold value of 87 nmol/l for serum cortisol 15 min
after CRH administration (PPV 100% and NPV 90%). The
2-day DST (2 days of dexamethasone suppression without
CRH stimulation) also performed reasonably well (cut-off
50 nmol/l; PPV 92% and NPV 89%), but both its PPV as
well as its NPV further increased after adding CRH
stimulation, although these results are based on a
relatively small sample size. In contrast, a study conducted
by Martin et al. showed no improvement in the diagnostic
accuracy of the 2-day DST when CRH was administered
additionally. However, compared with our survey, there
was a significant difference in the inclusion of patients
with Cushing’s syndrome (pituitary and adrenal vs
pituitary only) and the number of dexamethasone doses
(nine vs eight) (15).
Differences in reliability of the Dex–CRH test in the
above-mentioned studies can possibly be explained by the
use of different protocols for the Dex–CRH test, adminis-
tration of different CRH preparations (ovine or human),
differences in CRH dosage (1 mg/kg or 100 mg), variation
in cortisol and ACTH assays, in particular with respect
to measurements in the low range, and absence of
uniform criteria to define PCS. Despite the fact that the
test is relatively expensive and impractical (hospital admis-
sion is required), the Dex–CRH test, based on its relatively
high diagnostic accuracy, can still be a valuable tool in cases
with indeterminate results of first-line screening tests.
Because it is most difficult to differentiate between CD
and PCS in patients with mild ACTH-dependent hyper-
cortisolism, a clinically relevant observation in our study
is that the diagnostic performance of all evaluated tests
was not different when CD patients with UFC levels within
two times the upper limit of normal were compared with
PCS patients.
Combining second-line tests did not improve diag-
nostic accuracy, possibly due to the relatively small sample
size of the PCS group. As always, whenmore tests are used,
discrepancies between test results can occur. Generally,
within individual patients, the different tests used
indicated the same diagnosis. We found in only four
patients (CDZ3 and PCSZ1) discrepancies between
MserC and post Dex–CRH-stimulated cortisol levels
which were just below or above the cut-off value and
i.e. because they demonstrated a corticotroph adenoma
with positive ACTH staining, these patients cannot be
classified. In the clinical scenario where test results are
discordant in a patient withmild hypercortisolism, follow-
up is recommended for monitoring progression of
symptoms and for repeat testing (1).
ACTH-secreting pituitary adenomas are known to
show overexpression of receptors for CRH and vasopressin
in corticotroph cells. Stimulation with either CRH or
desmopressin, a synthetic vasopressin analog, results in a
direct release of ACTH (40, 41, 42). Tirabassi et al. (43)
reported excellent diagnostic performance as well as
perfect diagnostic agreement for the human CRH test
and the desmopressin test in a study with a small number
of patients with PCS (nZ12), which should be confirmed
by future studies.
The strength of our current survey is its prospective
design and the clear biochemical criteria used to define
PCS (abnormal result in DST and/or elevated UFC on at
least two occasions). The limitations are UFC measure-
ment without solvent extraction, the relatively small
number of PCS patients, no measurement of plasma
dexamethasone levels during DST and Dex–CRH testing
and the fact that not all tests were performed in all
participating patients.
Conclusion
In the present study, the Dex–CRH test as well as
measurement of cortisol in saliva or serum collected at
midnight showed high diagnostic accuracy in distinguish-
ing between true CD and PCS. Results of the different tests
were concordant in most patients and combining tests did
not increase the diagnostic yield. Considering its con-
venience, its high diagnostic accuracy as a first-line
screening test as well as its ability to differentiate between
CD and PCS, the use of midnight salivary cortisol
assessment as a first-choice test seems rational. Depending
on the protocol and assay(s) used, it is important for
diagnostic centers to validate these tests and their
threshold values.
Declaration of interest
A J van der Lely is a consultant for Novartis Pharma, Pfizer International,
and Ipsen Pharma International. WW de Herder is a consultant for Novartis
Pharma and Ipsen Pharma International. R A Feelders is a consultant for
Novartis Pharma. The other authors have nothing to disclose.
Funding
This research did not receive any specific grant from any funding agency in
the public, commercial or not-for-profit sector.
Europea
nJournal
ofEn
docrinology
Clinical Study R A Alwani, L W SchmitJongbloed and others
Differentiating CS and PCS 170 :4 484
www.eje-online.org
The ROC curve for MserC is shown in Fig. 2. The optimal
threshold value to detect true CD was 243 nmol/l (PPV
98%, NPV 95%, and AUCZ0.994). All CD patients except
one showed MserC levels in excess of 243 nmol/l
(sensitivity 98%). Nineteen out of 20 patients with PCS
recorded MserC levels of %243 nmol/l (specificity 95%).
Late-night salivary cortisol
Cortisol in saliva wasmeasured in 33 patients with CD and
11 patients with PCS (Fig. 3). Mean LNSC levels were
significantly higher (P!0.001) in the CD group (35.0G
6.4 nmol/l) than in the PCS group (7.7G1.0 nmol/l).
According to the ROC curve (Fig. 3), the cut-off value
yielding the best PPV and NPV was 9.3 nmol/l (AUCZ
0.962). This value corresponds to a sensitivity of 100%,
a specificity of 83%, a PPV of 94%, and an NPV of 100%.
Dex–CRH test
The Dex–CRH test was performed in 35 patients with CD
and 19 patients with PCS. Sixteen out of 19 patients with
PCS had suppressed levels of serum cortisol below
50 nmol/l after 2 days of dexamethasone administration.
The mean cortisol level after dexamethasone suppression
and before CRH administration in the PCS group was
35 nmol/l (G3.0; range 27–78).
Serum cortisol levels were higher than 50 nmol/l in
33/35 patients with CD after 2 days of dexamethasone
suppression. The mean cortisol level after dexamethasone
suppression (before CRH stimulation) in the CD group was
288 nmol/l (G51; range 28–1283). Using a cut-off value
of 50 nmol/l, this 2-day DST (without subsequent CRH
stimulation) demonstrated a sensitivity of 94% and a
specificity of 84% (PPV 92% and NPV 89%).
Additional CRH stimulation (Dex–CRH test) led to a
correct classification of three more patients with PCS
(19/19). This resulted in a further improvement of the
above-mentioned predictive values. The highest diagnos-
tic accuracy of the Dex–CRH test was achieved when the
serum cortisol concentration 15 min after CRH adminis-
tration was used as the criterion. Patients with CD had
significantly higher levels of CRH-stimulated serum
cortisol than patients with PCS: 365G42.9 vs 41G
4.5 nmol/l (P!0.001). Measurement of plasma ACTH or
serum cortisol at other time points did not improve the
performance of the Dex–CRH test (data not shown).
The results of the Dex–CRH test are shown in Fig. 4.
ROC curve analysis showed an optimal cut-off value
of 87 nmol/l for CRH-stimulated serum cortisol at
TZ15 min (sensitivity of 94%, specificity 100%, PPV
100%, and NPV 90%). The AUC provided by the ROC
curve is 0.995 (Fig. 4).
Mild hypercortisolism
The diagnostic value of the described second-line tests did
not significantly differ when only CD patients with mild
hypercortisolism (i.e. UFC within two times the upper
limit of normal; nZ28) were compared with PCS patients
(Table 2).
Combined assessment of second-line tests
Combined assessment of MserC concentration and
Dex–CRH test was performed in 53 patients (35 CD and
18 PCS). The results of the two tests in these patients are
plotted in Fig. 5. Discordant test results were found in four
patients (Table 3).
Owing to the relatively small sample size of the PCS
group in our study, a leave-one-out cross validation
procedure failed to demonstrate any benefit of combining
the results of the two second-line tests; the discriminatory
200100
80
60
40Sen
sitiv
ity
20
00 20 40 60 80 100
100-Specificity
175
150
125
100
75
Cor
tisol
in s
aliv
a (n
mol
/l)
50
25
0CD PCS
9.3 nmol/l
Figure 3
(Left) Dot diagram showing midnight cortisol levels in saliva of
33 patients with Cushing’s disease (CD) and 11 patients with
pseudo-Cushing’s syndrome (PCS). (Right) Receiver operating
characteristic (ROC) curve of the late-night cortisol measure-
ment in saliva (LNSC). A threshold value of 9.3 nmol/l results in a
positive predictive value of 94% to distinguish authentic CD
from PCS (negative predictive value 100%, sensitivity 100%,
specificity 83%, and area under ROC curveZ0.962).
European
JournalofEndocrinology
Clinical Study R A Alwani, L W SchmitJongbloed and others
Differentiating CS and PCS 170 :4 481
www.eje-online.org
Differentiating between Cushing’s diseaseand pseudo-Cushing’s syndrome: comparisonof four testsR A Alwani*, L W Schmit Jongbloed*, F H de Jong, A J van der Lely,
W W de Herder and R A Feelders
Division of Endocrinology, Room H555, Department of Internal Medicine, Erasmus Medical Centre, PO Box 2040,
3000 CA Rotterdam, The Netherlands*(R A Alwani and L W Schmit Jongbloed contributed equally to this work)
Correspondence
should be addressed
to R A Alwani
Abstract
Objective: To evaluate the diagnostic performance of four different tests in order to differentiate between Cushing’s disease
(CD) and pseudo-Cushing’s syndrome (PCS).
Methods: In this prospective study, a total of 73 patients with clinical features of hypercortisolism and insufficient suppression
of serum cortisol after 1 mg overnight dexamethasone and/or an elevated excretion of cortisol in 24-h urine samples were
included. The circadian rhythm of serum cortisol levels as well as midnight serum cortisol (MserC) levels were assessed in all
73 patients. Late-night salivary cortisol (LNSC) concentrations were obtained in 44 patients. The dexamethasone–CRH
(Dex–CRH) test was performed in 54 patients.
Results: Fifty-three patients were diagnosed with CD and subsequently treated. Twenty patients were classified as having
PSC. Serum cortisol circadian rhythm: the diurnal rhythmicity of cortisol secretion was retained in PCS. A cortisol
midnight:morning ratio of O0.67 is highly suggestive of CD (positive predictive value (PPV) 100% and negative predictive
value (NPV) 73%). MserC concentration O243 nmol/l has a PPV of 98% in predicting true CD (NPV 95%). LNSC level
O9.3 nmol/l predicted CD in 94% of patients (NPV 100%). Dex–CRH test: after 2 days of dexamethasone suppression, a
CRH-stimulated cortisol level O87 nmol/l (TZ15 min) resulted in a PPV of 100% and an NPV of 90%.
Conclusion: The Dex–CRH test as well as a single measurement of cortisol in serum or saliva at late (mid-) night demonstrated
high diagnostic accuracy in differentiating PCS from true CD.
European Journal of
Endocrinology
(2014) 170, 477–486
Introduction
Cushing’s disease (CD) is caused by an adrenocortico-
tropin (ACTH)-secreting pituitary adenoma leading to
chronic overproduction of cortisol. This results in a clinical
phenotype with features like a full plethoric face, central
obesity, and muscle and skin atrophy. The diagnosis can
be difficult due to gradual development of symptoms and
due to overlap with features of metabolic syndrome (1).
In addition, it can be challenging to differentiate cases
with mild ACTH-dependent hypercortisolism from
conditions that are accompanied by (physiologic) over-
activity of the hypothalamic–pituitary–adrenal axis
referred to as pseudo-Cushing’s syndrome (PCS). PCS can
present with a similar clinical phenotype and is associated
with chronic alcoholism, psychiatric disorders, severe
obesity, poorly controlled diabetes, and extreme physical
stress. Treatment of these underlying conditions will lead
Europea
nJournal
ofEn
docrinology
Clinical StudyR A Alwani, L W SchmitJongbloed and others
Differentiating CS and PCS 170 :4 477–486
www.eje-online.org ! 2014 European Society of EndocrinologyDOI: 10.1530/EJE-13-0702 Printed in Great Britain
Published by Bioscientifica Ltd.
LNSC level 9.3 nmol/l predicted CD in 94% of pt

! Vantaggi • Buona sensibilità e specificità per la “presentazione moderna” della sindrome
di Cushing
• Possibilità di campionamenD mulDpli (3 campioni) in ambiente ambulatoriale, non-‐stressato
• Semplice, poco costoso
! Svantaggi • Specificità (evening stress, ritmo sonno-‐veglia, uso di liquirizia e tabacco,
contaminazione dei tamponi di raccolta)
• Interferenza dei sistemi di raccolta (cotone, polieDlene, polistere…)
• Livelli di riferimento dipendenD dalla metodica: necessità di «costruire» livelli di riferimento locali su larga fascia di popolazione
CORTISOLO SALIVARE

DST 1 mg overnight
and by the Mann-Whitney U test for nonparametric data. Forcategorical variables, differences were analyzed by means of the!2 test and Fisher’s exact test. Levels of statistical significancewere set at P ! 0.05. A multiple regression analysis was per-formed when appropriate. All analyses were performed using theStatistica software package (Microsoft Corp., Tulsa, OK).
Results
A total of 813 consecutive patients with type 2 diabeteswere enrolled. They were 428 men (52.6%) and 385women (47.4%) aged 25–70 yr (median 60 yr) with amedian duration of diabetes of 8 yr (range 1–20 yr). Of thewhole cohort, 17.9% of patients were treated with insulin,62.2% with oral hypoglycemic agents, 13.7% with a com-bined therapy, whereas 6.2% were on diet alone; patientson glitazones were excluded from the study because thesedrugs reportedly interfere with the HPA axis (13). Overall,71.7% of the patients were hypertensive, 56.5% of whomwere treated with two or more drugs, 58.7% had low-
density lipoprotein cholesterol greater than 100 mg/dl,and 79.9% were dyslipidemic, 46.8% of whom were onpharmacological treatment.
All subjects underwent a first screening step for Cush-ing’s syndrome using the overnight 1-mg DST. In a mul-tiple regression analysis including as candidate predictivevariables age, BMI, systolic and diastolic blood pressure,glycosylated hemoglobin (HbA1c), and fasting glucoselevels, post-DST cortisol levels were associated with sys-tolic blood pressure (" " 0.09, P " 0.02) and HbA1cvalues (" " 0.12, P " 0.001). However, the model ac-counted only for 2% (r2) of the total variation (P " 0.007).The patients with HbA1c greater than 7% had post-DSTcortisol levels higher than the remainder [1.73 # 2.28vs. 1.36 # 1.23 #g/dl (48 # 63 vs. 38 # 34 nmol/liter)P " 0.02].
Forty patients (4.9%) failed to suppress cortisol lessthan 5.0 #g/dl (138 nmol/liter) after the 1-mg DST (Fig. 2).They were 21 men and 19 women aged 20–70 yr (median56.5 yr). The patients failing to suppress cortisol wereslightly younger with similar duration of disease and BMI
FIG. 2. Cortisol values after 1-mg DST. FIG. 3. Cortisol values after 2-mg 2-day DST in the 40 non-suppressorpatients.
TABLE 2. Comparison of patients with post-DSTcortisol 5 #g/dl or less (DST suppressors) and post-DSTcortisol greaster than 5 #g/dl (DST nonsuppressors)
DSTsuppressors(n ! 773)
DSTnonsuppressors
(n ! 34)aP
valueAge (yr) 58.6 # 8.8 56.4 # 9.8 NSBMI (kg/m2) 32.1 # 6.1 30.9 # 4.6 NSDuration of
disease (yr)9.8 # 7.9 8.9 # 5.2 NS
Fasting glucose(mg/dl)
172.5 # 65.1 236.8 # 100.8 !0.0001
HbA1c (%) 8.4 # 1.9 9.2 # 2.0 0.01Systolic blood
pressure(mm Hg)
137.9 # 17.2 147.7 # 16.4 0.04
Diastolic bloodpressure(mm Hg)
82.6 # 10.1 80.7 # 10.9 NS
Data are expressed as mean values and SD. NS, Not significant.a Patients with confirmed Cushing’s syndrome have been excluded.
TABLE 3. Comparison of patients with false -DSTresults and true -positive DST results (confirmedCushing’s syndrome)
False-positiveDST (n ! 34)
True positiveDST (n ! 6)
Pvalue
Age (yr) 56.4 # 9.8 49.7 # 20.8 NSBMI (kg/m2) 30.9 # 4.6 35.9 # 12.6 NSDuration of
disease (yr)8.9 # 5.2 8.0 # 8.2 NS
Fasting glucose(mg/dl)
236.8 # 100.8 232.7 # 28.3 NS
HbA1c (%) 9.2 # 2.0 9.2 # 2.2 NSSystolic blood
pressure(mm Hg)
147.7 # 16.4 145.8 # 19.6 NS
Diastolic bloodpressure(mm Hg)
81.6 # 10.9 78.0 # 11.3 NS
Data are expressed as mean values and SD. NS, Not significant.
3470 Terzolo et al. Cushing’s Syndrome and Type 2 Diabetes J Clin Endocrinol Metab, October 2012, 97(10):3467–3475
The Endocrine Society. Downloaded from press.endocrine.org by [${individualUser.displayName}] on 18 March 2014. at 05:28 For personal use only. No other uses without permission. . All rights reserved.
Quale cut-‐off?
5 mcg/dl
1,8 mcg/dl
Screening of Cushing’s Syndrome in Outpatients withType 2 Diabetes: Results of a Prospective MulticentricStudy in Italy
Massimo Terzolo, Giuseppe Reimondo, Iacopo Chiodini, Roberto Castello,Roberta Giordano, Enrica Ciccarelli, Paolo Limone, Claudio Crivellaro,Irma Martinelli, Marcella Montini, Olga Disoteo, Bruno Ambrosi, Roberto Lanzi,Maura Arosio, Sanzio Senni, Antonio Balestrieri, Erica Solaroli, Bruno Madeo,Raffaella De Giovanni, Felice Strollo, Rodolfo Battista, Alessandro Scorsone,Vito A. Giagulli, Daniela Collura, Aldo Scillitani, Renato Cozzi,Marco Faustini-Fustini, Anna Pia, Roberta Rinaldi, Barbara Allasino, Giulia Peraga,Francesco Tassone, Piernicola Garofalo, Enrico Papini, and Giorgio Borretta*
Context: Cushing’s syndrome may remain unrecognized among patients referred for metabolicsyndrome; thus, a proactive screening has been suggested in certain patient populations withfeatures of the disorder. However, conflicting data have been reported on the prevalence ofCushing’s syndrome in patients with type 2 diabetes.
Objective: Our aim was to evaluate the prevalence of unsuspected Cushing’s syndrome amongoutpatients with type 2 diabetes.
Design and Setting: This was a cross-sectional prospective study in 24 diabetes clinics across Italy.
Patients: Between June 2006 and April 2008, 813 patients with known type 2 diabetes withoutclinically overt hypercortisolism were evaluated. Follow-up of the study was closed in September2010. Patients were not selected for characteristics conferring a higher pretest probability ofhypercortisolism. Patients underwent a first screening step with the 1-mg overnight dexametha-sone suppression test.
Results: Forty patients failed to suppress serum cortisol less than 5.0 !g/dl (138 nmol/liter) andunderwent a standard 2-d, 2-mg dexamethasone suppression test, after which six patients (0.6%of the overall series) failed to suppress cortisol less than 1.8 !g/dl (50 nmol/liter), receiving adefinitive diagnosis of Cushing’s syndrome that was adrenal dependent in five patients. Fourpatients were cured, being able to discontinue, or reduce, the glucose-lowering agents.
Conclusions: The present data do not support widespread screening of patients with type 2 dia-betes for Cushing’s syndrome; however, the disorder is less rare than previously thought whenconsidering epidemiology of type 2 diabetes. Our results support a case-finding approach in pa-tients with uncontrolled diabetes and hypertension despite appropriate treatment. (J Clin Endo-crinol Metab 97: 3467–3475, 2012)
Subtle clinical presentations of Cushing’s syndrome,characterized by a paucity of signs and symptoms
due to mild cortisol hypersecretion, are increasinglyfound in clinical practice. In parallel, the metabolicsyndrome epidemic is leading to a boost in the numberof patients with a Cushingoid phenotype, who could
be potentially candidate to be tested for hypercortiso-lism (1).
The Endocrine Society guidelines for the diagnosis ofCushing’s syndrome recommended against widespreadtesting for the condition, unless in patients with unusualfeatures for age or multiple and progressive features, par-
ISSN Print 0021-972X ISSN Online 1945-7197Printed in U.S.A.Copyright © 2012 by The Endocrine Societydoi: 10.1210/jc.2012-1323 Received February 5, 2012. Accepted June 18, 2012.First Published Online July 5, 2012
*Author affiliations are shown at the bottom of the next pageAbbreviations: BMI, Body mass index; CT, computerized tomography; DST, dexametha-sone suppression test; HbA1c, glycosylated hemoglobin; HPA, hypothalamus-pituitary-adrenal; MRI, magnetic resonance imaging.
O R I G I N A L A R T I C L E
E n d o c r i n e C a r e
J Clin Endocrinol Metab, October 2012, 97(10):3467–3475 jcem.endojournals.org 3467
The Endocrine Society. Downloaded from press.endocrine.org by [${individualUser.displayName}] on 18 March 2014. at 05:28 For personal use only. No other uses without permission. . All rights reserved.ticularly those that are more predictive of Cushing’s syn-drome (2). However, unsuspected Cushing’s syndromewas found to be more frequent than previously expectedin different series of diabetic patients submitted to routinescreening (3–5). Thus, a number of patients with Cush-ing’s syndrome may not be recognized while they aremanaged for diabetes, either because of a mild clinicalpresentation or because of insufficient awareness of theirphysicians. Missing a diagnosis of Cushing’s syndromemay have detrimental consequences on patient outcomebecause hypercortisolism is expected to worsen metaboliccontrol and increases the probability of future cardiovas-cular events (6).
The results of the above-mentioned studies may arguein favor of a systematic screening of Cushing’s syn-drome in type 2 diabetes. However, data were mostly gen-erated in academic centers on hospitalized patients, thusraising the possibility of a selection bias toward patients atgreater risk of Cushing’s syndrome than the general dia-betic population (7).
The aim of our study was to screen patients attendingdiabetes clinics in an outpatient setting and in conditionsof standard clinical practice. Cohorts of consecutive pa-tients were enrolled in different Italian diabetes clinicsrather than selecting groups of patients at higher risk forCushing’s, i.e. those who were hypertensive or overweightand who had poor glycemic control.
Patients and Methods
PatientsThe study was conducted under the auspices of the Associa-
zione Medici Endocrinologi (Association of Clinical Endocri-nologists) at 24 diabetes clinics across Italy. Written informedconsent was obtained from all patients, and the institutionalreview board at each center approved the study. Each partici-pating center was requested to recruit consecutively at least 20diabetic patients fulfilling all inclusion criteria and without ex-
clusion criteria, who were attending the center for an ordinaryoutpatient visit from June 2006 to April 2008. Follow-up for thisstudy was closed in September 2010. Patients had to meet thefollowing inclusioncriteria: agebetween18and70yr, bodymassindex (BMI) greater than 25 kg/m2 and known diagnosis of type2 diabetes on active follow-up from at least 1 yr before the study.Exclusion criteria were presence of specific Cushingoid features[easy bruising, facial plethora, proximal myopathy and striae(2)], any severe acute illness, treatment with drugs known toaffect the hypothalamus-pituitary-adrenal (HPA) axis or dexa-methasone metabolism, current or previous history of alcoholabuse or major mood disorders that required psychiatric inter-vention, history of recent surgery or trauma, and pregnancy. Anysubject with a BMI greater than 30 kg/m2 was categorized asobese (8). Any subject with systolic blood pressure greater than140 mm Hg, diastolic blood pressure greater than 90 mm Hg, oron antihypertensive treatment was categorized as hypertensive(9). Dyslipidemia was defined following the Adult TreatmentPanel III criteria as follows: total cholesterol level greater than200 mg/dl, high-density lipoprotein cholesterol levels less than40 mg/dl, serum triglyceride levels greater than 150 mg/dl, andlow-density lipoprotein cholesterol levels greater than 160 mg/dl(10). Patients were also considered dyslipidemic if any specifictreatment was given. The main characteristics of the evaluatedpatients are shown in Table 1.
Medicina Interna I (M.T., G.R., B.Al., G.P.), Dipartimento di Scienze Cliniche e Biologiche, Azienda Ospedaliera Universitaria San Luigi Gonzaga, and Dipartimento di Scienze Cliniche eBiologiche (R.G.), Azienda Ospedaliera Universitaria San Luigi Gonzaga e Endocrinologia, Diabetologia, e Metabolismo, Azienda Ospedaliera Universitaria Molinette, Dipartimento diMedicina Interna, Universita di Torino, 10043 Torino, Italy; Dipartimento di Endocrinologia e Diabetologia (I.C.), Ospedale Maggiore Policlinico Instituto di Ricovero e Cura a CarattereScientifico, Divisione di Endocrinologia e Diabetologia (B.Am.), Dipartimento di Scienze Medico-Chirurgiche, Instituto di Ricovero e Cura a Carattere Scientifico Policlinico San Donato,Divisione di Endocrinologia e Diabetologia (M.A.), Dipartimento di Scienze Mediche, Ospedale San Giuseppe, Universita di Milano, 20122 Milano, Italy; Dipartimento di Medicina Generalee Endocrinologia (R.Ca.), Azienda Ospedaliera Universitaria Integrata Verona, Verona, Italy; SS Patologie Endocrine e Metaboliche (E.C.), Ospedale E. Valdese, 10138 Torino, Italy; StrutturaComplessa di Endocrinologia, Diabetologia e Malattie del Metabolismo (P.L.), Azienda Ospedaliera Ordine Mauriziano, 10125 Torino, Italy; Divisione di Endocrinologia, Dipartimento diMedicina Interna (C.C.), Ospedale Centrale di Bolzano, 39100 Bolzano, Italy; Dipartimento di Endocrinologia (I.M.), Ospedale S. Antonio Abate, 21013 Gallarate, Italy; Dipartimento diEndocrinologia (M.M.), Ospedali Riuniti di Bergamo, 24128 Bergamo, Italy; Dipartimento di Diabetologia (O.D.) and Dipartimento di Endocrinologia (R.Co.), Ospedale Niguarda, 20162Milano, Italy; Divisione di Endocrinologia (R.L.), Dipartimento di Medicina Interna e Specialistica, Instituto di Ricovero e Cura a Carattere Scientifico Fondazione Centro San Raffaele delMonte Tabor, 20132 Milano, Italy; Unità Operativa Semplice Endocrinologia (S.S.), AUSL Ravenna, 48100 Ravenna, Italy; Dipartimento di Malattie Metaboliche e Diabetologia (A.B.),Ospedale M. Bufalini, 47023 Cesena, Italy; Dipartimento di Endocrinologia (E.S., M.F.-F.), Ospedale Maggiore Bellaria, Bologna, Italy; Dipartimento di Medicina, Endocrinologia,Metabolismo, e Geriatria (B.M.), Nuovo Ospedale Civile S. Agostino-Estense di Baggiovara, 41100 Modena, Italy; Dipartimento di Medicina Generale (R.D.G.), Ospedale Ceccarini, 47900Riccione, Italy; Unità Operativa di Endocrinologia (F.S.), Istituto Nazionale di Ricovero e Cura per Anziani, Instituto di Ricovero e Cura a Carattere Scientifico, 00164 Roma, Italy; CentroDiabetologico Ospedale Santissima (R.B.), Trinita, Frosinone, Italy; Unità Operative Complessa Diabetologia (A.Sco.), Ospedale Civico Partinico, 90047 Palermo, Italy; Dipartimento diMalattie Metaboliche ed Endocrinologia (V.A.G.), Presidio Ospedaliero Monopoli-Conversano, 70043 Bari, Italy; Centro Catanese di Medicina e Chirurgia (D.C.), 95029 Catania, Italy;Dipartimento di Endocrinologia (A.Sci.), Ospedale “Casa Sollievo della Sofferenza,” Instituto di Ricovero e Cura a Carattere Scientifico, San Giovanni Rotondo, 71013 Italy; Dipartimentodi Endocrinologia (A.P., F.T., G.B.), Azienda Ospedaliera Santa Croce e Carle, 12100 Cuneo, Italy; Dipartimento di Endocrinologia e Malattie Metaboliche (R.R., E.P.), Ospedale ReginaApostolurum, 00041 Albano Laziale, Italy; and Dipartimento di Endocrinologia dell’Eta Evolutiva (P.G.), Ospedale Cervello, 90146 Palermo, Italy
TABLE 1. Main characteristics of the patients
VariableAge (yr) 58.9 ! 8.9BMI (kg/m2) 32.1 ! 6.1Duration of disease (yr) 9.8 ! 7.9Fasting glucose (mg/dl) 174.7 ! 67.7HbA1C (%) 8.4 ! 1.9Systolic blood pressure (mm Hg) 138.2 ! 17.2Diastolic blood pressure (mm Hg) 82.6 ! 10.1Total cholesterol (mg/dl) 186.9 ! 48.7HDL cholesterol (mg/dl) 45.9 ! 23.7LDL cholesterol (mg/dl) 106.9 ! 45.6Triglycerides (mg/dl) 171.2 ! 157.2
Data are expressed as mean values and SD. HDL, High-densitylipoprotein; LDL, low-density l;ipoprotein.
3468 Terzolo et al. Cushing’s Syndrome and Type 2 Diabetes J Clin Endocrinol Metab, October 2012, 97(10):3467–3475
The Endocrine Society. Downloaded from press.endocrine.org by [${individualUser.displayName}] on 18 March 2014. at 05:28 For personal use only. No other uses without permission. . All rights reserved.
Cushing probabile
Cushing improbabile

Falsi positivi
Falsi negativi
Falsi positivi
Falsi positivi

Arlt et al., 2011

UFC IN PATIENTS WITH CUSHING’S SYNDROME 6000
3500
1000
750
500
250
0
100
Cushing’s Disease n = 288
Adrenal Adenoma n = 80
Adrenal Carcinoma n = 25
Ectopic SecrePon n = 26
(% upper limit) Invitti et al., 1999

The Diagnosis of Cushing’s Syndrome:
An Endocrine Society Clinical Practice Guideline
GUIDELINESCLINICAL T h e E n d o c r i n e S o c i e t y ’ s
Authors: Lynnette K. Nieman, Beverly M. K. Biller, James W. Findling, John Newell-Price, Martin O. Savage,Paul M. Stewart, and Victor M. Montori
Affiliations: Program on Reproductive and Adult Endocrinology (L.K.N.), National Institute of Child Health andHuman Development, National Institutes of Health, Bethesda, Maryland 20892; NeuroendocrineUnit/Massachusetts General Hospital (B.M.K.B.), Boston, Massachusetts 02114; Medical College of Wisconsin(J.W.F.), Milwaukee, Wisconsin 53226; University of Sheffield (J.N.-P.), Sheffield S102JF, United Kingdom;William Harvey Research Institute, Queen Mary, University of London (M.O.S.), London EC1M6BQ, UnitedKingdom; University of Birmingham (P.M.S.), Birmingham B15 2TT, United Kingdom; and Mayo Clinic(V.M.M.), Rochester, Minnesota 55905
Co-Sponsoring Association: European Society of Endocrinology
Disclaimer Statement: Clinical practice guidelines are developed to be of assistance to physicians by providingguidance and recommendations for particular areas of practice. The guidelines should not be considered inclusiveof all proper approaches or methods, or exclusive of others. The guidelines cannot guarantee any specific outcome,nor do they establish a standard of care. The guidelines are not intended to dictate the treatment of a particularpatient. Treatment decisions must be made based on the independent judgment of health care providers and eachpatient's individual circumstances.
The Endocrine Society makes no warranty, express or implied, regarding the guidelines and specificallyexcludes any warranties of merchantability and fitness for a particular use or purpose. The Endocrine Society shallnot be liable for direct, indirect, special, incidental, or consequential damages related to the use of the informationcontained herein.
First published in the Journal of Clinical Endocrinology & Metabolism, May 2008, 93(5):1526–1540
© The Endocrine Society, 2008
Commercial Reprint InformationFor information on reprint requests of more than 101 and commercial reprints contact:
Heather EdwardsReprint Sales SpecialistCadmus Professional Communications
Phone: 410.691.6214Fax: 410.684.2789 Email: [email protected]
Single Reprint InformationFor information on reprints of 100 and fewer, complete the guideline order form and return using one of thefollowing methods:
Mail: The Endocrine Societyc/o Bank of AmericaP.O. Box 630721Baltimore, MD 21263-0736
Fax: 301.941.0257Email: [email protected]
Questions & CorrespondencesThe Endocrine SocietyAttn: Government & Public Affairs Department8401 Connecticut Avenue, Suite 900Chevy Chase, MD 20815
Phone: 301.941.0200Email: [email protected]: www.endo-society.org
For more information on The Endocrine Society’s Clinical Practice Guidelines or to download the completeversion of this guideline, visit http://www.endo-society.org/publications/guidelines/index.cfm.
MMTD07
THE
ENDO
CRIN
E SO
CIET
Y’S
CLIN
ICAL
GUI
DELI
NES
4
SUMMARY OF RECOMMENDATIONS
3.0. DIAGNOSIS OF CUSHING’S SYNDROME
Who should be tested3.1. We recommend obtaining a thorough drug history toexclude excessive exogenous glucocorticoid exposure leadingto iatrogenic Cushing’s syndrome before conductingbiochemical testing (1| ).
3.2. We recommend testing for Cushing’s syndrome in thefollowing groups:• Patients with unusual features for age (e.g. osteoporosis,
hypertension) (Table 1) (1| )• Patients with multiple and progressive features,
particularly those who are more predictive of Cushing’ssyndrome (Table 1) (1| )
• Children with decreasing height percentile and increasingweight (1| )
• Patients with adrenal incidentaloma compatible withadenoma (1| ).
3.3. We recommend against widespread testing for Cushing’ssyndrome in any other patient group (1| ).
Initial testing3.4. For the initial testing for Cushing’s syndrome, werecommend one of the following tests based on its suitabilityfor a given patient (Fig. 1) (1| ):
3.4.1. Urine free cortisol (UFC; at least two measurements)3.4.2. Late-night salivary cortisol (two measurements)3.4.3. 1-mg overnight dexamethasone suppression test
(DST)3.4.4. Longer low-dose DST (2 mg/d for 48 h)
3.5. We recommend against the use of the following to test forCushing’s syndrome (1| ):• Random serum cortisol or plasma ACTH levels• Urinary 17-ketosteroids• Insulin tolerance test• Loperamide test• Tests designed to determine the cause of Cushing’s
syndrome (e.g. pituitary and adrenal imaging, 8 mg DST).
3.6. In individuals with normal test results in whom thepretest probability is high (patients with clinical featuressuggestive of Cushing’s syndrome and adrenal incidentalomaor suspected cyclic hypercortisolism), we recommend furtherevaluation by an endocrinologist to confirm or exclude thediagnosis (1| ).
3.7. In other individuals with normal test results (in whomCushing’s syndrome is very unlikely), we suggest reevaluationin 6 months if signs or symptoms progress (2| ).
3.8. In individuals with at least one abnormal test result (forwhom the results could be falsely positive or indicateCushing’s syndrome), we recommend further evaluation by anendocrinologist to confirm or exclude the diagnosis(1| ).
Subsequent evaluation3.9. For the subsequent evaluation of abnormal initial testresults, we recommend performing another recommended test(Fig. 1, 1| ).
3.9.1. We suggest the additional use of the dexamethasone-CRH test or the midnight serum cortisol test in specificsituations (Fig. 1, 1| ).
3.9.2. We suggest against the use of the desmopressintest, except in research studies, until additional data validateits utility (2| ).
3.9.3. We recommend against any further testing forCushing’s syndrome in individuals with concordantly negativeresults on two different tests (except in patients suspected ofhaving the very rare case of cyclical disease) (1| ).
3.9.4. We recommend tests to establish the cause ofCushing’s syndrome in patients with concordantly positiveresults from two different tests, provided there is no concernregarding possible non-Cushing’s hypercortisolism (Table 2)(1| ).
3.9.5. We suggest further evaluation and follow-up forthe few patients with concordantly negative results who aresuspected of having cyclical disease and also for patients withdiscordant results, especially if the pretest probability ofCushing’s syndrome is high (2| ).
4.0. SPECIAL POPULATIONS/CONSIDERATIONS
4.1. Pregnancy: We recommend the use of UFC and againstthe use of dexamethasone testing in the initial evaluation ofpregnant women (1| ).
4.2. Epilepsy: We recommend against the use ofdexamethasone testing in patients receiving antiepilepticdrugs known to enhance dexamethasone clearance andrecommend instead measurements of nonsuppressed cortisolin blood, saliva, or urine (1| ).
4.3. Renal failure: We suggest using the 1-mg overnight DSTrather than UFC for initial testing for Cushing’s syndrome inpatients with severe renal failure (2| ).
4.4. Cyclic Cushing’s syndrome: We suggest use of UFC ormidnight salivary cortisol tests rather than DSTs in patientssuspected of having cyclic Cushing’s syndrome (2| ).
4.5. Adrenal incidentaloma: We suggest use of the 1-mg DSTor late-night cortisol test, rather than UFC, in patientssuspected of having mild Cushing’s syndrome (2| ).

- cortisolo libero urinario ( x 2 volte; escludere interferenze)
- cortisolo salivare/sierico alle h 23-h24
- DST 1 mg / 2 mg (cut – off variabile)
- test al CRH / CRH-DST / CRH-Desmopressina
DIAGNOSI di SINDROME di CUSHING
- DST 8 mg
- cortisolo salivare/sierico (< 2 mcg/dl) alle h8 - Test ACTH
NEL POSTINTERVENTO
DURANTE TERAPIA FARMACOLOGICA
- cortisolo libero urinario
remissione
recidiva
- cortisolo libero urinario - cortisolo salivare/sierico alle h 23-h24 - cortisolo sierico dopo DST
- cortisolo salivare/sierico alle h24 - cortisolo sierico dopo DST
- cortisolo libero urinario
Scegliere il test più ada`o alla situazione
clinica in esame, eventualmente
ripetendolo, secondo le disponibilità locali

The Diagnosis of Cushing’s Syndrome:
An Endocrine Society Clinical Practice Guideline
GUIDELINESCLINICAL T h e E n d o c r i n e S o c i e t y ’ s
Authors: Lynnette K. Nieman, Beverly M. K. Biller, James W. Findling, John Newell-Price, Martin O. Savage,Paul M. Stewart, and Victor M. Montori
Affiliations: Program on Reproductive and Adult Endocrinology (L.K.N.), National Institute of Child Health andHuman Development, National Institutes of Health, Bethesda, Maryland 20892; NeuroendocrineUnit/Massachusetts General Hospital (B.M.K.B.), Boston, Massachusetts 02114; Medical College of Wisconsin(J.W.F.), Milwaukee, Wisconsin 53226; University of Sheffield (J.N.-P.), Sheffield S102JF, United Kingdom;William Harvey Research Institute, Queen Mary, University of London (M.O.S.), London EC1M6BQ, UnitedKingdom; University of Birmingham (P.M.S.), Birmingham B15 2TT, United Kingdom; and Mayo Clinic(V.M.M.), Rochester, Minnesota 55905
Co-Sponsoring Association: European Society of Endocrinology
Disclaimer Statement: Clinical practice guidelines are developed to be of assistance to physicians by providingguidance and recommendations for particular areas of practice. The guidelines should not be considered inclusiveof all proper approaches or methods, or exclusive of others. The guidelines cannot guarantee any specific outcome,nor do they establish a standard of care. The guidelines are not intended to dictate the treatment of a particularpatient. Treatment decisions must be made based on the independent judgment of health care providers and eachpatient's individual circumstances.
The Endocrine Society makes no warranty, express or implied, regarding the guidelines and specificallyexcludes any warranties of merchantability and fitness for a particular use or purpose. The Endocrine Society shallnot be liable for direct, indirect, special, incidental, or consequential damages related to the use of the informationcontained herein.
First published in the Journal of Clinical Endocrinology & Metabolism, May 2008, 93(5):1526–1540
© The Endocrine Society, 2008
Commercial Reprint InformationFor information on reprint requests of more than 101 and commercial reprints contact:
Heather EdwardsReprint Sales SpecialistCadmus Professional Communications
Phone: 410.691.6214Fax: 410.684.2789 Email: [email protected]
Single Reprint InformationFor information on reprints of 100 and fewer, complete the guideline order form and return using one of thefollowing methods:
Mail: The Endocrine Societyc/o Bank of AmericaP.O. Box 630721Baltimore, MD 21263-0736
Fax: 301.941.0257Email: [email protected]
Questions & CorrespondencesThe Endocrine SocietyAttn: Government & Public Affairs Department8401 Connecticut Avenue, Suite 900Chevy Chase, MD 20815
Phone: 301.941.0200Email: [email protected]: www.endo-society.org
For more information on The Endocrine Society’s Clinical Practice Guidelines or to download the completeversion of this guideline, visit http://www.endo-society.org/publications/guidelines/index.cfm.
MMTD07
particularly in patients with very mild disease in whomthe benefits of intervention are unproven. Conversely,once the clinical scenario suggests a high pretestprobability of the disorder, sensitivity needs to be highso that cases are not missed. This approach also seeksto use more convenient and less expensive tests.
Initial testing3.4. For the initial testing for Cushing’s syndrome, werecommend one of the following tests based on itssuitability for a given patient (Fig. 1) (1| ):
3.4.1. UFC (at least two measurements)3.4.2. Late-night salivary cortisol (two measurements)3.4.3. 1-mg overnight DST3.4.4. Longer low-dose DST (2 mg/d for 48 h)
THE
ENDO
CRIN
E SO
CIET
Y’S
CLIN
ICAL
GUI
DELI
NES
10
3.5. We recommend against the use of the followingto test for Cushing’s syndrome (1| ):• Random serum cortisol or plasma ACTH levels• Urinary 17-ketosteroids• Insulin tolerance test• Loperamide test• Tests designed to determine the cause of Cushing’s
syndrome (e.g. pituitary and adrenal imaging, 8 mg DST).
3.6. In individuals with normal test results in whomthe pretest probability is high (patients with clinicalfeatures suggestive of Cushing’s syndrome and adrenal incidentaloma or suspected cyclic hyper-cortisolism), we recommend further evaluation by anendocrinologist to confirm or exclude the diagnosis(1| ).
Cushing’s syndrome suspected(consider endocrinological consultation)
Exclude exogenous glucocorticoid exposure
Perform one of the following tests
ANY ABNORMAL RESULT Normal (CS unlikely)
Consult endocrinologist
Perform 1 or 2 other studies shown above
Suggest consider repeating the abnormal studySuggest Dex-CRH or midnight serum cortisol in certain populations (see text)
Discrepant ABNORMAL Normal (CS unlikely)(Suggest additional evaluation)
Cushing’s syndrome
Exclude physiologic causes of hypercortisolism (Table 2)
24-h UFC (≥2 tests) Overnight Late-night salivary1-mg DST cortisol (≥2 tests)
Consider caveats for each test (see text)Use 48-h, 2-mg DST in certain populations (see text)
Figure 1. Algorithm for testing patients suspected of having Cushing’s syndrome (CS). All statements are recommendations except forthose prefaced by suggest. Diagnostic criteria that suggest Cushing’s syndrome are UFC greater than the normal range for the assay,serum cortisol greater than 1.8 µg/dl (50 nmol/liter) after 1 mg dexamethasone (1-mg DST), and late-night salivary cortisol greater than145 ng/dl (4 nmol/liter).

Terapia Farmacologica: quando e cosa ?