
Sara Mazzucco e Gianni Bioloˆ una condizione caratterizzata da perdita di massa e forza muscolare...
39
X-FILES IN NUTRIZIONE CLINICA ED ARTIFICIALE ONCOLOGIA E NUTRIZIONE, DALLA PREVENZIONE ALLA TERAPIA Centro Internazionale di Studi Fondazione Germana Gaslini Genova, 7-8 Giugno 2012 Targeting: fabbisogno di amino acidi ed attività motoria nella sarcopenia cancro-correlata Sara Mazzucco e Gianni Biolo Dipartimento di Scienze Mediche, Chirurgiche e della Salute Clinica Medica Università di Trieste
Transcript of Sara Mazzucco e Gianni Bioloˆ una condizione caratterizzata da perdita di massa e forza muscolare...

X-FILES IN NUTRIZIONE CLINICA ED ARTIFICIALE ONCOLOGIA E NUTRIZIONE, DALLA PREVENZIONE ALLA TERAPIA
Centro Internazionale di Studi Fondazione Germana Gaslini
Genova, 7-8 Giugno 2012
Targeting: fabbisogno di amino acidi ed attività motoria nella sarcopenia cancro-correlata
Sara Mazzucco e Gianni Biolo
Dipartimento di Scienze Mediche, Chirurgiche e della Salute Clinica Medica
Università di Trieste

È una condizione caratterizzata da perdita di massa e forza muscolare
SARCOPENIA: sarx (carne) + penia (perdita)
• Perdita di funzionalità muscolare • Aumento incidenza di cadute • Aumento ospedalizzazione • Perdita di autonomia

È una condizione caratterizzata da perdita di massa e forza muscolare
SARCOPENIA: sarx (carne) + penia (perdita)
DEGRADAZIONE PROTEICA
↑ sistemi di degradazione proteici
SINTESI PROTEICA
↓ sensibilità anabolica
↑ sintesi proteine della fase acuta
Acharyya & Guttridge, Clin Cancer Res 2007; Tisdale, Physiol Rev. 2009
• Perdita di funzionalità muscolare • Aumento incidenza di cadute • Aumento ospedalizzazione • Perdita di autonomia

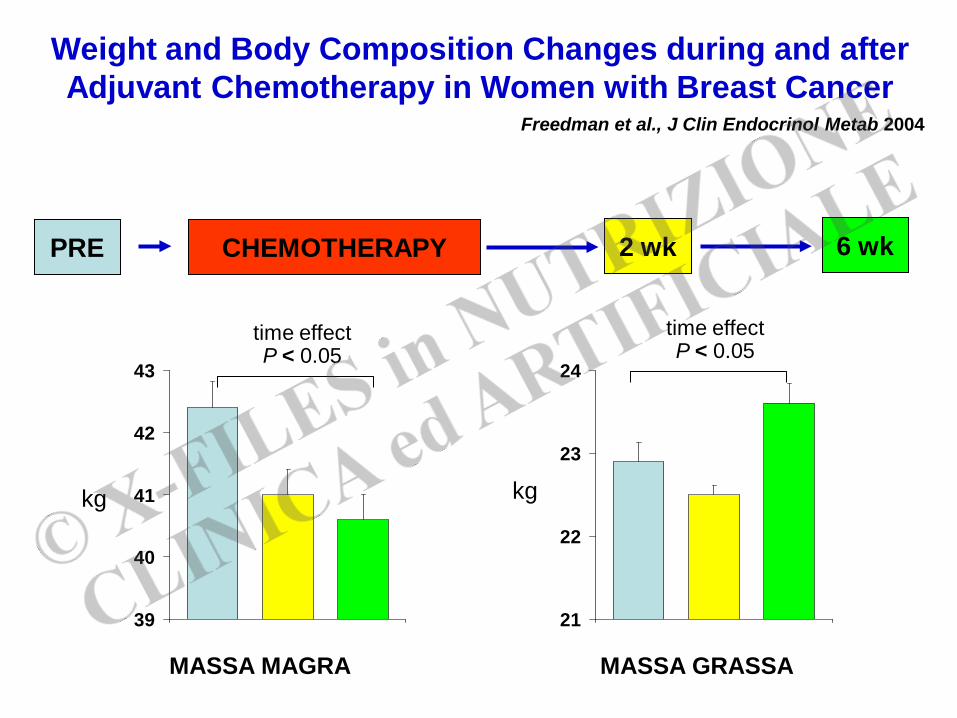
Weight and Body Composition Changes during and after Adjuvant Chemotherapy in Women with Breast Cancer
Freedman et al., J Clin Endocrinol Metab 2004
CHEMOTHERAPY PRE 2 wk 6 wk
MASSA MAGRA
39
40
41
42
43
21
22
23
24
kg kg
time effect P < 0.05
time effect P < 0.05
MASSA GRASSA

2115 cancer patients
15% obesity
15% sarcopenic obesity
SURVIVAL
Prevalence and clinical implications of sarcopenic obesity in patients with solid tumours of the respiratory and gastrointestinal tracts: a population-based study. Prado et al., Lancet Oncol 2008
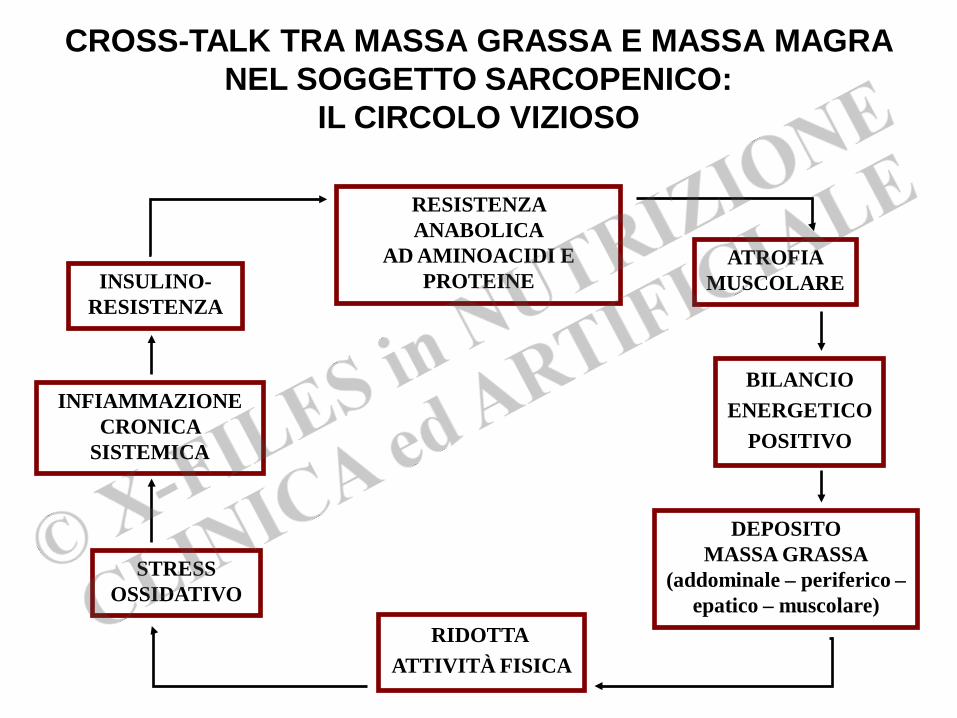
RESISTENZA ANABOLICA
AD AMINOACIDI E PROTEINE
BILANCIO ENERGETICO
POSITIVO
INFIAMMAZIONE CRONICA
SISTEMICA
RIDOTTA ATTIVITÀ FISICA
CROSS-TALK TRA MASSA GRASSA E MASSA MAGRA NEL SOGGETTO SARCOPENICO:
IL CIRCOLO VIZIOSO
ATROFIA MUSCOLARE INSULINO-
RESISTENZA
DEPOSITO MASSA GRASSA
(addominale – periferico – epatico – muscolare)
STRESS OSSIDATIVO
RUOLO DEL BILANCIO ENERGETICO:
1. EFFETTI DEL BILANCIO ENERGETICO POSITIVO
2. EFFETTI DEL BILANCIO ENERGETICO NEGATIVO
TRATTAMENTO DELLA RESISTENZA ANABOLICA:
1. EFFETTI DI UNA DIETA IPERPROTEICA
2. EFFETTI DI UNA COSTANTE ATTIVITÀ FISICA
3. EFFETTI COMBINATI DI DIETA IPERPROTEICA E UNA COSTANTE ATTIVITÀ FISICA
RUOLO DEI NUTRIENTI FUNZIONALI
SARCOPENIA CANCRO-CORRELATA
Weight and Body Composition Changes during and after Adjuvant Chemotherapy in Women with Breast Cancer
Freedman et al., J Clin Endocrinol Metab 2004
CHEMOTHERAPY PRE 2 wk 6 wk
MASSA MAGRA
39
40
41
42
43
21
22
23
24
kg kg
time effect P < 0.05
time effect P < 0.05
MASSA GRASSA

5000
5250
5500
5750
6000 time effect P = 0.02.
RMR
REDUCED ENERGY NEEDS WITH CHEMOTHERAPY
PHYSICAL ACTIVITY
ENERGY INTAKE
(kJ/
d)
Reduced rates of metabolism and decreased physical activity in breast cancer patients receiving adjuvant chemotherapy.
Demark-Wahnefried et al., Am J Clin Nutr. 1997

Variazioni di massa GRASSA (bioimpedenza)
Bilancio energetico positivo
Bilancio energetico neutro
Variazioni dello spessore vastus lateralis
(ecografia)
*, p<0.05 statisticamente diverso da zero; §, p<0.05 versus bilancio energetico neutro
∆ (c
m)
∆ (k
g)
-5
-4
-3
-2
-1
0
*§
*
-0,5
-0,4
-0,3
-0,2
-0,1
0
*§
0
1
2
3 * §
∆ (k
g)
Variazioni di massa MAGRA (bioimpedenza)
Positive energy balance is associated with accelerated muscle atrophy and increased erythrocyte glutathione turnover during 5 wk of bed rest
Biolo et al., Am J Clin Nutr. 2008
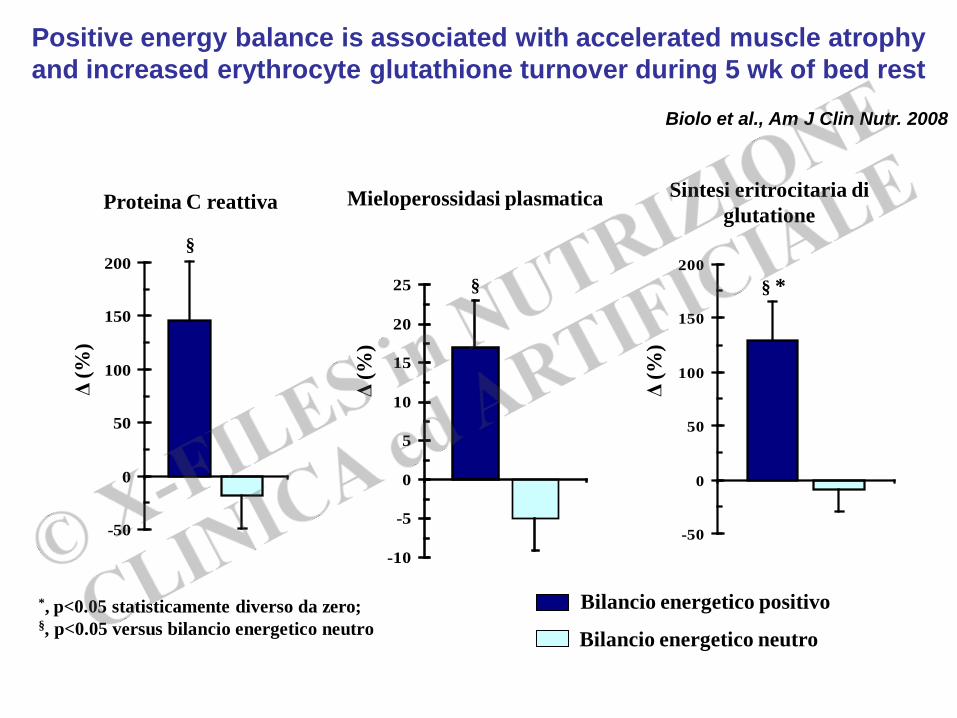
Bilancio energetico positivo
Bilancio energetico neutro
*, p<0.05 statisticamente diverso da zero; §, p<0.05 versus bilancio energetico neutro
Δ (%
)
Δ (%
)
Proteina C reattiva Mieloperossidasi plasmatica Sintesi eritrocitaria di glutatione
Δ (%
)
-50
0
50
100
150
200§
-10
-5
0
5
10
15
20
25 §
-50
0
50
100
150
200§ *
Positive energy balance is associated with accelerated muscle atrophy and increased erythrocyte glutathione turnover during 5 wk of bed rest
Biolo et al., Am J Clin Nutr. 2008
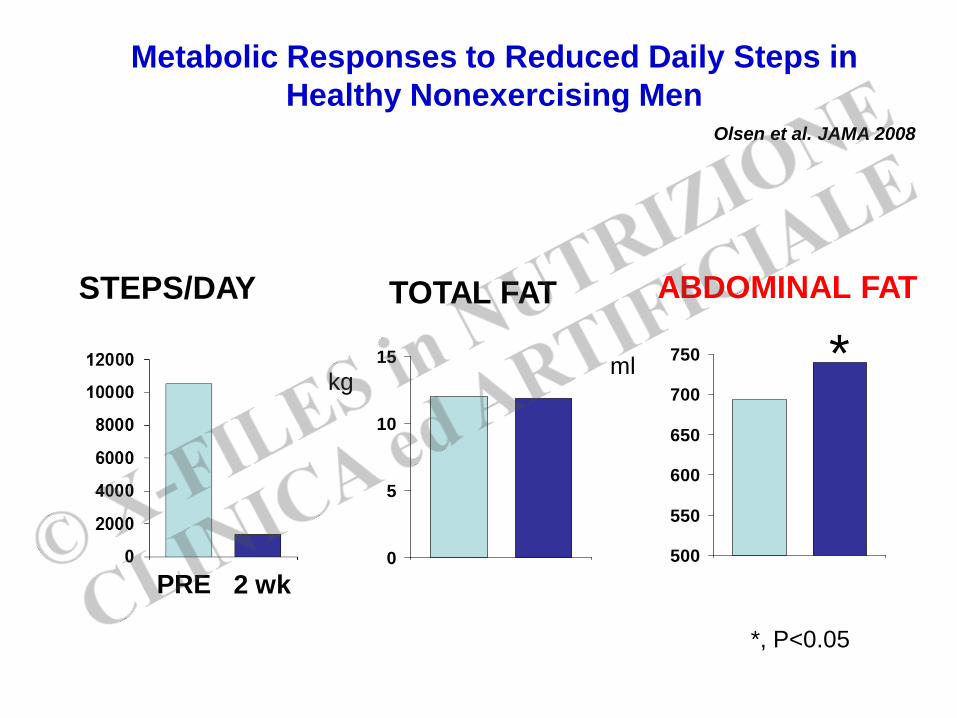
0
5
10
15
500
550
600
650
700
750
STEPS/DAY TOTAL FAT ABDOMINAL FAT
kg ml *
*, P<0.05
Metabolic Responses to Reduced Daily Steps in Healthy Nonexercising Men
Olsen et al. JAMA 2008
2 wk PRE

Calorie restriction accelerates the catabolism of lean body mass during 2 wk of bed rest
Biolo et al., Am J Clin Nutr 2007
-1,4
-1
-0,6
-0,2
0,2
a,b,c
Deambulazione
Bed rest sperimentale
Δ m
assa
mag
ra (D
EXA
) (k
g)
Bilancio energetico NEGATIVO
Bilancio energetico NEUTRO
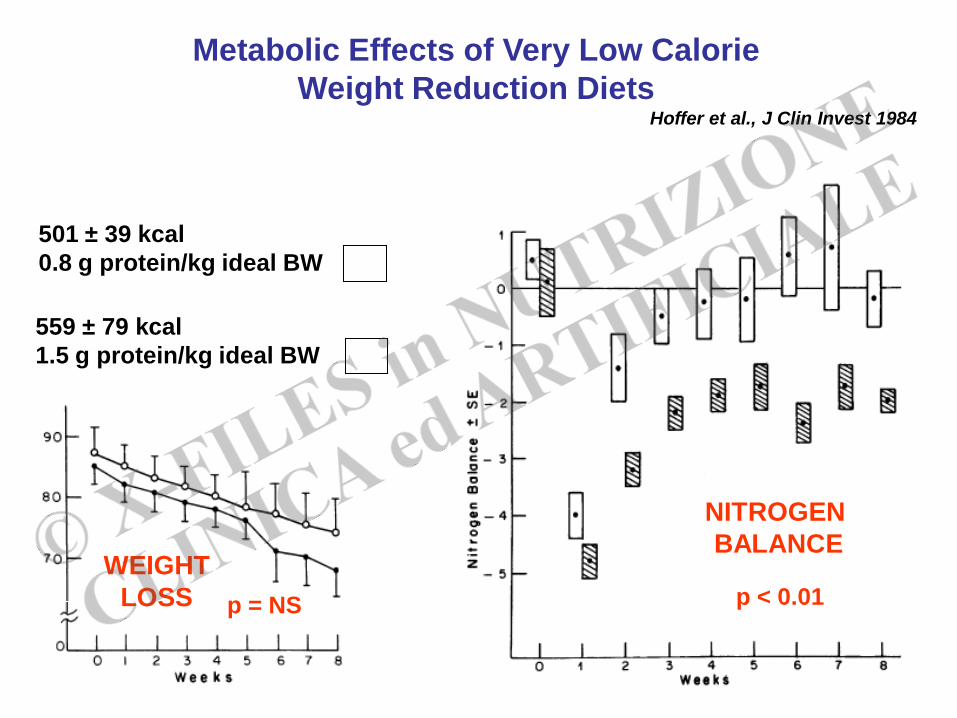
501 ± 39 kcal 0.8 g protein/kg ideal BW
559 ± 79 kcal 1.5 g protein/kg ideal BW
WEIGHT LOSS p = NS p < 0.01
NITROGEN BALANCE
Metabolic Effects of Very Low Calorie Weight Reduction Diets
Hoffer et al., J Clin Invest 1984

BILANCIO ENERGETICO POSITIVO ACCELERA L’ATROFIA MUSCOLARE PER AUMENTO DI STRESS OSSIDATIVO E ATTIVAZIONE DELLA FLOGOSI
BILANCIO ENERGETICO NEGATIVO ACCELERA L’ATROFIA MUSCOLARE
RESTRIZIONE CALORICA DEVE ESSERE ASSOCIATA AD
1. AUMENTO INTROITO PROTEICO
2. IDONEO PROGRAMMA DI ESERCIZIO FISICO
CONCLUSIONE (I)

Effects of amino acid infusion on skeletal muscle protein balance in severely burned patients
Biolo & Wolfe, Clinical Nutrition (abstract) 2001
-80
0
80
feni
lala
nina
(nm
ol/m
in/1
00 m
l)
Digiuno Infusione aminoacidi
*
Volontari sani
Pazienti ustionati
*, P<0.05 vs. digiuno #, P<0.05 vs. volontari sani
*#
#
BIL
AN
CIO
PR
OTE
ICO
MU
SCO
LAR
E
RESISTENZA ANABOLICA: ruolo dell’infiammazione

Short-term bed rest impairs amino acid-induced protein anabolism in humans
Biolo et al., J Physiol 2004
*
*, P<0.05 vs. ambulatory condition
*#
#
RESISTENZA ANABOLICA: ruolo dell’inattività fisica

Inactivity amplifies the catabolic response of skeletal muscle to cortisol
Ferrando et al., J Clin Endocrinol & Metab, 1999
Bed rest 14-days
Ambulatory 5-days
12-h hydrocortisone infusion (120 microg/kg/h)
-75
-50
-25
0
nmol
phe
nyla
lani
ne/
/min
/100
ml l
eg v
ol.
MUSCLE PROTEIN BALANCE
Activity Inactivity
P<0.05
RESISTENZA ANABOLICA: ruolo combinato di infiammazione ed inattività fisica
NUTRIZIONE ENTERALE NEL TRATTAMENTO DELLA SARCOPENIA CANCRO-CORRELATA:
LINEE GUIDA – FABBISOGNO PROTEICO

… …

NUTRIZIONE ENTERALE NEL TRATTAMENTO DELLA SARCOPENIA CANCRO-CORRELATA:
LINEE GUIDA

PROTEIN REQUIREMENT IN CRITICAL ILLNESS AT ADEQUATE ENERGY INTAKE
Wolfe et al., Ann Surg 1983; Ishibashi et al., Crit Care Med 1998 Hoffer Am J Clin Nutr 2003
200
130
80 45
PROTEIN REQUIREMENT IN CRITICAL ILLNESS AT ADEQUATE ENERGY INTAKE
Wolfe et al., Ann Surg 1983; Ishibashi et al., Crit Care Med 1998 Hoffer Am J Clin Nutr 2003
-2
-1.5
-1
-0.5
0
Who
le-b
ody
prot
ein
loss
(k
g / 2
wee
ks)
-2
-1.5
-1
-0.5
0
Who
le-b
ody
prot
ein
loss
(k
g / 2
wee
ks)
g protein / kg IBW per day
≈ 1.5 ≈ 2.2
200
130
80 45
≈ 0.7 ≈ 1.0
Non-protein calories – to – nitrogen ratio

Muscle protein synthesis in cancer patients can be stimulated with a specially formulated medical food
Deutz et al., Clinical Nutrition 2011
*
*, compared to postabsorptive state
Design: Randomized, controlled, double-blind, parallel-group design 25 patients with cancer. Experimental group (EXP, n=13): 40 g proteins (casein + whey protein) and enriched with 10% free leucine. Control group (n=12): casein protein (24 g). Conclusions: In cancer patients, conventional nutritional supplementation is ineffective in stimulating muscle protein synthesis. This anabolic resistance can be overcome with a specially formulated nutritional supplement.
Objective: Maintenance of muscle mass is crucial to improving outcome and quality of life in cancer patients. Stimulating muscle protein synthesis is the metabolic basis for maintaining muscle mass, but in cancer patients normal dietary intake has minimal effects on muscle protein synthesis.
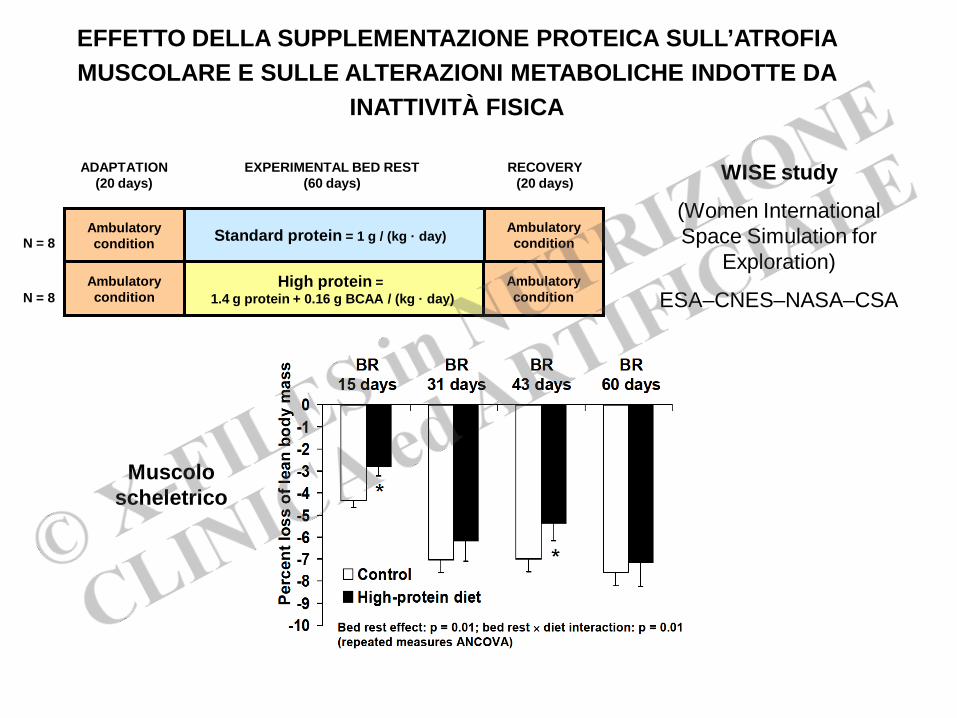
WISE study
(Women International Space Simulation for
Exploration)
ESA–CNES–NASA–CSA
EFFETTO DELLA SUPPLEMENTAZIONE PROTEICA SULL’ATROFIA MUSCOLARE E SULLE ALTERAZIONI METABOLICHE INDOTTE DA
INATTIVITÀ FISICA
Muscolo scheletrico
RECOVERY (20 days)
ADAPTATION (20 days)
EXPERIMENTAL BED REST (60 days)
N = 8
N = 8
Standard protein = 1 g / (kg · day) Ambulatory condition
High protein = 1.4 g protein + 0.16 g BCAA / (kg · day)
Ambulatory condition
Ambulatory condition
Ambulatory condition

EFFETTO DELLA SUPPLEMENTAZIONE PROTEICA SULL’ATROFIA MUSCOLARE E SULLE ALTERAZIONI METABOLICHE INDOTTE DA
INATTIVITÀ FISICA
Mus
colo
ca
rdia
co
WISE

WISE study
(Women International Space Simulation for
Exploration)
ESA–CNES–NASA–CSA
EFFETTO DELLA SUPPLEMENTAZIONE PROTEICA SULL’ATROFIA MUSCOLARE E SULLE ALTERAZIONI METABOLICHE INDOTTE DA
INATTIVITÀ FISICA
Sensibilità insulinica
RECOVERY (20 days)
ADAPTATION (20 days)
EXPERIMENTAL BED REST (60 days)
N = 8
N = 8
Standard protein = 1 g / (kg · day) Ambulatory condition
High protein = 1.4 g protein + 0.16 g BCAA / (kg · day)
Ambulatory condition
Ambulatory condition
Ambulatory condition
basale 60 gg bed rest

American Cancer Society Guidelines 2006
LINEE GUIDA – ATTIVITÀ FISICA
…
…
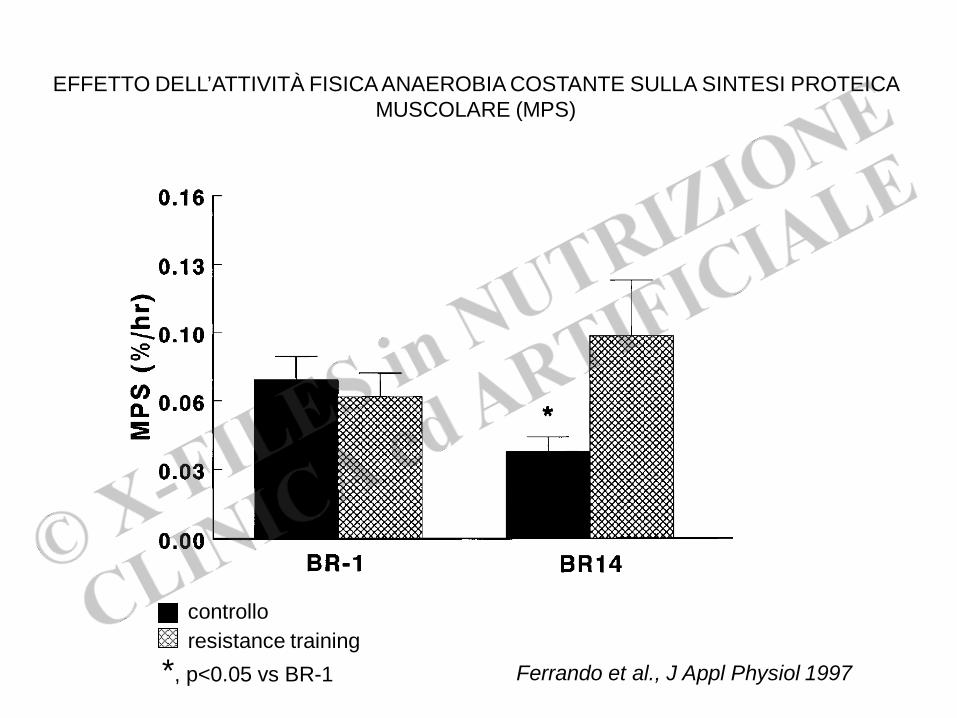
Ferrando et al., J Appl Physiol 1997
EFFETTO DELL’ATTIVITÀ FISICA ANAEROBIA COSTANTE SULLA SINTESI PROTEICA MUSCOLARE (MPS)
controllo resistance training
*, p<0.05 vs BR-1

Recreational Physical Activity and the Risk of Breast Cancer in Postmenopausal Women The Women’s Health
Initiative Cohort Study Mc Tiernan et al., JAMA 2003
Conclusions These data suggest that increased physical activity is associated with reduced risk for breast cancer in postmenopausal women, longer duration provides most benefit, and that such activity need not be strenuous.
Design Prospective cohort study in 74171 women aged 50 to 79 years

Effects of Aerobic and Resistance Exercise in Breast Cancer Patients Receiving Adjuvant Chemotherapy: A Multicenter
Randomized Controlled Trial Courneya et al., J Clin Oncol 2007
Purpose Breast cancer chemotherapy may cause unfavorable changes in physical functioning, body composition, psychosocial functioning, and quality of life (QOL). We evaluated the relative merits of aerobic and resistance exercise in blunting these effects. Patients and Methods Multicenter randomized controlled trial in Canada between 2003 and 2005 that randomly assigned 242 breast cancer patients initiating adjuvant chemotherapy to usual care (n 82), supervised resistance exercise (n 82), or supervised aerobic exercise (n 78) for the duration of their chemotherapy (median, 17 weeks). Results The follow-up assessment rate for our primary end point was 92.1%, and adherence to the supervised exercise was 70.2%. Aerobic exercise was superior to usual care for improving self-esteem (P= .015), aerobic fitness (P= .006), and percent body fat (adjusted P=.076). Resistance exercise was superior to usual care for improving self-esteem (P .018), muscular strength (P= .001), lean body mass (P= .015), and chemotherapy completion rate (P= .033). Exercise did not cause lymphedema or adverse events. Conclusion Neither aerobic nor resistance exercise significantly improved cancer-specific quality of life in breast cancer patients receiving chemotherapy, but they did improve self-esteem, physical fitness, body composition, and chemotherapy completion rate without causing lymphedema or significant adverse events.
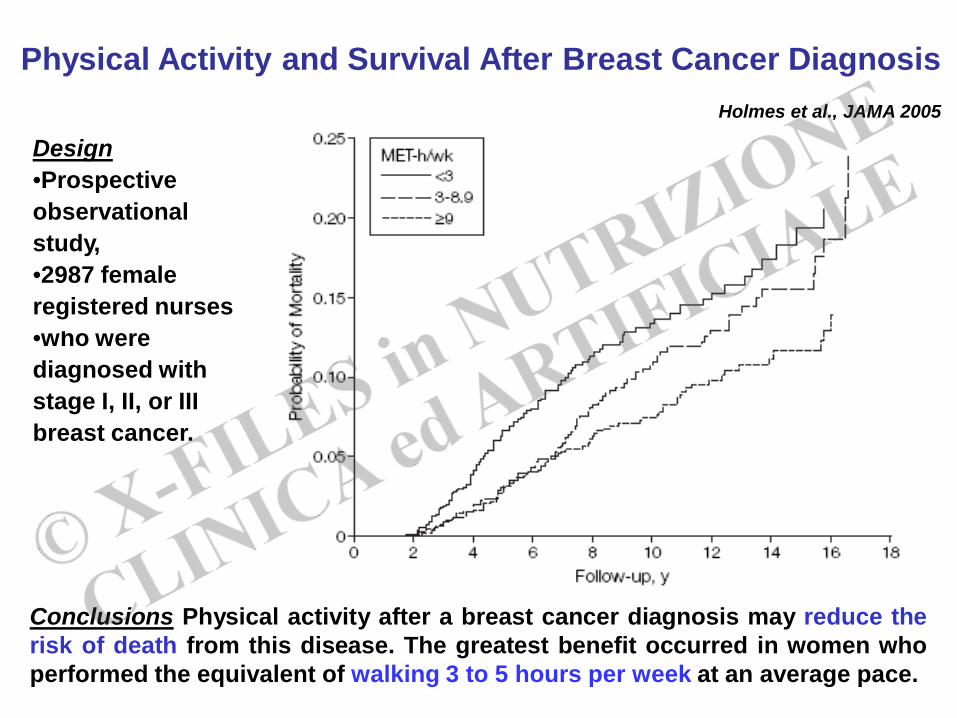
Physical Activity and Survival After Breast Cancer Diagnosis
Holmes et al., JAMA 2005
Conclusions Physical activity after a breast cancer diagnosis may reduce the risk of death from this disease. The greatest benefit occurred in women who performed the equivalent of walking 3 to 5 hours per week at an average pace.
Design •Prospective observational study, •2987 female registered nurses •who were diagnosed with stage I, II, or III breast cancer.
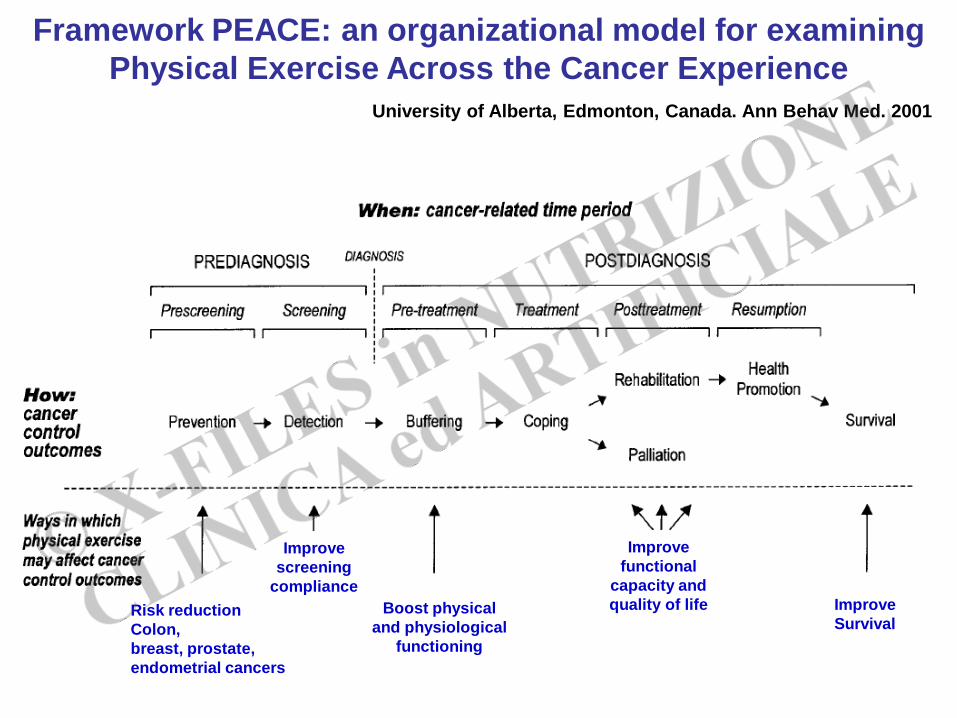
Framework PEACE: an organizational model for examining Physical Exercise Across the Cancer Experience
University of Alberta, Edmonton, Canada. Ann Behav Med. 2001
Risk reduction Colon, breast, prostate, endometrial cancers
Improve screening
compliance Boost physical
and physiological functioning
Improve functional
capacity and quality of life Improve
Survival

Adjusting for covariates (age at inclusion, BMI at inclusion, and BMD of the femoral neck at inclusion) a significant (P < 0.05) difference was seen in the response to training of bone mineral density between the two groups.
Strength improvements from 6 to 24 wk, a significant difference was apparent between groups: nutrient group, 9±3% vs. control, 1±2% (P < 0.05).
Protein-containing nutrient supplementation following
strength training enhances the effect on muscle mass,
strength, and bone formation in postmenopausal women
Holm et al., J Appl Physiol 2008

Timing of postexercise protein intake is important for muscle hypertrophy with resistance training in elderly humans
Esmarck et al., J Physiol 2001

FATTORI CHIAVE NELLO SVILUPPO DI RESISTENZA ANABOLICA SONO:
1. ATTIVAZIONE FLOGOSI
2. DIMINUZIONE DELL’ATTIVITÀ FISICA
FABBISOGNO PROTEICO AUMENTA: MINIMO 1.2 g/kg/die
ATTIVITÀ FISICA È ANABOLICA DI PER SE E MIGLIORA L’EFFETTO ANABOLICO DELLA SUPPLEMENTAZIONE PROTEICA
CONCLUSIONI (II)
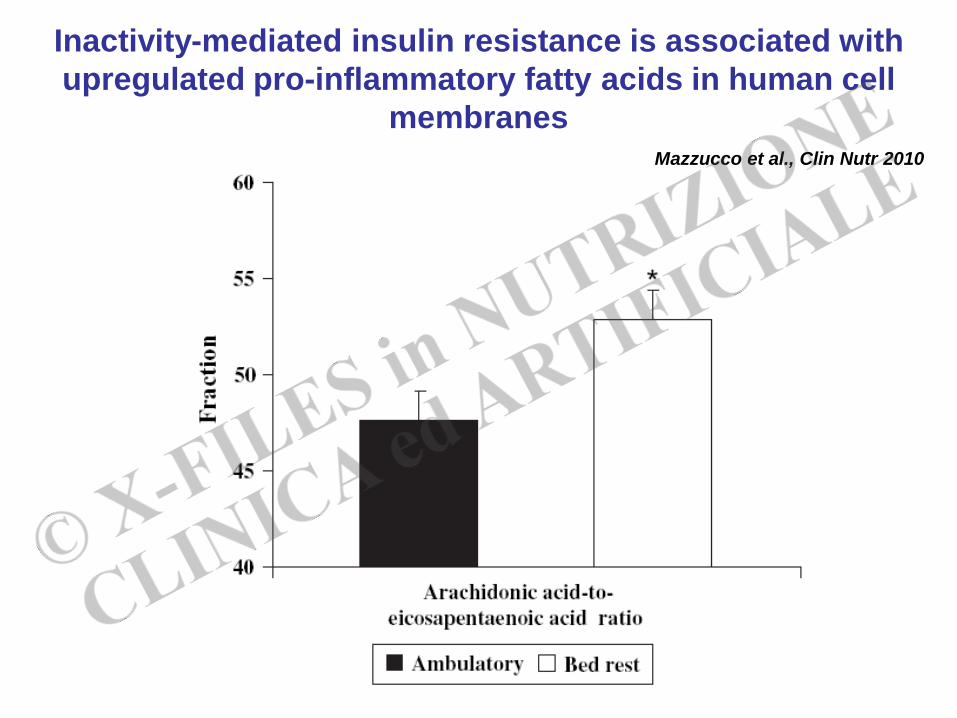
*
Inactivity-mediated insulin resistance is associated with upregulated pro-inflammatory fatty acids in human cell
membranes Mazzucco et al., Clin Nutr 2010
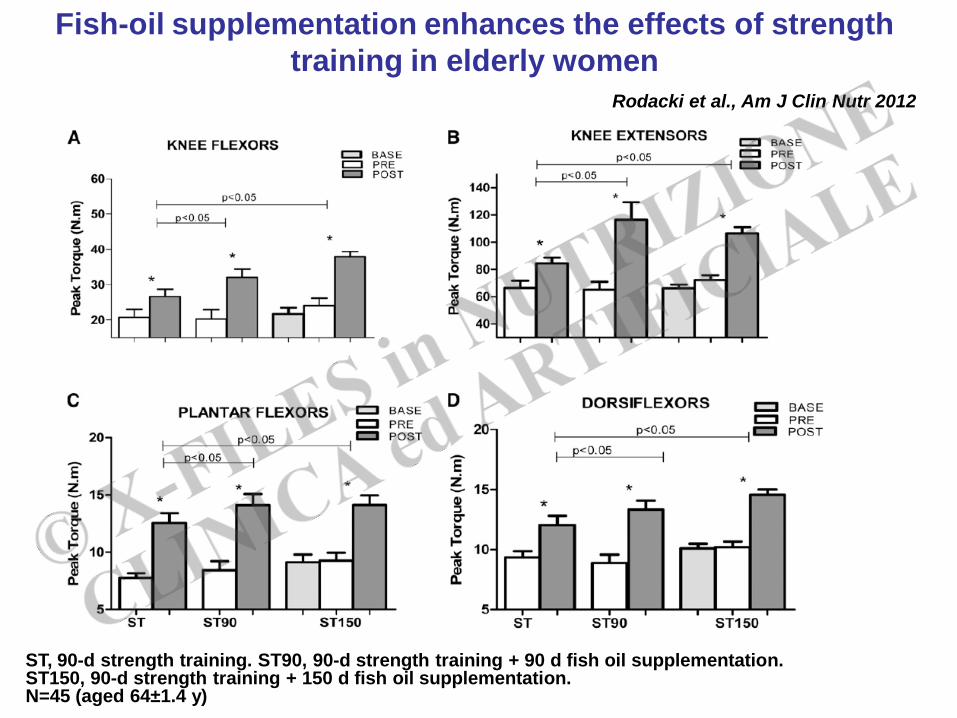
Fish-oil supplementation enhances the effects of strength training in elderly women
Rodacki et al., Am J Clin Nutr 2012
ST, 90-d strength training. ST90, 90-d strength training + 90 d fish oil supplementation. ST150, 90-d strength training + 150 d fish oil supplementation. N=45 (aged 64±1.4 y)

8 weeks supplementation
Dietary omega-3 fatty acid supplementation increases the rate of muscle protein synthesis in older adults: a randomized controlled trial Smith et al., Am J Clin Nutr 2011
n=7
n=8
FSR, fractional synthesis rate a, P < 0.01 in the corn oil group, clamp vs basal (ANOVA) b, P < 0.01 in the omega-3 fatty acid group, clamp vs basal (ANOVA) c, P < 0.01 in the omega-3 fatty acid group, different from the corresponding value before omega-3 fatty acid supplementation CLAMP=insulin + glucose + aminoacid infusion

GLI ACIDI GRASSI ω3
• MIGLIORANO L’AUMENTO DI FORZA MUSCOLARE INDOTTO DALL’ESERCIZIO FISICO
• MIGLIORANO LA STIMOLAZIONE ANABOLICA INDOTTA DA SOMMINISTRAZIONE DI AMINOACIDI
CONCLUSIONI (III)





![5 sistema digerente [modalità compatibilità] · costituenti organici specifici. ... ¾Elaborazione metabolica dei nutrienti ¾Detossificazione o degradazione ¾Sintesi delle proteine](https://static.fdocumenti.com/doc/165x107/5c65887109d3f29b6e8ceb65/5-sistema-digerente-modalita-compatibilita-costituenti-organici-specifici.jpg)










