Quello che le placche coronariche non dicono: enigmi del ... · F Prati San Giovanni Hospital, Rome...
89
F Prati San Giovanni Hospital, Rome Quello che le placche coronariche non dicono: enigmi del cardiologo clinico e speranze dell'interventista Rome Heart Research Lucca, Dicembre 2013
Transcript of Quello che le placche coronariche non dicono: enigmi del ... · F Prati San Giovanni Hospital, Rome...

F Prati
San Giovanni Hospital, Rome
Quello che le placche coronariche non dicono: enigmi del cardiologo clinico e
speranze dell'interventista
Rome Heart Research
Lucca, Dicembre 2013
Cosa Non Dice la Coronarografia
Può non vedere:• Placche aterosclerotiche• Trombosi locale come segno
di instabilità
Limiti della Coronarografia
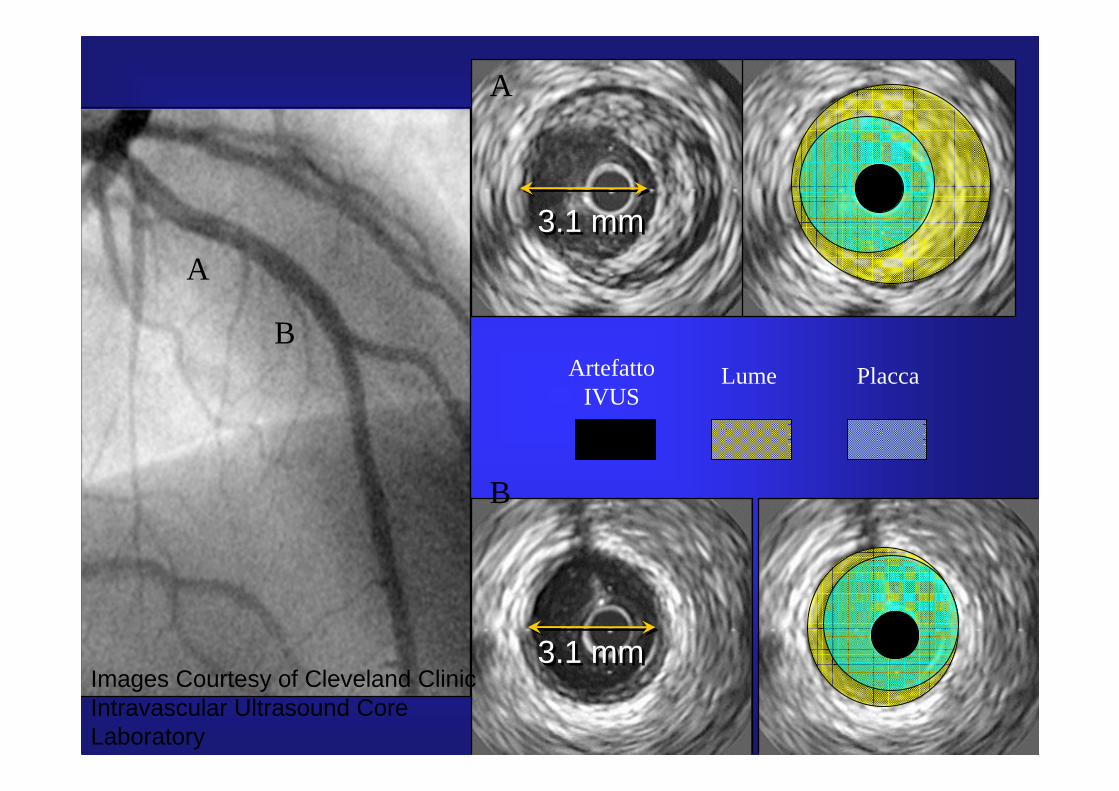
3.1 mm3.1 mm
3.1 mm3.1 mm
A
B
A
PlaccaArtefatto IVUS
Lume
B
Images Courtesy of Cleveland ClinicIntravascular Ultrasound Core Laboratory

OCT: Ruptured plaque with mild
thrombus
LP
Thrombus
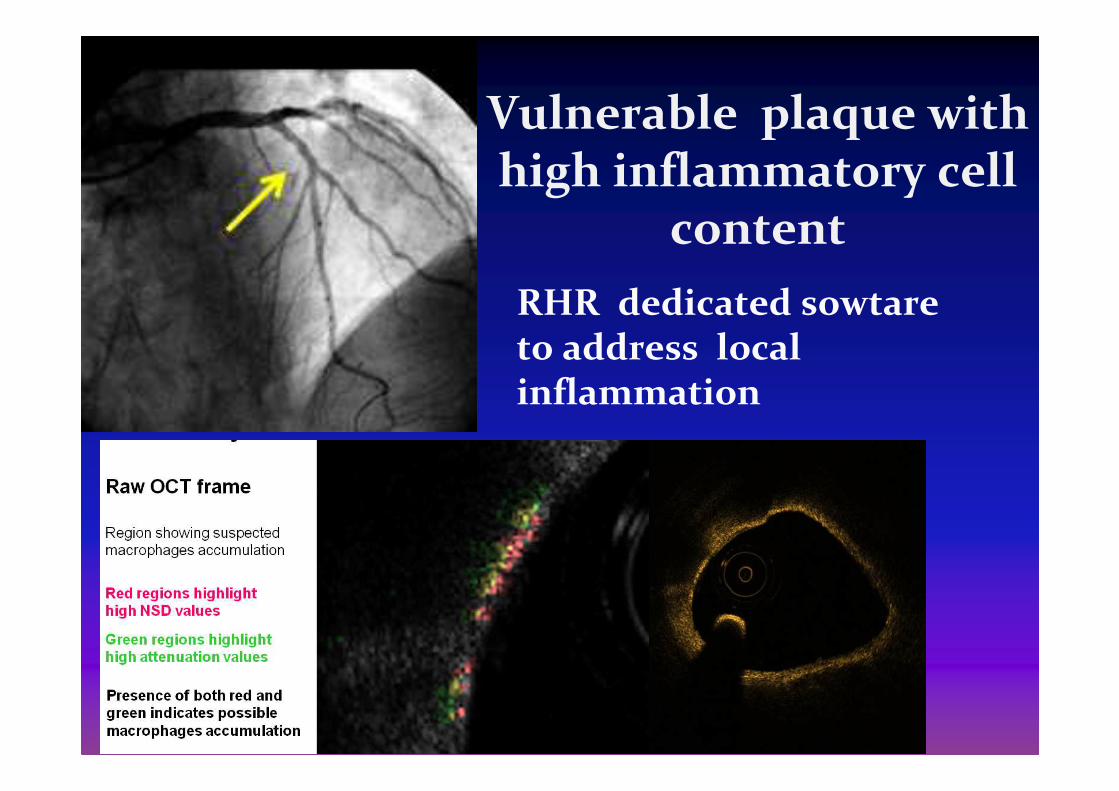
Vulnerable plaque with high inflammatory cell
content
RHR dedicated sowtare to address local inflammation
Condurre alla diagnosi errata di instabilizzazione
contemporanea di piùplacche
Limiti della Coronarografia
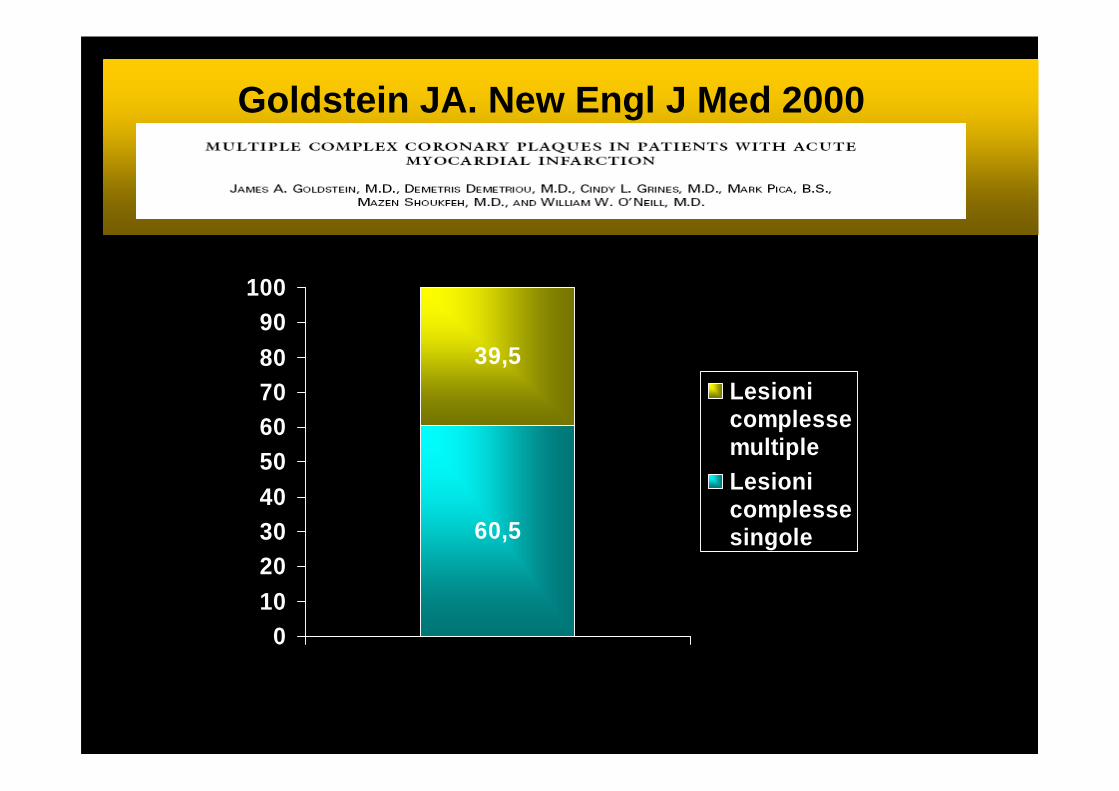
60,5
39,5
0102030405060708090
100
LesionicomplessemultipleLesionicomplessesingole
Goldstein. New.Engl.J.Med 2000Goldstein JA. New Engl J Med 2000
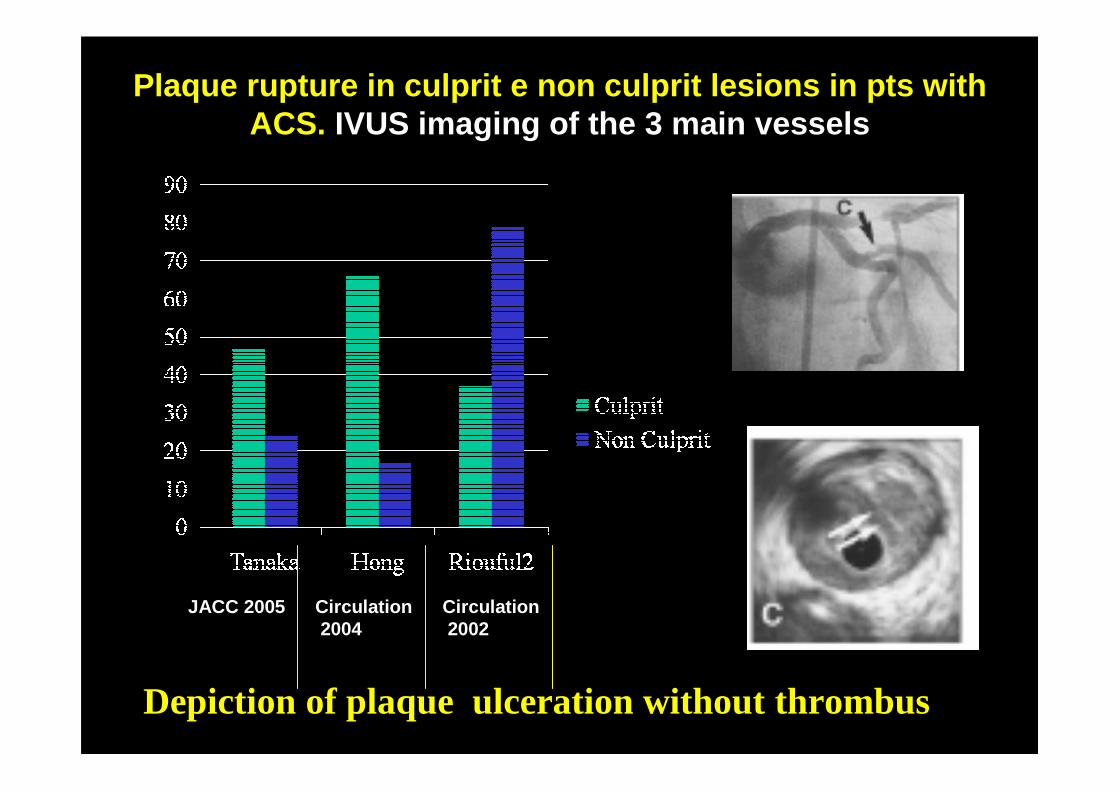
Plaque rupture in culprit e non culprit lesions in pts with ACS. IVUS imaging of the 3 main vessels
Depiction of plaque ulceration without thrombus
Circulation2004
JACC 2005 Circulation2002

2010, 2011,2013: Placca ulcerata con tromboTrattare con PCI
2010, 2011,2013: Placca ulcerata senza trombo2010 Trattare con PCI2011-2013 NON TRATTARE (non èacuta)
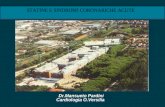
LCxMarzo2010. Uomo di 78 anni con STEMI inferiore
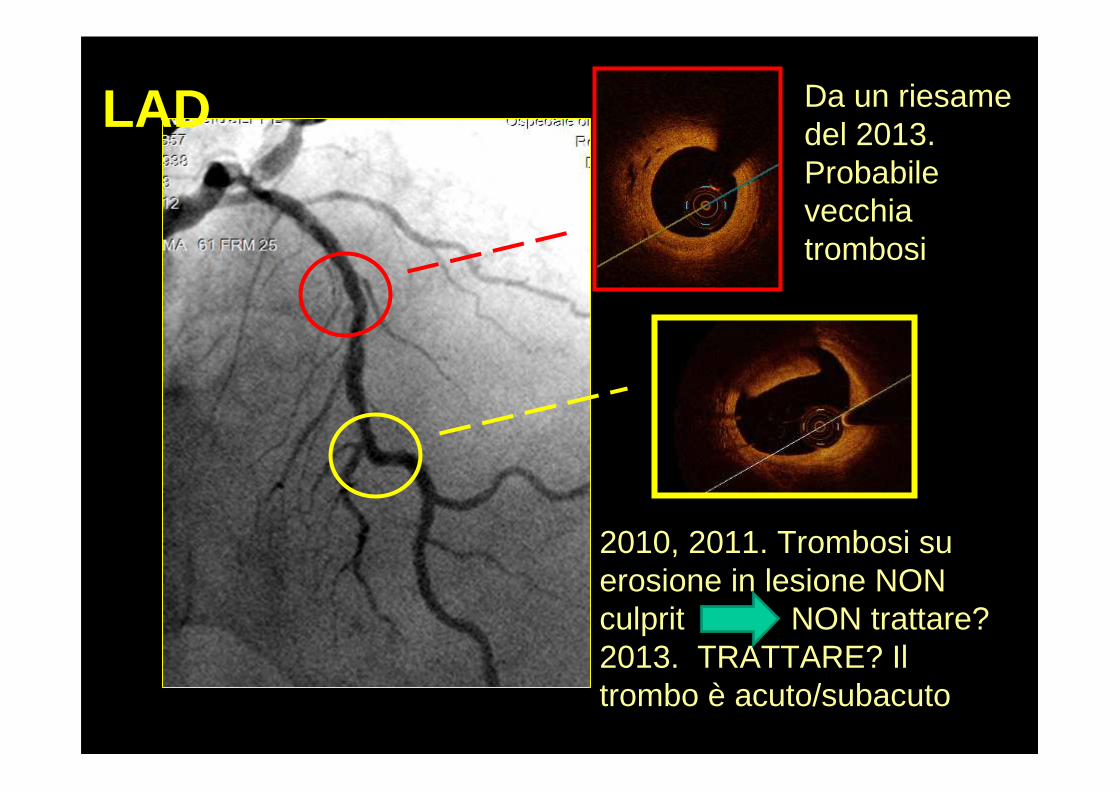
LAD
2010, 2011. Trombosi su erosione in lesione NON culprit NON trattare? 2013. TRATTARE? Il trombo è acuto/subacuto
Da un riesame del 2013.Probabile vecchia trombosi
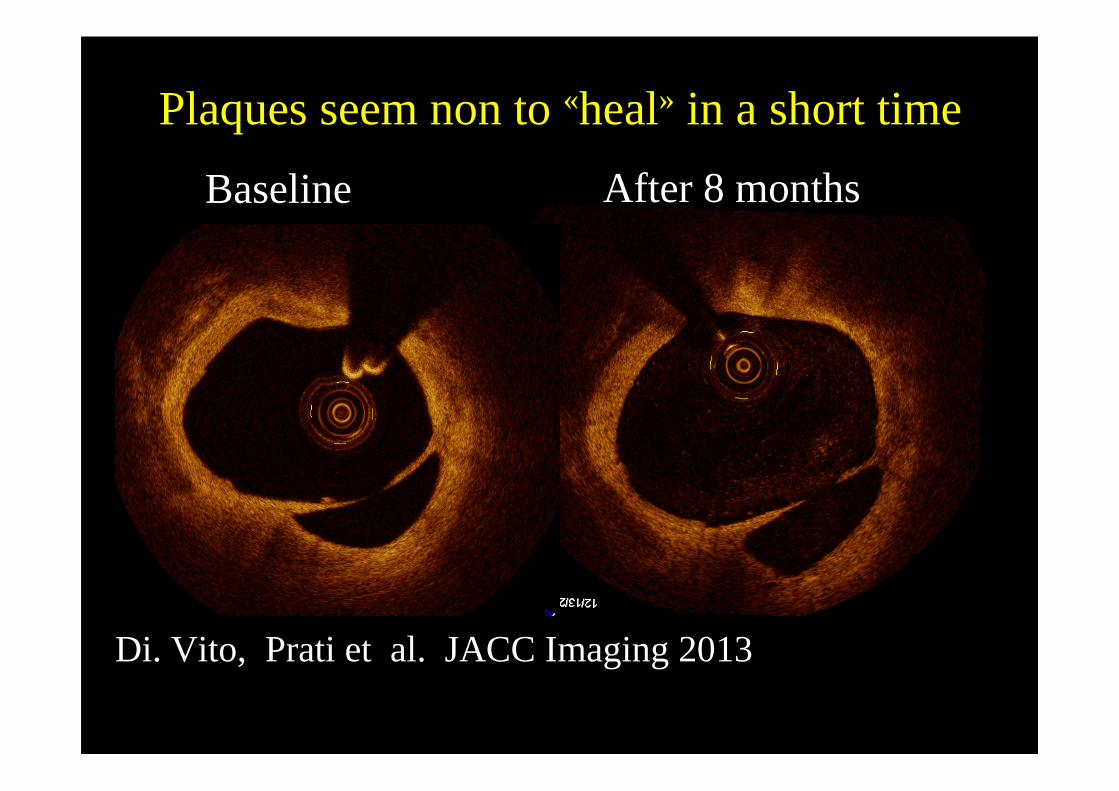
Baseline After 8 months
Plaques seem non to «heal» in a short time
Di. Vito, Prati et al. JACC Imaging 2013
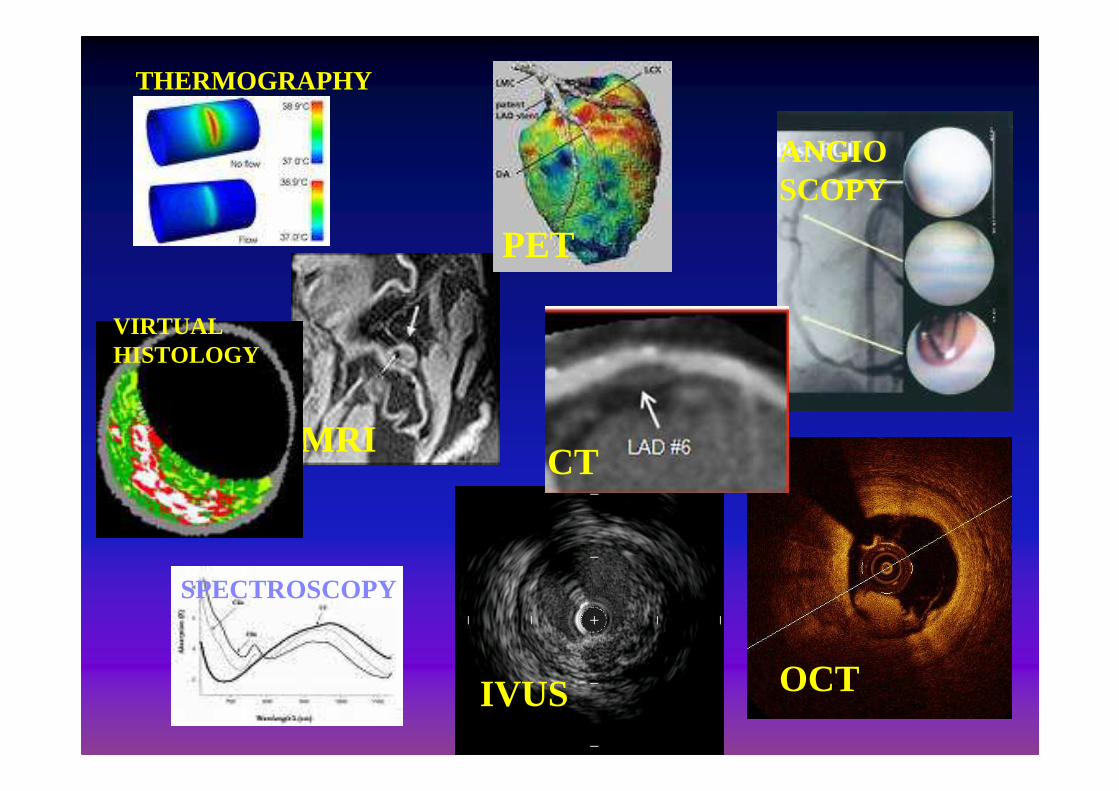
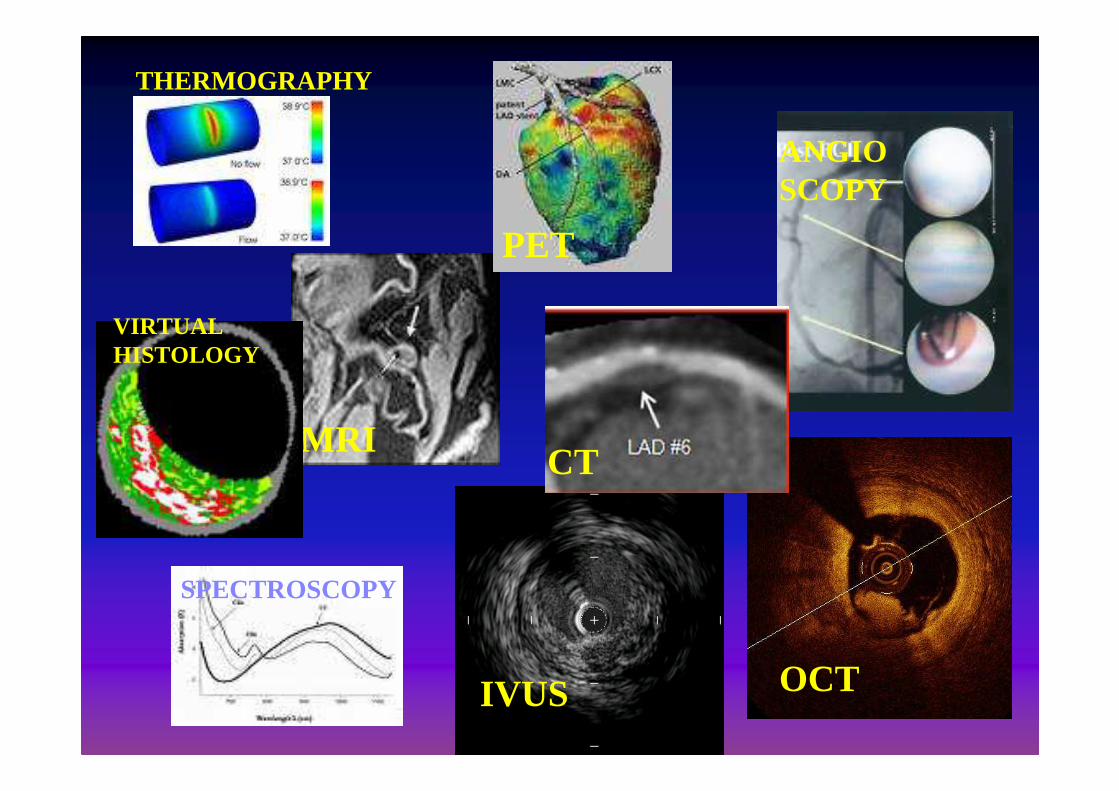
MRI
ANGIOSCOPY
THERMOGRAPHY
IVUS OCT
SPECTROSCOPY
VIRTUALHISTOLOGY
CT
PET
Lascia ipotizzare che le placche che causano l’infarto siano piccole
Limiti della Coronarografia
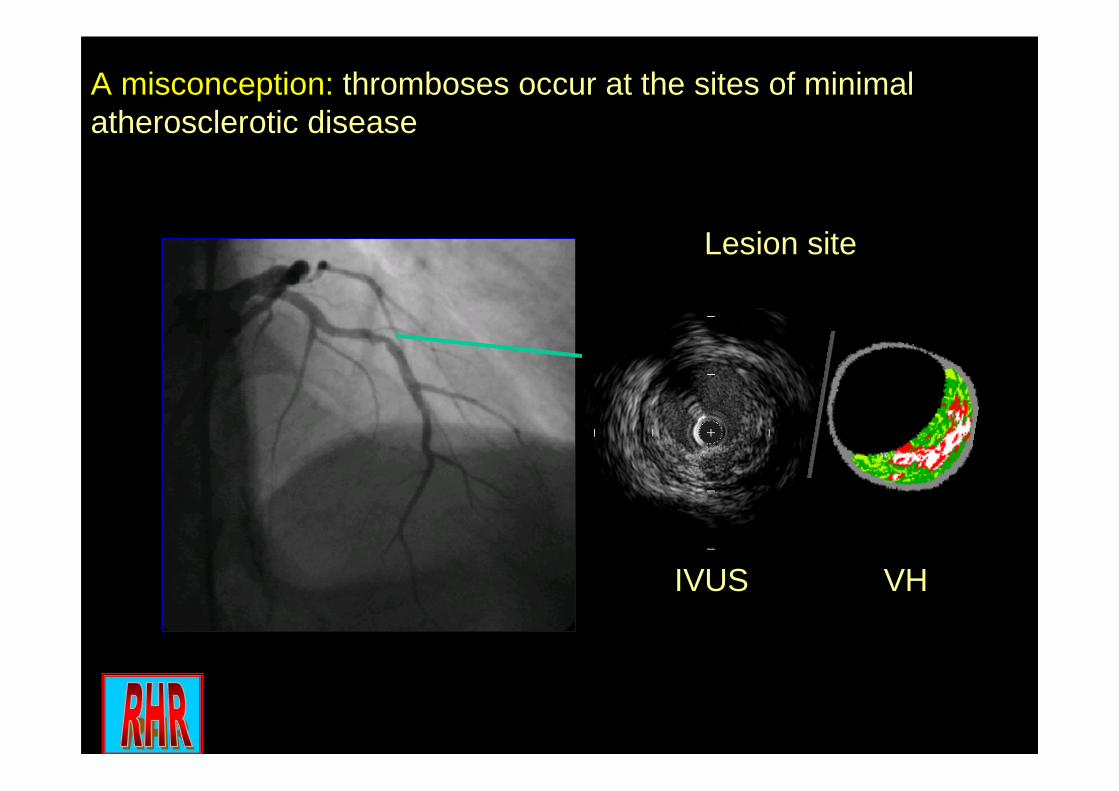
Lesion site
IVUS VH
A misconception: thromboses occur at the sites of minimal atherosclerotic disease
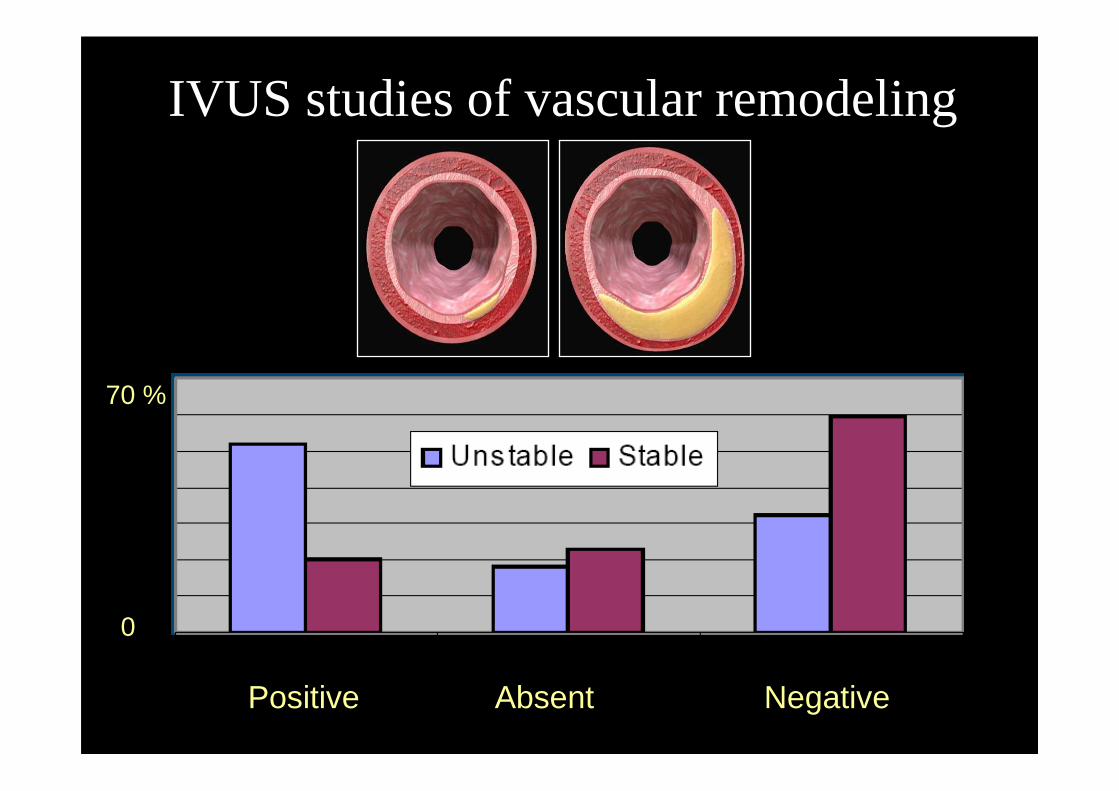
IVUS studies of vascular remodeling
Positive Absent Negative
70 %
0
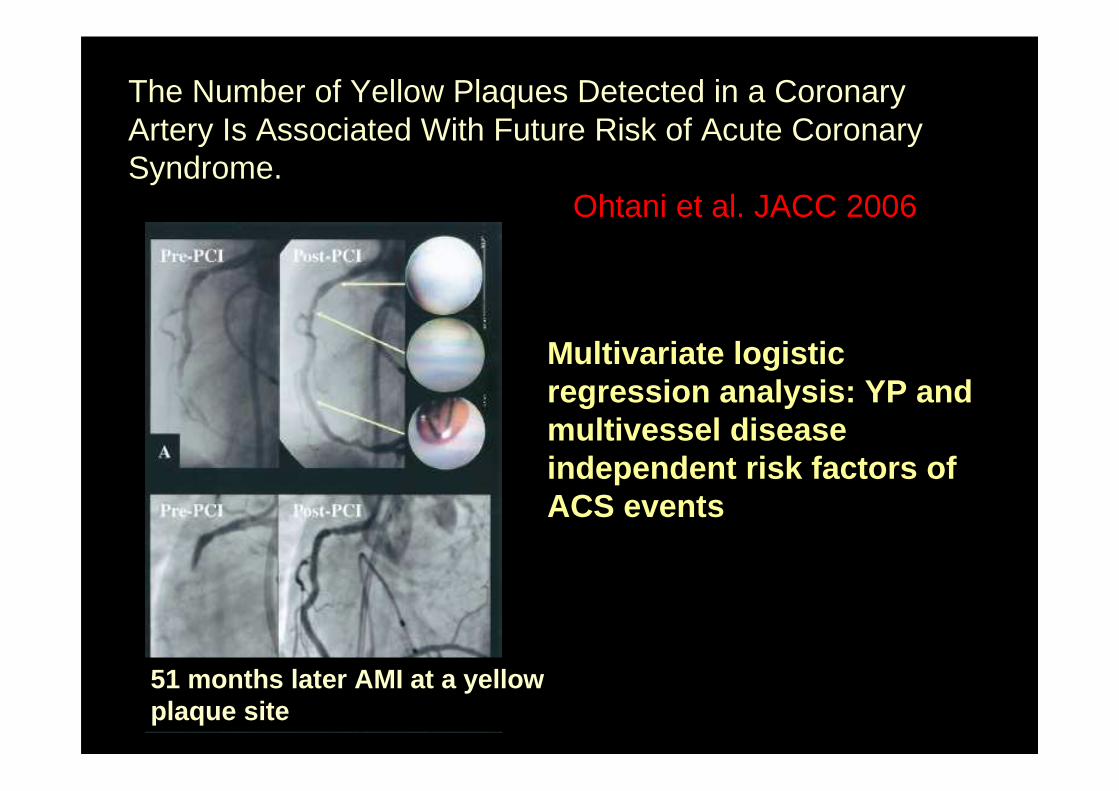
The Number of Yellow Plaques Detected in a Coronary Artery Is Associated With Future Risk of Acute Coronary Syndrome.
Ohtani et al. JACC 2006
Multivariate logistic regression analysis: YP and multivessel disease independent risk factors of ACS events
51 months later AMI at a yellow plaque site
JACC 2013
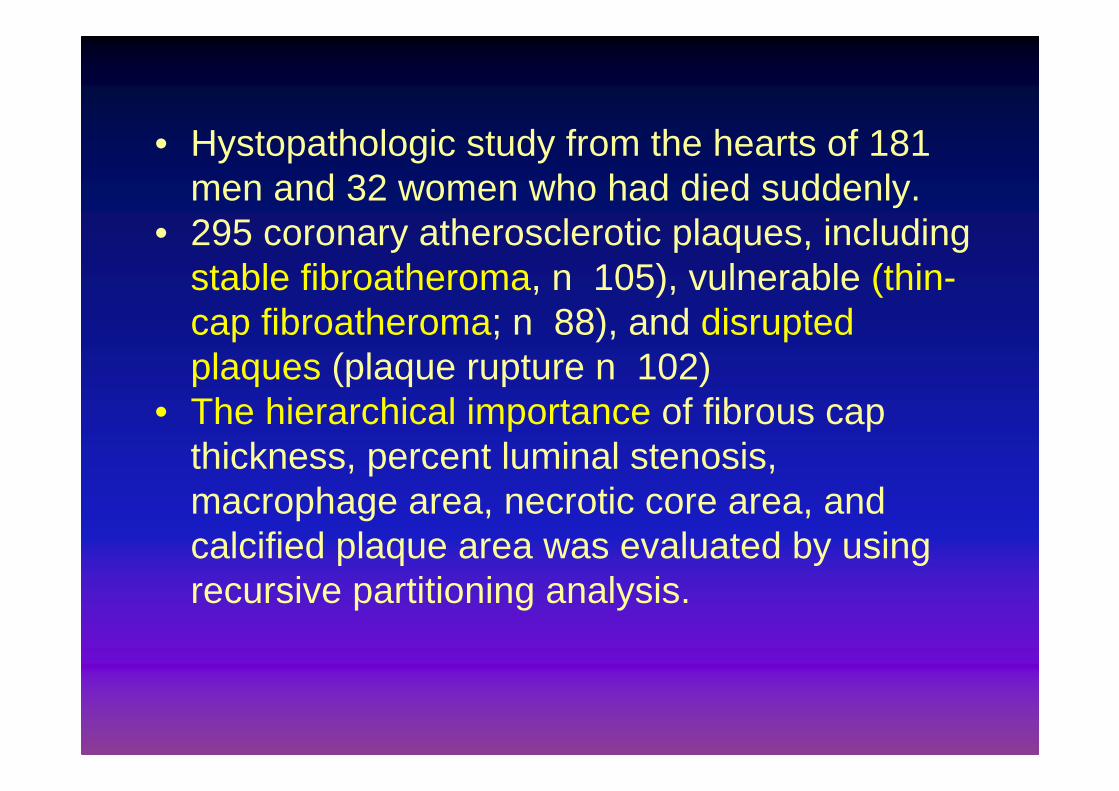
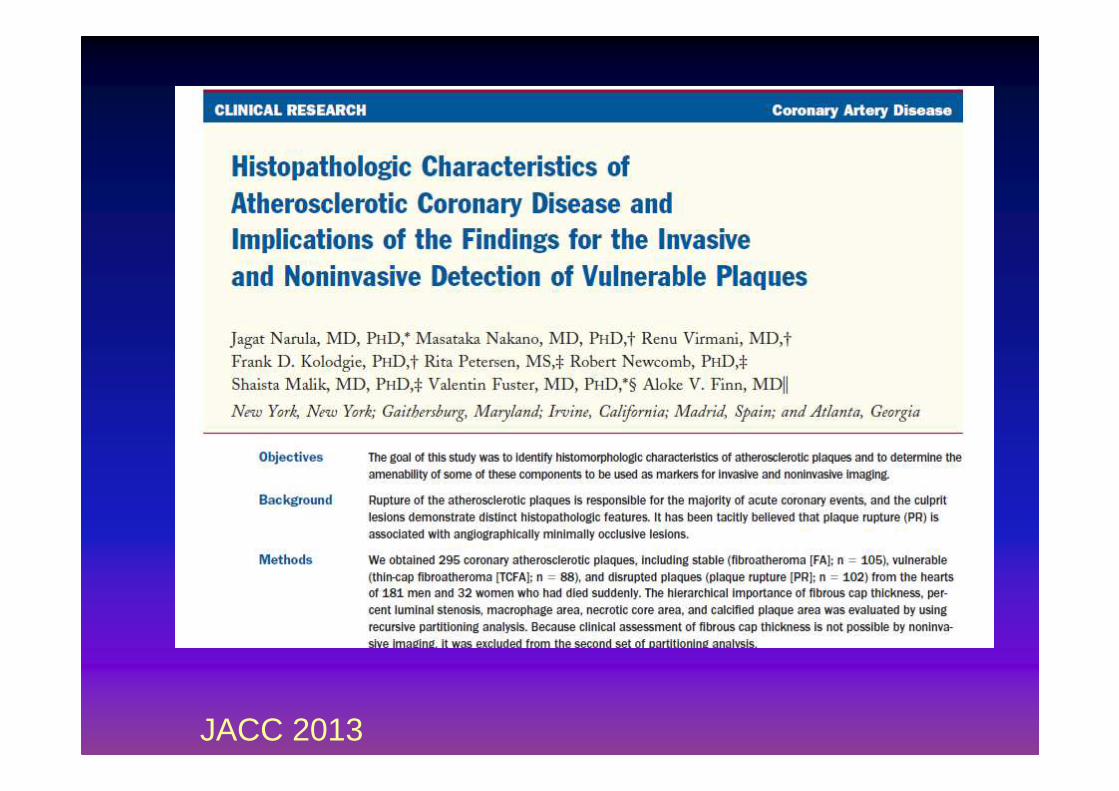
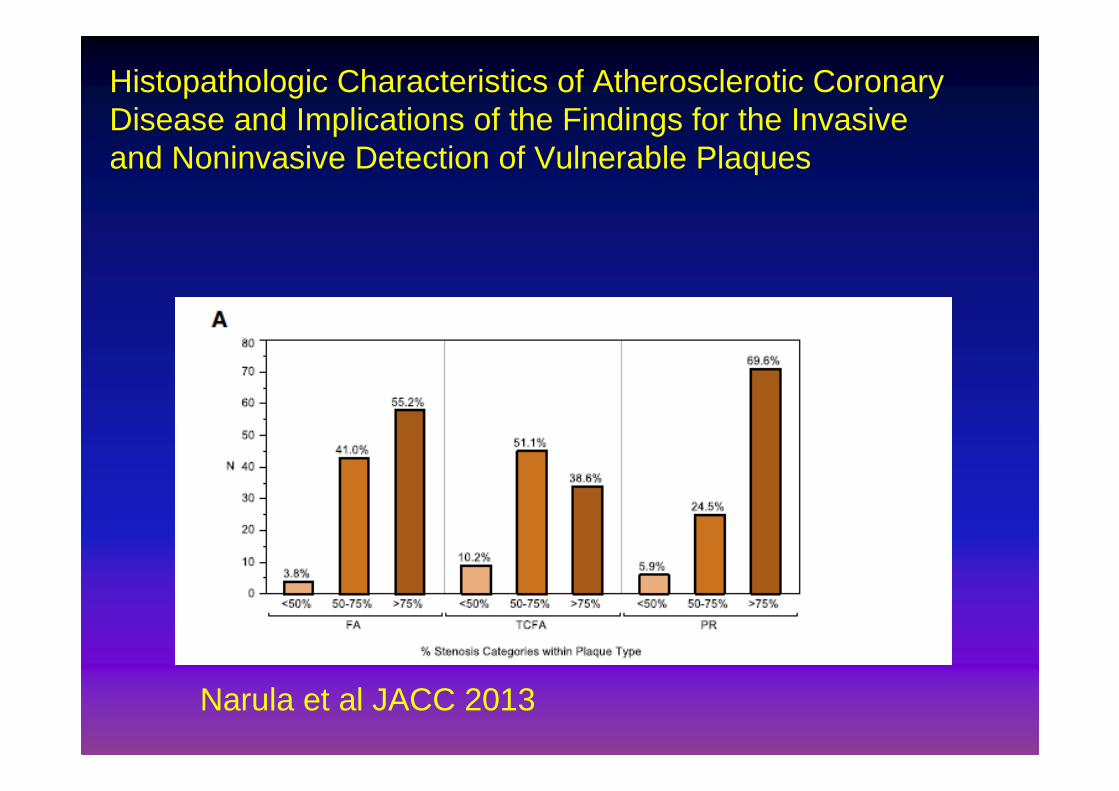
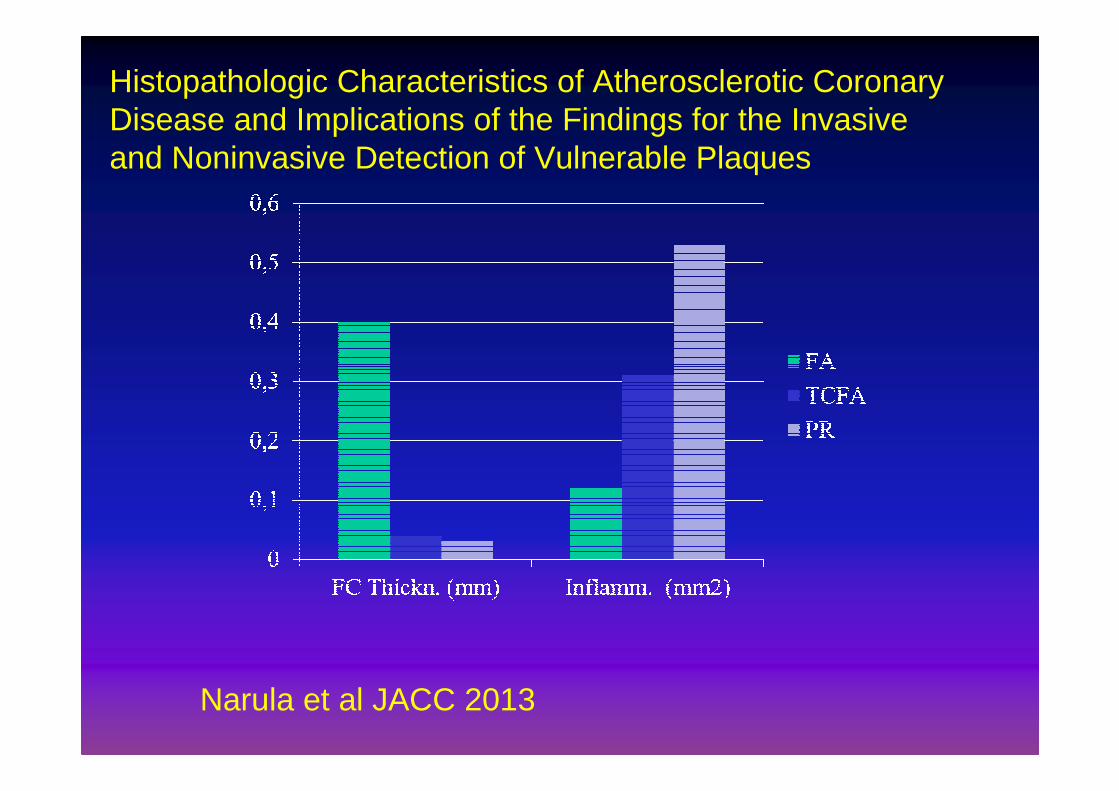
• Hystopathologic study from the hearts of 181 men and 32 women who had died suddenly.
• 295 coronary atherosclerotic plaques, including stable fibroatheroma, n 105), vulnerable (thin-cap fibroatheroma; n 88), and disrupted plaques (plaque rupture n 102)
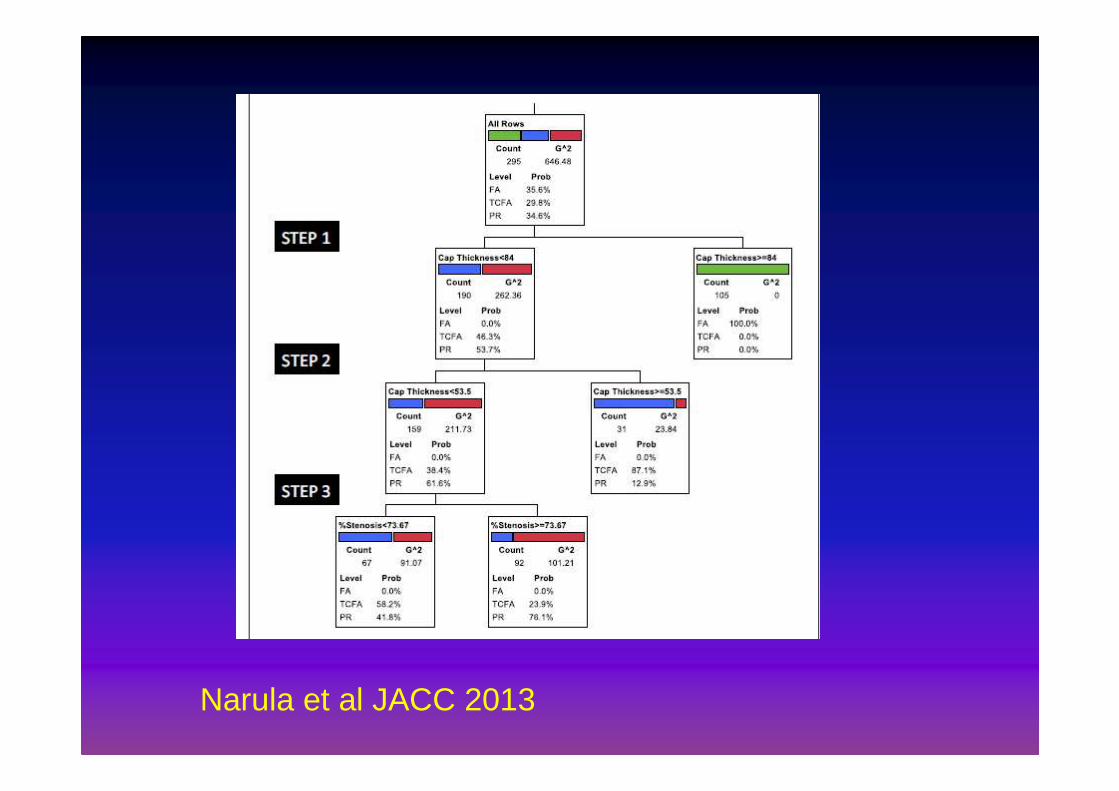
• The hierarchical importance of fibrous cap thickness, percent luminal stenosis, macrophage area, necrotic core area, and calcified plaque area was evaluated by using recursive partitioning analysis.
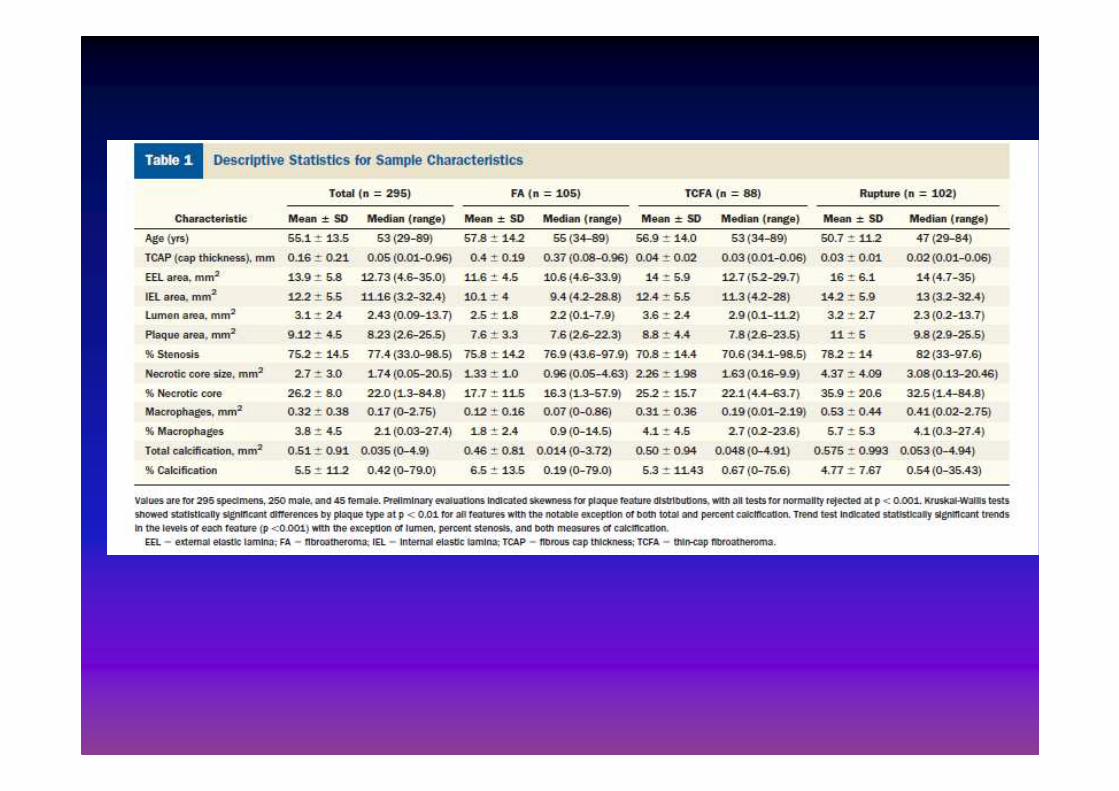
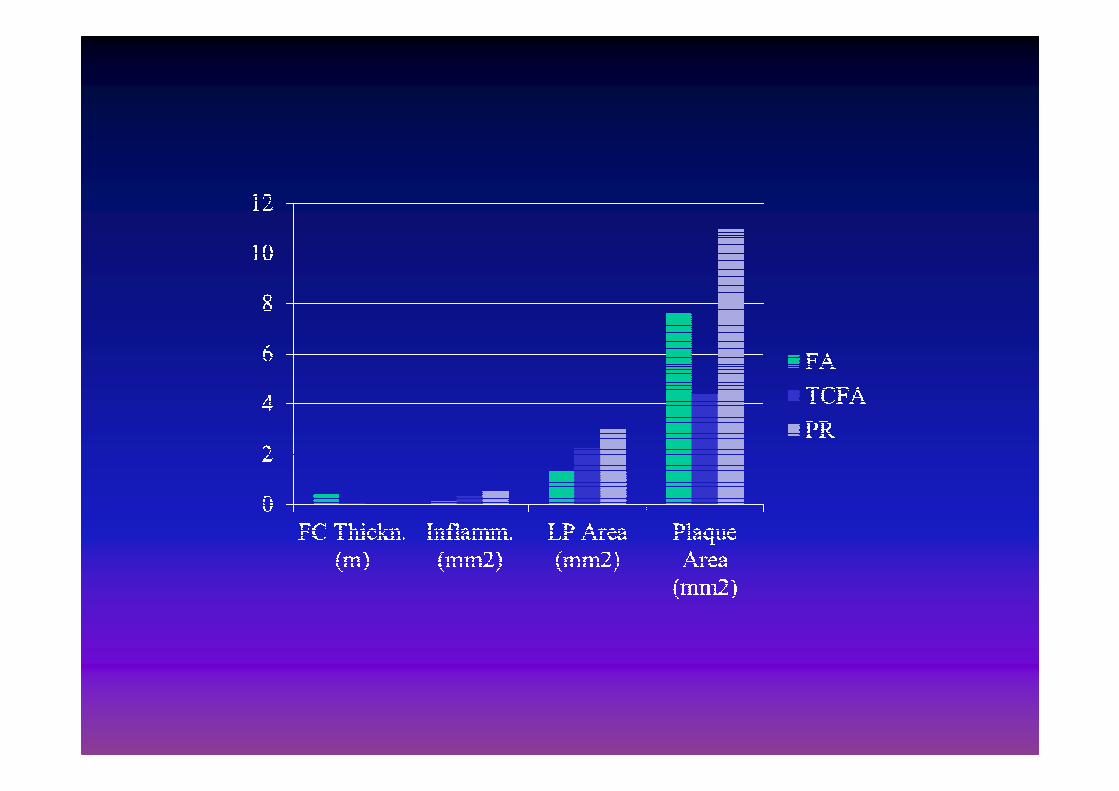
Histopathologic Characteristics of Atherosclerotic Coronary Disease and Implications of the Findings for the Invasiveand Noninvasive Detection of Vulnerable Plaques
Narula et al JACC 2013
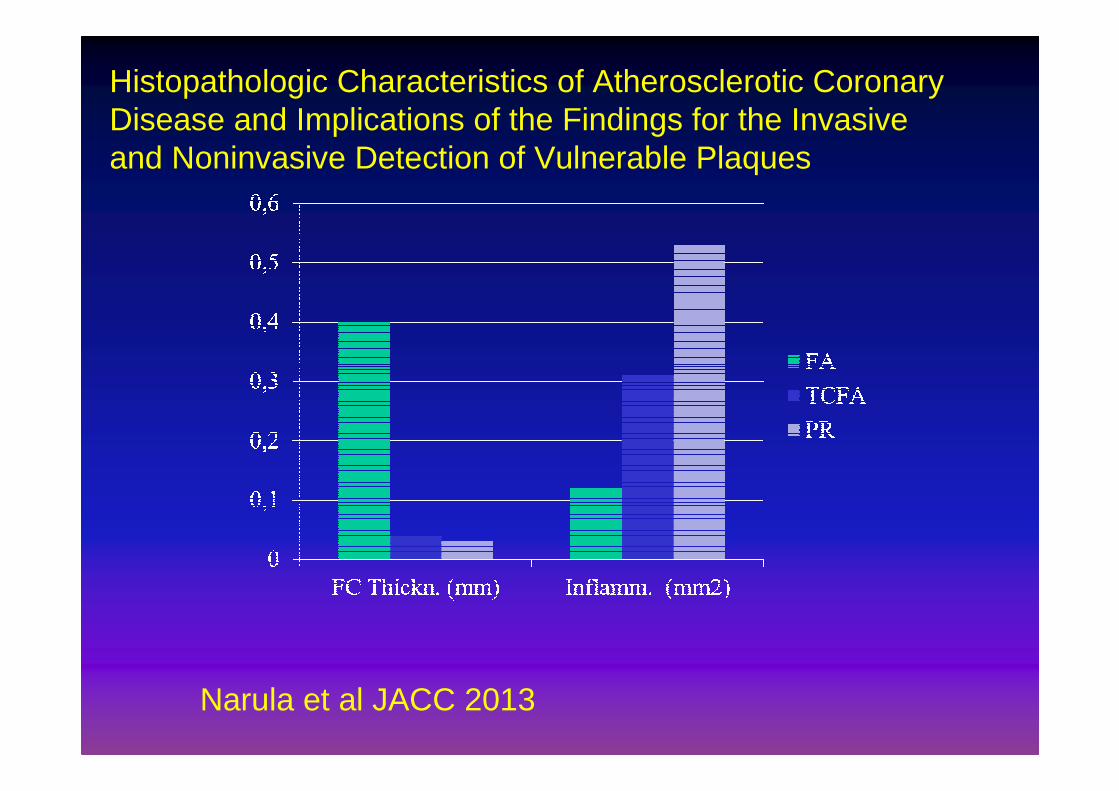
Histopathologic Characteristics of Atherosclerotic Coronary Disease and Implications of the Findings for the Invasiveand Noninvasive Detection of Vulnerable Plaques
Narula et al JACC 2013
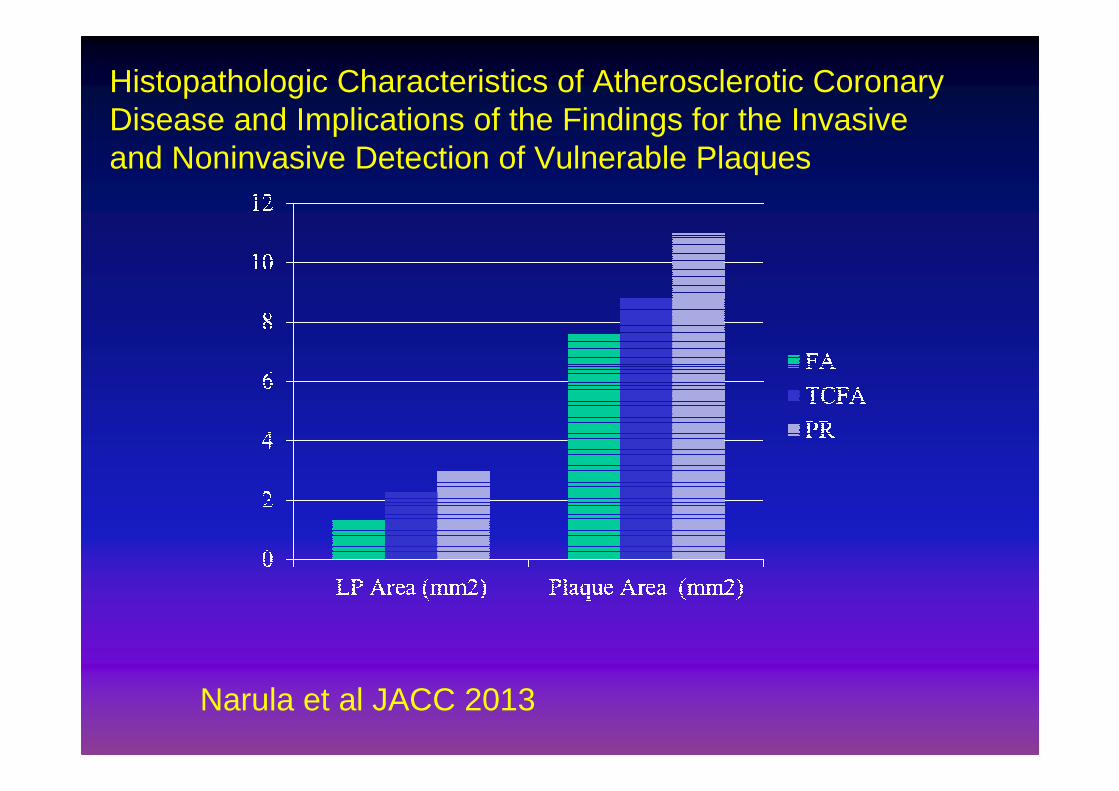
Histopathologic Characteristics of Atherosclerotic Coronary Disease and Implications of the Findings for the Invasiveand Noninvasive Detection of Vulnerable Plaques
Narula et al JACC 2013
Narula et al JACC 2013
Il nesso tra placche ad alto contenuto
lipidico e insorgenza dell’infarto
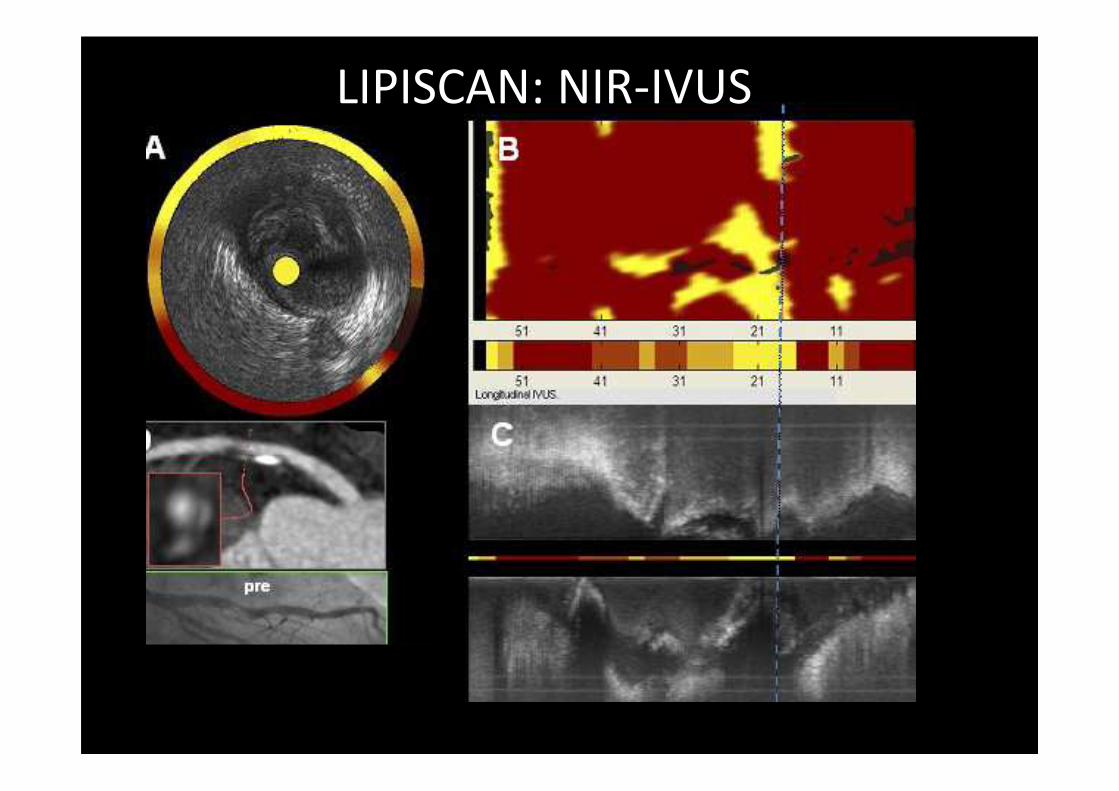
LIPISCAN: NIR-IVUS
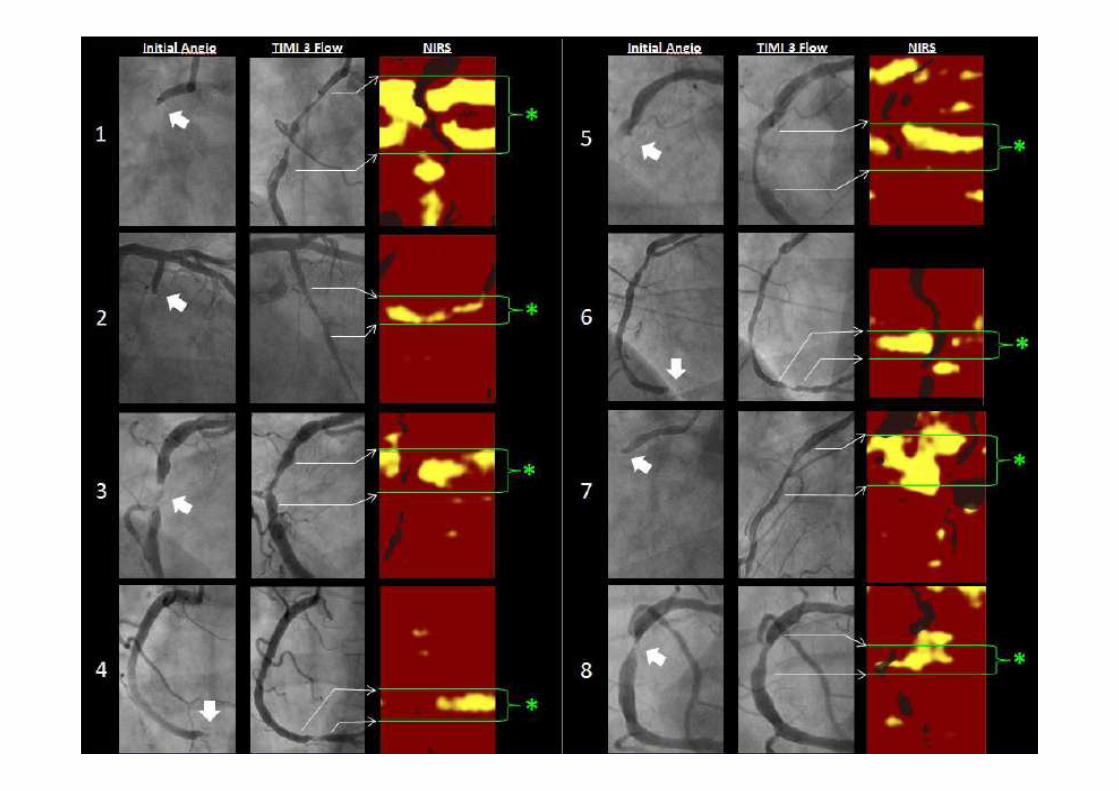
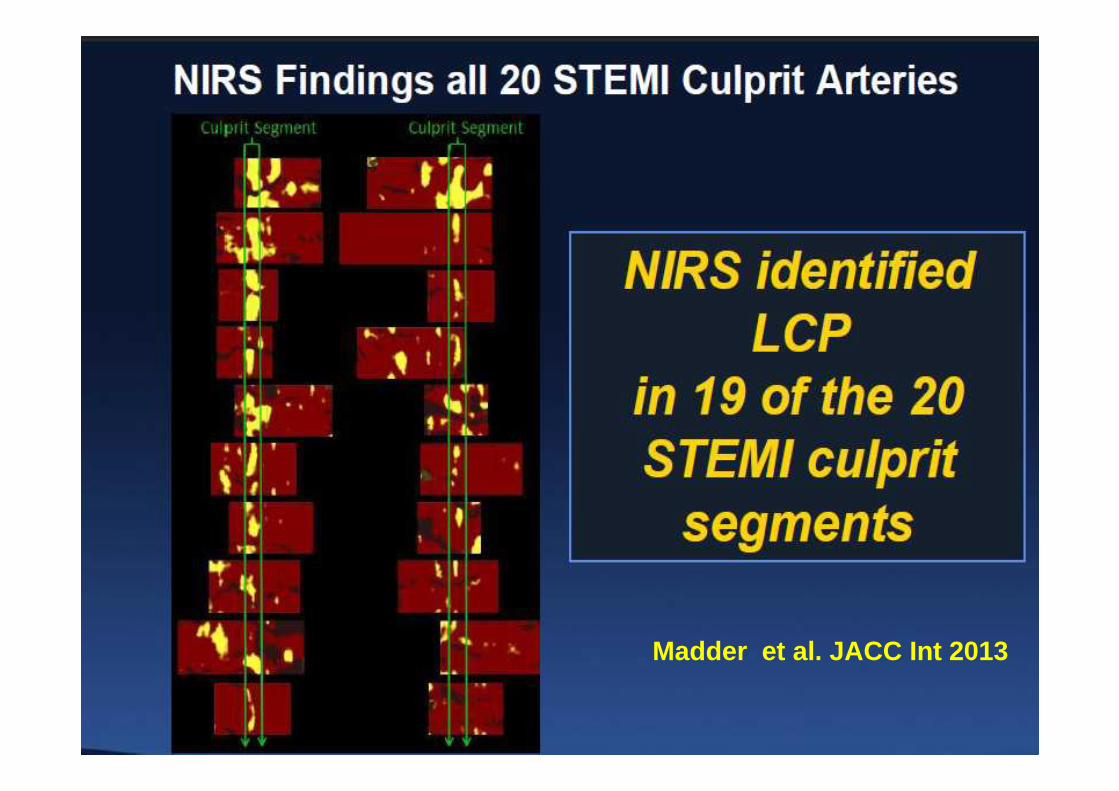
Madder et al. JACC Int 2013
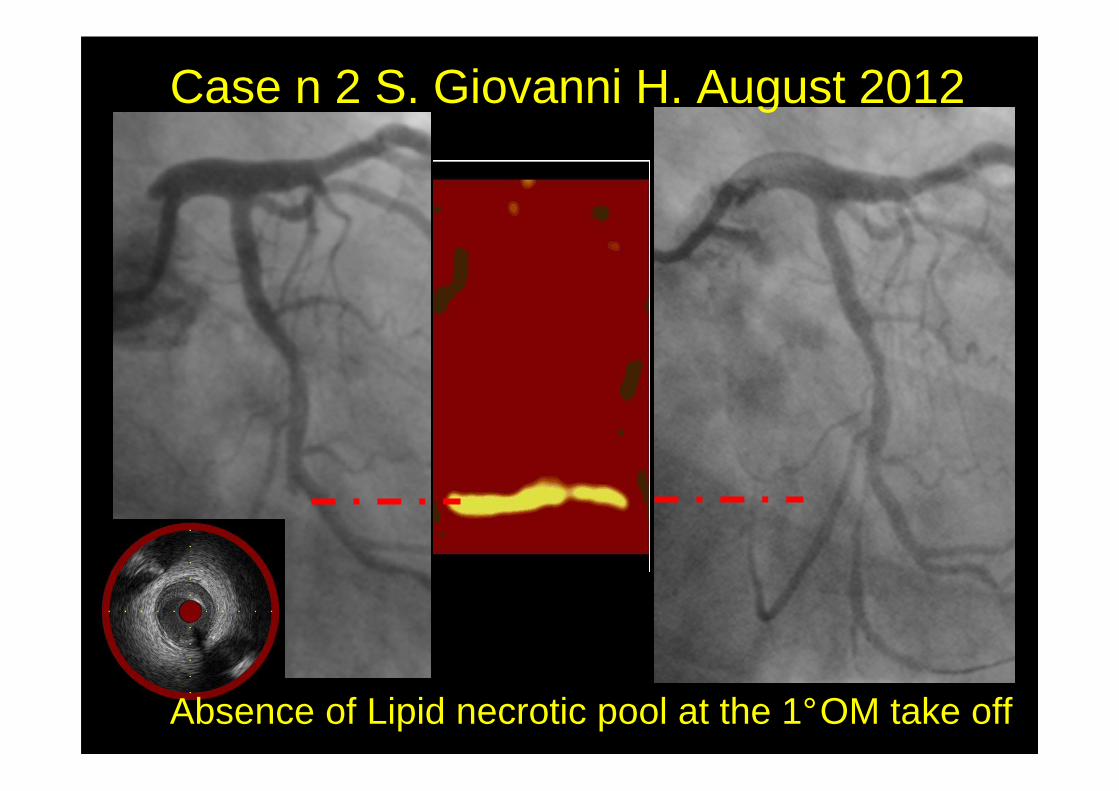
Case n 2 S. Giovanni H. August 2012
Absence of Lipid necrotic pool at the 1°OM take off
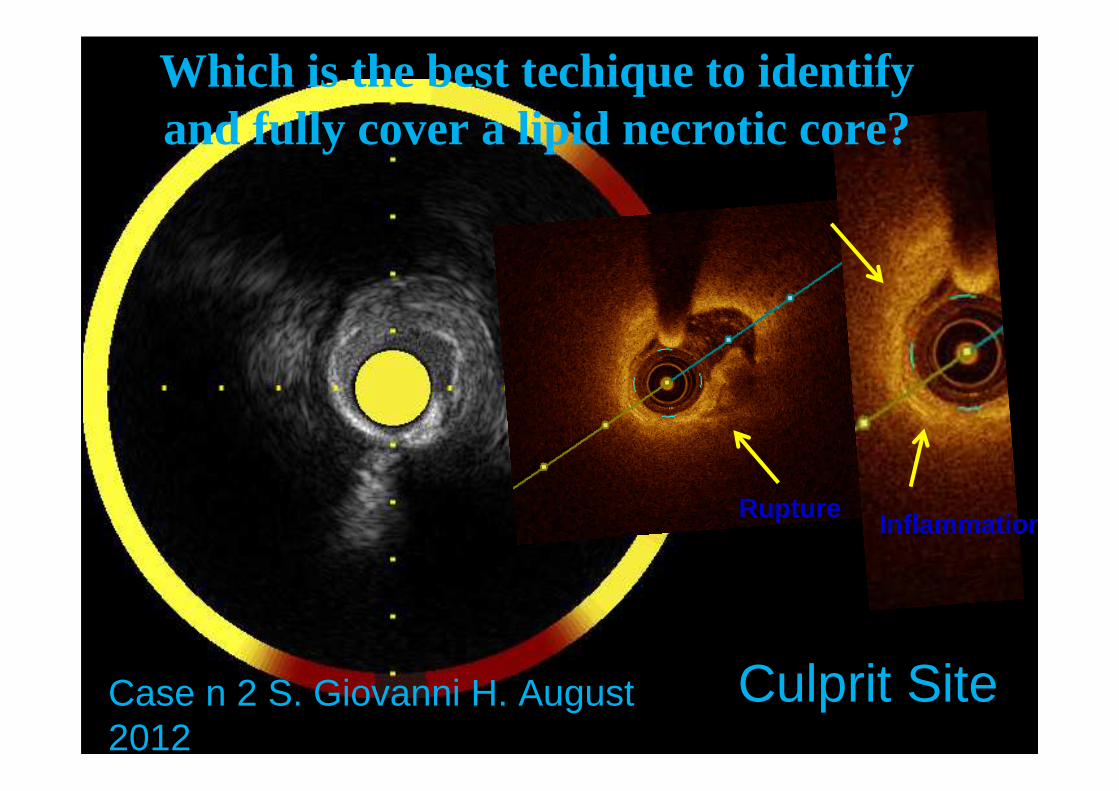
RuptureInflammation
Case n 2 S. Giovanni H. August 2012
Culprit Site
Which is the best techique to identify and fully cover a lipid necrotic core?
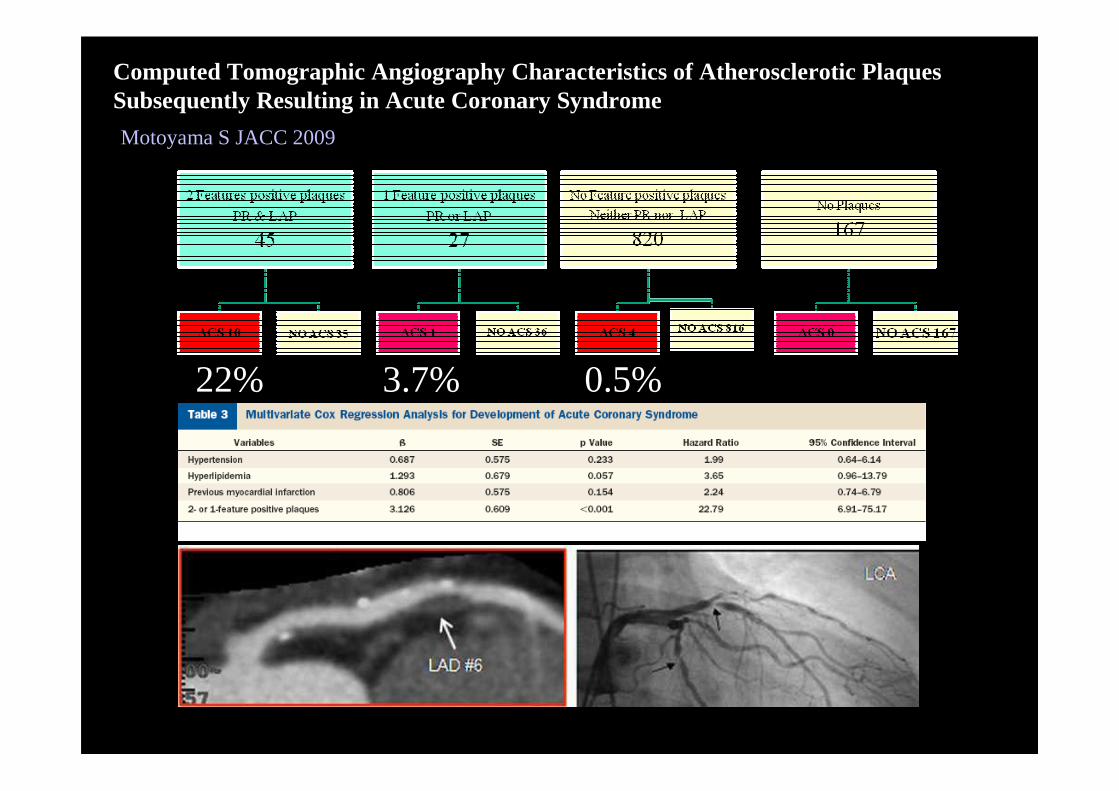
Computed Tomographic Angiography Characteristics of Atherosclerotic PlaquesSubsequently Resulting in Acute Coronary Syndrome
Motoyama S JACC 2009
22% 3.7% 0.5%
2) Vulnerable plaques are not so
many

86,8%
1,5%10,5%1,2%
Non Atheroscl. Thin Fibrous capMedium-Thick Fibrous cap Ruptured plaques
Frequencies of ruptured plaque and fibrous cap athe roma in all hearts studied provided as a percentage of the total 3,639 coronary intervals of length 3 mm examined.

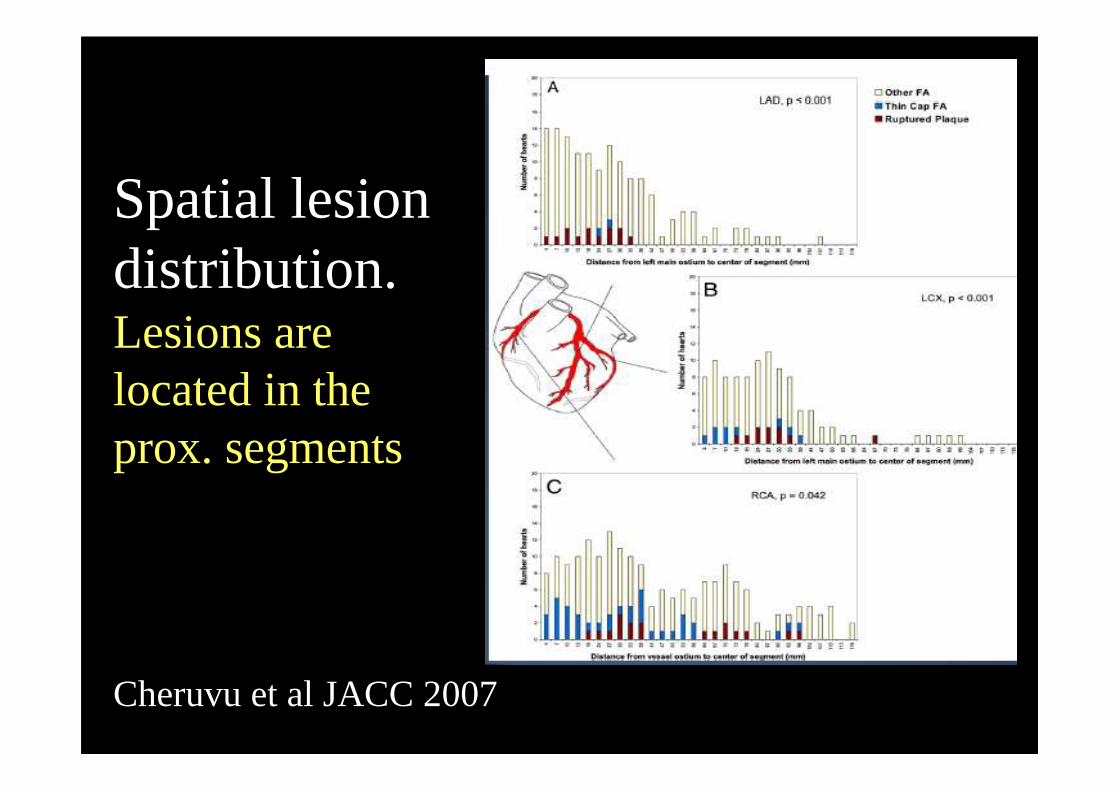
Spatial lesion distribution.Lesions are located in the prox. segments
Cheruvu et al JACC 2007
4. Il concetto di vulnerabilità di placca èstato confuso con quello di instabilizzazione
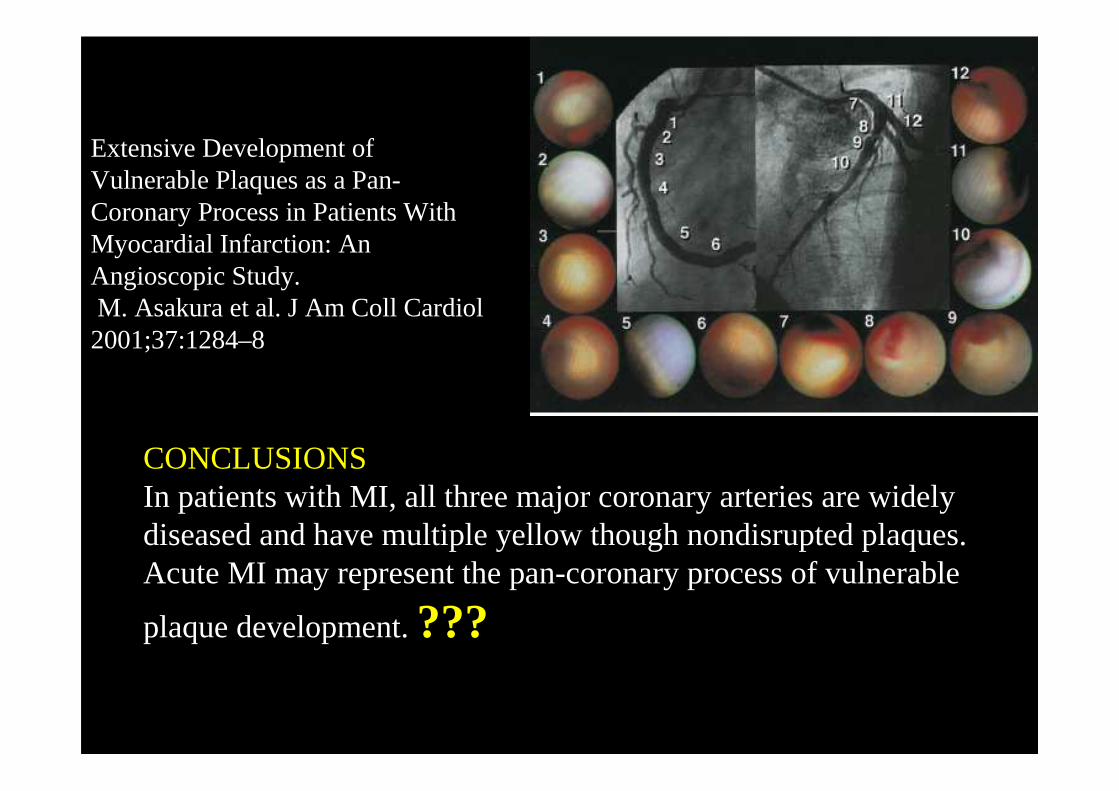
CONCLUSIONS In patients with MI, all three major coronary arteries are widely diseased and have multiple yellow though nondisrupted plaques. Acute MI may represent the pan-coronary process of vulnerable
plaque development. ???
Extensive Development of Vulnerable Plaques as a Pan-Coronary Process in Patients With Myocardial Infarction: An Angioscopic Study.M. Asakura et al. J Am Coll Cardiol 2001;37:1284–8
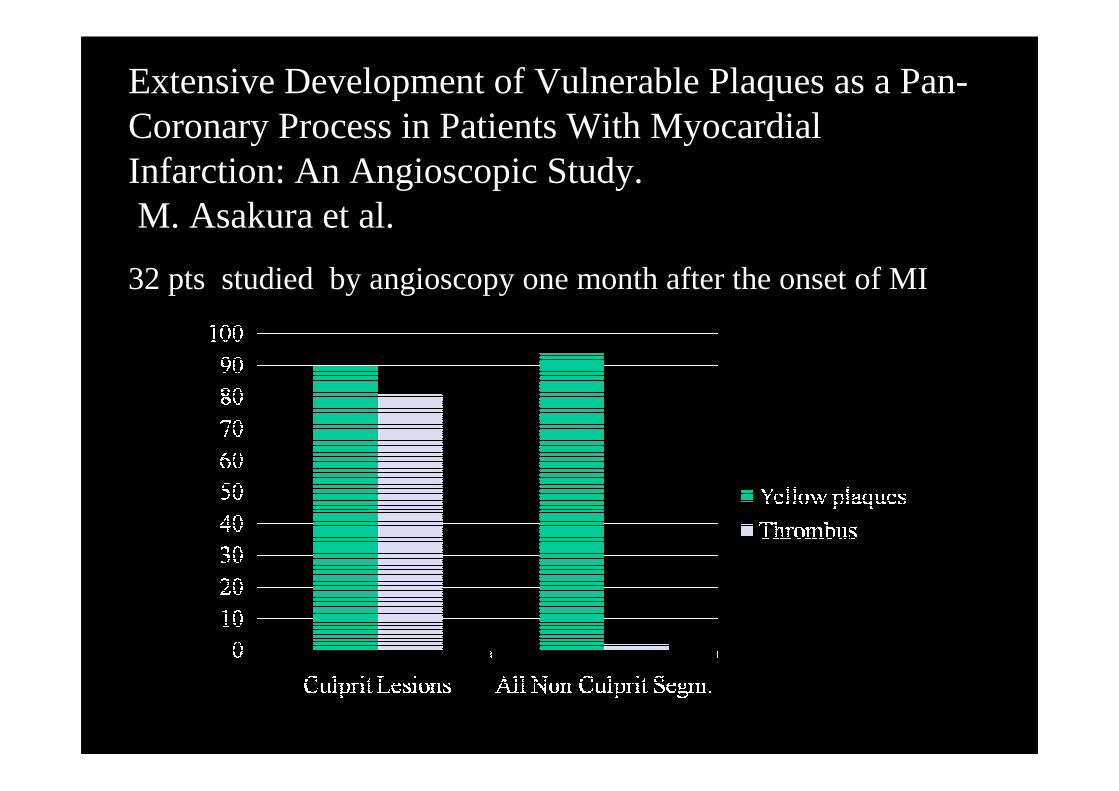
Extensive Development of Vulnerable Plaques as a Pan-Coronary Process in Patients With Myocardial Infarction: An Angioscopic Study.M. Asakura et al.
32 pts studied by angioscopy one month after the onset of MI
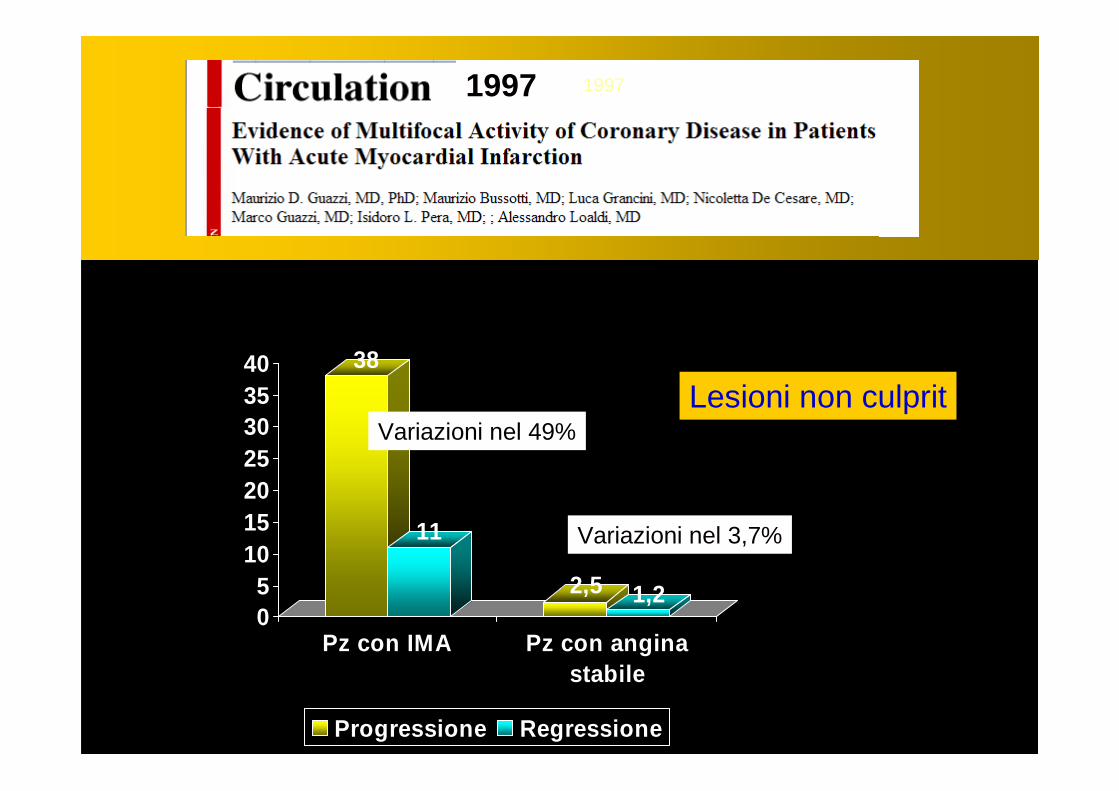
38
11
2,5 1,205
10152025303540
Pz con IMA Pz con anginastabile
Progressione Regressione
Variazioni nel 49%
Variazioni nel 3,7%
19971997
Confronto tra 23 pazienti con IMA e 23 con angina s tabileValutazione coronarografica basale e ad 1 mese
Lesioni non culprit
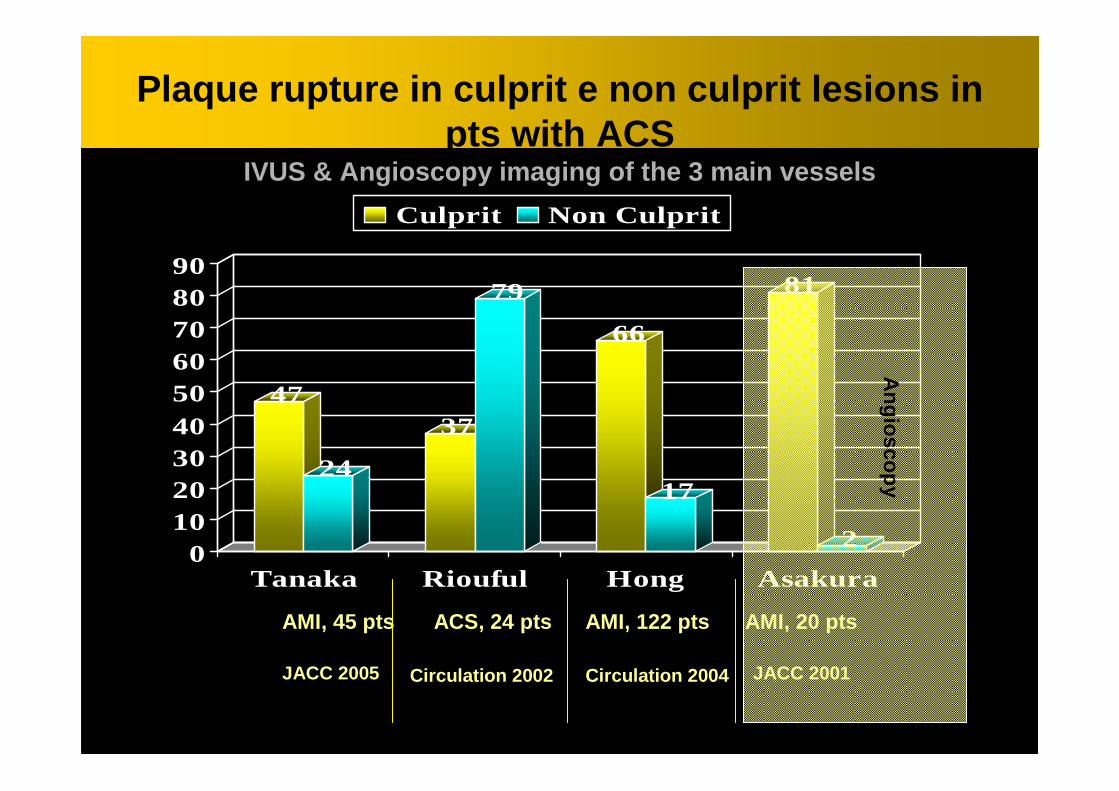
47
24
37
79
66
17
81
20
102030405060708090
Tanaka Riouful Hong Asakura
Culprit Non Culprit
Plaque rupture in culprit e non culprit lesions in pts with ACS
IVUS & Angioscopy imaging of the 3 main vessels
AMI, 45 pts AMI, 20 pts AMI, 122 pts ACS, 24 pts
Circulation 2004JACC 2005 Circulation 2002 JACC 2001
Angioscopy
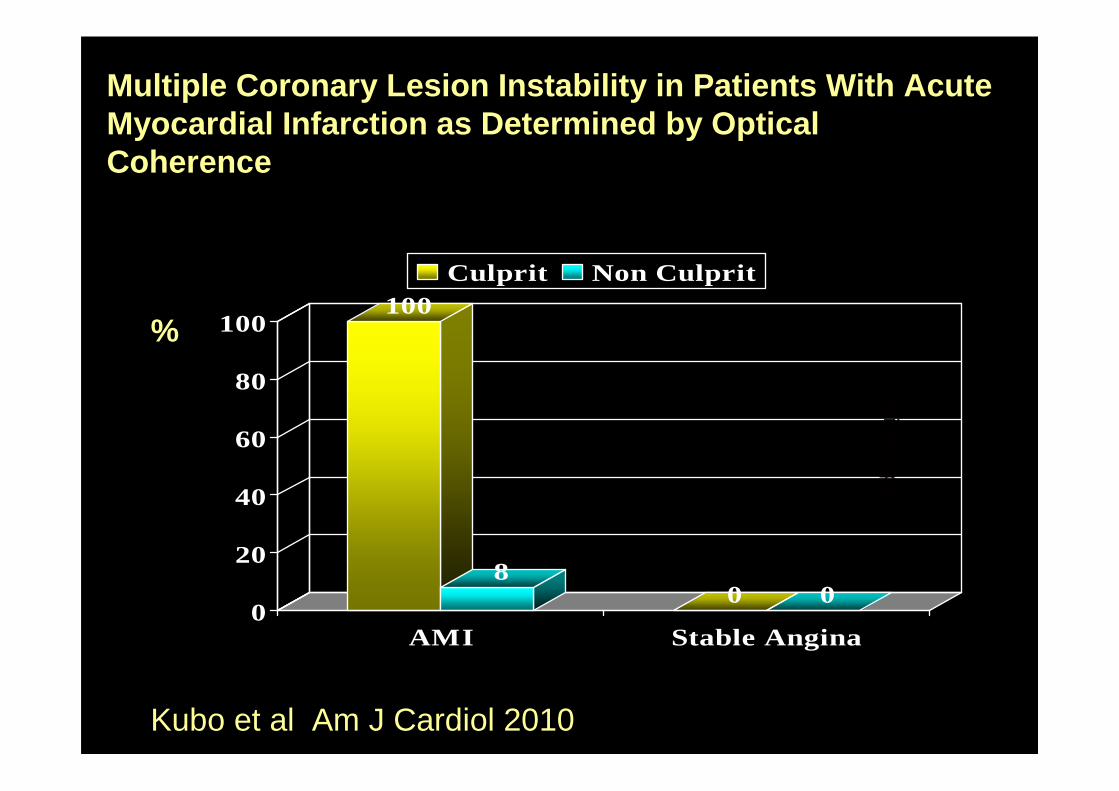
100
80 0
0
20
40
60
80
100
AMI Stable Angina
Culprit Non Culprit
Multiple Coronary Lesion Instability in Patients Wi th Acute Myocardial Infarction as Determined by OpticalCoherence
Angioscopy
Kubo et al Am J Cardiol 2010
%

Abbiamo impiegato in passato la tecnica giusta per studiare l’aterosclerosi ? …..E ora ne abbiamo di migliori?
Che cosa dobbiamo cercare con le tecniche di imaging coronarico?
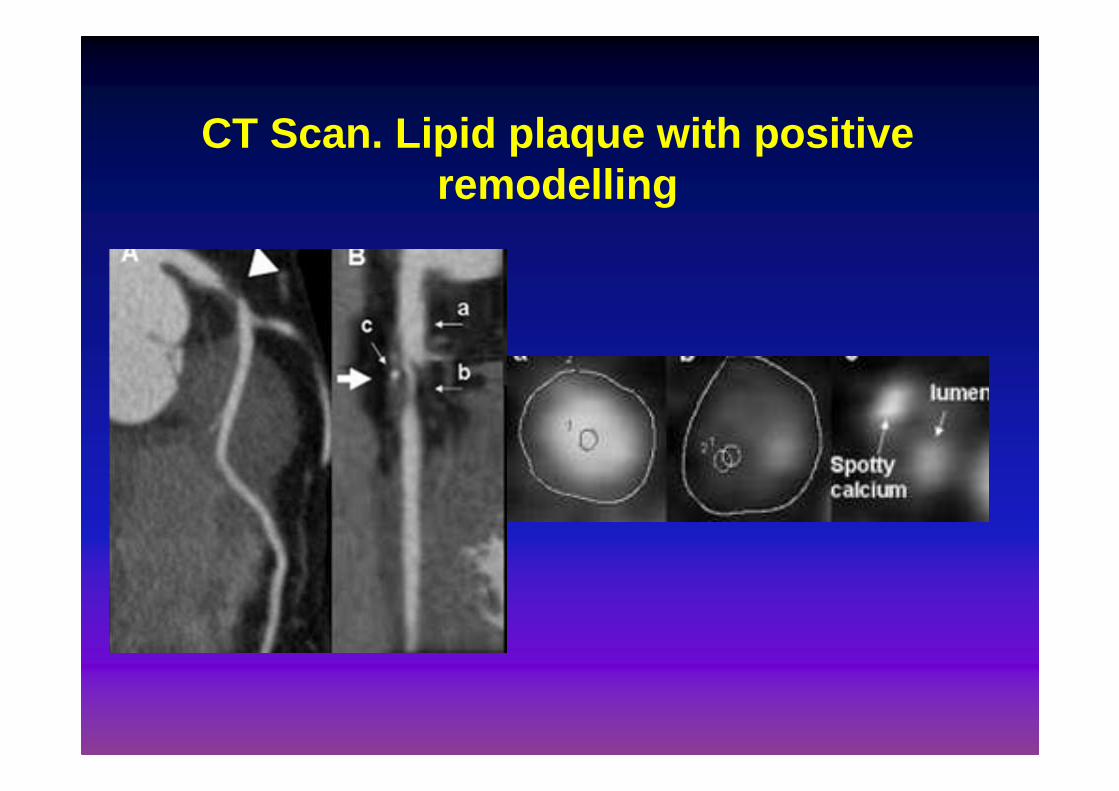
CT Scan. Lipid plaque with positive remodelling
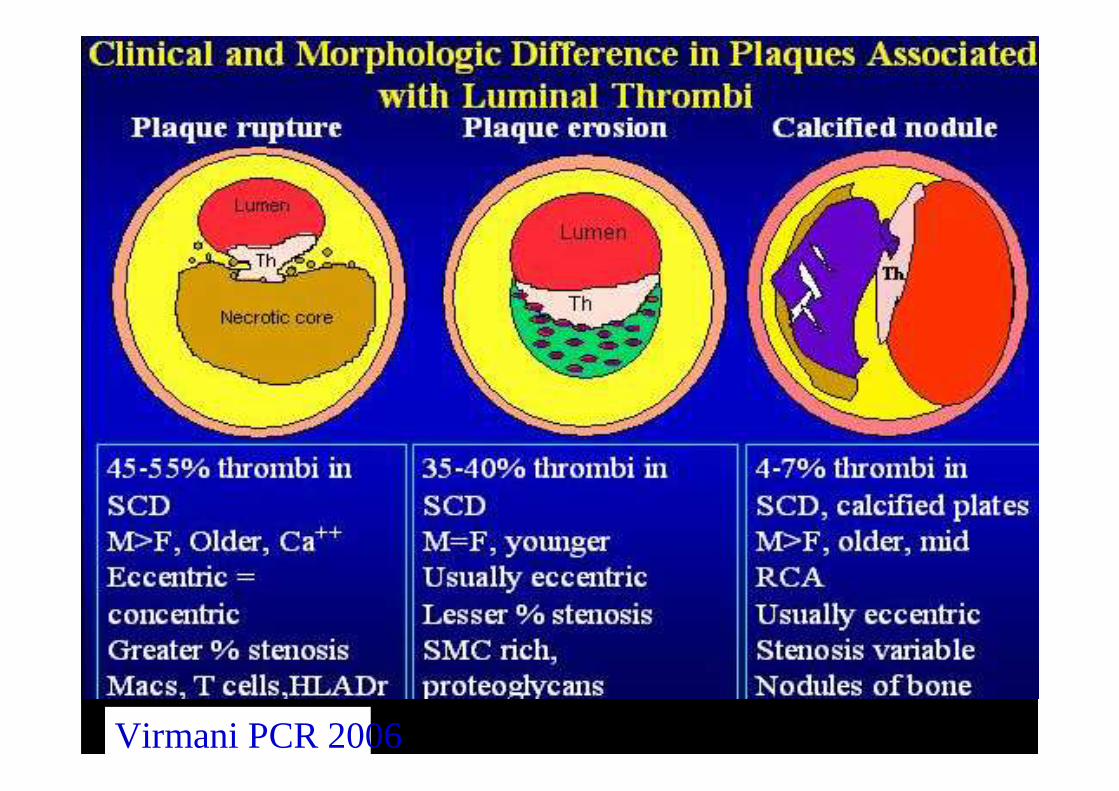
Virmani PCR 2006
MRI
ANGIOSCOPY
THERMOGRAPHY
IVUS OCT
SPECTROSCOPY
VIRTUALHISTOLOGY
CT
PET
…..yet 88.2% of patients with similar plaques did not have a major adverse cardiovascular event in a nonculprit lesion during 3.4 years of follow-up.
Attilio Maseri, Enrico Ammirati, Francesco Prati
Correspondence N Engl J Med 2011
Il trombo che si orgazizza può essere il substrato di nuovi
episodi infartuali ?

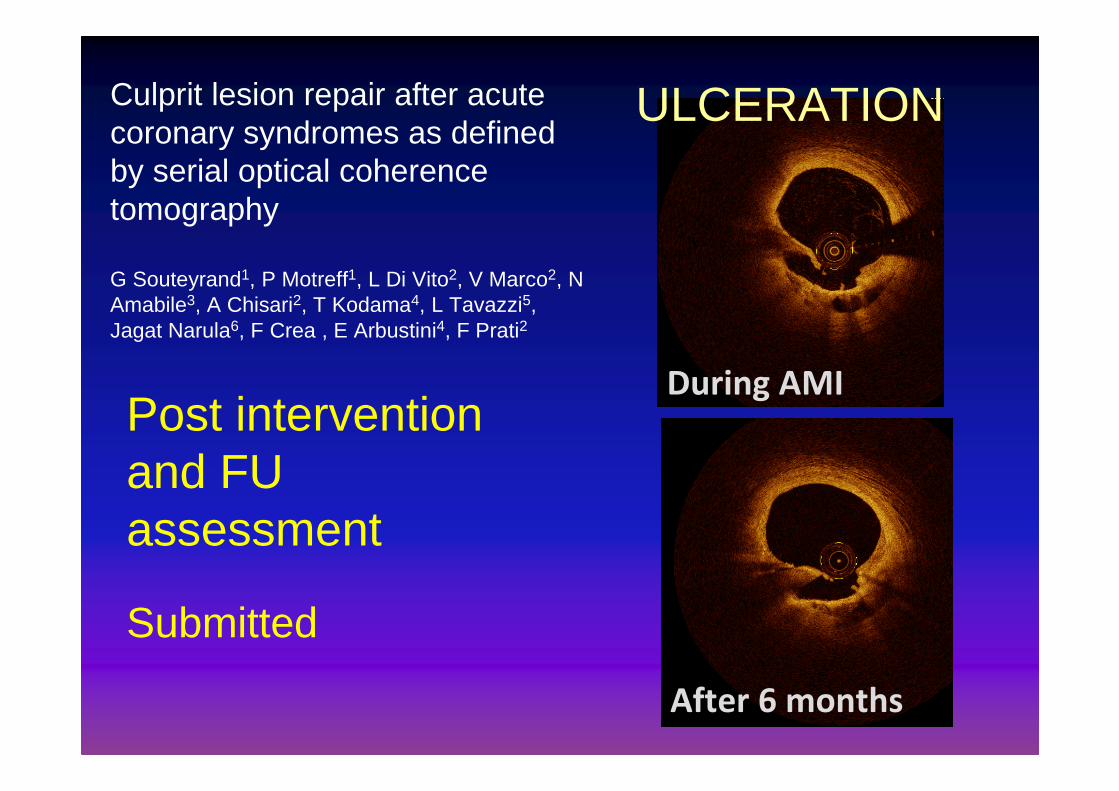
Culprit lesion repair after acute coronary syndromes as defined by serial optical coherence tomography
G Souteyrand1, P Motreff1, L Di Vito2, V Marco2, N Amabile3, A Chisari2, T Kodama4, L Tavazzi5, Jagat Narula6, F Crea , E Arbustini4, F Prati2
Post intervention and FU assessment
Submitted
EROSION
Culprit lesion repair after acute coronary syndromes as defined by serial optical coherence tomography
G Souteyrand1, P Motreff1, L Di Vito2, V Marco2, N Amabile3, A Chisari2, T Kodama4, L Tavazzi5, Jagat Narula6, F Crea , E Arbustini4, F Prati2
Post intervention and FU assessment
Submitted
After 6 months
During AMI
ULCERATION

E’ noto che molte trombosi intracoronariche sono silenti….. Tuttavia…….
•Quante sono le placche instabili in un soggetto con infarto?
•Una volta instabilizzatisi, per un meccanismo il piùdelle volta ulcerativo, la fissurazione della placca si rimargina subito?
•Il trombo che si orgazizza può essere il substrato di nuovi episodi infartuali ?
•Qual’è il contributo dell’infiammazione focale?

0
2
4
6
8
10
12
14
16
0-1 >2 >5
P=0,02
NYP NYP NYP
%
Multivariate logistic regression analysis: YP and mult ivessel di sease independent risk factors of ACS events .
Number of Yellow Plaques Detected in a Coronary Artery Is Associated With Future Risk of Acute Coronary SyndromeOhtani et al. JACC 2006
552 ptsFU 57.3 m
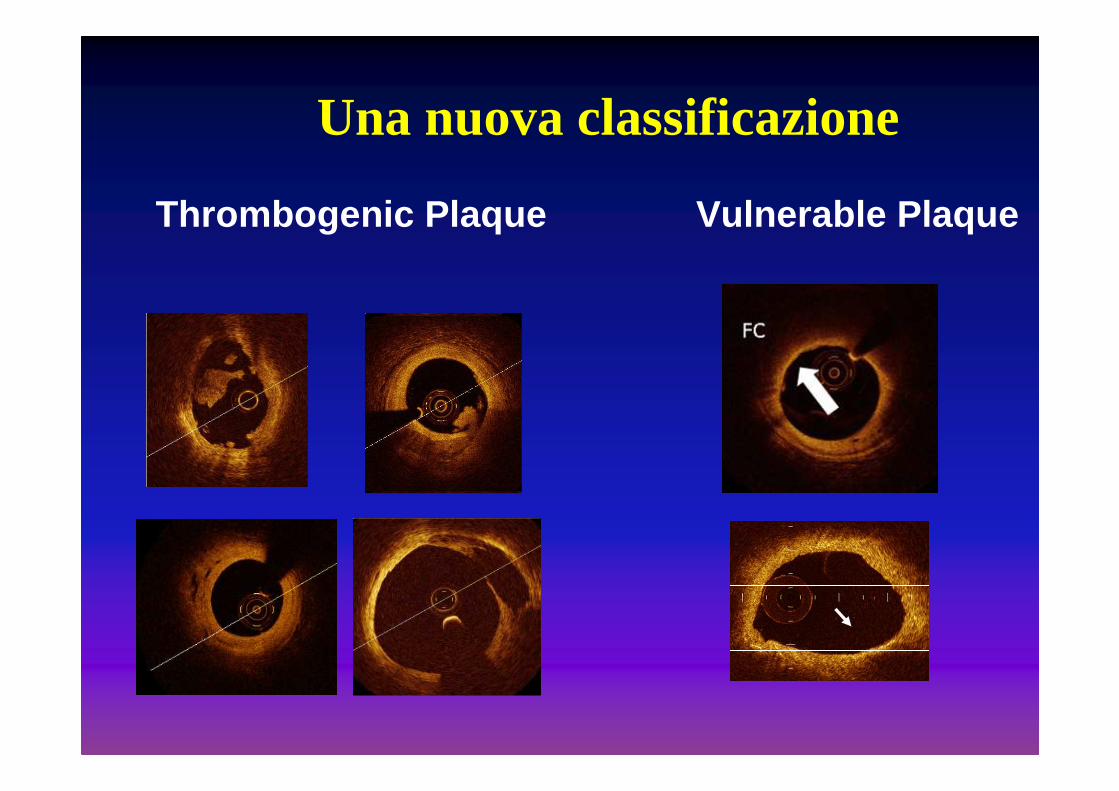
Thrombogenic Plaque Vulnerable Plaque
Una nuova classificazione
Quello che le placche non
dicono
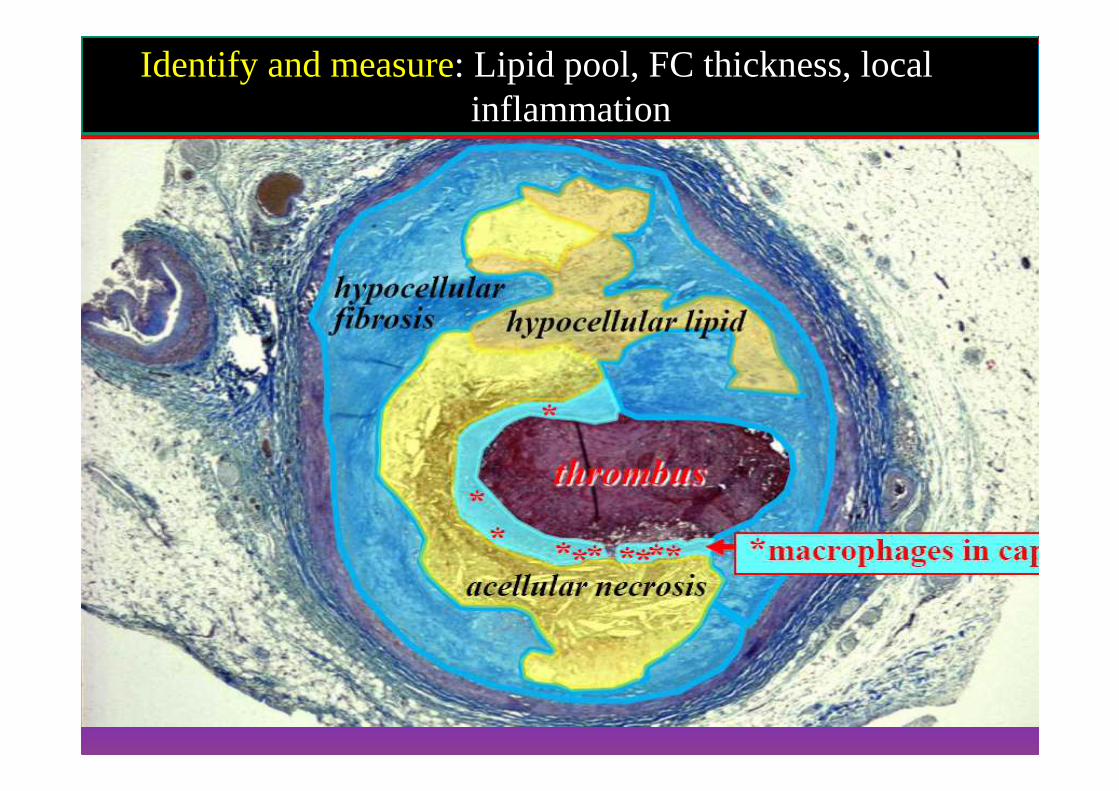
Identify and measure: Lipid pool, FC thickness, local inflammation
The role of local inflammation?
Quello che le placche non dicono
Histopathologic Characteristics of Atherosclerotic Coronary Disease and Implications of the Findings for the Invasiveand Noninvasive Detection of Vulnerable Plaques
Narula et al JACC 2013
Can OCT depict inflammation?

V liv. Vetrino 83 Fr 69CD 68 V liv. Vetrino 93
MOVAT IV liv. Vetrino 79 DAM II
Anche l’OCT ha dei limiti
LP
• Fusion of FD-OCT with other
Intravascular Imaging Modalities
( IVUS + NIRS)
From CLI Foundation and
Sansavini Foundation
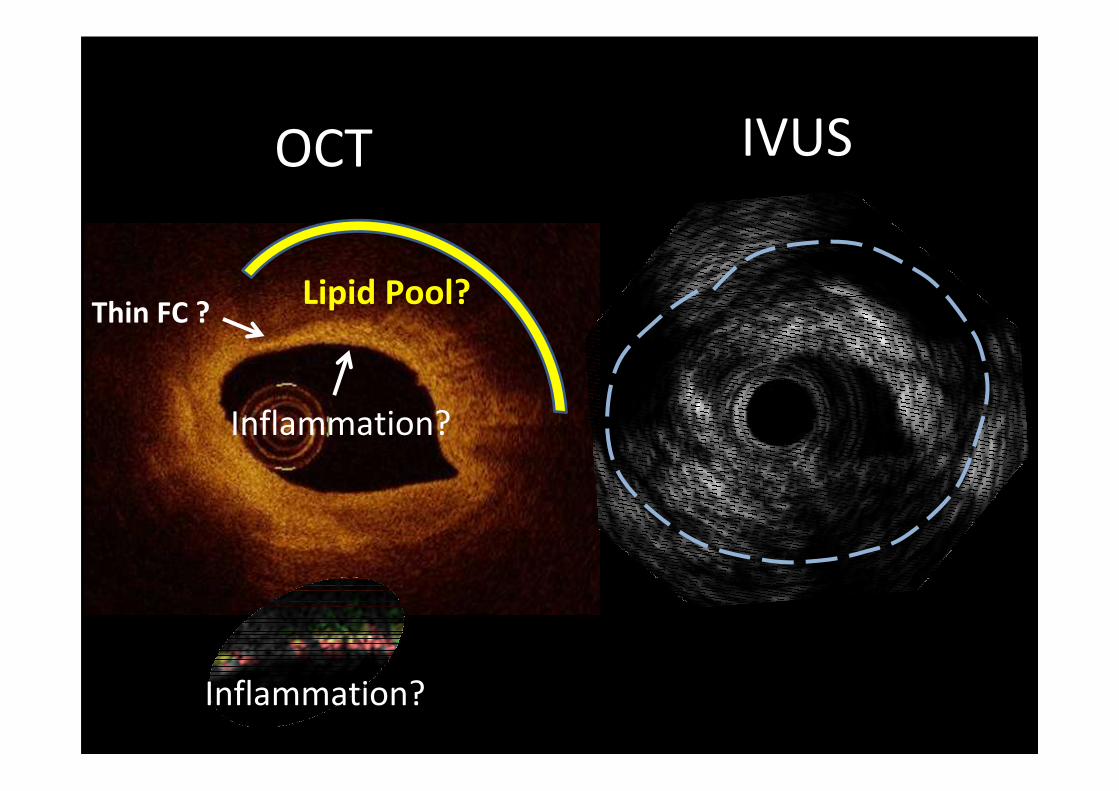
Lipid Pool?
Inflammation?
Thin FC ?
OCT IVUS
Inflammation?
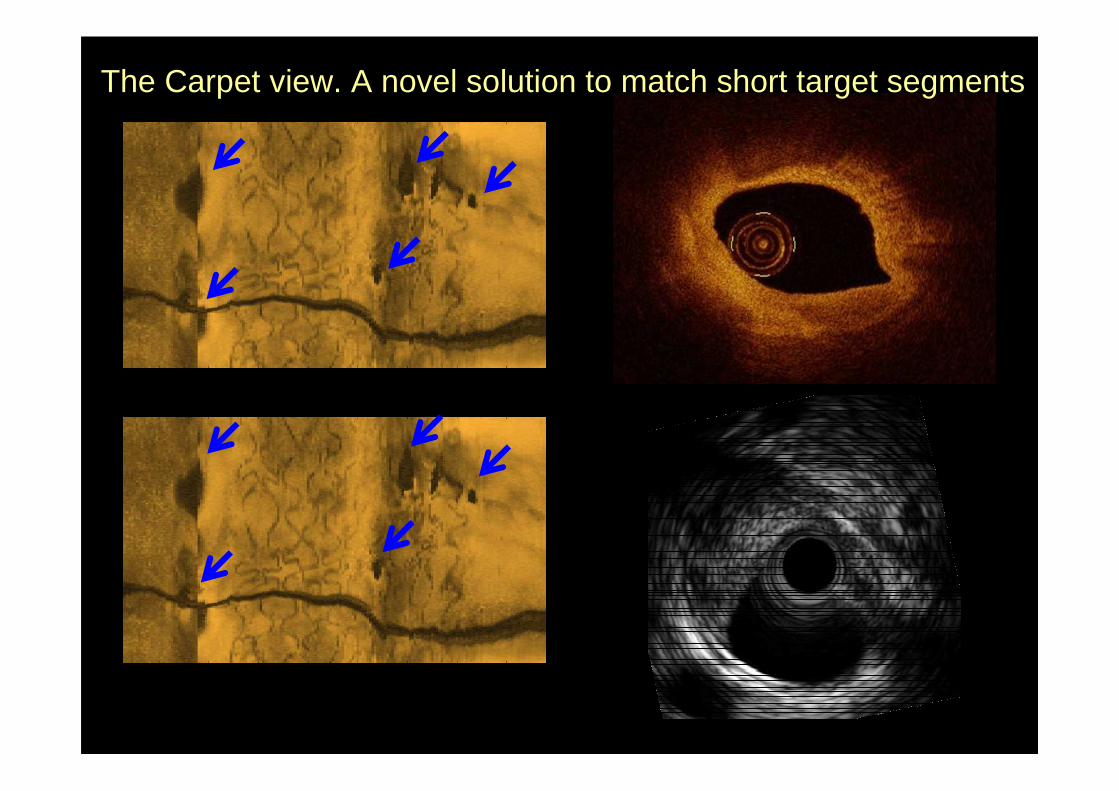
The Carpet view. A novel solution to match short target segments

The Future
Fusion of IVUS and FD-OCT
Fluorescence
Identification of vulnerable plaque causing ACS due to erosion is very difficult
What plaques don’t tell
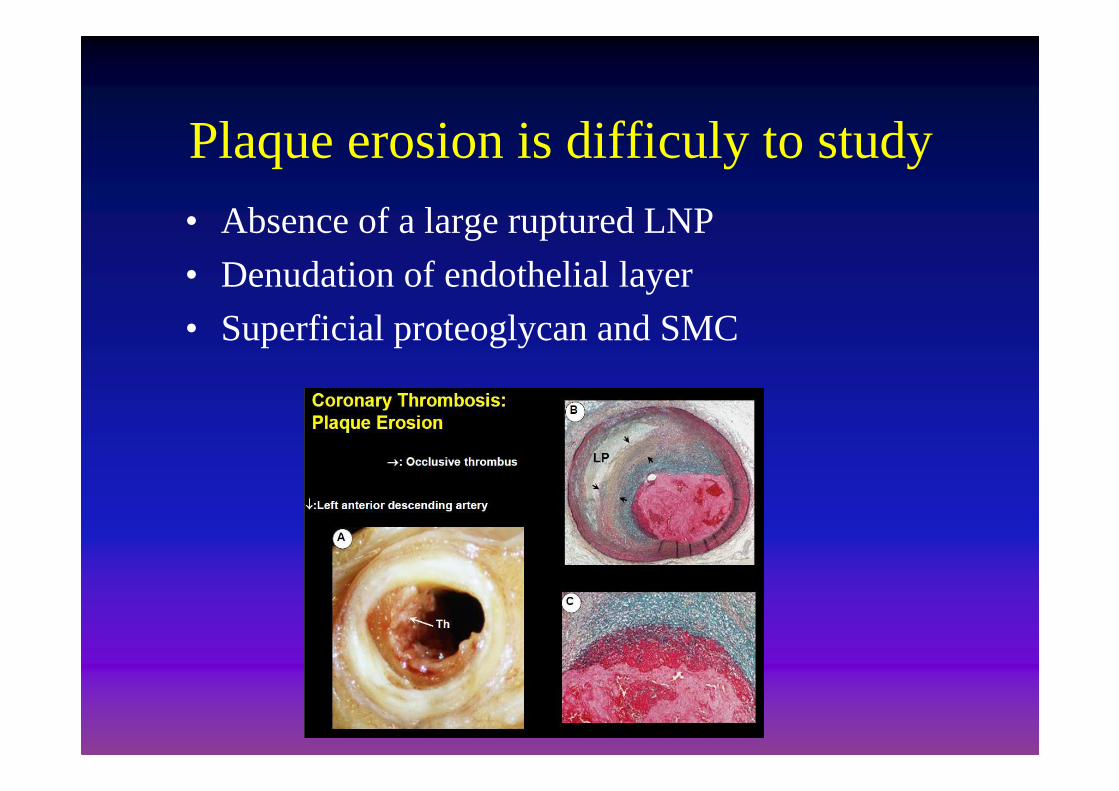
Plaque erosion is difficuly to study
• Absence of a large ruptured LNP
• Denudation of endothelial layer
• Superficial proteoglycan and SMC

Erosion Ulceration
Pts with an eroded plaque have significantly higher level of MPO as compared to those with a ruptured plaque [2500 vs. 707 ng/ml), p=0.001
Giuseppe Ferrante G, Nakano M, Prati F et al.Circulation 2010
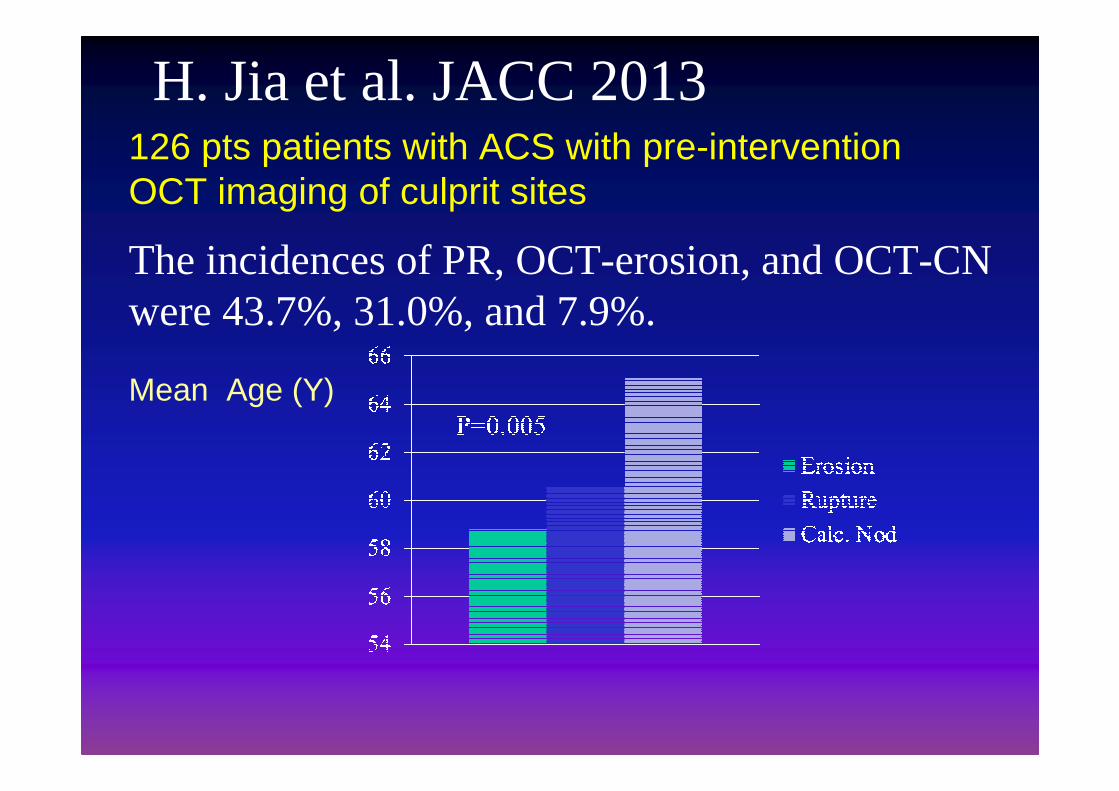
The incidences of PR, OCT-erosion, and OCT-CN were 43.7%, 31.0%, and 7.9%.
Mean Age (Y)
H. Jia et al. JACC 2013 126 pts patients with ACS with pre-intervention OCT imaging of culprit sites
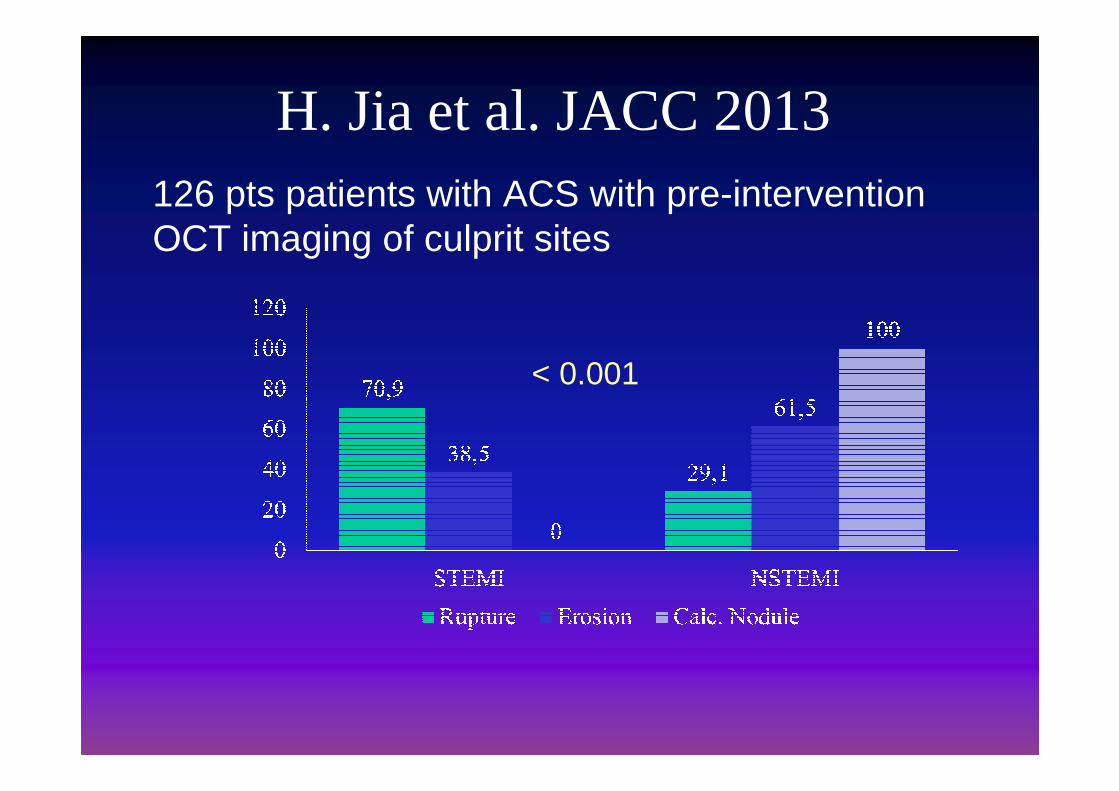
H. Jia et al. JACC 2013 126 pts patients with ACS with pre-intervention OCT imaging of culprit sites
< 0.001

I.C. imaging modalities don’t seem suited to study Hemorragy
What plaques don’t tell
L’imaging coronarico ha una utilità clinica?
1 4
5 4 3 2 1
2 3 5
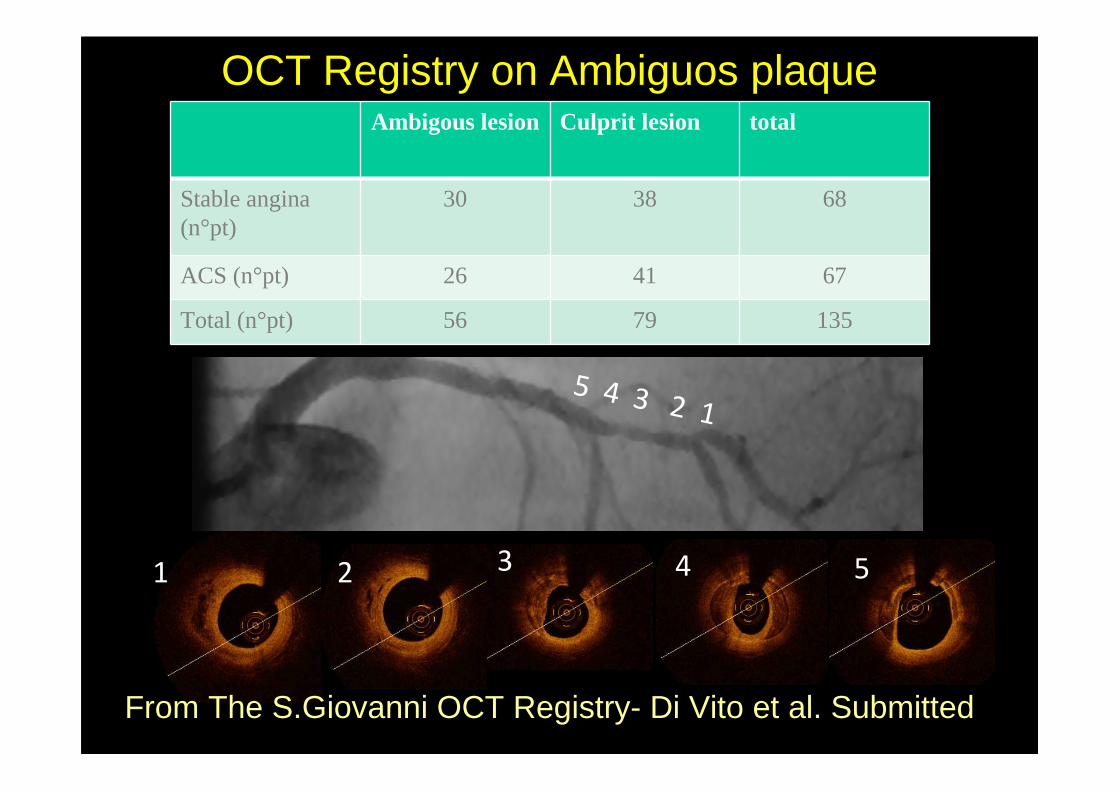
Ambigous lesion Culprit lesion total
Stable angina (n°pt)
30 38 68
ACS (n°pt) 26 41 67
Total (n°pt) 56 79 135
From The S.Giovanni OCT Registry- Di Vito et al. Submitted
OCT Registry on Ambiguos plaque
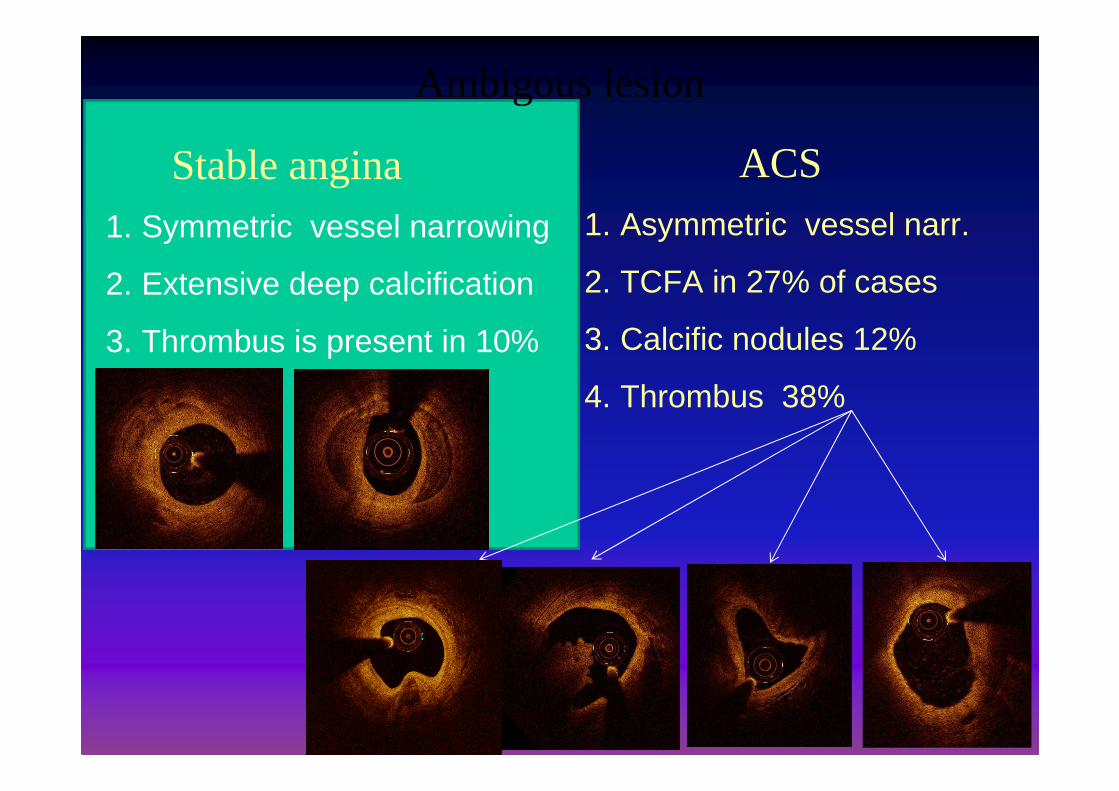
Ambigous lesion
Stable angina ACS
1. Symmetric vessel narrowing
2. Extensive deep calcification
3. Thrombus is present in 10%
1. Asymmetric vessel narr.
2. TCFA in 27% of cases
3. Calcific nodules 12%
4. Thrombus 38%
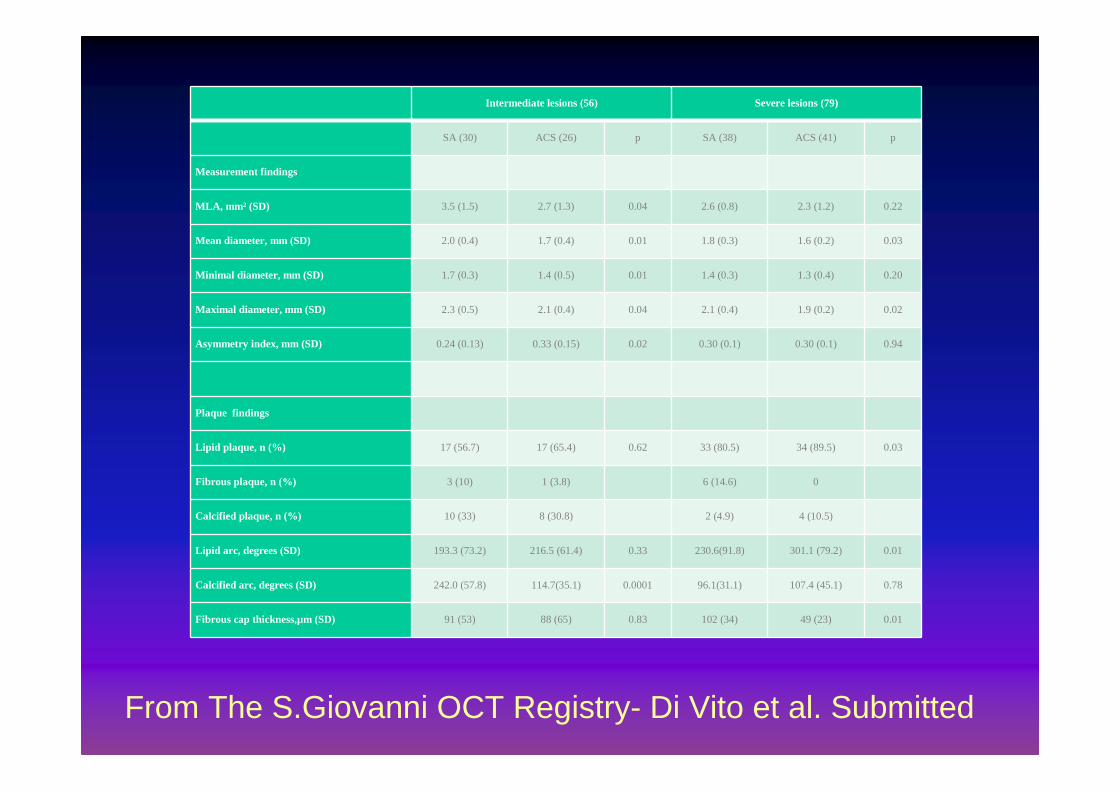
Intermediate lesions (56) Severe lesions (79)
SA (30) ACS (26) p SA (38) ACS (41) p
Measurement findings
MLA, mm 2 (SD) 3.5 (1.5) 2.7 (1.3) 0.04 2.6 (0.8) 2.3 (1.2) 0.22
Mean diameter, mm (SD) 2.0 (0.4) 1.7 (0.4) 0.01 1.8 (0.3) 1.6 (0.2) 0.03
Minimal diameter, mm (SD) 1.7 (0.3) 1.4 (0.5) 0.01 1.4 (0.3) 1.3 (0.4) 0.20
Maximal diameter, mm (SD) 2.3 (0.5) 2.1 (0.4) 0.04 2.1 (0.4) 1.9 (0.2) 0.02
Asymmetry index, mm (SD) 0.24 (0.13) 0.33 (0.15) 0.02 0.30 (0.1) 0.30 (0.1) 0.94
Plaque findings
Lipid plaque, n (%) 17 (56.7) 17 (65.4) 0.62 33 (80.5) 34 (89.5) 0.03
Fibrous plaque, n (%) 3 (10) 1 (3.8) 6 (14.6) 0
Calcified plaque, n (%) 10 (33) 8 (30.8) 2 (4.9) 4 (10.5)
Lipid arc, degrees (SD) 193.3 (73.2) 216.5 (61.4) 0.33 230.6(91.8) 301.1 (79.2) 0.01
Calcified arc, degrees (SD) 242.0 (57.8) 114.7(35.1) 0.0001 96.1(31.1) 107.4 (45.1) 0.78
Fibrous cap thickness,µm (SD) 91 (53) 88 (65) 0.83 102 (34) 49 (23) 0.01
From The S.Giovanni OCT Registry- Di Vito et al. Submitted
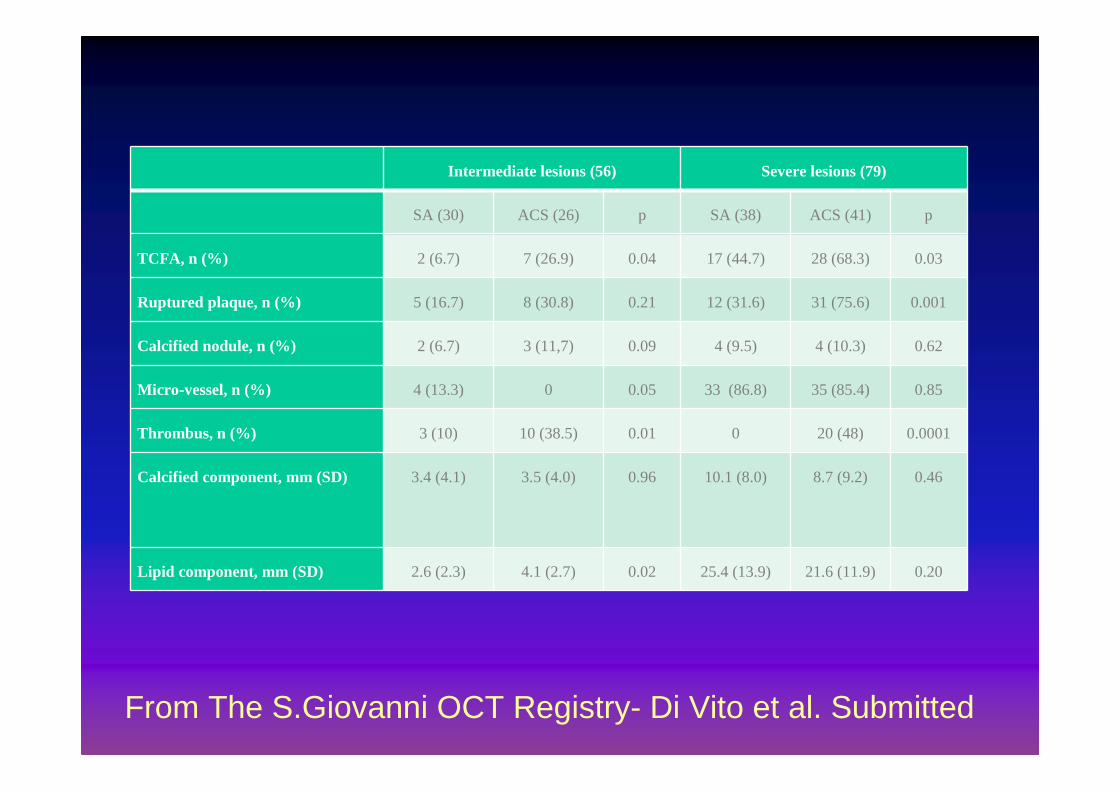
Intermediate lesions (56) Severe lesions (79)
SA (30) ACS (26) p SA (38) ACS (41) p
TCFA, n (%) 2 (6.7) 7 (26.9) 0.04 17 (44.7) 28 (68.3) 0.03
Ruptured plaque, n (%) 5 (16.7) 8 (30.8) 0.21 12 (31.6) 31 (75.6) 0.001
Calcified nodule, n (%) 2 (6.7) 3 (11,7) 0.09 4 (9.5) 4 (10.3) 0.62
Micro-vessel, n (%) 4 (13.3) 0 0.05 33 (86.8) 35 (85.4) 0.85
Thrombus, n (%) 3 (10) 10 (38.5) 0.01 0 20 (48) 0.0001
Calcified component, mm (SD) 3.4 (4.1) 3.5 (4.0) 0.96 10.1 (8.0) 8.7 (9.2) 0.46
Lipid component, mm (SD) 2.6 (2.3) 4.1 (2.7) 0.02 25.4 (13.9) 21.6 (11.9) 0.20
From The S.Giovanni OCT Registry- Di Vito et al. Submitted
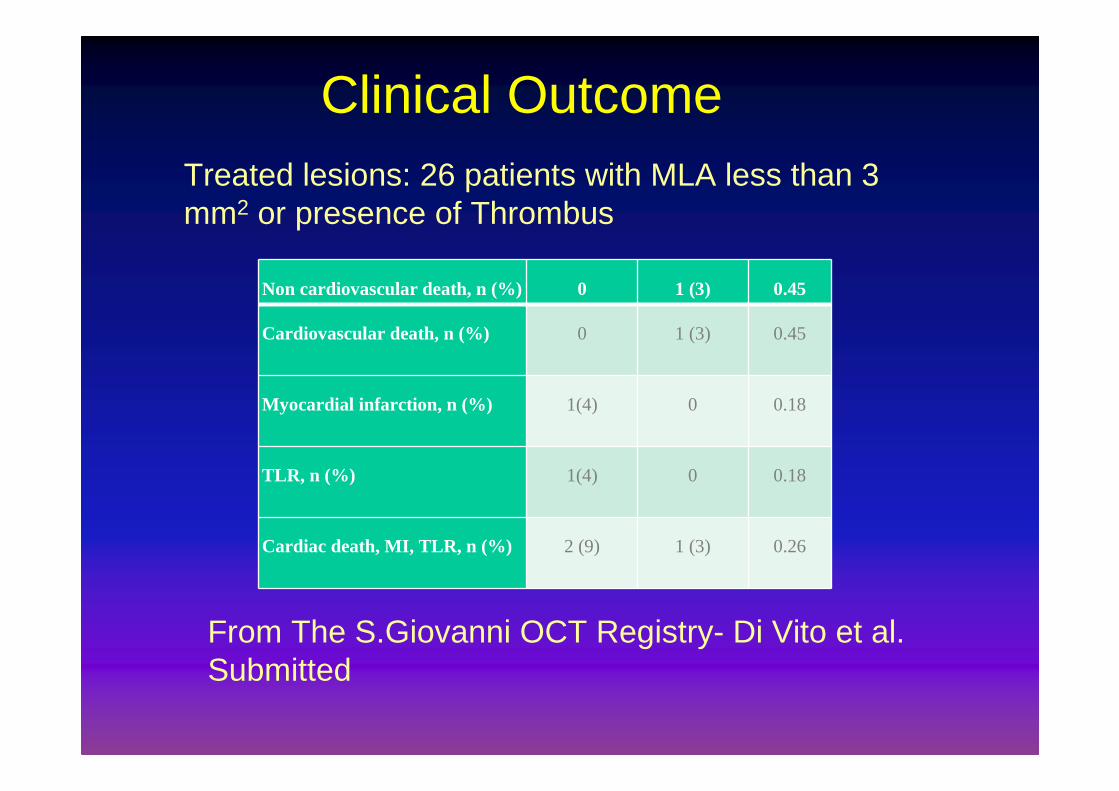
Non cardiovascular death, n (%) 0 1 (3) 0.45
Cardiovascular death, n (%) 0 1 (3) 0.45
Myocardial infarction, n (%) 1(4) 0 0.18
TLR, n (%) 1(4) 0 0.18
Cardiac death, MI, TLR, n (%) 2 (9) 1 (3) 0.26
From The S.Giovanni OCT Registry- Di Vito et al. Submitted
Treated lesions: 26 patients with MLA less than 3 mm2 or presence of Thrombus
Clinical Outcome
� OCT can identify acute plaque ulceration with or without thrombus. �Identification of FC rupture with thrombus has important clinical implications.
Conclusions

Conclusions
– Imaging modalities provide additional information compared to angiography.
– Their extensive use will broaden ourknowledge of the mechanism of local coronary thrombosis
– Use IC imaging to avoid useless interventions
– Use IC imaging to identify culprit lesions in patients with ACS (fresh thrombus)

• Che cosa c’è di nuovo nello studio OPPOSITES ?
• E’ uno studio “outliers” in cui si confrontano soggetti molto diversi tra loro: pz con recidiva infartuale ad un anno e pz con angina stabile da almeno 3 anni
• Applica nuovi concetti fisiopatologici ed in particolare la distinzione tra placche trombogeniche e vulnerabili.
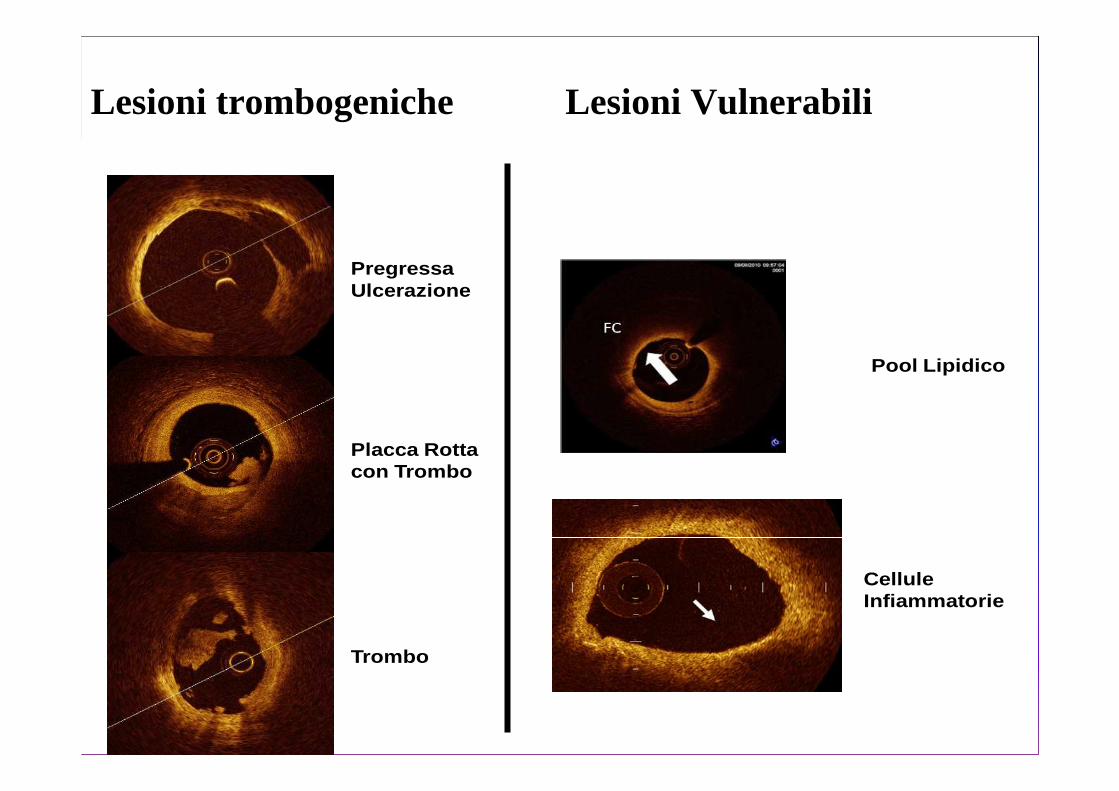
PregressaUlcerazione
Placca Rottacon Trombo
Trombo
Pool Lipidico
CelluleInfiammatorie
Lesioni trombogeniche Lesioni Vulnerabili
Metodi•Analisi del trombo aspirato
•Prelievi per via sistemica
•Effettuazione di FD-OCT più IVUS-NIRS in almeno 2 rami principali

Vulnerable plaque with high inflammatory cell
content
L’impiego dell’OCT con software dedicati per studiare l’infiammazione
OBIETTIVI DELLO STUDIO OPPOSITES
• Valutazione, mediante OCT, della prevalenza di siti trombogenici (escluso il vaso colpevole ) e di siti vulnerabili nell’albero coronarico di pazienti con primo IMA oppure con recidiva di IMA entro 1 anno in confronto a pazienti con cardiopatia ischemica cronica (angina stabile o ischemia da almeno 3 anni .
Alcune analisi esploratorie
• Valutazione delle caratteristiche infiammatorie nel sangue periferico(parametri infiammatori citochinici e linfocitari e della lipoproteina Lp(a).
• Valutazione delle caratteristiche distintive del trombo aspirato.
• Valutazione della presenza e del grado di “slow flow” in rami non correlati all’infarto.
• Definizione della prevalenza di siti trombogenici multipli e di tutte le variabili primarie e secondarie e correlazione con la presenza di angina preinfartuale
• Definizione della frequenza con cui la lesione colpevole presenta stratificazione di trombi, aventi età diversa.
Altre osservazioni• Non abbiamo ancora a disposizione la
tecnica di imaging ideale.
• La fusione di metodiche con l’OCT sembra essere la soluzione ottimale.
• Dobbiamo impiegare le tecniche di imaging per studiare nuovi aspetti fisiopatologici
• Utile effettuare studi seriati per studiare le variazioni dell’aterosclerosi
• Va applicata una nuova classificazione dell’aterosclerosi (placche vulnerabili vs trombogeniche)