Le linee-guida (LG): razionale, utilizzo, pregi e limiti · Bologna 26 Marzo 2010 Carlo Cammà...
83
Bologna 26 Marzo 2010 Carlo Cammà Cattedra di Gastroenterologia Università di Palermo [email protected] Le linee-guida (LG): razionale, utilizzo, pregi e limiti
Transcript of Le linee-guida (LG): razionale, utilizzo, pregi e limiti · Bologna 26 Marzo 2010 Carlo Cammà...

Bologna 26 Marzo 2010
Carlo CammàCattedra di Gastroenterologia
Università di [email protected]
Le linee-guida (LG): razionale, utilizzo, pregi e limiti

LG:
• razionale
• utilizzo: HCV, HBV, HCC, CD.
•pregi e limiti
LG in gastroenterologia
Definizione“Raccomandazioni di comportamentoclinico, prodotte attraverso un processosistematico, allo scopo di assistere medicie pazienti nel decidere quali siano lemodalità di assistenza più appropriate inspecifiche circostanze cliniche”.
Sono basate sulle migliori evidenze disponibili
Sono di aiuto ai clinici, ma non ne ostituiscono il sapere e le capacità.
LG: razionale

RCTs
Sistematic Reviews/MA
PRACTICE GUIDELINES
HealthPolicy
Clinicalpractice
Patientsinformation
OtherEvidence
LG: razionale

5
I problemi di traslazione delle “evidenze” dagli RCTs alla pratica hanno determinato l’intermediazione di specialisti clinici e di metodologi e l’elaborazione di linee-guida per un accesso facilitato dei medici alle “evidenze”.
RCTs
Specialisti
Specialisti clinici e metodologi:
• Ricerca di RCTs e di altre evidenze
• Loro selezione• Interpretazione• Integrazione e traduzione in raccomandazioni
Linee-guida
La maggioranza dei clinici
EBM EBM
LG: razionale

Obbiettivi• Migliorare la qualità dell'assistenza • Ottimizzare l'esito degli interventi sui pazienti • Scoraggiare l'uso di interventi inefficaci o
pericolosi• Migliorare e garantire l'appropriatezza delle cure • Identificare zone grigie della pratica clinica in cui
vi è insufficiente evidenza• Aiutare a bilanciare costi e risultati
LG: razionale
Priorità• Rilevanza clinica:
– Elevata frequenza– Alto rischio– Alti costi– Variabilità
• Multidisciplinarietà
• Alta qualità delle evidenze disponibili (?)
LG: razionale
Metodologia di Produzione• Obiettivi • Opzioni (Soc vs ??)• Esiti o risultati • Evidenze • Valori (Metodo di Consenso)• Benefici, danni e costi • Raccomandazioni • Validazione • Sponsor
LG: razionale

Livelli di prova e forza delle raccomandazioni
due informazioni parzialmente complementari e largamente indipendenti
LIVELLI DI PROVA• valutano la qualità
metodologica delle evidenze disponibili
FORZA DELLE RACCOMANDAZIONI
• Valuta anche:– la fattibilità, – i benefici attesi e la loro
rilevanza– le implicazioni
organizzative, economiche, sociali e finanziarie di uno specifico intervento
0
5000
10000
15000
20000
25000
1982-1992 1995-2005
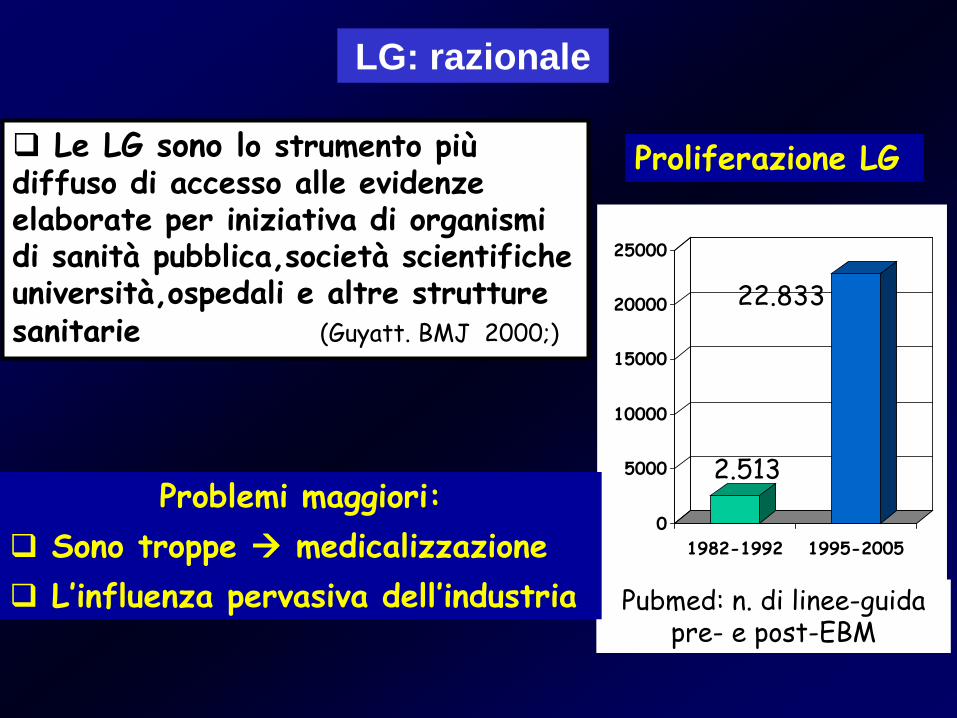
Pubmed: n. di linee-guida pre- e post-EBM
2.513
22.833
Le LG sono lo strumento più diffuso di accesso alle evidenze elaborate per iniziativa di organismi di sanità pubblica,società scientifiche università,ospedali e altre strutture sanitarie (Guyatt. BMJ 2000;)
Proliferazione LG
Problemi maggiori: Sono troppe medicalizzazione L’influenza pervasiva dell’industria
LG: razionale
11
NICE (National Institute for Health and Clinical Excellence) Clinical GuidelinesSIGN (Scottish Intercollegiate Guidelines Network)US Preventive Services Task Force GuidelinesNational Academies USA GuidelinesAmerican College of Physicians Guidelines (ACP) Piano nazionale linee Guida (PNLG)
LG: razionale

Fattori che favoriscono l’aderenza alle linee-guida
• LG centrate su priorità reali di terapia o prevenzione• Panel multidisciplinari• Qualità delle evidenze (trial randomizzati concordanti) • Raccomandazioni chiare, specifiche, concise, • Gradi di evidenza e forza delle raccomandazioni • Adeguamento sistematico a nuove evidenze dalla ricercascientifica (Manutenzione)
• Implementazione efficace e continua
LG: razionale
• E inoltre: Molte linee-guida forniscono indicazioni che integrano
il trattamento o la prevenzione con la diagnosi, loscreening, o la valutazione dei fattori di rischio –p.es, sono così strutturate circa la metà delle linee-guida del NICE pubblicate in sintesi nel BMJ nel 2007 e 2008, e delle linee guida presentate nel sito online di PNLG.
Fattori che favoriscono l’aderenza alle linee-guida
LG: razionale

1. Tendono a medicalizzare soggetti sani per remoti fattori di rischio: “The last well person” (Meador CK, N Engl J Med 1994; 330: 440-41)
2. Non sempre sono applicabili in pazienti con comorbidità (Boyd CM & al,JAMA 2005: 294:716-24;
van Weel C, Schellevis FG Lancet 2006; 367: 550-1)3. Accettazione e compliance incomplete da parte dei
medici (Cabana MD, & al. JAMA 1999; 282: 1458-65;Farquhar CM& al. MJA 2002; 177: 502-6)
4. Conflitti d’interesse non risolti (Choudhry NK & al. JAMA 2002; 287: 612-7; Taylor R, Giles J. Nature 2005; 437: 1070-71)
LG: razionale
Problemi per la valutazione delle LG

1. Tendono a medicalizzare soggetti sani
Problemi per la valutazione delle LG
L’uso delle LG Europee 2003 per la prevenzione CV classifica il 76% dei norvegesi ≥ 20 anni e il 90% di quelli ≥ 50 anni come soggetti con colesterolo e/o pressione arteriosa a rischio.
Esistono importanti dilemmi etici sull’implementazione delle LG, relative alla medicalizzazione, all’allocazione delle risorse, e alla sostenibilità nel sistema sanitario.
LG: razionale

Nonconoscenzadelle LG,
incapacitàdi accesso
Mancanza di fiducia, disaccordo:
con le LG in generale (“cookbook medicine”) con una particolare
LG (p. es, non evidence-based)
Incapacità di modificare lo stile di vita dei pz (p. es,
stop al fumo) comorbidità, molti
farmaci
ConoscenzaAtteggiamento
Paziente
Il non uso di LG appropriatamente elaborate causa la sotto-utilizzazione di procedure mediche efficaci
3. Ostacoli all’uso delle linee-guida
Problemi per la valutazione delle LG
LG: razionale

Choudhry NK & al. Studio su 192 AA di 44 LG, 1991-99: il 59% degli AA di LG avevano rapportid’interesse con ditte farmaceutiche i cui prodotti erano raccomandati nelle LG da essi elaborate. JAMA 2002; 287: 612-7.
4. Conflitti d’interesse non risolti
Problemi per la valutazione delle LG
“At present, the financial ties between guidelines panels and industry are extensive”
LG: razionale

• La diffusione passiva è insufficiente a modificare lapratica clinica
• Perché una LG sia efficace occorre che sia disseminatacon adeguato materiale di supporto (quick references,flow chart, reminder)
• Importanza della condivisione e dell’adattamento allecondizioni locali seguendo una metodologia esplicita.
Disseminazione ed adattamento locale
LG: razionale

Valutazione di efficacia
• L’efficacia delle LG deve essere “misurata”attraverso adeguati audit clinici di verifica deicomportamenti assistenziali.
• Selezionare per ciascuna LG indicatori specificiper misurarne l’efficacia (indicatori di processo,indicatori di esito).
LG: razionale

LG:
• razionale
• utilizzo: HCV, HBV, HCC.
•pregi e limiti
LG: Utilizzo
HCV
LG: Utilizzo

• To be released, february 2009
• To be released, mid 2010
•To be released, 2010
• 2007
• 2008
New HCV guidelines: issues for debate

New HCV guidelines: issues for debate• Whom to treat ? How to treat ?• Response-guided therapy as:
• short therapy for G2 and G3 (all ?)• short therapy for G1 LVL • long therapy for slow responders
• What is the appropriate dose of:• PEG IFN ? PEG a-2a vs. PEG a-2b ?• RBV ?
• Retreatment of NR / Maintenance Therapy ?

New HCV guidelines: issues for debate
• Whom to treat?• Response- guided therapy as:
• short therapy for G2 and G3 (all?)• short therapy for G1 LVL • long therapy for slow responders
• What is the appropriate dose of:• PEG IFN? PEG a-2a vs. PEG a-2b ? • RBV?
•Retreatment of nonresponders

What is the appropriate dose of PEG IFN ?
A noprofit RCT in 311 genotype 1 naïve pts.
2004

What is the appropriate dose of PEG IFN?
SVR=41%
PEG-IFN a2-b 1.5 µg/Kg
SVR = 42% (1)
(1) Manns Lancet 2001
genotype 1 naïve pts.

What is the appropriate dose of PEG IFN?

0
20
40
60
80
38%41%
% P
azie
nti c
onU
ndet
ecta
ble
HC
V R
NA
PEG 2b 1.0 /R(n=1016)
PEG 2a /R(n=1035)
40%
PEG 2b 1.5 /R(n=1019)
PEG-IFN alfa-2b 1.5/RBV vs. PEG-IFN alfa-2a 180/RBV, P= 0.57
PEG-IFN alfa-2b 1.5/RBV vs. PEG-IFN alfa-2b 1.0/RBV, P= 0.20
IDEAL
Genotype 1
What is the appropriate dose of PEG IFN?

New HCV guidelines: issues for debate
••
•••
•••
•
PEG a-2a vs. PEG a-2b ?
• Whom to treat?• Response- guided therapy as:
• short therapy for G2 and G3 (all ?)• short therapy for G1 LVL • long therapy for slow responders
• What is the appropriate dose of:• PEG IFN? PEG a-2a vs. PEG a-2b ? • RBV?
•Retreatment of nonresponders
• Maintenance therapy
New HCV guidelines: issues for debate

Maintenance therapy
2004
New HCV guidelines: issues for debate

Correlation between STAGING improvementand virological response

2001
Maintenance therapy
New HCV guidelines: issues for debate

Favors SR Favors Control
No significant heterogeneity
IFN treatment and incidence of HCC
Sustained Responders vs untreated controls
HCV-related cirrhosis (Child A)

Maintenance therapyNew HCV guidelines: issues for debate

HALT-C
Maintenance therapy
New HCV guidelines: issues for debate

R
T
C
???
Ethics in clinical research
Risk/benefit
Risk/benefit
Uncertainty principle
New HCV guidelines: issues for debate

New HCV guidelines: issues for debate

• Whom to treat?• Response- guided therapy as:
• short therapy for G2 and G3 (all ?)• short therapy for G1 LVL • long therapy for slow responders
• What is the appropriate dose of:• PEG IFN? PEG a-2a vs. PEG a-2b ? • RBV?
•Retreatment of nonresponders• Maintenance therapy
New HCV guidelines: issues for debate

Retreatment of nonresponders
Released, 2009
Relatore
Note di presentazione
Slide 38. Comparative data: conclusions PEGASYS® has demonstrated higher SVR rates than pegylated interferon alfa-2b (12KD) in a number of randomised trials using similar ribavirin doses or reduction protocols. There is also accumulating data from real-world cohort studies that demonstrates higher rates of SVR achieved with PEGASY® compared to pegylated interferon alfa-2b (12KD) Patients and physicians alike consider the PEGASYS® pre-filled syringe to be more user friendly than the pegylated interferon alfa-2b (12KD) Redipen.

FULL PAPERS
ABSTRACTS
SVR after retreatment of non-responders to (PEG) IFN and RBV: a meta-analysis of 5,576 patients from 20 studies
Sustained Virological Response

3) due to its low probability of clinical benefit the decision to retreat subjects infected with HCV genotype 1 should be assessed in the individual patient according to the likelihood of disease progression and of adverse events.
Retreatment of nonrespondersWhat are the implications of this meta-analysis for current practice?
1) the modest overall efficacy and tolerability, and the inconsistency in the reported SVR rates amongst trials, argue against indiscriminate retreatment for all NR pts;
2) restricting retreatment to non-overweight patients or to those with genotype 2 or 3 optimizes the potential benefit;
Relatore
Note di presentazione
Slide 38. Comparative data: conclusions PEGASYS® has demonstrated higher SVR rates than pegylated interferon alfa-2b (12KD) in a number of randomised trials using similar ribavirin doses or reduction protocols. There is also accumulating data from real-world cohort studies that demonstrates higher rates of SVR achieved with PEGASY® compared to pegylated interferon alfa-2b (12KD) Patients and physicians alike consider the PEGASYS® pre-filled syringe to be more user friendly than the pegylated interferon alfa-2b (12KD) Redipen.

HBV
LG: Utilizzo
• AASLD : febbraio 2007
• AISF – SIMIT – SIMAST : maggio 2008
• EASL : ottobre 2008
• NIH : gennaio 2009 - Scritte da un comitato di non esperti
- Assenza conflitto di interessi.
- Rigorosamente “ Evidence – based “
New HBV guidelines: issues for debate
LG: Utilizzo

J Hep 2009
Reliable surrogates ?

Shamliyan. Ann Intern Med 2009;
Data synthesis on clinical outcomes (death, HCC, liver failure, prevalence and incidence of cirrhosis) :• In 16 RCTs (4431 pts), drug treatment (IFN a2b, Peg a2a or NUCs) did not improve clinical outcome, however none were of sufficient size or duration or were designed to assess clinical outcome.
Conclusions:• Evidence was insufficient to assess treatment effect on clinical outcome or determine whether improvements in selected intermediate measures are reliable surrogates.• Individual studies reported very few events and compared different drugs and patients precluding definitive conclusions
TRUE OUTCOMES
LG: Utilizzo
• Lack of standardized criteria of response
• Combined assessment of outcomes of different relevance
• PEG-IFN: Shorter/Longer therapy and lower doses; How to use in combination with NUCs
• A “weak” comparator, or placebo
Biases of sponsored trials in HBV
New HBV guidelines: issues for debate

Standard of care
New Standard
Marked heterogeneity in study samples, interventions, and measured outcomes preclude definitive conclusions.
PEG-IFN LAM ADF ETV TDFLtD
Standard of care
New Standard

HCC
LG: Utilizzo

JNCI 2008
Med Clin (Barc) 2009
Hepatology 2005/ 2010
New HCC guidelines: issues for debate
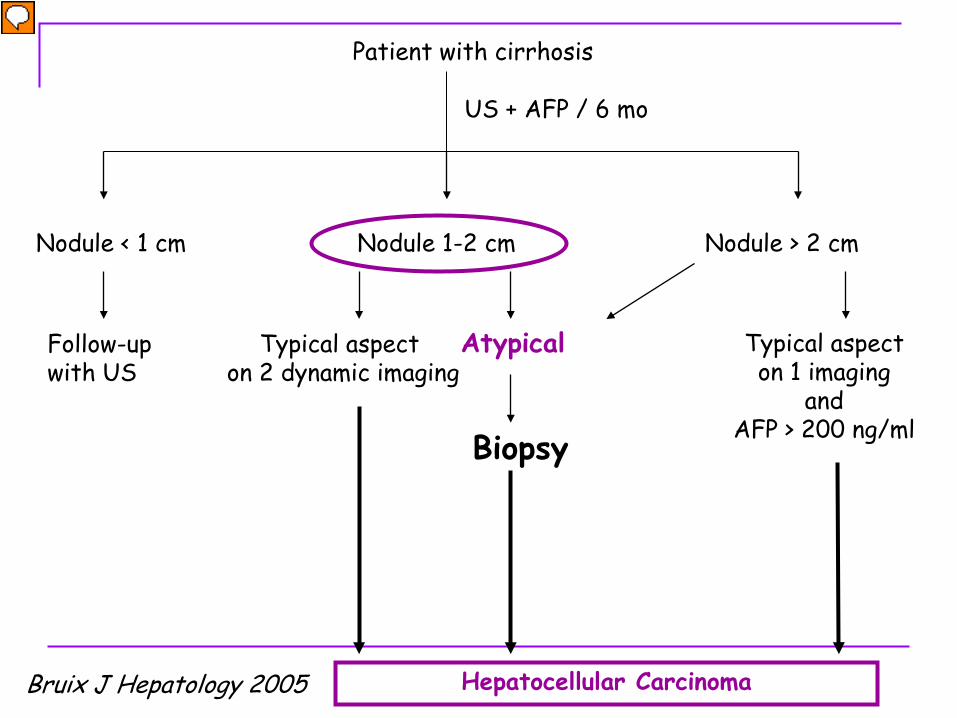
Patient with cirrhosis
Nodule < 1 cm
US + AFP / 6 mo
Nodule 1-2 cm Nodule > 2 cm
Follow-up with US
Typical aspect on 2 dynamic imaging
Atypical
Biopsy
Hepatocellular Carcinoma
Typical aspecton 1 imaging
andAFP > 200 ng/ml
Bruix J Hepatology 2005
Relatore
Note di presentazione
Ultrasonography Biopsy is considered only when nodule is
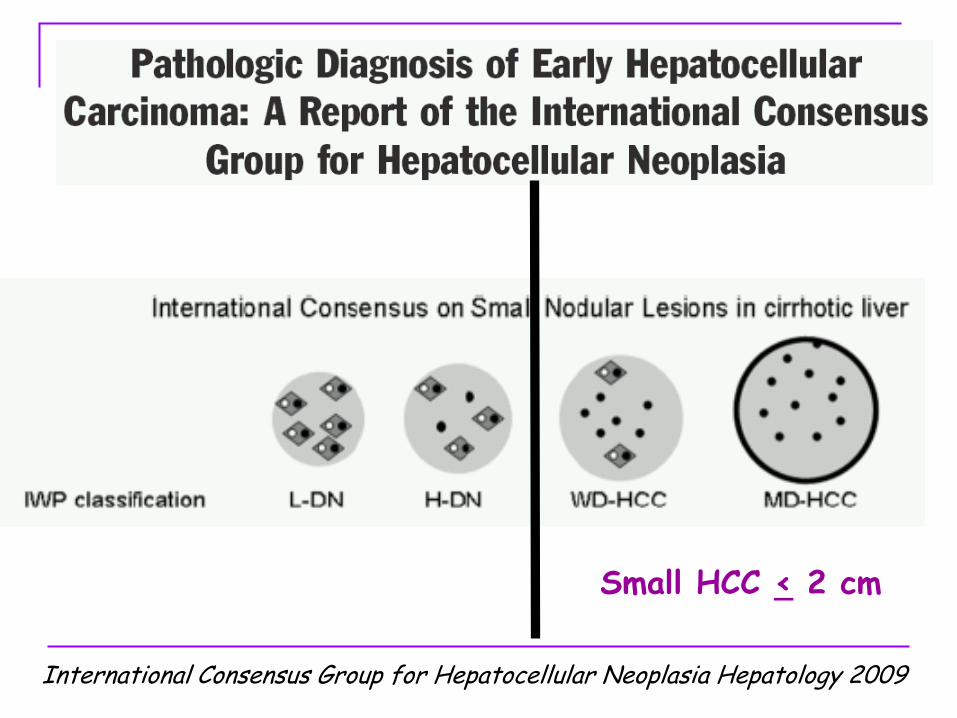
International Consensus Group for Hepatocellular Neoplasia Hepatology 2009
Small HCC < 2 cm

Performance depends on …
Location & Accessibility of the nodule
Procedure of the biopsy Fine needle aspiration (20-25 G)
Only cytology Needle core biopsy (14-18 G)
Cytology and Histology that allows analysis of architecture of the proliferation
More performant for the differential diagnosis of hepatocellular nodules
Sampling error Dg features may miss in minute
biopsy specimens

Performance of Biopsy Could/Should Be Improved
Surrogate molecular markers

Patient with cirrhosis
Nodule < 1 cm
US + AFP / 6 mo
Nodule 1-2 cm Nodule > 2 cm
Follow-up with US
Typical aspect on 2 dynamic imaging
Atypical
Biopsy
Hepatocellular Carcinoma
Typical aspecton 1 imaging
andAFP > 200 ng/ml
Bruix J Hepatology 2005
Relatore
Note di presentazione
Ultrasonography Biopsy is considered only when nodule is

Nodules < 10 mmWait and see policy ?
Caturelli E et al Gut 2004
HCC diagnosis based on histology in 72.7 % (24/33)

Very early stage (0) Single< 2cm.
Portal pressure/ bilirubin
PST >2, Child-Pugh C
Terminal stage (D)
PST 0-2, Child-Pugh A-BStage A - C Stage D
Normal
Single 3 nodules <3cm
Associated diseasesIncreased
No Yes
Early stage ( A)Single or 3 nodules < 3cm, PS 0
Intermediate stage ( B)Multinodular, PS 0
Advanced stage (C)Portal invasion, N1,M1, PS 1-2
Stage 0PST 0, Child-Pugh A
BCLC Staging and Treatment Strategy HCC
Liver Transplantation (CLT / LDLT)
ChemoembolizationResection PEI/RF
Sympt. Treat. (20%)
Curative Treatments (30%)40% - 75% at 5 years
Non-curative treatments (50%)3 year survival 10-40%
Sorafenib

LG: Utilizzo

AUROC for BCLC, CLIP and GRETCH in 178 treated patients.
LG: Utilizzo

AUROC for BCLC, CLIP and GRETCH in 228 untreated patients.
LG: Utilizzo

Portalpressure/bilirubin
New BCLC staging classification – 2008
Llovet JM et al. J Natl Cancer Inst 2008;100: 698 – 711
HCC
Stage 0PST 0, Child-Pugh A
Stage A-CPST 0-2, Child-Pugh A-B
Stage DPST>2, Child-Pugh C
Early stage (A)Single or 3 nodules
< 3 cm, PST 0
Intermediate stage (B)Multinodular, PST 0
Advanced stage (C)Portal invasion,
N1, M1, PST 1-2
Terminalstage (D)
Very early stage (O)Single < 2 cm
(carcinoma in situ)
Single 3 modules ≤ 3 cm
Normal No Yes
AssociateddiseasesIncreased
Resection Liver Transplantation(CLT/LDLT) PEI/RF Chemoembolization Sorafenib
Curative treatments (prevalence 30%)
5 yr survival: 50 - 70%
RCT (prevalence 50%)
3 yr survival: 20 - 40%
Symptomatic t. (prevalence 20%)
1 yr survival: 10 - 20%
Unresectable HCC
Milano in Milano out
About 70% of pts with HCC are diagnosed at BCLC B, C or D stages.
In this setting different palliative treatments (chemoembolization, systemic chemo- , immuno-,
hormonal therapy and sorafenib) have been proposed.
ResectionVs
OLT??????
Stopping Early for Benefit
LG: Utilizzo

RCTs can overestimate the magnitude of the treatment effectdepending on the timing (ie, expected number of events) of the decision to stop.
Lack of adequate safety data may affect the risk-benefit ratios (underestimating the risk) of implementing the intervention in clinical practice.
These considerations suggest that clinicians should view results of RCTs stopped early for benefit with skepticism.
143 RCTs
JAMA 2005
The results of a single trial should be interpreted with caution. When it is difficult to predict how trial specific factors influence the results, the best way to evaluate the performance of a treatment is to use multiple trials.
LG: Utilizzo
Standard of care
New Standard
1 RCT Stopping early
?
• chance variation• subject selection• design and execution of the trial• treatment administration or dosage• concomitant exposures• outcome assessment• local health care system• the way the investigational site is organized• statistical methods used in the analysis.
It is often impossible to identify exactly which factor(s) caused the differences between the results. This (unexplained) heterogeneity means that study results must be interpreted with caution.
Even when multiple trials are designed to address the same question, their results and conclusions may differ.Possible explanations for these differences are:
LG: Utilizzo

Range 0 – 75% Range 0 – 50%
Untreated control groups of 30 RCTs
17.5% 7.3%
1 year OS 2 year OS

CROHN DISEASE
• Ampia variabilità clinica
• Terapie multiple
• End points surrogati di difficile valutazione
LG: Utilizzo

- Prognostic stratification
- Sample size
- Intrepretation of results

RECTAL CANCER

JAMA 2000
14 RCTs
22 yrs

2009

Standard of care
New Standard
There is an urgent need for better RCTs in gastroenterology
RCTs: indipendenti (Conflitto di interessi)gruppi collaborativi
MAMIPD

194 RCTs
MIPD
Non tutto ciò che può essere misurato conta, e non tutto ciò che conta può essere misurato. . Albert Einstein