La gestione ospedaliera: stratificazione del rischio e ... · SC Pneumologia e UTIR AO C.Poma,...
100
Workshop. Respiro è Vita: il 2009 anno per la Salute del Respiro La BPCO: gestione clinica e organizzativa. Dagli aspetti concettuali alla vita 26 Settembre 2009 Università di Milano La gestione ospedaliera: stratificazione del rischio e costi dell'ospedalizzazione Carlo Sturani SC Pneumologia e UTIR AO C.Poma, Mantova
Transcript of La gestione ospedaliera: stratificazione del rischio e ... · SC Pneumologia e UTIR AO C.Poma,...
Workshop. Respiro è Vita: il 2009 anno per la Salute del RespiroLa BPCO: gestione clinica e organizzativa.
Dagli aspetti concettuali alla vita
26 Settembre 2009 Università di Milano
La gestione ospedaliera:
stratificazione del rischio
e costi dell'ospedalizzazione
Carlo Sturani
SC Pneumologia e UTIR AO C.Poma, Mantova


Stratificazione del rischio e costi dell’ospedalizzazione
• La stratificazione del rischio è uno dei punti chiave della gestione delle malattie cronicheprogressive, invalidanti e potenzialmente mortali nelle fasi di riacutizzazioni
• La stratificazione del rischio dal punto di vista concettuale, epidemiologico, del risk management e dell’equità distributiva è un processo complesso e ricco di conseguenze

Stratificazione del rischio e costi dell’ospedalizzazione
La stratificazione del rischio
• è uno dei punti chiave per la gestione appropriata gestione appropriata dell’ospedalizzazione
• ed influenza i costi
Stratificazione del rischio e costi dell’ospedalizzazione
La stratificazione del rischio
• Nella fase cronica stabile
• Nella fase cronica avanzata• Nella fase cronica avanzata
• Nella fase cronica d’insufficienza d’organo
• Nelle fasi di riacutizzazione
The COPD screw ERS 2009
INCREASED-EXACERBATIONS-H. ADMISSIONS-MORTALITY-PREVALENCE
INSUFFICIENTDIAGNOSISTREATMENT
-PREVALENCE
HUGENUMBER WITH ADVANCED STAGE/CHRONIC RESPIRATORY FAILURE
TREATMENT

Epidemiologia delle malattie
respiratorie croniche,
mortalità e costimortalità e costi
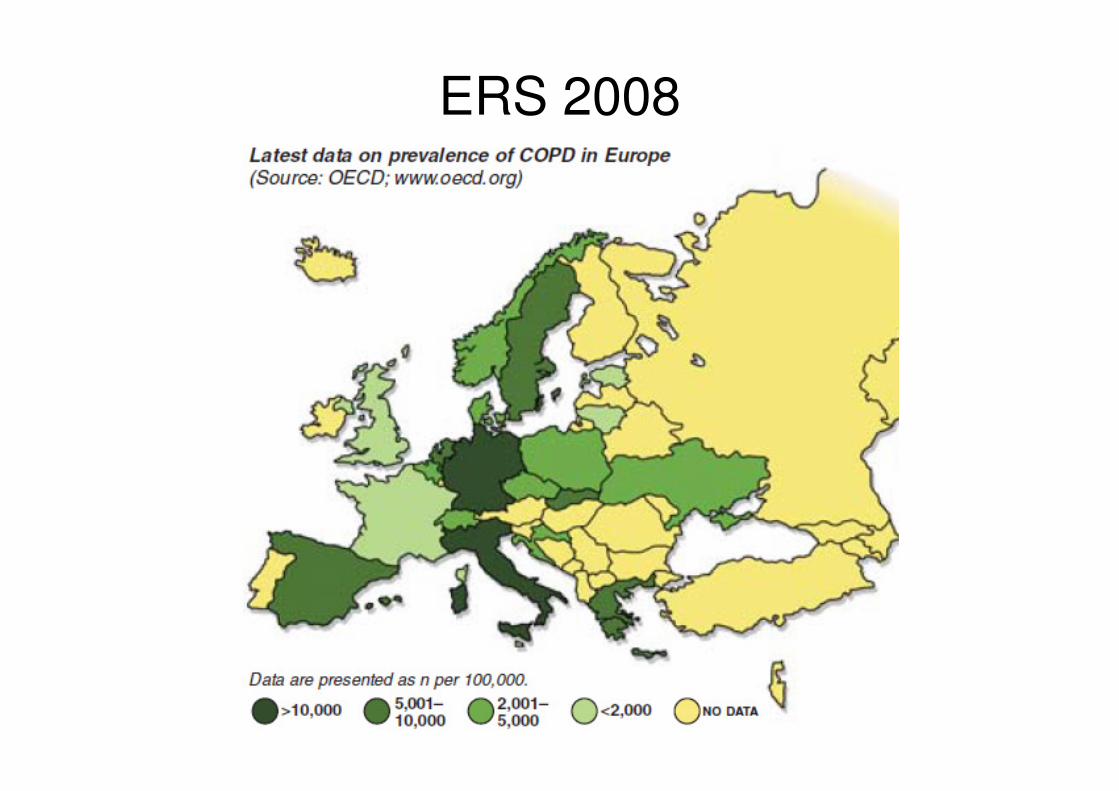
ERS 2008

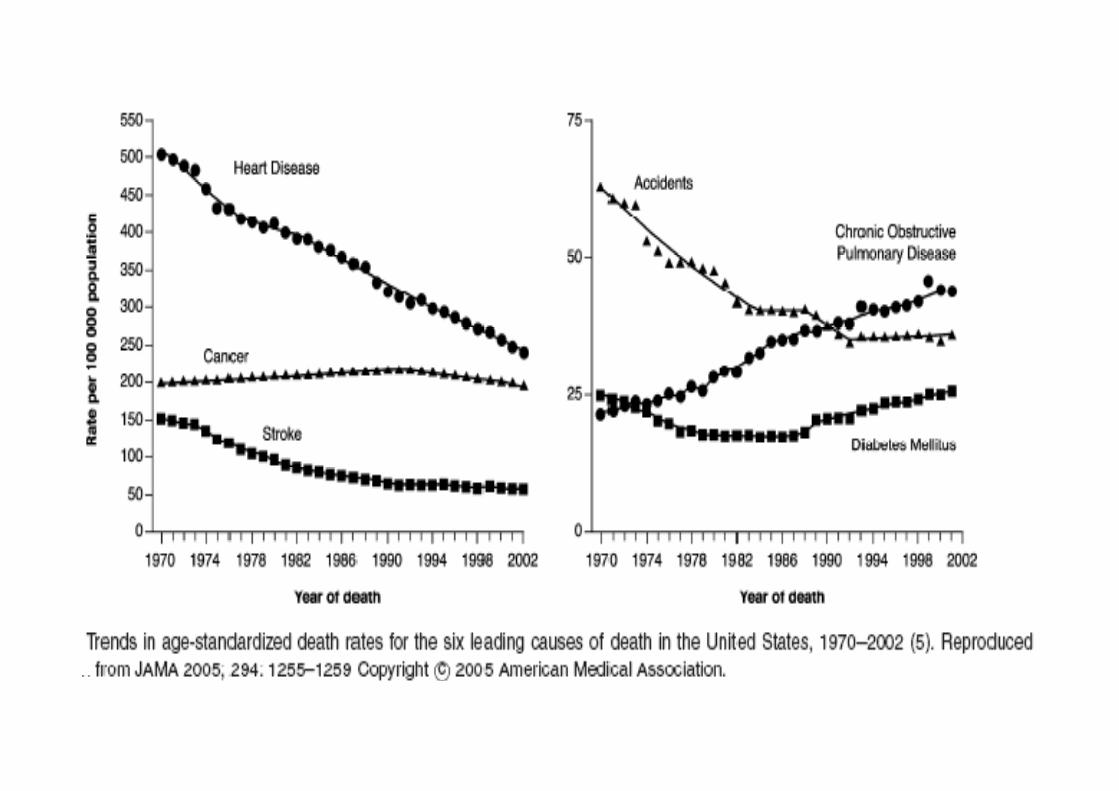
MMWR Sept 2004; 53CDC indicators for chronic disease
surveillance
1. Le previsioni più ottimistiche indicano che la
mortalità per BPCO aumenterà ulteriormente,
Healthy people 2010 objectives:
Reduce deaths from COPD among adults
mortalità per BPCO aumenterà ulteriormente,
del 50% nei prossimi 15 anni

J COPD 2008;5:187-200
J c
op

COPD CORONARY ARTERY
DISEASE
Unstable COPD: Unstable angina:
� Worsening of dyspnoea cough or sputum
� Worsening of chest pain
� RR < 24 � No ECG changes
� Dyspnoea < 4 on 0-10 scale � Normal laboratory results
Celli and Barnes, ERJ 2007
Exacerbation: Myocardial infarction:
� Worsening of dyspnoea cough orsputum
� Chest pain
� Dyspnoea ≥ 4 on 0-10 scale � Abnormal ECG- Abnormal serum enzyme
Ventilatory insufficiency: Cardiogenic shock :
� Same plus elevation of PaCO2 in
arterial blood gases
� Same syndrome plus shock

Mortality comparisons across diseases
COPD Myocardial Infarction
69
Moderate
Severe
3
50
35
0 20 40 60 80
No Shock
Shock
Moderate
%
Swedish Registry 2008, GUSTO-1 Trial 2007
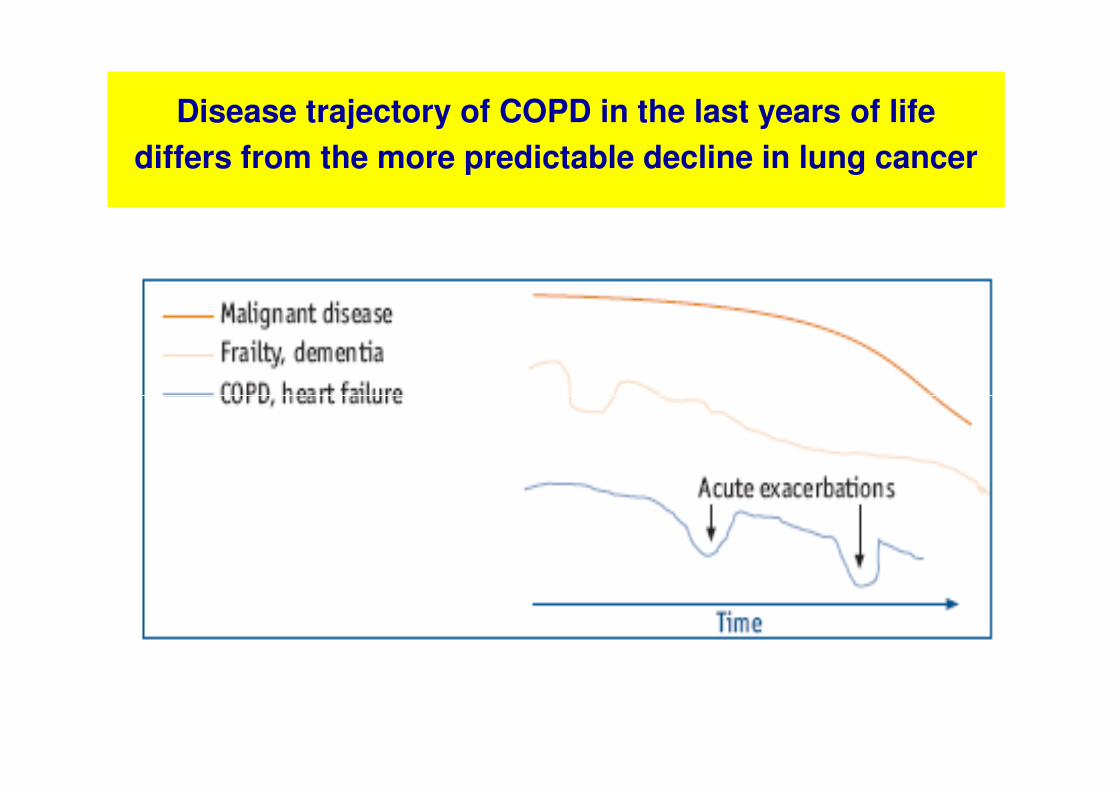
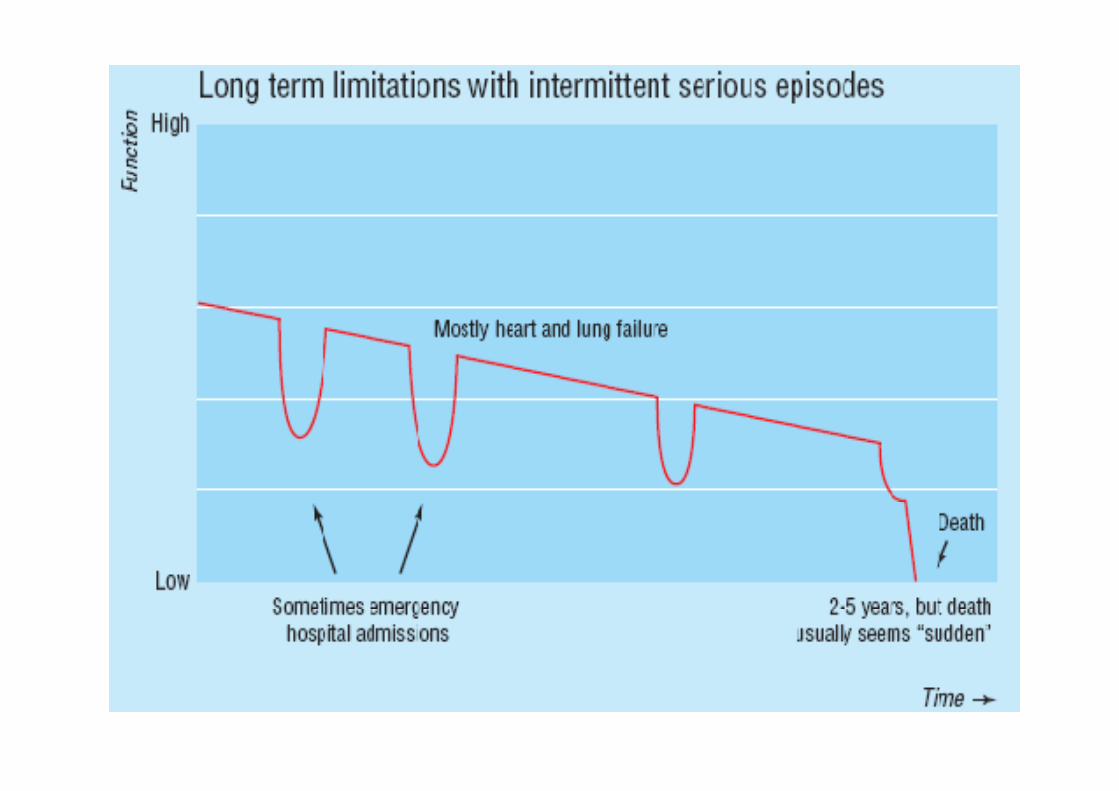
Disease trajectory of COPD in the last years of life
differs from the more predictable decline in lung cancer

Differences in Health Care Utilization at the End of Life Among Patients With COPD and Patients With Lung Cancer.
Arch Intern Med. 2006;166:326-331
Patients with COPD
• were more likely to have been hospitalized (39.8% for COPD vs 18.5% for lung cancer)
• had 5 times the odds of spending more than 2 weeks in an ICU
• and had twice the odds of being readmitted to the ICU
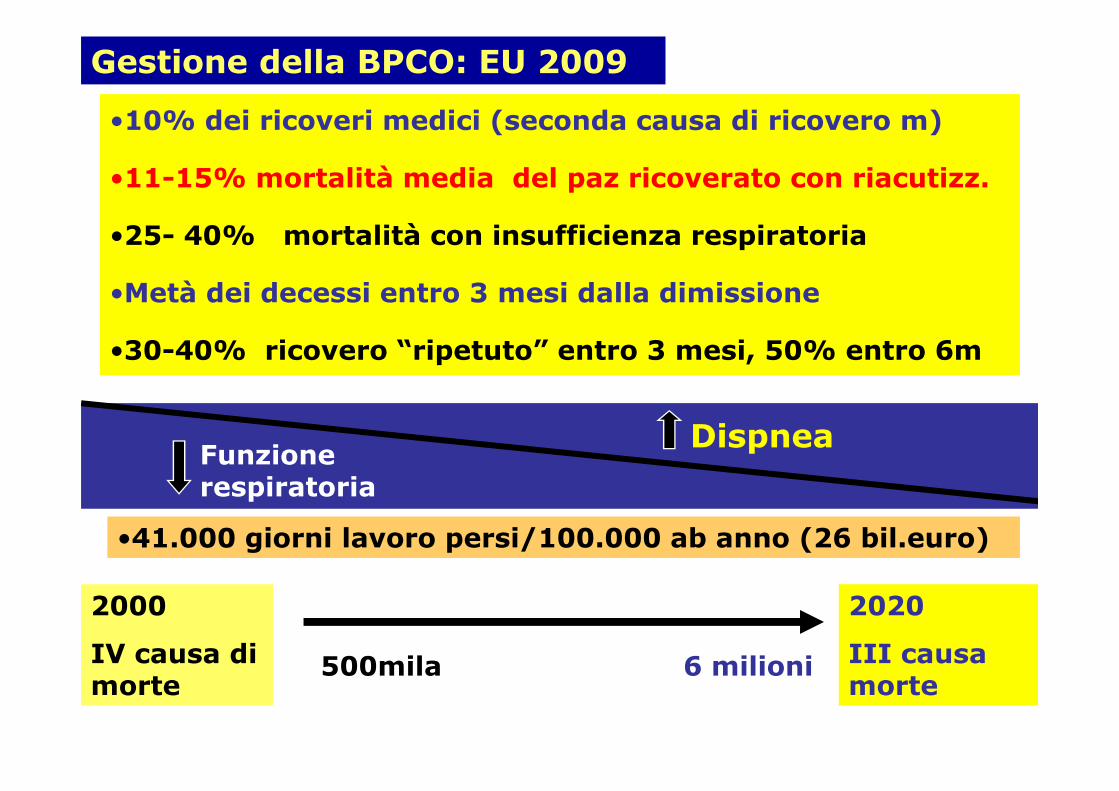
Gestione della BPCO: EU 2009
•10% dei ricoveri medici (seconda causa di ricovero m)
•11-15% mortalità media del paz ricoverato con riacutizz.
•25- 40% mortalità con insufficienza respiratoria
•Metà dei decessi entro 3 mesi dalla dimissione
•30-40% ricovero “ripetuto” entro 3 mesi, 50% entro 6m
DispneaFunzione respiratoria
•41.000 giorni lavoro persi/100.000 ab anno (26 bil.euro)
2000
IV causa di morte
2020
III causa morte
500mila 6 milioni
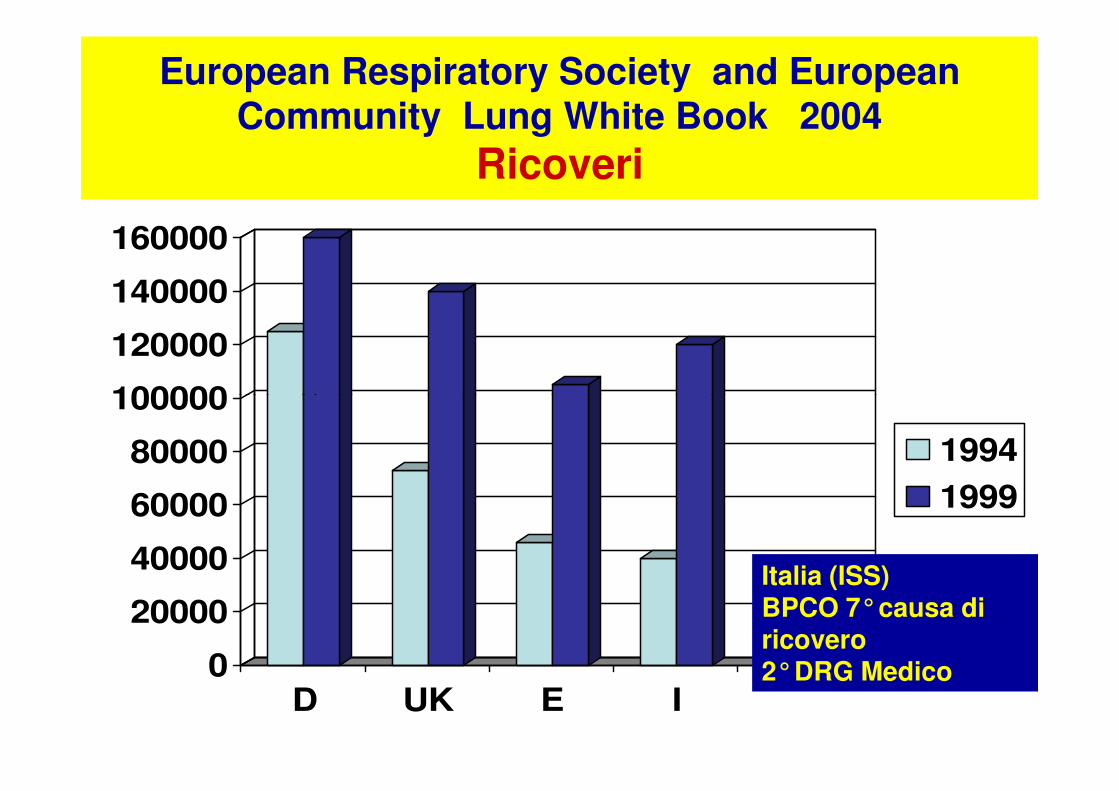
European Respiratory Society and European Community Lung White Book 2004
Ricoveri
100000
120000
140000
160000
0
20000
40000
60000
80000
100000
D UK E I
1994
1999
Italia (ISS)BPCO 7°causa di ricovero 2°DRG Medico
Johnston AK, Mannino DM. Epidemiology of COPD exacerbations.In: Wedzicha JA, Martinez F, editors. Exacerbations Of Chronic
Obstructive Pulmonary Disease (COPD). New York: InformaHealthcare; 2008.
• In-hospital mortality varies between less than 10% and 60%,between less than 10% and 60%,
• based on the severity level of the population studied.
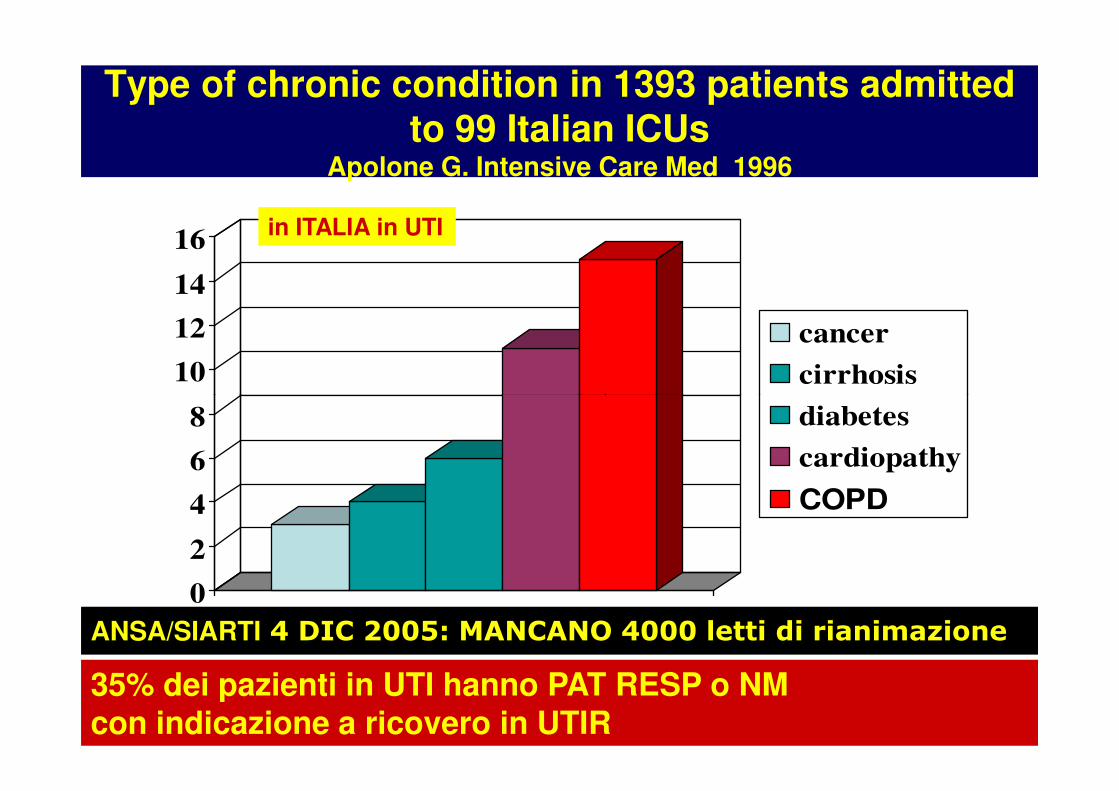
Type of chronic condition in 1393 patients admitted to 99 Italian ICUs
Apolone G. Intensive Care Med 1996
10
12
14
16
cancer
cirrhosis
in ITALIA in UTI
0
2
4
6
8 diabetes
cardiopathy
COPD
ANSA/SIARTI 4 DIC 2005: MANCANO 4000 letti di rianimazione
35% dei pazienti in UTI hanno PAT RESP o NM con indicazione a ricovero in UTIR

Health Policy 2005: 289-301
Nazione % letti UTI %rifiuto ricovero UTI
% occupazione letti UTI
USA 15% 3% <75%
Svezia 9%
Olanda 7%Olanda 7%
Francia 6% 25%
Germania 5%
Inghilterra 4% 31%
Spagna 4%
Grecia 3%
Italia 1.7% >60% >120%
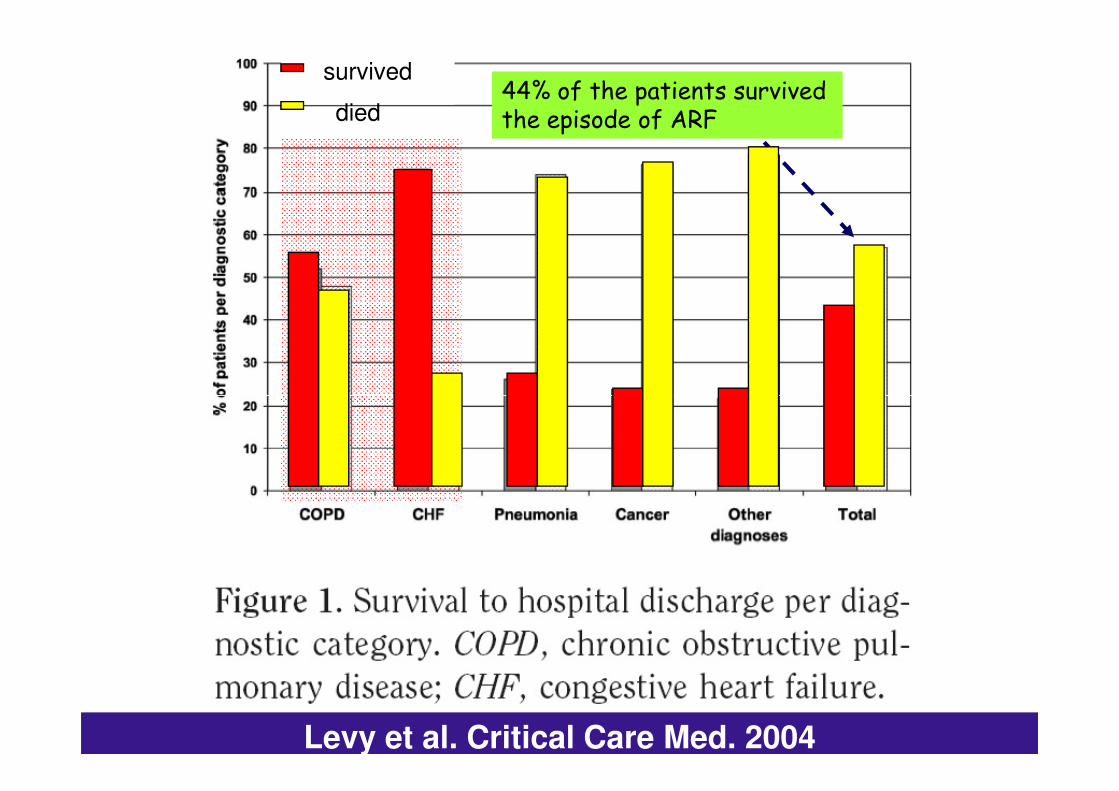
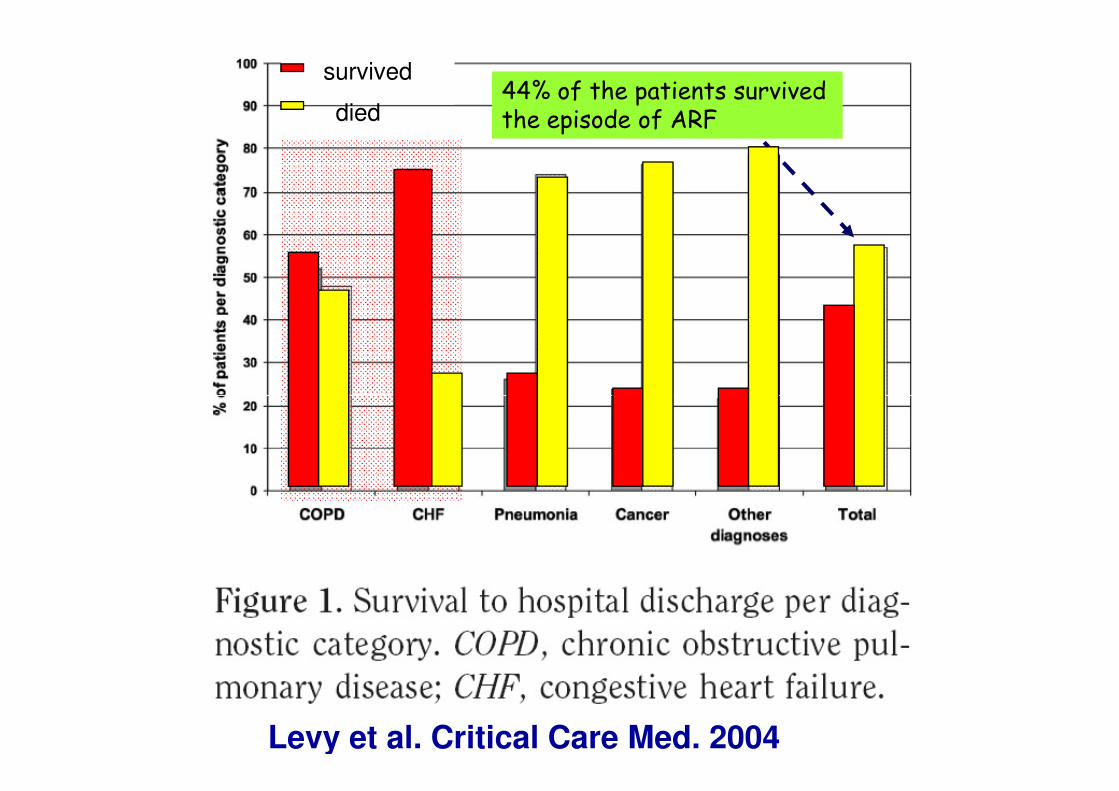
44% of the patients survived the episode of ARF
survived
died
Levy et al. Critical Care Med. 2004
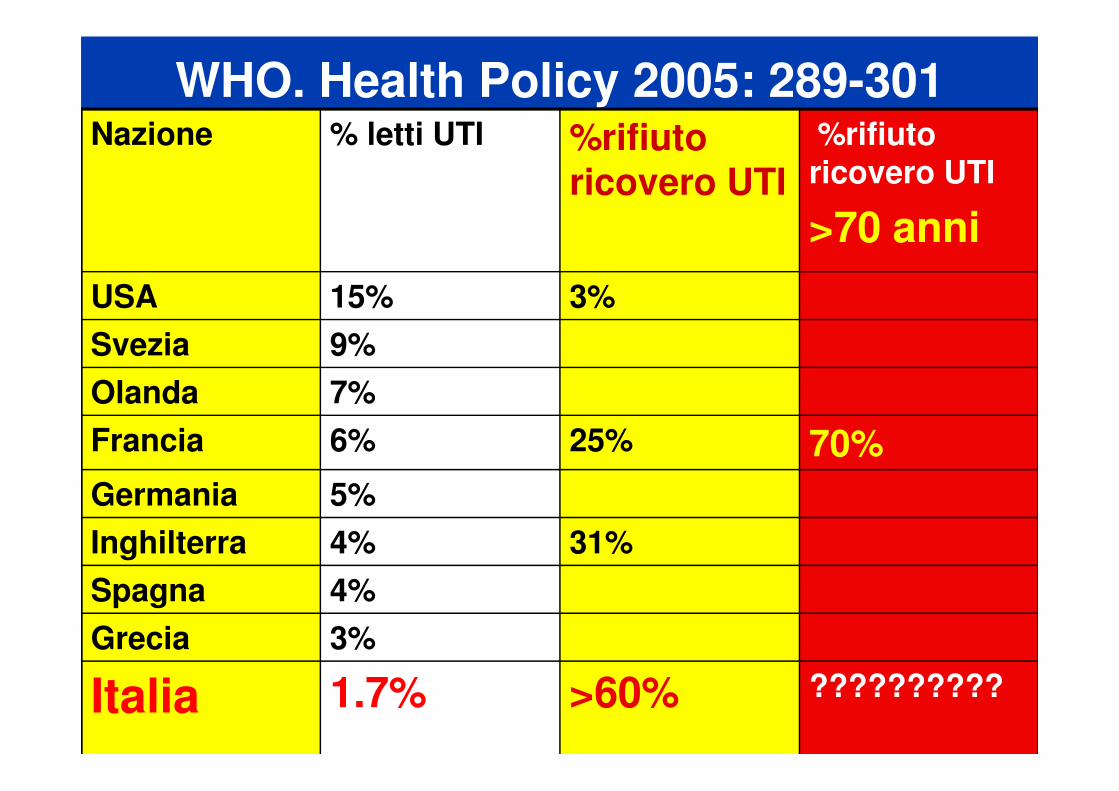
WHO. Health Policy 2005: 289-301Nazione % letti UTI %rifiuto
ricovero UTI
%rifiuto ricovero UTI
>70 anni
USA 15% 3%
Svezia 9%
Olanda 7%Olanda 7%
Francia 6% 25% 70%
Germania 5%
Inghilterra 4% 31%
Spagna 4%
Grecia 3%
Italia 1.7% >60% ??????????

��1616 %% ofof hospitalhospital admissionsadmissions inin EUEU
��2525--6565%% needneed HospitalizationHospitalization
THE COSTS OF COPD EXACERBATIONSTHE COSTS OF COPD EXACERBATIONS
Wedzicha and Seemungal, Lancet 2007
“COPD exacerbations are now
the most common cause of medical
hospital admission in the EU”

Epidemiology and costs of COPD.Chapman K.R., Mannino D.M., Soriano J.B. et al. ERJ. 2006; 27: 188–207.
• Some studies have shown that
the cost of hospital stay represents
40–63% of the total direct costs,40–63% of the total direct costs,
• reaching up to 63% in severe
patients

Economic consequences
Observational studies performed in
primary care Centres observed that
16-22% of patients having16-22% of patients having
exacerbations were admitted
during 1 yr
Pena VS, Miravitlles M, et al. Geographicvariations in prevalence
and underdiagnosis of COPD:results of the IBERPOC multicentre
Epidemiological study. Chest 2000; 118: 981–989.
Exacerbations of COPD. B.R. Celli and P.J. BarnesEur Respir J 2007; 29: 1224–1238
Economic consequences
Failure implies a cost that is three times
higher than the cost of management of the higher than the cost of management of the
exacerbation,
Particularly due to the high cost of
hospitalisation.

Miravitlles M et al. Characteristics of a population of COPD patients identified from a population-based study. Respir Med 2005; 99: 985–995
Economic consequences
This is particularly important considering that a
recent study demonstrated that
• patients with st IV COPD (FEV1 ,35% p) had
a significantly greater percentage of failures
than successful exacerbations,
• with 52% of failures requiring hospitalisation.
Exacerbations of COPD. B.R. Celli and P.J. BarnesEur Respir J 2007; 29: 1224–1238
Economic consequences
However, these costs may not be applicable to
other Countries because of the differences in other Countries because of the differences in
• reference prices,
• management practices
• and healthcare systems.
The burden of COPD in Italy:resultsfrom the Confronting COPD survey.
Dal Negro R, Rossi A, Cerveri I. Respir Med, 2003. 97:s43–50.
A nation-wide survey in 2003 the cost was
confirmed to vary as a function of clinical
severity of COPD, severity of COPD,
• reaching 7000/patient/year in the most
severe cases.
• Mean cost/patient/year 2100
• Hospital admission has been found to
account for 75% of the total cost

Costs of chronic obstructive pulmonary disease (COPD) in Italy: The SIRIO study (Social Impact of Respiratory Integrated Outcomes). Respir Med, 2008. 102:92–101.
• As assessed in the US and in Italy, mean annual cost of COPD has progressively increased over the progressively increased over the last few years,
• increasing by 35% (2003����2008) to reach an average of 2720/patient


The impact of aging and smoking on the future burden of copd: a model analysis in the Netherlands.
Am J Respir Crit Care Med 2001; 164: 590–596.
Economic consequences
• The costs of managing acute • The costs of managing acute exacerbations of COPD are high,
• particularly because of the high costs associated with relapse

Discharge planning and home care for endstage COPD.
J. Escarrabill Eur Respir J 2009; 34: 507–512
• the Risk Factors of COPD Exacerbation
Study (EFRAM) found that 63% of
patients were readmitted during the
year following an exacerbationyear following an exacerbation
• For this reason, discharge support for the
most seriously ill patients is a key issue in
minimising the impact of the current acute
episode and preventing future relapses.
The impact of aging and smoking on the future burden of copd: a model analysis in the Netherlands.
Am J Respir Crit Care Med 2001; 164: 590–596.
Economic consequences
Strategies to improve the outcome of ambulatory
treatment of exacerbations should be very cost-
effective, especially in more severe patients who
are at increased risk of being admitted to hospital
as a consequence of therapeutic failure.

Resource use and risk factors in high-cost exacerbations of COPD.
Oostenbrink JB. Respir Med 2004. 98:883–91.
•A small proportion of COPD (10-20%),
experiencing acute exacerbations, experiencing acute exacerbations,
accounts for over 70 percent of costs
as a result of COPD due to
emergency visits and hospitalizations.
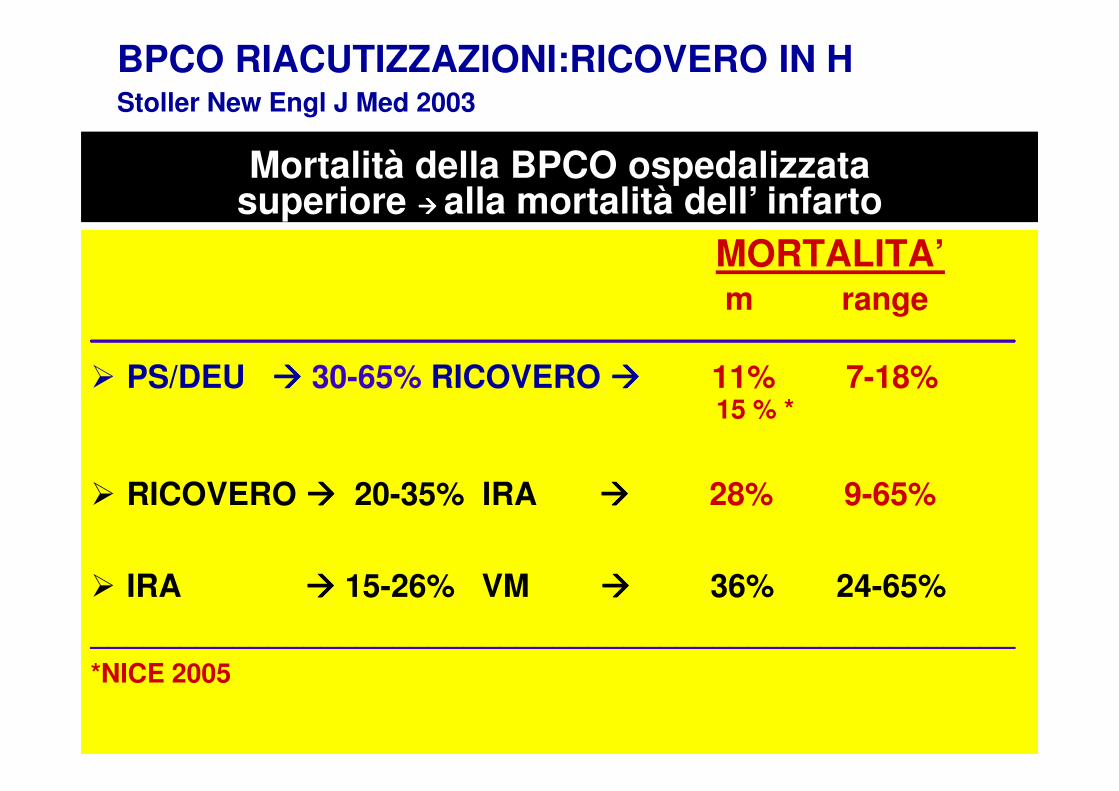
BPCO RIACUTIZZAZIONI:RICOVERO IN HStoller New Engl J Med 2003
MORTALITA’m range
____________________________________________________
� PS/DEU ���� 30-65% RICOVERO ���� 11% 7-18%15 % *
Mortalità della BPCO ospedalizzata superiore ���� alla mortalità dell’ infarto
15 % *
� RICOVERO ���� 20-35% IRA ���� 28% 9-65%
� IRA ���� 15-26% VM ���� 36% 24-65%
____________________________________________________
*NICE 2005

Stratificazione del rischio e costi dell’ospedalizzazione
La stratificazione del rischio
• A domicilio
• Nei DEU
• In degenza generale e specialistica
• In Terapia semi intensiva Respiratoria
• ed intensiva generale



Variables including
• using long term oxygen therapy,
• having low health status
• or poor health related quality of life
• and not having routine physical activity
were all associated with an increased risk
of admission and readmission to hospital.

• PaCO2 was shown to be• PaCO2 was shown to be
• an independent risk factor for hospital
admission for an acute exacerbation of
COPD
In this review, 3 predictive factors:
• “previous hospital admission”, • “previous hospital admission”,
• “dyspnea”
• “oral corticosteroids”
were all found to be significant risk factors of readmissions.
• Comorbidity does not appear to be a risk factor
for frequent exacerbations,
• but a risk factor for severe life threatening • but a risk factor for severe life threatening
exacerbations that can provoke admission.
• special attention should be paid to the diagnosis of
coexisting disease and its association with COPD
admission.
• Older age was associated with shorter time to
first readmission and increased risk of
hospitalization in several studies
(Lau et al 2001; Soler-Cataluna et al 2005; Gadoury
et al 2005).
• This may be related to the higher degree of
disability and comorbidity in the older population.


• it has been demonstrated that prompt treatment by a physician
• is associated with better outcomes
Use and utility of an early presentation and intervention in COPD.Hurst JR. ERS Wien 15 sept 09
• Unit of Respiratory Medicine
• Established telephone service (24h, 7/7d) for patients and
carers with COPD to facilitate early treatment
• Recruitment of patients with high risk of HA
(previous AECOPD and or severe disease)
• Medications optimized,pts were given an emergency course of
AB and steroids to have at home
• 24H access to health care professionals
who knew them and who they knew….
Use and utility of an early presentation and intervention in COPD (EPIC).Hurst JR. ERS Wien 15 sept 09
• 45 patients with complete 6 mos fup
• 14 died• 14 died
Use and utility of an early presentation and intervention in COPD (EPIC).Hurst JR. ERS Wien 15 sept 09
• 80% patients made unplanned calls to the service
• Average rate call per patient 1 every 53 patient days
(13-183)(13-183)
• Average call duration 9 mins
• 3% overnight
• 36% of calls concerned symptoms deterioration
• Satisfaction 4.8/5 (1 peggio-5molto meglio)

Use and utility of an early presentation and intervention in COPD (EPIC).Hurst JR. ERS Wien 15 sept 09
• Most patients are willing to use a 24/7 COPD advice lineadvice line
• These data will be of use in determining the cost effectiveness of such services

ACIDOSI E OSPEDALIZZAZIONE
• DEVONO ESSERE RICOVERATI SOLO I PAZIENTI IPERCAPNICI E/O CON ACIDOSI?
• PERCHE’ più di >20 linee guida • PERCHE’ più di >20 linee guida internazionali indicano ulteriori criteri (da 7 a 18 criteri) di per se sufficienti a considerare necessaria l’ospedalizzazione?
Acidosis in COPD exacerbations admitted to hospitals – the UK national COPD audit 2008. Roberts C. Clinical Effectiveness Unit.
Royal College of Physicians, London. ERS Wien 15 sept 09, 605s
Few data of the true prevalence of acidosis in HA
232 Hospitals, data in 9716 COPD m73 yrs
• 87% ABG on HA• 87% ABG on HA
• 20% acidotic (pH<7.35)
• 7% very severe acidosis (pH<7.26)
Acidosis in COPD exacerbations admitted to hospitals – the UK national COPD audit 2008. Roberts C. Clinical
Effectiveness Unit. Royal College of Physicians, London. ERS Wien 15 sept 09, 605s
• 30% in ambulance and DEA FIO2 > 35
(recorded only 50%)
• 7% non acidotic became later acidotic• 7% non acidotic became later acidotic
• 26% cumulative acidotic
• 12 hours post HA lowest pH
(64% receiving FIO2>28)!
NIV mortality in clinical practice – the UK national COPD audit 2008.Roberts C. Clinical Effectiveness Unit. Royal College of Physicians, London. ERS Wien 15 sept 09, 604s
• 1077/9716 patients received NIV
• 102 patients with pH>7.35
• 25 % in H mortality• 33% 90 days mortality
• The high mortality observed in 2004 was repeated in 2008

NIV mortality in clinical practice – the UK national COPD audit 2008. Roberts C. Clinical
Effectiveness Unit. Royal College of Physicians, London.
ERS Wien 15 sept 09, 604s
HA AECOPD treated with NIV
% Mortality during admission/90d
ABG pH <7.26 7.26-7.34 >7.34ABG pH <7.26 7.26-7.34 >7.34
Lowest pH on HA 27/35 17/26 32/37
Lowest pH post HA 49/52 32/35 8/14
Acidosis in COPD exacerbations admitted to hospitals – the UK national COPD audit 2008. Roberts C. Clinical
Effectiveness Unit. Royal College of Physicians, London. ERS Wien 15 sept 09, 605s
• Outcome are worse for those ventilated with the lowest pH later in the admission.
• There are a number of COPD pts with a normal pH admission who receive NIV who have a high mortality.
• This group needs further investigation.
When AECOPD leads to an acidotic state,
patients often require admission to the patients often require admission to the
intensive care unit for assisted ventilation,
with a poor prognosis in survivors
after discharge.
mortality was independently related to
• age,
• hypercapnia, • hypercapnia,
• and frequency of severe exacerbations,
• particularly if these require admission to hospital.
Nonacidotic AECOPD
also accounts for
considerable hospitalization
A study of patients hospitalized for nonacidotic AECOPD found that independent predictors of
mortality were
• Quality of life, • Quality of life,
• marital status,
• depressive symptoms,
• prior hospital admission,
• and comorbidity,

• 10% died
Predictors of 6-Month Mortality in Elderly Patients with
Mild Chronic Obstructive Pulmonary DiseaseDischarged After Acute Nonacidotic Exacerbation
• 15 transferred to the intensive care
unit
Tasso di ospedalizzazione?
A clinical audit of COPD hospitalizations in 3 Scandinavian Hospitals.Liaaen ED. ERS Wien 15 sept 2009, 601s
• AE COPD requiring HA represent and independent predictor fo poor patient prognosis
• Scandinavia 26(28-24) COPD HA /10000inh
• Spain 25(30-16) COPD HA /10000inh in 7 health regions from 30 to 16

A clinical audit of COPD hospitalizations in 3 Scandinavian Hospitals.
Liaaen ED. ERS Wien 15 sept 2009, 601s
• COPD HA /10000inh 26(28-24)
• Mean LOS d 7.7 – 9.2
• Current smokers % 35 – 26
• Patients on LTOT % 15 – 21
• Received NIV % 22 – 8
• Received AB % 59 – 71
A clinical audit of COPD hospitalizations in 3 Scandinavian Hospitals.
Liaaen ED. ERS Wien 15 sept 2009, 601s
• Significant differences with respect to treatments with NIV and AB were observed between centres and countriesobserved between centres and countries
• Some of these findings may reflect different organization of health care
AUDIPOC. National clinical audit on COPD exacerbations in Spain. Mortality and readmissions. Influence of hospitalization department.
Hernandez C. ERS Wien 15 sept 2009, 601s
• 1203 COPD, 30 public hospitals in Spain
• 43% clinical relevant comorbidity (CI 2.7)
• 55% admitted to the Pneumology dept
• 39% admitted to Internal Med dept

National clinical audit on COPD exacerbations in Spain. Mortality and readmissions.Influence of hospitalization department.
AUDIPOC. Hernandez C. ERS Wien 09, 601s
Department Pneumology Internal med
1203 COPD, 30 public hospitals in Spain, 43% clinical relevant comorbidity (CI 2.7)
% HA 55 39
Mortality in H % 3.5 6.3*
Mortality 90 d % 8.3 11.2
Readmission 90 d % 36 39
AUDIT nei DEA
Complex admission decisions

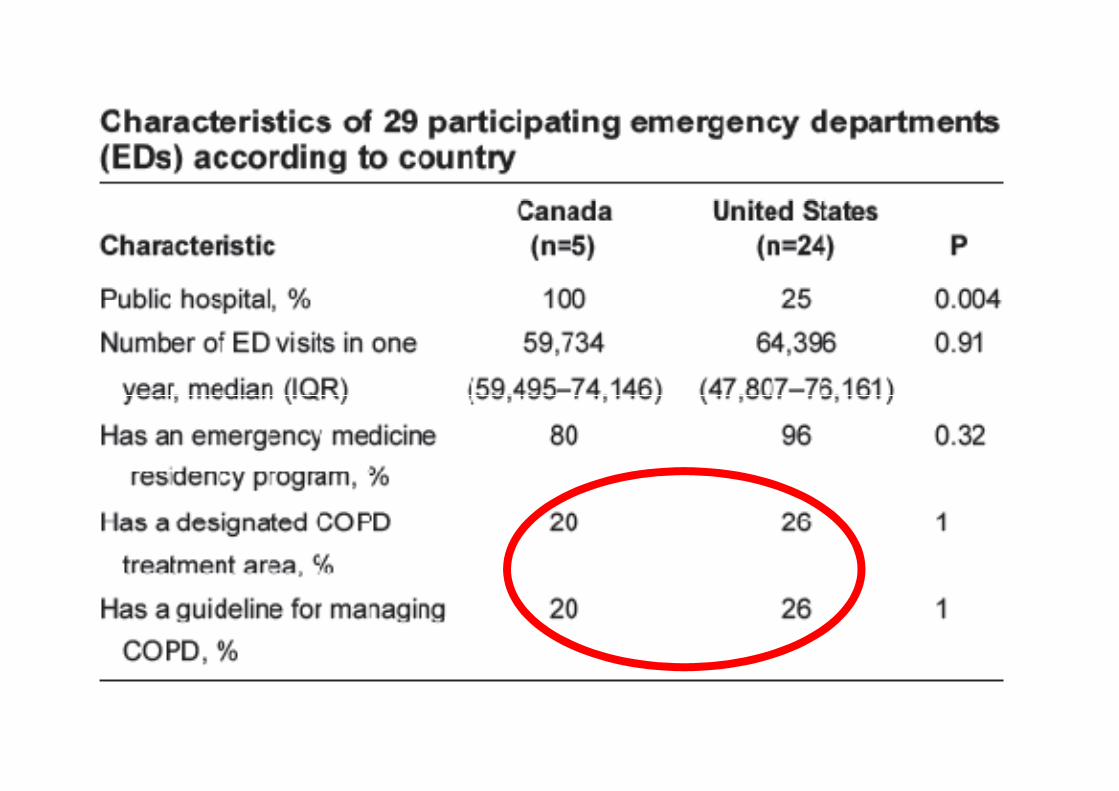
• The authors confirmed five of
the seven testable indications
Factors associated with hospital admission among emergency department patients with COPD exacerbation.
Tsai CL. Acad Emerg Med. 2007 Jan;14(1):6-14.
the seven testable indications
for hospital admission in the
GOLD guidelines.

Regione Lombardia 2007
• Most patients (70%) presented to the
Acute exacerbations of COPD: delay in presentation and the risk of hospitalization.
Chandra D. COPD. 2009 Apr;6(2):95-103
ED > 24 hours after symptom onset,
and most (61%) were hospitalized
• On multivariate logistic regression analysis,
after adjusting for 12 potential confounders
Acute exacerbations of COPD: delay in presentation and the risk of hospitalization.
Chandra D. COPD. 2009 Apr;6(2):95-103
• a delay in presentation > or = 24
hours was associated with a over two-
fold increase in the odds of admission
• Early presentation should be
emphasized to patients and
caregivers to advance efforts
Acute exacerbations of COPD: delay in presentation and the risk of hospitalization.
Chandra D. COPD. 2009 Apr;6(2):95-103
caregivers to advance efforts
to decrease the morbidity,
mortality, and costs of AECOPD
treatment.

• Approximately one third of exacerbations
were recurrent exacerbations.
Temporal clustering of exacerbations in COPD.
Hurst JR, Wedzicha JA. BMC Med. 2009 Aug 7; 7:40.
• Exacerbations are not random events but
cluster together in time such that there is a
high-risk period for recurrent exacerbation in
the 8-week period after an initial excerbation.

Risk factors and outcomes associated with COPD exacerbations requiring hospitalization.
BBahadori K. Jul;16(4):e43-9. Can Respir J. 2009 Jul;16(4):e43-9.
• During the study period, 38% of subjects were readmitted at least once.
• Comparative analysis among the three hospitals identified a significant difference in readmission rates
(54%, 36% and 18%, respectively).
Risk factors and outcomes associated with COPD exacerbations requiring hospitalization.BBahadori K. Can Respir J. 2009. Jul;16(4):e43-9.
Independently associated with frequent readmissions for AE.
�preadmission home oxygen use (P=0.001),
�other chronic respiratory disease P=0.03)
�shorter length of hospital stay (P=0.021)

Exacerbations de BPCO:
Audit de pratique dans les services d’urgences en FranceRev Mal Respir 2006; 23:49-57
La mission première du service d’urgence
serait donc plutot d’èvaluer la gravitè
de ces patients a fin de les orienter vers
• un service de pneumologie,
• des soins intensifs de pneumologie
• or de reanimation

Current and Projected Workforce Requirements for Care of the Critically Ill and Patients with Pulmonary Disease.
Can we meet the Requirements of an Aging population? COMPACCS.
ANNI PNEUM
% G
G/1000 ab PNEUM
2010
UTI/UTIR
2010
<65 32 38<65 32 38
65-75 37 261
>75 31 634
BPCO , IR, Polmonite
85 JAMA 2000 284:2762
+35% +30%
In EU c’è un impellente bisogno di Terapie semi intensive
ad alta intensità e specializzazioneTask force soc europea TI . Intens Care Med 2008
• Riduzione totale del n PL ospedale
• Aumento indicazioni a ventilazione meccanica non
invasiva (VMNI) in particolare per BPCO
• Aumento relativo di pazienti critici RESPIRATORI E
CARDIACI in H
• “Disinvoltura” interventistica (operare tutto a qualsiasi
costo)
• Aumento dei pazienti dipendenti da VM
• Aumento inappropriato delle tracheostomie
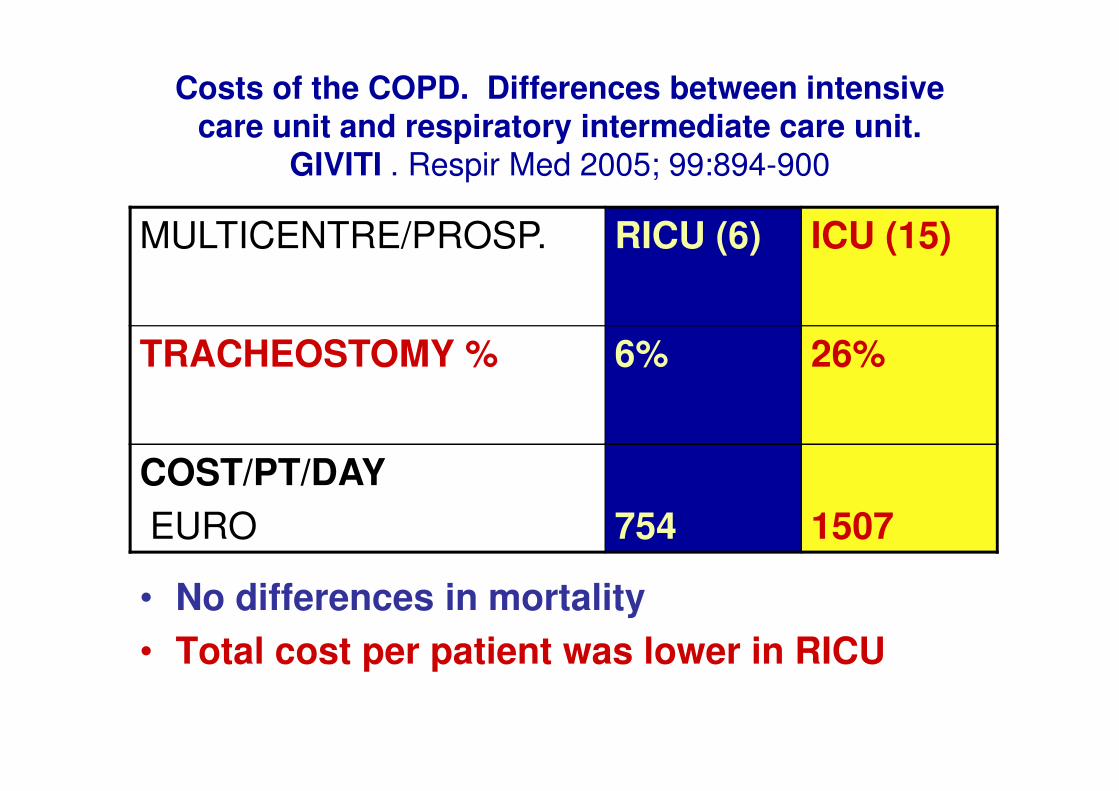
Costs of the COPD. Differences between intensive care unit and respiratory intermediate care unit.
GIVITI . Respir Med 2005; 99:894-900
MULTICENTRE/PROSP. RICU (6) ICU (15)
TRACHEOSTOMY % 6% 26%
• No differences in mortality
• Total cost per patient was lower in RICU
COST/PT/DAY
EURO 754 1507
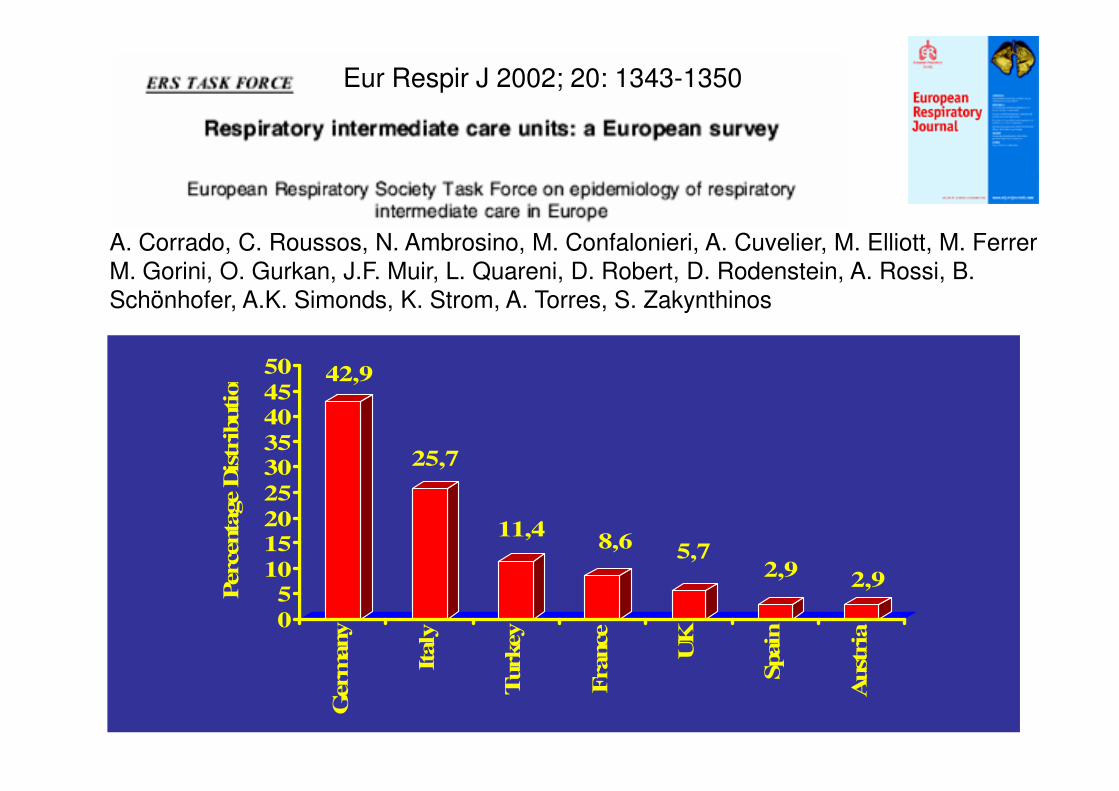
Eur Respir J 2002; 20: 1343-1350
A. Corrado, C. Roussos, N. Ambrosino, M. Confalonieri, A. Cuvelier, M. Elliott, M. Ferrer,
M. Gorini, O. Gurkan, J.F. Muir, L. Quareni, D. Robert, D. Rodenstein, A. Rossi, B.
Schönhofer, A.K. Simonds, K. Strom, A. Torres, S. Zakynthinos
42,945
50
Percenta
ge D
istr
ibution
25,7
11,48,6
5,72,9
2,9
0
510
15
20
25
3035
40
45
Percenta
ge D
istr
ibution
Germ
any
Italy
Turkey
France
UK
Spain
Aust
ria
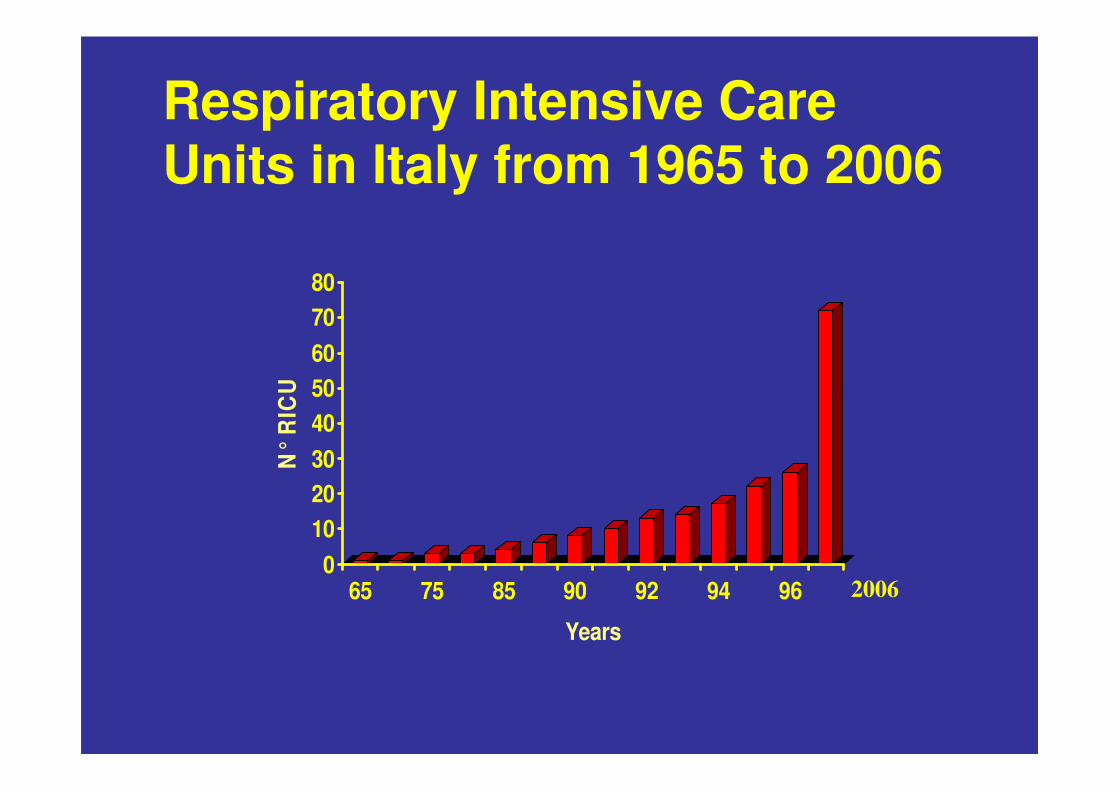
Respiratory Intensive Care Units in Italy from 1965 to 2006
50
60
70
80N
° R
ICU
0
10
20
30
40
50
N°
RIC
U
65 75 85 90 92 94 96
Years
2006

Riconosciute Totali
(n.49) (n.72)
Nord 61,2% 57,0%
Centro 20,4% 20,8%
Sud-isole 18,4% 22,2%3(2)
10(9)
2(2)
3(2)
2(1)
13(10)
2(2)
3(2)
0(0)
6(3)
4(3)
3(2)
3(2)
8(4)
0(0)
Distribuzionegeografica
20062006
5(2)6(3)
1(1)
3(3)
1(0)
0(0)
0(0)
1996 totale 26Nord = 17 (65.4%)Centro = 5 (15,4%)Sud+Isole = 4 (19,2%)

326 centres providing HMV IN EUROPE
> 21,000 patients on HMV
QUESTIONNAIRE FROM SELECTED CENTERS
14
17
2
17
16
Eurovent
IX/2001 – VI/ 2002
44 CENTRI CHE DIMETTONO PAZIENTI ASSISTITI CON VMD
In ITALIA hanno risposto al questionario
4614
5
22
20
9
17
44
7
15
58
15
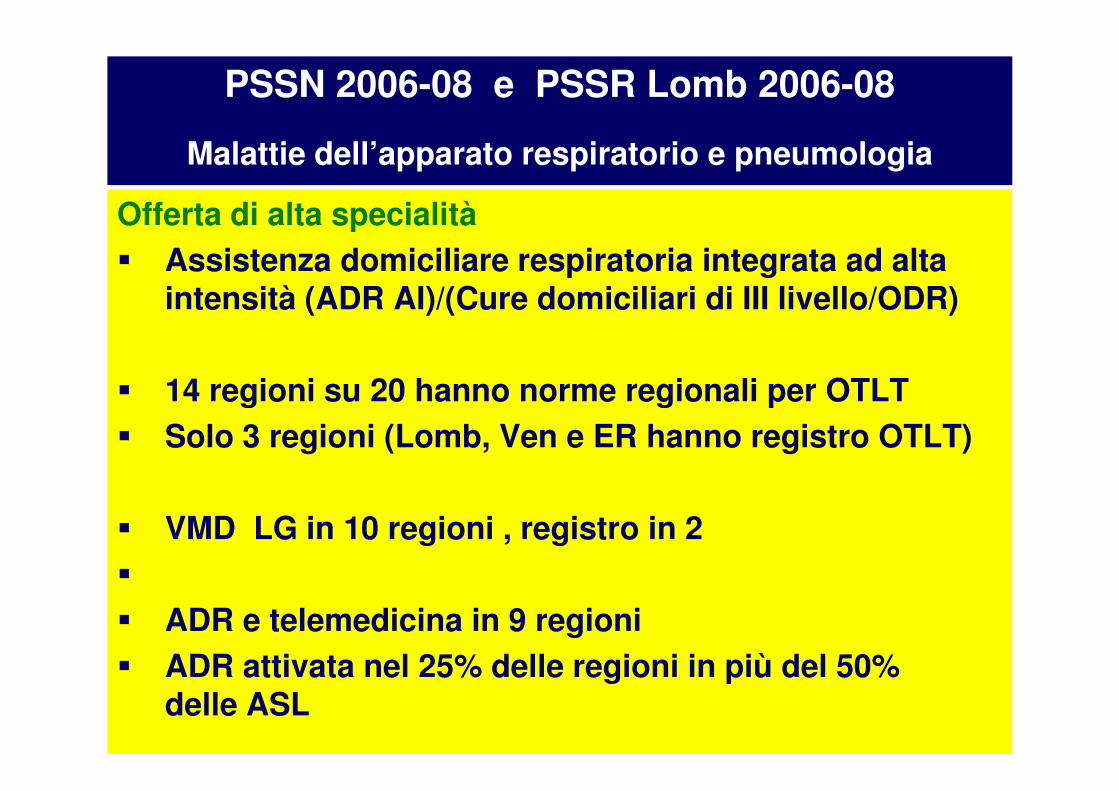
PSSN 2006-08 e PSSR Lomb 2006-08
Malattie dell’apparato respiratorio e pneumologia
Offerta di alta specialità
� Assistenza domiciliare respiratoria integrata ad alta intensità (ADR AI)/(Cure domiciliari di III livello/ODR)
� 14 regioni su 20 hanno norme regionali per OTLT� 14 regioni su 20 hanno norme regionali per OTLT
� Solo 3 regioni (Lomb, Ven e ER hanno registro OTLT)
� VMD LG in 10 regioni , registro in 2
�
� ADR e telemedicina in 9 regioni
� ADR attivata nel 25% delle regioni in più del 50% delle ASL

Commissione Mal Respir. Regione Lombardia 2001-7GAT BPCO e Insufficienza respiratoria 2009
Setting di ospedalizzazione vs gravità della BPCO riacutizzata
•Unità operativa complessa di Medicina generale:
-insufficienza respiratoria assente, -non stadio III –IV
• Unità operativa complessa di Pneumologia :
-stadio II-IV,
-acidosi respiratoria con pHa da 7.35 a 7.30se livello di monitoraggio ed assist. Adeguati (almeno 240min)se livello di monitoraggio ed assist. Adeguati (almeno 240min)
Unità di cura per l’insufficienza respiratoria avanzata(semintensiva): -rischio di acidosi respiratoria,
-acidosi respiratoria pH da 7.35 a 7.20,-comorbilità,
-pazienti già in O2-terapia o in ventilazione meccanica domiciliare,
-necessità di ventilazione meccanica non invasiva
•Unità di terapia intensiva generale:-pH <7.20 e/o MOF
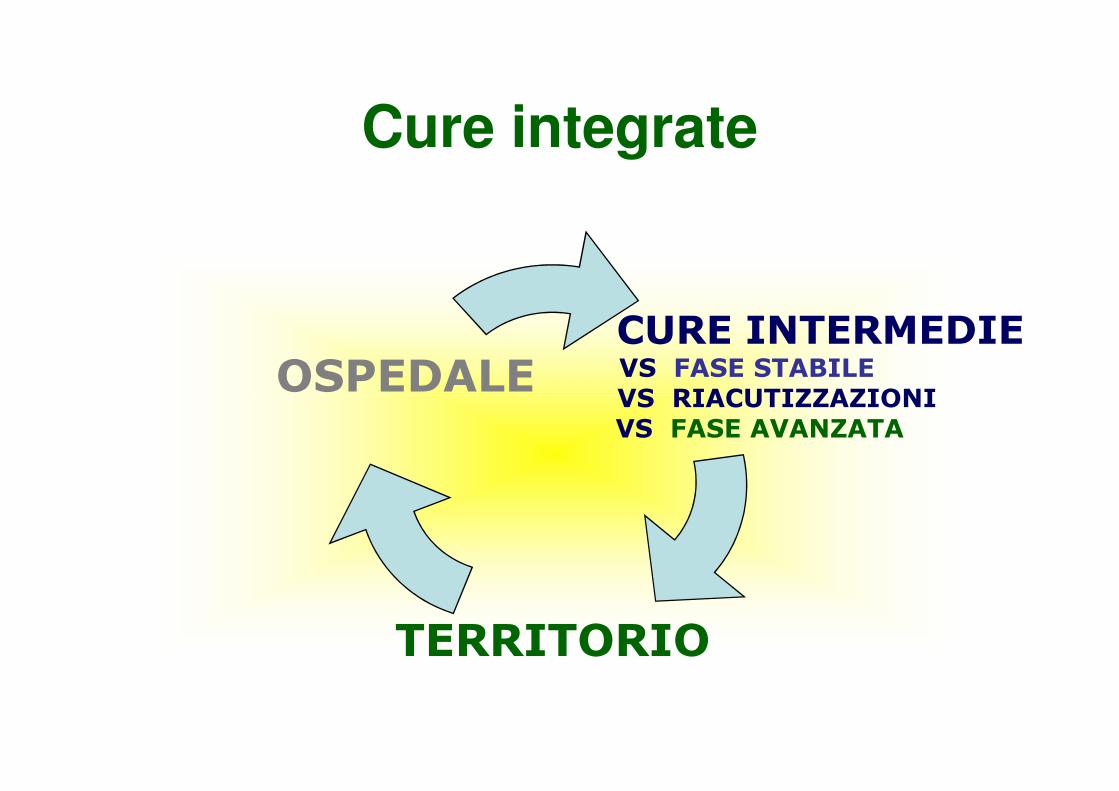
Cure integrate
CURE INTERMEDIEVS FASE STABILEVS RIACUTIZZAZIONI
OSPEDALEVS RIACUTIZZAZIONIVS FASE AVANZATA
TERRITORIO
OSPEDALE
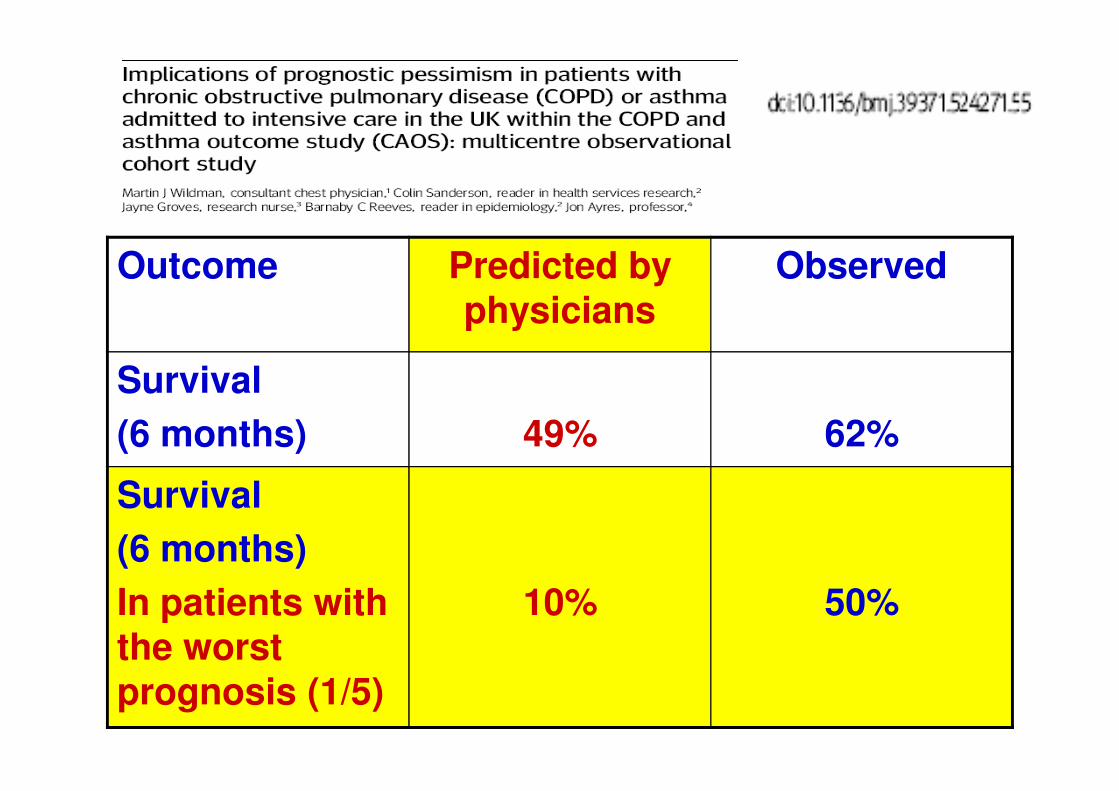
Outcome Predicted by physicians
Observed
Survival Survival
(6 months) 49% 62%
Survival
(6 months)
In patients with the worst prognosis (1/5)
10% 50%
44% of the patients survived the episode of ARF
survived
died
Levy et al. Critical Care Med. 2004

Comunità scientifica
(pneumologica)
27 dicembre 2008
L’insufficienza respiratoria (DRG87)
ESCE DALLA
FASCIA PROTETTA
DEI RICOVERI DA RIMBORSARE ALLE
“aziende “ Ospedaliere
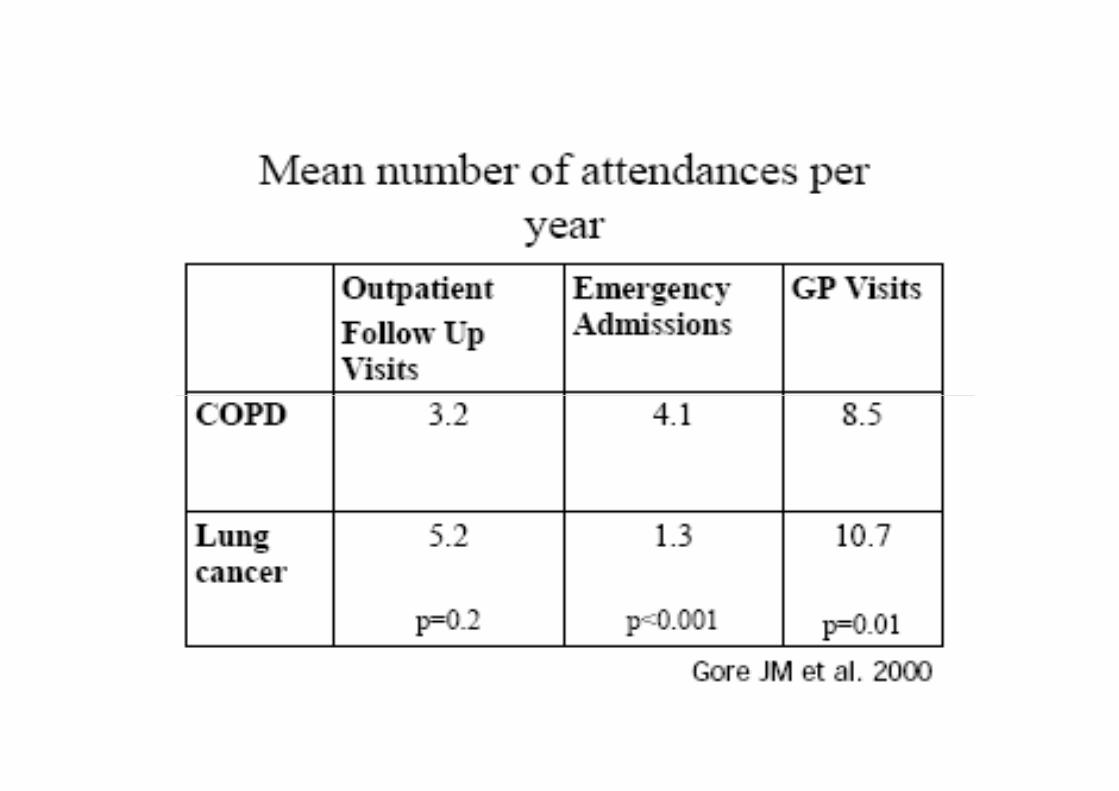
Cronicità. Le cure negate?How well do we care for patients with COPD?
A Comparison of care and quality of life in COPD and
lung cancer.Gore JM.Thorax 2000;55:1000-06
• I malati con tumore polmonare hanno
più assistenza più assistenza
• rispetto ai malati con malattie croniche
respiratorie nonostante gravità dei sintomi
e necessità assistenziali
• siano molto simili













![INDICE - philipwillan.com1].pdf · Tamigi, che interveniva prontamente con una motolancia, il cui equipaggio era composto dagli agenti Michael Stewart, John Johnston e Donald Bartliff.](https://static.fdocumenti.com/doc/165x107/5bfe1a1409d3f2740f8cb2b5/indice-1pdf-tamigi-che-interveniva-prontamente-con-una-motolancia-il-cui.jpg)