
La genetica al servizio della clinica nelle ... · La genetica al servizio della clinica nelle...
46
La geneca al servizio della clinica nelle immunodeficienze primive Dr. Boaz Palterer Diparmento di Medicina Clinica e Sperimentale Scuola di Specializzazione in Allergologia e Immunologia Clinica Università degli Studi di Firenze FIRENZE 11 – 12 Novembre 2016
Transcript of La genetica al servizio della clinica nelle ... · La genetica al servizio della clinica nelle...

La genetica al servizio della clinica nelle immunodeficienze primitive
Dr. Boaz PaltererDipartimento di Medicina Clinica e SperimentaleScuola di Specializzazione in Allergologia e Immunologia ClinicaUniversità degli Studi di Firenze
FIRENZE 11 – 12 Novembre 2016
FIRENZE 11 – 12 Novembre 2016
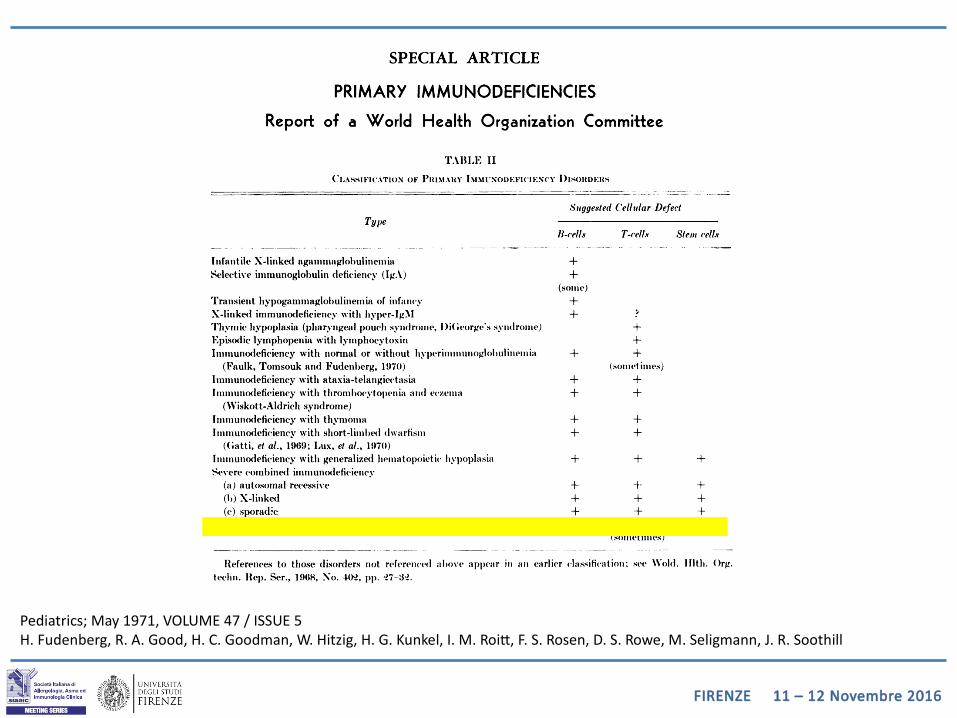
Pediatrics; May 1971, VOLUME 47 / ISSUE 5H. Fudenberg, R. A. Good, H. C. Goodman, W. Hitzig, H. G. Kunkel, I. M. Roitt, F. S. Rosen, D. S. Rowe, M. Seligmann, J. R. Soothill
FIRENZE 11 – 12 Novembre 2016
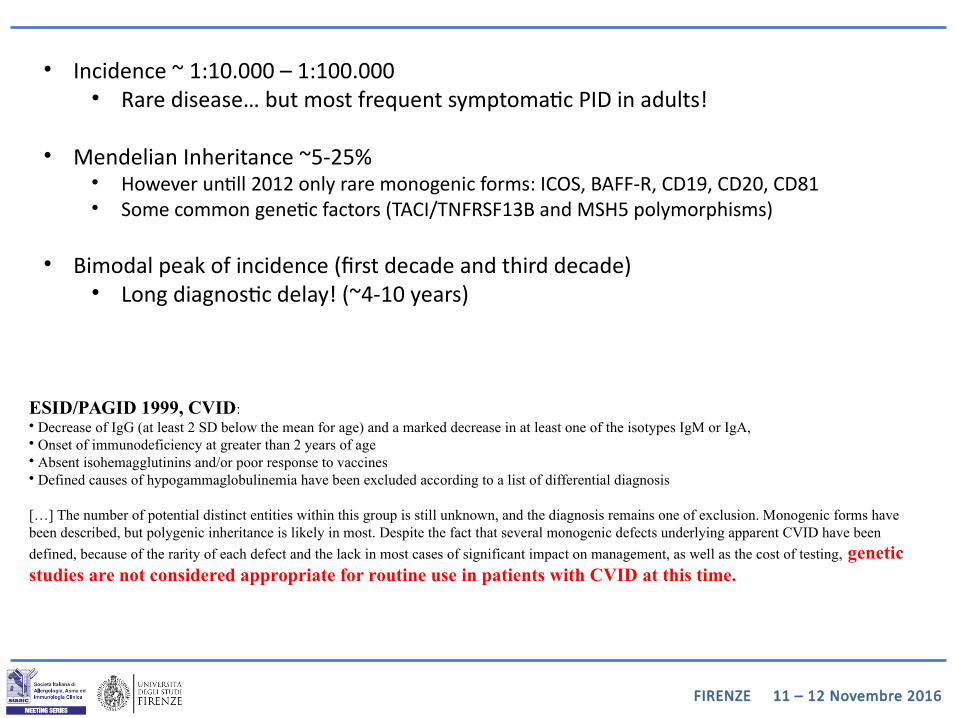
ESID/PAGID 1999, CVID:• Decrease of IgG (at least 2 SD below the mean for age) and a marked decrease in at least one of the isotypes IgM or IgA, • Onset of immunodeficiency at greater than 2 years of age• Absent isohemagglutinins and/or poor response to vaccines• Defined causes of hypogammaglobulinemia have been excluded according to a list of differential diagnosis
[…] The number of potential distinct entities within this group is still unknown, and the diagnosis remains one of exclusion. Monogenic forms have been described, but polygenic inheritance is likely in most. Despite the fact that several monogenic defects underlying apparent CVID have been
defined, because of the rarity of each defect and the lack in most cases of significant impact on management, as well as the cost of testing, genetic studies are not considered appropriate for routine use in patients with CVID at this time.
• Incidence ~ 1:10.000 – 1:100.000• Rare disease… but most frequent symptomatic PID in adults!
• Mendelian Inheritance ~5-25%• However untill 2012 only rare monogenic forms: ICOS, BAFF-R, CD19, CD20, CD81• Some common genetic factors (TACI/TNFRSF13B and MSH5 polymorphisms)
• Bimodal peak of incidence (first decade and third decade)• Long diagnostic delay! (~4-10 years)
FIRENZE 11 – 12 Novembre 2016
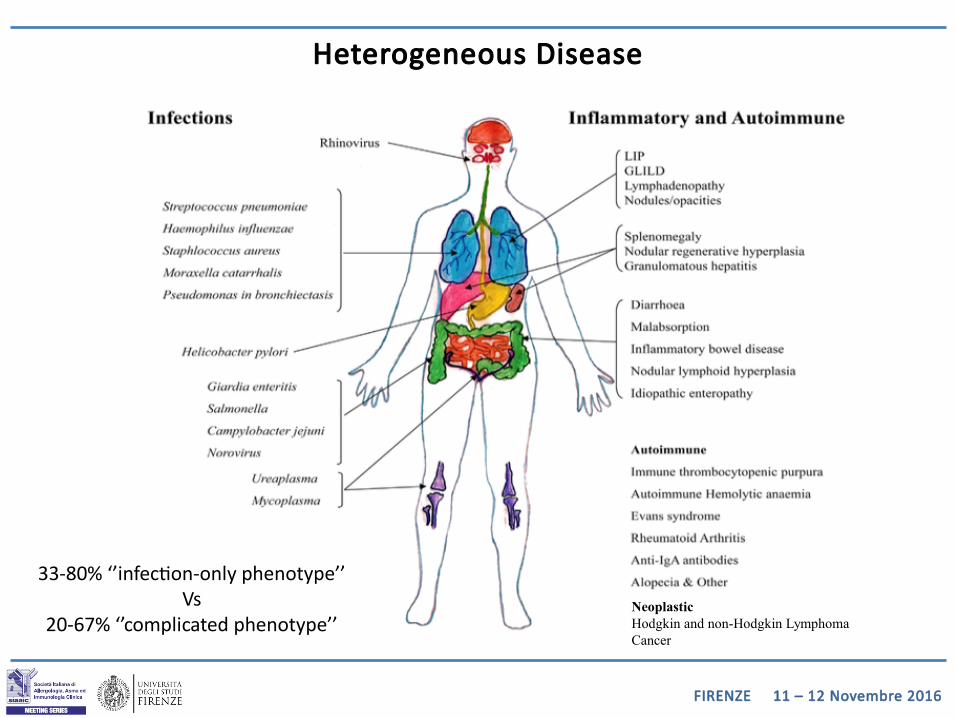
NeoplasticHodgkin and non-Hodgkin Lymphoma Cancer
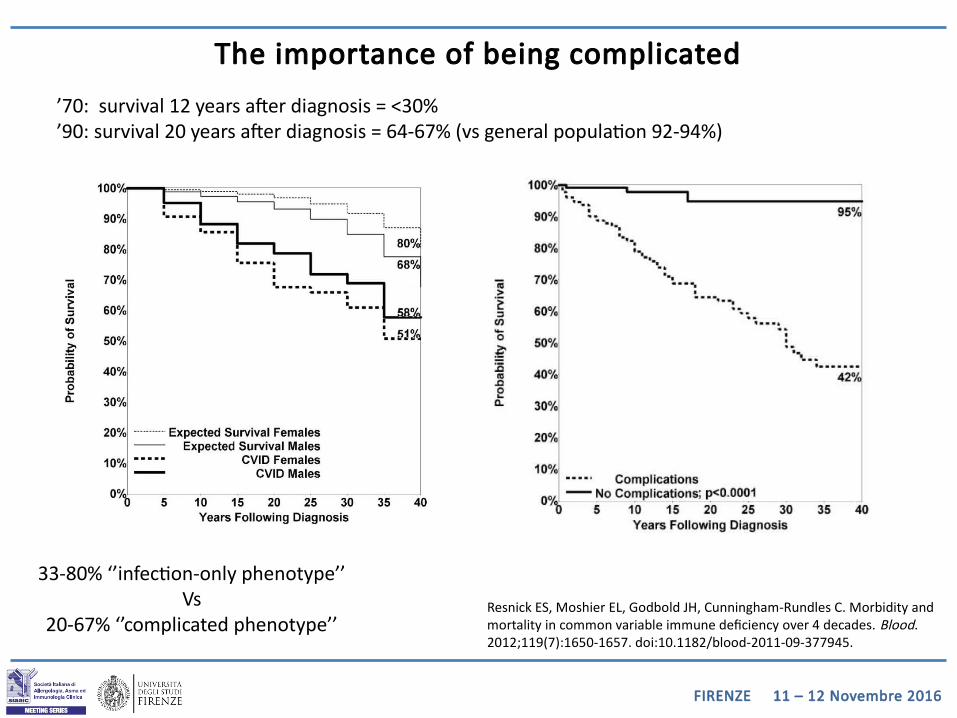
33-80% ‘’infection-only phenotype’’Vs
20-67% ‘’complicated phenotype’’
Heterogeneous Disease
FIRENZE 11 – 12 Novembre 2016
Resnick ES, Moshier EL, Godbold JH, Cunningham-Rundles C. Morbidity and mortality in common variable immune deficiency over 4 decades. Blood. 2012;119(7):1650-1657. doi:10.1182/blood-2011-09-377945.
33-80% ‘’infection-only phenotype’’Vs
20-67% ‘’complicated phenotype’’
The importance of being complicated
’70: survival 12 years after diagnosis = <30%’90: survival 20 years after diagnosis = 64-67% (vs general population 92-94%)
FIRENZE 11 – 12 Novembre 2016
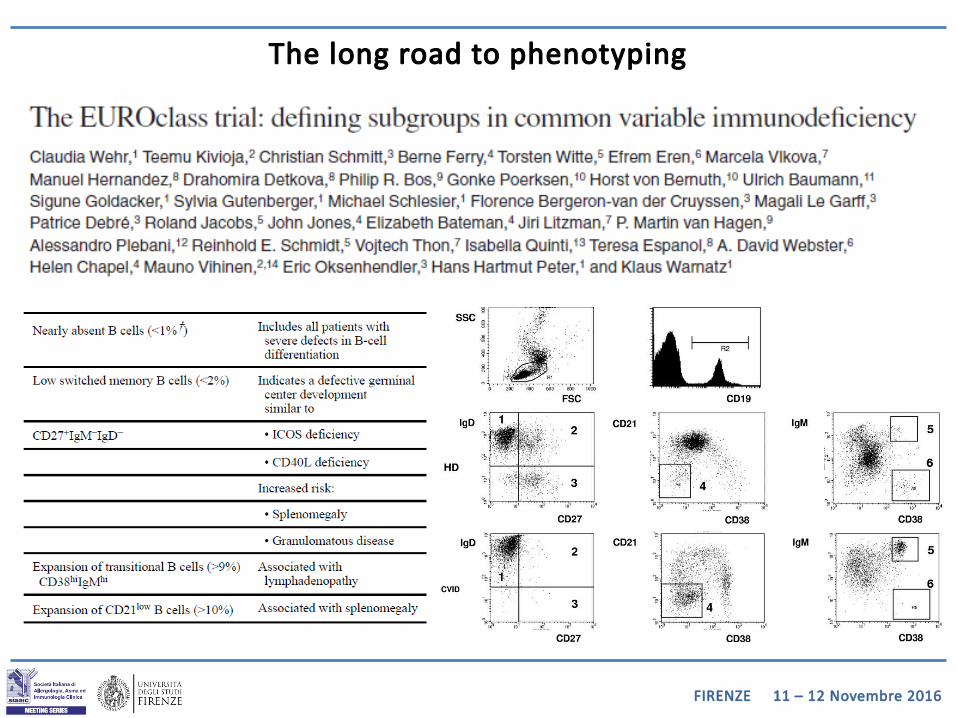
The long road to phenotyping
FIRENZE 11 – 12 Novembre 2016
FIRENZE 11 – 12 Novembre 2016
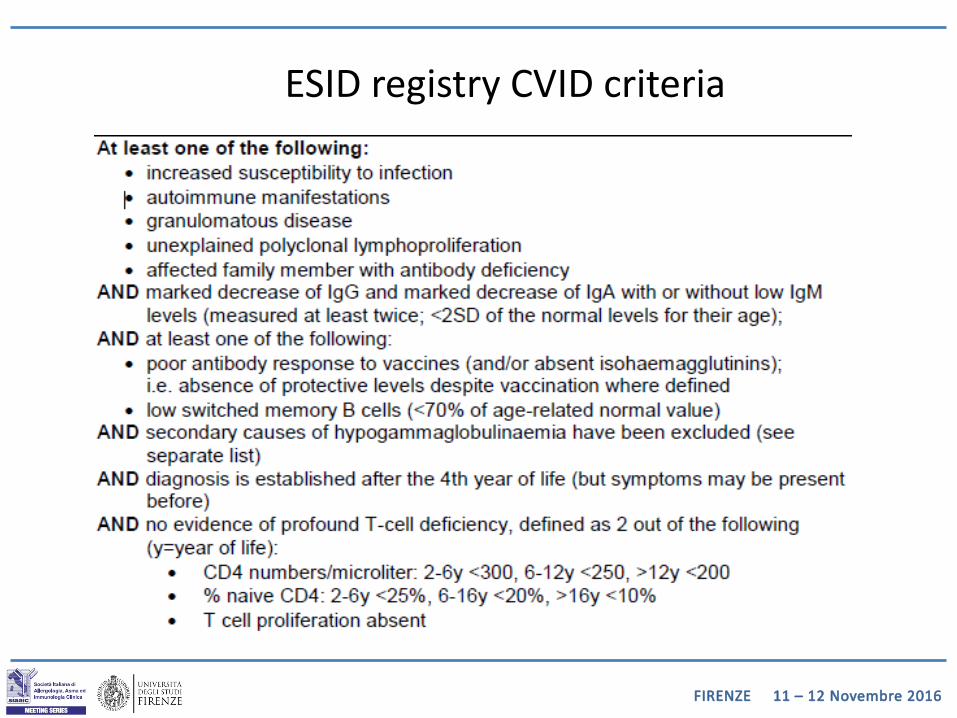
ESID registry CVID criteria
FIRENZE 11 – 12 Novembre 2016
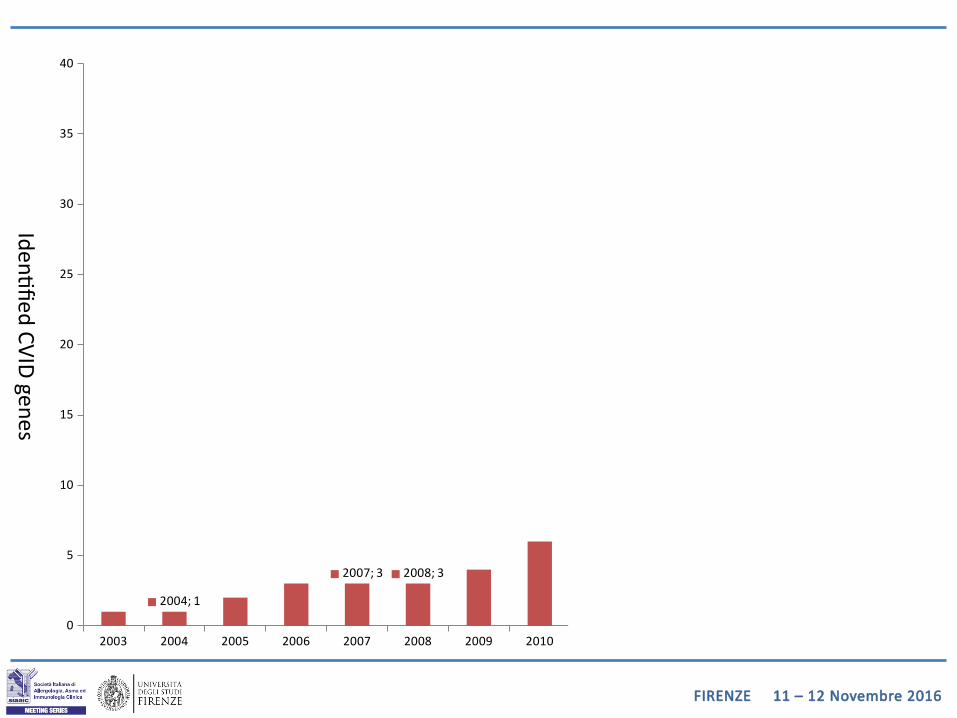
2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 20160
5
10
15
20
25
30
35
40
2004; 1
2007; 3 2008; 3
2011; 6
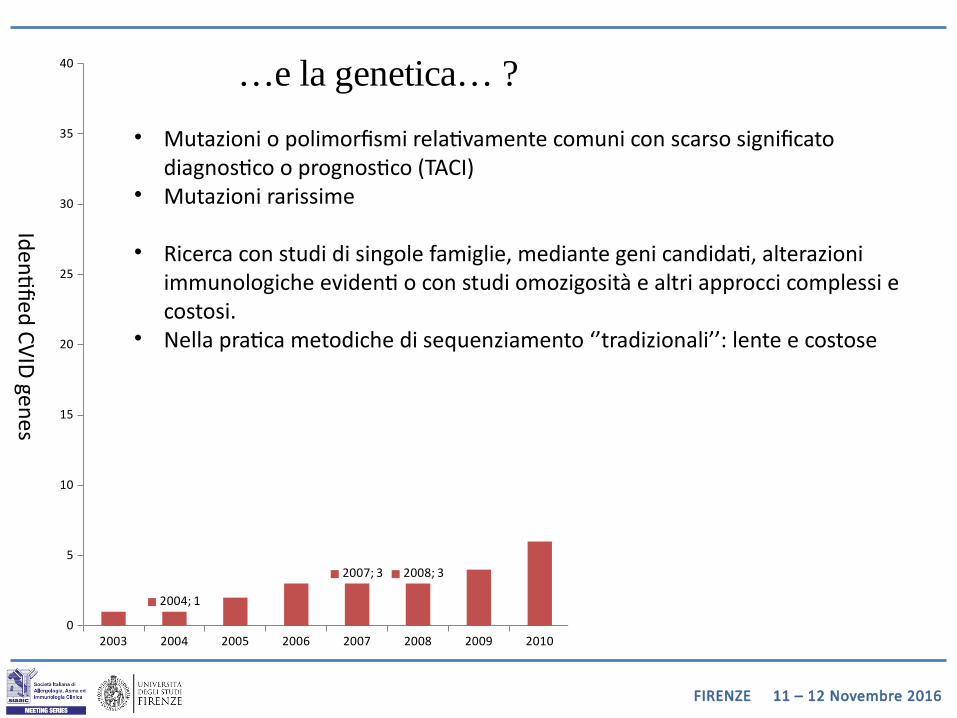
…e la genetica… ?
Identifie d CVID g enes
• Mutazioni o polimorfismi relativamente comuni con scarso significato diagnostico o prognostico (TACI)
• Mutazioni rarissime
• Ricerca con studi di singole famiglie, mediante geni candidati, alterazioni immunologiche evidenti o con studi omozigosità e altri approcci complessi e costosi.
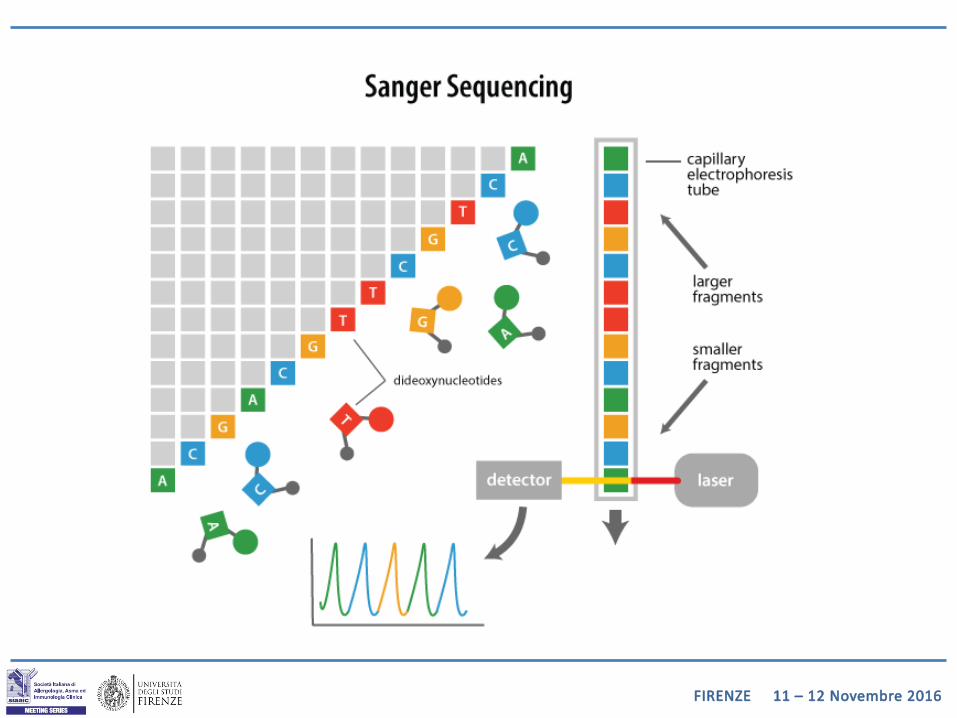
• Nella pratica metodiche di sequenziamento ‘’tradizionali’’: lente e costose
FIRENZE 11 – 12 Novembre 2016
FIRENZE 11 – 12 Novembre 2016
FIRENZE 11 – 12 Novembre 2016
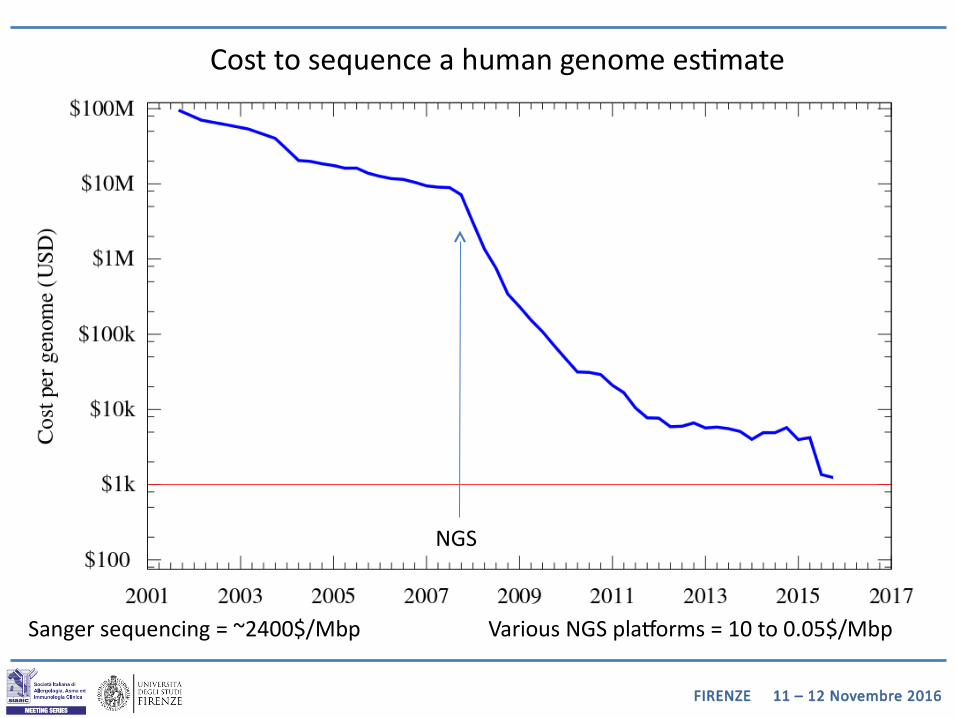
Sanger sequencing = ~2400$/Mbp
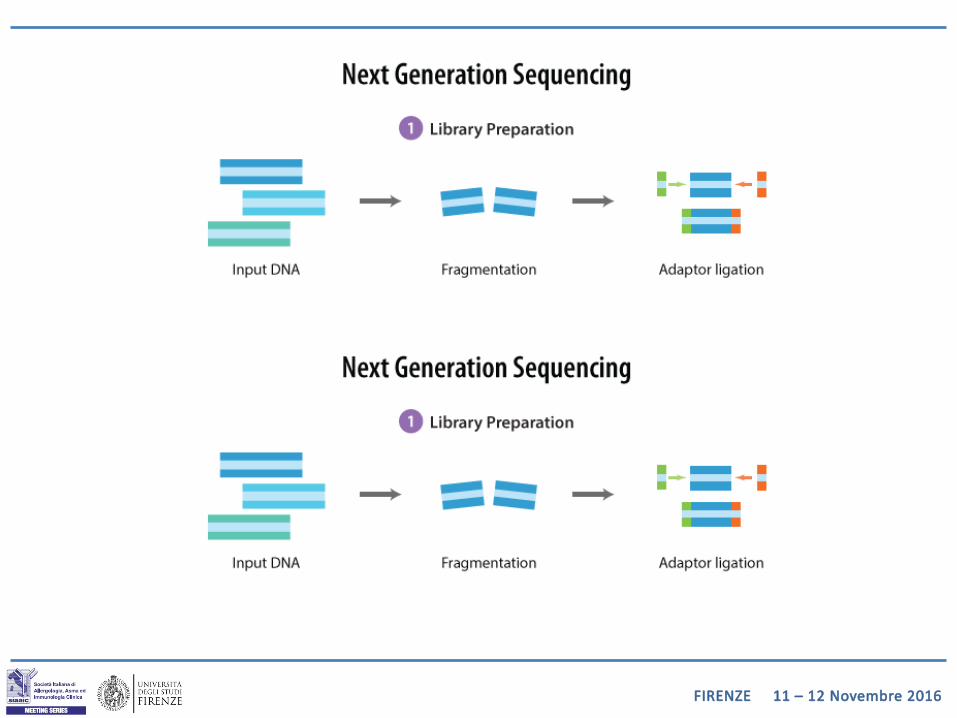
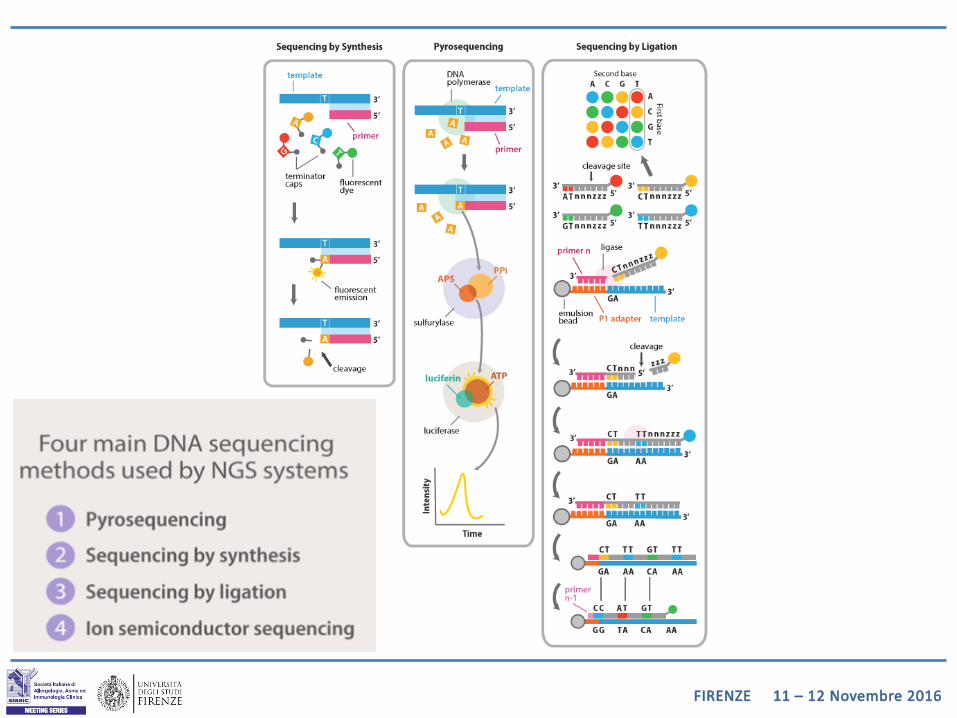
NGS
Various NGS platforms = 10 to 0.05$/Mbp
Cost to sequence a human genome estimate
FIRENZE 11 – 12 Novembre 2016
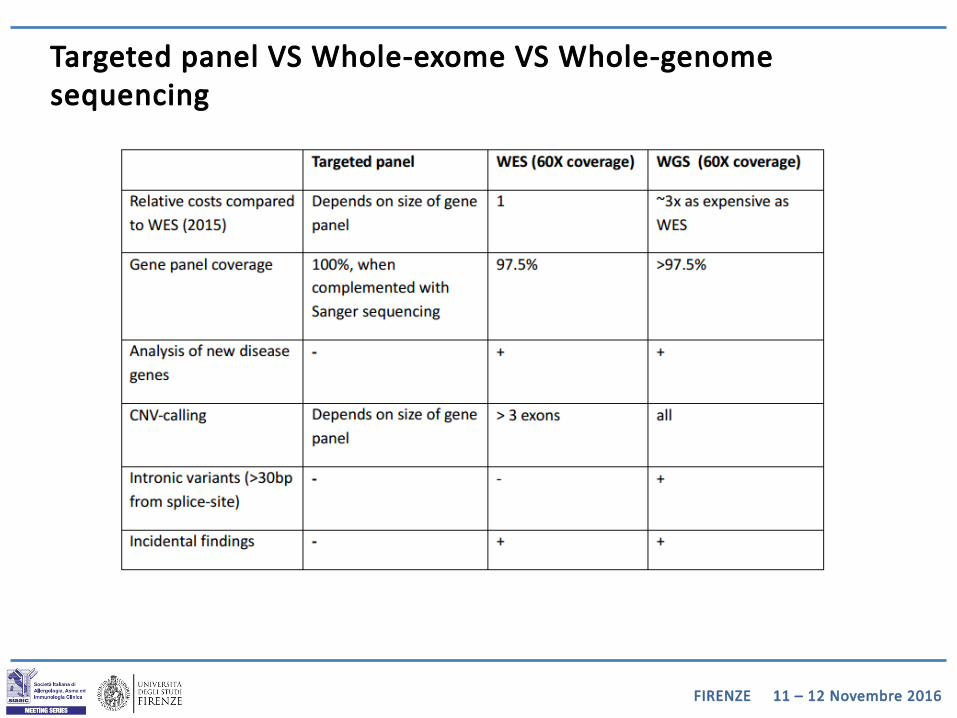
Targeted panel VS Whole-exome VS Whole-genome sequencing
FIRENZE 11 – 12 Novembre 2016
2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 20160
5
10
15
20
25
30
35
40
2004; 1
2007; 3 2008; 3
2011; 6
Identifie d CVID g enes
FIRENZE 11 – 12 Novembre 2016
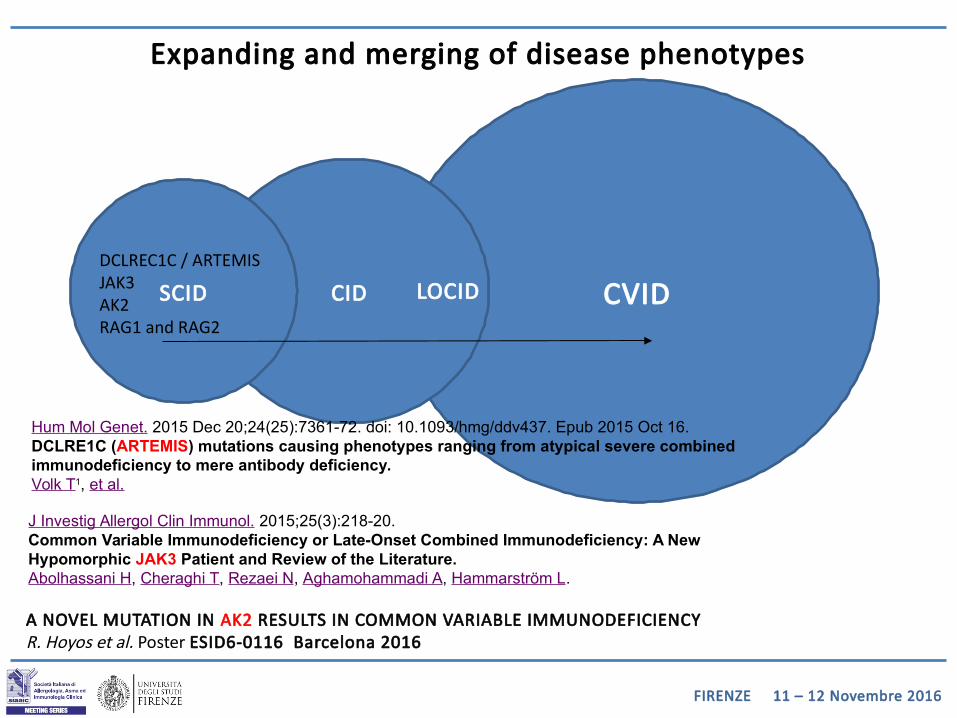
Expanding and merging of disease phenotypes
CVIDCIDSCID LOCIDDCLREC1C / ARTEMISJAK3 AK2RAG1 and RAG2
Hum Mol Genet. 2015 Dec 20;24(25):7361-72. doi: 10.1093/hmg/ddv437. Epub 2015 Oct 16.DCLRE1C (ARTEMIS) mutations causing phenotypes ranging from atypical severe combined immunodeficiency to mere antibody deficiency.Volk T1, et al.
J Investig Allergol Clin Immunol. 2015;25(3):218-20.Common Variable Immunodeficiency or Late-Onset Combined Immunodeficiency: A New Hypomorphic JAK3 Patient and Review of the Literature.Abolhassani H, Cheraghi T, Rezaei N, Aghamohammadi A, Hammarström L.
A NOVEL MUTATION IN AK2 RESULTS IN COMMON VARIABLE IMMUNODEFICIENCY R. Hoyos et al. Poster ESID6-0116 Barcelona 2016
FIRENZE 11 – 12 Novembre 2016
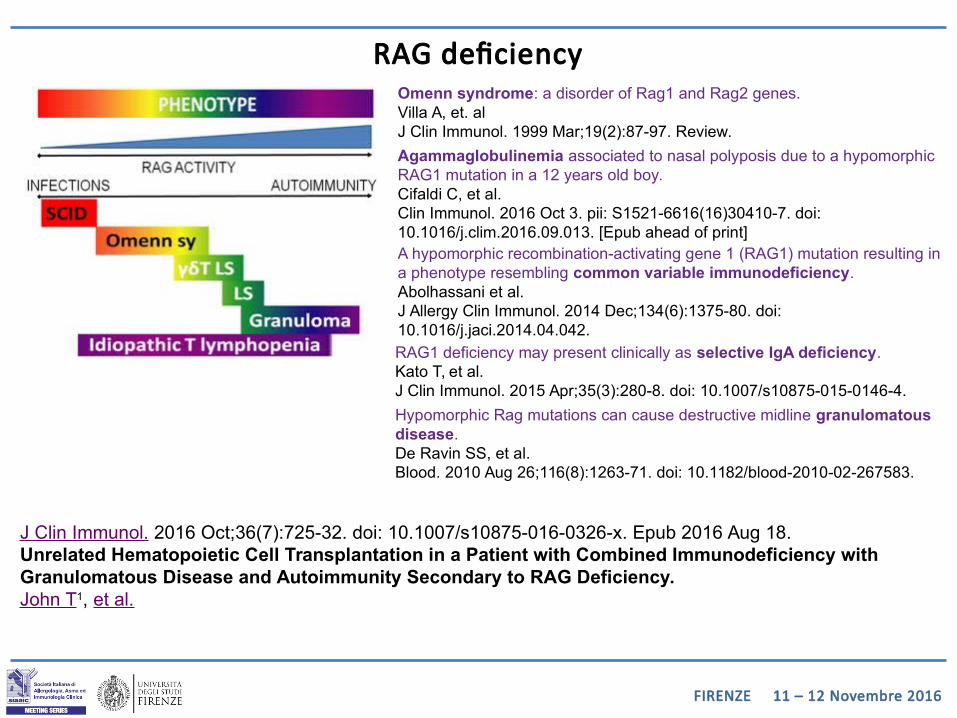
RAG deficiency
Agammaglobulinemia associated to nasal polyposis due to a hypomorphic RAG1 mutation in a 12 years old boy.Cifaldi C, et al.Clin Immunol. 2016 Oct 3. pii: S1521-6616(16)30410-7. doi: 10.1016/j.clim.2016.09.013. [Epub ahead of print]
RAG1 deficiency may present clinically as selective IgA deficiency.Kato T, et al.J Clin Immunol. 2015 Apr;35(3):280-8. doi: 10.1007/s10875-015-0146-4.
A hypomorphic recombination-activating gene 1 (RAG1) mutation resulting in a phenotype resembling common variable immunodeficiency.Abolhassani et al.J Allergy Clin Immunol. 2014 Dec;134(6):1375-80. doi: 10.1016/j.jaci.2014.04.042.
Omenn syndrome: a disorder of Rag1 and Rag2 genes.Villa A, et. alJ Clin Immunol. 1999 Mar;19(2):87-97. Review.
J Clin Immunol. 2016 Oct;36(7):725-32. doi: 10.1007/s10875-016-0326-x. Epub 2016 Aug 18.Unrelated Hematopoietic Cell Transplantation in a Patient with Combined Immunodeficiency with Granulomatous Disease and Autoimmunity Secondary to RAG Deficiency.John T1, et al.
Hypomorphic Rag mutations can cause destructive midline granulomatous disease.De Ravin SS, et al.Blood. 2010 Aug 26;116(8):1263-71. doi: 10.1182/blood-2010-02-267583.
FIRENZE 11 – 12 Novembre 2016
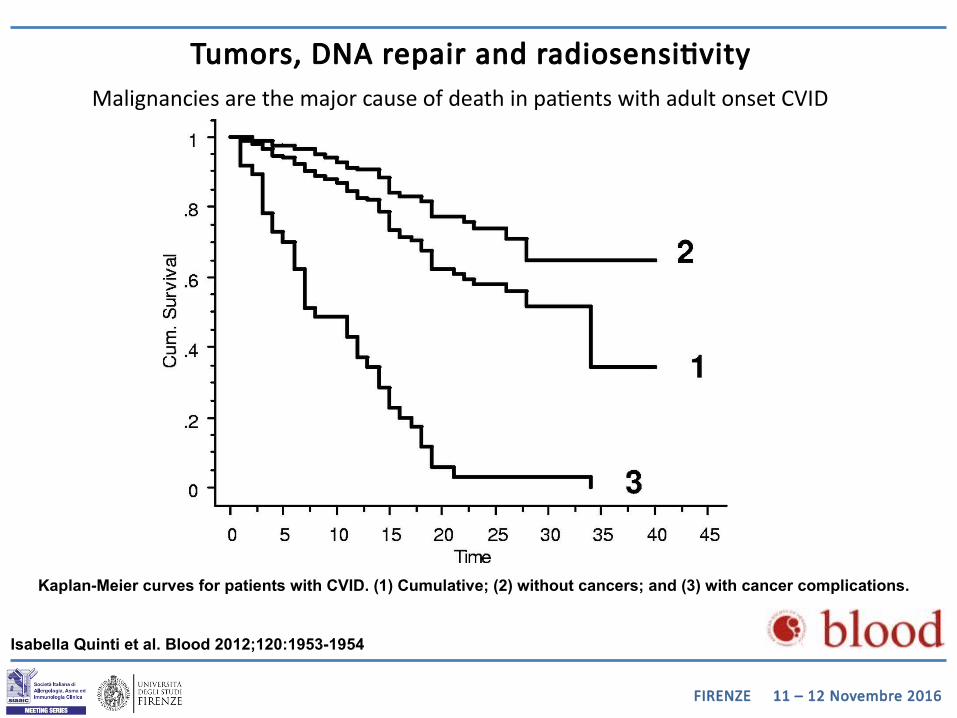
Kaplan-Meier curves for patients with CVID. (1) Cumulative; (2) without cancers; and (3) with cancer complications.
Isabella Quinti et al. Blood 2012;120:1953-1954
Tumors, DNA repair and radiosensitivityMalignancies are the major cause of death in patients with adult onset CVID
FIRENZE 11 – 12 Novembre 2016
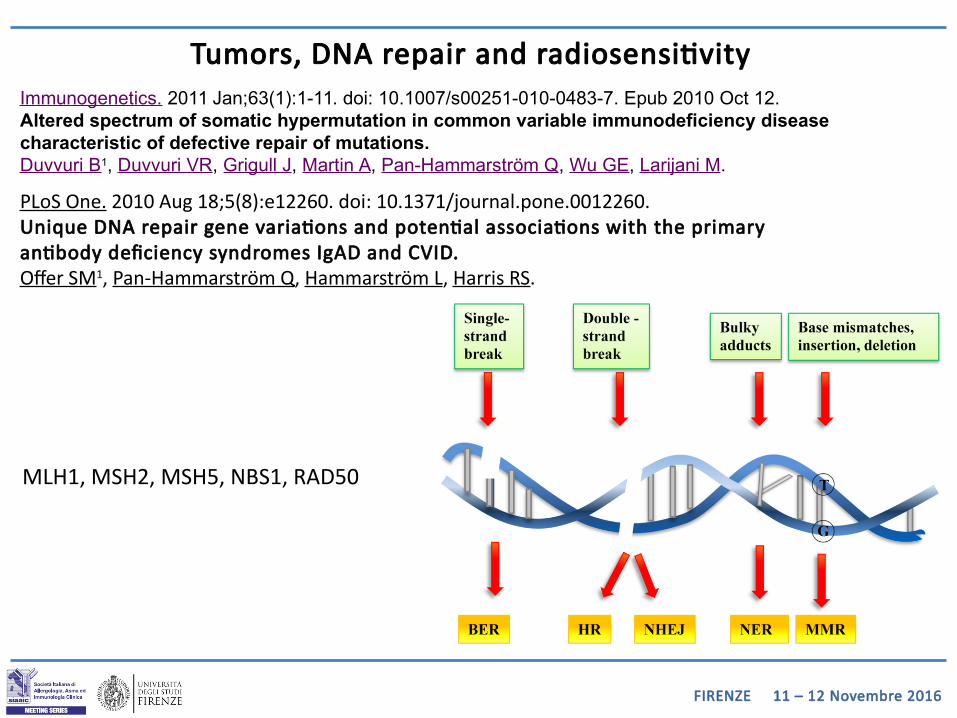
Immunogenetics. 2011 Jan;63(1):1-11. doi: 10.1007/s00251-010-0483-7. Epub 2010 Oct 12.Altered spectrum of somatic hypermutation in common variable immunodeficiency disease characteristic of defective repair of mutations.Duvvuri B1, Duvvuri VR, Grigull J, Martin A, Pan-Hammarström Q, Wu GE, Larijani M.
PLoS One. 2010 Aug 18;5(8):e12260. doi: 10.1371/journal.pone.0012260.Unique DNA repair gene variations and potential associations with the primary antibody deficiency syndromes IgAD and CVID.Offer SM1, Pan-Hammarström Q, Hammarström L, Harris RS.
MLH1, MSH2, MSH5, NBS1, RAD50
Tumors, DNA repair and radiosensitivity
FIRENZE 11 – 12 Novembre 2016
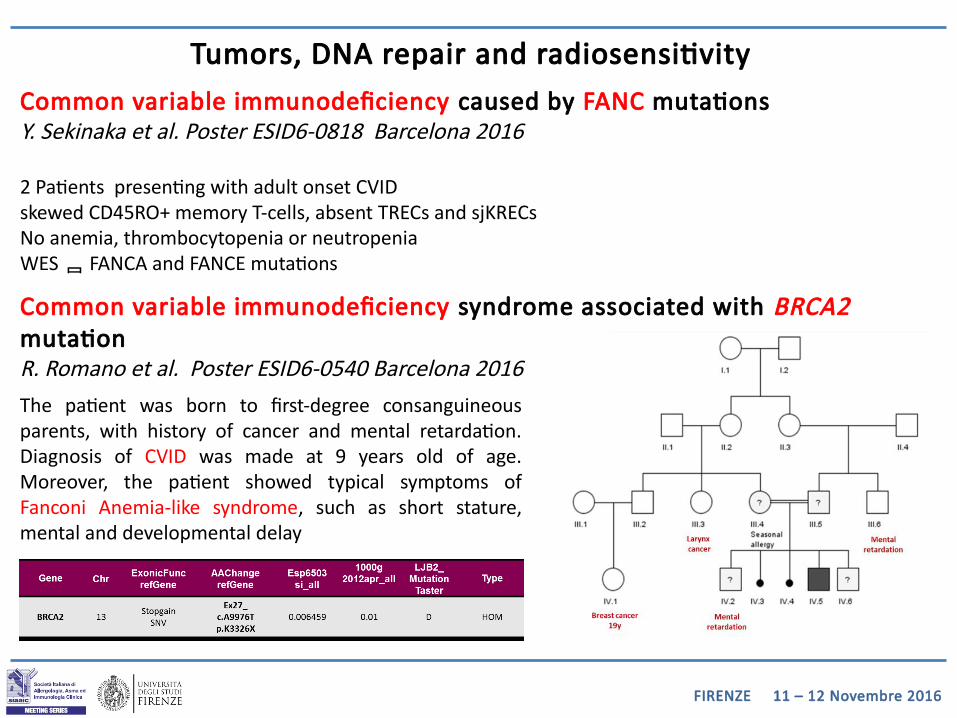
Common variable immunodeficiency caused by FANC mutations Y. Sekinaka et al. Poster ESID6-0818 Barcelona 2016
2 Patients presenting with adult onset CVIDskewed CD45RO+ memory T-cells, absent TRECs and sjKRECsNo anemia, thrombocytopenia or neutropeniaWES FANCA and FANCE mutations
Common variable immunodeficiency syndrome associated with BRCA2 mutationR. Romano et al. Poster ESID6-0540 Barcelona 2016
The patient was born to first-degree consanguineous parents, with history of cancer and mental retardation. Diagnosis of CVID was made at 9 years old of age. Moreover, the patient showed typical symptoms of Fanconi Anemia-like syndrome, such as short stature, mental and developmental delay
Tumors, DNA repair and radiosensitivity
FIRENZE 11 – 12 Novembre 2016
Tumors, DNA repair and radiosensitivity
Implicazioni nella gestione clinica:• Uso di radiazioni ionizzanti ?• Uso di chemioterapici alchilanti ?
Implicazioni prognostiche ed etiche:• Screening per tumori più stretto ?• Rischio di tumori nella famiglia ?
FIRENZE 11 – 12 Novembre 2016
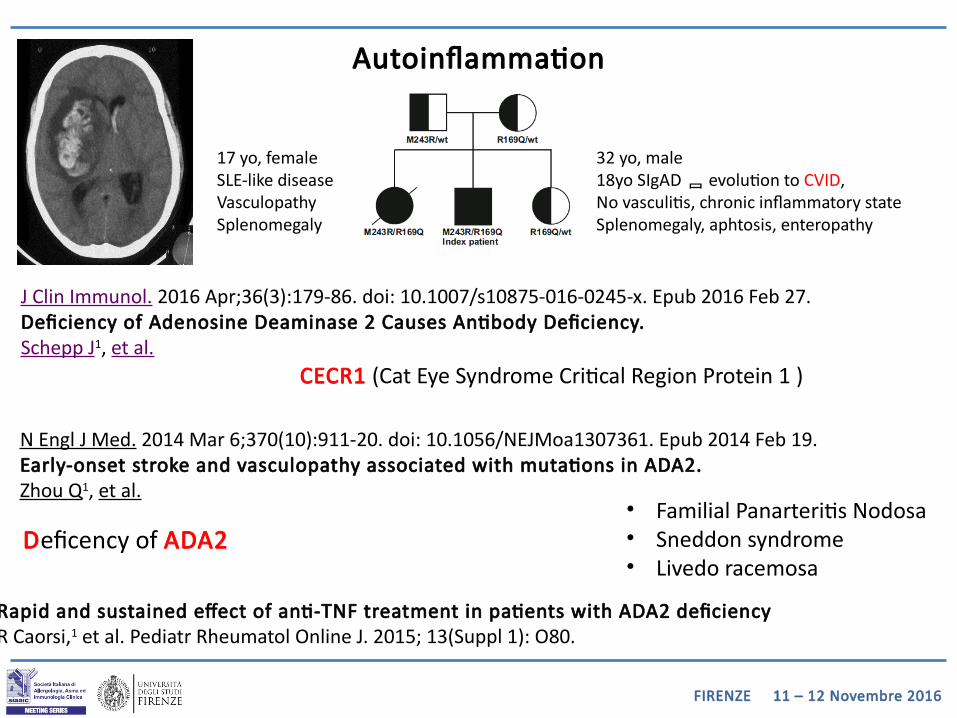
J Clin Immunol. 2016 Apr;36(3):179-86. doi: 10.1007/s10875-016-0245-x. Epub 2016 Feb 27.Deficiency of Adenosine Deaminase 2 Causes Antibody Deficiency.Schepp J1, et al.
Autoinflammation
N Engl J Med. 2014 Mar 6;370(10):911-20. doi: 10.1056/NEJMoa1307361. Epub 2014 Feb 19.Early-onset stroke and vasculopathy associated with mutations in ADA2.Zhou Q1, et al.
Deficency of ADA2 • Familial Panarteritis Nodosa• Sneddon syndrome• Livedo racemosa
17 yo, femaleSLE-like diseaseVasculopathySplenomegaly
32 yo, male18yo SIgAD evolution to CVID,No vasculitis, chronic inflammatory stateSplenomegaly, aphtosis, enteropathy
CECR1 (Cat Eye Syndrome Critical Region Protein 1 )
Rapid and sustained effect of anti-TNF treatment in patients with ADA2 deficiencyR Caorsi,1 et al. Pediatr Rheumatol Online J. 2015; 13(Suppl 1): O80.
FIRENZE 11 – 12 Novembre 2016
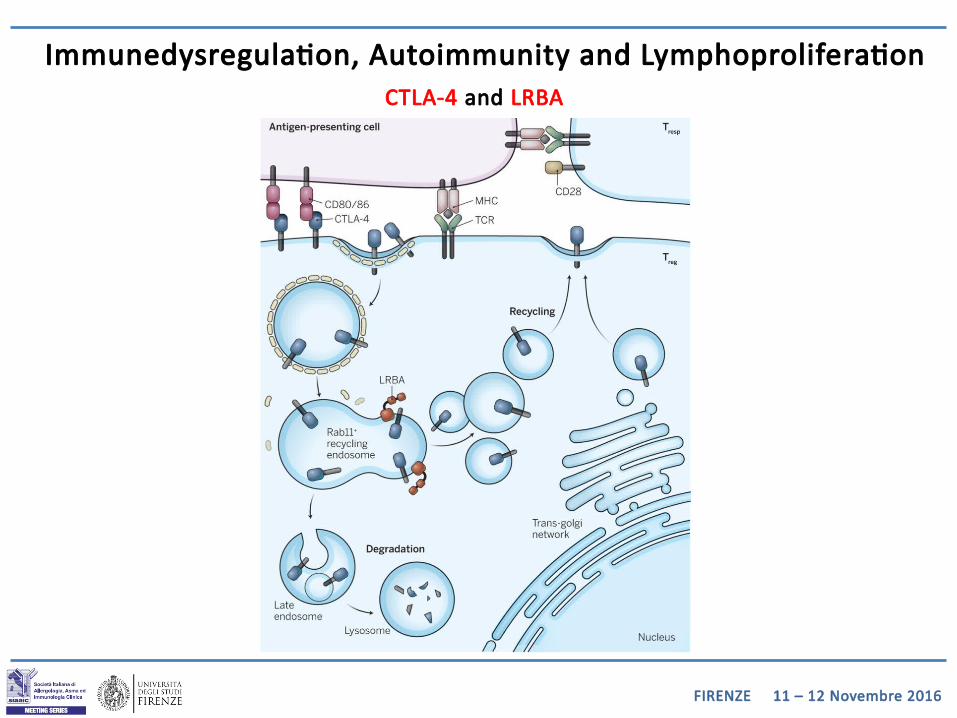
CTLA-4 and LRBA
Immunedysregulation, Autoimmunity and Lymphoproliferation
FIRENZE 11 – 12 Novembre 2016
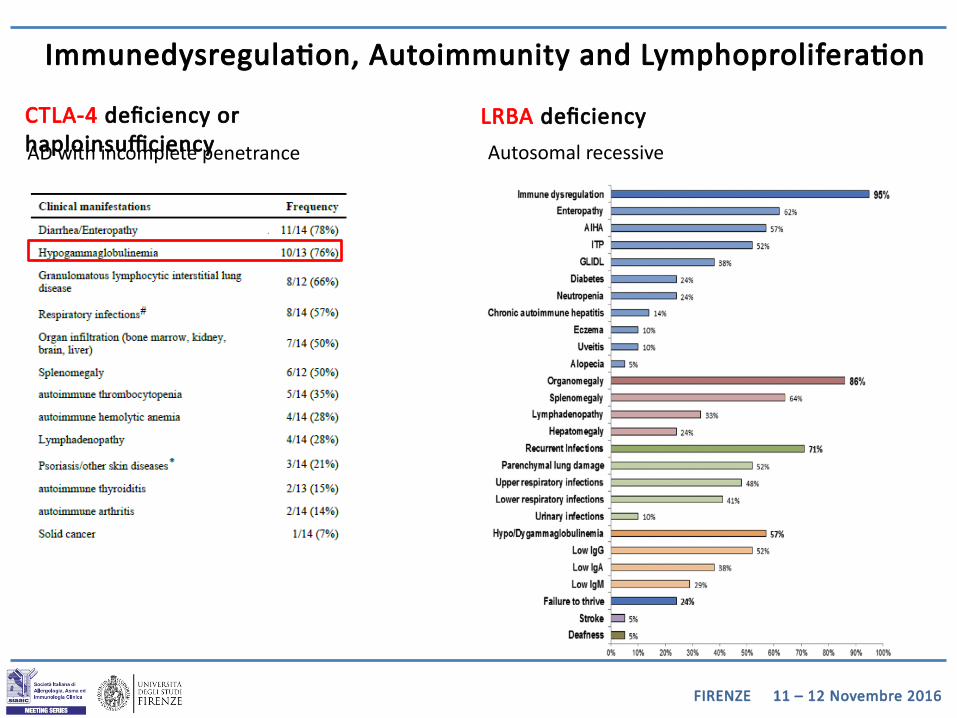
CTLA-4 deficiency or haploinsufficiency
Immunedysregulation, Autoimmunity and Lymphoproliferation
AD with incomplete penetrance
LRBA deficiency
Autosomal recessive
FIRENZE 11 – 12 Novembre 2016
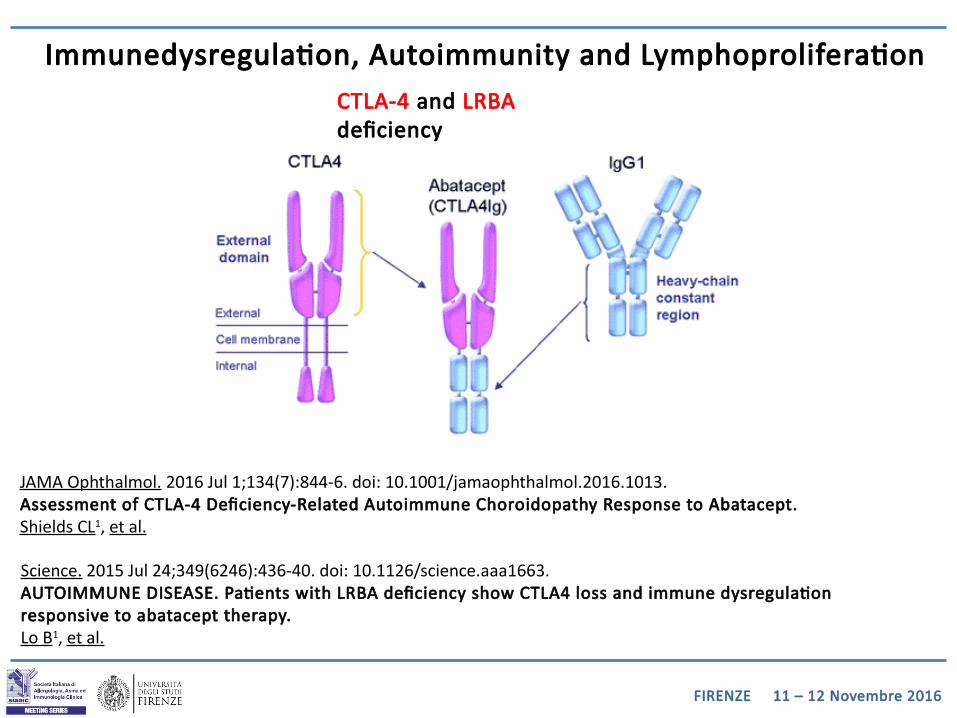
Science. 2015 Jul 24;349(6246):436-40. doi: 10.1126/science.aaa1663.AUTOIMMUNE DISEASE. Patients with LRBA deficiency show CTLA4 loss and immune dysregulation responsive to abatacept therapy.Lo B1, et al.
Immunedysregulation, Autoimmunity and LymphoproliferationCTLA-4 and LRBA deficiency
JAMA Ophthalmol. 2016 Jul 1;134(7):844-6. doi: 10.1001/jamaophthalmol.2016.1013.Assessment of CTLA-4 Deficiency-Related Autoimmune Choroidopathy Response to Abatacept.Shields CL1, et al.
FIRENZE 11 – 12 Novembre 2016
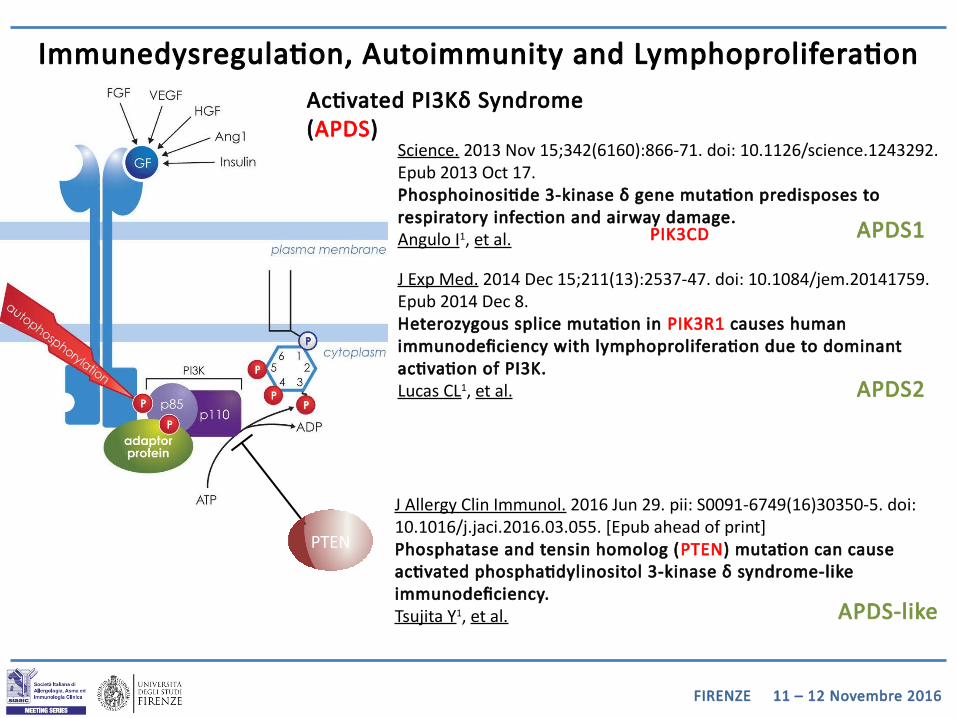
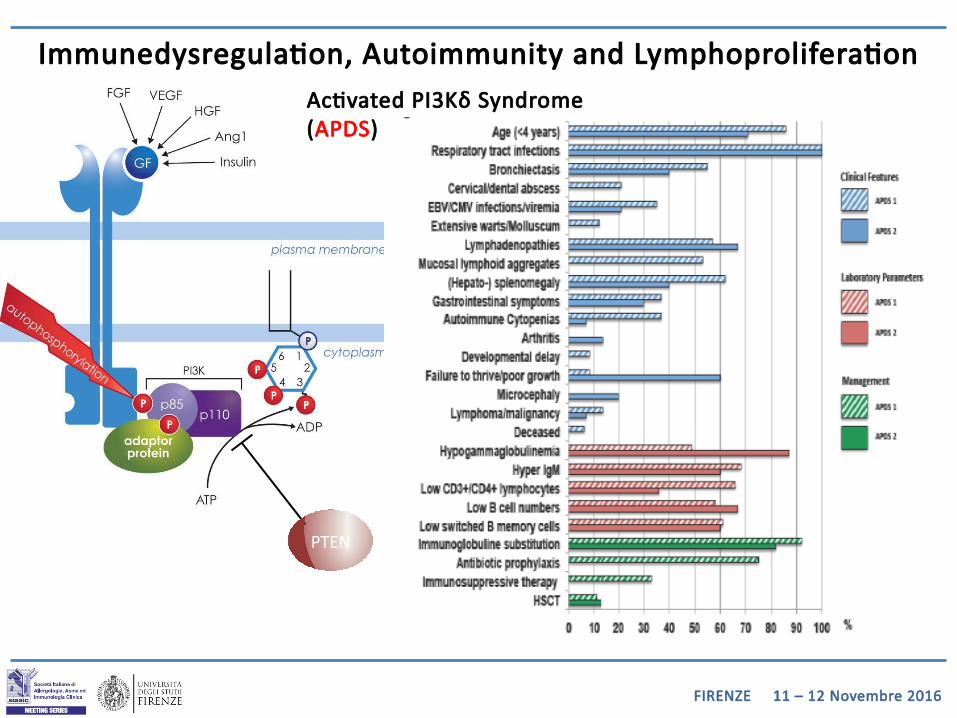
Immunedysregulation, Autoimmunity and LymphoproliferationActivated PI3Kδ Syndrome (APDS)
Science. 2013 Nov 15;342(6160):866-71. doi: 10.1126/science.1243292. Epub 2013 Oct 17.Phosphoinositide 3-kinase δ gene mutation predisposes to respiratory infection and airway damage.Angulo I1, et al.
J Exp Med. 2014 Dec 15;211(13):2537-47. doi: 10.1084/jem.20141759. Epub 2014 Dec 8.Heterozygous splice mutation in PIK3R1 causes human immunodeficiency with lymphoproliferation due to dominant activation of PI3K.Lucas CL1, et al.
PIK3CD
J Allergy Clin Immunol. 2016 Jun 29. pii: S0091-6749(16)30350-5. doi: 10.1016/j.jaci.2016.03.055. [Epub ahead of print]Phosphatase and tensin homolog (PTEN) mutation can cause activated phosphatidylinositol 3-kinase δ syndrome-like immunodeficiency.Tsujita Y1, et al.
PTEN
APDS-like
APDS1
APDS2
FIRENZE 11 – 12 Novembre 2016
Immunedysregulation, Autoimmunity and LymphoproliferationActivated PI3Kδ Syndrome (APDS)
PTEN

FIRENZE 11 – 12 Novembre 2016
Immunedysregulation, Autoimmunity and LymphoproliferationActivated PI3Kδ Syndrome (APDS)
FIRENZE 11 – 12 Novembre 2016
FIRENZE 11 – 12 Novembre 2016
FIRENZE 11 – 12 Novembre 2016
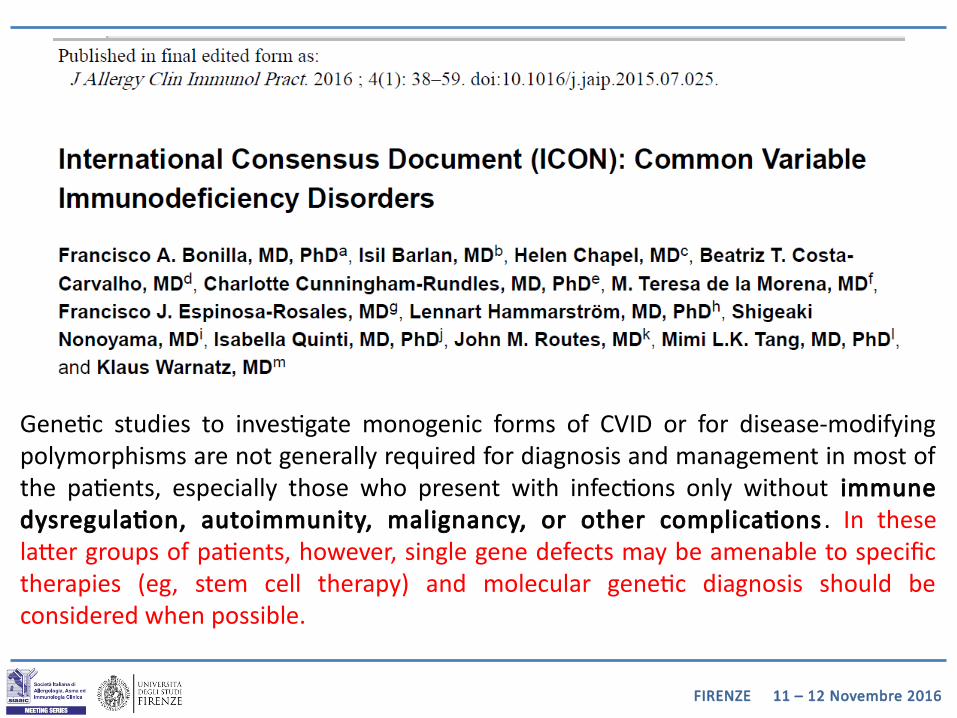
Genetic studies to investigate monogenic forms of CVID or for disease-modifying polymorphisms are not generally required for diagnosis and management in most of the patients, especially those who present with infections only without immune dysregulation, autoimmunity, malignancy, or other complications. In these latter groups of patients, however, single gene defects may be amenable to specific therapies (eg, stem cell therapy) and molecular genetic diagnosis should be considered when possible.
FIRENZE 11 – 12 Novembre 2016
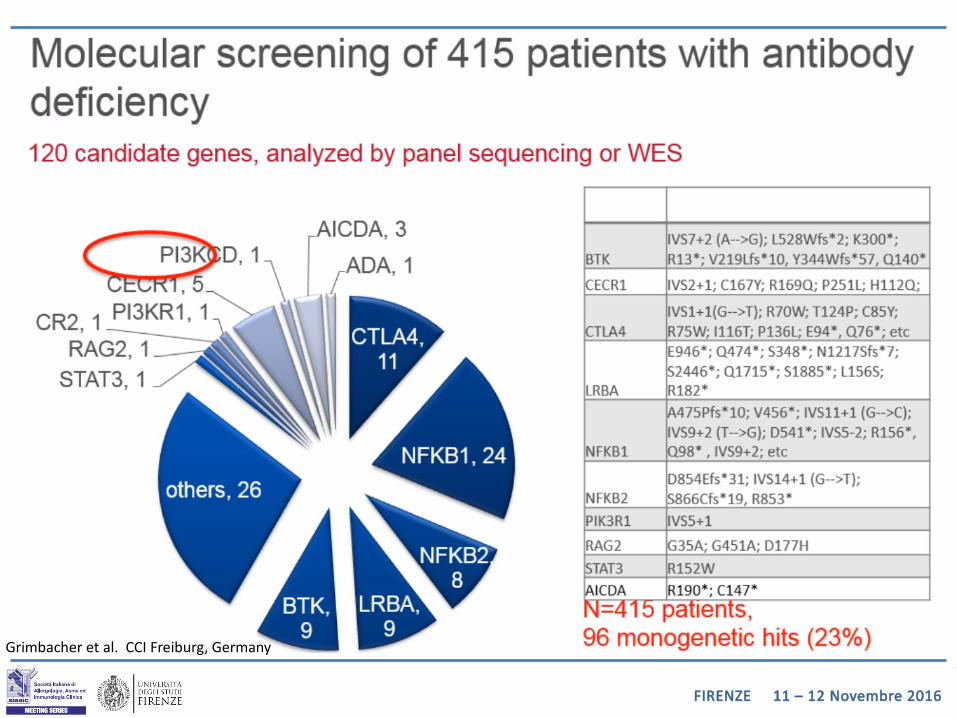
Grimbacher et al. CCI Freiburg, Germany
FIRENZE 11 – 12 Novembre 2016
FIRENZE 11 – 12 Novembre 2016
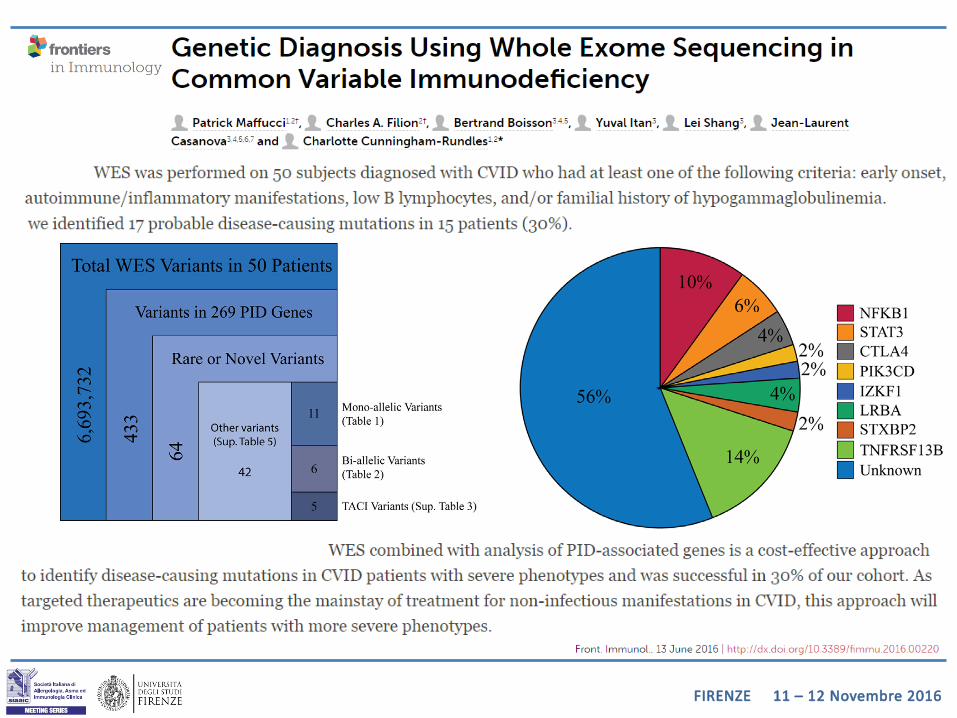
J Allergy Clin Immunol. 2016 Oct;138(4):957-969. doi: 10.1016/j.jaci.2016.08.003.
Exome and genome sequencing for inborn errors of immunity.Meyts I, Casanova JL et al.
[…] Whole-exome sequencing (WES) is presently the most cost-effective approach for research and diagnostics, although whole-genome sequencing offers several advantages.
The scientific or diagnostic challenge consists in selecting 1 or 2 candidate variants among thousands of NGS calls.
[…] Subsequent functional validation of the disease-causing effect of the candidate variant is critical. Even the most up-to-date dry lab cannot clinch this validation without a seasoned wet lab. […] Finding the needle in the haystack takes patience, prudence, and discernment.
FIRENZE 11 – 12 Novembre 2016
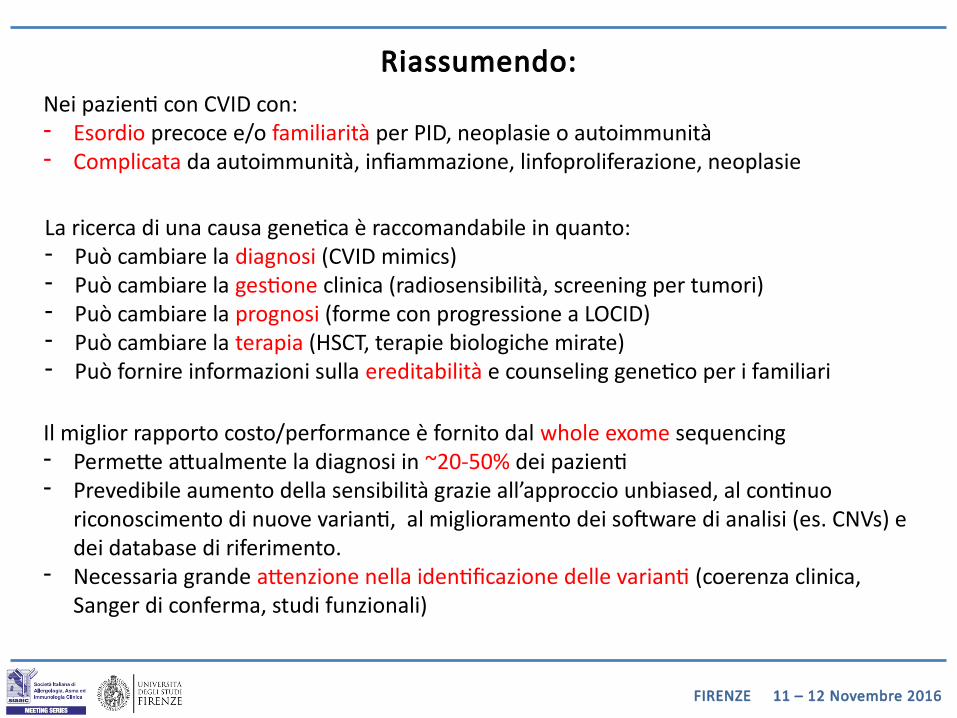
Riassumendo:Nei pazienti con CVID con:- Esordio precoce e/o familiarità per PID, neoplasie o autoimmunità- Complicata da autoimmunità, infiammazione, linfoproliferazione, neoplasie
Il miglior rapporto costo/performance è fornito dal whole exome sequencing- Permette attualmente la diagnosi in ~20-50% dei pazienti - Prevedibile aumento della sensibilità grazie all’approccio unbiased, al continuo
riconoscimento di nuove varianti, al miglioramento dei software di analisi (es. CNVs) e dei database di riferimento.
- Necessaria grande attenzione nella identificazione delle varianti (coerenza clinica, Sanger di conferma, studi funzionali)
La ricerca di una causa genetica è raccomandabile in quanto:- Può cambiare la diagnosi (CVID mimics)- Può cambiare la gestione clinica (radiosensibilità, screening per tumori)- Può cambiare la prognosi (forme con progressione a LOCID)- Può cambiare la terapia (HSCT, terapie biologiche mirate)- Può fornire informazioni sulla ereditabilità e counseling genetico per i familiari
FIRENZE 11 – 12 Novembre 2016
In conclusione….

FIRENZE 11 – 12 Novembre 2016
In conclusione….

Vi ringrazio per l’attenzione…
FIRENZE 11 – 12 Novembre 2016
Prof. Fabio AlmerigognaDott. Daniele CammelliDott. Andrea MatucciDott.ssa Alessandra VultaggioDr.ssa Maria Grazia GiudiziDr.ssa Roberta Biagiot
Prof. Enrico MaggiProf.ssa Paola ParronchiProf. Francesco AnnunziatoProf. Lorenzo CosmiProf. Francesco Liotta
Azienda Ospedaliero Universitaria di Careggi
SOD Immunologia e Terapie Cellulari SOD Immunoallergologia
Gli specializzandi della Scuola di Allergologia e Immunologia Clinica
I tecnici del laboratorio di Immunoallergologia
FIRENZE 11 – 12 Novembre 2016
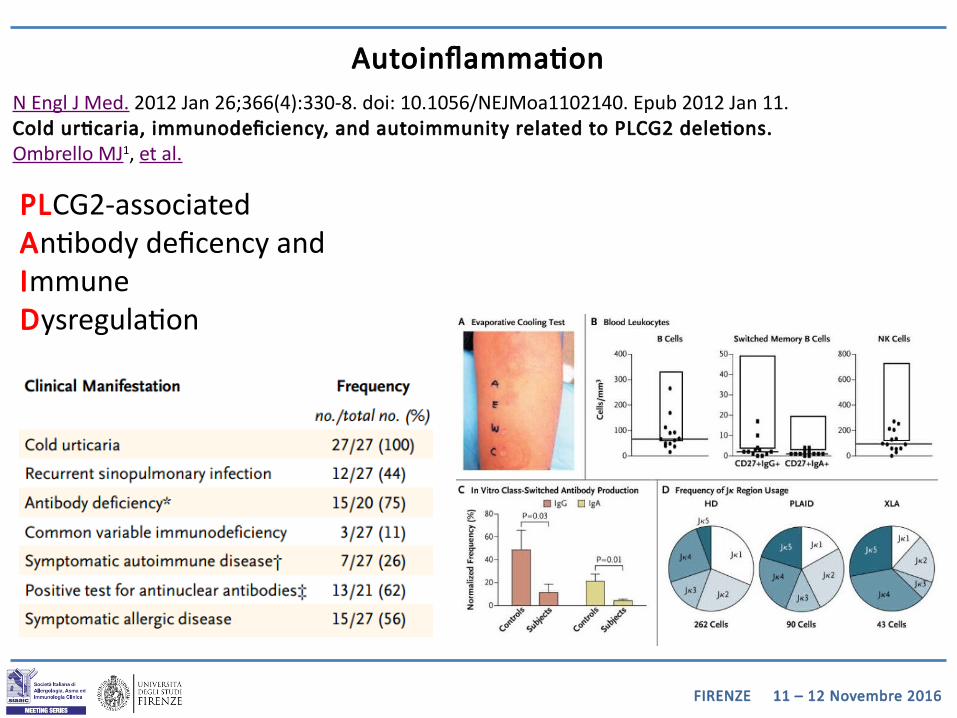
AutoinflammationN Engl J Med. 2012 Jan 26;366(4):330-8. doi: 10.1056/NEJMoa1102140. Epub 2012 Jan 11.Cold urticaria, immunodeficiency, and autoimmunity related to PLCG2 deletions.Ombrello MJ1, et al.
PLCG2-associated Antibody deficency andImmuneDysregulation
FIRENZE 11 – 12 Novembre 2016
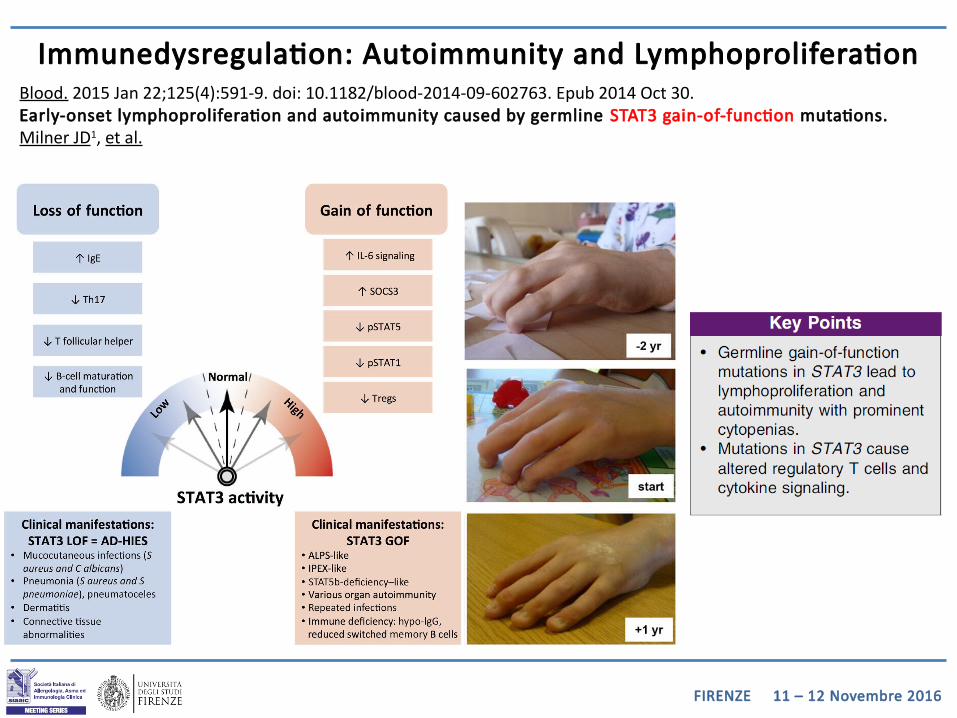
Immunedysregulation: Autoimmunity and LymphoproliferationBlood. 2015 Jan 22;125(4):591-9. doi: 10.1182/blood-2014-09-602763. Epub 2014 Oct 30.Early-onset lymphoproliferation and autoimmunity caused by germline STAT3 gain-of-function mutations.Milner JD1, et al.
FIRENZE 11 – 12 Novembre 2016
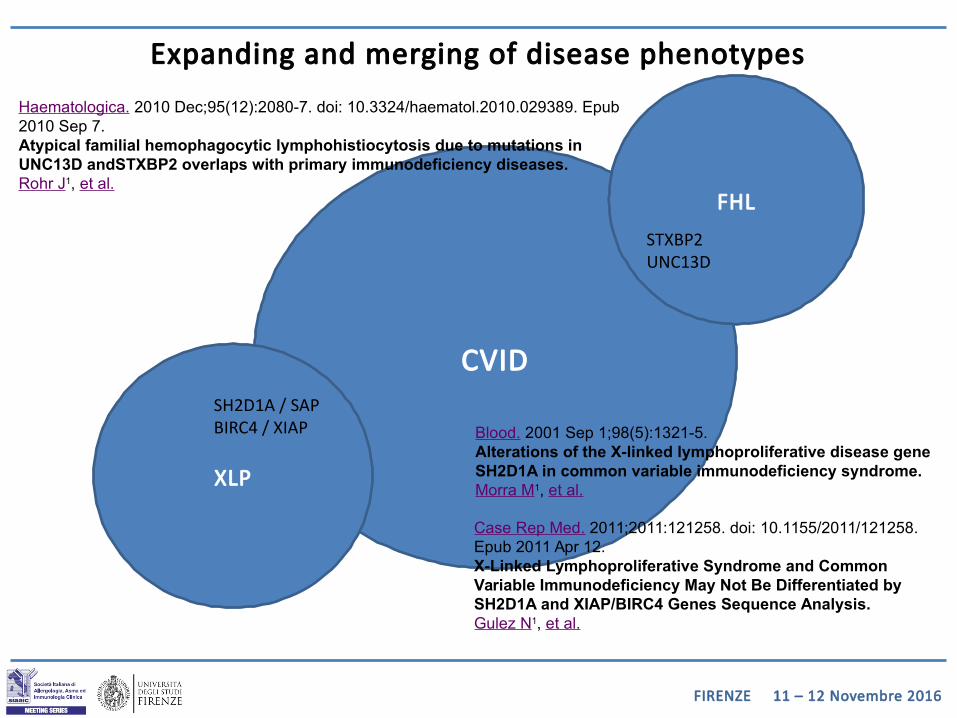
Expanding and merging of disease phenotypes
CVID
FHL
STXBP2UNC13D
Blood. 2001 Sep 1;98(5):1321-5.Alterations of the X-linked lymphoproliferative disease gene SH2D1A in common variable immunodeficiency syndrome.Morra M1, et al.
XLP
SH2D1A / SAPBIRC4 / XIAP
Case Rep Med. 2011;2011:121258. doi: 10.1155/2011/121258. Epub 2011 Apr 12.X-Linked Lymphoproliferative Syndrome and Common Variable Immunodeficiency May Not Be Differentiated by SH2D1A and XIAP/BIRC4 Genes Sequence Analysis.Gulez N1, et al.
Haematologica. 2010 Dec;95(12):2080-7. doi: 10.3324/haematol.2010.029389. Epub 2010 Sep 7.Atypical familial hemophagocytic lymphohistiocytosis due to mutations in UNC13D andSTXBP2 overlaps with primary immunodeficiency diseases.Rohr J1, et al.
FIRENZE 11 – 12 Novembre 2016
Expanding and merging of disease phenotypes
CVID
Other Ab deficencies
Agammaglobulinemia
BTK
Clin Exp Immunol. 2001 Jun;124(3):465-9.Assessment of male CVID patients for mutations in the Btk gene: how many have been misdiagnosed?Weston SA1, Prasad ML, Mullighan CG, Chapel H, Benson EM.
FIRENZE 11 – 12 Novembre 2016
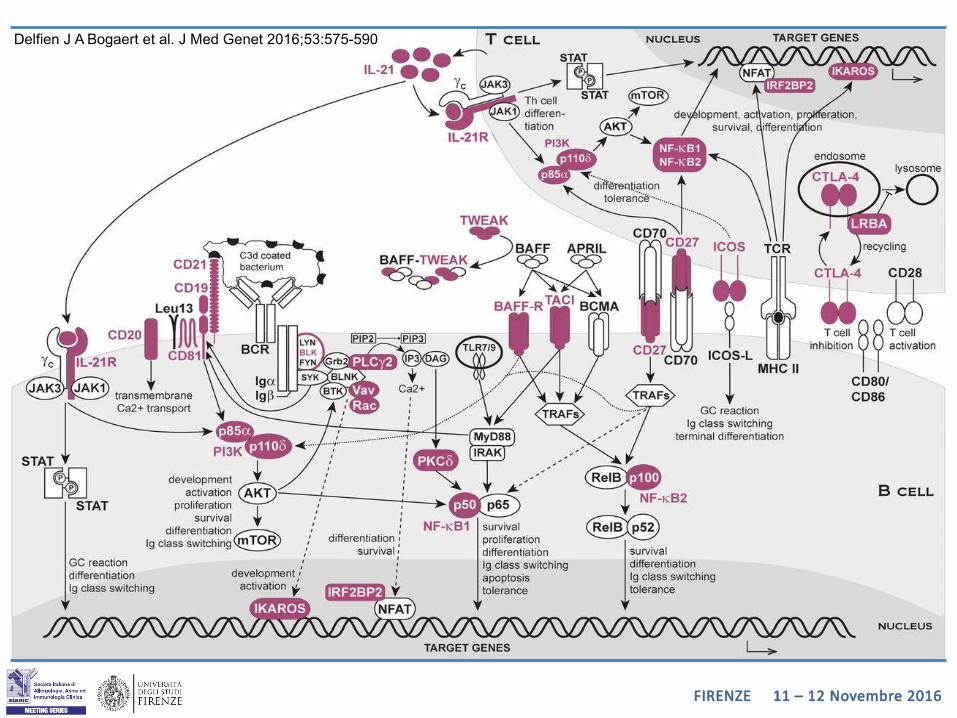
Delfien J A Bogaert et al. J Med Genet 2016;53:575-590
FIRENZE 11 – 12 Novembre 2016
FIRENZE 11 – 12 Novembre 2016
FIRENZE 11 – 12 Novembre 2016
FIRENZE 11 – 12 Novembre 2016
Common Variable Immunodeficiency and Circulating TFHAna Coraglia,1 Nora Galassi,2 Diego S. Fernández Romero,3 M. Cecilia Juri,3Marta Felippo,2 Alejandro Malbrán,3 and María M. E. de Bracco1,2
Journal of Immunology Research, Volume 2016 (2016), Article ID 4951587, 10 pages
Expansion of inflammatory innate lymphoid cells in patients with common variable immune deficiency. Cols M, Rahman A, Maglione PJ, et al. The Journal of allergy and clinical immunology. 2016;137(4):1206-1215.e6. doi:10.1016/j.jaci.2015.09.013.








![Glossario Di Genetica [Dispense Genetica Biologia]](https://static.fdocumenti.com/doc/165x107/5460bdb1af795949708b53b0/glossario-di-genetica-dispense-genetica-biologia.jpg)








