IN COSA SI DIFFERENZIANO LE PSICOTERAPIE? · In Gabbard GO (ed). Le Psicoterapie. Cortina 2010,...
31
1 IN COSA SI DIFFERENZIANO LE PSICOTERAPIE? Obiettivi • Riduzione dei sintomi • Integrazione di parti scisse di sé • Esperienze emozionali correttive • Struttura dell’identità (reframing storia personale, senso di agency, blocchi evolutivi) Setting • Individuale / gruppo (famiglia) • Durata delle sedute (da 45’ a 2h) • Frequenza delle sedute (da 4/settimana a mensili) Contratto terapeutico • Assenze • Pagamenti • Audio/video registrazione • Durata della terapia (da «brevi» a «lungo periodo» • Uso di farmaci Tecniche • Chiarificazione / Confrontazione / Interpretazione • Prescrizioni comportamentali • Homeworks • Ascolto / Comprensione / Empatia • Diagnosi / Motivazione (intrinseca vs estrinseca) Una delle peculiarità della psicologia, rispetto alle altre discipline scientifiche, è la mancanza di un nucleo fondamentale di principi unanimemente condivisi dagli addetti ai lavori e di conseguenza un diverso modo di definire l'oggetto di studio, i meccanismi del funzionamento psichico e i criteri metodologici utilizzabili nella ricerca e nelle applicazioni. Fin dalle origini si sono sviluppate diverse tradizioni di ricerca che hanno determinato suddivisioni e contrapposizioni tra gli psicologi che si riconoscevano in differenti teorie psicologiche. Una delle ragioni principali di questo fenomeno può essere identificata nella complessità dell'oggetto di studio e nel fatto che ciascuna teoria ha scelto di focalizzare la propria attenzione su certi aspetti, piuttosto che su altri, del funzionamento psicologico.
Transcript of IN COSA SI DIFFERENZIANO LE PSICOTERAPIE? · In Gabbard GO (ed). Le Psicoterapie. Cortina 2010,...

1
IN COSA SI DIFFERENZIANO LE PSICOTERAPIE?Obiettivi
• Riduzione dei sintomi• Integrazione di parti scisse di sé• Esperienze emozionali correttive• Struttura dell’identità (reframing storia personale, senso di agency, blocchi evolutivi)
Setting• Individuale / gruppo (famiglia)• Durata delle sedute (da 45’ a 2h)• Frequenza delle sedute (da 4/settimana a mensili)
Contratto terapeutico• Assenze • Pagamenti • Audio/video registrazione• Durata della terapia (da «brevi» a «lungo periodo»• Uso di farmaci
Tecniche• Chiarificazione / Confrontazione / Interpretazione• Prescrizioni comportamentali• Homeworks• Ascolto / Comprensione / Empatia• Diagnosi / Motivazione (intrinseca vs estrinseca)
Una delle peculiarità della psicologia, rispetto alle altre discipline scientifiche, è la mancanza di un nucleo fondamentale di principi unanimemente condivisi dagli addetti ai lavori e di conseguenza un diverso modo di definire l'oggetto di studio, i meccanismi del funzionamento psichico e i criteri metodologici utilizzabili nella ricerca e nelle applicazioni.
Fin dalle origini si sono sviluppate diverse tradizioni di ricerca che hanno determinato suddivisioni e contrapposizioni tra gli psicologi che si riconoscevano in differenti teorie psicologiche.
Una delle ragioni principali di questo fenomeno può essere identificata nella complessità dell'oggetto di studio e nel fatto che ciascuna teoria ha scelto di focalizzare la propria attenzione su certi aspetti, piuttosto che su altri, del funzionamento psicologico.

2
Ogni teoria ha spesso sviluppato un proprio lessico non condiviso, o solo parzialmente condiviso, dalle altre. Se dalla psicologia si passa a considerare la psicoterapia questo fenomeno si ripresenta in misura forse ancora più accentuata. Gli psicoterapeuti si sono divisi per scuole, parrocchie, gruppi e sottogruppi, spesso tanto più agguerriti, gli uni contro gli altri, quanto maggiori erano le somiglianze fra le teorie di partenza.
Negli ultimi anni, con i progressi della conoscenza la situazione si è de-radicalizzata nell' ambito sia psicologico sia psicoterapeutico, con una maggiore disponibilità al dialogo fra i diversi orientamenti, un'accentuata tendenza a un interscambio di concetti teorici e lo sforzo nel considerare fenomeni che precedentemente sembravano essere appannaggio di una sola delle teorie esistenti, riformulandoli in coerenza con i concetti e nel linguaggio caratteristico della propria teoria.
1. una relazione interpersonale di tipo del tutto particolare fra paziente e terapeuta che comporta un' alleanza a esclusivo beneficio del paziente;
2. un luogo specifico - il setting - all' interno del quale si svolge questa relazione, luogo sicuro nel quale tutto ciò che avviene è confidenziale e distinto dal resto delle normali attività e relazioni interpersonali;
3. l'offerta, da parte del terapeuta, di nuove prospettive, nuovi modi di vedere o fare le cose diversi da quelli abituali e in grado di dare un senso a sensazioni confuse e indefinite;
4. un insieme di procedure o tecniche che specificano il modo di operare del terapeuta.
Parafrasando Frank (1961) si può affermare che qualsiasi tipo di psicoterapia condivide almeno quattro caratteristiche fondamentali:
3
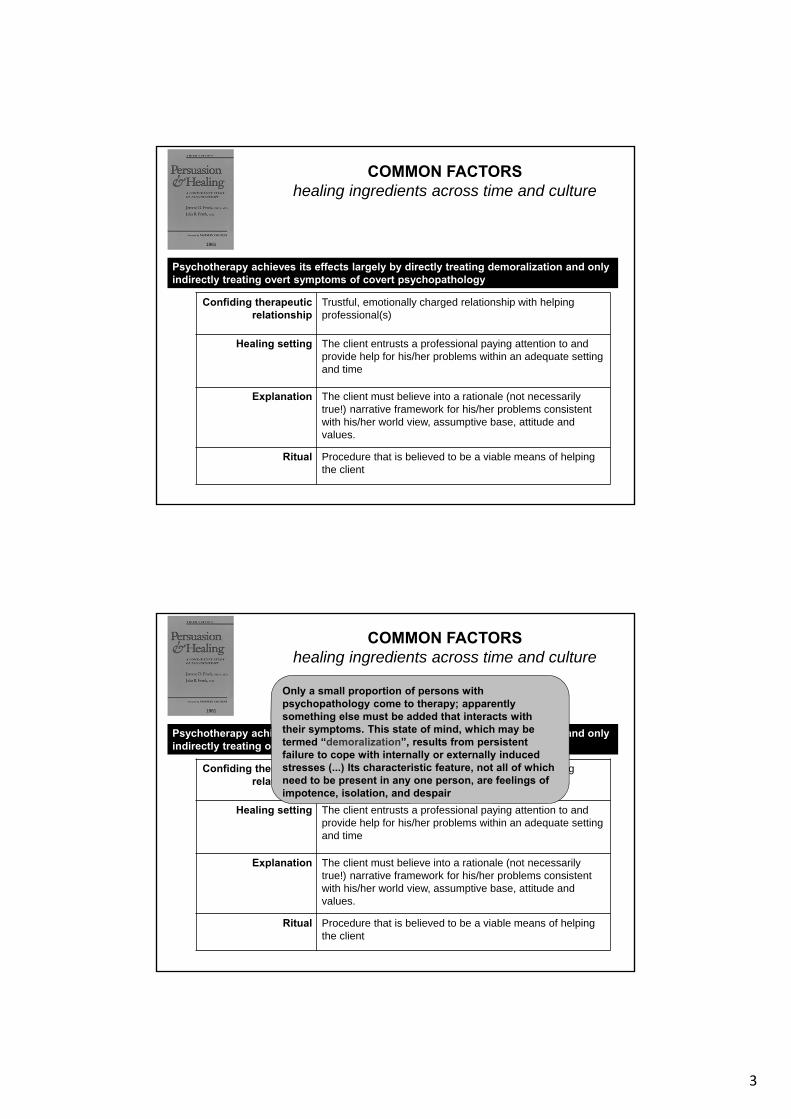
COMMON FACTORShealing ingredients across time and culture
Confiding therapeuticrelationship
Trustful, emotionally charged relationship with helping professional(s)
Healing setting The client entrusts a professional paying attention to and provide help for his/her problems within an adequate setting and time
Explanation The client must believe into a rationale (not necessarily true!) narrative framework for his/her problems consistent with his/her world view, assumptive base, attitude and values.
Ritual Procedure that is believed to be a viable means of helping the client
Psychotherapy achieves its effects largely by directly treating demoralization and only indirectly treating overt symptoms of covert psychopathology
1961
COMMON FACTORShealing ingredients across time and culture
Confiding therapeuticrelationship
Trustful, emotionally charged relationship with helping professional(s)
Healing setting The client entrusts a professional paying attention to and provide help for his/her problems within an adequate setting and time
Explanation The client must believe into a rationale (not necessarily true!) narrative framework for his/her problems consistent with his/her world view, assumptive base, attitude and values.
Ritual Procedure that is believed to be a viable means of helping the client
Psychotherapy achieves its effects largely by directly treating demoralization and only indirectly treating overt symptoms of covert psychopathology
1961
Only a small proportion of persons with psychopathology come to therapy; apparently something else must be added that interacts with their symptoms. This state of mind, which may be termed “demoralization”, results from persistent failure to cope with internally or externally induced stresses (...) Its characteristic feature, not all of which need to be present in any one person, are feelings of impotence, isolation, and despair
4
Beitman BD & Manring J. Teoria e pratica dell’integrazione delle psicoterapie.In Gabbard GO (ed). Le Psicoterapie. Cortina 2010, Cap.26
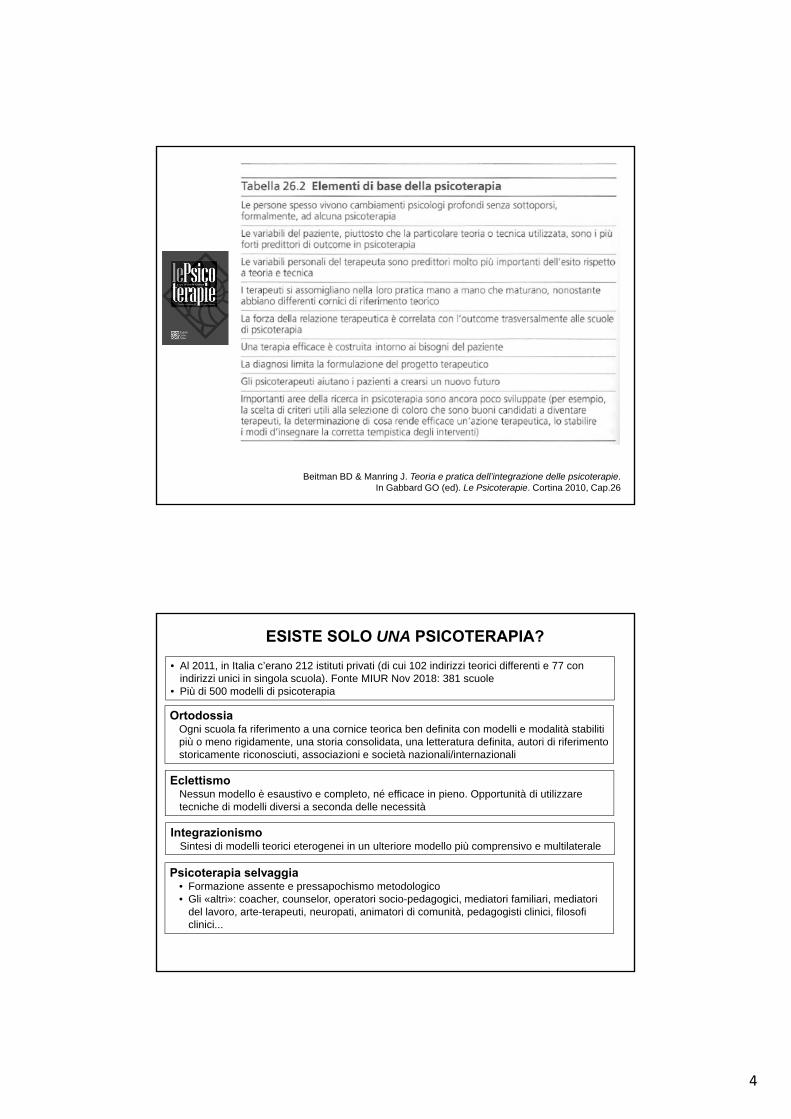
ESISTE SOLO UNA PSICOTERAPIA?
• Al 2011, in Italia c’erano 212 istituti privati (di cui 102 indirizzi teorici differenti e 77 con indirizzi unici in singola scuola). Fonte MIUR Nov 2018: 381 scuole
• Più di 500 modelli di psicoterapia
OrtodossiaOgni scuola fa riferimento a una cornice teorica ben definita con modelli e modalità stabiliti più o meno rigidamente, una storia consolidata, una letteratura definita, autori di riferimento storicamente riconosciuti, associazioni e società nazionali/internazionali
Eclettismo Nessun modello è esaustivo e completo, né efficace in pieno. Opportunità di utilizzare tecniche di modelli diversi a seconda delle necessità
Integrazionismo Sintesi di modelli teorici eterogenei in un ulteriore modello più comprensivo e multilaterale
Psicoterapia selvaggia• Formazione assente e pressapochismo metodologico• Gli «altri»: coacher, counselor, operatori socio-pedagogici, mediatori familiari, mediatori
del lavoro, arte-terapeuti, neuropati, animatori di comunità, pedagogisti clinici, filosofi clinici...
5
ESISTE SOLO LA PSICOTERAPIA?
Sostegno psicologico
• Benessere (wellbeing) generale in situazioni difficili, qui-e-ora e inevitabili (fase di vita, evento catastrofico, malattia acuta o cronica o terminale)
• Accompagnare la persona nella crisi attuale
• Mobilitare le risorse per obiettivi concreti e realistici
• Stimolare la capacità di programmare e effettuare scelte (decision making)
Counseling psicologico-clinico
• Maggiore direttività dello psicologo: non solo «essere-con» ma soprattutto «fare-con»
• Aiuto a identificare il focus del problema
• Aiuto al problem solving / decision making (impasse momentanea che non invalida la propria identità personale) riorganizzando priorità scelte esistenziali
• Validare le risorse già presenti e utilizzarle ai fini del cambiamento adattivo
• Intervento breve (10-12 sedute) in un tempo prestabilito all’inizio
The informed and intentional application of clinical methods and interpersonal stances derived from established psychological principles for the purpose of assisting people to modify their behaviors, cognitions, emotions, and/or other personal characteristics in directions that the participants deem desirable
Norcross, J.C. (1990). An eclectic definition of psychotherapy. In J.K. Zeig & W.M. Munion (Eds.), What is psychotherapy? Contemporary perspectives (218-220). San Francisco, CA: Jossey-Bass
WHAT IS PSYCHOTHERAPY ?
A primarily interpersonal treatment that is
(a) based on psychological principles;
(b) involves a trained therapist and a client who is seeking help for a mentaldisorder, problem or complaint;
(c) is intended by the therapist to be remedial for the client disorder, problem or complaint;
(d) is adapted or individualized for the particular client and his/her disorder, problem or complaint.
Wamplod B.E. & Imel Z.E. (2015). The great psychotherapy debate. The evidence for what makes psychotherapy work (p.37). Routledge
6
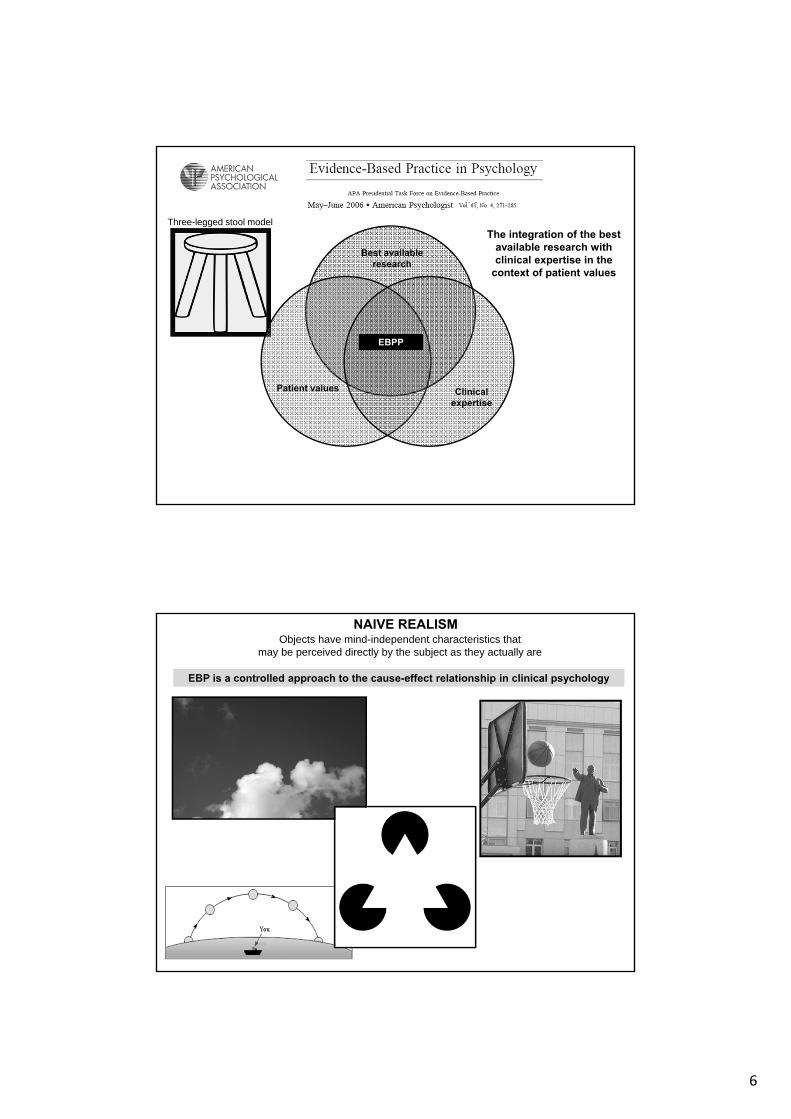
The integration of the best available research with clinical expertise in the
context of patient values
Best available research
Patient values Clinical expertise
EBPP
Three-legged stool model
Objects have mind-independent characteristics thatmay be perceived directly by the subject as they actually are
EBP is a controlled approach to the cause-effect relationship in clinical psychology
NAIVE REALISM
7
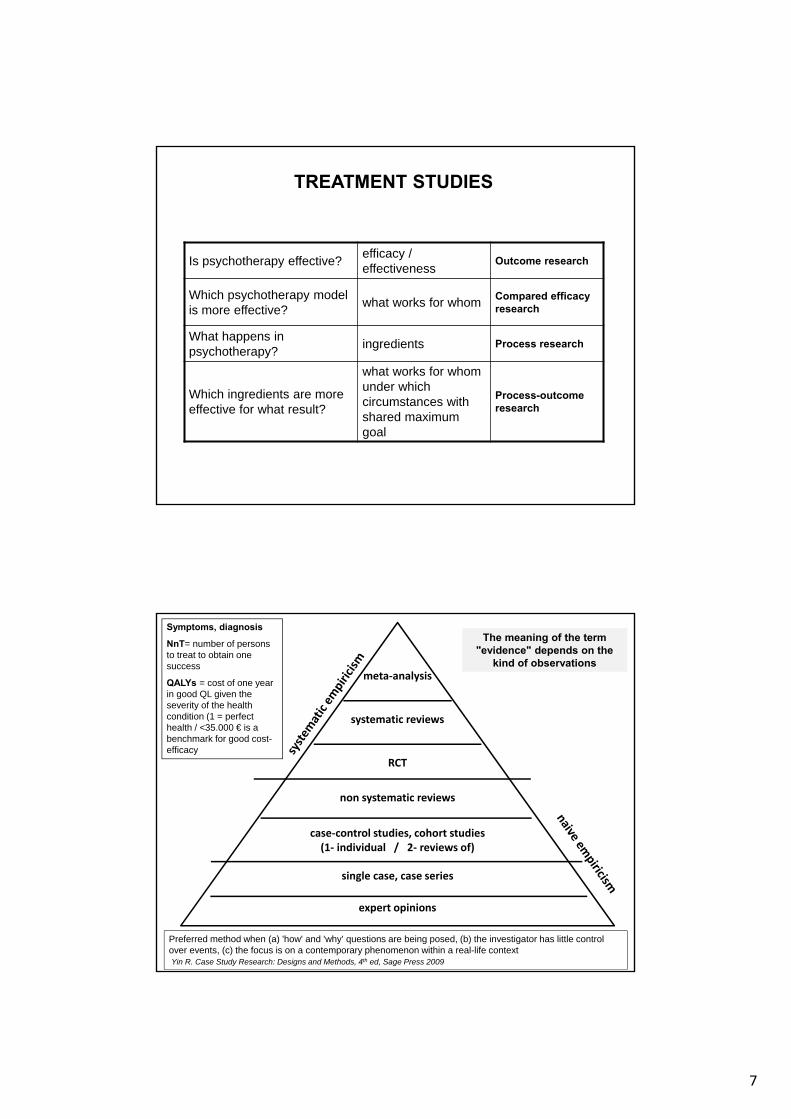
TREATMENT STUDIES
Is psychotherapy effective?efficacy / effectiveness
Outcome research
Which psychotherapy model is more effective?
what works for whomCompared efficacy research
What happens in psychotherapy?
ingredients Process research
Which ingredients are more effective for what result?
what works for whomunder whichcircumstances with shared maximum goal
Process-outcome research
expert opinions
single case, case series
case‐control studies, cohort studies(1‐ individual / 2‐ reviews of)
non systematic reviews
RCT
systematic reviews
meta‐analysis
The meaning of the term"evidence" depends on the
kind of observations
Symptoms, diagnosis
NnT= number of personsto treat to obtain onesuccess
QALYs = cost of one yearin good QL given the severity of the healthcondition (1 = perfecthealth / <35.000 € is a benchmark for good cost-efficacy
Preferred method when (a) 'how' and 'why' questions are being posed, (b) the investigator has little control over events, (c) the focus is on a contemporary phenomenon within a real-life contextYin R. Case Study Research: Designs and Methods, 4th ed, Sage Press 2009
8
VALUTARE IL CAMBIAMENTO
• Pre/post in gruppi trattati/controllo: non fornisce informazioni su variabilità individuale
• Significatività statistica (p<0.5!) indica che la differenza fra gruppi non è dovutasemplicemente al caso
• Significatività clinica si riferisce al raggiungimento di obiettivi giudicati essenziali daclinici, ricercatori, pazienti, familiari, amici, colleghi
Differenza significativa con buon effect size di miglior efficacia di un trattamento xper l'obesità. In termini reali, la differenza di peso corrisponde a circa 1 kg.
Si può considerarlo clinicamente significativo e soggettivamente soddisfacente?
• Bias
• Effect size
• Effectiveness
• Efficacy
• Errore di tipo I (o errore )
• Errore di tipo II (o errore )
• Meta-analisi
• NnT
• Outcome research
• Process research
• RCT
• Significatività clinica
• Significatività statistica
• Variabile di mediazione
• Variabile di moderazione

9
EFFICACY EFFECTIVENESS
in circostanze ideali (RCT) nella pratica clinica (real-world)
GENERALIZZABILITA’
(sfida dell’EBM)
Validità interna
Validità ecologica
Validità ecologica
Validità interna
EFFICACIAse / quanto un intervento X produce un risultato atteso sul problema Y
Miglior indicatore: p-value Miglior indicatore: effect size
EFFICACY EFFECTIVENESS
in circostanze ideali (RCT) nella pratica clinica (real-world)
GENERALIZZABILITA’
(sfida dell’EBM)
Validità interna
Validità ecologica
Validità ecologica
Validità interna
EFFICACIAse / quanto un intervento X produce un risultato atteso sul problema Y
Validità interna
È possibile ricondurre causalmente alla variazione della variabile indipendente una determinata variazione della variabile dipendente. Validità esterna
I risultati non sono riconducibili soltanto alle specifiche circostanze in cui la ricerca è stata condotta.
Miglior indicatore: p-value Miglior indicatore: effect size
10
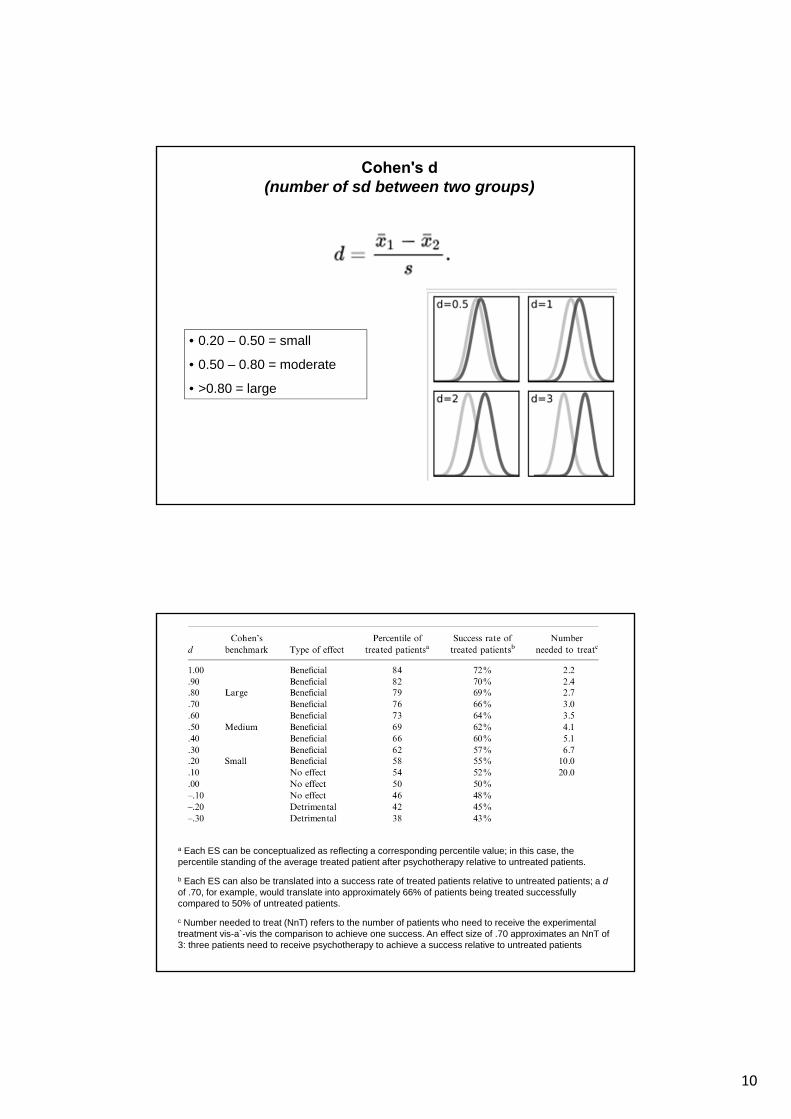
• 0.20 – 0.50 = small
• 0.50 – 0.80 = moderate
• >0.80 = large
Cohen's d(number of sd between two groups)
a Each ES can be conceptualized as reflecting a corresponding percentile value; in this case, the percentile standing of the average treated patient after psychotherapy relative to untreated patients.
b Each ES can also be translated into a success rate of treated patients relative to untreated patients; a dof .70, for example, would translate into approximately 66% of patients being treated successfully compared to 50% of untreated patients.
c Number needed to treat (NnT) refers to the number of patients who need to receive the experimental treatment vis-a`-vis the comparison to achieve one success. An effect size of .70 approximates an NnT of 3: three patients need to receive psychotherapy to achieve a success relative to untreated patients

11
Empirically Supported Treatments (EST)
Specific psychological treatments for a specific population/disorder (e.g., individuals with Panic Disorder) that have been proven effective in controlled research.
Invalidated treatments
Treatments that have been studied in RCT and found not to work
Unvalidated treatments
Treatments that have not yet or not sufficiently studied in RCT
Mechanisms of psychological treatment
The steps or processes through which therapy (or some independent variable) actually unfolds and produces the change. Mechanisms explain how the intervention translates into events that lead to the outcome(Kazdin AE. Mediators and mechanisms of change in psychotherapy. Annu Rev Clin Psychol 2007; 3: 1–27)
EBPP is not EST!
Am J Orthopsychiatry 1936; 6: 412-415
J Consult Psychol 1952; 16: 319-324
This review fails to prove that psychotherapy, Freudian or otherwise, facilitates the recovery of neurotic patients. They show that roughly two-thirds of a group of neurotic patients will recover or improve to a marked extent within about two years of the onset of their illness, whether they are treated by means of psychotherapy or not.
The theory that the specific techniques that are applied in different types and schools of psychotherapy serve a very limited purpose (such as a shared myth to believe in), and that most of the positive effect that is gained from psychotherapy is due to factors that the schools have in common, namely the therapeutic effect of having a relationship with a therapist who is warm, respectful and friendly.
12
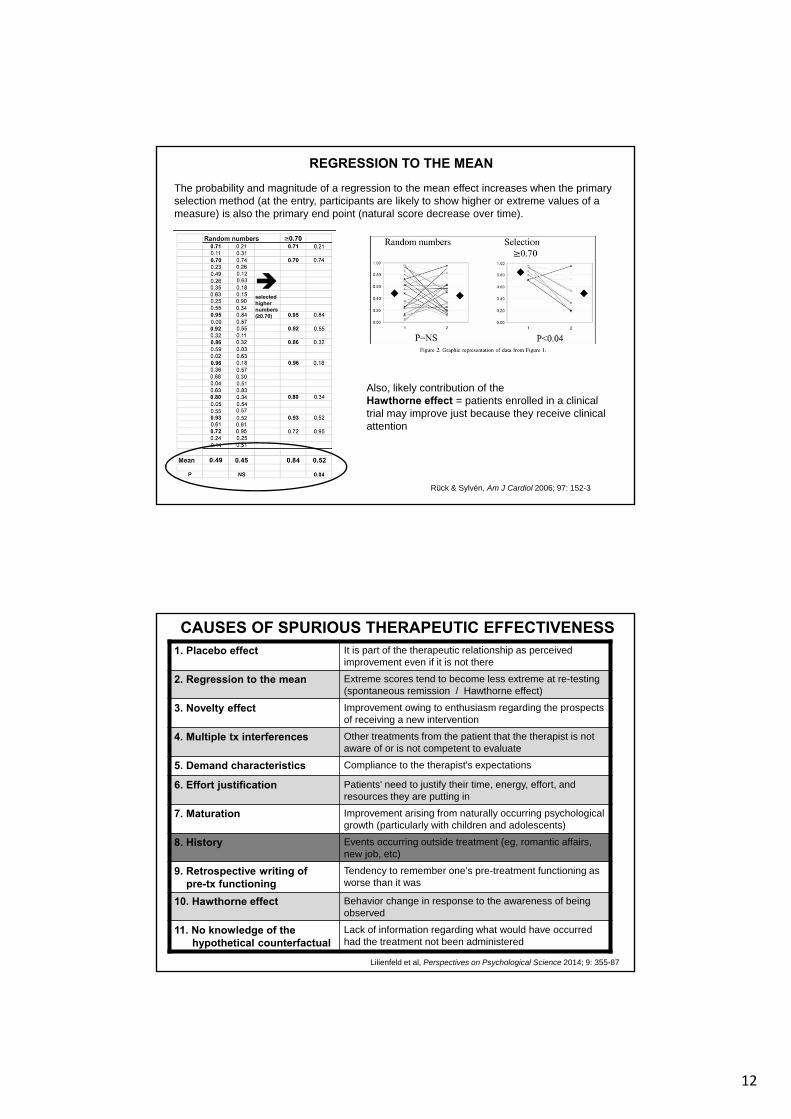
REGRESSION TO THE MEAN
Rück & Sylvén, Am J Cardiol 2006; 97: 152-3
The probability and magnitude of a regression to the mean effect increases when the primary selection method (at the entry, participants are likely to show higher or extreme values of a measure) is also the primary end point (natural score decrease over time).
selectedhighernumbers(≥0.70)
Also, likely contribution of the Hawthorne effect = patients enrolled in a clinical trial may improve just because they receive clinical attention
CAUSES OF SPURIOUS THERAPEUTIC EFFECTIVENESS
Lilienfeld et al, Perspectives on Psychological Science 2014; 9: 355-87
1. Placebo effect It is part of the therapeutic relationship as perceived improvement even if it is not there
2. Regression to the mean Extreme scores tend to become less extreme at re-testing (spontaneous remission / Hawthorne effect)
3. Novelty effect Improvement owing to enthusiasm regarding the prospects of receiving a new intervention
4. Multiple tx interferences Other treatments from the patient that the therapist is not aware of or is not competent to evaluate
5. Demand characteristics Compliance to the therapist's expectations
6. Effort justification Patients' need to justify their time, energy, effort, and resources they are putting in
7. Maturation Improvement arising from naturally occurring psychological growth (particularly with children and adolescents)
8. History Events occurring outside treatment (eg, romantic affairs, new job, etc)
9. Retrospective writing ofpre-tx functioning
Tendency to remember one’s pre-treatment functioning asworse than it was
10. Hawthorne effect Behavior change in response to the awareness of being observed
11. No knowledge of the hypothetical counterfactual
Lack of information regarding what would have occurred had the treatment not been administered

13
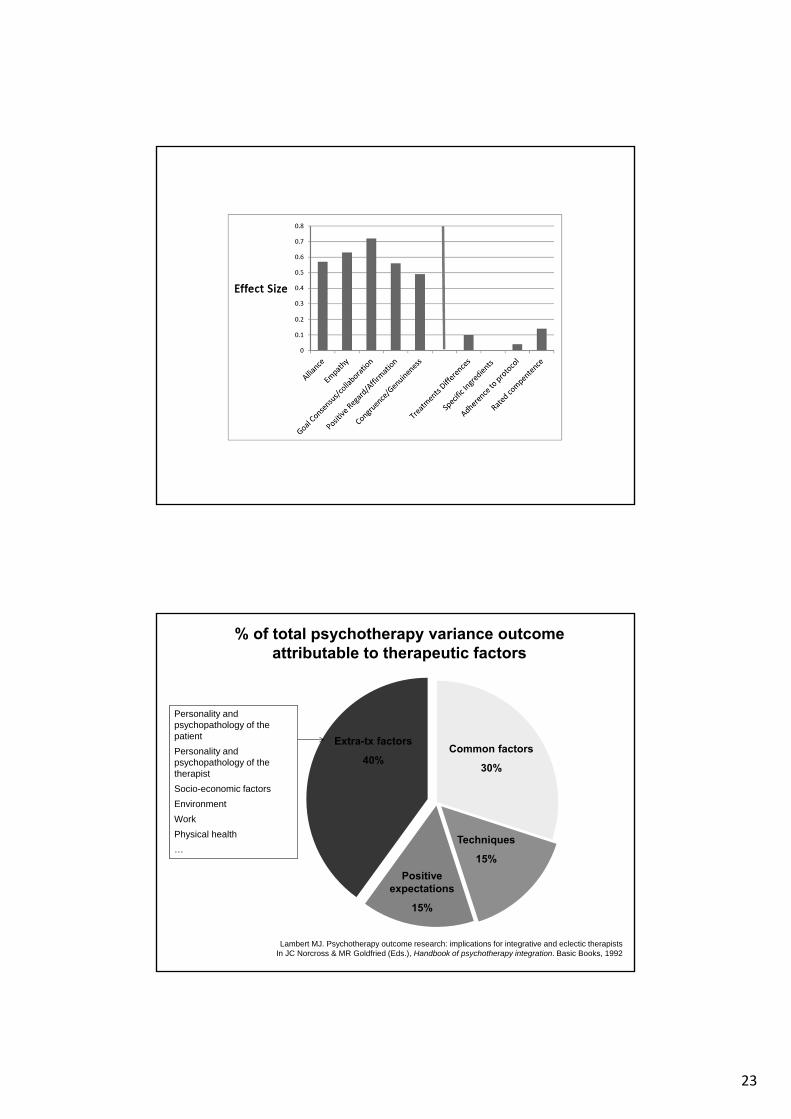
Fattori terapeutici Circa il 40% dell’esito di una psicoterapia non è spiegabile in base a fattori a noi noti e circa il 30% è dovuto ai fattori comuni: solo il 10-15% è dovuto alle tecniche specifiche impiegate.
Regressione verso la media
All’ingresso di una ricerca in psicoterapia, è altamente probabile che i pazienti presentino un livello di disagio che si traduce in punteggi estremi di una misurazione. Lo stesso strumento o set di criteri viene ovviamente usato per valutare l’efficacia della psicoterapia e tende a mostrare cambiamenti elevati e statisticamente significativi rispetto alla baseline. Se invece all’ingresso si avessero valori random di misurazione o assessment multi-metodo, le differenze post-intervento sarebbero molto meno evidenti e probabilmente non significative.
Effetto Hawthorne Le persone tendono ad alterare i propri comportamenti se sono sotto osservazione per cui i pazienti arruolati in un trial di psicoterapia possono star meglio per il semplice fatto di ricevere attenzione.
Allegiance Livello di fiducia che un ricercatore ha nei confronti della psicoterapia X: i risultati sono maggiori se gli autori di una ricerca praticano o sono convinti della validità della psicoterapia sotto indagine e sono peggiori se sono mal disposti verso quella psicoterapia.
Operazionaliz-zazione delle variabili
Analizzare l’efficacia di una psicoterapia X sulla depressione significa tradurre il costrutto di “depressione” in strumenti di assessment che valutano alcuni aspetti del costrutto, non l’intero costrutto (Beck o Hamilton?). Inoltre l’efficacia di una psicoterapia è maggiore se depressione con Hamilton e minore se con Beck.
CRITICITA' METODOLOGICHE
RCT - features RCT - criticisms
RCT = comparison of experimental group (pts receiving a treatment whose efficacy is evaluated) with controls (pts who are receiving no active treatment, eg placebo)
Placebo-like psychological treatments are not ‘neutral’ (as they are in drug trials) because they produce psychological effects (eg, allocation to placebo arm may mean being assigned to a less desirable treatment)
Strict diagnostic homogeneityDiagnostic precision is not emphasized in psychotherapy. Comorbidity is the rule.
Randomization procedure for allocationPts in psychotherapy actively choose their own treatment
Double-blind research designPts are required to actively participate and therapists know what they are administering: no one can be blinded
Standardization of treatment procedure (all pts receive the same treatment in the same way)
Psychotherapy is hard to standardize. ‘Something’ can be produced in sessions that cannot be predicted and standardized (generalization from “RCT lab” to routine clinical practice)
Fixed duration of psychotherapyVery few medium/long-term follow-up to ascertain relapse rates and use of alternative treatments
Starcevic V. Australian Psychiatry 2003; 11: 278-281
14
1. La maggior parte dei pazienti ha un problema primario o può essere trattato come se ne avesse uno solo
• I pazienti che entrano nei RCT hanno problemi simili a quelli nella pratica clinica
• Difficilmente un pz richiede tx per un unico disturbo DSM (ho una depressione maggiore ma per il resto va tutto bene nella mia vita)
• La maggior parte dei pz hanno comorbilità di Asse I – II (tassi di 50% fino al 90%)
• La maggior parte dei pz hanno sintomi sotto-soglia di Asse I – II
2. I sintomi psicopatologici possono essere compresi e trattati prescin-dendo dalla personalità
• Trattamenti basati sui sintomi sono più facilmente verificabili
• Comorbilità di Asse II predittore di insuccesso
• Tratti di personalità (es nevroticismo, disregolazione affettiva) sono predisponenti a tutta la psicopatologia non-psicotica
• Tutti i pz con la stessa diagnosi Asse I beneficiano dello stesso trattamento (es. depressione secondaria a licenziamento = a orientamento sex conflittuale?) (assunto non testato)
Westen et al, Psychol Bull 2004; 130: 631-663
I peccati capitali degli EST
3. I RCT sono il gold standard per valutare l’efficacia della psicoterapia
• Condizioni artificiali di manualizzazione, durata, controlli, allocazione nei bracci, livello di esperienza dei terapeuti
• Manualizzazione (quasi) impossibile con la comorbilità e nella pratica clinica
• Durata media RCT 4-20 sedute mentre studi naturalistici indicano che i trattamenti lunghi almeno 1 anno sono più efficaci nella comunità
• Controlli irrealistici (liste d’attesa, TAU)
• Randomizzazione prescinde dalla motivazione (rigidi criteri inclusione-esclusione rigidi)
• Terapeuti esperti vs terapeuti in formazione
4. Gli outcome terapeutici sono verificati con strumenti semplici
• Nella clinica, gli indicatori non sono gli effect sizes ma altri:
• Percentuale di drop-outs
• Proporzione di miglioramento sintomi
• Presenza di sintomi residuali post-trattamento
• Percentuale di pazienti non ri-trattati successivamente
I peccati capitali degli ESTWesten et al, Psychol Bull 2004; 130: 631-663

15
The informed and intentional application of clinical methods and interpersonal stances derived from established psychological principles for the purpose of assisting people to modify their behaviors, cognitions, emotions, and/or other personal characteristics in directions that the participants deem desirable Norcross, J.C. (1990). An eclectic definition of psychotherapy. In J.K. Zeig & W.M. Munion (Eds.), What is psychotherapy? Contemporary perspectives (218-220). San Francisco, CA: Jossey-Bass
WHAT IS PSYCHOTHERAPY ?
A primarily interpersonal treatment that is
(a) based on psychological principles;
(b) involves a trained therapist and a client who is seeking help for a mentaldisorder, problem or complaint;
(c) is intended by the therapist to be remedial for the client disorder, problem or complaint;
(d) is adapted or individualized for the particular client and his/her disorder, problem or complaint.
Wamplod B.E. & Imel Z.E. (2015). The great psychotherapy debate. The evidence for what makes psychotherapy work (p.37). Routledge
LE COMPETENZE PROFESSIONALI DELLO PSICOTERAPEUTA
• Conoscenza dei modelli teorici e delle tecniche di intervento
• Capacità di effettuare assessment psicologico-clinico
• Capacità di gestire gli aspetti relazionali della situazione di terapia (alleanza terapeutica e rotture dell’alleanza terapeutica)
• Caratteristiche personali di saper ascoltare, lasciare spazio all’interlocutore, saper leggere il comportamento non-verbale
• Accountability: conoscenza dello stato dell'arte sulla psicoterapia, assumersi la responsabilità del trattamento, render conto dei motivi del successo o dell'insuccesso terapeutico
Maffei et al, Giornale Italiano di Psicologia 2013; 40(3): 459-75
16
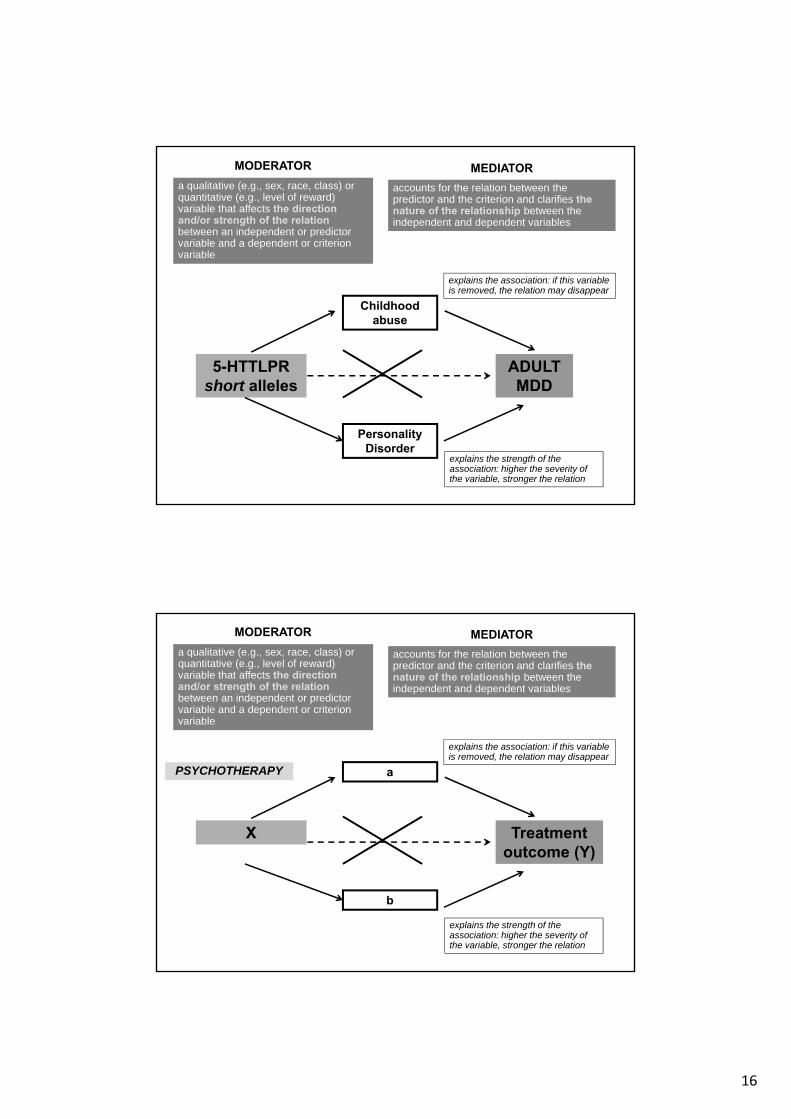
MODERATOR
a qualitative (e.g., sex, race, class) or quantitative (e.g., level of reward) variable that affects the direction and/or strength of the relationbetween an independent or predictor variable and a dependent or criterion variable
MEDIATOR
accounts for the relation between the predictor and the criterion and clarifies the nature of the relationship between the independent and dependent variables
5-HTTLPR short alleles
ADULT MDD
Childhood abuse
explains the association: if this variable is removed, the relation may disappear
Personality Disorder
explains the strength of the association: higher the severity of the variable, stronger the relation
MODERATOR
a qualitative (e.g., sex, race, class) or quantitative (e.g., level of reward) variable that affects the direction and/or strength of the relationbetween an independent or predictor variable and a dependent or criterion variable
MEDIATOR
accounts for the relation between the predictor and the criterion and clarifies the nature of the relationship between the independent and dependent variables
X Treatment outcome (Y)
a
explains the association: if this variable is removed, the relation may disappear
b
explains the strength of the association: higher the severity of the variable, stronger the relation
PSYCHOTHERAPY
17
1. The patient comes to psychotherapy with reasonably intact personality integration but a high level of subjectively felt distress
2009
CHARACTERISTICS THAT ARE GENERALLY RELATED TO OUTCOME
(1)
2. The patient is motivated to receive psychotherapy, hopes to change how he or she is feeling or behaving, and expects that the treatment will help accomplish this change
The involuntary patient, the pessimistic patient, and the skeptical patient can all benefit from psychotherapy if the therapist is sufficiently skillful to get them involved in and enthusiastic about the treatment process. However, because getting treatment under way is less difficult if therapists do not have to surmount any major obstacles to change, patients who come to therapy already motivated, hopeful, and optimistic will have better prospects for improvement on average than those who do not.
3. The patient is a likeable and appealing person
The more therapists regard their patients as appealing and worthwhile human beings, the more readily they will be able to display toward these patients the interest and respect that contribute to a helpful treatment relationship.
4. The patient is ‘‘psychologically minded’’ and able to express and reflect on his or her experience
Therapists’ understanding of a patient derives from what the person is able to communicate to them; the more fully patients can express themselves, the more information therapists have to work with
CHARACTERISTICS THAT ARE GENERALLY RELATED TO OUTCOME
(2)

18
- Other things being equal, people who have previously demonstrated competence in life situations tend to have relatively good prospects for benefiting from psychotherapy
2009
CHARACTERISTICS OCCASIONALLY RELATED TO OUTCOME
- People with average or better intelligence and intellectual skills tend to derive more benefit from psychotherapy than those who are less intelligent
- Ethnic and racial background of a patient may affect the course of therapy
There is nothing about a person’s race or ethnicity that, taken by itself, would make that person more or less amenable to psychotherapy. Some findings do suggest, however, that certain patients may have difficulty getting involved in and benefiting from psychotherapy provided by a therapist from a markedly different cultural background
CHARACTERISTICS GENERALLY UNRELATED TO OUTCOME
Age (younger better than older?) – Sex (same-sex therapist?) – Marital status (married better
than single/divorced/widowed? ) – Socioeconomic status (middle-upper class better than lower class?)
• The general or average effects of psychotherapy are widely accepted to be significant, large and quite constant across most diagnostic conditions, with variations being more influenced by general severity than by particular diagnoses (ie, variations in outcome are more heavily influenced by patient characteristics as, for example, chronicity, complexity, social support, and intensity) and by clinician and context factors than by particular diagnoses or specific treatment “brands”
• The results of psychotherapy tend to last longer and be less likely to require additional treatment courses than psychopharmacological treatments
• Comparisons of different forms of psychotherapy most often result in relatively non-significant difference, and contextual and relationship factors often mediate or moderate outcomes

19
• The effects produced by psychotherapy exceed or are comparable to the size of effects produced by many pharmacological treatments and procedures for the same condition, and some of the medical treatments and procedures have many adverse side effects and are relatively expensive vis-à-vis the cost of psychotherapy
• Courses of psychotherapy reduce overall medical utilization and expense: the overall medical costs reduced by 17% compared with a 12.3% increase in medical costs for those with no treatment for their mental disorder
• Psychotherapy is cost-effective, reduces disability, morbidity, and mortality, improves work functioning, decreases use of psychiatric hospitalization, and at times also leads to reduction in the unnecessary use of medical and surgical services including for those with serious mental illness. Psychological treatment of individuals with chronic disease in small group sessions resulted in medical care cost savings of $10 for every $1 spent
Overallefficacy of psychotherapy
• Average effect size: 0.75 – 0.85 (high)
• 14% of variance is explained by treatment-specific factors while 86% by factors related to patient, therapist and relation, or variance-related factors
• Of the 14% of variance explained by treatment-specific factors:
– 36-57% (5-8% of the total variance) explained by the characteristics of the therapist (1% due to the duration and kind of training of the therapist)
– 36-53% (5-7.5% of the total variance) explained by the therapeutic alliance, with high ES (d = 0.54)
• Differences of treatments = 1% (d = 0.20)
20
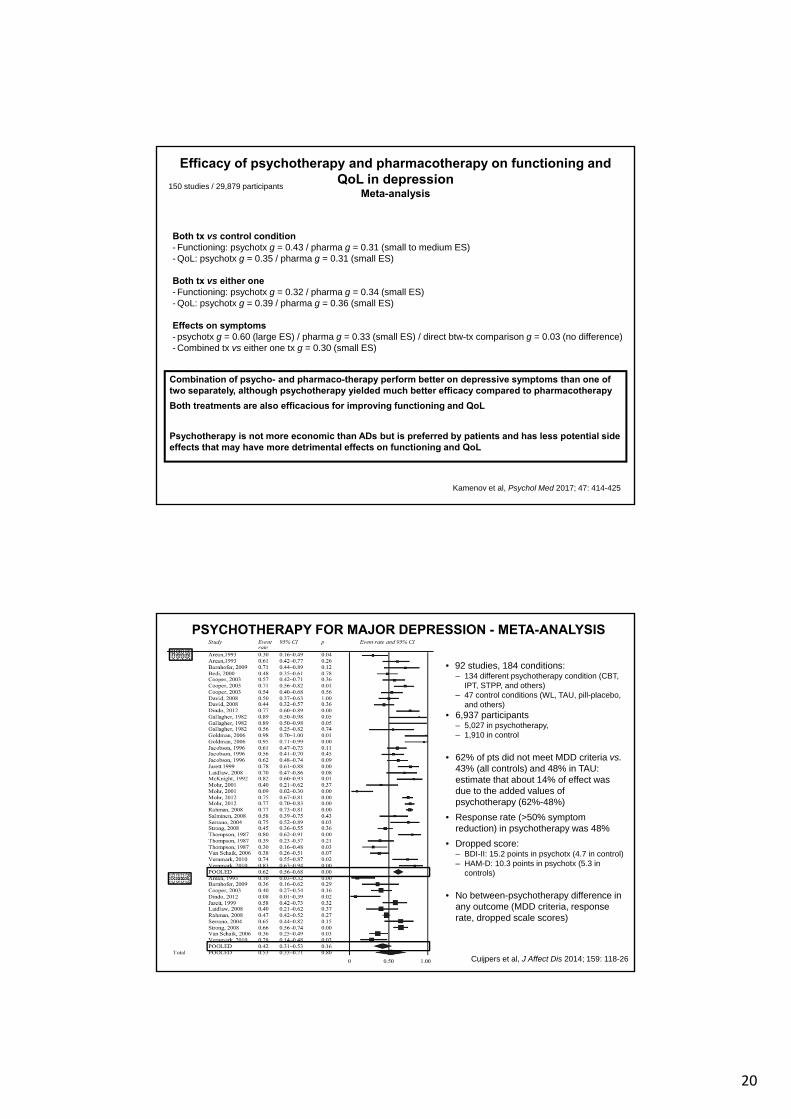
Efficacy of psychotherapy and pharmacotherapy on functioning and QoL in depression
Meta-analysis150 studies / 29,879 participants
Kamenov et al, Psychol Med 2017; 47: 414-425
Both tx vs control condition- Functioning: psychotx g = 0.43 / pharma g = 0.31 (small to medium ES)- QoL: psychotx g = 0.35 / pharma g = 0.31 (small ES)
Both tx vs either one- Functioning: psychotx g = 0.32 / pharma g = 0.34 (small ES)- QoL: psychotx g = 0.39 / pharma g = 0.36 (small ES)
Effects on symptoms- psychotx g = 0.60 (large ES) / pharma g = 0.33 (small ES) / direct btw-tx comparison g = 0.03 (no difference)- Combined tx vs either one tx g = 0.30 (small ES)
Combination of psycho- and pharmaco-therapy perform better on depressive symptoms than one of two separately, although psychotherapy yielded much better efficacy compared to pharmacotherapy
Both treatments are also efficacious for improving functioning and QoL
Psychotherapy is not more economic than ADs but is preferred by patients and has less potential side effects that may have more detrimental effects on functioning and QoL
PSYCHOTHERAPY FOR MAJOR DEPRESSION - META-ANALYSIS
Cuijpers et al, J Affect Dis 2014; 159: 118-26
• 92 studies, 184 conditions:– 134 different psychotherapy condition (CBT,
IPT, STPP, and others)– 47 control conditions (WL, TAU, pill-placebo,
and others)• 6,937 participants
– 5,027 in psychotherapy,– 1,910 in control
• 62% of pts did not meet MDD criteria vs. 43% (all controls) and 48% in TAU: estimate that about 14% of effect was due to the added values of psychotherapy (62%-48%)
• Response rate (>50% symptom reduction) in psychotherapy was 48%
• Dropped score:– BDI-II: 15.2 points in psychotx (4.7 in control)– HAM-D: 10.3 points in psychotx (5.3 in
controls)
• No between-psychotherapy difference in any outcome (MDD criteria, response rate, dropped scale scores)

21
Psychotherapy: Preventing relapse in MDD pts after recovery from depressionMeta-analysis
Clarke et al, Clin Psychol Rev 2015; 39: 58-70
People recovered from depressive episode have a 60% risk of relapse, regardless of remission spontaneously or after ADRemission symptom reduction below the
diagnostic threshold for depressionRecovery >6 mo. remissionRelapse depressive episode after remissionRecurrencedepressive episode after recovery
22 RCTs
Psychotherapy may reduce the risk of relapse within the following year by 22% that is maintained in the second year
NnT=8.3 in the low baseline risk populationNnT=4.8 in the high baseline risk population
These figures are similar to that previously reported for continuing medication, but without the need for continued treatment throughout the follow-up period.
Long-term outcomeMeta-analysis
Karolien et al, J Affect Disord 2015; 174: 400-10
• 25 studies (2,055 pts) and 30 contrasts (RCT w/ multiple contrasts): adults, recurrent MDD, in remission, randomization, controls as TAU or ADM
• CBT (13 contrasts), IPT (6 contrasts), MB-CT (7 contrasts). No PST/PDT study met inclusion criteria.
1. Psychological interventions were considerably more effective than TAU in preventing relapse or recurrences over 2 yrs (RR = 0.64 or 36% of risk reduction in favor of psychotx compared to TAU, p<0.001; NnT = 5)
2. Psychological interventions were more effective in reducing the risk of a relapse or recurrence compared to ADM (RR = 0.83 or 17% of risk reduction of psychotxcompared to ADM, p=0.02; NnT = 13)
3. The ES of the different psychological interventions were roughly similar
22
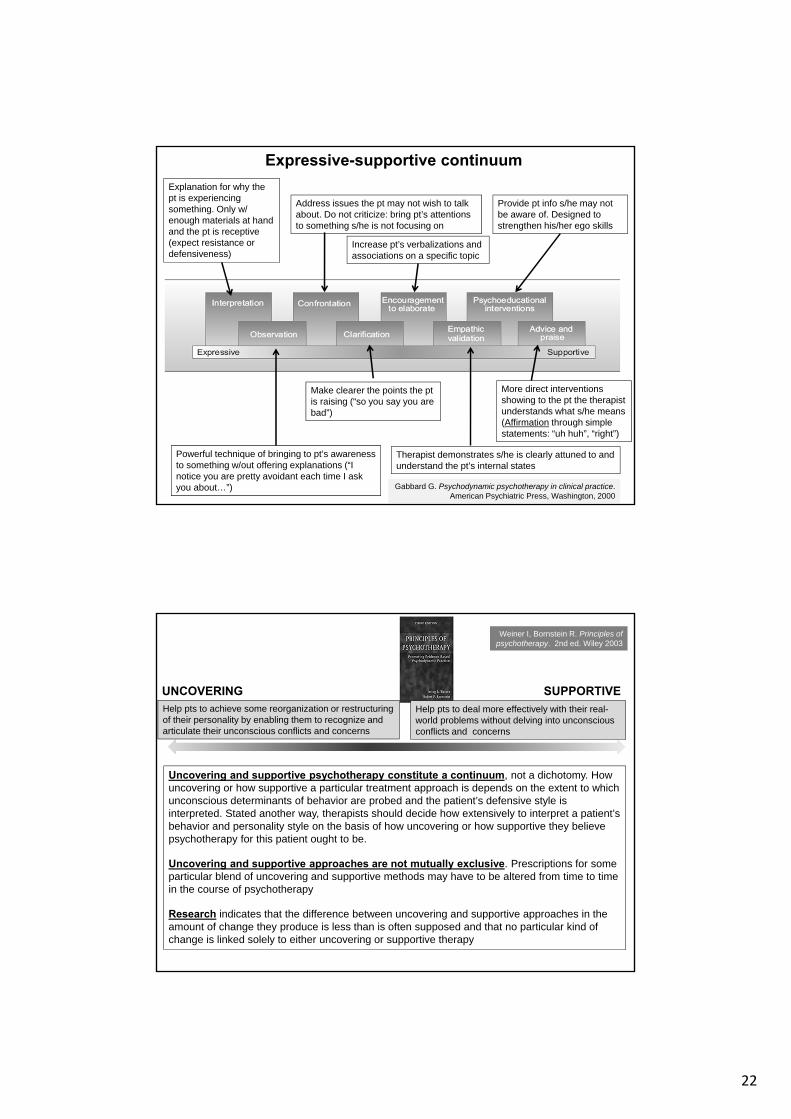
Expressive-supportive continuum
More direct interventions showing to the pt the therapist understands what s/he means (Affirmation through simple statements: “uh huh”, “right”)
Provide pt info s/he may not be aware of. Designed to strengthen his/her ego skills
Therapist demonstrates s/he is clearly attuned to and understand the pt’s internal states
Increase pt’s verbalizations and associations on a specific topic
Make clearer the points the ptis raising (“so you say you are bad”)
Address issues the pt may not wish to talk about. Do not criticize: bring pt’s attentions to something s/he is not focusing on
Powerful technique of bringing to pt’s awareness to something w/out offering explanations (“I notice you are pretty avoidant each time I ask you about…”)
Explanation for why the pt is experiencing something. Only w/ enough materials at hand and the pt is receptive (expect resistance or defensiveness)
Gabbard G. Psychodynamic psychotherapy in clinical practice. American Psychiatric Press, Washington, 2000
Help pts to achieve some reorganization or restructuring of their personality by enabling them to recognize and articulate their unconscious conflicts and concerns
UNCOVERING
Help pts to deal more effectively with their real-world problems without delving into unconscious conflicts and concerns
SUPPORTIVE
Uncovering and supportive psychotherapy constitute a continuum, not a dichotomy. How uncovering or how supportive a particular treatment approach is depends on the extent to which unconscious determinants of behavior are probed and the patient’s defensive style is interpreted. Stated another way, therapists should decide how extensively to interpret a patient’s behavior and personality style on the basis of how uncovering or how supportive they believe psychotherapy for this patient ought to be.
Uncovering and supportive approaches are not mutually exclusive. Prescriptions for some particular blend of uncovering and supportive methods may have to be altered from time to time in the course of psychotherapy
Research indicates that the difference between uncovering and supportive approaches in the amount of change they produce is less than is often supposed and that no particular kind of change is linked solely to either uncovering or supportive therapy
Weiner I, Bornstein R. Principles of psychotherapy. 2nd ed. Wiley 2003
23
Common factors
30%
Extra-tx factors
40%
Techniques
15%
Positive expectations
15%
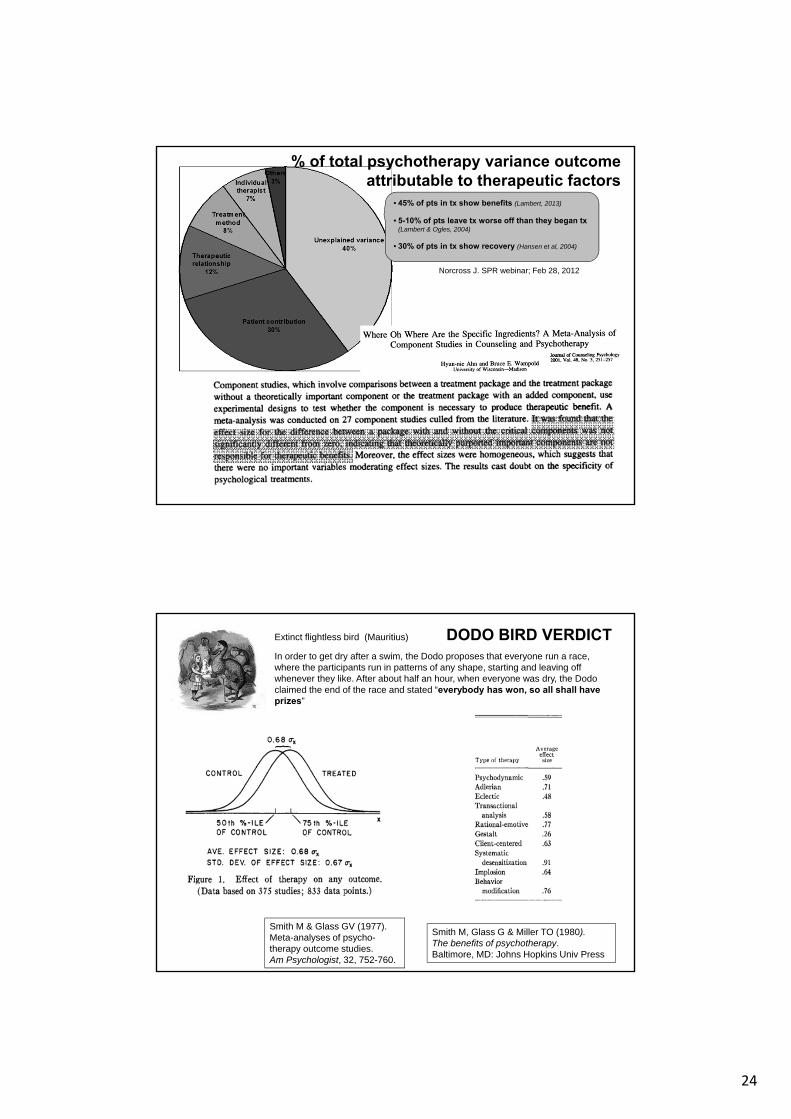
% of total psychotherapy variance outcome attributable to therapeutic factors
Lambert MJ. Psychotherapy outcome research: implications for integrative and eclectic therapists In JC Norcross & MR Goldfried (Eds.), Handbook of psychotherapy integration. Basic Books, 1992
Personality and psychopathology of the patient
Personality and psychopathology of the therapist
Socio-economic factors
Environment
Work
Physical health
…
24
Norcross J. SPR webinar; Feb 28, 2012
% of total psychotherapy variance outcome attributable to therapeutic factors
• 45% of pts in tx show benefits (Lambert, 2013)
• 5-10% of pts leave tx worse off than they began tx(Lambert & Ogles, 2004)
• 30% of pts in tx show recovery (Hansen et al, 2004)
DODO BIRD VERDICTExtinct flightless bird (Mauritius)
In order to get dry after a swim, the Dodo proposes that everyone run a race, where the participants run in patterns of any shape, starting and leaving off whenever they like. After about half an hour, when everyone was dry, the Dodo claimed the end of the race and stated “everybody has won, so all shall have prizes”
Smith M & Glass GV (1977). Meta-analyses of psycho-therapy outcome studies. Am Psychologist, 32, 752-760.
Smith M, Glass G & Miller TO (1980). The benefits of psychotherapy. Baltimore, MD: Johns Hopkins Univ Press
25
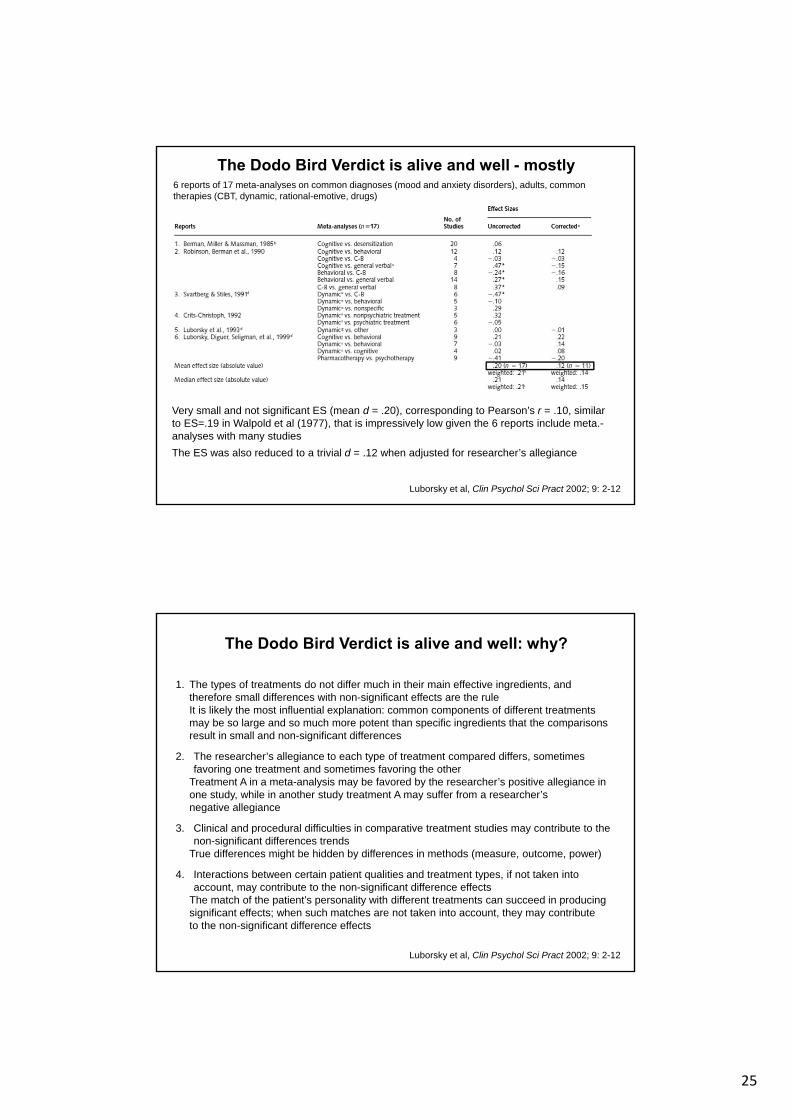
The Dodo Bird Verdict is alive and well - mostly6 reports of 17 meta-analyses on common diagnoses (mood and anxiety disorders), adults, common therapies (CBT, dynamic, rational-emotive, drugs)
Very small and not significant ES (mean d = .20), corresponding to Pearson’s r = .10, similar to ES=.19 in Walpold et al (1977), that is impressively low given the 6 reports include meta.-analyses with many studies
The ES was also reduced to a trivial d = .12 when adjusted for researcher’s allegiance
Luborsky et al, Clin Psychol Sci Pract 2002; 9: 2-12
The Dodo Bird Verdict is alive and well: why?
1. The types of treatments do not differ much in their main effective ingredients, and therefore small differences with non-significant effects are the ruleIt is likely the most influential explanation: common components of different treatments may be so large and so much more potent than specific ingredients that the comparisons result in small and non-significant differences
2. The researcher’s allegiance to each type of treatment compared differs, sometimes favoring one treatment and sometimes favoring the other
Treatment A in a meta-analysis may be favored by the researcher’s positive allegiance in one study, while in another study treatment A may suffer from a researcher’snegative allegiance
3. Clinical and procedural difficulties in comparative treatment studies may contribute to the non-significant differences trends
True differences might be hidden by differences in methods (measure, outcome, power)
4. Interactions between certain patient qualities and treatment types, if not taken into account, may contribute to the non-significant difference effects
The match of the patient’s personality with different treatments can succeed in producing significant effects; when such matches are not taken into account, they may contributeto the non-significant difference effects
Luborsky et al, Clin Psychol Sci Pract 2002; 9: 2-12
26
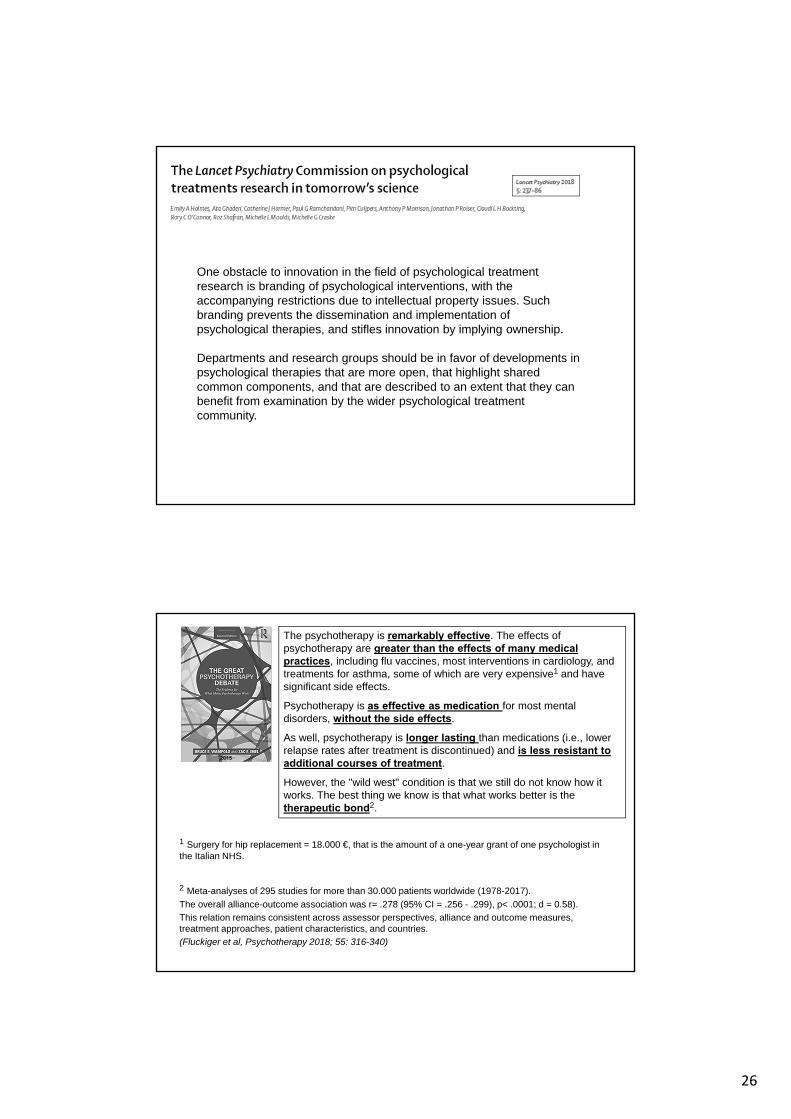
One obstacle to innovation in the field of psychological treatment research is branding of psychological interventions, with the accompanying restrictions due to intellectual property issues. Such branding prevents the dissemination and implementation of psychological therapies, and stifles innovation by implying ownership.
Departments and research groups should be in favor of developments in psychological therapies that are more open, that highlight shared common components, and that are described to an extent that they can benefit from examination by the wider psychological treatment community.
The psychotherapy is remarkably effective. The effects of psychotherapy are greater than the effects of many medical practices, including flu vaccines, most interventions in cardiology, and treatments for asthma, some of which are very expensive1 and have significant side effects.
Psychotherapy is as effective as medication for most mental disorders, without the side effects.
As well, psychotherapy is longer lasting than medications (i.e., lower relapse rates after treatment is discontinued) and is less resistant to additional courses of treatment.
However, the "wild west" condition is that we still do not know how it works. The best thing we know is that what works better is the therapeutic bond2.
2015
1 Surgery for hip replacement = 18.000 €, that is the amount of a one-year grant of one psychologist in the Italian NHS.
2 Meta-analyses of 295 studies for more than 30.000 patients worldwide (1978-2017).
The overall alliance-outcome association was r= .278 (95% CI = .256 - .299), p< .0001; d = 0.58).
This relation remains consistent across assessor perspectives, alliance and outcome measures, treatment approaches, patient characteristics, and countries.
(Fluckiger et al, Psychotherapy 2018; 55: 316-340)
27
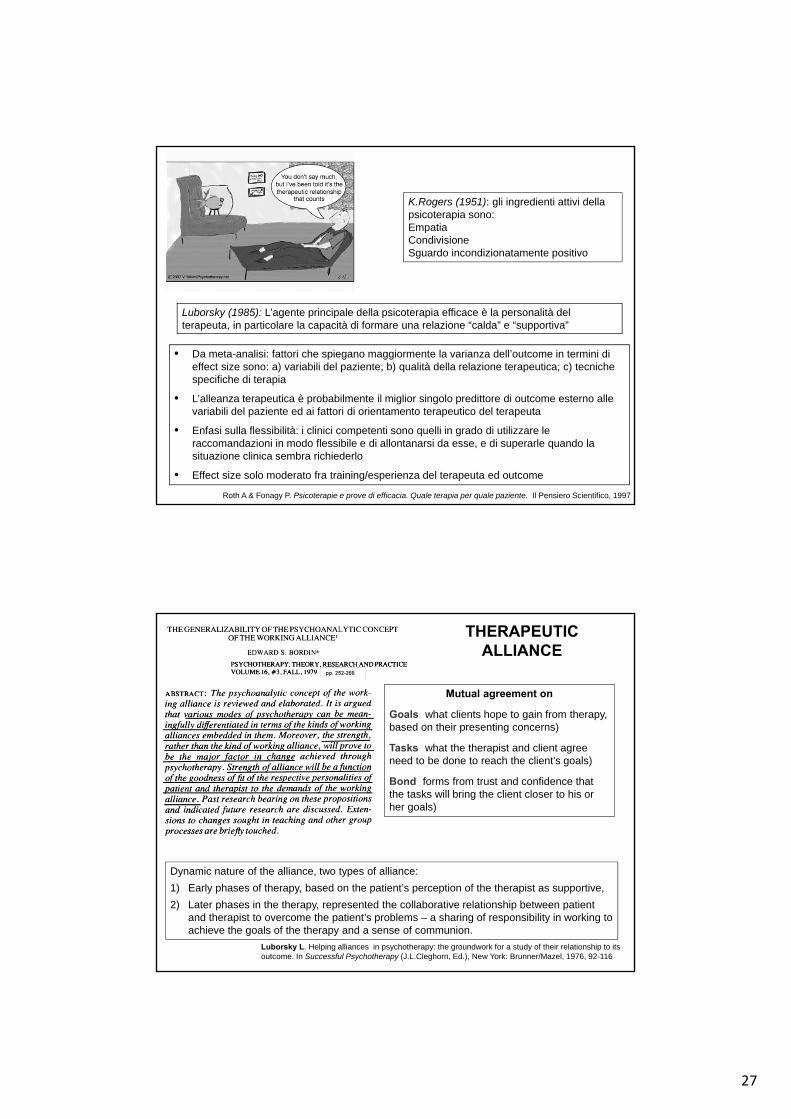
Luborsky (1985): L’agente principale della psicoterapia efficace è la personalità del terapeuta, in particolare la capacità di formare una relazione “calda” e “supportiva”
Roth A & Fonagy P. Psicoterapie e prove di efficacia. Quale terapia per quale paziente. Il Pensiero Scientifico, 1997
• Da meta-analisi: fattori che spiegano maggiormente la varianza dell’outcome in termini di effect size sono: a) variabili del paziente; b) qualità della relazione terapeutica; c) tecniche specifiche di terapia
• L’alleanza terapeutica è probabilmente il miglior singolo predittore di outcome esterno alle variabili del paziente ed ai fattori di orientamento terapeutico del terapeuta
• Enfasi sulla flessibilità: i clinici competenti sono quelli in grado di utilizzare le raccomandazioni in modo flessibile e di allontanarsi da esse, e di superarle quando la situazione clinica sembra richiederlo
• Effect size solo moderato fra training/esperienza del terapeuta ed outcome
K.Rogers (1951): gli ingredienti attivi della psicoterapia sono: EmpatiaCondivisioneSguardo incondizionatamente positivo
THERAPEUTIC ALLIANCE
Mutual agreement on
Goals (what clients hope to gain from therapy, based on their presenting concerns)
Tasks (what the therapist and client agree need to be done to reach the client's goals)
Bond (forms from trust and confidence that the tasks will bring the client closer to his or her goals)
pp. 252-260
Dynamic nature of the alliance, two types of alliance:
1) Early phases of therapy, based on the patient’s perception of the therapist as supportive,
2) Later phases in the therapy, represented the collaborative relationship between patient and therapist to overcome the patient’s problems – a sharing of responsibility in working to achieve the goals of the therapy and a sense of communion.
Luborsky L. Helping alliances in psychotherapy: the groundwork for a study of their relationship to its outcome. In Successful Psychotherapy (J.L.Cleghorn, Ed.), New York: Brunner/Mazel, 1976, 92-116

28
HISTORY OF THERAPEUTIC ALLIANCE
• Eysenck (1952)The efficacy of psychotherapy had not been demonstrated and any improvements were the result of so-called spontaneous remission (regression to the mean)
• Strupp & Hadley (1979)The outcome of a psychotherapeutic process is often influenced by so-called nonspecific factors, namely the personal characteristics of the therapist and the positive feelings that arise in the patient – feelings which can lead to the creation of a positive therapeutic climate from an emotional and interpersonal perspective
• Orlinky & Howard (1986)What is effectively therapeutic about psychotherapy?
Outcome research: analyses the results of the therapyprocess research: various aspects of the therapeutic process, which can also be measured during the course of therapy regardless of outcome
• Migone (1996)3 partially overlapping phases in the history of psychotherapy research:
1. 1950s to 1970s: research focused on the outcome of psychotherapy and there was a proliferation of meta-analysis
2. 1960s to 1980s: growing interest for research into the relationship between process and outcome (the Vanderbilt Project is the most famous example of this)
3. from the 1970s onward: interest shifted to the therapeutic process and the desire for a greater understanding of the “micro-processes” involved in therapy
• Rogers (1951)The active components in the therapeutic relationship: empathy, congruence, and unconditional positive regard
• Luborsky (1976)2 types of alliance:
1. the first, found in the early phases of therapy, is based on the patient’s perception of the therapist as supportive,
2. a second type, more typical of later phases in the therapy, represented the collaborative relationship between patient and therapist to overcome the patient’s problems – a sharing of responsibility in working to achieve the goals of the therapy and a sense of communion
• Bordin (1979)A collaborative relationship between patient and therapist in the common fight to overcome the patient’s suffering and self-destructive behavior. TA consists of three essential elements: agreement on the goals of the treatment, agreement on the tasks, and the development of a personal bond made up of reciprocal positive feelings
HISTORY OF THERAPEUTIC ALLIANCE
29
THERAPEUTIC ALLIANCE
THE V-SHAPED PATTERN
TA may be a simple effect of the temporal progression of the therapy rather than an important causal factor. On the basis of this hypothesis, we would expect a development in the alliance to be characterized by a linear growth pattern over the course of the therapy, and alliance ratings obtained in the early phases to be weaker predictors of outcome than those obtained toward the end of the therapy. However, according to the findings of numerous researchers, this is not the case
• Safran (1951)The positive outcome of therapy was more closely associated with the successful resolution of ruptures in the alliance than with a linear growth pattern as the therapy proceeds
• Hartley & Strupp (1983)Ratings obtained during the first session and then during sessions representing 25, 50, 75, and 100% of the treatment. Among successful patients, increase in the alliance rating between the first session and the session representing the 25% mark, whereas among unsuccessful patients, the alliance rating declined over the same period.
• Tracey (1989)The more successful the outcome, the more curvilinear the pattern of client and therapist session satisfaction (high–low–high) over the course of treatment. When the outcome was worse, the curvilinear pattern was weaker
• Safran & Muran (2000); Stiles et al (2004); Samstag et al (2004)The alliance ruptures represent opportunities for clients to learn about their problems relating to others, and repairs represented such opportunities having been taken in the here-and-now of the therapeutic relationship
therapist and therapeutic alliance
• Meta-analyses indicate that it is the therapist’s (not the patient’s) contribution to the TA that is a statistically significant predictor of outcome, even when accounting for a number of covariates as number of axis II diagnosis, research design (whether RCT or not), rater of the TA (whether the patient, the therapist or an observer) and alliance measure (different types of instruments)
• The therapist variability in the TA seems more important than the patient variability for improved patient outcomes.
• However meta-analyses cannot tell us much about how therapists contribute to the alliance because some therapists might form an effective TA with certain types of patients while other therapists with some other types of patients, that is therapists may be more responsive to some types of patients and not others, develop stronger alliances with their patients (irrespective of diagnosis) and these therapists are more likely to obtain more benefits for patients at the conclusion of treatment
• Baldwin et al (2007), J Consult Clin Psychology, 75, 842-852• Dinger et al (2008), J Clin Psychology, 64, 344-354• Zuroff et al (2010), J Clin Psychology, 66, 681-697• Del Re et al (2012), Clin Psychol Rev, 32, 642-649
30
May therapeutic alliance be a simple effect of the temporal progression of the therapy rather than an important causal factor?
On the basis of this hypothesis, we would expect a development in the alliance to be characterized by a linear growth pattern over the course of the therapy, and alliance ratings obtained in the early phases to be weaker predictors of outcome than those obtained toward the end of the therapy. However, according to the findings of numerous researchers, this is not the case.
The positive outcome of therapy was more closely associated with the successful resolution of ruptures in the alliance than with a linear growth pattern as the therapy proceeds.
An alliance rupture consists of an impairment or fluctuation in the quality of the alliance between the therapist and client. Alliance ruptures vary in intensity, duration and frequency, depending on the particular therapist-client dyad. In more extreme cases, the client may overtly indicate negative sentiments to the therapist or even terminate therapy prematurely. At the other end of the continuum are minor fluctuations in the quality of the therapeutic alliance which may be extremely difficult for the outside observer or for even the skilled therapist to detect.
Psychotherapy 1990; 27: 154-165
31
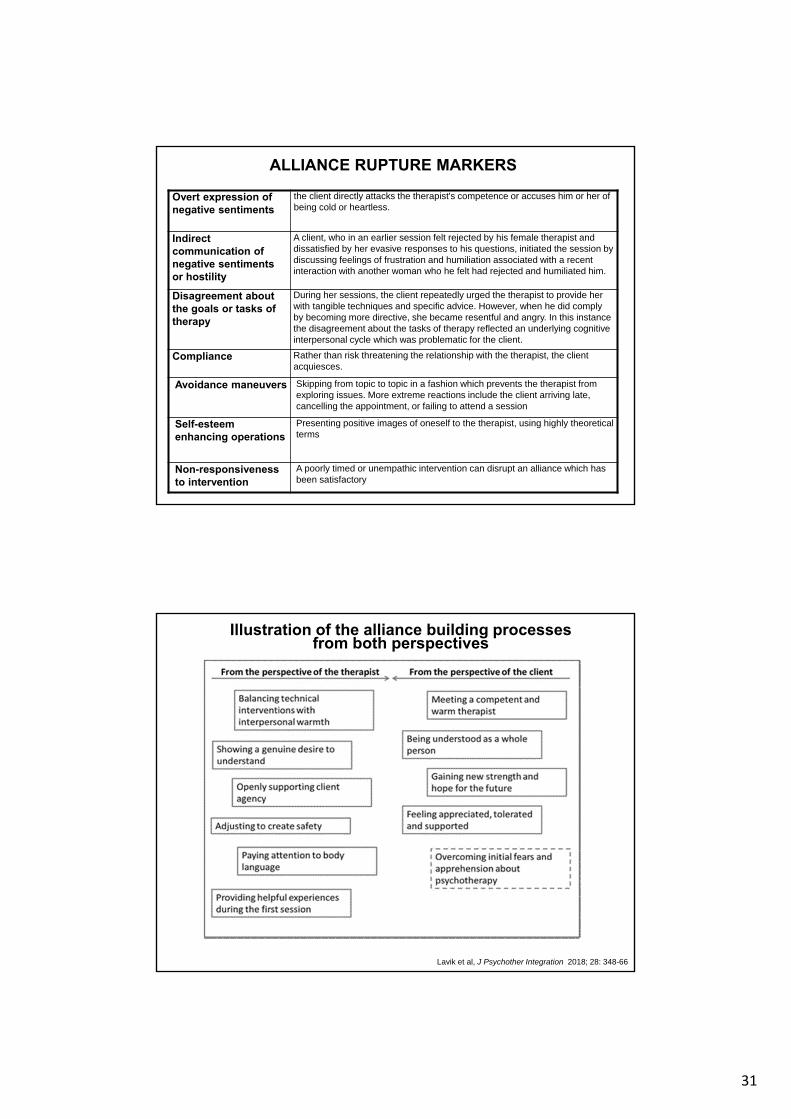
Overt expression of negative sentiments
the client directly attacks the therapist's competence or accuses him or her of being cold or heartless.
Indirect communication of negative sentimentsor hostility
A client, who in an earlier session felt rejected by his female therapist and dissatisfied by her evasive responses to his questions, initiated the session by discussing feelings of frustration and humiliation associated with a recent interaction with another woman who he felt had rejected and humiliated him.
Disagreement about the goals or tasks oftherapy
During her sessions, the client repeatedly urged the therapist to provide her with tangible techniques and specific advice. However, when he did comply by becoming more directive, she became resentful and angry. In this instance the disagreement about the tasks of therapy reflected an underlying cognitive interpersonal cycle which was problematic for the client.
Compliance Rather than risk threatening the relationship with the therapist, the client acquiesces.
Avoidance maneuvers Skipping from topic to topic in a fashion which prevents the therapist from exploring issues. More extreme reactions include the client arriving late, cancelling the appointment, or failing to attend a session
Self-esteemenhancing operations
Presenting positive images of oneself to the therapist, using highly theoretical terms
Non-responsiveness to intervention
A poorly timed or unempathic intervention can disrupt an alliance which has been satisfactory
ALLIANCE RUPTURE MARKERS
Illustration of the alliance building processes from both perspectives
Lavik et al, J Psychother Integration 2018; 28: 348-66