
I CARCINOMI NON INFILTRANTI DELLA MAMMELLA · • Caratteristiche architetturali DCIS. 38 DCIS...
84
1 TORINO 18 GIUGNO 2008 Dr.ssa Daniela Terribile Chirurgia Senologica Pol.Univ.”A.Gemelli” Roma FOCUS ON I CARCINOMI NON INFILTRANTI DELLA MAMMELLA
Transcript of I CARCINOMI NON INFILTRANTI DELLA MAMMELLA · • Caratteristiche architetturali DCIS. 38 DCIS...

1
TORINO 18 GIUGNO 2008
Dr.ssa Daniela TerribileChirurgia Senologica Pol.Univ.”A.Gemelli” Roma
FOCUS ON
I CARCINOMI NON INFILTRANTI
DELLA MAMMELLA

2
FREQUENZA DI ETA' PER IL DCIS e LCIS
0
5
10
15
20
25
0 10 20 30 40 50 60 70 80ETA'
N°CASI
DCIS
LCIS
FORME NON INVASIVE DELLA MAMMELLA
3
LCISCARCINOMA LOBULARE IN SITU
definito ora come
NEOPLASIA LOBULARE INTRAEPITELIALE (LIN)
• Riscontro occasionale
• Non necessita di alcun trattamento se diag pre-op
• Se presente sui margini non richiede ri-escissione
• Non richiede terapie complementari
• Può rappresentare criterio di inclusione in trials di chemioprevenzione
4
FORME NON INVASIVE DELLA MAMMELLA
LCISThe management of lobular carcinoma in situ (LCIS)Is the same as ductal carcinoma in situ (DCIS) ?
NO !Lakhani SR, Audretsch W, Cleton-Jensen AM, Cutuli B, Ellis I, Eusebi V,
Greco M, Houslton RS, Kuhl CK, Kurtz J, Palacios J, Peterse H, Rochard F, Rutgers E; (Eusoma Group) E.J. of Cancer 2001
5
EPOCA PRE SCREENING
~5% di tutti i carcinomioperabili
ATTUALMENTE
30% Unità di Senologia Centri di riferimento per lo Scr. Mammog.
CARCINOMA DUTTALE IN SITU ( DCIS )

6
DIFFUSIONE SCREENING MAMMOGRAFICI :NEGLI ULTIMI 10 ANNI
INCREMENTO DEL 328 % DELL’INCIDENZA DEL DCIS
DEL 16% PER CARCINOMA INFILTRANTE.ERNSTER ’97 ; BORDELAU L. 2001
DCIS
7
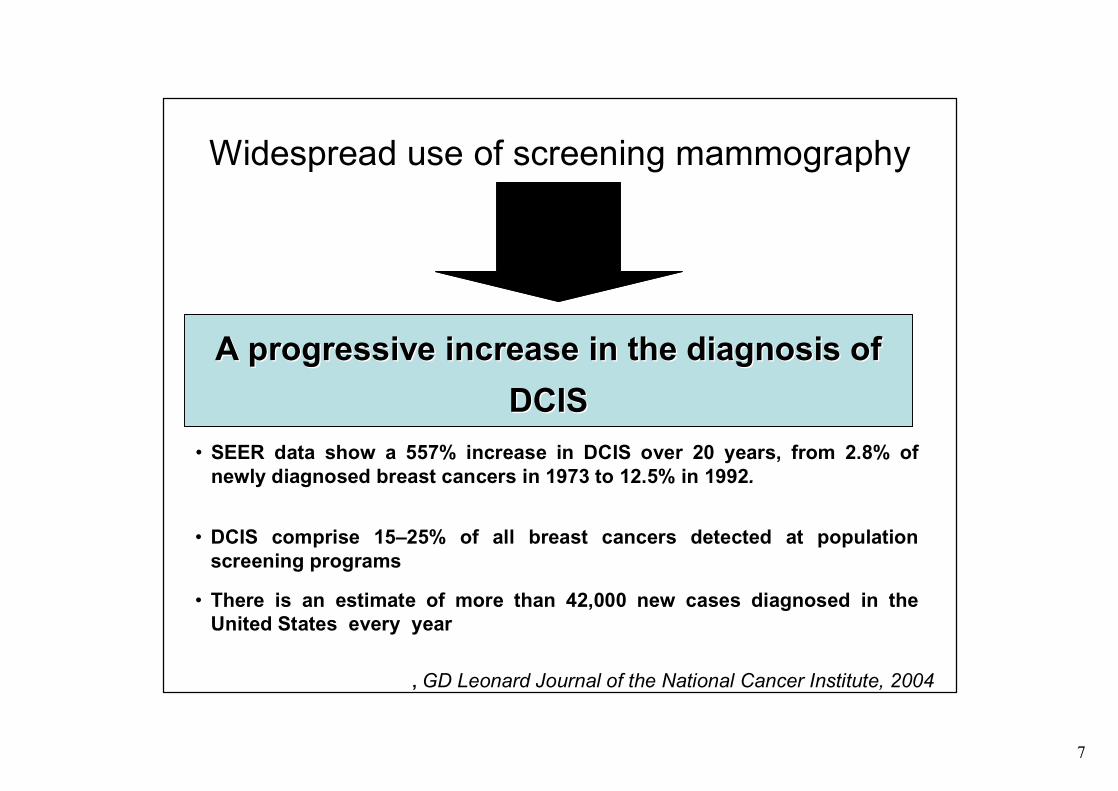
A progressive A progressive increaseincrease in the in the diagnosisdiagnosis of of DCISDCIS
Widespread use of screening mammography
, GD Leonard Journal of the National Cancer Institute, 2004
• DCIS comprise 15–25% of all breast cancers detected at population screening programs
• SEER data show a 557% increase in DCIS over 20 years, from 2.8% of newly diagnosed breast cancers in 1973 to 12.5% in 1992.
• There is an estimate of more than 42,000 new cases diagnosed in the United States every year

8
15- 30% of all breast cancer
90% non palpable
85% detected at mammographyHistology:
Comedo Type 40%Non-Comedo Type 30%Mixed 30%
Mammography:Clustered microcalcifications DCIS 45%Contralateral DCIS : 15% in 20 years
DCIS
Wang H., 2000

9
IERI
LA MAGGIOR PARTE DEI DCIS
PALPABILI , ASSOCIATI A SECREZIONE EMATICA
DCIS

10
IERIDCIS
UNICA MALATTIACON
UNICO TRATTAMENTO
MASTECTOMIA

11
OGGIINSIEME ETEROGENEO DI LESIONI
INDISPENSABILE MODULAZIONEAPPROCCIO CHIRURGICO /
TERAPEUTICO
DCIS
12
“THE DILEMMAOF THEDCIS “
SILVERSTEIN M.J. 1997
““THE SEA OF UNCERTAINITY THE SEA OF UNCERTAINITY SURROUNDING DUCTAL SURROUNDING DUCTAL CARCINOMA IN SITU CARCINOMA IN SITU ““
H.G.WelchH.G.Welch , , 20082008 2007
13
• DIFFICOLTA’CLASSIFICATIVE
• DIFFICOLTA’ DI INQUADRAMENTO BIOPATOLOGICO-CLINICO
• DIFFICOLTA’ DI CORRELAZIONE CLINICO -TERAPEUTICA
DCIS

14
• Riproducibilità della definizione istologica
• Work-up strumentale ( rx/cito /isto ) pre operatorio
• Scelta del trattamento chirurgico ( mammella e ascella )
• Definizione e Importanza dei margini negativi
Problemi apertiDCIS
15
DCIS Problemi aperti
• Ruolo della radioterapia
• Ruolo dell’ormonoterapia adiuvantechemiopreventiva
• Significato della recidiva locale

16
problemi con la letteratura corrente
• Differenze nella popolazione studiata
• Differenze nei criteri di definizione di margini negativi
• Differenze nella definizione di microinvasione
• Differenze nel trattamento• Numero limitato di pazienti
DCIS
17
DCIS
DIFFICOLTÀ’ DI RIPRODUCIBILITÀ’DELLA DEFINIZIONE
“Discrepancies in the diagnosis of intraductal proliferative lesions of the breast and its management implications: results of a multinational survey
Ghofrani et Tavassoli Virchows Arch.2006

18
DCIS“Diagnosis of in situ lesions and other pre-
invasive conditions demands skilledpathologists “
• Pre-op diagnosis• Margins work-up• Definitive diagnosis ( microinv.issue/biological
subgroups ) Wang H, 2000

19
Estensione DCIS……It is important to realize that because of the pathologic characteristics of DCIS, it isfrequently difficult to determine the exactsize of the DCIS, and many pathologistsare reluctant to do so.
Some studies report DCIS size in millimeters, others in the number of slideswith DCIS, and still others by using itsmammographic size, all of these makecomparisons between studies difficult. …….
M.Morrow , 2007

20
DCIS: DCIS: 7575--80% 80% rilievo rilievo esclusivamente mammograficoesclusivamente mammografico
difficile determinazione difficile determinazione intraoperatoriaintraoperatoriadelldell’’adeguatezza delladeguatezza dell’’exeresiexeresi
ESTENSIONE DCIS

21
MAMMOGRAFICAL DCIS SIZE FREQUENTLY DO NOT CORRELATE WITH THE HISTOLOGICAL DCIS SIZE

22
THE OCCULT DIFFUSES SPREAD OF DCIS CELLS INTO THE DUCTAL TREE MAKES DIFFICULT ITS RADICAL EXCISION

23
WORK UP PREOPERATORIO PER LA DETERMINAZIONE DELL’ESTENSIONE DELLA
LESIONE
Determination of the presenceand extent of pure ductalcarcinoma in situ bymammography and magneticresonance imaging.Menell JK Breast J.2005 ]
MRI of the breast for the detection and assessment of the size of ductal carcinoma in situ. [ Kim Do Y Korean J Radiol. 2007]
24
MULTICENTRIC OR MULTIFOCAL ?
• By applying a correlated radiologic-pathologic technique in combination witha subgross sectioning and extensivesampling, Holland demonstrated that the tumor foci are more likely to be distributedwithin a given region (breast quadrant).
HollandHolland,Sem ,Sem D.Pat.D.Pat.,1994,1994
DCIS
25
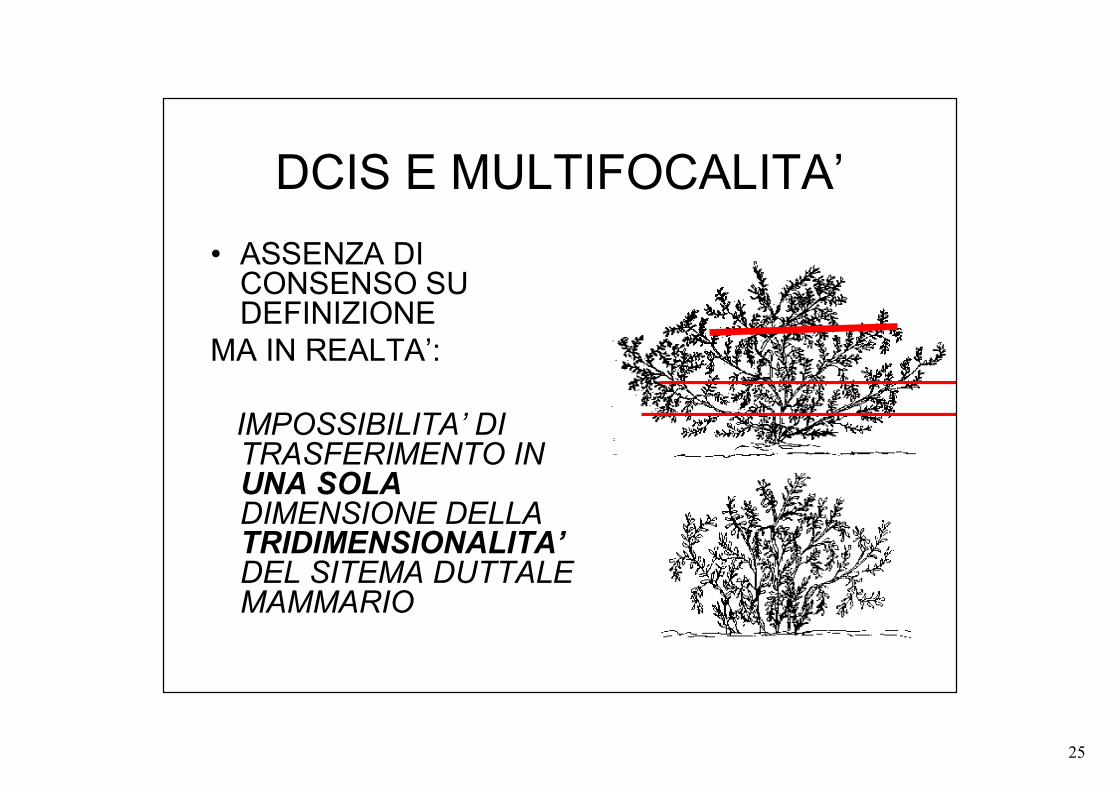
DCIS E MULTIFOCALITA’• ASSENZA DI
CONSENSO SU DEFINIZIONE
MA IN REALTA’:
IMPOSSIBILITA’ DI TRASFERIMENTO IN UNA SOLA DIMENSIONE DELLA TRIDIMENSIONALITA’DEL SITEMA DUTTALE MAMMARIO
26
DCIS Work up pre-operatorio per la
determinazione di natura della lesione
• Fine needle biopsy : inadeguata per definizione invasività
• Core biopsy / Bio vuoto-assistita : buona definizione invasività ( minore per microinvasività )

27
ESAME ISTOLOGICO ESAME ISTOLOGICO ESTEMPORANEO ESTEMPORANEO
SEMPRESEMPREINADEGUATOINADEGUATO
ESAME ISTOLOGICO ESAME ISTOLOGICO DEFINITIVODEFINITIVO
28
DCIS
Work up pre-operatorio per la determinazione di natura della lesione
La % di diagnosi preoperatorie di lesioni non palpabili è correlata alla % di exeresi adeguate e con margini indenni ad un unico intervento
Foncam 2005/Gisma 2006

29
DCIS
Work up pre-operatorio per la determinazione di natura della lesione
tuttavia :
…...Despite recent technological advances (including Stereotactic-guided directional vacuum-assisted biopsy), mammographicallyguided- wire biopsy remains the "gold-standard" for obtaining a histological diagnosis in patients with non-palpable, mammographically detected DCIS …..
Sakorafas GH, Surg Oncol. 2003
30
TRATTAMENTOTRATTAMENTO
Il Il GOLD STANDARD èè rappresentato rappresentato dalla conservazione del seno con dalla conservazione del seno con cosmesi ottimale e minimo rischio di cosmesi ottimale e minimo rischio di recidiva o di carcinoma invasivo recidiva o di carcinoma invasivo
DCIS
31
ConservativeConservativeSurgerySurgery
Conservative Conservative SurgerySurgery
+ RT+ RT
1515--40%40% 5-20%RecurrenceRecurrence ratesrates
HalfHalf of the of the recurrencesrecurrences are invasive !!!!!are invasive !!!!!
DCIS

32
DCIS
…. We are unable to predict which DCIS will progress to invasive cancer, and weare unable to predict the time interval tothe development of recurrent DCIS or invasive carcinoma…..
M.Morrow 2007

33
CHIRURGIACONSERVATIVA
Trattamento più semplicema
più alto rischio recidivalocale infiltrante
CHIRURGIA CONS + RT
• Se recidiva infiltrantepreclusione di iter
conservativa iterativa
• Se recidiva estesa preclude buon risultatoricostruzione-protesi
DCIS
34
MASTECTOMIA
-Netta riduzione rischio di recidiva
Ma
- Netto peggioramento dellaqualità di vita.
+ TAM
Tossicita’FarmacologicaEffetti collateraliSoprattutto in premenopausa
DCIS
CCD ID ISS

35
Biological variables and prognosis of DCIS.
To guide optimal treatment histological classification is not sufficient and additional biological factors are being investigated for their ability to predict outcome for individualpatients with DCIS
At present, insufficient knowledge on prognostic and predictive factors in DCIS is available
Integration of translational studies into clinical trials aimed at optimising the treatment of DCIS are required to achieve this goal.
van de Vijver MJ 2005.

36
NUOVE CLASSIFICAZIONI Ductal carcinoma in situ of the breast: a new phenotype classification system and its relation to prognosis.
Warnberg F, Breast Cancer Res Treat. 2002
Basal phenotype of ductal carcinoma in situ: recognition and immunohistologic profile.
Dabbs DJ,: Mod Pathol. 2006
Ductal carcinoma in situ with basal-like phenotype: a possible precursor to invasive basal-like breast cancer.
Bryan BB, Mod Pathol. 2006

37
““CLASSIFICAZIONI TRADIZIONALICLASSIFICAZIONI TRADIZIONALI””
•• Grado nucleareGrado nucleare
•• ++ NecrosiNecrosi
•• Caratteristiche architetturaliCaratteristiche architetturali
DCIS

38
DCIS
GRADO NUCLEARE
“ …Nuclear grading is probably the most important pathological factor that affects clinical outcome and correlates with distinct genetic pathways …….”
Tang P et Al Curr Opin Obstet Gynecol. 2007

39
CONFRONTO TRA PROPOSTEDI CLASSIFICAZIONI
LAGIOSLAGIOS NOTTINGHAMNOTTINGHAM EORTCEORTCmicropapillaremicropapillare
cribriformecribriformeDCIS senza DCIS senza
necrosinecrosi ben differenziatoben differenziato
cribriforme con cribriforme con anaplasiaanaplasia DCIS con necrosiDCIS con necrosi moderatamente moderatamente
differenziatodifferenziato
comedocomedocribriforme con cribriforme con
necrosinecrosicomedocomedo scarsamente scarsamente
differenziatodifferenziato
MorrowMorrow 19971997
CCD ID ISS

40
““THE VAN NUYS THE VAN NUYS PROGNOSTIC INDEX (VNPI)PROGNOSTIC INDEX (VNPI)””
Alto grado con o senza necrosi
Basso grado con necrosi
Basso grado senza necrosi
< 1 mm1 – 9 mm>10 mmMargini
> 41 mm16 – 40 mm< 15 mmT
321Punteggio
Silverstein MJ, Ductal Carcinoma in Situ of the Breast Silverstein MJ, Ductal Carcinoma in Situ of the Breast -- 19971997
ANATOMIAPATOLOGICA
CCD ID ISS
41
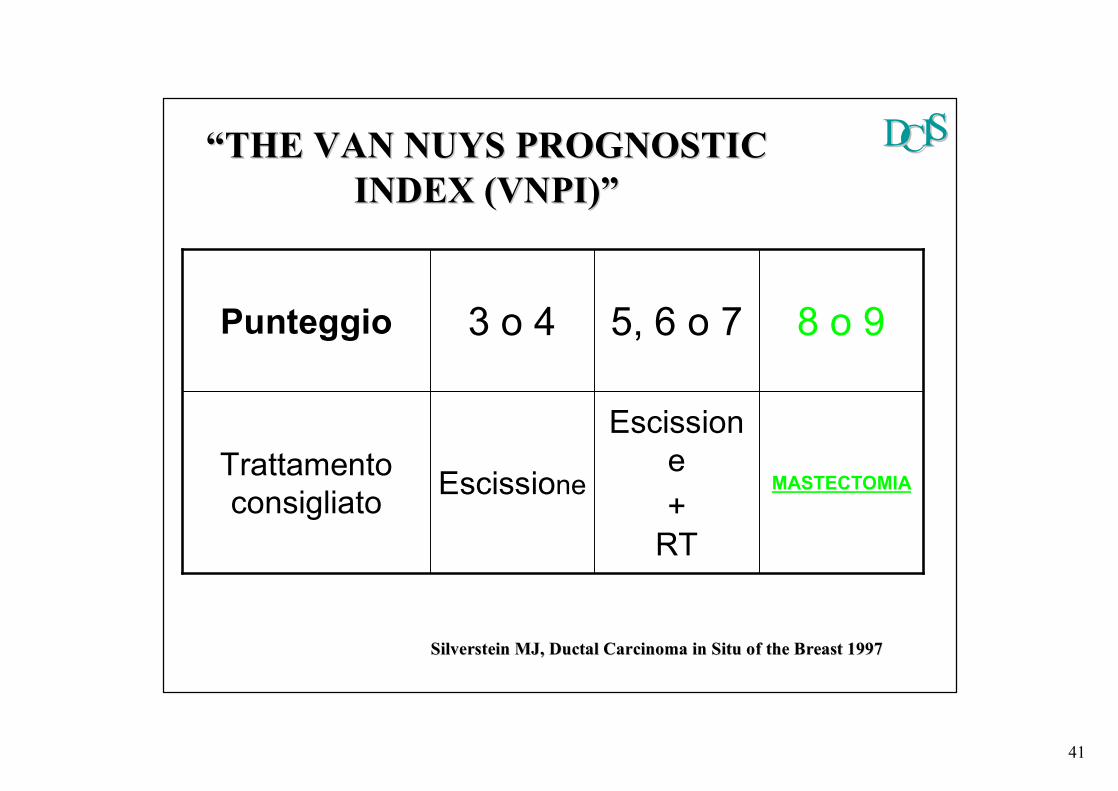
MASTECTOMIA
Escissione +
RT
EscissioneTrattamento consigliato
8 o 95, 6 o 73 o 4Punteggio
Silverstein MJ, Ductal Carcinoma in Situ of the Breast 1997Silverstein MJ, Ductal Carcinoma in Situ of the Breast 1997
““THE VAN NUYS PROGNOSTIC THE VAN NUYS PROGNOSTIC INDEX (VNPI)INDEX (VNPI)””
CCD ID ISS
42
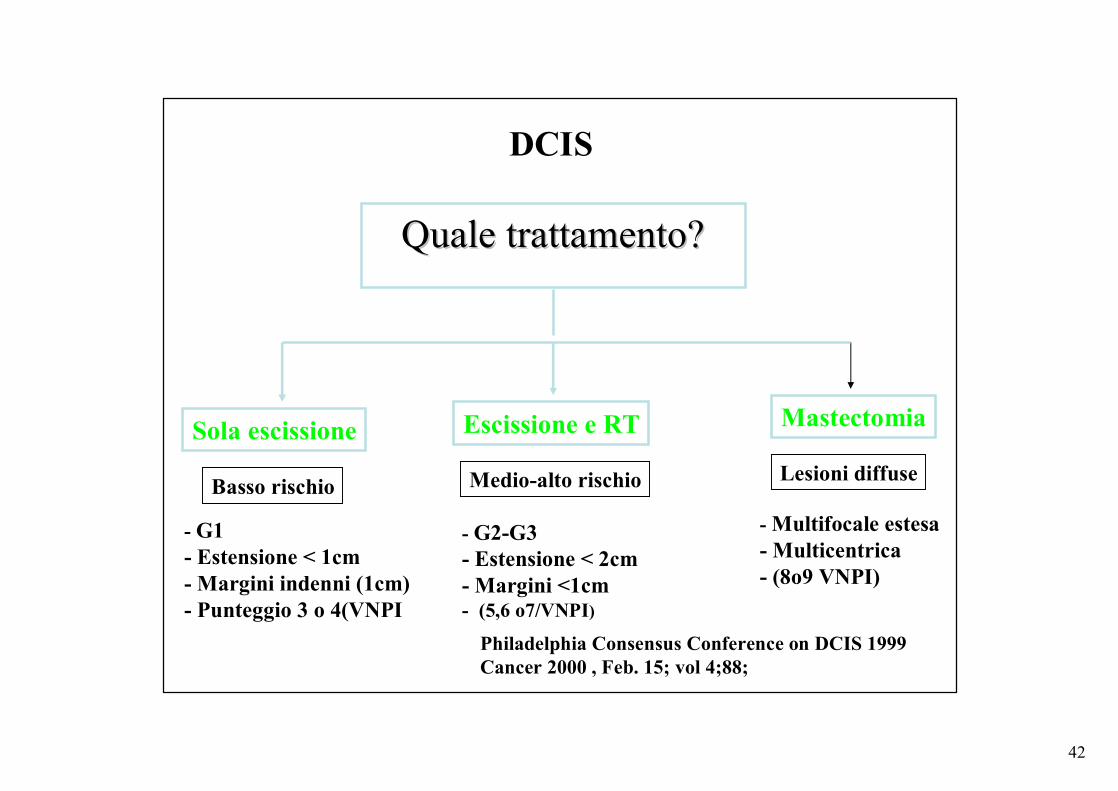
Quale trattamento?Quale trattamento?
Sola escissione Escissione e RT Mastectomia
- G1- Estensione < 1cm- Margini indenni (1cm)- Punteggio 3 o 4(VNPI
- G2-G3- Estensione < 2cm- Margini <1cm- (5,6 o7/VNPI)
Basso rischio Medio-alto rischio Lesioni diffuse
- Multifocale estesa- Multicentrica - (8o9 VNPI)
Philadelphia Consensus Conference on DCIS 1999Cancer 2000 , Feb. 15; vol 4;88;
DCIS
43
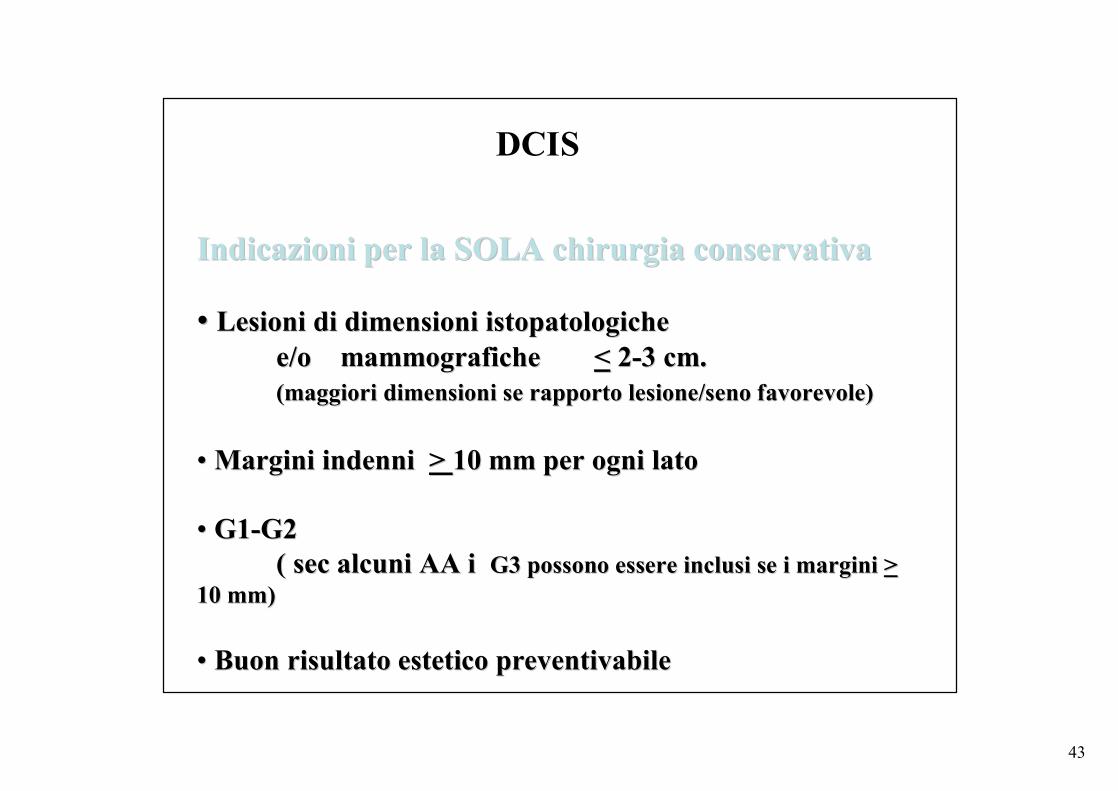
Indicazioni per la SOLA chirurgia conservativaIndicazioni per la SOLA chirurgia conservativa
•• Lesioni di dimensioni Lesioni di dimensioni istopatologicheistopatologichee/o mammografiche e/o mammografiche << 22--3 cm. 3 cm. (maggiori dimensioni se rapporto lesione/seno favorevole)(maggiori dimensioni se rapporto lesione/seno favorevole)
•• Margini indenni Margini indenni > > 10 mm per ogni lato10 mm per ogni lato
•• G1G1--G2 G2 ( sec alcuni AA i ( sec alcuni AA i G3 possono essere inclusi se i margini G3 possono essere inclusi se i margini > >
10 mm)10 mm)
•• Buon risultato estetico preventivabileBuon risultato estetico preventivabile
DCIS
44
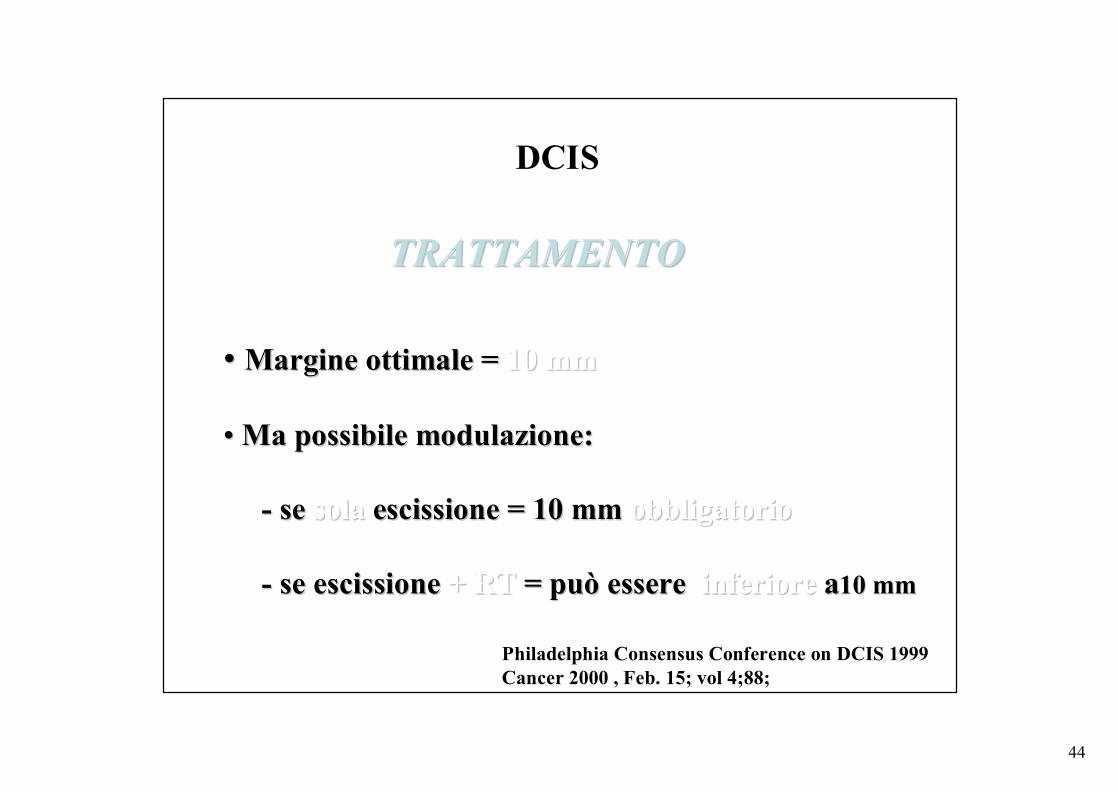
TRATTAMENTOTRATTAMENTO
•• Margine ottimale = Margine ottimale = 10 mm10 mm
•• Ma possibile modulazione:Ma possibile modulazione:
-- se se solasola escissione = 10 mm escissione = 10 mm obbligatorioobbligatorio
-- se escissione se escissione + RT + RT = può essere = può essere inferiore inferiore aa10 mm10 mm
DCIS
Philadelphia Consensus Conference on DCIS 1999Cancer 2000 , Feb. 15; vol 4;88;
45
MARGINS STATUS IN DCIS
Margin width as the sole determinant of local recurrence after breastconservation in patients with ductalcarcinoma in situ of the breast.
Macdonald HR, Silverstein MJ, …, LagiosM Am J Surg. 2006

46
DCIS E MARGINI
• ASSENZA DI CONSENSO SULLA DEFINIZIONE DI MARGINE “NEGATIVO”
• > 1 MM• > 2 MM• > 4 MM• > 10 MM
47
MARGIN STATUS IN DCISSubstantial controversy exists regarding the definition of a negative pathologic margin in DCIS. Controversy arises out of the heterogeneity of the disease, difficulties in distinguishing the spectrum of hyperplasticconditions, anatomic considerations of the location of the margin, and inadequate prospective data on prognosticfactors in DCIS.
Margins greater than 10 mm are widely accepted asnegative (but may be excessive and may lead to a lessoptimal cosmetic outcome).
Margins less than 1 mm are considered inadequate.
There are insufficient data to make definitive statementsregarding margins between 1 and 10 mm.
NCCN® Practice Guidelines in Oncology – v.2.2007

48
DIAMETRO LESIONE
ESTENSIONE AREA A
”RIDOSSO”
MULTIFOCALITA’
CCD ID ISS
49
MARGINS STATUS IN DCIS
….Re-excision to achieve clear margins was deemedappropriate if an initial attempt was unsuccessful.
How many attempts at re-excision were acceptablebefore admitting that clear margins could not beachieved was not clear.
A majority of the panelists did concur that, at least in theory, whatever might be necessary to clear the margins was acceptable, consistent with the patient's desire for breast conservation and the final aesthetic result.
CCD ID ISS
50
MARGINS STATUS IN DCIS
• Re-excision for ductal carcinoma in situ: the surgeon's least favorite operation.
Ward BA, Cancer J. 2006
• Long-term outcome for mammographicallydetected ductal carcinoma in situ managedwith breast conservation treatment: prognostic significance of reexcision.
Vapiwala N Solin LJ. Cancer J. 2006
51
DCIS
J Surg Oncol. 2007 Dec 1;96(7):569-74.
Residual disease after re-excision for tumour-positive surgical margins in both ductal carcinoma in situ and invasive carcinoma of the breast: The effect of time.
Schouten van der Velden AP, Van de Vrande SL, Boetes C, Bult P, Wobbes T.Department of Surgical Oncology, Radboud University Nijmegen Medical Centre, Nijmegen, The Netherlands.

52
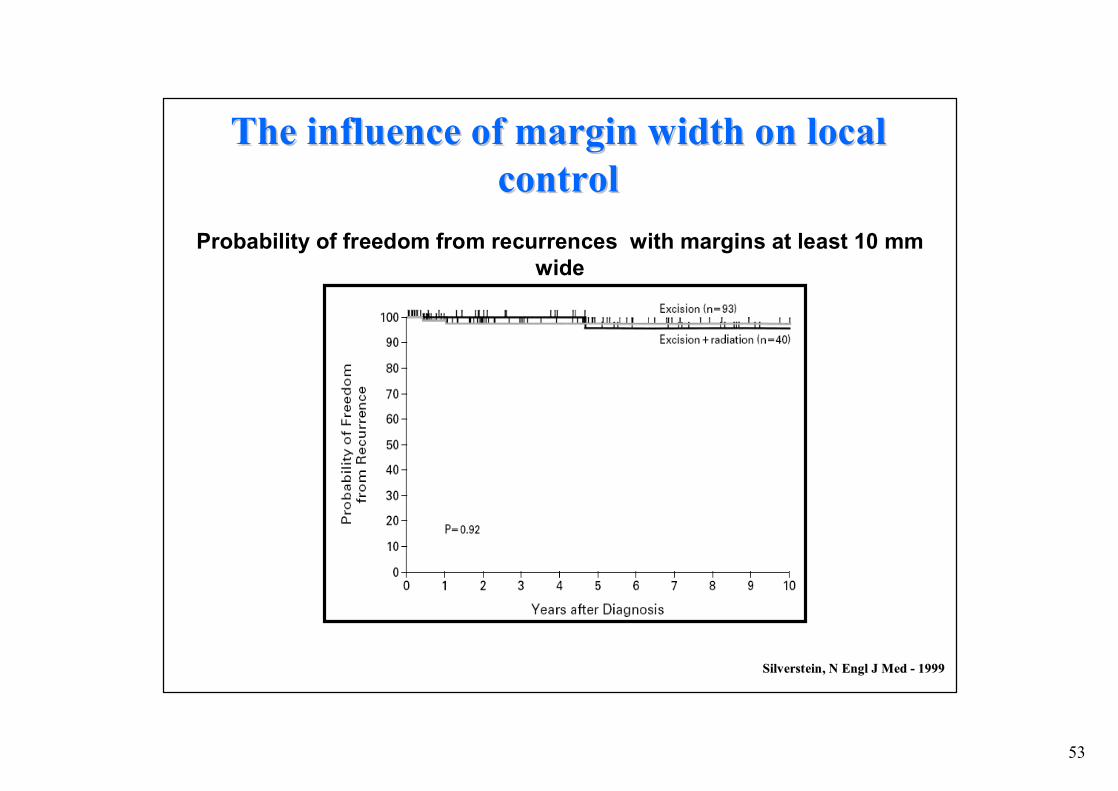
SilversteinSilverstein, N , N EnglEngl J J MedMed -- 19991999
Probability of freedom from recurrences with margins less than 1 mm wide
The The influenceinfluence of of marginmargin widthwidth on on locallocalcontrolcontrol
Probability of freedom from recurrences with margins 1 to 10 mm wide
53
SilversteinSilverstein, N , N EnglEngl J J MedMed -- 19991999
Probability of freedom from recurrences with margins at least 10 mm wide
The The influenceinfluence of of marginmargin widthwidth on on locallocalcontrolcontrol

54
yearsyears after after diagnosisdiagnosis
0
20
40
60
80
100
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
EL+RT; free marg
EL; free marg
EL+RT; involved marg
EL; involved marg
BijkerBijker N, J N, J ClinClin OncolOncol -- 20012001
EORTC trial 10853EORTC trial 10853
Time to local recurrence according to margin status and treatment
The The influenceinfluence of of marginmargin widthwidth on on locallocal controlcontrol
55
Clinical presentation and surgical quality in treatment of ductal carcinoma in situ of the breast
…..However, the cornerstone in prevention of recurrent disease is the quality of the primary surgicalprocedure. Residual tumour within the treatedbreast probably will give rise to a tumour recurrence……
Schouten A.P,et Al Acta Oncologica 2006
CCD ID ISS
56
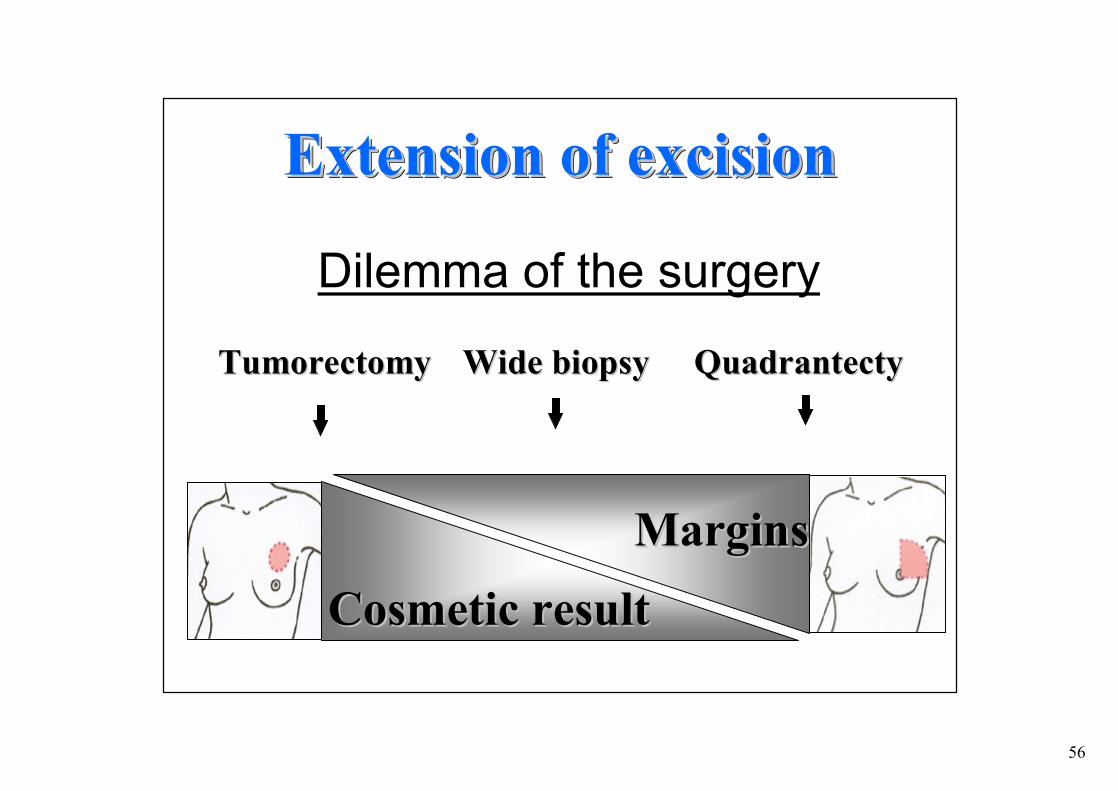
Dilemma of the surgery
TumorectomyTumorectomy
Extension of excisionExtensionExtension of of excisionexcision
Wide Wide biopsybiopsy QuadrantectyQuadrantecty
MarginsMargins
CosmeticCosmetic resultresult
57
•• Exeresi piExeresi piùù radicaliradicali
•• òò rischio di recidive localirischio di recidive locali
•• Migliori risultati esteticiMigliori risultati estetici
Chirurgia Chirurgia OncoplasticaOncoplasticaIntegrazione tra tecniche di Integrazione tra tecniche di
chirurgia oncologica e chirurgia chirurgia oncologica e chirurgia plasticaplastica
Consente di ottenere: Consente di ottenere:

58
il dcis multifocale può essere trattato conservativamente ?
DCIS “MULTIFOCALE”
NON E’ UGUALE A
DCIS “ESTESO “
59
Margin width may be more importantthan RT in avoing the risk of local
recurrence after breast-conservationsurgery
MarginMargin widthwidth maymay bebe more more importantimportantthanthan RT in RT in avoingavoing the the riskrisk of of locallocal
recurrencerecurrence after after breastbreast--conservationconservationsurgerysurgery

60
Do Do allall patientspatients treatedtreated withwith
breastbreast--conservationconservation surgerysurgery
requirerequire postexcisionalpostexcisional
radiationradiation therapytherapy ??
61
WhyWhy notnot givegive RT RT toto everyeveryconservativelyconservatively treatedtreated patientpatient withwith DCISDCIS??
•• RT RT isis expensiveexpensive and time and time consumingconsuming•• RT RT isis accompainedaccompained byby significantsignificant side side effectseffects in a in a
smallsmall percentagepercentage of of patientspatients ((cardiaccardiac and and pulmonarypulmonary))•• RadiationRadiation fibrosisfibrosis of the of the breastbreast makesmakes
mammographicmammographic followfollow--up more up more difficultdifficult•• RT RT precludesprecludes itsits useuse ifif anan invasive invasive recurrencerecurrence
developsdevelops at a at a laterlater datedate•• RT RT withwith itsits skinskin and and vascularvascular changeschanges makemake skinskin--
sparingsparing mastectomymastectomy ifif neededneeded in the future more in the future more difficultdifficult toto performperform
Silverstein, V Annual Multidisciplinary Symposium on Breast DiseSilverstein, V Annual Multidisciplinary Symposium on Breast Disease ase -- 20002000

62
DCIS and RT
Br J Cancer. 2007 Sep 17;97(6):725-9.
Radiotherapy following breast-conserving surgery for screen-detected ductalcarcinoma in situ: indications and utilisation in the UK. Interim findings from the Sloane Project.
Dodwell D,, Leeds, UK
63
DCIS and RT
Schouten van der Velden Br J Cancer. 2007
Local recurrences after different treatment strategies for ductal carcinoma in situ of the breast: a population-based
study in the East Netherlands.
CONCLUSIONS: In a defined population outside a trial setting, RT after BCS for DCIS lowered recurrence rates. Besides the use of RT, a microscopically complete excision of DCIS is essential. This is especially true for patients with symptomatically detected DCIS and with tumors that contain comedo necrosis, as these groups are at particular high risk
64
DCIS and RT
65
DCIS and RT
66
DCIS e MASTECTOMIA
QUANDO?
< 25% DEI DCIS
DCIS

67
MARGINS STATUS IN DCIS
Well-performed mastectomy and reconstruction were consideredpreferable to multiple attempts at re-excision that destroy the contour and size of the breast.

68
DCIS e MASTECTOMIA
QUANDO ?
• MULTICENTRICITA’ ESTESA
• CONTROINDICAZIONI RT ( SE G> 1 )
• RISULTATO ESTETICO SFAVOREVOLE DELLA CHIRURGIA CONSERVATIVA
• ( ESTENSIONE DCIS/ DIMENSIONI MAMMELLA)
• IMPOSSIBILITA’ DI OTTENERE MARGINI INDENNI
• VNPI: da 10 a 12Schwartz GF 2002
69
Vantaggi Vantaggi
SvantaggiSvantaggi
•• Prevenzione di recidive localiPrevenzione di recidive locali
•• Trattamento di foci occulti multicentriciTrattamento di foci occulti multicentrici
•• Trattamento di foci occulti invasiviTrattamento di foci occulti invasivi
•• ImpattoImpatto psicologicopsicologico
•• MorbiditMorbiditàà
•• Maggiori costi Maggiori costi ““ospedalieriospedalieri””
Mastectomia per DCISMastectomia per DCIS

70
DCIS e MASTECTOMIA
COME ?MASTECTOMIA SEMPLICE
+/-RICOSTRUZIONE
“SKIN SPARING MASTECTOMY”
71
DCIS e MASTECTOMIA
COME ?
LA RICOSTRUZIONE DEVE ESSERE OFFERTA AD OGNI DONNA CANDIDATA ALLA MASTECTOMIA

72
CCD ID ISSTRATTAMENTOTRATTAMENTO
Linfoadenectomia ascellareLinfoadenectomia ascellare
DCISDCIS SE DCIS PURO:SE DCIS PURO:Coinvolgimento ascellare < 1%Coinvolgimento ascellare < 1%
NON INDICATANON INDICATABiopsia del linfonodo sentinella?

73
Silverstein, J Am Coll Surg, 2001
Metastasi in linfonodi ascellari Metastasi in linfonodi ascellari in selezione di studi con DCIS and DCISMin selezione di studi con DCIS and DCISM

74
Silverstein, J Am Coll Surg, 2001
Metastasi in linfonodi sentinella in pazienti Metastasi in linfonodi sentinella in pazienti con DCIScon DCIS

75
Distribuzione dei carcinomi in situ peresecuzione del LS e grado della lesione
Basso
Basso
Medio
Medio
Alto
Alto ?
?
0% 20% 40% 60% 80% 100%
LS non eseguito
LS eseguito

76
Biopsia linfonodo sentinella in pazienti Biopsia linfonodo sentinella in pazienti con DCIScon DCIS
IndicazioniIndicazioni
• Tumori estesi
• Micro-invasione su core biopsy
• Previsione di mastectomia
Silverstein, 2000, Cox 2004.2006,Cody 2006, Giuliano 2007

77
DCIS and SN biopsy Sentinel node biopsy is not a standard procedure in ductal carcinoma in situ of the breast: the experience of the European institute of oncology on 854 patients in 10 years. Intra M, Ann Surg. 2008 Feb;
Outcomes for women with ductal carcinoma-in-situ and a positive sentinel node: a multi-institutional audit.
Moore KH, Sweeney KJ, Wilson ME, Goldberg JI, Buchanan CL, Tan LK, Liberman L, Turner RR, Lagios MD, Cody Iii HS, Giuliano AE, Silverstein
MJ, Van Zee KJ. Ann Surg Oncol. 2007

78
TRATTAMENTOTRATTAMENTORecidiva dopo Recidiva dopo sola chirurgia conservativasola chirurgia conservativa
RIRI--ESCISSIONE + RT*ESCISSIONE + RT*
Recidiva dopo Recidiva dopo chirurgia conservativa + RTchirurgia conservativa + RT
RIRI--ESCISSIONE O MASTECTOMIA* ESCISSIONE O MASTECTOMIA*
*in relazione al rapporto lesione/mammella*in relazione al rapporto lesione/mammella
CCD ID ISS

79

80
TRATTAMENTOTRATTAMENTO CCD ID ISS
RADIOLOGORADIOLOGO
CHIRURGOCHIRURGO++
PAZIENTEPAZIENTE
PATOLOGOPATOLOGO
RX RX PREPRE--OPERATORIOOPERATORIO
RX PEZZORX PEZZOOPERATORIOOPERATORIO
RX POSTRX POST--OPERATORIOOPERATORIO
ACCURATO STUDIO ACCURATO STUDIO DEL PEZZODEL PEZZO
CARATTERIZZAZIONECARATTERIZZAZIONEBIOPATOLOGICABIOPATOLOGICA
SCELTA DEL TRATTAMENTO PIÙ IDONEO
RADIOTERAPISTA
81
La complessitLa complessitàà degli aspetti biologici e degli aspetti biologici e terapeutici del terapeutici del DCIS DCIS possono possono provocare nelle pazienti un trauma provocare nelle pazienti un trauma psicologicopsicologico MAGGIORE MAGGIORE che per che per carcinomi invasivicarcinomi invasivi
DCIS
Risk perceptions and psychosocial outcomesof women with ductal carcinoma in situ: longitudinal results from a cohort study.
Partridge A, Winer E et Al J Natl Cancer Inst. 2008

82
OVERTREATMENT RISK
CAVEATCAVEATRISK/BENEFIT FOR A HIGH RATE CURABLE RISK/BENEFIT FOR A HIGH RATE CURABLE DISEASE :DISEASE :
•• Side Side effectseffects of the treatmentof the treatment•• UnsatisfactoryUnsatisfactory cosmeticscosmetics•• ImplantImplant or flap or flap complicationscomplications•• BreastBreast fibrosisfibrosis•• II II malignancesmalignances of of RtRt and and tamoxifentamoxifen
DCIS
83
DCIS
Understanding the carcinogenesis of ductalcarcinoma in situ at the molecular level may lead to an optimal individualized therapy with minimal over or undertreatment.
Tang P et Al Curr Opin Obstet Gynecol. 2007
84
Il trattamento del Il trattamento del DCIS DCIS èè costantemente costantemente sotto valutazione e revisione e può essere sotto valutazione e revisione e può essere repentinamente modificato da nuove repentinamente modificato da nuove osservazioni.osservazioni.
I provvedimenti terapeutici devono essere I provvedimenti terapeutici devono essere presi dal medico responsabile presi dal medico responsabile concon la la partecipazione della pazientepartecipazione della paziente
DCIS


















