
Gennaro CiceGennaro Cice Cattedra di Cardiologia Seconda Università di Napoli Terapia Farmacologica...
43
Gennaro Cice Cattedra di Cardiologia Seconda Università di Napoli Terapia Farmacologica della Insufficienza Cardiaca Cronica: è in arrivo una rivoluzione? 60 ° CONGRESSO NAZIONALE SIGG NAPOLI, 25 - 28 NOVEMBRE 2015
Transcript of Gennaro CiceGennaro Cice Cattedra di Cardiologia Seconda Università di Napoli Terapia Farmacologica...

Gennaro Cice
Cattedra di Cardiologia
Seconda Università di Napoli
Terapia Farmacologica della
Insufficienza Cardiaca Cronica: è
in arrivo una rivoluzione?
60° CONGRESSO NAZIONALE SIGGNAPOLI, 25-28 NOVEMBRE 2015
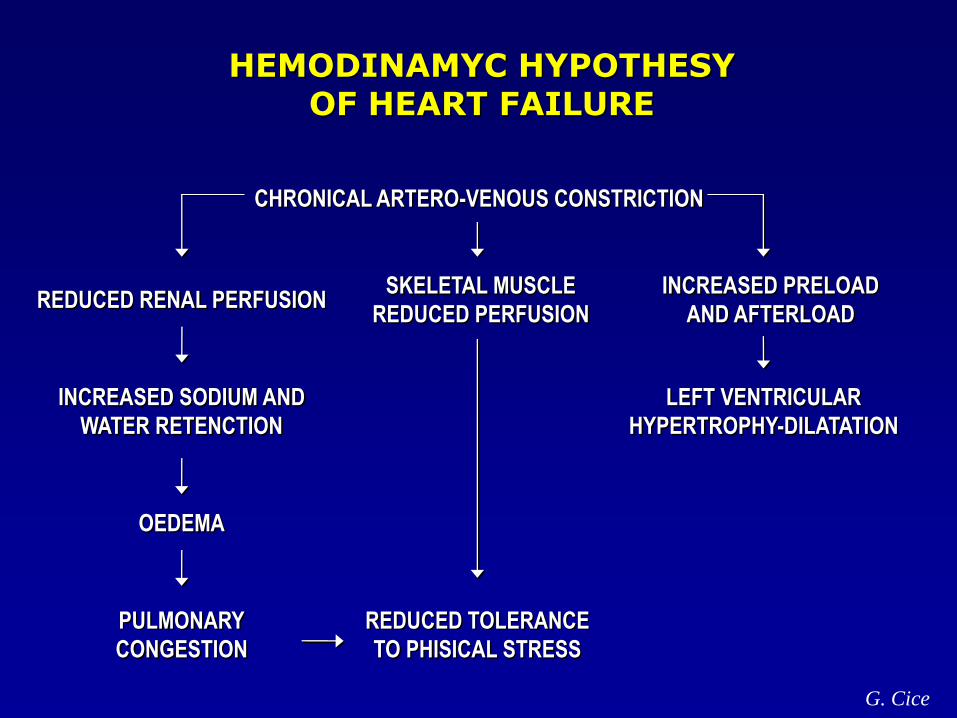
HEMODINAMYC HYPOTHESYOF HEART FAILURE
CHRONICAL ARTERO-VENOUS CONSTRICTION
REDUCED RENAL PERFUSIONSKELETAL MUSCLE
REDUCED PERFUSION
INCREASED PRELOAD
AND AFTERLOAD
LEFT VENTRICULAR
HYPERTROPHY-DILATATION
INCREASED SODIUM AND
WATER RETENCTION
OEDEMA
PULMONARY
CONGESTION
REDUCED TOLERANCE
TO PHISICAL STRESS
G. Cice
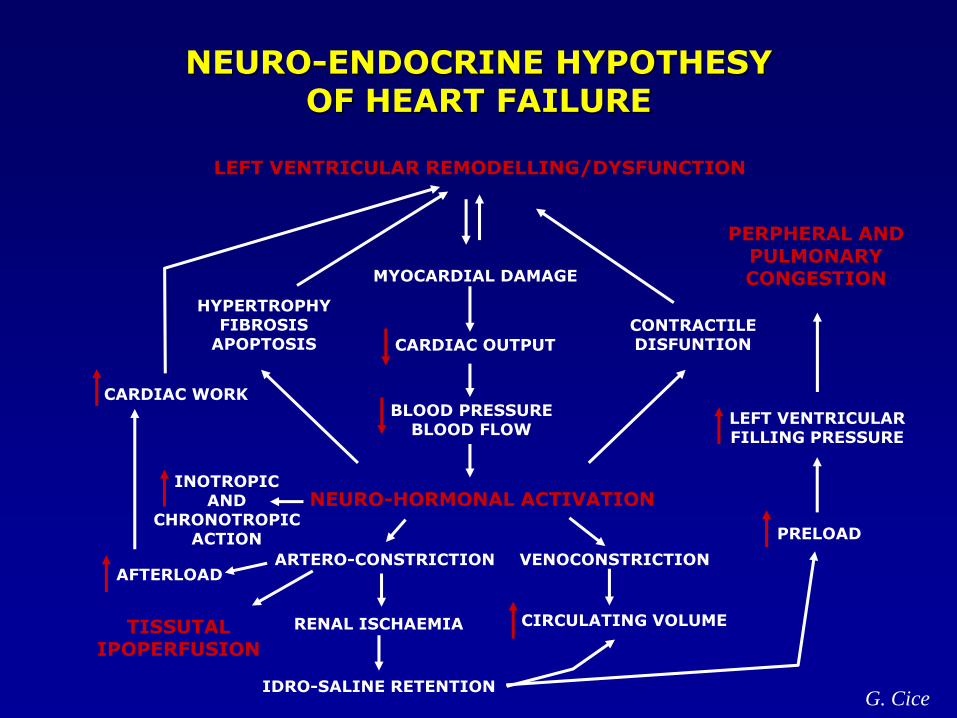
NEURO-ENDOCRINE HYPOTHESYOF HEART FAILURE
NEURO-HORMONAL ACTIVATION
LEFT VENTRICULAR REMODELLING/DYSFUNCTION
PERPHERAL ANDPULMONARYCONGESTIONMYOCARDIAL DAMAGE
CARDIAC OUTPUT
BLOOD PRESSUREBLOOD FLOW
INOTROPICAND
CHRONOTROPICACTION
CARDIAC WORK
HYPERTROPHYFIBROSIS
APOPTOSISCONTRACTILEDISFUNTION
AFTERLOAD
LEFT VENTRICULARFILLING PRESSURE
PRELOAD
VENOCONSTRICTION
CIRCULATING VOLUME
IDRO-SALINE RETENTION
RENAL ISCHAEMIA
ARTERO-CONSTRICTION
TISSUTALIPOPERFUSION
G. Cice
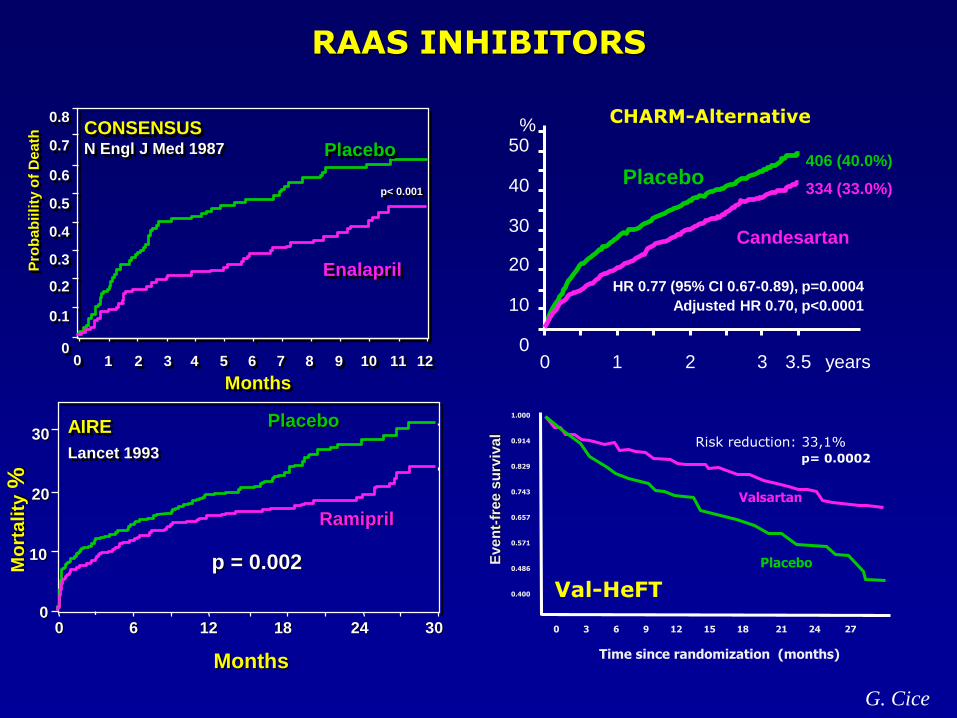
RAAS INHIBITORS
Placebo
Enalapril
12111098765
Pro
bab
iili
ty o
f D
eath
Months
0.1
0.8
0
0.2
0.3
0.7
0.4
0.5
0.6p< 0.001
CONSENSUSN Engl J Med 1987
43210
Months
302412 180 6
10
30
20
0
Placebo
Ramipril
p = 0.002Mo
rta
lity
%
AIRE
Lancet 1993
G. Cice
0 1 2 3 years0
10
20
30
40
50
Placebo
Candesartan
%
HR 0.77 (95% CI 0.67-0.89), p=0.0004
Adjusted HR 0.70, p<0.0001
3.5
406 (40.0%)
334 (33.0%)
CHARM-Alternative
Eve
nt-
fre
e s
urv
iva
l
0 3 6 9 12 15 18 21 24 27
Time since randomization (months)
Risk reduction: 33,1%p= 0.0002
1.000
0.914
0.829
0.743
0.657
0.571
0.486
0.400
Valsartan
Placebo
Val-HeFT
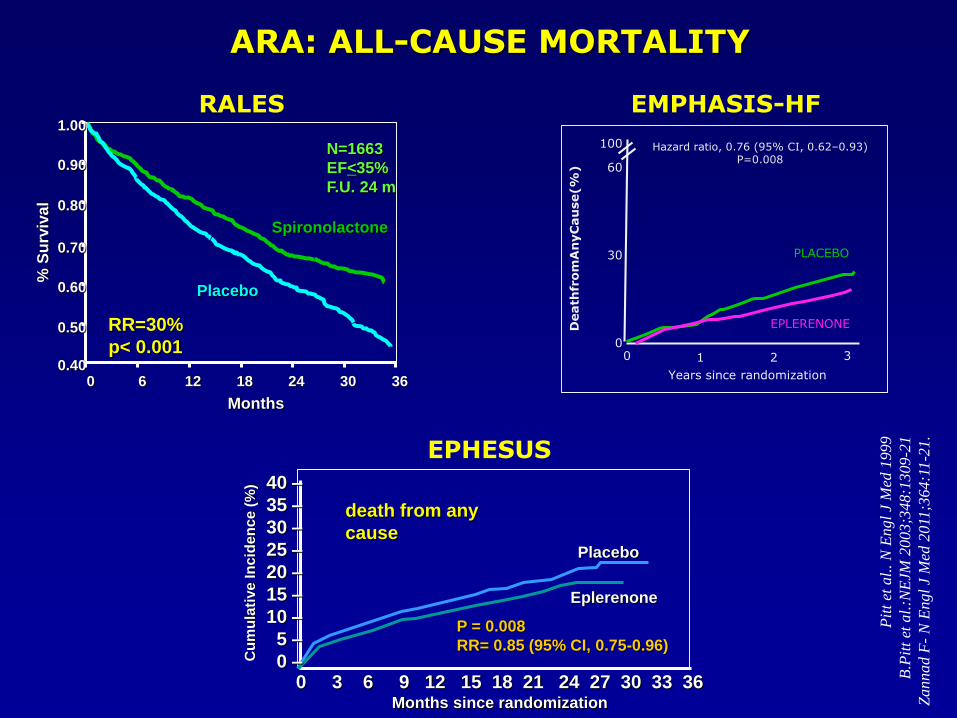
1.00
0.90
0.80
0.70
0.60
0.50
0.400 6 12 18 24 30 36
Placebo
Spironolactone
% S
urv
iva
l
Months
RR=30%
p< 0.001
N=1663
EF<35%
F.U. 24 m
0 3 6 9 12 15 18 21 24 27 30 33 36Months since randomization
P = 0.008
RR= 0.85 (95% CI, 0.75-0.96)
Placebo
Eplerenone
40 –
35 –
30 –
25 –
20 –
15 –
10 –
5 –
0 –Cu
mu
lati
ve
In
cid
en
ce
(%
)
death from any
cause
Death
from
An
yC
au
se(%
)
Years since randomization
100
60
30
00 1 2 3
Hazard ratio, 0.76 (95% CI, 0.62–0.93)P=0.008
EPLERENONE
PLACEBO
RALES
EPHESUS
EMPHASIS-HF
Pit
t et
al.
. N
Engl
J M
ed 1
999
B.P
itt
et a
l.:N
EJM
20
03;3
48:1
309
-21
Zannad F
-N
Engl
J M
ed 2
011
;364:1
1-2
1.
ARA: ALL-CAUSE MORTALITY
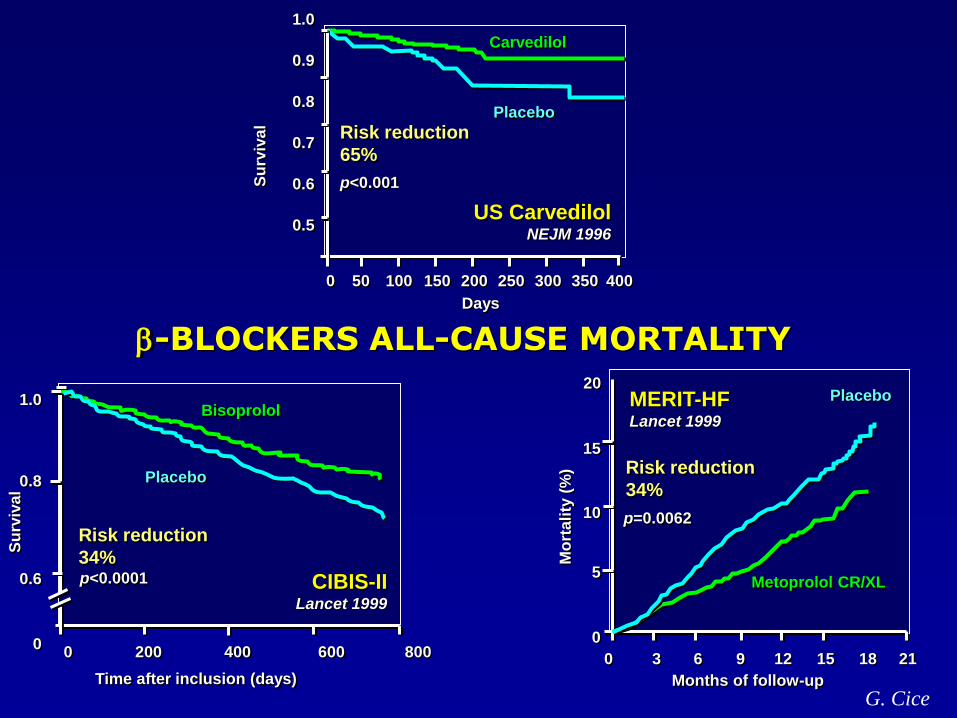
-BLOCKERS ALL-CAUSE MORTALITY
0 200 400 600 800
1.0
0.8
0.6
0
Bisoprolol
Placebo
Time after inclusion (days)
p<0.0001
Su
rviv
al
Risk reduction
34%
CIBIS-IILancet 1999
Months of follow-up
Mo
rtali
ty (
%)
0 3 6 9 12 15 18 21
20
15
10
5
0
Placebo
Metoprolol CR/XL
p=0.0062
Risk reduction
34%
MERIT-HFLancet 1999
Su
rviv
al
Carvedilol
Placebo
Days
0 50 100 150 200 250 300 350 400
1.0
0.9
0.8
0.7
0.6
0.5
Risk reduction
65%
p<0.001
US CarvedilolNEJM 1996
G. Cice
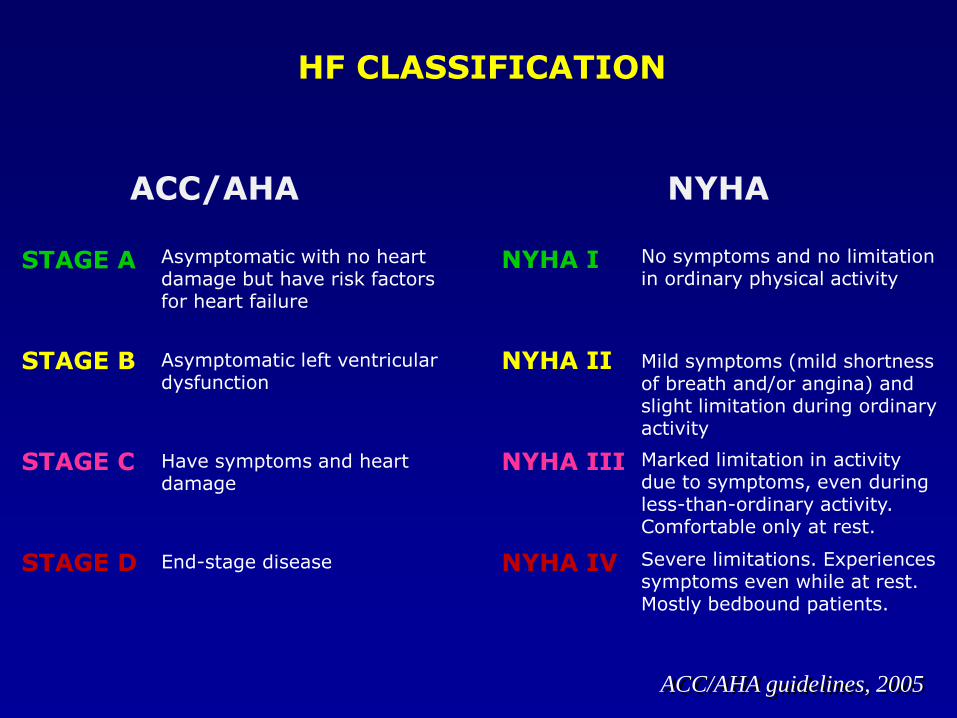
ACC/AHA NYHA
STAGE A Asymptomatic with no heart damage but have risk factors for heart failure
STAGE B Asymptomatic left ventricular dysfunction
STAGE C Have symptoms and heart damage
STAGE D End-stage disease
NYHA I No symptoms and no limitation in ordinary physical activity
NYHA II Mild symptoms (mild shortness of breath and/or angina) and slight limitation during ordinary activity
NYHA III Marked limitation in activity due to symptoms, even during less-than-ordinary activity. Comfortable only at rest.
NYHA IV Severe limitations. Experiences symptoms even while at rest. Mostly bedbound patients.
HF CLASSIFICATION
ACC/AHA guidelines, 2005
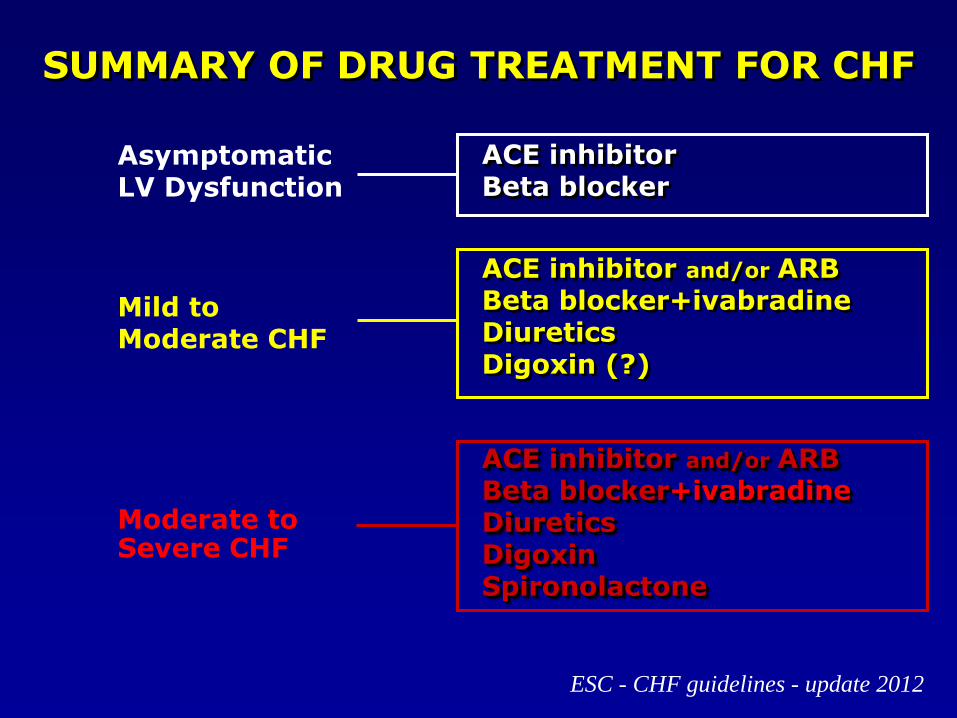
SUMMARY OF DRUG TREATMENT FOR CHF
AsymptomaticLV Dysfunction
Mild toModerate CHF
Moderate toSevere CHF
ESC - CHF guidelines - update 2012
ACE inhibitorBeta blocker
ACE inhibitor and/or ARBBeta blocker+ivabradineDiureticsDigoxin (?)
ACE inhibitor and/or ARBBeta blocker+ivabradineDiureticsDigoxinSpironolactone
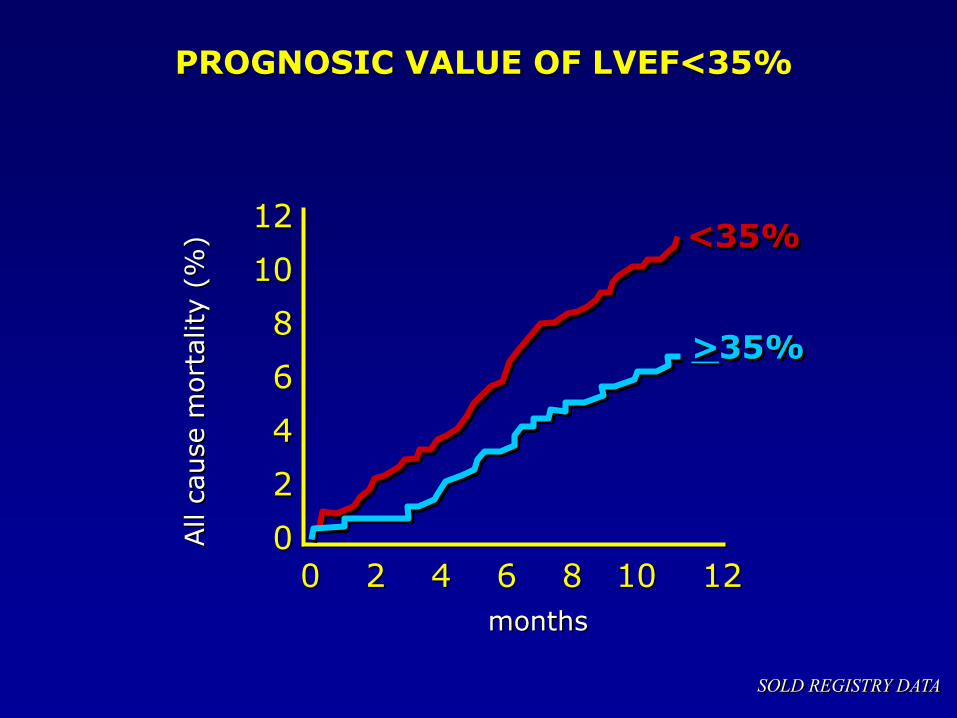
SOLD REGISTRY DATA
0 2 4 6 8 10 12
months
12
10
8
6
4
2
0All c
ause m
ort
ality
(%
)
PROGNOSIC VALUE OF LVEF<35%
<35%
>35%
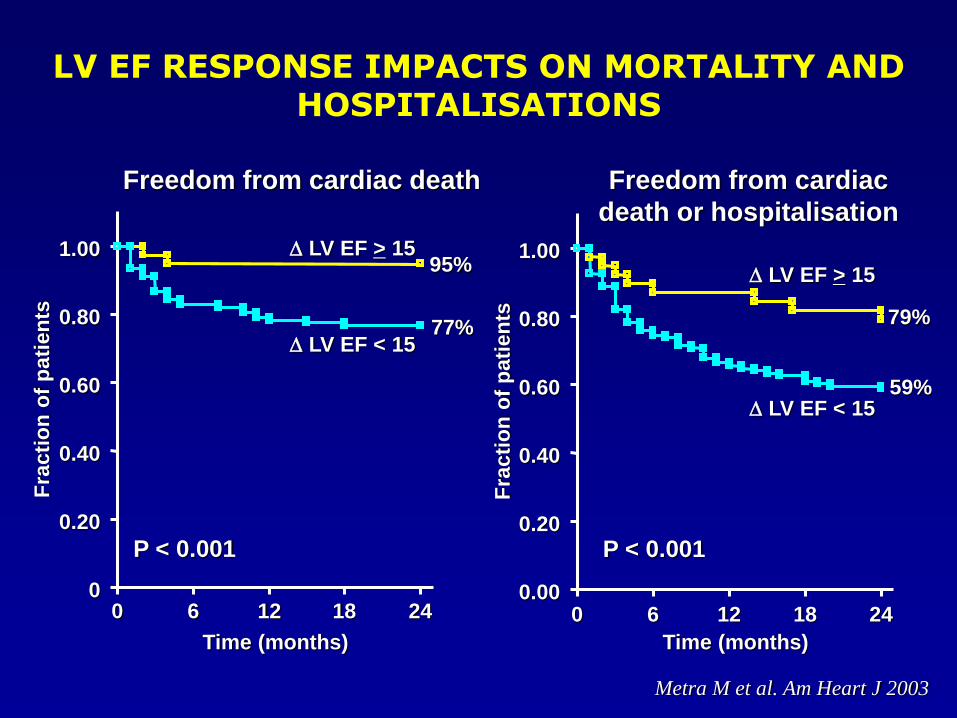
LV EF RESPONSE IMPACTS ON MORTALITY AND HOSPITALISATIONS
Freedom from cardiac
death or hospitalisation
0.00
0.20
0.40
0.60
0.80
1.00
0 6 12 18 24
Time (months)
Fra
cti
on
of
pati
en
ts
P < 0.001
LV EF > 15
LV EF < 15
79%
59%
Freedom from cardiac death
0
0.20
0.40
0.60
0.80
1.00
0 6 12 18 24
Time (months)
Fra
cti
on
of
pati
en
ts
P < 0.001
LV EF > 15
LV EF < 15
95%
77%
Metra M et al. Am Heart J 2003
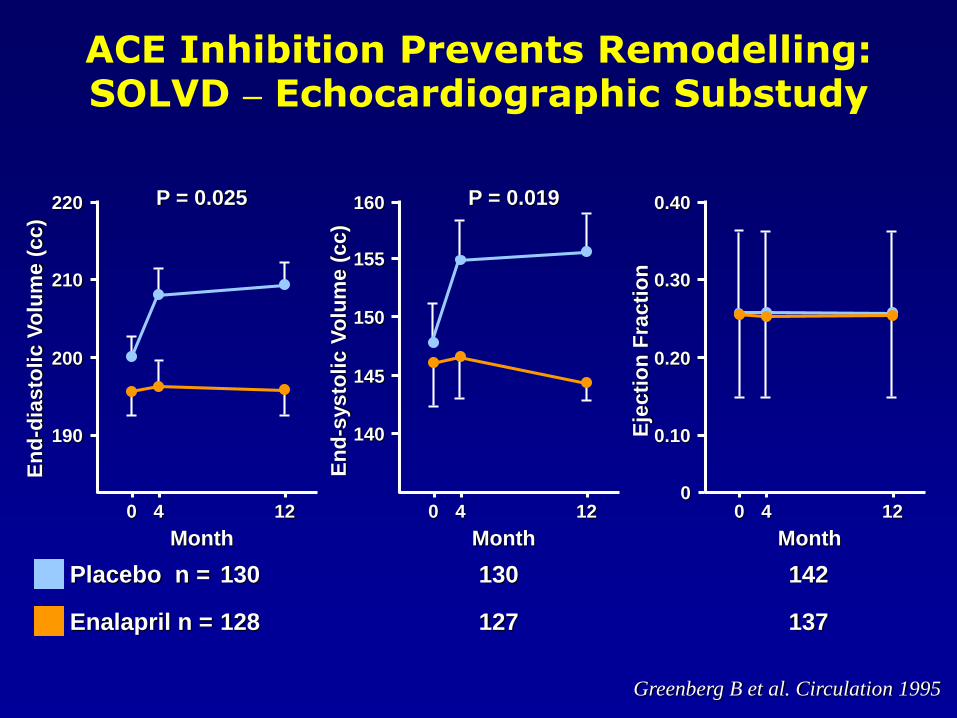
ACE Inhibition Prevents Remodelling:SOLVD – Echocardiographic Substudy
Greenberg B et al. Circulation 1995
220
210
200
190
4 120
Month
En
d-d
iasto
lic V
olu
me (
cc)
P = 0.025 160
155
150
140
4 120
Month
P = 0.019
145
En
d-s
ysto
lic V
olu
me (
cc)
0.40
0.30
0.20
0.10
4 120
Month
Eje
cti
on
Fra
cti
on
0
Placebo n = 130 130 142
Enalapril n = 128 127 137
LV
ES
VI (b
ipla
ne
) [m
l/m
2]
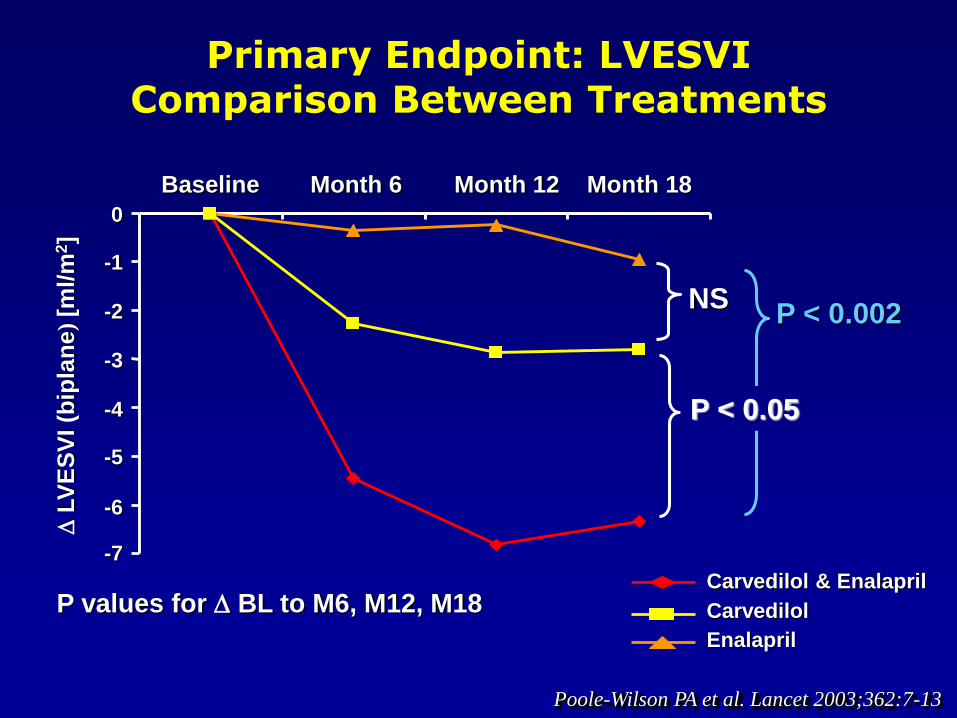
P values for BL to M6, M12, M18
Primary Endpoint: LVESVI Comparison Between Treatments
Carvedilol & Enalapril
Carvedilol
Enalapril
-7
Month 6 Month 12 Month 18Baseline
NSP < 0.002
-6
-5
-4
-3
-2
-1
0
P < 0.05
Poole-Wilson PA et al. Lancet 2003;362:7-13
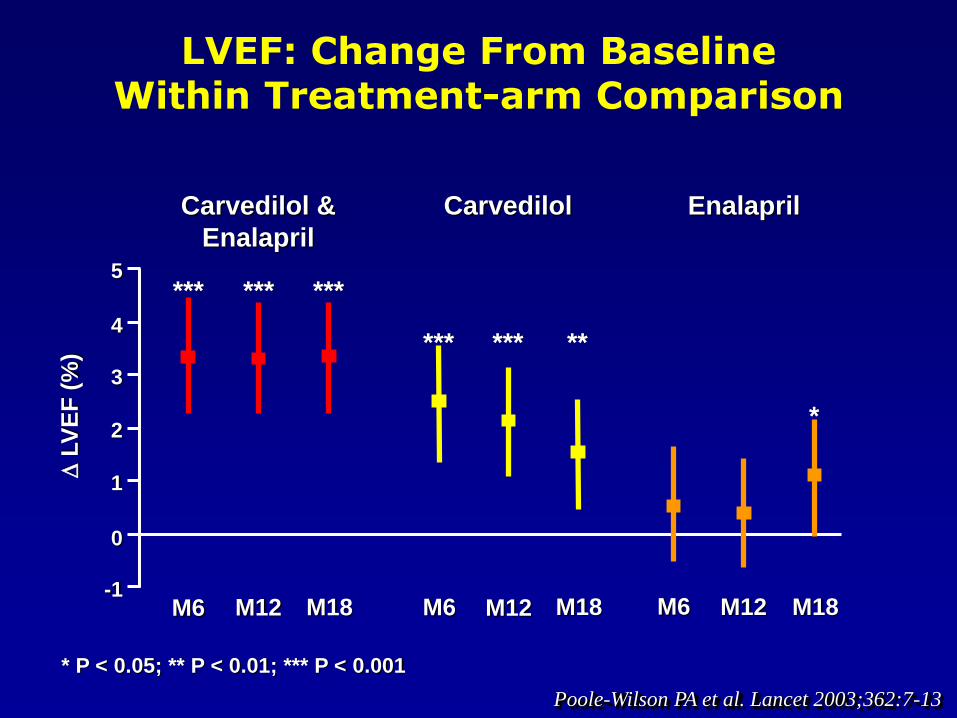
LVEF: Change From BaselineWithin Treatment-arm Comparison
* P < 0.05; ** P < 0.01; *** P < 0.001
EnalaprilCarvedilol &
Enalapril
Carvedilol
-1
0
1
2
3
4
5
LV
EF
(%
)
*** *** ***
*** *** **
*
M6 M12 M18 M6 M18M12 M6 M12 M18
Poole-Wilson PA et al. Lancet 2003;362:7-13
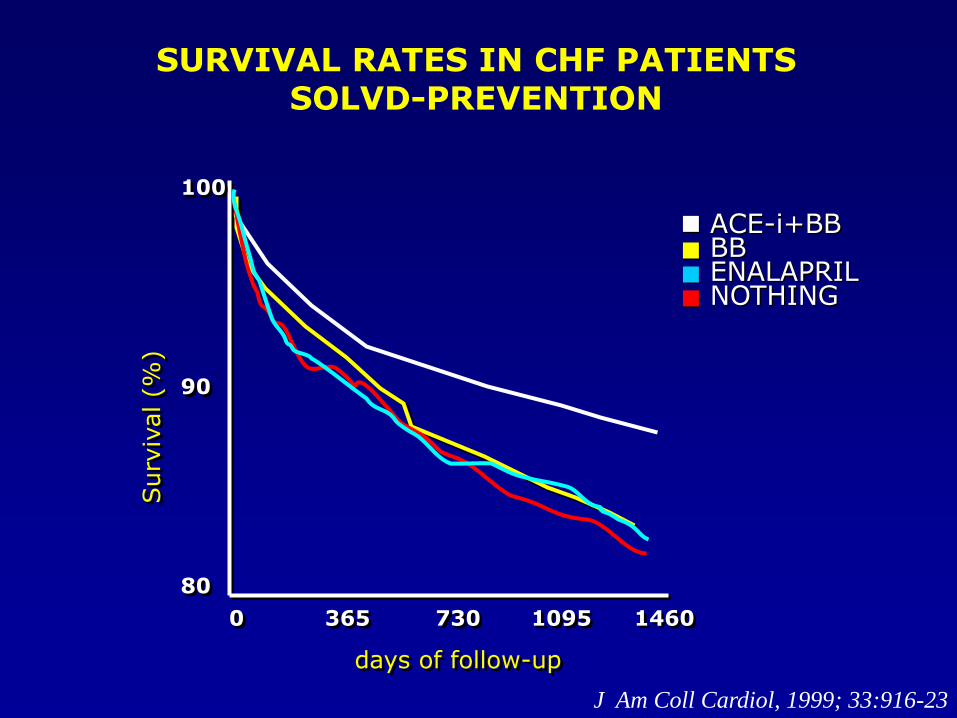
SURVIVAL RATES IN CHF PATIENTSSOLVD-PREVENTION
BBENALAPRILNOTHING
ACE-i+BB
100
90
80
0 365 730 1095 1460
days of follow-up
Surv
ival (%
)
J Am Coll Cardiol, 1999; 33:916-23
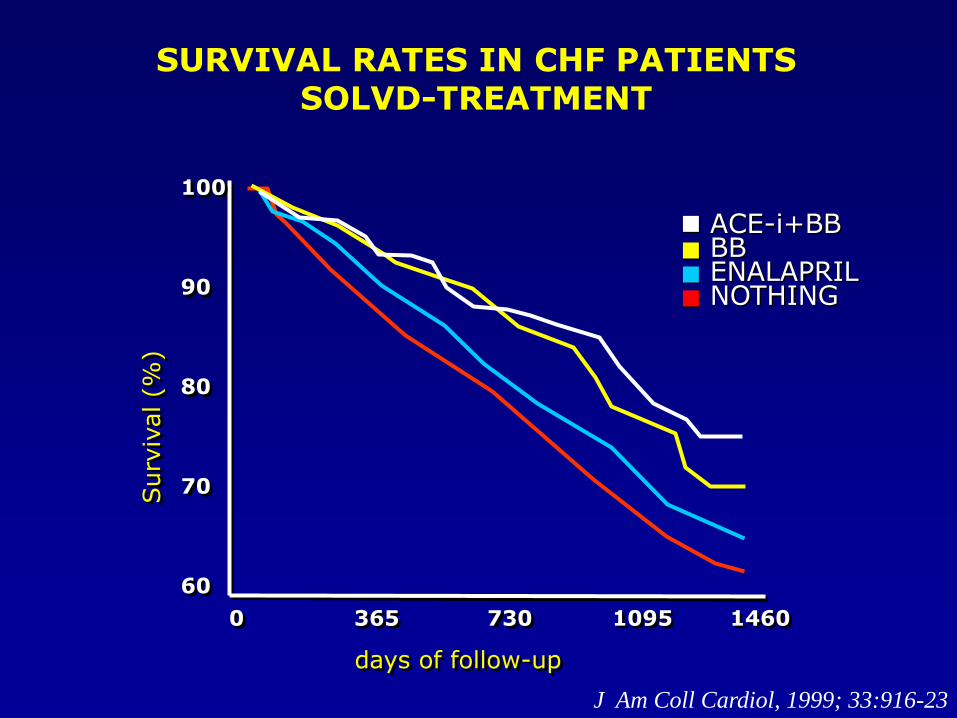
SURVIVAL RATES IN CHF PATIENTSSOLVD-TREATMENT
BBENALAPRILNOTHING
ACE-i+BB
100
90
80
70
60
0 365 730 1095 1460
days of follow-up
Surv
ival (%
)
J Am Coll Cardiol, 1999; 33:916-23
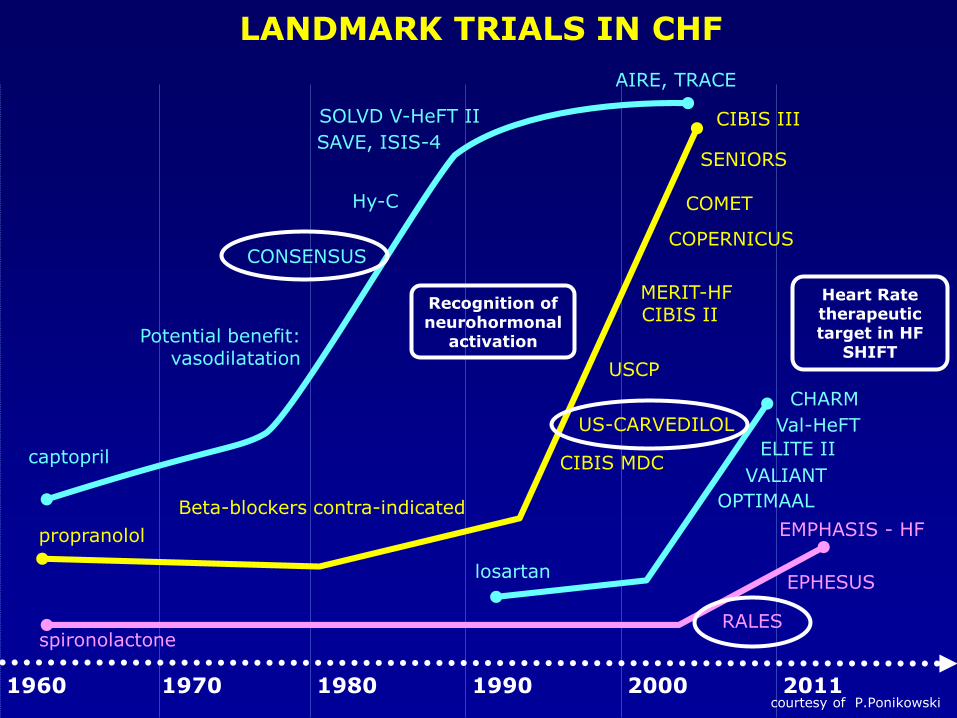
LANDMARK TRIALS IN CHF
ELITE II
CHARM
Val-HeFT
OPTIMAAL
VALIANT
losartan
CONSENSUS
captopril
Potential benefit:vasodilatation
SOLVD V-HeFT II
Hy-C
AIRE, TRACE
SAVE, ISIS-4
Heart Ratetherapeutictarget in HF
SHIFT
Recognition ofneurohormonal
activation
1960 1970 1980 1990 2000 2011courtesy of P.Ponikowski
EPHESUS
spironolactoneRALES
EMPHASIS - HF
SENIORS
propranolol
Beta-blockers contra-indicated
CIBIS MDC
USCP
MERIT-HFCIBIS II
COPERNICUS
COMET
CIBIS III
US-CARVEDILOL
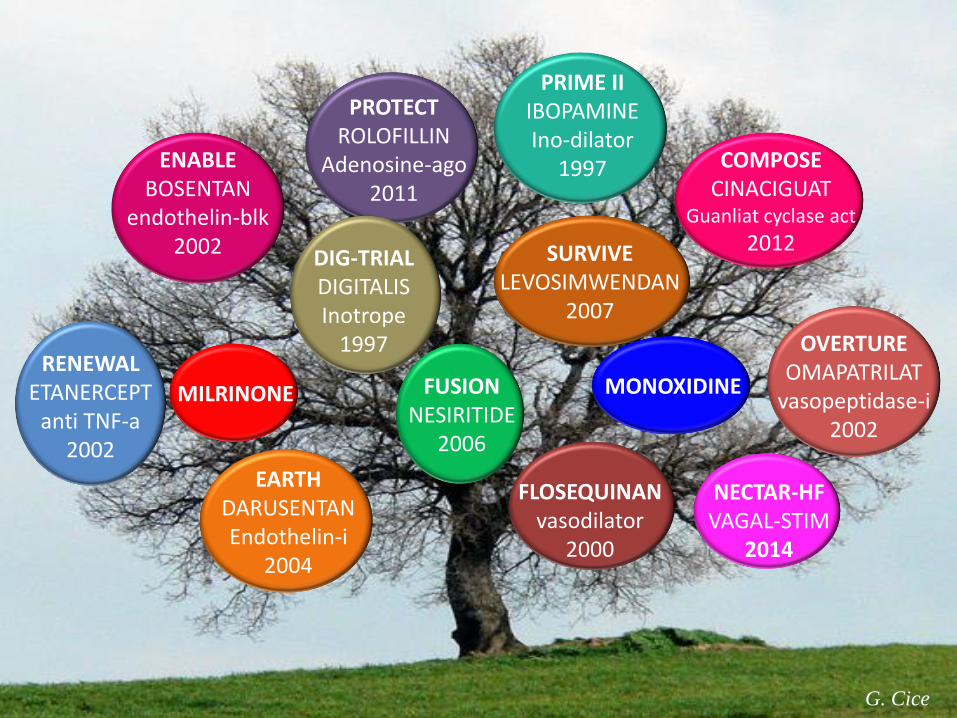
RENEWAL ETANERCEPT
anti TNF-a2002
OVERTUREOMAPATRILAT
vasopeptidase-i2002
ENABLEBOSENTAN
endothelin-blk2002
COMPOSECINACIGUAT
Guanliat cyclase act
2012
EARTHDARUSENTANEndothelin-i
2004
PROTECTROLOFILLIN
Adenosine-ago2011
FLOSEQUINANvasodilator
2000
PRIME IIIBOPAMINEIno-dilator
1997
DIG-TRIALDIGITALISInotrope
1997
MILRINONE MONOXIDINEFUSIONNESIRITIDE
2006
SURVIVELEVOSIMWENDAN
2007
G. Cice
NECTAR-HFVAGAL-STIM
2014
G. Cice
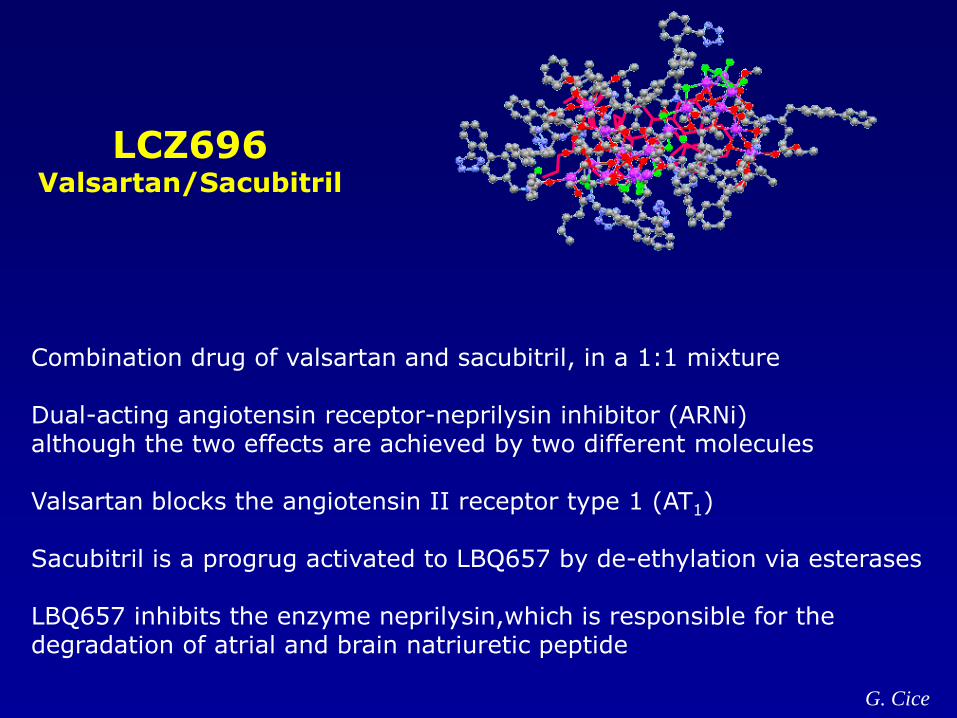
Combination drug of valsartan and sacubitril, in a 1:1 mixture
Dual-acting angiotensin receptor-neprilysin inhibitor (ARNi)although the two effects are achieved by two different molecules
Valsartan blocks the angiotensin II receptor type 1 (AT1)
Sacubitril is a progrug activated to LBQ657 by de-ethylation via esterases
LBQ657 inhibits the enzyme neprilysin,which is responsible for the degradation of atrial and brain natriuretic peptide
LCZ696Valsartan/Sacubitril
G. Cice
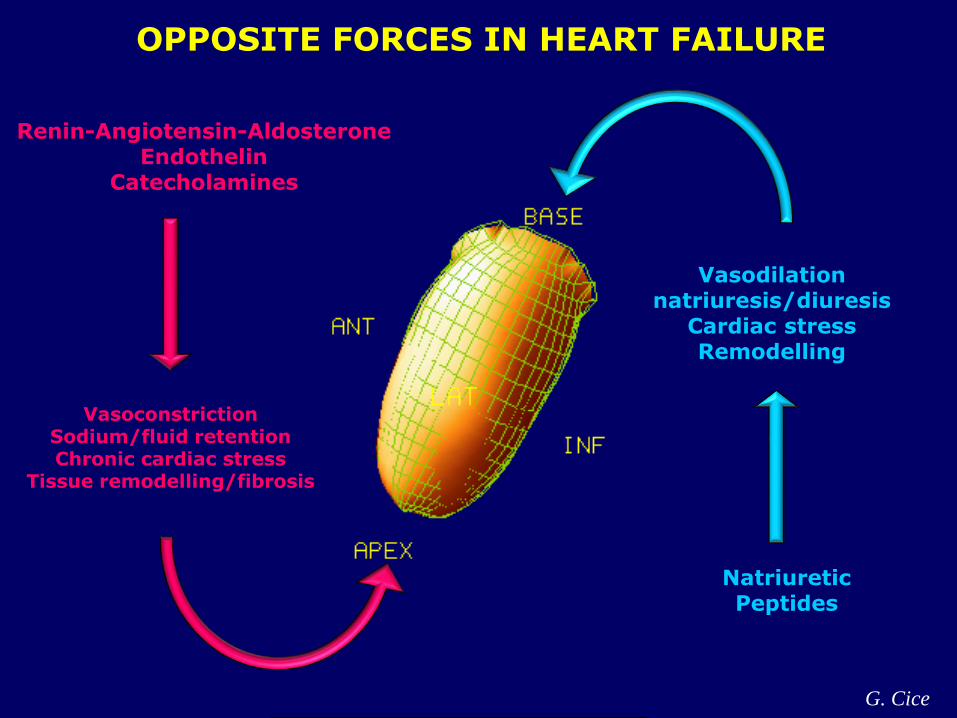
Vasodilationnatriuresis/diuresis
Cardiac stressRemodelling
NatriureticPeptides
VasoconstrictionSodium/fluid retentionChronic cardiac stress
Tissue remodelling/fibrosis
OPPOSITE FORCES IN HEART FAILURE
Renin-Angiotensin-AldosteroneEndothelin
Catecholamines
G. Cice
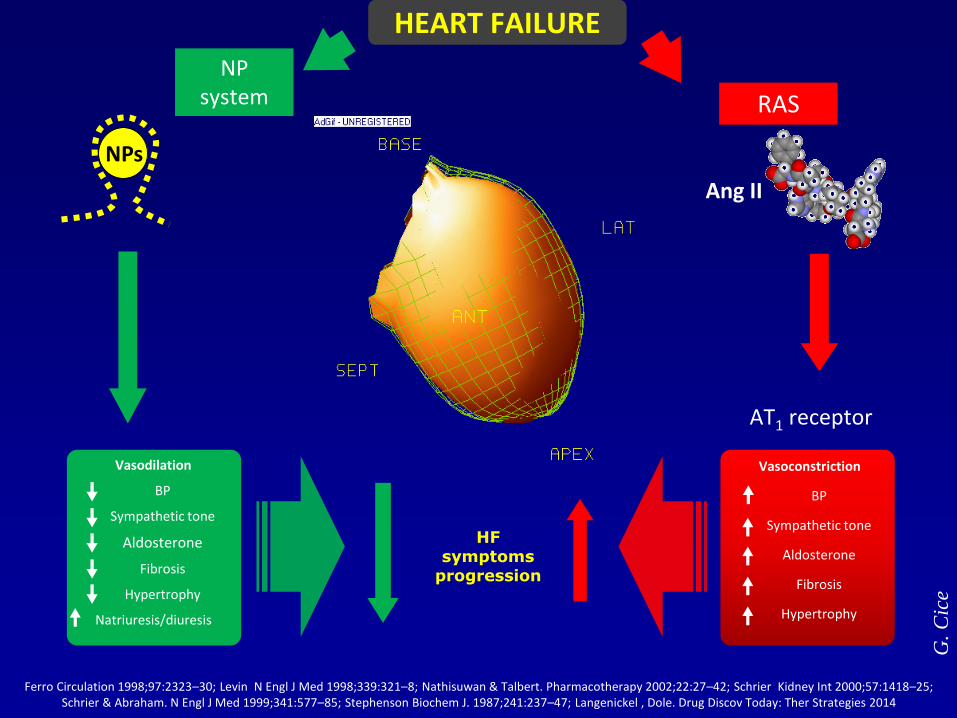
Ferro Circulation 1998;97:2323–30; Levin N Engl J Med 1998;339:321–8; Nathisuwan & Talbert. Pharmacotherapy 2002;22:27–42; Schrier Kidney Int 2000;57:1418–25; Schrier & Abraham. N Engl J Med 1999;341:577–85; Stephenson Biochem J. 1987;241:237–47; Langenickel , Dole. Drug Discov Today: Ther Strategies 2014
NP system
Ang II
AT1 receptor
RAS
HFsymptoms
progression
Vasodilation
BP
Sympathetic tone
Aldosterone
Fibrosis
Hypertrophy
Natriuresis/diuresis
Vasoconstriction
BP
Sympathetic tone
Aldosterone
Fibrosis
Hypertrophy
HEART FAILURE
NPs
G. C
ice
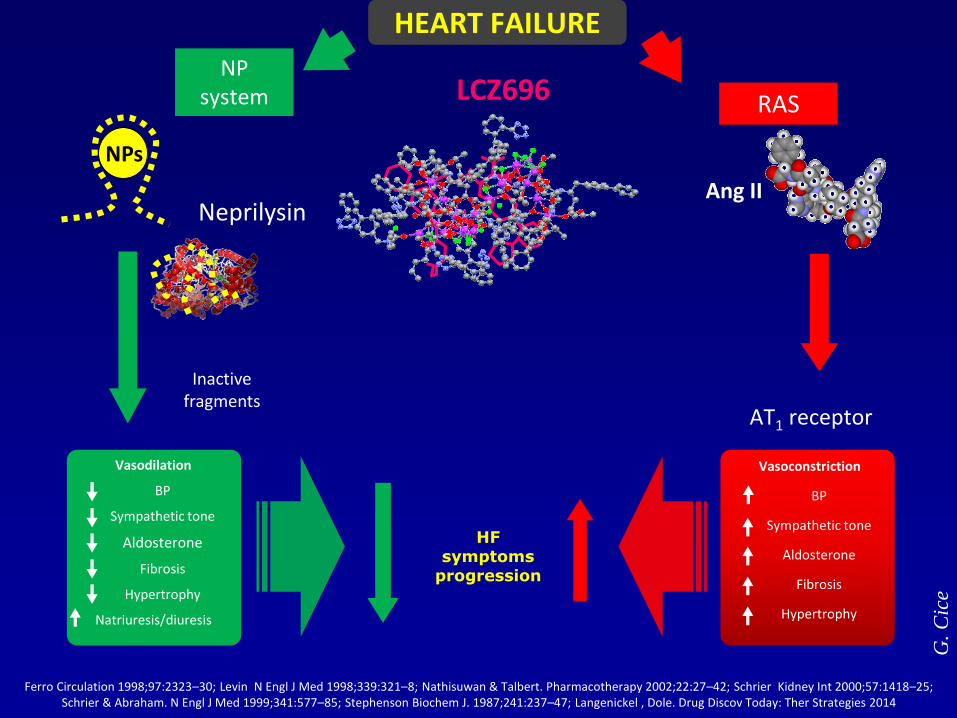
Ferro Circulation 1998;97:2323–30; Levin N Engl J Med 1998;339:321–8; Nathisuwan & Talbert. Pharmacotherapy 2002;22:27–42; Schrier Kidney Int 2000;57:1418–25; Schrier & Abraham. N Engl J Med 1999;341:577–85; Stephenson Biochem J. 1987;241:237–47; Langenickel , Dole. Drug Discov Today: Ther Strategies 2014
NP system
Ang II
AT1 receptor
RAS
HFsymptoms
progression
Vasodilation
BP
Sympathetic tone
Aldosterone
Fibrosis
Hypertrophy
Natriuresis/diuresis
Vasoconstriction
BP
Sympathetic tone
Aldosterone
Fibrosis
Hypertrophy
Inactive fragments
HEART FAILURE
Neprilysin
NPs
LCZ696
G. C
ice
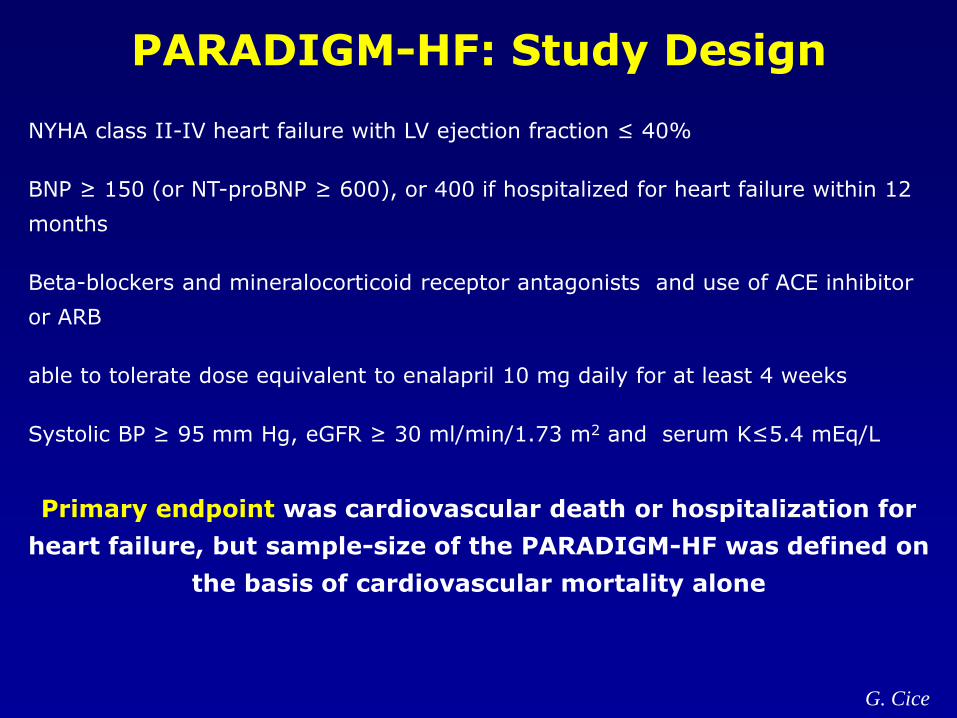
PARADIGM-HF: Study Design
NYHA class II-IV heart failure with LV ejection fraction ≤ 40%
BNP ≥ 150 (or NT-proBNP ≥ 600), or 400 if hospitalized for heart failure within 12
months
Beta-blockers and mineralocorticoid receptor antagonists and use of ACE inhibitor
or ARB
able to tolerate dose equivalent to enalapril 10 mg daily for at least 4 weeks
Systolic BP ≥ 95 mm Hg, eGFR ≥ 30 ml/min/1.73 m2 and serum K≤5.4 mEq/L
Primary endpoint was cardiovascular death or hospitalization for
heart failure, but sample-size of the PARADIGM-HF was defined on
the basis of cardiovascular mortality alone
G. Cice
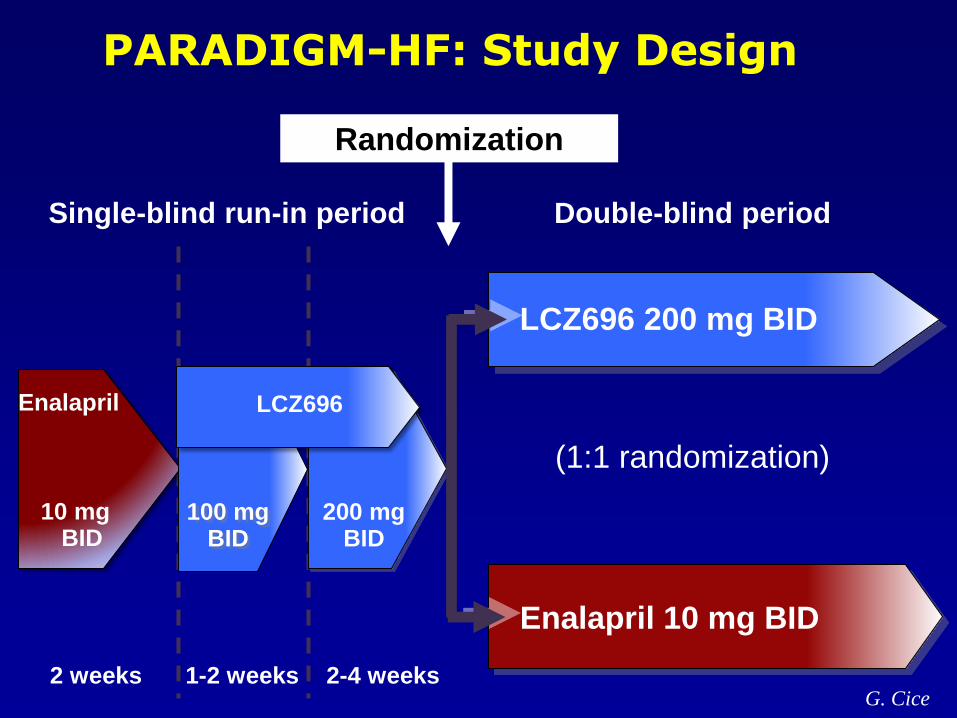
2 weeks 1-2 weeks 2-4 weeks
Single-blind run-in period Double-blind period
(1:1 randomization)
Enalapril
10 mgBID
Enalapril 10 mg BID
LCZ696 200 mg BID
PARADIGM-HF: Study Design
Randomization
100 mgBID
200 mgBID
LCZ696
G. Cice
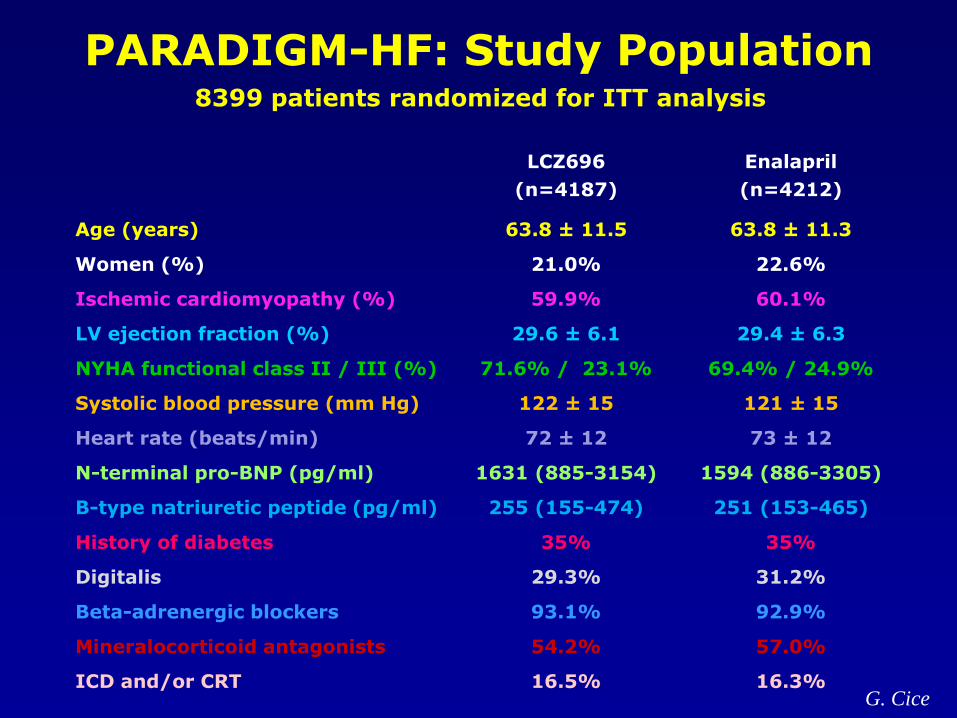
8399 patients randomized for ITT analysis
LCZ696
(n=4187)
Enalapril
(n=4212)
Age (years) 63.8 ± 11.5 63.8 ± 11.3
Women (%) 21.0% 22.6%
Ischemic cardiomyopathy (%) 59.9% 60.1%
LV ejection fraction (%) 29.6 ± 6.1 29.4 ± 6.3
NYHA functional class II / III (%) 71.6% / 23.1% 69.4% / 24.9%
Systolic blood pressure (mm Hg) 122 ± 15 121 ± 15
Heart rate (beats/min) 72 ± 12 73 ± 12
N-terminal pro-BNP (pg/ml) 1631 (885-3154) 1594 (886-3305)
B-type natriuretic peptide (pg/ml) 255 (155-474) 251 (153-465)
History of diabetes 35% 35%
Digitalis 29.3% 31.2%
Beta-adrenergic blockers 93.1% 92.9%
Mineralocorticoid antagonists 54.2% 57.0%
ICD and/or CRT 16.5% 16.3%
PARADIGM-HF: Study Population
G. Cice
0
16
32
40
24
8
Enalapril(n=4212)
360 720 10800 180 540 900 1260
Days After Randomization
4187
4212
3922
3883
3663
3579
3018
2922
2257
2123
1544
1488
896
853
249
236
LCZ696
Enalapril
Patients at Risk
1117
Kap
lan
-Meie
r E
sti
mate
of
Cu
mu
lati
ve R
ate
s (
%)
914
LCZ696(n=4187)
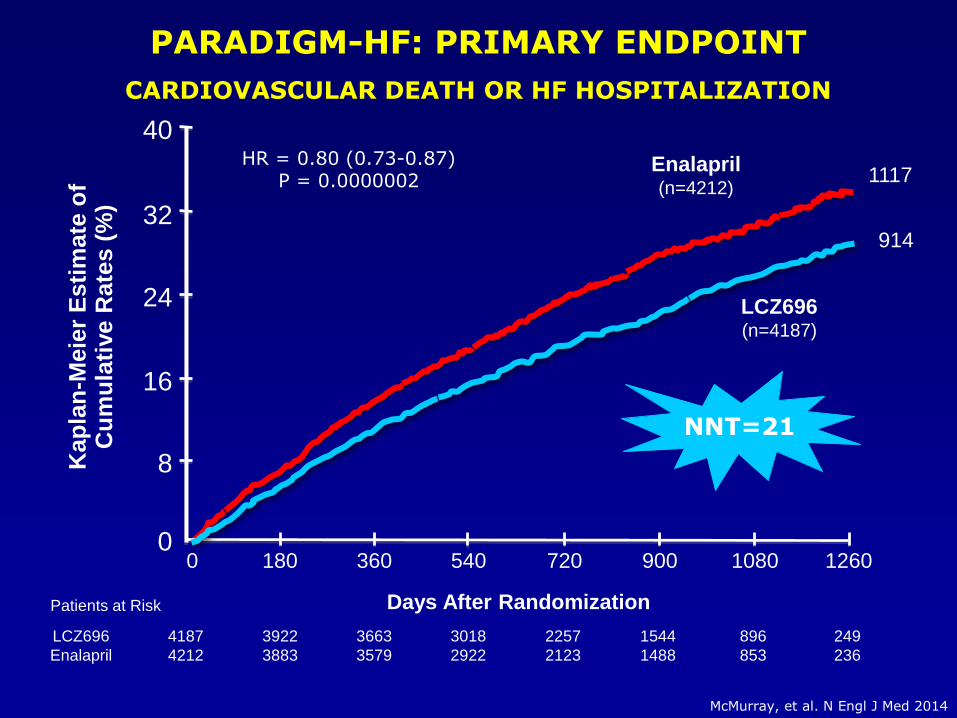
PARADIGM-HF: PRIMARY ENDPOINT
CARDIOVASCULAR DEATH OR HF HOSPITALIZATION
HR = 0.80 (0.73-0.87)P = 0.0000002
NNT=21
McMurray, et al. N Engl J Med 2014
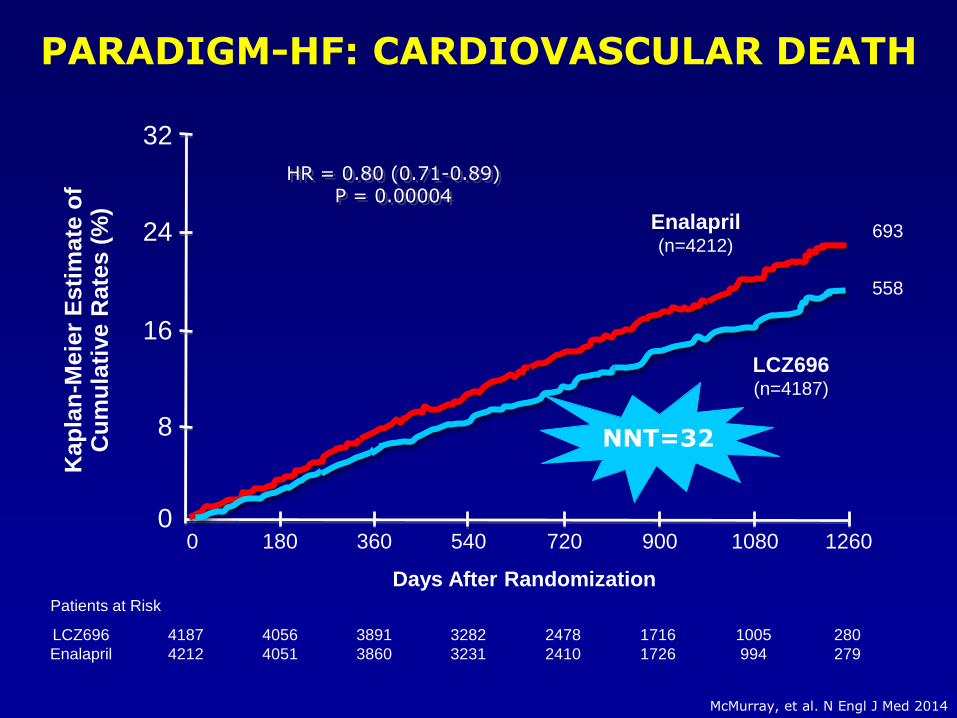
HR = 0.80 (0.71-0.89)P = 0.00004
Enalapril(n=4212)
LCZ696(n=4187)
Kap
lan
-Meie
r E
sti
mate
of
Cu
mu
lati
ve R
ate
s (
%)
Days After Randomization
4187
4212
4056
4051
3891
3860
3282
3231
2478
2410
1716
1726
1005
994
280
279
LCZ696
Enalapril
Patients at Risk
360 720 10800 180 540 900 12600
16
32
24
8
693
558
PARADIGM-HF: CARDIOVASCULAR DEATH
NNT=32
McMurray, et al. N Engl J Med 2014
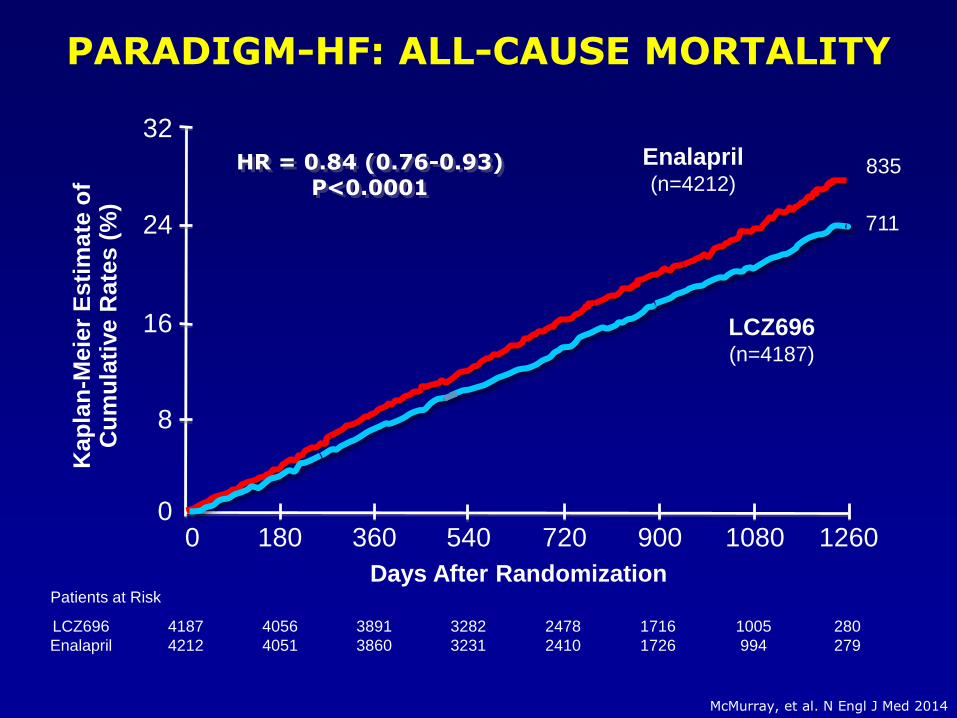
PARADIGM-HF: ALL-CAUSE MORTALITY
4187
4212
4056
4051
3891
3860
3282
3231
2478
2410
1716
1726
1005
994
280
279
LCZ696
Enalapril
Enalapril(n=4212)
LCZ696(n=4187)
HR = 0.84 (0.76-0.93)P<0.0001
Kap
lan
-Meie
r E
sti
mate
of
Cu
mu
lati
ve R
ate
s (
%)
Days After RandomizationPatients at Risk
360 720 10800 180 540 900 12600
16
32
24
8
835
711
McMurray, et al. N Engl J Med 2014
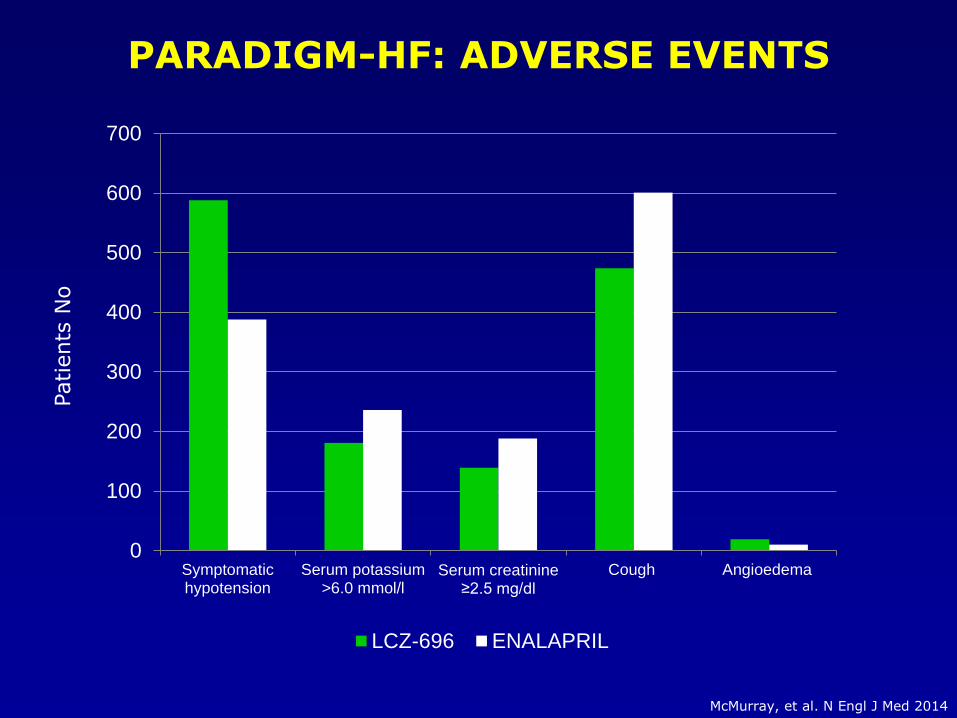
0
100
200
300
400
500
600
700
Symptomatichypotension
Serum potassium>6.0 mmol/l
Serum creatinine ≥2.5 mg/dl
Cough Angioedema
LCZ-696 ENALAPRIL
PARADIGM-HF: ADVERSE EVENTS
McMurray, et al. N Engl J Med 2014
Patients
No
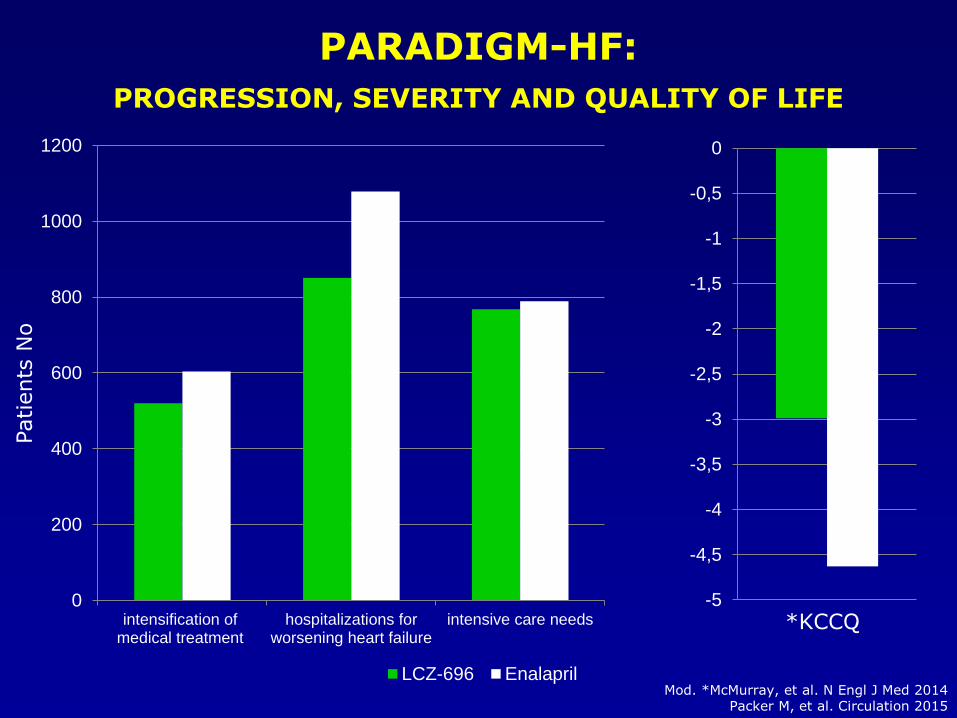
0
200
400
600
800
1000
1200
intensification ofmedical treatment
hospitalizations forworsening heart failure
intensive care needs
LCZ-696 Enalapril
Patients
No
-5
-4,5
-4
-3,5
-3
-2,5
-2
-1,5
-1
-0,5
0
*KCCQ
PARADIGM-HF:
PROGRESSION, SEVERITY AND QUALITY OF LIFE
Mod. *McMurray, et al. N Engl J Med 2014Packer M, et al. Circulation 2015
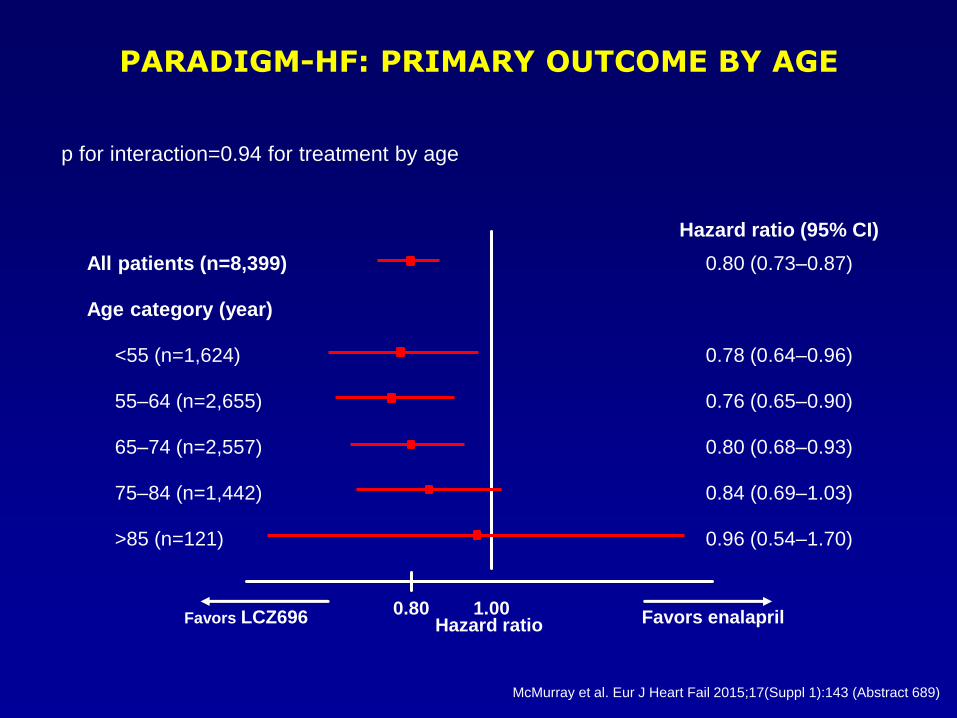
McMurray et al. Eur J Heart Fail 2015;17(Suppl 1):143 (Abstract 689)
PARADIGM-HF: PRIMARY OUTCOME BY AGE
Hazard ratio (95% CI)
All patients (n=8,399) 0.80 (0.73–0.87)
Age category (year)
<55 (n=1,624) 0.78 (0.64–0.96)
55–64 (n=2,655) 0.76 (0.65–0.90)
65–74 (n=2,557) 0.80 (0.68–0.93)
75–84 (n=1,442) 0.84 (0.69–1.03)
>85 (n=121) 0.96 (0.54–1.70)
1.000.80Favors LCZ696 Favors enalaprilHazard ratio
p for interaction=0.94 for treatment by age

McMurray, et al. N Engl J Med 2014; ePub ahead of print: DOI: 10.1056/NEJMoa1409077.
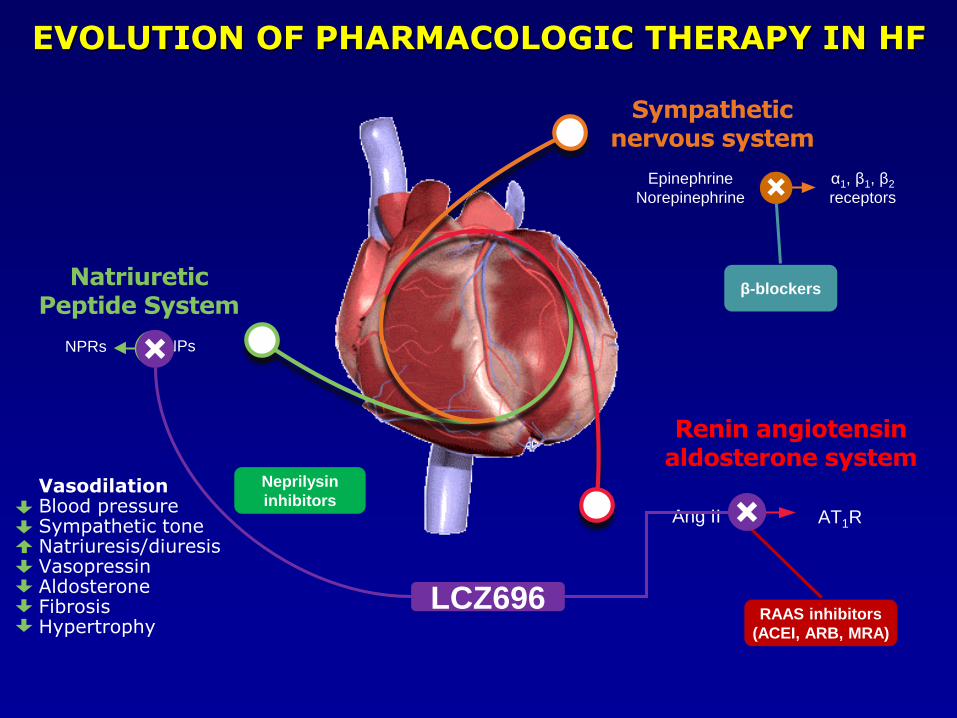
Sympathetic nervous system
Renin angiotensinaldosterone system
Ang II AT1R
NatriureticPeptide System
NPRs NPs
Epinephrine
Norepinephrine
α1, β1, β2
receptors
β-blockers
RAAS inhibitors
(ACEI, ARB, MRA)
Neprilysin
inhibitorsVasodilationBlood pressureSympathetic toneNatriuresis/diuresisVasopressinAldosteroneFibrosisHypertrophy
LCZ696
EVOLUTION OF PHARMACOLOGIC THERAPY IN HF
Thanks…for not having left the conference hall!
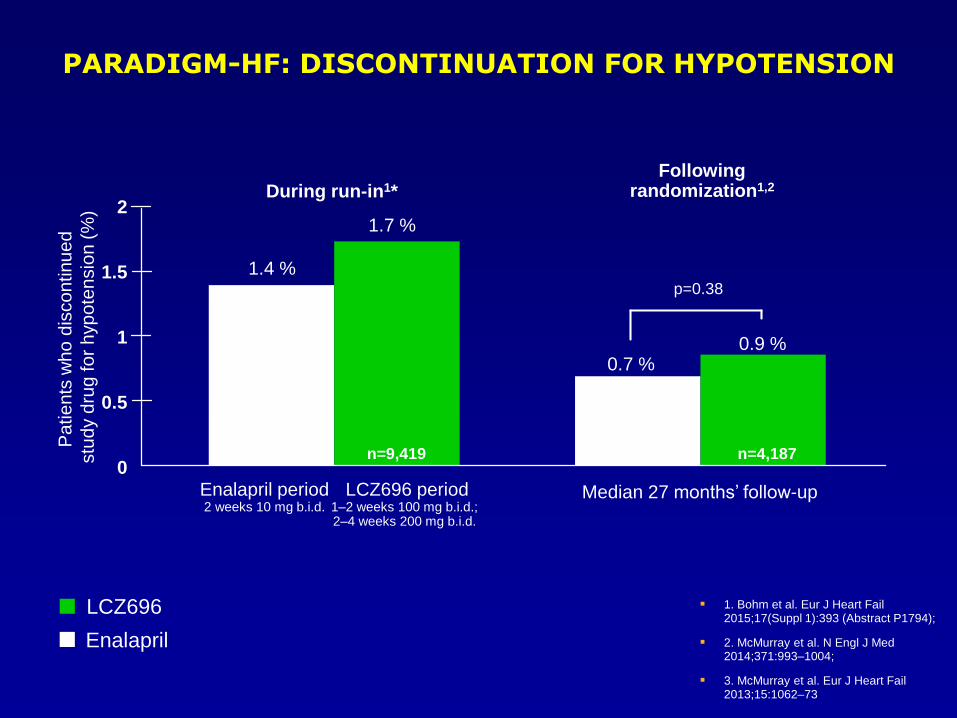
1. Bohm et al. Eur J Heart Fail 2015;17(Suppl 1):393 (Abstract P1794);
2. McMurray et al. N Engl J Med 2014;371:993–1004;
3. McMurray et al. Eur J Heart Fail 2013;15:1062–73
PARADIGM-HF: DISCONTINUATION FOR HYPOTENSION
Following randomization1,2During run-in1*
LCZ696
Enalapril
0
1
2
p=0.38
0.9 %0.7 %
1.7 %
1.4 %
Pa
tie
nts
wh
o d
isco
ntinu
ed
stu
dy d
rug
fo
r h
yp
ote
nsio
n (
%)
1.5
0.5
Enalapril period 2 weeks 10 mg b.i.d.
LCZ696 period1–2 weeks 100 mg b.i.d.; 2–4 weeks 200 mg b.i.d.
n=10,513 n=9,419 n=4,212 n=4,187
Median 27 months’ follow-up
“…angiotensin receptor–neprilysin inhibition with LCZ696 was superior to ACEinhibition alone in reducing the risks of death and of hospitalization for HF”
“The magnitude of the beneficial effect of LCZ696, as compared with enalapril,on CV mortality was at least as large as that of long-term treatment withenalapril, as compared with placebo.”
“This robust finding provides strong evidence that combined inhibition of theangiotensin receptor and neprilysin is superior to inhibition of the RAS alone inpatients with chronic HF.”
“…results are applicable to a broad spectrum of patients with HF, including those who are currently taking an ACE inhibitor or ARB or who are likely to be able to take such an agent without having unacceptable side effects.”
McMurray, et al. N Engl J Med 2014; ePub ahead of print: DOI: 10.1056/NEJMoa1409077.
PARADIGM-HF: TAKE HOME MESSAGES
CONCLUSIONS FROM PUBLICATION
G. Cice
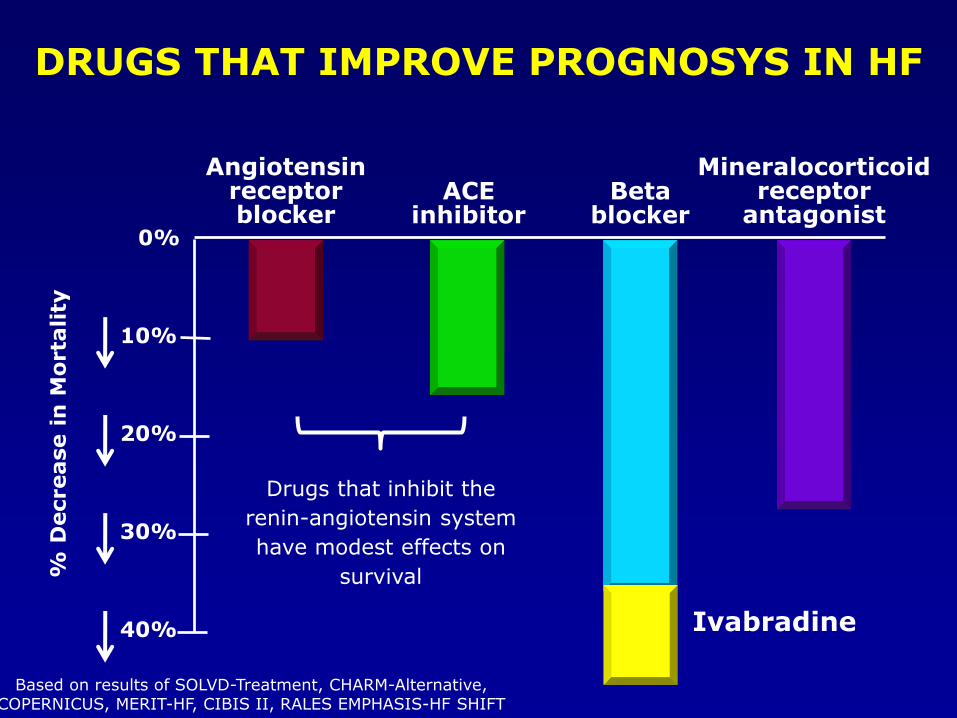
DRUGS THAT IMPROVE PROGNOSYS IN HF
Drugs that inhibit the
renin-angiotensin system
have modest effects on
survival
Based on results of SOLVD-Treatment, CHARM-Alternative,COPERNICUS, MERIT-HF, CIBIS II, RALES EMPHASIS-HF SHIFT
10%
20%
30%
40%
0%
% D
ecrease i
n M
orta
lity
Betablocker
Mineralocorticoidreceptor
antagonist
Angiotensinreceptorblocker
ACEinhibitor
Ivabradine
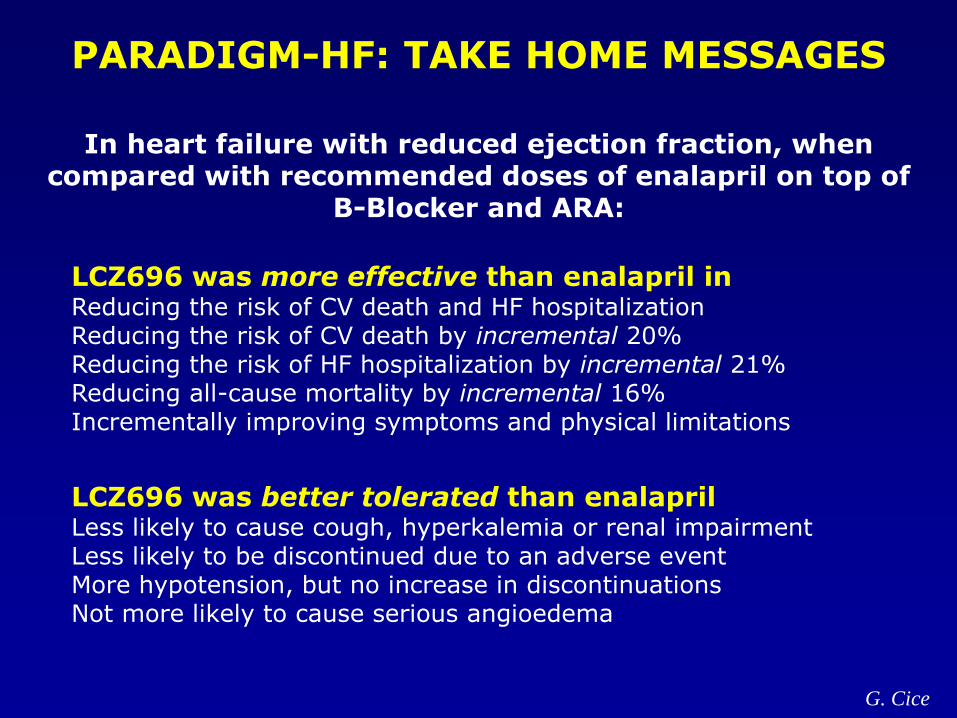
In heart failure with reduced ejection fraction, when compared with recommended doses of enalapril on top of
B-Blocker and ARA:
PARADIGM-HF: TAKE HOME MESSAGES
LCZ696 was more effective than enalapril inReducing the risk of CV death and HF hospitalizationReducing the risk of CV death by incremental 20%Reducing the risk of HF hospitalization by incremental 21%Reducing all-cause mortality by incremental 16%Incrementally improving symptoms and physical limitations
LCZ696 was better tolerated than enalaprilLess likely to cause cough, hyperkalemia or renal impairmentLess likely to be discontinued due to an adverse eventMore hypotension, but no increase in discontinuationsNot more likely to cause serious angioedema
G. Cice

Increase in Life Expectancy by Enalapril in Combined SOLVD Trials
Years after Randomization
Mo
rtality
0 1 2 3 4 5 6 7 8 9 10 11 12
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
Enalapril (n=472)*Placebo (n=448)*
Median Life ExpectancyDifference of9.4 months
p=0.004
http://www.phri.ca/x-solvd/ * Number of patients alive at 12 years
“PARADIGM-HF may well represent a new threshold of hopefor patients with HF”
“Now, a novel drug, LCZ696, a dual inhibitor of angiotensin IIreceptor and neprilysin, may prove to be the first disruptiveagent to the heart-failure treatment algorithm, which hasremained essentially unchanged for a decade”
“The beneficial results seen in PARADIGM-HF may apply to awide spectrum of patients, even those who are currentlyreceiving the best possible therapy”
Jessup. N Engl J Med 2014; ePub ahead of print: DOI: 10.1056/NEJMe1409898G. Cice
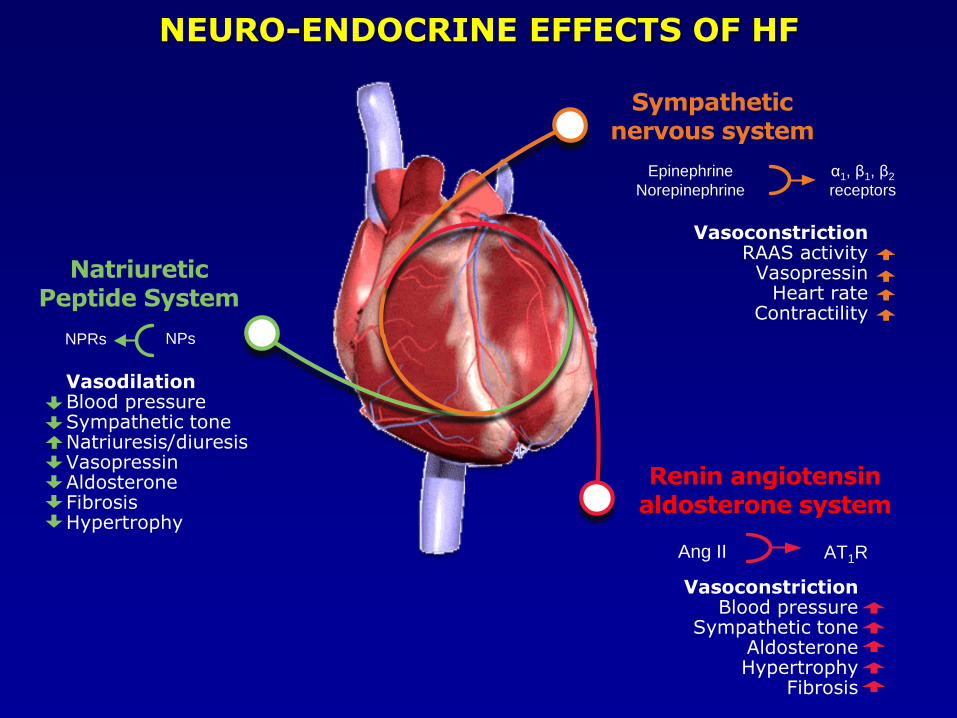
Sympathetic nervous system
Renin angiotensinaldosterone system
VasoconstrictionBlood pressure
Sympathetic toneAldosteroneHypertrophy
Fibrosis
Ang II AT1R
NatriureticPeptide System
VasodilationBlood pressureSympathetic toneNatriuresis/diuresisVasopressinAldosteroneFibrosisHypertrophy
NPRs NPs
Epinephrine
Norepinephrine
α1, β1, β2
receptors
VasoconstrictionRAAS activity
VasopressinHeart rate
Contractility
NEURO-ENDOCRINE EFFECTS OF HF
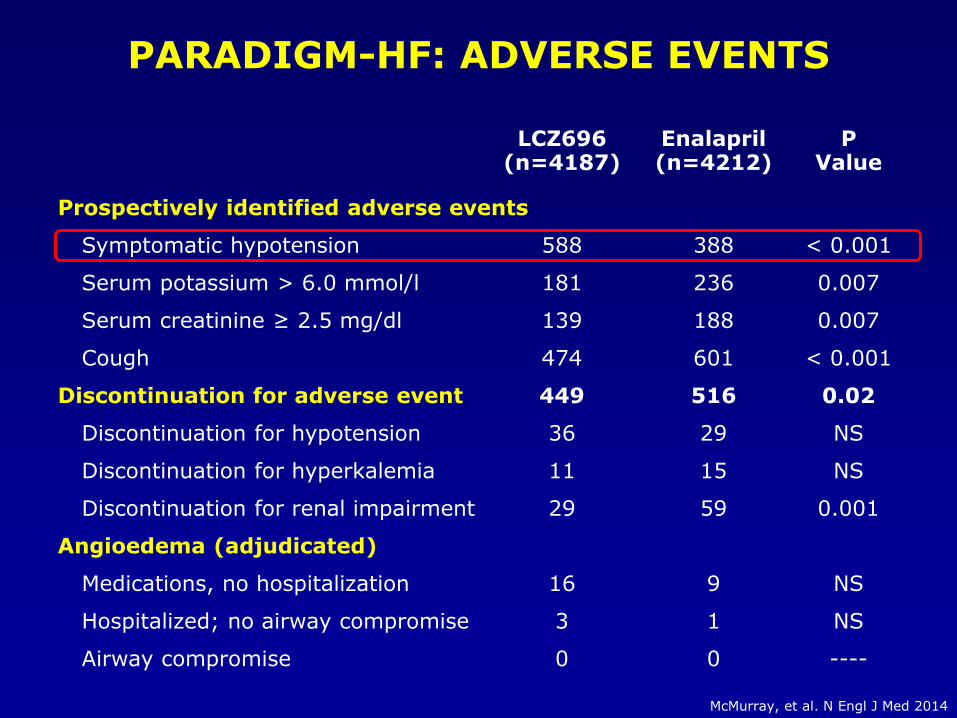
PARADIGM-HF: ADVERSE EVENTS
LCZ696(n=4187)
Enalapril(n=4212)
PValue
Prospectively identified adverse events
Symptomatic hypotension 588 388 < 0.001
Serum potassium > 6.0 mmol/l 181 236 0.007
Serum creatinine ≥ 2.5 mg/dl 139 188 0.007
Cough 474 601 < 0.001
Discontinuation for adverse event 449 516 0.02
Discontinuation for hypotension 36 29 NS
Discontinuation for hyperkalemia 11 15 NS
Discontinuation for renal impairment 29 59 0.001
Angioedema (adjudicated)
Medications, no hospitalization 16 9 NS
Hospitalized; no airway compromise 3 1 NS
Airway compromise 0 0 ----
McMurray, et al. N Engl J Med 2014


















