Fisioterapia e riabilitazione strumentale -...
32
Num. 1 | 2016 Fisioterapia e riabilitazione strumentale Casi di riabilitazione fisioterapica con l’ausilio di elettromedicali EME Scientific Lab
Transcript of Fisioterapia e riabilitazione strumentale -...

Num. 1 | 2016
Fisioterapia eriabilitazione strumentale
Casi di riabilitazione fisioterapica con l’ausilio di elettromedicali
EME Scientific Lab

Fisioterapia e riabilitazione strumentale | Num. 1 2016
EME Scientific Lab
è un open-ended project che coinvolge diverse figure professionali in ambito riabilitativo
fisioterapico sul territorio nazionale, destinato ad essere sviluppato nei prossimi anni
anche all’estero.
I professionisti che partecipano al progetto - come fisiatri, ortopedici e fisioterapisti - si
pongono, insieme ad EME, obiettivi ambiziosi:
• Offrire nel panorama internazionale della riabilitazione medicale un importante
contributo alla Evidence Based Medicine (EBM);
• Fornire precise informazioni cliniche sull’utilizzo delle tecnologie più innovative
presenti nei mercati internazionali;
• Sviluppare protocolli di lavoro sempre più efficaci ed efficienti integrando i diversi
mezzi fisici utilizzati in riabilitazione e medicina dello sport;
• Rendere gli operatori sempre più consapevoli dell’utilizzo delle tecnologie
elettromedicali come fondamentale strumento all’interno di un più ampio
programma terapeutico riabilitativo;
• Rendere più semplice e chiaro l’utilizzo delle tecnologie anche ai neofiti;
• Perfezionare le tecnologie che EME mette a disposizione dei propri clienti;
• Migliorare le performance che i professionisti della riabilitazione fisioterapica
posso garantire in termini di incremento % di risoluzione delle patologie trattate;
• Dare spazio a coloro che desiderano promuoversi, tramite l’elaborazione di casi o
studi clinici condotti con tecnologie elettromedicali EME.
Un ringraziamento sincero e particolare ai professionisti attualmente coinvolti che hanno dato un fondamentale contributoper far decollare questo progetto:
Fisioterapisti
Burini E. - Pesaro
Buscaroli M. - Imola
De Cicco M. - Pescara
Domenicucci A. - Pesaro
Gregori S. - Trento
Longobardo V. - Napoli
Romeo F. - Napoli
Corvasce M. - Torino
Medici, Ortopedici, Fisiatri
Marvulli G. - Bari
Mercusa P. - Imola
Ricchiuti M. - Pesaro

FIsioterapia e riabilitazione strumentale | Num. 1 2016
CONTENUTI
Patologie arti superiori
Trattamento di tendinite calcifica della spalla con onda d’urto 2
Trattamento di epicondilite con laser ad alta potenza 6
Trattamento di tendinopatia CLB con endodiatermia 10
Patologie arti inferiori
Trattamento di tendinite rotulea con onda d’urto 15
Trattamento di tendinite della zampa d’oca con laser ad alta potenza 19
Trattamento di distorsione di caviglia (di grado 1 e 2) con diatermia 23
EME Scientific Lab Fisioterapia e riabilitazione strumentale Num. 1 | 2016
INTRODUZIONE
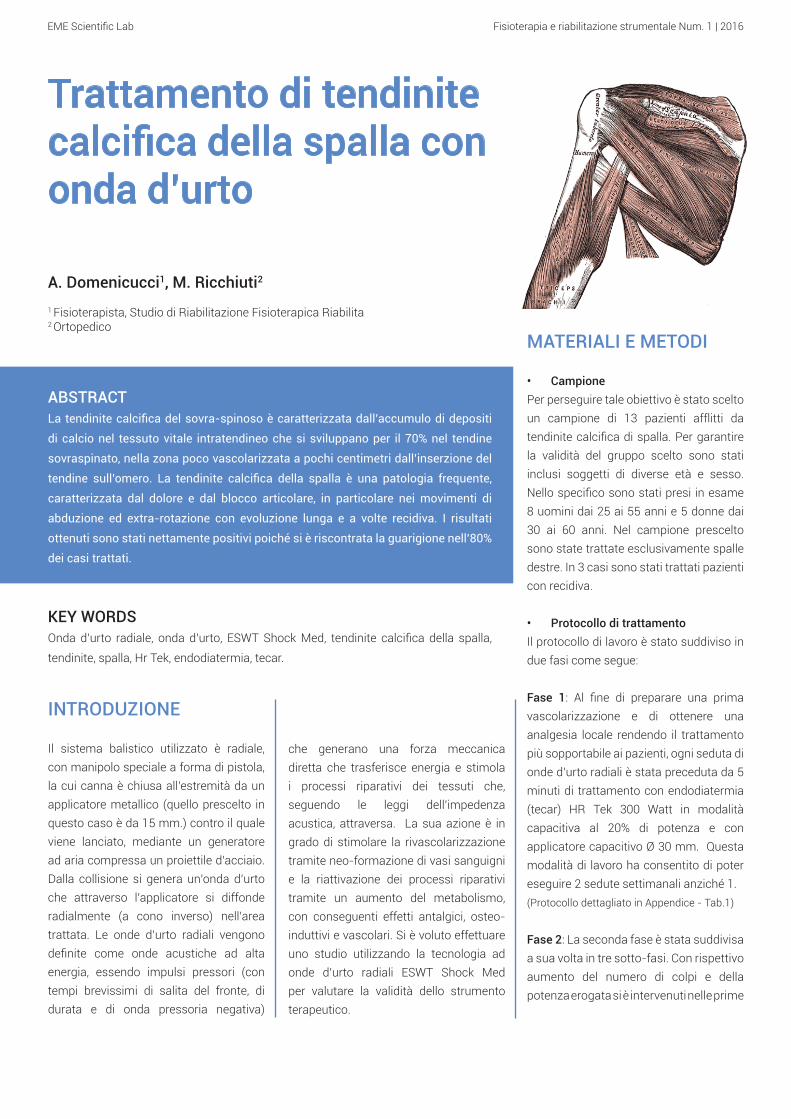
Il sistema balistico utilizzato è radiale, con manipolo speciale a forma di pistola, la cui canna è chiusa all’estremità da un applicatore metallico (quello prescelto in questo caso è da 15 mm.) contro il quale viene lanciato, mediante un generatore ad aria compressa un proiettile d’acciaio. Dalla collisione si genera un’onda d’urto che attraverso l’applicatore si diffonde radialmente (a cono inverso) nell’area trattata. Le onde d’urto radiali vengono definite come onde acustiche ad alta energia, essendo impulsi pressori (con tempi brevissimi di salita del fronte, di durata e di onda pressoria negativa)
Trattamento di tendinite calcifica della spalla con onda d’urto
A. Domenicucci1, M. Ricchiuti2
1 Fisioterapista, Studio di Riabilitazione Fisioterapica Riabilita2 Ortopedico
ABSTRACTLa tendinite calcifica del sovra-spinoso è caratterizzata dall’accumulo di depositi
di calcio nel tessuto vitale intratendineo che si sviluppano per il 70% nel tendine
sovraspinato, nella zona poco vascolarizzata a pochi centimetri dall’inserzione del
tendine sull’omero. La tendinite calcifica della spalla è una patologia frequente,
caratterizzata dal dolore e dal blocco articolare, in particolare nei movimenti di
abduzione ed extra-rotazione con evoluzione lunga e a volte recidiva. I risultati
ottenuti sono stati nettamente positivi poiché si è riscontrata la guarigione nell’80%
dei casi trattati.
KEY WORDSOnda d’urto radiale, onda d’urto, ESWT Shock Med, tendinite calcifica della spalla,
tendinite, spalla, Hr Tek, endodiatermia, tecar.
che generano una forza meccanica diretta che trasferisce energia e stimola i processi riparativi dei tessuti che, seguendo le leggi dell’impedenza acustica, attraversa. La sua azione è in grado di stimolare la rivascolarizzazione tramite neo-formazione di vasi sanguigni e la riattivazione dei processi riparativi tramite un aumento del metabolismo, con conseguenti effetti antalgici, osteo-induttivi e vascolari. Si è voluto effettuare uno studio utilizzando la tecnologia ad onde d’urto radiali ESWT Shock Med per valutare la validità dello strumento terapeutico.
MATERIALI E METODI
• CampionePer perseguire tale obiettivo è stato scelto un campione di 13 pazienti afflitti da tendinite calcifica di spalla. Per garantire la validità del gruppo scelto sono stati inclusi soggetti di diverse età e sesso. Nello specifico sono stati presi in esame 8 uomini dai 25 ai 55 anni e 5 donne dai 30 ai 60 anni. Nel campione prescelto sono state trattate esclusivamente spalle destre. In 3 casi sono stati trattati pazienti con recidiva.
• Protocollo di trattamentoIl protocollo di lavoro è stato suddiviso in due fasi come segue:
Fase 1: Al fine di preparare una prima vascolarizzazione e di ottenere una analgesia locale rendendo il trattamento più sopportabile ai pazienti, ogni seduta di onde d’urto radiali è stata preceduta da 5 minuti di trattamento con endodiatermia (tecar) HR Tek 300 Watt in modalità capacitiva al 20% di potenza e con applicatore capacitivo Ø 30 mm. Questa modalità di lavoro ha consentito di poter eseguire 2 sedute settimanali anziché 1.(Protocollo dettagliato in Appendice - Tab.1)
Fase 2: La seconda fase è stata suddivisa a sua volta in tre sotto-fasi. Con rispettivo aumento del numero di colpi e della potenza erogata si è intervenuti nelle prime
EME Scientific Lab Fisioterapia e riabilitazione strumentale Num. 1 | 2016
4. Moretti, B. et al., Medium-energy shock wave therapy in the treatment of rotator cuff calcifying tendinitis, Knee Surg Sports Traumatol Arthrosc 20055. Sabeti, M. et al., A comparison of two different treatments with navigated extracorporeal shock-wave therapy for calcifying tendinitis - a randomized controlled trial, Wien Klin Wochenschr 20076. Sabeti-Aschraf, M. et al., Extracorporeal shock wave therapy in the treatment of
2 sotto-fasi sull’articolazione della spalla interessata mentre nella terza sotto-fase ci si è concentrati prevalentemente nella zona dell’inserzione del tendine sovra-spinoso sull’omero.(Protocollo dettagliato in Appendice - Tab.2)
RISULTATI
L’utilizzo delle tecnologie e dei protocolli sopra indicati ha consentito la risoluzione dell’80% delle patologie.Aver lavorato combinando l’utilizzo dell’onda d’urto radiale con quello della endodiatermia (tecar) ha consentito di poter eseguire 2 sedute settimanali anziché 1 con accelerazione dei tempi di recupero del 200%.
CONCLUSIONI
Lo studio condotto ha dimostrato l’efficacia dell’apparecchiatura Shock Med (onda d’urto) nella risoluzione della patologia presa in esame. Inoltre, a seguito dei trattamenti effettuati e della valutazione dei risultati, è stato possibile evidenziare come la combinazione delle due tecnologie: endodiatermia e onda d’urto, abbia ridotto i tempi di recupero del 200%, assicurando un trattamento non solo efficace e al tempo stesso molto rapido.
BIBLIOGRAFIA
1. Albert, J. D. et al., High-energy extracorporeal shock-wave therapy for calcifying tendinitis of the rotator cuff: A RANDOMISED TRIAL, J Bone Joint Surg Br 20072. Cacchio, A. et al., Effectiveness of radial shock-wave therapy for calcific tendinitis of the shoulder: single-blind, randomized clinical study, Phys-Ther 20063. Hsu, C. J. et al. Extracorporeal shock wave therapy for calcifying tendinitis of the shoulder, J Shoulder Elbow Surg 2007
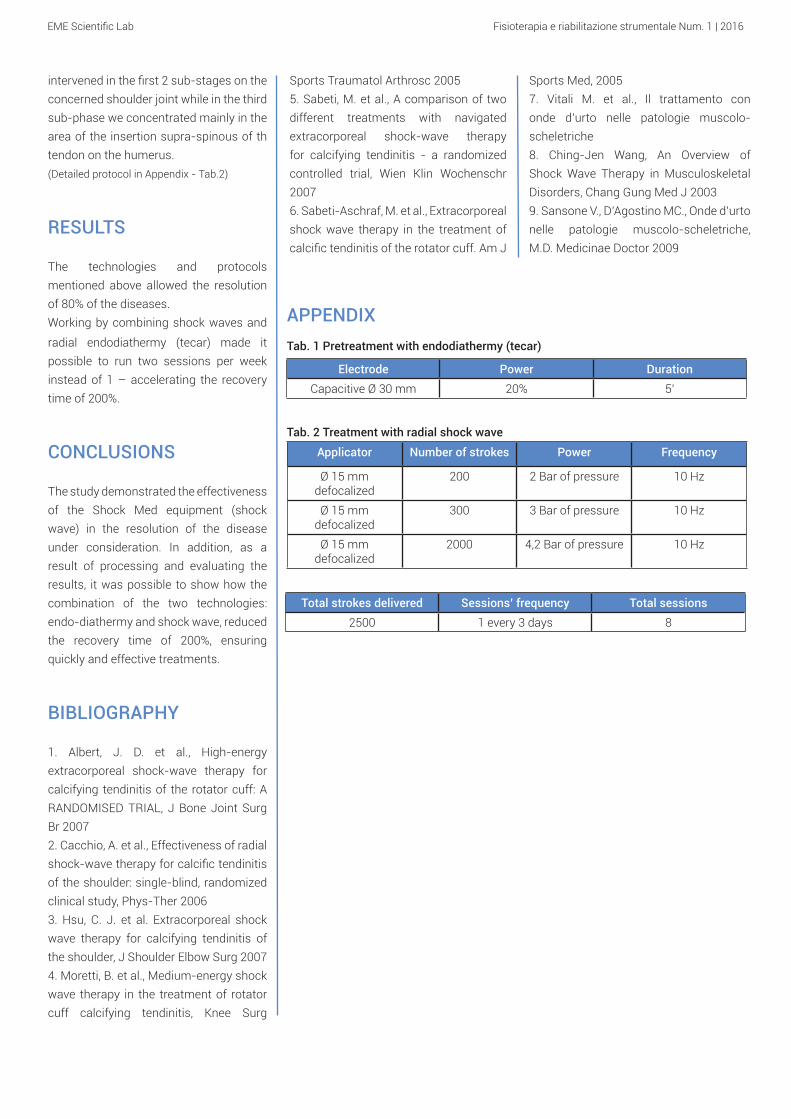
Totale colpi erogati Frequenza sedute Totale sedute2500 1 ogni 3 giorni 8
Elettrodo Potenza erogata Durata dell'applicazioneCapacitivo Ø 30 mm 20% 5’
APPENDICETab. 1 Pre-trattamento con endodiatermia (tecar)
Tab. 2 Trattamento con onda d’urto radiale
Applicatore Numero colpi erogati
Potenza di lavoro Frequenza di lavoro
Ø 15 mmDefocalizzato
200 2 Bar di pressione 10 Hz
Ø 15 mmDefocalizzato
300 3 Bar di pressione 10 Hz
Ø 15 mmDefocalizzato
2000 4,2 Bar di pressione 10 Hz
calcific tendinitis of the rotator cuff. Am J Sports Med, 20057. Vitali M. et al., Il trattamento con onde d’urto nelle patologie muscolo-scheletriche8. Ching-Jen Wang, An Overview of Shock Wave Therapy in Musculoskeletal Disorders, Chang Gung Med J 20039. Sansone V., D’Agostino MC., Onde d’urto nelle patologie muscolo-scheletriche, M.D. Medicinae Doctor 2009
EME Scientific Lab Fisioterapia e riabilitazione strumentale Num. 1 | 2016
INTRODUCTION
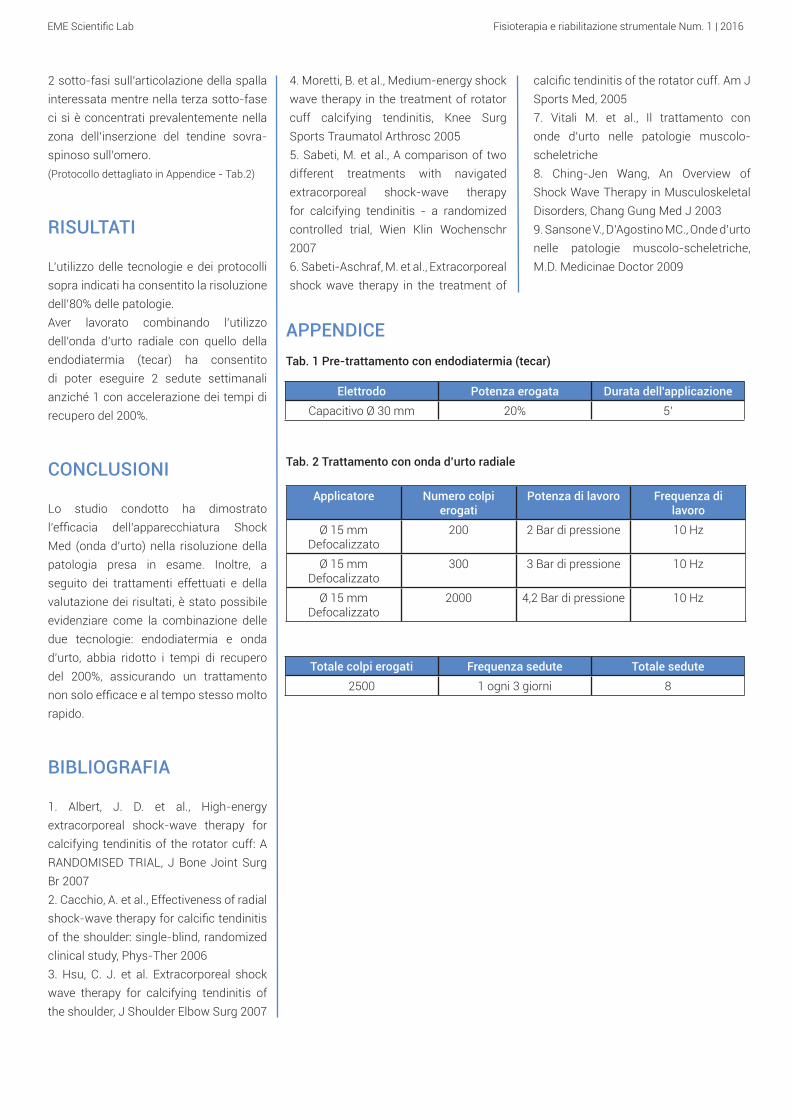
The ballistic system used is radial, with special hand-gun-shaped handpiece, whose barrel is closed at the end by a metal applicator (in this case it is 15 mm) against which is cast, by means of an air operated generator tablet, a bullet of steel. The collision generates a shock wave that spreads radially through the applicator (reverse cone) to the treated area. The radial shock waves are defined as high-energy acoustic waves, because they are like pressure pulses (with a very short time of ascent of the front, of
Treatment of calcific tendinitis of the shoulder with shock wave
A. Domenicucci1, M. Ricchiuti2
1 Physiotherapist, Studio di Riabilitazione Fisioterapica Riabilita2 Orthopedist
ABSTRACTThe calcific tendinitis of the supraspinatus is characterized by accumulation of
calcium deposits in the vital tissue intratendineo that grow 70% in the supraspinatus
tendon, in the area just a few centimeters vascularized by the insertion of the tendon
on the humerus. The calcific tendinitis of the shoulder is a frequent pathology,
characterized by pain and articular block, in particular in the movements of abduction
and extra-rotation with evolution long and sometimes relapse. The results obtained
were clearly positive since it was found healing in 80% of treated cases.
KEY WORDSRadial shock wave, shock wave, ESWT Shock Med, calcific tendinitis of the shoulder,
tendinitis, shoulder, Hr Tek, endodiathermy, tecar.
duration and negative pressure wave) that generate a direct mechanical force that transfers energy and stimulates the reparative processes of the tissues. Its action is to stimulate revascularisation by neo-formation of blood vessels and the reactivation of the healing process by increasing the metabolism, resulting in analgesic, osteo-inductive and vascular effects. We carried out a study using the radial shock wave ESWT Shock Med Compact technology to evaluate the validity of the therapeutic tool.
TOOLS AND METHODS
• SampleTo pursue this goal we selected a sample of 13 patients afflicted by calcific tendinitis of the shoulder. To ensure the validity of the chosen group we included subjects of different ages and sex. Specifically we examined 8 men from 25 to 55 years and 5 women aged 30 to 60 years. In the chosen sample we treated exclusively right shoulders. In 3 cases we treated patients with disease recurrence.
• Treatment protocolThe working protocol was divided into two phases as follows:
Phase 1: In order to prepare an initial vasculature and gain a local analgesia making treatment more tolerable to patients, each session of radial shock wave was preceded by a 5 minute
treatment with endodiathermy (tecar) HR Tek 300 watts in the capacitive mode 20% power and with capacitive applicator Ø 30 mm. This method made it possible to run two sessions per week instead of one.(Detailed protocol in Appendix - Tab.1)
Phase 2: The second phase was in turn subdivided into three sub-phases. With respective increase in the number of strokes and the supplied power we
EME Scientific Lab Fisioterapia e riabilitazione strumentale Num. 1 | 2016
Sports Traumatol Arthrosc 20055. Sabeti, M. et al., A comparison of two different treatments with navigated extracorporeal shock-wave therapy for calcifying tendinitis - a randomized controlled trial, Wien Klin Wochenschr 20076. Sabeti-Aschraf, M. et al., Extracorporeal shock wave therapy in the treatment of calcific tendinitis of the rotator cuff. Am J
intervened in the first 2 sub-stages on the concerned shoulder joint while in the third sub-phase we concentrated mainly in the area of the insertion supra-spinous of th tendon on the humerus.(Detailed protocol in Appendix - Tab.2)
RESULTS
The technologies and protocols mentioned above allowed the resolution of 80% of the diseases.Working by combining shock waves and
radial endodiathermy (tecar) made it possible to run two sessions per week instead of 1 – accelerating the recovery time of 200%.
CONCLUSIONS
The study demonstrated the effectiveness of the Shock Med equipment (shock wave) in the resolution of the disease under consideration. In addition, as a result of processing and evaluating the results, it was possible to show how the combination of the two technologies: endo-diathermy and shock wave, reduced the recovery time of 200%, ensuring quickly and effective treatments.
BIBLIOGRAPHY
1. Albert, J. D. et al., High-energy extracorporeal shock-wave therapy for calcifying tendinitis of the rotator cuff: A RANDOMISED TRIAL, J Bone Joint Surg Br 20072. Cacchio, A. et al., Effectiveness of radial shock-wave therapy for calcific tendinitis of the shoulder: single-blind, randomized clinical study, Phys-Ther 20063. Hsu, C. J. et al. Extracorporeal shock wave therapy for calcifying tendinitis of the shoulder, J Shoulder Elbow Surg 20074. Moretti, B. et al., Medium-energy shock wave therapy in the treatment of rotator cuff calcifying tendinitis, Knee Surg
Total strokes delivered Sessions’ frequency Total sessions2500 1 every 3 days 8
Electrode Power DurationCapacitive Ø 30 mm 20% 5’
APPENDIXTab. 1 Pretreatment with endodiathermy (tecar)
Tab. 2 Treatment with radial shock wave
Applicator Number of strokes Power Frequency
Ø 15 mmdefocalized
200 2 Bar of pressure 10 Hz
Ø 15 mmdefocalized
300 3 Bar of pressure 10 Hz
Ø 15 mmdefocalized
2000 4,2 Bar of pressure 10 Hz
Sports Med, 20057. Vitali M. et al., Il trattamento con onde d’urto nelle patologie muscolo-scheletriche8. Ching-Jen Wang, An Overview of Shock Wave Therapy in Musculoskeletal Disorders, Chang Gung Med J 20039. Sansone V., D’Agostino MC., Onde d’urto nelle patologie muscolo-scheletriche, M.D. Medicinae Doctor 2009
EME Scientific Lab Fisioterapia e riabilitazione strumentale Num. 1 | 2016
Trattamento di epicondilite con laserad alta potenza
M. Buscaroli1, P. Mercusa2
1 Fisioterapista, Poliambulatorio Selice 1022 Fisiatra, Poliambulatorio Selice 102
ABSTRACTL’epicondilite è un’infiammazione localizzata all’altezza dell’articolazione del
gomito. Meglio nota come gomito del tennista, è una patologia tendinea inserzionale
che colpisce l’inserzione dei muscoli epicondilei nell’epicondilo generando dolore.
Nella maggior parte dei casi di tratta di una condizione dovuta a movimenti scorretti
o sovraccarico.
Nel presente studio clinico, per il trattamento della suddetta patologia, è stato
utilizzato il laser di alta potenza Crystal Yag 25 Watt e lunghezza d’onda 1064 nm.
il quale si è dimostrato un valido strumento terapeutico conducendo i pazienti alla
totale guarigione.
KEY WORDSLaser in fibra ottica HPLS (High Power Laser System) 1064 nm, Crystal Yag 25 Watt,
epicondilite, gomito del tennista.
INTRODUZIONE
Il laser Crystal Yag da 25 Watt con lunghezza d’onda 1064 nm è un laser ad alta potenza con alta capacità di penetrazione tissutale, capace di trattare gli stati infiammatori muscolo-scheletrici superficiali e profondi. La sua azione permette di ottenere importanti effetti fotochimici sulla membrana cellulare e sui mitocondri con conseguenti effetti di stimolazione metabolica, analgesici, antiedemigeni e antiflogistici. Il presente studio si pone l’obiettivo di valutare il grado di efficacia dell’apparecchiatura Crystal Yag nella risoluzione della epicondilite.
MATERIALI E METODI
• CampioneSono stati trattati 13 pazienti afflitti da epicondilite di diverse età e sesso, nello specifico sono stati scelti 4 donne dai 32 ai 62 anni e 9 uomini dai 25 ai 69 anni.
• Protocollo di trattamentoIl protocollo di trattamento è stato suddiviso in due fasi. Entrambe le fasi sono state suddivise a loro volta in tre sottofasi seguendo la seguente modalità: riduzione della frequenza con aumento della potenza di modo da arrivare in profondità sempre maggiori con l’effetto terapeutico.
La prima fase è stata caratterizzata da una veloce scansione su tutti i distretti muscolari dell’avambraccio (estensori e flessori del polso) al fine di sciogliere la muscolatura contratta.(Protocollo dettagliato in Appendice - Tab.1)
La seconda fase è stata contraddistinta da una scansione lenta al fine di consolidare il risultato ottenuto su tutte le fasce muscolari interessate (flessori ed estensori del braccio).(Protocollo dettagliato in Appendice -Tab.2)
Le sedute sono state effettuate a giorni alterni per una durata complessiva di circa tre settimane. Nelle prime sedute si è lavorato per ridurre in maniera significativa il dolore, mentre in quelle successive ci si è focalizzati sulla risoluzione della patologia di modo da permettere ai pazienti il ritorno alle loro condizioni di normalità. La percentuale di successo è stata di 13 pazienti su 13 trattati.
RISULTATI
Al termine delle sedute previste (mediamente 9) 13 pazienti su 13 trattati hanno ottenuto una risoluzione dello stato doloroso e della patologia.
EME Scientific Lab Fisioterapia e riabilitazione strumentale Num. 1 | 2016
APPENDICE
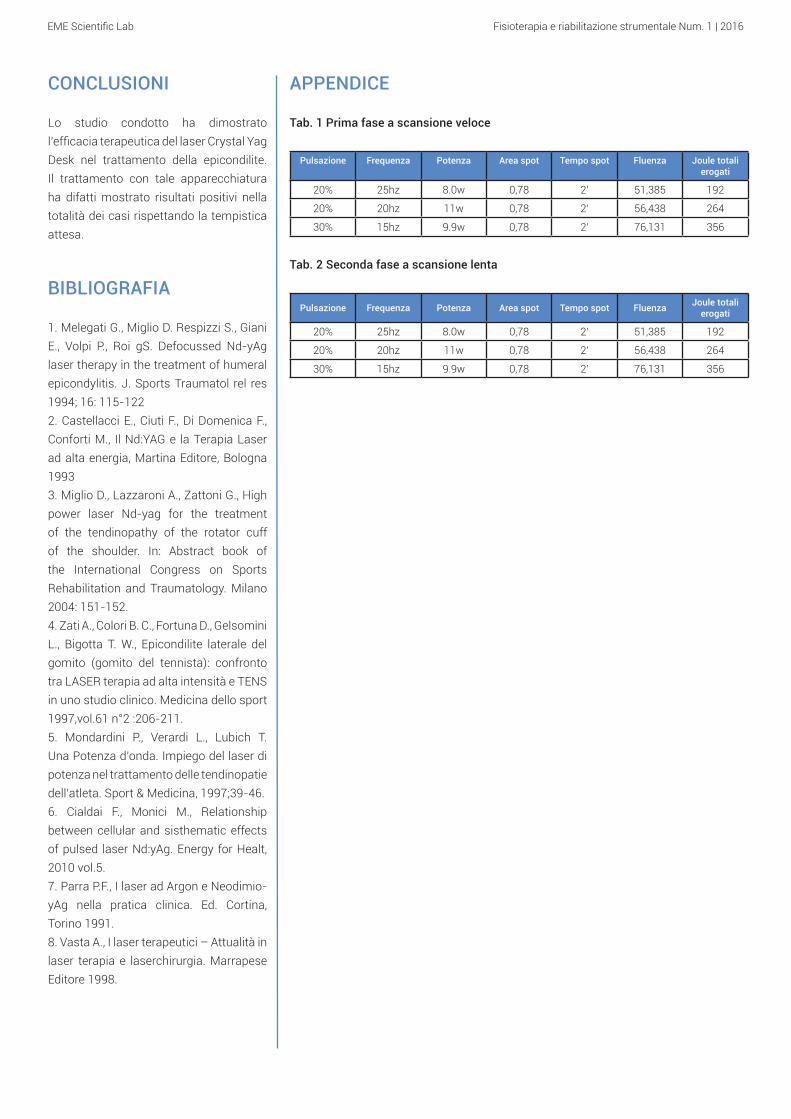
Tab. 1 Prima fase a scansione veloce
Pulsazione Frequenza Potenza Area spot Tempo spot Fluenza Joule totali erogati
20% 25hz 8.0w 0,78 2’ 51,385 192
20% 20hz 11w 0,78 2’ 56,438 264
30% 15hz 9.9w 0,78 2’ 76,131 356
Tab. 2 Seconda fase a scansione lenta
Pulsazione Frequenza Potenza Area spot Tempo spot Fluenza Joule totali erogati
20% 25hz 8.0w 0,78 2’ 51,385 192
20% 20hz 11w 0,78 2’ 56,438 264
30% 15hz 9.9w 0,78 2’ 76,131 356
CONCLUSIONI
Lo studio condotto ha dimostrato l’efficacia terapeutica del laser Crystal Yag Desk nel trattamento della epicondilite. Il trattamento con tale apparecchiatura ha difatti mostrato risultati positivi nella totalità dei casi rispettando la tempistica attesa.
BIBLIOGRAFIA
1. Melegati G., Miglio D. Respizzi S., Giani E., Volpi P., Roi gS. Defocussed Nd-yAg laser therapy in the treatment of humeral epicondylitis. J. Sports Traumatol rel res 1994; 16: 115-1222. Castellacci E., Ciuti F., Di Domenica F., Conforti M., Il Nd:YAG e la Terapia Laser ad alta energia, Martina Editore, Bologna 1993 3. Miglio D., Lazzaroni A., Zattoni G., High power laser Nd-yag for the treatment of the tendinopathy of the rotator cuff of the shoulder. In: Abstract book of the International Congress on Sports Rehabilitation and Traumatology. Milano 2004: 151-152.4. Zati A., Colori B. C., Fortuna D., Gelsomini L., Bigotta T. W., Epicondilite laterale del gomito (gomito del tennista): confronto tra LASER terapia ad alta intensità e TENS in uno studio clinico. Medicina dello sport 1997,vol.61 n°2 :206-211.5. Mondardini P., Verardi L., Lubich T. Una Potenza d’onda. Impiego del laser di potenza nel trattamento delle tendinopatie dell’atleta. Sport & Medicina, 1997;39-46.6. Cialdai F., Monici M., Relationship between cellular and sisthematic effects of pulsed laser Nd:yAg. Energy for Healt, 2010 vol.5.7. Parra P.F., I laser ad Argon e Neodimio-yAg nella pratica clinica. Ed. Cortina, Torino 1991.8. Vasta A., I laser terapeutici – Attualità in laser terapia e laserchirurgia. Marrapese Editore 1998.
EME Scientific Lab Fisioterapia e riabilitazione strumentale Num. 1 | 2016
Treatment of epicondylitis with high power laser
M. Buscaroli1, P. Mercusa2
1 Physiotherapist, Poliambulatorio Selice 1022 Physiatrist, Poliambulatorio Selice 102
ABSTRACTEpicondylitis is a localized inflammation at the elbow joint. Better known as “tennis
elbow”, it is a pathology of the insertional tendon that affects the attachment of
epicondylar muscles in the epicondyle that generates pain. In the majority of cases
is a condition due to incorrect movements or overload.
In the present clinical study, for the treatment of the above mentioned pathology,
it has been used the high power laser Crystal Yag 25 Watt with wavelength 1064
nm. which it has proved to be a valuable therapeutic tool leading patients to total
healing.
KEY WORDSFiber lasers HPLS (High Power Laser System) 1064 nm, Crystal YAG 25 Watt,
epicondylitis, tennis elbow.
INTRODUCTION
The Crystal Yag laser 25 Watt with a wavelength 1064 nm is a high power laser with high capacity of tissue penetration, capable of treating inflammatory musculoskeletal states superficially and in depth. Its action allows to obtain important photochemical effects on the cell membrane and mitochondria with consequent effects of metabolic stimulation, analgesics, anti-inflammatory and anti-edema effects. This study aims to assess the degree of effectiveness of the equipment Crystal Yag in the healing of epicondylitis.
TOOLS AND METHODS
• Sample13 patients suffering from epicondylitis of different age and sex, were specifically chosen 4 women aged 32 to 62 years and 9 men aged 25 to 69 years.
• Treatment protocolThe treatment protocol was divided into two phases. Both phases were in turn subdivided into three sub-phases according to the following mode: reduction of the frequency with increase of the power so as to arrive in ever greater depths with the therapeutic effect.
The first phase was characterized by a quick scan of all the muscle groups of the forearm (wrist flexors and extensors) in order to dissolve the contracted muscles.
(Detailed protocol in Appendix - Tab.1)
The second phase was characterized by a slow scan in order to consolidate the results obtained on all the muscles involved (flexors and extensors of the arm).
(Detailed protocol in Appendix - Tab.2)
The sessions were carried out on alternate days for a total duration of about three weeks. In the first sessions we worked to significantly reduce the pain, while in the following ones we focused on the resolution of the disease so as to allow patients to return to their normal conditions. The success rate was 13 of 13 patients treated.
RESULTS
At the end of the sessions provided (average 9) 13 of 13 patients achieved a resolution of the state of painful disease.
EME Scientific Lab Fisioterapia e riabilitazione strumentale Num. 1 | 2016
APPENDIX
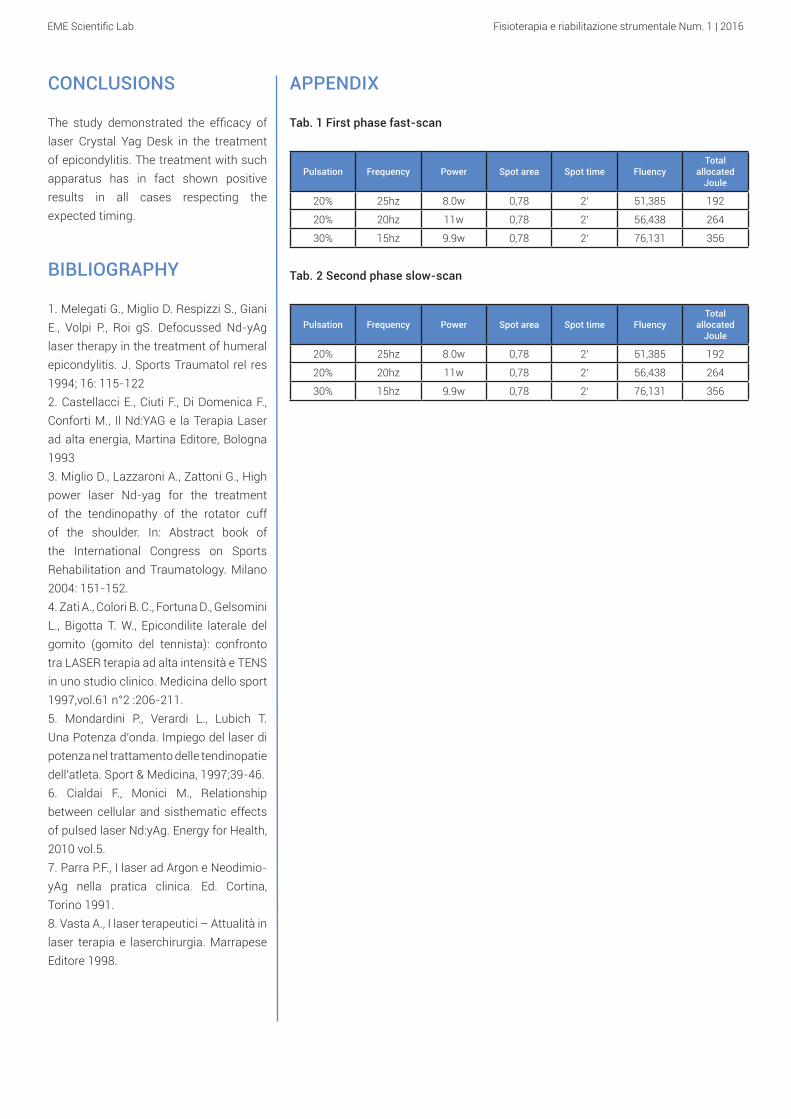
Tab. 1 First phase fast-scan
Pulsation Frequency Power Spot area Spot time FluencyTotal
allocated Joule
20% 25hz 8.0w 0,78 2’ 51,385 192
20% 20hz 11w 0,78 2’ 56,438 264
30% 15hz 9.9w 0,78 2’ 76,131 356
Tab. 2 Second phase slow-scan
Pulsation Frequency Power Spot area Spot time FluencyTotal
allocated Joule
20% 25hz 8.0w 0,78 2’ 51,385 192
20% 20hz 11w 0,78 2’ 56,438 264
30% 15hz 9.9w 0,78 2’ 76,131 356
CONCLUSIONS
The study demonstrated the efficacy of laser Crystal Yag Desk in the treatment of epicondylitis. The treatment with such apparatus has in fact shown positive results in all cases respecting the expected timing.
BIBLIOGRAPHY
1. Melegati G., Miglio D. Respizzi S., Giani E., Volpi P., Roi gS. Defocussed Nd-yAg laser therapy in the treatment of humeral epicondylitis. J. Sports Traumatol rel res 1994; 16: 115-1222. Castellacci E., Ciuti F., Di Domenica F., Conforti M., Il Nd:YAG e la Terapia Laser ad alta energia, Martina Editore, Bologna 1993 3. Miglio D., Lazzaroni A., Zattoni G., High power laser Nd-yag for the treatment of the tendinopathy of the rotator cuff of the shoulder. In: Abstract book of the International Congress on Sports Rehabilitation and Traumatology. Milano 2004: 151-152.4. Zati A., Colori B. C., Fortuna D., Gelsomini L., Bigotta T. W., Epicondilite laterale del gomito (gomito del tennista): confronto tra LASER terapia ad alta intensità e TENS in uno studio clinico. Medicina dello sport 1997,vol.61 n°2 :206-211.5. Mondardini P., Verardi L., Lubich T. Una Potenza d’onda. Impiego del laser di potenza nel trattamento delle tendinopatie dell’atleta. Sport & Medicina, 1997;39-46.6. Cialdai F., Monici M., Relationship between cellular and sisthematic effects of pulsed laser Nd:yAg. Energy for Health, 2010 vol.5.7. Parra P.F., I laser ad Argon e Neodimio-yAg nella pratica clinica. Ed. Cortina, Torino 1991.8. Vasta A., I laser terapeutici – Attualità in laser terapia e laserchirurgia. Marrapese Editore 1998.
EME Scientific Lab Fisioterapia e riabilitazione strumentale Num. 1 | 2016
INTRODUZIONE
L’endodiatermia è una terapia endogena che ha come obiettivo l’efficace e rapido recupero funzionale nelle patologie osteoarticolari e muscoloscheletriche. Si realizza attraverso il richiamo di cariche elettriche, presenti sotto forma di ioni nei tessuti, nell’area dolorante di interesse. L’interazione energia-tessuto innalza il metabolismo locale favorendo il richiamo di ossigeno quindi
Trattamento di tendinopatia CLB con endodiatermia
M. Buscaroli1, P. Mercusa2
1 Fisioterapista, Poliambulatorio Selice 1022 Fisiatra, Poliambulatorio Selice 102
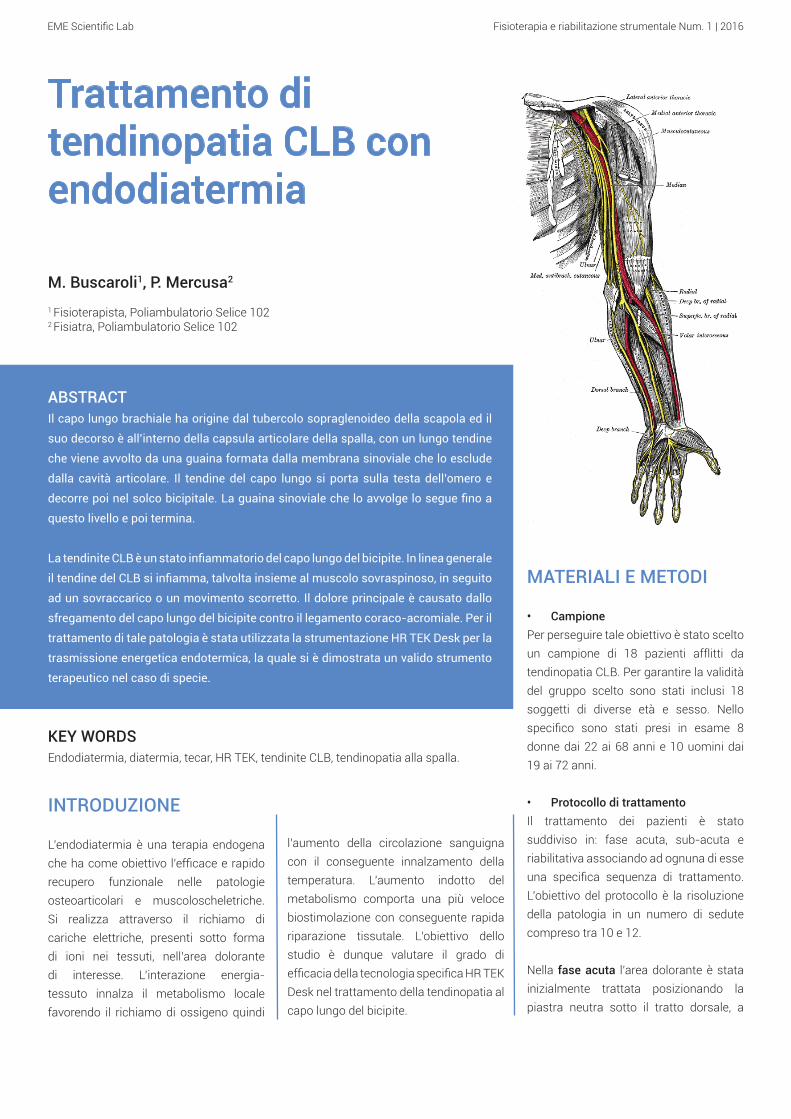
ABSTRACTIl capo lungo brachiale ha origine dal tubercolo sopraglenoideo della scapola ed il
suo decorso è all’interno della capsula articolare della spalla, con un lungo tendine
che viene avvolto da una guaina formata dalla membrana sinoviale che lo esclude
dalla cavità articolare. Il tendine del capo lungo si porta sulla testa dell’omero e
decorre poi nel solco bicipitale. La guaina sinoviale che lo avvolge lo segue fino a
questo livello e poi termina.
La tendinite CLB è un stato infiammatorio del capo lungo del bicipite. In linea generale
il tendine del CLB si infiamma, talvolta insieme al muscolo sovraspinoso, in seguito
ad un sovraccarico o un movimento scorretto. Il dolore principale è causato dallo
sfregamento del capo lungo del bicipite contro il legamento coraco-acromiale. Per il
trattamento di tale patologia è stata utilizzata la strumentazione HR TEK Desk per la
trasmissione energetica endotermica, la quale si è dimostrata un valido strumento
terapeutico nel caso di specie.
KEY WORDSEndodiatermia, diatermia, tecar, HR TEK, tendinite CLB, tendinopatia alla spalla.
l’aumento della circolazione sanguigna con il conseguente innalzamento della temperatura. L’aumento indotto del metabolismo comporta una più veloce biostimolazione con conseguente rapida riparazione tissutale. L’obiettivo dello studio è dunque valutare il grado di efficacia della tecnologia specifica HR TEK Desk nel trattamento della tendinopatia al capo lungo del bicipite.
MATERIALI E METODI
• CampionePer perseguire tale obiettivo è stato scelto un campione di 18 pazienti afflitti da tendinopatia CLB. Per garantire la validità del gruppo scelto sono stati inclusi 18 soggetti di diverse età e sesso. Nello specifico sono stati presi in esame 8 donne dai 22 ai 68 anni e 10 uomini dai 19 ai 72 anni.
• Protocollo di trattamentoIl trattamento dei pazienti è stato suddiviso in: fase acuta, sub-acuta e riabilitativa associando ad ognuna di esse una specifica sequenza di trattamento. L’obiettivo del protocollo è la risoluzione della patologia in un numero di sedute compreso tra 10 e 12.
Nella fase acuta l’area dolorante è stata inizialmente trattata posizionando la piastra neutra sotto il tratto dorsale, a
EME Scientific Lab Fisioterapia e riabilitazione strumentale Num. 1 | 2016
lungo del bicipite mantenendo la piastra neutra sotto la scapola omolaterale. Tale fase ha avuto durata pari a 10’. Successivamente si è posizionato l’elettrodo sul CLB ad una potenza del 15% chiedendo al paziente di effettuare esercizi: di estensione di controresistenza per rafforzare il tricipite brachiale (3-4 serie da 10 ripetizioni), muscolari eccentrici (2-3 serie da 10 ripetizioni) e di flessione ponendo resistenza per far lavorare il muscolo in fase concentrica (2-3 serie da 10 ripetizioni). Successivamente si è proceduto con l’utilizzo dell’elettrodo capacitivo ad una potenza del 50-60% (effetto termico non rilevante) massaggiando per 10’ i muscoli deltoide, tricipite e bicipite al fine di defaticarli.
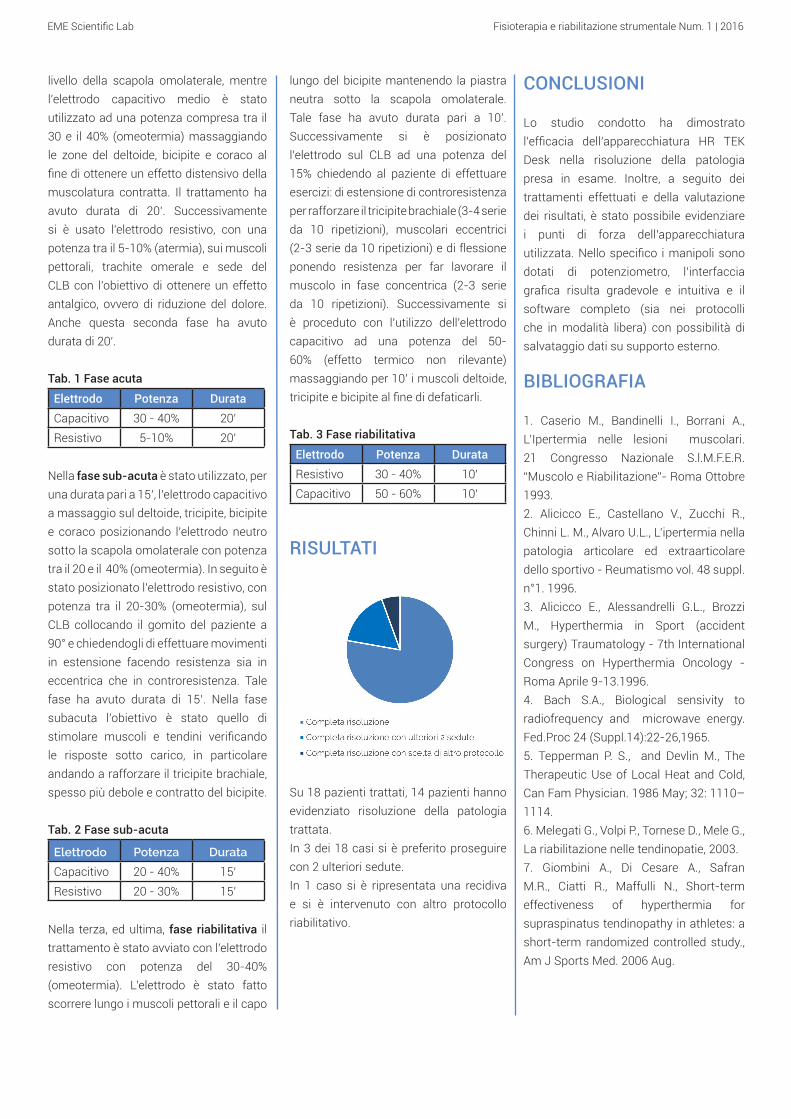
Tab. 3 Fase riabilitativa
Elettrodo Potenza DurataResistivo 30 - 40% 10’Capacitivo 50 - 60% 10’
RISULTATI
Su 18 pazienti trattati, 14 pazienti hanno evidenziato risoluzione della patologia trattata. In 3 dei 18 casi si è preferito proseguire con 2 ulteriori sedute. In 1 caso si è ripresentata una recidiva e si è intervenuto con altro protocollo riabilitativo.
livello della scapola omolaterale, mentre l’elettrodo capacitivo medio è stato utilizzato ad una potenza compresa tra il 30 e il 40% (omeotermia) massaggiando le zone del deltoide, bicipite e coraco al fine di ottenere un effetto distensivo della muscolatura contratta. Il trattamento ha avuto durata di 20’. Successivamente si è usato l’elettrodo resistivo, con una potenza tra il 5-10% (atermia), sui muscoli pettorali, trachite omerale e sede del CLB con l’obiettivo di ottenere un effetto antalgico, ovvero di riduzione del dolore. Anche questa seconda fase ha avuto durata di 20’.
Tab. 1 Fase acuta
Elettrodo Potenza DurataCapacitivo 30 - 40% 20’Resistivo 5-10% 20’
Nella fase sub-acuta è stato utilizzato, per una durata pari a 15’, l’elettrodo capacitivo a massaggio sul deltoide, tricipite, bicipite e coraco posizionando l’elettrodo neutro sotto la scapola omolaterale con potenza tra il 20 e il 40% (omeotermia). In seguito è stato posizionato l’elettrodo resistivo, con potenza tra il 20-30% (omeotermia), sul CLB collocando il gomito del paziente a 90° e chiedendogli di effettuare movimenti in estensione facendo resistenza sia in eccentrica che in controresistenza. Tale fase ha avuto durata di 15’. Nella fase subacuta l’obiettivo è stato quello di stimolare muscoli e tendini verificando le risposte sotto carico, in particolare andando a rafforzare il tricipite brachiale, spesso più debole e contratto del bicipite.
Tab. 2 Fase sub-acuta
Elettrodo Potenza Durata
Capacitivo 20 - 40% 15’Resistivo 20 - 30% 15’
Nella terza, ed ultima, fase riabilitativa il trattamento è stato avviato con l’elettrodo resistivo con potenza del 30-40% (omeotermia). L’elettrodo è stato fatto scorrere lungo i muscoli pettorali e il capo
CONCLUSIONI
Lo studio condotto ha dimostrato l’efficacia dell’apparecchiatura HR TEK Desk nella risoluzione della patologia presa in esame. Inoltre, a seguito dei trattamenti effettuati e della valutazione dei risultati, è stato possibile evidenziare i punti di forza dell’apparecchiatura utilizzata. Nello specifico i manipoli sono dotati di potenziometro, l’interfaccia grafica risulta gradevole e intuitiva e il software completo (sia nei protocolli che in modalità libera) con possibilità di salvataggio dati su supporto esterno.
BIBLIOGRAFIA
1. Caserio M., Bandinelli I., Borrani A., L’Ipertermia nelle lesioni muscolari. 21 Congresso Nazionale S.l.M.F.E.R. “Muscolo e Riabilitazione”- Roma Ottobre 1993.2. Alicicco E., Castellano V., Zucchi R., Chinni L. M., Alvaro U.L., L’ipertermia nella patologia articolare ed extraarticolare dello sportivo - Reumatismo vol. 48 suppl. n°1. 1996. 3. Alicicco E., Alessandrelli G.L., Brozzi M., Hyperthermia in Sport (accident surgery) Traumatology - 7th International Congress on Hyperthermia Oncology - Roma Aprile 9-13.1996. 4. Bach S.A., Biological sensivity to radiofrequency and microwave energy. Fed.Proc 24 (Suppl.14):22-26,1965.5. Tepperman P. S., and Devlin M., The Therapeutic Use of Local Heat and Cold, Can Fam Physician. 1986 May; 32: 1110–1114.6. Melegati G., Volpi P., Tornese D., Mele G., La riabilitazione nelle tendinopatie, 2003.7. Giombini A., Di Cesare A., Safran M.R., Ciatti R., Maffulli N., Short-term effectiveness of hyperthermia for supraspinatus tendinopathy in athletes: a short-term randomized controlled study., Am J Sports Med. 2006 Aug.

EME Scientific Lab Fisioterapia e riabilitazione strumentale Num. 1 | 2016
INTRODUCTION
The endodiathermy is an endogenous therapy which aims the effective and rapid functional recovery in bone, joint and musculoskeletal diseases. It is implemented through the call of electric charges, present in the form of ions in the tissues, in the injured area of interest. The energy-tissue interaction raises the local metabolism favoring the recall of oxygen
so the increase in blood circulation with the consequent rise in temperature. The induced increase in metabolism results in faster bio-stimulation resulting in rapid tissue repair. The aim of the study was therefore to evaluate the effectiveness of the specific technology HR TEK Desk
treating tendinopathy of the long head of
the biceps brachii muscle.
TOOLS AND METHODS
• SampleTo pursue this goal has been selected a sample of 18 patients suffering from LHB tendonitis. To ensure the validity of the chosen group we included 18 persons of different age and sex. Specifically, we examined 8 women aged 22 to 68 years and 10 men aged 19 to 72 years.
• Treatment protocolThe treatment has been divided into: acute, sub-acute and rehabilitative phase associating to each of them a specific treatment sequence. The objective of the protocol is the resolution of the pathology in a number of sessions between 10 and 12.
In the acute phase the pain area was initially treated by placing the neutral plate below the shoulder portion at the level of the ipsilateral scapula, while the medium
Treatment of LHB tendonitis withendodiathermy
M. Buscaroli1, P. Mercusa2
1 Physiotherapist, Poliambulatorio Selice 1022 Physiatrist, Poliambulatorio Selice 102
ABSTRACTThe long head of the biceps brachii muscle originates from supraglenoid tubercle of
the scapula and it runs inside the joint capsule of the shoulder, with a long tendon
that is wrapped in a sheath formed by the synovial membrane that excludes it from
the joint cavity. The tendon of the long head of the biceps brachii muscle moves to
the head of the humerus and runs then in the bicipital groove. The synovial sheath
that surrounds it follows up to this level and then ends.
LHB tendonitis is an inflammatory condition of the long head. In general, the LHB
tendon becomes inflamed, sometimes with the supraspinatus muscle, as a result
of an overload or an incorrect movement. The main pain is caused by the rubbing
of the long head against the coracoacromial ligament. For the treatment of this
pathology has been used HR TEK Desk for endothermic energy transmission, which
has proved to be a valuable therapeutic tool in the present case.
KEY WORDSEndodiathermy, diathermy, tecar, HR TEK, LHB tendonitis, shoulder tendonitis.

EME Scientific Lab Fisioterapia e riabilitazione strumentale Num. 1 | 2016
the electrode was positioned on the LHB with a power of 15% asking the patient to perform exercises: extension, against resistance, to strengthen the brachial triceps (3-4 sets of 10 repetitions), muscular eccentrics (2-3 sets of 10 repetitions) and flexural strength by putting resistance on the muscle that works in the concentric phase (2-3 sets of 10 repetitions). Afterwards, we proceeded with the capacitive electrode with a power of 50-60% (thermal effect not significant) massaging for 10’ the deltoid muscles, triceps and biceps in order to decompress them.
Tab. 3 Rehabilitative phase
Electrode Power DurationResistive 30 - 40% 10’Capacitive 50 - 60% 10’
RESULTS
capacitive electrode was used at a power of between 30 and 40% (homeothermy) massaging the areas of the deltoid, biceps and coraco in order to obtain a relaxing effect of the muscles contracted. The treatment had lasting 20’. We later used the resistive electrode, with an output between 5-10% (athermy), on pectoral muscles, humeral trachyte and seat of LHB in order to obtain an analgesic effect. Even this second phase lasted 20’.
Tab. 1 Acute phase
Electrode Power DurationCapacitive 30 - 40% 20’Resistive 5-10% 20’
During the sub-acute phase has been used, for a duration of 15’, the capacitive electrode massaging the deltoid, triceps, biceps and coraco placing the electrode under the ipsilateral scapula with power between 20 and 40% (homeothermy). It has subsequently been positioned the resistive electrode, with a power range of 20-30% (homeothermy), on LHB placing the patient’s elbow at 90° and asking him to perform extension movements doing resistance in both eccentric and counterforce. This phase has had a duration of 15’. In the sub-acute phase the aim was to stimulate the muscles and tendons by checking the answers under load, especially going to strengthen the brachial triceps, often weaker and more contracted than the biceps.
Tab. 2 Sub-acute phase
Electrode Power DurationCapacitive 20 - 40% 15’
Resistive 20 - 30% 15’
During the third and last rehabilitative phase, the treatment started with the resistive electrode with a power of 30-40% (homeothermy). The electrode slid along the pectoral muscles and long head biceps muscle maintaining the neutral plate under the ipsilateral scapula . This phase has had a duration of 10’. Subsequently,
the treatments and the results evaluation, it has been possible to highlight the strengths of the equipment used. Specifically, the handles are provided with potentiometer, the GUI is attractive, intuitive and the software is complete (both with protocols and free mode) with the possibility of saving data on external support.
BIBLIOGRAPHY
1. Caserio M., Bandinelli I., Borrani A., L’Ipertermia nelle lesioni muscolari. 21 Congresso Nazionale S.l.M.F.E.R. “Muscolo e Riabilitazione”- Roma Ottobre 1993.2. Alicicco E., Castellano V., Zucchi R., Chinni L. M., Alvaro U.L., L’ipertermia nella patologia articolare ed extraarticolare dello sportivo - Reumatismo vol. 48 suppl. n°1. 1996. 3. Alicicco E., Alessandrelli G.L., Brozzi M., Hyperthermia in Sport (accident surgery) Traumatology - 7th International Congress on Hyperthermia Oncology - Roma Aprile 9-13.1996. 4. Bach S.A., Biological sensivity to radiofrequency and microwave energy. Fed.Proc 24 (Suppl.14):22-26,1965.5. Tepperman P. S., and Devlin M., The Therapeutic Use of Local Heat and Cold, Can Fam Physician. 1986 May; 32: 1110–1114.6. Melegati G., Volpi P., Tornese D., Mele G., La riabilitazione nelle tendinopatie, 2003.7. Giombini A., Di Cesare A., Safran M.R., Ciatti R., Maffulli N., Short-term effectiveness of hyperthermia for supraspinatus tendinopathy in athletes: a short-term randomized controlled study., Am J Sports Med. 2006 Aug.
14 patients out of 18 patients treated showed resolution of the condition treated.In 3 of the 18 cases it was decided to proceed with 2 further sessions.In 1 case it has been necessary to change the rehabilitation protocol.
CONCLUSIONS
The study demonstrated the effectiveness of the equipment TEK HR Desk in resolving the disease under consideration. In addition, as a result of

EME Scientific Lab Fisioterapia e riabilitazione strumentale Num. 1 | 2016
INTRODUZIONE
Il sistema balistico utilizzato è radiale, con manipolo speciale a forma di pistola, la cui canna è chiusa all’estremità da un applicatore metallico (quello prescelto in questo caso è da 15 mm.) contro il quale viene lanciato, mediante un generatore ad aria compressa, un proiettile d’acciaio. Dalla collisione si genera un’onda d’urto che attraverso l’applicatore si diffonde radialmente (a cono inverso) nell’area trattata. Le onde d’urto radiali vengono definite come onde acustiche ad alta energia, essendo impulsi pressori (con
Trattamento di tendinite rotulea con onda d’urto
A. Domenicucci1, M. Ricchiuti2
1 Fisioterapista, Studio di Riabilitazione Fisioterapica Riabilita2 Ortopedico
ABSTRACTIl tendine rotuleo collega, nell’articolazione del ginocchio, la rotula con la tuberosità
della tibia (parte superiore della tibia) ed è la porzione distale del tendine comune
del quadricipite femorale. É un tendine dalla forma piatta, resistente, lungo circa 8
cm e largo 3,4 cm. La sua porzione centrale (terzo centrale) può essere utilizzata
negli interventi di ricostruzione del legamento crociato anteriore.
Per tendinite si intende una infiammazione del tendine, ma il termine più corretto
da usare sarebbe “peritendinite”, cioè infiammazione del peritenonio, una sottile
lamina connettivale a fibre intrecciate che avvolge tutto il tendine. Questa patologia,
molto comune fra gli sportivi, è dovuta ad un continuo sollecitamento anormale
ed intenso. Lo studio clinico presenta eccellenti risultati poiché si è riscontrata la
guarigione nell’85% dei casi trattati.
KEY WORDSOnda d’urto radiale, onda d’urto, ESWT Shock Med Compact, tendinite rotulea,
tendinite, ginocchio, HLLT, Crystal Yag Desk, laser 1064 nm.
tempi brevissimi di salita del fronte, di durata e di onda pressoria negativa) che generano una forza meccanica diretta che trasferisce energia e stimola i processi riparativi dei tessuti che, seguendo le leggi dell’impedenza acustica, attraversa. La sua azione è in grado di stimolare la rivascolarizzazione tramite neo-formazione di vasi sanguigni e la riattivazione dei processi riparativi tramite un aumento del metabolismo, con conseguenti effetti antalgici, osteo-induttivi e vascolari. Si è voluto effettuare
uno studio utilizzando la tecnologia ad onde d’urto radiali ESWT Shock Med Compact per valutare la validità dello strumento terapeutico.
MATERIALI E METODI
• CampionePer perseguire tale obiettivo è stato scelto un campione di 10 pazienti afflitti da tendinite rotulea. Per garantire la validità del gruppo scelto sono stati inclusi soggetti di diverse età e sesso. Nello specifico sono stati presi in esame pazienti tra i 25 ed i 45 anni.
• Protocollo di trattamentoIl protocollo di lavoro è stato suddiviso in due fasi come segue:
Fase 1: La prima fase è stata suddivisa a sua volta in tre sotto-fasi, con rispettivo aumento del numero di colpi e della potenza erogata concentrandosi sul tendine rotuleo.(Protocollo dettagliato in Appendice - Tab.1)

EME Scientific Lab Fisioterapia e riabilitazione strumentale Num. 1 | 2016
3. Ching-Jen Wang, An Overview of Shock Wave Therapy in Musculoskeletal Disorders, Chang Gung Med J 20034. Sansone V., D’Agostino MC., Onde d’urto nelle patologie muscolo-scheletriche, M.D. Medicinae Doctor 2009 5. Hsu RW, Hsu WH, Tai CL, Lee KF, Effect of shock-wave therapy on patellar tendinopathy in a rabbit model, J Orthop Res. 2004 6. J.E. Taunton, MD, K.M. Taunton, BSc, K.M. Khan, Treatment of patellar tendinopathy with extracorporeal shock
Fase 2: Al fine di stimolare ulteriormente la vascolarizzazione del distretto interessato e per ottenere una migliore analgesia locale rendendo il post-trattamento più sopportabile ai pazienti, ogni seduta di onde d’urto radiali è stata succeduta da 2 minuti di trattamento con laser di alta potenza Crystal Yag Desk 12 Watt 1064 nm.Questa modalità di lavoro ha consentito di poter eseguire 2 sedute settimanali anziché 1.(Protocollo dettagliato in Appendice - Tab.2)
RISULTATI
L’utilizzo delle tecnologie e dei protocolli sopra indicati ha consentito la risoluzione dell’85% delle patologie. Aver lavorato combinando l’utilizzo dell’onda d’urto radiale con quello del laser ha consentito di poter eseguire 2 sedute settimanali anziché 1 con accelerazione dei tempi di recupero del 200%.
CONCLUSIONI
Lo studio condotto ha dimostrato l’efficacia dell’apparecchiatura Shock Med Compact nella risoluzione della patologia presa in esame, nel rispetto dei tempi attesi. Inoltre grazie al ricorso al laser di alta potenza (nello specifico Crystal Yag 1064 nm) si è riusciti nell’intento di accelerare i tempi di recupero garantendo ai pazienti la guarigione in 8 sedute con onda d’urto radiale accompagnate da 2 sedute post-trattamento con laser ad alta potenza.
BIBLIOGRAFIA
1. Wang, C. J. et al., Extracorporeal shockwave for chronic patellar tendinopathy, Am J Sports Med 20072. Vitali M. et al., Il trattamento con onde d’urto nelle patologie muscolo-scheletriche
wave therapy, BCMJ 20037. MT van Leeuwen, J Zwerver, I van den Akker-Scheek, Extracorporeal shockwave therapy for patellar tendinopathy: a review of the literature, Br J Sports Med 20098. Peers KH, Lysens RJ, Brys P, Bellemans J., Cross-sectional outcome analysis of athletes with chronic patellar tendinopathy treated surgically and by extracorporeal shock wave therapy, Clin J Sport Med. 2003
APPENDICE
Tab. 1 Trattamento con onda d’urto radiale
Tab. 2 Post-trattamento con HLLT
Applicatore Numero colpi erogati Potenza di lavoro Frequenza di
lavoro
Ø 15 mmDefocalizzato 200 1,5 Bar di pressione 8 Hz
Ø 15 mm Defocalizzato 300 2,5 Bar di pressione 8 Hz
Ø 15 mm Defocalizzato 1300 3,2 Bar di pressione 8 Hz
Totale colpi erogati Frequenza sedute Totale sedute1800 1 ogni 3 giorni 8
Frequenza Densità Durata dell'applicazione5000 Hz 3,5 J x cm2 2’
EME Scientific Lab Fisioterapia e riabilitazione strumentale Num. 1 | 2016
INTRODUCTION
The ballistic system used is radial, with special hand-gun-shaped handpiece, whose barrel is closed at the end by a metal applicator (in this case it is 15 mm) against which is cast, by means of an air operated generator tablet, a bullet of steel. The collision generates a shock wave that spreads radially through the applicator (reverse cone) to the treated area. The radial shock waves are defined as high-energy acoustic waves, because they are like pressure pulses (with a very short time of ascent of the front, of
Treatment of patellar tendinitis with shock waveA. Domenicucci1, M. Ricchiuti2 1 Physiotherapist, Studio di Riabilitazione Fisioterapica Riabilita2 Orthopedist
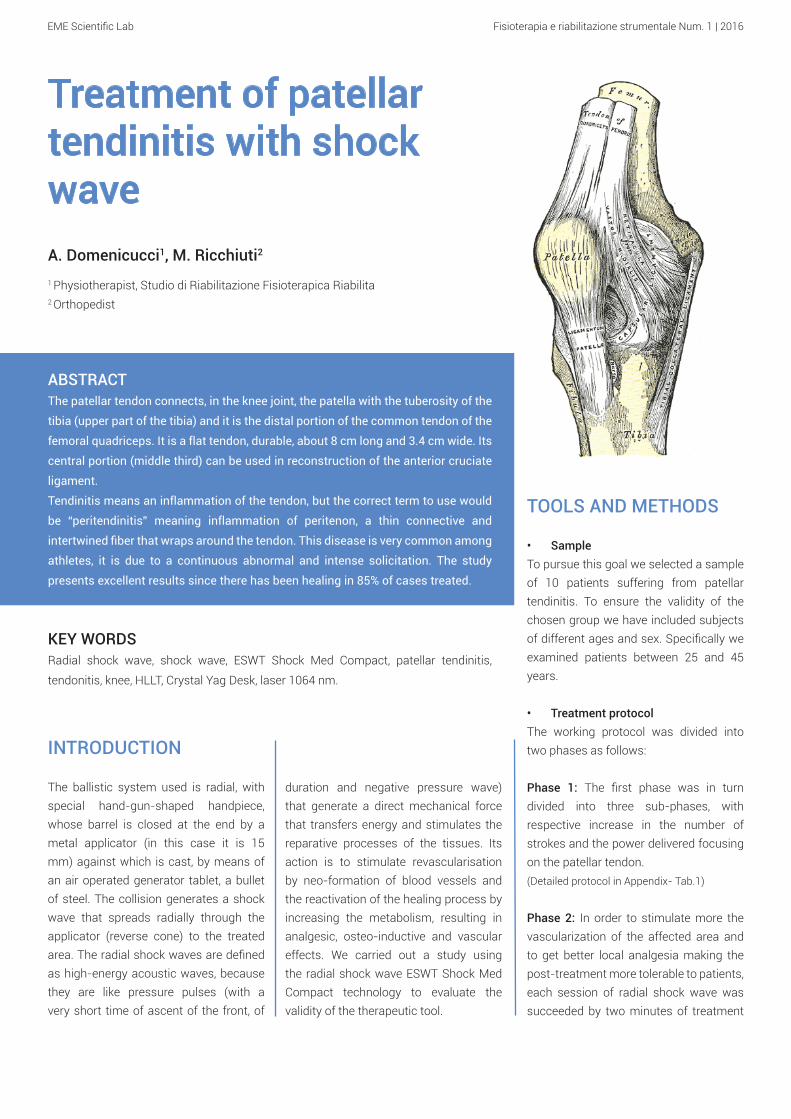
ABSTRACTThe patellar tendon connects, in the knee joint, the patella with the tuberosity of the
tibia (upper part of the tibia) and it is the distal portion of the common tendon of the
femoral quadriceps. It is a flat tendon, durable, about 8 cm long and 3.4 cm wide. Its
central portion (middle third) can be used in reconstruction of the anterior cruciate
ligament.
Tendinitis means an inflammation of the tendon, but the correct term to use would
be “peritendinitis” meaning inflammation of peritenon, a thin connective and
intertwined fiber that wraps around the tendon. This disease is very common among
athletes, it is due to a continuous abnormal and intense solicitation. The study
presents excellent results since there has been healing in 85% of cases treated.
KEY WORDSRadial shock wave, shock wave, ESWT Shock Med Compact, patellar tendinitis,
tendonitis, knee, HLLT, Crystal Yag Desk, laser 1064 nm.
duration and negative pressure wave) that generate a direct mechanical force that transfers energy and stimulates the reparative processes of the tissues. Its action is to stimulate revascularisation by neo-formation of blood vessels and the reactivation of the healing process by increasing the metabolism, resulting in analgesic, osteo-inductive and vascular effects. We carried out a study using the radial shock wave ESWT Shock Med Compact technology to evaluate the validity of the therapeutic tool.
TOOLS AND METHODS
• SampleTo pursue this goal we selected a sample of 10 patients suffering from patellar tendinitis. To ensure the validity of the chosen group we have included subjects of different ages and sex. Specifically we examined patients between 25 and 45 years.
• Treatment protocolThe working protocol was divided into two phases as follows:
Phase 1: The first phase was in turn divided into three sub-phases, with respective increase in the number of strokes and the power delivered focusing on the patellar tendon.(Detailed protocol in Appendix- Tab.1)
Phase 2: In order to stimulate more the vascularization of the affected area and to get better local analgesia making the post-treatment more tolerable to patients, each session of radial shock wave was succeeded by two minutes of treatment
EME Scientific Lab Fisioterapia e riabilitazione strumentale Num. 1 | 2016
Res. 2004 6. J.E. Taunton, MD, K.M. Taunton, BSc, K.M. Khan, Treatment of patellar tendinopathy with extracorporeal shock wave therapy, BCMJ 20037. MT van Leeuwen, J Zwerver, I van den Akker-Scheek, Extracorporeal shockwave therapy for patellar tendinopathy: a review
with high-power laser Crystal Yag Desk 12 Watt 1064 nm.This method made it possible to run two sessions per week instead of 1.(Detailed protocol in Appendix - Tab.1)
RESULTS
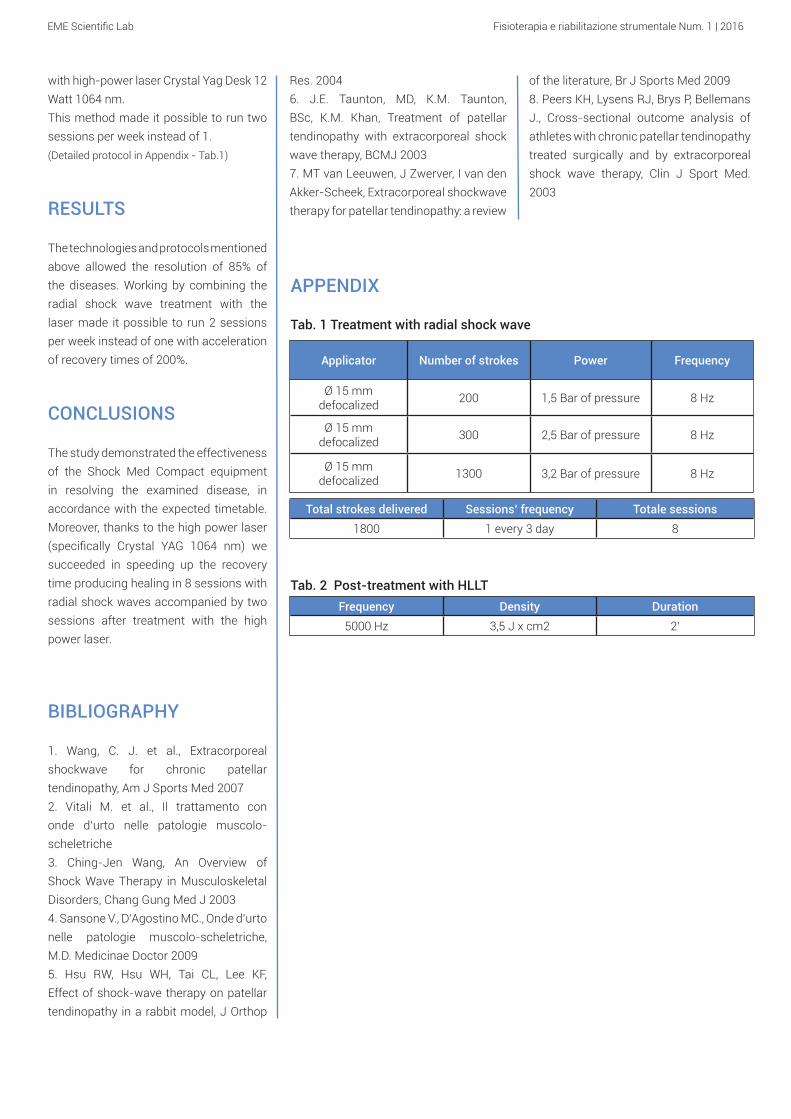
The technologies and protocols mentioned above allowed the resolution of 85% of the diseases. Working by combining the radial shock wave treatment with the laser made it possible to run 2 sessions per week instead of one with acceleration of recovery times of 200%.
CONCLUSIONS
The study demonstrated the effectiveness of the Shock Med Compact equipment in resolving the examined disease, in accordance with the expected timetable. Moreover, thanks to the high power laser (specifically Crystal YAG 1064 nm) we succeeded in speeding up the recovery time producing healing in 8 sessions with radial shock waves accompanied by two sessions after treatment with the high power laser.
BIBLIOGRAPHY
1. Wang, C. J. et al., Extracorporeal shockwave for chronic patellar tendinopathy, Am J Sports Med 20072. Vitali M. et al., Il trattamento con onde d’urto nelle patologie muscolo-scheletriche3. Ching-Jen Wang, An Overview of Shock Wave Therapy in Musculoskeletal Disorders, Chang Gung Med J 20034. Sansone V., D’Agostino MC., Onde d’urto nelle patologie muscolo-scheletriche, M.D. Medicinae Doctor 2009 5. Hsu RW, Hsu WH, Tai CL, Lee KF, Effect of shock-wave therapy on patellar tendinopathy in a rabbit model, J Orthop
of the literature, Br J Sports Med 20098. Peers KH, Lysens RJ, Brys P, Bellemans J., Cross-sectional outcome analysis of athletes with chronic patellar tendinopathy treated surgically and by extracorporeal shock wave therapy, Clin J Sport Med. 2003
APPENDIX
Tab. 1 Treatment with radial shock wave
Tab. 2 Post-treatment with HLLT
Applicator Number of strokes Power Frequency
Ø 15 mmdefocalized 200 1,5 Bar of pressure 8 Hz
Ø 15 mm defocalized 300 2,5 Bar of pressure 8 Hz
Ø 15 mm defocalized 1300 3,2 Bar of pressure 8 Hz
Total strokes delivered Sessions’ frequency Totale sessions1800 1 every 3 day 8
Frequency Density Duration 5000 Hz 3,5 J x cm2 2’
EME Scientific Lab Fisioterapia e riabilitazione strumentale Num. 1 | 2016
INTRODUZIONE
Il laser Crystal Yag da 25 Watt con lunghezza d’onda 1064 nm è un laser ad alta potenza con alta capacità di penetrazione tissutale, capace di trattare gli stati infiammatori muscolo-scheletrici superficiali e profondi. La sua azione permette di ottenere importanti effetti fotochimici sulla membrana cellulare e sui mitocondri con conseguenti effetti di stimolazione metabolica, analgesici, antiedemigeni e antiflogistici. Il presente studio si pone l’obiettivo di valutare il grado di efficacia dell’apparecchiatura Crystal Yag Desk nella risoluzione della tendinite della zampa d’oca.
Trattamento di tendinite della zampa d’oca con laser ad altapotenzaM. Buscaroli1, P. Mercusa2
1 Fisioterapista, Poliambulatorio Selice 1022 Fisiatra, Poliambulatorio Selice 102
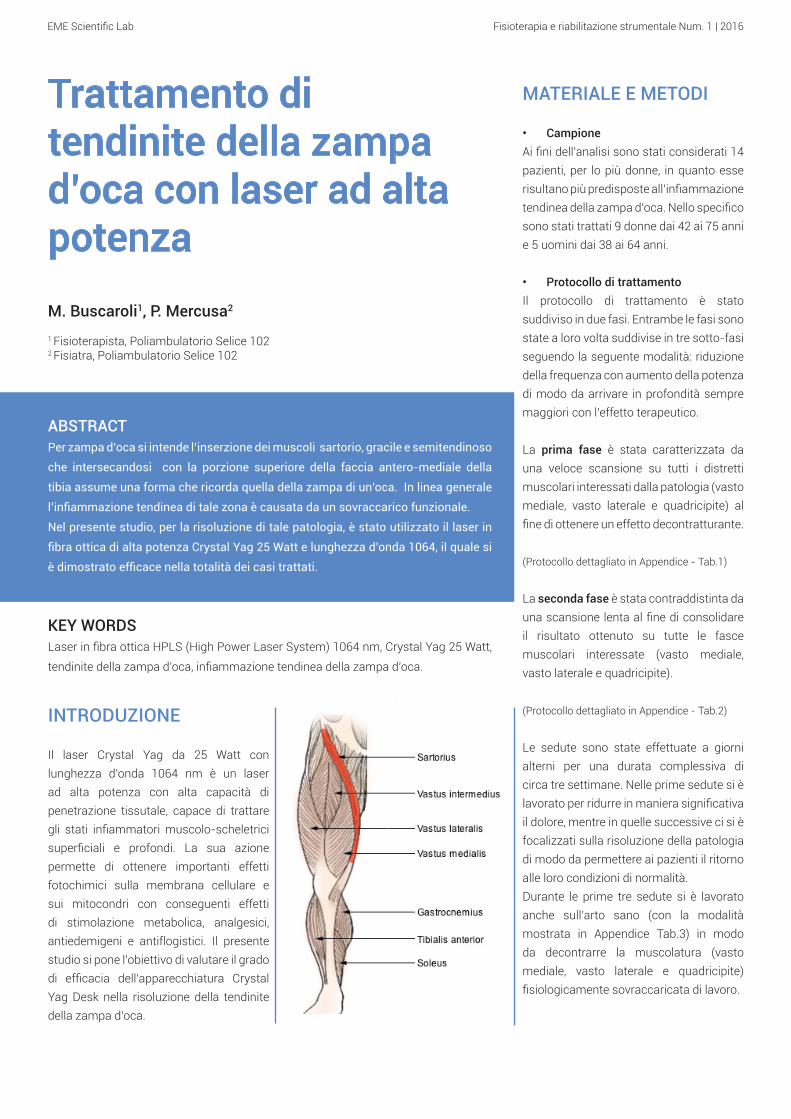
ABSTRACTPer zampa d’oca si intende l’inserzione dei muscoli sartorio, gracile e semitendinoso
che intersecandosi con la porzione superiore della faccia antero-mediale della
tibia assume una forma che ricorda quella della zampa di un’oca. In linea generale
l’infiammazione tendinea di tale zona è causata da un sovraccarico funzionale.
Nel presente studio, per la risoluzione di tale patologia, è stato utilizzato il laser in
fibra ottica di alta potenza Crystal Yag 25 Watt e lunghezza d’onda 1064, il quale si
è dimostrato efficace nella totalità dei casi trattati.
KEY WORDSLaser in fibra ottica HPLS (High Power Laser System) 1064 nm, Crystal Yag 25 Watt,
tendinite della zampa d’oca, infiammazione tendinea della zampa d’oca.
MATERIALE E METODI
• CampioneAi fini dell’analisi sono stati considerati 14 pazienti, per lo più donne, in quanto esse risultano più predisposte all’infiammazione tendinea della zampa d’oca. Nello specifico sono stati trattati 9 donne dai 42 ai 75 anni e 5 uomini dai 38 ai 64 anni.
• Protocollo di trattamentoIl protocollo di trattamento è stato suddiviso in due fasi. Entrambe le fasi sono state a loro volta suddivise in tre sotto-fasi seguendo la seguente modalità: riduzione della frequenza con aumento della potenza di modo da arrivare in profondità sempre maggiori con l’effetto terapeutico.
La prima fase è stata caratterizzata da una veloce scansione su tutti i distretti muscolari interessati dalla patologia (vasto mediale, vasto laterale e quadricipite) al fine di ottenere un effetto decontratturante.
(Protocollo dettagliato in Appendice - Tab.1)
La seconda fase è stata contraddistinta da una scansione lenta al fine di consolidare il risultato ottenuto su tutte le fasce muscolari interessate (vasto mediale, vasto laterale e quadricipite).
(Protocollo dettagliato in Appendice - Tab.2)
Le sedute sono state effettuate a giorni alterni per una durata complessiva di circa tre settimane. Nelle prime sedute si è lavorato per ridurre in maniera significativa il dolore, mentre in quelle successive ci si è focalizzati sulla risoluzione della patologia di modo da permettere ai pazienti il ritorno alle loro condizioni di normalità. Durante le prime tre sedute si è lavorato anche sull’arto sano (con la modalità mostrata in Appendice Tab.3) in modo da decontrarre la muscolatura (vasto mediale, vasto laterale e quadricipite) fisiologicamente sovraccaricata di lavoro.
EME Scientific Lab Fisioterapia e riabilitazione strumentale Num. 1 | 2016
APPENDICE
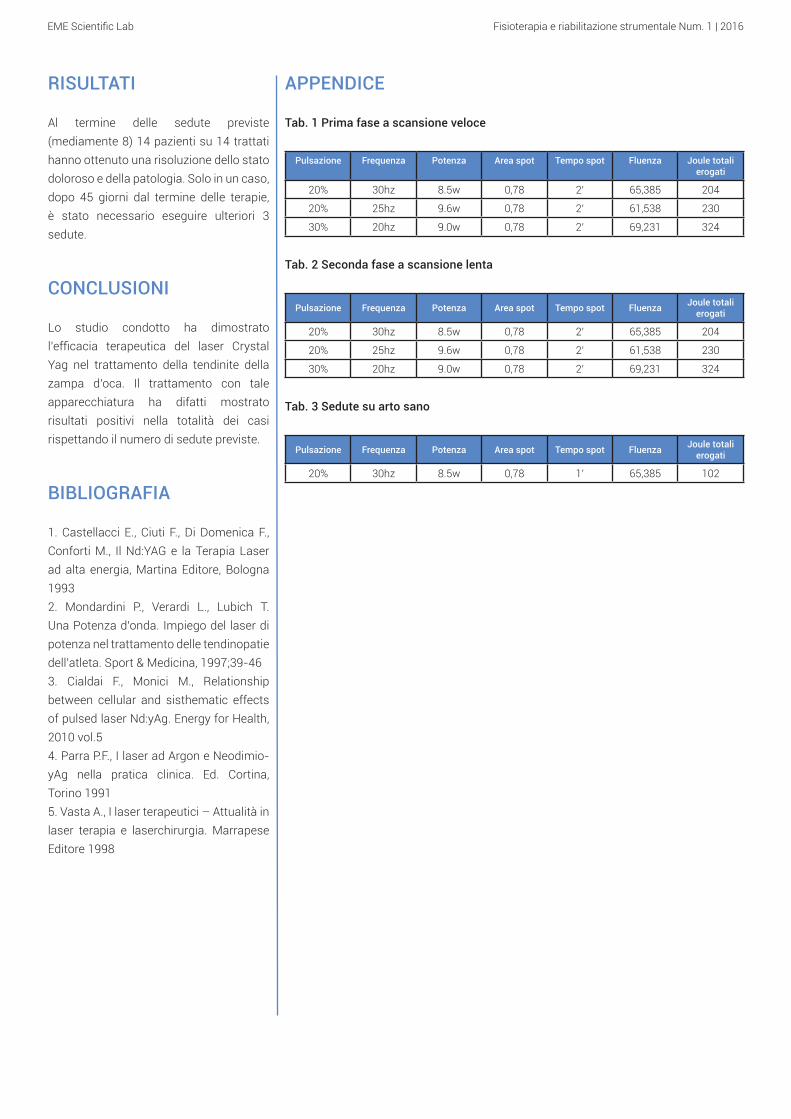
Tab. 1 Prima fase a scansione veloce
Pulsazione Frequenza Potenza Area spot Tempo spot Fluenza Joule totali erogati
20% 30hz 8.5w 0,78 2’ 65,385 204
20% 25hz 9.6w 0,78 2’ 61,538 230
30% 20hz 9.0w 0,78 2’ 69,231 324
Tab. 2 Seconda fase a scansione lenta
Pulsazione Frequenza Potenza Area spot Tempo spot Fluenza Joule totali erogati
20% 30hz 8.5w 0,78 2’ 65,385 204
20% 25hz 9.6w 0,78 2’ 61,538 230
30% 20hz 9.0w 0,78 2’ 69,231 324
Tab. 3 Sedute su arto sano
Pulsazione Frequenza Potenza Area spot Tempo spot Fluenza Joule totali erogati
20% 30hz 8.5w 0,78 1’ 65,385 102
RISULTATI
Al termine delle sedute previste (mediamente 8) 14 pazienti su 14 trattati hanno ottenuto una risoluzione dello stato doloroso e della patologia. Solo in un caso, dopo 45 giorni dal termine delle terapie, è stato necessario eseguire ulteriori 3 sedute.
CONCLUSIONI
Lo studio condotto ha dimostrato l’efficacia terapeutica del laser Crystal Yag nel trattamento della tendinite della zampa d’oca. Il trattamento con tale apparecchiatura ha difatti mostrato risultati positivi nella totalità dei casi rispettando il numero di sedute previste.
BIBLIOGRAFIA
1. Castellacci E., Ciuti F., Di Domenica F., Conforti M., Il Nd:YAG e la Terapia Laser ad alta energia, Martina Editore, Bologna 1993 2. Mondardini P., Verardi L., Lubich T. Una Potenza d’onda. Impiego del laser di potenza nel trattamento delle tendinopatie dell’atleta. Sport & Medicina, 1997;39-463. Cialdai F., Monici M., Relationship between cellular and sisthematic effects of pulsed laser Nd:yAg. Energy for Health, 2010 vol.54. Parra P.F., I laser ad Argon e Neodimio-yAg nella pratica clinica. Ed. Cortina, Torino 19915. Vasta A., I laser terapeutici – Attualità in laser terapia e laserchirurgia. Marrapese Editore 1998

EME Scientific Lab Fisioterapia e riabilitazione strumentale Num. 1 | 2016
INTRODUCTION
The Crystal Yag laser 25 Watt with a wavelength 1064 nm is a high power laser with high capacity of tissue penetration, capable of treating musculoskeletal inflammatory states superficially and in depth. Its action allows to obtain important photochemical effects on the cell membrane and mitochondria with consequent effects of metabolic stimulation, analgesics, anti-inflammatory and anti-edema effects. This study aims to assess the degree of effectiveness of the equipment Yag Crystal Desk in resolving the goosefoot tendinitis.
Treatment of goosefoot tendonitis with high power laserM. Buscaroli1, P. Mercusa2
1 Physiotherapist, Poliambulatorio Selice 1022 Physiatrist, Poliambulatorio Selice 102
ABSTRACT“Goosefoot” refers to the attachment of sartorius, gracilis and semitendinosus
muscles that intersecting with the upper portion of the anteromedial face of the
tibia, assumes a shape that resembles the paw of a goose. In general, the tendon
inflammation of that area is caused by a functional overload. In the present study,
for the resolution of this pathology, it has been used the high-power optical-fiber
laser Crystal Yag 25 Watt with wavelength 1064, which was effective in all cases
treated.
KEY WORDSFiber lasers HPLS (High Power Laser System) 1064 nm, Crystal YAG 25 Watt, tendonitis
goosefoot, inflammation of the goosefoot.
TOOLS AND METHODS
• SampleFor the purposes of this analysis there were considered 14 patients, mostly women, since they are more prone to inflammation of the goosefoot tendon. Specifically were treated 9 women aged 42 to 75 years and 5 men aged 38 to 64 years.
• Treatment protocolThe treatment protocol was divided into two phases. Both phases were in turn subdivided into three sub-phases according to the following mode: reduction of the frequency with increase of the power so as to arrive in ever greater depths with the therapeutic effect.
The first phase was characterized by a quick scan of all the muscle groups of the forearm (vastus medialis, vastus lateralis and quadriceps) in order to dissolve the contracted muscles.
(Detailed protocol in Appendix - Tab.1)
The second phase was characterized by a slow scan in order to consolidate the results obtained on all the muscles involved (vastus medialis, vastus lateralis and quadriceps).
(Detailed protocol in Appendix - Tab.2)
The sessions were carried out on alternate days for a total duration of about three weeks. In the first sessions we worked to significantly reduce the pain, while in the following ones we focused on the resolution of the disease so as to allow patients to return to their normal conditions. During the first three sessions we also worked on the healthy limb, with the mode shown in Table 3, so the muscles to relax (vastus medialis, vastus lateralis and quadriceps) physiologically overloaded with work.
EME Scientific Lab Fisioterapia e riabilitazione strumentale Num. 1 | 2016
APPENDIX
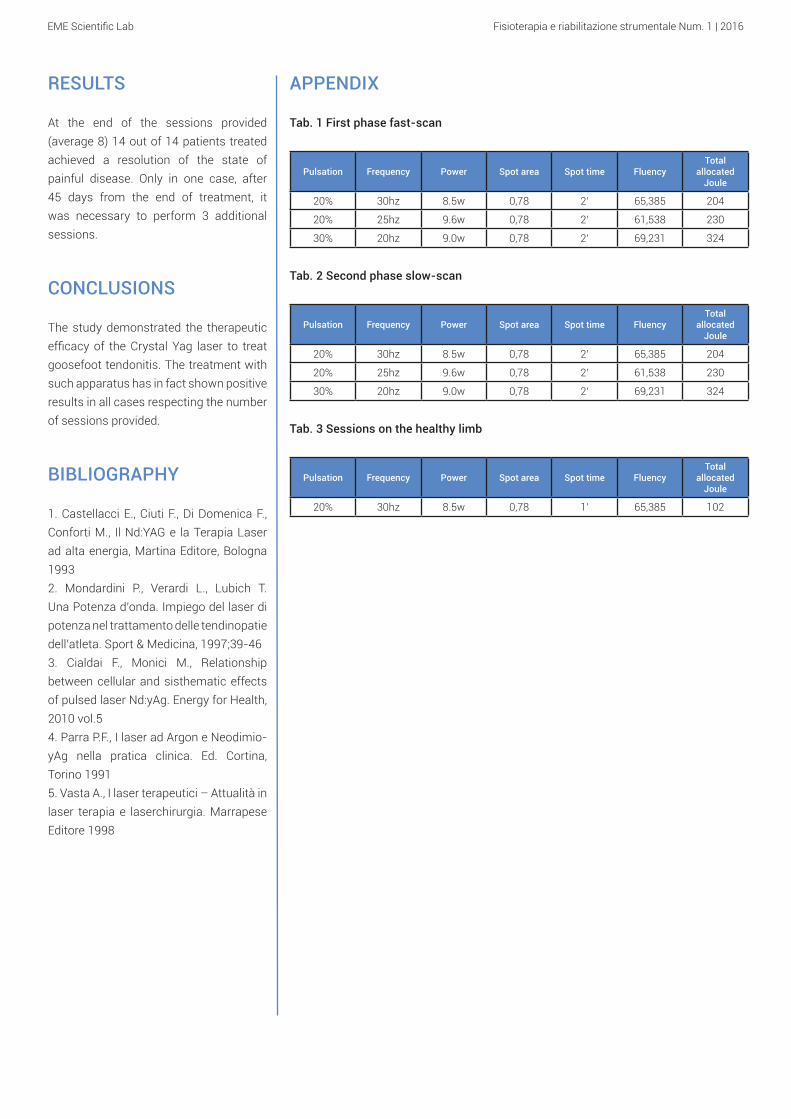
Tab. 1 First phase fast-scan
Pulsation Frequency Power Spot area Spot time FluencyTotal
allocated Joule
20% 30hz 8.5w 0,78 2’ 65,385 204
20% 25hz 9.6w 0,78 2’ 61,538 230
30% 20hz 9.0w 0,78 2’ 69,231 324
Tab. 2 Second phase slow-scan
Pulsation Frequency Power Spot area Spot time FluencyTotal
allocated Joule
20% 30hz 8.5w 0,78 2’ 65,385 204
20% 25hz 9.6w 0,78 2’ 61,538 230
30% 20hz 9.0w 0,78 2’ 69,231 324
Tab. 3 Sessions on the healthy limb
Pulsation Frequency Power Spot area Spot time FluencyTotal
allocated Joule
20% 30hz 8.5w 0,78 1’ 65,385 102
RESULTS
At the end of the sessions provided (average 8) 14 out of 14 patients treated achieved a resolution of the state of painful disease. Only in one case, after 45 days from the end of treatment, it was necessary to perform 3 additional sessions.
CONCLUSIONS
The study demonstrated the therapeutic efficacy of the Crystal Yag laser to treat goosefoot tendonitis. The treatment with such apparatus has in fact shown positive results in all cases respecting the number of sessions provided.
BIBLIOGRAPHY
1. Castellacci E., Ciuti F., Di Domenica F., Conforti M., Il Nd:YAG e la Terapia Laser ad alta energia, Martina Editore, Bologna 1993 2. Mondardini P., Verardi L., Lubich T. Una Potenza d’onda. Impiego del laser di potenza nel trattamento delle tendinopatie dell’atleta. Sport & Medicina, 1997;39-463. Cialdai F., Monici M., Relationship between cellular and sisthematic effects of pulsed laser Nd:yAg. Energy for Health, 2010 vol.54. Parra P.F., I laser ad Argon e Neodimio-yAg nella pratica clinica. Ed. Cortina, Torino 19915. Vasta A., I laser terapeutici – Attualità in laser terapia e laserchirurgia. Marrapese Editore 1998
EME Scientific Lab Fisioterapia e riabilitazione strumentale Num. 1 | 2016
INTRODUZIONE
Cit. Estratto dal Quaderno del Ministero della Salute Nr. 8 marzo-aprile 2011: “La diatermia per contatto è costituita da un’apparecchiatura a radiofrequenza che somministra energia ad una frequenza relativamente bassa (intorno a 0,5
Trattamento di distorsione di caviglia (di grado 1 e 2) condiatermiaA. Domenicucci1, M. Ricchiuti2
1 Fisioterapista, Studio di Riabilitazione Fisioterapica Riabilita2 Ortopedico
ABSTRACTLa caviglia è la regione di raccordo fra gamba e piede e comprende l’articolazione
tibio-tarsica o l’articolazione talo-crucrale, tra le estremità distali di tibia e fibula (o
perone) e dell’astragalo (o talo) del piede (articolazione talocrurale). Le distorsioni
di caviglia sono uno dei tipi di lesione più comune fra gli atleti e rappresentano
un trauma frequente anche per chi non pratica attività sportiva. Le lesioni che
interessano il distretto della caviglia si possono suddividere in a) Fratture, b)
Lussazioni, c) Distorsioni. Quest’ultime vendono suddivise a loro volta in grado I,
II, III.
In questo studio si è scelto di trattare le distorsioni di caviglia di grado I e II per la
maggior frequenza della patologia. Più in particolare sono stati trattati 13 pazienti
di cui 5 con distorsione di grado II ed 8 con distorsione di grado I. I risultati ottenuti
sono stati assolutamente positivi poiché si è riscontrata la guarigione nell’80% dei
casi trattati. In 3 dei 13 casi si sono dovute eseguire ulteriori 3 sedute (con gli stessi
parametri dell’ultima seduta indicata in tabella).
KEY WORDSHr Tek, endodiatermia, endodiatermia, diatermia, tecar, distorsione di caviglia,
distorsione, distorsione di grado I, distorsione di grado II.
Mhz), attraverso due elettrodi a contatto con la cute, uno dei quali può essere elettricamente isolato per interposizione di uno strato isolante fra elettrodo e cute. Gli effetti biologici sono condizionati da: tensione applicata, dimensione
degli elettrodi, impedenza dei tessuti. L’effetto termico nei tessuti è dovuto ad effetto joule per passaggio di corrente all’agitazione di “dipoli cellulari” sottoposti a campo elettrico alternato. Al variare dell’intensità di trattamento si possono ottenere effetti biologici diversificati, quali per esempio incremento del microcircolo, biostimolazione cellulare, analgesia, microiperemia capillare e precapillare, ossigenazione intracellulare e tissutale, aumento del metabolismo, vasodilatazione, aumento della temperatura”.Si è voluto effettuare uno studio utilizzando la tecnologia Hr Tek per verificare la validità dello strumento terapeutico nei traumi distorsivi alla caviglia di grado I e II. Per le distorsioni di grado I sono stati eseguiti 8 trattamenti, per le distorsioni di grado II sono stati eseguiti 12 trattamenti.
MATERIALI E METODI
• CampionePer perseguire tale obiettivo è stato scelto un campione di 13 pazienti afflitti da distorsione di caviglia di grado I e II. Per garantire la validità del gruppo scelto sono stati inclusi soggetti di diverse età e sesso. Nello specifico sono stati presi in esame 8 uomini e 5 donne dai 15 ai 40 anni.

EME Scientific Lab Fisioterapia e riabilitazione strumentale Num. 1 | 2016
due volte a settimana. Per le distorsioni di grado I sono stati eseguiti 8 trattamenti, per le distorsioni di grado II sono stati eseguiti 12 trattamenti. In questa fase si è voluto dapprima recuperare il ROM articolare per poi rinforzare prima attivamente, poi anche in contro resistenza l’articolazione.
Nella 5° seduta gli ultimi 5 minuti di trattamento sono stati eseguiti mobilizzando la caviglia passivamente in flesso estensione.
Nella 6° seduta gli ultimi 10 minuti di trattamento sono stati eseguiti mobilizzando la caviglia passivamente in tutti e quattro i movimenti.
Dalla 7° seduta in poi, a seconda della durata del ciclo terapeutico (8/12 sedute), gli ultimi 10 minuti di trattamento sono stati eseguiti mobilizzando la caviglia passivamente in tutti e quattro i movimenti, poi attivamente e, quando possibile, contro resistenza.(Protocollo dettagliato in Appendice - Tab.3)
RISULTATI
L’utilizzo delle tecnologie e dei protocolli sopra indicati ha consentito la risoluzione dell’80% delle patologie nei tempi prefissati.
CONCLUSIONI
Lo studio condotto ha dimostrato l’efficacia dell’apparecchiatura HR Tek nella risoluzione della patologia presa in esame. Inoltre, a seguito dei trattamenti effettuati e della valutazione dei risultati è stato possibile evidenziare come principali punti di forza le alte performance della tecnologia in termini di calore erogato dall’apparecchio e percepito (sia dal paziente che dall’operatore) così come l’utilità dei manipoli dotati di potenziometro.
• Protocollo di trattamentoIl trattamento dei pazienti è stato suddiviso in: fase acuta, sub-acuta e riabilitativa associando ad ognuna di esse una specifica sequenza di trattamento. L’obiettivo del protocollo è la risoluzione della patologia in un numero di sedute compreso tra 8 e 12.
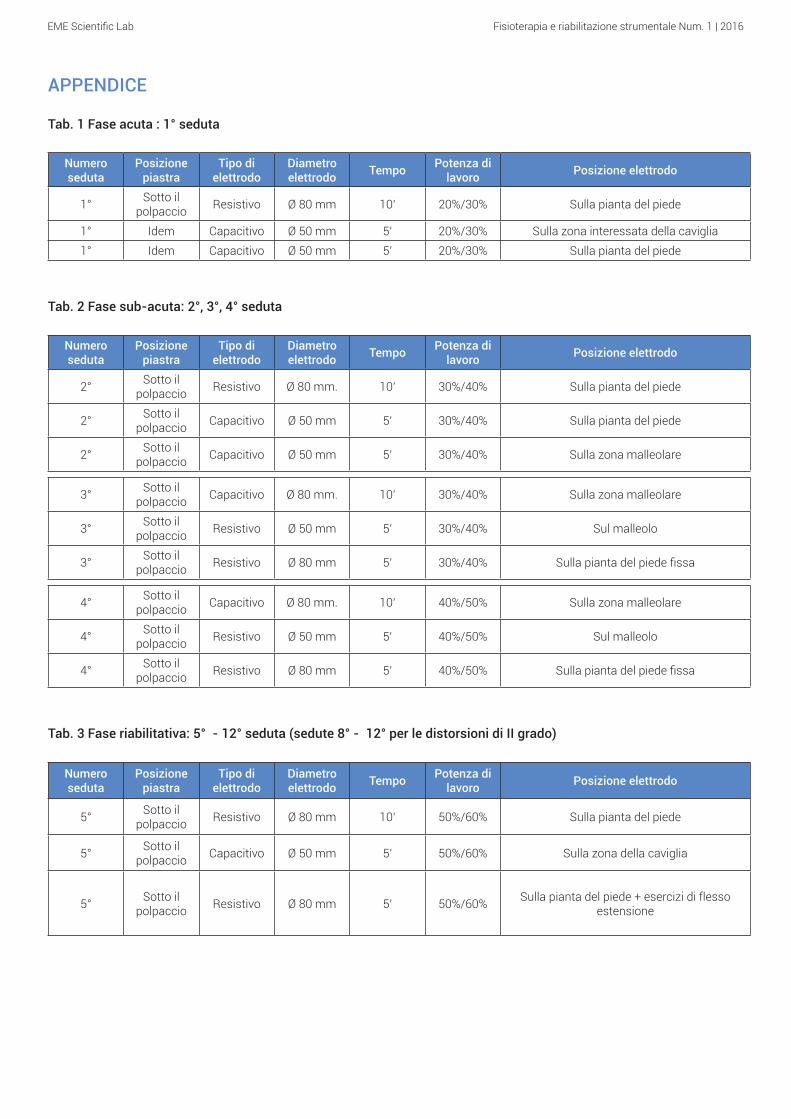
Nella fase acuta (1° seduta eseguita entro 48 ore dal trauma) l’area dolorante, per aiutare il drenaggio linfatico locale e per diminuire o meglio ancora togliere il dolore, è stata così trattata: a) posizionando la piastra neutra sotto il polpaccio ed utilizzando l’elettrodo resistivo Ø 80 mm sulla pianta del piede tenendo il manipolo sostanzialmente fermo e lavorando ad una potenza di circa il 20% / 30% per circa 10 minuti; b) mantenendo la piastra neutra sotto il polpaccio ed utilizzando l’elettrodo capacitivo Ø 50 mm nella zona principalmente interessata della caviglia, tenendo il manipolo sostanzialmente fermo e lavorando ad una potenza di circa il 20% / 30% per circa 5 minuti; c) mantenendo la piastra neutra sotto il polpaccio ed utilizzando l’elettrodo capacitivo Ø 50 mm sulla pianta del piede tenendo il manipolo sostanzialmente fermo e lavorando ad una potenza di circa il 20% / 30% per circa 5 minuti.(Protocollo dettagliato in Appendice- Tab.1)
Nella fase sub-acuta (2°, 3° e 4° seduta) i trattamenti sono stati eseguiti a giorni alterni. I parametri indicato hanno consentito un aumento del metabolismo locale, il riassorbimento dell’ematoma, un notevole effetto antalgico sui pazienti e favorito la cicatrizzazione dell’apparato capsulo legamentoso interessato. Nelle prime 3 sedute a fine terapia è stato eseguito taping e bendaggio per blocco alla caviglia. I trattamenti della fase sub-acuta sono stati eseguiti come in tabella n. 2 in Appendice.
Nella fase riabilitativa (dalla 5° alla 8°/10° seduta) i trattamenti sono stati eseguiti
BIBLIOGRAFIA
1. Caserio M., Bandinelli I., Borrani A., L’Ipertermia nelle lesioni muscolari. 21 Congresso Nazionale S.l.M.F.E.R. “Muscolo e Riabilitazione”- Roma Ottobre 1993.2. Alicicco E., Castellano V., Zucchi R., Chinni L. M., Alvaro U.L., L’ipertermia nella patologia articolare ed extraarticolare dello sportivo - Reumatismo vol. 48 suppl. n°1. 1996. 3. Alicicco E., Alessandrelli G.L., Brozzi M., Hyperthermia in Sport (accident surgery) Traumatology - 7th International Congress on Hyperthermia Oncology - Roma Aprile 9-13.1996. 4. Bach S.A., Biological sensivity to radiofrequency and microwave energy. Fed.Proc 24 (Suppl.14):22-26,1965.5. Tepperman P. S., and Devlin M., The Therapeutic Use of Local Heat and Cold, Can Fam Physician. 1986 May; 32: 1110–1114.6. Melegati G., Volpi P., Tornese D., Mele G., La riabilitazione nelle tendinopatie, 2003.7. Giombini A., Di Cesare A., Safran M.R., Ciatti R., Maffulli N., Short-term effectiveness of hyperthermia for supraspinatus tendinopathy in athletes: a short-term randomized controlled study., Am J Sports Med. 2006 Aug.8. Mohannad Hawamdeh, The effectiveness of Capacitive Resistive Diathermy (Tecartherapy®) in acute and chronic musculoskeletal lesions and pathologies9. G. Melegati, D. Tornese, M. Bandi, L’impiego della tecarterapia nei traumi distorsivi di caviglia, Clinical Evidence 200310. E. Parolo, M.P. Onesta, Ipertermia a trasferimento energetico resistivo e capacitivo nel trattamento di lesioni muscolo-scheletriche acute e croniche, Clinical Evidence 200311. G.P.Ganzit, L.Stefanini, G.Stesina, La tecarterapia nel trattamento di patolgie acute e croniche da sport, Clinical Evidence 2003
EME Scientific Lab Fisioterapia e riabilitazione strumentale Num. 1 | 2016
APPENDICE
Tab. 1 Fase acuta : 1° seduta
Numero seduta
Posizione piastra
Tipo di elettrodo
Diametro elettrodo Tempo Potenza di
lavoro Posizione elettrodo
1° Sotto il polpaccio Resistivo Ø 80 mm 10’ 20%/30% Sulla pianta del piede
1° Idem Capacitivo Ø 50 mm 5’ 20%/30% Sulla zona interessata della caviglia1° Idem Capacitivo Ø 50 mm 5’ 20%/30% Sulla pianta del piede
Tab. 2 Fase sub-acuta: 2°, 3°, 4° seduta
Numero seduta
Posizione piastra
Tipo di elettrodo
Diametro elettrodo Tempo Potenza di
lavoro Posizione elettrodo
2° Sotto il polpaccio Resistivo Ø 80 mm. 10’ 30%/40% Sulla pianta del piede
2° Sotto il polpaccio Capacitivo Ø 50 mm 5’ 30%/40% Sulla pianta del piede
2° Sotto il polpaccio Capacitivo Ø 50 mm 5’ 30%/40% Sulla zona malleolare
3° Sotto il polpaccio Capacitivo Ø 80 mm. 10’ 30%/40% Sulla zona malleolare
3° Sotto il polpaccio Resistivo Ø 50 mm 5’ 30%/40% Sul malleolo
3° Sotto il polpaccio Resistivo Ø 80 mm 5’ 30%/40% Sulla pianta del piede fissa
4° Sotto il polpaccio Capacitivo Ø 80 mm. 10’ 40%/50% Sulla zona malleolare
4° Sotto il polpaccio Resistivo Ø 50 mm 5’ 40%/50% Sul malleolo
4° Sotto il polpaccio Resistivo Ø 80 mm 5’ 40%/50% Sulla pianta del piede fissa
Tab. 3 Fase riabilitativa: 5° →- 12° seduta (sedute 8° -→ 12° per le distorsioni di II grado)
Numero seduta
Posizione piastra
Tipo di elettrodo
Diametro elettrodo Tempo Potenza di
lavoro Posizione elettrodo
5° Sotto il polpaccio Resistivo Ø 80 mm 10’ 50%/60% Sulla pianta del piede
5° Sotto il polpaccio Capacitivo Ø 50 mm 5’ 50%/60% Sulla zona della caviglia
5° Sotto il polpaccio Resistivo Ø 80 mm 5’ 50%/60% Sulla pianta del piede + esercizi di flesso
estensione
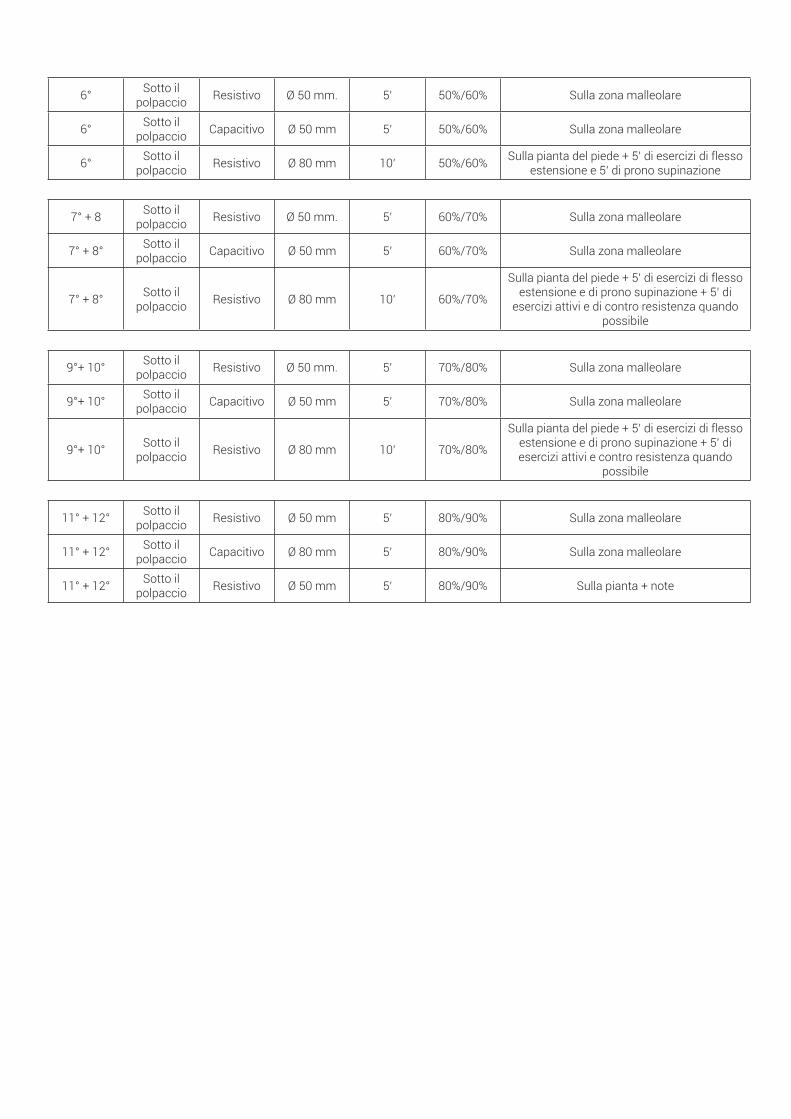
6° Sotto il polpaccio Resistivo Ø 50 mm. 5’ 50%/60% Sulla zona malleolare
6° Sotto il polpaccio Capacitivo Ø 50 mm 5’ 50%/60% Sulla zona malleolare
6° Sotto il polpaccio Resistivo Ø 80 mm 10’ 50%/60% Sulla pianta del piede + 5’ di esercizi di flesso
estensione e 5’ di prono supinazione
7° + 8 Sotto il polpaccio Resistivo Ø 50 mm. 5’ 60%/70% Sulla zona malleolare
7° + 8° Sotto il polpaccio Capacitivo Ø 50 mm 5’ 60%/70% Sulla zona malleolare
7° + 8° Sotto il polpaccio Resistivo Ø 80 mm 10’ 60%/70%
Sulla pianta del piede + 5’ di esercizi di flesso estensione e di prono supinazione + 5’ di
esercizi attivi e di contro resistenza quando possibile
9°+ 10° Sotto il polpaccio Resistivo Ø 50 mm. 5’ 70%/80% Sulla zona malleolare
9°+ 10° Sotto il polpaccio Capacitivo Ø 50 mm 5’ 70%/80% Sulla zona malleolare
9°+ 10° Sotto il polpaccio Resistivo Ø 80 mm 10’ 70%/80%
Sulla pianta del piede + 5’ di esercizi di flesso estensione e di prono supinazione + 5’ di esercizi attivi e contro resistenza quando
possibile
11° + 12° Sotto il polpaccio Resistivo Ø 50 mm 5’ 80%/90% Sulla zona malleolare
11° + 12° Sotto il polpaccio Capacitivo Ø 80 mm 5’ 80%/90% Sulla zona malleolare
11° + 12° Sotto il polpaccio Resistivo Ø 50 mm 5’ 80%/90% Sulla pianta + note
EME Scientific Lab Fisioterapia e riabilitazione strumentale Num. 1 | 2016
INTRODUCTION
Quote from the Quaderno del Ministero della Salute Nr. 8 March-April 2011:“The diathermy by contact is formed by a radio frequency apparatus that administers energy at a relatively low frequency (around 0.5 MHz), via two electrodes in contact with the skin, one of which can be electrically isolated by interposition of a insulating layer between electrode and skin. The biological effects
Treatment of ankle sprain (degree 1 and 2) with diathermyA. Domenicucci1, M. Ricchiuti2
1 Physiotherapist, Studio di Riabilitazione Fisioterapica Riabilita2 Orthopedist
ABSTRACTThe ankle is the region of connection between leg and foot and includes the ankle
joint or lead joint, between the distal ends of tibia, fibula and the talus of the foot (lead
joint). The ankle sprains are one of the most common types of injury among athletes
and represent a frequent trauma even for those who do not practice sports. The
lesions affecting the ankle district can be divided into a) Fractures, b) Dislocations,
c) Distortions. Distortions are in turn subdivided in degree I, II, III.
In this study it was decided to treat ankle sprains grade I and II because of the greater
frequency of the disease. More in particular were treated 13 patients of which 5 with
distortion of grade II and 8 with distortion of degree I. The results obtained were
absolutely positive since it was found healing in 80% of treated cases. In 3 of the 13
cases it occurred to perform 3 additional sessions (with the same parameters as
the last session indicated in the table).
KEY WORDSHr Tek, endodiathermy, diathermy, tecar, ankle sprain, sprains, fractures, Grade I
sprain, Grade II sprain.
are conditioned by: the applied voltage, size of the electrodes, tissue impedance. The thermal effect in the tissues is due to the joule effect caused by the agitation of “cellular dipoles” subjected to alternating electric field. By varying the intensity of treatment you can get diverse biological effects, such as for instance increase of microcirculation, cellular bio-stimulation, analgesia, capillary and precapillary
microiperemia, intracellular and tissue oxygenation, increased metabolism, vasodilatation, increase in temperature.” We wanted to carry out a study using Hr Tek technology to verify the validity of the therapeutic instrument in the ankle sprain grade I and II. For the distortions of grade I were performed 8 treatments, for the distortions of grade II were performed 12 treatments.
TOOLS AND METHODS
• SampleIn order to pursue this goal we selected a sample of 13 patients suffering from ankle sprain grade I and II. To ensure the validity of the chosen group we included subjects of different ages and sex. Specifically examined were 8 men and 5 women aged 15 to 40 years.
• Treatment protocolThe treatment has been divided into: acute, sub-acute and rehabilitative phase associating each of them to a specific treatment sequence. The objective of the protocol is the resolution of the pathology in a number of sessions between 8 and 12
In the acute phase (1st session performed within 48 hours from the injury) in orderd

EME Scientific Lab Fisioterapia e riabilitazione strumentale Num. 1 | 2016
treatment were carried out by mobilizing the ankle passively in all four movements.
From the 7th session on, depending on the length of the therapeutic cycle (8/12 sessions), the last 10 minutes of treatment were carried out by mobilizing the ankle passively in all four movements, then actively and, when possible, against resistance.(Detailed protocol in Appendix - Tab.3)
RESULTS
The use of the mentioned technologies and protocols allowed the resolution of 80% of the diseases on schedule.
CONCLUSIONS
The study demonstrated the effectiveness of the HR Tek equipment in resolving the examined pathology. In addition, as a result of processing and evaluating the we managed to detect as key strengths the high performance of the technology in terms of heat output from the unit and perceived (both the patient and the operator) as well as the usefulness of the handpieces with potentiometer.
BIBLIOGRAPHY
1. Caserio M., Bandinelli I., Borrani A., L’Ipertermia nelle lesioni muscolari. 21 Congresso Nazionale S.l.M.F.E.R. “Muscolo e Riabilitazione”- Roma Ottobre 1993.2. Alicicco E., Castellano V., Zucchi R., Chinni L. M., Alvaro U.L., L’ipertermia nella patologia articolare ed extraarticolare dello sportivo - Reumatismo vol. 48 suppl. n°1. 1996. 3. Alicicco E., Alessandrelli G.L., Brozzi M., Hyperthermia in Sport (accident surgery) Traumatology - 7th International Congress on Hyperthermia Oncology - Roma Aprile 9-13.1996.
to help the local lymphatic drainage and to reduce or better yet remove the pain, the painful área was treated in this way: a) positioning the neutral plate below the calf, and using the resistive electrode Ø 80 mm on the sole of the foot holding the handpiece stationary and working with a power of about 20%/30% for about 10 minutes; b) placing the neutral plate below the calf, and using the capacitive electrode Ø 50 mm on the ankle area, holding the handpiece stationary and working with a power of about 20%/30% for about 5 minutes; c) placing the neutral plate below the calf, and using the capacitive electrode Ø 50 mm on the sole of the foot holding the handpiece stationary and working with a power of about 20%/30% for about 5 minutes;(Detailed protocol in Appendix - Tab.1)
In the sub-acute phase (2nd, 3rd and 4th session) the treatments were performed on alternate days. The parameters shown allowed an increase in local metabolism, resorption of the hematoma, a significant analgesic effect on patients and favored the healing of apparatus capsular ligamentous concerned. In the first three sessions at the end of therapy was performed taping and bandage for ankle lock. The treatments of the sub-acute phase were performed as showed in Tab. 2 in Appendix.
In the rehabilitation phase (from the 5th to the 8th/10th session) treatments were performed twice a week. For the distortions of grade I were performed 8 treatments, for the distortions of grade II were performed 12 treatments. At this stage it was decided to first recover the joint ROM and reinforce actively, then also against resistance, the articulation.
In the 5th session the last 5 minutes of treatment were carried out by mobilizing the ankle passively in flexion-extension.In the 6th session the last 10 minutes of
4. Bach S.A., Biological sensivity to radiofrequency and microwave energy. Fed.Proc 24 (Suppl.14):22-26,1965.5. Tepperman P. S., and Devlin M., The Therapeutic Use of Local Heat and Cold, Can Fam Physician. 1986 May; 32: 1110–1114.6. Melegati G., Volpi P., Tornese D., Mele G., La riabilitazione nelle tendinopatie, 2003.7. Giombini A., Di Cesare A., Safran M.R., Ciatti R., Maffulli N., Short-term effectiveness of hyperthermia for supraspinatus tendinopathy in athletes: a short-term randomized controlled study., Am J Sports Med. 2006 Aug.8. Mohannad Hawamdeh, The effectiveness of Capacitive Resistive Diathermy (Tecartherapy®) in acute and chronic musculoskeletal lesions and pathologies9. G. Melegati, D. Tornese, M. Bandi, L’impiego della tecarterapia nei traumi distorsivi di caviglia, Clinical Evidence 200310. E. Parolo, M.P. Onesta, Ipertermia a trasferimento energetico resistivo e capacitivo nel trattamento di lesioni muscolo-scheletriche acute e croniche, Clinical Evidence 200311. G.P.Ganzit, L.Stefanini, G.Stesina, La tecarterapia nel trattamento di patolgie acute e croniche da sport, Clinical Evidence 2003
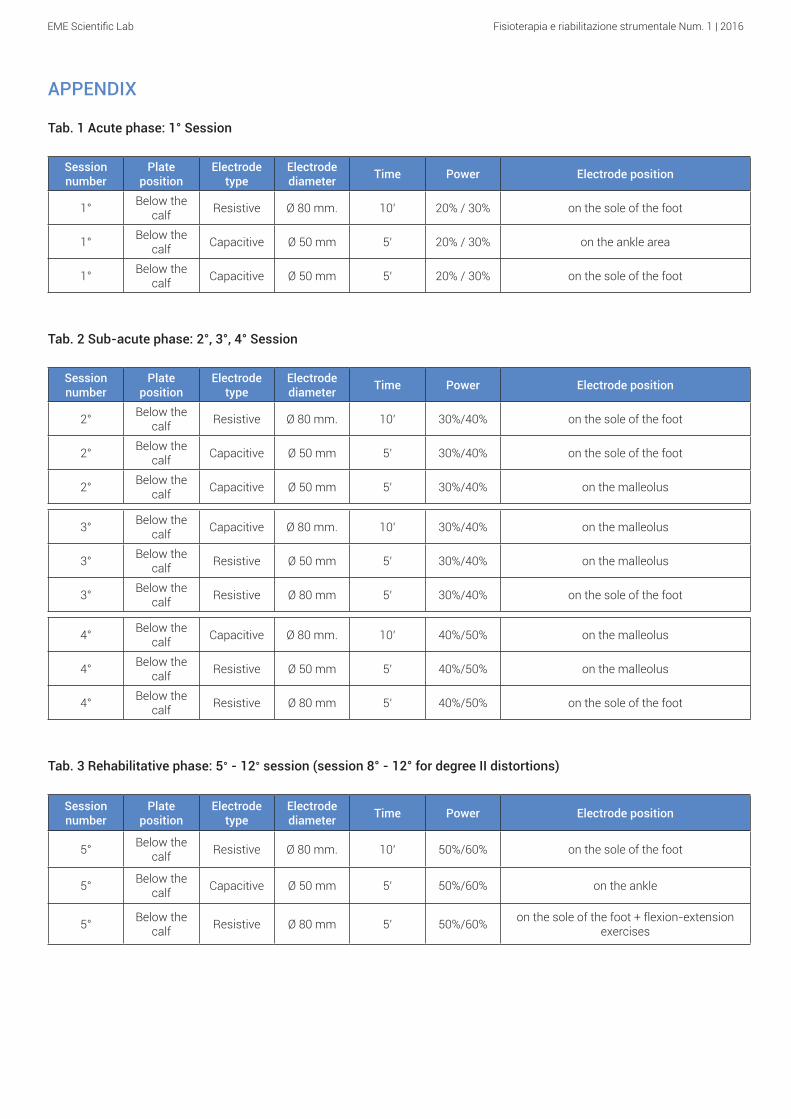
EME Scientific Lab Fisioterapia e riabilitazione strumentale Num. 1 | 2016
APPENDIX
Tab. 1 Acute phase: 1° Session
Session number
Plate position
Electrode type
Electrode diameter Time Power Electrode position
1° Below the calf Resistive Ø 80 mm. 10’ 20% / 30% on the sole of the foot
1° Below the calf Capacitive Ø 50 mm 5’ 20% / 30% on the ankle area
1° Below the calf Capacitive Ø 50 mm 5’ 20% / 30% on the sole of the foot
Tab. 2 Sub-acute phase: 2°, 3°, 4° Session
Session number
Plate position
Electrode type
Electrode diameter Time Power Electrode position
2° Below the calf Resistive Ø 80 mm. 10’ 30%/40% on the sole of the foot
2° Below the calf Capacitive Ø 50 mm 5’ 30%/40% on the sole of the foot
2° Below the calf Capacitive Ø 50 mm 5’ 30%/40% on the malleolus
3° Below the calf Capacitive Ø 80 mm. 10’ 30%/40% on the malleolus
3° Below the calf Resistive Ø 50 mm 5’ 30%/40% on the malleolus
3° Below the calf Resistive Ø 80 mm 5’ 30%/40% on the sole of the foot
4° Below the calf Capacitive Ø 80 mm. 10’ 40%/50% on the malleolus
4° Below the calf Resistive Ø 50 mm 5’ 40%/50% on the malleolus
4° Below the calf Resistive Ø 80 mm 5’ 40%/50% on the sole of the foot
Tab. 3 Rehabilitative phase: 5° - 12° session (session 8° - 12° for degree II distortions)
Session number
Plate position
Electrode type
Electrode diameter Time Power Electrode position
5° Below the calf Resistive Ø 80 mm. 10’ 50%/60% on the sole of the foot
5° Below the calf Capacitive Ø 50 mm 5’ 50%/60% on the ankle
5° Below the calf Resistive Ø 80 mm 5’ 50%/60% on the sole of the foot + flexion-extension
exercises
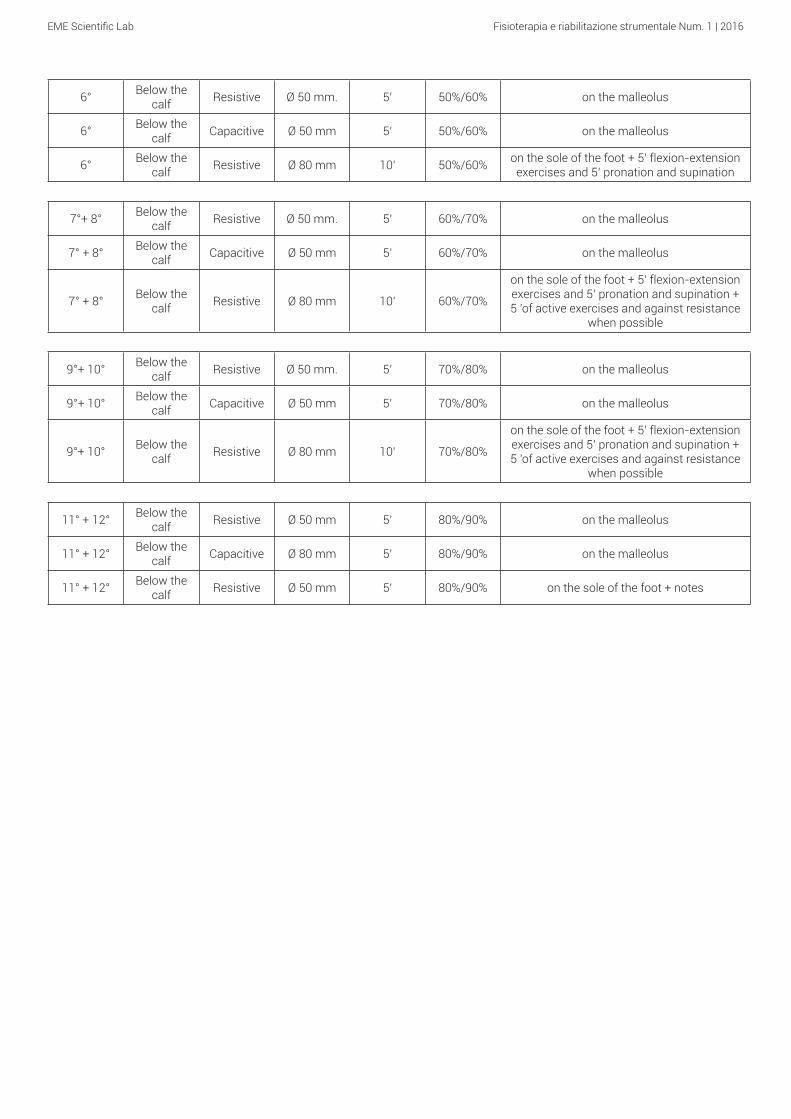
EME Scientific Lab Fisioterapia e riabilitazione strumentale Num. 1 | 2016
6° Below the calf Resistive Ø 50 mm. 5’ 50%/60% on the malleolus
6° Below the calf Capacitive Ø 50 mm 5’ 50%/60% on the malleolus
6° Below the calf Resistive Ø 80 mm 10’ 50%/60% on the sole of the foot + 5’ flexion-extension
exercises and 5’ pronation and supination
7°+ 8° Below the calf Resistive Ø 50 mm. 5’ 60%/70% on the malleolus
7° + 8° Below the calf Capacitive Ø 50 mm 5’ 60%/70% on the malleolus
7° + 8° Below the calf Resistive Ø 80 mm 10’ 60%/70%
on the sole of the foot + 5’ flexion-extension exercises and 5’ pronation and supination + 5 'of active exercises and against resistance
when possible
9°+ 10° Below the calf Resistive Ø 50 mm. 5’ 70%/80% on the malleolus
9°+ 10° Below the calf Capacitive Ø 50 mm 5’ 70%/80% on the malleolus
9°+ 10° Below the calf Resistive Ø 80 mm 10’ 70%/80%
on the sole of the foot + 5’ flexion-extension exercises and 5’ pronation and supination + 5 'of active exercises and against resistance
when possible
11° + 12° Below the calf Resistive Ø 50 mm 5’ 80%/90% on the malleolus
11° + 12° Below the calf Capacitive Ø 80 mm 5’ 80%/90% on the malleolus
11° + 12° Below the calf Resistive Ø 50 mm 5’ 80%/90% on the sole of the foot + notes
EME Scientific Lab
www.eme-srl.com | [email protected] | +39 0721.400791 | Facebook | Linkedin
Num. 1 | 2016