EPIDEMIOLOGIA & PREVENZIONE - unipa.it · 2020. 3. 6. · PubblicazionebimestraleRegistrazione...
156
Transcript of EPIDEMIOLOGIA & PREVENZIONE - unipa.it · 2020. 3. 6. · PubblicazionebimestraleRegistrazione...


Pubblicazione bimestrale Registrazionedel Tribunale di Milanon. 239/1977 Spedizione in AP - 45% - art. 2 comma 20b legge662/96 - Milano.
Iscrizione al Registro degli Operatoridi Comunicazione (ROC) n. 11747.
Una copia: 13,50 euro.
Abbonamento annuo: informazioni e condizioni sul sitowww.epiprev.it
Gestione abbonamenti: ufficio abbonamentitel. 02 48702283, fax 02 48706089.
I dati necessari per l’invio della rivista sono trattati elettronicamentee utilizzati dall’editore Inferenze scarl per la spedizione della pre-sente pubblicazione e di altro materiale medico-scientifico. Aisensi dell’art.13 Legge 675/96 è possibile in qualsiasi momentoe gratuitamente consultare, modificare e cancellare i dati, o sem-plicemente opporsi al loro utilizzo scrivendo a: Inferenze scarl,responsabile dati, via Ricciarelli 29, 20148 Milano.
IVA assolta dall’editore ai sensi dell’art. 74 lettera C del DPR26/10/1972 n.633 e successive modificazioni e integrazioni non-ché ai sensi del DM 29/12/1989. Non si rilasciano quindi fatture(art. 1 c. 5 DM 29/12/1989).
StampaArti grafiche Ancora srl - Milano
Anno 37 (4-5) 2013
Rivista fondata da Giulio A. Maccacaro
Epidemiologia & Prevenzioneè indicizzata in Medline,Science Citation Index Expanded,Journal Citation Reports/Science Edition
EPIDEMIOLOGIA& PREVENZIONE
Testata associata
A.N.E.S.ASSOCIAZIONE NAZIONALEEDITORIA PERIODICA SPECIALIZZATA
via Ricciarelli 29, 20148 [email protected]
Direttore scientificoEugenio Paci
Vicedirettore scientificoFrancesco Forastiere
Past directorBenedetto Terracini
Direttrice responsabileMaria Luisa Clementi
Segreteria scientificaLiliana Cori
RedazioneMarco Crespi, Cinzia Tromba, Maria Cristina Porro
Segreteria di redazionevia Giusti 4, 21053 Castellanza (VA)e-mail: [email protected]
ImpaginazioneStefano Montagnana
Comitato di direzioneFabio Barbone, Annibale Biggeri, Dolores Catelan, Dario Consonni, EmanueleCrocetti, Marina Davoli, Paolo Giorgi Rossi, Chiara Marinacci, Andrea Ranzi,Lorenzo Richiardi, Antonia Stazi, Giuseppe Traversa.
Comitato editorialeAlessandro Barchielli, Antonella Bena, Carla Bietta, Achille Cernigliaro, FabrizioFaggiano, Emilio Gianicolo, Ursula Kirchmayer, Paola Michelozzi, Alessio Petrelli(AIE); Franco Berrino, Annibale Biggeri, Pietro Comba, Gemma Gatta, LuigiMara, AlbertoMartinelli, EnzoMerler, FrancoMerletti, Salvatore Panico, SilvanoPiffer (Coop. Epidemiologia & Prevenzione Giulio A. Maccacaro);Fabio Barbone, Pier Alberto Bertazzi, Fabrizio Bianchi, Piero Borgia, SilviaCandela, Franco Carnevale, Ugo Fedeli, Stefano Ferretti, Alba Finarelli, LiviaGiordano, Roberto Grilli, David Kriebel, AndreaMicheli, Roberta Pirastu, RenatoPizzuti, Walter Ricciardi, Roberto Romizi, Stefania Salmaso, Rodolfo Saracci,Salvatore Scondotto, Paolo Vineis, Marco Zappa (membri invitati dalla DirezioneScientifica, non in rappresentanza della proprietà).
Modalità di abbonamentoPagamento con carta di credito (American Express, Carta Sì, VISA, Eurocard,Master Card) telefonando allo 02-48702283 dal lunedì al venerdì dalle 9 alle13 oppure utilizzando il servizio PayPal sul sito web della rivista www.epiprev.itVersamento su conto corrente postale n. 55195440 intestato a Inferenze scarl,via Ricciarelli n. 29, 20148 Milano (segnalare la causale del versamento).Accredito tramite c/c bancario presso: UNIPOL BANCA Piazza Wagner n. 8,20145 Milano, IBAN: IT53P 03127 01600 000000003681 intestato all’im-presa editoriale Inferenze scarl, via Ricciarelli n. 29, 20148 Milano.
Si ringrazia la Fondazione IRCCS Istituto nazionale dei tumori di Milanoche ospita la Cooperativa.
© Inferenze scarl, Milano
EPIDEMIOLOGIA& PREVENZIONE

I TUMORI IN ITALIA - RAPPORTO 2013
Tumori multipliITALIAN CANCER FIGURES - REPORT 2013
Multiple tumours
AIRTUMWorking GroupAssociazione italiana
registri tumori
CCMCentro nazionaleper la prevenzione
e il controllo delle malattieMinistero della salute
AIRTUMWorking Group
WWW.EPIPREV.IT

I tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI
2 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
■ Registro tumori dell’Alto Adige, TumorregisterSüdtirol, Servizio di anatomia e istologia patologica,Ospedale di Bolzano. Guido Mazzoleni, Andreas Bulatko, ElenaDevigli, Birgit Tschugguel, Elena De Valiere, Gerlinde Facchinelli,Markus Falk, Tomas Dal Cappello■ Registro tumori Piemonte, Provincia di Biella, CPO,Centro di riferimento regionale per l’epidemiologia e laprevenzione dei tumori. Adriano Giacomin, Pier CarloVercellino, Simona Andreone■ Registro tumori Area Vasta Emilia Centrale, AziendaUSL Ferrara. Stefano Ferretti, Laura Marzola, Elena Migliari,Nada Carletti, Patrizia Biavati, Chiara Petrucci■ Registro tumori toscano, UO di epidemiologia clinicae descrittiva, Istituto per lo studio e la prevenzioneoncologica (ISPO). Emanuele Crocetti, Carlotta Buzzoni, AdeleCaldarella, Antonella Corbinelli, Teresa Intrieri, GianfrancoManneschi, Libuse Nemcova, Cristina Ocello, Claudio Sacchettini,Marco Zappa, Eugenio Paci■ Registro tumori del Friuli Venezia Giulia, Direzionecentrale salute, Udine. Diego Serraino, Tiziana Angelin, EttoreBidoli, Silvia Birri, Luigino Dal Maso, Margherita De Dottori, EmiliaDe Santis, Ornella Forgiarini, Antonella Zucchetto, Loris Zanier■ Registro tumori Regione Liguria, UOS epidemiologiadescrittiva (Registro tumori), IRCSS AOU San Martino -IST, Genova / Università di Genova*. Luigina Bonelli, ClaudiaCasella, Enza Marani, Antonella Puppo, Maria Vittoria Celesia,Roberta Cogno, Elsa Garrone,Alberto Quaglia, Marina Vercelli*■ Registro tumori di popolazione della Provincia diLatina. Fabio Pannozzo, Susanna Busco, Ivan Rashid, ValerioRamazzotti, Maria Cecilia Cercato, Maurilio Natali,Walter Battisti,Isabella Sperduti, Leonarda Macci, Ester Bugliarello, EdvigeBernazza, Lucilla Tamburo, Miriana Rossi, Simonetta Curatella,Silvana Tamburrino, Silvia Fattoruso, Giuseppina Serafini,Orsola Valerio■ Registro tumori di Milano, ASL di Milano.MariangelaAutelitano, Simona Ghilardi, Rosanna Leone, Luisa Filipazzi,Annamaria Bonini, Cinzia Giubelli■ Registro Tumori della Provincia di Modena, Centrooncologico modenese.Massimo Federico, Maria Elisa Artioli,Katia Valla, Barbara Braghiroli, Claudia Cirilli, Francesco Iachetta,Stefano Luminari, Monica Pirani, Lorenza Ferrari■ Registro tumori di popolazione della RegioneCampania, c/o ASL Napoli 3 Sud.Mario Fusco, CaterinaBellatalla, Maria Fusco, Margherita Panico, Carmela Perrotta,Biagio Vassante, Maria Francesca Vitale■ Registro tumori della Provincia di Parma, UO dioncologia, Azienda ospedaliera universitaria di Parma.Maria Michiara, Francesco Bozzani, Paolo Sgargi■ Registro tumori della Provincia di Ragusa,Dipartimento di prevenzione medica, Azienda sanitariaprovinciale ASP7 Ragusa. Rosario Tumino, Giuseppe Cascone,Graziella Frasca, Maria Concetta Giurdanella, CaterinaMartorana, Gabriele Morana, Carmela Nicita, Patrizia ConcettaRollo, Maria Grazia Ruggeri, Aurora Sigona, Eugenia Spata,Stefania Vacirca■ Registro tumori reggiano ASMN-IRCCS, Unità diepidemiologia, Dipartimento di sanità pubblica, AziendaUSL di Reggio Emilia. Lucia Mangone, Enza Di Felice,Annamaria Pezzarossi, Stefania Caroli, Carlotta Pellegri, MassimoVicentini, Stefania D’Angelo, Paola Balottari■ Registro tumori della Romagna, IRCCS Istituto tumoridella Romagna (IRST). Fabio Falcini, Americo Colamartini,Lauro Bucchi, Chiara Balducci, Mila Ravegnani, Benedetta Vitali,Carlo Cordaro, Licia Caprara, Orietta Giuliani, Stefania Giorgetti,Monica Palumbo, Rosa Vattiato, Alessandra Ravaioli, SilviaMancini
■ Registro tumori della Provincia di Salerno. LuigiCremone, Claudia Gaudiano, Arturo Iannelli, Gennaro Senatore,Arrigo Zevola■ Registro tumori della Provincia di Sassari, Servizio diepidemiologia, ASL1, Sassari. Ornelia Sechi, RosariaCesaraccio, Daniela Pirino, Donatella Carboni, Giovanna Fiori,Marcella Soddu, Gianpaolo Mameli, Francesco Mura■ Registro tumori della Provincia di Siracusa, ASPSiracusa.Maria Lia Contrino, Anselmo Madeddu, FrancescoTisano, Salvatore Sciacca, Angela Muni, Margherita Mizzi, MariaRusso, Giorgio Sacco, Paoletta Aletta, Antonino Colanino Ziino■ Registro tumori di Sondrio, ASL della Provincia diSondrio, Osservatorio epidemiologico. Sergio Maspero,Anna Clara Fanetti, Jacqueline Frizza, Elena Moroni, Ivan Cometti,Monica Lucia Annulli, Lorella Cecconami, Roberto Tessandori■ Registro tumori Piemonte, Centro di riferimento perl’epidemiologia e la prevenzione oncologica (CPO)Piemonte, AOU S.Giovanni Battista - Molinette, Torino.Roberto Zanetti, Stefano Rosso, Silvia Patriarca, Rossana Prandi,Irene Sobrato, Franca Gilardi, Paola Busso■ Registro tumori della Provincia di Trento, Servizioepidemiologia clinica e valutativa, Azienda provincialeper i servizi sanitari, Centro per i servizi sanitari. SilvanoPiffer, Maria A. Gentilini, Roberto Rizzello, Maddalena Cappelletti,Fernanda Dalsasso■ Registro tumori umbro di popolazione, Dipartimentodi specialità medico chirurgiche e sanità pubblica,Sezione di sanità pubblica, Università degli Studi diPerugia. Francesco La Rosa, Fabrizio Stracci, Daniela D’Alò,Massimo Scheibel, Daniela Costarelli, Francesco Spano, StefaniaRossini, Cinzia Santucci, Anna Maria Petrinelli, Clotilde Solimene,Fortunato Bianconi, Valerio Brunori■ Registro tumori della Lombardia, Provincia di Varese,Istituto nazionale per la ricerca sul cancro (INT). GiovannaTagliabue, Paolo Contiero, Lucia Preto, Andrea Tittarelli, SabrinaFabiano, Anna Maghini, Tiziana Codazzi, Emanuela Frassoldi,Daniela Gada, Laura di Grazia■ Registro tumori del Veneto, Padova. Angelo Paolo DeiTos, Maddalena Baracco, Emanuela Bovo, Antonella Dal Cin,Anna Rita Fiore, Alessandra Greco, Stefano Guzzinati, DanieleMonetti, Alberto Rosano, Carmen Stocco, Sandro Tognazzo■ Registro tumori dell’ASL di Brescia, Dipartimentoprogrammazione, acquisto e controllo, ASL di Brescia.Michele Magoni, Giuseppe Zani, Ornella Salvi, Maria Puleio,Claudia Gerevini, Cinzia Gasparotti, Roberta Chiesa, Fulvio Lonati■ Registro tumori della Provincia di Macerata, Scuola discienze mediche veterinarie, Università di Camerino.Susanna Vitarelli■ Registro tumori della Provincia di Trapani, Serviziosanitario Regione Sicilia, Dipartimento di prevenzione,Area igiene e sanità pubblica, ASP Trapani. GiuseppinaCandela, Tiziana Scuderi, Barbara Lottero, Michele Ribaudo■ Registro tumori della Provincia di Mantova,Dipartimento PAC, Osservatorio epidemiologico ASLProvincia di Mantova. Paolo Ricci, Linda Guarda, LucianaGatti, Annalaura Bozzeda, Maria Dall’Acqua, Vanda Pironi■ Registro tumori della Provincia di Catanzaro, ASP diCatanzaro, Servizio di epidemiologia e statisticasanitaria. Antonella Sutera Sardo, Adriana Mazzei, Anna MariaLavecchia, Pierina Mancuso■ Registro tumori di Nuoro, UO Registro tumori diNuoro, ASL di Nuoro e ASL di Lanusei.Mario Usala,Filomena Pala, Giovanna Maria Sini, Nicolina Pintori, Luisa Canu,Giuliana Demurtas, Nina Doa■ Registro tumori di Palermo e Provincia e Registrotumori della mammella di Palermo, UOC epidemiologia
clinica con Registro tumori di Palermo e Provincia,Dipartimento di scienze per la promozione della salute ematerno infantile “G. D’Alessandro”. Francesco Vitale,Rosanna Cusimano, Adele Traina, Agnese Guttadauro, MariaAntonietta Cascio, Rita Mannino, Barbara Ravazzolo, MariaAngela Brucculeri, Giuseppa Rudisi, Maria Stella Adamo, RosalbaAmodio, Alessandro Costa, Maurizio Zarcone, Raffaella Sunseri,Giovanni Bucalo, Carlo Trapani, Rosalba Staiti■ Registro tumori della Provincia di Como, ASL dellaProvincia di Como, Registro tumori e screening. GemmaGola, Mariangela Corti, Luigi Grandi■ Registro tumori integrato di Catania e Messina,Università degli studi di Catania, Dipartimento "GF.Ingrassia", Area igiene e sanità pubblica. Salvatore Sciacca,Salvatore Sciacchitano, Melchiorre Fidelbo, Giovanni Benedetto,Enrico Vasquez, Francesca Bella, Laura Calabretta, MarineCastaing, Alessia Di Prima, Antonio Ieni, Anna Leone,Paola Pesce, Carlo Sciacchitano, Antonina Torrisi, AntoniettaTorrisi, Massimo Varvarà■ Registro tumori della Provincia di Bergamo, Servizioepidemiologico aziendale, ASL della Provincia diBergamo. Giuseppe Sampietro, Silvia Ghisleni, Luisa Giavazzi,Andreina Zanchi, Alberto Zucchi■ Registro tumori dell’ASL Milano 1, Osservatorioepidemiologico e registri specializzati. Antonio GiampieroRusso, Maria Quattrocchi, Rosalba Distefano, Monica Sandrini,Alessandro Civaschi■ Registro tumori della provincia di Cremona, Servizioepidemiologia e registri di popolazione, ASL dellaProvincia di Cremona. Sabrina Bizzoco, Cristiano Belluardo,Chiara Davini, Silvia Lucchi, Marco Villa, Emanuela Anghinoni■ Registro tumori di Piacenza. Elisabetta Borciani, PietroSeghini, Rita Prazzoli■ Registro tumori di Lecce, UOC Epidemiologia estatistica, Azienda ASL Lecce. Anna Melcarne, FabrizioQuarta, Maria Grazia Golizia, Anna Maria Raho, Valentina DeMaria■ Registro tumori di Taranto, SC statisticaepidemiologia, Settore Registro Tumori. Sante Minerba,Antonia Minicuzzi, Simona Carone, Margherita Tanzarella■ Registro dei tumori infantili del Piemonte, SCDU Unitàdi epidemiologia dei tumori, Università di Torino, Centrodi riferimento per l’epidemiologia e la prevenzioneoncologica in Piemonte (CPO) Piemonte. Franco Merletti,Corrado Magnani, Guido Pastore, Benedetto Terracini, DanielaAlessi, Tiziana Cena, Fulvio Lazzarato, Vanda Macerata, MilenaMaule, Maria Luisa Mosso, Carlotta Sacerdote■ Registro dei tumori colorettali di Modena,Dipartimento di medicine e specialità mediche, Medicina1, Policlinico universitario di Modena.Maurizio Ponz deLeon, Federica Domati, Giuseppina Rossi, Carlo Alberto Goldoni,Shaniko Kaleci, Federica Rossi, Piero Benatti, Luca Roncucci,Carmela Di Gregorio, Giulia Magnani, Monica Pedroni, StefaniaMaffei, Francesco Mariani, Luca Reggiani-Bonetti■ Registro tumori infantili e negli adolescenti RegioneMarche, Centro ricerche igienistiche, sanitarie eambientali, Università di Camerino.Mario Cocchioni,Cristiana Pascucci■ Registro mesoteliomi Liguria, Istituto Nazionale per laricerca sul cancro (IST), Genova. Valerio Gennaro, LuciaBenfatto, Cecilia Lando, Giovanna Mazzucco
■ Banca dati Airtum, c/o Ispo Firenze.Emanuele Crocetti, Carlotta Buzzoni
Cancer Registries and AIRTUM contributors
AIRTUMWorking GroupCoordinators: Carlotta Buzzoni,1 Emanuele Crocetti1
Scientific contributors: Francesca Bella,2 Luigina Bonelli,3Adele Caldarella,1 Marine Castaing,2 Maria Cecilia Cercato,4
Luigino Dal Maso,5 Angelo Paolo Dei Tos,6 Stefano Ferretti,7
Adriano Giacomin,8 Fabio Pannozzo,9 Guido Mazzoleni,10
Silvia Patriarca,11 Saba Petrucci,12 Paola Pisani,13
Maurizio Ponz de Leon,14 Alberto Quaglia,3
Valerio Ramazzotti,4 Rosario Tumino,15 Marina Vercelli3,16
Representative of the AIRTUM Steering Board:Emanuele CrocettiCorresponding author: Carlotta Buzzoni, Istitutoper lo studio e la prevenzione oncologica (ISPO), Firenze;e-mail: [email protected]
1 Registro tumori toscano, Istituto per lo studio e la prevenzioneoncologica (ISPO), Firenze
2 Registro tumori integrato, Dipartimento di igiene e sanitàpubblica, Università di Catania
3 Registro tumori Regione Liguria, UOS prevenzione secondariae screening, IRCSS AOU S. Martino-IST, Genova
4 Istituto nazionale tumori “Regina Elena”, Roma5 Epidemiologia e biostatistica, Centro di riferimento oncologicoIRCSS, Aviano
6 Registro tumori del Veneto, Padova7 Università di Ferrara, Registro tumori Area VastaEmilia Centrale, Azienda USL Ferrara
8 Registro tumori Piemonte, Provincia di Biella, Centrodi riferimento per l’epidemiologia e la prevenzione oncologica(CPO) Piemonte, Centro di riferimento regionale
per l’epidemiologia e la prevenzione dei tumori9 Registro tumori di Latina10 Registro tumori dell’Alto Adige, Bolzano10 Registro Tumori Piemonte, Centro di riferimento perl’epidemiologia e la prevenzione oncologica (CPO) Piemonte,AOU S. Giovanni Battista-Molinette, Torino
11 Registro tumori umbro di popolazione, Dipartimento dispecialità medico-chirurgiche e sanità pubblica, Sezionedi sanità pubblica, Università degli studi di Perugia
12 Registro tumori infantili Piemonte, CPO Piemonte13 Registro tumori colorettali della Provincia di Modena,Policlinico universitario, Modena
14 Registro tumori della Provincia di Ragusa, Dipartimento di pre-venzione medica, Azienda sanitaria provinciale (ASP 7) Ragusa
15 Dipartimento di scienze della salute, Università di Genova

IndiceContents
3 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
I tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI
PREFAZIONE/FOREWORD . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
INTRODUZIONE/INTRODUCTION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
RIASSUNTO/ABSTRACT. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
DATI AIRTUMAIRTUM DATA
1 MATERIALI E METODI . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11MATERIALS AND METHODS
2 L’INCIDENZA DI SECONDI TUMORI IN PAZIENTI ONCOLOGICI IN ITALIA . . . . . . . . . . . . . . . . . . . . . 18INCIDENCE OF SECOND PRIMARY CANCERS IN ITALY
3 GUIDA ALLA LETTURA DELLE SCHEDE SPECIFICHE PER TUMORE . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31A GUIDE TO THE CANCER-SPECIFIC DATA SHEETS
4 RISULTATI: SCHEDE SPECIFICHE PER TUMORE . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39RESULTS: CANCER-SPECIFIC DATA SHEETS
WWW.EPIPREV.IT
TUTTI I TUMORI, . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 40ESCLUSO TUMORE DELLA CUTEALL SITES BUT SKIN CANCER
TUMORI DELLA TESTA E DEL COLLO . . . . . . . 42HEAD AND NECK CANCERS
TUMORE DELLA CAVITÀ ORALE . . . . . . . . . . . . . 44ORAL CAVITY CANCER
TUMORE DELLA FARINGE . . . . . . . . . . . . . . . . . . . . 46PHARYNX CANCER
TUMORE DELLA LARINGE . . . . . . . . . . . . . . . . . . . . 48LARYNX CANCER
TUMORE DELL’ESOFAGO . . . . . . . . . . . . . . . . . . . . . 50OESOPHAGUS CANCER
TUMORE DELLO STOMACO . . . . . . . . . . . . . . . . . . 52STOMACH CANCER
TUMORE DEL COLON RETTO . . . . . . . . . . . . . . . . . 54COLON RECTUM CANCER
TUMORE DEL COLON . . . . . . . . . . . . . . . . . . . . . . . . . . 56COLON CANCER
TUMORE DEL RETTO . . . . . . . . . . . . . . . . . . . . . . . . . . . 58RECTUM CANCER
TUMORE DEL FEGATO . . . . . . . . . . . . . . . . . . . . . . . . . 60LIVER CANCER
TUMORE DELLA COLECISTI . . . . . . . . . . . . . . . . . . 62GALLBLADDER CANCER
TUMORE DEL PANCREAS . . . . . . . . . . . . . . . . . . . . . 64PANCREAS CANCER
TUMORE DEL POLMONE . . . . . . . . . . . . . . . . . . . . . . 66LUNG CANCER
MELANOMA CUTANEO . . . . . . . . . . . . . . . . . . . . . . . . 68SKIN MELANOMA
MESOTELIOMA . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 70MESOTHELIOMA
SARCOMA DI KAPOSI . . . . . . . . . . . . . . . . . . . . . . . . . 72KAPOSI SARCOMA
TUMORE DEI TESSUTI MOLLI . . . . . . . . . . . . . . . . 74SOFT TISSUE CANCER
TUMORE DELL’OSSO . . . . . . . . . . . . . . . . . . . . . . . . . . . 76BONE CANCER
TUMORE DEL RENE . . . . . . . . . . . . . . . . . . . . . . . . . . . 78E DELLA PELVI RENALEKIDNEY AND RENAL PELVIS CANCER
TUMORE DELLA VESCICA . . . . . . . . . . . . . . . . . . . . 80E DELLE VIE URINARIEBLADDER AND URINARY TRACT CANCER
TUMORE DELLA VESCICA . . . . . . . . . . . . . . . . . . . . 82URINARY BLADDER CANCER
TUMORE DELLE VIE URINARIE . . . . . . . . . . . . . . 84URINARY TRACT CANCER
>>

WWW.EPIPREV.IT
4 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
I tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI
5 VALUTAZIONE DELLE ASSOCIAZIONI TRA SOGGETTI CON TRE O PIÙ TUMORI . . . . . . . . . . .109EVALUATION OF ASSOCIATIONS IN SUBJECTS WITH THREE OR MORE CANCERS
6 RUOLO DELLE CLASSIFICAZIONI NELLE DEFINIZIONI DI TUMORI MULTIPLI . . . . . . . . . . . . . . .114ROLE OF CLASSIFICATION SYSTEMS IN THE DEFINITION OF MULTIPLE PRIMARY CANCERS
7 I TUMORI MULTIPLI SINCRONI . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .120SYNCHRONOUS MULTIPLE CANCERS
8 VALUTAZIONE DEL RISCHIO DI SECONDI TUMORI DELLE NEOPLASIE . . . . . . . . . . . . . . . . . . . . . .125DELL’APPARATO EMOLINFOPOIETICO ALLA LUCE DELLA CLASSIFICAZIONEWHO 2008RISK ASSESSMENT OF SECOND CANCER INCIDENCE OF TUMOURS OF THE HAEMATOPOIETICAND LYMPHOID TISSUE IN LIGHT OF THE 2008WHO CLASSIFICATION
9 RISCHIO DI SECONDO TUMORE IN DIVERSE FASCE D’ETÀ. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .133RISK OF SECOND PRIMARY CANCER IN DIFFERENT AGE GROUPS
10 IL SIGNIFICATO CLINICO DEI TUMORI MULTIPLI . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .147CLINICAL INTERPRETATION OF MULTIPLE PRIMARY CANCERS
APPENDICEAPPENDIX
LA RETE DEI REGISTRI AIRTUM . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .149THE NETWORK OF THE AIRTUM CANCER REGISTRIES
TUMORE DELL’ENCEFALO . . . . . . . . . . . . . . . . . . . 86E DEL SISTEMA NERVOSO CENTRALEBRAIN AND CENTRALNERVOUS SYSTEM CANCER
TUMORE DELLA TIROIDE . . . . . . . . . . . . . . . . . . . . 88THYROID CANCER
LINFOMA DI HODGKIN . . . . . . . . . . . . . . . . . . . . . . . 90HODGKIN LYMPHOMA
LINFOMA NON-HODGKIN . . . . . . . . . . . . . . . . . . . 92NON-HODGKIN LYMPHOMA
MIELOMA . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 94MYELOMA
LEUCEMIE . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 96LEUKAEMIAS
LEUCEMIE LINFOIDI . . . . . . . . . . . . . . . . . . . . . . . . . . 98LYMPHOID LEUKAEMIAS
LEUCEMIE MIELOIDI . . . . . . . . . . . . . . . . . . . . . . . . . . 100MYELOID LEUKAEMIAS
TUMORE DELLA MAMMELLA . . . . . . . . . . . . . . . . 102BREAST CANCER
TUMORE DELLA CERVICE . . . . . . . . . . . . . . . . . . . . . 104UTERINACERVIX UTERI CANCER
TUMORE DEL CORPO DELL'UTERO . . . . . . . . . 105CORPUS UTERI CANCER
TUMORE DELL’OVAIO . . . . . . . . . . . . . . . . . . . . . . . . . 106OVARY CANCER
TUMORE DELLA PROSTATA . . . . . . . . . . . . . . . . . . 107PROSTATE CANCER
TUMORE DEL TESTICOLO . . . . . . . . . . . . . . . . . . . . . 108TESTIS CANCER
>> RISULTATI: SCHEDE SPECIFICHE PER TUMORERESULTS: CANCER-SPECIFIC DATA SHEETS
MATERIALE AGGIUNTIVO ON-LINE www.epiprev.itONLINE SUPPLEMENTARY MATERIALSchede singole complete per sede di primo tumore in file formato ExcelComplete Excel sheets for site of first cancer
Schede per sede di primo tumore con SIR completi di Intervallo di Confidenza in file unico in formato ExcelExcel sheets for site of first cancer including SIR with confidence intervals

WWW.EPIPREV.IT PrefazioneForeword
5 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
I tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI
E’ con piacere che introduco i lettori a un nuovo lavorodell’AIRTUM, innanzitutto perché costituisce un’occasioneper sottolineare che la collaborazione tra l’Associazione e ilMinistero della salute/CCM, iniziata nel 2005, è uno deglielementi che contribuisce a una produzione scientifica si-gnificativa e ampia, utile non solo alla ricerca, ma anche -forse soprattutto - alle iniziative di sanità pubblica.Lo studio del rischio di sviluppare tumori multipli nel no-stro Paese non sarebbe stato possibile senza l’ampliamentodella popolazione italiana coperta da un Registro tumori,senza la creazione e il rafforzamento della Banca Dati AIR-TUM e senza la standardizzazione dei metodi e dei criterioperativi dei singoli Registri, tutte attività che sono state og-getto delle convenzioni e degli accordi tra Ministero dellasalute/CCM e AIRTUM negli ultimi anni.Così come per le precedenti pubblicazioni, l’obiettivo di farsì che le scelte di sanità pubblica, sia a livello nazionale siaregionale, siano guidate dall’evidenza scientifica e dalla suaconoscenza si può dire soddisfatto.Tra i risultati dello studio illustrato nel presente Rapportomi sembra particolarmente importante sottolineare l’indi-cazione che i malati di cancro hanno un rischio aumentatodi sviluppare ulteriori tumori rispetto alla popolazione ge-nerale (quantificabile in circa il 10%) per le sedi tumoraliche condividono la medesima esposizione a fattori cance-rogeni del primo tumore (si veda, per esempio, il caso deitumori correlati a fumo e alcol).Le attività di prevenzione, quindi, volte a modificare gli stilidi vita in direzioni più salutari, possono avere un effetto po-sitivo non solo nella popolazione generale, ma anche in sot-togruppi di popolazione ai quali sia già stato diagnosticatoun tumore, e tali interventi devono essere sempre racco-mandati e attuati.Ringraziando AIRTUM per lo sforzo compiuto, non possoche augurare un’ampia diffusione e un’attenta lettura del-l’opera.
Giuseppe RuoccoDirettore generale della prevenzione
Ministero della salute
It is with pleasure that I introduce readers to a new work byAIRTUM, primarily because it is an opportunity to highlighthow the collaboration between the Association and the Ministryof Health/CCM, which began in 2005, contributes to a sig-nificant, extensive scientific production. This is useful for re-search, but also – and perhaps more importantly – for publichealth initiatives.It would not have been possible to study the risk of developingmultiple tumours in our Country if it had not been for the ex-pansion of the cancer registry coverage of the Italian population,the creation and ongoing improvement of the AIRTUMData-base, and the standardization of methods and procedures amongregistries. All these were achieved thanks to the cooperation be-tween the Ministry of Health/CCM and AIRTUM in recentyears.This publication, as was the case with the previous ones, makesit possible to base public health policy – at both national andregional levels – on scientific evidence.Among the results of the study presented in this monograph, Ifind it particularly important to stress that cancer patients havean increased risk (estimated at about 10%) of developing ad-ditional cancers, compared to the general population, for cancersites that share the same exposure to carcinogenic factors as thefirst (e.g., smoke- and alcohol-related cancer).Consequently, prevention measures that promote healthierlifestyles can have a positive effect not only within the generalpopulation but even among cancer patients, and must thereforealways be recommended and implemented.I want to thank AIRTUM for this work, which I hope willbe widely disseminated and receive due attention.
Giuseppe RuoccoDirector General of Prevention
Ministry of Health

WWW.EPIPREV.IT IntroduzioneIntroduction
I tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI
Questa nuova pubblicazione affronta un aspetto nuovodella malattia oncologica rispetto agli indicatori epidemio-logici di incidenza, mortalità, sopravvivenza e prevalenza.I tumori non sono osservati nella popolazione generale, matra i pazienti che hanno già avuto un’esperienza oncologica.La monografia ha proprio come obiettivo principale la valu-tazione del rischio di sviluppare un secondo tumore in chi hagià avuto una precedente diagnosi, e affronta anche le situa-zioni meno frequenti di coesistenza di tre o più neoplasie.Le persone che vivono dopo una diagnosi di tumore sonosempre più numerose e rappresentano oltre il 4% della po-polazione italiana. Lo studio dei tumori successivi al primoè importante per molti aspetti. Prima di tutto per quanti-ficare, per sede di primo e sede di secondo tumore, sequesto rischio sia diverso per i pazienti rispetto alla popo-lazione generale. Poi per i clinici, per contribuire con datiquantitativi, specifici per sesso e sede, e stratificati pertempo dalla diagnosi, alla definizione del follow-up più ap-propriato dei loro pazienti. Ma anche per aumentare le co-noscenze sull’eziopatogenesi dei tumori, attraverso l’evi-denza di associazioni, spesso bidirezionali, fra sedi tumoraliche condividono le stesse esposizioni e per suggerire nuoveipotesi eziologiche. I tumori multipli possono essere espres-sione di sindromi ereditarie e anche effetto di trattamentiiatrogeni. Si tratta di elementi che speriamo siano utili a ot-timizzare le strategie di prevenzione, diagnosi precoce e te-rapia, in un’ottica di efficienza ed equità.Nella pubblicazione sono ampiamente discussi anche gliaspetti metodologici, spesso sottovalutati, che devono essereinvece ben chiari per una corretta interpretazione del dato.Sono quindi molteplici i punti di vista dai quali è possibile“leggere” i dati di questa pubblicazione, sia relativi alle schedespecifiche per tumore sia ai capitoli di commento, e sono tantigli utenti ai quali AIRTUM offre questo nuovo prodottofrutto dello sforzo collaborativo dei Registri tumori italiani.Questa monografia nasce col supporto che il Centro per ilcontrollo e la prevenzione delle malattie (CCM) del Mini-stero della salute da molti anni concede ad AIRTUM. Il no-stro ringraziamento si accompagna all’augurio che AIR-TUM possa essere presto legittimata per quello che è già neifatti: una rete di sorveglianza, basata sulla qualità e la con-frontabilità dei dati, ben rappresentata nel territorio nazio-nale e orientata a una sempre maggiore e più dettagliata co-noscenza della patologia oncologica nel nostro Paese.
Consiglio DirettivoAssociazione italiana registri tumori (AIRTUM)
This publication of the Italian Association of Cancer Registries(AIRTUM) deals with a particular aspect of cancer which isa new addition to the traditional epidemiological indicatorsof incidence, mortality, survival, and prevalence published bythe association.Cancer is measured and described here not in the general pop-ulation, but among patients who have already had a cancerexperience.The main objective of this monograph is to assess the risk ofdeveloping a second cancer in subjects who have already hada previous cancer diagnosis, in comparison with the generalpopulation. The work focuses on the risk of second cancers, butalso addresses the less frequent situations of coexistence of threeor more tumours.People living with a cancer diagnosis are more andmore numerousand represent more than 4% of the Italian population.The studyof second cancers is important in many respects. First of all, forpatients, to quantify whether their risk is different from that ofthe general population. Then for clinicians, to help them definethe most appropriate follow-up of their patients, by providingquantitative data, both sex- and site-specific, as well as stratifiedby time since diagnosis. But also to increase the knowledge onthe aetiopathogenesis of cancer, through the evidence of, oftenbi-directional, associations between cancer sites that share thesame exposure, and to suggest new possible etiological hypotheses.Multiple tumours may be an expression of hereditary syndromesand even of the iatrogenic effect of treatments. All these elementsmay prove useful to optimize strategies for prevention, early di-agnosis, and therapy, in the interest of efficiency and fairness.The publication includes an extensive discussion of the method-ological aspects, which are often underrated, whereas they needto be well understood to ensure that data is correctly interpreted.The data presented in the cancer-specific fact sheets and ineach chapter can be “read” from many points of view, addressinga broad readership.This monograph was made possible by the support that theCentre for Disease Control and Prevention (CCM) of the Min-istry of Health has provided to AIRTUM for many years. Ourthank for this vital support is accompanied by the wish thatAIRTUM may soon receive official recognition for the role italready plays in practice, that of a surveillance network thatcan rely on high data quality and comparability, is well repre-sented throughout the Country and strives to achieve an evergreater and more detailed knowledge of cancer in our Country.
Steering CommitteeItalian Association of Cancer Registries (AIRTUM)
6 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152

WWW.EPIPREV.IT
OBIETTIVI.Questo studio collaborativo, basato sui dati rac-colti dai registri dell’Associazione italiana dei registri tumori(AIRTUM), fornisce stime aggiornate del rischio di inci-denza di tumori multipli (MP). L’obiettivo è di evidenziaree quantificare le associazioni tra diverse patologie oncolo-giche. La quantificazione dell’eccesso o del difetto di rischiodi ulteriori neoplasie, rispetto alla popolazione generale, neipazienti già affetti da un tumore può contribuire a com-prenderne l’eziologia e a indirizzare il follow-up clinico.
MATERIALI E METODI. I dati sono forniti dai registri tumoridi popolazione facenti parte dell’AIRTUM, che attualmentecopre il 47% della popolazione italiana. Sono stati utilizzatii dati della Banca dati AIRTUM (dicembre 2012) inclu-dendo le informazioni raccolte su tutti i tumori maligni dia-gnosticati tra il 1976 e 2010. Tutti i casi sono codificati se-condo ICD-O-3. Sono stati esclusi i tumori nonmelanomatosi della cute, i casi diagnosticati sulla base del solocertificato di morte, i casi autoptici con diagnosi post morteme quelli con tempo di follow-up pari a zero. E’ stata adottatala definizione dei tumori multipli di IARC-IACR(http://www.iacr.com.fr/MPrules_july2004.pdf). I dati sonostati sottoposti ai consueti controlli di qualità previsti dal pro-tocollo di gestione della Banca dati AIRTUM e a controlli diqualità specifici per il fenomeno in studio. Una coorte di pa-zienti oncologici è stata seguita nel tempo, dalla diagnosi delprimo tumore fino all’eventuale diagnosi di secondo tumoreo al decesso o alla data di fine follow-up, con l’obiettivo divalutare se il numero di secondi tumori diagnosticati fosse su-periore o inferiore rispetto a quanto atteso nella popolazionegenerale. Gli anni-persona a rischio (PY) sono stratificati persede del primo tumore, area geografica (Nord, Centro, Sude Isole), età compiuta e periodo temporale.Tutti i secondi tu-mori diagnosticati nei pazienti della coorte sono stati inclusinel numero di casi osservati. Il numero di casi attesi è statocalcolato moltiplicando la somma dei PY per i tassi di rife-rimento, calcolati sulla casistica della Banca dati AIRTUM,stratificando per sede tumorale, area geografica, età e periododi calendario. E’ stato calcolato il rapporto standardizzato diincidenza (Standardized Incidence Ratio - SIR) come rapportotra numero di casi osservati e attesi. E’ stato calcolato anchel’eccesso assoluto di rischio (Excess Absolute Risk - EAR) di se-condo tumore (rispetto al valore atteso) sottraendo al numerodei casi osservati il numero dei casi attesi. La differenza è statapoi divisa per gli anni-persona a rischio; il numero di casi in
OBJECTIVES.This collaborative study, based on data collectedby the network of Italian association of cancer registries (AIR-TUM), provides updated estimates on the incidence risk ofmultiple primary cancer (MP). The objective is to highlightand quantify the bidirectional associations between differentoncological diseases. The quantification of the excess or decreasedrisk of further cancers in cancer patients, in comparison withthe general population, may contribute to understand the ae-tiology of cancer and to address clinical follow-up.
MATERIAL AND METHODS.Data herein presented were pro-vided by AIRTUM population-based cancer registries, whichcover nowadays 47% of the Italian population.This monograph utilizes the AIRTUM Database (December2012), considering all malignant cancer cases diagnosed between1976 and 2010. All cases are coded according to ICD-O-3.Non-melanoma skin cancer cases, cases based on death certificateonly, cases based on autopsy only, and cases with follow-up timeequal to zero were excluded. To define multiple primaries,IARC-IACR rules were adopted (http://www.iacr.com.fr/MPrules_july2004.pdf ).Data were subjected to standard quality control procedures(described in the AIRTUM data management protocol) andspecific quality control checks defined for the present study. Acohort of cancer patients was followed over time from firstcancer diagnosis until the date of second cancer diagnosis, death,or the end of follow-up, to evaluate whether the number of ob-served second cancer cases was greater than expected. Person-years at risk (PY) were computed by first cancer site, geographicarea (North, Centre, South and Islands), attained age, andattained calendar-year group. All second cancers diagnosed inthe cohort’s patients were included in the observed numbers ofcases. The expected number of cancer cases was computed mul-tiplying the accumulated PY by the expected rates, calculatedfrom the AIRTUMDatabase stratified by cancer site, geographicarea, age, and calendar-year group.The Standardized IncidenceRatio (SIR) was calculated as the ratio of observed to expectedcancer cases. The Excess Absolute Risk (EAR) beyond the ex-pected amount were calculated subtracting the expected numberof subsequent cancers from the observed number of cancer cases;the difference was then divided by the PY and the number ofcancer cases in excess (or deficit) was expressed per 1,000 PY.Confidence intervals were stated at 95%.The two months (60days) after first cancer diagnosis were defined as “synchronicityperiod”, and in the main analysis observed and expected cases
RiassuntoAbstract
7 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
I tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI

Epidemiol Prev 37 (4-5) Suppl 1:1-152 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.it8
I tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI Riassunto
during this period were excluded. It was estimated the excessrisk in the period after first diagnosis (≥ 0 months), excludingthe synchronicity period (≥ 2 months), and during the followingperiods: 2-11, 12-59, 60-119 and 120 months after diagnosis.First-cancer-site-and-gender-specific sheets are presented, re-porting both SIRs and EARs.
RESULTS. For 5,979,338 person-years a cohort of 1,635,060cancer patients (880,361 males and 754,699 females) diag-nosed between 1976 and 2010 was followed. The mean fol-low-up length was 14 years. Overall, 85,399 metachronous(latency ≥2 months) cancers were observed, while 77,813 wereexpected during the study period: SIR: 1.10 (95%CI 1.09-1.10), EAR: 1.32 x 1,000 person-years (95%CI 1.19 - 1.46).The SIR was 1.08 (95%CI 1.08-1.09) for men (54,518 ob-served and 50,260 expected) and 1.12 (95%CI 1.11-1.13)for women (30,881/27,553), and the EAR 1.61 (95%CI1.37-1.84) and 1.08 x 1,000 person-years (95%CI 0.93-1.24), respectively. Moreover, during the first two months afterfirst cancer diagnosis (synchronous period) 14,807 cancers wereobserved while 3,536 were expected (SIR: 4.16; 95%CI 4.09-4.22); the SIR was 4.08 (95%CI 4.00-4.16) for men and4.32 (95%CI 4.20-4.45) for women.The mean age of patientsat first cancer diagnosis was 67.0 years among males and 65.8among females. The risk of MP was related to age being higherfor younger patients and lower for older ones. In relation tothe time of first cancer diagnosis, the SIR was very high at thebeginning and then decreased, although remaining constantlyover 1, and then rose over time. No strong differences were ev-ident across the different incidence periods, which all showedan increased MP risk.Women had higher SIRs than expectedfor 18 cancer sites, men for 12. The statistically significantlySIRs lower than 1 were 2 and 8, respectively. Increased overallMP risk was observed for patients of both sexes with a firstprimary in the oral cavity (SIR men: 1.93; SIR women: 1.48),pharynx (SIR men: 2.13; SIR women: 1.99), larynx (SIRmen: 1.57; SIR women: 1.79), oesophagus (SIR men: 1.45;SIR women: 1.41), lung (SIR men: 1.09; SIR women: 1.13),kidney (SIR men: 1.14; SIR women: 1.15), urinary bladder(SIR men: 1.29; SIR women: 1.22), thyroid (SIR: 1.22 inboth sexes), Hodgkin lymphoma (SIR men: 1.59; SIR women:1.94), and non-Hodgkin lymphoma (SIR men: 1.13; SIRwomen: 1.12), and for the heterogeneous group “other sites”(SIR men: 1.09; SIR women: 1.07). Moreover, men had ahigher MP risk if the first cancer was in the testis (SIR: 1.24),while the same was true for women with gallbladder (SIR:1.21), skin melanoma (SIR: 1.17), bone (SIR: 1.41), breast(SIR: 1.12), cervix uteri (SIR: 1.23) and corpus uteri (SIR:1.23), and ovarian cancer (SIR: 1.18). On the contrary, afirst liver or pancreas cancer were associated with a decreasedMP risk in both sexes (liver SIR: 0.86 and 0.81 for men andwomen, respectively; pancreas SIR: 0.70 and 0.78 for menand women, respectively), as were those of colon (SIR: 0.93),
eccesso o in difetto è stato espresso per 1.000 anni-persona.Sono stati calcolati gli intervalli di confidenza al 95%. I 2mesi (60 giorni) successivi alla diagnosi di primo tumore sonostati definiti periodo di sincronicità e, nelle analisi principali,sono stati esclusi i casi osservati e attesi durante questo pe-riodo, poiché a seguito della diagnosi di un tumore un pa-ziente è sottoposto a una serie di accertamenti con l’obiettivodi definire la natura e l’estensione della neoplasia; questiesami possono portare anche all’identificazione di altre neo-plasie presenti ma non (ancora) sintomatiche. L’eccesso di ri-schio è stato misurato in tutto il periodo successivo allaprima diagnosi (≥0 mesi), con esclusione del periodo di sin-cronicità (≥2 mesi) e nei seguenti periodi: 2-11, 12-59, 60-119 e 120 mesi dalla diagnosi. Nella monografia sono pre-sentate schede specifiche per sede di primo tumore e genere,nelle quali è riportato l’eccesso di rischio di incidenza di se-condo tumore, sia in termini di SIR, sia in termini di EAR.
RISULTATI. E’ stata seguita una coorte di 1.635.060 pazienti(880.361 maschi e 754.699 femmine) a cui è stato diagno-sticato un tumoremaligno tra il 1976 e il 2010.Tali casi sonostati seguiti per un follow-up pari a 5.979.338 anni-persona,con una durata media del follow-up di circa 14 anni. Nelcomplesso sono stati osservati 85.399 secondi tumori meta-croni (latenza fra diagnosi del primo e del secondo tumore ≥2mesi), mentre erano attesi 77.813 tumori in base all’incidenzadella popolazione generale. Il rapporto fra tassi standardizzatid’incidenza è 1,10 (IC95% 1,09-1,10), l’EAR è 1,32 per1.000 anni-persona (IC95% 1,19-1,46). Il SIR è 1,08(IC95% 1,08-1,09) per gli uomini (54.518 osservati vs.50.260 attesi) e 1,12 (IC95% 1,11-1,13) per le donne(30.881 vs. 27.553), con EAR 1,61 (IC95% 1,37-1,84) e1,08 (IC95% 0,93-1,24) per 1.000 anni-persona, rispettiva-mente. Il rischio diMP cambia in relazione all’età, essendo piùelevato nei pazienti più giovani e più basso in quelli più an-ziani. Rispetto alla diagnosi del primo tumore i SIR sonomolto elevati all’inizio, poi diminuiscono, pur mantenendosisempre oltre l’unità, e successivamente tornano a crescere: du-rante i primi duemesi dopo la prima diagnosi di tumore (pe-riodo sincrono) si sono osservati 14.807 tumori contro 3.537attesi (SIR: 4,16; IC95% 4,09-4,22); il SIR era 4,08 (IC95%4,00-4,16) per gli uomini e 4,32 (IC95% 4,20-4,45) per ledonne. L’età media al primo tumore era di 67,0 anni nei ma-schi e 65,8 nelle femmine. Non sono state osservate differenzesostanziali fra i diversi periodi di incidenza; in tutti è presenteun aumento del rischio di MP. Le donne presentano un SIRmaggiore dell’unità per 18 sedi tumorali, gli uomini per 12.I SIR statisticamente significativi inferiori a 1 sono rispettiva-mente 2 e 8. Un aumento del rischio complessivo di MP èpresente per i pazienti di entrambi i sessi, con un primo tu-more della cavità orale (SIR uomini: 1,93; SIR donne: 1,48),della faringe (SIR uomini: 2,13; SIR donne: 1,99), della la-ringe (SIR uomini: 1,57; SIR donne: 1,79), dell’esofago (SIR

Epidemiol Prev 37 (4-5) Suppl 1:1-152 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.it9
I tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI Riassunto
rectum (SIR: 0.83), gallbladder (SIR: 0.80), prostate (SIR:0.93), mesothelioma (SIR: 0.65), and central nervous system(SIR: 0.82) among men. Among the cancers for which theEAR is statistically significant, those with higher Excess AbsoluteRisk of MP were those of the oral cavity (EAR: 16.0 x 1,000person-years in men and 5.4 in women), pharynx (17.6 and9.1), larynx (11.4 and 8.8), and oesophagus (8.5 and 4.8).
DISCUSSION.This descriptive study provides quantitative in-formation on the risk of developing a second cancer in anItalian population-based cohort of approximately 1.65 millioncancer patients, compared to the risk of the general population.During the follow-up time (on average 14 years) cancer patientshad an MP risk that was 10% higher in comparison to thegeneral population and an Excess Absolute Risk of 1.32 x 1,000person-years. Study of MPs and their risk measures are depend-ent on methods used in the calculation. The definition of MPis not univocal and using different rules can greatly change thenumber of cancers in a patient with MPs. However, the AIR-TUM cancer registries adopt the same recommendations forMP definition. This monograph was therefore made possibleby the shared rules and standards used by AIRTUM registries.The cancer site-specific sheets, which represent the core of themonograph, can be useful to highlight and quantify the bidi-rectional associations among different diseases and thereforeprovide indications for clinical follow-up. Lifestyle changes inmore healthful directions can have a positive effect in the cancerpatient population and should always be recommended.
Keywords:cancer, second primary, registries, Italy, risk assessment
uomini: 1,45; SIR donne: 1,41), del polmone (SIR uomini:1,09; SIR donne: 1,13), del rene (SIR uomini: 1,14; SIRdonne: 1,15), della vescica (SIR uomini: 1,29; SIR donne:1,22), della tiroide (SIR: 1,22 in entrambi i sessi), linfoma diHodgkin (SIR uomini: 1,59; SIR donne: 1,94), e linfomanon-Hodgkin (SIR uomini: 1,13; SIR donne: 1,12) e per ilgruppo eterogeneo “altre sedi” (SIR uomini: 1,09; SIR donne:1,07). Inoltre, tra gli uomini si osserva un rischio aumentatodi MP se la sede di primo tumore è il testicolo (SIR: 1,24),tra le donne se la sede del primo tumore è la colecisti (SIR:1,21), il melanoma cutaneo (SIR: 1,17), l’osso (SIR: 1,41), lamammella (SIR: 1,12), la cervice uterina (SIR: 1,23) e il corpodell’utero (SIR: 1,23) o l’ovaio (SIR: 1,18). Al contrario, unprimo tumore del fegato o del pancreas sono associati, in en-trambi i sessi, a un rischio ridotto di MP (SIR fegato: 0,86 e0,81 per uomini e donne rispettivamente; SIR pancreas: 0,70e 0,78 per uomini e donne rispettivamente), così come, tra gliuomini, lo è il tumore del colon (SIR: 0,93), del retto (SIR:0,83), della colecisti (SIR: 0,80), della prostata (SIR: 0,93),il mesotelioma (SIR: 0.65) e i tumori del sistema nervoso cen-trale (SIR: 0,82).Tra le neoplasie per le quali l’EAR è statisti-camente significativo, quelle con valori più elevati sono i tu-mori del cavo orale (EAR: 16,0 per 1.000 persone l’anno negliuomini e 5,4 nelle donne), della faringe (17,6 e 9,1), della la-ringe (11,4 e 8,8) e dell’esofago (8,5 e 4,8).
DISCUSSIONE.Questo studio descrittivo fornisce informa-zioni quantitative sul rischio di sviluppare un secondo tu-more in una coorte su base di popolazione di circa1.650.000 malati di cancro diagnosticati in Italia rispetto alrischio della popolazione generale. Durante un periodo me-dio di follow-up di 14 anni, i malati di tumore hanno mo-strato un aumento del rischio di MP del 10% in confrontoalla popolazione generale e un eccesso assoluto di rischio di1,32 x 1.000 anni-persona. Lo studio sui tumori multipli ele relative misure di rischio sono fortemente dipendenti daimetodi adottati per il loro calcolo. La definizione stessa ditumori multipli è variabile e l’uso di regole diverse può no-tevolmente modificare il numero di tumori MP in un pa-ziente. Tuttavia i registri tumori AIRTUM adottano le stesseraccomandazioni per la definizione dei MP. E’ stato quindipossibile produrre una monografia su questo tema grazie allacondivisione di regole e standard operata da AIRTUM. Letabelle specifiche per sede di primo tumore, che rappresen-tano il nucleo della monografia, possono essere utili per evi-denziare e quantificare le associazioni bidirezionali tra diversepatologie e guidare il follow-up clinico. Le modifiche deglistili di vita in direzioni più salutari possono avere un effettopositivo anche nella popolazione oncologica e devono esseresempre raccomandate.
Parole chiave:cancro, tumori multipli, registri, Italia, valutazione del rischio


WWW.EPIPREV.IT
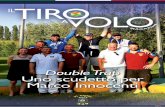
LA RETE DEI REGISTRI TUMORI ITALIANIL’Associazione italiana dei registri tumori italiani (AIR-TUM)1 raccoglie i dati dei Registri tumori di popolazionegenerali e specializzati e, dopo averne verificato qualità ecompletezza, li utilizza per studi collaborativi di tipo descrit-tivo e attività di ricerca sull’epidemiologia oncologica in Ita-lia.2-4 L’attività di registrazione si è sviluppata nel nostroPaese a partire dagli anni Settanta con una graduale e co-stante crescita delle esperienze e della parte di popolazioneitaliana interessata.AIRTUM attualmente include 38 Registri tumori generali ecinque specializzati: il Registro dei tumori colorettali della Pro-vincia diModena, il Registro dei tumori della mammella fem-minile della Provincia di Palermo, il Registro dei mesoteliomidella Regione Liguria e i due Registri dei tumori infantili eadolescenziali delle Regioni Piemonte e Marche (figura 1).La copertura regionale varia dallo 0% per alcune regioni (Ba-silicata, Abruzzo, Molise e Valle d’Aosta) al 100% per altre(Umbria, Friuli Venezia Giulia e Trentino-Alto Adige).Oggi circa 30 milioni di cittadini italiani, pari al 48% dellapopolazione, risiedono in un’area in cui è attivo un Registro
THE ITALIAN NETWORK OF CANCER REGISTRIESThe Italian Network of Cancer Registries (AIRTUM)1 collectsdata from both general and specialized population-based can-cer registries. AIRTUM verifies data quality and completenessand uses data for collaborative studies on cancer epidemiologyin Italy.2-4 Cancer registration in Italy started in the Seventiesand has gradually expanded, involving a growing proportionof the Italian resident population.AIRTUM includes 38 general cancer registries and five special-ized ones: the Colorectal cancer registry in the Province ofModena, the Female breast cancer registry in the Province ofPalermo, the Mesothelioma cancer registry in the Region of Lig-uria, and the two specialized childhood registries in the Regionsof Piedmont and Marche (figure 1).Regional coverage ranges from 0% for some regions (Basilicata,Abruzzo, Molise, and Valle d’Aosta) up to 100% (Umbria,Friuli Venezia Giulia, and Trentino-Alto Adige).Overall, the AIRTUM cancer registries today monitor almost30 million people, or 48% of the Italian population (59% inthe North-West, 70% in the North-East, 27% in the Centre,and 39% in the South and Islands) (table 1).Since 2005, AIRTUM has had a central database, whichstores the data from all accredited cancer registries.5 In theAIRTUM Database it is possible to identify many patientswith multiple primary cancers,6-9 thanks both to the extremelylarge number of cancer registries and to the presence of histor-ical registries operating since the Eighties.
DATA SELECTION AND QUALITYThis monograph uses data from the AIRTUM Database (atDecember 2012) regarding all cancer cases, except non-melanoma skin cancer, diagnosed between 1976 and 2010 inthe general cancer registries.All cases sent to the AIRTUM Database are coded accordingto the ICD-O-3.10
Non-malignant tumours were excluded, with the exception ofthose of the urinary bladder because of the variations in reg-istration and classification of behaviour for this cancer site.11
The Brescia Cancer Registry was excluded as it was unable toprovide a continuous set of data. In addition, data don’t in-clude:A. cases based on death certificate only;B. cases based on autopsy only;C. cases with follow-up time equal to zero.
Materiali e metodiMaterials and methods
Capitolo 1
11 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
I tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI
NORTH-WEST 59%
NORTH-EAST 70%
CENTRE 27%
SOUTH AND ISLAND 39%
Figura 1. Aree coperte dai registritumori AIRTUM nel 2013.Figure 1. Italian areas covered byAIRTUM cancer registries in 2013.

In order to define multiple primaries, AIRTUM follows theIARC-IACR rules.12
The same cancer sites were analyzed both for first and for sec-ond cancer (table 2).Data are double checked (by each registry and by the centraldatabase) with the DEPedits program. In addition, otherchecks were carried out based on the software developed byAIRTUM (CheckAIRTUM).13 CheckAIRTUM comparesdata from a particular registry with the weighted average ofthe other registries in the database.A specific quality evaluation was performed for this mono-graph. For each registry, both sexes, and all cancer sites together,the percentage analyzed were the following:■ the percentage of multiple cancer cases out of all cancer cases;■ the percentage of multiple cancer cases diagnosed within 5years of the previous cancer diagnosis out of all cancer cases;■ the percentage of multiple cancer cases out of all cancer cases,by period of incidence;■ the percentage of hematopoietic and lymphoid neoplasms (lym-phoma, leukaemia, or multiple myeloma) subsequent to cancer inthe same sites out of all hematopoietic and lymphoid cancer cases;
Materiali e metodiI tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI
12 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
REGION ITALIAN RESIDENTS IN AREASPOPULATION COVERED BY GENERAL
CANCER REGISTRIES
No. No. %Piemonte (general and specialized) 4 357 663 1 629 321 37Valle d’Aosta 126 620 0 0Lombardia 9 700 881 6 800 70 70Liguria 1 567 339 853 939 54
NORTH-WEST 15 752 503 9 283 965 59Trentino-Alto Adige 1 029 585 1 029 585 100Veneto 4 853 657 2 311 112 48Friuli Venezia Giulia 1 217 780 1 217 780 100Emilia-Romagna 4 341 240 3 427 272 79
NORTH-EAST 11 442 262 7 985 749 70Toscana 3 667 780 1 217 531 33Umbria 883 215 883 215 100Marche (general and specialized) 1 540 688 537 667 35Lazio 5 500 022 544 887 10
CENTRE 11 591 705 3 183 300 27Abruzzo 1 306 416 0 0Molise 313 145 0 0Campania 5 764 424 1 659 608 29Puglia 4 050 072 1 385 399 34Basilicata 577 562 0 0Calabria 1 958 418 234 334 12Sicilia 4 999 854 4 107 051 82Sardegna 1 637 846 706 845 43
SOUTH AND ISLANDS 20 607 737 8 093 237 39
ITALY 59 394 207 28 546 251 48
Tabella 1. Distribuzione della popolazione italiana totale e residente nelle areecoperte dai registri tumori AIRTUM, per regione e macroarea. Italia, ISTAT 2012.Table 1. Distribution of the Italian resident population overall and in areas coveredby AIRTUM cancer registries, by region and macroarea. Italy, ISTAT 2012.
tumori di popolazione, con percentuali che variano da un’areaall’altra del Paese (59% nel Nord-Ovest, 70% nel Nord-Est,27% nel Centro e 39% nel Sud e Isole) (tabella 1).Dal 2005 AIRTUM si è dotata di una banca dati informa-tica che raccoglie i dati prodotti da tutti i Registri tumoriaccreditati.5 Nella Banca dati AIRTUM è possibile identi-ficare un numeroso gruppo di pazienti con tumori multi-pli6-9 grazie sia al numero crescente di registri che la costi-tuiscono, sia alla presenza di registri storici, che hannoavviato la loro attività agli inizi degli anni Ottanta e che oggirendono disponibili dati per la valutazione dell’incidenza inun periodo di quasi trent’anni.
QUALITÀ DEI DATI E CRITERI DI INCLUSIONESono stati selezionati i dati della Banca dati (dicembre2012) relativi a tutti i tumori maligni esclusi i tumori nonmelanomatosi della cute diagnosticati dai Registri tumorigenerali tra il 1976 e il 2010.Tutti i casi inviati alla Banca dati AIRTUM sono codificatisecondo ICD-O-3.10 I tumori a comportamento non ma-ligno sono stati esclusi, a eccezione del tumore della vescicaurinaria, data l’eterogeneità osservata nella registrazione enella classificazione del comportamento per questa sede tu-morale.11 E’ stato escluso il Registro tumori di Brescia peril quale non era disponibile una serie continua di dati.Sono stati esclusi i primi tumori:A. diagnosticati sulla base del solo certificato di morte;B. autoptici con diagnosi post mortem;C. con tempo di follow-up pari a zero.Per la definizione dei tumori multipli, AIRTUM adotta leregole IARC-IACR.12
Sono state analizzate 36 sedi tumorali sia per i primi sia peri secondi tumori (tabella 2).I dati sono sottoposti a due ordini di controlli di qualità (ef-fettuati dal registro e a livello centrale dalla Banca dati) conil software DEPedits. Inoltre, vengono effettuate ulteriorivalutazioni di qualità per mezzo di un software prodottodall’Associazione (CheckAIRTUM),13 che confronta i valoridi una serie di indicatori calcolati sulla casistica di un regi-stro specifico con quelli ottenuti sull’insieme della casisticadi tutti gli altri registri.Nell’ambito della produzione di questa monografia sonostati effettuati controlli di qualità specifici. Per ogni registrotumori, per maschi e femmine assieme e per il totale dei tu-mori, sono stati valutati:■ la percentuale di tumori multipli sul totale della casisticadisponibile;■ la percentuale di tumori multipli diagnosticati entrocinque anni dal primo tumore sul totale della casistica di-sponibile;■ la percentuale di tumori multipli sul totale della casisticadisponibile per periodo di incidenza;■ la percentuale di tumori emolinfopoietici (linfoma, leu-

Materiali e metodiI tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI
13 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
CANCER SITE ICD-O-3, ICD-O-3, ICD-O-3,TOPOGRAPHY MORPHOLOGY BEHAVIOURCODE CODE CODE
Upper aerodigestive tract C019-C069, C090-C148,C320-C329 excluding 9590-9989, and 9050-9055, 9140 3Oral cavity C019-C029, C030-C069 excluding 9590-9989, and 9050-9055, 9140 3Pharynx C090-C139,C140,C142-C148 excluding 9590-9989, and 9050-9055, 9140 3Larynx C320-C329 excluding 9590-9989, and 9050-9055, 9140 3Oesophagus C150-C159 excluding 9590-9989, and 9050-9055, 9140 3Stomach C160-C169 excluding 9590-9989, and 9050-9055, 9140 3Colon rectum C180-C189, C199-C218, C260 excluding 9590-9989, and 9050-9055, 9140 3Colon C180-C189, C260 excluding 9590-9989, and 9050-9055, 9140 3Rectum C199-C218 excluding 9590-9989, and 9050-9055, 9140 3Liver C220-C221 excluding 9590-9989, and 9050-9055, 9140 3Gallbladder C239-C249 excluding 9590-9989, and 9050-9055, 9140 3Pancreas C250-C259 excluding 9590-9989, and 9050-9055, 9140 3Lung C340-C349 excluding 9590-9989, and 9050-9055, 9140 3Skin melanoma C440-C449 8720-8790 3Soft tissue C380, C470-C479, C490-C499 excluding 9590-9989, and 9050-9055, 9140 3Bone C400-C419 excluding 9590-9989, and 9050-9055, 9140 3Breast C500-C509 excluding 9590-9989, and 9050-9055, 9140 3Cervix uteri C530-C539 excluding 9590-9989, and 9050-9055, 9140 3Corpus uteri C540-C549 excluding 9590-9989, and 9050-9055, 9140 3Ovary C569 excluding 9590-9989, and 9050-9055, 9140 3Prostate C619 excluding 9590-9989, and 9050-9055, 9140 3Testis C620-C629 excluding 9590-9989, and 9050-9055, 9140 3Kidney and renal pelvis C649, C659 excluding 9590-9989, and 9050-9055, 9140 3Bladder and urinary tract C669, C670-C679, C680-C689 excluding 9590-9989, and 9050-9055, 9140 0,1,2,3
of bladderBladder C670-C679 excluding 9590-9989, and 9050-9055, 9140 0,1,2,3Urinary tract C669,C680-C689 excluding 9590-9989, and 9050-9055, 9140 3Brain and central C700-C729 excluding 9590-9989, and 9050-9055, 9140 3nervous systemThyroid C739 excluding 9590-9989, and 9050-9055, 9140 3Hodgkin lymphoma C000-C809 9650-9667 3Non-Hodgkin lymphoma C000-C809 9823, 9827 3
C000-C419, C422-C423, C440-C809 9590-9596, 9670-9729 3Multiple myeloma C000-C809 9731-9732, 9734 3Leukaemia C000-C809 9820, 9826, 9832-9837, 9840, 9860-9861, 9863, 3
9866, 9867, 9871-9876, 9891, 9895-9897, 9910,9920, 9930, 9945, 9946
C420, C421, C424 9823 3Lymphoid leukaemia C000-C809 9820, 9826, 9832-9837, 9940 3
C420, C421, C424 9823 3Myeloid leukaemia C000-C809 9840, 9860-9861, 9863, 9866, 9867, 9871-9876, 3
9891, 9895-9897, 9910, 9920, 9930, 9945, 9946Kaposi sarcoma C000-C809 9140 3Mesothelioma C000-C750 9050-9055 3All cancer type (but skin) C000-C809 All
excluding non-melanoma skin cancerAll cancer type (but skin C000-C809 Alland site of first cancer) excluding non-melanoma skin cancer
and site of first cancer
Tabella 2. Codici topografici, morfologici e comportamentali della classificazione ICD-O-3 per le sedi tumorali considerate.Table 2. Cancer sites under examination by topographic, morphological and behavioural ICD-O-3 codes.

cemia o mieloma multiplo) successivi a tumori della stessasede sul totale dei primi tumori emolinfopoietici;■ la percentuale di tumori multipli citoistologicamenteconfermati sul totale dei tumori multipli.Nella tabella 3 è presentata la numerosità della casistica ana-lizzata e una sintesi degli indicatori sopraccitati. Alcune dif-ferenze emerse tra i vari registri tumori possono essere do-vute ai diversi livelli di incidenza (più elevati al Nord,inferiori al Sud) e alla differente lunghezza del periodo diosservazione. Gli indicatori di qualità mostrano in generaleun livello elevato di qualità e completezza che rende possi-bile il confronto tra aree.
■ the percentage of multiple cancer cases microscopically con-firmed out of all multiple primaries.Table 3 shows the number of analyzed cases and a summaryof quality indicators.Some differences across registries may be due to different inci-dence levels (incidence decreases from North to South) and dif-ferent length of periods of observation. Overall, quality indi-cators generally show good quality and completeness of data,allowing for reliable comparisons among geographic areas.
Materiali e metodiI tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI
14 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
AREA / REGISTRY ANALYZED ANALYZED PATIENTS FIRST OF 2+ 1ST OF 2+ 2ND CANCERS/ 2ND CANCERSPERIOD YEARS CANCER CASES CANCER CASES No. OF PATIENTS WITHIN 5 YEARS/
WITHIN 5 YEARS No. OF PATIENTS
No. No. No. No. % %
NORTH-EASTAlto Adige 1995-2005 11 24 195 1 475 1 269 6 5Ferrara 1991-2007 17 40 148 2 804 1 929 7 5Friuli Venezia Giulia 1995-2007 13 100 972 6 959 5 468 7 5Modena 1988-2008 21 72 596 5 025 3 076 7 4Parma 1978-2009 32 71 854 4 961 2 567 7 4Reggio Emilia 1996-2007 12 32 378 1 629 1 258 5 4Romagna 1986-2008 23 122 593 9 938 6 361 8 5Trento 1995-2006 12 28 529 1 331 1 082 5 4Veneto 1987-2006 20 213 289 15 200 10 323 7 5
NORTH-WESTBiella 1995-2007 13 15 727 1 029 781 7 5Como 2003-2007 5 15 577 552 552 4 4Genova 1986-2006 21 112 350 7 690 4 997 7 4Mantova 1999-2005 7 16 147 529 514 3 3Milano 1999-2006 8 67 873 3 121 2 873 5 4Sondrio 1998-2010 13 13 864 841 621 6 4Torino 1985-2008 24 114 788 8 495 5 133 7 4Varese 1976-2007 32 113 761 8 473 4 840 7 4
CENTREFirenze-Prato 1985-2005 21 135 753 7 751 4 752 6 4Latina 1990-2008 19 33 758 1 414 926 4 3Macerata 1991-2001 11 17 223 792 655 5 4Umbria 1994-2008 15 71 401 4 796 3 489 7 5
SOUTH AND ISLANDSCatania-Messina 2003-2005 3 22 604 413 413 2 2Catanzaro 2003-2005 3 3 117 79 79 2 2Napoli 1996-2008 13 24 022 735 550 3 2Nuoro 2003-2008 6 6 188 164 162 2 2Palermo 2003-2006 4 20 971 323 323 2 2Ragusa 1981-2007 27 25 880 1 174 656 5 3Salerno 1996-2005 10 40 232 970 791 2 2Sassari 1992-2009 18 34 351 1 842 1 270 5 4Siracusa 1999-2007 9 14 017 401 361 3 3Trapani 2002-2006 5 8 902 273 273 3 3
Tabella 3. Registro, periodo considerato, numero di anni considerati, numero di pazienti, numero di secondi tumori primitivi in pazienti con 2 o più tumori, numero di seconditumori primitivi in pazienti con 2 o più tumori diagnosticati entro 5 anni dal primo, secondi tumori/numero di pazienti, secondi tumori entro 5 anni/numero di pazienti, per registro.Table 3. Registry, period under examination, number of years, number of patients, number of second primaries of 2+ cancer cases, number of second primaries of 2+cancer cases diagnosed within 5 years since first cancer, second cancers/number of patients, second cancers within 5 years/number of patients, by cancer registry.

Epidemiol Prev 37 (4-5) Suppl 1:1-152 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.it15
I tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI Materiali e metodi
STUDY DESIGN AND STATISTICAL METHODSA retrospective cohort design was used for this analysis. The ob-jective was to determine whether the observed number of sub-sequent cancers occurs more or less frequently in people havinghad a cancer diagnosis than would be expected in the generalpopulation.
Cohort definitionAll cancer patients whose first cancer diagnosis occurred duringthe registry’s activity period and who met the above-mentionedinclusion criteria were considered.Second cancer incidence was evaluated for each cancer site, for«all cancer sites but non-melanoma skin cancer» (see Tables e4online) and for «all cancer sites but non-melanoma skincancer and site of first cancer», as listed in table 2. Since theIARC-IACR recommendations for the definition of multipleprimaries do not allow multiple cancers in the same anatomicsite unless they belong to different morphology groups, two (oreven more) cancer diagnoses are unusual in the same site. It wastherefore decided to compute multiple primary incidence ex-cluding the site of first cancer onset from both the observed andthe expected cancer cases. Moreover, in the site-specific datasheet for «all cancer sites but non-melanoma skin cancer» (pp.40-41), the indicators for all subsequent cancer excluding thesite of first cancer were computed.The length of the period examined varies by cancer registry,ranging from 32 years (Varese and Parma) to 3 years (Catan-zaro, Catania-Messina).
Person-years at risk (PY)PY were defined as the period going from the first cancer di-agnosis to the first date among the following:■ the date of second cancer diagnosis;■ the date of last known vital status;■ the date of death;■ 31 December of the most recent available year of registration(different in each cancer registry).
Person-years at risk (PY) were computed by:■ first cancer site;■ geographic area (North, Centre, South and Islands);■ attained age (5-year groups: 0-4 years, 5-9 years, … , 85+years);■ attained calendar-year group (<1985, 1985-1989, 1990-1994, 1995-1999, 2000-2004, 2005+).
Observed number of casesAll second cancers (excluding non-melanoma skin cancers) di-agnosed in the cohort patients were included in the observednumber of cases. In case the second cancer was a non-melanoma skin cancer, the third cancer was considered as the“second”. The association of three or more cancers is analyzedin chapter 5 (pp. 109-113).
DISEGNO DELLO STUDIO E METODI STATISTICINel presente studio è stato utilizzato il disegno di coorte re-trospettivo, con l’obiettivo di valutare se il numero di seconditumori diagnosticati nei pazienti oncologici fosse superiore oinferiore rispetto a quanto avviene nella popolazione generale.
Definizione della coorteSono stati considerati tutti i pazienti con prima diagnosi ditumore avvenuta nel periodo di attività del registro che ri-spettavano i criteri di inclusione sopra definiti.L’incidenza dei secondi tumori è stata valutata per singolasede tumorale, per il totale dei tumori maligni esclusi i car-cinomi della cute (vd. tabelle e4 on-line), e per il totale deitumori maligni esclusi i carcinomi della cute e la sede delprimo tumore (tabella 2); è stata calcolata escludendo i casiosservati e attesi nella medesima sede del primo tumore,poiché le raccomandazioni IARC-IACR per la definizionedei tumori multipli non rendono possibile l’inserimento dipiù tumori nella stessa sede anatomica, a meno che non ap-partengano a gruppi morfologici differenti, solitamentepoco frequenti. Nella scheda specifica per sede relativa a«Tutti i tumori esclusa cute» (pp. 40-41) gli indicatorisono stati calcolati relativamente a tutti i secondi tumoriesclusi quelli insorti nella stessa sede del primo.La durata del periodo analizzato varia da un registro all’altro,con un valore massimo (32 anni) per Varese e Parma e unvalore minimo (3 anni) per Catanzaro e Catania-Messina.
Anni-persona a rischio (Person-years at risk, PY)Sono stati definiti come l’intervallo che intercorre tra laprima diagnosi di tumore avvenuta nel periodo di attivitàdi ogni singolo registro e il primo tra i seguenti eventi:■ diagnosi del secondo tumore (evento di interesse);■ ultimo aggiornamento dello stato in vita;■ decesso;■ 31 dicembre dell’anno di registrazione più recente dispo-nibile (diverso in ogni registro).
Gli anni-persona a rischio sono stati stratificati per:■ sede del primo tumore;■ area geografica (Nord, Centro, Sud e Isole);■ età compiuta (gruppi quinquennali: 0-4 anni, 5-9 anni, ...,85+ anni);■ periodo temporale (<1985, 1985-1989, 1990-1994,1995-1999, 2000-2004, 2005+).
Numero di casi osservatiTutti i secondi tumori (esclusi i tumori non melanomatosidella cute) diagnosticati nei pazienti della coorte sono stati in-clusi nel numero di casi osservati. Quando il secondo tumorefosse un carcinoma della cute, è stato considerato come “se-condo” il terzo tumore insorto. Nel capitolo 5 (pp. 109-113)è presentata un’analisi dell’associazione di tre o più tumori.

Epidemiol Prev 37 (4-5) Suppl 1:1-152 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.it16
I tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI Materiali e metodi
Expected number of casesThe expected number of cancer cases was computed multiplyingthe accumulated PY by the expected rates. Cancer incidencerates were calculated from the AIRTUMDatabase, includingall cases independently from sequentiality, stratified by cancersite, geographic area (North, Centre, South and Islands), age(5-year groups: 0-4 years, 5-9 years, … , 85+ years) and cal-endar-year group (<1985, 1985-1989, 1990-1994, 1995-1999, 2000-2004, 2005+).For each initial cancer site grouping, the PY and observed casesof cancer were stratified according to the same category as theexpected rates. A discussion about the impact of using referencerates calculated on all cases (regardless of whether the canceris a first or a subsequent cancer) is included in chapter 2 (pp.18-30).
Standardized Incidence Ratio (SIR)The SIR was calculated as the ratio between the observednumber of second cancers and the number that would be ex-pected if patients in the cohort experienced the same cancerrates as the general reference population.14 The StandardizedIncidence Ratio is frequently referred to as the “relative risk”because it compares the incidence rate of the event of interestto the baseline incidence rate. Tests on the statistical signifi-cance of the SIRs were performed under the assumption thatthe observed number of subsequent cancers followed a Poissondistribution, and that no variation was associated with the ex-pected number of cases. Byar’s accurate approximation to theexact Poisson distribution was used to calculate 95% confi-dence intervals.15 The observed/expected ratios, for which the95% confidence interval excluded 1.0, were designated as sta-tistically significant (p <0.05).
Excess Risk (beyond the expected amount)The excess risk of second cancer was computed subtracting theexpected number of subsequent cancers from the observednumber of cancer cases; the difference was then divided by thePYs, and the number of excess or deficit of cancer cases was ex-pressed per 1,000 PYs. Normal approximation was used to cal-culate 95% confidence intervals.
Synchronous cancerThe first two months after first cancer diagnosis were consid-ered as synchronous period and the indicators were computedboth excluding and including the observed and the expectedcases during this period. The site-specific tables show theresults based on metachronous cancers (diagnosed 2 or moremonths after the first cancer), as well as the results based onthe full follow-up period. The issue is addressed in chapter 7(pp. 120-124).For the analysis, theMP-SIR session of SEER*Stat 8.0.1 (a pub-licly available, interactive, Windows-based program producedby NCI)16 and the software STATA, version 12, were used.
Numero di casi attesiE’ stato calcolatomoltiplicando la somma dei PY per i tassi diriferimento; i tassi di incidenza nella popolazione generale sonostati calcolati sull’intera casistica della Banca dati AIRTUM.Sono stati inclusi tutti i tumori indipendentemente dalla se-quenzialità, stratificando per sede tumorale, area geografica(Nord, Centro, Sud e Isole), età (gruppi quinquennali: 0-4anni, 5-9 anni, ..., 85+ anni) e periodo di calendario (<1985,1985-1989, 1990-1994, 1995-1999, 2000-2004, 2005+).Per ogni sede tumorale, i PY e i casi osservati sono stati stra-tificati secondo la stessa classificazione adottata per i tassiattesi. La scelta di utilizzare come riferimento i tassi calcolatisu tutta la casistica AIRTUM, indipendentemente che si trattidi primo o successivo, è discussa nel capitolo 2 (pp. 18-30).
Rapporto standardizzato di incidenza (osservati/attesi)E’ stato calcolato dividendo il numero osservato di secondi tu-mori per il numero di casi che sarebbero stati diagnosticati tra ipazienti della coorte se questi avessero sperimentato gli stessi li-velli di incidenza della popolazione generale.14 Il rapporto osser-vati/attesi è solitamente definito “rapporto standardizzato diincidenza” (Standardized Incidence Ratio, SIR) ed è frequente-mente interpretato come un rischio relativo, poiché confrontail tasso di incidenza dell’evento di interesse nella popolazione stu-diata conquello nella popolazionedi riferimento. E’ stata assuntauna distribuzione di Poisson per il numero di casi osservati e at-tesi; si è inoltre ipotizzato che la variabilità dei casi attesi sia nulla.E’ stata utilizzata l’approssimazione di Byar per il calcolo degliintervalli di confidenza al 95%.15 I rapporti osservati/attesi, peri quali l’intervallo di confidenza al 95% non include 1,0, sonostati considerati statisticamente significativi (p <0,05).
Eccesso assoluto di rischio di secondo tumore(rispetto al valore atteso)E’ stato calcolato sottraendo il numero dei casi attesi al nu-mero dei casi osservati; la differenza è stata divisa per glianni-persona a rischio; il numero di casi in eccesso o in di-fetto è stato espresso per 1.000 anni-persona. Per il calcolodegli IC al 95% è stata utilizzata l’approssimazione normale.
Tumori sincroniCome periodo di sincronicità, sono stati considerati i duemesi successivi alla diagnosi del primo tumore e sono stateeffettuate le analisi sia includendo sia escludendo i casi os-servati e attesi durante questo periodo.Tuttavia, nelle schedespecifiche per sede, oltre ai risultati delle analisi condotte suisoli tumori metacroni (diagnosticati 2 o più mesi dopo ilprimo), sono presentati anche quelli condotti sull’interoperiodo di follow-up. Gli effetti di queste scelte sono com-mentate nel capitolo 7 (pp. 120-124). Per l’analisi sono statiutilizzati la sessione MP-SIR del software SEER*Stat 8.0.1(un programma gratuito, interattivo,Windows-based, pro-dotto dall’NCI)16 e il software STATA, versione 12.

Materiali e metodiI tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI
17 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
BIBLIOGRAFIA/REFERENCES
1. www.registri-tumori.it2. AIRTUMWorking Group; CCM; AIEOP Working Group. Italian can-
cer figures, report 2012: Cancer in children and adolescents. Epi-demiol Prev 2013;37(1) Suppl 1:1-225.
3. AIRTUM Working Group. Italian cancer figures, report 2011: Sur-vival of cancer patients in Italy. Epidemiol Prev 2011;35(5-6) Suppl3:1-200.
4. AIRTUMWorking Group. Italian cancer figures, report 2010: Cancerprevalence in Italy. Patients living with cancer, long-term survivorsand cured patients. Epidemiol Prev 2010;34(5-6) Suppl 2:1-188.
5. http://www.registri-tumori.it/cms/files/Protocollo2010.pdf6. Crocetti E, Lecker S, Buiatti E, Storm HH. Problems related to the
coding of multiple primary cancers. Eur J Cancer 1996;32A(8):1366-70.
7. Buiatti E, Crocetti E, Gafà L et al. Agreement estimate amongthree Italian cancer registries in the coding of multiple primary can-cers. Tumori 1996;82(6):533-8.
8. Buiatti E, Crocetti E, Acciai S et al. Incidence of second primary can-cers in three Italian population-based cancer registries. Eur J Cancer1997;33(11):1829-34.
9. Crocetti E, Buiatti E, Falini P; Italian Multiple Primary Cancer Work-ing Group. Multiple primary cancer incidence in Italy. Eur J Cancer2001;37(18):2449-56.
10.Fritz A, Percy C, Jack A et al (eds). International classification of dis-eases for Oncology. Third Edition. Geneva, World Health Organi-zation, 2000.
11.Patriarca S, Gafà L, Ferretti S et al. Coding criteria of bladdercancer: effects on estimating survival. Epidemiol Prev 2001;25(3)Suppl:42-7.
12.IACR-IARC. International rules for multiple primary cancers. Thirdedition. International Report No. 2004/02. Lione, IARC, 2004.Available at: http://www.iacr.com.fr/MPrules_july2004.pdf
13. http://www.registri-tumori.it/cms/it/node/37214.Curtis RE, Boice JD Jr, Kleinerman RA, Flannery JT, Fraumeni JF Jr.
Summary: multiple primary cancers in Connecticut, 1935-82. NatlCancer Inst Monogr 1985;68:219-42.
15.Breslow NE, Day NE. Statistical methods in cancer research. VolumeII – The design and analysis of cohort studies. IARC Sci Publ1987;(82):1-406.
16.http://seer.cancer.gov/seerstat/

WWW.EPIPREV.IT
La quantificazione del rischio di ulteriori neoplasie nei pazientigià affetti da un tumore può contribuire a comprenderne l’ezio-logia (per un’esposizione condivisa, per gli effetti a lungo ter-mine del trattamento del primo tumore, per predisposizione ge-netica eccetera) e a indirizzare il follow-up clinico. La valutazionedei tumori multipli è stata condotta in diversi studi su base dipopolazione.1-10 Anche l’Associazione italiana dei registri tumori(AIRTUM) ha condotto fin dai suoi esordi11,12 studi collabo-rativi sui secondi tumori (MP), valutando sia il rischio comples-sivo di MP,13,14 sia il rischio per una sede tumorale specifica.15
Nel corso del tempoAIRTUMènotevolmente cresciuta in ter-mini di numero di registri membri e durata del follow-up deipazienti (www.registri-tumori.it). Inoltre, vi è stato unmiglio-ramento della sopravvivenza complessiva per tumore.16 Infine,nel 2005AIRTUMha sviluppato un database centralizzato checomprende un grande archivio con più di 2 milioni di casi.Tutti questi aspetti hanno stimolato l’interesse ad aggiornarela valutazione dell’incidenza deiMP con un nuovo studio col-laborativo AIRTUM per fornire dati aggiornati sul rischio diMP nei pazienti oncologici italiani. I materiali e metodi sonoampiamente descritti nel capitolo 1 (pp. 11-17).
COORTE. E’ stata seguita una coorte di 1.635.060 pazientiaffetti da tumore (880.361 maschi e 754.699 femmine),escludendo gli epiteliomi cutanei e i tumori non maligni.Tali casi, incidenti tra il 1976 e il 2010, sono stati seguitiper un follow-up pari a 5.979.338 anni-persona.INCIDENZA CUMULATIVA. La figura 1 mostra l’incidenza cu-mulativa di MP stimata sull’intero database AIRTUM apartire dal momento della diagnosi del primo tumore. Laprobabilità di sviluppare unMP, tenendo in considerazionela mortalità competitiva per altre cause, è in media, rispet-tivamente per donne e uomini:■ del 4% e del 6% a 5 anni,■ del 6% e del 10% a 10 anni,■ dell’8 % e del 12% a 15 anni,■ del 10% e del 14% a 20 anni,■ dell’11% e del 15% a 25 anni,■ del 12% e del 16% a 30 anni.PERIODO METACRONO.Nel complesso sono stati osservati85.399 secondi tumori metacroni (latenza fra diagnosidel primo e del secondo tumore ≥2 mesi), mentre erano at-tesi 77.813,4 tumori in base all’incidenza della popolazionegenerale.
Quantification of the risk of further cancers in cancer patientsmay contribute to understanding the aetiology of cancer(shared exposure, long term effects of treatment, genetic predis-position, etc.) and to address clinical follow-up. This issue hasbeen analyzed in several population-based contexts.1-10 Even theItalian network of cancer registries (AIRTUM) has carried outcollaborative studies on multiple primaries (MPs) since its be-ginnings,11,12 evaluating both the overall risk of second primarycancers13,14 and the risk for a specific cancer site.15
Over time, AIRTUM has greatly increased the number ofmember cancer registries and the length of patient follow-up(www.registri-tumori.it). Moreover, there has been an im-provement in overall cancer survival.16 In 2005, AIRTUM de-veloped a centralized database that includes a huge archive ofmore than 2 millions cases. All these issues combined to prompta new AIRTUM collaborative study to provide updated dataon MP risk for Italian cancer patients.Material and methods are described in detail in chapter 1 (pp.11-17).
COHORT.For 5,979,338 person-years, a cohort of 1,635,060cancer patients was followed-up (880,361 males and 754,699females). Skin epithelioma and non-malignant tumours wereexcluded; cases were incident between 1976 and 2010.
L’incidenza di secondi tumoriin pazienti oncologici in ItaliaIncidence of second primary cancers in Italy
18 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
I tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI
Figura 1. Probabilità cumulativa di sviluppare un secondo tumore, per genere etempo trascorso dalla diagnosi del primo tumore. Tutti i tumori esclusi i nonmelanomatosi della cute. Tumori sincroni e metacroni.Figure 1. Cumulative probability of developing a second cancer, by gender andtime since first cancer diagnosis.All cancers excluding non-melanoma skin cancer.Synchronous and metachronous cancers.
CUMULATIVE INCIDENCE OF DEVELOPING A SECOND CANCER AMONG PATIENTSALL CANCER SITES BY GENDER
YEARS AFTER INITIAL CANCER DIAGNOSIS
CUMULATIVEPROBABILITY
.15
Capitolo 2
.1
.05
0
0 10 20 30

CUMULATIVE INCIDENCE. Figure 1 shows cumulative MP in-cidence since first cancer diagnosis, estimated on the entire AIR-TUMDatabase. The probability of developing MPs, account-ing for competitive mortality, is, on average, for women andman, respectively:■ 4% and 6% up to 5 years after first cancer diagnosis;■ 6% and 10% up to 10 years;■ 8% and 12% up to 15 years;■ 10% and 14% up to 20 years;■ 11% and 15% up to 25 years;■ 12% and 16% up to 30 years.METACHRONOUS PERIOD. Overall, 85,399 metachronous(latency ≥2 months) cancers were observed, while 77,813.4were expected during the study period; the Standardized In-cidence Ratio (SIR) was 1.10 (95%CI 1.09-1.10); the ExcessAbsolute Risk (EAR) was 1.32 per 1,000 person-years(95%CI 1.19-1.46) (table 1).SIR.The Standardized Incidence Ratio (SIR) was 1.10 (95%CI1.09-1.10). SIRwas 1.08 (95%CI 1.08-1.09) for men (54,518observed and 50,260.8 expected) and 1.12 (95%CI 1.11-1.13)for women (30,881 vs. 27,552.5).EAR.The Excess Absolute Risk was 1.32 (95%CI 1.19-1.46)per 1,000 person-years. EARwas 1.61 (95%CI 1.37-1.84) and
L’incidenza di secondi tumori in pazienti oncologici in ItaliaI tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI
19 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
SIR. Il rapporto fra tassi standardizzati d’incidenza (Standa-rdized Incidence Ratio - SIR) è 1,10 (IC95% 1,09-1,10). IlSIR è 1,08 (IC95% 1,08-1,09) per gli uomini (54.518 os-servati vs. 50.260,8 attesi) e 1,12 (IC95% 1,11-1,13) perle donne (30.881 vs. 27.552,5) (tabella 1).EAR.L’eccesso di rischio assoluto (Excess Absolute Risk - EAR)è 1,32 per 1.000 anni-persona (IC95% 1,19-1,46). L’EARè 1,61 (IC95% 1,37-1,84) per gli uomini e 1,08 (IC95%0,93-1,24) per le donne, per 1.000 anni-persona (tabella 1).PERIODO SINCRONO. Durante i primi due mesi dopo laprima diagnosi di tumore (periodo sincrono) ci sono stati14.807 tumori osservati e 3.536,5 attesi (SIR: 4,16; IC95%4,09-4,22); il SIR era 4,08 (IC95% 4,00-4,16) per gli uo-mini e 4,32 (IC95% 4,20-4,45) per le donne (tabella 1).ETÀ. L’età media dei pazienti al momento della diagnosi delprimo tumore era 67,0 anni tra gli uomini e 65,8 tra ledonne. Il rischio di MP cambia in relazione all’età, essendomaggiore nei pazienti più giovani e minore per quelli più an-ziani (tabella 1).ANDAMENTO.Rispetto alla diagnosi del primo tumore, comegià descritto, i SIR sono molto elevati all’inizio e successiva-mente diminuiscono, pur mantenendosi sempre oltre l’unità,per poi tornare a crescere. Non sono state osservate differenze
OBSERVED EXPECTED PY RISK SIR EAR(95%CI) (95%CI)
ALL CASES 85 399 77 813 5 725 524 1.10 1.32(1.09;1.10) (1.19;1.46)
GENDER Men 54 518 50 260 2 651 889 1.08 1.61(1.08;1.09) (1.37;1.84)
Women 30 881 27 552 3 073 635 1.12 1.08(1.11;1.13) (0.93;1.24)
AGE 0-49 5 707 3 584 1 135 680 1.59 1.87(YEARS) (1.55;1.63) (1.7;2.04)
50-59 13 681 10 145 1 148 209 1.35 3.08(1.33;1.37) (2.82;3.34)
60-69 28 950 25 315 1 627 871 1.14 2.23(1.13;1.16) (1.95;2.51)
70-79 28 593 28 684 1 355 384 1.00 -0.07(0.99;1.01) (-0.41;0.28)
80+ 8 468 10 084 458 379 0.84 -3.53(0.82;0.86) (-4.1;-2.95)
LATENCY (0-1) 14 807 3 563 253 814 4.16 44.30(MONTHS) (4.09;4.22) (43.3;45.3)
2-11 14 284 13 416 993 436 1.06 0.87(1.05;1.08) (0.55;1.2)
12-59 38 529 35 693 2 663 953 1.08 1.06(1.07;1.09) (0.87;1.26)
60-119 21 540 19 233 1 396 039 1.12 1.65(1.11;1.14) (1.37;1.93)
120+ 11 046 9 471 672 094 1.17 2.34(1.14;1.19) (1.93;2.76)
PERIOD 1978-1987 44 880 40 886 2 963 469 1.10 1.35(1.09;1.11) (1.16;1.54)
1988-1997 12 637 11 654 944 415 1.08 1.04(1.07;1.10) (0.72;1.36)
1998-2010 27 882 25 272 1 817 640 1.10 1.44(1.09;1.12) (1.19;1.68)
Tabella 1.Numero di secondi tumorimetacroni osservati e attesi (esclusala sede del primo tumore), anni-persona a rischio, rapporto fra tassistandardizzati di incidenza (SIR; conintervallo di confidenza la 95%), edeccesso assoluto di rischio (EAR per1.000 anni-persona; con intervallo diconfidenza al 95%), totali e specificiper genere, età, periodo e tempotrascorso dalla diagnosi del primotumore. I primi due mesi dopo ladiagnosi del primo tumore sonoconsiderato solo per la stratificazioneper tempo di latenza.Table 1. Number of observed andexpectedmetachronous second cancers(excluding cancer occurred in the samesite of first cancer), person-years at risk,Standardized Incidence Ratio (SIR;95% confidence interval), and ExcessAbsolute Risk (EAR per 1,000 person-years; 95% confidence interval), overalland gender-, age-, period-, and timesince first cancer diagnosis-specific.The first two months after first cancerdiagnosis are considered for latencystratification only.

L’incidenza di secondi tumori in pazienti oncologici in ItaliaI tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI
20 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
FIRST CANCER SITE MEN WOMEN
OBSERVED EXPECTED PY RISK SIR EAR OBSERVED EXPECTED PY RISK SIR EAR
Oral cavity 1 151 596 34 591 1.93* 16.03* 286 192 17 303 1.48* 5.40*
Pharynx 937 439 28 319 2.13* 17.55* 157 78 8 572 1.99* 9.13*
Larynx 3 863 2 460 123 653 1.57* 11.35* 233 130 11 649 1.79* 8.80*
Oesophagus 290 200 10 532 1.45* 8.50* 58 41 3 470 1.41* 4.84
Stomach 2 291 2 360 114 046 0.97 -0.61 1 044 1 114 93 324 0.94 -0.76
Colon 5 145 5 556 260 357 0.93* -1.58* 3 086 2 974 263 285 1.04 0.42
Rectum 2 378 2 854 133 421 0.83* -3.57* 1 299 1 316 112 555 0.99 -0.16
Liver 662 768 38 090 0.86* -2.79* 160 197 16 417 0.81* -2.26*
Gallbladder 173 215 9 673 0.80* -4.35* 209 172 13 942 1.21* 2.59
Pancreas 187 268 13 693 0.70* -5.97* 129 166 14 542 0.78* -2.57*
Lung 3 377 3 089 177 728 1.09* 1.62* 587 518 49 229 1.13* 1.39*
Melanoma 1 117 1 107 79 529 1.01 0.12 1 008 858 105 155 1.17* 1.42*
Soft tissue 258 246 18 553 1.05 0.62* 159 140 16 708 1.13 1.09
Bone 65 61 7 618 1.06 0.46 54 38 6 647 1.41* 2.37*
Breast 221 198 9 402 1.11 2.36 10 597 9 496 1 274 882 1.12* 0.86*
Uteri cervix 870 708 87 454 1.23* 1.84*
Uteri corpus 2 614 2 128 201 941 1.23* 2.41*
Ovary 853 724 84 295 1.18* 1.53*
Prostate 10 956 11 806 547 058 0.93* -1.55*
Testis 246 198 54 475 1.24* 0.87*
Kidney 2 476 2 175 114 765 1.14* 2.62* 858 743 67 755 1.15* 1.68*
Urinary bladder 11 030 8 540 417 343 1.29* 5.97* 1 531 1 257 102 871 1.22* 2.65*
Urinary tract 353 324 13 871 1.09 2.06 72 63 4 836 1.14 1.85
CNS 160 195 25 033 0.82* -1.41* 110 126 22 048 0.87 -0.74
Thyroid 417 343 34 797 1.22* 2.12* 980 803 125 846 1.22* 1.40*
Hodgkin lymphoma 311 195 35 127 1.59* 3.30* 251 129 31 941 1.94* 3.81*
Non-Hodgkin lymph. 1 991 1 767 111 563 1.13* 2.00* 1 219 1 093 110 539 1.12* 1.14*
Myeloma 620 673 31 535 0.92 -1.68* 402 400 33 521 1.00 0.05
Lymphoid leukaemia 927 881 49 445 1.05 0.91 411 395 38 207 1.04 0.40
Myeloid leukaemia 252 254 18 856 0.99 -0.10 141 138 17 350 1.02 0.12
Other leukaemias 23 28 1 990 0.81 -2.71 16 16 1 749 1.00 -0.03
Mesothelioma 58 89 4 604 0.65* -6.75 25 21 1 987 1.19 1.97
Kaposi sarcoma 238 215 12 084 1.11 1.88 60 58 4 522 1.03 0.35
Other sites 2 345 2 149 120 123 1.09* 1.63* 1 402 1 305 129 079 1.07* 0.74*
All sites 54 518 50 260 2 651 889 1.08* 1.61* 30 881 27 552 3 073 635 1.12* 1.08*
* statistically significant (p <0.05)
Tabella 2. Numero di secondi tumori metacroni osservati e attesi (esclusa la sede del primo tumore) per genere e sede del primo tumore, anni-persona a rischio, rapportofra tassi standardizzati di incidenza (SIR) ed eccesso assoluto di rischio (EAR) per 1.000 anni-persona, totali e specifici per genere, età, periodo e tempo trascorso dalladiagnosi del primo tumore.Table 2. Number of observed and expected metachronous second cancers (excluding cancer occurred in the same site of first cancer), by gender and site of first cancer,person-years at risk, Standardized Incidence Ratio (SIR), and Excess Absolute Risk (EAR) per 1,000 person-years overall and gender-, age-, period- and time since firstcancer diagnosis-specific.
sostanziali fra i diversi periodi di incidenza; in tutti è presenteun aumento del rischio di MP (tabella 1).SINGOLE SEDI.Nella tabella 2 sono indicati gli eccessi e i di-fetti di rischio di MP (in termini sia di SIR, sia di EAR, persesso e sede del primo tumore) per tutte le 36 sedi tumoralianalizzate. Sono indicati con asterisco i SIR statisticamentesignificativi (per i quali l’intervallo di confidenza al 95%non contiene il valore 1) e gli EAR statisticamente signifi-cativi (per i quali l’intervallo di confidenza al 95% non con-tiene il valore 0).Di seguito sono commentate le associazioni con SIR stati-
1.08 per 1,000 person-years (95%CI 0.93-1.24), respectively(table 1).SYNCHRONOUS PERIOD.Moreover, during the first two monthsafter first cancer diagnosis (synchronous period) there were 14,807other cancers observed and 3,536.5 expected (SIR: 4.16; 95%CI4.09-4.22), the SIR was 4.08 (95%CI 4.00-4.16) for men and4.32 (95%CI 4.20-4.45) for women (table 1).AGE. The mean age of patients at first cancer diagnosis was67.0 years among males and 65.8 among females. The MPrisk was higher with age being higher for younger patients andlower for older ones (table 1).

sticamente significativi. Le donne presentano un SIR mag-giore dell’unità per 18 sedi tumorali, gli uomini per 12. ISIR statisticamente significativi inferiori a 1 sono rispetti-vamente 2 e 8.
ECCESSI E DIFETTIENTRAMBI I SESSI.Un aumento del rischio complessivo diMP è presente per i pazienti di entrambi i sessi con unprimo tumore:■ della cavità orale (SIR uomini: 1,93; SIR donne: 1,48),■ della faringe (SIR uomini: 2,13; SIR donne: 1,99),■ della laringe (SIR uomini: 1,57; SIR donne: 1,79),■ dell’esofago (SIR uomini: 1,45; SIR donne: 1,41),■ del polmone (SIR uomini: 1,09; SIR donne: 1,13),■ del rene (SIR uomini: 1,14; SIR donne: 1,15),■ della vescica (SIR uomini: 1,29; SIR donne: 1,22),■ della tiroide (SIR: 1,22 in entrambi i sessi),■ linfoma diHodking (SIR uomini: 1,59; SIR donne: 1,94),■ linfomanon-Hodgkin (SIRuomini: 1,13; SIRdonne: 1,12)■ gruppo eterogeneo «altre sedi» (SIR uomini: 1,09; SIRdonne: 1,07) (tabella 2).Un primo tumore del fegato o del pancreas sono associati,in entrambi i sessi, a un rischio ridotto di MP (SIR fegato:0,86 e 0,81 per uomini e donne rispettivamente; SIR pan-creas: 0,70 e 0,78 per uomini e donne rispettivamente), cosìcome accade tra gli uomini per il tumore del colon (SIR:0,93), del retto (SIR: 0,83), della cistifellea (SIR: 0,80),della prostata (SIR: 0,93), il mesotelioma (SIR: 0,65) e i tu-mori del sistema nervoso centrale (SIR: 0,82).UOMINI. Inoltre, tra gli uomini si osserva un rischio aumentatodiMP se la sede di primo tumore è il testicolo (SIR: 1,24).DONNE.Tra le donne, se la sede del primo tumore è la colecisti(SIR: 1,21), il melanoma cutaneo (SIR: 1,17), l’osso (SIR:1,41), la mammella (SIR: 1,12), la cervice dell’utero (SIR:1,23), il corpo dell’utero (SIR: 1,23) o l’ovaio (SIR: 1,18), siosserva un rischio aumentato di MP (tabella 2).EAR.Tra le sedi tumorali per le quali l’EAR è statisticamentesignificativo, quelle con valori più elevati sono i tumori dellacavità orale (EAR uomini: 16,0 per 1.000 persone all’anno;EAR donne: 5,4), della faringe (EAR uomini: 17,6; EARdonne: 9,1), della laringe (EAR uomini: 11,4; EAR donne:8,8) e dell’esofago (EAR uomini: 8,5; EAR donne: 4,8).
LE SEDI PIU’ FREQUENTINelle tabelle specifiche per sede di primo tumore presentatein questa monografia il rischio di MP è presentato persede di secondo tumore, sesso e latenza dalla diagnosi delprimo tumore. La tabella 3 è un esempio dell’enormequantità di dati disponibili nelle schede specifiche per sede,che rappresentano il cuore della presente monografia. Inquesta tabella sono riportate alcune delle associazioni messein evidenza. Per le dieci sedi tumorali più frequenti in ter-mini di incidenza del primo tumore in entrambi i sessi,
TREND.With respect to the time of first cancer diagnosis, SIRswere, as previously described, very high at the beginning, thendecreased, although remaining constantly above one, and laterdisplayed again an increasing trend (table 1).No strong differences were evident across the different periodsof incidence, all showing an increased MP risk (table 1).SINGLE CANCER SITES. Table 2 shows the excess or decreasedrisks of MPs in terms of SIR and EAR, by gender and site offirst cancer. All 36 cancer sites analyzed in the monograph arepresented. An asterisk marks statistically significant SIRs (forwhich the 95% confidence interval does not contain the value1) and statistically significant EARs (for which the 95% con-fidence interval does not contain the value 0).
The following notes are associated with the statistically signif-icant SIRs.Women had higher SIRs than expected for 18 can-cer sites, men for 12. The statistically significantly SIRs lowerthan 1 were 2 and 8, respectively.
INCREASES AND DECREASESBOTH GENDERS. Increased overall MP risk was shown for pa-tients of both sexes with a first primary in:■ oral cavity (SIR men: 1.93; SIR women: 1.48)■ pharynx (SIR men: 2.13; SIR women: 1.99)■ larynx (SIR men: 1.57; SIR women: 1.79)■ oesophagus (SIR men: 1.45; SIR women: 1.41)■ lung (SIR men: 1.09; SIR women: 1.13)■ kidney (SIR men: 1.14; SIR women: 1.15)■ urinary bladder (SIR men: 1.29; SIR women: 1.22)■ thyroid (SIR: 1.22 in both genders)■ Hodgkin lymphoma (SIR men: 1.59; SIR women: 1.94)■ non-Hodgkin lymphoma (SIRmen: 1.13; SIR women: 1.12)■ heterogeneous «other sites» group (SIR men: 1.09; SIRwomen: 1.07) (table 2).A first liver or pancreas cancer were associated with a decreasedMP risk in both sexes (liver, SIR: 0.86 and 0.81 for men andwomen, respectively; pancreas, SIR: 0.70 and 0.78 for menand women, respectively), as were first cancers of the colon(SIR: 0.93), rectum (SIR: 0.83), gallbladder (SIR: 0.80),prostate (SIR: 0.93), mesothelioma (SIR: 0.65), and CNS(SIR: 0.82) among men.MEN.Moreover, men had a higher MP risk if the primary can-cer was in the testis (SIR: 1.24).WOMEN. The same was true for women with gallbladder(SIR: 1.21), skin melanoma (SIR: 1.17), bone (SIR: 1.41),breast (SIR: 1.12), cervix uteri (SIR: 1.23), corpus uteri(SIR: 1.23), and ovary cancers (SIR: 1.18) (table 2).EAR.Among cancer sites for which the EAR was statistically sig-nificant, those with the highest absolute MP risk were those ofthe oral cavity (EAR: 16.0 x 1,000 person-years in men and5.4 in women), pharynx (17.6 and 9.1), larynx (11.4 and8.8), and oesophagus (8.5 and 4.8).
L’incidenza di secondi tumori in pazienti oncologici in ItaliaI tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI
21 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152

L’incidenza di secondi tumori in pazienti oncologici in ItaliaI tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI
22 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
FIRST CANCER SITE MEN WOMEN
SECOND CANCER OBS. EXPEC. SIR EAR SECOND CANCER OBS. EXPEC. SIR EAR
Breast Kidney and renal pelvis 14 6 2.31* 0.84 Corpus uteri 1 222 628 1.94* 0.47*
# Myeloid leukaemia 223 145 1.53* 0.06*
# Soft tissue 83 54 1.53* 0.02*
Lung Oral cavity 111 37 3.00* 0.42* Larynx 8 1 4.52* 0.13*
Pharynx 93 33 2.76* 0.33* Pharynx 6 1 3.81* 0.09
Larynx 179 91 1.97* 0.50* Urinary bladder 40 19 2.06* 0.42*
Colon Thyroid 45 23 1.89* 0.08* Ovary 151 100 1.51* 0.19*
Kidney and renal pelvis 250 183 1.36* 0.26* Kidney and renal pelvis 104 80 1.29* 0.09
# Corpus uteri 181 140 1.29* 0.15*
Prostate Thyroid 80 53 1.50* 0.05*
Skin melanoma 251 191 1.31* 0.11*
Kidney and renal pelvis 543 434 1.25* 0.20*
Urinary bladder Lung 3 074 1 672 1.84* 3.36* Lung 242 83 2.89* 1.54*
Larynx 326 205 1.58* 0.29* Larynx 10 3 2.63* 0.06
Myeloid leukaemia 140 99 1.41* 0.10* Pharynx 8 3 2.47* 0.05
Stomach Pancreas 108 68 1.58* 0.35* Pancreas 85 52 1.61* 0.35*
Myeloid leukaemia 41 26 1.56* 0.13 #
Oesophagus 38 26 1.44* 0.10 #
Rectum # Lung 152 86 1.75* 0.58*
# Thyroid 32 20 1.54* 0.10
# Corpus uteri 86 59 1.44* 0.23
Non-Hodgkin Kaposi's sarcoma 22 4 5.52* 0.16* Kaposi's sarcoma 7 1 4.76* 0.05
lymphoma Hodgkin lymphoma 19 4 4.31* 0.13* Hodgkin lymphoma 8 3 2.66* 0.05
Testis 11 3 2.83* 0.06* Liver 67 29 2.26* 0.34*
Liver Pharynx 20 6 2.92* 0.35* Pharynx 3 0 5.91* 0.15
Oral cavity 21 7 2.79* 0.35* #
Oesophagus 17 8 2.08* 0.23 #
Kidney and renal Thyroid 25 10 2.36* 0.13* Soft tissue 10 3 3.17* 0.10
pelvis Myeloid leukaemia 36 22 1.60* 0.12 Thyroid 37 13 2.81* 0.35*
Skin melanoma 50 32 1.54* 0.15 Urinary bladder 75 27 2.77* 0.71*
Corpus uteri Soft tissue 18 9 1.96* 0.04
Kidney and renal pelvis 93 54 1.71* 0.19*
Lung 220 141 1.55* 0.39*
Thyroid Soft tissue 5 1 3.36* 0.10 Myeloid leukaemia 18 8 2.07* 0.07
Mesothelioma 6 1 3.12* 0.12 Kidney and renal pelvis 32 18 1.70* 0.11
Myeloma 20 11 1.69* 0.06
Larynx Oral cavity 129 25 5.03* 0.84* Pharynx 7 0 18.61* 0.57*
Oesophagus 124 27 4.47* 0.78* Kaposi's sarcoma 2 0 11.94* 0.16
Pharynx 84 23 3.56* 0.49* Oesophagus 6 0 9.51* 0.46*
Ovary Myeloid leukaemia 15 8 1.83* 0.08
Urinary bladder 37 23 1.55* 0.16
Rectum 47 30 1.52* 0.19
* statistically significant p < 0.05# statistically significant SIR >1 not available.Among patients with pancreas cancer (included in the first ten most frequent cancer sites) no statistically significant SIR >1 is available.
Tabella 3. Le 10 sedi tumorali più frequenti (primo tumore) fra uomini e donne e i 3 secondi tumori metacroni con SIR statisticamente significativo >1. Numero di seconditumori osservati e attesi, SIR ed eccesso assoluto di rischio (EAR) per 1.000 anni-persona, per genere.Table 3. Ten most frequent cancer sites (first cancer) among men and women, three second metachronous cancer sites with statistically significant Standardized IncidenceRatio >1. Number of observed and expected second cancers, Standardized Incidence Ratio (SIR) and Excess Absolute Risk (EAR) per 1,000 person-years, by gender.

sono stati selezionati i tre MP con il SIR più elevato e sta-tisticamente significativo (>1), se presente.Si sottolineano le associazioni tra:■ polmone e faringe (SIR uomini: 2,76; SIR donne: 3,81)■ polmone e cavità orale (SIR uomini: 3,00)■ polmone e laringe (SIR uomini: 1,97; SIR donne: 4,52)■ polmone e vescica (SIR donne: 2,06)■ vescica e polmone (SIR uomini: 1,84; SIR donne: 2,89)■ vescica e laringe (SIR uomini: 1,58; SIR donne: 2,63)■ vescica e faringe (SIR donne: 2,47)■ laringe e faringe (SIR uomini: 3,56; SIR donne: 18,6)■ faringe ed esofago (SIR uomini: 18,1; SIR donne: 25,6)■ fegato e faringe (SIR uomini: 2,9; SIR donne: 5,9).
Tra ledonne con tumore al seno, le associazioni conSIRpiù ele-vato si osservano con i tumori del corpo dell’utero (SIR: 1,94).Tra i pazienti con linfoma non-Hodgkin, in entrambi isessi si osservano SIR più elevati per il sarcoma di Kaposie il linfoma di Hodgkin.Tra i pazienti con tumore della prostata, i tumori della ti-roide (SIR: 1,50), il melanoma (SIR: 1,31) e i tumori direne e pelvi renali (SIR: 1,25) sono le tre sedi di secondotumore con SIR più elevato.Tra i pazienti con primo tumore del colon, in entrambi isessi i tumori di rene e pelvi renali sono stati il secondoMPpiù frequente rispetto all’atteso.Tra i pazienti affetti da cancro dello stomaco, in entrambii sessi il tumore del pancreas è stato il primo (in termini dirapporto tra casi osservati e attesi) tra i MP.Tra gli uomini con cancro del colon, i tumori della tiroidesono al primo posto in termini di incidenza di MP, al se-condo tra le donne con tumore del retto.Tra i pazienti con tumore di rene e pelvi renali, i tumoridella tiroide risultano al primo posto tra gli uomini e al se-condo tra le donne.Tra i pazienti con tumore del fegato, i tumori della faringesono quelli con SIR più elevato (uomini: 2,92; donne: 5,91).
DISCUSSIONEQuesto studio descrittivo fornisce informazioni quantitativesul rischio di sviluppare MP in una coorte su base di popo-lazione di circa 1.650.000 malati di cancro diagnosticati inItalia (54% maschi).In media l’incidenza cumulativa di MP è dell’8% e del 12%dopo 10 e 20 anni, rispettivamente.L’incidenza cumulativa è una misura assoluta (dipendenteda struttura per età, sopravvivenza, incidenza di base ecce-tera) che non rivela se i MP osservati sono diversi da quelliattesi nella popolazione generale.Durante un periodo medio di follow-up di 14,2 anni, i malatidi tumore hanno mostrato un aumento del rischio di MP del10%(SIRdonne: 1,12; SIRuomini: 1,08) in confronto alla po-polazione generale e un eccesso assoluto di rischio di 1,32 per
MORE FREQUENT CANCER SITESIn the site-specific tables in this monograph the MP risk isshown by site of second primary cancer, gender, and latency. Intable 3, as a short summary of the data available in the site-specific tables, some of the associations highlighted by thisstudy are presented. For the ten most frequent incident cancersites in both sexes, the two MPs with the highest and statisti-cally significant SIR were selected, if any.It was showcased the associations between:■ lung and pharynx (SIR men: 2.76; SIR women: 3.81)■ lung and oral cavity (SIR men: 3.00)■ lung and larynx (SIR men: 1.97; SIR women: 4.52)■ lung and urinary bladder (SIR women: 2.06)■ urinary bladder and lung (SIRmen: 1.84; SIRwomen: 2.89)■ urinary bladder and larynx (SIR men: 1.58; SIR women:2.63)■ urinary bladder and pharynx (SIR women: 2.47)■ larynx and pharynx (SIR men: 3.56; SIR women: 18.6)■ pharynx and oesophagus (SIR men: 18.1; SIR women:25.6)■ liver and pharynx (SIR men: 2.9; SIR women: 5.9)
The association with the highest SIR for women with breastcancer was with corpus uteri (SIR: 1.94).In both sexes the highest SIR for MP in non-Hodgkin lym-phoma patients were for Kaposi’s sarcoma and Hodgkin lym-phoma.The first three MPs with the highest SIR in prostate cancerpatients were thyroid (SIR: 1.50) and melanoma (SIR: 1.31),kidney and pelvis (SIR: 1.25).Kidney and pelvis cancers were the second most frequent (com-pared to the expected) among colon cancer patients in both sexes.Pancreas was the first (with the highest SIR) among MPs instomach cancer patients in both genders.Thyroid ranked first among MPs in men with colon cancerand second in women with rectum cancer.Thyroid ranked first and second among male and female pa-tients with kidney and pelvis cancers, respectively.Pharynx showed the highest SIR after liver cancer in both men(SIR: 2.92) and women (SIR: 5.91).
DISCUSSIONThis descriptive study provides quantitative information on therisk of developing MPs in an Italian population-based cohortof approximately 1,650,000 cancer patients (54% males).On average, the cumulative incidence of MPs is 8% and12% after 10 and 20 years, respectively. This is just anabsolute measure – dependent on age-structure, survival, base-line incidence etc. – which does not say whether MPs are dif-ferent than in the general population.During an average period of 14.2 years of follow-up, cancerpatients showed a 10% greater MP risk (SIR women: 1.12;SIR men: 1.08) in comparison with the general population,
L’incidenza di secondi tumori in pazienti oncologici in ItaliaI tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI
23 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152

L’incidenza di secondi tumori in pazienti oncologici in ItaliaI tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI
24 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
1.000 anni-persona (EAR donne: 1,08; EAR uomini: 1,61).In questa monografia sono stati prodotti sia SIR sia EAR,poiché queste due misure esprimono un diverso tipo di in-formazione, come spiegato nel capitolo di guida alla letturadelle schede specifiche per sede tumorale (pp. 31-38).La scelta operata è stata di garantire la maggiore rappresenta-tività possibile, includendo quindi i dati di tutti i registri AIR-TUM, pur a scapito di una diversa lunghezza del follow-up.
Definizione di secondo tumorePrima di analizzare più in dettaglio i risultati è necessariosottolineare che lo studio sui MP e le relative misure di ri-schio sono fortemente dipendenti dai metodi adottati peril loro calcolo. La definizione stessa di MP è variabile e l’usodi regole diverse può notevolmente modificare il numerodi tumori MP in un paziente.17 Il problema della classifi-cazione è discusso al capitolo 6 (pp. 114-119).Tutti i registri tumori AIRTUMadottano le stesse raccoman-dazioni IARC-IACRper la definizione deiMP.18Queste regolenon prevedonoMP nella stessa sede anatomica del primo tu-more, a meno che questi non appartengano a gruppi morfo-logici diversi.Tale criterio rende piuttosto raro avere due (o più)tumori nella stessa sede anatomica. Tra i 101.179MP analiz-zati, solo 973 (1%) si sono verificati nella stessa sede anatomica;al contrario, tra i 92.586,6 secondi tumori attesi, 11.209,8(12%) sono relativi alla stessa sede anatomica.Pertanto, a differenza di quanto fatto in lavori precedenti,13,14
si è qui deciso di calcolare la frequenza deiMPanche escludendola sede di insorgenza del primo tumore, sia per quanto riguardai casi osservati sia per quelli attesi.3 L’effetto di questa scelta suiSIR è rilevante, soprattutto per le sedi tumorali più frequenti,poiché iMPosservati nella stessa sede sono in genere pochi (perla biologia e per le regole adottate), mentre il numero deitumori attesi può essere enorme. Per esempio, il SIR per MPnelle pazienti con carcinoma mammario è 1,12 escludendo lasede «seno»,ma è 0,82 includendola, perché iMPosservati nellamammella sono solo 43, mentre quelli attesi, secondo tassi diincidenza della popolazione generale, sono 3.539. Le stimecomplessive che includono la sede del primo tumore sono di-sponibili nel materiale aggiuntivo on-line. Entrambe questestime sono distorte: quelle che includono la sede del primo tu-more sono sottostimate, anche notevolmente, come descrittonell’esempio del tumore della mammella femminile; quelleche escludono la sede del primo tumore sono leggermente so-vrastimate. A nostro parere, queste ultime si avvicinano mag-giormente al rischio vero di MP dei pazienti.
Definizione di incidenzaUn’altra fonte di riflessione possibile è la definizione dell’in-cidenza da utilizzare per il calcolo dei MP attesi. L’obiettivodello studio era di valutare se la frequenza di secondi tumoriin pazienti affetti da cancro fosse diversa dal quella di primitumori in soggetti sani. Pertanto, come tasso di riferimento
and a 1.32 x 1,000 person-years Excess Absolute Risk (EARwomen:1.08; ERA men: 1.61).Both SIRs and EARs were provided, because they express a dif-ferent type of information, as explained in the guide to the can-cer-specific data sheets (pp. 31-38).In this monograph, it was decided to offer the highest degreepossible of representativeness by including the data producedby all AIRTUM registries, although at the expense of a differentfollow-up length.
Definition of second cancerBefore analyzing the results in greater detail, it is necessary to stressthat the study of MPs and their measures of risk are strongly de-pendent on the methods adopted for their computation.The definition itself of MP is debated and the use of differentrules may greatly modify the number of MPs in a patient.17
This issue is discussed in chapter 6 (pp. 114-119). All AIR-TUM cancer registries adopt the same IARC-IACR recommen-dations for MP definition.18 The above-mentioned rules do notallow MPs in the same anatomic site unless they belong to dif-ferent morphology groups. This makes it rather unusual to havetwo (or more) cancers in the same anatomic site. Among the101,179 analyzed second cancers, only 973 (1%) occurred inthe same anatomic site. Therefore, unlike in previous pa-pers,13,14 it was decided to compute MP frequency even exclud-ing the site of first cancer onset from both the observed and theexpected cancer cases.3 Among the 92,586.6 expected secondcancers 11,209.8 (12%) were in the same anatomic site. Theeffect of this choice in modifying the SIRs is impressive, espe-cially for frequent cancer sites, because the observed MPs in thesame site are usually few (due to both biology and rules),while the expected MPs are a huge number. For example, forMPs in female breast cancer patients the risk is 1.12 excludingthe breast, but it is 0.82 including it because the second MPsobserved in the breast are only 43 while the expected ones, ac-cording to breast cancer incidence rates, are 3,539. Estimatesincluding first cancer site are available in the supplementaryonline material. Both estimates are biased: estimates includingthe site of first cancer are underestimated, even strongly, as inthe example of female breast cancer, whereas estimates whichexclude the site of first cancer are slightly overestimated. In ouropinion the latter are closer to the real risk of patients.
Definition of incidenceAnother possible source of debate is the definition of thebaseline incidence in the general population which is necessaryfor expected MP computation. The objective of this study wasto evaluate whether the frequency of second cancers in cancerpatients was different from the frequency of first cancers inhealthy subjects. Therefore, the incidence in the general pop-ulation based on first primary cancers only should have beenused as reference rates. However, cancer incidence in a popu-lation is traditionally based on all cancer, first primaries and

Epidemiol Prev 37 (4-5) Suppl 1:1-152 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.it25
I tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI L’incidenza di secondi tumori in pazienti oncologici in Italia
subsequent cancers,19 and the issue of the length of cancer reg-istry activity was never addressed in the most famous collabo-rative study on cancer incidence, “Cancer Incidence in 5 Con-tinents”.19 For this reason, first and subsequent cancers wereused to express the incidence in the general population. As de-scribed in the «Materials and methods» chapter (pp. 11-17),the length of the registration period varies among cancer reg-istries, as does the frequency of MPs. In the AIRTUM Data-base, MPs (second or subsequent) are on average 4% of the to-tal cases. Therefore, the choice of using global incidence and notincidence based on primary cancers only may have increasedby around 4% the number of expected MPs and then under-estimated the “true” risk of MPs in cancer patients.
Diagnostic pressureAt the time of first cancer diagnosis, a number of exams is per-formed to define the cancer’s nature and extension. This diag-nostic pressure may lead to the detection of other not yet symp-tomatic cancers. This, together with the lack of comparablereference, causes very high SIRs. This point is addressed in chap-ter 7 (pp. 120-124). It was decided to exclude from observedand expected MPs the first 2 months after first cancer diagno-sis.1,4-6,14However, estimates of MP risk that include the com-plete period are also provided.
SequentialityMoreover, accuracy in the definition of sequentiality dependson the length of the period of activity in each cancer registry,as accuracy is presumably better for longer periods. As time ofactivity increases, the risk of defining «first» a cancer which ac-tually follows a prevalent one decreases. MP incidence couldtherefore be more highly underestimated in newly activatedcancer registries than in longstanding ones.
MigrationThe number of MPs registered by cancer registries may be re-duced due to patient migration, since information is not col-lected on further cancers incident in subjects previously residentin a registry area who then migrated. However, as also high-lighted in a previous paper,14 in Italy the migration rate fromthe municipality of residence is rather low: in 2001 it was, onaverage, 2.2%.20 Moreover, most cancer registries involved inthis study covered an area which included several municipal-ities. Therefore, part of the migration rate was towards othermunicipalities included in the same registry area. Presumablythe underestimation of MP due to migration is negligible.
Focusing again on the results of this study and taking intoaccount the above-mentioned issues in the interpretation ofSIR and EAR, it could be observed that the overall MP riskwas higher in both genders (SIR: 1.08 and 1.12 amongmen and women, respectively). Moreover, the absolute num-ber of MPs in excess was about 50% higher among men
si sarebbe dovuta utilizzare l’incidenza nella popolazione ge-nerale basata soltanto sui primi tumori. Tuttavia l’incidenzadel cancro in una popolazione è tradizionalmente misuratasu tutti i tumori, primi e successivi,19 e la questione della lun-ghezza del periodo di attività di un registro, che condizionail numero di tumori successivi al primo, non è stata mai af-frontata nel “Cancer Incidence in Five Continents”, il più fa-moso studio collaborativo condotto sul confronto dell’inci-denza delle patologie oncologiche a livello mondiale.19
Per questo motivo, per esprimere l’incidenza nella popola-zione generale è stata considerata l’incidenza basata sia suiprimi tumori sia sui successivi. Come descritto nel capitolo«Materiali e metodi» (pp. 11-17), la durata del periodo diattività varia da registro a registro, così come la frequenzadei MP. Nella Banca dati AIRTUM i tumori multipli (se-condi o successivi) sono in media il 4% del totale dei casi.La scelta di utilizzare l’incidenza globale e non quella basatasolo sui primi tumori può aver aumentato di circa il 4% (deltotale) il numero dei MP attesi, quindi anche sottostimatoil rischio “vero” di MP nei pazienti oncologici.
Pressione diagnosticaAl momento della diagnosi di tumore il paziente è sottopostoa numerosi esami con lo scopodi definire la natura e l’estensionedel tumore stesso.Questa pressione diagnostica può portare al-l’identificazione di altri tumori presenti ma non ancora sinto-matici.Tale fenomeno, assieme allamancanza di un termine diriferimento adeguato, in prossimità della diagnosi del primo tu-more determina SIR diMPmolto elevati.Questo punto è trat-tato al capitolo 7 (pp. 120-124). Per la presente monografia èstato deciso di escludere sia i MP osservati sia quelli attesi neiprimi 2 mesi dopo la diagnosi del primo.1,4-6,14 Tuttavia sonostate prodotte e presentate anche le stime del rischio diMP cheincludono il periodo completo.
SequenzialitàLa precisione nella definizione della sequenzialità dei tumorisuccessivi al primo dipende dalla durata del periodo di attivitàin ciascun registro, presumibilmentemigliore per quelli con unperiodo più lungo. Infatti, con il prolungarsi dell’attività dimi-nuisce il rischio di definire «primo» un tumore che in realtà èsuccessivo a un altro incidente prima dell’attivazione del registro(prevalente). Pertanto, l’incidenza deiMP potrebbe essere sot-tovalutata in registri tumori di nuova attivazione rispetto a quellidi attività più prolungata.
MigrazioneIl numero di MP registrati potrebbe essere ridotto a causadella migrazione dei pazienti. Infatti, i Registri non raccol-gono informazioni su quei soggetti che sono stati residentinell’area di attività del registro quando emigrano al di fuoridi questa. Tuttavia, come dimostrato anche in un lavoroprecedente,14 in Italia il tasso di emigrazione dal comune di

Epidemiol Prev 37 (4-5) Suppl 1:1-152 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.it26
I tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI L’incidenza di secondi tumori in pazienti oncologici in Italia
(EAR: 1.61 x 1,000 men-years) than women (1.08 x 1,000women-years) (table 1). In the AIRTUMDatabase the num-ber of second cancers diagnosed among men is almost doublethan among women; even the number of expected casesamong men is almost double than among women; thereforethe SIRs in the two genders are quite similar, only slightlyhigher in women (1.08 vs. 1.12). On the contrary, the num-ber of person-years at risk, that is the denominator of the EAR,is almost the same in the two groups, only slightly higheramong women, determining an Excess Absolute Risk that ishigher for men than women (1.61 vs. 1.08 x 1,000 PYs).This is due to the different incidence rates observed amongmales and females and to the different case-mix of first can-cers, which strongly influences the pattern of second cancer in-cidence (i.e., cancers with poor prognosis, such as lung cancer,are more frequently diagnosed in men, reducing the totalnumber of person-years at risk).Even though the relative risk of developing MPs (in comparisonto the general population) is almost the same for males and fe-males, the absolute number of cases in excess is higher amongmen, which is important in the follow-up perspective.The risk of further cancers is higher among younger cancer pa-tients and it decreases with increasing age. Older patientsshow lower MP incidence than expected.3 The relationship be-tween age and MP incidence is described and discussed inchapter 9 (pp. 133-146).This study encompasses a wide incidence period which goesfrom the late 1970s to the end of the early 2000s. However,the pattern of MP risk for cancer patients seems quite homo-geneous over time.The most important factor modifying the results is follow-uptime; this issue is discussed in depth in chapter 7 (pp. 120-124).SIR estimates were substantially homogeneous over time.This monograph presents for each first cancer site the overalland site-specific risk of MPs depending on the time sincecancer diagnosis.In the present monograph, SIRs stratified by first and secondsite, sex and time since diagnosis, resulting in a large numberof multiple comparisons for each initial cancer site, were pre-sented. Due to the huge numbers many SIRs are statisticallysignificant, showing either excesses or deficits in the risk of fur-ther cancers. In fact, multiple testing of stratified data tends toidentify a number of statistically significant risks of subsequentcancer that may have occurred by chance alone,21 greater thanone in 20 if we use p-value equal to 0.05 as it is usually done.
ExposureIt is confirmed that Italian cancer patients have a higher riskof MPs from anatomic sites that share the same carcinogenicexposure with the first one. This is the case, for example, of to-bacco-related cancers. Patients with a first cancer of the lungor oral cavity, oesophagus, larynx, or bladder have a high andbidirectional (site-site) risk of developing another cancer in the
residenza è piuttosto basso, in media il 2,2% nel 2001.20
Inoltre, la maggior parte dei registri tumori coinvolti in que-sto studio interessa un’area che comprende più comuni.Una parte della migrazione (che potrebbe essere consistente)è quindi diretta in altri comuni della stessa area di attivitàdel registro. La sottostima della frequenza dei MP legata allamigrazione dovrebbe perciò essere trascurabile.
Tornando ai risultati dello studio, e tenendo conto delle que-stioni sopra menzionate nell’interpretazione dei SIR e degliEAR, il rischio complessivo di MP appare più elevato in en-trambi i sessi rispetto alla popolazione generale (SIR uomini:1,08; SIR donne: 1,12). Inoltre, il numero assoluto di seconditumori in eccesso è più elevato tra gli uomini (EAR: 1,61 per1.000 uomini/anno) rispetto alle donne (EAR: 1,08 per 1.000donne/anno) (tabella 1).Nella Banca dati AIRTUM il numerodiMP diagnosticati tra gli uomini è quasi il doppio rispetto aquello diagnosticato tra le donne; così come il numero diMPattesi. Quindi i SIR nei due sessi sono sostanzialmente simili,solo leggermente più alto quello nel sesso femminile (1,08 vs.1,12). Al contrario, il numero di anni-persona a rischio, cioèil denominatore degli EAR, è quasi lo stesso nei due gruppi,un po’ più elevato tra le donne: ciò determina un eccesso di ri-schio assoluto maggiore tra gli uomini rispetto alle donne(1,61 vs. 1,08 per 1.000 persone-anno). Questo risultato è le-gato ai diversi tassi di incidenza osservati tra uomini e donnee al diverso case-mix di primo tumore, che influenza fortementeil modello di incidenza diMP (per esempio, i tumori con pro-gnosi infausta, come quello del polmone, sono più frequentinegli uomini, aspetto che contribuisce a rendere il numero dianni-persona a rischio più basso nel sesso maschile).Anche se il rischio relativo di sviluppare un MP (in con-fronto alla popolazione generale) è quasi lo stesso per uo-mini e donne, il numero assoluto di casi in eccesso è più ele-vato tra gli uomini; questo è un aspetto rilevante per ladefinizione dei follow-up clinici.Il rischio di MP è maggiore tra i pazienti più giovani e di-minuisce con l’aumentare dell’età. I pazienti più anzianimostrano un’incidenza di MP inferiore a quanto atteso.3 Larelazione tra età e incidenza dei MP è descritta e discussaal capitolo 9 (pp. 133-146).Il presente studio comprende un periodo di incidenza am-pio, che va dalla fine degli anni Settanta alla fine della primadecade degli anni Duemila. Tuttavia, l’eccesso di rischio diMP sembra abbastanza omogeneo nel tempo. Il fattoreche modifica maggiormente i risultati è il tempo di follow-up (si rimanda al capitolo di riflessione sui tumori sincroni,pp. 120-124). Le stime dei SIR risultano essere sostanzial-mente omogenee nel tempo.In questamonografia per ogni sede di primo tumore è presen-tato il rischio complessivo e specifico per sede di MP e pertempo dalla diagnosi. Si presentano, infatti, SIR stratificati persede di primo e secondo tumore, sesso e tempo dalla diagnosi.

Epidemiol Prev 37 (4-5) Suppl 1:1-152 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.it27
I tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI L’incidenza di secondi tumori in pazienti oncologici in Italia
tobacco-related sites, in both sexes and especially amongmales.3,22 Moreover, women with cervix uteri cancer have anincreased risk for some smoking-related sites as oral cavity, lar-ynx, lung, and urinary bladder.The reciprocal association among different sites is present alsofor sites which are alcohol-related, such as oral cavity, pharynx,oesophagus, larynx and liver.3,22
A common role of hormonal factors,23 nutritional factors,24 andoverweight 24,25 may also explain the higher and reciprocal MPrisk present among female breast, colorectal, corpus uteri, andovarian cancer.26-28 The need for and the positive effects oflifestyle changes correcting unhealthy behaviour in cancer patientshave been evaluated and should routinely be included in follow-up recommendations.29
Although the first two months after first cancer diagnosis wereexcluded, at least some of the MP excesses may be due to a resid-ual detection bias which follows the synchronous period, andwhich may explain, for example, the relationship betweenprostate cancer (SIR: 1.39 after urinary bladder cancer) andurinary bladder cancer (SIR: 1.12 after prostate cancer).30
The role of certain infective agents may contribute to explainsome of the associations identified. For example, the high riskfor cervix cancer as MP component for patients with a firstcancer in the pharynx (SIR: 5.0) and oesophagus (SIR: 5.76)may be due to Human Papillomavirus (HPV).31 Even humandeficiency virus, Human Herpesvirus 8, Epstein-Barr virus,hepatitis B, hepatitis C and Helicobacter pylori infectionsmay have contributed to some of the detected associations.3,32
The association between Hodgkin and non-Hodgkin lym-phomas with Kaposi sarcoma could be related to acquired ortherapy-related immunodepression.
Questo significa che sono stati condotti moltissimi confrontiper ciascuna sede di primo tumore; quindi a causa dell’elevatanumerosità, molti SIR risultano statisticamente significativi,cioè mettono in luce un eccesso o un difetto di MP.Nelle analisi che coinvolgono un numero di stratificazionielevato sono identificati una serie di rischi definiti «statisti-camente significativi» semplicemente per effetto del caso,21
in generale uno ogni venti confronti effettuati se si utilizzaun p-value pari a 0,05, come è consuetudine.
EsposizioneSi conferma, infine, che la popolazione oncologica italiana pre-senta un rischio aumentato diMPper le sedi tumorali che con-dividono la medesima esposizione a fattori cancerogeni delprimo tumore, come i tumori legati al fumo. I pazienti con unaprima diagnosi di tumore del polmone, cavità orale, esofago,laringe o vescica presentano un rischio aumentato e bidirezio-nale (sede-sede) di sviluppare un altroMP nelle stesse sedi tu-morali associate al fumo di tabacco, in entrambi i sessi, special-mente tra gli uomini.3,22 Inoltre, le donne con il tumore delcollo dell’utero hanno un eccesso di rischio per alcune sedi tu-morali associate al fumo, come la cavità orale, la laringe, il pol-mone e la vescica urinaria. L’associazione reciproca tra lediverse sedi tumorali è presente anche per i tumori legati all’al-col, come cavità orale, faringe, esofago, laringe e fegato.3,22
Un ruolo comune di fattori ormonali,23 nutrizionali24 e sovrap-peso24,25 può contribuire a spiegare l’eccesso di rischio bidire-zionale diMP per i tumori dellamammella femminile, del co-lon retto, del corpo dell’utero e dell’ovaio, associazionidimostrate già da tempo.26-28 I bisogni e gli effetti positivi delcambiamento degli stili di vita non salutari nei pazienti on-cologici sono stati valutati e dovrebbero essere inclusi di routinenelle raccomandazioni del follow-up.29
Nonostante siano stati esclusi dalle analisi i primi due mesidi follow-up dopo la diagnosi di primo tumore, alcunidegli eccessi di rischio di MP potrebbero essere attribuiti aun detection bias che supera il periodo definito «di sincro-nicità»; questo potrebbe spiegare, per esempio, l’associa-zione emersa tra tumore della prostata successivo a tumoredella vescica (SIR: 1,39) e tumore della vescica successivoa tumore della prostata (SIR: 1,12).30 Inoltre, il ruolo dicerti agenti infettivi può contribuire a spiegare alcune delleassociazioni evidenziate; per esempio, l’alto rischio per ilcancro della cervice tra le pazienti con un primo tumoredella faringe (SIR: 5,0) e dell’esofago (SIR: 5,76) può esserecorrelato alla presenza del Papillomavirus umano (HPV).31
Anche le infezioni dovute a virus dell’immunodeficienzaumana, Herpes virus umano 8, Epstein-Barr virus, epatiteB, epatite C o Helicobacter pylori possono aver avuto unruolo nel determinare alcune fra le associazioni eviden-ziate.3,32L’associazione tra linfomi di Hodgkin e non-Hodg-kin con il sarcoma di Kaposi potrebbe essere legata all’im-munodepressione acquisita oppure alla terapia.

Epidemiol Prev 37 (4-5) Suppl 1:1-152 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.it28
I tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI L’incidenza di secondi tumori in pazienti oncologici in Italia
TreatmentSome of the excess MP risk of cancer patients may be due totreatment performed for the first cancer. Unfortunately, dataon therapy are not routinely available in the AIRTUMData-base. However, the effect of chemotherapy or radiotherapymay explain some of the associations found, e.g., the increasedrisk of leukaemia, myeloid leukaemia in particular,1,33 lung,34
and breast cancer35 after Hodgkin lymphoma. In addition, theincreased risk found for urinary bladder cancer after cervixuteri cancer may be related to radiation treatment, as previ-ously shown.3,36,37 Moreover, the association between bone andconnective tissue cancers may be treatment-related.3
Genetic susceptibilityAt least some of the detected associations may be the expressionof a genetic susceptibility to cancer and familial clusters.22,38
This point is touched on in chapter 5 (pp. 109-113) and inchapter 9 (pp. 133-146). For example, the early onset of coloncancer may be related to synchronous and metachronous en-dometrial, stomach, ovarian, pancreas, ureter and renal pelvis,biliary tract, and brain cancer and carcinoma of the smallbowel in Lynch syndrome.39,40 Among other familial cancer syn-dromes, in case of an early onset of breast cancer and soft tissuesarcomas, osteosarcomas, brain tumours, acute leukaemias,and adrenocortical tumours in children and young adults, theLi-Fraumeni syndrome should also be suspected.41,42
In women with germline mutations of BRCA1/2 the early on-set of breast cancer is usually associated with MPs in the con-tralateral breast (not measured in this study) and ovariancancer. The association of melanoma and prostate cancershown in this study has been described among men withBRCA2 mutations.43 The associations of melanoma, prostate,endometrial and breast cancers are associated with an in-creased expression of EZH2.44
Limitations of the studySeveral SIRs significantly lower than 1 were recorded when site-specific risks were evaluated. These results are difficult to in-terpret as a protective effect of cancer against other cancers.Some of these results may be related to problems in cancer reg-istration. For example, the lower risk of further rectum cancersin patients with colon cancers (SIR: 0.89, men and women)and vice versa (SIR: 0.78) may be related to the difficulties indifferentiating MPs from relapses in these two organs, whichare anatomically and histological identical.On the contrary, misclassification may be involved in the in-creased and bidirectional risk between Hodgkin and non-Hodgkin lymphomas,3 although a cellular immune dysfunctionhas been shown in longstanding Hodgkin lymphoma pa-tients.45
Reduced SIRs may also be due to reduced cancer registrationwhen metastases are suspected: this may partially explain thelow risk for lung cancer in, for example, stomach (SIR: 0.87,
TrattamentoParte dell’eccesso di rischio di MP nei pazienti oncologicipuò essere correlato al trattamento effettuato per il primotumore. Purtroppo i dati sulla terapia non sono disponibilidi routine nella Banca dati AIRTUM.Tuttavia, l’effetto dichemioterapia o radioterapia può spiegare alcune fra le as-sociazioni messe in evidenza, per esempio l’aumento del ri-schio di leucemie, in questo studio quelle mieloidi,1,33 deltumore del polmone34 e dei tumori della mammella fem-minile35 successivi al linfoma di Hodgkin.Inoltre, l’eccesso di rischio evidenziato per il cancro della ve-scica dopo il tumore del collo dell’utero può essere associatoal trattamento radioterapico, come rilevato da studi prece-denti.3,36,37 Anche le associazioni messe in luce tra tumoridell’osso e tumori dei tessuti connettivi può essere legata altrattamento.3
Predisposizione geneticaAlmeno alcune delle associazioni evidenziate possono essereespressione di una predisposizione genetica e di raggruppa-menti familiari.22,38 Questo aspetto è affrontato nel capitolo 5(pp. 109-113) e nel capitolo 9 (pp. 133-146). A titolo esem-plificativo, l’insorgenza in giovane età di un tumore del colonpuò essere associata a tumori sincroni e metacroni dell’endo-metrio, dello stomaco, dell’ovaio, del pancreas, dell’uretere epelvi renali, delle vie biliari, dei tumori cerebrali e del piccolointestino nella sindrome di Lynch.39,40Tra le altre sindromi tu-morali familiari, in caso di insorgenza precoce di tumore dellamammella, sarcomi dei tessuti molli, osteosarcomi, tumori ce-rebrali, leucemie acute e carcinomi della corteccia surrenale neibambini e nei giovani adulti deve essere presa in considerazioneanche la sindrome di Li-Fraumeni.41,42Nelle donne con mu-tazioni germinali di BRCA1/2 l’insorgenza precoce del tu-more al seno è di solito associata con MP nella mammellacontrolaterale (non misurati in questo studio) e tumori ova-rici. L’associazione di melanoma e tumore della prostata evi-deziato in questo studio è stata descritta tra gli uomini conmutazioni BRCA2.43 L’associazione di melanoma, tumoridella prostata, endometrio e mammella può essere in rela-zione con un sovraespressione di EZH2.44
Limiti dello studioNella valutazione dei rischi di MP per singola sede tumoralesono stati evidenziati anche alcuni SIR significativamente in-feriori a 1. Questi risultati sono difficili da interpretare comeun effetto protettivo nei confronti di un cancro attribuibile allapresenza di altri tumori. Alcuni di questi risultati potrebberoessere ascrivibili a problemi nella registrazione della casistica.Per esempio, il più basso rischio di tumori del retto in pazienticon una diagnosi di cancro del colon (SIR: 0,89 uomini edonne assieme) e viceversa (SIR: 0,78) può essere attribuito alladifficoltà di differenziareMP da recidive in questi due organi,che sono anatomicamente e istologicamente identici. Al con-

trario, l’eccesso di rischio osservato bidirezionalmente tra lin-fomi di Hodgkin e non-Hodgkin3 può essere legato alla pre-senza di errori di classificazione, anche se nei pazienti con lin-foma di Hodgkin ammalati da lungo periodo è stataevidenziata una disfunzione immunitaria cellulare.45
La presenza di SIR inferiori all’unità può anche essere dovutaa una sottoregistrazione dei secondi tumori nel caso in cui visia il sospetto dimetastasi, questo può in parte spiegare il bassorischio perMPdel polmone successivo a tumore dello stomaco(SIR: 0,87 uomini e donne assieme), del colon (SIR: 0,90) odella prostata (SIR: 0,74), o il basso rischio per cancro alfegato successivo a tumore dello stomaco (SIR: 0,64), delcolon (SIR: 0,75), del retto (SIR: 0,65), melanoma (SIR:0,59) o della mammella femminile (SIR: 0,85).In aggiunta, la rimozione chirurgica di un organo per il trat-tamento del primo tumore può contribuire a spiegare il rischioridotto perMPnello stesso organo. Può essere il caso dell’utero,per il quale si osserva una frequenza ridotta diMPbidirezionaletra corpo e collo (SIR: 0,25 e 0,27, rispettivamente).3,36
Infine, alcuni dei SIR inferiori all’unità possono anche essere do-vuti alla bassa intensità delle indagini mediche, come per i pa-zienti di età superiore a 70 anni (SIR: 0,96; uomini e donne).
CONCLUSIONIIn conclusione, i pazienti oncologici italiani presentano un ec-cesso di rischio di MP rispetto alla popolazione generale: ciòcorrisponde a più di 1 tumore ogni 1.000 anni-persona di fol-low-up previsto. Lamisura sintetica qui stimata, che quantificacomplessivamente l’eccesso di rischio rispetto alla popolazionegenerale, è pari al 10% (8% uomini e 12% donne) e dipendedalle ipotesi di base adottate. Presumibilmente, l’interesse deipazienti e dei clinici non è limitato solo a queiMP che soddi-sfano le definizioni utilizzate dai registri tumori. Perciò inambito clinico l’eccesso di rischio diMP sarà presumibilmentedi entità superiore.Questo studio intende comunicare che i malati di cancrohanno un rischio aumentato di sviluppare ulteriori tumori.Le tabelle specifiche per sede di primo tumore (pp. 40-108),che rappresentano il nucleo della monografia, possono es-sere utili per evidenziare e quantificare le associazioni bidi-rezionali, sia già note sia sconosciute, tra diverse patologiee guidare il follow-up clinico. Le modifiche degli stili di vitain direzioni più salutari possono avere un effetto positivoanche nella popolazione oncologica e devono sempre essereraccomandate.
men and women), colon (SIR: 0.90), or prostate cancers (SIR:0.74), or the low risk for liver cancer after stomach (SIR:0.64), colon (SIR: 0.75), rectum (SIR: 0.65), melanoma(SIR: 0.59), or female breast (SIR: 0.85) cancer.Moreover, the surgical removal of an organ for the treatment ofthe first cancer may contribute to explain the reduced MP riskin the same organ. This may be the case of the uterus for whichit was found a bidirectional decrease in MP frequency betweencorpus and cervix (SIR: 0.25 and 0.27, respectively).3,36
Finally, some of the lower SIRs may also be due to a less inten-sive medical scrutiny, as for patients older than 70 years (over-all SIR: 0.96, men and women).
CONCLUSIONSIn conclusion, Italian cancer patients have an increased riskof MPs compared to the general population; this corresponds tomore than 1 cancer expected every 1,000 person-years of fol-low-up. The overall measure of relative risks provided, 10%(8% men and 12% women), depends on the assumptionsadopted. Presumably, the interest of patients and clinicians isnot limited only to the MPs which fulfil the definitions usedby cancer registries. Therefore, in the clinical setting the MPrisk will presumably be greater.The general message of this study is that cancer patients havean increased risk of developing further cancers. The site-specifictables (pp. 40-108) which are the core of this monograph maybe useful to highlight and quantify known and unknownbidirectional cancer associations, directing the clinical fol-low-up. Lifestyle changes have been proven effective evenamong cancer patients and should be recommended.
L’incidenza di secondi tumori in pazienti oncologici in ItaliaI tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI
29 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152

L’incidenza di secondi tumori in pazienti oncologici in ItaliaI tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI
30 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
BIBLIOGRAFIA/REFERENCES
1. Curtis RE, Boice JD Jr, Kleinerman RA, Flannery JT, Fraumeni JF Jr.Summary: multiple primary cancers in Connecticut, 1935-82. NatlCancer Inst Monogr 1985;68:219-42.
2. Heard A, Roder D, Luke C. Multiple primary cancers of separate organsites: implications for research and cancer control (Australia). CancerCauses Control 2005;16(5):475-81.
3. Curtis RE, Freedman DM, Ron E et al (eds). NewMalignancies AmongCancer Survivors: SEER Cancer Registries, 1973-2000. NIH Publ. No.05-5302. Bethesda (MD), National Cancer Institute, 2006.
4. Levi F, Randimbison L, Te VC, Rolland-Portal I, Franceschi S, La VecchiaC. Multiple primary cancers in the Vaud Cancer Registry, Switzerland,1974-89. Br J Cancer 1993;67(2):391-5.
5. Youlden DR, Baade PD. The relative risk of second primary cancersin Queensland, Australia: a retrospective cohort study. BMC Cancer2011;11:83.
6. Cluze C, Delafosse P, Seigneurin A, Colonna M. Incidence of secondcancer within 5 years of diagnosis of a breast, prostate or colorectalcancer: a population-based study. Eur J Cancer Prev 2009;18(5):343-8.
7. Tsukuma H, Fujimoto I, Hanai A, Hiyama T, Kitagawa T, Kinoshita N.Incidence of second primary cancers in Osaka residents, Japan, withspecial reference to cumulative and relative risks. Jpn J Cancer Res1994;85(4):339-45.
8. ColemanMP. Multiple primary malignant neoplasms in England andWales, 1971-1981. Yale J Biol Med 1986;59(5):517-31.
9. Teppo L, Pukkala E, Saxén E. Multiple cancer – an epidemiologic ex-ercise in Finland. J Natl Cancer Inst 1985;75(2):207-17.
10.Karahalios E, English D, Thursfield V, Simpson J, Farrugia H, GrahamG. Second primary cancers in Victoria. Melbourne, Victorian CancerRegistry, Cancer Epidemiology Centre, CAncer Council Victoria, 2009.Available at: http://www.cancervic.org.au/about-our-research/epidemiology/second-primary-cancers-victoria
11.Crocetti E, Lecker S, Buiatti E, Storm HH. Problems related to the cod-ing of multiple primary cancers. Eur J Cancer 1996;32A(8):1366-70.
12.Buiatti E, Crocetti E, Gafà L et al. Agreement estimate among threeItalian cancer registries in the coding of multiple primary cancers. Tu-mori 1996;82(6):533-8.
13.Buiatti E, Crocetti E, Acciai S et al. Incidence of second primary can-cers in three Italian population-based cancer registries. Eur J Cancer1997;33(11):1829-34.
14.Crocetti E, Buiatti E, Falini P; Italian Multiple Primary Cancer WorkingGroup. Multiple primary cancer incidence in Italy. Eur J Cancer2001;37(18):2449-56.
15.Crocetti E, Guzzinati S, Paci E et al. The risk of developing a second,different, cancer among 14 560 survivors of malignant cutaneousmelanoma: a study by AIRTUM (the Italian Network of Cancer Reg-istries).Melanoma Res 2008;18(3):230-4.
16.AIRTUMWorking Group. Italian cancer figures, report 2011:Survivalof cancer patient in Italy. Epidemiol Prev 2011;35(5-6) Suppl 3:1-200.
17.Crocetti E, Buiatti E. Re: multiple neoplasias: an oncologic reality.J Natl Cancer Inst 1997;89(21):1634-6.
18.Pheby D, Martinez C, Roumagnac M, Schouten L. Recommendationsfor coding Multiple Primaries. 2000. Available at: http://www.encr.com.fr/multpeng.pdf
19.Curado MP, Edwards B, Shin HR et al (eds). Cancer Incidence in FiveContinents, Vol. IX. IARC Scientific publications n.160. Lyon 2007.
20.Statistiche demografiche ISTAT. Available at: http://demo.istat.it/bil2002/index.html
21.Goodman SN. Multiple comparisons, explained. Am J Epidemiol1998;147(9):807-12.
22.Hemminki K, Boffetta P. Multiple primary cancers as clues to environ-mental and heritable causes of cancer and mechanisms of carcino-genesis. IARC Sci Publ 2004;(157):289-97.
23.Henderson BE, Feigelson HS. Hormonal carcinogenesis. Carcinogen-esis 2000;21(3):427-33.
24.World Cancer Research Fund; American Institute for Cancer Re-search. Food, Nutrition, Physical Activity, and the Prevention of Can-cer: a Global Perspective. Washington (DC), AICR, 2007.
25.Renehan AG, Tyson M, Egger M, Heller RF, Zwahlen M. Body-massindex and incidence of cancer: a systematic review andmeta-analysisof prospective observational studies. Lancet 2008;371(9612):569-78.
26.Ahsan H, Insel BJ, Neugut AI. Risk estimates for second primary can-cers. In: Neugut AI, Meadows AT, Robinson E (eds).Multiple primarycancers. Philadelphia (PA), Lippincott Williams and Wilkins, 1999;pp. 27-53.
27.Schatzkin A, Baranovsky A, Kessler LG. Diet and cancer. Evidencefrom associations of multiple primary cancers in the SEER program.Cancer 1988;62(7):1451-7.
28.Neugut AI, Murray TI, LeeWC, Robinson E. The association of breastcancer and colorectal cancer in men. An analysis of Surveillance, epi-demiology, and results program data. Cancer 1991;68(9):2069-73.
29.Pinto BM, Trunzo JJ. Health behaviours during and after a cancer di-agnosis. Cancer 2005;104(11) Suppl:2614-23.
30.Kellen E, Zeegers MP, Dirx M et al. Occurrence of both bladder andprostate cancer in five cancer registries in Belgium, The Netherlandsand the United Kingdom. Eur J Cancer 2007;43(11):1694-700.
31.Chaturvedi AK, Kleinerman RA, Hildesheim A et al. Second cancersafter squamous cell carcinoma and adenocarcinoma of the cervix.J Clin Oncol 2009;27(6):967-73.
32.Hisada M, Rabkin CS. Viral causes of cancer. In: Shields PG (ed). Can-cer risk assessment. Boca Raton, Taylor & Francis, 2005; pp. 287-311.
33.van Leeuwen FE, Travis LB. Second cancers. In: DeVita VT Jr, Hell-man S, Rosenberg SA (eds). Cancer Principles and Practice of On-cology, 6th ed. Philadelphia, Lippincott Williams & Wilkins, 2001;pp. 2939-64.
34.Travis LB, Gospodarowicz M, Curtis RE et al. Lung cancer followingchemotherapy and radiotherapy for Hodgkin’s disease. J Natl CancerInst 2002;94(3):182-92.
35.Preston DL, Mattsson A, Holmberg E, Shore R, Hildreth NG, Boice JDJr. Radiation effects on breast cancer risk: a pooled analysis of eightcohorts. Radiat Res 2002;158(2):220-35.
36.Crocetti E, Paci E. Prevalence of hysterectomy and its effect onuteran cancer incidence rates. Gynecol Oncol 2000;79(2):337-8.
37.Boice JD Jr, Day NE, Andersen A et al. Second cancer following ra-diation treatment for cervical cancer. An international collaborationamong cancer registries. J Natl Cancer Inst 1985;74(5):955-75.
38.Kerber RA, O’Brien E. A cohort study of cancer risk in relation to fam-ily histories of cancer in the Utah population database. Cancer2005;103(9):1906-15.
39.Lin KM, Shashidharan M, Thorson AG et al. Cumulative incidence ofcolorectal and extracolonic cancers in MLH1 andMSH2mutation car-riers of hereditary nonpolyposis colorectal cancer. J Gastrointest Surg1998;2(1):67-71.
40.Umar A, Boland CR, Terdiman JP et al. Revised Bethesda Guidelinesfor hereditary nonpolyposis colorectal cancer (Lynch syndrome) andmicrosatellite instability. J Natl Cancer Inst 2004;96(4):261-8.
41.Li FP, Fraumeni JF Jr. Soft-tissue sarcomas, breast cancer, and otherneoplasms. A familial syndrome? Ann Intern Med 1969;71(4):747-52.
42.Hisada M, Garber JE, Fung CY, Fraumeni JF Jr, Li FP. Multiple primarycancers in families with Li-Fraumeni syndrome. J Natl Cancer Inst1998;90(8):606-11.
43.Cancer risks in BRCA2 mutation carriers. The Breast Cancer LinkageConsortium. J Natl Cancer Inst 1999;91(15):1310-6.
44.Bachmann IM, Halvorsen OJ, Collett K et al. EZH2 expression is as-sociated with high proliferation rate and aggressive tumor subgroupsin cutaneous melanoma and cancers of the endometrium, prostate,and breast. J Clin Oncol 2006;24(2):268-73.
45.Poppema S. Immunology of Hodgkin’s disease. Baillieres Clin Haema-tol 1996;9(3):447-57.

WWW.EPIPREV.IT Guida alla letturadelle schede specifiche per tumoreA guide to the cancer-specific data sheets
31 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
I tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI
In ognuna delle schede presentate in questa sezione è statapresa in considerazione una sede di primo tumore: sonostate selezionate 34 sedi tumorali per le donne e 33 per gliuomini; a queste si aggiunge la scheda relativa al complessodi «Tutti i tumori».Le schede riportano un indicatore di rischio (eccesso o di-fetto) di sviluppare un seconda neoplasia dopo una primadiagnosi di tumore rispetto alla popolazione generale.Nelle schede troviamo le informazioni che ci permettonodi rispondere a domande come questa:PROSPETTIVA INDIVIDUALE: «Una donna, a cui è stato diagno-sticato un tumore della mammella, presenta un rischio mag-giore di sviluppare un nuovo tumore in altre sedi, per esem-pio dell’utero, rispetto a chi non ha mai avuto un tumore?»PROSPETTIVA DI POPOLAZIONE: «Tra le 500.000 donne ita-liane con una pregressa diagnosi di tumore della mammellasono attesi un numero maggiore o minore di secondi tu-more in altre sedi, per esempio l’utero, rispetto alla popo-lazione generale?»
Le risposte a queste domande serviranno a indirizzare il fol-low-up dei pazienti dopo la neoplasia, a suggerire eventualistrategie di prevenzione, a indirizzare la ricerca eziologia (peresempio evidenziando un’esposizione condivisa, come nelcaso dei tumori del polmone e della laringe), a studiare glieffetti a lungo termine del trattamento del primo tumore,e a migliorare la programmazione sanitaria.
This publication presents a set of data sheets for each first can-cer site (34 sites among women and 33 among men). A sheetfor «All cancer» is also included.For each cancer site we report indicators of the risk (excess orreduction) of developing a second cancer after first diagnosiscompared to the general population.Information in the sheet allows us to answer the following ques-tions:INDIVIDUAL PERSPECTIVE: «Does a woman diagnosed withbreast cancer have an increased risk of developing a newcancer in other sites (i.e., uterus) compared to the general pop-ulation?»POPULATION PERSPECTIVE: «Among the 500,000 Italianwomen living with a diagnosis of breast cancer, how many sec-ond cancers will be diagnosed? A higher or lower number com-pared to the general population?»
The answers to these questions will contribute to the pro-gramming of cancer patient follow-up, suggest possible preven-tion strategies, direct research aetiology (e.g., highlightingshared exposures, as in the case of lung and larynx cancer),study the long-term effects of first cancer treatment, and im-prove public health planning.
Capitolo 3
PRIMO TUMORE. Detto anche tumore indice,è il primo tumore diagnosticato nel periodo diattività dei singoli registri (come di consueto,nella presente Monografia sono esclusi i tu-mori non melanomatosi della cute).
SECONDO TUMORE. E’ il tumore temporal-mente successivo al primo diagnosticato nelperiodo di attività del registro.
TUMORI SUCCESSIVI. Nelle schede è analiz-zata solo l’incidenza dei secondi tumori; i suc-cessivi (terzo, quarto eccetera) non sono in-clusi, ma c’è un capitolo specifico che valutale associazioni di tre o più tumori (pp. 109-113). I primi e secondi tumori analizzati sonotumori primitivi secondo la definizione ripor-tata di seguito.
TUMORE PRIMITIVO.Un tumore è primitivo oprimario quando origina in una sede o tessutoe non è estensione, recidiva o metastasi diuna precedente neoplasia.
METASTASI. Un tumore è definito metastasiquando si sviluppa per diffusione del tumoreprimitivo in una sede anatomica diversa daquella di origine.
RECIDIVA. La recidiva è un tumore che si ma-nifesta nella stessa sede anatomica in cui si èpresentato il tumore primitivo ed è dovutaalla permanenza di alcune cellule che hannoresistito alla terapia.
TUMORI SINCRONI. Sono detti sincroni duetumori diagnosticati a meno di due mesi di di-
stanza l’uno dall’altro. Questa definizione è ar-bitraria anche se è la più frequente negli studidi popolazione (vedi capitolo sui tumori sin-croni, pp. 120-124).
TUMORI METACRONI. Sono metacroni duetumori diagnosticati a più di due mesi di di-stanza l’uno dall’altro. Questa definizione è ar-bitraria anche se è la più frequente negli studidi popolazione (vedi pp. 120-124).
POPOLAZIONE ONCOLOGICA (in questo stu-dio). Insieme delle persone che hanno avutouna diagnosi di primo tumore.
POPOLAZIONE GENERALE (in questo studio).Insieme delle persone che non hanno mai ri-cevuto una diagnosi di tumore.
GLOSSARIO

REGISTRY CONTRIBUTION IN THE EVALUATIONOF MULTIPLE PRIMARIESThe occurrence of multiple primaries (MPs) is present in the lit-erature in 3 main types of studies: a. case reports, b. clinical series,and c. population-based studies on cancer registry (CR) data.Apart from the case-report studies, which aim to present peculiarsituations and highlight “sentinel” events, the other types ofstudies have classic epidemiological study designs: case-controland cohort studies.Analyses from clinical series collect detailed information onclinical variables, to evaluate the effects of different anti-cancerdrugs and treatments, but they are mostly restricted to a specificprimary cancer site.Population-based studies include a large number of subjects, al-lowing the detection of even small risks and the evaluation oftemporal trends related to the evolution of cancer treatments. Se-lection bias due to using different populations for the computa-tion of observed and expected cases is avoided in this type of study.However, population-based studies offer scanty information ondrugs, dosages, and radiation treatments. A further limit is rep-resented by the under-registration ofMPs in people who migratedoutside the area covered by the CR. CRs are addressing these lim-its by collecting more precise information on biological variablesof major cancer sites and on treatment protocols. A study on mi-gration in Italy, furthermore, found that the rate of migrationis low, and mainly involves migration to nearby towns coveredby the same CR.Population-based studies ensure the appropriate sample sizeand length of follow-up required for an analysis of MPs; the lackof accuracy in defining the type and degree of association betweenrisk factors is compensated by the importance that incidence playsin public health.The study on the occurrence of MPs complements the contribu-tion of CRs to cancer epidemiology, adding, for a representativearea of Italy, a further indicator besides those of incidence, mor-tality, survival, and prevalence.
Guida alla lettura delle schedeI tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI
32 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
FIRST CANCER. Also called index cancer. It isthe first cancer diagnosed during the registra-tion period of each cancer registry (as usual, inthis study we excluded non-melanoma skincancer).SECOND CANCER.A subsequent (to first) can-cer diagnosed during the registration period ofeach cancer registry.SUBSEQUENT CANCERS. In site-specific sheetswe analyzed only the incidence of secondcancers; subsequent (third, fourth, etc.) can-cers were not included, but a specific chapterevaluates the associations among three ormore cancers, pp. 109-113).First and second cancers are both “primary
cancers” according to the following definition.PRIMARY CANCER.A cancer is defined as pri-mary when it originates from a specific site ortissue and it is not an extension, recurrence, ormetastasis of a previous cancer.METASTASIS.A cancer is defined as metastaticwhen it spreads to sites other than the site oforigin of the primary cancer.RELAPSE. Relapse, or recurrence, occurs whena cancer develops in the same site where theprimary cancer was diagnosed. It is caused byresidual treatment-resistant cells.SYNCHRONOUS CANCERS. Two cancers aresynchronous if the second cancer is diag-nosed within two months after the first one.
Although this definition is arbitrary, it is theone most used in population-based studies(see chapter on synchronous tumours, pp.120-124).METACHRONOUS CANCERS. Two cancers aremetachronous if the second cancer is diag-nosed two or more months after the first one.Although this definition is arbitrary, it is theone most used in population-based studies(see pp. 120-124).CANCER POPULATION (in this study). Peoplewho were diagnosed with cancer.GENERAL POPULATION (in this study). Peoplewho were never diagnosed with cancer.
GLOSSARY
CONTRIBUTO DEI REGISTRI ALLA VALUTAZIONEDEI TUMORI MULTIPLIL’occorrenza dei tumori multipli (MP) è presente in lette-ratura attraverso 3 principali tipi di studio: a. case-report, b.casistiche cliniche, c. studi di incidenza prodotti da Registritumori di popolazione (RT). A prescindere dai case-report,che hanno la finalità di presentare situazioni peculiari edevidenziare eventi sentinella, le altre tipologie sono ricon-ducibili a classici studi di coorte e caso-controllo.Le analisi di casistiche cliniche si basano su informazionidettagliate sul percorso diagnostico-terapeutico finalizzatealla valutazione degli effetti dei trattamenti, ma presentanoi limiti dovuti all’impossibilità di monitorare l’intero ambitonosologico della patologia.Gli studi di popolazione sono basati su un’ampia popola-zione monitorata e permettono, quindi, di evidenziare rischianche di modesta entità e documentare trend temporali inrelazione all’evoluzione dei trattamenti terapeutici. Nonsono soggetti a bias derivanti dall’uso di popolazioni diverseper il calcolo di casi osservati e attesi. Tuttavia presentano unbasso livello informativo sull’iter diagnostico-terapeutico eun limite connesso alla sottoregistrazione in soggetti emi-grati. I RT stanno ovviando a tali limiti ampliando le infor-mazioni raccolte (studi ad alta risoluzione su fattori biologicie protocolli terapeutici). Inoltre i dati indicano che in Italiale migrazioni nelle aree coperte da RT riguardano una quotarelativamente bassa di soggetti e che avvengono prevalente-mente tra municipalità dello stesso RT.Gli studi di popolazione hanno la numerosità campionariae l’estensione temporale necessarie per fornire dati reali sul-l’incidenza dei MP; la carenza di accuratezza nel definire tipoe grado di associazione tra i fattori di rischio è compensatadalla rilevanza che il dato di incidenza riveste in sanità pub-blica. Con il contributo conoscitivo sulla frequenza di MP,i RT italiani aggiungono un ulteriore indicatore a quelli diincidenza, mortalità, sopravvivenza e prevalenza.

Guida alla lettura delle schedeI tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI
33 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
1
23
4
1
2
3
4
5
POPOLAZIONE IN STUDIO / POPULATION
TEMPO DALLA DIAGNOSI / FOLLOW-UP PERIOD
NUMERO DI SOGGETTI / NUMBER OF SUBJECTS
ANNI-PERSONA DI OSSERVAZIONE / PERSON-YEARS
INDICATORI: SIR ED EAR / INDICATORS: SIR AND EAR
5
POPOLAZIONE IN STUDIO(POOL AIRTUM 1976-2010)
Le stime del rischio sono state prodotte utilizzando i dati AIR-TUM provenienti dai RT italiani attivi tra il 1976 e il 2010.In questo lasso di tempo l’ampiezza della popolazione sorve-gliata dai RT è di molto aumentata, passando dai pochi puntipercentuali degli anni Settanta (2%della popolazione italiana)all’attuale copertura di circa il 50%. Le difficoltà tecniche do-vute all’inclusione nel pool AIRTUM 1976-2010 di un nu-mero sempre crescente di Registri sono valutate e discusse nelcapitolo di commento (capitolo 10, pp. 147-148).
1 STUDY POPULATION(AIRTUM 1976-2010 POOL)
The risk estimates were produced using AIRTUM data col-lected by the Italian cancer registries that were active between1976 and 2010. During this period, population coverage bycancer registries greatly increased, from a few percentage pointsin the 1970s (2% of the Italian population) to the current cov-erage of about 50%.The technical difficulties arising from theinclusion of a growing number of registries in the AIRTUM1976-2010 pool are addressed in a specific chapter (Chapter10, pp. 147-148).
1

TEMPO DALLA DIAGNOSI(FOLLOW-UP: ≥0 MESI; ≥2 MESI; 2-11 MESI …)
Per i pazienti con tumore il rischio di sviluppare una se-conda neoplasia nel periodo immediatamente successivoalla prima diagnosi varia nel tempo, per esempio, è più ele-vato rispetto a quello della popolazione generale, come de-scritto nel capitolo sui tumori sincroni (pp. 120-124). Pertale motivo le stime del rischio sono state calcolate per di-versi intervalli temporali.Le intestazioni di colonna indicano il tempo di follow-up,ovvero il tempo trascorso dopo la prima diagnosi di tumore.≥0 MESI Il rischio è calcolato su tutto il periodo successivoalla prima diagnosi.≥2 MESI Il rischio è calcolato escludendo i tumori sincroni,ovvero i tumori diagnosticati e attesi entro 2 mesi dallaprima diagnosi. Questo è il dato più importante (vediprima colonna per i SIR, penultima per gli EAR) perché almomento della diagnosi di tumore il paziente è sottopostoa numerosi esami che hanno lo scopo di definire la naturae l’estensione del tumore stesso. Questa pressione diagno-stica può portare all’identificazione di altri tumori presentima non ancora sintomatici e, in alcuni casi, a sovradiagnosi,cioè identificazione di tumori asintomatici che non si sareb-bero mai manifestati nel corso della vita della persona.Questo fenomeno, assieme alla mancanza di un termine diriferimento adeguato, determina, in prossimità della dia-gnosi del primo tumore, SIR ed EARmolto elevati (vedi ca-pitolo tumori sincroni pp. 120-124).0-1 MESI Il rischio è calcolato fino al 2° mese incluso dopola diagnosi (sincroni).2-11 MESI Il rischio è calcolato limitatamente al 1° anno,escludendo i tumori sincroni.12-59 MESI Il rischio è calcolato dal 2° al 5° anno.60-119 MESI Il rischio è calcolato dal 6° al 10° anno.≥120 MESI Il rischio è calcolato oltre il 10° anno.
NUMERO DI SOGGETTI
Numero di soggetti vivi all’inizio dell’intervallo indica ilnumero di pazienti oncologici che (a partire da un deter-minato periodo di tempo) vengono seguiti nel tempo. Manmano che il tempo dalla prima diagnosi passa, il numero deipazienti seguiti diminuisce (a causa dei decessi o del veri-ficarsi dell’evento di interesse − diagnosi del secondo tu-more).
ANNI-PERSONA DI OSSERVAZIONE
Numero di anni-persona a rischio. E’ il numero totale dianni/persona durante i quali la popolazione in studio è stata
2
3
4
Guida alla lettura delle schedeI tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI
34 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 2013; 37 (1) suppl 1: 1-296
TIME SINCE DIAGNOSIS(FOLLOW-UP: ≥0 MONTHS; ≥2 MONTHS;2-11 MONTHS…)
The risk for cancer patients of developing another cancer, incomparison with the general population, varies according totime; for example, it is high immediately after the first cancerdiagnosis, as described in the chapter on synchronous cancers(pp. 120-124). For this reason the estimates are provided fordifferent time intervals.The column headers show the follow-up period, i.e., the timesince the diagnosis of the first cancer.≥0 MONTHSThis is the risk for the whole period after the firstdiagnosis.≥2 MONTHSThe risk is computed excluding the cancers diag-nosed (and expected) within the first two months (synchronouscancers). This is the most relevant result (see the first columnfor the SIR and the second to last for the EAR), becauseduring the diagnostic period of the first cancer, patients undergowide-range testing to define the behaviour and the extensionof their cancer. This high diagnostic pressure may lead to thediagnosis of other non-symptomatic cancers, with a certainamount of overdiagnosis for tumours that would have never be-come clinically evident during the life of the patients. This, to-gether with the lack of an appropriate control group, make theSIR and EAR very high close to diagnosis.0-1 MONTH The risk is computed within the 2nd month afterdiagnosis (synchronous period).2-11 MONTHS The risk is computed for the 1st year excludingthe synchronous period.12-59 MONTHSThe risk is computed between the 2nd and the5th year.60-119 MONTHSThe risk is computed between the 6th and the10th year.≥120 MONTHS The risk is computed after 10 years.
NUMBER OF SUBJECTS
Number of subjects alive at interval beginning indicatesthe number of cancer patients who (from a given period oftime) are followed over time. The longer the time from first di-agnosis, the lower the number of patients to follow (due todeath or occurrence of the event of interest, i.e., the diagnosisof the second cancer).
PERSON-YEARS
Person-years at risk. Total number of person-years duringwhich the study population was followed, or was exposed to therisk of developing a second cancer. It is calculated by addingup the time in which each patient was observed. For example,
2
3
4

Guida alla lettura delle schedeI tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI
35 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
5
seguita, ovvero è stata esposta al rischio di sviluppare il se-condo tumore. Si calcola sommando il tempo in cui ognisingolo paziente è stato osservato. Per esempio, se si segue1 paziente per 7 anni e un altro per 5, si ottiene un totaledi 12 anni-persona a rischio, lo stesso valore che si osserve-rebbe seguendo un solo paziente per 12 anni, o tre pazientiper 4 anni e così via.
GLI INDICATORI: SIR ED EAR
SIRSIR (Standardized Incidence Ratio) è il rapporto standardiz-zato di incidenza, dato dal rapporto tra:
Casi osservati (misura reale)
Casi attesi (misura teorica)
doveCasi osservati = è il numero di secondi tumori registrati nellapopolazione in studio (misura reale);Casi attesi = è il numero di secondi tumori che avremmo os-servato nella popolazione in studio se questa avesse sperimen-tato i livelli di incidenza della popolazione generale di parisesso ed età (è una misura di confronto fittizia, teorica).
Come si deve leggere il SIR riportato nelle tabelledi questa monografia?
SIR >1 Se il SIR supera l’unità significa che il rischio di svi-luppare un (secondo) tumore nella popolazione oncologicaè superiore al rischio di sviluppare un (primo) tumore nellapopolazione generale.Per esempio, se vogliamo sapere se i soggetti di sesso ma-schile ammalati di tumore del polmone presentano un ri-schio maggiore di sviluppare un tumore della vescica, an-diamo a leggere la scheda relativa al polmone e, per ilperiodo di follow-up ≥2 mesi, troviamo un SIR =1,56, que-sto dato ci dice che il rischio di questi pazienti supera del56% quello sperimentato dalla popolazione generale.
SIR =1 Se il SIR è pari a 1 significa che il rischio di sviluppareun (secondo) tumore nella popolazione oncologica è ugualeal rischio di sviluppare un (primo) tumore nella popolazionegenerale. Per esempio, se vogliamo sapere se i soggetti di sessomaschile ammalati di tumore del polmone presentano un ri-schio maggiore di sviluppare un tumore del colon retto, an-diamo a leggere la scheda relativa al polmone e, per il periododi follow-up ≥2mesi, troviamo un SIR =0,99 cioè prossimoa uno; questo dato ci dice che l’incidenza osservata in questipazienti è simile a quello della popolazione generale.
SIR <1 Infine, se il SIR è inferiore all’unità significa che ilrischio di sviluppare un (secondo) tumore nella popolazione
if you follow 1 patient for 7 years, and another for 5, you geta total of 12 person-years at risk, the same value that wouldbe observed following a single patient for 12 years, or three pa-tients for 4 years, and so on.
INDICATORS: SIR AND EAR
SIRThe SIR is the Standardized Incidence Ratio; it is calculated as:
Observed Cases (actual measure)
Expected Cases (theoretical measure)
whereObserved Cases = number of second cancers observed in thestudy population (actual measure) andExpected Cases = number of second cancers that would havebeen observed in the study population if it had experienced thelevels of incidence of the general population (without prior di-agnosis of cancer) of the same age and sex. It is a fictional (the-oretical) measure of comparison.
How should the SIR be interpreted in the tablesreported in this monograph?
SIR >1 An SIR value higher than 1 means that the risk of de-veloping a (second) tumour in the cancer population is higherthan the risk of developing a (first) tumour in the general pop-ulation.For example, if we are interested in finding out the excess (orreduced) risk of developing bladder cancer among men withlung cancer, the lung cancer sheet tells us that, for the periodof follow-up ≥2 months, the SIR is 1.56, meaning that the riskamong these patients is 56% higher compared to the generalpopulation.
SIR =1 An SIR value equal to 1means that the risk of developinga (second) tumour in the cancer population is equal to the riskof developing a (first) tumour in the general population.For example, if we are interested in finding out the excess (orreduced) risk of developing colorectal cancer among men withlung cancer, the lung cancer sheet tells us that, for the periodof follow-up ≥2 months, the SIR is 0.99, that is, close to one,meaning that the incidence observed in these patients is similarto that of the general population.
SIR <1 Finally, an SIR value lower than 1means that the riskof developing a (second) tumour in the cancer population islower than the risk of developing a (first) tumour in thegeneral population.It is tricky to interpret this kind of results as a protective effectof a cancer against another cancer. Part of these results couldbe attributed to registration problems. For example, the lower
5

oncologica è inferiore al rischio di sviluppare un (primo) tu-more nella popolazione generale. E’ difficile interpretareeventuali risultati in questa direzione come un effetto pro-tettivo di un tumore nei confronti di un altro tumore.Alcuni di questi risultati potrebbero essere ascrivibili a pro-blemi di registrazione della casistica. Per esempio il piùbasso rischio di tumori del retto in pazienti con una diagnosidi cancro del colon può essere attribuito alla difficoltà di dif-ferenziare tumori multipli da recidive in questi due organi,che sono anatomicamente e istologicamente identici.
Variabilità (gli intervalli di confidenza)Solitamente quando si presenta un indicatore (nel nostrocaso SIR ed EAR) lo si correda anche di un’informazionesul grado di fiducia che abbiamo nella stima prodotta; peravere stime solide occorre esaminare tanti casi, ma non sem-pre questo è possibile. A volte le stime si devono basare for-zatamente su pochi (o pochissimi) casi, il che può portarea risultati piuttosto incerti, che risentono dell’effetto delcaso. Per esempio, nel caso dei tumori della cistifellea suc-cessivi a tumori dell’osso tra gli uomini, il SIR è uguale a3,34 (periodo di follow-up ≥2 mesi): ciò si dovrebbe inter-pretare come “rischio aumentato di oltre 3 volte,” secondola definizione precedente, ma questa stima è basata su 2 solisecondi tumori rilevati tra 1.567 soggetti. Per segnalare que-sto problema, solitamente gli indicatori sono corredati daicosiddetti intervalli di confidenza, un intervallo numericoall’interno del quale è probabile che ricada il valore reale.Quando il dato è basato su un grande numero di soggettistudiati, l’intervallo di confidenza è molto piccolo, quandoil dato è più incerto, l’intervallo di confidenza è più ampio.Nel nostro esempio il SIR 3,34 ha un intervallo di confi-denza amplissimo che va da 0,37 (forte riduzione del ri-schio) a 12,05 (rischio aumentato di 12 volte). Quindi, sea prima vista la stima ci dice che il rischio (di avere un tu-more della cistifellea dopo un tumore dell’osso) è più chetriplicato rispetto alla popolazione generale, l’intervallo diconfidenza ci dice che quella stima va presa con moltacautela, perché, a causa della bassa numerosità del feno-meno, il rischio effettivo può variare in un intervallo moltoampio per il solo effetto del caso.Al fine di produrre tabelle che potessero essere contenute inun’unica scheda e che potessero veicolare rapidamente l’in-formazione, abbiamo deciso di non riportare tutti gli inter-valli di confidenza come consueto, ma di limitarci ai soliSIR, fornendo un’indicazione sintetica, seppur meno esau-stiva, sull’ampiezza dell’intervallo di confidenza: con unascelta arbitraria abbiamo evidenziato in colore le situazioniin cui gli intervalli di confidenza al 95% sono molto piccoli.Tutti i dati relativi agli intervalli di confidenza sono comun-que disponibili sul sito Internet dell’AIRTUM.Nelle schede alcuni SIR sono evidenziati in verde scuro overde chiaro. L’interpretazione è la seguente:
Epidemiol Prev 37 (4-5) Suppl 1:1-152 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.it36
I tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI Guida alla lettura delle schede
risk of rectal cancer in patients with a diagnosis of coloncancer can be attributed to the difficulty of differentiating mul-tiple tumours from relapse in these two organs, which areanatomically and histologically identical.
Variability (confidence intervals)Usually, when indicators are presented (in our case SIRs andEARs), information on the degree of confidence with which weshould accept the estimates is also provided; in order to obtainrobust estimates, it is necessary to examine many cases, but thisis not always possible. Sometimes the estimates need to bebased on a few (or even very few) cases, which can lead to un-certain results, because of the effect of randomness. For example,in the case of gallbladder cancer after bone cancer among men,the SIR is 3.34 (period of follow-up ≥2 months), whichshould be interpreted as “excess risk of more than 3 timescompared to the general population”, according to the previousdefinition – however, this estimate is based on only 2 secondtumours detected among 1,567 subjects. To overcome thisproblem, indicators are presented with their confidence inter-vals, a numeric range within which it is likely that the realvalue falls.When the data is based on many subjects, the confidence in-terval is very small, whereas when the estimate is less “solid”,the confidence interval is wider. In our example, the 3.34 SIRhas a very wide confidence interval, ranging from 0.37 (highlyprotective effect) to 12.05 (12-fold increased risk). Conse-quently, although at first view the estimate shows that the risk(of developing gallbladder cancer after bone cancer) is 3times higher compared to the general population, the confidenceinterval says that the estimate should be taken with caution:due to the low number of subjects, the actual risk may varywidely, as a matter of chance.In order to produce tables that could be contained in a singlepage and quickly disseminate information, we decided not toprovide all the confidence intervals: we reported only the SIRs,along with a brief, and thus perforce less thorough, indicationon the amplitude of the confidence interval, using colour tohighlight SIRs with 95% confidence intervals that do not in-clude 1. All data relating to the confidence intervals are stillavailable on the AIRTUM website. SIRs may be highlightedin dark green or light green. The interpretation is as follows:
■■ SIR IS HIGHLIGHTED IN DARK GREEN: the lower limit ofthe interval (95%) is greater than 1. The SIR is statisti-cally significantly higher.SIR IS NOT HIGHLIGHTED: the lower limit of the interval(95%) is lower than 1 and the upper limit is greater than1. The SIR is not statistically significant.
■■ SIR IS HIGHLIGHTED IN LIGHT GREEN: the upper limit ofthe interval (95%) is lower than 1. The SIR is statisticallysignificantly lower.

Epidemiol Prev 37 (4-5) Suppl 1:1-152 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.it37
I tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI Guida alla lettura delle schede
■■ SIR EVIDENZIATO IN VERDE SCURO: il limite inferioredell’intervallo di confidenza (al 95%) è maggiore di 1.SIR statisticamente significativo in eccesso. E’ verosi-mile che la differenza sia “reale”, non casuale.SIR NON EVIDENZIATO: il limite inferiore dell’intervallodi confidenza (al 95%) è minore di 1 mentre il limitesuperiore è maggiore di 1. SIR non statisticamente si-gnificativo.
■■ SIR EVIDENZIATO IN VERDE CHIARO: il limite superioredell’intervallo di confidenza (al 95%) è minore di 1.SIR statisticamente significativo in difetto.
ATTENZIONE! I SIR sono calcolati su una popolazione spe-cifica, quindi forniscono un’informazione relativa a quelladata popolazione (che avrà una specifica distribuzione peretà e genere eccetera); per questo, quando si confrontanoSIR di popolazioni differenti (come uomini vs. donne, gio-vani vs. anziani) bisogna ricordare che questo indicatore èinfluenzato dalla distribuzione per età o per sede di primotumore, che è diversa, per esempio, nei due sessi.
EAR
EAR (Excess Absolute Risk) è l’eccesso assoluto di rischio disecondo tumore rispetto al valore atteso. E’ dato da:
Casi osservati - Casi attesi
anni-persona a rischio
doveCasi osservati = è il numero di secondi tumori registrati nellapopolazione in studio (misura reale);Casi attesi = è il numero di secondi tumori che avremmo os-servato nella popolazione in studio se questa avesse sperimen-tato i livelli di incidenza della popolazione generale (senza dia-gnosi pregressa di tumore). E’ una misura fittizia, teorica;Anni-persona a rischio = rappresentano il numero totale di anni-persona durante i quali la popolazione in studio è stata seguita,ovvero è stata a rischio di sviluppare il secondo tumore.L’EAR è espresso per 1.000 anni-persona.L’interpretazione è la seguente:VALORI >0 Esprime il numero assoluto di secondi tumoriosservati in eccesso nella popolazione oncologica rispettoalla popolazione generale ogni 1.000 anni-persona. E’ ve-rosimile che la differenza sia “reale”, non casuale.VALORI =0 Il numero assoluto di secondi tumori osservatinella popolazione oncologica è uguale a quello osservatonella popolazione generale.VALORI <0 Esprime il numero assoluto di secondi tumoriosservati in difetto nella popolazione oncologica rispettoalla popolazione generale ogni 1.000 anni/persona. E’ ve-rosimile che la differenza sia “reale”, non casuale.
CAUTION!Wemust keep in mind that SIRs are calculatedon a specific population: they provide information on theexcess (or reduced) risk of developing a second cancer in aspecific population (with a specific distribution by age andgender, etc.). Therefore, when comparing SIRs of differentpopulations (e.g., men vs. women, young vs. old, etc.), wemust keep in mind that these indicators can be influencedby the age-at-first-cancer distribution or by the first-can-cer-site distribution, which are different, for example, in thetwo sexes
EAR
The EAR (Excess Absolute Risk) is the absolute risk of secondcancer compared to the expected value. It is calculated by theformula:
Observed Cases - Expected Cases
Person-years at risk
Observed Cases = number of second cancers observed in thestudy population (actual measure) andExpected Cases = number of second cancers that would havebeen observed in the study population if it had experienced thelevels of incidence of the general population (without prior di-agnosis of cancer) of the same age and sex. It is a fictional (the-oretical) measure of comparison.Person-years at risk = the total number of person-years duringwhich the study population was followed (i.e., was at risk ofdeveloping a second cancer). The EAR is expressed per 1,000person-years.The interpretation is as follows:VALUE >0The absolute number of excess (second) cancers ob-served in the study population compared to the general popu-lation per 1,000 person-years.VALUE =0 The absolute number of (second) cancers observedin the study population is equal to the number of (first)cancers observed in the general population.VALUE <0The absolute number of fewer (second) cancers ob-served in the study population compared to the general popu-lation per 1,000 person-years.
In the site-specific pages, a number of EARs are highlighted indark green or light green.The interpretation is as follows:■■ EAR HIGHLIGHTED IN DARK GREEN: the 95% confidence
interval does not include 0, the lower limit is >0. TheEAR is statistically significantly higher.EAR NOT HIGHLIGHTED: the 95% confidence interval in-cludes 0. The EAR is not statistically significant.
■■ EAR HIGHLIGHTED IN LIGHT GREEN: the 95% confidenceinterval does not include 0, the upper limit is <0. TheEAR is statistically significantly lower.

Guida alla lettura delle schedeI tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI
38 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
Nelle schede alcuni EAR sono evidenziati in verde scuro overde chiaro. L’interpretazione è la seguente:
■■ EAR EVIDENZIATO IN VERDE SCURO: l’intervallo di con-fidenza al 95% non contiene 0, il limite inferiore è >0.EAR statisticamente significativo in eccesso.EAR NON EVIDENZIATO: l’intervallo di confidenza al95% contiene 0. EAR non statisticamente significativo.
■■ EAR EVIDENZIATO INVERDE CHIARO: l’intervallo di con-fidenza al 95% non contiene 0, il superiore <0. EARstatisticamente significativo in difetto.
COME LEGGERE LA SCHEDA «TUTTI I TUMORI»
Si noti che nella scheda ALL SITES BUT SKIN il numero di se-condi tumori osservati in una macrosede (per esempio:COLON RECTUM) è diverso dalla somma dei casi osservatinelle sue sottosedi (per esempio: COLON e RECTUM). Ciò èdeterminato dalla scelta di calcolare l’incidenza dei seconditumori escludendo i casi osservati e attesi nella medesimasede del primo tumore, in accordo con le raccomandazioniIARC/IACR per la definizione dei tumori multipli cheimpediscono l’inserimento di più tumori nella stessa sedeanatomica, a meno che non appartengano a gruppi morfo-logici differenti, solitamente poco frequenti.Di conseguenza:■ se analizziamo i secondi tumori del colon retto (successivia un primo tumore qualunque) escludiamo i secondi tu-mori della macrosede colon retto;
■ se analizziamo i secondi tumori del colon (successivi a unprimo tumore qualunque) escludiamo i soli secondi tu-mori della sede colon;
■ se analizziamo i secondi tumori del retto (successivi a unprimo tumore qualunque) escludiamo i soli secondi tu-mori della sede retto.
HOWTO READ THE «ALL SITES BUT SKIN» DATA SHEET
In this data sheet, the number of second primaries observed in amacro-site (e.g., COLON RECTUM) is different from the sum of thecases observed in its two sub-sites (e.g., COLON and RECTUM).This is due to the method employed: as stated in the chapter«Material and methods», the incidence of second cancers wascalculated excluding the observed and expected cases in thesame site as the first cancer, as recommended by theIARC/IACR rules for the definition of multiple primaries.
As a consequence:■ When we analyze second colorectal cancer (subsequent to
any first cancer) we exclude the second colorectal cancer.■ When we analyze any second colon cancer (subsequent to
any first cancer) we exclude the second colon cancer only.■ When we analyze the second rectal cancer (subsequent to
any first cancer) we exclude the second rectal cancer only.
COLON RECTUM ≠ COLON + RECTUM

RISULTATISCHEDE SPECIFICHE PER TUMORE
RESULTSCANCER-SPECIFIC DATA SHEETS

� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECO
NDCANCERSITE
757446
8803
6188
0361
7574
4651
8850
1971
2565
829
7574
4688
0361
2651889
2787
669
1357
8051
5386
1279
790
6050
0325
1709
2651
889
2787
669
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
EAR
EAR
5451
81.0
864
648
1.2
310
130
4.0
899
081.0
725
357
1.0
713
261
1.1
159
921.1
51.6
14.2
7
2379
1.1
925
971.2
321
81.9
944
31.
0912
001.2
253
81.2
119
81.
140.1
50.1
9
759
1.5
185
81.6
399
3.7
715
01.5
237
31.5
416
71.4
769
1.4
80.1
00.1
2
659
1.4
972
81.5
669
2.9
312
61.4
233
11.5
315
01.5
252
1.31
0.0
80.0
9
1399
1.2
216
761.3
827
74.3
823
61.
0171
21.2
732
61.2
912
51.2
80.1
00.1
7
871
1.5
211
391.8
926
89.0
815
11.3
740
91.4
823
21.7
679
1.4
40.1
10.1
9
3182
0.97
3422
0.99
240
1.4
450
50.8
215
390.
9881
11.
0532
71.
04-0
.04
-0.0
1
6722
1.0
375
161.1
079
42.4
510
980.9
232
391.0
516
761.0
870
91.0
80.
100.2
9
4901
1.0
358
851.1
898
44.2
377
70.9
023
901.0
611
941.
0454
01.
090.
060.3
5
2275
1.00
2528
1.0
525
32.2
141
30.
9711
021.
0154
31.
0021
70.
960.
000.
05
1901
0.8
622
090.9
630
82.8
731
50.7
782
50.7
852
91.
0223
21.
05-0
.11
-0.0
4
559
0.9
159
80.
9339
1.30
940.
8426
90.
9313
80.
9358
0.91
-0.0
2-0
.02
1533
1.01
1620
1.02
871.
1928
61.
0468
80.
9537
51.
0318
41.1
60.
000.
01
1110
11.2
213
033
1.3
719
324.6
816
631.
0351
951.1
829
361.3
513
071.4
50.8
21.3
7
900
1.2
198
41.2
684
2.4
214
91.
1240
91.1
724
01.3
310
21.2
80.0
60.0
8
292
1.00
329
1.08
372.7
040
0.77
154
1.11
721.
0326
0.86
0.00
0.01
173
1.4
619
91.6
026
4.3
539
1.7
684
1.4
936
1.30
141.
170.0
20.0
3
229
1.2
025
11.2
622
2.3
739
1.12
101
1.12
711.5
618
0.91
0.01
0.0
2
541.
1060
1.16
62.
329
0.94
261.
1013
1.16
61.
300.
000.
00
134
1.13
150
1.2
116
2.7
423
1.05
631.
1237
1.31
110.
910.
010.
01
8587
1.0
610
059
1.1
814
723.6
018
751.2
936
030.
9920
631.
0310
461.
030.2
30.7
0
691.
1292
1.4
323
7.5
412
1.02
371.
2614
1.00
60.
990.
000.0
1
2087
1.2
827
801.6
269
38.6
266
52.1
983
91.0
739
81.
0318
51.
130.1
80.4
0
5950
1.1
581
171.4
921
677.8
911
481.1
529
521.1
912
531.
0559
71.2
20.3
51.1
4
5798
1.1
779
121.5
121
148.0
011
341.1
828
921.2
112
001.
0457
21.2
10.3
71.1
3
254
0.93
326
1.1
472
5.3
936
0.73
108
0.84
731.
1137
1.29
-0.0
10.
01
522
0.8
554
60.8
524
0.78
910.7
823
20.7
912
80.
9071
1.20
-0.0
3-0
.04
371
1.5
947
31.9
310
29.0
585
1.9
517
51.5
666
1.21
451.9
20.0
50.0
8
109
1.03
146
1.3
237
6.7
225
1.21
440.
8629
1.21
111.
110.
000.0
1
1541
1.02
1771
1.1
223
03.1
127
30.
9874
31.
0334
90.
9817
61.
150.
010.0
7
657
0.8
971
80.
9361
1.6
811
50.
8530
90.8
916
50.
9468
0.90
-0.0
3-0
.02
1373
1.0
915
611.1
818
82.9
622
30.
9566
21.1
134
81.1
714
01.
100.0
40.0
9
530
0.8
868
01.
0815
04.8
799
0.87
237
0.8
313
80.
9856
0.95
-0.0
30.
02
761
1.3
179
41.3
033
1.16
110
1.04
381
1.3
919
51.4
075
1.25
0.0
70.0
7
870.
9495
0.98
81.
6214
0.78
471.
0717
0.79
91.
000.
000.
00
2219
0.7
825
830.8
736
42.6
335
90.7
010
360.7
755
60.8
126
80.
90-0
.24
-0.1
5
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
40 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
TUTTIITUMORIESCLUSA
CUTE
POOLAIRTUM1976-2010,UOMINI:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
ALLSITESBUTSKIN
POOLAIRTUM1976-2010,MEN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
FIRSTCANCERSITE
ALLSITESBUTSKIN
MEN
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECO
NDCANCERSITE
757446
8803
6188
0361
7574
4651
8850
1971
2565
829
7574
4688
0361
2651889
2787
669
1357
8051
5386
1279
790
6050
0325
1709
2651
889
2787
669
ALLSITES,BUTSKINANDSITE
OFFIRSTCANCER
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
PROSTATE
TESTIS
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
EAR
EAR

EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
EAR
EAR
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECO
NDCANCERSITE
41 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
ALLSITESBUTSKIN
POOLAIRTUM1976-2010,WOMEN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
TUTTIITUMORIESCLUSA
CUTE
POOLAIRTUM1976-2010,DONNE:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRSTCANCERSITE
ALLSITESBUTSKIN
WOMEN
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
EAR
EAR
668179
7546
9975
4699
6681
7950
6027
2367
5896
800
6681
7975
4699
3073635
3191
669
1180
3447
8050
1384
163
7910
3642
0386
3073
635
3191
669
ALLSITES,BUTSKINANDSITE
OFFIRSTCANCER
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
CERVIXUTERI
CORPUSUTERI
OVARY
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECO
NDCANCERSITE
3088
11.1
235
558
1.2
446
774.3
243
761.0
513
172
1.1
182
791.1
450
541.1
91.0
82.1
7
476
1.1
750
81.2
032
2.1
058
0.97
208
1.1
813
91.2
971
1.13
0.0
20.0
3
260
1.1
927
91.2
319
2.3
232
1.01
110
1.18
741.
2744
1.25
0.01
0.0
2
130
1.4
114
31.5
013
3.7
713
0.94
571.4
043
1.7
817
1.27
0.0
10.0
1
134
1.3
515
71.5
223
6.1
320
1.34
641.4
835
1.34
151.
010.0
10.0
2
216
1.4
125
81.6
242
6.9
929
1.28
991.5
148
1.19
401.6
50.0
20.0
3
1807
1.03
1924
1.0
611
71.6
520
70.7
781
11.
0747
71.
0431
21.1
90.
020.
03
4581
1.1
251
581.2
157
73.6
660
71.
0219
571.1
212
411.1
377
61.1
70.1
80.3
2
3418
1.1
040
051.2
458
74.9
446
01.
0214
581.1
192
01.1
158
01.1
50.1
10.2
7
1423
1.0
816
051.1
818
23.5
620
21.
0362
81.1
136
01.
0323
31.1
50.0
40.0
8
713
0.8
780
30.
9490
2.8
483
0.6
829
50.8
421
10.
9712
40.
94-0
.04
-0.0
2
505
0.7
756
20.8
257
2.1
753
0.5
322
30.7
913
20.7
697
0.95
-0.0
5-0
.04
1365
1.0
914
051.0
940
0.87
159
0.89
552
1.05
392
1.1
726
21.2
50.0
40.0
4
2689
1.3
731
211.5
443
26.2
532
51.1
811
521.3
873
31.3
847
91.4
70.2
40.3
5
708
1.2
079
41.3
086
4.0
281
0.94
321
1.2
520
11.2
910
51.
180.0
40.0
6
851.
0196
1.10
113.6
710
0.84
401.
1215
0.66
201.
410.
000.
00
431.
0353
1.22
105.9
39
1.43
170.
9611
1.00
60.
890.
000.
00
208
1.5
722
71.6
519
3.8
027
1.37
771.3
460
1.7
144
2.1
50.0
20.0
3
501.3
854
1.4
34
2.77
81.
4214
0.88
161.
6912
2.2
90.
000.
01
5446
1.1
362
351.2
478
93.6
583
31.
0423
421.1
114
551.2
081
61.1
90.3
50.6
4
401
0.95
499
1.1
398
5.6
583
1.20
174
0.90
100
0.94
440.
82-0
.01
0.02
1991
1.4
427
121.8
972
113.6
721
41.
0287
11.4
357
41.5
933
21.6
70.2
10.4
3
1218
1.2
313
851.3
516
74.4
521
91.4
751
21.1
828
81.
1119
91.3
70.0
80.1
2
1050
1.4
113
931.8
034
312.5
530
02.8
038
41.2
123
21.1
613
41.
120.1
00.2
0
1436
1.2
716
231.3
818
74.2
822
91.3
861
11.2
736
01.1
923
61.2
90.1
00.1
5
1374
1.3
015
501.4
117
64.3
222
21.4
358
61.3
134
41.2
222
21.3
00.1
10.1
5
800.
9696
1.11
165.0
213
1.08
300.
8522
0.98
151.
080.
000.
00
380
0.8
240
00.8
420
1.17
440.6
515
40.7
711
30.
9369
0.98
-0.0
3-0
.02
828
1.3
990
71.4
779
3.7
812
31.4
137
71.4
322
41.4
210
41.
200.0
80.1
0
961.
2111
61.4
020
6.2
917
1.33
441.
2222
1.10
131.
230.
010.0
1
1146
1.01
1299
1.1
015
33.5
816
10.
9644
20.9
033
71.
1120
61.
150.
000.0
4
480
0.8
952
90.
9549
2.3
778
0.98
193
0.8
411
80.8
391
1.07
-0.0
2-0
.01
895
1.1
896
11.2
266
2.2
189
0.7
842
51.3
026
21.3
111
91.
010.0
50.0
6
289
0.8
633
90.
9750
3.7
037
0.7
212
90.
8983
0.94
400.
79-0
.02
0.00
541
1.4
755
61.4
615
1.07
470.
8726
51.6
916
21.6
667
1.15
0.0
60.0
6
681.
0571
1.05
31.
116
0.60
321.
1518
1.06
121.
200.
000.
00
1731
0.7
91977
0.8
7246
2.9
4257
0.8
071
50.7
745
90.7
930
00.8
4-0
.15
-0.1
0

EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
HEADANDNECK
POOLAIRTUM1976-2010,MEN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
TESTAECO
LLO
POOLAIRTUM1976-2010,UOMINI:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRSTCANCERSITE
HEADANDNECK
MEN
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
42 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
ALLSITES,BUTSKINANDHEADANDNECK
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
PROSTATE
TESTIS
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
42368
4528
445
284
4236
832
693
1408
355
9342
368
4528
4
186565
1938
3572
7031
178
8464
446
742
2400
118
6565
9383
5
5513
1.6
262
621.7
874
96.6
265
91.3
525
241.7
514
811.6
184
91.5
111.2
814.1
4
480
2.9
671
94.2
823
938.9
576
2.8
823
43.2
111
72.8
453
2.4
61.7
02.8
4
221
5.8
628
47.2
663
44.4
939
6.4
110
26.0
552
5.3
928
5.5
00.9
81.2
6
155
4.4
217
24.7
317
12.6
522
3.8
174
4.6
539
4.4
120
4.4
40.6
40.7
0
104
1.16
263
2.8
415
947.0
815
1.04
581.4
526
1.14
50.4
20.
080.8
8
333
8.3
347
711.5
214
499.9
448
7.7
716
19.1
896
9.2
328
4.7
81.5
72.2
5
295
1.3
830
91.4
014
1.8
530
0.93
134
1.4
670
1.24
611.8
50.4
40.4
5
510
1.06
527
1.06
171.
0855
0.81
228
1.13
151
1.16
760.
940.
160.
16
338
1.03
347
1.03
90.
8536
0.79
144
1.06
108
1.21
500.
890.
060.
05
172
1.13
180
1.14
81.
5519
0.85
841.2
943
1.05
261.
060.
100.
11
231
1.6
025
81.7
227
5.5
534
1.6
210
51.7
059
1.5
233
1.42
0.4
60.5
6
391.
0740
1.07
10.
843
0.58
150.
9913
1.32
81.
290.
010.
01
116
1.2
211
91.2
13
0.95
201.
4750
1.25
261.
0120
1.27
0.11
0.11
2065
3.2
024
203.6
335
515.8
424
52.5
499
73.5
954
33.1
928
02.8
07.6
19.0
4
410.
8242
0.81
10.
606
0.83
100.4
715
1.11
101.
23-0
.05
-0.0
5
110.
5812
0.61
11.
640
0.00
70.
882
0.39
20.
62-0
.04
-0.0
4
70.
968
1.06
13.
941
0.92
41.
281
0.52
10.
870.
000.
00
60.
496
0.48
00.
000
0.00
30.
582
0.62
10.
52-0
.03
-0.0
3
30.
924
1.18
18.
180
0.00
32.
080
0.00
00.
000.
000.
00
60.
806
0.77
00.
001
0.91
41.
250
0.00
10.
82-0
.01
-0.0
1
582
0.8
660
20.8
720
0.98
570.6
523
60.8
617
50.
9311
40.
93-0
.50
-0.4
8
51.
236
1.41
15.
651
1.33
42.
070
0.00
00.
000.
000.
01
124
1.09
142
1.2
118
4.7
219
1.15
491.
0131
1.02
251.
390.
060.
13
627
1.5
966
21.6
335
2.6
569
1.22
281
1.6
917
91.6
998
1.5
31.2
51.3
2
610
1.6
264
21.6
532
2.5
368
1.25
277
1.7
416
81.6
697
1.5
81.2
51.3
0
171.
0120
1.15
35.4
11
0.42
40.
5711
2.4
21
0.35
0.00
0.01
330.
7934
0.78
10.
671
0.1
615
0.82
70.
6410
1.60
-0.0
5-0
.05
261.5
879
4.6
453
91.7
213
5.1
810
1.39
10.
232
0.83
0.05
0.3
2
60.
818
1.04
26.
850
0.00
61.
790
0.00
00.
00-0
.01
0.00
125
1.2
413
91.3
314
4.1
116
1.09
571.3
232
1.19
201.
240.
130.1
8
320.7
033
0.7
01
0.65
50.
7611
0.57
110.
895
0.66
-0.0
7-0
.07
941.
1910
21.2
58
2.9
614
1.21
361.
0725
1.18
191.
500.
080.
10
240.6
232
0.80
86.0
15
0.88
60.3
69
0.88
40.
67-0
.08
-0.0
4
641.8
264
1.7
60
0.00
91.
7825
1.6
916
1.69
142.3
90.1
50.1
4
61.
136
1.09
00.
000
0.00
52.
190
0.00
11.
230.
000.
00
196
1.10
227
1.2
331
5.1
721
0.82
981.3
142
0.88
351.
180.
100.2
2
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECO
NDCANCERSITE
42368
4528
445
284
4236
832
693
1408
355
9342
368
4528
4
186565
1938
3572
7031
178
8464
446
742
2400
118
6565
1938
35
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
EAR
EAR

EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
43 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
HEADANDNECK
POOLAIRTUM1976-2010,WOMEN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
TESTAECO
LLO
POOLAIRTUM1976-2010,DONNE:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
ALLSITES,BUTSKINANDHEADANDNECK
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
CERVIXUTERI
CORPUSUTERI
OVARY
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
FIRSTCANCERSITE
HEADANDNECK
WOMEN
628
1.5
871
81.7
390
5.6
985
1.3
130
61.7
515
51.5
182
1.4
66.1
17.7
7
7714.7
010
419.1
027
129.3
410
11.5
933
14.2
526
19.4
48
11.0
81.9
12.5
2
4616.5
558
20.0
812
109.0
95
11.1
219
15.7
018
25.0
94
9.9
61.1
51.4
1
1815.3
718
14.7
70
0.00
210.0
48
15.1
16
20.4
12
13.4
50.4
50.4
3
1310.1
028
20.9
215
293.5
73
14.0
36
10.4
22
6.13
211.6
60.3
10.6
8
3819.4
448
23.6
110
126.8
71
3.14
2327.1
612
23.8
12
7.00
0.9
61.1
8
271.
1630
1.24
33.
064
1.03
111.
098
1.35
41.
230.
100.
15
741.
2178
1.22
41.
6512
1.21
311.
1619
1.19
121.
340.
340.
36
430.
9846
1.00
31.
738
1.13
140.
7314
1.22
71.
08-0
.03
0.00
311.7
932
1.7
81
1.44
41.
4117
2.2
45
1.12
52.
050.3
60.3
6
141.
3414
1.29
00.
001
0.60
61.
337
2.5
80
0.00
0.09
0.08
50.
605
0.57
00.
001
0.73
20.
552
0.93
00.
00-0
.09
-0.0
9
140.
8814
0.85
00.
002
0.80
60.
893
0.72
31.
23-0
.05
-0.0
6
165
6.5
119
27.3
027
28.0
315
3.7
691
8.2
938
5.7
421
5.5
83.7
24.2
4
40.
536
0.77
26.
901
0.82
20.
601
0.52
00.
00-0
.09
-0.0
5
10.
921
0.89
00.
000
0.00
12.
130
0.00
00.
000.
000.
00
23.
832
3.67
00.
000
0.00
28.
900
0.00
00.
000.
040.
04
74.1
98
4.6
01
15.2
21
3.67
56.7
90
0.00
14.
260.
140.1
6
24.
432
4.25
00.
001
13.1
50
0.00
00.
001
16.7
00.
040.
04
125
1.20
145
1.3
320
4.8
323
1.33
561.
2036
1.36
100.
720.
550.9
3
132.4
014
2.4
81
4.29
11.
038
3.2
02
1.53
23.
180.
200.
21
201.
0620
1.02
00.
003
0.96
50.
595
1.04
72.8
30.
030.
01
80.
639
0.68
11.
951
0.47
20.
351
0.31
42.
36-0
.13
-0.1
1
101.
0412
1.20
25.
450
0.00
61.
433
1.19
10.
710.
010.
05
171.
1317
1.09
00.
002
0.83
101.
544
1.02
10.
450.
050.
04
171.
2217
1.17
00.
002
0.90
101.
664
1.10
10.
490.
080.
06
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.03
-0.0
3
30.
524
0.66
14.
401
1.06
10.
390
0.00
11.
24-0
.07
-0.0
5
121.
5921
2.6
89
30.8
06
4.8
03
0.88
10.
522
2.07
0.12
0.3
4
11.
011
0.97
00.
000
0.00
12.
220
0.00
00.
000.
000.
00
201.
3423
1.48
35.1
74
1.66
111.
684
1.04
10.
470.
140.
19
60.
876
0.84
00.
001
0.90
20.
671
0.56
22.
02-0
.02
-0.0
3
121.
2312
1.19
00.
000
0.00
51.
185
1.99
21.
440.
060.
05
40.
934
0.89
00.
000
0.00
10.
533
2.71
00.
00-0
.01
-0.0
1
71.
527
1.46
00.
000
0.00
31.
502
1.67
22.
980.
060.
06
11.
251
1.20
00.
000
0.00
12.
900
0.00
00.
000.
010.
00
280.
9734
1.13
65.1
64
0.86
161.
293
0.40
51.
16-0
.02
0.10
8984
9611
9611
8984
6713
2850
1082
8984
9611
37525
3907
115
4764
8617
114
9281
4643
3752
539
071
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
EAR
EAR
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECO
NDCANCERSITE

EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
44 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
ORALCAVITY
POOLAIRTUM1976-2010,MEN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
CAVITÀORALE
POOLAIRTUM1976-2010,UOMINI:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRSTCANCERSITE
ORA
LCAVITY
MEN
ALLSITES,BUTSKINANDORA
LCAVITY
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
PROSTATE
TESTIS
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
10051
1083
310
833
1005
170
8225
1385
010
051
1083
3
34592
3632
517
3371
0016
359
7892
3241
3459
236
325
1151
1.9
314
062.2
525
59.4
717
21.5
757
22.1
429
11.9
711
61.6
216.0
321.5
4
174
6.1
726
18.8
287
62.2
629
5.0
892
6.9
242
6.4
811
4.0
44.2
16.3
7
365.3
847
6.6
911
33.3
46
4.4
515
4.7
711
7.1
14
6.1
30.8
51.1
0
6510.3
278
11.8
013
41.8
013
10.1
736
12.0
211
7.6
35
8.5
91.7
01.9
7
734.8
013
68.5
263
83.2
910
3.2
441
5.7
320
5.7
32
1.35
1.6
73.3
0
113
16.3
014
620.1
033
99.4
318
13.3
358
18.0
828
17.0
19
12.3
63.0
73.8
2
491.3
855
1.4
86
3.5
08
1.17
281.7
58
0.93
51.
230.
390.
49
861.
0691
1.08
51.
3914
0.96
411.
1421
1.03
101.
000.
150.
18
551.
0057
0.99
20.
8310
1.02
210.
8616
1.15
81.
150.
00-0
.02
311.
2034
1.26
32.
554
0.84
201.7
35
0.79
20.
650.
150.
19
512.0
958
2.2
77
6.3
46
1.33
221.9
913
2.1
610
3.4
90.7
70.8
9
81.
328
1.26
00.
002
1.81
51.
871
0.66
00.
000.
060.
05
221.
3622
1.30
00.
008
2.7
110
1.39
30.
751
0.51
0.17
0.14
339
3.1
642
33.7
684
16.6
947
2.3
018
43.7
684
3.2
424
1.9
76.7
08.5
5
80.
898
0.85
00.
003
1.84
10.
254
1.79
00.
00-0
.03
-0.0
4
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.09
-0.0
9
10.
792
1.51
116
.73
00.
001
1.74
00.
000
0.00
-0.0
10.
02
31.
413
1.35
00.
000
0.00
22.
080
0.00
14.
020.
030.
02
23.
523
5.0
31
35.4
20
0.00
27.
630
0.00
00.
000.
040.
07
10.
771
0.74
00.
000
0.00
11.
720
0.00
00.
00-0
.01
-0.0
1
970.
8510
30.
876
1.28
80.4
241
0.83
321.
0716
1.05
-0.4
9-0
.43
11.
141
1.08
00.
000
0.00
12.
350
0.00
00.
000.
000.
00
241.
2326
1.28
22.
283
0.84
111.
246
1.25
41.
780.
130.
15
102
1.5
510
91.5
97
2.34
131.
0738
1.29
362.2
215
1.8
91.0
51.1
1
991.5
810
31.5
74
1.40
121.
0338
1.35
342.1
915
1.9
81.0
51.0
3
31.
066
2.04
323.4
81
1.94
00.
002
2.86
00.
000.
010.
08
40.
555
0.66
12.
930
0.00
30.
900
0.00
11.
26-0
.09
-0.0
7
92.9
416
5.0
07
50.5
14
6.9
64
2.83
00.
001
3.06
0.17
0.3
5
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.04
-0.0
4
261.
4930
1.6
54
5.0
75
1.55
131.
656
1.40
20.
990.
250.
33
60.
786
0.74
00.
000
0.00
20.
582
1.04
22.
15-0
.05
-0.0
6
181.
3420
1.43
23.
215
1.99
61.
006
1.83
10.
630.
130.
16
30.
465
0.73
26.
541
0.81
10.
341
0.63
00.
00-0
.10
-0.0
5
152.5
215
2.4
10
0.00
43.
645
1.89
53.3
91
1.36
0.2
60.
24
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.03
-0.0
3
431.4
356
1.7
813
9.4
25
0.90
211.
5710
1.35
71.
900.
370.6
8
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECO
NDCANCERSITE
10051
1083
310
833
1005
170
8225
1385
010
051
1083
3
34592
3632
517
3371
0016
359
7892
3241
3459
236
325
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
EAR
EAR

ORALCAVITY
POOLAIRTUM1976-2010,WOMEN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
CAVITÀORALE
POOLAIRTUM1976-2010,DONNE:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRSTCANCERSITE
ORA
LCAVITY
WOMEN
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
45 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
ALLSITES,BUTSKINANDORA
LCAVITY
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
CERVIXUTERI
CORPUSUTERI
OVARY
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
286
1.4
833
11.6
445
5.1
851
1.4
514
21.6
267
1.4
126
1.17
5.4
07.1
7
4919.8
558
22.4
79
80.3
95
11.0
021
18.6
218
29.7
65
17.7
52.6
93.0
6
2921.5
133
23.4
14
65.1
03
12.1
710
16.4
513
38.9
73
18.7
41.6
01.7
5
1120.7
011
19.8
00
0.00
00.
006
24.2
94
31.1
91
17.6
10.6
10.5
8
915.2
614
22.7
25
189.6
12
18.3
75
18.3
21
6.99
115
.43
0.4
90.7
4
2323.6
729
28.5
36
133.5
91
5.61
1534.3
67
29.1
00
0.00
1.2
71.5
5
60.
517
0.57
11.
771
0.45
20.
383
1.04
00.
00-0
.33
-0.3
0
300.
9931
0.98
10.
733
0.55
161.
188
1.06
30.
84-0
.01
-0.0
3
180.
8319
0.84
11.
022
0.51
70.
727
1.29
20.
77-0
.21
-0.2
0
121.
4212
1.36
00.
001
0.65
92.3
51
0.48
11.
030.
210.
18
30.
583
0.55
00.
001
1.05
20.
850
0.00
00.
00-0
.13
-0.1
4
30.
713
0.68
00.
001
1.27
10.
531
0.96
00.
00-0
.07
-0.0
8
50.
635
0.60
00.
002
1.41
20.
571
0.50
00.
00-0
.17
-0.1
8
574.7
066
5.2
19
17.0
28
3.7
234
6.2
212
3.9
33
2.05
2.5
92.9
5
20.
573
0.82
16.
580
0.00
21.
250
0.00
00.
00-0
.09
-0.0
4
11.
971
1.89
00.
000
0.00
14.
360
0.00
00.
000.
030.
03
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.02
-0.0
2
67.5
56
7.2
30
0.00
16.
924
11.0
60
0.00
110
.85
0.3
00.2
9
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.01
-0.0
1
601.
2470
1.3
910
4.6
516
1.8
024
1.08
151.
275
0.93
0.68
1.08
41.
625
1.93
18.
450
0.00
21.
711
1.74
14.
170.
090.
13
121.
3912
1.33
00.
002
1.26
10.
254
1.91
55.3
40.
200.
17
30.
504
0.64
13.
701
0.90
10.
361
0.69
00.
00-0
.17
-0.1
2
51.
096
1.25
15.
010
0.00
41.
931
0.87
00.
000.
020.
07
40.
544
0.52
00.
000
0.00
30.
901
0.54
00.
00-0
.20
-0.2
1
40.
584
0.56
00.
000
0.00
30.
971
0.58
00.
00-0
.17
-0.1
8
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.03
-0.0
3
10.
372
0.70
18.
221
2.01
00.
000
0.00
00.
00-0
.10
-0.0
5
51.
479
2.5
34
27.3
34
6.4
61
0.63
00.
000
0.00
0.09
0.30
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.03
-0.0
3
131.
8314
1.8
81
3.16
32.
335
1.54
42.
271
1.22
0.34
0.36
41.
194
1.14
00.
001
1.64
10.
660
0.00
25.
100.
040.
03
40.
834
0.79
00.
000
0.00
20.
922
1.68
00.
00-0
.05
-0.0
6
10.
471
0.45
00.
000
0.00
11.
040
0.00
00.
00-0
.07
-0.0
7
31.
323
1.27
00.
000
0.00
10.
982
3.54
00.
000.
040.
03
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.02
-0.0
2
151.
0318
1.18
34.
453
1.13
81.
231
0.27
31.
670.
020.
15
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
EAR
EAR
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECO
NDCANCERSITE
4608
4899
4899
4608
3312
1306
459
4608
4899
17303
1809
679
232
7580
9741
3217
9917
303
1809
6

PHARYNX
POOLAIRTUM1976-2010,MEN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
FARINGE
POOLAIRTUM1976-2010,UOMINI:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRSTCANCERSITE
PHARYNX
MEN
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
46 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
ALLSITES,BUTSKINANDPHARYNX
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
PROSTATE
TESTIS
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
937
2.1
312
962.8
035
915.2
615
41.6
747
92.3
722
02.2
384
1.7
817.5
527.7
9
934.1
423
39.8
014
0106.7
215
2.9
153
4.9
117
3.6
78
4.2
32.4
96.9
8
5610.4
910
117.8
945
146.0
59
7.4
133
12.8
810
9.0
44
8.7
81.7
93.1
8
61.
166
1.10
00.
001
0.84
31.
201
0.95
12.
380.
030.
02
312.5
912
69.9
695
135.3
55
1.82
172.9
76
2.44
32.
960.6
73.7
8
9618.0
516
930.0
773
240.8
718
15.1
849
19.5
023
20.4
76
12.1
33.2
05.4
5
401.5
943
1.6
13
2.06
61.
0717
1.46
91.
658
3.1
40.
520.
55
831.4
190
1.4
57
2.25
131.
0736
1.33
241.7
910
1.54
0.8
50.9
3
561.4
059
1.4
03
1.44
80.
9824
1.32
192.0
85
1.11
0.56
0.56
271.
4231
1.5
54
3.8
95
1.25
121.
375
1.18
52.
510.
280.
37
412.2
554
2.8
113
13.2
910
2.6
121
2.4
86
1.49
42.
090.8
01.1
6
20.
472
0.45
00.
000
0.00
10.
521
1.05
00.
00-0
.08
-0.0
8
191.
6119
1.53
00.
003
1.22
91.
673
1.14
43.
110.
250.
22
318
3.9
939
54.6
977
17.2
351
2.9
317
54.7
170
4.0
622
2.7
78.4
110.3
7
50.
716
0.81
12.
771
0.69
20.
610
0.00
22.
72-0
.07
-0.0
5
20.
802
0.76
00.
000
0.00
21.
740
0.00
00.
00-0
.02
-0.0
2
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.03
-0.0
3
21.
242
1.18
00.
000
0.00
11.
331
2.82
00.
000.
010.
01
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.02
-0.0
2
11.
041
0.99
00.
000
0.00
12.
250
0.00
00.
000.
000.
00
770.
9381
0.93
41.
0016
1.01
300.
8125
1.26
60.
59-0
.21
-0.2
0
11.
341
1.26
00.
000
0.00
12.
700
0.00
00.
000.
010.
01
151.
0024
1.52
911.3
84
1.28
60.
863
0.90
21.
290.
000.
27
601.
2664
1.27
41.
557
0.70
321.
4616
1.50
50.
980.
430.
46
581.
2762
1.29
41.
627
0.73
321.5
214
1.37
51.
030.
430.
46
20.
992
0.94
00.
000
0.00
00.
002
4.46
00.
000.
000.
00
50.
885
0.84
00.
001
0.81
00.
003
2.45
11.
86-0
.02
-0.0
3
41.
5813
4.8
89
68.6
63
5.6
81
0.84
00.
000
0.00
0.05
0.3
5
21.
822
1.72
00.
000
0.00
23.
800
0.00
00.
000.
030.
03
141.
0620
1.44
68.5
31
0.36
101.
640
0.00
32.
210.
030.
20
40.
725
0.85
13.
321
0.85
10.
392
1.60
00.
00-0
.06
-0.0
3
191.9
721
2.0
62
3.75
31.
458
1.80
52.
353
2.97
0.33
0.36
40.
846
1.19
27.
531
0.97
10.
452
1.91
00.
00-0
.03
0.03
143.2
814
3.1
10
0.00
22.
226
3.0
83
3.15
36.4
50.3
40.3
2
11.
701
1.60
00.
000
0.00
13.
710
0.00
00.
000.
010.
01
401.8
750
2.2
210
8.5
32
0.44
242.4
613
2.7
41
0.43
0.6
60.9
2
9448
1041
310
413
9448
6320
1928
608
9448
1041
3
28320
2996
216
4265
2513
706
5771
2318
2832
029
962
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECO
NDCANCERSITE
9448
1041
310
413
9448
6320
1928
608
9448
1041
3
28320
2996
216
4265
2513
706
5771
2318
2832
029
962
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
EAR
EAR

PHARYNX
POOLAIRTUM1976-2010,WOMEN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
FARINGE
POOLAIRTUM1976-2010,DONNE:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRSTCANCERSITE
PHARYNX
WOMEN
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
47 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
ALLSITES,BUTSKINANDPHARYNX
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
CERVIXUTERI
CORPUSUTERI
OVARY
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
157
1.9
920
12.4
544
12.8
024
1.7
886
2.5
131
1.5
816
1.41
9.1
313.2
6
1514.0
532
28.7
217
364.7
43
16.2
86
12.8
25
18.9
81
6.59
1.6
33.4
5
1120.4
918
32.1
47
302.0
82
22.2
35
21.6
24
29.5
90
0.00
1.2
21.9
5
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.03
-0.0
3
414.9
914
50.3
210
875.8
21
21.7
91
8.45
115
.23
127
.09
0.44
1.5
3
925.5
811
29.9
32
126.9
20
0.00
746.8
72
22.4
50
0.00
1.0
11.1
9
102.5
311
2.6
51
5.25
22.
875
2.95
11.
012
3.51
0.71
0.77
100.
8912
1.02
24.
064
2.12
20.
423
1.04
10.
59-0
.15
0.03
70.
879
1.07
25.
723
2.25
00.
003
1.46
10.
82-0
.12
0.07
30.
933
0.89
00.
001
1.82
21.
430
0.00
00.
00-0
.03
-0.0
4
52.
755
2.64
00.
000
0.00
22.
603
6.4
10
0.00
0.37
0.35
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.17
-0.1
7
20.
732
0.70
00.
000
0.00
21.
740
0.00
00.
00-0
.09
-0.1
0
357.2
344
8.7
39
44.7
14
5.0
624
11.6
36
4.8
61
1.33
3.5
24.3
5
00.
001
0.59
114
.48
00.
000
0.00
00.
000
0.00
-0.1
9-0
.08
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.03
-0.0
2
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.01
-0.0
1
12.
972
5.70
168
.70
00.
001
6.78
00.
000
0.00
0.08
0.18
110
.93
110
.46
00.
000
0.00
00.
000
0.00
180.9
00.
110.
10
261.
1531
1.32
55.1
15
1.27
131.
306
1.09
20.
650.
400.
83
65.0
06
4.7
70
0.00
14.
345
9.0
90
0.00
00.
000.
560.
53
40.
994
0.95
00.
001
1.43
10.
560
0.00
23.
670.
00-0
.02
31.
153
1.10
00.
000
0.00
00.
000
0.00
38.4
40.
040.
03
42.
135
2.55
112
.80
00.
001
1.24
24.
191
3.48
0.25
0.34
72.5
87
2.48
00.
001
2.23
43.
472
2.88
00.
000.
500.
47
72.7
77
2.6
60
0.00
12.
394
3.7
22
3.09
00.
000.
520.
49
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.02
-0.0
2
10.
861
0.83
00.
000
0.00
11.
970
0.00
00.
00-0
.02
-0.0
2
52.
716
3.1
21
13.1
12
6.32
11.
210
0.00
28.
030.
370.
46
14.
451
4.26
00.
000
0.00
19.
900
0.00
00.
000.
090.
09
31.
035
1.64
216.1
20
0.00
32.
380
0.00
00.
000.
010.
22
10.
791
0.76
00.
000
0.00
11.
840
0.00
00.
00-0
.03
-0.0
4
21.
142
1.09
00.
000
0.00
22.
640
0.00
00.
000.
030.
02
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.09
-0.0
9
22.
342
2.24
00.
000
0.00
25.
460
0.00
00.
000.
130.
12
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.02
-0.0
2
61.
218
1.54
28.
891
1.19
41.
901
0.79
00.
000.
120.
31
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
EAR
EAR
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECO
NDCANCERSITE
2221
2423
2423
2221
1596
622
245
2221
2423
8572
8958
386
1568
3875
2037
1092
8572
8958

LARYNX
POOLAIRTUM1976-2010,MEN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
LARINGE
POOLAIRTUM1976-2010,UOMINI:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
FIRSTCANCERSITE
LARYNX
MEN
48 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
ALLSITES,BUTSKINANDLARYNX
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
PROSTATE
TESTIS
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
3863
1.5
742
251.6
736
25.4
640
21.3
316
891.6
710
751.5
469
71.5
411.3
513.3
2
213
1.9
122
51.9
612
3.5
032
2.0
789
1.8
258
1.9
334
2.0
10.8
20.8
6
129
5.0
313
65.1
57
9.0
024
6.8
254
4.8
431
4.4
420
5.0
20.8
40.8
6
843.5
688
3.6
24
5.4
78
2.4
235
3.3
627
4.2
514
4.0
00.4
90.5
0
00.0
01
0.0
21
0.52
00.0
00
0.0
00
0.0
00
0.0
0-0
.50
-0.4
9
124
4.4
716
25.6
838
47.1
512
3.2
954
4.5
745
5.9
013
2.8
10.7
81.0
5
206
1.3
521
11.3
45
1.14
160.
8189
1.3
953
1.25
481.8
20.4
30.4
2
341
1.00
346
0.99
50.
5628
0.6
815
11.
0910
61.
0956
0.87
0.01
-0.0
2
227
0.98
231
0.97
40.
6618
0.66
991.
0673
1.10
370.
83-0
.04
-0.0
5
114
1.06
115
1.04
10.
3410
0.74
521.
1633
1.08
190.
980.
050.
03
139
1.3
614
61.3
97
2.5
118
1.42
621.4
740
1.39
191.
030.3
00.3
2
291.
1130
1.12
11.
441
0.32
90.
8511
1.49
81.
610.
020.
03
751.
1278
1.13
31.
679
1.10
311.
1320
1.05
151.
200.
060.
07
1408
3.0
816
023.4
119
415.0
214
72.5
163
83.3
338
93.0
623
42.9
37.6
98.8
7
280.
8228
0.80
00.
002
0.48
70.
5011
1.14
81.
26-0
.05
-0.0
5
90.
6810
0.74
12.
940
0.00
50.
942
0.53
20.
79-0
.03
-0.0
3
61.
186
1.15
00.
001
1.55
31.
421
0.71
11.
090.
010.
01
10.1
21
0.1
20
0.00
00.
000
0.00
10.
420
0.00
-0.0
6-0
.06
10.
441
0.43
00.
000
0.00
11.
030
0.00
00.
00-0
.01
-0.0
1
40.
764
0.74
00.
001
1.53
20.
920
0.00
11.
04-0
.01
-0.0
1
408
0.8
541
80.8
510
0.86
330.6
216
50.
8811
80.
8592
0.95
-0.5
7-0
.56
31.
224
1.57
111
.62
12.
602
1.77
00.
000
0.00
0.00
0.01
851.
0792
1.13
73.2
612
1.23
320.
9822
0.99
191.
330.
050.
08
465
1.6
648
91.7
024
3.1
549
1.4
221
11.8
312
71.6
178
1.5
21.5
01.5
8
453
1.6
947
71.7
324
3.2
949
1.4
820
71.8
812
01.5
977
1.5
71.5
01.5
8
121.
0012
0.98
00.
000
0.00
40.
827
2.06
10.
440.
000.
00
240.
8224
0.80
00.
000
0.0
012
0.97
40.
508
1.63
-0.0
4-0
.05
131.
2050
4.4
737
120.0
66
4.2
65
1.09
10.
331
0.54
0.02
0.3
0
40.
816
1.17
212.6
30
0.00
41.
830
0.00
00.
00-0
.01
0.01
851.
2189
1.23
42.
0910
1.15
341.
1726
1.32
151.
180.
120.
13
220.
6822
0.66
00.
004
1.01
80.
607
0.76
30.
50-0
.08
-0.0
9
571.
0261
1.06
42.
586
0.86
220.
9514
0.89
151.
490.
010.
03
170.
6321
0.75
45.2
73
0.87
40.3
56
0.79
40.
84-0
.08
-0.0
5
351.
4035
1.37
00.
003
0.98
141.
388
1.13
102.1
40.
080.
07
51.
305
1.26
00.
000
0.00
42.
470
0.00
11.
540.
010.
01
113
0.89
121
0.93
82.3
314
0.90
531.
0219
0.5
327
1.14
-0.1
1-0
.07
22869
2403
824
038
2286
919
291
9642
4135
2286
924
038
123654
1275
4838
9517
553
5458
033
079
1844
112
3654
1275
48
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECO
NDCANCERSITE
22869
2403
824
038
2286
919
291
9642
4135
2286
924
038
123654
1275
4838
9517
553
5458
033
079
1844
112
3654
1275
48
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
EAR
EAR

LARYNX
POOLAIRTUM1976-2010,WOMEN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
LARINGE
POOLAIRTUM1976-2010,DONNE:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRSTCANCERSITE
LARYNX
WOMEN
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
49 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
ALLSITES,BUTSKINANDLARYNX
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
CERVIXUTERI
CORPUSUTERI
OVARY
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
233
1.7
925
71.9
124
6.3
217
1.00
101
1.8
470
1.9
545
1.9
78.8
010.2
1
137.6
414
8.0
01
19.9
22
8.9
46
8.3
43
6.4
02
6.94
0.9
71.0
2
66.7
17
7.6
11
39.3
90
0.00
410.7
81
4.02
16.
210.
440.5
1
718.6
17
18.0
60
0.00
238.8
52
12.1
92
19.4
11
17.3
80.5
70.5
5
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.04
-0.0
4
69.5
18
12.3
22
110.1
70
0.00
13.
833
17.2
02
17.2
80.4
60.6
1
111.
4712
1.56
14.
481
1.02
41.
294
1.96
21.
500.
300.
36
341.7
035
1.7
01
1.76
51.
9713
1.58
81.
448
2.19
1.20
1.20
181.
2618
1.22
00.
003
1.66
71.
194
1.00
41.
500.
310.
27
162.8
317
2.9
31
6.09
22.
736
2.55
42.
564
4.0
10.8
90.9
3
61.
756
1.70
00.
000
0.00
21.
434
4.2
10
0.00
0.22
0.21
20.
742
0.72
00.
000
0.00
10.
891
1.34
00.
00-0
.06
-0.0
7
71.
367
1.32
00.
000
0.00
20.
962
1.39
33.
000.
160.
14
738.7
182
9.5
29
38.6
03
2.87
339.5
820
8.5
517
10.9
55.5
56.1
1
20.
852
0.82
00.
001
3.22
00.
001
1.53
00.
00-0
.03
-0.0
4
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.03
-0.0
3
211.9
42
11.6
10
0.00
00.
002
29.0
30
0.00
00.
000.
160.
15
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.05
-0.0
5
16.
881
6.68
00.
001
50.6
20
0.00
00.
000
0.00
0.07
0.07
391.
1644
1.27
54.9
72
0.44
191.
3115
1.63
30.
550.
460.
78
31.
723
1.67
00.
000
0.00
11.
281
2.20
14.
030.
110.
10
40.
644
0.62
00.
000
0.00
31.
111
0.59
00.
00-0
.19
-0.2
0
20.
482
0.47
00.
000
0.00
10.
560
0.00
11.
47-0
.19
-0.1
9
10.
311
0.30
00.
000
0.00
10.
760
0.00
00.
00-0
.19
-0.1
9
61.
226
1.19
00.
001
1.63
31.
491
0.73
11.
100.
090.
08
61.
326
1.28
00.
001
1.75
31.
611
0.79
11.
180.
120.
11
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.03
-0.0
3
10.
521
0.51
00.
000
0.00
00.
000
0.00
13.
01-0
.08
-0.0
8
20.
876
2.54
457.4
40
0.00
10.
991
1.59
00.
00-0
.02
0.30
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.03
-0.0
3
40.
824
0.79
00.
001
1.60
31.
470
0.00
00.
00-0
.08
-0.0
9
10.
441
0.43
00.
000
0.00
00.
001
1.59
00.
00-0
.11
-0.1
1
61.
906
1.85
00.
000
0.00
10.
773
3.44
23.
520.
240.
23
32.
143
2.08
00.
000
0.00
00.
003
7.7
40
0.00
0.14
0.13
21.
342
1.30
00.
000
0.00
00.
000
0.00
27.
290.
040.
04
13.
951
3.83
00.
000
0.00
19.
640
0.00
00.
000.
060.
06
70.
768
0.84
13.
800
0.00
41.
061
0.39
21.
15-0
.19
-0.1
2
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
EAR
EAR
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECO
NDCANCERSITE
2155
2289
2289
2155
1805
922
378
2155
2289
11649
1201
736
816
4451
4231
1217
5211
649
1201
7

OESOPHAGUS
POOLAIRTUM1976-2010,MEN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
ESOFAGO
POOLAIRTUM1976-2010,UOMINI:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRSTCANCERSITE
OESOPHAGUS
MEN
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
50 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
ALLSITES,BUTSKINANDOESOPHAGUS
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
PROSTATE
TESTIS
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
7598
9562
9562
7598
2977
479
150
7598
9562
10533
1196
314
3140
5545
1114
2853
910
533
1196
3
290
1.4
541
11.8
112
14.4
582
1.11
146
1.7
747
1.5
515
1.13
8.5
015.3
3
768.1
996
9.0
920
15.5
816
4.4
744
11.1
211
8.6
65
10.6
16.3
37.1
4
3114.1
634
13.6
63
10.0
48
9.5
518
19.2
64
13.1
91
8.78
2.7
42.6
3
2713.1
336
15.4
29
32.4
17
8.8
813
14.6
44
14.2
63
30.1
32.3
72.8
1
183.5
826
4.5
38
11.3
11
0.51
136.1
03
4.37
13.
881.2
31.6
9
10.
421
0.37
00.
001
1.11
00.
000
0.00
00.
00-0
.13
-0.1
4
121.
0022
1.6
010
5.5
65
1.07
51.
042
1.17
00.
000.
000.
69
230.
8530
0.97
71.
917
0.70
110.
995
1.20
00.
00-0
.39
-0.0
7
160.
8623
1.09
72.8
15
0.74
70.
924
1.39
00.
00-0
.24
0.16
70.
827
0.72
00.
002
0.63
41.
141
0.78
00.
00-0
.15
-0.2
3
121.
4519
2.0
37
6.3
35
1.64
41.
161
0.80
23.
800.
360.
81
31.
463
1.28
00.
002
2.62
11.
210
0.00
00.
000.
090.
06
50.
9210
1.62
56.7
34
1.99
10.
450
0.00
00.
00-0
.04
0.32
742.0
412
83.1
054
10.6
918
1.32
412.7
413
2.4
52
0.89
3.5
97.2
5
20.
692
0.62
00.
000
0.00
21.
640
0.00
00.
00-0
.08
-0.1
0
21.
792
1.59
00.
000
0.00
12.
121
5.70
00.
000.
080.
06
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.04
-0.0
4
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.07
-0.0
7
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.02
-0.0
2
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.04
-0.0
4
280.
7232
0.73
40.
816
0.4
414
0.87
50.
783
1.06
-1.0
5-1
.01
14.
311
3.79
00.
000
0.00
00.
000
0.00
199.0
50.
070.
06
60.
9312
1.64
67.1
02
0.85
31.
111
1.03
00.
00-0
.04
0.39
231.
0523
0.92
00.
009
1.10
111.
222
0.61
10.
680.
10-0
.17
200.
9520
0.84
00.
008
1.02
91.
052
0.63
10.
71-0
.09
-0.3
2
33.
093
2.71
00.
001
2.76
25.
070
0.00
00.
000.
190.
16
31.
273
1.12
00.
000
0.00
22.
021
2.91
00.
000.
060.
03
11.
062
1.88
18.
631
2.95
00.
000
0.00
00.
000.
010.
08
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.04
-0.0
4
20.
352
0.31
00.
000
0.00
10.
420
0.00
12.
67-0
.36
-0.3
8
10.
381
0.34
00.
001
1.03
00.
000
0.00
00.
00-0
.15
-0.1
6
20.
443
0.58
11.
571
0.59
00.
001
1.51
00.
00-0
.24
-0.1
8
10.
451
0.40
00.
001
1.19
00.
000
0.00
00.
00-0
.11
-0.1
3
10.
502
0.88
13.
600
0.00
00.
001
3.30
00.
00-0
.09
-0.0
2
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.03
-0.0
3
141.
3920
1.7
46
4.2
25
1.32
51.
234
2.65
00.
000.
370.
71
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECO
NDCANCERSITE
7598
9562
9562
7598
2977
479
150
7598
9562
10533
1196
314
3140
5545
1114
2853
910
533
1196
3
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
EAR
EAR

OESOPHAGUS
POOLAIRTUM1976-2010,WOMEN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
ESOFAGO
POOLAIRTUM1976-2010,DONNE:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRSTCANCERSITE
OESOPHAGUS
WOMEN
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
51 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
581.4
177
1.6
519
3.4
521
1.43
221.
2711
1.70
41.
494.
847.7
5
916.8
611
18.2
62
29.0
74
21.4
42
8.80
335.2
50
0.00
2.4
42.6
6
26.
992
6.16
00.
001
9.88
18.
370
0.00
00.
000.
490.
43
325.7
94
30.6
21
69.8
11
24.9
81
19.6
41
54.2
70
0.00
0.83
0.99
430.5
35
33.9
31
61.2
22
44.0
80
0.00
297.1
30
0.00
1.11
1.2
4
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.06
-0.0
6
20.
793
1.02
12.
481
1.01
10.
970
0.00
00.
00-0
.16
0.01
101.
5510
1.36
00.
004
1.71
20.
753
2.97
12.
321.
020.
68
71.
517
1.32
00.
003
1.78
10.
522
2.74
13.
190.
680.
44
31.
663
1.46
00.
001
1.52
11.
331
3.57
00.
000.
340.
24
21.
793
2.36
16.
400
0.00
12.
161
5.81
00.
000.
260.
44
11.
121
0.97
00.
001
2.94
00.
000
0.00
00.
000.
03-0
.01
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.49
-0.4
9
83.0
316
5.3
78
23.7
22
2.20
54.4
71
2.34
00.
001.
543.3
3
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.21
-0.2
1
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.03
-0.0
3
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.02
-0.0
2
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.05
-0.0
5
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.01
-0.0
1
90.
8711
0.95
21.
583
0.85
51.
121
0.60
00.
00-0
.37
-0.1
4
35.7
64
6.7
81
14.3
62
10.5
70
0.00
113
.21
00.
000.
710.
87
21.
072
0.95
00.
000
0.00
00.
001
3.33
18.
200.
04-0
.03
10.
791
0.70
00.
000
0.00
00.
000
0.00
112
.47
-0.0
8-0
.11
22.
003
2.66
17.
950
0.00
24.
710
0.00
00.
000.
290.
48
10.
631
0.55
00.
001
1.74
00.
000
0.00
00.
00-0
.17
-0.2
1
10.
681
0.60
00.
001
1.88
00.
000
0.00
00.
00-0
.14
-0.1
7
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.03
-0.0
3
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.17
-0.1
7
11.
512
2.72
113
.90
14.
700
0.00
00.
000
0.00
0.10
0.32
110
.86
19.
590
0.00
00.
001
25.1
30
0.00
00.
000.
260.
23
21.
302
1.15
00.
000
0.00
11.
520
0.00
19.
690.
130.
07
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.21
-0.2
1
32.
944
3.42
16.
822
5.27
12.
370
0.00
00.
000.
570.
72
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.13
-0.1
3
36.2
54
7.3
11
15.0
02
11.4
91
5.03
00.
000
0.00
0.73
0.88
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.02
-0.0
3
10.
332
0.57
12.
200
0.00
10.
810
0.00
00.
00-0
.59
-0.3
8
ALLSITES,BUTSKINANDOESOPHAGUS
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
CERVIXUTERI
CORPUSUTERI
OVARY
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
2291
2954
2954
2291
920
168
6422
9129
54
3471
3908
438
1213
1511
540
208
3471
3908
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
EAR
EAR
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECO
NDCANCERSITE

STOMACH
POOLAIRTUM1976-2010,MEN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
STOMACO
POOLAIRTUM1976-2010,UOMINI:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRSTCANCERSITE
STOMACH
MEN
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
52 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
2291
0.97
3144
1.2
585
35.2
635
80.7
110
591.
0555
81.
0431
61.
00-0
.61
5.0
9
950.
9612
51.
1830
4.2
316
0.72
380.
8728
1.32
131.
12-0
.03
0.16
170.
7428
1.14
116.8
12
0.39
70.
707
1.40
10.
36-0
.05
0.03
221.
1026
1.21
42.
836
1.33
70.
798
1.86
10.
420.
020.
04
561.
0071
1.19
153.6
98
0.63
240.
9713
1.09
111.
710.
000.
09
381.4
478
2.7
740
20.9
77
1.19
181.
588
1.39
51.
530.
100.4
1
20.0
118
0.1
016
1.23
20.0
50
0.0
00
0.0
00
0.0
0-1
.46
-1.3
4
356
1.02
586
1.5
723
09.5
854
0.7
317
31.1
781
1.01
481.
000.
061.7
4
232
0.97
413
1.6
218
111.1
630
0.6
011
51.
1452
0.94
351.
05-0
.06
1.2
9
124
1.12
173
1.4
649
6.2
924
1.00
581.
2329
1.16
130.
900.
120.4
5
670.6
911
61.
1249
7.3
912
0.58
350.
8411
0.5
09
0.70
-0.2
60.
10
301.
0836
1.21
63.0
55
0.84
151.
286
0.95
41.
060.
020.
05
108
1.5
812
11.6
613
2.7
512
0.83
531.8
330
1.9
213
1.39
0.3
50.3
9
393
0.8
951
81.
0912
53.9
858
0.6
017
00.
8910
11.
0364
1.14
-0.4
40.
36
381.
1742
1.22
41.
9810
1.54
120.
8811
1.45
51.
060.
050.
06
70.
579
0.69
22.
560
0.00
10.
192
0.70
42.
27-0
.05
-0.0
3
20.
393
0.55
12.
740
0.00
20.
920
0.00
00.
00-0
.03
-0.0
2
111.
3012
1.33
11.
741
0.56
61.
674
2.07
00.
000.
020.
02
31.
343
1.24
00.
000
0.00
22.
040
0.00
13.
720.
010.
00
91.
699
1.58
00.
002
1.77
41.
782
1.65
11.
390.
030.
03
438
0.9
052
11.
0083
2.6
057
0.5
820
41.
0012
11.
0656
0.80
-0.4
30.
02
62.
427
2.6
41
5.74
23.
543
2.69
11.
900
0.00
0.03
0.04
710.
9413
81.7
167
13.3
315
0.95
361.
1114
0.81
60.
59-0
.04
0.4
7
331
1.1
738
61.2
855
2.8
160
1.00
160
1.3
360
0.94
511.3
60.4
30.6
9
320
1.1
937
21.2
952
2.7
759
1.02
154
1.3
458
0.95
491.3
70.4
50.6
9
110.
8814
1.04
33.
461
0.38
61.
132
0.69
21.
16-0
.01
0.00
190.
7020
0.69
10.
544
0.69
70.
606
0.99
20.
58-0
.07
-0.0
7
111.
1312
1.16
11.
620
0.00
81.
903
1.35
00.
000.
010.
01
00.0
04
0.80
411.6
80
0.00
00.
000
0.00
00.
00-0
.04
-0.0
1
721.
0513
81.8
866
14.2
413
0.90
341.
1615
0.95
101.
080.
030.5
3
310.
9236
1.00
52.
106
0.83
100.
7011
1.43
40.
88-0
.02
0.00
751.2
810
71.7
032
7.5
811
0.86
331.
3223
1.7
38
1.04
0.14
0.3
6
270.
9747
1.5
720
9.9
75
0.82
100.
849
1.43
30.
84-0
.01
0.14
411.5
652
1.8
511
5.9
45
0.89
181.
6214
2.3
34
1.13
0.13
0.2
0
71.
548
1.63
12.
761
0.95
52.
580
0.00
11.
830.
020.
03
800.6
011
70.8
237
3.9
213
0.4
635
0.6
220
0.65
120.
65-0
.47
-0.2
2
ALLSITES,BUTSKINANDSTOMACH
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
PROSTATE
TESTIS
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
42022
5369
753
697
4202
223
028
7538
3090
4202
253
697
114047
1219
8479
3725
320
5020
924
897
1362
111
4047
1219
84
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECO
NDCANCERSITE
42022
5369
753
697
4202
223
028
7538
3090
4202
253
697
114047
1219
8479
3725
320
5020
924
897
1362
111
4047
1219
84
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
EAR
EAR

STOMACH
POOLAIRTUM1976-2010,WOMEN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
STOMACO
POOLAIRTUM1976-2010,DONNE:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRSTCANCERSITE
STOMACH
WOMEN
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
53 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
ALLSITES,BUTSKINANDSTOMACH
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
CERVIXUTERI
CORPUSUTERI
OVARY
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
1044
0.9
414
781.2
543
46.3
517
70.8
246
20.
9926
10.
97144
0.89
-0.7
62.9
8
151.
0318
1.17
33.
363
1.06
60.
983
0.86
31.
430.
010.
03
70.
858
0.92
12.
002
1.28
30.
882
1.00
00.
00-0
.01
-0.0
1
51.
716
1.93
15.
500
0.00
32.
390
0.00
25.
100.
020.
03
30.
884
1.11
14.
761
1.48
00.
001
1.25
12.
140.
000.
00
71.
0816
2.3
29
21.3
31
0.78
62.
230
0.00
00.
000.
010.
09
50.0
615
0.1
610
1.64
30.1
61
0.0
31
0.0
50
0.0
0-0
.88
-0.7
9
210
1.06
341
1.6
213
110.5
125
0.6
510
61.2
862
1.28
170.5
80.
121.3
1
160
1.12
264
1.7
410
411.6
318
0.65
861.4
543
1.23
130.
610.
181.1
3
500.
9077
1.3
127
7.6
67
0.64
200.
8619
1.42
40.
51-0
.06
0.18
160.4
725
0.70
94.2
54
0.61
70.
503
0.37
20.
40-0
.19
-0.1
1
210.
7331
1.01
105.3
43
0.53
80.
677
1.01
30.
72-0
.08
0.00
851.6
192
1.6
57
2.17
90.
9141
1.9
121
1.61
141.
700.3
50.3
6
570.7
674
0.94
173.8
73
0.2
123
0.75
150.
8216
1.40
-0.1
9-0
.05
130.
6715
0.73
21.
771
0.27
80.
983
0.64
10.
35-0
.07
-0.0
6
20.
693
0.98
16.
050
0.00
00.
001
1.40
12.
19-0
.01
0.00
10.
582
1.08
18.
980
0.00
11.
400
0.00
00.
00-0
.01
0.00
51.
046
1.18
13.
452
2.17
10.
502
1.72
00.
000.
000.
01
10.
751
0.70
00.
000
0.00
11.
760
0.00
00.
000.
000.
00
254
0.94
332
1.1
678
4.8
158
1.11
970.
8560
0.93
391.
02-0
.17
0.46
140.
9715
0.98
11.
044
1.31
60.
954
1.23
00.
000.
000.
00
480.
9954
1.05
62.
054
0.42
271.
308
0.70
91.
370.
000.
03
441.
2460
1.5
916
7.3
16
0.86
221.
469
1.06
71.
410.
090.2
3
260.
9363
2.1
237
22.4
38
1.52
90.
775
0.73
40.
95-0
.02
0.3
4
511.
0561
1.19
103.3
415
1.62
160.
8013
1.10
70.
960.
030.
10
491.
0957
1.20
82.8
814
1.63
160.
8612
1.09
71.
040.
040.
09
20.
564
1.06
29.3
51
1.52
00.
001
1.13
00.
00-0
.02
0.00
110.
6713
0.75
22.
050
0.00
50.
734
1.01
20.
84-0
.06
-0.0
4
161.
0318
1.10
22.
312
0.68
91.
355
1.34
00.
000.
010.
02
10.
391
0.36
00.
000
0.00
10.
890
0.00
00.
00-0
.02
-0.0
2
360.
8376
1.6
540
15.3
38
0.96
180.
997
0.66
30.
47-0
.08
0.3
0
140.
6525
1.09
118.1
64
0.95
50.
552
0.38
30.
96-0
.08
0.02
300.
9445
1.33
157.4
25
0.80
181.
364
0.52
30.
65-0
.02
0.11
90.
6422
1.46
1314.2
52
0.71
50.
851
0.29
10.
50-0
.06
0.07
201.
3721
1.35
11.
103
1.07
121.9
83
0.84
20.
920.
060.
06
10.
332
0.61
14.
920
0.00
10.
790
0.00
00.
00-0
.02
-0.0
1
660.6
791
0.86
254.0
012
0.63
210.5
223
0.94
100.
66-0
.35
-0.1
4
30778
3918
739
187
3077
817
318
6467
2768
3077
839
187
93325
9911
857
9318
776
4028
021
886
1238
393
325
9911
8
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
EAR
EAR
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECO
NDCANCERSITE

COLONRECTUM
POOLAIRTUM1976-2010,MEN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
COLONRETTO
POOLAIRTUM1976-2010,UOMINI:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRSTCANCERSITE
COLONRECTUM
MEN
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
54 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
101421
1148
2711
4827
1014
2176
634
2910
610
289
1014
2111
4827
393779
4116
7517
896
7290
419
0769
9101
339
093
3937
7941
1675
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECO
NDCANCERSITE
101421
1148
2711
4827
1014
2176
634
2910
610
289
1014
2111
4827
393779
4116
7517
896
7290
419
0769
9101
339
093
3937
7941
1675
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
EAR
EAR
ALLSITES,BUTSKINANDCO
LONRECTUM
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
PROSTATE
TESTIS
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
7069
0.9
082
871.
0112
183.6
510
810.8
032
060.8
718
700.
9791
21.
02-2
.02
0.21
285
0.8
329
90.8
414
0.90
410.6
514
90.
9068
0.86
270.
81-0
.14
-0.1
4
680.
8572
0.86
41.
1115
1.02
340.
8814
0.75
50.
62-0
.03
-0.0
3
520.7
557
0.78
51.
577
0.54
300.
8812
0.76
30.
45-0
.04
-0.0
4
165
0.86
170
0.8
55
0.57
190.5
385
0.91
420.
9519
1.02
-0.0
7-0
.08
820.
8998
1.02
163.9
217
1.03
360.
8221
0.97
80.
82-0
.03
0.00
501
0.8
854
40.9
143
1.7
057
0.5
723
70.
8814
41.
0563
1.00
-0.1
8-0
.13
468
0.3
793
60.7
146
88.8
796
0.4
526
20.4
462
0.2
048
0.3
2-2
.03
-0.9
3
240
0.2
763
70.7
039
711.0
444
0.3
012
60.3
137
0.1
733
0.3
2-1
.61
-0.6
6
228
0.5
829
90.7
371
4.2
352
0.77
136
0.7
425
0.2
615
0.3
4-0
.42
-0.2
7
264
0.7
435
50.
9591
5.9
446
0.7
410
40.6
176
0.88
380.
96-0
.24
-0.0
4
800.7
986
0.82
61.
418
0.4
732
0.6
829
1.16
110.
92-0
.05
-0.0
5
189
0.7
620
00.7
711
1.06
370.
8871
0.6
152
0.85
291.
00-0
.15
-0.1
4
1348
0.8
615
300.9
318
22.6
619
70.7
160
40.8
137
91.
0016
80.
98-0
.58
-0.2
8
138
1.15
153
1.2
215
3.0
819
0.95
641.
1436
1.21
191.
330.
050.
07
370.
8041
0.85
42.
125
0.64
210.
979
0.79
20.
37-0
.02
-0.0
2
201.
0622
1.12
22.
432
0.61
101.
136
1.33
20.
920.
000.
01
240.
7931
0.97
75.4
43
0.57
110.
778
1.07
20.
57-0
.02
0.00
40.
524
0.50
00.
000
0.00
10.
272
1.11
11.
26-0
.01
-0.0
1
170.
8820
1.00
33.
693
0.91
70.
775
1.06
20.
90-0
.01
0.00
1712
0.9
419
421.
0223
03.1
325
00.8
374
80.8
848
61.
0622
81.
06-0
.28
0.11
111.
3713
1.55
25.
291
0.65
61.
533
1.67
11.
340.
010.
01
358
1.3
159
12.0
723
320.3
610
12.1
616
21.2
563
0.94
321.
040.2
10.7
4
1013
0.99
1216
1.1
420
34.6
814
60.8
349
71.
0423
40.
9413
61.
17-0
.02
0.3
7
965
0.99
1159
1.1
419
44.6
714
40.
8647
61.
0422
20.
9312
31.
11-0
.03
0.3
5
481.
0757
1.22
94.8
12
0.2
721
1.00
121.
0813
2.4
10.
010.
02
670.6
971
0.7
04
0.95
120.
6922
0.4
716
0.69
171.
65-0
.08
-0.0
7
601.6
766
1.7
66
3.9
112
1.89
331.9
211
1.29
41.
060.0
60.0
7
120.
7616
0.96
45.4
84
1.35
30.
395
1.37
00.
00-0
.01
0.00
218
0.8
726
21.
0144
4.1
937
0.87
960.8
254
0.89
311.
09-0
.08
0.00
970.8
010
20.8
15
0.97
170.
8242
0.74
280.
9410
0.71
-0.0
6-0
.06
199
0.95
232
1.06
333.6
527
0.75
981.
0049
0.96
251.
05-0
.03
0.03
890.
9011
91.
1530
6.9
411
0.63
390.
8327
1.13
121.
09-0
.03
0.04
991.
0410
21.
033
0.75
130.
8152
1.18
210.
9013
1.17
0.01
0.01
110.
7111
0.68
00.
003
1.09
70.
961
0.27
00.
00-0
.01
-0.0
1
333
0.6
839
30.7
860
2.9
539
0.4
815
20.6
786
0.7
256
0.96
-0.3
9-0
.27

COLONRECTUM
POOLAIRTUM1976-2010,WOMEN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
COLONRETTO
POOLAIRTUM1976-2010,DONNE:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRSTCANCERSITE
COLONRECTUM
WOMEN
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
55 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
4125
1.0
447
801.1
565
54.0
961
90.
9618
591.
0410
681.
0557
91.
070.
381.6
3
560.
9657
0.93
10.
425
0.53
281.
0616
1.08
70.
88-0
.01
-0.0
1
300.
9131
0.91
10.
772
0.39
130.
909
1.06
61.
28-0
.01
-0.0
1
110.
9211
0.88
00.
002
0.99
61.
093
1.02
00.
000.
000.
00
151.
0815
1.04
00.
001
0.43
91.
424
1.16
10.
560.
000.
00
210.
8522
0.86
11.
013
0.77
121.
104
0.63
20.
57-0
.01
-0.0
1
311
1.00
336
1.04
251.9
031
0.6
114
41.
0475
0.95
611.4
40.
000.
03
288
0.3
749
40.6
220
66.7
162
0.5
114
20.4
242
0.2
142
0.3
9-1
.28
-0.7
8
125
0.2
328
80.5
016
37.4
030
0.3
456
0.2
323
0.1
616
0.2
0-1
.14
-0.7
4
163
0.7
620
60.
9343
4.9
532
0.93
860.
9019
0.3
526
0.90
-0.1
3-0
.04
900.6
711
10.7
921
3.8
99
0.4
237
0.6
229
0.84
150.
79-0
.12
-0.0
7
610.5
675
0.6
614
3.1
17
0.4
029
0.6
010
0.3
615
0.97
-0.1
3-0
.10
181
0.88
187
0.87
60.
7523
0.73
790.
8852
0.96
270.
87-0
.07
-0.0
7
413
1.3
746
01.4
747
4.0
446
0.98
192
1.4
411
51.4
760
1.3
80.3
00.3
7
901.
1410
51.2
815
4.8
314
1.10
330.
9231
1.5
412
1.13
0.03
0.06
80.
6511
0.86
36.4
61
0.53
40.
741
0.31
21.
12-0
.01
0.00
81.
159
1.25
13.
550
0.00
41.
324
2.24
00.
000.
000.
00
170.
8920
1.01
33.
967
2.29
30.
355
1.03
20.
75-0
.01
0.00
40.
775
0.93
14.
551
1.15
10.
432
1.54
00.
000.
000.
00
1218
1.1
014
051.2
218
74.1
820
31.
1155
21.0
931
41.1
314
91.
040.3
00.
65
621.
1181
1.3
919
7.6
78
0.80
331.
2615
1.13
60.
950.
020.
06
267
1.3
331
41.5
147
5.7
128
0.83
119
1.2
976
1.5
344
1.7
70.1
80.2
7
192
1.3
521
51.4
523
3.9
648
2.0
510
81.6
823
0.6
513
0.71
0.1
30.1
7
146
1.2
926
22.2
211
626.4
533
1.8
568
1.3
532
1.09
130.
810.0
90.3
7
235
1.2
428
31.4
448
6.4
346
1.5
594
1.13
551.
1240
1.4
70.1
20.2
2
214
1.2
225
91.4
245
6.4
944
1.6
084
1.09
511.
1235
1.39
0.1
00.2
0
211.
5224
1.6
83
5.6
72
0.96
101.
684
1.11
52.
380.
020.
02
550.
8257
0.82
20.
753
0.2
826
0.87
160.
9510
1.11
-0.0
3-0
.03
911.3
495
1.3
44
1.47
110.
9646
1.4
623
1.37
111.
330.
060.
06
101.
0011
1.06
12.
312
1.15
40.
862
0.83
21.
700.
000.
00
163
0.93
182
1.00
192.7
526
0.93
630.
8052
1.17
220.
92-0
.03
0.00
690.
8172
0.81
30.
8813
0.96
230.6
117
0.78
161.
36-0
.04
-0.0
4
113
0.92
127
1.00
142.8
29
0.4
658
1.07
290.
9217
0.99
-0.0
30.
00
460.
8556
0.99
104.4
84
0.45
220.
9112
0.87
81.
09-0
.02
0.00
540.
9457
0.96
31.
325
0.55
301.
1912
0.81
70.
86-0
.01
-0.0
1
131.
1614
1.20
12.
160
0.00
61.
225
1.71
21.
240.
000.
01
244
0.6
427
80.7
034
2.2
642
0.7
199
0.6
070
0.7
133
0.5
9-0
.36
-0.3
0
ALLSITES,BUTSKINANDCO
LONRECTUM
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
CERVIXUTERI
CORPUSUTERI
OVARY
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
89720
1014
5210
1452
8972
067
604
2801
711
076
8972
010
1452
375841
3916
6415
823
6437
017
3550
9207
945
842
3758
4139
1664
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
EAR
EAR
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECO
NDCANCERSITE

COLO
NPO
OL
AIR
TUM
1976
-201
0,M
EN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
COLO
NPO
OL
AIR
TUM
1976
-201
0,U
OM
INI:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRS
TCA
NCE
RSI
TE
COLO
NM
EN
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
56 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
5145
0.9
360
141.0
486
93.6
781
90.8
623
420.8
913
470.
9863
71.
04-1
.58
0.8
1
194
0.8
620
50.8
611
1.06
260.6
210
10.
9247
0.89
200.
92-0
.13
-0.1
2
470.
8850
0.90
31.
2510
1.03
210.
8212
0.96
40.
76-0
.02
-0.0
2
300.6
534
0.7
04
1.88
20.2
319
0.84
70.
662
0.46
-0.0
6-0
.05
117
0.92
121
0.91
40.
6814
0.5
961
0.98
280.
9414
1.15
-0.0
4-0
.05
540.
8765
1.01
114.0
010
0.91
250.
8414
0.95
50.
78-0
.03
0.00
337
0.8
836
80.
9231
1.8
435
0.5
315
20.8
410
31.
1047
1.14
-0.1
7-0
.11
228
0.2
730
40.3
476
2.1
354
0.3
813
30.3
326
0.1
215
0.1
5-2
.40
-2.1
5
70.0
122
0.0
415
0.61
30.0
33
0.0
11
0.0
10
0.0
0-2
.24
-2.1
8
221
0.8
428
21.
0361
5.4
251
1.13
130
1.05
250.3
915
0.5
2-0
.16
0.03
189
0.7
925
11.
0062
5.9
832
0.77
740.6
555
0.94
281.
08-0
.20
0.00
570.
8461
0.86
41.
394
0.3
525
0.78
201.
178
1.02
-0.0
4-0
.04
144
0.86
152
0.87
81.
1426
0.92
560.7
140
0.96
221.
15-0
.09
-0.0
8
882
0.8
310
120.9
213
02.8
214
80.8
037
90.7
525
10.
9810
40.
92-0
.67
-0.3
4
103
1.2
711
41.3
511
3.3
415
1.11
461.
2229
1.43
131.
380.
080.1
1
230.
7326
0.79
32.
321
0.19
161.
085
0.64
10.
28-0
.03
-0.0
2
181.
4219
1.43
11.
802
0.91
91.
505
1.62
21.
400.
020.
02
150.
7321
0.98
66.9
23
0.86
70.
734
0.79
10.
43-0
.02
0.00
40.
784
0.75
00.
000
0.00
10.
412
1.66
11.
950.
000.
00
141.
0817
1.26
35.4
71
0.45
60.
995
1.56
21.
380.
000.
01
1271
1.03
1416
1.1
014
52.8
918
40.
9054
90.
9537
01.1
916
81.1
90.
140.4
8
101.
8911
1.98
14.
030
0.00
62.
323
2.47
12.
020.
020.
02
250
1.3
640
62.1
215
620.2
072
2.3
011
21.2
944
0.97
221.
090.2
60.7
9
670
0.98
793
1.1
112
34.2
097
0.83
341
1.05
149
0.88
831.
09-0
.06
0.2
9
639
0.97
757
1.1
111
84.2
196
0.85
326
1.05
142
0.88
751.
03-0
.06
0.27
311.
0136
1.13
53.9
21
0.20
151.
057
0.92
82.
250.
000.
02
500.
7751
0.7
51
0.35
100.
8715
0.4
815
0.96
101.
49-0
.06
-0.0
6
451.8
949
1.9
74
3.9
19
2.14
221.9
310
1.75
41.
630.0
80.0
9
111.
0515
1.37
48.3
04
2.06
30.
594
1.63
00.
000.
000.
01
150
0.89
187
1.07
375.2
027
0.94
660.
8333
0.80
241.
29-0
.07
0.04
760.
9377
0.90
10.
2915
1.08
340.
8922
1.08
50.
54-0
.02
-0.0
3
124
0.88
146
0.99
223.6
119
0.78
630.
9531
0.89
110.
71-0
.07
0.00
540.
8173
1.05
196.5
26
0.52
260.
8215
0.92
70.
98-0
.05
0.01
610.
9564
0.96
31.
1110
0.92
321.
0715
0.94
40.
55-0
.01
-0.0
1
90.
879
0.83
00.
003
1.65
51.
031
0.40
00.
00-0
.01
-0.0
1
233
0.7
126
60.7
833
2.4
028
0.5
110
40.6
861
0.7
540
1.05
-0.3
6-0
.28
OSI
RO
SIR
OSI
RO
SIR
OSI
RO
SIR
OSI
REA
REA
R
66941
7637
676
376
6694
150
217
1946
468
7466
941
7637
6
260358
2722
1511
858
4790
012
6020
6093
925
498
2603
5827
2215
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
ALL
SITE
S,BU
TSK
INA
ND
COLO
N
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
PROSTATE
TESTIS
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECO
ND
CAN
CER
SITE

COLO
NPO
OL
AIR
TUM
1976
-201
0,W
OM
EN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
COLO
NPO
OL
AIR
TUM
1976
-201
0,D
ON
NE:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRS
TCA
NCE
RSI
TE
COLO
NW
OM
EN
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
57 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
ALL
SITE
S,BU
TSK
INA
ND
COLO
N
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
CERVIXUTERI
CORPUSUTERI
OVARY
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
3086
1.0
435
781.1
649
24.1
147
20.
9914
161.0
677
91.
0241
91.
040.
421.7
6
431.
0344
1.02
10.
604
0.60
180.
9615
1.41
61.
070.
010.
00
241.
0325
1.03
11.
092
0.55
80.
779
1.48
51.
500.
000.
00
91.
079
1.03
00.
001
0.71
51.
293
1.43
00.
000.
000.
00
101.
0210
0.98
00.
001
0.62
51.
123
1.22
10.
800.
000.
00
130.
7414
0.76
11.
412
0.73
60.
773
0.65
20.
79-0
.02
-0.0
2
235
1.06
250
1.08
151.
6121
0.5
910
91.
1158
1.01
471.5
60.
050.
07
163
0.3
020
80.3
745
2.0
631
0.3
691
0.3
818
0.1
323
0.3
0-1
.46
-1.3
2
140.0
422
0.0
58
0.51
30.0
59
0.0
51
0.0
11
0.0
2-1
.45
-1.4
2
149
0.98
186
1.1
837
6.0
228
1.16
821.
2117
0.4
322
1.07
-0.0
10.
10
640.6
782
0.82
184.6
87
0.4
626
0.6
118
0.72
130.
96-0
.12
-0.0
6
480.6
159
0.7
211
3.4
36
0.48
230.6
69
0.4
410
0.91
-0.1
2-0
.08
139
0.94
143
0.93
40.
7015
0.67
651.
0138
0.97
210.
95-0
.03
-0.0
4
261
1.2
129
61.3
335
4.2
230
0.90
122
1.2
970
1.25
391.
270.1
70.2
6
591.
0670
1.21
115.0
19
1.01
230.
9218
1.25
91.
210.
010.
04
50.
578
0.88
39.0
21
0.74
10.
261
0.44
21.
59-0
.01
0.00
71.
408
1.54
14.
990
0.00
41.
843
2.31
00.
000.
010.
01
120.
8914
0.99
23.
725
2.33
20.
333
0.86
21.
07-0
.01
0.00
30.
824
1.05
16.
470
0.00
10.
612
2.15
00.
000.
000.
00
865
1.1
199
31.2
212
84.0
514
41.
1339
41.1
123
11.1
796
0.96
0.3
20.6
6
421.
0851
1.26
95.1
98
1.16
221.
2110
1.07
20.
450.
010.
04
181
1.2
920
81.4
227
4.6
621
0.89
861.3
351
1.4
523
1.33
0.1
50.2
3
151
1.5
116
81.6
117
4.1
540
2.4
484
1.8
516
0.63
110.
850.1
90.2
3
104
1.2
919
52.3
391
29.1
721
1.6
748
1.34
231.
1012
1.07
0.09
0.4
1
175
1.3
020
61.4
731
5.8
336
1.7
272
1.21
421.
1925
1.30
0.1
50.2
4
160
1.2
818
81.4
528
5.6
734
1.7
565
1.18
401.
2221
1.18
0.1
30.2
1
151.
5118
1.7
53
7.9
22
1.35
71.
632
0.76
42.
660.
020.
03
440.
9345
0.92
10.
531
0.1
320
0.95
131.
0810
1.59
-0.0
1-0
.01
591.
2561
1.24
21.
057
0.88
321.4
616
1.36
40.
700.
040.
04
71.
008
1.10
13.
300
0.00
30.
922
1.17
22.
430.
000.
00
123
0.99
137
1.06
142.8
522
1.12
460.
8342
1.31
130.
770.
000.
03
490.
8152
0.83
31.
249
0.94
180.
6712
0.77
101.
20-0
.04
-0.0
4
760.
8786
0.95
102.8
34
0.2
940
1.03
200.
8812
0.99
-0.0
4-0
.02
290.
7537
0.92
85.0
42
0.32
140.
818
0.80
50.
96-0
.04
-0.0
1
400.
9842
0.99
21.
242
0.31
231.
288
0.75
71.
210.
000.
00
70.
877
0.84
00.
000
0.00
30.
864
1.90
00.
000.
000.
00
172
0.6
319
00.6
718
1.68
310.
7569
0.5
846
0.6
426
0.6
5-0
.38
-0.3
4
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
OSI
RO
SIR
OSI
RO
SIR
OSI
RO
SIR
OSI
REA
REA
R
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECO
ND
CAN
CER
SITE
62667
7140
171
401
6266
746
789
1984
378
3762
667
7140
1
263286
2743
7511
090
4466
912
1186
6528
232
148
2632
8627
4375

RECT
UM
POO
LA
IRTU
M19
76-2
010,
MEN
:Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
RETT
OPO
OL
AIR
TUM
1976
-201
0,U
OM
INI:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRS
TCA
NCE
RSI
TE
RECT
UM
MEN
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
58 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
ALL
SITE
S,BU
TSK
INA
ND
RECT
UM
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
PROSTATE
TESTIS
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
2378
0.8
331
701.0
779
26.6
135
40.7
211
170.8
458
40.8
532
30.
94-3
.57
1.4
0
910.7
994
0.7
83
0.58
150.
7048
0.86
210.
817
0.60
-0.1
8-0
.19
210.
7922
0.79
10.
845
1.01
131.
012
0.33
10.
36-0
.04
-0.0
4
220.
9423
0.94
10.
945
1.13
110.
965
0.95
10.
44-0
.01
-0.0
1
480.7
449
0.7
21
0.34
50.4
124
0.76
140.
965
0.76
-0.1
2-0
.13
280.
9333
1.05
53.7
57
1.28
110.
767
1.00
30.
90-0
.02
0.01
164
0.87
176
0.89
121.
4322
0.6
585
0.96
410.
9216
0.73
-0.1
8-0
.15
240
0.5
863
21.4
739
222.9
642
0.6
012
90.6
736
0.3
633
0.6
5-1
.29
1.4
5
233
0.8
261
52.0
938
233.0
841
0.86
123
0.94
360.5
233
0.92
-0.3
72.3
0
70.0
517
0.1
310
1.81
10.0
46
0.1
00
0.0
00
0.0
0-0
.92
-0.8
5
750.6
410
40.
8529
5.8
614
0.69
300.5
521
0.76
100.
73-0
.31
-0.1
3
230.
7025
0.73
21.
464
0.72
70.4
69
1.14
30.
72-0
.07
-0.0
6
450.5
648
0.5
73
0.89
110.
8015
0.4
012
0.62
70.
70-0
.27
-0.2
6
466
0.9
051
80.
9652
2.3
349
0.5
322
50.
9212
81.
0564
1.07
-0.3
9-0
.16
350.
8939
0.95
42.
544
0.61
180.
987
0.73
61.
24-0
.03
-0.0
1
140.
9415
0.97
11.
684
1.61
50.
724
1.11
10.
54-0
.01
0.00
20.
333
0.47
13.
760
0.00
10.
351
0.70
00.
00-0
.03
-0.0
2
90.
9010
0.96
12.
380
0.00
40.
864
1.68
10.
82-0
.01
0.00
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.02
-0.0
2
30.
473
0.46
00.
002
1.84
10.
340
0.00
00.
00-0
.02
-0.0
3
441
0.7
552
60.8
685
3.6
366
0.6
819
90.7
311
60.7
960
0.81
-1.1
1-0
.62
10.
372
0.70
17.
721
1.87
00.
000
0.00
00.
00-0
.01
-0.0
1
108
1.20
185
1.9
777
20.6
829
1.8
750
1.18
190.
8810
0.94
0.13
0.6
5
343
1.03
423
1.2
280
5.6
849
0.85
156
1.00
851.
0653
1.31
0.07
0.5
4
326
1.02
402
1.2
176
5.6
348
0.87
150
1.00
801.
0548
1.25
0.05
0.4
9
171.
1821
1.40
46.7
31
0.41
60.
905
1.44
52.
710.
020.
04
170.5
220
0.5
93
2.15
20.
347
0.4
51
0.1
37
1.94
-0.1
2-0
.10
151.
2417
1.35
23.
933
1.40
111.
901
0.35
00.
000.
020.
03
10.
191
0.1
80
0.00
00.
000
0.00
10.
830
0.00
-0.0
3-0
.03
680.
8375
0.88
72.
0610
0.71
300.
7921
1.08
70.
72-0
.10
-0.0
7
210.5
325
0.6
14
2.40
20.
298
0.4
46
0.63
51.
03-0
.14
-0.1
2
751.
1086
1.21
113.7
48
0.67
351.
1018
1.11
141.
690.
050.
11
351.
0846
1.36
117.8
15
0.87
130.
8512
1.57
51.
310.
020.
09
381.
2338
1.18
00.
003
0.57
201.
406
0.81
92.3
40.
050.
04
20.
392
0.37
00.
000
0.00
20.
840
0.00
00.
00-0
.02
-0.0
2
100
0.6
312
70.7
727
4.1
111
0.4
148
0.6
525
0.6
616
0.80
-0.4
3-0
.27
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECO
ND
CAN
CER
SITE
OSI
RO
SIR
OSI
RO
SIR
OSI
RO
SIR
OSI
REA
REA
R
34480
3845
138
451
3448
026
417
9642
3415
3448
038
451
133422
1394
6060
3825
004
6474
930
074
1359
513
3422
1394
60

RECT
UM
POO
LA
IRTU
M19
76-2
010,
WO
MEN
:Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
RETT
OPO
OL
AIR
TUM
1976
-201
0,D
ON
NE:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRS
TCA
NCE
RSI
TE
RECT
UM
WO
MEN
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
59 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
ALL
SITE
S,BU
TSK
INA
ND
RECT
UM
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
CERVIXUTERI
CORPUSUTERI
OVARY
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
1299
0.99
1654
1.2
135
56.7
020
20.
9357
20.
9732
81.
0019
71.
08-0
.16
2.4
2
130.
7613
0.73
00.
001
0.35
101.
301
0.24
10.
43-0
.04
-0.0
4
60.
646
0.61
00.
000
0.00
51.
190
0.00
10.
74-0
.03
-0.0
3
20.
562
0.54
00.
001
1.63
10.
610
0.00
00.
00-0
.01
-0.0
1
51.
235
1.18
00.
000
0.00
42.
141
1.01
00.
000.
010.
01
81.
148
1.10
00.
001
0.87
61.
941
0.57
00.
000.
010.
01
760.
8586
0.93
102.6
210
0.66
350.
8817
0.77
141.
15-0
.12
-0.0
6
125
0.5
728
61.2
416
118.1
331
0.86
510.5
224
0.4
319
0.6
0-0
.85
0.4
8
111
0.7
026
61.6
115
524.4
327
1.05
470.6
722
0.5
515
0.65
-0.4
30.8
6
140.2
320
0.3
16
2.37
40.3
94
0.1
42
0.1
34
0.47
-0.4
3-0
.38
260.6
829
0.73
31.
942
0.32
110.
6511
1.15
20.
36-0
.11
-0.0
9
130.4
216
0.4
93
2.30
10.
196
0.4
31
0.1
35
1.12
-0.1
6-0
.14
420.7
244
0.7
32
0.88
80.
8714
0.5
514
0.95
60.
67-0
.14
-0.1
4
152
1.7
516
41.8
212
3.6
016
1.16
701.8
245
2.0
521
1.6
50.5
80.6
3
311.
3335
1.4
54
4.3
95
1.31
100.
9513
2.2
53
0.95
0.07
0.09
30.
853
0.82
00.
000
0.00
31.
930
0.00
00.
000.
00-0
.01
10.
511
0.49
00.
000
0.00
00.
001
2.06
00.
00-0
.01
-0.0
1
50.
906
1.04
14.
522
2.19
10.
402
1.45
00.
000.
000.
00
10.
661
0.63
00.
001
3.77
00.
000
0.00
00.
000.
00-0
.01
353
1.08
412
1.2
159
4.4
759
1.07
158
1.05
831.
0453
1.25
0.23
0.6
1
201.
1930
1.7
110
13.4
30
0.00
111.
395
1.29
42.
110.
030.
11
861.4
410
61.7
020
8.1
97
0.68
331.
1925
1.7
321
2.8
00.2
30.3
7
410.
9847
1.08
63.5
18
1.13
241.
267
0.69
20.
37-0
.01
0.03
421.
2767
1.9
625
19.7
412
2.2
820
1.36
91.
081
0.21
0.08
0.2
8
601.
1177
1.3
717
7.9
110
1.14
220.
9213
0.95
151.9
00.
050.
18
541.
0771
1.3
617
8.5
110
1.23
190.
8611
0.87
141.9
20.
030.
16
61.
556
1.50
00.
000
0.00
31.
792
2.03
11.
680.
020.
02
110.
5612
0.59
11.
282
0.62
60.
683
0.62
00.
00-0
.08
-0.0
7
321.5
434
1.5
72
2.42
41.
1314
1.44
71.
407
2.7
80.
100.
11
31.
013
0.97
00.
002
3.76
10.
720
0.00
00.
000.
000.
00
400.
7945
0.85
52.
504
0.48
170.
7510
0.79
91.
28-0
.10
-0.0
7
200.
8220
0.78
00.
004
0.99
50.
465
0.82
61.
74-0
.04
-0.0
5
371.
0541
1.12
42.
785
0.86
181.
159
1.02
51.
010.
020.
04
171.
0919
1.17
23.
092
0.76
81.
154
1.04
31.
410.
010.
02
140.
8515
0.88
11.
533
1.12
70.
964
0.97
00.
00-0
.02
-0.0
2
61.
867
2.08
17.
410
0.00
32.
121
1.23
24.
290.
020.
03
720.6
788
0.7
916
3.7
111
0.63
300.6
424
0.89
70.4
4-0
.31
-0.2
0
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
OSI
RO
SIR
OSI
RO
SIR
OSI
RO
SIR
OSI
REA
REA
R
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECO
ND
CAN
CER
SITE
27053
3005
130
051
2705
320
815
8174
3239
2705
330
051
112555
1172
8947
3419
701
5236
426
797
1369
311
2555
1172
89

LIV
ERPO
OL
AIR
TUM
1976
-201
0,M
EN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
FEG
ATO
POO
LA
IRTU
M19
76-2
010,
UO
MIN
I:Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRS
TCA
NCE
RSI
TE
LIV
ERM
EN
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
60 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
ALL
SITE
S,BU
TSK
INA
ND
LIV
ER
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
PROSTATE
TESTIS
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
662
0.8
693
41.0
827
22.8
419
90.7
337
10.
9180
1.06
120.
75-2
.79
1.63
712.1
984
2.2
913
3.0
819
1.60
462.7
06
2.03
00.
001.0
11.1
0
212.7
924
2.8
33
3.10
72.5
714
3.5
40
0.00
00.
000.3
50.3
6
202.9
220
2.5
90
0.00
52.
0012
3.3
23
4.75
00.
000.3
50.2
9
301.6
640
1.9
610
4.2
17
1.05
202.1
13
1.85
00.
000.
310.4
6
172.0
830
3.2
513
12.2
13
1.02
143.2
60
0.00
00.
000.
230.4
8
370.
8446
0.92
91.
517
0.4
426
1.14
30.
721
1.09
-0.1
8-0
.09
830.7
710
30.
8520
1.50
280.
7444
0.77
100.
931
0.43
-0.6
6-0
.44
540.7
371
0.85
171.8
617
0.66
290.
747
0.94
10.
61-0
.54
-0.2
9
290.
8632
0.84
30.
7111
0.92
150.
843
0.90
00.
00-0
.13
-0.1
4
20.0
62
0.0
50
0.0
01
0.0
81
0.0
60
0.00
00.
00-0
.84
-0.8
5
40.
475
0.52
10.
921
0.33
20.
441
1.21
00.
00-0
.12
-0.1
1
90.4
213
0.5
44
1.50
10.1
36
0.53
10.
471
2.18
-0.3
2-0
.26
117
0.8
318
21.
1565
3.6
040
0.79
630.
8513
0.98
10.
36-0
.62
0.54
80.
7311
0.90
32.
351
0.27
40.
683
2.62
00.
00-0
.08
-0.0
3
10.
235
1.03
47.8
01
0.67
00.
000
0.00
00.
00-0
.09
0.00
42.
344
2.07
00.
001
1.62
33.
330
0.00
00.
000.
060.
05
62.
257
2.33
13.
033
3.20
10.
712
7.56
00.
000.
090.
09
00.
001
1.28
111
.08
00.
000
0.00
00.
000
0.00
-0.0
20.
01
10.
591
0.52
00.
000
0.00
00.
001
5.99
00.
00-0
.02
-0.0
2
110
0.6
816
20.
8952
2.7
333
0.6
063
0.7
312
0.72
20.
56-1
.37
-0.4
5
11.
381
1.22
00.
000
0.00
00.
000
0.00
151
.32
0.01
0.00
180.
7329
1.05
113.6
84
0.47
70.
546
2.45
11.
93-0
.17
0.03
810.
9011
71.
1536
3.1
829
0.90
430.
908
0.92
10.
55-0
.24
0.36
780.
9011
21.
1534
3.1
329
0.94
400.
888
0.96
10.
57-0
.22
0.34
30.
825
1.22
24.
250
0.00
31.
570
0.00
00.
00-0
.02
0.02
20.2
22
0.1
90
0.00
00.
001
0.20
11.
130
0.00
-0.1
9-0
.20
30.
828
1.95
511.8
91
0.79
10.
511
2.65
00.
00-0
.02
0.09
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.04
-0.0
4
301.
3435
1.39
51.
817
0.89
181.
525
2.28
00.
000.
200.
23
111.
0713
1.13
21.
536
1.65
40.
740
0.00
14.
620.
020.
03
130.
7322
1.10
93.9
16
0.94
60.
640
0.00
12.
79-0
.12
0.05
91.
0515
1.55
65.3
84
1.29
40.
890
0.00
16.
040.
010.
12
40.
506
0.66
21.
962
0.70
20.
480
0.00
00.
00-0
.11
-0.0
7
00.
001
0.75
16.
050
0.00
00.
000
0.00
00.
00-0
.03
-0.0
1
350.
8753
1.17
183.5
18
0.56
190.
907
1.79
11.
16-0
.13
0.18
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECO
ND
CAN
CER
SITE
OSI
RO
SIR
OSI
RO
SIR
OSI
RO
SIR
OSI
REA
REA
R
24256
3372
433
724
2425
611
886
1708
255
2425
633
724
38090
4286
347
7213
671
2002
536
4275
238
090
4286
3

LIV
ERPO
OL
AIR
TUM
1976
-201
0,W
OM
EN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
FEG
ATO
POO
LA
IRTU
M19
76-2
010,
DO
NN
E:Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRS
TCA
NCE
RSI
TE
LIV
ERW
OM
EN
61 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
160
0.8
121
60.
9756
2.1
055
0.78
760.7
624
1.13
50.
93-2
.26
-0.4
2
83.1
98
2.8
10
0.00
11.
125
3.9
11
3.68
114
.89
0.33
0.28
32.
163
1.91
00.
001
2.04
11.
420
0.00
126
.14
0.10
0.08
35.9
13
5.2
20
0.00
00.
003
11.5
70
0.00
00.
000.
150.
13
23.
252
2.87
00.
000
0.00
13.
181
15.2
50
0.00
0.08
0.07
33.
034
3.54
17.
100
0.00
24.
011
9.32
00.
000.
120.
15
110.
9413
0.96
21.
115
1.16
50.
861
0.80
00.
00-0
.05
-0.0
3
160.4
926
0.71
102.2
47
0.61
40.2
44
1.14
11.
09-1
.00
-0.5
9
120.5
121
0.79
92.8
04
0.48
40.3
43
1.17
11.
50-0
.69
-0.3
0
40.
445
0.49
10.
803
0.92
00.0
01
1.04
00.
00-0
.31
-0.2
8
00.0
01
0.1
41
1.15
00.
000
0.00
00.
000
0.00
-0.3
9-0
.34
10.
212
0.37
11.
460
0.00
00.
001
2.04
00.
00-0
.23
-0.1
8
50.
585
0.51
00.
001
0.33
30.
681
1.04
00.
00-0
.22
-0.2
6
110.
8316
1.06
52.
901
0.22
71.
032
1.35
12.
66-0
.14
0.05
30.
904
1.06
12.
350
0.00
21.
170
0.00
110
.34
-0.0
20.
01
11.
762
3.14
114
.21
15.
120
0.00
00.
000
0.00
0.03
0.07
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.02
-0.0
2
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.05
-0.0
5
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.01
-0.0
1
370.
7752
0.96
152.3
914
0.82
190.
774
0.77
00.
00-0
.67
-0.1
2
62.
526
2.21
00.
002
2.27
32.
491
4.15
00.
000.
220.
18
50.
548
0.77
32.
512
0.61
10.
211
1.04
14.
43-0
.25
-0.1
3
30.
493
0.43
00.
001
0.45
10.
321
1.54
00.
00-0
.19
-0.2
1
30.
604
0.71
11.
552
1.15
10.
390
0.00
00.
00-0
.12
-0.0
9
101.
2416
1.75
65.4
44
1.40
61.
470
0.00
00.
000.
120.
37
101.
3316
1.8
86
5.8
44
1.50
61.
580
0.00
00.
000.
150.
40
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.03
-0.0
3
20.
652
0.58
00.
000
0.00
10.
641
3.05
00.
00-0
.06
-0.0
8
51.
616
1.73
12.
721
0.93
21.
252
5.81
00.
000.
120.
14
12.
331
2.05
00.
000
0.00
14.
590
0.00
00.
000.
030.
03
60.
778
0.90
21.
943
1.09
20.
501
1.18
00.
00-0
.11
-0.0
5
61.
606
1.41
00.
002
1.49
21.
052
4.96
00.
000.
140.
09
50.
965
0.84
00.
003
1.59
20.
760
0.00
00.
00-0
.01
-0.0
5
31.
303
1.13
00.
003
3.52
00.
000
0.00
00.
000.
040.
02
20.
822
0.72
00.
000
0.00
21.
620
0.00
00.
00-0
.03
-0.0
4
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.03
-0.0
3
120.
7819
1.09
73.1
95
0.91
70.
910
0.00
00.
00-0
.20
0.08
ALL
SITE
S,BU
TSK
INA
ND
LIV
ER
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
CERVIXUTERI
CORPUSUTERI
OVARY
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
OSI
RO
SIR
OSI
RO
SIR
OSI
RO
SIR
OSI
REA
REA
R
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECO
ND
CAN
CER
SITE
10720
1571
215
712
1072
050
1875
114
010
720
1571
2
16417
1858
721
6958
7983
5417
5942
516
417
1858
7

GA
LLBL
AD
DER
POO
LA
IRTU
M19
76-2
010,
MEN
:Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
COLE
CIST
IPO
OL
AIR
TUM
1976
-201
0,U
OM
INI:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRS
TCA
NCE
RSI
TE
GA
LLBL
AD
DER
MEN
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
62 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
173
0.8
027
51.1
410
23.7
545
0.6
684
0.87
280.
7916
1.07
-4.3
53.
01
80.
978
0.86
00.
002
0.74
41.
062
1.57
00.
00-0
.03
-0.1
2
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.20
-0.2
0
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.17
-0.1
7
81.
718
1.52
00.
002
1.29
41.
892
2.79
00.
000.
340.
25
20.
923
1.22
13.
540
0.00
22.
030
0.00
00.
00-0
.02
0.05
141.
0628
1.8
614
7.7
03
0.68
61.
024
1.89
11.
170.
081.1
9
210.
7054
1.6
133
8.7
91
0.1
117
1.28
20.
401
0.47
-0.9
11.8
8
150.
7339
1.6
924
9.3
51
0.1
611
1.20
20.
581
0.68
-0.5
71.4
6
60.
6415
1.43
97.5
70
0.00
61.
440
0.00
00.
00-0
.34
0.41
50.
5713
1.31
87.2
52
0.71
10.
251
0.70
11.
66-0
.39
0.28
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.25
-0.2
6
71.
199
1.35
22.
673
1.60
41.
520
0.00
00.
000.
110.
22
330.
8741
0.96
81.
658
0.65
140.
827
1.14
41.
59-0
.51
-0.1
6
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.29
-0.2
9
10.
911
0.81
00.
000
0.00
00.
001
5.43
00.
00-0
.01
-0.0
2
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.05
-0.0
5
11.
381
1.23
00.
000
0.00
00.
001
8.32
00.
000.
030.
02
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.02
-0.0
2
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.05
-0.0
5
300.
7037
0.77
71.
349
0.68
140.
735
0.69
20.
63-1
.32
-1.0
1
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.02
-0.0
2
81.
2522
3.0
614
18.0
14
1.99
41.
390
0.00
00.
000.
161.3
6
190.
7726
0.94
72.
239
1.14
60.
550
0.0
04
2.38
-0.5
8-0
.16
190.
8126
0.98
72.
339
1.19
60.
570
0.0
04
2.49
-0.4
7-0
.05
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.11
-0.1
1
41.
694
1.50
00.
001
1.31
21.
870
0.00
16.
270.
170.
12
11.
152
2.07
110
.00
00.
001
2.54
00.
000
0.00
0.01
0.10
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.04
-0.0
4
30.
504
0.60
11.
360
0.00
10.
382
2.04
00.
00-0
.30
-0.2
5
20.
693
0.92
12.
680
0.00
21.
560
0.00
00.
00-0
.09
-0.0
2
40.
796
1.05
23.
000
0.00
41.
780
0.00
00.
00-0
.11
0.03
10.
423
1.10
26.
320
0.00
10.
930
0.00
00.
00-0
.14
0.03
20.
882
0.78
00.
000
0.00
21.
980
0.00
00.
00-0
.03
-0.0
5
12.
661
2.32
00.
000
0.00
16.
040
0.00
00.
000.
060.
05
100.
8613
0.99
31.
993
0.81
20.
393
1.56
22.
48-0
.16
-0.0
1
ALL
SITE
S,BU
TSK
INA
ND
GA
LLBL
AD
DER
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
PROSTATE
TESTIS
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECO
ND
CAN
CER
SITE
OSI
RO
SIR
OSI
RO
SIR
OSI
RO
SIR
OSI
REA
REA
R
5866
8650
8650
5866
2588
509
164
5866
8650
9674
1087
111
9731
4943
9914
9962
796
7410
871

GA
LLBL
AD
DER
POO
LA
IRTU
M19
76-2
010,
WO
MEN
:Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
COLE
CIST
IPO
OL
AIR
TUM
1976
-201
0,D
ON
NE:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRS
TCA
NCE
RSI
TE
GA
LLBL
AD
DER
WO
MEN
63 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
ALL
SITE
S,BU
TSK
INA
ND
GA
LLBL
AD
DER
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
CERVIXUTERI
CORPUSUTERI
OVARY
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
209
1.2
134
81.7
713
95.7
556
1.03
911.2
443
1.4
119
1.30
2.59
9.5
1
20.
932
0.82
00.
000
0.00
11.
091
2.67
00.
00-0
.01
-0.0
3
21.
662
1.46
00.
000
0.00
11.
971
4.64
00.
000.
060.
04
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.03
-0.0
3
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.04
-0.0
4
11.
092
1.91
17.
480
0.00
12.
610
0.00
00.
000.
010.
06
90.
7630
2.2
021
11.7
71
0.27
51.
013
1.42
00.
00-0
.20
1.0
3
431.4
975
2.2
832
7.8
612
1.33
211.7
45
0.96
51.
981.
022.6
5
331.5
954
2.2
821
7.1
810
1.55
151.
735
1.33
31.
630.
881.9
1
101.
2421
2.2
811
9.5
82
0.79
61.
760
0.00
22.
930.
140.7
4
40.
779
1.51
56.6
62
1.21
20.
910
0.00
00.
00-0
.09
0.19
10.
241
0.20
00.
000
0.00
00.
000
0.00
12.
77-0
.23
-0.2
4
182.3
520
2.2
92
1.84
62.
548
2.5
22
1.41
22.
840.7
40.7
1
100.
9016
1.27
64.0
23
0.88
20.
435
2.50
00.
00-0
.08
0.22
31.
063
0.93
00.
001
1.14
00.
001
2.00
14.
150.
01-0
.01
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.03
-0.0
3
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.02
-0.0
2
00.
001
1.25
110
.35
00.
000
0.00
00.
000
0.00
-0.0
50.
01
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.01
-0.0
1
561.3
885
1.8
529
5.2
516
1.24
181.
0317
2.4
55
1.53
1.11
2.4
5
20.
944
1.65
26.
451
1.41
11.
090
0.00
00.
00-0
.01
0.10
60.
806
0.70
00.
001
0.41
41.
230
0.00
11.
73-0
.11
-0.1
6
234.3
229
4.7
86
8.0
97
4.1
113
5.7
23
3.27
00.
001.2
71.4
4
30.
7217
3.5
914
25.1
02
1.55
10.
560
0.00
00.
00-0
.08
0.7
7
50.
718
0.99
33.
000
0.00
31.
011
0.78
11.
59-0
.15
0.00
40.
617
0.93
33.
230
0.00
20.
731
0.84
11.
72-0
.18
-0.0
3
11.
991
1.74
00.
000
0.00
14.
790
0.00
00.
000.
040.
03
10.
401
0.35
00.
000
0.00
00.
001
2.26
00.
00-0
.11
-0.1
2
20.
823
1.09
13.
241
1.29
10.
920
0.00
00.
00-0
.03
0.02
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.03
-0.0
3
20.
317
0.94
55.5
90
0.00
20.
720
0.00
00.
00-0
.32
-0.0
3
20.
622
0.54
00.
000
0.00
10.
740
0.00
13.
69-0
.09
-0.1
1
61.
299
1.69
34.
453
2.03
21.
031
1.20
00.
000.
100.
23
10.
481
0.42
00.
000
0.00
11.
150
0.00
00.
00-0
.08
-0.0
9
31.
406
2.45
39.8
82
2.98
00.
001
2.59
00.
000.
060.
22
24.
572
3.97
00.
001
7.27
15.
560
0.00
00.
000.
110.
09
110.
7819
1.17
83.8
70
0.0
05
0.85
31.
153
2.31
-0.2
30.
17
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
OSI
RO
SIR
OSI
RO
SIR
OSI
RO
SIR
OSI
REA
REA
R
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECO
ND
CAN
CER
SITE
9396
1381
113
811
9396
3442
756
260
9396
1381
1
13942
1587
419
3245
2160
1223
4010
6913
942
1587
4

PAN
CREA
SPO
OL
AIR
TUM
1976
-201
0,M
EN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
PAN
CREA
SPO
OL
AIR
TUM
1976
-201
0,U
OM
INI:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRS
TCA
NCE
RSI
TE
PAN
CREA
SM
EN
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
64 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
ALL
SITE
S,BU
TSK
INA
ND
PAN
CREA
S
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
PROSTATE
TESTIS
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
187
0.7
043
61.3
124
93.9
263
0.4
989
0.91
210.
6814
1.13
-5.9
76.1
8
151.
3219
1.35
41.
484
0.71
71.
683
2.54
12.
300.
260.
29
41.
504
1.21
00.
000
0.00
11.
022
7.15
19.
450.
100.
04
31.
245
1.68
23.
560
0.00
22.
241
4.06
00.
000.
040.
12
81.
2710
1.28
21.
324
1.29
41.
740
0.00
00.
000.
120.
13
31.
027
1.93
45.6
81
0.71
10.
941
3.15
00.
000.
010.
20
160.
9638
1.8
222
5.2
65
0.62
101.
661
0.53
00.
00-0
.05
1.0
2
200.5
364
1.3
844
4.9
84
0.2
315
1.09
10.
230
0.00
-1.2
81.
05
140.5
443
1.36
294.8
24
0.3
39
0.96
10.
330
0.00
-0.8
60.
67
60.
5121
1.43
155.3
40
0.0
06
1.38
00.
000
0.00
-0.4
30.
38
30.2
711
0.80
83.0
51
0.19
20.
490
0.00
00.
00-0
.59
-0.1
7
31.
017
1.91
45.5
91
0.72
10.
930
0.00
17.
000.
000.
20
00.0
00
0.0
00
0.00
00.
000
0.00
00.
000
0.00
-0.5
4-0
.55
350.
7387
1.4
652
4.4
79
0.3
912
0.69
101.
864
1.94
-0.9
61.6
2
20.
534
0.86
22.
412
1.14
00.
000
0.00
00.
00-0
.13
-0.0
4
10.
701
0.57
00.
000
0.00
11.
890
0.00
00.
00-0
.03
-0.0
5
11.
701
1.37
00.
001
3.54
00.
000
0.00
00.
000.
030.
02
00.
001
0.86
14.
580
0.00
00.
000
0.00
00.
00-0
.07
-0.0
1
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.02
-0.0
2
11.
711
1.38
00.
001
3.60
00.
000
0.00
00.
000.
030.
02
370.6
865
0.98
282.2
717
0.68
150.
753
0.46
20.
75-1
.26
-0.0
9
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.02
-0.0
2
80.
9532
3.0
824
12.3
81
0.25
72.
250
0.00
00.
00-0
.03
1.2
9
210.
6947
1.24
263.5
66
0.4
19
0.81
10.
295
3.5
6-0
.70
0.54
190.
6541
1.13
223.1
55
0.3
68
0.75
10.
305
3.7
3-0
.75
0.28
21.
546
3.7
14
12.6
41
1.63
12.
130
0.00
00.
000.
050.
26
10.
322
0.52
11.
380
0.00
10.
870
0.00
00.
00-0
.16
-0.1
1
10.
801
0.66
00.
000
0.00
00.
001
7.28
00.
00-0
.02
-0.0
3
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.04
-0.0
4
60.
7816
1.69
105.6
05
1.37
10.
350
0.00
00.
00-0
.12
0.39
00.
002
0.45
22.
310
0.00
00.
000
0.00
00.
00-0
.26
-0.1
5
50.
8011
1.41
63.9
42
0.67
31.
310
0.00
00.
00-0
.09
0.19
41.
328
2.13
45.4
62
1.38
21.
820
0.00
00.
000.
070.
25
10.
363
0.86
22.
960
0.00
10.
970
0.00
00.
00-0
.13
-0.0
3
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.03
-0.0
3
80.
5619
1.08
113.2
13
0.45
40.
780
0.00
11.
44-0
.45
0.08
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECO
ND
CAN
CER
SITE
OSI
RO
SIR
OSI
RO
SIR
OSI
RO
SIR
OSI
REA
REA
R
14940
2241
022
410
1494
040
7649
315
514
940
2241
0
13693
1678
930
9565
8451
2614
4753
613
693
1678
9

PAN
CREA
SPO
OL
AIR
TUM
1976
-201
0,W
OM
EN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
PAN
CREA
SPO
OL
AIR
TUM
1976
-201
0,D
ON
NE:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRS
TCA
NCE
RSI
TE
PAN
CREA
SW
OM
EN
65 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
ALL
SITE
S,BU
TSK
INA
ND
PAN
CREA
S
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
CERVIXUTERI
CORPUSUTERI
OVARY
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
129
0.7
834
31.6
621
45.3
151
0.6
454
0.88
170.
947
1.00
-2.5
77.6
6
20.
923
1.11
11.
941
0.96
11.
230
0.00
00.
00-0
.01
0.02
21.
662
1.34
00.
001
1.76
12.
240
0.00
00.
000.
050.
03
00.
001
1.79
19.
620
0.00
00.
000
0.00
00.
00-0
.03
0.02
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.04
-0.0
4
11.
131
0.90
00.
001
2.34
00.
000
0.00
00.
000.
01-0
.01
50.
4621
1.52
165.4
61
0.19
20.
510
0.00
24.
32-0
.40
0.41
200.
7358
1.6
838
5.5
25
0.3
810
0.99
41.
331
0.84
-0.5
21.3
2
150.
7647
1.8
932
6.4
54
0.42
60.
824
1.83
11.
15-0
.33
1.2
5
50.
6511
1.14
63.1
21
0.27
41.
420
0.00
00.
00-0
.18
0.08
20.
417
1.14
54.0
20
0.00
21.
110
0.00
00.
00-0
.20
0.05
30.
7619
3.8
216
15.5
01
0.52
21.
400
0.00
00.
00-0
.06
0.7
9
00.0
01
0.1
11
0.54
00.
000
0.00
00.
000
0.00
-0.5
0-0
.46
121.
0927
1.9
815
5.7
24
0.77
51.
232
1.65
12.
100.
070.7
5
31.
013
0.83
00.
000
0.00
21.
780
0.00
17.
660.
00-0
.04
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.03
-0.0
3
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.02
-0.0
2
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.05
-0.0
5
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.01
-0.0
1
310.
7475
1.4
744
4.6
214
0.71
110.
705
1.11
10.
59-0
.73
1.3
4
00.
001
0.38
11.
970
0.00
00.
000
0.00
00.
00-0
.15
-0.0
9
70.
9210
1.07
31.
732
0.55
41.
401
1.26
00.
00-0
.04
0.04
71.
3319
2.9
112
9.5
96
2.37
10.
510
0.00
00.
000.
120.7
0
30.
7325
4.9
022
22.5
63
1.53
00.
000
0.00
00.
00-0
.08
1.1
2
60.
8818
2.1
212
7.0
71
0.31
20.
803
4.02
00.
00-0
.05
0.53
50.
7916
2.0
311
6.9
91
0.33
10.
433
4.33
00.
00-0
.09
0.46
12.
052
3.26
18.
020
0.00
15.
570
0.00
00.
000.
040.
08
10.
413
0.98
23.
451
0.85
00.
000
0.00
00.
00-0
.10
0.00
41.
466
1.82
23.
691
0.81
32.
790
0.00
00.
000.
090.
15
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.03
-0.0
3
40.
629
1.13
53.2
53
0.97
10.
420
0.00
00.
00-0
.17
0.06
30.
978
2.08
56.5
11
0.67
10.
881
3.03
00.
00-0
.01
0.23
30.
6810
1.81
76.2
21
0.47
21.
240
0.00
00.
00-0
.10
0.25
21.
028
3.2
56
11.8
61
1.04
11.
400
0.00
00.
000.
000.
31
10.
492
0.78
11.
940
0.00
11.
330
0.00
00.
00-0
.07
-0.0
3
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.03
-0.0
3
120.
9020
1.19
82.
315
0.78
51.
031
0.66
11.
66-0
.09
0.18
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
OSI
RO
SIR
OSI
RO
SIR
OSI
RO
SIR
OSI
REA
REA
R
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECO
ND
CAN
CER
SITE
15686
2350
023
500
1568
642
3454
815
415
686
2350
0
14542
1779
732
5568
2155
2416
0958
914
542
1779
7

LUNG
POOLAIRTUM1976-2010,MEN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
POLMONE
POOLAIRTUM1976-2010,UOMINI:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRSTCANCERSITE
LUNG
MEN
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
116474
1491
6714
9167
1164
7448
891
8861
2908
1164
7414
9167
177729
1998
2722
098
6320
376
983
2656
610
976
1777
2919
9827
66 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
ALLSITES,BUTSKINANDLUNG
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
PROSTATE
TESTIS
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
3377
1.0
938
721.1
249
51.3
190
40.8
614
931.1
368
81.3
929
21.2
81.6
22.0
3
383
2.3
743
52.3
952
2.5
510
51.8
119
12.7
268
2.8
419
1.9
71.2
41.2
7
111
3.0
012
22.9
311
2.3
838
2.8
954
3.3
616
2.8
93
1.32
0.4
20.4
0
932.7
610
52.7
712
2.8
623
1.9
151
3.4
714
2.8
05
2.53
0.3
30.3
4
179
1.9
720
82.0
329
2.5
144
1.35
862.1
838
2.8
311
2.0
40.5
00.5
3
751.8
587
1.9
012
2.3
515
1.05
341.9
417
2.7
69
3.4
00.1
90.2
1
239
1.05
270
1.05
311.
0471
0.88
900.
9356
1.6
222
1.41
0.06
0.06
502
0.99
568
1.00
661.
0713
10.7
621
91.
0110
71.3
045
1.17
-0.0
4-0
.01
356
1.03
402
1.03
461.
1099
0.85
147
1.00
721.
2738
1.4
20.
050.
06
146
0.90
166
0.92
201.
0032
0.5
872
1.04
351.
377
0.60
-0.0
9-0
.08
115
0.7
513
60.7
921
1.12
190.3
646
0.6
935
1.4
415
1.39
-0.2
2-0
.18
411.
0444
0.99
30.
6110
0.74
211.
267
1.12
31.
020.
010.
00
109
1.09
119
1.06
100.
8136
1.06
431.
0123
1.44
70.
940.
050.
03
920.1
316
50.2
173
0.85
140.0
645
0.1
523
0.2
210
0.2
1-3
.35
-3.0
4
390.
7941
0.74
20.
3512
0.74
150.
7110
1.22
20.
52-0
.06
-0.0
7
60.3
19
0.4
13
1.32
20.
313
0.36
00.
001
0.67
-0.0
8-0
.06
111.
4511
1.29
00.
004
1.50
20.
625
4.3
40
0.00
0.02
0.01
171.
3719
1.37
21.
325
1.18
61.
146
3.0
70
0.00
0.03
0.03
10.
301
0.27
00.
000
0.00
00.
001
2.02
00.
00-0
.01
-0.0
1
101.
2712
1.36
22.
083
1.12
10.
303
2.40
35.2
60.
010.
02
603
0.8
367
60.8
473
0.87
159
0.6
726
80.8
711
70.
9659
1.02
-0.6
8-0
.66
10.
291
0.26
00.
001
0.80
00.
000
0.00
00.
00-0
.01
-0.0
1
173
1.4
821
31.6
340
2.8
861
1.5
578
1.5
525
1.33
91.
060.3
20.4
1
645
1.5
372
91.5
484
1.6
114
81.
0231
61.7
612
31.8
558
1.9
11.2
61.2
8
629
1.5
671
11.5
782
1.6
414
31.
0330
81.7
912
11.9
057
1.9
71.2
71.2
9
160.
8918
0.89
20.
905
0.82
81.
052
0.70
10.
75-0
.01
-0.0
1
290.6
832
0.6
63
0.57
100.
6715
0.81
30.
451
0.35
-0.0
8-0
.08
231.
4631
1.7
78
4.4
110
1.89
91.
332
0.79
21.
800.
040.
07
40.
556
0.74
22.
183
1.16
10.
320
0.00
00.
00-0
.02
-0.0
1
890.
8510
30.
8814
1.11
200.5
638
0.85
191.
1412
1.59
-0.0
9-0
.07
300.6
240
0.7
310
1.66
50.3
010
0.4
813
1.69
20.
56-0
.10
-0.0
7
871.
0410
41.
1017
1.60
230.
7936
1.01
221.6
96
1.01
0.02
0.05
320.
7944
0.96
122.3
37
0.49
130.
759
1.44
31.
08-0
.05
-0.0
1
461.
2349
1.16
30.
6413
1.01
171.
0713
2.1
93
1.08
0.05
0.03
91.
5711
1.68
22.
503
1.43
62.
480
0.00
00.
000.
020.
02
145
0.7
618
50.8
640
1.6
851
0.78
510.6
226
0.87
171.
21-0
.25
-0.1
5
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECONDCANCERSITE
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
EAR
EAR

LUNG
POOLAIRTUM1976-2010,WOMEN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
POLMONE
POOLAIRTUM1976-2010,DONNE:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRSTCANCERSITE
LUNG
WOMEN
67 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
587
1.1
367
71.1
790
1.4
616
00.
9427
91.2
210
51.2
543
1.23
1.3
91.7
7
202.8
120
2.5
10
0.00
62.
558
2.5
36
5.2
20
0.00
0.2
60.2
2
61.
596
1.42
00.
002
1.62
21.
202
3.22
00.
000.
050.
03
63.8
16
3.4
10
0.00
23.
791
1.42
312.1
50
0.00
0.09
0.08
84.5
28
4.0
50
0.00
23.
395
6.3
61
3.56
00.
000.1
30.
11
62.
278
2.6
92
6.10
22.
293
2.58
12.
340
0.00
0.07
0.09
220.
7025
0.71
30.
746
0.57
100.
734
0.81
20.
96-0
.19
-0.1
9
106
1.2
511
71.2
311
1.07
270.
9747
1.26
221.
5810
1.69
0.43
0.40
781.2
886
1.2
68
1.09
221.
1036
1.35
121.
198
1.86
0.35
0.32
281.
1731
1.16
31.
045
0.63
111.
0510
2.5
82
1.23
0.08
0.08
140.
9415
0.90
10.
551
0.20
50.
776
2.48
21.
94-0
.02
-0.0
3
90.
7811
0.85
21.
381
0.26
51.
001
0.54
22.
59-0
.05
-0.0
3
351.6
039
1.5
94
1.50
70.
9921
2.2
16
1.65
10.
630.
270.
26
110.3
124
0.6
013
3.1
20
0.0
03
0.1
95
0.84
31.
17-0
.50
-0.2
9
121.
1913
1.16
10.
881
0.31
81.
792
1.20
11.
460.
040.
03
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.03
-0.0
3
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.01
-0.0
1
41.
755
1.96
13.
742
2.67
10.
991
2.70
00.
000.
030.
04
23.
263
4.36
113
.54
00.
000
0.00
220.3
80
0.00
0.03
0.04
141
0.99
159
1.01
181.
1141
0.88
721.
1420
0.88
80.
88-0
.02
0.02
101.
4011
1.37
11.
145
2.01
20.
632
1.86
12.
480.
060.
05
190.
7321
0.72
20.
674
0.46
100.
865
1.20
00.
00-0
.15
-0.1
5
160.
9219
0.98
31.
465
0.86
50.
654
1.45
21.
79-0
.03
-0.0
1
221.6
122
1.45
00.
0010
2.2
79
1.50
31.
320
0.00
0.17
0.12
422.0
244
1.8
82
0.79
121.
7623
2.5
22
0.58
53.4
10.4
30.3
8
402.0
642
1.9
32
0.86
101.
5823
2.7
12
0.63
53.6
70.4
20.3
7
21.
382
1.23
00.
002
4.21
00.
000
0.00
00.
000.
010.
01
80.
989
0.99
11.
061
0.37
20.
563
2.25
23.
620.
000.
00
161.
6024
2.1
78
7.5
96
1.86
61.
343
1.84
11.
560.
120.2
4
00.
003
2.08
319.5
60
0.00
00.
000
0.00
00.
00-0
.03
0.03
211.
0127
1.16
62.
457
1.02
111.
202
0.59
10.
700.
000.
07
121.
2513
1.20
10.
863
0.95
81.
891
0.64
00.
000.
050.
04
181.
3522
1.47
42.
431
0.23
101.
715
2.32
22.
210.
090.
13
61.
029
1.36
34.
060
0.00
31.
163
3.22
00.
000.
000.
04
111.
7312
1.69
11.
301
0.48
62.
162
1.92
24.
480.
090.
09
10.
921
0.82
00.
000
0.00
12.
130
0.00
00.
000.
000.
00
320.
8247
1.08
153.0
912
0.94
130.
774
0.63
31.
09-0
.14
0.06
ALLSITES,BUTSKINANDLUNG
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
CERVIXUTERI
CORPUSUTERI
OVARY
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
EAR
EAR
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECONDCANCERSITE
29949
3850
538
505
2994
913
242
2594
825
2994
938
505
49229
5490
956
8016
479
2198
577
6030
0549
229
5490
9

SKINMELANOMA
POOLAIRTUM1976-2010,MEN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
MELANOMACUTANEO
POOLAIRTUM1976-2010,UOMINI:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRSTCANCERSITE
SKINMELANOMA
MEN
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
68 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
ALLSITES,BUTSKINANDSKINMELANOMA
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
PROSTATE
TESTIS
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
1117
1.01
1183
1.03
661.7
721
01.2
451
71.
0127
20.
9511
80.
840.
120.
46
310.6
232
0.6
21
0.58
81.
0218
0.77
40.3
21
0.1
7-0
.24
-0.2
4
50.4
15
0.4
00
0.00
10.
533
0.53
10.
320
0.00
-0.0
9-0
.09
90.
799
0.76
00.
004
2.27
40.
751
0.34
00.
00-0
.03
-0.0
3
170.
6518
0.66
11.
073
0.71
110.
882
0.30
10.
33-0
.12
-0.1
1
80.
668
0.64
00.
002
1.05
20.
352
0.65
21.
35-0
.05
-0.0
6
600.
9662
0.95
20.
8912
1.19
290.
999
0.57
101.
33-0
.03
-0.0
4
134
0.87
137
0.86
30.
5918
0.77
630.
9038
0.95
150.
75-0
.24
-0.2
6
910.
8792
0.85
10.
2910
0.63
370.
7731
1.13
130.
94-0
.18
-0.2
0
430.
8945
0.90
21.
238
1.08
261.
177
0.56
20.
33-0
.07
-0.0
6
210.4
723
0.5
02
1.32
30.
447
0.3
48
0.70
30.
53-0
.30
-0.2
8
131.
1614
1.21
12.
593
1.71
61.
163
1.05
10.
710.
020.
03
321.
0634
1.09
21.
973
0.65
151.
088
1.02
61.
540.
020.
03
140
0.7
415
90.8
119
2.8
935
1.18
520.5
936
0.75
170.
73-0
.62
-0.4
5
10.0
51
0.0
50
0.00
00.
000
0.0
00
0.0
01
0.39
-0.2
3-0
.23
121.
9313
2.0
31
4.98
22.
187
2.48
21.
221
1.21
0.07
0.08
10.
391
0.38
00.
000
0.00
10.
830
0.00
00.
00-0
.02
-0.0
2
61.
387
1.56
16.
910
0.00
52.
491
0.89
00.
000.
020.
03
65.2
76
5.0
90
0.00
316.4
82
3.70
00.
001
7.77
0.06
0.06
52.
035
1.96
00.
000
0.00
21.
763
4.67
00.
000.
030.
03
259
1.1
726
71.1
78
1.13
421.
3011
61.
1672
1.23
290.
970.
480.
48
10.
311
0.30
00.
000
0.00
10.
610
0.00
00.
00-0
.03
-0.0
3
721.9
285
2.1
913
10.5
720
3.5
636
2.0
813
1.32
30.
620.4
30.5
6
120
0.99
121
0.96
10.
2428
1.49
601.
0726
0.84
60.3
9-0
.02
-0.0
5
116
1.00
117
0.97
10.
2527
1.50
581.
0825
0.84
60.4
10.
00-0
.04
40.
784
0.75
00.
001
1.25
20.
841
0.76
00.
00-0
.01
-0.0
2
161.
1317
1.16
12.
092
0.92
60.
916
1.64
21.
150.
020.
03
283.9
729
3.9
91
4.49
76.8
614
4.3
35
2.65
22.
200.2
60.2
6
41.
295
1.55
19.
132
4.02
00.
001
1.28
12.
960.
010.
02
421.
2345
1.28
32.
644
0.77
211.
339
1.02
81.
860.
100.
12
191.
3120
1.34
12.
044
1.79
81.
205
1.34
21.
080.
060.
06
251.
0025
0.96
00.
006
1.52
141.
204
0.63
10.
320.
00-0
.01
141.
1614
1.12
00.
004
2.10
81.
422
0.65
00.
000.
020.
02
100.
8710
0.85
00.
002
1.13
50.
952
0.68
10.
70-0
.02
-0.0
2
10.
641
0.62
00.
000
0.00
11.
350
0.00
00.
00-0
.01
-0.0
1
621.
1067
1.15
52.
586
0.68
321.
2217
1.17
70.
980.
070.
10
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECONDCANCERSITE
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
EAR
EAR
16345
1685
116
851
1634
513
847
6312
2312
1634
516
851
79529
8229
927
7012
567
3806
120
175
8726
7952
982
299

SKINMELANOMA
POOLAIRTUM1976-2010,WOMEN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
MELANOMACUTANEO
POOLAIRTUM1976-2010,DONNE:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRSTCANCERSITE
SKINMELANOMA
WOMEN
69 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
ALLSITES,BUTSKINANDSKINMELANOMA
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
CERVIXUTERI
CORPUSUTERI
OVARY
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
1008
1.1
710
541.2
046
2.0
014
61.3
742
31.1
627
51.1
316
41.
141.4
21.6
0
151.
3116
1.36
13.
303
2.13
51.
036
1.84
10.
510.
030.
04
81.
339
1.46
16.
382
2.75
41.
591
0.58
10.
960.
020.
03
31.
093
1.06
00.
000
0.00
00.
003
3.83
00.
000.
000.
00
41.
464
1.42
00.
001
2.95
10.
862
2.58
00.
000.
010.
01
30.
773
0.75
00.
002
4.12
00.
001
0.91
00.
00-0
.01
-0.0
1
451.
0046
1.00
10.
7811
1.87
201.
049
0.73
50.
690.
000.
00
136
1.09
138
1.08
20.
6014
0.91
490.
9339
1.10
341.5
70.
110.
09
102
1.14
103
1.12
10.
429
0.82
370.
9932
1.26
241.
540.
120.
10
340.
9635
0.96
11.
045
1.13
120.
807
0.70
101.
67-0
.01
-0.0
1
170.
8517
0.82
00.
001
0.40
91.
074
0.71
30.
86-0
.03
-0.0
3
80.5
08
0.4
90
0.00
10.
496
0.88
00.0
01
0.37
-0.0
8-0
.08
310.
9931
0.97
00.
001
0.26
151.
1610
1.12
50.
890.
00-0
.01
691.3
082
1.5
113
9.6
212
1.91
281.
2818
1.18
111.
150.
150.2
6
10.0
51
0.0
50
0.00
00.
001
0.1
20
0.0
00
0.00
-0.1
8-0
.18
41.
765
2.15
117
.66
00.
001
1.07
11.
532
4.75
0.02
0.02
21.
952
1.90
00.
001
7.63
00.
000
0.00
15.
720.
010.
01
102.6
010
2.5
30
0.00
12.
084
2.42
21.
843
4.74
0.06
0.06
10.
951
0.93
00.
000
0.00
00.
001
3.46
00.
000.
000.
00
329
1.3
234
21.3
413
1.9
832
1.05
141
1.3
310
11.4
355
1.3
50.7
70.8
0
90.
669
0.64
00.
002
1.08
30.
492
0.53
21.
05-0
.04
-0.0
5
441.
0645
1.06
10.
915
0.98
201.
1414
1.19
50.
720.
020.
02
280.
9829
0.99
11.
2911
3.0
69
0.73
70.
871
0.22
0.00
0.00
381.8
538
1.8
00
0.00
176.8
913
1.52
81.
360
0.00
0.1
70.1
6
421.3
943
1.3
91
1.25
61.
6221
1.6
611
1.28
40.
760.
110.
11
391.
3940
1.39
11.
346
1.74
201.7
09
1.13
40.
810.
100.
10
31.
433
1.39
00.
000
0.00
11.
142
3.37
00.
000.
010.
01
110.
8711
0.85
00.
000
0.00
30.
564
1.12
41.
89-0
.02
-0.0
2
341.5
034
1.4
60
0.00
51.
7919
1.9
49
1.38
10.
280.
110.
10
31.
014
1.30
110
.84
12.
361
0.72
11.
260
0.00
0.00
0.01
371.
1542
1.28
55.8
73
0.76
161.
1811
1.21
71.
290.
050.
08
151.
0917
1.20
25.
405
2.92
40.
692
0.51
41.
680.
010.
03
231.
1624
1.18
11.
823
1.19
121.
415
0.90
30.
920.
030.
03
111.
2911
1.25
00.
001
0.91
51.
362
0.84
32.
170.
020.
02
121.
2313
1.29
13.
782
1.63
71.
683
1.08
00.
000.
020.
03
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.01
-0.0
1
540.
9157
0.94
31.
909
1.10
240.
989
0.55
121.
21-0
.05
-0.0
3
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
EAR
EAR
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECONDCANCERSITE
18162
1860
118
601
1816
215
921
8507
3575
1816
218
601
105155
1082
2230
6614
166
4737
628
905
1470
810
5155
1082
22

MESOTHELIOMA
POOLAIRTUM1976-2010,MEN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
MESOTELIOMA
POOLAIRTUM1976-2010,UOMINI:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRSTCANCERSITE
MESOTHELIOMA
MEN
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
70 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
ALLSITES,BUTSKINANDMESOTHELIOMA
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
PROSTATE
TESTIS
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
580.6
576
0.7
418
1.28
240.5
529
0.77
50.
900
0.00
-6.7
5-5
.14
20.
512
0.44
00.
000
0.00
21.
200
0.00
00.
00-0
.42
-0.4
8
11.
071
0.93
00.
000
0.00
12.
530
0.00
00.
000.
01-0
.01
11.
141
0.99
00.
000
0.00
12.
670
0.00
00.
000.
030.
00
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.46
-0.4
7
11.
001
0.86
00.
000
0.00
12.
360
0.00
00.
000.
00-0
.03
71.
398
1.37
11.
212
0.80
52.
380
0.00
00.
000.
430.
41
70.
588
0.58
10.
534
0.68
20.
401
1.32
00.
00-1
.09
-1.1
2
50.
616
0.63
10.
773
0.74
10.
291
1.90
00.
00-0
.71
-0.6
7
20.
532
0.46
00.
001
0.54
10.
630
0.00
00.
00-0
.38
-0.4
4
00.0
00
0.0
00
0.00
00.
000
0.00
00.
000
0.00
-0.8
0-0
.81
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.20
-0.2
0
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.52
-0.5
3
40.2
513
0.71
93.5
53
0.38
10.1
50
0.00
00.
00-2
.55
-1.0
0
00.
001
0.67
15.
200
0.00
00.
000
0.00
00.
00-0
.28
-0.0
9
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.11
-0.1
1
15.
371
4.62
00.
000
0.00
112
.76
00.
000
0.00
0.18
0.15
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.07
-0.0
7
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.02
-0.0
2
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.04
-0.0
4
160.
9020
0.97
41.
448
0.92
50.
663
2.54
00.
00-0
.41
-0.1
2
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.02
-0.0
2
51.
767
2.13
24.
572
1.44
32.
490
0.00
00.
000.
470.
70
50.
515
0.44
00.
002
0.42
30.
730
0.00
00.
00-1
.03
-1.1
9
50.
545
0.46
00.
002
0.44
30.
770
0.00
00.
00-0
.93
-1.0
9
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.09
-0.0
9
21.
932
1.67
00.
000
0.00
24.
550
0.00
00.
000.
210.
15
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.09
-0.0
9
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.04
-0.0
4
10.
391
0.34
00.
001
0.80
00.
000
0.00
00.
00-0
.34
-0.3
7
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.25
-0.2
5
42.
044
1.75
00.
001
1.03
22.
431
8.31
00.
000.
440.
33
11.
041
0.90
00.
000
0.00
12.
470
0.00
00.
000.
01-0
.02
22.
272
1.96
00.
001
2.30
00.
001
18.3
60
0.00
0.24
0.18
18.
201
7.00
00.
000
0.00
119
.64
00.
000
0.00
0.19
0.16
30.
683
0.58
00.
001
0.46
21.
070
0.00
00.
00-0
.31
-0.4
1
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECONDCANCERSITE
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
EAR
EAR
3832
4368
4368
3832
1702
130
2838
3243
68
4605
5289
684
2208
1983
298
116
4605
5289

MESOTHELIOMA
POOLAIRTUM1976-2010,WOMEN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
MESOTELIOMA
POOLAIRTUM1976-2010,DONNE:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRSTCANCERSITE
MESOTHELIOMA
WOMEN
71 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
ALLSITES,BUTSKINANDMESOTHELIOMA
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
CERVIXUTERI
CORPUSUTERI
OVARY
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
251.
1929
1.20
41.
3211
1.17
121.
322
1.14
00.
001.
972.
16
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.14
-0.1
4
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.07
-0.0
7
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.03
-0.0
3
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.04
-0.0
4
220.1
62
17.4
90
0.00
00.
002
47.3
70
0.00
00.
000.
960.
84
10.
931
0.80
00.
000
0.00
12.
230
0.00
00.
00-0
.04
-0.1
1
20.
642
0.56
00.
001
0.71
10.
750
0.00
00.
00-0
.56
-0.7
0
20.
892
0.78
00.
001
0.98
11.
050
0.00
00.
00-0
.12
-0.2
5
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.44
-0.4
5
11.
841
1.60
00.
001
3.95
00.
000
0.00
00.
000.
230.
17
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.21
-0.2
1
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.40
-0.4
1
00.
001
0.64
15.
070
0.00
00.
000
0.00
00.
00-0
.69
-0.2
5
12.
481
2.19
00.
000
0.00
00.
001
27.7
90
0.00
0.30
0.24
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.03
-0.0
3
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.01
-0.0
1
111
.34
19.
930
0.00
125
.65
00.
000
0.00
00.
000.
460.
40
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.01
-0.0
1
30.
524
0.62
11.
302
0.81
10.
400
0.00
00.
00-1
.37
-1.1
1
26.
932
6.08
00.
001
7.92
17.
780
0.00
00.
000.
860.
74
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.53
-0.5
3
22.
933
3.86
110
.50
13.
331
3.36
00.
000
0.00
0.66
0.99
23.
843
5.0
51
13.5
10
0.00
28.
860
0.00
00.
000.
741.
07
11.
311
1.13
00.
001
2.85
00.
000
0.00
00.
000.
120.
05
11.
401
1.22
00.
001
3.06
00.
000
0.00
00.
000.
140.
08
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.03
-0.0
3
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.16
-0.1
6
12.
361
2.11
00.
000
0.00
15.
260
0.00
00.
000.
290.
23
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.03
-0.0
3
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.40
-0.4
1
12.
801
2.44
00.
000
0.00
00.
001
36.4
40
0.00
0.32
0.26
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.24
-0.2
5
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.11
-0.1
1
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.12
-0.1
2
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.02
-0.0
2
52.
865
2.47
00.
003
3.10
23.
410
0.00
00.
001.
311.
06
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
EAR
EAR
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECONDCANCERSITE
1466
1689
1689
1466
668
8118
1466
1689
1987
2251
264
848
886
181
7219
8722
51

KAPOSISARCOMA
POOLAIRTUM1976-2010,MEN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
SARCOMADIKAPOSI
POOLAIRTUM1976-2010,UOMINI:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRSTCANCERSITE
KAPOSISARCOMA
MEN
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
72 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
238
1.11
257
1.1
619
3.0
050
1.7
610
41.
0859
0.98
250.
832.
831.
88
70.
867
0.83
00.
001
0.88
41.
070
0.00
21.
88-0
.11
-0.1
0
21.
012
0.98
00.
000
0.00
11.
110
0.00
13.
800.
000.
00
21.
172
1.13
00.
001
4.23
00.
000
0.00
14.
440.
020.
02
30.
673
0.65
00.
000
0.00
31.
460
0.00
00.
00-0
.13
-0.1
2
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.18
-0.1
8
90.
6910
0.74
12.
493
1.68
20.
342
0.56
21.
18-0
.27
-0.3
3
341.
1637
1.22
33.
537
1.84
110.
8411
1.32
51.
190.
540.
38
160.
7917
0.81
11.
723
1.15
50.
565
0.86
31.
02-0
.31
-0.3
6
181.9
820
2.1
32
7.40
43.
316
1.47
62.
362
1.59
0.8
50.
74
121.
3713
1.44
13.
841
0.86
41.
016
2.45
10.
820.
320.
27
62.
356
2.29
00.
001
2.98
21.
753
4.21
00.
000.
270.
29
30.
493
0.48
00.
001
1.27
10.
370
0.00
11.
15-0
.26
-0.2
5
180.4
920
0.5
32
1.81
40.
818
0.4
95
0.50
10.
20-1
.40
-1.5
2
41.
315
1.60
111
.56
00.
002
1.50
22.
260
0.00
0.15
0.08
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.09
-0.0
9
11.
621
1.56
00.
000
0.00
00.
001
5.93
00.
000.
030.
03
33.
813
3.70
00.
001
9.55
00.
002
8.9
90
0.00
0.18
0.18
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.02
-0.0
2
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.04
-0.0
4
561.3
557
1.3
31
0.87
101.
9324
1.31
151.
267
1.13
1.14
1.20
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.04
-0.0
4
71.
129
1.40
211.1
01
1.24
31.
082
1.13
11.
130.
210.
06
190.
7819
0.76
00.
006
1.85
70.
643
0.44
30.
88-0
.49
-0.4
5
190.
8119
0.79
00.
006
1.93
70.
673
0.46
30.
92-0
.40
-0.3
6
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.09
-0.0
9
10.
411
0.40
00.
001
3.02
00.
000
0.00
00.
00-0
.12
-0.1
2
11.
011
0.98
00.
000
0.00
12.
290
0.00
00.
000.
000.
00
24.
262
4.11
00.
002
27.6
10
0.00
00.
000
0.00
0.12
0.13
304.9
334
5.4
34
22.0
59
11.1
217
6.2
44
2.34
00.
002.2
21.9
8
62.
037
2.30
111
.53
00.
006
4.5
50
0.00
00.
000.
320.
25
71.
317
1.28
00.
000
0.00
52.
081
0.67
11.
380.
120.
14
41.
594
1.54
00.
000
0.00
21.
751
1.43
12.
930.
110.
12
31.
263
1.23
00.
000
0.00
32.
820
0.00
00.
000.
040.
05
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.04
-0.0
4
131.
0716
1.28
38.4
02
1.25
71.
293
0.87
10.
580.
280.
07
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECONDCANCERSITE
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
EAR
EAR
ALLSITES,BUTSKINANDKAPOSISARCOMA
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
PROSTATE
TESTIS
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
2445
2605
2605
2445
1960
990
355
2445
2605
12085
1250
642
118
1855
7432
5014
4312
085
1250
6

KAPOSISARCOMA
POOLAIRTUM1976-2010,WOMEN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
SARCOMADIKAPOSI
POOLAIRTUM1976-2010,DONNE:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRSTCANCERSITE
KAPOSISARCOMA
WOMEN
73 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
601.
0366
1.09
63.1
810
1.18
281.
0114
0.90
81.
220.
351.
22
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.15
-0.1
5
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.09
-0.0
9
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.03
-0.0
3
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.03
-0.0
3
13.
141
3.04
00.
000
0.00
16.
540
0.00
00.
000.
150.
14
20.
492
0.48
00.
000
0.00
21.
020
0.00
00.
00-0
.45
-0.4
7
111.
1311
1.09
00.
004
2.85
40.
861
0.38
21.
810.
270.
20
91.
279
1.23
00.
002
1.97
41.
191
0.53
22.
480.
420.
36
20.
752
0.72
00.
002
5.10
00.
000
0.00
00.
00-0
.15
-0.1
6
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.42
-0.4
2
21.
272
1.23
00.
000
0.00
11.
331
2.41
00.
000.
090.
08
20.
722
0.70
00.
000
0.00
00.
002
2.66
00.
00-0
.17
-0.1
8
20.
573
0.82
18.
960
0.00
21.
200
0.00
00.
00-0
.34
-0.1
4
33.
344
4.3
21
35.2
31
7.89
00.
001
4.12
19.
640.
470.
66
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.03
-0.0
3
18.
341
8.05
00.
000
0.00
00.
001
32.7
70
0.00
0.19
0.19
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.05
-0.0
5
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.01
-0.0
1
131.
0415
1.16
24.
931
0.55
61.
014
1.21
21.
420.
120.
45
11.
541
1.49
00.
000
0.00
13.
170
0.00
00.
000.
080.
07
10.
451
0.44
00.
000
0.00
00.
000
0.00
14.
12-0
.27
-0.2
7
10.
591
0.57
00.
000
0.00
11.
240
0.00
00.
00-0
.15
-0.1
6
21.
552
1.50
00.
000
0.00
11.
640
0.00
16.
720.
160.
14
31.
233
1.19
00.
001
2.87
10.
871
1.53
00.
000.
130.
10
31.
333
1.29
00.
001
3.09
10.
931
1.65
00.
000.
160.
14
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.04
-0.0
4
11.
251
1.21
00.
000
0.00
00.
000
0.00
111
.17
0.04
0.04
11.
391
1.35
00.
000
0.00
00.
001
5.11
00.
000.
060.
06
18.
342
16.0
91
228.3
60
0.00
00.
001
33.1
50
0.00
0.19
0.40
62.8
96
2.8
00
0.00
13.
304
4.0
31
1.82
00.
000.
870.
82
10.
931
0.90
00.
000
0.00
11.
950
0.00
00.
00-0
.02
-0.0
2
10.
612
1.18
118
.59
00.
000
0.00
12.
300
0.00
-0.1
40.
06
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.16
-0.1
6
11.
331
1.29
00.
000
0.00
00.
001
5.00
00.
000.
060.
05
00.
001
5.65
1185.0
50
0.00
00.
000
0.00
00.
00-0
.04
0.18
50.
945
0.91
00.
002
2.64
31.
190
0.00
00.
00-0
.07
-0.1
0
ALLSITES,BUTSKINANDKAPOSISARCOMA
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
CERVIXUTERI
CORPUSUTERI
OVARY
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
EAR
EAR
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECONDCANCERSITE
904
950
950
904
756
377
130
904
950
4523
4677
154
683
2166
1186
488
4523
4677

SOFTTISSUE
POOLAIRTUM1976-2010,MEN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
TESSUTIMOLLI
POOLAIRTUM1976-2010,UOMINI:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRSTCANCERSITE
SOFTTISSUE
MEN
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
74 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
258
1.05
278
1.09
202.1
049
1.28
106
1.01
611.
0142
0.98
0.62
1.14
141.
3115
1.35
12.
404
2.35
61.
294
1.53
00.
000.
180.
20
31.
173
1.12
00.
001
2.49
21.
800
0.00
00.
000.
020.
02
20.
852
0.82
00.
001
2.71
00.
001
1.73
00.
00-0
.02
-0.0
2
91.
5710
1.68
14.
362
2.15
41.
603
2.15
00.
000.
180.
21
00.
001
0.36
19.
600
0.00
00.
000
0.00
00.
00-0
.14
-0.0
9
110.
7412
0.77
11.
632
0.82
60.
933
0.83
00.
00-0
.21
-0.1
8
411.
2243
1.23
21.
559
1.74
161.
1310
1.21
61.
020.
400.
42
251.
0927
1.13
22.
284
1.14
131.
345
0.88
30.
740.
110.
17
161.
5016
1.45
00.
005
3.00
30.
665
1.91
31.
650.
290.
26
60.
616
0.59
00.
002
1.31
10.
241
0.42
21.
19-0
.20
-0.2
2
20.
772
0.74
00.
000
0.00
00.
001
1.56
12.
25-0
.03
-0.0
4
30.
453
0.43
00.
001
0.97
10.
351
0.60
00.
00-0
.20
-0.2
0
300.
7133
0.75
31.
796
0.89
150.
833
0.2
96
0.86
-0.6
5-0
.56
30.
763
0.74
00.
000
0.00
21.
210
0.00
11.
40-0
.05
-0.0
6
32.
353
2.27
00.
001
5.26
23.
740
0.00
00.
000.
090.
09
35.1
23
4.93
00.
001
10.6
70
0.00
17.
051
10.3
30.
130.
12
11.
041
1.00
00.
000
0.00
00.
000
0.00
16.
150.
000.
00
310.9
33
10.5
20
0.00
00.
002
16.7
60
0.00
122
.59
0.15
0.14
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.03
-0.0
3
611.3
165
1.3
44
2.31
81.
1527
1.40
211.8
25
0.57
0.77
0.86
00.
001
1.26
137
.85
00.
000
0.00
00.
000
0.00
-0.0
40.
01
91.
1512
1.48
310.2
80
0.00
30.
902
1.03
42.
910.
060.
20
271.
0029
1.03
21.
884
0.94
80.
698
1.20
71.
51-0
.01
0.04
271.
0429
1.08
21.
964
0.98
80.
728
1.26
71.
580.
060.
11
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.06
-0.0
6
30.
983
0.94
00.
000
0.00
00.
001
1.34
23.
930.
00-0
.01
42.
844
2.75
00.
001
4.85
00.
001
2.83
28.
070.
140.
13
11.
381
1.33
00.
000
0.00
13.
140
0.00
00.
000.
010.
01
30.
413
0.39
00.
001
0.89
10.
320
0.00
10.
79-0
.23
-0.2
4
30.
923
0.89
00.
000
0.00
10.
720
0.00
23.
57-0
.01
-0.0
2
81.
3710
1.65
28.
574
4.3
03
1.20
00.
001
1.03
0.12
0.20
31.
075
1.71
217.7
72
4.45
10.
830
0.00
00.
000.
010.
11
51.
925
1.85
00.
002
4.86
21.
800
0.00
12.
260.
130.
12
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.02
-0.0
2
201.
5420
1.48
00.
005
2.45
111.
994
1.25
00.
000.
380.
34
ALLSITES,BUTSKINANDSOFTTISSUE
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
PROSTATE
TESTIS
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECONDCANCERSITE
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
EAR
EAR
3994
4303
4303
3994
3106
1374
584
3994
4303
18554
1924
469
129
2881
8445
6928
7218
554
1924
4

SOFTTISSUE
POOLAIRTUM1976-2010,WOMEN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
TESSUTIMOLLI
POOLAIRTUM1976-2010,DONNE:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRSTCANCERSITE
SOFTTISSUE
WOMEN
75 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
159
1.13
170
1.17
112.1
728
1.35
671.
1637
1.01
271.
041.
091.
40
10.
551
0.53
00.
000
0.00
11.
340
0.00
00.
00-0
.05
-0.0
5
11.
051
1.01
00.
000
0.00
12.
590
0.00
00.
000.
000.
00
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.03
-0.0
3
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.03
-0.0
3
11.
541
1.48
00.
001
10.2
60
0.00
00.
000
0.00
0.02
0.02
81.
038
0.99
00.
001
0.82
30.
941
0.50
32.
150.
01-0
.01
200.
9620
0.93
00.
001
0.33
91.
072
0.37
82.
05-0
.05
-0.0
9
140.
9414
0.90
00.
000
0.00
71.
171
0.26
62.
12-0
.06
-0.0
9
61.
026
0.98
00.
001
1.13
20.
831
0.65
21.
850.
01-0
.01
10.
291
0.28
00.
000
0.00
00.
000
0.00
11.
54-0
.15
-0.1
5
10.
361
0.35
00.
000
0.00
00.
000
0.00
11.
96-0
.11
-0.1
1
20.
382
0.36
00.
000
0.00
10.
481
0.72
00.
00-0
.20
-0.2
0
171.9
718
2.0
21
3.32
32.
436
1.73
73.1
01
0.60
0.50
0.52
41.
387
2.33
330.5
13
7.2
40
0.00
00.
001
1.86
0.07
0.23
12.
741
2.65
00.
000
0.00
16.
850
0.00
00.
000.
040.
04
00.
001
5.47
1145.1
40
0.00
00.
000
0.00
00.
00-0
.01
0.05
11.
611
1.55
00.
001
10.6
70
0.00
00.
000
0.00
0.02
0.02
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.01
-0.0
1
501.
3253
1.3
63
2.28
112.
0117
1.09
161.
636
0.88
0.73
0.80
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.13
-0.1
3
71.
078
1.18
14.
321
1.04
31.
103
1.77
00.
000.
030.
07
51.
115
1.07
00.
001
1.48
21.
060
0.00
22.
500.
030.
02
72.
117
2.04
00.
001
2.09
10.
743
3.45
23.
170.
220.
21
50.
995
0.95
00.
000
0.00
52.
460
0.00
00.
000.
00-0
.01
40.
854
0.82
00.
000
0.00
42.
110
0.00
00.
00-0
.04
-0.0
5
12.
821
2.72
00.
000
0.00
17.
130
0.00
00.
000.
040.
04
10.
482
0.93
113
.46
00.
001
1.16
00.
000
0.00
-0.0
6-0
.01
51.
576
1.83
19.
781
2.26
21.
511
1.20
11.
730.
110.
16
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.03
-0.0
3
71.
347
1.30
00.
000
0.00
62.8
21
0.74
00.
000.
110.
09
41.
724
1.66
00.
000
0.00
44.2
30
0.00
00.
000.
100.
09
51.
475
1.42
00.
001
1.95
21.
442
2.28
00.
000.
100.
09
21.
342
1.29
00.
000
0.00
11.
631
2.61
00.
000.
030.
03
31.
843
1.78
00.
001
4.15
11.
511
2.36
00.
000.
080.
08
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.02
-0.0
2
70.
617
0.59
00.
003
1.36
30.
760
0.00
10.
53-0
.23
-0.2
4
ALLSITES,BUTSKINANDSOFTTISSUE
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
CERVIXUTERI
CORPUSUTERI
OVARY
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
EAR
EAR
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECONDCANCERSITE
3458
3714
3714
3458
2711
1213
560
3458
3714
16709
1730
659
725
4071
9942
5027
2016
709
1730
6

ALLSITES,BUTSKINANDBONE
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
PROSTATE
TESTIS
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
BONE
POOLAIRTUM1976-2010,MEN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
OSSO
POOLAIRTUM1976-2010,UOMINI:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRSTCANCERSITE
BONE
MEN
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
651.
0668
1.06
31.
1911
1.19
210.
8317
1.06
161.
480.
460.
51
41.
414
1.35
00.
001
2.28
21.
661
1.38
00.
000.
150.
13
22.
942
2.83
00.
001
9.71
13.
510
0.00
00.
000.
170.
16
11.
561
1.50
00.
000
0.00
00.
001
6.13
00.
000.
050.
04
10.
661
0.63
00.
000
0.00
11.
540
0.00
00.
00-0
.07
-0.0
7
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.09
-0.0
9
41.
094
1.05
00.
001
1.68
10.
650
0.00
23.
390.
050.
02
30.
373
0.35
00.
000
0.00
10.
301
0.46
10.
68-0
.68
-0.7
0
20.
362
0.35
00.
000
0.00
00.
001
0.69
11.
01-0
.46
-0.4
7
10.
371
0.36
00.
000
0.00
10.
900
0.00
00.
00-0
.22
-0.2
3
10.
421
0.41
00.
000
0.00
00.
000
0.00
12.
46-0
.18
-0.1
9
23.
342
3.19
00.
000
0.00
00.
001
6.53
19.
880.
180.
17
10.
631
0.61
00.
000
0.00
00.
000
0.00
13.
62-0
.08
-0.0
8
90.
869
0.83
00.
001
0.62
51.
140
0.00
31.
76-0
.18
-0.2
3
21.
782
1.72
00.
000
0.00
00.
002
6.64
00.
000.
110.
11
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.04
-0.0
4
16.
781
6.50
00.
000
0.00
116
.14
00.
000
0.00
0.11
0.11
13.
731
3.60
00.
000
0.00
19.
070
0.00
00.
000.
100.
09
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.01
-0.0
1
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.02
-0.0
2
110.
9912
1.04
12.
332
1.28
00.0
06
2.02
31.
41-0
.02
0.05
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.06
-0.0
6
31.
473
1.42
00.
002
6.89
11.
200
0.00
00.
000.
130.
11
131.9
714
2.0
31
3.58
21.
975
1.82
52.
921
0.88
0.84
0.90
132.0
514
2.1
11
3.73
22.
065
1.89
53.
051
0.92
0.87
0.94
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.03
-0.0
3
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.12
-0.1
2
12.
141
2.08
00.
001
16.8
30
0.00
00.
000
0.00
0.07
0.07
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.04
-0.0
4
31.
543
1.49
00.
000
0.00
22.
500
0.00
12.
850.
140.
12
11.
281
1.23
00.
000
0.00
13.
080
0.00
00.
000.
030.
02
32.
053
1.97
00.
000
0.00
11.
631
2.67
14.
100.
200.
19
22.
842
2.72
00.
000
0.00
00.
001
5.62
18.
730.
170.
16
11.
521
1.46
00.
000
0.00
13.
660
0.00
00.
000.
040.
04
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.01
-0.0
1
20.
653
0.94
17.
591
2.10
00.
000
0.00
11.
92-0
.14
-0.0
2
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECONDCANCERSITE
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
EAR
EAR
76 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
1567
1692
1692
1567
1212
562
248
1567
1692
7618
7890
272
1140
3220
1948
1310
7618
7890

ALLSITES,BUTSKINANDBONE
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
CERVIXUTERI
CORPUSUTERI
OVARY
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
BONE
POOLAIRTUM1976-2010,WOMEN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
OSSO
POOLAIRTUM1976-2010,DONNE:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRSTCANCERSITE
BONE
WOMEN
1240
1327
1327
1240
969
490
241
1240
1327
6647
6861
214
917
2714
1748
1268
6647
6861
541.4
156
1.4
12
1.46
71.
3115
0.99
181.7
614
1.8
42.
372.
39
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.07
-0.0
7
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.04
-0.0
4
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.02
-0.0
2
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.02
-0.0
2
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.02
-0.0
2
31.
523
1.46
00.
001
3.25
00.
002
3.91
00.
000.
150.
14
61.
126
1.08
00.
000
0.00
20.
943
2.13
10.
970.
100.
07
61.
586
1.52
00.
000
0.00
21.
333
2.99
11.
350.
330.
30
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.23
-0.2
3
11.
172
2.24
128
.95
00.
000
0.00
14.
500
0.00
0.02
0.16
11.
441
1.38
00.
000
0.00
13.
540
0.00
00.
000.
050.
04
10.
771
0.74
00.
000
0.00
11.
960
0.00
00.
00-0
.05
-0.0
5
31.
363
1.31
00.
000
0.00
22.
330
0.00
12.
190.
120.
10
33.
233
3.13
00.
001
8.75
00.
001
3.95
14.
640.
310.
30
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.01
-0.0
1
122
.27
121
.41
00.
000
0.00
00.
001
85.4
10
0.00
0.14
0.14
15.
491
5.31
00.
000
0.00
00.
001
20.7
20
0.00
0.12
0.12
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.01
-0.0
1
100.
9311
0.99
12.
832
1.39
30.
721
0.34
41.
81-0
.11
-0.0
1
23.
082
2.98
00.
000
0.00
00.
001
5.90
18.
070.
200.
19
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.27
-0.2
7
21.
582
1.52
00.
000
0.00
11.
971
2.96
00.
000.
110.
10
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.13
-0.1
3
43.
114
3.00
00.
001
5.41
23.
930
0.00
13.
980.
410.
39
43.
344
3.22
00.
001
5.80
24.
220
0.00
14.
260.
420.
40
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.01
-0.0
1
23.
392
3.28
00.
000
0.00
00.
001
6.52
18.
690.
210.
20
65.3
86
5.2
30
0.00
00.
001
2.43
26.
483
11.3
60.
730.
71
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.03
-0.0
3
10.
701
0.68
00.
000
0.00
00.
001
2.63
00.
00-0
.06
-0.0
7
11.
691
1.63
00.
001
11.6
90
0.00
00.
000
0.00
0.06
0.06
55.4
95
5.2
90
0.00
17.
402
5.44
14.
211
5.88
0.62
0.59
37.5
63
7.2
70
0.00
00.
002
12.2
61
9.77
00.
000.
390.
38
12.
261
2.18
00.
000
0.00
00.
000
0.00
111
.44
0.08
0.08
114
.20
113
.62
00.
001
90.6
60
0.00
00.
000
0.00
0.14
0.14
10.
401
0.38
00.
000
0.00
00.
001
1.51
00.
00-0
.23
-0.2
3
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
EAR
EAR
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECONDCANCERSITE
77 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so

ALLSITES,BUTSKINANDKIDNEYANDRENALPELVIS
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
PROSTATE
TESTIS
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
KIDNEYANDRENALPELVIS
POOLAIRTUM1976-2010,MEN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
RENEEPELVIRENALE
POOLAIRTUM1976-2010,UOMINI:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRSTCANCERSITE
KIDNEY
ANDRENALPELVIS
MEN
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
2476
1.1
430
791.3
760
37.6
842
41.3
310
971.1
365
61.1
129
91.
012.6
26.9
2
910.
9796
0.99
51.
3714
0.94
430.
9922
0.91
121.
12-0
.02
-0.0
1
241.
0925
1.09
11.
186
1.73
90.
886
1.04
31.
160.
020.
02
211.
0521
1.01
00.
001
0.31
101.
067
1.35
31.
330.
010.
00
460.
9050
0.94
41.
987
0.85
241.
009
0.68
61.
02-0
.05
-0.0
3
90.3
817
0.69
88.9
01
0.27
50.
463
0.48
00.
00-0
.13
-0.0
6
121
0.91
129
0.94
81.
5824
1.20
490.
8334
0.96
140.
81-0
.10
-0.0
7
325
1.06
336
1.06
111.
0140
0.90
145
1.07
101
1.20
390.
900.
160.
15
243
1.1
525
41.1
611
1.49
290.
9610
71.
1676
1.3
131
1.03
0.28
0.30
820.
8582
0.82
00.
0011
0.77
380.
8825
0.95
80.
62-0
.13
-0.1
5
680.7
691
0.98
237.0
89
0.68
230.5
719
0.79
171.
43-0
.19
-0.0
1
180.
7818
0.75
00.
004
1.19
90.
894
0.63
10.
30-0
.04
-0.0
5
711.
1875
1.20
41.
8611
1.26
250.
9422
1.34
131.
540.
090.
11
357
0.91
476
1.1
711
98.1
439
0.6
615
90.
9010
81.
0351
1.00
-0.3
00.5
9
501.5
455
1.6
35
4.4
513
2.7
821
1.46
141.
572
0.44
0.15
0.1
8
151.
2518
1.46
37.2
53
1.76
50.
956
1.83
10.
590.
030.
05
20.
453
0.64
15.
920
0.00
10.
500
0.00
11.
66-0
.02
-0.0
1
91.
1614
1.75
517.8
61
0.87
51.
453
1.43
00.
000.
010.
05
21.
002
0.97
00.
000
0.00
11.
101
1.91
00.
000.
000.
00
81.
688
1.62
00.
000
0.00
52.
352
1.54
11.
540.
030.
03
670
1.5
087
21.8
920
213.4
413
82.2
428
41.4
616
91.3
579
1.22
1.9
53.4
5
51.
836
2.11
18.
881
2.13
32.
270
0.00
13.
650.
020.
03
30.0
435
0.4
732
12.5
01
0.1
01
0.0
31
0.0
50
0.0
0-0
.60
-0.3
3
323
1.3
147
91.8
715
617.3
882
2.2
515
41.4
061
0.91
260.
770.6
61.8
7
313
1.3
345
91.8
814
616.9
981
2.3
314
91.4
259
0.92
240.
750.6
71.8
0
100.
9420
1.8
210
26.0
71
0.65
51.
072
0.69
21.
33-0
.01
0.08
250.
9725
0.93
00.
005
1.27
100.
855
0.73
51.
54-0
.01
-0.0
1
252.3
628
2.5
63
7.9
42
1.26
132.7
15
1.75
53.7
40.1
30.1
4
40.
898
1.71
422.5
82
2.76
10.
481
0.86
00.
000.
000.
03
811.2
789
1.3
58
3.4
99
0.96
401.4
121
1.22
111.
290.
150.
19
381.
3142
1.4
04
3.8
15
1.18
171.
339
1.14
71.
740.
080.
10
581.
1776
1.4
818
9.8
07
0.95
301.
3616
1.19
50.
750.
070.2
1
200.
8437
1.4
917
19.0
54
1.11
70.
657
1.09
20.
64-0
.03
0.10
361.6
037
1.5
91
1.23
30.
9222
2.2
28
1.30
30.
950.
120.
12
20.
612
0.58
00.
000
0.00
10.
681
1.14
00.
00-0
.01
-0.0
1
101
0.89
116
0.99
153.6
614
0.85
490.
9930
0.97
80.5
0-0
.10
-0.0
1
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECONDCANCERSITE
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
EAR
EAR
78 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
25527
2834
428
344
2552
719
549
9127
3422
2552
728
344
114765
1192
2344
5718
399
5359
329
666
1310
811
4765
1192
23

ALLSITES,BUTSKINANDKIDNEYANDRENALPELVIS
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
CERVIXUTERI
CORPUSUTERI
OVARY
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
KIDNEYANDRENALPELVIS
POOLAIRTUM1976-2010,WOMEN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
RENEEPELVIRENALE
POOLAIRTUM1976-2010,DONNE:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRSTCANCERSITE
KIDNEY
ANDRENALPELVIS
WOMEN
858
1.1
510
581.3
720
07.4
916
11.4
936
11.
1021
91.
0711
71.
131.6
84.0
9
30.3
14
0.40
12.
891
0.71
10.
231
0.38
00.
00-0
.10
-0.0
9
20.
382
0.37
00.
001
1.35
00.
001
0.69
00.
00-0
.05
-0.0
5
10.
481
0.46
00.
000
0.00
11.
060
0.00
00.
00-0
.02
-0.0
2
00.
001
0.41
111
.62
00.
000
0.00
00.
000
0.00
-0.0
3-0
.02
10.
271
0.26
00.
001
1.88
00.
000
0.00
00.
00-0
.04
-0.0
4
300.6
834
0.74
42.
383
0.46
130.
6710
0.83
40.
65-0
.21
-0.1
7
136
1.15
139
1.13
30.
7123
1.36
551.
0735
1.06
231.
350.
260.
23
981.
1510
01.
132
0.66
181.
4837
1.00
271.
1416
1.29
0.19
0.17
381.
1539
1.13
10.
835
1.04
181.
248
0.87
71.
510.
070.
07
200.
9733
1.5
513
17.6
54
1.36
70.
785
0.87
41.
33-0
.01
0.17
50.3
17
0.4
22
3.36
00.
003
0.43
20.
450
0.00
-0.1
6-0
.14
461.4
947
1.4
71
0.92
71.
629
0.68
141.
6116
3.4
00.
220.
21
641.3
087
1.7
123
13.5
115
2.1
729
1.36
141.
026
0.83
0.22
0.5
1
171.
2320
1.40
36.2
32
1.01
101.
634
1.05
10.
520.
050.
08
10.
481
0.46
00.
000
0.00
11.
100
0.00
00.
00-0
.02
-0.0
2
11.
001
0.97
00.
000
0.00
00.
001
3.64
00.
000.
000.
00
103.1
713
3.9
73
26.7
21
2.19
53.6
03
3.45
12.
250.
100.1
4
11.
171
1.13
00.
000
0.00
00.
001
4.28
00.
000.
000.
00
211
1.11
280
1.4
269
10.0
842
1.4
988
1.03
571.
1024
0.95
0.30
1.1
7
90.
9410
1.01
12.
674
2.62
30.
682
0.80
00.
00-0
.01
0.00
401.
1552
1.4
412
9.5
23
0.58
251.5
95
0.53
71.
550.
080.
23
200.
8521
0.86
11.
161
0.28
100.
956
0.94
30.
96-0
.05
-0.0
5
10.0
54
0.2
13
4.57
10.
370
0.0
00
0.0
00
0.00
-0.2
6-0
.22
762.6
110
93.6
133
31.8
822
5.3
138
3.0
112
1.48
40.
940.6
91.1
2
752.7
710
73.8
232
33.2
421
5.4
538
3.2
312
1.59
41.
020.7
11.1
2
10.
492
0.94
113
.75
13.
470
0.00
00.
000
0.00
-0.0
20.
00
110.
9811
0.95
00.
001
0.62
30.
615
1.63
21.
290.
00-0
.01
372.8
140
2.9
33
6.6
24
2.09
142.3
613
3.6
16
3.4
40.3
50.3
8
10.
562
1.08
114
.81
00.
001
1.24
00.
000
0.00
-0.0
10.
00
371.
2942
1.4
15
4.9
26
1.45
120.
9516
2.0
23
0.75
0.12
0.18
120.
9014
1.01
24.
175
2.59
61.
030
0.0
01
0.53
-0.0
20.
00
221.
1826
1.34
45.8
72
0.74
101.
226
1.16
41.
520.
050.
09
101.
2213
1.52
39.8
11
0.82
51.
373
1.33
10.
900.
030.
06
91.
0110
1.09
13.
151
0.79
41.
032
0.81
21.
550.
000.
01
31.
923
1.85
00.
000
0.00
11.
491
2.30
14.
360.
020.
02
470.
8563
1.10
168.0
414
1.79
180.
767
0.4
68
0.97
-0.1
20.
08
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
EAR
EAR
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECONDCANCERSITE
79 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
14286
1580
615
806
1428
610
970
5379
2188
1428
615
806
67755
7025
324
9810
298
3073
518
080
8642
6775
570
253

ALLSITES,BUTBLADDERANDURINARYTRACT
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
PROSTATE
TESTIS
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
BLADDERANDURINARYTRACT
POOLAIRTUM1976-2010,MEN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
VESCICAEVIEURINARIE
POOLAIRTUM1976-2010,UOMINI:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRSTCANCERSITE
BLADDERAND
URINARYTRACT
MEN
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
1128
11.2
812
517
1.3
812
364.2
020
721.6
248
331.2
129
331.2
514
431.2
75.7
97.7
0
537
1.4
355
41.4
217
1.26
881.5
025
31.4
213
71.4
259
1.3
90.3
70.3
7
110
1.2
611
41.2
64
1.30
171.
2753
1.30
271.
1913
1.28
0.05
0.05
941.2
498
1.2
54
1.47
161.
3549
1.3
620
1.03
91.
060.
040.
04
333
1.5
734
21.5
59
1.17
551.6
415
11.5
090
1.6
537
1.5
50.2
80.2
7
115
1.15
122
1.18
72.
0117
1.13
491.
0638
1.4
611
0.90
0.04
0.04
578
0.94
598
0.94
200.
9371
0.7
726
60.
9416
81.
0473
0.96
-0.0
8-0
.09
1416
1.04
1476
1.05
601.3
319
40.
9961
81.
0038
81.
0521
61.1
90.
120.
15
988
1.05
1028
1.06
401.
3012
40.
9344
91.
0626
31.
0315
21.2
00.
110.
13
428
1.01
448
1.02
201.
3970
1.12
169
0.87
125
1.10
641.
180.
010.
02
424
1.08
442
1.09
181.
3456
0.96
185
1.02
126
1.2
157
1.14
0.07
0.08
104
0.94
108
0.95
41.
0823
1.43
480.
9624
0.81
90.
62-0
.01
-0.0
1
306
1.1
431
81.1
512
1.34
461.
1914
41.1
972
1.00
441.
240.
090.
09
3147
1.8
234
871.9
534
05.7
037
81.4
614
071.7
692
02.0
244
22.0
63.2
93.8
0
145
1.14
157
1.1
912
2.9
617
0.95
691.
2040
1.15
191.
080.
040.
06
490.
9953
1.03
42.
514
0.57
241.
0713
0.96
81.
190.
000.
00
130.
6214
0.65
11.
371
0.32
80.
833
0.55
10.
38-0
.02
-0.0
2
431.
3143
1.26
00.
008
1.67
140.
9312
1.36
92.
090.
020.
02
131.
5313
1.48
00.
001
0.75
71.
764
1.83
11.
010.
010.
01
261.
2527
1.25
11.
434
1.32
151.
577
1.25
00.
000.
010.
01
2703
1.3
933
141.6
561
19.8
488
93.2
710
111.1
653
30.
9927
01.
011.7
52.9
2
121.
3817
1.8
95
15.7
72
1.44
71.
692
0.91
11.
060.
010.
02
371
1.2
642
71.4
056
5.7
710
92.5
611
40.
8595
1.20
531.3
80.1
80.2
8
135
0.1
217
80.1
543
1.13
370.2
257
0.1
126
0.0
915
0.1
0-2
.28
-2.1
9
830.0
811
50.1
032
0.88
310.2
037
0.0
88
0.0
37
0.0
5-2
.29
-2.2
2
521.
0863
1.26
116.8
76
0.86
200.
9218
1.38
81.
240.
010.
03
850.8
087
0.7
92
0.54
90.
5635
0.7
130
1.07
110.
84-0
.05
-0.0
5
411.
0642
1.05
10.
781
0.1
821
1.18
90.
8710
2.08
0.01
0.00
181.
0419
1.06
11.
590
0.00
111.
345
1.12
21.
000.
000.
00
263
0.97
274
0.98
111.
2230
0.76
135
1.09
630.
8735
1.00
-0.0
2-0
.01
138
1.05
144
1.06
61.
3619
0.99
631.
0637
1.05
191.
110.
020.
02
265
1.1
627
21.1
57
0.89
361.
0612
51.
2075
1.24
291.
000.
090.
08
102
0.94
107
0.96
51.
3312
0.74
521.
0426
0.91
120.
89-0
.01
-0.0
1
147
1.4
314
81.3
91
0.29
231.
5367
1.4
442
1.5
215
1.11
0.1
00.0
9
160.
9417
0.96
11.
611
0.38
60.
767
1.58
20.
980.
000.
00
469
0.9
050
90.
9440
2.2
769
0.90
204
0.8
613
20.
9464
0.92
-0.1
3-0
.07
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECONDCANCERSITE
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
EAR
EAR
80 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
89641
9500
595
005
8964
173
015
3445
412
760
8964
195
005
431215
4466
0115
386
6721
320
3505
1111
5449
343
4312
1544
6601

ALLSITES,BUTBLADDERANDURINARYTRACT
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
CERVIXUTERI
CORPUSUTERI
OVARY
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
BLADDERANDURINARYTRACT
POOLAIRTUM1976-2010,WOMEN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
VESCICAEVIEURINARIE
POOLAIRTUM1976-2010,DONNE:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRSTCANCERSITE
BLADDERAND
URINARYTRACT
WOMEN
1585
1.2
117
491.2
916
43.5
522
81.1
869
61.1
843
01.2
023
11.3
22.5
13.4
8
271.6
027
1.5
50
0.00
41.
6115
1.9
85
1.09
31.
350.
090.
09
90.
959
0.92
00.
001
0.73
40.
952
0.77
21.
540.
00-0
.01
82.3
68
2.28
00.
001
1.94
53.2
11
1.11
12.
400.
040.
04
102.5
110
2.4
20
0.00
23.
346
3.3
12
1.88
00.
000.
060.
05
131.
8213
1.76
00.
001
0.95
72.
212
1.03
33.
090.
050.
05
800.
8981
0.87
10.
3012
0.88
390.
9721
0.87
80.
69-0
.09
-0.1
1
216
0.97
229
0.99
131.
6735
1.08
930.
9454
0.89
341.
12-0
.06
-0.0
1
165
1.03
176
1.06
111.
9624
1.03
791.
1142
0.95
200.
900.
040.
09
510.
8353
0.83
20.
9111
1.20
140.5
112
0.72
141.
72-0
.10
-0.1
0
431.
0945
1.10
21.
442
0.34
201.
1413
1.20
81.
490.
030.
04
270.
8428
0.84
10.
863
0.63
130.
917
0.81
40.
94-0
.05
-0.0
5
831.3
885
1.3
72
0.97
121.
4035
1.34
171.
0219
2.2
10.
210.
21
242
2.7
628
43.1
342
14.2
229
2.3
210
72.7
769
2.8
437
3.0
11.4
31.7
3
251.
1028
1.20
33.
900
0.00
111.
0911
1.77
30.
980.
020.
04
41.
124
1.08
00.
000
0.00
10.
632
2.01
11.
970.
000.
00
31.
463
1.41
00.
001
3.30
00.
001
1.79
13.
560.
010.
01
132.3
516
2.8
03
15.7
72
2.49
72.8
52
1.32
22.
670.
070.0
9
32.
003
1.93
00.
001
4.34
11.
481
2.48
00.
000.
010.
01
363
1.1
538
81.1
925
2.2
742
0.89
158
1.11
105
1.2
358
1.4
30.
440.5
5
241.
5142
2.5
518
29.9
77
2.7
610
1.35
61.
461
0.55
0.08
0.2
3
560.
9883
1.4
127
13.3
911
1.27
220.
8418
1.18
50.
71-0
.01
0.2
1
431.
0645
1.07
21.
395
0.82
231.
2510
0.91
50.
960.
020.
03
491.4
957
1.6
88
7.2
310
2.1
321
1.44
90.
999
1.98
0.15
0.2
1
260.4
742
0.7
416
8.3
311
1.37
60.2
57
0.4
62
0.2
6-0
.27
-0.1
3
190.3
734
0.6
415
8.4
211
1.48
40.1
83
0.2
11
0.1
4-0
.30
-0.1
7
71.
748
1.92
17.
200
0.00
21.
144
3.60
11.
730.
030.
03
190.
9920
1.00
11.
513
1.06
70.
818
1.52
10.
390.
000.
00
251.
3026
1.31
11.
543
1.06
171.9
53
0.58
20.
820.
050.
06
51.
735
1.66
00.
001
2.21
21.
492
2.64
00.
000.
020.
02
541.
0757
1.09
31.
716
0.81
180.
7917
1.23
131.9
20.
030.
04
210.
8523
0.90
22.
305
1.37
100.
915
0.74
10.
30-0
.03
-0.0
2
320.
9032
0.87
00.
005
0.95
120.
7613
1.34
20.
42-0
.03
-0.0
4
100.
6310
0.61
00.
003
1.26
30.
423
0.71
10.
49-0
.05
-0.0
6
201.
2020
1.16
00.
002
0.83
81.
099
1.97
10.
440.
030.
03
20.
612
0.59
00.
000
0.00
10.
691
1.11
00.
00-0
.01
-0.0
1
115
1.05
125
1.10
102.5
828
1.7
547
0.98
290.
9611
0.71
0.05
0.10
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
EAR
EAR
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECONDCANCERSITE
81 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
22375
2406
824
068
2237
517
595
8675
3362
2237
524
068
107708
1115
7338
6516
453
4936
528
631
1325
910
7708
1115
73

ALLSITES,BUTURINARYBLADDER
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
PROSTATE
TESTIS
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
URINARYBLADDER
POOLAIRTUM1976-2010,MEN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
VESCICA
POOLAIRTUM1976-2010,UOMINI:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRSTCANCERSITE
URINARYBLADDER
MEN
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
1103
01.2
912
228
1.3
911
984.2
220
301.6
447
071.2
128
741.2
514
191.2
85.9
77.8
8
526
1.4
554
31.4
417
1.31
871.5
424
51.4
313
61.4
558
1.4
00.3
90.3
9
108
1.2
811
21.2
84
1.35
171.
3252
1.32
261.
1913
1.32
0.06
0.06
921.2
696
1.2
74
1.54
161.
4047
1.35
201.
069
1.09
0.04
0.05
326
1.5
833
51.5
79
1.22
541.6
714
61.5
090
1.7
036
1.5
50.2
90.2
8
113
1.17
119
1.19
61.
8016
1.10
491.
0937
1.4
711
0.93
0.04
0.04
563
0.95
580
0.94
170.
8270
0.7
825
40.
9316
81.
0771
0.96
-0.0
7-0
.08
1364
1.03
1422
1.04
581.3
418
70.
9959
51.
0037
21.
0421
01.1
90.
110.
14
954
1.05
992
1.06
381.
2911
90.
9343
21.
0625
51.
0314
81.2
00.
110.
13
410
1.00
430
1.01
201.
4568
1.13
163
0.86
117
1.06
621.
180.
000.
01
409
1.07
425
1.08
161.
2456
0.99
174
0.99
122
1.2
157
1.18
0.07
0.07
100
0.94
104
0.94
41.
1220
1.29
480.
9924
0.84
80.
57-0
.02
-0.0
1
300
1.1
631
21.1
712
1.40
461.
2314
11.2
071
1.02
421.
220.
100.
10
3074
1.8
434
041.9
733
05.7
737
01.4
813
731.7
889
62.0
343
52.0
93.3
63.8
7
141
1.14
153
1.2
012
3.0
817
0.99
671.
2139
1.15
181.
060.
040.
06
491.
0253
1.07
42.
624
0.59
241.
1113
1.00
81.
230.
000.
01
120.
5913
0.62
11.
421
0.33
80.
862
0.38
10.
39-0
.02
-0.0
2
421.
3242
1.28
00.
008
1.73
140.
9711
1.29
92.
160.
020.
02
121.
4612
1.41
00.
001
0.78
71.
823
1.42
11.
040.
010.
01
261.
2927
1.29
11.
494
1.37
151.
637
1.29
00.
000.
010.
01
2625
1.3
932
121.6
558
79.8
687
13.3
397
71.1
651
60.
9926
11.
011.7
72.9
3
121.
4317
1.9
65
16.4
22
1.50
71.
742
0.95
11.
100.
010.
02
366
1.2
941
61.4
150
5.3
710
52.5
711
30.
8795
1.2
453
1.4
30.1
90.2
8
850.0
812
00.1
135
0.96
210.1
329
0.0
624
0.0
811
0.0
8-2
.39
-2.3
1
330.0
357
0.0
524
0.69
150.1
09
0.0
26
0.0
23
0.0
2-2
.40
-2.3
4
521.
1263
1.3
111
7.2
06
0.90
200.
9518
1.43
81.
280.
010.
03
840.
8186
0.8
02
0.57
90.
5835
0.73
291.
0611
0.87
-0.0
5-0
.05
381.
0239
1.01
10.
811
0.18
191.
108
0.80
102.1
50.
000.
00
181.
0719
1.09
11.
660
0.00
111.
395
1.16
21.
030.
000.
00
250
0.96
261
0.97
111.
2828
0.74
126
1.06
620.
8934
1.00
-0.0
3-0
.02
134
1.06
140
1.07
61.
4218
0.98
601.
0437
1.09
191.
140.
020.
02
256
1.1
626
31.1
57
0.93
341.
0412
31.2
271
1.21
281.
000.
090.
08
100
0.96
105
0.97
51.
3911
0.70
511.
0626
0.94
120.
92-0
.01
-0.0
1
140
1.4
114
11.3
71
0.30
221.
5266
1.4
638
1.4
214
1.07
0.1
00.0
9
160.
9717
1.00
11.
681
0.39
60.
787
1.63
21.
010.
000.
00
464
0.92
503
0.96
392.3
169
0.94
202
0.88
130
0.96
630.
93-0
.10
-0.0
5
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECONDCANCERSITE
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
EAR
EAR
82 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
86278
9120
891
208
8627
870
523
3337
512
352
8627
891
208
417343
4321
3514
792
6483
319
6924
1076
8447
901
4173
4343
2135

ALLSITES,BUTURINARYBLADDER
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
CERVIXUTERI
CORPUSUTERI
OVARY
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
URINARYBLADDER
POOLAIRTUM1976-2010,WOMEN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
VESCICA
POOLAIRTUM1976-2010,DONNE:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRSTCANCERSITE
URINARYBLADDER
WOMEN
1531
1.2
216
861.3
015
53.5
921
71.1
867
01.1
942
11.2
222
31.3
22.6
53.6
1
261.6
226
1.5
60
0.00
41.
7015
2.0
85
1.14
20.
940.
100.
09
80.
898
0.86
00.
001
0.77
41.
002
0.80
10.
80-0
.01
-0.0
1
82.4
78
2.3
90
0.00
12.
055
3.3
71
1.16
12.
500.
050.
04
102.6
310
2.5
40
0.00
23.
536
3.4
72
1.96
00.
000.
060.
06
131.9
113
1.85
00.
001
1.01
72.
322
1.07
33.
220.
060.
06
760.
8977
0.87
10.
3211
0.86
370.
9720
0.87
80.
72-0
.09
-0.1
1
201
0.95
213
0.97
121.
6532
1.04
860.
9151
0.87
321.
10-0
.11
-0.0
6
153
1.00
164
1.03
112.1
123
1.05
721.
0639
0.92
190.
900.
000.
05
480.
8249
0.81
10.
499
1.04
140.5
312
0.75
131.
67-0
.10
-0.1
1
421.
1144
1.13
21.
542
0.37
201.
1913
1.25
71.
360.
040.
05
260.
8527
0.85
10.
923
0.66
130.
966
0.72
40.
98-0
.04
-0.0
4
831.4
585
1.4
42
1.04
121.
4935
1.40
171.
0619
2.3
10.2
50.2
4
242
2.8
927
93.2
337
13.4
429
2.4
710
72.9
169
2.9
737
3.1
41.5
41.8
1
251.
1627
1.21
22.
780
0.00
111.
1411
1.85
31.
030.
030.
04
41.
174
1.14
00.
000
0.00
10.
672
2.10
12.
060.
010.
00
31.
543
1.48
00.
001
3.50
00.
001
1.86
13.
710.
010.
01
112.0
914
2.5
73
16.9
02
2.64
72.9
90
0.00
22.
780.
060.
08
32.
103
2.03
00.
001
4.60
11.
551
2.58
00.
000.
020.
01
347
1.1
537
21.1
925
2.4
241
0.93
149
1.09
103
1.2
654
1.3
90.
450.5
7
231.
5240
2.5
517
30.2
17
2.9
210
1.41
51.
271
0.58
0.08
0.2
3
530.
9780
1.4
227
14.2
811
1.35
210.
8416
1.10
50.
74-0
.01
0.2
2
421.
0843
1.07
10.
745
0.87
231.
3110
0.95
40.
800.
030.
03
471.5
054
1.6
77
6.7
88
1.81
211.
519
1.03
92.
070.
150.2
0
150.2
927
0.5
012
6.7
05
0.66
30.1
35
0.3
42
0.2
8-0
.36
-0.2
6
80.1
619
0.3
811
6.6
25
0.71
10.0
51
0.0
71
0.1
5-0
.39
-0.2
9
71.
838
2.03
17.
800
0.00
21.
204
3.7
61
1.81
0.03
0.04
191.
0320
1.05
11.
613
1.12
70.
858
1.59
10.
410.
010.
01
241.
3125
1.32
11.
633
1.12
161.9
13
0.60
20.
850.
050.
06
51.
815
1.74
00.
001
2.34
21.
562
2.75
00.
000.
020.
02
531.
1056
1.12
31.
846
0.86
170.
7917
1.28
132.0
10.
050.
06
200.
8522
0.90
22.
475
1.46
90.
865
0.77
10.
32-0
.03
-0.0
2
310.
9131
0.88
00.
005
1.01
120.
7912
1.29
20.
44-0
.03
-0.0
4
100.
6710
0.64
00.
003
1.34
30.
443
0.74
10.
52-0
.05
-0.0
5
191.
2019
1.16
00.
002
0.88
81.
148
1.83
10.
460.
030.
02
20.
642
0.62
00.
000
0.00
10.
731
1.15
00.
00-0
.01
-0.0
1
105
1.00
115
1.06
102.7
724
1.6
041
0.89
291.
0011
0.74
0.00
0.06
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
EAR
EAR
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECONDCANCERSITE
83 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
21034
7179
022
506
2103
416
704
8321
3225
2103
471
790
102871
1064
9536
2415
558
4714
627
456
1271
110
2871
1064
95

ALLSITES,BUTURINARYTRACT
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
PROSTATE
TESTIS
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
URINARYTRACT
POOLAIRTUM1976-2010,MEN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
VIEURINARIE
POOLAIRTUM1976-2010,UOMINI:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRSTCANCERSITE
URINARYTRACT
MEN
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
353
1.09
410
1.2
157
4.1
864
1.19
174
1.16
790.
9536
0.95
2.06
4.9
7
110.
8911
0.85
00.
001
0.46
81.
341
0.33
10.
81-0
.10
-0.1
4
20.
692
0.66
00.
000
0.00
10.
721
1.38
00.
00-0
.07
-0.0
7
20.
782
0.75
00.
000
0.00
21.
630
0.00
00.
00-0
.04
-0.0
5
71.
017
0.96
00.
001
0.82
51.
500
0.00
11.
460.
00-0
.02
20.
593
0.84
16.
741
1.72
00.
001
1.17
00.
00-0
.10
-0.0
4
150.
7418
0.85
33.
291
0.28
121.
270
0.0
02
0.88
-0.3
8-0
.22
521.
1654
1.16
21.
077
0.96
231.
1216
1.38
61.
110.
520.
51
341.
1036
1.12
21.
565
1.00
171.
218
0.99
41.
040.
220.
26
181.
3118
1.26
00.
002
0.87
60.
948
2.28
21.
270.
310.
25
151.
1717
1.27
23.
700
0.00
111.
844
1.22
00.
000.
150.
25
41.
124
1.07
00.
003
5.0
60
0.00
00.
001
2.28
0.03
0.02
60.
686
0.65
00.
000
0.00
30.
741
0.44
21.
87-0
.21
-0.2
3
731.2
883
1.3
910
4.0
78
0.83
341.
2824
1.6
77
1.09
1.15
1.6
2
40.
954
0.91
00.
000
0.00
21.
051
0.90
11.
89-0
.01
-0.0
3
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.12
-0.1
2
11.
481
1.42
00.
000
0.00
00.
001
5.87
00.
000.
020.
02
10.
931
0.89
00.
000
0.00
00.
001
3.61
00.
00-0
.01
-0.0
1
13.
791
3.62
00.
000
0.00
00.
001
15.3
60
0.00
0.05
0.05
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.05
-0.0
5
781.
2010
21.5
124
9.3
218
1.7
634
1.16
170.
999
1.12
0.95
2.3
9
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.02
-0.0
2
50.
5111
1.08
615.0
34
2.51
10.
220
0.00
00.
00-0
.34
0.06
501.3
858
1.5
48
5.2
216
2.6
628
1.6
82
0.2
24
0.95
1.00
1.4
1
501.4
558
1.6
28
5.4
916
2.7
928
1.7
72
0.2
34
0.99
1.12
1.5
3
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.12
-0.1
2
10.
291
0.28
00.
000
0.00
00.
001
1.16
00.
00-0
.17
-0.1
8
32.
443
2.35
00.
000
0.00
23.
501
3.12
00.
000.
130.
12
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.04
-0.0
4
131.
4513
1.39
00.
002
1.35
92.
171
0.43
10.
940.
290.
25
40.
924
0.89
00.
001
1.38
31.
510
0.00
00.
00-0
.02
-0.0
4
91.
209
1.15
00.
002
1.58
20.
584
2.11
11.
150.
110.
08
20.
562
0.53
00.
001
1.64
10.
600
0.00
00.
00-0
.11
-0.1
2
72.
077
1.99
00.
001
1.78
10.
654
4.6
11
2.45
0.26
0.24
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.04
-0.0
4
50.2
96
0.3
31
1.34
00.
002
0.2
62
0.45
10.
47-0
.88
-0.8
3
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECONDCANCERSITE
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
EAR
EAR
84 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
3363
3797
3797
3363
2492
1079
408
3363
3797
13872
1446
659
423
8065
8134
7014
4213
872
1446
6

ALLSITES,BUTURINARYTRACT
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
CERVIXUTERI
CORPUSUTERI
OVARY
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
URINARYTRACT
POOLAIRTUM1976-2010,WOMEN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
VIEURINARIE
POOLAIRTUM1976-2010,DONNE:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRSTCANCERSITE
URINARYTRACT
WOMEN
721.
1486
1.3
014
4.3
917
1.47
311.
0915
0.97
91.
181.
853.
89
11.
291
1.22
00.
000
0.00
00.
000
0.00
110
.84
0.05
0.04
12.
271
2.16
00.
000
0.00
00.
000
0.00
118
.66
0.12
0.11
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.03
-0.0
3
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.04
-0.0
4
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.07
-0.0
7
40.
964
0.91
00.
001
1.25
21.
061
1.01
00.
00-0
.03
-0.0
7
151.
4616
1.48
11.
913
1.59
71.
523
1.19
21.
570.
971.
02
121.
6112
1.53
00.
001
0.74
72.
103
1.63
11.
070.
940.
82
31.
064
1.35
16.
892
3.82
00.
000
0.00
12.
960.
040.
20
10.
551
0.52
00.
000
0.00
00.
000
0.00
14.
45-0
.17
-0.1
8
10.
671
0.64
00.
000
0.00
00.
001
2.80
00.
00-0
.10
-0.1
1
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.58
-0.5
8
00.0
05
1.16
524.8
10
0.00
00.
000
0.00
00.
00-0
.85
0.14
00.
001
0.92
119
.90
00.
000
0.00
00.
000
0.00
-0.2
1-0
.02
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.03
-0.0
3
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.02
-0.0
2
27.
852
7.48
00.
000
0.00
00.
002
31.4
40
0.00
0.36
0.34
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.01
-0.0
1
161.
1116
1.06
00.
001
0.38
91.
372
0.56
42.
360.
320.
17
11.
392
2.63
126
.36
00.
000
0.00
15.
860
0.00
0.06
0.24
31.
173
1.12
00.
000
0.00
10.
852
3.19
00.
000.
090.
06
10.
542
1.02
110
.66
00.
000
0.00
00.
001
4.62
-0.1
80.
01
21.
313
1.88
113
.49
27.
420
0.00
00.
000
0.00
0.10
0.28
114.2
915
5.5
64
30.4
96
12.7
53
2.61
23.
180
0.00
1.7
42.4
2
114.6
415
6.0
24
33.2
36
13.8
73
2.83
23.
440
0.00
1.7
82.4
6
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.04
-0.0
4
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.18
-0.1
8
11.
191
1.14
00.
000
0.00
12.
620
0.00
00.
000.
030.
02
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.03
-0.0
3
10.
431
0.41
00.
000
0.00
10.
940
0.00
00.
00-0
.28
-0.2
9
10.
881
0.83
00.
000
0.00
11.
940
0.00
00.
00-0
.03
-0.0
4
10.
601
0.58
00.
000
0.00
00.
001
2.48
00.
00-0
.14
-0.1
5
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.15
-0.1
5
11.
301
1.23
00.
000
0.00
00.
001
5.25
00.
000.
050.
04
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.03
-0.0
3
101.
9410
1.84
00.
004
4.1
66
2.61
00.
000
0.00
1.00
0.90
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
EAR
EAR
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECONDCANCERSITE
85 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
1341
1562
1562
1341
891
354
137
1341
1562
4837
5078
241
895
2219
1175
548
4837
5078

ALLSITES,BUTSKINANDBRAINANDCNS
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
PROSTATE
TESTIS
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
BRAINANDCENTRALNERVOUSSYSTEM
POOLAIRTUM1976-2010,MEN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
ENCEFALOESISTEMANERVOSOCENTRALE
POOLAIRTUM1976-2010,UOMINI:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRSTCANCERSITE
BRAINANDCENTRAL
NERVOUSSYSTEM
MEN
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
160
0.8
221
80.
9758
1.9
655
0.77
470.6
737
1.10
211.
03-1
.41
-1.4
1
111.
0911
0.95
00.
002
0.54
41.
073
1.76
22.
110.
040.
04
31.
223
1.08
00.
001
1.14
11.
101
2.35
00.
000.
020.
02
31.
273
1.12
00.
001
1.19
00.
001
2.44
14.
300.
030.
03
50.
945
0.82
00.
000
0.00
31.
541
1.15
12.
12-0
.01
-0.0
1
31.
353
1.18
00.
002
2.42
00.
001
2.68
00.
000.
030.
03
50.
465
0.3
90
0.00
10.
242
0.51
10.
541
0.95
-0.2
4-0
.24
210.
8026
0.86
51.
257
0.73
80.
866
1.32
00.
00-0
.20
-0.2
0
160.
9120
0.99
41.
487
1.10
40.
655
1.64
00.
00-0
.06
-0.0
6
50.
586
0.61
10.
770
0.00
41.
301
0.67
00.
00-0
.14
-0.1
4
50.
637
0.77
21.
630
0.00
20.
711
0.75
22.
52-0
.12
-0.1
2
31.
613
1.38
00.
001
1.43
00.
001
3.14
15.
270.
050.
05
10.
201
0.1
70
0.00
00.
000
0.00
11.
140
0.00
-0.1
6-0
.16
190.5
640
1.01
213.8
89
0.69
50.4
13
0.53
20.
61-0
.60
-0.6
0
51.
297
1.63
24.
553
2.48
10.
690
0.00
12.
100.
050.
05
10.
971
0.85
00.
001
2.66
00.
000
0.00
00.
000.
000.
00
611.5
16
10.1
70
0.00
423.2
72
10.0
60
0.00
00.
000.2
20.2
2
11.
121
1.00
00.
001
3.47
00.
000
0.00
00.
000.
000.
00
13.
271
2.95
00.
000
0.00
18.
340
0.00
00.
000.
030.
03
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.02
-0.0
2
290.
8538
0.96
91.
686
0.47
40.3
411
1.85
82.
07-0
.21
-0.2
1
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.05
-0.0
5
60.
8710
1.28
44.2
14
1.65
10.
401
0.83
00.
00-0
.03
-0.0
3
70.3
310
0.4
03
0.89
50.
632
0.2
60
0.00
00.
00-0
.57
-0.5
7
70.3
410
0.4
23
0.93
50.
652
0.2
70
0.00
00.
00-0
.54
-0.5
4
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.03
-0.0
3
10.
332
0.59
12.
580
0.00
00.
001
1.85
00.
00-0
.08
-0.0
8
53.
066
3.3
51
6.27
24.
221
1.59
00.
002
9.5
80.
130.
13
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.04
-0.0
4
60.
927
0.95
11.
152
0.90
41.
660
0.00
00.
00-0
.02
-0.0
2
20.
813
1.05
12.
591
1.10
00.
001
2.35
00.
00-0
.02
-0.0
2
81.
7113
2.4
25
7.1
71
0.60
42.
332
2.42
12.
110.
130.
13
20.
877
2.6
55
14.7
21
1.21
11.
180
0.00
00.
00-0
.01
-0.0
1
62.8
86
2.51
00.
000
0.00
33.
942
5.38
14.
490.
160.
16
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.01
-0.0
1
151.
5319
1.6
74
2.63
30.
846
1.70
52.
911
0.98
0.21
0.21
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECONDCANCERSITE
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
EAR
EAR
86 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
11743
1408
814
088
1174
354
4215
5261
111
743
1408
8
25033
2718
621
5266
5710
293
5110
2973
2503
327
186

ALLSITES,BUTSKINANDBRAINANDCNS
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
CERVIXUTERI
CORPUSUTERI
OVARY
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
BRAINANDCENTRALNERVOUSSYSTEM
POOLAIRTUM1976-2010,WOMEN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
ENCEFALOESISTEMANERVOSOCENTRALE
POOLAIRTUM1976-2010,DONNE:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRSTCANCERSITE
BRAINANDCENTRAL
NERVOUSSYSTEM
WOMEN
110
0.87
144
1.01
342.0
826
0.6
641
0.86
271.
1516
0.98
-0.7
40.
05
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.08
-0.0
8
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.04
-0.0
4
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.02
-0.0
2
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.02
-0.0
2
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.02
-0.0
2
50.
836
0.86
11.
040
0.00
31.
352
1.88
00.
00-0
.05
-0.0
4
120.
6916
0.81
41.
603
0.53
30.
473
0.96
31.
37-0
.24
-0.1
6
60.
498
0.57
21.
121
0.25
10.
222
0.91
21.
28-0
.28
-0.2
5
61.
188
1.37
22.
772
1.21
21.
061
1.09
11.
570.
040.
09
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.13
-0.1
4
10.
441
0.38
00.
001
1.33
00.
000
0.00
00.
00-0
.06
-0.0
7
10.
252
0.43
11.
590
0.00
10.
690
0.00
00.
00-0
.14
-0.1
1
91.
2712
1.48
32.
984
1.73
31.
161
0.78
11.
080.
090.
16
30.
963
0.87
00.
000
0.00
21.
670
0.00
12.
13-0
.01
-0.0
2
13.
371
2.95
00.
000
0.00
00.
000
0.00
125
.74
0.03
0.03
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.01
-0.0
1
00.
001
1.48
114
.20
00.
000
0.00
00.
000
0.00
-0.0
30.
01
00.
001
4.37
147
.51
00.
000
0.00
00.
000
0.00
-0.0
10.
03
210.5
529
0.6
98
1.86
60.
538
0.55
50.
702
0.40
-0.7
7-0
.55
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.11
-0.1
1
91.
399
1.23
00.
001
0.49
31.
234
3.39
11.
230.
110.
07
71.
587
1.41
00.
001
0.73
31.
781
1.22
23.
620.
120.
09
72.
447
2.15
00.
004
4.3
33
2.83
00.
000
0.00
0.19
0.16
20.
493
0.64
11.
651
0.74
00.
000
0.00
11.
91-0
.10
-0.0
7
10.
262
0.45
11.
771
0.79
00.
000
0.00
00.
00-0
.13
-0.1
0
13.
931
3.39
00.
000
0.00
00.
000
0.00
131
.50
0.03
0.03
00.
001
0.44
13.
910
0.00
00.
000
0.00
00.
00-0
.09
-0.0
5
81.
9910
2.3
12
6.30
00.
003
1.91
44.7
21
1.59
0.18
0.24
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.03
-0.0
3
81.
719
1.70
11.
632
1.36
31.
722
2.32
11.
650.
150.
16
10.
526
2.70
517.5
60
0.00
11.
410
0.00
00.
00-0
.04
0.16
62.
038
2.3
72
4.86
22.
152
1.79
23.
670
0.00
0.14
0.19
43.
106
4.0
72
10.8
12
4.80
12.
051
4.28
00.
000.
120.
19
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.06
-0.0
7
28.
492
7.39
00.
000
0.00
111
.33
122
.34
00.
000.
080.
07
91.
1413
1.43
43.
421
0.40
31.
023
2.05
21.
960.
050.
16
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
EAR
EAR
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECONDCANCERSITE
87 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
9778
1196
811
968
9778
4419
1375
600
9778
1196
8
22049
2386
918
2053
5089
2146
9030
8722
049
2386
9

ALLSITES,BUTSKINANDTHYROID
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
PROSTATE
TESTIS
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
THYROID
POOLAIRTUM1976-2010,MEN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
TIROIDE
POOLAIRTUM1976-2010,UOMINI:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRSTCANCERSITE
THYROID
MEN
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
417
1.2
245
01.2
733
3.0
148
1.03
184
1.1
913
01.4
655
1.05
2.1
22.6
7
110.
6512
0.68
11.
803
1.26
40.
522
0.46
20.
79-0
.17
-0.1
5
00.0
00
0.0
00
0.00
00.
000
0.00
00.
000
0.00
-0.1
2-0
.12
10.
241
0.24
00.
000
0.00
10.
540
0.00
00.
00-0
.09
-0.0
9
101.
1511
1.22
13.
443
2.42
30.
752
0.91
21.
580.
040.
06
30.
794
1.03
18.
090
0.00
31.
750
0.00
00.
00-0
.02
0.00
251.
4025
1.36
00.
003
1.19
101.
2310
2.1
92
0.78
0.21
0.18
551.
1955
1.15
00.
008
1.30
221.
0619
1.56
60.
840.
250.
20
411.
3141
1.27
00.
006
1.45
151.
0714
1.69
61.
220.
280.
24
140.
9414
0.91
00.
002
0.98
71.
035
1.29
00.
00-0
.03
-0.0
4
120.
8613
0.90
12.
220
0.00
60.
954
1.11
20.
95-0
.06
-0.0
4
30.
933
0.90
00.
001
2.27
00.
002
2.40
00.
00-0
.01
-0.0
1
70.
778
0.85
13.
470
0.00
51.
220
0.00
21.
43-0
.06
-0.0
4
540.
9469
1.17
157.9
46
0.76
230.
8816
1.09
91.
06-0
.09
0.28
60.
868
1.11
29.6
70
0.00
41.
282
1.09
00.
00-0
.03
0.02
63.1
26
3.0
30
0.00
13.
992
2.33
35.9
50
0.00
0.12
0.11
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.02
-0.0
2
53.3
65
3.2
50
0.00
00.
003
4.45
12.
591
4.42
0.10
0.10
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.01
-0.0
1
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.02
-0.0
2
871.3
489
1.3
32
1.02
70.
8343
1.4
827
1.5
710
0.97
0.63
0.61
21.
093
1.59
116
.43
13.
631
1.15
00.
000
0.00
0.00
0.03
342.7
837
2.9
43
7.9
65
3.07
132.3
611
3.4
45
2.63
0.6
30.6
8
401.
0940
1.05
00.
005
0.99
191.
1411
1.16
50.
900.
090.
06
391.
1039
1.07
00.
005
1.03
191.
1910
1.09
50.
940.
110.
07
10.
701
0.68
00.
000
0.00
00.
001
2.68
00.
00-0
.01
-0.0
1
112.1
911
2.1
20
0.00
00.
007
3.0
63
2.32
11.
340.
170.
16
10.
337
2.27
665.4
81
2.44
00.
000
0.00
00.
00-0
.06
0.11
21.
462
1.41
00.
001
4.92
00.
001
2.90
00.
000.
020.
02
151.
3317
1.46
25.
631
0.65
81.
573
1.02
31.
740.
110.
15
61.
397
1.58
17.
171
1.71
21.
032
1.78
11.
530.
050.
07
121.
5612
1.51
00.
002
1.86
41.
144
2.02
21.
770.
120.
11
51.
345
1.30
00.
001
1.91
10.
592
2.10
11.
830.
040.
03
71.
997
1.92
00.
001
2.06
31.
882
2.18
11.
900.
100.
09
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.01
-0.0
1
211.
2524
1.39
35.4
73
1.30
50.
669
2.07
41.
580.
120.
19
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECONDCANCERSITE
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
EAR
EAR
88 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
6644
7072
7072
6644
5604
2757
1023
6644
7072
34797
3593
911
4250
6616
204
8765
4762
3479
735
939

ALLSITES,BUTSKINANDTHYROID
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
CERVIXUTERI
CORPUSUTERI
OVARY
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
THYROID
POOLAIRTUM1976-2010,WOMEN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
TIROIDE
POOLAIRTUM1976-2010,DONNE:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRSTCANCERSITE
THYROID
WOMEN
980
1.2
210
331.2
553
2.5
212
91.3
637
91.1
227
31.2
019
91.3
91.4
01.6
1
80.
7110
0.86
26.
812
1.50
40.
841
0.31
10.
49-0
.03
-0.0
1
30.
533
0.52
00.
002
3.06
00.
000
0.00
10.
96-0
.02
-0.0
2
00.
002
0.65
225.5
00
0.00
00.
000
0.00
00.
00-0
.02
-0.0
1
51.
845
1.80
00.
000
0.00
43.
501
1.31
00.
000.
020.
02
51.
628
2.5
23
37.8
32
5.75
00.
002
2.25
11.
680.
020.
04
421.
2844
1.31
22.
232
0.52
201.
4813
1.38
71.
160.
070.
08
122
1.15
125
1.15
31.
1013
1.08
601.3
731
1.01
180.
900.
130.
12
911.
2193
1.21
21.
059
1.06
421.
3726
1.20
140.
980.
130.
12
310.
9932
1.00
11.
234
1.10
181.
395
0.56
40.
700.
000.
00
100.
6210
0.60
00.
002
1.08
10.1
54
0.86
30.
98-0
.05
-0.0
5
90.
7310
0.79
13.
001
0.69
40.
790
0.00
41.
74-0
.03
-0.0
2
361.4
736
1.4
40
0.00
72.6
211
1.12
111.
547
1.45
0.09
0.08
681.4
388
1.8
120
17.0
912
2.2
721
1.08
171.
2418
1.9
90.
160.3
0
180.
8219
0.84
11.
726
2.24
40.
424
0.65
41.
10-0
.03
-0.0
3
20.
953
1.39
119
.43
14.
281
1.17
00.
000
0.00
0.00
0.01
11.
211
1.18
00.
000
0.00
00.
001
4.25
00.
000.
000.
00
41.
054
1.02
00.
000
0.00
21.
221
0.94
11.
540.
000.
00
32.
783
2.70
00.
000
0.00
24.
210
0.00
15.
970.
020.
01
327
1.2
233
31.2
16
0.85
361.
1214
31.2
588
1.18
601.
310.4
70.4
5
90.
5910
0.64
12.
261
0.50
40.
591
0.24
31.
32-0
.05
-0.0
4
581.3
359
1.31
10.
877
1.33
191.
0222
1.7
910
1.31
0.11
0.11
481.6
749
1.6
61
1.29
61.
7115
1.22
172.1
210
2.05
0.1
50.1
5
321.7
033
1.7
11
2.12
94.2
17
0.90
61.
1110
2.8
70.
110.
11
331.
3233
1.28
00.
001
0.35
111.
0712
1.66
91.
890.
060.
06
311.
3231
1.28
00.
001
0.38
111.
1410
1.47
92.
020.
060.
05
21.
292
1.26
00.
000
0.00
00.
002
4.40
00.
000.
000.
00
110.
8811
0.86
00.
001
0.66
20.
385
1.44
31.
40-0
.01
-0.0
1
00.0
014
0.4
414
16.2
50
0.0
00
0.0
00
0.0
00
0.0
0-0
.25
-0.1
4
61.
706
1.65
00.
001
1.97
42.
431
1.09
00.
000.
020.
02
371.
2238
1.22
11.
275
1.41
141.
1011
1.28
71.
290.
050.
05
201.6
921
1.7
31
3.28
32.
228
1.64
61.
763
1.36
0.06
0.07
241.
4225
1.44
12.
193
1.49
91.
2710
2.08
20.
670.
060.
06
50.
715
0.69
00.
002
2.36
10.
342
1.00
00.
00-0
.02
-0.0
2
182.0
719
2.1
31
4.33
10.
977
1.92
83.2
42
1.29
0.07
0.08
10.
871
0.85
00.
000
0.00
12.
100
0.00
00.
000.
000.
00
470.
9954
1.12
75.7
28
1.31
130.
689
0.68
171.9
60.
000.
04
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
EAR
EAR
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECONDCANCERSITE
89 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
21992
2292
522
925
2199
219
139
1010
940
9421
992
2292
5
125847
1295
8737
4117
113
5699
733
645
1809
212
5847
1295
87

ALLSITES,BUTSKINANDHODGKINLYMPHOMA
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
PROSTATE
TESTIS
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
HODGKINLYMPHOMA
POOLAIRTUM1976-2010,MEN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
LINFOMADIHODGKIN
POOLAIRTUM1976-2010,UOMINI:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRSTCANCERSITE
HODGKIN
LYMPHOMA
MEN
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
311
1.5
932
71.6
316
2.8
323
0.99
115
1.5
771
1.3
510
22.2
13.3
03.5
0
151.
4416
1.49
13.
430
0.00
71.
764
1.44
41.
650.
130.
15
62.
296
2.23
00.
000
0.00
22.
053
4.24
11.
560.
100.
09
31.
184
1.53
115
.08
00.
002
2.11
11.
460
0.00
0.01
0.04
61.
146
1.11
00.
000
0.00
31.
460
0.00
32.
600.
020.
02
73.1
38
3.4
71
15.3
30
0.00
11.
180
0.00
611.3
40.
140.
16
151.
3915
1.35
00.
001
0.70
40.
945
1.77
52.
190.
120.
11
281.
1128
1.08
00.
001
0.33
101.
077
1.03
101.
640.
080.
06
160.
9516
0.92
00.
000
0.00
40.
644
0.88
81.
94-0
.02
-0.0
4
121.
4312
1.39
00.
001
0.99
61.
913
1.33
21.
010.
100.
09
101.
3210
1.28
00.
003
3.33
62.
110
0.00
10.
550.
070.
06
31.
703
1.64
00.
000
0.00
11.
490
0.00
24.
950.
040.
03
102.
0110
1.95
00.
000
0.00
42.
161
0.75
54.1
50.
140.
14
722.2
277
2.3
15
5.0
02
0.49
272.1
416
1.8
627
3.8
01.1
31.2
1
81.
728
1.68
00.
000
0.00
10.
602
1.54
54.1
00.
100.
09
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.03
-0.0
3
34.
683
4.56
00.
002
27.3
01
4.06
00.
000
0.00
0.07
0.06
21.
932
1.88
00.
000
0.00
12.
561
3.55
00.
000.
030.
03
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.01
-0.0
1
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.01
-0.0
1
361.
1336
1.10
00.
003
0.82
100.
877
0.82
161.9
30.
120.
09
20.
762
0.75
00.
000
0.00
10.
961
1.31
00.
00-0
.02
-0.0
2
91.
2911
1.54
210.8
52
2.56
20.
783
1.59
21.
150.
060.
11
211.
0324
1.14
34.
912
0.80
70.
917
1.28
51.
070.
020.
08
211.
0724
1.19
35.1
12
0.83
70.
947
1.33
51.
110.
040.
11
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.02
-0.0
2
20.
602
0.59
00.
000
0.00
21.
580
0.00
00.
00-0
.04
-0.0
4
94.1
810
4.5
41
20.9
40
0.00
33.
862
3.33
47.1
60.1
90.2
2
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.04
-0.0
4
283.9
329
3.9
61
5.31
33.
7312
4.5
17
3.5
96
3.5
00.5
90.6
0
31.
243
1.20
00.
001
3.44
11.
111
1.54
00.
000.
020.
01
153.1
116
3.2
21
6.97
11.
6910
5.4
13
2.32
10.
920.2
90.3
1
20.
873
1.26
114
.58
00.
001
1.13
11.
630
0.00
-0.0
10.
02
125.4
212
5.2
60
0.00
13.
748
9.4
82
3.33
11.
990.2
80.2
7
13.
321
3.21
00.
000
0.00
18.
320
0.00
00.
000.
020.
02
131.
3214
1.38
13.
372
1.65
41.
074
1.51
31.
310.
090.
11
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECONDCANCERSITE
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
EAR
EAR
90 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
5378
5615
5615
5378
4676
2677
1321
5378
5615
35127
3604
291
541
7114
201
9671
7085
3512
736
042

ALLSITES,BUTSKINANDHODGKINLYMPHOMA
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
CERVIXUTERI
CORPUSUTERI
OVARY
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
HODGKINLYMPHOMA
POOLAIRTUM1976-2010,WOMEN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
LINFOMADIHODGKIN
POOLAIRTUM1976-2010,DONNE:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRSTCANCERSITE
HODGKIN
LYMPHOMA
WOMEN
251
1.9
425
61.9
35
1.53
171.
2374
1.5
970
1.9
190
2.7
63.8
13.7
7
42.
384
2.32
00.
000
0.00
23.
361
2.10
12.
290.
070.
07
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.03
-0.0
3
48.8
44
8.6
40
0.00
00.
002
12.7
01
7.80
18.
250.
110.
11
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.01
-0.0
1
12.
161
2.10
00.
000
0.00
00.
000
0.00
19.
140.
020.
02
61.
096
1.06
00.
001
1.40
31.
411
0.67
10.
870.
020.
01
201.
2820
1.24
00.
003
1.68
61.
055
1.15
61.
590.
140.
12
181.
6318
1.59
00.
003
2.38
51.
245
1.63
51.
870.
220.
20
20.
432
0.42
00.
000
0.00
10.
590
0.00
10.
90-0
.08
-0.0
8
20.
852
0.82
00.
000
0.00
22.
240
0.00
00.
00-0
.01
-0.0
1
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.06
-0.0
6
51.
405
1.36
00.
000
0.00
21.
521
1.01
22.
350.
040.
04
243.5
924
3.5
00
0.00
00.
006
2.53
73.7
511
6.4
00.5
40.5
2
112.5
111
2.4
60
0.00
12.
444
2.60
64.5
90
0.00
0.21
0.20
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.01
-0.0
1
17.
001
6.79
00.
000
0.00
00.
000
0.00
133
.61
0.03
0.03
68.4
66
8.2
60
0.00
00.
000
0.00
419.7
52
11.9
00.1
70.1
6
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.01
-0.0
1
711.7
371
1.6
90
0.00
30.
7617
1.20
131.
1038
3.4
00.9
40.8
9
20.
672
0.65
00.
000
0.00
00.
002
2.28
00.
00-0
.03
-0.0
3
61.
006
0.98
00.
000
0.00
31.
412
1.19
10.
640.
000.
00
40.
894
0.87
00.
001
2.08
00.
003
2.34
00.
00-0
.02
-0.0
2
103.5
911
3.8
61
14.2
24
13.5
14
4.0
10
0.00
22.
850.2
30.2
5
92.4
19
2.3
50
0.00
00.
001
0.73
32.
895
5.6
30.
170.
16
82.
298
2.23
00.
000
0.00
10.
783
3.09
44.8
00.
140.
13
14.
191
4.06
00.
000
0.00
00.
000
0.00
118
.32
0.02
0.02
20.
972
0.95
00.
000
0.00
11.
301
1.71
00.
000.
000.
00
122.0
514
2.3
42
17.8
01
1.90
31.
486
3.4
32
1.28
0.19
0.25
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.04
-0.0
4
234.7
723
4.6
50
0.00
11.
928
4.5
46
4.3
78
6.8
60.5
70.5
5
21.
162
1.13
00.
002
10.0
50
0.00
00.
000
0.00
0.01
0.01
207.0
120
6.8
20
0.00
00.
008
7.3
98
10.0
44
6.3
00.5
40.5
2
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.04
-0.0
4
1912.7
219
12.3
90
0.00
00.
008
14.3
48
18.9
53
8.6
80.5
50.5
3
14.
951
4.79
00.
000
0.00
00.
000
0.00
124
.63
0.02
0.02
101.
3412
1.56
29.2
00
0.00
41.
431
0.48
52.
910.
080.
13
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
EAR
EAR
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECONDCANCERSITE
91 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
4685
4850
4850
4685
4074
2443
1252
4685
4850
31941
3273
679
536
3312
696
9154
6458
3194
132
736

ALLSITES,BUTSKINANDNON-HODGKINLYMPHOMA
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
PROSTATE
TESTIS
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
NON-HODGKINLYMPHOMA
POOLAIRTUM1976-2010,MEN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
LINFOMANON-HODGKIN
POOLAIRTUM1976-2010,UOMINI:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRSTCANCERSITE
NON-HODGKIN
LYMPHOMA
MEN
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
1991
1.1
323
331.2
734
24.5
029
30.
9891
91.1
053
51.2
124
41.2
52.0
04.2
1
911.
1810
71.3
316
4.7
312
0.89
491.
3320
1.07
101.
270.
130.
23
211.
1424
1.25
33.
801
0.32
101.
147
1.55
31.
540.
020.
04
150.
8919
1.08
45.5
65
1.72
50.
623
0.73
21.
12-0
.02
0.01
551.
3264
1.4
79
4.8
06
0.81
341.7
010
1.00
51.
200.
120.1
8
130.
6716
0.79
33.
522
0.59
30.3
25
1.05
31.
47-0
.06
-0.0
4
116
1.10
122
1.10
61.
2325
1.33
490.
9735
1.36
70.
650.
090.
10
236
0.95
308
1.1
972
6.8
427
0.6
510
20.
8874
1.19
331.
19-0
.10
0.4
3
176
1.04
233
1.3
257
7.9
517
0.6
078
0.98
551.
2826
1.34
0.05
0.4
8
600.7
875
0.93
154.4
710
0.76
240.6
619
0.98
70.
83-0
.16
-0.0
5
105
1.4
411
51.5
110
3.1
822
1.7
738
1.10
331.8
312
1.51
0.2
90.3
4
160.
8518
0.91
22.
393
0.93
101.
122
0.42
10.
49-0
.03
-0.0
2
430.
8845
0.88
20.
954
0.49
170.
7414
1.14
81.
46-0
.05
-0.0
5
403
1.2
946
91.4
366
4.7
460
1.10
186
1.2
510
91.4
248
1.4
60.8
01.2
2
501.8
053
1.8
33
2.77
30.
6826
2.0
315
2.0
76
1.78
0.2
00.2
1
141.
4316
1.57
25.
052
1.26
61.
324
1.60
21.
740.
040.
05
225.5
229
6.9
67
39.4
16
8.6
610
5.2
82
2.05
49.4
00.1
60.2
1
162.4
317
2.4
71
3.61
32.
736
1.95
74.2
00
0.00
0.0
80.0
9
21.
143
1.63
112
.88
00.
001
1.19
12.
340
0.00
0.00
0.01
51.
286
1.47
16.
020
0.00
10.
542
2.04
24.
610.
010.
02
335
0.94
386
1.04
513.5
138
0.6
616
20.
9889
0.97
461.
10-0
.18
0.14
112.8
312
2.9
81
6.64
11.
607
3.8
82
2.01
12.
190.
060.0
7
791.3
710
91.8
130
12.5
433
3.4
422
0.81
161.
098
1.22
0.19
0.4
2
235
1.1
827
41.3
239
4.4
821
0.6
212
61.3
457
1.15
311.
440.
320.5
7
229
1.2
026
61.3
437
4.4
521
0.6
412
31.3
755
1.16
301.
450.
340.5
8
60.
698
0.89
25.
280
0.00
30.
732
0.93
11.
06-0
.02
-0.0
1
221.
0223
1.02
11.
094
1.09
131.
273
0.56
20.
850.
000.
00
131.
3614
1.41
12.
714
2.63
61.
363
1.21
00.
000.
030.
03
194.3
128
6.0
99
48.1
51
1.32
62.8
89
8.2
53
6.2
30.1
30.2
0
100.1
913
0.2
43
1.34
20.2
22
0.0
82
0.1
54
0.68
-0.3
9-0
.36
90.3
89
0.3
70
0.00
10.
253
0.2
74
0.68
10.
39-0
.13
-0.1
3
531.
2959
1.3
76
3.2
811
1.54
281.
449
0.88
51.
140.
110.
14
120.
6117
0.82
55.6
53
0.87
50.
533
0.62
10.
48-0
.07
-0.0
3
382.0
439
2.0
01
1.23
82.5
221
2.4
06
1.29
31.
470.1
70.1
7
31.
103
1.04
00.
000
0.00
21.
510
0.00
13.
790.
000.
00
830.
8995
0.98
122.9
410
0.63
420.
9620
0.86
111.
07-0
.09
-0.0
2
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECONDCANCERSITE
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
EAR
EAR
92 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
26591
2980
029
800
2659
119
817
8724
3093
2659
129
800
111563
1162
3546
7218
984
5288
127
698
1200
111
1563
1162
35

ALLSITES,BUTSKINANDNON-HODGKINLYMPHOMA
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
CERVIXUTERI
CORPUSUTERI
OVARY
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
NON-HODGKINLYMPHOMA
POOLAIRTUM1976-2010,WOMEN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
LINFOMANON-HODGKIN
POOLAIRTUM1976-2010,DONNE:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRSTCANCERSITE
NON-HODGKIN
LYMPHOMA
WOMEN
1219
1.1
214
161.2
519
74.5
316
80.
9952
71.
0634
71.2
017
71.2
81.1
42.4
3
271.8
530
1.9
83
5.2
63
1.33
131.9
66
1.56
52.
700.
110.1
3
162.0
618
2.2
32
6.57
21.
698
2.29
31.
443
2.95
0.07
0.09
41.
235
1.48
17.
940
0.00
21.
341
1.18
12.
480.
010.
01
71.
977
1.90
00.
001
1.79
31.
842
2.16
12.
300.
030.
03
50.
938
1.43
313.5
32
2.38
20.
820
0.00
11.
470.
000.
02
580.
9263
0.96
51.
805
0.49
311.
0815
0.91
70.
93-0
.05
-0.0
2
187
1.09
226
1.2
639
5.6
130
1.12
811.
0454
1.18
221.
010.
140.4
1
141
1.14
168
1.3
127
5.4
321
1.10
611.
1041
1.25
181.
140.
160.3
4
460.
9558
1.15
126.0
79
1.18
200.
9113
1.02
40.
67-0
.02
0.07
672.2
679
2.5
612
9.7
98
1.71
282.0
821
2.6
910
2.7
00.3
40.4
2
160.
6917
0.70
11.
013
0.80
30.2
89
1.49
10.
35-0
.06
-0.0
6
521.
1754
1.17
21.
125
0.74
190.
9616
1.34
122.0
40.
070.
07
941.3
110
81.4
514
5.0
612
1.11
331.
0233
1.7
116
1.69
0.20
0.2
9
341.5
636
1.5
92
2.48
41.
2317
1.7
310
1.70
31.
050.
110.
12
61.
947
2.18
18.
681
2.18
32.
171
1.20
12.
390.
030.
03
74.7
611
7.1
84
64.2
84
17.1
73
4.52
00.
000
0.00
0.05
0.0
8
91.
899
1.82
00.
000
0.00
41.
853
2.38
23.
300.
040.
04
10.
781
0.75
00.
000
0.00
00.
000
0.00
16.
580.
000.
00
300
1.02
352
1.1
552
4.6
037
0.81
127
0.94
821.
0554
1.4
60.
050.
40
120.
7914
0.88
23.
142
0.79
50.
702
0.52
31.
77-0
.03
-0.0
2
460.
8751
0.93
52.
435
0.60
220.
9115
1.09
40.
62-0
.06
-0.0
3
290.
8130
0.81
10.
703
0.53
120.
738
0.86
61.
39-0
.06
-0.0
6
401.4
656
1.9
616
15.1
714
3.3
613
1.05
81.
095
1.40
0.11
0.2
4
511.
2156
1.28
52.
949
1.38
251.
3214
1.25
30.
560.
080.
11
501.
2854
1.33
42.
539
1.48
251.
4213
1.25
30.
600.
100.
12
10.
342
0.65
18.
290
0.00
00.
001
1.26
00.
00-0
.02
-0.0
1
171.
0318
1.05
11.
534
1.55
50.
666
1.38
20.
970.
000.
01
401.7
847
2.0
27
8.8
97
2.12
171.
688
1.33
82.6
80.1
60.2
1
82.6
611
3.5
13
24.7
01
2.05
21.
432
2.58
38.6
80.
050.0
7
180.4
219
0.4
31
0.59
50.
767
0.3
63
0.2
73
0.56
-0.2
2-0
.22
70.3
68
0.4
01
1.27
10.
335
0.57
10.
200
0.00
-0.1
1-0
.11
301.
1032
1.13
21.
761
0.23
141.
1313
1.81
20.
600.
020.
03
10.0
83
0.2
42
3.92
00.
000
0.0
00
0.00
10.
71-0
.10
-0.0
8
292.2
229
2.1
30
0.00
10.
4914
2.3
713
3.7
41
0.60
0.1
40.1
3
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.02
-0.0
2
760.
9592
1.10
164.8
27
0.56
431.
2020
0.94
60.
58-0
.04
0.08
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
EAR
EAR
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECONDCANCERSITE
93 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
24563
2762
327
623
2456
318
491
8737
3337
2456
327
623
110539
1148
6943
2917
530
5115
328
749
1310
711
0539
1148
69

ALLSITES,BUTSKINANDMYELOMA
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
PROSTATE
TESTIS
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
MYELOMA
POOLAIRTUM1976-2010,MEN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
MIELOMA
POOLAIRTUM1976-2010,UOMINI:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRSTCANCERSITE
MYELOMA
MEN
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
620
0.9
279
21.1
217
24.6
313
50.
9230
10.8
413
71.
0347
1.4
3-1
.68
2.4
6
281.
0533
1.17
53.3
05
0.82
120.
828
1.59
32.
720.
040.
14
91.
4410
1.51
12.
852
1.42
41.
181
0.84
27.
430.
090.
10
81.
448
1.36
00.
002
1.59
20.
663
2.86
14.
460.
080.
06
110.
7415
0.95
44.6
61
0.29
60.
744
1.44
00.
00-0
.13
-0.0
2
111.
5612
1.61
12.
502
1.26
61.
582
1.48
13.
190.
130.
14
370.
8840
0.90
31.
216
0.62
190.
859
1.11
31.
53-0
.16
-0.1
4
800.
8610
21.
0322
4.3
014
0.69
450.
9117
0.91
40.
85-0
.43
0.10
540.
8476
1.12
226.3
19
0.65
330.
979
0.69
30.
90-0
.32
0.25
260.
8926
0.84
00.
005
0.77
120.
778
1.39
10.
71-0
.10
-0.1
5
311.
1441
1.4
310
6.6
711
1.84
130.
896
1.13
10.
780.
120.
37
70.
949
1.14
24.
753
1.82
30.
761
0.68
00.
00-0
.01
0.03
191.
0319
0.97
00.
007
1.74
70.
713
0.81
22.
120.
02-0
.02
121
1.02
163
1.3
042
6.2
927
1.02
610.
9624
1.05
91.
650.
081.1
4
90.
9911
1.15
24.
292
1.06
40.
832
1.06
12.
100.
000.
04
61.
729
2.4
63
16.5
24
5.4
41
0.54
00.
001
5.65
0.08
0.16
42.
756
3.9
12
24.0
91
3.06
33.
860
0.00
00.
000.
080.
13
20.
872
0.82
00.
001
1.99
10.
810
0.00
00.
00-0
.01
-0.0
1
00.
001
1.58
128
.53
00.
000
0.00
00.
000
0.00
-0.0
20.
01
21.
392
1.31
00.
001
3.18
00.
001
3.49
00.
000.
020.
01
106
0.7
914
31.
0137
5.2
222
0.78
520.7
322
0.79
101.
44-0
.91
0.04
00.
001
1.39
126
.37
00.
000
0.00
00.
000
0.00
-0.0
20.
01
241.
1740
1.8
516
14.5
44
0.90
100.
918
1.94
21.
990.
110.5
5
740.
9789
1.11
153.5
414
0.84
350.
8622
1.47
30.
81-0
.06
0.26
731.
0088
1.15
153.7
114
0.87
350.
9021
1.47
30.
850.
010.
34
10.
301
0.29
00.
000
0.00
00.
001
1.51
00.
00-0
.07
-0.0
8
111.
4711
1.40
00.
003
1.82
51.
242
1.38
12.
930.
110.
09
20.
704
1.33
213.6
10
0.00
21.
300
0.00
00.
00-0
.03
0.03
43.
184
3.01
00.
001
3.50
00.
001
4.22
237.7
20.
090.
08
50.2
76
0.3
01
0.98
00.0
03
0.3
01
0.27
11.
09-0
.44
-0.4
2
00.0
00
0.0
00
0.00
00.
000
0.0
00
0.00
00.
00-0
.29
-0.2
9
130.
8313
0.78
00.
001
0.28
80.
961
0.32
33.
93-0
.09
-0.1
1
10.1
31
0.1
30
0.00
00.
001
0.25
00.
000
0.00
-0.2
1-0
.21
101.
4210
1.34
00.
001
0.64
71.
871
0.72
12.
830.
090.
08
21.
732
1.63
00.
000
0.00
00.
000
0.00
236.3
90.
030.
02
240.6
731
0.82
73.4
86
0.76
110.
587
0.98
00.
00-0
.37
-0.2
0
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECONDCANCERSITE
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
EAR
EAR
94 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
9893
1129
011
290
9893
7391
2242
504
9893
1129
0
31536
3328
817
5270
7417
113
5997
1352
3153
633
288

ALLSITES,BUTSKINANDMYELOMA
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
CERVIXUTERI
CORPUSUTERI
OVARY
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
MYELOMA
POOLAIRTUM1976-2010,WOMEN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
MIELOMA
POOLAIRTUM1976-2010,DONNE:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRSTCANCERSITE
MYELOMA
WOMEN
402
1.00
483
1.1
581
3.7
976
0.89
218
1.03
821.
0326
1.09
0.05
1.7
4
81.
578
1.49
00.
001
0.93
51.
862
1.97
00.
000.
090.
07
41.
434
1.36
00.
001
1.71
21.
371
1.78
00.
000.
040.
03
10.
931
0.89
00.
000
0.00
00.
001
4.74
00.
000.
000.
00
32.
433
2.31
00.
000
0.00
34.
580
0.00
00.
000.
050.
05
00.
001
0.46
18.
940
0.00
00.
000
0.00
00.
00-0
.06
-0.0
3
321.
2633
1.23
10.
695
0.89
201.
495
1.03
21.
400.
200.
17
610.
9482
1.20
216.0
316
1.16
330.
9712
0.93
00.0
0-0
.11
0.39
481.
0362
1.27
145.6
114
1.41
261.
068
0.86
00.
000.
050.
37
130.
7220
1.05
77.1
12
0.51
70.
734
1.12
00.
00-0
.15
0.03
171.
4819
1.56
23.
190
0.00
91.
485
2.20
34.
390.
160.
19
70.
767
0.72
00.
001
0.49
61.
230
0.00
00.
00-0
.07
-0.0
8
281.6
529
1.6
21
1.10
92.5
113
1.47
30.
873
2.72
0.33
0.31
291.
1239
1.4
310
7.4
75
0.93
161.
187
1.33
10.
600.
090.
33
121.
7314
1.9
32
5.67
10.
7010
2.7
41
0.71
00.
000.
150.
19
21.
872
1.78
00.
000
0.00
23.
570
0.00
00.
000.
030.
02
11.
712
3.25
130
.62
00.
001
3.26
00.
000
0.00
0.01
0.04
00.
001
0.58
111
.56
00.
000
0.00
00.
000
0.00
-0.0
5-0
.02
12.
212
4.18
140
.06
00.
000
0.00
111
.44
00.
000.
020.
04
760.7
794
0.91
183.5
28
0.3
841
0.79
190.
978
1.42
-0.6
6-0
.26
20.
404
0.75
27.
090
0.00
10.
370
0.00
14.
07-0
.09
-0.0
4
150.
8318
0.94
33.
154
1.03
80.
832
0.56
11.
00-0
.09
-0.0
3
252.0
127
2.0
62
3.00
82.9
88
1.21
72.8
62
2.84
0.3
70.3
9
141.
4321
2.0
47
13.8
45
2.45
40.
784
2.02
11.
640.
130.
30
181.
1323
1.37
55.8
62
0.59
111.
324
1.26
11.
020.
060.
18
161.
0821
1.35
56.3
11
0.32
101.
294
1.35
11.
100.
040.
15
21.
772
1.68
00.
001
4.19
11.
690
0.00
00.
000.
030.
02
71.
207
1.14
00.
004
3.21
30.
970
0.00
00.
000.
030.
02
50.
796
0.91
13.
233
2.33
20.
600
0.00
00.
00-0
.04
-0.0
2
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.03
-0.0
3
20.1
32
0.1
30
0.00
00.
001
0.1
21
0.33
00.
00-0
.39
-0.4
0
00.0
00
0.0
00
0.00
00.
000
0.0
00
0.00
00.
00-0
.22
-0.2
2
171.
6417
1.56
00.
001
0.45
101.
834
1.96
23.
310.
200.
17
10.
221
0.20
00.
000
0.00
00.
001
1.12
00.
00-0
.11
-0.1
1
163.3
116
3.1
50
0.00
10.
9710
3.9
43
3.10
26.
770.3
30.3
1
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.03
-0.0
3
230.
7425
0.77
21.
183
0.45
140.
865
0.81
10.
52-0
.24
-0.2
2
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
EAR
EAR
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECONDCANCERSITE
95 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
10191
1138
411
384
1019
176
4223
7960
010
191
1138
4
33521
3531
117
9072
7017
918
6528
1806
3352
135
311

ALLSITES,BUTSKINANDLEUKAEMIAS
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
PROSTATE
TESTIS
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
LEUKAEMIAS
POOLAIRTUM1976-2010,MEN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
LEUCEMIE
POOLAIRTUM1976-2010,UOMINI:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRSTCANCERSITE
LEUKAEMIAS
MEN
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
1197
1.04
1432
1.1
823
53.9
320
70.
9559
41.
0529
21.
0810
41.
120.
683.0
2
551.
1762
1.25
72.8
27
0.75
271.
1412
1.13
92.6
10.
110.
17
151.
3516
1.37
11.
740
0.00
50.
906
2.36
44.7
10.
060.
06
70.
709
0.86
23.
940
0.00
40.
802
0.88
11.
33-0
.04
-0.0
2
331.
2737
1.35
42.
857
1.35
181.
374
0.69
42.
170.
100.
13
70.
579
0.70
23.
080
0.00
50.
811
0.36
11.
08-0
.07
-0.0
5
680.
9574
0.98
61.
4812
0.84
350.
9718
1.12
30.
57-0
.05
-0.0
2
181
1.13
213
1.2
632
3.8
625
0.83
931.
1843
1.13
201.
510.
290.6
0
122
1.11
145
1.2
523
4.0
817
0.83
611.
1328
1.06
161.
730.
170.
40
591.
1768
1.29
93.3
98
0.83
321.
2915
1.28
41.
010.
120.
20
310.6
636
0.73
52.
047
0.78
170.
735
0.46
20.
54-0
.23
-0.1
8
50.3
96
0.4
41
1.44
00.
005
0.79
00.
000
0.00
-0.1
1-0
.10
210.
6623
0.69
21.
213
0.50
100.
646
0.80
20.
77-0
.15
-0.1
4
255
1.2
533
81.5
883
7.6
645
1.14
125
1.2
372
1.5
413
0.84
0.7
31.6
8
402.4
444
2.5
64
5.2
25
1.72
192.4
012
2.9
64
2.62
0.3
40.3
6
71.
169
1.42
26.
870
0.00
62.
031
0.68
00.
000.
010.
04
145.3
619
6.9
05
35.4
12
3.91
64.6
14
6.6
92
9.8
40.1
60.2
2
61.
447
1.59
14.
701
1.27
31.
461
1.01
12.
840.
030.
04
00.
001
0.80
116
.23
00.
000
0.00
00.
000
0.00
-0.0
20.
00
51.
996
2.27
17.
721
2.11
21.
612
3.37
00.
000.
040.
05
203
0.89
216
0.90
131.
1433
0.79
102
0.91
500.
8918
0.92
-0.3
7-0
.33
10.
473
1.36
221.8
31
2.72
00.
000
0.00
00.
00-0
.02
0.01
551.5
468
1.8
213
7.3
324
3.6
320
1.14
80.
943
1.01
0.2
80.4
1
125
0.96
158
1.15
334.7
723
0.91
640.
9928
0.92
100.
97-0
.08
0.27
121
0.97
153
1.16
324.8
321
0.87
641.
0326
0.89
101.
01-0
.06
0.29
40.
705
0.83
13.
342
1.85
00.
002
1.50
00.
00-0
.02
-0.0
1
231.7
126
1.8
43
4.37
41.
5615
2.2
52
0.64
21.
850.
140.
16
112.0
212
2.1
11
3.99
11.
033
1.14
21.
505
9.7
50.
080.
09
62.
217
2.45
17.
530
0.00
21.
543
4.68
13.
670.
050.
06
250.
7528
0.80
31.
784
0.64
110.
678
1.01
20.
73-0
.12
-0.0
9
40.2
67
0.4
33
3.64
10.
343
0.39
00.
000
0.00
-0.1
6-0
.13
70.2
510
0.3
43
1.99
10.
183
0.2
23
0.47
00.
00-0
.29
-0.2
6
10.0
73
0.2
12
2.76
10.
380
0.0
00
0.00
00.
00-0
.18
-0.1
5
60.
496
0.46
00.
000
0.00
30.
493
1.04
00.
00-0
.09
-0.1
0
00.
001
0.47
18.
310
0.00
00.
000
0.00
00.
00-0
.03
-0.0
2
490.
7960
0.92
113.3
28
0.67
210.
6914
0.97
61.
19-0
.19
-0.0
7
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECONDCANCERSITE
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
EAR
EAR
96 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
18874
2280
022
800
1887
413
490
5371
1745
1887
422
800
70293
7369
233
9913
121
3431
716
547
6307
7029
373
692

ALLSITES,BUTSKINANDLEUKAEMIAS
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
CERVIXUTERI
CORPUSUTERI
OVARY
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
LEUKAEMIAS
POOLAIRTUM1976-2010,WOMEN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
LEUCEMIE
POOLAIRTUM1976-2010,DONNE:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRSTCANCERSITE
LEUKAEMIAS
WOMEN
565
1.04
670
1.1
810
53.8
310
71.
0923
80.
9116
21.2
358
1.11
0.39
1.6
6
81.
169
1.24
12.
901
0.80
20.
603
1.78
22.
990.
020.
03
61.
577
1.75
15.
281
1.47
10.
552
2.13
25.
240.
040.
05
10.
681
0.65
00.
000
0.00
00.
001
2.83
00.
00-0
.01
-0.0
1
10.
611
0.58
00.
000
0.00
11.
270
0.00
00.
00-0
.01
-0.0
1
20.
713
1.02
16.
851
1.96
10.
740
0.00
00.
00-0
.01
0.00
441.
2745
1.23
10.
528
1.22
211.
2412
1.48
30.
980.
160.
14
108
1.2
411
61.2
68
1.78
171.
0750
1.19
271.
2714
1.68
0.36
0.40
801.2
784
1.2
74
1.24
141.
2337
1.23
161.
0413
2.1
40.
300.
30
281.
1532
1.25
43.
143
0.67
131.
1011
1.88
10.
440.
060.
11
130.
8415
0.92
22.
470
0.00
70.
943
0.80
32.
08-0
.04
-0.0
2
120.
9613
0.98
11.
482
0.85
50.
824
1.34
10.
87-0
.01
0.00
210.
9021
0.86
00.
003
0.73
90.
826
1.05
31.
28-0
.04
-0.0
6
571.6
574
2.0
417
10.0
714
2.3
020
1.22
161.8
67
2.01
0.3
90.6
3
151.
5019
1.8
24
8.5
61
0.58
71.
497
2.8
40
0.00
0.09
0.14
10.
702
1.34
114
.86
00.
001
1.48
00.
000
0.00
-0.0
10.
01
11.
231
1.17
00.
000
0.00
12.
560
0.00
00.
000.
000.
00
20.
863
1.23
18.
721
2.40
00.
000
0.00
14.
26-0
.01
0.01
11.
441
1.37
00.
000
0.00
00.
000
0.00
114
.57
0.01
0.00
127
0.94
161
1.14
345.1
516
0.66
570.
8844
1.35
100.
78-0
.13
0.33
50.
706
0.80
12.
631
0.72
20.
572
1.23
00.
00-0
.04
-0.0
3
100.4
213
0.5
23
2.50
10.
224
0.3
43
0.52
20.
92-0
.24
-0.2
0
130.
7616
0.90
33.
474
1.27
50.
613
0.74
10.
64-0
.07
-0.0
3
181.
3823
1.6
85
7.8
39
3.9
04
0.64
41.
241
0.77
0.09
0.16
231.
0730
1.33
76.3
79
2.3
24
0.3
99
1.72
10.
480.
030.
12
211.
0528
1.34
76.8
68
2.22
30.3
19
1.85
10.
520.
020.
12
21.
292
1.23
00.
001
3.66
11.
360
0.00
00.
000.
010.
01
101.
2511
1.31
12.
512
1.37
51.
302
1.03
11.
300.
030.
04
121.
2513
1.30
12.
374
2.43
51.
111
0.42
21.
850.
040.
05
42.
496
3.5
62
27.2
01
3.63
11.
382
5.08
00.
000.
040.
07
200.
9722
1.02
21.
954
1.08
70.
716
1.19
31.
51-0
.01
0.01
30.3
15
0.49
23.
980
0.00
30.
640
0.00
00.
00-0
.12
-0.0
9
30.2
16
0.3
93
3.95
10.
371
0.1
41
0.29
00.
00-0
.20
-0.1
5
00.0
02
0.29
25.
780
0.00
00.
000
0.00
00.
00-0
.11
-0.0
8
30.
454
0.57
12.
911
0.82
10.
311
0.61
00.
00-0
.06
-0.0
5
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.02
-0.0
2
350.
8142
0.93
73.1
28
1.03
170.
838
0.76
20.
47-0
.14
-0.0
6
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
EAR
EAR
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECONDCANCERSITE
97 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
14787
1828
518
285
1478
710
451
4376
1555
1478
718
285
57308
5999
726
8910
199
2703
813
892
6179
5730
859
997

ALLSITES,BUTSKINANDLYMPHOIDLEUKAEMIAS
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
PROSTATE
TESTIS
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
LYMPHOIDLEUKAEMIAS
POOLAIRTUM1976-2010,MEN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
LEUCEMIELINFOIDI
POOLAIRTUM1976-2010,UOMINI:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRSTCANCERSITE
LYMPHOID
LEUKAEMIAS
MEN
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
927
1.05
1058
1.1
613
14.0
714
61.
0545
31.
0324
01.
0688
1.15
0.91
2.8
1
351.
0040
1.10
53.7
23
0.51
181.
018
0.94
62.
250.
000.
07
80.
978
0.94
00.
000
0.00
20.
484
1.97
23.
060.
00-0
.01
60.
827
0.92
13.
610
0.00
30.
802
1.11
11.
77-0
.03
-0.0
1
211.
0825
1.24
45.2
93
0.91
131.
312
0.42
32.
060.
030.
09
40.
434
0.42
00.
000
0.00
30.
640
0.00
11.
34-0
.11
-0.1
1
510.
9456
0.99
52.
338
0.88
230.
8317
1.27
30.
68-0
.07
-0.0
1
140
1.15
147
1.16
71.
5915
0.79
731.
2134
1.08
181.
660.
370.
41
101
1.20
104
1.20
31.
0010
0.77
541.
3023
1.05
141.8
40.
350.
33
391.
0343
1.09
42.
855
0.83
191.
0011
1.14
41.
240.
020.
07
240.
6727
0.73
32.
305
0.88
130.
734
0.44
20.
67-0
.24
-0.1
9
30.3
13
0.3
00
0.00
00.
003
0.61
00.
000
0.00
-0.1
4-0
.14
170.
7018
0.72
11.
143
0.79
70.
585
0.80
20.
94-0
.15
-0.1
4
204
1.3
226
01.6
256
9.6
829
1.16
103
1.3
260
1.5
412
0.95
1.0
01.9
4
312.5
834
2.7
43
7.4
14
2.24
152.5
79
2.8
23
2.55
0.3
80.4
2
71.
529
1.89
212.7
50
0.00
62.
641
0.82
00.
000.
050.
08
115.6
815
7.4
64
54.1
22
6.31
33.
084
8.2
82
12.2
10.1
80.2
5
61.
946
1.87
00.
001
2.04
31.
961
1.26
13.
570.
060.
05
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.02
-0.0
2
31.
594
2.04
114
.56
00.
001
1.06
24.
110
0.00
0.02
0.04
163
0.93
167
0.92
40.
6624
0.91
780.
9145
0.96
161.
00-0
.24
-0.2
8
10.
812
1.57
122
.96
15.
270
0.00
00.
000
0.00
0.00
0.01
391.4
645
1.6
26
6.3
317
4.1
014
1.05
50.
723
1.27
0.25
0.3
4
102
1.03
123
1.19
215.7
321
1.33
490.
9924
0.95
80.
940.
050.
39
981.
0311
81.
2020
5.7
019
1.26
491.
0322
0.91
80.
990.
060.
38
40.
915
1.10
16.
232
2.90
00.
002
1.78
00.
00-0
.01
0.01
161.
6117
1.65
12.
733
1.88
112.2
01
0.40
11.
180.
120.
13
61.
576
1.52
00.
001
1.71
10.
541
1.01
38.1
60.
040.
04
63.1
77
3.5
71
14.4
70
0.00
22.
213
6.2
91
4.78
0.08
0.10
140.5
614
0.5
40
0.00
20.
515
0.4
06
0.94
10.
45-0
.22
-0.2
3
10.0
81
0.0
80
0.00
00.
001
0.1
70
0.00
00.
00-0
.22
-0.2
2
60.2
96
0.2
80
0.00
10.
293
0.2
82
0.38
00.
00-0
.30
-0.3
1
10.1
01
0.1
00
0.00
10.
600
0.0
00
0.00
00.
00-0
.18
-0.1
9
50.
545
0.52
00.
000
0.00
30.
652
0.84
00.
00-0
.09
-0.0
9
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.03
-0.0
3
380.
8148
0.98
105.7
17
0.93
180.
778
0.66
51.
20-0
.19
-0.0
2
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECONDCANCERSITE
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
EAR
EAR
98 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
10570
1152
411
524
1057
087
3939
9413
1310
570
1152
4
49446
5127
318
2779
9224
299
1240
947
4549
446
5127
3

ALLSITES,BUTSKINANDLYMPHOIDLEUKAEMIAS
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
CERVIXUTERI
CORPUSUTERI
OVARY
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
LYMPHOIDLEUKAEMIAS
POOLAIRTUM1976-2010,WOMEN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
LEUCEMIELINFOIDI
POOLAIRTUM1976-2010,DONNE:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRSTCANCERSITE
LYMPHOID
LEUKAEMIAS
WOMEN
411
1.04
473
1.1
562
4.4
072
1.20
166
0.88
133
1.2
840
0.95
0.40
1.6
0
51.
025
0.98
00.
001
1.34
10.
422
1.54
11.
910.
000.
00
31.
083
1.05
00.
001
2.44
00.
001
1.36
13.
260.
010.
00
11.
001
0.97
00.
000
0.00
00.
001
3.86
00.
000.
000.
00
10.
871
0.84
00.
000
0.00
11.
790
0.00
00.
000.
000.
00
10.
482
0.92
113
.27
00.
001
1.00
00.
000
0.00
-0.0
30.
00
341.
3134
1.26
00.
006
1.46
141.
1111
1.66
31.
150.
210.
18
781.
2182
1.23
41.
7411
1.13
361.
1723
1.35
81.
160.
360.
39
581.
2560
1.24
21.
229
1.29
271.
2214
1.13
81.
590.
300.
30
201.
1222
1.19
23.
082
0.73
91.
049
1.93
00.
000.
060.
09
100.
8610
0.83
00.
000
0.00
50.
903
0.98
21.
64-0
.04
-0.0
5
80.
859
0.92
12.
861
0.68
30.
664
1.64
00.
00-0
.04
-0.0
2
150.
8615
0.83
00.
003
1.17
80.
972
0.43
21.
01-0
.07
-0.0
8
441.7
455
2.1
011
12.8
48
2.17
181.
5014
2.0
64
1.41
0.4
90.7
3
101.
4913
1.88
313.1
81
1.02
30.
956
3.3
90
0.00
0.09
0.15
10.
962
1.86
129
.38
00.
001
2.04
00.
000
0.00
0.00
0.02
11.
631
1.58
00.
000
0.00
13.
410
0.00
00.
000.
010.
01
21.
213
1.76
117
.33
14.
040
0.00
00.
001
5.40
0.01
0.03
12.
021
1.95
00.
000
0.00
00.
000
0.00
118
.27
0.01
0.01
961.
0411
91.2
423
7.0
114
0.99
420.
9432
1.33
80.
840.
100.
59
30.
633
0.61
00.
001
1.27
10.
431
0.86
00.
00-0
.05
-0.0
5
60.3
67
0.4
11
1.66
10.
382
0.2
53
0.70
00.
00-0
.28
-0.2
6
100.
8413
1.05
36.9
14
2.15
30.
522
0.65
10.
82-0
.05
0.02
121.
2713
1.33
13.
106
4.3
22
0.44
31.
181
0.96
0.07
0.08
171.
0623
1.39
610.6
65
2.09
20.2
69
2.13
10.
580.
030.
16
171.
1523
1.50
611.4
95
2.26
20.
289
2.3
01
0.63
0.06
0.19
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.03
-0.0
3
71.
228
1.35
14.
972
2.30
20.
732
1.34
11.
630.
030.
05
50.
865
0.83
00.
002
2.30
20.
730
0.00
11.
41-0
.02
-0.0
3
32.
835
4.5
72
57.1
10
0.00
12.
162
7.21
00.
000.
050.
10
130.
8713
0.84
00.
000
0.00
50.
705
1.27
31.
89-0
.05
-0.0
6
10.1
41
0.1
30
0.00
00.
001
0.29
00.
000
0.00
-0.1
6-0
.16
30.2
84
0.3
61
2.56
10.
611
0.19
10.
360
0.00
-0.2
0-0
.18
00.0
01
0.20
15.
480
0.00
00.
000
0.00
00.
00-0
.13
-0.1
0
30.
613
0.59
00.
001
1.36
10.
431
0.77
00.
00-0
.05
-0.0
5
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.02
-0.0
2
250.
7728
0.84
32.
604
0.83
110.
728
0.94
20.
56-0
.19
-0.1
4
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
EAR
EAR
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECONDCANCERSITE
99 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
7694
8497
8497
7694
6350
3033
1143
7694
8497
38208
3954
613
3857
9617
895
9889
4628
3820
839
546

ALLSITES,BUTSKINANDMYELOIDLEUKAEMIAS
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
PROSTATE
TESTIS
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
MYELOIDLEUKAEMIAS
POOLAIRTUM1976-2010,MEN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
LEUCEMIAMIELOIDE
POOLAIRTUM1976-2010,UOMINI:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRSTCANCERSITE
MYELOID
LEUKAEMIAS
MEN
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
252
0.99
348
1.2
596
3.8
353
0.7
213
41.
1050
1.15
150.
97-0
.10
3.4
1
201.8
222
1.8
32
1.98
41.
299
1.69
42.
093
4.33
0.48
0.49
72.6
68
2.7
91
4.27
00.
003
2.37
24.
242
11.4
40.
230.
25
10.
412
0.76
14.
860
0.00
10.
860
0.00
00.
00-0
.08
-0.0
3
122.0
112
1.84
00.
004
2.32
51.
732
2.00
12.
850.
320.
27
31.
105
1.68
27.
580
0.00
21.
521
2.18
00.
000.
020.
10
150.
9816
0.94
10.
603
0.65
111.
471
0.41
00.
00-0
.02
-0.0
5
361.
0458
1.5
222
6.4
07
0.70
191.
158
1.34
20.
940.
070.9
8
170.
7234
1.31
177.2
65
0.74
60.
534
0.98
21.
37-0
.35
0.40
191.7
224
1.9
85
4.5
72
0.63
132.4
64
2.11
00.
000.
420.5
9
50.
497
0.62
21.
982
0.67
30.
610
0.00
00.
00-0
.28
-0.2
1
20.
743
1.00
13.
500
0.00
21.
530
0.00
00.
00-0
.04
0.00
40.
585
0.66
11.
460
0.00
30.
911
0.86
00.
00-0
.15
-0.1
3
451.
0268
1.4
023
5.1
614
1.07
190.
8911
1.52
10.
400.
050.
96
82.
009
2.08
13.
101
0.99
42.
123
3.76
00.
000.
210.
23
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.07
-0.0
7
34.
954
6.0
21
17.0
00
0.00
310.2
10
0.00
00.
000.
130.
16
00.
001
0.94
111
.36
00.
000
0.00
00.
000
0.00
-0.0
50.
00
00.
001
3.26
139
.83
00.
000
0.00
00.
000
0.00
-0.0
10.
03
23.
602
3.28
00.
001
6.36
13.
760
0.00
00.
000.
080.
07
380.
7846
0.86
81.
698
0.58
231.
005
0.58
20.
63-0
.56
-0.3
6
00.
001
1.16
123
.10
00.
000
0.00
00.
000
0.00
-0.0
40.
01
161.9
921
2.3
95
6.8
27
3.1
76
1.57
32.
050
0.00
0.42
0.6
0
210.
7433
1.06
124.2
01
0.1
214
1.03
40.
852
1.22
-0.3
80.
10
210.
7833
1.11
124.3
91
0.1
314
1.08
40.
892
1.27
-0.3
20.
16
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.06
-0.0
6
61.
898
2.31
27.
071
1.15
31.
981
1.73
14.
740.
150.
22
53.3
66
3.7
71
9.41
00.
002
2.89
13.
162
15.5
00.
190.
22
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.04
-0.0
4
111.
4514
1.69
34.
302
0.96
61.
662
1.47
12.
030.
180.
28
20.
605
1.35
38.8
41
1.02
10.
620
0.00
00.
00-0
.07
0.06
10.1
74
0.60
34.
870
0.00
00.
001
1.00
00.
00-0
.27
-0.1
3
00.
002
0.63
26.
840
0.00
00.
000
0.00
00.
00-0
.15
-0.0
6
10.
371
0.33
00.
000
0.00
00.
001
2.19
00.
00-0
.09
-0.1
0
00.
001
2.09
120
.63
00.
000
0.00
00.
000
0.00
-0.0
20.
03
100.
7510
0.68
00.
001
0.26
30.
465
2.25
11.
33-0
.18
-0.2
3
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECONDCANCERSITE
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
EAR
EAR
100 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
7431
9849
9849
7431
4298
1254
395
7431
9849
18857
2025
113
9446
2191
0937
7613
5018
857
2025
1

ALLSITES,BUTSKINANDMYELOIDLEUKAEMIAS
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
CERVIXUTERI
CORPUSUTERI
OVARY
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
MYELOIDLEUKAEMIAS
POOLAIRTUM1976-2010,WOMEN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
LEUCEMIAMIELOIDE
POOLAIRTUM1976-2010,DONNE:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRSTCANCERSITE
MYELOID
LEUKAEMIAS
WOMEN
141
1.02
179
1.1
938
3.1
531
0.87
650.
9728
1.05
171.7
40.
121.
51
31.
674
2.05
16.
650
0.00
11.
161
2.82
17.
520.
070.
11
33.
184
3.9
01
12.2
20
0.00
12.
211
5.45
114
.64
0.12
0.16
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.02
-0.0
2
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.02
-0.0
3
11.
571
1.43
00.
001
5.83
00.
000
0.00
00.
000.
020.
02
101.
3011
1.30
11.
252
0.92
71.
851
0.77
00.
000.
130.
14
261.
2828
1.26
21.
055
0.92
111.
124
1.06
64.5
60.
320.
31
191.
3120
1.26
10.
734
1.03
81.
142
0.74
55.3
00.
260.
22
71.
208
1.25
11.
851
0.64
31.
062
1.85
12.
690.
070.
09
30.
885
1.33
25.
870
0.00
21.
200
0.00
14.
92-0
.02
0.07
41.
454
1.31
00.
001
1.29
21.
480
0.00
16.
490.
070.
05
50.
985
0.89
00.
000
0.00
10.
413
3.21
13.
05-0
.01
-0.0
3
80.
9614
1.55
68.1
93
1.41
10.
251
0.62
34.9
8-0
.02
0.27
31.
014
1.25
14.
690
0.00
21.
421
1.58
00.
000.
000.
04
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.02
-0.0
2
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.01
-0.0
1
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.04
-0.0
4
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.01
-0.0
1
300.
7840
0.97
103.4
02
0.2
214
0.76
121.
542
0.67
-0.4
8-0
.07
20.
913
1.27
15.
820
0.00
10.
941
2.35
00.
00-0
.01
0.03
30.
455
0.70
23.
780
0.00
20.
630
0.00
12.
11-0
.21
-0.1
1
30.
663
0.61
00.
000
0.00
20.
911
1.13
00.
00-0
.09
-0.1
0
51.
568
2.29
310.8
13
3.66
10.
651
1.61
00.
000.
100.
24
61.
226
1.12
00.
004
3.04
20.
840
0.00
00.
000.
060.
03
40.
874
0.80
00.
003
2.45
10.
450
0.00
00.
00-0
.03
-0.0
5
25.
962
5.42
00.
001
11.0
31
6.18
00.
000
0.00
0.10
0.09
31.
463
1.35
00.
000
0.00
33.
040
0.00
00.
000.
050.
04
72.
048
2.20
14.
942
2.83
31.
881
1.27
12.
960.
210.
24
11.
991
1.86
00.
001
8.76
00.
000
0.00
00.
000.
030.
02
71.
379
1.62
24.
504
3.06
20.
811
1.01
00.
000.
110.
19
20.
884
1.61
29.3
50
0.00
21.
820
0.00
00.
00-0
.02
0.08
00.
001
0.27
13.
120
0.00
00.
000
0.00
00.
00-0
.19
-0.1
4
00.
001
0.62
17.
010
0.00
00.
000
0.00
00.
00-0
.08
-0.0
3
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.09
-0.1
0
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.02
-0.0
2
90.
9312
1.13
33.
173
1.15
61.
280
0.00
00.
00-0
.04
0.08
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
EAR
EAR
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECONDCANCERSITE
101 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
6364
8572
8572
6364
3716
1224
374
6364
8572
17351
1855
312
0239
8183
1336
4414
1417
351
1855
3

ALLSITES,BUTSKINANDBREAST
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
PROSTATE
TESTIS
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
BREAST
POOLAIRTUM1976-2010,MEN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
MAMMELLA
POOLAIRTUM1976-2010,UOMINI:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRSTCANCERSITE
BREAST
MEN
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
221
1.11
236
1.1
515
2.3
734
1.19
109
1.17
581.
0920
0.84
2.36
3.17
121.
5412
1.49
00.
002
1.67
51.
333
1.49
22.
420.
450.
40
42.
174
2.10
00.
001
3.58
11.
131
2.09
15.
020.
230.
22
31.
843
1.78
00.
001
4.01
11.
261
2.38
00.
000.
150.
13
51.
155
1.12
00.
000
0.00
31.
431
0.90
12.
200.
070.
05
31.
453
1.40
00.
000
0.00
22.
031
1.85
00.
000.
100.
09
151.
2215
1.18
00.
001
0.54
111.
883
0.93
00.
000.
290.
24
281.
0228
0.99
00.
004
1.02
161.
256
0.81
20.
600.
05-0
.04
241.
2724
1.23
00.
004
1.50
131.
485
0.97
20.
850.
540.
46
40.
474
0.45
00.
000
0.00
30.
741
0.44
00.
00-0
.49
-0.5
0
70.
897
0.86
00.
000
0.00
30.
812
0.96
22.
17-0
.09
-0.1
1
31.
383
1.33
00.
000
0.00
10.
981
1.73
13.
870.
090.
08
61.
116
1.07
00.
001
1.29
10.
394
2.75
00.
000.
060.
04
330.
9643
1.21
108.9
25
0.99
150.
938
0.88
51.
27-0
.14
0.78
20.
732
0.71
00.
000
0.00
00.
001
1.35
12.
90-0
.08
-0.0
8
21.
952
1.89
00.
000
0.00
24.
210
0.00
00.
000.
100.
10
12.
361
2.29
00.
000
0.00
14.
940
0.00
00.
000.
060.
06
11.
471
1.42
00.
000
0.00
00.
001
5.51
00.
000.
030.
03
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.02
-0.0
2
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.05
-0.0
5
511.
3052
1.29
10.
8410
1.85
231.
2715
1.40
30.
601.
251.
19
14.
752
9.1
71
132.4
40
0.00
00.
001
19.3
20
0.00
0.08
0.18
142.3
115
2.4
01
5.29
55.8
15
1.76
21.
232
2.74
0.84
0.90
231.
0423
1.00
00.
002
0.62
151.
445
0.84
10.
380.
090.
01
221.
0422
1.00
00.
002
0.65
151.
514
0.71
10.
400.
080.
01
11.
041
1.01
00.
000
0.00
00.
001
3.84
00.
000.
000.
00
31.
373
1.33
00.
000
0.00
21.
921
1.74
00.
000.
090.
08
22.
372
2.29
00.
002
16.2
10
0.00
00.
000
0.00
0.12
0.12
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.04
-0.0
4
30.
544
0.70
15.
711
1.26
20.
770
0.00
00.
00-0
.27
-0.1
8
10.
381
0.37
00.
000
0.00
10.
800
0.00
00.
00-0
.17
-0.1
8
20.
442
0.42
00.
000
0.00
00.
002
1.65
00.
00-0
.27
-0.2
8
10.
461
0.44
00.
000
0.00
00.
001
1.75
00.
00-0
.13
-0.1
3
10.
491
0.47
00.
000
0.00
00.
001
1.81
00.
00-0
.11
-0.1
2
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.04
-0.0
4
80.
769
0.83
12.
961
0.66
40.
812
0.71
10.
80-0
.27
-0.1
9
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECONDCANCERSITE
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
EAR
EAR
102 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
1904
1982
1982
1904
1620
755
258
1904
1982
9402
9726
323
1458
4562
2391
991
9402
9726

ALLSITES,BUTSKINANDBREAST
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
CERVIXUTERI
CORPUSUTERI
OVARY
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
BREAST
POOLAIRTUM1976-2010,WOMEN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
MAMMELLA
POOLAIRTUM1976-2010,DONNE:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRSTCANCERSITE
BREAST
WOMEN
1059
71.1
211
137
1.1
454
02.2
311
321.
0044
321.0
930
921.1
519
411.2
10.8
61.0
7
178
1.04
187
1.07
92.
0616
0.78
720.
9856
1.16
341.
200.
010.
01
991.
1010
11.
102
0.89
70.
6642
1.10
321.
2518
1.17
0.01
0.01
421.
0645
1.11
32.
844
0.81
160.
9113
1.17
91.
480.
000.
00
370.
8941
0.96
43.
705
0.99
140.
7811
0.94
71.
040.
000.
00
811.3
488
1.4
27
4.5
98
1.12
291.
1320
1.17
242.3
00.
020.0
2
758
1.0
877
51.0
817
0.92
700.
8133
31.
1021
51.0
914
01.2
20.
040.
04
2124
1.1
021
711.1
047
0.97
232
1.02
910
1.1
159
91.
0938
31.1
50.1
50.1
5
1511
1.0
915
461.0
935
1.02
164
1.02
633
1.0
942
71.
0828
71.1
90.1
00.1
0
613
1.1
262
51.1
112
0.86
681.
0427
71.1
817
21.
1196
1.05
0.05
0.05
271
0.8
527
90.8
58
1.00
370.
9811
30.
8471
0.7
850
0.89
-0.0
4-0
.04
208
0.8
221
40.8
26
0.91
120.3
990
0.83
630.
8743
0.99
-0.0
4-0
.04
515
1.05
526
1.05
110.
9344
0.79
197
0.97
175
1.2
499
1.11
0.02
0.02
823
1.02
929
1.1
210
65.4
194
1.02
326
0.96
235
1.01
168
1.17
0.01
0.0
8
309
1.2
134
61.3
237
5.5
626
0.83
148
1.3
385
1.18
501.
240.0
40.0
6
290.
8430
0.85
11.
215
1.28
110.
765
0.50
81.
260.
000.
00
80.5
09
0.55
12.
451
0.53
20.
303
0.66
20.
71-0
.01
-0.0
1
831.5
383
1.4
90
0.00
60.
9133
1.41
261.7
018
2.0
20.0
20.0
2
151.
0315
1.00
00.
001
0.54
60.
944
0.99
41.
770.
000.
00
430.0
163
0.0
220
0.2
11
0.0
014
0.0
122
0.0
26
0.0
1-2
.74
-2.7
2
186
1.02
188
1.00
20.
3731
1.23
780.
9354
1.11
230.
950.
000.
00
1222
1.9
413
022.0
280
4.8
894
1.22
539
1.9
737
12.0
921
82.1
70.4
70.5
0
596
1.4
261
51.4
319
1.7
064
1.22
234
1.2
717
11.4
612
71.9
30.1
40.1
4
442
1.4
349
71.5
755
7.2
211
83.2
914
81.
1311
41.2
862
1.15
0.1
00.1
4
520
1.1
153
41.1
114
1.21
561.
0321
01.
0716
41.2
290
1.09
0.04
0.04
496
1.1
450
91.1
413
1.20
531.
0520
31.
1115
61.2
584
1.10
0.0
50.0
5
240.
7425
0.75
11.
263
0.81
70.
518
0.86
61.
02-0
.01
-0.0
1
138
0.7
314
20.7
44
0.82
140.
6163
0.7
833
0.6
228
0.90
-0.0
4-0
.04
376
1.3
740
11.4
225
3.3
942
1.21
168
1.3
811
91.5
547
1.15
0.0
80.0
9
300.
9437
1.12
77.3
86
1.36
120.
826
0.71
61.
350.
000.
00
453
0.95
489
1.00
362.9
846
0.81
177
0.87
138
1.01
921.
14-0
.02
0.00
201
0.93
209
0.95
81.
4821
0.83
820.
9055
0.90
431.
17-0
.01
-0.0
1
377
1.2
538
41.2
47
0.90
300.
8218
01.3
911
31.3
254
1.07
0.0
60.0
6
132
1.00
138
1.01
61.
7313
0.80
641.
1241
1.10
140.
640.
000.
00
223
1.5
322
41.5
01
0.27
140.
8110
91.7
566
1.6
034
1.37
0.0
60.0
6
220.
9122
0.88
00.
003
1.02
70.
686
0.87
61.
470.
000.
00
654
0.7
368
70.7
533
1.4
758
0.5
527
10.7
119
70.7
812
80.8
2-0
.19
-0.1
7
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
EAR
EAR
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECONDCANCERSITE
103 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
215809
2222
4622
2246
2158
0919
3012
1034
6942
199
2158
0922
2246
1274882
1311
356
3647
417
0096
5783
4934
5731
1807
0712
7488
213
1135
6

ALLSITES,BUTSKINANDCERVIXUTERI
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
CERVIXUTERI
CORPUSUTERI
OVARY
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
CERVIXUTERI
POOLAIRTUM1976-2010,WOMEN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
CERVICEUTERINA
POOLAIRTUM1976-2010,DONNE:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRSTCANCERSITE
CERVIXUTERI
WOMEN
870
1.2
399
91.3
712
97.0
011
71.4
531
11.2
521
91.1
522
31.1
81.8
43.0
2
232.4
124
2.4
51
4.15
00.
0012
3.6
37
2.7
14
1.55
0.1
50.1
6
112.2
912
2.4
41
8.30
00.
005
3.07
32.
323
2.23
0.07
0.08
52.
085
2.03
00.
000
0.00
22.
343
4.55
00.
000.
030.
03
72.9
97
2.9
20
0.00
00.
005
6.0
81
1.59
11.
610.
050.
05
51.
635
1.59
00.
000
0.00
21.
911
1.24
22.
330.
020.
02
451.
2545
1.21
00.
0011
2.4
111
0.85
111.
1712
1.32
0.10
0.09
139
1.3
914
61.4
37
2.6
615
1.32
451.
3138
1.4
341
1.4
90.4
50.4
9
881.
2493
1.2
85
2.69
91.
1329
1.20
281.
4922
1.11
0.20
0.23
511.7
653
1.7
82
2.58
61.
7816
1.58
101.
2919
2.4
50.2
50.2
6
150.
9415
0.91
00.
001
0.55
30.
557
1.68
40.
88-0
.01
-0.0
2
141.
0914
1.06
00.
000
0.00
51.
124
1.19
51.
430.
010.
01
271.
1327
1.10
00.
006
2.25
121.
514
0.63
50.
710.
030.
03
123
2.9
313
03.0
27
6.7
912
2.6
651
3.6
335
3.1
025
2.0
60.9
30.9
7
191.
2020
1.23
12.
511
0.56
101.
744
0.92
41.
010.
040.
04
42.
214
2.16
00.
000
0.00
11.
691
2.07
23.
670.
030.
02
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.01
-0.0
1
51.
605
1.56
00.
000
0.00
10.
891
1.19
33.
730.
020.
02
11.
161
1.13
00.
001
9.27
00.
000
0.00
00.
000.
000.
00
182
0.8
620
50.
9423
4.3
123
0.97
710.
9348
0.83
400.
74-0
.35
-0.1
4
10.0
815
1.15
1437.3
00
0.00
10.
200
0.00
00.
00-0
.13
0.02
90.2
573
1.9
764
69.5
65
1.22
00.0
01
0.1
03
0.3
2-0
.31
0.4
0
170.
6921
0.84
46.1
98
2.8
05
0.57
10.1
53
0.49
-0.0
9-0
.05
191.
1622
1.31
37.3
85
2.80
20.
365
1.12
71.
520.
030.
06
692.9
172
2.9
63
4.84
103.7
533
4.1
15
0.80
213.1
30.5
20.5
3
693.1
272
3.1
83
5.1
910
4.0
233
4.4
05
0.85
213.3
60.5
40.5
5
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.02
-0.0
2
80.
768
0.74
00.
000
0.00
30.
804
1.42
10.
36-0
.03
-0.0
3
180.
9719
1.00
12.
220
0.00
81.
185
0.97
51.
10-0
.01
0.00
73.0
57
2.9
60
0.00
26.
383
3.23
11.
681
2.18
0.05
0.05
291.
1132
1.19
34.
505
1.71
50.
5510
1.42
91.
270.
030.
06
110.
9811
0.96
00.
002
1.57
30.
783
1.01
30.
970.
00-0
.01
201.
2520
1.21
00.
003
1.58
81.
424
0.94
51.
180.
050.
04
71.
007
0.98
00.
002
2.41
20.
811
0.54
21.
090.
000.
00
121.
5312
1.49
00.
001
1.10
62.
182
0.96
31.
430.
050.
04
10.
831
0.80
00.
000
0.00
00.
001
3.20
00.
000.
000.
00
611.3
573
1.5
712
9.6
77
1.32
171.
0919
1.60
181.
440.
180.2
9
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
EAR
EAR
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECONDCANCERSITE
104 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
14511
1518
215
182
1451
112
063
6295
3321
1451
115
182
87455
8992
824
7311
059
3405
723
368
1897
287
455
8992
8

ALLSITES,BUTSKINANDCORPUSUTERI
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
CERVIXUTERI
CORPUSUTERI
OVARY
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
CORPUSUTERI
POOLAIRTUM1976-2010,WOMEN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
CORPODELL’UTERO
POOLAIRTUM1976-2010,DONNE:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRSTCANCERSITE
CORPUSUTERI
WOMEN
2614
1.2
328
211.2
920
73.7
731
51.2
710
721.2
970
61.1
852
11.1
62.4
13.0
7
200.
6921
0.71
11.
335
1.46
90.
784
0.49
20.
34-0
.04
-0.0
4
100.
6610
0.64
00.
002
1.15
61.
021
0.23
10.
30-0
.03
-0.0
3
40.
625
0.75
15.
601
1.23
20.
751
0.55
00.
00-0
.01
-0.0
1
60.
836
0.81
00.
002
2.28
10.
342
0.99
10.
71-0
.01
-0.0
1
60.
586
0.56
00.
001
0.85
30.
762
0.68
00.
00-0
.02
-0.0
2
126
1.02
127
1.00
10.
319
0.62
491.
0332
0.92
361.
340.
010.
00
458
1.3
548
11.3
823
2.7
040
1.04
196
1.5
113
11.3
691
1.21
0.5
80.6
4
326
1.3
434
01.3
614
2.3
226
0.95
147
1.5
991
1.3
262
1.14
0.4
10.4
4
132
1.3
714
11.4
29
3.6
114
1.24
491.
3040
1.4
729
1.41
0.1
70.2
0
480.
8250
0.83
21.
373
0.46
190.
8615
0.91
110.
81-0
.05
-0.0
5
420.
9142
0.89
00.
002
0.38
170.
979
0.70
141.
36-0
.02
-0.0
3
921.
0792
1.04
00.
004
0.43
341.
0725
1.02
291.
410.
030.
02
220
1.5
523
41.6
114
4.0
610
0.64
105
1.9
560
1.4
945
1.4
10.3
90.4
3
581.4
361
1.4
63
2.82
71.
4418
1.10
161.
4117
2.1
10.
090.
09
91.
489
1.45
00.
001
1.51
52.
182
1.16
10.
720.
010.
01
20.
702
0.68
00.
001
3.10
10.
940
0.00
00.
000.
000.
00
181.9
618
1.9
10
0.00
00.
007
1.93
62.
345
2.61
0.04
0.04
41.
594
1.55
00.
002
6.49
00.
002
2.85
00.
000.
010.
01
841
1.4
488
41.4
843
2.7
411
71.6
434
11.4
423
11.4
215
21.3
61.2
81.3
8
80.2
720
0.65
1213.3
34
0.99
30.2
31
0.1
20
0.0
0-0
.11
-0.0
5
00.0
013
0.1
113
4.3
30
0.0
00
0.0
00
0.0
00
0.0
0-0
.55
-0.4
8
450.6
310
91.4
864
32.9
926
2.9
612
0.4
14
0.2
03
0.2
2-0
.13
0.1
7
931.7
110
81.9
315
11.2
024
3.9
339
1.8
617
1.09
131.
090.1
90.2
5
981.
1810
71.2
69
4.4
19
0.97
481.5
321
0.89
201.
070.
080.
11
931.
2110
21.2
99
4.7
28
0.93
441.5
121
0.96
201.
150.
080.
11
50.
885
0.86
00.
001
1.65
41.
920
0.00
00.
000.
000.
00
411.
2343
1.26
22.
314
1.02
141.
0614
1.49
91.
300.
040.
04
521.
2653
1.25
10.
879
1.72
271.5
611
0.97
50.
700.
050.
05
91.
759
1.70
00.
000
0.00
52.
333
2.14
11.
080.
020.
02
901.
0793
1.08
31.
4210
1.04
290.
8929
1.22
221.
230.
030.
03
391.
0140
1.01
11.
032
0.45
120.
8114
1.29
111.
300.
000.
00
641.
2065
1.19
10.
735
0.81
271.
3224
1.6
08
0.68
0.05
0.05
190.
8020
0.83
11.
632
0.72
70.
765
0.75
50.
99-0
.02
-0.0
2
391.5
439
1.5
00
0.00
31.
0418
1.8
516
2.2
42
0.35
0.07
0.06
61.
396
1.36
00.
000
0.00
21.
233
2.49
11.
010.
010.
01
131
0.85
143
0.90
123.1
220
1.15
520.
9033
0.76
260.
73-0
.11
-0.0
7
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
EAR
EAR
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECONDCANCERSITE
105 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
34142
3549
735
497
3414
229
060
1540
673
3934
142
3549
7
201942
2077
4458
0226
265
8467
155
061
3594
520
1942
2077
44

ALLSITES,BUTSKINANDOVARY
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
CERVIXUTERI
CORPUSUTERI
OVARY
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
OVARY
POOLAIRTUM1976-2010,WOMEN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
OVAIO
POOLAIRTUM1976-2010,DONNE:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRSTCANCERSITE
OVARY
WOMEN
853
1.1
815
862.0
973
320.3
315
11.
1434
61.
1021
41.3
114
21.2
71.5
39.3
6
131.
3115
1.44
24.
180
0.00
10.
238
3.5
54
2.60
0.04
0.05
71.
388
1.51
14.
050
0.00
00.
005
4.3
12
2.45
0.02
0.03
31.
253
1.19
00.
000
0.00
00.
002
3.67
12.
830.
010.
01
31.
224
1.55
18.
370
0.00
10.
921
1.81
12.
710.
010.
02
51.
546
1.75
15.
780
0.00
10.
721
1.37
35.7
20.
020.
03
521.3
959
1.4
97
3.2
25
0.68
231.
4217
2.0
57
1.24
0.17
0.22
157
1.4
729
42.6
213
724.8
034
1.7
362
1.3
536
1.4
925
1.47
0.6
02.0
6
110
1.4
521
72.7
210
727.2
622
1.58
431.
3226
1.51
191.
550.4
01.5
5
471.5
277
2.3
730
18.7
712
2.0
919
1.42
101.
446
1.26
0.19
0.5
0
110.
6315
0.82
44.2
51
0.30
30.
405
1.29
20.
71-0
.08
-0.0
4
130.
9414
0.96
11.
292
0.75
81.
353
0.98
00.
00-0
.01
-0.0
1
351.
3535
1.28
00.
007
1.48
111.
0110
1.70
71.
600.
110.
09
461.
0255
1.16
94.1
05
0.62
150.
7813
1.26
131.
740.
010.
09
140.
8915
0.92
11.
434
1.46
40.
585
1.38
10.
41-0
.02
-0.0
2
21.
033
1.47
110
.97
00.
001
1.21
00.
001
3.02
0.00
0.01
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.01
-0.0
1
20.
623
0.89
16.
420
0.00
10.
711
1.38
00.
00-0
.01
0.00
11.
121
1.07
00.
000
0.00
00.
000
0.00
17.
860.
000.
00
267
1.2
532
71.4
660
6.0
330
0.78
127
1.3
468
1.4
042
1.32
0.6
41.1
7
70.
6027
2.2
020
33.9
14
1.76
20.
380
0.00
10.
66-0
.06
0.1
7
350.
9246
711.6
743
2238.1
522
3.1
37
0.4
14
0.47
20.
36-0
.04
4.8
4
10.0
410
0.3
89
7.2
51
0.21
00.0
00
0.0
00
0.00
-0.2
9-0
.19
211.
1941
2.2
220
23.5
07
2.21
81.
054
1.00
20.
700.
040.2
6
371.4
447
1.7
510
7.5
45
1.06
131.
197
1.21
122.8
80.
140.2
3
371.5
545
1.7
98
6.4
75
1.14
131.
277
1.29
123.1
00.
160.2
3
00.
002
1.11
222.0
90
0.00
00.
000
0.00
00.
00-0
.02
0.00
50.
456
0.51
11.
830
0.00
30.
612
0.80
00.
00-0
.07
-0.0
6
181.
0019
1.01
11.
363
0.99
101.
251
0.23
41.
470.
000.
00
52.
265
2.15
00.
002
4.87
21.
991
1.99
00.
000.
030.
03
250.
9130
1.04
53.7
05
1.00
80.
676
0.96
61.
39-0
.03
0.01
70.
589
0.71
23.
222
0.90
30.
582
0.74
00.
00-0
.06
-0.0
4
221.
3022
1.24
00.
003
0.94
121.
646
1.59
10.
380.
060.
05
20.2
72
0.2
60
0.00
00.
001
0.31
10.
610
0.00
-0.0
6-0
.07
151.8
315
1.74
00.
002
1.32
71.
985
2.70
10.
770.
080.
07
53.8
85
3.6
70
0.00
13.
994
7.2
50
0.00
00.
000.
040.
04
531.
0971
1.3
918
6.9
610
1.12
210.
9814
1.30
81.
040.
050.
22
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
EAR
EAR
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECONDCANCERSITE
106 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
21956
2585
225
852
2195
616
049
5727
2427
2195
625
852
84295
8823
539
3915
477
3813
619
106
1157
684
295
8823
5

ALLSITES,BUTSKINANDPROSTATE
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
PROSTATE
TESTIS
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
PROSTATE
POOLAIRTUM1976-2010,MEN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
PROSTATA
POOLAIRTUM1976-2010,UOMINI:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRSTCANCERSITE
PROSTATE
MEN
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
1095
60.9
313
186
1.0
822
304.9
022
441.0
957
580.9
024
100.8
854
40.8
7-1
.55
1.6
2
396
0.7
941
60.8
020
0.93
680.7
122
90.8
386
0.82
130.
62-0
.19
-0.1
8
810.6
984
0.6
93
0.61
90.4
052
0.80
170.
683
0.58
-0.0
7-0
.07
830.
8487
0.84
40.
9217
0.87
490.
8917
0.85
00.0
0-0
.03
-0.0
3
232
0.8
224
50.8
313
1.07
420.
7712
80.8
252
0.87
100.
83-0
.09
-0.0
9
118
0.8
212
70.
859
1.54
281.
0758
0.7
429
0.91
30.
43-0
.05
-0.0
4
825
0.9
086
40.9
139
1.09
135
0.8
446
60.
9519
00.
8934
0.6
7-0
.16
-0.1
5
2294
1.1
023
891.1
095
1.21
403
1.1
312
471.1
151
21.
0413
21.
150.3
80.3
9
1600
1.1
016
681.1
068
1.26
272
1.11
894
1.1
535
01.
0084
1.03
0.2
60.2
8
694
1.1
072
11.1
027
1.10
131
1.18
353
1.03
162
1.11
481.4
70.
110.
11
368
0.6
338
50.6
317
0.74
720.6
917
40.5
510
60.8
016
0.5
5-0
.40
-0.3
9
140
0.8
214
70.8
37
1.11
160.5
688
0.97
290.
717
0.71
-0.0
5-0
.05
395
0.96
410
0.96
150.
9785
1.21
192
0.87
960.
9922
0.96
-0.0
3-0
.03
1871
0.7
421
450.8
227
42.7
637
80.8
497
90.7
143
00.7
584
0.6
6-1
.20
-0.8
4
251
1.3
127
31.3
822
3.0
852
1.5
912
61.2
260
1.3
413
1.27
0.1
10.1
3
971.2
410
41.2
87
2.38
141.
0457
1.3
324
1.32
20.
510.
030.
04
381.
2344
1.37
65.0
86
1.12
191.
1512
1.66
10.
570.
010.
02
561.
1558
1.15
21.
088
0.95
301.
1515
1.31
31.
120.
010.
01
131.
1314
1.17
12.
085
2.33
50.
803
1.18
00.
000.
000.
00
300.
9636
1.11
65.0
57
1.30
150.
897
0.96
10.
600.
000.
01
20.0
06
0.0
04
0.0
30
0.0
01
0.0
01
0.0
00
0.0
0-5
.75
-5.7
2
30.3
26
0.61
37.4
31
0.56
10.
191
0.50
00.
00-0
.01
-0.0
1
543
1.2
564
61.4
310
36.1
222
72.9
621
70.
9284
0.84
150.
680.2
00.3
4
1845
1.1
132
961.9
014
5122.7
842
41.4
698
61.1
033
70.8
698
1.09
0.3
32.7
5
1782
1.1
232
091.9
414
2723.4
241
01.4
895
81.1
232
20.8
792
1.08
0.3
52.7
3
630.
8487
1.12
248.6
714
1.11
280.
7015
0.83
61.
34-0
.02
0.02
132
0.89
138
0.89
61.
0030
1.10
580.7
135
1.06
91.
29-0
.03
-0.0
3
801.5
086
1.5
56
2.73
212.1
039
1.31
171.
513
1.39
0.0
50.0
5
170.
7524
1.02
77.3
96
1.41
90.
732
0.41
00.
00-0
.01
0.00
400
1.00
429
1.03
291.8
885
1.21
200
0.92
890.
9626
1.24
0.00
0.02
198
0.99
211
1.02
131.
7237
1.08
115
1.08
370.
789
0.81
0.00
0.01
339
0.99
376
1.06
372.8
251
0.86
179
0.98
891.
1120
1.06
0.00
0.04
141
0.89
170
1.03
294.6
225
0.88
720.
8433
0.90
111.
29-0
.03
0.01
182
1.16
188
1.15
61.
0223
0.86
100
1.19
501.
339
1.01
0.05
0.04
160.
6518
0.70
22.
063
0.69
70.
546
1.03
00.
00-0
.02
-0.0
1
507
0.6
356
20.6
855
1.8
685
0.6
326
90.6
312
00.6
233
0.6
9-0
.54
-0.4
7
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECONDCANCERSITE
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
EAR
EAR
107 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
135708
1432
4114
3241
1357
0811
4414
4419
995
6713
5708
1432
41
547059
5702
0723
148
1039
8030
1800
1167
5624
523
5470
5957
0207

ALLSITES,BUTSKINANDTESTIS
HEADANDNECK
ORALCAVITY
PHARYNX
LARYNX
OESOPHAG
US
STOMACH
COLONRECTUM
COLON
RECTUM
LIVER
GALLBLADDER
PANCREAS
LUNG
SKINMELANOMA
MESOTHELIOMA
KAPOSISARCOMA
SOFTTISSUE
BONE
BREAST
PROSTATE
TESTIS
KIDNEY
ANDRENALPELVIS
BLADDER
ANDURINARY
TRACT
URINARY
BLADDER
URINARY
TRACT
BRAINANDCENTRALNERVOUSSYSTEM
THYROID
HODGKINLYMPHOMA
NON-HODGKINLYMPHOMA
MYELOMA
LEUKAEM
IAS
LYMPHOIDLEUKAEM
IAS
MYELOIDLEUKAEM
IAS
OTHER
LEUKAEM
IAS
OTHER
ANDILLDEFINED
SITES
TESTIS
POOLAIRTUM1976-2010,MEN:
Num
bero
fsubjectsa
liveatthebeginningoftheinterval,person-yearsa
trisk
(PY),num
bero
fObserved(O)
second
cancers,Standardized
IncidenceRatio
(SIR)and
ExcessAb
soluteRisk
(EAR
)x1000
cancerpatientsb
ysecond
cancersiteandfollow-upperio
d.
TESTICOLO
POOLAIRTUM1976-2010,UOMINI:
Num
erodisoggettiviviall’iniziodell’intervallo,annipersona
arischio(PY),num
erodiseconditum
ori
osservati(O),rapporto
standardizzato
diincidenza(SIR)edeccessoassoluto
dirischio
(EAR
)x1000
pazientipersededisecondotumoreeperio
dodifollow-up.
FIRSTCANCERSITE
TESTIS
MEN
EAR
Exce
ssAb
solu
teRi
skEc
cess
oas
solu
todi
risch
ioSIR
Stan
dard
ized
Incid
ence
Ratio
Rapp
orto
stan
dard
izzat
odi
incid
enza
OO
bser
ved
case
sCa
sios
serv
ati
Decr
ease
/Dife
ttoIn
crea
se/E
cces
so
246
1.2
425
61.2
710
3.2
127
1.8
861
1.05
651.
1693
1.3
30.8
70.9
8
131.
0813
1.07
00.
001
1.18
20.
565
1.43
51.
220.
020.
01
41.
234
1.21
00.
000
0.00
00.
002
2.09
21.
810.
010.
01
41.
244
1.22
00.
000
0.00
00.
002
2.10
21.
800.
010.
01
50.
905
0.89
00.
001
2.50
21.
201
0.63
10.
53-0
.01
-0.0
1
20.
842
0.82
00.
000
0.00
00.
001
1.46
11.
18-0
.01
-0.0
1
141.
3814
1.35
00.
001
1.24
20.
633
1.05
82.4
10.
070.
07
301.
1930
1.17
00.
004
2.33
70.
9810
1.41
90.
970.
090.
08
261.5
526
1.53
00.
003
2.65
71.
498
1.71
81.
280.
170.
16
40.
474
0.47
00.
001
1.71
00.
002
0.83
10.
33-0
.08
-0.0
8
91.
229
1.20
00.
000
0.00
31.
451
0.48
51.
810.
030.
03
42.
504
2.46
00.
000
0.00
00.
002
4.51
23.
530.
040.
04
61.
206
1.18
00.
000
0.00
00.
003
2.13
31.
640.
020.
02
270.
9029
0.95
24.
214
1.84
70.
797
0.83
90.
85-0
.06
-0.0
3
111.
5911
1.57
00.
001
1.81
20.
884
1.96
41.
950.
080.
07
10.
961
0.95
00.
000
0.00
00.
000
0.00
12.
460.
000.
00
22.
162
2.12
00.
000
0.00
12.
911
3.65
00.
000.
020.
02
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.03
-0.0
3
12.
031
1.99
00.
000
0.00
00.
001
7.35
00.
000.
010.
01
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.01
-0.0
1
291.
0230
1.04
12.
671
0.59
81.
149
1.19
110.
900.
010.
02
00.0
00
0.0
00
0.00
00.
000
0.00
00.
000
0.00
-0.0
9-0
.09
121.
4815
1.8
33
25.6
51
1.82
31.
283
1.28
51.
750.
070.
12
261.
3326
1.31
00.
002
1.43
61.
053
0.55
152.1
60.
120.
11
261.
3926
1.36
00.
002
1.49
61.
103
0.57
152.2
50.
130.
12
00.
000
0.00
00.
000
0.00
00.
000
0.00
00.
00-0
.01
-0.0
1
61.
426
1.39
00.
000
0.00
21.
412
1.63
21.
620.
030.
03
102.8
811
3.1
11
15.9
01
3.33
43.
362
1.94
33.
160.
120.
13
31.
294
1.68
116
.55
27.
100
0.00
00.
001
2.38
0.01
0.03
131.
4513
1.42
00.
006
8.2
93
1.03
31.
151
0.36
0.07
0.07
10.
413
1.21
253.1
40
0.00
00.
000
0.00
11.
15-0
.03
0.01
142.6
414
2.5
90
0.00
36.7
14
2.32
42.
663
1.85
0.1
60.
15
62.
426
2.38
00.
003
15.1
30
0.00
22.
841
1.26
0.06
0.06
72.7
67
2.7
10
0.00
00.
004
4.7
32
2.78
11.
330.
080.
08
13.
441
3.37
00.
000
0.00
00.
000
0.00
112
.53
0.01
0.01
121.
1512
1.13
00.
000
0.00
72.
141
0.34
41.
180.
030.
02
� � �
≥2months
≥0months
0-1months
2-11
months
12-59months
60-119
months
≥120
months
≥2months
≥0months
mo
nth
saf
ter
firs
tca
nce
r
No.ofsubjectsaliveatintervalbeginning
Person-years
SECONDCANCERSITE
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
OSIR
EAR
EAR
108 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
7739
7954
7954
7739
6951
4234
2115
7739
7954
54475
5578
213
0761
1521
837
1554
410
979
5447
555
782

Capitolo 5
I tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI
Epidemiol Prev 37 (4-5) Suppl 1:1-152 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.it109
Valutazione delle associazionitra soggetti con tre o più tumoriEvaluation of associationsin subjects with three or more cancers
As a result of earlier and more accurate diagnoses, improvedtreatment, and greater life expectancy, occurrence of secondcancers has become more likely among long-term cancer sur-vivors.1-3 Although rarer, even individuals diagnosed with morethan two cancers are not an exceptional finding in the literature(case reports, clinical series).4-6
The large number of cases analyzed in this monograph (over1.6 million cancer patients followed for 14.2 years on average)allowed the authors to evaluate not just the incidence of secondcancers, but also the association of three or more cancers.Because of the special nature of individuals with three or morecancers, all cancers diagnosed during the period of observation,synchronous and metachronous, were included in the analysishere presented. The objective is to define common profiles ofassociations.In this regard, it is important to point out that, unlike in therest of the monograph, results in this chapter are not presentedas comparisons between observed and expected number of cases.A merely descriptive analysis is presented, because an evaluationof incidence for all possible cancer site combinations was notconsidered feasible. If all types of association had been consideredand listed by order of frequency, a huge number of unmanage-able indicators would have resulted, and the only way to analyzethem would have been to make this chapter disproportionatelyimbalanced compared to the others. It was chosen to discussthe results in a manner that is more descriptive, but nonethelessuseful and exhaustive, since this is a field that has yet to be ex-plored in population-based studies.The patients evaluated were 5,565, diagnosed with three ormore malignant tumours (excluding non-melanoma skin can-cer), equal to 0.3% of all subjects examined in this monograph(table 1); among these, 246 patients were diagnosed with fourcancers, 9 with five cancers.The total number of subjects with three or more cancers wassignificantly higher among males than among females (4,127vs. 1,438, M/F: 3) (table 1).This discrepancy can be interpreted by analyzing the distributionof cancers by site: in men the most frequent malignancy is prostatecancer, which is present in 50% of patients with three cancers andin 58% of those with four cancers (data not shown in the table).The most plausible hypothesis is that this apparent disparity islinked to the increasing use of spontaneous screening by Prostatic
L’incremento delle capacità diagnostiche e la maggiore effi-cacia delle strategie terapeutiche, congiuntamente al continuoaumento dell’aspettativa di vita, hanno portato a considerareil fenomeno dei secondi tumori come un’evenienza non tra-scurabile negli individui lungo sopravviventi a una primaneoplasia.1-3 E’ più raro, ma non eccezionale, il riscontro inletteratura (case report, serie cliniche) di individui con diagnosiin vita di un numero di neoplasie superiore a due.4-6
La numerosità della casistica analizzata nella presente mono-grafia (oltre 1.600.000 pazienti oncologici seguiti per una du-rata di follow-up medio tra i registri di 14,2 anni) ha reso pos-sibile la valutazione dell’incidenza non solo dei seconditumori, ma anche dell’associazione di tre o più tumori.Considerata la peculiarità di questa casistica di individui conalmeno tre neoplasie, nell’analisi dei dati qui presentatisono stati inclusi tutti i tumori, sincroni e metacroni, dia-gnosticati nel corso del periodo di rilevazione, al fine di de-lineare profili comuni delle associazioni.A tal proposito, appare opportuno specificare che, a differenzadelle altre sezioni della presentemonografia, i risultati di questocapitolo non sono espressi in termini di confronto fra osservatie attesi, poiché non è stato ritenuto perseguibile l’obiettivo divalutare l’incidenza di tutte le combinazioni di sedi possibili. In-fatti le tipologie di associazione, conservandone l’ordine, sareb-bero state troppo numerose e ingestibili per l’analisi, se non acosto di un approfondimento specifico e pesante che avrebbesbilanciato i contenuti a sfavore degli altri argomenti del lavoro.Si è quindi preferito presentare i risultati in formapiù descrittiva,ma che si ritiene comunque utile ed esaustiva in un ambito cheperaltro non trova molti riscontri in letteratura.Sono stati individuati 5.565 pazienti con diagnosi di tre o piùtumori maligni (esclusi i tumori non melanomatosi dellacute), pari allo 0,3% di tutti i soggetti considerati (tabella 1);di questi, in 246 pazienti è stata posta diagnosi di quattro tu-mori, mentre in 9 di cinque.L’analisi della casistica stratificata per genere evidenzia per ilsesso maschile un numero di soggetti con tre o più tumorinettamente superiore a quello riscontrabile nel sesso femmi-nile (4.127 vs. 1.438; M/F: 3) (tabella 1).Tale sproporzione appare interpretabile analizzando la distri-buzione per sede dei tumori: negli uomini è preponderanteil ruolo svolto dal tumore della prostata, presente nel 50% dei
WWW.EPIPREV.IT

Specific Antigen (PSA) testing, which may be followed by ad-ditional specific diagnostic procedures; these could be responsiblefor a proportion of over-diagnosed cases, which would haveotherwise remained indolent.This hypothesis is corroborated by observing how in men withthree cancers the proportion of prostate cancer out of the totalnumber of cases is different if the period considered is up to1992 or after 1992. This cut-off was defined on the basis ofthe dramatic increase in prostate cancer incidence observedsince 1992, potentially associated with the use of PSA as anopportunistic screening test.7
Ultimately, if the data on prostate cancer were to be consideredas an “artefact” and prostate cancer were excluded from theevaluation of the associations, there would be a significant re-duction in differences among males and females (M/F: 1.5).In the coming years, it is likely that other cancers characterizedby growing diagnostic intensity will increase in incidence, in-cluding incidence in combinations of multiple primaries, es-pecially if they have a good prognosis.8 This is the case, for ex-ample, of thyroid cancer: it currently represents 8% of the as-sociations of three cancers in women and 2% of those in men.Analyzing the cases as a whole, it can be observed that amongpatients with three or more cancers the median age of firstcancer onset is 64 years for women and 68 for men; the meaninterval between 1st and 2nd diagnosis is about 4 years, it isabout 3 years between 2nd and 3rd diagnosis, and about 2 yearsbetween 3rd and 4th diagnosis.Grouping the sites by system, the most frequent regions are thegenitourinary tract, prostate, lung and bowel for men; breast,bowel and reproductive system for women. This figure is inagreement with the high incidence of cancers arising in the or-gans involved and the increased survival observed for specificsites (cancer of the breast, prostate, colon, bladder).9
In line with data from clinical series, colorectal cancer was foundto be a common event, present in 38% of all associations.4
The considerations offered in the chapter on second cancer riskamong cancer patients (pp. 18-30) are also valid for the in-terpretation of associations in subjects with three or more cancers.
Valutazione delle associazioni tra soggetti con tre o più tumoriI tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI
110 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
casi con associazione di tre tumori e nel 58% di quelli conquattro (dati non mostrati in tabella).L’ipotesi più plausibile è che tale evidente disparità sia legataalla crescente diffusione dello screening spontaneo individualeattraverso il dosaggio del marcatore sierologico PSA (ProstaticSpecific Antigen), seguito da eventuali ulteriori esami strumen-tali specifici, potenzialmente responsabile di una quota di casisovradiagnosticati, ovvero di neoplasie che sarebbero state al-trimenti caratterizzate da un decorso occulto o che comunquenon avrebbero inciso sulla durata della vita.Una conferma circa la plausibilità di tale ipotesi si ottiene os-servando che negli uomini con 3 neoplasie il tumore dellaprostata assume un peso relativo sul totale della casisticamolto diverso se questa viene considerata per il periodo finoal 1992 oppure dopo il 1992 come periodo temporale di in-cidenza del tumore prostatico. Tale spartiacque è stato de-finito sulla base dell’evidenza dell’incremento drammaticodell’incidenza di neoplasie maligne della prostata a partiredal 1992, potenzialmente associabile all’utilizzo del PSAcome test di screening opportunistico.7
In definitiva, se considerassimo il dato sul tumore della prostatacome un “artefatto” e lo escludessimo dalla valutazione delleassociazioni di tre o più tumori, si osserverebbe una riduzionenotevole delle differenze di genere (M/F: 1,5). E’ prevedibileche nel corso dei prossimi anni altre neoplasie, per le quali esi-ste un incremento dell’attività e della pressione diagnostica, au-mentino la loro incidenza, quindi anche nelle combinazionidi più tumori, in particolare se caratterizzate da una buona so-pravvivenza.8 E’ il caso, per esempio, delle neoplasie della ti-roide, attualmente presenti nell’8%delle associazioni di tre tu-mori nelle donne e nel 2% di quelle degli uomini.Dall’analisi della casistica nel suo insieme si osserva che tra isoggetti con tre o più diagnosi oncologiche l’età mediana diinsorgenza della prima neoplasia è 64 anni per le donne e 68per gli uomini; l’intervallo medio di diagnosi è di circa 4 annitra la prima e la seconda, circa 3 anni tra la seconda e la terza,circa 2 anni tra la terza e la quarta.Raggruppando le sedi per apparato, i distretti che compa-
NUMBER OF CANCERS NUMBER OF PATIENTS
MEN WOMEN TOTALNo. % No. % No. %
Only one cancer 819 732 92.6 722 306 95.3 1 542 038 93.8
2 cancers 61 086 6.9 34 528 4.6 95 614 5.8
3 cancers 3 924 0.4 1 386 0.2 5 310 0.3
4 cancers 197 <0.1 49 <0.1 246 <0.1
5 cancers 6 <0.1 3 <0.1 9 <0.1
Total 884 945 100.0 758 272 100.0 1 643 217 100.0
Tabella 1. Pazienti analizzati nel presente studio (esclusi tumori non melanomatosi della cute) per numero di tumori malignie genere. Numero assoluto e percentuale sul numero totale di pazienti.Table 1. Patients analyzed in the present monograph (excluding non-melanoma skin cancer), by number of malignancies andgender. Absolute number and percentage out of the total number of patients.

Valutazione delle associazioni tra soggetti con tre o più tumoriI tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI
111 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
iono con maggior frequenza sono quello genitourinario, laprostata, il polmone e il distretto intestinale per gli uomini;la mammella, il distretto intestinale e quello ginecologico perle donne. Tale dato è in linea con l’incidenza elevata delleneoplasie insorgenti negli organi interessati e con la maggioresopravvivenza osservata per alcune sedi (tumore della mam-mella, prostata, colon, vescica).9 In accordo con quanto ri-portato nelle serie cliniche, il tumore del colon retto rappre-senta un evento comune, presente nel 38% di tutte leassociazioni considerando la totalità della casistica.4
Nell’interpretazione di alcune associazioni osservate nei sog-getti con tre o più neoplasie sono valide le considerazioni fattenel capitolo sul rischio di secondi tumori nei pazienti onco-logici, al quale si rimanda per maggiore dettaglio (pp. 18-30).A grandi linee, dal punto di vista eziopatogenetico i tumoriprimitivi multipli possono essere classificati secondo le se-guenti categorie, non mutuamente esclusive:1. tumori che condividono fattori di rischio;2. tumori insorti nell’ambito di sindromi da predisposizionegenetica al cancro;3. tumori indotti da trattamento antineoplastico.2
Generally, from an aetiopathogenetic perspective, multiple pri-mary cancers can be classified into the following categories,which are not mutually exclusive:1. cancers that share risk factors;2. cancers arising in patients with genetic predisposition syn-dromes;3. cancers related to first cancer treatment late effects.2
Table 2 shows the first ten associations of three cancers bygender; table e1 (see on-line supplementary table) presents allthe associations of 4 cancers by gender (age of first cancer onsetis shown). In accordance with the literature, the associationbetween prostate cancer and cancers of the urinary tract, bladderin particular, is common in men.6,10 This figure is primarilyattributable to incidental detection during examination per-formed in the diagnostic phase, staging, and follow-up for thefirst cancer. Furthermore, association among multiple cancersin the urinary tract (pelvis, ureter, bladder, urethra) is docu-mented, considering the high frequency of multicentric cancersoriginating from the transitional epithelium.The shared risk factors (e.g., smoking, alcohol) of organs char-acterized by the same cellular matrix (e.g., squamous epithelium)
SEQUENCE No. AGE LATENCY LATENCYAT 1ST CANCER 1ST - 2ND CANCER 2ND- 3RD CANCER
YEARS (MEDIAN YEARS (MEDIAN YEARS (MEDIANQ1-Q3) Q1-Q3) Q1-Q3)
MENLung - Prostate - Urinary bladder 239 70.0 (64.0;74.0) 1.3 (0.1;4.3) 2.0 (0.7;4.5)
Colon - Prostate - Urinary bladder 157 71.0 (66.0;75.0) 2.8 (0.7;6.2) 1.5 (0.4;3.8)
Prostate - Kidney and renal pelvis - Urinary bladder 92 67.0 (62.5;74.0) 0.8 (0.1;4.9) 1.2 (0.1;3.7)
Larynx - Lung - Urinary bladder 64 65.0 (61.5;70.5) 3.0 (1.5;5.3) 1.9 (0.9;4.3)
Rectum - Prostate - Urinary bladder 64 71.0 (65.0;73.0) 1.4 (0.0;5.3) 2.3 (0.2;4.3)
Larynx - Prostate - Urinary bladder 61 63.0 (59.0;70.0) 3.9 (1.3;8.9) 0.7 (0.2;2.7)
Stomach - Prostate - Urinary bladder 61 72.0 (67.0;76.0) 2.1 (0.5;4.7) 2.3 (0.6;4.1)
Colon - Lung - Urinary bladder 55 69.0 (63.0;75.0) 3.4 (1.4;6.8) 2.5 (0.5;4.5)
Colon - Lung - Prostate 54 69.0 (64.0;74.0) 3.0 (1.1;5.4) 1.5 (0.6;3.6)
Colon - Rectum - Prostate 42 73.5 (69.0;77.0) 1.0 (0.1;4.2) 1.1 (0.1;2.0)
WOMENColon - Breast - Corpus uteri 36 66.0 (58.5;73.0) 4.3 (1.6;7.6) 2.0 (1.3;4.6)
Breast - Corpus uteri - Ovary 20 56.0 (49.0;65.0) 1.2 (0.0;4.3) 0.2 (0.0;4.4)
Colon - Rectum - Breast 19 73.0 (57.0;81.0) 2.3 (0.1;6.4) 1.4 (0.3;3.8)
Colon - Breast - Kidney and renal pelvis 18 67.0 (61.0;75.0) 5.0 (1.9;7.2) 1.7 (0.5;4.0)
Colon - Breast - Urinary bladder 17 69.0 (57.0;75.0) 2.1 (0.4;5.7) 1.9 (0.6;5.8)
Breast - Corpus uteri - Urinary bladder 17 65.0 (61.0;70.0) 4.6 (1.9;8.4) 2.3 (0.9;3.7)
Breast - Corpus uteri - Kidney and renal pelvis 15 63.0 (53.0;70.0) 3.3 (0.3;8.3) 1.7 (0.2;4.3)
Lung - Breast - Corpus uteri 14 56.0 (48.0;70.0) 5.1 (2.9;7.0) 4.6 (3.1;7.9)
Colon - Corpus uteri - Ovary 13 53.0 (51.0;60.0) 0.0 (0.0;0.5) 1.8 (0.0;6.6)
Lung - Breast - Urinary bladder 13 65.0 (58.0;68.0) 5.1 (2.2;6.3) 2.3 (0.8;5.7)
Tabella 2. Pazienti analizzati nel presente studio con diagnosi di tre tumori maligni (esclusi tumori non melanomatosi della cute e la sede “altre e mal definite”), prime diecisequenze più frequenti (senza considerazione della cardinalità delle sedi) nei due generi, numero di soggetti, età all’incidenza (anni) del primo tumore (mediana, primo e terzoquartile), distanza tra le date di incidenza del primo e del secondo tumore (mediana, primo e terzo quartile) e distanza tra le date di incidenza del secondo e terzo tumore(mediana, primo e terzo quartile).Table 2. Patients analyzed in the present monograph with three malignant cancers (excluding non-melanoma skin cancer and “other and ill-defined sites”), first ten mostfrequent sequences (without considering the order of the sites) among men and women.Number of subjects, age (years) of first cancer diagnosis (median, first and third quartile),latency between first and second cancer diagnosis (median, first and third quartile), and between second and third cancer diagnosis (median, first and third quartile).

Nella tabella 2 sono riportate le prime dieci associazioni ditre tumori per genere; nella tabella e1 (vd. tabella supplemen-tare on-line) sono riportate tutte le associazioni di 4 tumorinei due sessi, così come l’età di insorgenza del primo tumore.In conformità con quanto riportato in letteratura, negli uo-mini è frequente il riscontro di associazione tra tumore dellaprostata e neoplasie delle vie urinarie, in particolare della ve-scica.6,10 Tale dato risulta imputabile in primo luogo al fattoche la seconda neoplasia può essere oggetto di rilevazione oc-casionale nel corso degli esami utilizzati in fase diagnostica,di stadiazione e di follow-up per la precedente neoplasia. Inol-tre, è nota l’associazione tra più sedi del distretto urinario,considerata la tendenza alla multicentricità delle neoplasie ori-ginanti dall’epitelio di transizione, comune a più sedi dell’ap-parato urinario (pelvi, uretere, vescica, uretra).La condivisione di fattori di rischio riconosciuti (per esempio,fumo e alcol) per organi caratterizzati da una stessa matricecellulare (come l’epitelio squamoso) rende conto di unaquota importante di associazioni osservate nel sesso maschile,che includono le sedi testa-collo, esofago, prime vie respira-torie e polmone. Inoltre, considerando anche altre sedi (ve-scica, fegato, vie urinarie) per le quali sono riconosciuti glistessi fattori eziologici, è possibile interpretare con la mede-sima chiave di lettura la maggior parte delle associazionipresenti tra gli uomini (tabella 2 e tabella e1 on-line).D’altro canto, l’associazione tra le neoplasie di mammella,ovaio, corpo dell’utero e colon, di frequente osservazione nelsesso femminile (tabella 2 e tabella e1 on-line), può essere im-putata a fattori prevalentemente di tipo ormonale, riprodut-tivo e dietetico.Tuttavia, nell’ambito di questo gruppo di as-sociazioni non può essere trascurata la componente relativaalla predisposizione genetica, soprattutto laddove la primaneoplasia sia insorta in età inferiore ai 50 anni (tabella e1 on-line). Tale considerazione scaturisce anche dai dati riportatiin tabella 2 per quelle associazioni caratterizzate da un’età me-diana di insorgenza della prima neoplasia minore (colon-corpo dell’utero-ovaio: 53 anni; mammella-corpo dell’utero-ovaio e polmone-mammella-corpo dell’utero: 56 anni).Rispetto alle serie cliniche, il livello di informazione dispo-nibile dalle banche dati di popolazione non consente di en-trare nel dettaglio di identificazione di casi con familiarità edi sindromi da predisposizione genetica. Inoltre, i limitiimposti dalle norme di registrazione dei tumori multipli nonconsentono la rilevazione di neoplasie multiple caratterizzatedallo stesso codice morfologico insorgenti nella stessa sede(per esempio, melanoma), come discusso nel capitolo 6 (pp.114-119).Talune associazioni osservate nelle donne possonotuttavia suggerire la possibile presenza di mutazioni a caricodei geni noti di suscettibilità al cancro, quali: BRCA1 eBRCA2 per le associazioni di mammella, ovaio e corpo del-l’utero; MNLH1, MSH2, MSH6 (cancro colorettale nonpoliposico ereditario o sindrome di Lynch II) per le associa-zioni di colon, corpo dell’utero, ovaio, stomaco, rene e pelvi
are related to a significant portion of the observed associationsin males, which include head and neck, oesophagus, respiratorytract and lung. In addition, considering other sites (bladder,liver, urinary tract) for which the same aetiological factors areimportant, we can analogously interpret most of the associationsamong men (table 2 and table e1 online).In women, the most frequent associations (breast, ovary, colon,and corpus uteri) are mainly related to hormonal, reproductive,and dietary factors (table 2 and table e1 online). However, withinthis group of associations, genetic predisposition cannot be neglected,especially when the first cancer occurs under the age of 50 years(table e1 online). This consideration also originates from table2, for associations characterized by a younger median age of firstcancer onset (colon-corpus uteri-ovary: 53 years; breast-corpusuteri-ovary and lung-breast-corpus uteri: 56 years).Compared to clinical series, the level of information availablein population databases does not make it possible to identifycases with a family history or genetic predisposition syndromes.In addition, the limits imposed by the multiple primaries reg-istration rules do not make it possible to detect multiple ma-lignancies characterized by the same morphology occurringin the same sites (e.g., melanoma), as discussed in chapter 6(pp. 114-119). However, some of the associations observedin women may suggest the possible presence of mutations incancer susceptibility genes known as: BRCA1 and BRCA2genes for breast, ovarian, and endometrial associations;MNLH1, MSH2, MSH6 (hereditary non-polyposis colorectalcancer or Lynch syndrome II) in case of colon, uterine corpus,ovary, stomach, kidney and renal pelvis, pancreas; STK11(Peutz-Jeghers syndrome) in case of colon, breast, ovary cancer.In this context, a detection system – such as already exists inNorthern Europe – for cancers with family groupings, e.g.,multiple endocrine neoplasia13 or mutation in the p53 gene(Li-Fraumeni syndrome),14 would be desirable.As well documented, some antineoplastic treatments for bothchildhood and adult cancers may have carcinogenic effects, de-termining the occurrence of second malignancies (e.g., sarcomasand other solid tumours occurring in sites treated with radiation;leukaemia after chemotherapy regimens; carcinomas of the en-dometrium following antioestrogen therapy). The occurrenceof cancers attributable to previous antineoplastic treatmentscannot be addressed here, as it requires a higher level of infor-mation: it may be object of further investigations in high-res-olution studies.Cancer registry data are known to be useful in the public healthfield; the evidence provided in this chapter is considered relevantin the clinical setting, as well, despite certain weaknesses in theinformation source. In the tables here presented, informationon frequency, age, and gender for all possible associations isavailable. This information allows oncologists to contextualizetheir experience in this field, which would otherwise be com-parable only with case report data, which are not frequent inthe literature.
Valutazione delle associazioni tra soggetti con tre o più tumoriI tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI
112 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152

renali, pancreas; STK11(sindrome di Peutz-Jeghers) per le as-sociazioni di colon, mammella, ovaio.11,12 A tal proposito sa-rebbe auspicabile la disponibilità, come peraltro esistente neiPaesi del Nord Europa, di un sistema di rilevazione dei casidi tumori per aggregazioni familiari, quali per esempio leneoplasie endocrine multiple13 o le mutazioni a carico delgene p53 (sindrome di Li-Fraumeni).14
E’ noto che alcuni dei trattamenti antineoplastici eseguiti perneoplasie insorte in età pediatrica o adulta possono esplicareun effetto cancerogenetico determinando l’insorgenza di se-condi tumori (per esempio, sarcomi o altri tumori solidi in-sorti in aree radiotrattate; leucemia dopo regimi chemiote-rapici; carcinomi dell’endometrio in seguito a terapiaantiestrogenica). La presenza di neoplasie imputabili a trat-tamenti antineoplastici precedenti non può essere affrontatain questa sede, poiché richiede un dettaglio di informazionedi livello superiore e potrà essere oggetto di ulteriori appro-fondimenti nell’ambito di studi ad alta risoluzione.I dati prodotti dai registri tumori di popolazione rivestonodi solito particolare utilità, soprattutto in ambito di sanitàpubblica; si ritiene che le evidenze disponibili in questo ca-pitolo, pur con alcune debolezze insite nella fonte informa-tiva utilizzata, siano di particolare rilevanza anche in ambitoclinico. Gli oncologi, infatti, potranno trovare nelle tabelleriscontro su tipologia, frequenza ed età, stratificate per ge-nere, delle varie associazioni di tumori multipli ricavate subase di popolazione in Italia. Tali informazioni darannomodo di inquadrare meglio la propria esperienza in questoambito nosologico che altrimenti troverebbe riscontro solonei dati prodotti da pubblicazioni su case report, peraltronon frequenti in letteratura.
Valutazione delle associazioni tra soggetti con tre o più tumoriI tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI
113 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
BIBLIOGRAFIA/REFERENCES
1. No authors listed. Cancer survivors: living longer, and now, better.Lancet 2004;364(9452):2153-4.
2. Travis LB, Rabkin CS, Brown LM et al. Cancer survivorship – geneticsusceptibility and second primary cancers: research strategies andrecommendations. J Natl Cancer Inst 2006;98(1):15-25.
3. Crocetti E, Buiatti E, Falini P; Italian Multiple Primary Cancer WorkingGroup. Multiple primary cancer incidence in Italy. Eur J Cancer 2001;37(18):2449-56.
4. Cercato MC, Colella E, Ferraresi V, DiodoroMG, Tonachella R. Reportof two cases of quintuple primary malignancies and review of the lit-erature. Anticancer Res 2008;28(5B):2953-8.
5. Aydiner A, Karadeniz A, Uygun K et al. Multiple primary neoplasmsat a single institution: differences between synchronous andmetachronous neoplasms. Am J Clin Oncol 2000;23(4):364-70.
6. Demandante CG, Troyer DA, Miles TP. Multiple primary malignantneoplasms: case report and a comprehensive review of the literature.Am J Clin Oncol 2003;26(1):79-83.
7. AIRTUM Working Group. Italian Cancer Figures, Report 2009:Cancer trend (1998-2005). Epidemiol Prev 2009;33(4-5) Suppl 1:1-168.
8. Dal Maso L, Lise M, Zambon P et al; AIRTUM Working Group. Inci-dence of thyroid cancer in Italy, 1991-2005: time trends and age-pe-riod-cohort effects. Ann Oncol 2011;22(4):957-63.
9. Rosso S, De Angelis R, Ciccolallo L et al; EUROCAREWorking Group.Multiple tumours in survival estimates. Eur J Cancer 2009;45(6):1080-94.
10.Matzkin H, Braf Z. Multiple primary malignant neoplasms in the gen-itourinary tract: occurrence and etiology. J Urol 1989;142(1):1-12.
11.Garber JE, Offit K. Hereditary cancer predisposition syndromes. J ClinOncol 2005;23(2):276-92.
12.Hemminki K, Granstrom C. Familial clustering of ovarian and en-dometrial cancers. Eur J Cancer 2004;40(1):90-5.
13.Lee M, Pellegata NS. Multiple endocrine neoplasia syndromes asso-ciated with mutation of p27. J Endocrinol Invest 2013 [Epub aheadof print].
14.Kast K, Krause M, Schuler M et al. Late onset Li-Fraumeni Syndromewith bilateral breast cancer and other malignancies: case reportand review of the literature. BMC Cancer 2012;12:217.

Capitolo 6
I tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI
Epidemiol Prev 37 (4-5) Suppl 1:1-152 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.it114
Ruolo delle classificazioni nelle definizionidi tumori multipliRole of classification systems in the definitionof multiple primary cancers
The concept of multiple primary cancer (MP) implies that itis possible to distinguish between two or more cancers, definingthem as independent from each other. In this context, multiplelesions in the same organ was considered as a single (multifocal)cancer and the first lesion and local recurrence after treatmentand metastasis as a single cancer, as well. These concepts are ap-plied in both clinical and epidemiological settings; in thecancer registration field, definitions need to be formalized toguarantee reproducibility of the site and morphology definition.Formalization of the concept follows the increasingly more de-tailed information available in the field of oncology, as sum-marized by the World Health Organization (WHO) in theBlue Books, a periodic publication which represents the refer-ence for international standards in cancer diagnosis.1 Theprogress in the understanding of diseases also has an impact ontheir classification, which must include increasing detail.The International Classification of Diseases for Oncology(IDC-O) published by theWHO is a specific classification forcancer. It is derived from the International Classification ofDiseases (ICD), which uses a single code to define each disease(for cancer, the code is mainly topographical). The ICD-O hasa two-dimensional structure, defining morphology and topog-raphy; topographical codes reflect the ICD codes, while mor-phological codes are ICD-O specific. The ICD-O contains allthe basic elements for cancer registration (codes, rules), includ-ing rules that define when two tumours of the same patient arein the “same site” or belong to the same “morphological group.”The major problems associated with classification systems since1991, when a clear definition of multiple primaries first ap-peared, were analyzed in detail.2
In 1976, in the WHO guidelines3 the only issue was whetherthe detected tumour should be classified as a different canceror the same one (i.e., as multifocal cancer or metastasis).In 1991, Muir and Percy2 pointed out the need of rules to de-fine multiple primaries.Because of their importance, these rules are here quoted:1. the recognition of the existence of two or more primary can-cers does not depend on time;2. a primary cancer is one that originates in a primary site ortissue and is thus neither an extension, a recurrence, nor ametastasis;
Il concetto di tumori multipli (MP) implica la possibilità didistinguere due o più lesioni neoplastiche definendole comeindipendenti fra loro, ovvero non espressione di un’unica le-sione originaria. In questo senso si considerano unici anchetumori che si esprimono attraverso lesioni multiple nel-l’ambito dello stesso organo (multifocali) oppure la ripresalocale dopo trattamento o la comparsa di lesioni metastati-che. Questi concetti, validi anche in ambito clinico, nelcampo della registrazione dei tumori necessitano una forma-lizzazione per rendere riproducibili la definizione della seded’origine e quella della morfologia della neoplasia.Questa formalizzazione è legata al progredire delle conoscenzespecifiche che l’Organizzazione mondiale della sanità (OMS)riassume in una serie di pubblicazioni periodiche note comeBlue Books; esse rappresentano il riferimento per gli standardinternazionali della diagnosi in oncologia.1 Il modificarsidelle conoscenze ha anche un effetto sui sistemi di classifica-zione delle malattie che devono tener conto del dettaglio no-sologico crescente. In campo oncologico esiste una classifi-cazione specifica, sempre a cura dell’OMS: la Classificazioneinternazionale delle malattie per l’oncologia (ICD-O).Questa classificazione deriva dalla Classificazione interna-zionale delle malattie (ICD) che si basa su un solo codiceper definire una malattia (per l’oncologia, tale codice èprevalentemente topografico). L’ICD-O ha una strutturabidimensionale, topografica e morfologica: i codici topogra-fici riprendono quelli dell’ICD, i codici morfologici sonospecifici. L’ICD-O contiene anche tutti gli elementi basenecessari per la registrazione (codici, regole). Tra le regolevi sono quelle che definiscono quando due tumori nel me-desimo paziente devono essere considerati nella “stessasede” o appartenere al medesimo “gruppo morfologico”.Di seguito si analizzano nel dettaglio le maggiori problema-tiche connesse con i sistemi di classificazione partendo dal1991, anno in cui compare una prima definizione chiara ditumori multipli.2
Nel 1976 nelle linee guida dell’OMS3 l’unica ragione di di-scussione era se il tumore rilevato dovesse essere classificatocome un diverso tumore o lo stesso, ma con carattere dimultifocalità o diffusione metastatica.Nel 1991 Muir e Percy2 richiamano la necessità di regole per
WWW.EPIPREV.IT

Epidemiol Prev 37 (4-5) Suppl 1:1-152 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.it115
I tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI Ruolo delle classificazioni nelle definizioni di tumori multipli
3. only one tumour shall be recognized in an organ or pair oforgans or tissue, as defined by the 3-digit rubric of the ICD(table 1).Rule 3 does not apply if the tumours in the same site are his-tologically different, as seen in table 2.4
Since the ICD-O is based on the ICD, it has followed the ICD’sevolution: ICD-O-1 is based on ICD-9 for the topographical codes,ICD-O-2 and ICD-O-3 follow the ICD-10 topographical codes.Due to this reason, the definition of “same site” and “same mor-phology” has evolved over time.5-8
In tables 1 and 2 only topographical and morphological codesdefining a single group as per MP definition are reported. Thegroup of topographic (or morphological) codes listed in the ta-bles 1 and 2 are considered as different sites (morphologies)with respect to MP definition.This development also has an impact on MP definition. Forexample, the definition of new homogeneous topographical cat-egories may determine a reduction in the number of MPs, asin the case of upper aerodigestive tract cancers. As regards“different” morphologies, over time our understanding of thelymphohematopoietic system has increased in detail, allowingfor the identification of new MPs.New classifications cannot be applied on historical data col-lected on the basis of less specific criteria. Close following of rec-ommendations may result in incomparability of data producedduring different periods. For example, multiple haematologicaltumours increased from ICD-O-2 to ICD-O-3; borderlineovarian tumours were defined as malignant only in ICD-O-2; myelodysplastic syndromes and myeloproliferative diseases be-came malignant with ICD-O-3; malignant carcinoids of theappendix became malignant with the ICD-O-3 update.9
The epidemiological criteria for MP definition (based on dif-ferent ICD-O editions, as well as different assumptions) mayinfluence the number of multiple primaries.10
The problems are due to the fact that not everyone uses the rulespublished in 2004 as a result of the joint work of the WHO,the International Agency for Research on Cancer (IARC), theInternational Association of Cancer Registries (IACR) and theEuropean Network of Cancer Registries (ENCR). Differentcancer registries may use different rules to define MPs.Moreover, the IARC-ENCR rules evolved over time, as theICD-O, on which the rules are based, went from 1st to 2nd edi-tion6 and finally on to its 3rd version, with two subsequent up-dates in 20007 and 2004.8
In the most recent edition of the most extensive report on cancerincidence worldwide (“Cancer Incidence in Five Continents”),11
data from 225 cancer registries were evaluated: 90% of partic-ipant registries declared the rules adopted for MP definition; ofthese, 80% adopted the IARC-ENCR rules, whereas the remain-ing 20% adopted different rules, either those of the “SurveillanceEpidemiology and End Results” (SEER) programme,12 combi-nations of different systems, only local, or unspecified rules.Among cancer registries using IARC-ENCR rules, 3% used
definire i tumori multipli anche per ragioni di comparabi-lità tra registri.Per la loro importanza, vengono qui ricordate per esteso:1. il reperimento dell’esistenza di due o più tumori è indi-pendente dal tempo;2. un tumore primitivo è un tumore che origina da un or-gano o tessuto primario e che non è un’estensione, una re-cidiva o una metastasi;3. solo un tumore deve essere riconosciuto in un organo opaio di organi o tessuti, definiti dal codice a 3 cifre della Clas-sificazione internazionale delle malattie (ICD) (tabella 1).La regola 3 non si applica se i tumori in un organo sonoistologicamente differenti, come mostrato in tabella 2.4
Essendo l’ICD-O una derivazione dell’ICD, ne ha nel tempoacquisito gli sviluppi riferendosi a ICD-9 per la parte topo-grafica di ICD-O-1 e a ICD-10 per ICD-O-2 e ICD-O-3.Per questo la definizione di “stessa sede” e “stessa morfologia”si è evoluta nel tempo,5-8come sintetizzato nelle tabelle 1 e 2,dove sono riportati soli i gruppi di codici topografici e mor-fologici che costituiscono un unico raggruppamento per la de-finizione dei tumori multipli. I codici topografici (o morfo-logici) elencati nelle tabelle 1 e 2 sono considerati come sedi(morfologie) distinte per la definizione dei tumori multipli.Questo sviluppo ha avuto effetti anche sui tumori multipli.Per esempio, la creazione di categorie topografiche consi-derate omogenee, come nel caso dei tumori delle vie aero-digestive superiori, ha determinato una riduzione del nu-mero dei MP. Per quanto riguarda le morfologie daconsiderare differenti, col passare del tempo c’è stato un det-taglio sempre maggiore per il sistema emolinfopoietico, cheha permesso l’identificazione di nuovi MP.Senza entrare nel merito, è evidente che una nuova edizionedi una classificazione, determinata dal miglioramento delleconoscenze, non può essere applicata sempre e comunquesu dati storici raccolti sulla base di criteri meno specifici.Questo può portare alla non confrontabilità dei dati pro-dotti in tempi diversi. Per esempio, per l’ematologico la pos-sibilità di definire MP è accresciuta passando dall’ICD-O-2 a ICD-O-3, ma sono possibili altri esempi, come nel casodei tumori borderline dell’ovaio che sono stati definiti comemaligni solo in ICD-O-2, mentre le sindromi mielodi-splastiche e alcune malattie mieloproliferative sono diven-tate maligne con ICD-O-3, e i carcinoidi dell’appendicesono diventati maligni con l’aggiornamento di ICD-O-3.9
I criteri utilizzati in campo epidemiologico per la defini-zione dei tumori multipli, collegati all’utilizzo di diverse edi-zioni dell’ICD-O, ma anche di assunti diversi, possono in-fluire fortemente sul numero dei tumori stessi.10
Il problema nasce dal fatto che non tutti i registri utilizzanole regole prodotte nel 2004, frutto della collaborazione fraOMS, Agenzia internazionale per la ricerca sul cancro(IARC), Associazione internazionale dei registri tumori(IACR) e il Network europeo dei registri tumori (ENCR).

Ruolo delle classificazioni nelle definizioni di tumori multipliI tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI
116 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
GROUP DESCRIPTION CODESICD-O-2 RULES ICD-O-3 RULES ICD-O-3 RULES
(1990) (2000) (2004)
1Base of tongue C01 C01 C01*Other and unspecified parts of tongue C02 C02 C02*Lip C00*Gum C03*
2 Floor of mouth C04*Palate C05 C05*Other and unspecified parts of mouth C06 C06*
3Parotid gland C07 C07Other and unspecified major salivary glands C08 C08Tonsil C09 C09*Oropharynx C10 C10*
4 Pyriform sinus C12 C12 C12*Hipopharynx C13 C13 C13*Other and unspecified sites in lip, oral cavity and pharynx C14*
5Rectosigmoid junction C19 C19 C19*Rectum C20 C20 C20*
6Gallbladder C23 C23*Other and unspecified parts of biliary tract C24 C24*
7Nasal cavity and middle ear C30Accessory sinuses C31
8Trachea C33 C33*Bronchus and lung C34 C34*Thymus C37
9 Heart, mediastinum C38.0/38.3Overlapping lesion of heart, mediastinum and pleura C38.8
10Bones, joints and articular cartilage of limbs C40 C40*Bones, joints and articular cartilage of limbs of other and unspecified sites C41 C41*Vulva C51
11Vagina C52Other specified parts of female genital organs C57.7Overlapping and unspecified lesions of female genital organs C57.8/57.9
12Penis C60Other and unspecified male genital organs C63Kidney C64Renal pelvis C65 C65*
13 Ureter C66 C66*Urinary bladder C67*Other and unspecified urinary organs C68 C68*
14Adrenal gland C74Other endocrine glands and related structures C75Non-Hodgkin lymphomas C82-C85#
15 Lymphoid leukaemia C91#
Unspecified leukaemia C95#
* A specific code is provided when two synchronous tumours belong to the same group.# Diseases listed in ICD-O-2 with ICD-10 codes.
Tabella 1. Sedi tumorali che costituiscono un unico raggruppamento topografico secondo le regole di classificazione International Classification of Diseases for Oncology2a edizone (WHO 1990), International Classification of Diseases for Oncology 3a edizione (WHO 2000), International rules for multiple primary cancers (IARC 2004).Table 1. Cancer sites constituting a unique topographical group on the basis of the International Classification of Diseases for Oncology 2nd Edition (WHO, 1990), theInternational Classification of Diseases for Oncology 3rd Edition (WHO, 2000), and the International rules for multiple primary cancers (IARC, 2004).

Ruolo delle classificazioni nelle definizioni di tumori multipliI tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI
117 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
GROUP DESCRIPTION CODESICD-O-2 RULES ICD-O-3 RULES ICD-O-3 RULES
(1990) (2000) (2004)1 CARCINOMAS Squamous 805-813 805-808, 812, 813 8051-8084, 8120-8131
Basal cell 809-811 8090-8110
Adenocarcinoma 814, 816, 818-823, 814, 816, 819-822, 8140-8149, 8160-8162,
825-855, 857, 894 826-833, 835-855, 8190-8221, 8260-8373,
857, 894 8350-8551, 8570-8756,
8940-8941
Other specified 803, 804, 815, 817, 824, 803-804, 815, 817, 818, 8030-8046, 8150-8157,
856, 858-867 823-825, 834, 856, 8160-8162, 8170-8180,
858-867 8230-8255, 8340-8347,
8560-8562, 8580-8671
Unspecified cancers a 801-802 801-802 8010-8015,
8020-8022, 8050
2 SARCOMAS 868-871, 880-892, 868-871, 880-892, 8680-8713, 8800-8921,
AND OTHER SOFT 899, 904, 905, 912-934, 899, 904, 912, 913, 8990-8991, 9040-9044,
TISSUE CANCERS 937, 949, 950, 954-958 915-925, 937, 949, 950, 9120-9125, 9130-9136,
954-958 9141-9252, 9370-9373,
9540-9582
3 MESOTHELIOMA 905* 9050-9055
4 HAEMATOPOIETIC Leukaemia 980-994, 995, 996, 998* Myeloid leukaemiaAND LYMPHATIC 9840, 9861-9931,
TISSUE CANCER 9945-9946, 9950,
9961-9964, 9980-9987*
Lymphoma 959-974 959-972* B-cell neoplasms
9670-9699, 9728,
9731-9734, 9761-9767,
9769, 9823-9826,
9833, 9836, 9940*
T-cell and NK-cell neoplasms 9700-9719, 9729, 9768,
9827-9831, 9834,
9837, 9948*
Hodgkin lymphoma 9650-9667*
Mast cell tumours 9740-9742*
Neoplasms of histiocytes and accessory 9750-9758*lymphoid cells
Unspecified cancers b 9590-9591, 9596, 9727,
9760, 9800-9801, 9805,
9820, 9832, 9835, 9860,
9960, 9970, 9975, 9989*
5 KAPOSI SARCOMA 914* 9140*
6 OTHER SPECIFIED 872-879, 893, 895-898, 872-879, 893, 895-898, 8720-8790, 8930-8936,
CANCERS 900-903, 906-911, 935, 900-903, 906-911, 8950-8983, 9000-9030,
936, 938-948, 952, 953 926-936, 938-953, 9060-9110, 9260-9365,
973-975, 976 9380-9539
7 UNSPECIFIED 800 800, 997 8000-8005CANCERS c
a. Unspecified carcinomas should not be considered different from the previous groups (since ICD-O-3 introduction).b. Unspecified haematological cancers should not be considered different from other specified tumours of the haematopoietic and lymphatic tissues (since IARC 2004 introduction).c. Unspecified cancers should not be considered different from other types of cancer previously presented in the table (since ICD-O-3 introduction).* Systemic cancers with possible location in different organs: cancers should be counted only once in each patient (for mesothelioma only in ICD-O-3).
Tabella 2.Morfologie che costituiscono un unico raggruppamento istologico secondo le regole di classificazione International Classification of Diseases for Oncology2a edizione (WHO 1990); International Classification of Diseases for Oncology 3a edizione (WHO 2000), International rules for multiple primary cancers (IARC 2004).L’ordinamento dei gruppi è differente nelle diverse citazioni; quello presentato è funzionale al quadro sinottico. In grassetto sono evidenziati i codici che nella regolasuccessiva sono stati in tutto o in parte ricollocati in altri gruppi. L’evidenziazione è presente sia nella regola precedente sia in quella successiva.Table 2. Morphologies constituting a single histological group, based on the International Classification of Diseases for Oncology 2nd Edition (WHO, 1990), theInternational Classification of Diseases for Oncology 3rd Edition (WHO, 2000), and the International rules for multiple primary cancers (IARC, 2004). Group order isdifferent in each classification system. Codes which were partly or fully moved to other groups in the subsequently established rule are in bold, both in the precedingand in the subsequent rule.

Inoltre le regole IARC-ENCR si sono evolute nel tempo pa-rallelamente allo sviluppo della classificazione ICD-O, sullaquale si basano la prima e la seconda versione,6 e infine laterza, e su quest’ultima con due successivi aggiornamentinel 20007 e nel 2004.8
Nell’ultima edizione della pubblicazione più importante cheraccoglie dati sull’incidenza dei tumori (“Cancer Incidencein Five Continents”)11 risulta che tra i 225 registri tumoriinclusi il 95% esplicita le regole utilizzate per i tumorimultipli; di questi l’80% dichiara di adottare regole IARC-ENCR, il restante 20% dichiara di adottare regole diverse,in parte del programma “Surveillance Epidemiology andEnd Results” (SEER),12 in parte combinazioni di sistemi di-versi, in parte solo regole locali o non specificate.Fra quelli che usano le regole IARC, il 3% utilizza quellebasate sull’ICD-O-1, il 26% sull’ICD-O-2,6 il 21% suICD-O-2 e ICD-O-3, il 13% sull’ICD-O-3 del 20007 e il18% sull’ICD-O-3 del 2004.8 L’effetto dell’utilizzo di ver-sioni differenti dell’ICD-O nel definire diverse sedi e mor-fologie, principio basilare sempre mantenuto, è schematiz-zato nelle tabelle 1 e 2.Per quanto riguarda le regole adottate dai registri statuni-tensi del programma SEER, queste si differenziano dalleprecedenti per alcuni aspetti, quali il considerare l’intervallotemporale fra tumori successivi, considerare indipendentigli organi pari, e prevedere la possibilità di più tumori nel-l’ambito della stessa sede topografica (per esempio, colon ocute) anche indipendentemente dalle differenze nella mor-fologia. Questo influenza il numero di MP soprattutto peralcune sedi tumorali. E’ stato documentato che utilizzare leregole SEER rispetto a quelle IARC-IACR determina unaumento del 5,7% dei tassi standardizzati per età dell’inci-denza del tumore della mammella femminile, di circa il 5%per il colon sia negli uomini sia nelle donne, del 4-5% peril melanoma, di circa il 2% per rene, testicolo e polmone.Questa classificazione determina anche un effetto com-plessivo sull’incidenza per il totale dei tumori che risulta in-crementa di circa l’1%.13 Come accade per le regole IARC-IACR-ENCR, anche quelle SEER sono oggetto di frequentiaggiornamenti successivi.14 Dal 2007 sono state prodotte re-gole specifiche per sede tumorale (tumori di polmone,mammella, colon, melanoma della cute, testa e collo, rene,pelvi renale/uretere/vescica, e tumori benigni e malignidell’encefalo) e anche regole, sia generali sia specifiche, perle altre sedi, oltre a regole relative alle istologie con raggrup-pamenti morfologici che differenziano fra tipologie nonspecificate (NAS), specificate, tipi, sottotipi e forme miste.La necessità di rendere maggiormente comparabili le casi-stiche prodotte secondo le regole IARC da quelle che si av-valgono delle regole SEER è esplicitata nelle raccomanda-zioni IARC del 2004, nella quali è suggerita la registrazionedi due tumori di differente lateralità ma stessa morfologiain alcuni organi pari, così come due o più tumori insorgenti
rules based on ICD-O-1, 26% used rules based on ICD-O-2,6 21% used rules based on ICD-O-2 and ICD-O-3, 13%used rules based on the 2000 version of ICD-O-3,7 and 18%on the 2004 version of ICD-O-3.8
The effect of using different ICD-O versions in cancer site andmorphology definitions is presented in tables 1 and 2.The rules adopted by US cancer registries in the SEER pro-gramme differ from the previous ones in some respects: consid-ering the interval time between subsequent cancers, consider-ing independent pair organs, allowing MPs in the same site(for example colon, skin) independently from the morphology.This may influence MP incidence. Using SEER rules insteadof IARC-IACR rules causes a 5.7% increase in the age-stan-dardized incidence rates of female breast cancer, a 5% increasefor colon cancer among both men and women, a 4-5% in-crease for melanoma, a 2% increase for kidney, testis, and lungcancers. This classification also determines an overall effect forthe all cancer incidence, which is about 1% higher.13 SEERrules are frequently updated.14 Since 2007, specific rules forlung, breast, colon, melanoma of the skin, head and neck, kid-ney, renal pelvis/ureter/bladder, and benign and malignantbrain cancer are available, as well as general and specific rulesfor other sites and rules relating to specified and unspecifiedmorphologies.The problem of comparability among data produced by cancerregistries (i.e., SEER vs. IARC-IACR) is addressed by theIARC 2004 recommendations: IARC suggests registration(but not inclusion among incident cases) of two cancers occur-ring in paired organs with the same morphology, as well as oftwo or more cancers in different subsites of the colon.8
Italian cancer registries follow the IARC-ENCR rules; AIR-TUM promotes the application of the most recent rules, whichto date are the ones published in 2004.In Italy, the AIRTUM Cancer Registration Handbook15 has fo-cused on a strategy to improve MP management, taking intoaccount the frequent changes in classifications and rules: it callsfor registration even of tumours not included among incidentcases, and subsequent case selection before publication.The classification system used influences MP definition and,consequently, MP frequency. AIRTUM suggests to separatedata collection – which should be as extensive as possible – anddata selection – which needs to be formalized.
Ruolo delle classificazioni nelle definizioni di tumori multipliI tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI
118 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152

Ruolo delle classificazioni nelle definizioni di tumori multipliI tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI
119 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
BIBLIOGRAFIA/REFERENCES
1. http://apps.who.int/bookorders/WHP/home1.jsp?sesslan=12. Jensen OM, Parkin DM, MacLennan R, Muir CS, Skeet RG (eds).
Cancer Registration: Principles and Methods. IARC Scientific Pub-lications n.95. Lyon, IARC, 1991.
3. World Health Organization. WHO Handbook for StandardizedCancer Registries. Geneva, WHO, 1976.
4. Berg JW. Morphologic classification of human cancer. In: Schotten-feld D, Fraumeni JF Jr (eds). Cancer Epidemiology and Prevention.Philadelphia, Saunders, 1982; pp.74-9.
5. Berg JW. Morphologic classification of human cancer. In: Schotten-feld D, Fraumeni JF Jr (eds). Cancer Epidemiology and Prevention.2nd edition. Chapter 3, Section 1: Basic Concepts. Oxford, NewYork, Oxford University Press, 1996; pp. 28-44.
6. Percy C, Van Holten V, Muir C (eds). International Classification ofDiseases for Oncology. 2nd Edition. Geneva, WHO, 1990.
7. Fritz A, Jack A, Parkin DM et al (eds). International Classification ofDiseases for Oncology. 3rd Edition. Geneva, WHO, 2000.
8. International Agency for Research on Cancer. International rules formultiple primary cancers (ICD-O Third Edition). Internal report No.2004/02. Lyon, IARC, 2004. Available at: http://www.iacr.com.fr/Mprules_july2004.pdf
9. International Agency for Researc on Cancer; World Health Organ-ization. Updates to the International Classification of Diseases forOncology, third edition (ICD-O-3). IARC/WHO 2011. Available at:http:/ /www.who.int/c lass i f icat ions/ icd/updates/ ICDO3Updates2011.pdf
10.Crocetti E, Buiatti E. Re: multiple neoplasias: an oncologic reality.J Natl Cancer Inst 1997;89(21):1634-6.
11.Curado MP, Edwards B, Shin HR et al. (eds). Cancer Incidence in FiveContinents, Vol. IX. IARC Scientific Pubblication No. 160. Lyon,IARC, 2007.
12.http://seer.cancer.gov/tools/mphrules/13.Parkin DM, Plummer M. Comparability and quality of data. In:
Parkin DM, Whelan SL, Ferlay J, Teppo L, Thomas DB (eds). CancerIncidence in Five Continents, Vol. VIII. IARC Scientific PubblicationNo. 155; pp. 57-74. Lyon, IARC, 2002.
14.http://seer.cancer.gov/tools/mphrules/revisions.html15.Ferretti S, Giacomin A; Gruppo di lavoro AIRTUM.Manuale di tec-
niche di registrazione dei tumori. Milano, Inferenze Editore, 2008.
in diverse sottosedi del colon, escludendoli dall’incidenza.8
I Registri tumori italiani utilizzano, e hanno utilizzato inpassato, le regole IARC-ENCR nelle varie declinazioni chesi sono succedute nel tempo; d’altro canto AIRTUM hasempre promosso l’applicazione delle regole più recenti, almomento rappresentate dalle regole IARC 2004.A livello nazionale, il Manuale di tecniche di registrazionedell’AIRTUM15 ha messo a fuoco una strategia per miglio-rare la gestione dei tumori multipli, soluzione che tieneconto dei frequenti mutamenti di classificazioni e regole: re-gistrazione estesa anche a quei tumori che in applicazionedelle regole in corso non entrano in incidenza, incluse neo-plasie non invasive e successiva selezione della casistica infase di pubblicazione.E’ evidente che la scelta di una classificazione è determi-nante nella definizione e quindi nella frequenza dei MP.L’indicazione di AIRTUM a mantenere separata la fasedella raccolta dei dati, che deve essere estensiva, da quella(formalizzata) dell’inclusione dei tumori sembra la più ade-guata per permettere di accogliere i continui miglioramenticlassificativi garantendo la comparabilità nel tempo.

WWW.EPIPREV.IT
Il presente studio sull’incidenza dei secondi tumori, basatosul confronto di quanto osservato con quanto atteso in baseall’esperienza della popolazione generale, affronta il temadella comparabilità tra due popolazioni: la popolazioneoncologica in studio e quella utilizzata come riferimento peril calcolo dell’incidenza attesa. Se l’assunto di confrontabi-lità tra le due popolazioni fosse violato, i risultati ottenutipotrebbero essere distorti. In questo contesto assume unruolo rilevante il problema di quei tumori definiti sincroni,cioè diagnosticati in un periodo ritenuto coincidente conla diagnosi del primo tumore.Infatti, a seguito della diagnosi di tumore un paziente è sot-toposto a una serie di accertamenti che hanno lo scopo di de-finirne la natura e l’estensione. Questi esami possono portareall’identificazione di altre neoplasie presenti ma non ancorasintomatiche, che vengono diagnosticate in quel momentoin virtù degli esami diagnostici e stadiativi prescritti perl’altro tumore, il primo. Confrontare una popolazione sot-toposta a molti esami con una esposta a un’intensità diagno-stica più bassa è scorretto, perché ci si aspetta, come infattiaccade, che tanto più numerosi sono gli esami tanti più sa-ranno i tumori trovati. Per esempio, negli USA è stato osser-vato che la frequenza dei melanomi cutanei è funzione dellafrequenza con la quale vengono effettuate le biopsie dilesioni cutanee: maggiori sono le biopsie tanto più numerosele diagnosi di melanoma.1 In alcuni studi l’aumentata sor-veglianza medica dei noduli tiroidei è associata all’aumentoosservato dell’incidenza del cancro della tiroide.2
In figura 1 sono presentati i rapporti standardizzati di inci-denza (Standardized Incidence Ratio - SIR), cioè i rapportifra il numero di secondi tumori incidenti osservati nella po-polazione dei pazienti con un tumore rispetto a quelli attesiin base all’incidenza dei tumori nella popolazione generale.I SIR sono presentati per intervalli mensili a partire dal mo-mento della diagnosi del primo tumore. Il numero di casiattesi è stato calcolato moltiplicando gli anni-persona a ri-schio di sviluppare il secondo tumore, età, periodo, generee area geografica specifici per i corrispondenti tassi di inci-denza della popolazione generale. E’ stata utilizzata la casi-stica analizzata in questa monografia relativa ai Registri tu-mori con almeno 10 anni di incidenza.Il grafico in figura 1 evidenzia quanto descritto finora: i SIRsono molto elevati nel periodo immediatamente successivoalla diagnosi del primo tumore (oltre sei volte i tumori attesi
The study of the incidence of multiple primaries (MPs) isusually based on the comparison of MPs observed among cancerpatients with those expected based on the incidence in thegeneral population. The two populations must be comparableor the results may be biased. In this context, the issue of cancersdetected synchronously, that is, diagnosed at the same time asthe first one, assumes a crucial role.When a cancer is suspected, a patient undergoes a number ofclinical exams which have the purpose of defining its natureand extent. However, these exams may also lead to the iden-tification of other cancers that are already present but not yetsymptomatic. These other cancers are diagnosed at that timeonly because of the diagnostic tests performed for the firstcancer. Comparing a population subjected to many exams toanother exposed to a lower intensity diagnostic activity is in-correct because it is expected that the greater the number ofthe exams the greater the number of cancers found. For example,in the USA it has been observed that the frequency of skinmelanomas is a function of the frequency of skin biopsies ofskin lesions: the greater the number of biopsies, the greater thenumber of melanoma diagnoses.1 The increase in the incidenceof thyroid cancer has also been related to the increased medicalsurveillance of thyroid nodules.2
Figure 1 presents the Standardized Incidence Ratios (SIRs);SIRs are the ratios between the number of observed second in-cident cancers in the population of patients with one cancerand those expected on the basis of the cancer incidence in thegeneral population. The SIRs are shown by monthly intervalsince first cancer diagnosis. The number of expected cases is cal-culated multiplying the age-, period-, gender-, and area-specificperson-years at risk of developing a second cancer by the corre-sponding incidence rates in the general population.The graph of figure 1 shows the previously described phenom-enon, i.e., very high SIRs in the period immediately followingthe diagnosis of the first cancer (more than six-fold the cancersexpected in the first month, about twice as high the numberin the second month, fifty percent higher in the third month)for the detection of many cancers compared to much lower ex-pected rates. The SIRs slightly decrease thereafter, presumablydue to this screening effect, and then tend to rise again.In order to have an unbiased comparison, a reference populationof non-cancer patients subjected to the same frequency of testsas cancer patients would be needed. Unfortunately, such a pop-ulation does not exist and this is the reason why a period of
I tumori multipli sincroniSynchronous multiple cancers
120 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
I tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI
Capitolo 7

variable length following the date of diagnosis of the first canceris excluded in studies on MP incidence. The definition of theperiod of synchronicity is arbitrary. The studies that have dealtwith population-based MP measures have adopted differenttime periods: 1 month,3,4 2 months,5-11 3 months,12,13 and 12months.14-16 Karahalios et al. have included in the analysis allcancers, synchronous and metachronous,17 and other authorshave performed the analyses with and without the synchronouscancers.3
WHAT IS THE EFFECT OF EXCLUDING OBSERVED ANDEXPECTED MPs IN THE PERIOD OF SYNCHRONICITY?To answer this question, it is necessary to address several issues.
Exclusion of indolent cancersSome of the synchronous cancers would never have been symp-tomatic in the lifetime of the patients, who would have re-mained unaware of the diseases, which are identified only be-cause of the intense investigative activity related to the firstcancer. This phenomenon, well known in screening programmesand early diagnosis activities, is defined as overdiagnosis.18
These types of cancers are also documented in autopsy studies, inwhich unsuspected (and undiagnosed in life) cancers are diagnosedpost mortem.19,20 The example of cancers diagnosed post mortemclarifies how a portion of casesmay be diagnosed during life just be-cause of clinical examinations performed with other ends.That is, if the patient hadn’t been diagnosed with the firstcancer, there would not have been the initial onset of the symp-toms for the second cancer and therefore the second cancerwould not have been diagnosed, and it would not had con-tributed to the incidence frequency.The exclusion during the synchronous period of these indolenttumours should therefore not have an effect on SIR estimatesand including them would result in an overestimation. Forthis specific aspect, the exclusion of the period of synchronicityproduces more accurate estimates.
Early diagnosisThe synchronous diagnosis of certain cancers anticipates theirnatural onset by a fewweeks, months, or years.This is the principleon which screening is based:21 to anticipate diagnosis to a stage inwhich treatment is able to modify the prognosis, resulting in a re-duction of cause-specific mortality. By excluding these cancersbecause of their synchronous nature, the real risk of MP in thepopulation of cancer patients would be underestimated.The un-derestimation is certain, but its amount is not quantifiable.
To obtain an unbiased estimate of the incidence of secondcancers the first group (indolent cases) should be excluded fromthe analysis and the second group (anticipated cases) shouldbe included. However, it is impossible to distinguish whethera second synchronous cancer is overdiagnosed (i.e., one thatwould never have been detected in the absence of investigative
I tumori multipli sincroniI tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI
121 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
nel primo mese, circa due volte nel secondo mese, il 50% inpiù nel terzo mese) per l’identificazione di molti tumori ri-spetto a un numero atteso di neoplasie inferiore. Successiva-mente i SIR si riducono, anche se in modo lieve, presumi-bilmente per l’effetto dello screening avvenuto nel periododi sincronicità, per poi tendere a risalire.Perché il confronto fra le due popolazioni non risulti distorto,sarebbe necessario avere una popolazione di riferimento nononcologica ma sottoposta agli stessi esami. Questa popola-zione non esiste: ecco il motivo per cui negli studi sull’inci-denza di secondi tumori viene escluso un periodo di varialunghezza successivo alla data di diagnosi del primo tumore.Il periodo di sincronicità è arbitrario e non ne esiste una de-finizione univoca. Gli studi che hanno affrontato la stima delrischio di secondi tumori in casistiche di popolazione hannoadottato periodi temporali diversi: 1 mese,3,4 2 mesi,5-11 3mesi12,13 e 12 mesi.14-16 Inoltre vi sono studi che hannoincluso nell’analisi tutti i tumori, sincroni e metacroni,17 e al-tri che hanno effettuato analisi con e senza esclusione.3
COSA HA DETERMINATO L’ESCLUSIONE DEI TUMORIOSSERVATI E ATTESI NEL PERIODO DI SINCRONICITÀ?Per poter rispondere a questa domanda è necessario conside-rare alcuni aspetti:
Esclusione di tumori indolentiUna parte dei tumori sincroni non avrebbero mai dato segniclinici nel corso della vita dei pazienti che avrebbero quindiconvissuto ignari con queste patologie, identificate solo acausa dell’intensa attività investigativa legata al primo tu-more. Questo fenomeno, particolarmente noto nel campodegli screening e di tutte le attività di diagnosi precoce, è de-finito sovradiagnosi.18
La presenza di questa tipologia di tumori è documentata an-che da studi autoptici che identificano la presenza di neopla-sie mai sospettate né diagnosticate in vita in pazienti decedutiper altra causa.19,20 L’esempio delle neoplasie diagnosticate postmortem serve a chiarire che anche una parte di quelle diagno-sticate in vita possono essere individuate solo per effettodegli esami eseguiti con altra finalità: se non ci fosse stato ilprimo tumore e l’iter diagnostico conseguente, i tumori in-dolenti non si sarebbero manifestati e quindi non avrebberocontribuito all’incidenza. L’esclusione nel periodo di sincro-nicità di questi tumori indolenti non dovrebbe pertantoavere effetto sulle stime dei SIR, mentre includerli causerebbeuna sovrastima. Per questo gruppo specifico, l’esclusione delperiodo di sincronicità produce stime più accurate.
Anticipazione diagnosticaLa diagnosi sincrona di alcuni tumori anticipa di qualche set-timana, mese o anno il loro normale decorso biologico cheli avrebbe resi sintomatici in tempi successivi. Questo è ilprincipio sul quale si basano gli screening,21 ovvero anticipare

I tumori multipli sincroniI tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI
122 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
la diagnosi in una fase preclinica di malattia nella quale la te-rapia sia in grado di modificare la prognosi determinando unariduzione della mortalità. Si tratta di tumori che si immaginasarebbero comparsi nel corso della vita di quei soggetti comesecondi tumori. Escluderli perché diagnosticati in prossimitàdella diagnosi del primo tumore sottostima il reale rischio disecondi tumori nella popolazione dei pazienti oncologici. Lasottostima è certa, ma l’entità non è quantificabile.
Per ottenere una stima non distorta dell’incidenza dei seconditumori, si dovrebbe escludere dalle analisi il primo gruppo (tu-mori indolenti) e includere il secondo (pur tenendo contodello spostamento temporale della diagnosi). Tuttavia nellapratica clinica è impossibile determinare se un secondo tumoresincrono sia stato sovradiagnosticato (cioè se non sarebbe maistato individuato in assenza dell’attività investigativa legata alprimo tumore) o soltanto anticipato (quindi diagnosticato inunmomento antecedente a quello in cui si sarebbe comunquemanifestato clinicamente), poiché tutti i cancri diagnosticativengono trattati, rendendo impossibile distinguere la storia na-turale della malattia dall’effetto del trattamento.
Lunghezza del periodo di sincronicitàE’ attesa una sottostima del rischio di incidenza di secondo tu-more nei periodi successivi a quello di sincronicità, dovuta al-l’assenza dei tumori che non sono diagnosticati perché laloro diagnosi è stata anticipata nel periodo di sincronicità, per-tanto esclusi dall’analisi.Tale sottostima sarà presumibilmentetanto maggiore quanto più esteso è il periodo di sincronicità.Gli studi citati in precedenza non sono tutti confrontabili,perché bisogna considerare anche altre variabili che possonocondizionare fortemente il numero di neoplasie in un sog-getto, per esempio se siano adottate diverse definizioni peri tumori multipli.22
In tabella 1, per i registri AIRTUM che avevano almeno 10anni di attività è stato valutato il rischio complessivo di svi-luppare un secondo tumore (esclusi osservati e attesi per lamedesima sede del primo tumore) in termini di SIR per en-trambi i sessi assieme e per tutti i tumori (esclusi gli epite-liomi cutanei).Se si considerano tutti i secondi tumori inclusi quelli sin-croni il rischio medio nel periodo complessivo di follow-upè del 23% (SIR: 1,23), se si esclude il primo mese questo ri-schio si dimezza (SIR: 1,12); se si escludono i primi tre mesiil numero dei secondi tumori osservati è del 9% più elevatodel numero atteso (SIR: 1,09); escludendo il primo anno,oppure il secondo o i primi 5 anni, il rischio risale. Quelloche si osserva nel lungo periodo, ovvero dopo alcuni anni,è un fenomeno complesso che risulta influenzato dall’assenzadi casi sovradiagnosticati osservati in coincidenza con ladiagnosi del primo tumore, ma anche dal deficit atteso pereffetto dell’anticipazione diagnostica. Inoltre, altri fattori chepossono determinare variazioni nell’incidenza sono gli effetti
activities related to the first cancer) or diagnosed early (diagnosedat a time prior to when it would be clinically evident). All di-agnosed cancers are treated, making it impossible to split thenatural history of the disease from the effect of treatment.
The length of the period of synchronicityAn underestimation of the risk of MP incidence is expectedafter the period of synchronicity, due to the absence of cancerswhose diagnosis has been anticipated in the period of syn-chronicity. This underestimation is likely to be greater the longerthe period of synchronicity.The aforementioned studies are not comparable, because theymay differ in other variables that can strongly influence thenumber of cancers in a subject, as, for example, the definitionof MP.22
In the following table, the MP SIRs have been analyzed fordifferent synchronicity cut-offs for AIRTUM registries with atleast 10 years of activity (both genders together and all cancersexcluding skin epithelioma). If all the cancers are considered,including synchronous ones, the average MP risk in the periodof follow-up is 23% (SIR: 1.23); if the first month after firstcancer diagnosis is excluded the risk is halved (SIR: 1.12 );excluding the first three months, the number of second cancersobserved is 9% higher than the number expected (SIR: 1.09);finally, excluding the first year, the second year, or the first 5years the risk increases. What can be seen in the long run, orafter a few years, is a complex phenomenon that is influencedby the absence of observed cases, because they are overdiagnosedsynchronously with the first cancer, but also influenced by theexpected deficit due to the anticipated diagnoses. Changes inincidence may also be due to treatment and the diagnostic fol-low-up pressure, and also to the possible occurrence of othercancers, related or unrelated to underlying genetic and envi-ronmental factors.On the contrary, excluding the first months after first cancerdiagnosis affects mainly the cases related with early diagnosisand over-diagnosis. The two-month period chosen by manyauthors and also adopted in this monograph seems to absorbthe whole effect of the diagnostic phase.
Length of follow-upThe exclusion of cancers whose diagnosis is anticipated will beeven more evident, with subsequent underestimated risk, whenthe total period of the study is short. For example, if a cancerregistry had only two months of activity, considering this periodas synchronous, SIRs for MPs would be zero. If the period islong or very long, the effect of the exclusion of synchronousevents, which is more evident in the months immediately fol-lowing the diagnosis, will be diluted the more the time of di-agnosis of the first cancer goes by, and the average risk will beonly marginally underestimated. In the present study, the timeof follow-up varies from registry to registry, from 3 to 32 years,with an average follow-up of 14.2 years.

OBS
ERVE
D/E
XPEC
TED
RATI
O(S
IR)
0.0
1.0
2.0
3.0
4.0
5.0
6.0
7.0
0 6 12 24 36 48 60
MONTHS SINCE DIAGNOSIS OF 1st CANCER
legati alle terapie e all’attività di follow-up e al possibile ma-nifestarsi di altri tumori legati a o indipendenti dalle carat-teristiche genetico-ambientali dei soggetti interessati.Al contrario, il “taglio” dei primi mesi si concentra prevalen-temente sugli aspetti di diagnosi precoce e sovradiagnosi le-gati alla definizione del primo tumore. I due mesi, scelti damolti autori e adottati anche in questa monografia, sembranoassorbire tutto l’effetto della fase diagnostica.
Lunghezza del periodo di follow-upL’esclusione di tumori la cui diagnosi è anticipata sarà piùevidente, con riduzione del rischio, nei periodi successivi alladiagnosi quando il periodo complessivo dello studio è breve.Per assurdo, se un registro avesse solo due mesi di attività,considerando questo periodo come sincrono, il SIR per i se-condi tumori sarebbe nullo. Se il periodo è lungo o moltolungo, l’effetto dell’esclusione di questi tumori, evidente neimesi immediatamente successivi, si diluirà tanto più ci si al-lontana dal momento della diagnosi del primo tumore e lamisura di rischio media complessiva sarà solo marginalmentesottostimata. Nello studio presentato in questa monografiail follow-up varia da registro a registro, da 3 a 32 anni, conun follow-up teorico medio di 14,2 anni.
CONCLUSIONIAdifferenza degli indicatori di incidenza, sopravvivenza e pre-valenza, per la determinazione dei quali i registri tumori adot-tano gli stessi standard e regole, per la stima dell’occorrenza deisecondi tumori in studi diversi sono effettuate scelte metodo-logiche differenti, a partire dalla definizione stessa di “tumorimultipli”, come discusso al capitolo 6 (pp. 114-119).E’ qui presentato l’effetto dell’esclusione degli eventi (tu-mori osservati e attesi) in un periodo presumibilmentecoincidente con quello della diagnosi del primo tumore (pe-riodo di sincronicità). Tale esclusione è motivata dalla ne-cessità di confrontare correttamente quanto osservato nellapopolazione generale con quanto atteso. Questo periodo hauna lunghezza arbitraria e la sua esclusione o inclusione puòportare a effetti anche rilevanti.Si conferma che l’effetto dell’esclusione sia una sottostimadel rischio di sviluppare secondi tumori, che diventa mag-
CONCLUSIONSTo compute incidence, survival, and prevalence, cancer registriesuse the same standards and rules,23,24 whereas for MP compu-tations different methodological choices have been applied indifferent studies, starting from the very definition of MP, asdiscussed in chapter 6 (pp. 114-119).In the present chapter, the effect of the exclusion of events (bothobserved and expected cancers) over a period presumably coin-ciding with that of the diagnosis of the first cancer (period ofsynchronicity) is discussed.This exclusion is justified by the needto properly compare what has been observed with the data expectedin the general population. This period has an arbitrary lengthand its exclusion or inclusion can lead to relevant effects.The effect of this exclusion is confirmed to be an underestimationof the risk of developing secondary cancers, which is greater themore extended the period of exclusion and the shorter the totalperiod of the study.In this monograph, it has been considered “synchronous”, inagreement with the choice of the majority of similar studies inthe literature,5-11 a period of two months from the date of di-
I tumori multipli sincroniI tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI
123 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
0+ 1+ 2+ 3+ 12+ 24+ 60+
O
94 424
O/E
1.23#
O
83 988
O/E
1.12#
O
80 989
O/E
1.10#
O
78 870
O/E
1.09#
O
68 159
O/E
1.11#
O
56 672
O/E
1.12#
O
32 303
O/E
1.14#
# p < 0.05
Tabella 1. Pool AIRTUM: Registri tumori con almeno 10 anni di incidenza disponibili nella Banca dati AIRTUM. Tutti i tumori maligni (esclusi i non melanomatosi dellacute) successivi a un primo tumore maligno (O): rapporto osservati/attesti (O/E) per periodo di follow-up.Table 1. AIRTUM Pool: Cancer registries with at least 10 years of incidence available in the AIRTUM Database, all malignancies (excluding non-melanoma skin cancer)subsequent to a first malignancy (O): ratio between observed/expected (O/E) cancers by period of follow-up.
Figura 1. Pool AIRTUM: registri tumori con almeno 10 anni di incidenza disponibilinella Banca dati AIRTUM. Rapporto standardizzato di incidenza fra secondi tumoriosservati e attesi (SIR), per tempo (mesi) dalla diagnosi del primo tumore.Figure 1. AIRTUM Pool: cancer registries with at least 10 years of incidenceavailable in the AIRTUM Database. Standardized Incidence Ratio betweenobserved and expected second cancers (SIR) by number of months since thediagnosis of the first cancer
FOLLOW-UP PERIOD (MONTHS)

giore tanto più esteso è il periodo escluso e tanto più breveè il periodo complessivo dello studio.In questa monografia abbiamo considerato “sincroni”, in ac-cordo con la scelta di maggioranza nella letteratura speci-fica,5-11 i tumori diagnosticati nei primi due mesi dalla dia-gnosi del primo, ma abbiamo anche scelto di presentare lestime complessive includendo questi tumori che sovrasti-mano il rischio oncologico dei pazienti poiché conteggianoanche una quota imprecisata di tumori indolenti; al contra-rio, la loro esclusione sottostima tale rischio per l’elimina-zione di una quota di tumori aggressivi la cui diagnosi è stataanticipata proprio in concomitanza della prima diagnosi.Il rischio oncologico “vero” di pazienti già affetti da un tu-more si collocherà fra le due stime, entrambe disponibili inquesta monografia.
agnosis of the first cancer, but the choose has been to presentthe estimates that include the first two months. Their inclusionoverestimates the MP risk for the inclusion of indolent cancers,their exclusion leads to an underestimation due to the elimi-nation of a portion of aggressive cancers whose diagnosis wasanticipated to the period of first diagnosis.The “true” MP risk for cancer patients will lie between thetwo estimates, both of which are available in this monograph.
I tumori multipli sincroniI tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI
124 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
BIBLIOGRAFIA/REFERENCES
1. Welch HG,Woloshin S, Schwartz LM. Skin biopsy rates and incidenceof melanoma: population based ecological study. BMJ 2005;331(7515):481.
2. Dal Maso L, Lise M, Zambon P et al; AIRTUM Working Group. Inci-dence of thyroid cancer in Italy, 1991-2005: time trends and age-pe-riod-cohort effects. Ann Oncol 2011;22(4):957-63.
3. Curtis RE, Boice JD Jr, Kleinerman RA, Flannery JT, Fraumeni JF Jr.Summary: multiple primary cancers in Connecticut, 1935-82. NatlCancer Inst Monogr 1985;68:219-42.
4. Curtis RE, Freedman DM, Ron E et al (eds). NewMalignancies AmongCancer Survivors: SEER Cancer Registries, 1973-2000. NIH Publ No.05-5302. Bethesda (MD), National Cancer Institute, 2006.
5. Storm HH, Jensen OM, Ewertz M et al. Summary: multiple primarycancers in Denmark, 1943-80. Natl Cancer Inst Monogr 1985;68:411-30.
6. Levi F, Randimbison L, Te VC, Rolland-Portal I, Franceschi S, La VecchiaC. Multiple primary cancers in the Vaud Cancer Registry, Switzerland,1974-89. Br J Cancer 1993;67(2):391-5.
7. Crocetti E, Buiatti E, Falini P; Italian Multiple Primary Cancer WorkingGroup. Multiple primary cancer incidence in Italy. Eur J Cancer2001;37(18):2449-56.
8. Tsukuma H, Fujimoto I, Hanai A, Hiyama T, Kitagawa T, Kinoshita N.Incidence of second primary cancers in Osaka residents, Japan, withspecial reference to cumulative and relative risks. Jpn J Cancer Res1994;85(4):339-45.
9. Tabuchi T, Ito Y, Ioka A, Miyashiro I, Tsukuma H. Incidence ofmetachronous second primary cancers in Osaka, Japan: update ofanalyses using population-based cancer registry data. Cancer Sci2012;103(6):1111-20.
10.Teppo L, Pukkala E, Saxén E. Multiple cancer – an epidemiologic ex-ercise in Finland. J Natl Cancer Inst 1985;75(2):207-17.
11.ColemanMP. Multiple primary malignant neoplasms in England andWales, 1971-1981. Yale J Biol Med 1986;59(5):517-31.
12.Karahalios E, English D, Thursfield V, Simpson J, Farrugia H, Giles G.Second primary cancers in Victoria. Victorian Cancer Registry, CancerEpidemiology Centre, The Cancer Council of Victoria, Australia.Melbourne 2009. Available at: http://www.cancervic.org.au/about-our-research/epidemiology/second-primary-cancers-victoria
13.Curado MP, Edwards B, Shin HR et al. Cancer Incidence in Five Con-tinents, Vol. IX. IARC Scientific Publication No. 160. Lyon, IARC, 2007.
14.Berrino F, Verdecchia A, Lutz JM, Lombardo C, Micheli A, CapocacciaR; EUROCAREWorking Group. Comparative cancer survival informa-tion in Europe. Eur J Cancer 2009,45(6):901-8.
15.Youlden DR, Baade PD. The relative risk of second primary cancersin Queensland, Australia: a retrospective cohort study. BMC Cancer2011;11:83.
16.Cluze C, Delafosse P, Seigneurin A, Colonna M. Incidence of secondcancer within 5 years of diagnosis of a breast, prostate or colorectalcancer: a population-based study. Eur J Cancer Prev 2009;18(5):343-8.
17.Heard A, Roder D, Luke C. Multiple primary cancers of separate organsites: implications for research and cancer control (Australia). CancerCauses Control 2005;16(5):475-81.
18.Puliti D, Duffy SW, Miccinesi G et al; EUROSCREEN Working Group.Overdiagnosis in mammographic screening for breast cancer in Eu-rope: a literature review. J Med Screen 2012;19 Suppl 1:42-56.
19.Breslow N, Chan CW, DhomG et al. Latent carcinoma of prostate atautopsy in seven areas. The International Agency for Research onCancer, Lyons, France. Int J Cancer 1977;20(5):680-8.
20.Sobrinho-Simôes MA, SambadeMC, Gonçalves V. Latent thyroid car-cinoma at autopsy: a study from Oporto, Portugal. Cancer 1979;43(5):1702-6.
21.Morrison AS. Screening in chronic disease. New York, Oxford Univer-sity Press, 1992.
22.Crocetti E, Buiatti E. Re: multiple neoplasias: an oncologic reality.J Natl Cancer Inst 1997;89(21):1634-6.

WWW.EPIPREV.IT
INTRODUZIONETra i registri tumori di tutto il mondo la Classificazione in-ternazionale delle malattie, X edizione (ICD-10) è da anniil riferimento per la pubblicazione dei dati di epidemiologiadescrittiva (incidenza, prevalenza, sopravvivenza, insorgenzadi tumori multipli), permettendo uniformità e sintesi nel-l’aggregazione delle diverse neoplasie e confronti tra areegeografiche diverse. Tutte le neoplasie maligne sono aggre-gate dall’ICD-10 in un centinaio di categorie principali, so-stanzialmente attraverso criteri di obiettività clinica, e spessoraggruppate in entità omogenee, utili a un’illustrazionedelle informazioni di base dei tumori principali. Questa sin-tesi è raggiunta a scapito della perdita di informazioni piùaccurate e spesso determinanti in ambito clinico o di sanitàpubblica; esse sono tuttavia custodite dai registri tumori cheper l’archiviazione dei casi utilizzano l’attuale terza versionedella ICD dedicata all’oncologia (International classificationof diseases for oncology, ICD-O-3), una nomenclatura concodici associati, e non propriamente una classificazione, spe-cificamente attrezzata per conservare informazioni detta-gliate su topografia e morfologia di ogni singola lesione.L’analisi dei dati presentati nelle schede specifiche per tu-more della presente monografia è basata sulla classificazioneICD-O-3 secondo le modalità di aggregazione previste inambito SEER, edizione 2003,1 come descritto nel capitolo«Materiali e metodi» (pp. 11-17).La classificazione delle neoplasie dell’apparato emolinfopo-ietico costituisce da molti anni un terreno estremamentecomplesso. Il cambio di paradigma classificativo (dallamorfologia degli anni Sessanta e Settanta alla tipizzazionefenotipica e alla biologia molecolare dei nostri giorni) ha fa-vorito continui aggiornamenti: il tempo necessario inevita-bile per la loro adozione su larga scala e l’indisponibilità(fino alla ICD-O-3 del 2000) di un sistema di codifica coe-rente hanno da sempre reso problematica l’analisi dell’in-cidenza di queste forme e soprattutto l’utilizzazione nellaclinica dei dati dei registri tumori.
FOREWORDThe International Classification of Diseases, tenth edition(ICD-10) has, for many years, been a benchmark for descrip-tive epidemiology publications (incidence, prevalence, survival,multiple primaries) allowing for a uniform, condensed ap-proach to grouping different neoplasms and comparing differ-ent areas. All malignant neoplasms are grouped in about ahundred main categories, mainly according to clinical criteria.These categories are further pooled into homogeneous entities,enabling us to outline basic information on cancer diffusion.This condensed approach works at the expense of accuracy andoften involves leaving out details that are important from theclinical perspective or from the point of view of public health.The information is stored by cancer registries, which use fortheir records the International Classification of Diseases forOncology, third edition (ICD-O-3), a list of diseases with as-sociated codes, to register the most detailed information avail-able on the topography and morphology of each lesion.Data on charts of the present Report have been classified ac-cording to the ICD-O-3 groups published by SEER, 2003 edi-tion1 (see chapter «Material and methods», pp. 11-17).Classification of haematopoietic and lymphoid cancer has longbeen an extremely complex task.The paradigm for classificationchanged over the past decades, from the morphological approachof the Sixties and Seventies to the phenotypic and biomolecularcharacterization of the last few years, prompting several classi-fication updates. The inevitable time gap between the publica-tion and the widespread use of a new classification, together withthe lack of a classification system with corresponding codes (untilICD-O-3 in 2000) have made it difficult to carry out a soundanalysis of these cancers and, consequently, impeded widespreaduse of cancer registry data in clinical research.In 2008, the fourthWorld Health Organisation (WHO) clas-sification of haematopoietic and lymphoid tumours was pub-lished, upending the weak correspondence between the cate-gories used by epidemiologists (ICD-10 and ICD-O-3) and thediagnoses made by pathologists and haematologists. This clas-
Valutazione del rischio di secondi tumoridelle neoplasie dell’apparatoemolinfopoietico alla lucedella classificazioneWHO 2008Risk assessment of second cancer incidenceof tumours of the haematopoietic and lymphoidtissue in light of the 2008WHO classification
125 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
I tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI
Capitolo 8

Nel 2008, è stata pubblicata la quarta classificazione del-l’Organizzazione mondiale della sanità (WHO) dei tumoridel tessuto emopoietico e linfatico,2 che sovverte la già fra-gile corrispondenza tra le aggregazioni basate su ICD-O-3e ICD-10 utilizzate dagli epidemiologi e le categorie di re-fertazione utilizzate in anatomia patologica e in oncoema-tologia. Questa classificazione abbandona l’ormai obsoletadistinzione tra neoplasie benigne e maligne, per assumerela tendenza più attuale a considerare i diversi livelli di ag-gressività di lesioni che debbono essere comunque registrati.Il riferimento al fenotipo biologico delle varie lesioni ha ri-voluzionato le categorie dell’ICD-10 e molti dei raggrup-pamenti di lesioni tradizionali: le forme mielodisplastichee mieloproliferative hanno ricevuto un riassestamento, conla separazione delle forme mature da quelle dei precursori.Il raggruppamento dei linfomi non-Hodgkin, ormai ana-cronistico, è stato disaggregato in base alle linee cellulariproliferanti (forme a precursori, cellule B mature, cellulemature T/NK); le forme plasmacellulari sono state ricon-dotte al loro progenitore fenotipico (linfocita B maturo).La caratterizzazione biologica sempre più accurata di questelesioni pone questioni importanti soprattutto negli studi suitumori multipli nello stesso paziente, che più di altri si fon-dano su comuni substrati biologici ed evolutivi di lesioni cli-nicamente differenti.Questo breve approfondimento è dedicato alla valutazionedi impatto della classificazione WHO 2008 delle neoplasieemolinfopoietiche sullo studio delle associazioni tra tumorimultipli a esse correlate, a titolo di modello di una possibileevoluzione nella pubblicazione di dati di epidemiologiadescrittiva più aderenti al debito informativo dei registri tu-mori nei confronti del mondo clinico.
MATERIALI E METODILe neoplasie dell’apparato emolinfopoietico codificate se-condo la ICD-O-3 nella Banca dati AIRTUM e analizzatein questo Rapporto sono state ricodificate e riattribuite aipazienti utilizzando i criteri della classificazione WHO2008; alle categorie di quest’ultima sono state associate, at-traverso i medesimi criteri biologici, morfologie tumoralipresenti nella ICD-O-3, ma non più considerate dalla clas-sificazione WHO (vd. tabella supplementare e2 on-line).Quale indicatore dei casi mal definiti, è stato consideratoa parte il gruppo di “linfomi e leucemie NAS”, presente inICD-O-3 e ovviamente non tra le categorie WHO. E’stata quindi riprodotta l’analisi di incidenza delle associa-zioni tra tumori multipli, attraverso i medesimi metodi e in-dicatori (rapporti standardizzati di incidenza - SIR e inter-valli di confidenza al 95% - IC95%) utilizzati nel presenteRapporto e una valutazione dell’impatto della classificazioneWHO 2008, proponendo alcune riflessioni critiche sui ri-sultati ottenuti.
sification abandons the obsolete distinction between benignand malignant tumours, opting for the more up to date ap-proach of assessing the different levels of aggressiveness of tu-mours, which are to be registered in any case. The phenotypicapproach of the new classification completely overturned theold ICD-10 categories. Myelodysplastic and myeloproliferativediseases were rearranged, as a separation was introduced be-tween precursor and mature forms. The outdated grouping of“non-Hodgkin lymphomas” was redistributed according toproliferative cell-lineage (precursor neoplasms, mature B-cell,mature T/NK-cell): plasma cell tumours were reassigned totheir own precursor (mature B-cell).The increasing accuracy in pathological characterization hasimportant consequences on multiple cancer incidence studies,since they are founded on common biological bases of (clini-cally) different diseases.This brief analysis focuses on the impact of the 2008 WHOclassification on the study of multiple primaries. It aims to sug-gest how data presentation by cancer registries might evolve tomeet the requirements of clinical research.
MATERIALS AND METHODSHaematological and lymphoid neoplasms coded according toICD-O-3 rules in the AIRTUM Database and analyzed in thepresent report were reassessed following the 2008WHO categories:ICD-O-3 entities no longer considered in theWHO classificationwere reassigned to biologically relatedWHO groups (see supple-mentary table e2 online). A group of NOS lymphomas andNOSleukaemias, which was not present in the WHO classification,was considered anyway, to quantify unknown morphologies. Ananalysis of incidence of multiple primaries in the same patient wasperformed according to the same methods and indexes as the pres-ent AIRTUMReport (Standard Incidence Ratio – SIR and Con-fidence Intervals 95% - 95%CI), evaluating the impact of the2008WHO classification.
RESULTSThe 157,199 lymphohematopoietic cancers analyzed in thepresent monograph were re-coded according to the 2008WHOclassification (table 1).Compared to the general population, a cancer patient has anincreased risk of developing an additional myelodysplastic syn-drome or acute myeloid leukaemia (SIR: 1.15; 95%CI 1.04-1.26 and SIR: 1.48; 95%CI 1.39-1.59, respectively). A de-creased incidence risk for mature B-cell neoplasms was alsoobserved (SIR: 0.93; 95%CI 0.90-0.95). Excesses and reduc-tions (when statistically significant) in the risk of developingsecond haematological malignancies are shown (separately foreach first cancer site) in table 2. An increased risk for myelo-proliferative neoplasms was observed in patients with previouscancers of the pharynx (SIR: 2.67; 95%CI 1.22-5.07), kidney(SIR: 1.71; 95%CI 1.16-2.45), and urinary bladder (SIR:1.29; 95%CI 1.05-1.58). An excess risk for further myelodys-
Rischio di secondi tumori dell’apparato emolinfopoieticoI tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI
126 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152

RISULTATILe 157.199 neoplasie del sistema emolinfopoietico, oggettodella presente monografia e ricodificate secondo la classifi-cazione WHO 2008, sono indicate in dettaglio in tabella 1.Rispetto alla popolazione generale, i pazienti portatori di unprimo tumore di qualunque sede mostrano un aumento diprobabilità di contrarre una sindrome mielodisplastica euna leucemia mieloide acuta, rispettivamente con SIR di1,15 (IC95% 1,04-1,26) e SIR di 1,48 (IC95% 1,39-1,59),mentre si è osservata una lieve diminuzione del rischio neiconfronti delle neoplasie a cellule B mature (SIR: 0,93;IC95% 0,90-0,95). La tabella 2 presenta in dettaglio gli ec-cessi e le riduzioni (statisticamente significative) di rischio diinsorgenza di seconde neoplasie ematologiche in rapportoalle singole sedi di primo tumore.Tra queste, l’aumento del rischio di insorgenza di neoplasiemieloproliferative è emerso in particolare nei maschi portatoridi neoplasie della faringe (SIR: 2,67; IC95% 1,22-5,07), delrene (SIR: 1,71; IC95% 1,16-2,45) e della vescica (SIR:1,29; IC95% 1,05-1,58). L’eccesso di sindromi mielodispla-stiche è stato rilevato soprattutto nei pazienti con precedentetumore dello stomaco (SIR: 1,68; IC95% 1,11-2,45), dellamammella femminile (SIR: 1,29; IC95% 1,00-1,65), dellacervice uterina (SIR: 3,54; IC95% 1,52-6,97) e del rene, spe-cie nei maschi (SIR: 1,79; IC95%1,02-2,91). Il rischio di leu-cemiamieloide acuta è aumentato sensibilmente dopo tumoridi diverse sedi anatomiche, in primis di prime vie aeree, sto-maco, polmone, tessuti molli, mammella e apparato genitale,rene e vie urinarie, sistema nervoso centrale nei maschi (SIR:3,80; IC95% 1,22-8,86) e tiroide prevalentemente nelle fem-mine (SIR: 2,36; IC95% 1,29-3,95). Nelle pazienti conprimo tumore ovarico si è riscontrato un aumento del rischioanche di leucemie acute di linea ambigua, che risulta invecediminuito nei pazienti con primo tumore prostatico.Il rischio di incidenza di neoplasie dei precursori linfoidi ap-pare particolarmente aumentato nel sesso femminile conprecedente tumore osseo (SIR: 38,75; IC95% 7,79-113,23)e nei pazienti con pregresso tumore testicolare.Rispetto alla popolazione generale, l’insorgenza di una neo-plasia a cellule B mature è diminuita in pazienti con pre-gresse neoplasie all’esofago, particolarmente nei maschi(SIR: 0,32; IC95% 0,06-0,93), allo stomaco soltanto nelledonne (SIR: 0,71; IC95% 0,53-0,93), nel colon e nelretto, nelle vie biliari e nel polmone. Un aumento del ri-schio si verifica invece dopo un precedente sarcoma di Ka-posi, specie nei maschi (SIR: 2,81; IC95% 1,88-4,04).Nelle donne con precedente neoplasia del retto si è osser-vato un aumento del rischio di forme a cellule T e NK ma-ture (SIR: 2,65; IC95% 1,14-5,21).L’insorgenza di un linfoma diHodgkin è inferiore all’atteso neipazienti con pregresso tumore dello stomaco e superiore dopoun sarcoma di Kaposi e un carcinoma della cervice uterina.Il rischio di insorgenza di secondi tumori nei vari organi
plastic syndromes was observed in the stomach (SIR: 1.68;95%CI 1.11-2.45), female breast (SIR: 1.29; 95%CI 1.00-1.65), cervix uteri (SIR: 3.54; 95%CI 1.52-6.97), kidney, es-pecially among male cancer patients (SIR: 1.79; 95%CI1.02-2.91).Risk of developing acute myeloid leukaemia was higher amongpatients with a first malignancy of the upper aerodigestivetract, stomach, lung, soft tissues, breast, genital and urinarytract, central nervous system in men (SIR: 3.80; 95%CI 1.22-8.86), and thyroid especially in women (SIR: 2.36; 95%CI1.29-3.95).Women with first ovarian malignancy showed an increasedrisk for acute leukaemia of ambiguous lineage. On the contrary,the risk was lower among men with a first cancer in theprostate (table 2).Further precursor lymphoid neoplasms are more frequent in fe-males with previous bone tumours (SIR: 38.75; 95%CI 7.79-113.23) and males with a testicular malignancy.The incidence risk of later mature B-cell neoplasms is lower inoesophageal cancer patients, especially among men (SIR: 0.32;95%CI 0.06-0.93), as well as in females with gastric cancer(SIR: 0.71; 95%CI 0.53-0.93) and in both sexes with colorec-tal, biliary tract and lung cancer. On the other hand, an in-creased risk was observed after Kaposi sarcoma, especiallyamong men (SIR: 2.81; 95%CI 1.88-4.04). Women withprevious rectal cancer showed an increased risk of mature T-cell/NK – cell neoplasms (SIR: 2.65; 95%CI 1.14-5.21).Hodgkin lymphoma risk was lower in patients with previousgastric cancer, but higher after Kaposi sarcoma and cancer ofthe cervix uteri.Several other associations between a first haematological cancer
Rischio di secondi tumori dell’apparato emolinfopoieticoI tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI
127 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
CASES %Myeloproliferative neoplasms 15 332 9.8Myeloid and lymphoid neoplasms with eosinofilia 0 –and abnormalities of PDGFRA, PDGFRB or FGFR1Myelodysplastic/myeloproliferative neoplasms 548 0.3Myelodysplastic syndromes 5 436 3.5Acute myeloid leukaemia and related 12 805 8.1precursor neoplasmsAcute leukaemias of ambiguous lineage 1 573 1.0Precursor lymphoid neoplasms 4 922 3.1Mature B-cell neoplasms 92 840 59.1Mature T-cell and NK-cell neoplasms 4 730 3.0Hodgkin lymphoma 10 850 6.9Histiocytic and dendritic cell neoplasms 277 0.2Post-transplants lymphoproliferative disorders 0 –Leukaemias/lymphomas NOS 7 886 5.0Total 157 199
Tabella 1. Pool AIRTUM, 1978-2010. Distribuzione delle neoplasie dell’apparatoemolinfopoietico dopo riclassificazione secondo la classificazione WHO 2008(include tutti i tumori indipendentemente dalla sequenzialità, primi e successivi).Table 1. Pool AIRTUM, 1978-2010. Haematological neoplasms reassignedaccording to the 2008 WHO classification (all cancers considered, independentlyfrom sequence, first or subsequent).

successivamente all’incidenza di neoplasie ematologiche ele associazioni osservate, spesso nel contesto dello stesso ap-parato, sono illustrate in dettaglio in tabella 3.La tabella 4 riporta i diversi esiti dell’analisi del rischio di se-condo tumore ematologico in conseguenza all’adozionedella classificazione WHO 2008, rispetto alle tradizionali ca-tegorie nosologiche utilizzate nella monografia. I pazienticon primo tumore ematologico classificato secondo i gruppiICD-O-3 presentano, rispetto alla classificazione WHO, di-verse analogie di rischio di secondo tumore, pur con diffe-renze compatibili con l’impostazione nosologica differente.
and further malignancies (often within the same body system)were observed. Detailed results are shown in table 3.The comparison between second cancer incidence analysisbased on the 2008WHO classification and second cancer in-cidence analysis based on traditional nosological categories arepresented in table 4. Patients with first haematological cancersclassified according to ICD-O-3, compared to theWHO clas-sification, show similarities in second cancer risk, althoughthere are variations compatible with the different nosologicalapproaches.
Rischio di secondi tumori dell’apparato emolinfopoieticoI tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI
128 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
Decrease SIR <1Increase SIR >1
FIRST CANCER SITE SECOND HEMATOLOGICAL CANCER OBSERVED SIR (95%IC)CASES
ORAL CAVITY AML and related precursor neoplasms 14 2.72 (1.49-4.57)
PHARYNX Myeloproliferative neoplasms 9 2.25 (1.02-4.26)
AML and related precursor neoplasms 12 3.73 (1.93-652)
LARYNX AML and related precursor neoplasms 26 1.59 (1.04-2.34)
OESOPHAGUS Mature B-cell neoplasms 5 0.42 (0.14-0.98)
STOMACH Myelodysplastic syndromes 27 1.68 (1.11-2.45)
AML and related precursor neoplasms 43 1.72 (1.24-2.31)
Hodgkin lymphoma 1 0.14 (0.00-0.77)
COLON Mature B-cell neoplasms 430 0.89 (0.81-0.98)
RECTUM Mature B-cell neoplasms 180 0.83 (0.71-0.96)
GALLBLADDER Mature B-cell neoplasms 9 0.44 (0.20-0.83)
LUNG AML and related precursor neoplasms 40 1.47 (1.05-2.00)
Mature B-cell neoplasms 168 0.82 (0.70-0.95)
SOFT TISSUE AML and related precursor neoplasms 7 2.62 (1.05-5.39)
BONE Precursor lymphoid neoplasms 3 15.55 (3.13-45.43)
BREAST Myelodysplastic syndromes 68 1.31 (1.02-1.66)
AML and related precursor neoplasms 173 1.79 (1.53-2.07)
Leukaemias/lymphomas NOS 42 0.71 (0.51-0.96)
CERVIX UTERI Myelodysplastic syndromes 8 3.54 (1.52-6.97)
Hodgkin lymphoma 7 3.05 (1.22-6.28)
CORPUS UTERI AML and related precursor neoplasms 27 1.62 (1.07-2.36)
OVARY Acute leukaemias of ambiguous lineage 4 6.79 (1.83-17.39)
PROSTATE AML and related precursor neoplasms 122 1.24 (1.03-1.48)
Acute leukaemias of ambiguous lineage 4 0.37 (0.10-0.96)
TESTIS Precursor lymphoid neoplasms 4 7.10 (1.91-18.17)
KIDNEY Myeloproliferative neoplasms 41 1.70 (1.22-2.31)
Myelodysplastic syndromes 21 1.70 (1.05-2.59)
AML and related precursor neoplasms 30 1.51 (1.02-2.15)
URINARY BLADDER Myeloproliferative neoplasms 114 1.32 (1.09-1.58)
AML and related precursor neoplasms 94 1.31 (1.06-1.60)
THYROID AML and related precursor neoplasms 18 2.19 (1.30-3.46)
KAPOSI SARCOMA Mature B-cell neoplasms 36 2.61 (1.83-3.62)
Hodgkin lymphoma 3 5.09 (1.02-14.87)
Leukaemias/lymphomas NOS 10 8.73 (4.18-16.06)
ALL SITES BUT SKIN Myelodysplastic syndromes 435 1.15 (1.04-1.26)
AML and related precursor neoplasms 895 1.48 (1.39-1.59)
Mature B-cell neoplasms 4 117 0.93 (0.90-0.95)
Leukaemias/lymphomas NOS 312 0.89 (0.80-1.00)
AML = Acute myeloid leukaemia.
Tabella 2. Incidenza di seconde neoplasie ematologiche metacrone per sede della prima neoplasia non ematologica (casi osservati eSIR statisticamente significativi, maschi e femmine).Table 2. Incidence of metachronous second haematological cancers by first non-haematological cancer site (number of observed cases,SIR, men and women).

Rischio di secondi tumori dell’apparato emolinfopoieticoI tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI
129 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
Decrease SIR <1Increase SIR >1
FIRST HEMATOLOGICAL CANCER SECOND CANCER SITE OBSERVED SIR (95%IC)CASES
MYELOPROLIFERATIVE NEOPLASMS Lung 119 1.24 (1.03-1.49)
Melanoma 21 1.77 (1.10-2.71)
Thyroid 14 1.88 (1.0-3.15)
Acute leukaemias of ambiguous lineage 5 8.81 (2.84-20.56)
MYELOPROLIFERATIVE/MELODYSPLASTIC NEOPL. Mature T-cell and NK-cell neoplasms 2 42.20 (4.74-152.37)
MYELODYSPLASTIC SYNDROMES Gallbladder 9 2.80 (1.28-5.32)
Myeloproliferative/myelodysplastic neoplasms 2 17.60 (1.98-63.55)
Acute leukaemias of ambiguous lineage 2 11.30 (1.27-40.81)
Mature T-cell and NK-cell neoplasms 3 5.95 (1.20-17.39)
Leukaemias/lymphomas NOS 7 7.62 (3.05-15.71)
Kaposi sarcoma 4 9.76 (2.63-24.99)
All sites but skin and site of first cancer 252 1.26 (1.11-1.43)
AML AND RELATED PRECURSOR NEOPLASMS Prostate 6 0.38 (0.14-0.82)
Urinary bladder 4 0.39 (0.10-0.99)
ACUTE LEUKAEMIAS OF AMBIGUOUS LINEAGE Melanoma 2 10.27 (1.15-37.09)
PRECURSOR LYMPHOID NEOPLASMS Thyroid 7 7.13 (2.86-14.69)
All sites but skin and site of first cancer 59 1.41 (1.08-1.82)
MATURE B-CELL NEOPLASMS Oral cavity 58 1.39 (1.05-1.79)
Rectum 177 0.85 (0.73-0.99)
Liver 231 1.34 (1.18-1.53)
Gallbladder 52 0.73 (0.54-0.96)
Lung 833 1.29 (1.20-1.38)
Melanoma 135 1.78 (1.49-2.11)
Soft tissue 34 1.88 (1.31-2.63)
Corpus uteri 59 0.74 (0.56-0.96)
Prostate 546 0.90 (0.83-0.98)
Testis 10 2.12 (1.02-3.90)
Kidney 190 1.38 (1.19-1.59)
Urinary bladder 435 1.12 (1.02-1.23)
Myeloproliferative neoplasms 21 0.54 (0.33-0.82)
AML and related precursor neoplasms 69 2.08 (1.62-2.63)
Hodgkin lymphoma 31 2.88 (1.96-4.09)
Leukaemias/lymphomas NOS 5 0.26 (0.09-0.62)
Mesothelioma 34 1.62 (1.12-2.26)
Kaposi sarcoma 39 4.27 (3.03-5.83)
All sites but skin and site of first cancer 5 007 1.09 (1.06-1.12)
MATURE T-CELL AND NK-CELL NEOPLASMS Urinary bladder 34 1.47 (1.02-2.05)
Thyroid 8 3.06 (1.32-6.04)
AML and related precursor neoplasms 7 3.75 (1.50-7.72)
Hodgkin lymphoma 8 12.47 (5.37-24.57)
Kaposi sarcoma 5 9.37 (3.02-21.88)
All sites but skin and site of first cancer 322 1.18 (1.05-1.32)
HODGKIN LYMPHOMA Oesophagus 8 2.96 (1.28-5.84)
Lung 96 2.46 (1.99-3.00)
Melanoma 19 2.10 (1.27-3.28)
Soft tissue 8 4.59 (1.98-9.04)
Breast 71 1.71 (1.34-2.16)
Kidney 19 1.95 (1.17-3.04)
Thyroid 21 2.62 (1.62-4.01)
AML and related precursor neoplasms 27 11.30 (7.45-16.45)
Mature B-cell neoplasms 51 3.01 (2.24-3.95)
Mature T-cell and NK-cell neoplasms 8 7.85 (3.38-15.47)
Kaposi sarcoma 4 5.10 (1.37-13.07)
All sites but skin and site of first cancer 582 1.73 (1.59-1.88)
LEUKAEMIAS/LYMPHOMAS NOS Lung 55 1.48 (1.12-1.93)
Mature B-cell neoplasms 6 0.41 (0.15-0.89)
AML = Acute myeloid leukaemia.
Tabella 3. Incidenza di secondi tumori metacroni in pazienti con prime neoplasie ematologiche (casi osservati e SIR statisticamente signi-ficativi, maschi e femmine).Table 3. Incidence of metachronous second cancers by first haematological cancer site (number of observed cases, SIR, men and women).

Decrease SIR <1Increase SIR >1
SECOND HAEMATOLOGICAL CANCER ACCORDING TO FIRST CANCER SITE SECOND HAEMATOLOGICAL CANCER ACCORDING TOWHO 2008 CLASSIFICATION ICD-O-3 CLASSIFICATION
AML and related precursor neoplasms ORAL CAVITY Non-Hodgkin lymphoma
Myeloid leukaemia PHARYNX Myeloid leukaemia
Myeloproliferative neoplasms
AML and related precursor neoplasms
AML and related precursor neoplasms LARYNX Myeloma
Mature B-cell neoplasms OESOPHAGUS –Myelodysplastic syndromes
AML and related precursor neoplasms
Hodgkin lymphoma STOMACH Myeloid leukaemia
Hodgkin lymphoma
Mature B-cell neoplasms COLON Lymphoid leukaemia
Mature B-cell neoplasms RECTUM Myeloma
Non-Hodgkin lymphoma
Mature B-cell neoplasms GALDBLADDER Non-Hodgkin lymphoma
AML and related precursor neoplasms
Mature B-cell neoplasms LUNG
Myeloma
AML and related precursor neoplasms SOFT TISSUE –Precursor lymphoid neoplasms BONE Lymphoid leukaemia
Myelodysplastic syndromes
AML and related precursor neoplasms
Leukaemias/lymphomas NOS BREAST Myeloid leukaemia
Melodysplastic syndromes
Hodgkin lymphoma CERVIX UTERI Hodgkin lymphoma
AML and related precursor neoplasms CORPUS UTERI Myeloid leukaemia
Acute leukaemias of ambiguous lineage OVARY Myeloid leukaemia
Lymphoid leukaemia
Other leukaemias
AML and related precursor neoplasms
Acute leukaemias of ambiguous lineage PROSTATE –Precursor lymphoid neoplasms TESTIS Myeloid leukaemia
Myeloproliferative neoplasms
Myelodysplastic syndromes
AML and related precursor neoplasms KIDNEY Myeloid leukaemia
Non-Hodgkin lymphoma
Myeloproliferative neoplasms
AML and related precursor neoplasms URINARY BLADDER Myeloid leukaemia
AML and related precursor neoplasms THYROID Myeloid leukaemia
Myeloma
Mature B-cell neoplasms
Hodgkin lymphoma
Leukaemias/lymphomas NOS KAPOSI SARCOMA Non-Hodgkin lymphoma
Hodgkin lymphoma
Myelodysplastic syndromes
AML and related precursor neoplasms
Mature B-cell neoplasms
Leukaemias/lymphomas NOS ALL SITES BUT SKIN Myeloid leukaemia
Myeloma
Lymphoid leukaemia
Tabella 4. Impatto delle diverse classificazioni nella valutazione del rischio di insorgenza di secondi tumori ematologici in rapportoalla sede di prima neoplasia (SIR statisticamente significativi).Table 4. Impact of different classifications in risk assessment of second haematological cancers by first cancer site (only statisticalsignificant SIRs).
Epidemiol Prev 37 (4-5) Suppl 1:1-152 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.it130
I tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI Rischio di secondi tumori dell’apparato emolinfopoietico

Epidemiol Prev 37 (4-5) Suppl 1:1-152 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.it131
I tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI Rischio di secondi tumori dell’apparato emolinfopoietico
DISCUSSIONThis brief report represents AIRTUM’s first experience with theuse of the newWHO 2008 classification system. The reclassi-fication of historical data exposes to unavoidable biases due tothe changes in classifications and coding over time, with dif-ferent effects which depend on the duration of registry activityand registration practices. Some entities (e.g., myelodysplasticsyndromes) have been more recently included into the cases tobe registered, whereas other lesions have been considered in dif-ferent ways over the course of time (from benign/borderline tomalignant and vice-versa; from “tumour-like” to neoplasms,etc.). Some ICD-O-3 NOS codes (e.g., 9591) include bothNOS cases and lesions classified in specific categories. All so-lutions adopted here to tackle these difficult problems representan attempt to lessen any classification bias.An overview on the outcomes of this new classification on can-cer registry data opens up new perspectives and suggests moresensitivity to clinical medicine and biology. Nevertheless, it pres-ents a number of risks: registries must deal with issues of ho-mogeneity and reproducibility in the application of classifica-tions, and accuracy of the collected morphological data.Especially in multiple cancer studies, a classification based onbiological phenotypes, such as WHO 2008, makes it muchmore possible to recognize common biological pathways than“clinical” classifications (ICD-10 and ICD-O-3) can do.Data already collected by cancer registries according to theICD-O-3 classification showed good compliance with the newWHO 2008 system and cases of leukaemias and lymphomaswithout an accurate definition (NOS) remained under 5%and were fewer in recent years.This introductory analysis confirms well-known associationsamong cancer types: patients with a first mature B-cell neo-plasm have an increased risk of developing further soft tissue,kidney and liver malignancies, and a lower risk for prostatecancer. Other well known associations are the one between ma-ture T/NK cells neoplasms and a “second” Kaposi sarcoma, aswell as the increased risk for thyroid cancer and Kaposi sarcomain patients previously affected by Hodgkin lymphoma, and foracute myeloid leukaemia in thyroid cancer patients. Even re-gardless of an in-depth analysis of observed associations and bi-ological pathways in multiple cancer incidence, this prelimi-nary study highlights the better accuracy of the WHO 2008classification in showing associations often barely identified byICD-10 and ICD-O-3 or previous classifications (e.g., for“precursor” forms, mature B/T/NK cell, etc.). This brief com-parison between the two approaches, although to be taken cau-tiously due to the differences in several basic criteria, allows usto identify a greater accuracy of the WHO 2008 categories inhighlighting associations based on common risk pathways orcombined effects of therapies.These preliminary evaluations suggest the need for further re-search, not only limited to haematological malignancies, to-ward morphological subcategories or groupings of homogeneous
DISCUSSIONEQuesto breve approfondimento rappresenta la prima espe-rienza che AIRTUM svolge nell’utilizzo del nuovo sistemaclassificativo WHO 2008, con la conversione dei dati storicisecondo i nuovi criteri. La riclassificazione di dati storiciespone a distorsioni inevitabili derivanti dai cambiamenti diclassificazioni e codifiche nel corso del tempo, con effetti di-versi in rapporto alla durata di attività dei singoli registri ealle pratiche di registrazione differenti: alcune entità in par-ticolare (per esempio, le sindromi mielodisplastiche) sonostate più recentemente comprese tra le forme da registraree alcune lesioni sono state considerate in modo diverso neltempo (da benigne/borderline a maligne e viceversa; da le-sioni “simil-tumorali” a neoplasie).3 Alcuni codici ICD-O-3 NAS (per esempio, 9591) raggruppano sia lesioni non spe-cificate, sia forme classificate in specifiche categorie. Si trattadi problemi complessi per i quali sono state qui adottatescelte ritenute più efficaci nel contenere le distorsioni.Esplorare la ricaduta di questa classificazione clinica sui datiraccolti dai registri tumori apre certamente nuove prospet-tive di riflessione e propone una sensibilità maggiore neiconfronti delle esigenze informative del mondo clinico. Sitratta di un’operazione non priva di rischi, per problemi diriproducibilità e omogeneità di applicazione dei vari sistemidi classificazione e di accuratezza dei dati morfologici a di-sposizione dei registri. Soprattutto nello studio dei tumorimultipli, la classificazione in riferimento al fenotipo biolo-gico (WHO 2008) consente l’osservazione di relazioni pa-togenetiche che le classificazioni basate sul quadro clinico(categorie ICD-O-3 e ICD-10) evidenziano più difficil-mente. Riguardo ai dati rilevati è innanzitutto interessanteosservare che gran parte dell’informazione richiesta dallanuova classificazione WHO delle neoplasie dell’apparatoemolinfopoietico è già disponibile presso i registri attraversoi sistemi di codifica correnti (ICD-O-3) con livelli di accu-ratezza accettabili. Le percentuali di linfomi e leucemiemaldefiniti e comunque non collocabili nelle nuove cate-gorie è contenuta entro il 5%, in progressivo calo negli annipiù recenti. Questa analisi preliminare conferma associa-zioni note in letteratura: pazienti con prima diagnosi di neo-plasie a cellule B mature presentano un aumento del rischionei confronti di ulteriori neoplasie di tessuti molli,4,5 rene6
e fegato7 e una diminuzione di rischio per carcinoma pro-statico.8 E’ nota l’associazione tra neoplasie a elementiT/NK e insorgenza di un successivo sarcoma di Kaposi,9
così come l’aumento di incidenza di tumori della tiroide10
e sarcoma di Kaposi11 in pazienti già affetti da linfoma diHodgkin, e di leucemia mieloide acuta nei pazienti con pre-gresso carcinoma della tiroide.12,13
Prescindendo da un’analisi dettagliata delle relazioni ri-scontrate e delle associazioni tra determinanti biologici, cheesula dagli scopi di questo approfondimento preliminare,è evidente la maggiore accuratezza della classificazione

WHO nel cogliere associazioni che spesso le categorie tra-dizionali ICD-O-3 e ICD-10 identificano ma non caratte-rizzano con precisione (forme precursore e mature, a feno-tipo B/T-NK eccetera). Il confronto sintetico presentato trai due approcci, pur con le dovute cautele per i diversicriteri di base, consente di cogliere la maggior precisionedelle categorie WHO 2008 nell’evidenziare associazionisulla base di percorsi comuni di rischio o di effetti combi-nati delle terapie adottate.Queste considerazioni invitano a identificare disaggrega-zioni e raggruppamenti morfologici (non solo per i tumoriematologici) in costante collegamento con i progressi cor-renti nella caratterizzazione delle neoplasie, per le valuta-zioni di impatto predittivo e prognostico sollecitate dalla cli-nica e dall’anatomia patologica.
CONCLUSIONILa suddivisione della casistica nei raggruppamenti conven-zionali delle classificazioni ICD-O-3 e ICD-10 rappresentae continuerà a rappresentare, fino alla sua prossima evolu-zione,14 lo standard di codifica e reportistica nell’epidemio-logia descrittiva dei tumori. Ma è opportuno considerarne ilimiti nei vari tipi di approccio allo studio dell’incidenza deitumori, nell’ottica di una comprensione migliore dei fattoridi rischio e dell’impatto dei percorsi diagnostici e assistenzialidei pazienti oncologici. La storia recente del rapporto tra i re-gistri tumori e gli ambienti della clinica e della sanità pubblicaha chiaramente illustrato le potenzialità, in larga parte ancorainespresse, dei dati dei registri a concorrere alla sorveglianzadi ogni settore della lotta contro i tumori, secondo criteri diefficacia, equità e appropriatezza.
lesions in several cancer sites, with a stronger predictive andprognostic impact, as already pointed out by pathology andclinical medicine.
CONCLUSIONSThe ICD-10 classification still represents, and will continueto represent in its future issues, an international standard forcoding tumours and publishing epidemiological data. But weshould consider its limits in the study of cancer incidence, witha view to achieve a better understanding of risk factors and theimpact of the diagnostic and therapeutic process undergone bycancer patients. The recent history of connection between can-cer registries, clinicians and public health care has clearly il-lustrated the potential of cancer registry data to support cancersurveillance, based on effective, fair, and suitable criteria.
Rischio di secondi tumori dell’apparato emolinfopoieticoI tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI
132 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
BIBLIOGRAFIA/REFERENCES
1. http://seer.cancer.gov/siterecode/icdo3_d01272003/2. Swerdlow SH, Campo E, Harris NL et al (eds).WHO Classification of
tumours of Hematopoietic and Lymphoid Tissues. Lyon, IARC, 2008.3. Fritz A, Percy C, Jack A, et al (eds). International Classification of
Disease for Oncology, third edition. Geneva, WHO, 2000.4. Tavani A, Pregnolato A, Negri E, et al. Diet and risk of lymphoid neo-
plasms and soft tissue sarcomas. Nutr Cancer 1997;27(3):256-60.5. Miligi L, Costantini AS, Veraldi A, Benvenuti A; WILL, Vineis P. Can-
cer and pesticides: an overview and some results of the Italian mul-ticenter case-control study on hematolymphopoietic malignancies.Ann N Y Acad Sci 2006;1076:366-77.
6. Liu H, Hemminki K, Sundquist J. Renal cell carcinoma as first andsecond primary cancer: etiological clues from the Swedish Family-Cancer Database. J Urol 2011;185(6):2045-9.
7. Tanaka H, Tsukuma H, Teshima H et al. Second primary cancers fol-lowing non-Hodgkin’s lymphoma in Japan: increased risk of hepa-tocellular carcinoma. Jpn J Cancer Res 1997;88(6):537-42.
8. Nielsen SF, Nordestgaard BG, Bojesen SE. Associations between firstand second primary cancers: a population-based study. CMAJ2012;184(1):E57-69.
9. Ariad S, Lewis D, Bezwoda WR. Kaposi’s sarcoma after alpha-inter-feron treatment for HIV-negative T-cell lymphoma. S Afr Med J1993;83(6):430-1.
10.Tward J, GlennM, Pulsipher M, Barnette P, Gaffney D. Incidence, riskfactors, and pathogenesis of second malignancies in patients withnon-Hodgkin lymphoma. Leuk Lymphoma 2007;48(8):1482-95.
11.Ulbright TM, Santa Cruz DJ. Kaposi’s sarcoma: relationship withhematologic, lymphoid, and thymic neoplasia. Cancer 1981;47(5):963-73.
12.Subramanian S, Goldstein DP, Parlea L et al. Second primary ma-lignancy risk in thyroid cancer survivors: a systematic review andmeta-analysis. Thyroid 2007;17(12):1277-88.
13.Sawka AM, Thabane L, Parlea L et al. Second primary malignancyrisk after radioactive iodine treatment for thyroid cancer: a system-atic review and meta-analysis. Thyroid 2009;19(5):451-7.
14.www.who.int/classifications/icd/revision/en/

WWW.EPIPREV.IT
BACKGROUND E OBIETTIVILa suscettibilità ai fattori di rischio per cancro può variare inmaniera importante in relazione all’età e al sesso degli indi-vidui. L’età al primo tumore gioca un ruolo fondamentale nelrischio di svilupparne un secondo e può riflettere la differenteinfluenza dei fattori di rischio in rapporto a modalità di espo-sizione, suscettibilità del paziente ad ammalarsi, tempo di la-tenza necessario a sviluppare un secondo tumore in relazioneall’attesa di vita, età e/o stadio del primo tumore.1
Il presente lavoro ha come scopo principale la presentazione distime di eccesso o difetto di rischio di sviluppare un secondo tu-more inuna coorte di pazienti condiagnosi pregressa di neoplasiarispetto alla popolazione generale di uguale sesso e fascia di età.
MATERIALI E METODILa coorte di pazienti in studio è stata costituita a partire dal-l’insieme dei database dei Registri tumori (RT) italiani accre-ditati nell’Associazione italiana registri tumori (AIRTUM).Sono stati considerati tutti i secondi tumori primitivi meta-croni (MP) diagnosticati durante il periodo di attività dei sin-goli registri che, come riportato nel capitolo «Materiali e me-todi» (pp. 11-17), varia da 3 a 33 anni. Sono stati consideratiMP solo i tumori diagnosticati almeno 2 mesi dopo la dia-gnosi della prima neoplasia (FPN) e, quindi, MP non regi-strati sono sottratti dalle misure di rischio possibili.Sono stati esclusi dallo studio i soggetti che avevano svilup-pato il primo tumore in età infantile o adolescenziale, inquanto il trattamento effettuato in età evolutiva potrebbe avercondizionato la loro suscettibilità a fattori eziologici in etàadulta e aver contribuito allo sviluppo del MP.Sulla base dell’età alla diagnosi della FPN la coorte è stata sud-divisa in tre fasce d’età: 20-49 anni, 50-69 anni e ≥70 anni,definite in relazione al diverso impatto potenziale deifattori/condizioni di rischio nelle diverse età e alla storia na-turale delle varie neoplasie. Per la fascia d’età più giovane (20-49 anni) è stato tentato anche un approccio più dettagliato,suddividendola in ulteriori fasce decennali per cercare di de-scrivere meglio gli eccessi di rischio osservati rispetto a unacomponente di predisposizione ereditaria possibile, che po-trebbe avere un peso differente nei diversi substrati di età: lanumerosità modesta dei casi e la conseguente instabilità dellestime di eccesso di rischio hanno precluso questa valutazioneper le singole neoplasie; si è quindi deciso di riportare solo levalutazioni effettuate sull’intera fascia d’età.
BACKGROUND AND AIMSIndividual susceptibility to cancer risk factors may show remark-able differences according to age and gender. Age at first primaryneoplasia (FPN) plays a major role on the risk of a second pri-mary and may reflect different scenarios, depending on individ-ual susceptibility to the cancer risk factors, exposure modalitiesand latency required for tumour development. Moreover, age atFPN and disease stage affect survival, and the probability of asecond primary is strongly related to life expectancy.1
This study presents the estimated excess (or reduced) risk of de-veloping a second primary neoplasm in a large population-based cohort of cancer patients, according to age at first cancerdiagnosis and gender, compared to the expected rate in the gen-eral population of the same age and gender.
MATERIAL AND METHODSThe study cohort was constructed from the databases of the can-cer registries (CRs) belonging to the Italian Association of Can-cer Registries (AIRTUM). All second metachronous primary tu-mours (MP) diagnosed during the activity period of eachcancer registry (range 3-33 years) were considered (see chapter«Materials and methods», pp. 11-17). Therefore, possible un-recorded MPs were excluded from the excess risk measure.Metachronous primary tumours were all primaries registeredat least two months after the date of diagnosis of the FPN. Pa-tients who developed their FPN during childhood or adoles-cence were excluded from this analysis, as the impact of cancertreatment during their growth years might have affected theirsusceptibility to etiological factors as adults, or might itself rep-resent a relevant risk factor for the development of an MP.According to age at FPN diagnosis, patients were split up intothree groups: 20-49 years, 50-69 years and ≥70 years. Thethree age groups were established according to the potential dif-ferent impact of factors/conditions of risk in the different ageclasses and to the natural history of the various cancers. For theyoungest group (20-49 years), due to the potential differenthost-response in the presence of etiological factors, a detailedage-decade group analysis was attempted to highlight the nat-ural history of MPs attributable to inherited predisposition;however, due to the small number of individuals in each sub-group, the risk estimates by site were unstable and did not pro-vide useful information; as a consequence only evaluations per-formed on the whole age group were reported.Excess or reduced risk estimates were calculated by using the Stan-
Rischio di secondo tumore in diversefasce d’etàRisk of second primary cancer in different age groups
133 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
I tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI
Capitolo 9

Le stime di eccesso o difetto di rischio sono state calcolateutilizzando il rapporto standardizzato di incidenza (SIR);questo indicatore è costituito dal rapporto tra il numero de-gli eventi (MP) osservati e di quelli attesi in una data po-polazione. La popolazione è caratterizzata per età (classiquinquennali), sesso e sede della FPN, quindi ogni quan-tificazione di eccesso o difetto di rischio è relativa alle suecaratteristiche specifiche. Sono pertanto validi confronti in-terni al singolo strato e non fra differenti strati che sono ca-ratterizzati da diversa popolazione di origine dei casi diFPN. Il SIR è statisticamente significativo (p <0,05)quando i limiti di confidenza non includono l’unità. Nelcaso di associazione positiva sono state considerate solo leassociazioni basate su un numero complessivo dei MP os-servati ≥5, mentre per le associazioni negative sono staticonsiderati tutti i SIR statisticamente significativi, indipen-dentemente dal numero di MP osservati.Le associazioni significative fra MP e FPN sono state pre-sentate sinteticamente in modo qualitativo (sede degli MPassociata alla FPN) per le tre fasce di età in tre doppie tabelle(tabelle a1, a2, b1, b2, c1 e c2, pp. 137-142), mentre i re-lativi SIR (e intervalli di confidenza) sono disponibili nelmateriale on-line (tabella e3). Per ogni neoplasia sono statiriportati gli MP associati positivamente (eccesso di rischio)o negativamente (difetto di rischio) con la FPN. L’eccessodi rischio di MP per ogni strato (età e sesso) è stato anchevalutato tenendo conto della durata del follow-up: <5 anni(in verde scuro nelle tabelle) e ≥5 anni (in verde chiaro nelletabelle) dalla diagnosi di FPN. Inoltre, in verde intermediosono indicate le associazioni con SIR significativi sia entrosia dopo i 5 anni dalla diagnosi di FPN.In base ai dati di letteratura sono state prese in considera-zione “famiglie” di fattori che possono accomunare FPN eMP: trattamento della prima neoplasia, possibile compo-nente genetica o familiare, dieta, componente ormonale,abitudini voluttuarie (fumo e alcol), esposizione lavorativaed esposizione ad agenti infettivi.1 Nelle tabelle a, b e c leassociazioni osservate tra FPN e MP sono state riportate percolonna in relazione al probabile (o possibile) fattore che leaccomuna. Sono state riunite in un unico insieme le asso-ciazioni tra neoplasie che condividevano fattori di rischiocollocati in colonne vicine, mentre sono state indicate conun asterisco le associazioni che potevano fare riferimento apiù fattori di rischio non presenti in colonne contigue. I MPsospettati di essere mediati dal meccanismo dell’immunu-soppressione (come il tumore di Kaposi) sono stati identi-ficati con un apposito simbolo (§). Sono stati trattati sepa-ratamente i MP in eccesso per i quali, in base alleconoscenze attuali, non è ipotizzabile una relazione con laFPN, e i MP per cui è stato segnalato il ruolo potenzialedella sovradiagnosi (diagnosi occasionale nel corso del fol-low-up clinico di FPN di tumori asintomatici che si sareb-bero manifestati clinicamente durante la vita del paziente).
dardized Incidence Ratio (SIR); this indicator was computed asthe ratio between the observed and expected number of events(MPs) in a defined population: this population was characterizedby age (5-year age groups), gender and site of FPN, therefore theexcess or reduction of risk is related to its specific characteristics.Only comparisons inside the single stratum are valid, because dif-ferent strata are characterized by a different population expressingthe cases of FPN.The SIR was statistically significant (p <0.05)when the 95% confidence interval (95%CI) did not include 1.0.Statistically significant increased SIRs were based on an observednumber of events ≥5; for negative associations (SIR <1.0) all sta-tistically significant SIRs were included.The statistically significant associations between FPN and MPare outlined by means of a qualitative representation model (MPsites associated to each considered FPN) by age strata (tables a1,a2, b1, b2, c1 and c2; pp. 137-142); the corresponding SIRsare available online (table e3). For each FPN site excess and re-duction of risk of MPs were reported. Furthermore, the excess orreduced MP was estimated by gender in each age group, accord-ing to the length of follow-up after the FPN: <5 years (in darkgreen in the tables) and ≥5 years (in light green in the tables)from diagnosis of the FPN. In addition, associations with sta-tistically significant SIRs both within and after 5 years from theFPN diagnosis are in intermediate green.According to the literature, groups of risk factors shared by FPNand MP were considered, namely: sequelae of cytotoxic treatmentsfor FPN, genetic or familial background, diet, hormonal envi-ronment, lifestyle habits (tobacco smoking and alcohol drinking),work-related exposure and viral infections.1
Tables a, b and c present the observed associations betweenFPN and MP in columns according to the probable or (poten-tial) common risk factors. Risk factors shared by FPN and MPwere arranged in a single box when located in close columnsor indicated by an asterisk when located in non contiguouscolumns. MPs potentially attributable to an immunologicdeficit (e.g., Kaposi sarcoma) were labelled with §. MPs forwhich a relationship could not be demonstrated were consid-ered separately, as well as MPs for which overdiagnosis cannotbe ruled out.
RESULTSTable 1 shows the excess risk of developing MPs in patients withFPN, according to age decades and gender: it can be observedthat the excess risk of developing MPs was high in the youngestage group for both sexes and tended to decrease in older groups.Tables a, b and c show all observed statistically significant excessor reduction of MP risk for each considered FPN, accordingto conditions potentially shared between them. The data werereported according to age at first cancer diagnosis, gender andlatency of the MP.The following paragraphs outline a number of associations be-tween FPN and MP, which may be of interest for the clinicalmanagement of cancer patients: genetic susceptibility, lifestyle
Rischio di secondo tumore in diverse fasce d’etàI tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI
134 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152

RISULTATIIn tabella 1 sono riportati, per decade di età e sesso, gli ec-cessi di rischio di sviluppare un MP in pazienti con una dia-gnosi di cancro: nella tabella si osserva che per entrambi isessi l’eccesso di rischio di sviluppare un MP è molto elevatonei substrati della fascia d’età più giovane (20-49 anni) e di-minuisce negli strati di età più anziani.Nelle tabelle a, b e c sono riportate le associazioni significative(eccesso o difetto di rischio di MP per le singole sedi di FPN)e le possibili condizioni che possono accomunare FPN e MPnelle diverse fasce d’età in cui è stata diagnosticata la FPN, persesso e in relazione alla latenza tra i due tumori. Per brevità, diseguito vengono riportate nel dettaglio associazioni tra FPN eMP che possono avere un ruolo nella gestione clinica del pa-ziente con tumore (effetti del trattamento della FPN, predispo-sizione genetica, stili di vita, possibile risultato di sovradiagnosi);per le associazioni restanti si rimanda alle tabelle e4 on-line.
Effetti del trattamento della FPNLe donne trattate per tumore della mammella nelle fasced’età 20-49 e 50-69 anni mostrano, sia complessivamente siaper periodi di latenza, un eccesso di rischio statisticamente si-gnificativo di sviluppare tumore dell’esofago (SIR: 3,02:IC95% 1,56-5,28 e SIR: 1,62; IC95% 1,18-2,17 rispettiva-mente) e del polmone (SIR: 1,60; IC95% 1,32-1,93 e SIR:1,18; IC95% 1,08-1,29 rispettivamente). Nelle due fasced’età si riscontra anche un eccesso di leucemie mieloidi (SIR:3,00; IC95%2,16-4,08 e SIR: 1,81; IC95%1,50-2,17 rispet-tivamente). Le pazienti con carcinoma mammario mostranoanche un eccesso di rischio di tumore dell’endometrio nelletre fasce d’età (SIR: 1,88; IC95% 1,61-2,19 – SIR: 1,92;IC95% 1,78-2,07 – SIR: 2.08; IC95% 1,86-2,31).Per le donne trattate per linfoma diHodgkin, nella fascia d’età20-49 anni si osserva un eccesso di rischio di carcinomamammario che si manifesta a partire dal quinto anno dalladiagnosi della FPN (SIR: 2,56; IC95% 1,78-3,54).Infine, un eccesso di rischio di leucemia mieloide ricorrenella fascia di età 20-49 anni in entrambi i sessi per i tumoridella tiroide (SIR: 5,83; IC95% 1,59-14,92 e SIR: 5,07;IC95% 2,53-9,08 in uomini e donne rispettivamente), negliuomini con tumori delle vie aerodigestive superiori e del te-sticolo (SIR: 4,04; IC95% 1,48-8,80 e SIR: 3,53; IC95%1,14-8,23 rispettivamente).Nella fascia d’età 50-69 anni le leucemie mieloidi si associano
habits, late effects of FPN treatment, and possible overdiagnosisof MPs. Detailed information on the remaining associationscan be found in supplementary online tables e4.
Late effects of FPN treatmentsWomenwith breast cancer diagnosed in the 20-49 and 50-69-yearage groups showed a statistically significant excess risk, both globallyand by latency period, for oesophageal cancer (SIR: 3.02; 95%CI1.56-5.28 and SIR: 1.62; 95%CI 1.18-2.17, respectively) andlung (SIR: 1.60; 95%CI1.32-1.93 and SIR: 1.18; 95%CI 1.08-1.29, respectively). In both age groups, an excess of myeloidleukaemia was also observed (SIR: 3.00; 95%CI 2.16-4.08 andSIR: 1.81; 95%CI 1.50-2.17, respectively). Patients with breastcancer also showed an overlapping excess risk of endometrial cancerin the three age groups (SIR: 1.88; 95%CI 1.61-2.19 – SIR: 1.92;95%CI 1.78-2.07 – SIR: 2.08; 95%CI 1.86-2.31).Women treated because of Hodgkin’s disease when aged 20-49showed an excess risk of breast cancer after 5 years from FPN di-agnosis (SIR: 2.56; 95%CI 1.78-3.54).Finally, an excess risk of myeloid leukaemia was observed in the20-49 age group in both sexes in individuals treated for thyroidcancer (SIR: 5.83; 95%CI 1.59-14.92 – SIR: 5.07; 95%CI2.53-9.08 in men and women, respectively), and for upperaerodigestive tract cancers and testicular cancer inmen (SIR: 4.04;95%CI 1.48-8.80 and SIR: 3.53, 95%CI 1.14-8.23, respec-tively). In men in the 50-69 years age range, myeloid leukaemiawas associated to upper aerodigestive tract cancer (SIR: 1.86;95%CI 1.31-2.56), stomach cancer (SIR: 1.94; 95%CI 1.19-3.00), and lung cancer (SIR: 1.60; 95%CI 1.05-2.33).
Genetic susceptibilityIn the 20-49 years age group, a high excess risk of MPs for se-lected FPNs was recorded. Individuals with colorectal cancershowed an excess of extracolonic MPs. High excess of urinarytract cancer (SIR: 11.89; 95%CI 5.13-23.42) and stomachcancer (SIR: 2.40; 95%CI 1.57-3.51) were observed forboth sexes combined; women showed a higher excess risk of en-dometrial (SIR: 4.25; 95%CI 3.02-5.81) and ovarian cancer(SIR: 3.21; 95%CI 1.99-4.90). Similarly, women affected byendometrial cancer showed an elevated SIR for colon cancer(SIR: 5.05; 95%CI 3.68-6.75).Women with breast cancer diagnosed when aged 20-49 yearshad a statistically significant excess risk of ovarian cancerwith overlapping SIRs within 5 years after the diagnosis of the
Rischio di secondo tumore in diverse fasce d’etàI tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI
135 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
AGE CLASS MEN WOMEN
YEARS OBSERVED EXPECTED SIR (95%CI) OBSERVED EXPECTED SIR (95%CI)
20-29 97 37.12 2.61 (2.12-3.19) 133 65.58 2.03 (1.70-2.40)30-39 318 175.20 1.82 (1.62-2.03) 671 419.47 1.60 (1.48-1.73)40-49 1 685 999.13 1.69 (1.61-1.77) 2 585 1 865.93 1.39 (1.33-1.44)20-49 2 100 1 211.45 1.73 (1.66-1.81) 3 389 2 350.98 1.44 (1.39-1.49)50-69 26 822 23 001.20 1.17 (1.15-1.18) 14 956 12 460.34 1.20 (1.18-1.22)70+ 24 319 26 038.68 0.93 (0.92-0.95) 11 880 12 730.53 0.93 (0.92-0.95)
Tabella 1. Rischio di secondi tumoridi tutte le sedi (escluso tumore dellacute e stessa sede) in relazione all’etàalla diagnosi del primo.Table 1. Risk of second primary in allsites (except for non-melanoma skincancer and same site) according toage at first primary diagnosis.

Epidemiol Prev 37 (4-5) Suppl 1:1-152 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.it136
I tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI Rischio di secondo tumore in diverse fasce d’età
FPN (SIR: 2.50; 95%CI 1.94-3.17) and later in the follow-up (SIR: 2.86; 95%CI 2.34-3.47). A statistically significantexcess of ovarian cancer was also observed among women aged50-69 for breast cancer, both within 5 years after diagnosis(SIR: 1.39; 95%CI 1.18-1.62) and after 5 years (SIR: 1.47;95%CI 1.24-1.72).Conversely, women who had an ovarian FPN at a young age(20-49 years) had an excess risk of colorectal cancer (SIR: 6.87;95%CI 4.31-10.41) and endometrial cancer (SIR: 5.09;95%CI 2.44-9.37) within 5 years from the FPN; after 5 yearsof follow up the excess of colorectal cancer persisted (SIR:3.58; 95%CI 2.24-5.42) and an excess of breast cancer (SIR:1.51; 95%CI 1.06-2.08) was also observed.Women who hadhad an ovarian cancer when aged 50-69 showed an excess ofcolorectal cancer within 5 years after diagnosis (SIR: 1.78;95%CI 1.34-2.33) and an excess of breast cancer with similarSIRs within 5 years after diagnosis (SIR: 1.33; 95%CI 1.08-1.62) and after (SIR: 1.44; 95%CI 1.11-1.84).
Lifestyle and occupational exposureTables a, b and c show for each age-group (and gender) associationsbetween cancer that share dietary habits (e.g., colorectal, breast,and endometrial cancers), alcohol and smoking consumption(e.g., upper aerodigestive tract, lung, pancreatic, and urinarytract cancers), occupational exposure (lung, upper aerodigestivetract, and urinary tract cancers). Relevant tables can be found inthe online tables e4. Remarkably, patients who developed anupper aerodigestive tract cancer before the age of 50 showed an ex-cess risk of a second upper aerodigestive tract cancer that is eight-fold the expected (SIR: 8.06; 95%CI 6.52-9.85). In the 50-69and ≥70 age groups the observed SIRs were 3.45 (95%CI 3.12-3.80) and 1.82 (95%CI 1.42-2.31), respectively. In all agegroups the excess risk was greater in women than in men.
Potential effect of over- and underdiagnosisIn tables a, b and c (last column to the right), an excess risk ofthyroid, kidney, prostate tumours and cutaneous melanoma wasobserved for several FPNs that cannot be attributable to sharedrisk factors.The data is remarkable in the 20-49 and 50-69 agegroups. Conversely, for the 50-69 and ≥70 years age groups alower number of MPs was observed for several FPNs.
DISCUSSIONConditions that contribute to the development of MPs, i.e., latesequelae of cytotoxic treatments, genetic susceptibility due to ger-minal mutations in major genes (e.g., BRCA, MMR), lifestylehabits, environmental determinants, or combination of these de-terminants (gene-environment interaction), as well as the resultsof a clinical and instrumental follow-up carried out with the aimof detecting disease progression as early as possible, may play a dif-ferent role on the incidence of MPs according to age at diagnosis.The risk reduction of developing the MPs observed in theolder age groups (table 1) could be partly explained by the excess
negli uomini con i tumori delle vie aerodigestive superiori(SIR: 1,86; IC95% 1,31-2,56), dello stomaco (SIR: 1,94;IC95% 1,19-3,00) e del polmone (SIR: 1,60; IC95% 1,05-2,33).
Predisposizione geneticaPer sedi selezionate, nella fascia d’età 20-49 anni si riscon-trano eccessi di rischio elevati di numerosi MP. Soggetti conun primo tumore in sede colorettale mostrano un eccesso dirischio (di entità sovrapponibile nei due sessi) di tumoridelle vie urinarie (SIR: 11,89; IC95% 5,13-23,42) e dellostomaco (SIR: 2,40; IC95% 1,57-3,51), mentre per le donnesi osserva anche un eccesso di rischio di tumore dell’endome-trio (SIR: 4,25; IC95% 3,02-5,81) e delle ovaie (SIR: 3,21;IC95% 1,99-4,90). In modo analogo, le donne con tumoredell’endometrio mostrano SIR elevati per tumore del colon(SIR: 5,05; IC95% 3,68-6,75).Le donne con tumore mammario diagnosticato nella fasciad’età 20-49 anni manifestano un eccesso di rischio di carci-noma dell’ovaio di entità pressoché sovrapponibile entro i 5anni dalla diagnosi della FPN (SIR: 2,50; IC95% 1,94-3,17) e dopo i 5 anni (SIR: 2,86; IC95% 2,34-3,47).Un eccesso statisticamente significativo di MP ovarico si os-serva anche nella fascia di età 50-69 anni, sia nei primi 5 annidalla diagnosi (SIR: 1,39; IC95% 1,18-1,62), sia dopo i 5anni (SIR: 1,47; IC95% 1,24-1,72).Una situazione peculiare si rileva per le donne che hannoavuto una FPN in sede ovarica: quando la diagnosi sia statafatta nella fascia d’età 20-49, entro i 5 anni dalla diagnosi dellaFPN si osserva un eccesso di rischio di carcinoma del colonretto (SIR: 6,87; IC95%4,31-10,41) e dell’endometrio (SIR:5,09; IC95% 2,44-9,37); nel periodo successivo persiste l’ec-cesso di tumore colorettale (SIR: 3,58; IC95%2,24-5,42) e siriscontra un eccesso di tumoremammario (SIR: 1,51; IC95%1,06-2,08). Donne con diagnosi di tumore ovarico in età 50-69 anni mostrano un eccesso di cancro colorettale limitato aiprimi 5 anni dalla diagnosi di FPN (SIR: 1,78; IC95% 1,34-2,33) e di carcinomamammario con valori sovrapponibili en-tro i 5 anni dalla diagnosi (SIR: 1,33; IC95%1,08-1,62) e nelperiodo successivo (SIR:1,44; IC95% 1,11-1,84).
Stili di vita ed esposizione lavorativaLe tabelle a, b e c mostrano nelle tre fasce d’età associazionitra tumori che condividono abitudini dietetiche (per esem-pio, colon retto, mammella, endometrio), esposizione all’alcole al fumo di tabacco (tumori delle vie aerodigestive superiori,del polmone, del pancreas e dell’apparato urinario) o espo-sizione lavorativa (tumori del polmone, delle vie aerodigestivesuperiori e dell’apparato urinario). I dati sono disponibilinelle tabelle e4 on-line. E’ da sottolineare che pazienti chehanno sviluppato un tumore del distretto delle vie aerodige-stive superiori prima dei 50 anni hanno un eccesso di rischiodi sviluppare un MP dello stesso distretto pari a circa 8 volte

INCREASED RISKDECREASED RISK
137�
Ulterio
ridatid
ispo
nib
ilisulsito
:w
ww
.registri-tu
mo
ri.itEp
idem
iolPrev
37(4-5)
Sup
pl1:1-152
UNKNOWN MISCLASSIFICATION TREATMENT/ RISK FACTORS TREATMENT GENETICS / DIET / ORMONAL/ SMOKE / ALCOHOL / INFECTIOUS UNKNOWN OVERDIAGNOSIS(METASTASIS, ETC) UNDERDIAGNOSIS FAMILIAL SEDENTARINESS OCCUPATION
20-49 years
TABLE A1:Patients 20-49 years old at first cancer diagnosis, men. Sites of second cancers
with statistically significant association (p <0.05), follow-up period(see legend) and risk factors.
TABELLA A1:Pazienti in età 20-49 anni all’insorgenza del primo tumore, uomini.
Sede di secondo tumore con associazione statisticamente significativa (p <0,05)per tempo di follow-up (vedi legenda) e fattori di rischio.
prostate UADT ML UADT UADT others thyroid(oral cavity, pharynx, (oral cavity, pharynx,oesophagus) oesophagus)
lungcolon / bladder / liver
STOMACH colon NHLlung
COLON RECTUM kidney bladder/ lung bladder / lungpancreas / urinay tract pancreas / urinay tract pancreas / urinay tract
stomachPANCREASLUNG rectum / pancreas/ UADT
kidney / bladder
UADTMELANOMA bladder thyroidTESTIS thyroidPROSTATEBLADDER & prostate* prostate* lung stomach kidney
URINARY TRACT prostate*KIDNEY & bladder* bladder* bladder* others prostate*RENAL PELVIS colon-rectum/ prostate* colon-rectum/ prostate*THYROID kidneyHD lung / NHL KS § stomach melanoma
oesophagusNHL ML kidney* kidney* bladder/ HD kidney*CML oral cavity thyroidALL
LEGEND* more risk factors involved
§ immunosuppression
ML myeloid leukaemia
HD Hodgkin’s disease
NHL Non-Hodgkin lymphoma
KS Kaposis sarcoma
CML chronic myeloyd leukaemia
CLL chronic lymphoid leukaemia
p<0.05 in follow-up period 0-59 months
p<0.05 in follow-up period 60+ months
p<0.05 in both follow-up periods
FIRST CANCER DIAGNOSIS
PATIENTS 20-49 YEARSMEN

TABLE A2:Patients 20-49 years old at first cancer diagnosis, women. Sites of second cancers
with statistically significant association (p <0.05), follow-up period(see legend) and risk factors.
TABELLA A2:Pazienti in età 20-49 anni all’insorgenza del primo tumore, donne.
Sede di secondo tumore con associazione statisticamente significativa (p <0,05)per tempo di follow-up (vedi legenda) e fattori di rischio.
FIRST CANCER DIAGNOSIS
PATIENTS 20-49 YEARSWOMEN
INCREASED RISKDECREASED RISK
UNKNOWN MISCLASSIFICATION TREATMENT/ RISK FACTORS TREATMENT GENETICS / DIET / ORMONAL/ SMOKE / ALCOHOL / INFECTIOUS UNKNOWN OVERDIAGNOSIS(METASTASIS, ETC) UNDERDIAGNOSIS FAMILIAL SEDENTARINESS OCCUPATION
20-49 years
UADT UADT UADT(oral cavity, pharynx, (oral cavity, pharynx,
oesophagus) oesophagus)lung / breast
STOMACH colon*/ ovary colon*COLON RECTUM ovary / SNC lung myeloma thyroid
bladder/ urinary tract othersuterus corpus
PANCREAS ovary ovaryLUNG others
MELANOMA breast kidneyHD BREAST ML, lung* melanoma colon stomach/ oesophagus* liver / others kidney
oesophagus* pancreasuterus corpus/ ovary lung* soft tissues
UTERUS CERVIX lung / bladder* HDUADT / rectum
UTERUS CORPUS leukaemia colon ovary SNC thyroidOVARY rectum/ uterus corpus rectum/ uterus corpus others
colon breastBLADDER & lung
URINARY TRACTKIDNEY & thyroidRENAL PELVISTHYROID ML HD breast/ ovaryHD UADT (pharynx)* UADT (pharynx)* UADT (pharynx)* melanoma
lung/ breast/ NHL KS §ML
NHL lung* lung*CML colonALL
138�
Ulterio
ridatid
ispo
nib
ilisulsito
:w
ww
.registri-tu
mo
ri.itEp
idem
iolPrev
37(4-5)
Sup
pl1:1-152
LEGEND* more risk factors involved
§ immunosuppression
ML myeloid leukaemia
HD Hodgkin’s disease
NHL Non-Hodgkin lymphoma
KS Kaposis sarcoma
CML chronic myeloyd leukaemia
CLL chronic lymphoid leukaemia
p<0.05 in follow-up period 0-59 months
p<0.05 in follow-up period 60+ months
p<0.05 in both follow-up periods

INCREASEDRISK
DECREASEDRISK
139 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
UNKNOWN
MISCLASSIFICATION
TREATM
ENT/
RISK
FACTORS
TREATM
ENT
GENETICS/
DIET/O
RMONAL/
SMOKE/ALCOHOL/
INFECTIOUS
UNKNOWN
OVERDIAGNOSIS
(METASTASIS,ETC)
UNDERDIAGNOSIS
FAMILIAL
SEDENTARINESS
OCCUPATION
50-69years
TABLEB1:
Patients5
0-69
yearso
ldat
firstcancerdiagnosis,m
en.Siteso
fsecondcancers
with
statisticallysig
nificanta
ssociatio
n(p
<0.05),follow-upperio
d(see
legend)and
riskfactors.
TABELLAB1:
Pazientiinetà50-69anniall’insorgenzadelprim
otumore,uomini.
Sede
disecondotumoreconassociazione
statisticam
entesig
nificativa(p
<0,05)
pertem
podifollow-up(vedilegenda)e
fatto
ridirischio.
prostate
UADT
ML
UADT
UADT
thyroid
myeloma/melanoma
(oralcavity,pharynx,(oralcavity,pharynx,
oesophagus)
oesophagus)
lung/stomach/liver/
NHL
bladder
others
STOMACH
ML
colon*
oesophagus/
pancreas
oesophagus
pancreas*
colon/bladder
UADT/others
pancreas/lung
COLONRECTUM
melanoma
kidney
thyroid
PANCREAS
lung
prostate
LUNG
ML
UADT
liver/KS
kidney
(oralcavity,pharynx,
oesophagus)/
colon/bladder
stomach
pancreas
UADT/bladder
MELANOMA
prostate
thyroid/kidney
oesophagus
TESTIS
NHL
gallbladder&B.T./
liver
PROSTATE
thyroid
colon-rectum/
colon-rectum/
UADT
mesothelioma
stomach/myeloma
urinarytract
urinarytract
(oralcavity)/bladder
softtissue
LLmelanoma
kidney
others/lung
BLADDER&
urinarytract
kidney
UADT(oralcavity,
softtissues
URINARYTRACT
pharynx)/lung
colon-rectum
others
liver
KIDNEY&
thyroid/leukaemia
colon
prostate
lung
RENALPELVIS
NHL
melanoma/bladder/
melanoma/bladder/
urinarytract
urinarytract
THYROID
kidney
colon
HD
lung/NHL
NHL
ML
kidney*
bladder
KS§
kidney*
lungliver
HD
prostate
MYELOMA
liver
CLL
lung*
kidney*
kidney*
lung*
HD*
mesothelioma
kidney*
KS§
melanoma
CML
KS§
prostate
AML
kidney*
kidney*
kidney*
FIRSTCA
NCERDIAGNOSIS
PATIENTS
50-69YEARS
MEN
LEGEND
*m
ore
risk
fact
orsi
nvol
ved
§im
mun
osup
pres
sion
ML
mye
loid
leuk
aem
ia
HD
Hodg
kin’
sdise
ase
NHL
Non
-Hod
gkin
lymph
oma
KSKa
posis
sarc
oma
CML
chro
nic
mye
loyd
leuk
aem
ia
CLL
chro
nic
lymph
oid
leuk
aem
ia
p<0.05infollow-upperiod0-59months
p<0.05infollow-upperiod60+months
p<0.05inbothfollow-upperiods

INCREASEDRISK
DECREASEDRISK
140 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
UNKNOWN
MISCLASSIFICATION
TREATM
ENT/
RISK
FACTORS
TREATM
ENT
GENETICS/
DIET/O
RMONAL/
SMOKE/ALCOHOL/
INFECTIOUS
UNKNOWN
OVERDIAGNOSIS
(METASTASIS,ETC)
UNDERDIAGNOSIS
FAMILIAL
SEDENTARINESS
OCCUPATION
50-69years
TABLEB2:
Patients5
0-69
yearso
ldat
firstcancerdiagnosis,w
omen.Siteso
fsecondcancers
with
statisticallysig
nificanta
ssociatio
n(p<0.05),follow-upperio
d(see
legend)and
riskfactors.
TABELLAB2:
Pazientiinetà50-69anniall’insorgenzadelprim
otumore,donne.
Sede
disecondotumoreconassociazione
statisticam
entesig
nificativa(p
<0,05)
pertem
podifollow-up(vedilegenda)e
fatto
ridirischio.
UADT
UADT
UADT
thyroid
(oralcavity,pharynx,(oralcavity,pharynx,
oesophagus)
oesophagus)
lung
colon-rectum
uterinecervix
STOMACH
ovary/colon*
bladder
oesophagus/colon
others
COLONRECTUM
uteruscorpus*
uteruscorpus*
lung/bladder
thyroid
breast
kidney
uteruscervix
ovary
PANCREAS
urinarytract
LUNG
UADT
liver
pharynx/colon
pancreas/bladder
MELANOMA
breast
kidney
BREAST
ML
colon
kidney
stomach
liver
thyroid
oesophagus*
ovary
uteruscorpus
oesophagus
kidney
melanoma
NHL
lung/bladder
uteruscorpus/ovary
UTERUSCERVIX
UADT
UADT
others
lung/bladder
pancreas
uteruscervix/ovary
UTERUSCORPUS
ML
colon-rectum/breastcolon-rectum/breast
lung
softtissues
melanoma
kidney
bladder
mesothelioma
uteruscorpus
OVARY
colon-rectum
UADT
breast
(oesophagus)/lung
BLADDER&
breast
breast
lung
softtissue/others
URINARYTRACT
NHL
UADT(pharynx,
oesophagus)
KIDNEY&
thyroid
pancreas
pancreas
lung
softtissues
RENALPELVIS
colon/breast/bladdercolon/breast/bladder
uteruscorpus
THYROID
ovary/breast
lung
kidney
bladder
HD
lung/NHL
kidney
kidney
bladder
ML
NHL
oralcavity*/thyroid
lung*/softtissues/
lung*/softtissues/
bladder*
KS§
kidney*/bladder*
breast
breast
oralcavity*
lung*
HD
ML
kidney*
kidney*
liver
breast
MYELOMA
ML
pancreas
CLL
lung
CML
AML
FIRSTCA
NCERDIAGNOSIS
PATIENTS
50-69YEARS
WOMEN
LEGEND
*m
ore
risk
fact
orsi
nvol
ved
§im
mun
osup
pres
sion
ML
mye
loid
leuk
aem
ia
HD
Hodg
kin’
sdise
ase
NHL
Non
-Hod
gkin
lymph
oma
KSKa
posis
sarc
oma
CML
chro
nic
mye
loyd
leuk
aem
ia
CLL
chro
nic
lymph
oid
leuk
aem
ia
p<0.05infollow-upperiod0-59months
p<0.05infollow-upperiod60+months
p<0.05inbothfollow-upperiods

INCREASEDRISK
DECREASEDRISK
141 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
UNKNOWN
MISCLASSIFICATION
TREATM
ENT/
RISK
FACTORS
TREATM
ENT
GENETICS/
DIET/O
RMONAL/
SMOKE/ALCOHOL/
INFECTIOUS
UNKNOWN
OVERDIAGNOSIS
(METASTASIS,ETC)
UNDERDIAGNOSIS
FAMILIAL
SEDENTARINESS
OCCUPATION
70+years
TABLEC1:
Patients7
0+yearso
ldat
firstcancerdiagnosis,m
en.Siteso
fsecondcancers
with
statisticallysig
nificanta
ssociatio
n(p<0.05),follow-upperio
d(see
legend)and
riskfactors.
TABELLAC1:
Pazientiinetà70+anniall’insorgenzadelprim
otumore,uomini.
Sede
disecondotumoreconassociazione
statisticam
entesig
nificativa(p
<0,05)
pertem
podifollow-up(vedilegenda)e
fatto
ridirischio.
UADT
oralcavity/oesophagusoralcavity/oesophagus
lung/bladder
UADT(pharynx)
UADT(pharynx)
stomach
others
liver
STOMACH
colon/lung
others
stomach/liver/lung/
COLONRECTUM
kidney*
kidney*
kidney*
prostate/SNC/NHL/
gallbladder&B.T./
LLpancreas/
mesothelioma
bladder
lung
PANCREAS
colon/pancreas/
liver/stomach/
LUNG
UADT(oralcavity)
kidney
prostate/myeloma/
mesothelioma
bladder
others
MELANOMA
mesothelioma
kidney
TESTIS
colon
others
lung
PROSTATE
colon
colon
bladder
kidney/melanoma
liver/urinarytract
rectum
rectum
rectum
stomach/SNC/others
BLADDER
ML
prostate
UADT/lung
breast
&URINARYTRACT
pancreas
oesophagus/rectum
lung
KIDNEY&
melanoma/prostate
melanoma/prostate
bladder
RENALPELVIS
THYROID
HD
pancreas
LLmyeloma
NHL
mesothelioma
UADT§/KS§
NHL
MYELOMA
NHL/myeloma
NHL/myeloma
CLL
CML
FIRSTCA
NCERDIAGNOSIS
PATIENTS
70+YEARS
MEN
LEGEND
*m
ore
risk
fact
orsi
nvol
ved
§im
mun
osup
pres
sion
ML
mye
loid
leuk
aem
ia
HD
Hodg
kin’
sdise
ase
NHL
Non
-Hod
gkin
lymph
oma
KSKa
posis
sarc
oma
CML
chro
nic
mye
loyd
leuk
aem
ia
CLL
chro
nic
lymph
oid
leuk
aem
ia
p<0.05infollow-upperiod0-59months
p<0.05infollow-upperiod60+months
p<0.05inbothfollow-upperiods

INCREASEDRISK
DECREASEDRISK
142 � Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
UNKNOWN
MISCLASSIFICATION
TREATM
ENT/
RISK
FACTORS
TREATM
ENT
GENETICS/
DIET/O
RMONAL/
SMOKE/ALCOHOL/
INFECTIOUS
UNKNOWN
OVERDIAGNOSIS
(METASTASIS,ETC)
UNDERDIAGNOSIS
FAMILIAL
SEDENTARINESS
OCCUPATION
70+years
TABLEC2:
Patients7
0+yearso
ldat
firstcancerdiagnosis,w
omen.Siteso
fsecondcancers
with
statisticallysig
nificanta
ssociatio
n(p<0.05),follow-upperio
d(see
legend)and
riskfactors.
TABELLAC2:
Pazientiinetà70+anniall’insorgenzadelprim
otumore,donne.
Sede
disecondotumoreconassociazione
statisticam
entesig
nificativa(p
<0,05)
pertem
podifollow-up(vedilegenda)e
fatto
ridirischio.
UADT
UADT(oralcavity)
UADT(oralcavity)
lung
pharynx/oesophaguspharynx/oesophagus
others
liver
STOMACH
lung/ovary
ovary
liver/
COLONRECTUM
breast/kidney
breast/kidney
lung
kidney*
others
gallbladder&B.T.
myeloma
pancreas
PANCREAS
others
LUNG
colon-rectum
bladder
rectum
MELANOMA
lung
kidney
ovary/NHL
liver/lung
BREAST
ML
thyroid
others
gallbladder&B.T./SNC
uteruscorpus
uteruscorpus
melanoma
UTERUSCERVIX
melanoma
others
ovary
UTERUSCORPUS
breast
lung
OVARY
BLADDER
lung
breast
thyroid
&URINARYTRACT
uteruscervix
KIDNEY
breast
breast
pancreas/NHL
&RENALPELVIS
bladder
THYROID
pancreas
pancreas
NHL
myeloma
HD
NHL
uteruscorpus
LLLL
NHL
liver
KS§
colon
MYELOMA
ovary
kidney
rectum
uteruscorpus
CLL
bladder
CML
FIRSTCA
NCERDIAGNOSIS
PATIENTS
70+YEARS
WOMEN
LEGEND
*m
ore
risk
fact
orsi
nvol
ved
§im
mun
osup
pres
sion
ML
mye
loid
leuk
aem
ia
HD
Hodg
kin’
sdise
ase
NHL
Non
-Hod
gkin
lymph
oma
KSKa
posis
sarc
oma
CML
chro
nic
mye
loyd
leuk
aem
ia
CLL
chro
nic
lymph
oid
leuk
aem
ia
p<0.05infollow-upperiod0-59months
p<0.05infollow-upperiod60+months
p<0.05inbothfollow-upperiods

Epidemiol Prev 37 (4-5) Suppl 1:1-152 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.it143
I tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI Rischio di secondo tumore in diverse fasce d’età
of mortality that occurs in these groups compared to the youngage groups (i.e., <50 years). It could be selectively stronger forsubjects with a higher risk of MP by reducing in these age classesthe probability of an MP surfacing a few years after FPN di-agnosis. Moreover, this reduction could be explained by under-diagnosis due to two main conditions:A. among the elderly, FPNs are frequently diagnosed at amore advanced stage compared to younger individuals;B. severe comorbidity and reduced life expectancy may con-traindicate invasive diagnostic procedures to evaluate signs orsymptoms of other cancers or other diseases in general.Of great importance are MPs that can be considered as late se-quelae of cytotoxic treatments of the FPN (bone marrow tox-icity or immunosuppression). In these circumstances the latencyof the MP may depend on the total dose of radiation and/orchemotherapy, the route of administration and the sensitivityof the target tissues: usually latency is shorter for leukaemiathan for lymphomas, thyroid, central nervous system, and ep-ithelial cancers. Immunodeficiency can also be induced by in-fective agents and, among the elderly, be the result of a normaldecline in immunologic function.1
The MP risk seems to be particularly relevant after treatmentfor breast cancer2 and for Hodgkin lymphoma.3 Nevertheless,it should be stressed that this study cohort includes patients re-cruited over a 30-year period (from the late Seventies to recentyears); during this span a substantial improvement has oc-curred in radiation therapy procedures, for instance, radiationtreatment for early breast cancer shifted from thoracic irradi-ation to intraoperative radiation therapy.The excess of oesophageal and lung cancers observed in patientswith breast cancer diagnosed in youth and middle age is in agree-ment with the results of studies carried out in cohorts of breastcancer patients who had thoracic irradiation as adjuvant therapy,and most of them were likely a sequela of this therapy.3-5 In thisstudy, an excess of myeloid leukaemia was observed in womenwith breast cancer diagnosed at a young age (20-49 years): it canprobably be ascribed to cytotoxic agents, e.g., alkylating agents,antimetabolites, and anthracyclines which in the past decadeswere administered at high cumulative doses even as adjuvanttreatment3,6,7 and, more recently, to the use of the bone marrowgrowth factor (G-CSF).8 However, it must be considered thatdata from the literature usually refer to acute myeloid leukaemiawhile, in the present study, myeloid leukaemias were treated asa whole; as a consequence, the observed excess risk could havebeen diluted. The observed excess of endometrial cancer after aprimary breast cancer must be largely attributed to the prolongeduse of the antiestrogen tamoxifen.9,10
Women treated for Hodgkin lymphoma at age 20-49 had anexcess of breast cancer 5 years or more after FPN diagnosis. Theobserved result is, in all likelihood, mostly due to the chest ir-radiation of cases with supradiaphragmatic disease. In thisstudy, the patients with supradiaphragmatic disease could notbe identified and, once again, it is possible that the result shown
l’atteso (SIR: 8,06; IC95% 6,52-9,85); nelle due successivefasce d’età il SIR scende rispettivamente a 3,45 (IC95%3,12-3,80) e 1,82 (IC95% 1,42-2,31). In tutte le fasce di etàl’eccesso di rischio è molto più elevato nelle donne che negliuomini.
Sovradiagnosi e sottodiagnosi potenzialiNell’ultima colonna a destra delle tabelle a, b e c per numerosesedi di FPN si osserva un eccesso di tumori della tiroide, delrene, della prostata e dimelanoma cutaneo non attribuibili allacondivisione di alcuno dei fattori eziologici considerati. Il ri-sultato è particolarmente evidente nelle fasce d’età 20-49 annie 50-69 anni. Per contro, nelle stesse tabelle si rilevano nume-rose sedi di FPN per le quali è stato stimato un difetto di MPrispetto all’atteso, praticamente solo per le fasce d’età 50-69 e≥70 anni.
DISCUSSIONEI possibili determinanti dello sviluppo di un MP, ossia effettodei trattamenti per FPN, predisposizione genetica per pre-senza di mutazione germinale in un gene maggiore (peresempio geni BRCA, MMR), stili di vita, esposizioni am-bientali, o loro combinazioni (interazione gene-ambiente), ef-fetto del follow-up condotto con lo scopo primario di anti-cipare la diagnosi di una possibile recidiva/progressione dimalattia possono avere un impatto molto diverso sull’inci-denza di MP in relazione al tipo di neoplasia e all’età allaquale è stata diagnosticata e trattata.In relazione al difetto di rischio di sviluppare un MP osser-vato nei gruppi di età più anziani (tabella 1) va consideratoche l’effetto di eccesso di mortalità rispetto alle classi di etàpiù giovani può essere selettivamente più forte nei soggetti amaggior rischio di MP, riducendo così in queste fasce d’etàla probabilità di un MP a pochi anni dall’occorrenza dellaFPN. Ciò può essere in parte spiegato con fenomeni di sot-todiagnosi correlati a due fattori:A. la prima neoplasia viene frequentemente diagnosticata instadio più avanzato rispetto a quanto si osserva nelle fasced’età giovani;B. sono spesso presenti comorbidità anche gravi che condi-zionano l’attesa di vita e controindicano l’approfondimentodiagnostico di eventuali segni/sintomi di altre malattie, nonnecessariamente solo neoplastiche.Di interesse rilevante sono i MP che risultano probabili se-quele di terapie di FPN: per esempio, terapia radiante e/omedica con effetti mielotossici o immunosoppressivi, doveil tempo di latenza del MP dipende da dose e via/campo disomministrazione del trattamento e dalla sensibilità deltessuto coinvolto (spesso il sistema emolinfopoietico), contempi di latenza minori per le leucemie rispetto ai tumoridella serie linfatica, della tiroide, del sistema nervoso cen-trale e, in ultimo, dei tumori di origine epiteliale. In parti-colare, gli effetti dell’immunosoppressione possono derivare

non solo dal trattamento della FPN, ma anche dall’azionedi agenti infettivi comuni o non comuni alla FPN e al MPe, negli anziani, da un deficit fisiologico dell’immunità.1 Ilrischio di MP associato al trattamento è risultato più rile-vante in presenza di FPN quali il tumore mammario2 e illinfoma di Hodgkin3. Occorre tuttavia sottolineare che lacoorte in esame copre un periodo di tempo di oltre 30 anniper cui nello stesso gruppo d’età sono compresi casi trattatidalla fine degli anni Settanta fino ad anni recenti; nel corsodi quest’arco di tempo il trattamento radioterapico ha su-bito un’evoluzione radicale fino a giungere di recente, peril tumore mammario, all’impiego della radioterapia in-traoperatoria nei casi in stadio precoce.L’eccesso di tumore del polmone e dell’esofago osservato nellepazienti con diagnosi di tumore mammario è coerente con irisultati di studi condotti su coorti di pazienti con carcinomamammario sottoposte a radioterapia.3-5 L’eccesso di leucemiemieloidi osservato nelle donne trattate per carcinomamamma-rio in giovane età (20-49 anni) è probabilmente da ascrivereall’impiego di farmaci chemioterapici (alchilanti, antimetabo-liti, antibiotici quali i derivati dell’adriamicina) impiegati so-prattutto negli anni Ottanta e Novanta a dosi cumulative im-portanti anche in fase adiuvante3,6,7 e, più recentemente, all’usodei fattori di crescitamidollari (G-CSF).8 Occorre, tuttavia, sot-tolineare che i dati in letteratura indicano un eccesso di leuce-mie acute, mentre nel presente studio le forme acuta e cronicasono state trattate come un’entità unica, quindi il rischio os-servato potrebbe risultare diluito. L’eccesso osservato di tumoredell’endometrio dopo tumore mammario è da attribuire ingran parte alla terapia prolungata con tamoxifene.9,10
Nelle donne giovani (20-49 anni) trattate per linfoma diHodgkin si è osservato un eccesso di carcinoma mammariorispetto all’atteso a partire dal quinto anno dopo la diagnosi.Probabilmente il risultato ottenuto è per lo più da ascrivereai casi con localizzazione sovradiaframmatica della neoplasia,che hanno subito trattamento radiante sulla zona toracica, manella casistica qui presentata non è stato possibile effettuarevalutazioni in relazione alle localizzazioni del linfoma diHodgkin. Questa informazione è tuttavia molto rilevante perla sorveglianza clinica nelle giovani donne considerate guarite,per quanto riguarda la FPN, in quanto hanno una probabilitàpiù elevata di sviluppare tumore mammario con caratteristi-che prognostiche sfavorevoli (ER-, Pgr-, G3).11-13
Nelle donne più giovani si osservano eccessi di rischio incro-ciati fra sedi (FPN in sede colorettale con MP endometrialiod ovarici e viceversa): buona parte dei casi osservati possonoessere dovuti a predisposizione genetica, in quanto questeneoplasie rientrano nello spettro della sindrome di Lynch.14,15
Analogamente, l’associazione mammella-ovaio nella stessa pa-ziente, specie se giovane, è frequente nelle donne portatricidi mutazione germinale nei geni BRCA1-2.16,17 I tumoriche hanno alla loro base una predisposizione ereditaria pre-sentano caratteristiche peculiari: le donne portatrici di mu-
here underestimated the true MP risk. This observation war-rants further investigation as this is an important piece of in-formation for clinical surveillance of these women, who havea high probability of developing breast cancer with un-favourable prognostic parameters (ER-, Pgr-, G3).11-13
In the youngest women (20-49 years) high excess MP risks wererecorded for selected FPN and MP sites (colorectal FPN with en-dometrial or ovarian MP or vice versa): a large part of cases canbe ascribed to the spectrum of the Lynch syndrome cancers.14,15
Similarly, the association of breast and ovarian cancer in thesame patient, at a young age, is frequently observed in BRCA1-2 mutation carriers.16,17 Tumours developed as a result of a spe-cific germinal mutation show certain peculiarities: e.g., womenwho carry a BRCA1 mutation frequently develop triple-negativebreast cancers18,19 (ER-/Pgr-/HER2-); in addition, they carry a60% lifetime risk of developing ovarian cancer and an 80% life-time risk of contralateral breast cancer.17
An excess MP risk in sites sharing the same risk factors as theFPN were observed when risky lifestyle habits (e.g., tobaccosmoking and alcohol drinking) were involved: the correspondingSIRs were high, particularly among young patients of both sexes.Individuals who developed cancer in the upper aerodigestive tractat a young age showed an excess risk of developing an MP in thesame area, but in all age groups the risk seemed to be greater forwomen than for men. In this body region the field effect plays amajor role.20 A prolonged exposition of tissue to environmentalsubstances, including carcinogens (e.g., tobacco smoking and al-cohol drinking) can generate a large area of genetically alteredcancer fields. Epithelial cells during their frequent self-renewalcan form hyperplastic tissue, which in turn may represent the ba-sis for malignant proliferation. Molecular signatures of field can-cerization have been well documented for several epithelial tu-mours and particularly for upper aerodigestive tract cancers.21
Tables a, b and c also take into account the possibility that partof selected MPs (thyroid, skin melanoma, kidney, prostatecancer) might have been overdiagnosed as a consequence of sur-veillance programmes aimed at diagnosing diseaserecurrence/progression as early as possible: the increasing sen-sitivity of new diagnostic tools (CT, MRI) might critically in-crease the burden of this outcome.22 Two circumstances seem tosupport this consideration:■ the highest SIRs were observed in the 20-49 and 50-69 agegroup and the risk is strongly reduced for the elderly;■ in most cases the risk was higher during the 5 year periodafter FPN diagnosis than thereafter, probably as a consequenceof close clinical surveillance in subjects who had been treatedwith radical intent.For several FPN sites a lower than expected MP incidence wasobserved (tables a, b and c). This event was only marginally ob-served in the 20-49 years age group and the frequency increasedin older age groups. SIRs <1.0 for MPs are more frequently ob-served in association with an FPN site that has poor prognosis(lung, pancreas) or as a consequence of an extensive surgical
Rischio di secondo tumore in diverse fasce d’etàI tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI
144 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152

tazione nel gene BRCA1 sviluppano molto frequentementetumori tripli negativi18,19 (ER-/Pgr-/HER2-) e hanno un ri-schio nel corso della vita di sviluppare un tumore dell’ovaioche può arrivare al 60% e della mammella controlaterale chepuò raggiungere l’80%.17
Un eccesso di MP che condividono gli stessi fattori di ri-schio della FPN si osserva nel caso di abitudini di vita no-cive, quali per esempio il consumo di alcol e il fumo di si-garetta. I SIR di MP in sedi sensibili a tali fattori di rischiosono molto elevati tra i giovani di entrambi i sessi e più mo-derati tra i più anziani. Infatti, i pazienti che sviluppano untumore del distretto delle vie aerodigestive superiori ingiovane età hanno un eccesso di rischio di svilupparne unsecondo nello stesso distretto e, a parità di età, il rischio èpiù elevato nelle donne rispetto agli uomini. In questo di-stretto anatomico ha sicuramente un ruolo preminente ilcosiddetto field effect.20 L’esposizione prolungata a cancero-geni (fumo di tabacco, alcol) può determinare precoce-mente la formazione di un’area vasta di campi cellulari chehanno subito alterazioni genetiche. Le cellule epiteliali a tur-nover cellulare elevato possono andare incontro a iperplasiae l’epitelio iperplastico può costituire la base per la trasfor-mazione neoplastica. Signaturemolecolari della field cance-rization sono state ben documentate per i tumori delle vieaerodigestive superiori.21
Nelle tabelle a, b e c è stata anche presa in considerazione lapossibilità che una parte dei secondi tumori diagnosticati insedi specifiche (tiroide, melanoma, rene, prostata) potesseessere il risultato di sovradiagnosi conseguente all’applicazionedi protocolli di follow-up originariamente mirati alla diagnosiprecoce di recidive/progressione di malattia; l’avvento dimezzi diagnostici sempre più sensibili (TC, RNM) potrebbeaver aumentato l’effetto oltre il desiderato.22 Questa conside-razione sembra essere suffragata da due circostanze:■ le frequenze più elevate si riscontrano nelle fasce d’età 20-49 e 50-69 anni, mentre appaiono abbastanza contenute neipiù anziani;■ nella maggior parte dei casi l’effetto più forte si osserva en-tro i 5 anni dalla diagnosi della FPN, periodo nel quale si con-centra la fase di stretta sorveglianza clinica per i soggetti conmalattia trattata con intento radicale.Sempre nelle tabelle a, b e c sono riportate anche le sedi di se-conda neoplasia per le quali è stato osservato un numero dicasi significativamente inferiore all’atteso. La situazione èmolto marginale nel gruppo d’età 20-49 anni e tende a esserepiù frequente nelle due fasce d’età successive. L’effetto si os-serva, in particolare, per le sedi di primo tumore a prognosigeneralmente sfavorevole (come polmone e pancreas), mentrenel caso dei tumori della sfera genitale femminile un rapportoosservati/attesi <1 (per esempio, diminuito rischio di tumoredell’ovaio dopo tumore dell’endometrio) può essere ascrittoall’estensione del trattamento chirurgico del primo.Un limite importante delle presenti analisi, soprattutto per
treatment that involved surrounding organs, especially for gynae-cological tumours (e.g., ovary removal during hysterectomy foruterine cancer, particularly in postmenopausal women).Finally, a number of individuals included in the presentanalysis might have been diagnosed with cancer before any can-cer registry had been established in their geographic area. Thecancer that in the present evaluation was registered as FPN wasactually an MP, and this may represent an important limita-tion, particularly for cancer registries with short registration pe-riods. This limitation may have an adverse impact particularlyin the 20-49 years age group for the identification of MPs witha genetic background or due to treatment-related sequelae.
CONCLUSIONThe age-grouped analysis may improve the understanding ofthe overall results and may help to address clinical surveillancefor patients affected by a particular cancer. Specifically, itcould be extremely important to help direct the follow-up pro-tocols (e.g., to decide on the exclusion of individuals with a pre-vious neoplasm from organized screening programmes or to re-fer them to intensive surveillance programmes).In these analyses, the availability of additional parameters, e.g.,histological characteristics, at least for the youngest subjects,may be of great importance. Indirect estimate of the burden ofdisease according to age at diagnosis, from large population-based cohorts of cancer patients rather than from clinical case-series, might provide important indications for planning ac-tivities related to genetic counselling, molecular biologylaboratories and clinical specialties.
Rischio di secondo tumore in diverse fasce d’etàI tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI
145 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
BIBLIOGRAFIA/REFERENCES
1. Travis LB, Demark Wahnefried W, Allan JM, Wood ME, Ng AK. Ae-tiology, genetics and prevention of secondary neoplasms in adultcancer survivors. Nat Rev Clin Oncol 2013;10(5):289-301.
2. Andersson M, Jensen MB, Engholm G, Storm H. Risk of second pri-mary cancer among patients with early operable breast cancer reg-istered or randomised in Danish Breast Cancer cooperative Group(DBCG) protocols of the 77, 82 and 89 programmes during 1977-2001. Acta Oncol 2008;47(4):755-64.
3. Royle JS, Baade P, Joske D, Fritschi L. Risk of second cancer after lym-phohematopoietic neoplasm. Int J Cancer 2011;129(4):910-9.
4. Henson KE, McGale P, Taylor C, Darby SC. Radiation-related mortalityfrom heart disease and lung cancer more than 20 years after radio-therapy for breast cancer. Br J Cancer 2013; 108(1):179-82.
5. Morton LM, Gilbert ES, Hall P et al. Risk of treatment-relatedesophageal cancer among breast cancer survivors. Ann Oncol2012;23(12):3081-91.
6. Curtis RE, Boice JD Jr, Stovall M et al. Risk of leukemia afterchemotherapy and radiation treatment for breast cancer. N Engl JMed 1992;326(26):1745-51.
7. Morton LM, Dores GM, Tucker MA et al. Evolving risk of therapy-re-lated acute myeloid leukemia following cancer chemotherapyamong adults in the United States, 1975-2008. Blood 2013;121(15):2996-3004.

quanto riguarda il gruppo d’età 20-49 anni, risiede nel fattoche neoplasie sviluppatesi in fasce di età successive potevanoavere un precedente in periodi antecedenti all’inizio dellaregistrazione (quindi essere un secondo tumore nel caso diregistri con breve periodo di attività): ciò potrebbe avere unimpatto soprattutto sulla valutazione di secondi tumori diorigine genetica o di tumori sequela di terapia.
CONCLUSIONIL’analisi effettuata nelle tre fasce d’età può aiutare nell’interpre-tazione del risultato generale e nel fornire indicazioni relativea benefici possibili e benefici ottenibili per il paziente affettoda neoplasie specifiche. In particolare potrebbe essere impor-tante per indirizzare i protocolli di follow-up (per esempio, perstabilire l’opportunità o meno di escludere soggetti con neo-plasia pregressa dai programmi di screening organizzato).L’introduzione in questo tipo di analisi, almeno per ilgruppo di età più giovane, di ulteriori fattori, quali le ca-ratteristiche istologiche dei tumori e il trattamento effet-tuato (solo chirurgia o terapia radiante e/o medica a scopoadiuvante), potrebbe aggiungere informazioni preziose perl’identificazione dei sottogruppi con reale eccesso di rischiodi una seconda neoplasia. Infine, poter stimare, seppure in-direttamente, il carico di malattia in relazione all’età in unapopolazione ampia che deriva da registri tumori di popo-lazione e non da case-serie cliniche potrebbe costituire un in-dicatore importante anche per la programmazione delle at-tività di consulenza genetica oncologica, del laboratorio dibiologia molecolare associato e della specialistica implicatenella sorveglianza clinica.
Rischio di secondo tumore in diverse fasce d’etàI tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI
146 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
8. Hershman D, Neugut AI, Jacobson JS et al. Acute myeloid leukemiaor myelodysplastic syndrome following use of granulocyte colony-stimulating factors during breast cancer adjuvant chemotherapy. JNatl Cancer Inst 2007;99(3):196-205.
9. Davies C, Pan H, Godwin J et al; Adjuvant Tamoxifen: Longer AgainstShorter (ATLAS) Collaborative Group. Long-term effects of contin-uing adjuvant tamoxifen to 10 years versus stopping at 5 years afterdiagnosis of oestrogen receptor-positive breast cancer: ATLAS, a ran-domised trial. Lancet 2013;381(9869):805-16.
10.Jones ME, van Leeuwen FE, Hoogendoorn WE et al. Endometrialcancer survival after breast cancer in relation to tamoxifen treat-ment: pooled results from three countries. Breast Cancer Res2012;14(3):R91.
11.Dores GM, Anderson WF, Beane Freeman LE, Fraumeni JF Jr, CurtisRE. Risk of breast cancer according to clinicopathologic featuresamong long-term survivors of Hodgkin’s lymphoma treated with ra-diotherapy. Br J Cancer 2010;103(7):1081-4.
12.Swerdlow AJ, Cooke R, Bates A et al. Breast cancer risk after supra-diaphragmatic radiotherapy for Hodgkin’s lymphoma in England andWales: a National Cohort Study. J Clin Oncol 2012;30(22):2745-52.
13.Colin C, de Vathaire F, Noël A et al. Updated relevance of mammo-graphic screening modalities in women previously treated with chestirradiation for Hodgkin disease. Radiology 2012;265(3):669-76.
14.Win AK, Lindor NM, Young JP et al. Risks of primary extracolonic can-cers following colorectal cancer in lynch syndrome. J Natl Cancer Inst2012;104(18):1363-72.
15.Vasen HF, Blanco I, Aktan-Collan K et al; Mallorca group. Revisedguidelines for the clinical management of Lynch syndrome (HNPCC):recommendations by a group of European experts. Gut 2013;62(6):812-23.
16.Metcalfe KA, Lynch HT, Ghadirian P et al. The risk of ovariancancer after breast cancer in BRCA1 and BRCA2 carriers. GynecolOncol 2005;96(1):222-6.
17.Mavaddat N, Peock S, Frost D et al; EMBRACE. Cancer Risks forBRCA1 and BRCA2mutation carriers: results from prospective analy-sis of EMBRACE. J Natl Cancer Inst 2013;105(11):812-22.
18.Reis-Filho JS, Tutt AN. Triple negative tumors: a critical review.Histopathology 2008;52(1):108-18.
19.Lips EH, Mulder L, Oonk A et al. Triple-negative breast cancer: BR-CAness and concordance of clinical features with BRCA1-mutationcarriers. Br J Cancer 2013;108(10):2172-7.
20.Dakubo GD, Jakupciak JP, Birch-Machin MA, Parr RL. Clinical impli-cations and utility of field cancerization. Cancer Cell Int 2007;7:2.
21.Roesch-Ely M, Nees M, Karsai S et al. Proteomic analysis reveals suc-cessive aberrations in protein expression from healthy mucosa to in-vasive head and neck cancer. Oncogene 2007;26(1):54-64.
22.Welch HG, Black WC. Overdiagnosis in cancer. J Natl Cancer Inst2010;102(9):605-13.

WWW.EPIPREV.IT
L’evenienza di tumori multipli richiede una riflessione sullestrategie di controllo in relazione ai diversi quadri clinici dipatologia neoplastica in cui possono insorgere.I tumori multipli possono essere sincroni o metacroni,possono riguardare la stessa sede anatomica o più sedi, epossono rientrare in differenti quadri eziologici e clinici:■ sindromi ereditarie a diverse penetranze, che possono es-sere clinicamente manifeste o rese note solo da alterazionimolecolari; ■ predisposizione genetica di forme sporadiche;■ nuova neoplasia che riconosce uno stesso agente eziolo-gico endogeno o esogeno della prima neoplasia; ■ secondotumore dopo pregresso trattamento di radioterapia e/ochemioterapia in un paziente guarito dalla prima neoplasia.Dalla molteplicità delle situazioni cliniche evidenziate con-segue che le differenti possibilità di sviluppo di tumorimultipli possano richiedere interventi sanitari correlatialla fase specifica della malattia neoplastica: ■ prevenzioneprimaria per le forme che riconoscono il medesimo rischioespositivo; ■ prevenzione secondaria per le neoplasie a rischiogenetico o a maggiore incidenza in gruppi clinicamente a ri-schio; ■ follow-up per i pazienti guariti con maggior rischiosporadico di insorgenza di una seconda neoplasia nella stessasede; e ■ follow-up per i tumori secondari di pazienti “guariti”da una prima neoplasia trattata con radioterapia e/o chemio-terapia per lo più in età infantile o giovanile. In tutti questisetting diversi per la scelta del programma o della strategia diintervento va sempre considerato il significato prognostico eil rischio evolutivo di ogni singola neoplasia. Nelle forme ere-ditarie, non frequenti, il rischio di un secondo tumore è dif-ferente a seconda della penetranza genetica, ma anche dellarilevanza già clinica di una sindrome o dello stato di soloportatore di alterazione genetica. Avremo così quadri clini-camente manifesti, come nella Sindrome di Gardner, nellaSindrome di Lynch, nella Familial Adenomatous Polyposis(FAP), nelleMultiple Endocrine Neoplasia (MEN) 1 e 2; op-pure situazioni di rischio più o meno elevato di sviluppareun secondo tumore su stessa base genetica, come nei tumoridella mammella e dell’ovaio BRCA1 e 2 positivi. In questesituazioni le misure di controllo riguardano esami specificiin relazione al rischio di sviluppare uno o più tumori suc-cessivi in una o più sedi, fino alla possibilità di una chirurgiaexeretica profilattica. Diverse sono lemisure sanitarie richiesteper i tumori correlati all’esposizione ad agenti cancerogeni eso-geni che possono essere in relazione allo stile di vita, come nel
Careful consideration of control strategies for multiple primarycancers is necessary, considering the various possible medical cases.Multiple primaries can be classified as synchronous ormetachronous; they can occur in the same anatomical site orin multiple sites; they can fall into different aetiological andclinical categories:■ hereditary cancer syndromes with varying degrees of pene-trance, which may be clinically manifest or made known onlyby molecular alterations;■ genetic predisposition of sporadic forms;■ new cancer with the same (endogenous or exogenous) aeti-ology as the first cancer;■ second cancer after previous radiotherapy and/or chemother-apy in a patient cured of the first cancer.
In consideration of the great variety of clinical situations ob-served, it is clear that different types of second cancers may re-quire different health interventions, based on specific diseasecharacteristics:■ primary prevention for cancers with common exposure;■ secondary prevention for cancers with genetic risk or for can-cers with higher incidence in high risk populations;■ follow-up for cured cancer patients with greater risk of de-veloping sporadic second cancer in the same site;■ follow-up for secondary cancer in cured cancer patientstreated with radiotherapy and/or chemotherapy, mainly inchildhood or youth.In these different settings, prognosis and risk of evolutionshould be evaluated to select the best intervention strategy.In hereditary forms, which are infrequent, the risk of devel-oping second cancers depends on genetic penetrance andwhether the syndrome already has clinical relevance or only ge-netic alteration status. There are evident medical cases, as inGardner syndrome, Lynch syndrome, familial adenomatous poly-posis (FAP), multiple endocrine neoplasia (MEN) type 1 and 2,or other situations with high or medium risk of developing a sec-ond cancer with the same genetic basis as the first cancer, as inbreast and ovarian cancers in BRCA1 and 2 positive patients.Control strategies depend on the risk of developing one or moresubsequent tumours in one or more sites, and even include the pos-sibility of prophylactic surgery.There are several possible health interventions for cancerrelated to exogenous carcinogens, whether lifestyle-related(e.g., tobacco smoke or alcohol habits, sexual habits as in
Il significato clinico dei tumori multipliClinical interpretation of multiple primary cancers
Carmine Pinto Segretario nazionale Associazione italiana di oncologia medica (AIOM)Oncologia medica, Policlinico S. Orsola-Malpighi, Bologna
147 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
I tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI
Capitolo 10

HPV infection) or known professional and/or environmentalcarcinogens (e.g., asbestos).A single carcinogen may cause one or more different types ofcancer, even with different latency time. For example, tobaccosmoke is a recognized cause of lung cancer and respiratory tractcancer, but it also consistently increases the risk of developingbladder cancer and head and neck cancer. HPV infection is arecognized cause for cervical cancer, but it is also involved indeveloping cancer of the oropharynx and anus. Asbestos is anenvironmental and occupational carcinogen, it causes malig-nant pleural and peritoneal mesothelioma, but it is also asso-ciated with lung cancer. In these cases health interventionsshould remove the carcinogenic risk factor and reduce syncar-cinogenic factors which may have a multiplier effect in cancerdevelopment (e.g., cigarette smoke for lung cancer in subjectsexposed or previously exposed to asbestos). Therefore, all diag-nostic assessments related to the risk of developing a second can-cer should be evaluated.Endogenous factors, including hormonal factors, may con-tribute to second cancer in the same site as first cancer, as inthe case of breast and colorectal cancer. In this case, risk of sec-ond cancer occurrence should be evaluated. The second cancermay be synchronous or it may occur during follow-up time,which should therefore be longer than required for usual con-trol of the first cancer.Advanced stage cancers (as Hodgkin and non-Hodgkin lym-phomas and testis cancer in childhood and adolescence) treatedwith chemotherapy and/or radiotherapy may be associatedwith second cancers diagnosed many years after therapy. Theseiatrogenic secondary cancers occurred in 2-3% of cancer pa-tients treated during the past years. Currently, as technologyand treatment keep improving, the risk is decreasing: never-theless, follow-up of these young cured patients should considerthis potential problem.In conclusion, the improvement in cancer control strategiesand the increase in survival are related to the risk of developingmultiple tumours. Patient care and subsequent follow-upshould consider this potential second cancer occurrence, witha balance among intervention, monitoring, and rehabilitation.
Il significato clinico dei tumori multipliI tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI
148 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
caso di fumo di tabacco e dell’abitudine all’alcool, ad abitudinisessuali come nel caso dell’infezione da HPV, o a cancerogeninoti professionali e/o ambientali, come nel caso dell’amianto.Uno stesso agente cancerogeno esogenopuò essere all’originedel-l’insorgenza di una o più neoplasie differenti, anche con tempidi latenza diversi. Così il fumodi tabacco, oltre a essere causa ri-conosciuta di insorgenza delle neoplasie polmonari e delle primevie respiratorie, aumenta consistentemente anche il rischio di svi-luppare tumori della vescica e del distretto testa-collo. L’infezionedaHPVriconosciuta come agente eziologicodel carcinomadellacervice uterina interviene anche nell’insorgenza del carcinomadell’orofaringe e dell’ano. Le fibre di amianto, cancerogeno pro-fessionale e ambientale, non sono solo agente causale delmeso-teliomamaligno pleurico e peritoneale,ma determinano ancheun importante incremento di rischio di insorgenza di carcinomadel polmone. In quest’ambito le misure di intervento sanitarioin fase di diagnosi, di stadiazione, di terapia e di follow-up de-vono essere indirizzate, quando possibile, sia all’eliminazionedell’agente di rischio cancerogeno che può produrre anche unasecondaneoplasia, sia alla riduzionedi fattori di sincancerogenesiche possono avere un effettomoltiplicativo, come il fumo di si-garetta negli esposti o ex-esposti ad amianto in relazione all’in-sorgenza di carcinoma polmonare. Vanno quindi sempre con-siderate tutte le valutazioni diagnostiche legate al rischio disviluppo di una seconda neoplasia correlata allo stesso agenteeziologico noto. Fattori endogeni, anche di tipo ormonale,possono intervenire nell’insorgenza di una secondaneoplasia cheinteressa lo stesso organo della prima, come nel caso del carci-noma dellamammella e del colon retto. In quest’ambito va va-lutata la possibilità di insorgenza di un secondo tumore, che puòessere sincrono, o più spesso puòmanifestarsi in corso di follow-up. Il follow-up deve quindi essere continuato in riferimento aquesto rischio potenziale per un periodo temporale prolungatorispetto a quanto richiesto dal controllo usuale della primama-lattia neoplastica. Tumori anche in fase avanzata, soprattuttodell’età infantile e giovanile, come i linfomi di Hodgkin e non-Hodgkin e i tumori del testicolo, suscettibili di guarigione contrattamenti di chemioterapia e/o radioterapia, possonopresentarea distanza di più di 10-20 anni dalla terapia lo sviluppo di unaseconda neoplasia legata al trattamento stesso. Con le cure pra-ticate nei decenni passati, questi tumori iatrogeni secondari po-tevano, a seconda del trattamento primario, insorgere nel 2-3%dei casi. Attualmente, con il miglioramento delle tecnologie edella selettività dei trattamenti questo rischio andrà sempre piùriducendosi,ma il follow-up dei giovani pazienti guariti deve inogni caso considerare questa possibile evenienza. In conclusione,il miglioramento delle strategie di controllo delle malattie neo-plastiche e l’aumento di sopravvivenza dei pazienti oncologici,con l’estensione progressiva della fascia dei pazienti guariti, si ri-flette anche nell’incidenza dei tumori multipli. La cura dei pa-zienti e il successivo follow-up deve oggi considerare sempre piùquesta potenziale evenienza, conun equilibrio tra intervento, sor-veglianza e riabilitazione sapiente e culturalmente maturo.

WWW.EPIPREV.IT Appendice / Appendix
149 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
I tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI
REGISTROTUMORI DELL’ALTOADIGETUMORREGISTER SÜDTIROLServizio di anatomia e istologia patologica,ospedale di Bolzanocorso Italia 13/M, 39100 Bolzanotel: +39 0471 907150 - fax: +39 0471 907144e-mail: [email protected]
Guido Mazzoleni, Andreas Bulatko,Elena Devigli, Birgit Tschugguel,Elena De Valiere, Gerlinde Facchinelli,Markus Falk, Tomas Dal Cappello
Si ringraziano per la collaborazione i medici dellestrutture ospedaliere provinciali pubbliche e privateconvenzionate e il dottor Francesco Bellù che no-nostante il pensionamento continua volontaria-mente la sua preziosa attività per il Registro.
REGISTRO TUMORI PIEMONTE,PROVINCIA DI BIELLACPO, Centro di riferimento regionale perl’epidemiologia e la prevenzione dei tumori c/oSOS di epidemiologia SC programmazionee qualità ASL BIvia Don Sturzo 20, 13900 Biellatel: +39 015 3503665 / 3503655fax: +39 015 8495222e-mail: [email protected];[email protected]
Adriano Giacomin, Pier Carlo Vercellino,Simona Andreone
Si ringraziano le direzioni sanitarie e i dirigenti sa-nitari delle strutture pubbliche e private coinvoltee gli uffici anagrafici comunali per la preziosa col-laborazione fornita. Un ringraziamento va a tutticoloro, in particolare alla direzione aziendale ealla Fondazione Edo ed Elvo Tempia, che hannocreduto e sostenuto il registro fin dall’avvio col-laborando alle iniziative di AIRTUM e dell’epide-miologia piemontese.
REGISTRO TUMORI DELL’AREAVASTA EMILIA CENTRALEAzienda USL di FerraraDipartimento di sanità pubblicaCorso Giovecca 203, 44121 Ferraratel: +39 0532 455513 / 238627fax: +39 0532 235375e-mail: [email protected]; [email protected]
Stefano Ferretti, Laura Marzola,Elena Migliari, Nada Carletti,Patrizia Biavati, Chiara Petrucci
Si ringraziano per la collaborazione e il sostegnoricevuti la Regione Emilia-Romagna, l’Aziendaospedaliera universitaria di Ferrara, l’Azienda USLdi Ferrara e tutti i colleghi che a vario titolo hannocontribuito all’attività del Registro tumori.
REGISTRO TUMORI TOSCANOIstituto per lo studio e la prevenzione oncologica(ISPO), UO di epidemiologia clinica e descrittivaVia delle Oblate 2, Ponte Nuovo, palazzina 28/A,50135 Firenzetel: +39 055 7972508 / 7972512fax: +39 055 7972588e-mail: [email protected]: emanuelecrocetti
Emanuele Crocetti, Carlotta Buzzoni, AdeleCaldarella, Antonella Corbinelli, TeresaIntrieri, Gianfranco Manneschi, LibuseNemcova, Cristina Ocello, ClaudioSacchettini, Marco Zappa, Eugenio Paci
Il Registro tumori è un’iniziativa della Regione To-scana e dell’Istituto tumori toscano.
REGISTRO TUMORIDEL FRIULI VENEZIA GIULIADirezione centrale salute, Udinec/o IRCCS CRO,Avianotel: +39 0434 659354 - fax: +39 0434 659231e-mail: [email protected]
Diego Serraino, Tiziana Angelin, EttoreBidoli, Silvia Birri, Luigino Dal Maso,Margherita De Dottori, Emilia De Santis,Ornella Forgiarini, Antonella Zucchetto,Loris Zanier
REGISTRO TUMORIREGIONE LIGURIAUOS epidemiologia descrittiva (Registro tumori),IRCCS AOU S. Martino - IST Istituto nazionalericerca sul cancrolargo Rosanna Benzi 10, 16132 Genovatel: +39 010 5558502 / 5558456fax: +39 010 5558302e-mail: [email protected]
Luigina Bonelli, Claudia Casella,Enza Marani, Antonella Puppo,Maria Vittoria Celesia, Roberta Cogno, ElsaGarrone, Alberto Quaglia,Marina Vercelli
Si ringraziano le aziende sanitarie ospedaliere, leASL liguri (in particolare quelle della Provincia diGenova) e i dirigenti sanitari (direzioni sanitarie, re-parti di cura, anatomie patologiche, radioterapieeccetera) che hanno interagito con il RTRL per age-volare la rilevazione degli operatori. Si ringrazianoil dottor SergioVigna, referente regionale c/oAgenziaregionale sanitaria Liguria, la dottoressa GabriellaPaoli, Assessorato alla sanità Regione Liguria, ladottoressa Elena Ricci, responsabile dell’Ufficio sta-tistico regionale per aver messo a disposizione iprincipali sistemi informativi regionali; un ringra-ziamento alle amministrazioni dei Comuni liguriper la collaborazione nel follow-up dei casi.
REGISTROTUMORI DI POPOLAZIONEDELLA PROVINCIA DI LATINAc/o direzione azienda AUSL LatinaCentro direzionale Latina Fioriviale PL. Nervi, 04100 Latinatel: +39 0773 6553437fax: +39 0773 6553499e-mail: [email protected]
Fabio Pannozzo, Susanna Busco,Ivan Rashid, Valerio Ramazzotti,Maria Cecilia Cercato, Mautilio Natali,Walter Battisti, Isabella Sperduti,Leonarda Macci, Ester Bugliarello,Edvige Bernazza, Lucilla Tamburo,Miriana Rossi, Simonetta Curatella,Silvana Tamburrino, Silvia Fattoruso,Giuseppina Serafini, Orsola Valerio
La rete dei Registri AIRTUMPersonale, contatti, ringraziamenti
The network of the AIRTUM Cancer RegistriesStaff, contacts, acknowledgements

La rete dei registri AIRTUMI tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI
150 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
REGISTRO TUMORI DI MILANOASL di Milano, ss di epidemiologiacorso Italia 19, 20122 Milanotel +39 02 85782114 / 85782100fax +39 02 85782128e-mail: [email protected]@asl.milano.it
Mariangela Autelitano, Simona Ghilardi,Rosanna Leone, Luisa Filipazzi, AnnamariaBonini, Cinzia Giubelli
Si ringraziano la Regione Lombardia, le strutturedi diagnosi e cura e i Servizi di anatomia patologicadi Milano.
REGISTRO TUMORIDELLA PROVINCIA DI MODENACentro oncologico modenesec/o azienda ospedaliera Policlinico di Modenavia del Pozzo 71, 41100 Modenatel: +39 059 4224337 - fax: +39 059 4224152e-mail: [email protected] internet: www.rtm.unimo.it
Massimo Federico, Maria Elisa Artioli,Katia Valla, Barbara Braghiroli, ClaudiaCirilli, Francesco Iachetta, StefanoLuminari, Monica Pirani, Lorenza Ferrari
REGISTRO TUMORI DI POPOLAZIONEDELLA REGIONE CAMPANIAc/o ASL NA3 Sudpiazza San Giovanni, 80031 Brusciano (NA)tel: +39 081 3174243 / 3174244 / 5190505fax: +39 081 5190505e-mail: [email protected]: mario.fusco57
Mario Fusco, Caterina Bellatalla,Maria Fusco, Margherita Panico,Carmela Perrotta, Biagio Vassante,Maria Francesca Vitale
REGISTRO TUMORIDELLA PROVINCIA DI PARMAUO oncologia,Azienda ospedaliera universitaria di Parmavia Abbeveratoia 4, 43100 Parmatel: +39 0521 702673 / 702660fax: +39 0521 995448e-mail: [email protected]
Maria Michiara, Francesco Bozzani,Paolo Sgargi
Si ringraziano il professor EnricoMaria Silini, diret-tore dell’Istituto di anatomia patologica,Universitàdi Parma, il dottor Alberto Tardini, del laboratorioCERB di Parma, e il dottor Giuseppe Ugolotti, labo-ratorio di citologia aziendaUSL Parma, la dottoressaDina Gnappi dell’Ufficiomobilità sanitaria,Aziendaunità sanitaria locale Parma.
REGISTRO TUMORIDELLA PROVINCIA DI RAGUSADipartimento di prevenzione medica,Azienda sanitaria provinciale (ASP 7) Ragusavia Dante 109, 97100 Ragusatel: +39 0932 600055 - fax: +39 0932 682169e-mail: [email protected]
Rosario Tumino, Giuseppe Cascone,Graziella Frasca, Maria ConcettaGiurdanella, Caterina Martorana, GabrieleMorana, Carmela Nicita, Patrizia ConcettaRollo, Maria Grazia Ruggeri, AuroraSigona, Eugenia Spata, Stefania Vacirca
Si ringraziano Regione Sicilia,Associazione Ibleaper la ricerca epidemiologica (AIRE) ONLUS, ana-grafi comunali Provincia di Ragusa e GiovannaSpata.
REGISTRO TUMORI REGGIANOASMN-IRCCS, Unità di epidemiologia,Dipartimento di sanità pubblica,Azienda USL di Reggio Emiliavia Amendola 2, 42100 Reggio nell’Emilia (RE)tel: +39 0522 335303 - fax: +39 0522 335460e-mail: [email protected]
Lucia Mangone, Enza Di Felice, AnnamariaPezzarossi, Stefania Caroli, CarlottaPellegri, Massimo Vicentini, StefaniaD’Angelo, Paola Balottari
Si ringraziano i medici delle strutture ospedalierepubbliche e private convenzionate provinciali perla collaborazione all’attività del registro tumori.
REGISTROTUMORI DELLA ROMAGNAIRCCS Istituto tumori della Romagna (IRST)via P. Maroncelli 40/42, 47014 Meldola (FC)tel: +39 0543 739450 - fax: +39 0543 739459e-mail: [email protected]@ausl.fo.it
Fabio Falcini, Americo Colamartini, LauroBucchi, Chiara Balducci, Mila Ravegnani,Benedetta Vitali, Carlo Cordaro, LiciaCaprara, Orietta Giuliani, Stefania Giorgetti,Silvia Salvatore, Monica Palumbo, RosaVattiato, Alessandra Ravaioli, Flavia Foca,Elisa Rinaldi, Silvia Mancini
Si rigraziano Marinella Amadori e Chiara Tonelli.
REGISTRO TUMORIDELLA PROVINCIA DI SALERNOvia V. Loria 24, 84129 Salernotel: +39 089 522024 / 522983fax: +39 089 338514e-mail: [email protected]@provincia.salerno.it
Luigi Cremone, Claudia Gaudiano, ArturoIannelli, Gennaro Senatore, Arrigo Zevola
REGISTRO TUMORIDELLA PROVINCIA DI SASSARIServizio di epidemiologia,ASL1, Sassarivia Tempio 5, 07100 Sassaritel: +39 079 2062442 / 2062452fax: +39 079 2062445e-mail: [email protected]
Ornelia Sechi, Rosaria Cesaraccio, DanielaPirino, Donatella Carboni, Giovanna Fiori,Marcella Soddu, Gianpaolo Mameli,Francesco Mura
REGISTRO TUMORIDELLA PROVINCIA DI SIRACUSAASP Siracusa - corso Gelone 17, 96100 Siracusatel: + 39 0931 484341 / 484172fax: +39 0931 484383e-mail: [email protected]
Maria Lia Contrino, Anselmo Madeddu,Francesco Tisano, Salvatore Sciacca,Angela Muni, Margherita Mizzi, MariaRusso, Giorgio Sacco, Paoletta Aletta,Antonino Colanino Ziino
REGISTRO TUMORI DI SONDRIOASL della Provincia di Sondrio,Osservatorio epidemiologicotel: +39 0342 555882 - fax: +39 0342 555859e-mail: [email protected] Internet: www.asl.sondrio.it/registro_tumori/
Sergio Maspero, Anna Clara Fanetti,Jaqueline Frizza, Elena Moroni,Ivan Cometti, Monica Lucia Annulli, LorellaCecconami, Roberto Tessandori
Si ringrazia l’Azienda ospedaliera della Valtellinae della Valchiavenna.
REGISTRO TUMORI PIEMONTECentro di riferimento per l’epidemiologiae la prevenzione oncologica (CPO) PiemonteAOU S.Giovanni Battista - Molinette, Torinovia S. Francesco da Paola 31, 10123 Torinotel: +39 011 5665355 - fax: +39 011 5665362e-mail: [email protected] Internet: www.cpo.it
Roberto Zanetti, Stefano Rosso, SilviaPatriarca, Rossana Prandi, Irene Sobrato,Franca Gilardi, Paola Busso
REGISTRO TUMORIDELLA PROVINCIA DI TRENTOServizio epidemiologia clinica e valutativa,Azienda provinciale per i servizi sanitari,Centro per i servizi sanitari -viale Verona, 38123 Trentotel: +39 0461 904638 - fax: +39 0461 904645e-mail: [email protected]
Silvano Piffer, Maria Gentilini,Roberto Rizzello, Maddalena Cappelletti,Fernanda Dalsasso

La rete dei registri AIRTUMI tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI
151 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.itEpidemiol Prev 37 (4-5) Suppl 1:1-152
REGISTRO TUMORI UMBRODI POPOLAZIONEDipartimento di specialità medico, chirurgichee sanità pubblica, Sezione di sanità pubblica,Università degli Studi di Perugiavia del Giochetto, 06100 Perugiatel: +39 075 5857366 / 5857335 / 5857329fax: +39 075 5857317e-mail: [email protected] Internet:www.unipg.it/~dipigmed/RTUP/RTUP.htm
Francesco La Rosa, Fabrizio Stracci, DanielaD’Alò, Massimo Scheibel, DanielaCostarelli, Francesco Spano, StefaniaRossini, Cinzia Santucci,Anna Maria Petrinelli, Clotilde Solimene,Fortunato Bianconi, Valerio Brunori
REGISTRO TUMORIDELLA LOMBARDIA,PROVINCIA DI VARESEIstituto nazionale per la ricerca sul cancro (INT)via Venezian 1, 20133 Milanotel: +39 02 23902501 / 23902502fax: +39 02 23902762e-mail: [email protected]
Giovanna Tagliabue, Paolo Contiero,Lucia Preto, Andrea Tittarelli,Sabrina Fabiano, Anna Maghini,Tiziana Codazzi, Emanuela Frassoldi,Daniela Gada, Laura di Grazia
Si ringraziano la Regione Lombardia, l’ASL diVarese,gli ospedali, le case di cura, i medici di medicinagenerale e i comuni della Provincia di Varese perla preziosa collaborazione.
REGISTRO TUMORI DEL VENETOPassaggio Gaudenzio 1, 35131 Padovatel: +39 049 8215605 - fax: +39 049 8215983e-mail: [email protected] Internet: www.registrotumoriveneto.it
Angelo Paolo Dei Tos, Maddalena Baracco,Emanuela Bovo, Antonella Dal Cin, AnnaRita Fiore, Alessandra Greco, StefanoGuzzinati, Daniele Monetti, AlbertoRosano, Carmen Stocco, SandroTognazzo
REGISTRO TUMORIDELL’ASL DI BRESCIADipartimento programmazione, aquistoe controllo,ASL di Bresciaviale Duca degli Abruzzi 15, 25124 Bresciatel: +39 030 3839334 / 3838009fax: +39 030 3838335e-mail: [email protected]@aslbrescia.it
Michele Magoni, Giuseppe Zani, OrnellaSalvi, Maria Puleio, Claudia Gerevini, CinziaGasparotti, Roberta Chiesa, Fulvio Lonati
REGISTRO TUMORIDELLA PROVINCIA DI MACERATAScuola di scienze mediche veterinarie,Università di Camerinovia Gentile III da Varano, 62032 Camerino (MC)tel: +39 0737 402403 - fax: +39 0737 402403e-mail: [email protected] Internet: www.unicam.it/tumori
Susanna Vitarelli, Silvia Antonini
REGISTRO TUMORIDELLA PROVINCIA DI TRAPANIServizio sanitario Regione Sicilia,Dipartimento di prevenzione,Area igienee sanità pubblica,ASP Trapanivia Ammiraglio Staiti 95, 91100 Trapanitel: +39 0923 543036 - fax: +39 0923 26363e-mail: [email protected]
Giuseppina Candela, Tiziana Scuderi,Barbara Lottero, Michele Ribaudo
REGISTRO TUMORIDELLA PROVINCIA DI MANTOVADipartimento PAC, Osservatorio epidemiologico,ASL Provincia di Mantovavia Dei Toscani 1, 46100 Mantovatel: + 39 0376 334508e-mail: [email protected]
Paolo Ricci, Linda Guarda, Luciana Gatti,Annalaura Bozzeda, Maria Dall'Acqua,Vanda Pironi
REGISTRO TUMORIDELLA PROVINCIA DI CATANZAROASP di Catanzaro, Serviziodi epidemiologiae statistica sanitariavia Purificato 18, 88100 Catanzarotel: +39 0961 728378e-mail: [email protected]
Antonella Sutera Sardo, Adriana Mazzei,Anna Maria Lavecchia, Pierina Mancuso
REGISTRO TUMORI DI NUOROUO Registro tumori di Nuoro,ASL di Nuoro e ASL di Lanuseivia Trieste 80, 08100 Nuorotel: + 39 0784 240843 / 240811e-mail: [email protected]
Mario Usala, Filomena Pala, GiovannaMaria Sini, Nicolina Pintori, Luisa Canu,Giuliana Demurtas, Nina Doa
REGISTRO TUMORI DI PALERMOE PROVINCIA E REGISTRO TUMORIDELLA MAMMELLA DI PALERMOUOC Epidemiologia clinica con Registro tumoridi Palermo e Provincia, Dipartimento di scienze perla promozione della salute materno-infantile “GD’Alessandro”via del Vespro 133, 90131 Palermotel: +39 091 6553687 / 6553631e-mail: [email protected]
Francesco Vitale, Rosanna Cusimano,Adele Traina, Agnese Guttadauro, MariaAntonietta Cascio, Rita Mannino, BarbaraRavazzolo, Maria Angela Brucculeri,Giuseppa Rudisi, Maria Stella Adamo,Rosalba Amodio, Alessandro Costa,Maurizio Zarcone, Raffaella Sunseri,Giovanni Bucalo, Carlo Trapani, RosalbaStaiti
REGISTRO TUMORIDELLA PROVINCIA DI COMOASL della Provincia di Como,Registro tumori e screeningvia Castelnuovo 1, 22100 Comotel: +39 031 370848e-mail: [email protected]@asl.como.it
Gemma Gola, Mariangela Corti,Luigi Grandi
REGISTRO TUMORI INTEGRATODI CATANIA E MESSINADipartimento GF Ingrassia,Area igiene e sanitàpubblica, Università degli studi di Cataniavia S. Sofia 87, 95123 Cataniatel/fax: +39 095 3782110e-mail: [email protected]
Salvatore Sciacca, Salvatore Sciacchitano,Melchiorre Fidelbo, Giovanni Benedetto,Enrico Vasquez, Francesca Bella, LauraCalabretta, Marine Castaing, Alessia DiPrima, Antonio Ieni, Anna Leone, PaolaPesce, Carlo Sciacchitano, Antonina Torrisi,Antonietta Torrisi, Massimo Varvarà
Si ringraziano per la collaborazione la Regione Si-cilia, il Dipartimento osservatorio epidemiologico,l’Azienda ospedaliero-universitaria Policlinico diCatania, l’AOOR Papardo-Piemonte di Messina,tutte le Aziende sanitarie di Catania, Messina, Si-racusa ed Enna, le strutture private convenzionate,tutti i Servizi che forniscono i loro archivi di ana-tomia patologica e di oncologia, e tutti i medici eoperatori sanitari che a vario titolo hanno contri-buito all’attività del Registro tumori integrato.

REGISTRO TUMORIDELLA PROVINCIA DI BERGAMOServizio epidemiologia aziendale,ASL della Provincia di Bergamovia Gallicciolli 4, 24121 Bergamotel: +39 035 385190 - fax: +39 035 385304e-mail: [email protected]@asl.bergamo.it
Giuseppe Sampietro, Silvia Ghisleni, Luisagiavazzi, Andreina Zanchi, Alberto Zucchi
REGISTRO TUMORIDELLA ASL MILANO 1Osservatorio epidemiologico e registri specializzativia al Donatore di sangue 50,20013 Magenta (MI)tel: +39 02 97973477 - fax: +39 02 97973484e-mail: [email protected]@aslmi1.mi.it
Antonio Giampiero Russo,Maria Quattrocchi, Rosalba Distefano,Monica Sandrini, Alessandro Civaschi
Si ringraziano la Regione Lombardia, la Direzionestrategica aziendale, le Direzioni delle aziende ospe-daliere e delle case di cura, i Servizi di anatomia pa-tologica e il Dipartimento oncologico aziendale XIe tutti i professionisti che sostengono l’attività delRegistro tumori.
REGISTRO TUMORIDELLA PROVINCIA DI CREMONAServizio epidemiologia e registri di popolazione,ASL della provincia di Cremonavia San Sebastiano 14, 26100 Cremonatel: +39 0372 497213 - fax: +39 0372 497610e-mail: [email protected]
Sabrina Bizzoco, Cristiano Belluardo,Chiara Davini, Silvia Lucchi, Marco Villa,Emanuela Anghinoni, Salvatore Mannino
Si ringraziano per il sostegno e la collaborazione:Regione Lombardia e la Direzione strategica azien-dale, le aziende ospedaliere e le case di cura chehanno contribuito alla collazione della documenta-zione clinica e tutti coloro che si sono prodigati perla realizzazione del Registro tumori
REGISTRO TUMORIDELLA PROVINCIA DI PIACENZADipartimento di sanità pubblica,UO di epidemiologia e comunicazione del rischio,AUSL di Piacenzapiazzale Milano 2, 29121 Piacenzatel: +39 0523 317905 - fax: +39 0523 317943e-mail: [email protected]@ausl.pc.it
Elisabetta Borciani, Pietro Seghini,Rita Prazzoli
REGISTRO TUMORIDELLA PROVINCIA DI LECCEUOC epidemiologia e statistica,Azienda ASL Leccevia Miglietta, 73100 Lecce;UO Registro tumori, Polo oncologico Vito Fazzipiazza Muratore, 73100 Leccetel: +39 0832 661921 / 661909fax: +39 0832 661917e-mail: [email protected]@ausl.le.it
Anna Melcarne, Fabrizio Quarta,Maria Graia Golizia, Anna Maria Raho,Valentina De Maria
REGISTRO TUMORIASL DI TARANTOSC statistica epidemiologia, Settore registrotumori, ASL Tarantoviale virgilio 31, 74121 Tarantotel: +39 099 778775fax: +39 099 7786819
Sante Minerba, Antonia Minicuzzi,Simone Carone, MArgherita Tanzarella
REGISTRO DEI TUMORI INFANTILIDEL PIEMONTESCDU Unità di epidemiologia dei tumori,Università di Torino, Centro di riferimentoper l’epidemiologia e la prevenzioneoncologica (CPO) Piemontevia Santena 7, 10126 Torinotel: +39 011 6334661e-mail: [email protected] Internet: www.cpo.it
Carlotta Sacerdote, Franco Merletti,Corrado Magnani, Guido Pastore,Benedetto Terracini, Daniela Alessi,Tiziana Cena, Fulvio Lazzarato,Vanda Macerata, Milena Maule,Maria Luisa Mosso
Si ringrazia il personale delle strutture ospedalierepiemontesi e in particolare del Reparto di oncoe-matologia pediatrica dell’Ospedale infantile ReginaElena Sant’Anna di Torino per la preziosa collabo-razione all’attività del Registro tumori.
REGISTRO DEI TUMORICOLORETTALI DI MODENAc/o Dipartimento di medicine e specialità mediche,Medicina 1, Policlinico universitario di Modenavia del Pozzo 71, 41100 Modenatel: +39 059 4224715 / 4222269 / 4223605fax: +39 059 4222958e-mail: [email protected],[email protected] Internet: www.tumoricolorettali.unimore.it
Maurizio Ponz de Leon, Federica Domati,Giuseppina Rossi, Carlo Alberto Goldoni,Shaniko Kaleci, Federica Rossi, PieroBenatti, Luca Roncucci, Carmela DiGregorio, Giulia Magnani, Monica Pedroni,Stefania Maffei, Francesco Mariani, LucaReggiani-Bonetti
Si ringrazia la Regione Emilia-Romagna per il con-tributo finanziario.
REGISTRO TUMORI INFANTILIE NEGLI ADOLESCENTIREGIONE MARCHEScuola in scienze del farmaco e dei prodottidella salute, Centro ricerche igienistichee sanitarie, ambientali, Università di Camerinovia Madonna delle Carceri 9,62032 Camerino (MC)tel: +39 0737 402400 / 402409fax: +39 0737 402438e-mail: [email protected],[email protected] Internet: www.unicam.it/tumori/registroinfantili/pag_inf_adol1IT.htm
Mario Cocchioni, Cristiana Pascucci
REGISTRO MESOTELIOMILIGURIACentro operativo regionale (COR Liguria), Registronazionale dei mesoteliomi (ReNaM),Epidemiologia descrittiva e Registro tumori, IRCCS,Azienda ospedale università San Martino,Istituto nazionale per la ricerca sul cancro (IST)largo Rosanna Benzi 10, 16132 Genovatel: +39 010 5737557 - fax: +39 010 5737336e-mail: [email protected]@[email protected]
Valerio Gennaro, Lucia Benfatto,Cecilia Lando, Giovanna Mazzucco
Si ringraziano pazienti e colleghi per la convintacollaborazione e la Regione Liguria per il contributofinanziario e organizzativo.
Epidemiol Prev 37 (4-5) Suppl 1:1-152 ➤ Ulteriori dati disponibili sul sito: www.registri-tumori.it152
I tumori in Italia • Rapporto AIRTUM 2013 • TUMORI MULTIPLI La rete dei registri AIRTUM

A CIASCUNO IL SUOABBONAMENTI 2014
E&P on-line + E&P on-line + E&P on-line +Suppl on-line Suppl on-line + versione cartacea+
versione cartacea supplementi cartacei
PRIVATI ITALIA
1 anno 72 euro 80 euro 95 euro2 anni 135 euro 150 euro 180 euro3 anni 190 euro 210 euro 250 euro
ENTI ITALIA AD ACCESSO UNICO ENTI ITALIA AD ACCESSO MULTIPLO: ABBONAMENTI DA CONCORDARE CON L’EDITORE
1 anno 148 euro 155 euro 170 euro2 anni 275 euro 290 euro 320 euro3 anni 390 euro 410 euro 450 euro
ENTI ESTERO
1 anno 165 euro 175 euro 195 euro2 anni 310 euro 325 euro 365 euro3 anni 425 euro 460 euro 510 euro
PRIVATI ESTERO
1 anno 85 euro 95 euro 115 euro2 anni 160 euro 180 euro 215 euro3 anni 225 euro 250 euro 305 euro
PROMOZIONI 2014■ Per giovani epidemiologi: abbonamento on-line a 45 euro per gli under 30.
■ Per generosi epidemiologi già abbonati a E&P: regala un abbonamento a E&P per il 2014.Costa solo 50 euro per l’edizione on-line e 60 euro per avere anche il cartaceo.Ovviamente, l’abbonamento sarà accompagnato da un biglietto che svelerà l’identità del donatoreper fare una gran bella figura e nello stesso tempo aiutare E&P.
■ Per epidemiologi “contagiosi”: se ti piace E&P e fai sottoscrivere due nuovi abbonamenti a chinon conosce la rivista o non è più abbonato da almeno due anni, il tuo abbonamentoo il tuo rinnovo è gratuito.
EPIDEMIOLOGIA & PREVENZIONE Modalità di abbonamento per il 2014
data ................................................. Abbonamento annuo a partire dal primo numero raggiungibile:
❐ Tipo di abbonamento .............................................................. ❐ euro ..............................................................
Modalità di pagamento:
❐ Versamento: a mezzo conto corrente postale n. 55195440 ❐ PayPal: sul sito www.epiprev.itintestato a Inferenze scarl, via Ricciarelli 29, 20148 Milano(allegare la ricevuta di versamento alla richiesta di abbonamento) ❐ Bonifico bancario: UGF BANCA, piazza Wagner 8, 20145 Milano
IBAN IT 53 P 03127 01600 0000 0000 3681 intestato a Inferenze scarl,via Ricciarelli 29, 20148 Milano (allegare la contabile alla richiesta di abbonamento)
❐ Carta di credito: ❐ American Express ❐ Carta Sì ❐ Master Card ❐ Eurocard ❐ VISA
cognome e nome .............................................................................................................................................................................................................................................
azienda ...........................................................................................................................................................................................................................................................
indirizzo ...........................................................................................................................................................................................................................................................
cap ....................................................... località ............................................................................................................................................................. prov. .....................
tel. ................................................................... fax. ................................................................... e-mail ........................................................................................................
numero _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ scadenza _ _ / _ _ / _ _ firma .......................................................................................................
cod. CV2 _ _ _ (ultime tre cifre stampate sul retro della carta, per una garanzia di sicurezza in più)
Compilare e inviare a Inferenze - via Ricciarelli 29, 20148 Milano; e-mail [email protected] o per fax allo 02 48706089
EPIDEMIOLOGIA& PREVENZIONE